#teen reproductive health
Text
Hello everyone!
I am starting my blog called “twenty one”!
A blog where teenagers and young adults living in the twenty first century can read about experiences that we have collectively gone through!
Whether it’s:
Education
Romance
Finances
Mental Health
Socioeconomic Factors
or Everyday Life
I wanted to have a page where everyone can be heard.
Our generation has gone through so much. School shootings, the uprise of police brutality, COVID-19, inflation, and countless more. This is a world where we can gather our feelings about these topics.
We are all heard!
We are all twenty one!
#blog#teen#teenager#young adult#self help#self healing#outreach#escape#reading#mental#mental help#mental health#dating#relationships#education#socioeconomic#black lives matter#asian lives matter#reproductive care#reproductive health#lgbtq community#lgbtq friendly#twenty one blog
2 notes
·
View notes
Text
Children of Grenada By Humanium.org
Grenada GDP per person is $14,000. Children make up a significant portion of the population; 25% of Grenadan inhabitants are between 0 and 14 years. On average, each woman has a little over two children.

In Their Report:
Children and young people, however, are most affected by extreme poverty where 56 percent of people under 25 live in poverty.
Two main health problems should still persist:
First, hygiene is a concern given that there are few indoor toilets installed. Second, sickle-cell anemia also has become a public health problem.
Adolescents are also the subjects of major health concerns; HIV/ AIDS and sexually transmitted diseases awareness education programs are lacking in Grenada.
Neither condom usage nor hormonal contraception have been widely accepted or used very often. As a result, there are a high number of teenage pregnancies among young mothers, who experience discrimination. Medical responsibility is slowly becoming established, but there is still a blatant lack of existing programs, especially with regards to abortion, mental health, and violence against children.
Children are not always registered when they are born, and may not receive a name until they are baptized, sometimes 3 to 4 months after birth. Birth certificates do not systematically record the father’s name.
#pregnancy#children#grenada#maternal health#reproductive justice#children rights#teen pregnancy#mothers#african diaspora
0 notes
Text
Roe
I woke this morning to sun, and the promise of new beginnings. Then I remembered.
SCOTUS’ opinion yesterday, to allow states to criminalize a woman’s right to choose, settled like a veil around me. How could we let this happen? It turns out there’s an easy answer.
We’ve allowed an illegitimate Supreme Court to bring their extreme religious/originalist interpretation of constitutional law to…

View On WordPress
0 notes
Note
sorry if you've talked about it already, but what is it that makes KOSA's idea of online safety wrong? I don't know much about the bill, what does it intend to do?
What do you think is a good way to protect kids from things like online predators or just seeing things that they shouldn't be seeing? (By which I mean sex and graphic violence, things which you'd need to be 16+ to see in a movie theater so I think it makes sense to not want pre-teens to see it)
From stopkosa.com:
Why is KOSA a bad bill?
KOSA uses two methods to “protect” kids, and both of them are awful.
First, KOSA would incentivize social media platforms to erase content that could be deemed “inappropriate” for minors. The problem is: there is no consensus on what is inappropriate for minors. All across the country we are seeing how lawmakers are attacking young people’s access to gender affirming healthcare, sex education, birth control, and abortion. Online communities and resources that queer and trans youth depend on as lifelines should not be subject to the whims of the most rightwing extremist powers and we shouldn’t give them another tool to harm marginalized communities.
Second, KOSA would ramp up the online surveillance of all internet users by expanding the use of age verification and parental monitoring tools. Not only are these tools needlessly invasive, they’re a massive safety risk for young people who could be trying to escape domestic violence and abuse.
I’ve heard there’s a new version of KOSA. What’s the deal?
The new version of KOSA makes some good changes: narrowing the ability of rightwing attorneys general to weaponize KOSA to target content they don’t like and limiting the problematic “duty of care. However, because the bill is still not content neutral, KOSA still invites the harms that civil rights advocates have warned about.
As LGBTQ and reproductive rights groups have said for months, the fundamental problem with KOSA is that its “duty of care” covers content specific aspects of content recommendation systems, and the new changes fail to address that. In fact, personalized recommendation systems are explicitly listed under the definition of a design feature covered by the duty of care in the new version. This means that a future Federal Trade Commission (FTC) could still use KOSA to pressure platforms into automated filtering of important, but controversial topics like LGBTQ issues and abortion, by claiming that algorithmically recommending such content “causes” mental health outcomes that are covered by the duty of care like anxiety and depression. Bans on inclusive books, abortion, and gender affirming healthcare have been passed on exactly that kind of rhetoric in many states recently. And we know that already existing content filtering systems impact content from marginalized creators exponentially more, resulting in discrimination and censorship.
It’s also important to remember that algorithmic recommendation includes, for example, showing a user a post from a friend that they follow, since most platforms do not show all users all posts, but curate them in some way. As long as KOSA’s duty of care isn’t content neutral, platforms will be likely to react the same way that they did to the broad liability imposed by SESTA/FOSTA: by engaging in aggressive filtering and suppression of important, and in some cases lifesaving, content.
Why it's bad:
The way it's written (even after being changed, which the website also goes over), it is still possible for this law to be used to restrict things like queer content, discussion of reproductive rights and resources, and sexual education.
It will restrict youth's ability to use the Internet independently, essentially cutting off life support to many vulnerable people who rely on the Internet to learn that they are queer, being abused, disabled, etc.
Better alternatives:
Stop relying on ageist ideas of purity and innocence. When we focus on protecting the "purity" of youth, we dehumanize them and it becomes more about soothing adult anxieties than actually improving the lives of children.
Making sure content (sexual, violent, etc.) is marked/tagged and made avoidable for anyone who doesn't want to engage with it.
Teach children why certain things may be upsetting and how best to avoid those things.
Teach children how to recognize grooming and abuse and empower them to stop it themselves.
Teach children how to recognize fear, discomfort, trauma, and how to cope with those experiences.
The Internet makes a great boogeyman. But the idea that it is uniquely corrupting the Pure Innocent Youth relies on the idea that all children are middle-class suburban White kids from otherwise happy homes. What about the children who see police brutality on their front lawns, against their family members? How are we protecting them from being traumatized? Or children who are seeing and experiencing physical and sexual violence in their own homes, by the parents who prevent them from realizing what's happening by restricting their Internet usage? How does strengthening parent's rights stop those kids from being groomed? Or the kids who grow up in evangelical Christian homes and are given graphic descriptions of the horrors of the Apocalypse and told if they ever question their parents, they'll be left behind?
Children live in the same world we do. There are children who are already intimately aware of violence and "adult" topics because of their lived experiences. Actually protecting children means being concerned about THEIR human rights, it means empowering them to save themselves, it means giving them the tools to understand their own feelings and traumas. KOSA is just another in a long line of attempts to "save the children!" by dehumanizing them and giving more power to the people most likely to abuse them. We need to stop trying to protect children's "innocence" and appreciate that children are already growing, changing people, learning to deal with discomfort and pain and the weight of the world the same as everyone else. What people often think keeps kids safe really just keeps them ignorant and quiet.
Another explanation as to why it's bad:
179 notes
·
View notes
Text
"Bria Peacock chose a career in medicine because the Black Georgia native saw the dire health needs in her community — including access to abortion care.
Her commitment to becoming a maternal health care provider was sparked early on when she witnessed the discrimination and judgment leveled against her older sister, who became a mother as a teen. When the Supreme Court overturned Roe v. Wade in 2022, Peacock was already in her residency program in California, and her thoughts turned back to women like her sister.
“I knew that the people — my people, my community back home — was going to be affected in a dramatic way, because they’re in the South and because they’re Black,” she said.
But even though Peacock attended the Medical College of Georgia, she’s doing her obstetrics and gynecology residency at the University of California-San Francisco, where she has gotten comprehensive training in abortion care.
“I knew as a trainee that’s what I needed,” said Peacock, who plans to return to her home state after her residency.
Ever since the Supreme Court decision, California has worked to become a sanctuary for people from states where abortion is restricted. In doing so, it joins 14 other states, including Colorado, New Mexico, and Massachusetts. Now, it’s addressing the fraught issue of abortion training for medical residents, which most doctors believe is crucial to comprehensive OB-GYN training.
A law enacted in September [2023] makes it easier for out-of-state trainees to get up to 90 days of in-person training under the supervision of a California-licensed doctor. The law eliminated the requirement for a training license and also permitted training at programs such as Planned Parenthood that are affiliated with accredited medical schools.
“By allowing physician residents to come to California, where there are more opportunities for abortion training, and by allowing them to be reimbursed for this work, we’re sending a message that abortion care is health care and an essential part of physician training,” said Lisa Folberg, CEO of the California Academy of Family Physicians, which supported the bill.
The question of how to provide complete OB-GYN training promises to become more urgent as the effects of abortion bans on medical education becomes clear: 18 states restrict or ban abortion to the point of effectively stripping 20% of OB-GYN medical residents of the opportunity to get abortion training, according to the Ryan Residency Training Program in Abortion and Family Planning. That’s 1,354 residents this year out of 5,962 OB-GYN residents nationwide.
The restrictions in some cases aim to reach beyond state borders, spooking medical students and residents who fear hostility from anti-abortion groups and right-wing legislators...
Pamela Merritt, executive director of Medical Students for Choice, pointed to a Kansas law that requires repayment of state medical school scholarships — with 15% interest — if residents perform abortions or work in clinics that perform them, except in cases of rape, incest, or a medical emergency.
Doctors point out that abortion training is not just about ending pregnancies. Peacock recalled a patient who started hemorrhaging badly shortly after a healthy delivery. Peacock and her team at UCSF performed a dilation and curettage — a procedure commonly used to terminate pregnancy.
“If we did not have that skill set, and the patient continued to bleed, it could have been life-taking,” said Peacock, chief OB-GYN resident at UCSF...
Peacock, for her part, is adamant about returning to Georgia, where abortions are banned after six weeks. “I’m still going to provide abortions, whether that’s in Georgia or I need to fly to a different state and work in abortion clinics for a week out of the month,” she said. “It would definitely be a big part of my work.”"
-via The 19th, January 2, 2024
#abortion#bodily autonomy#abortion rights#reproductive rights#reproductive justice#united states#us politics#california#georgia#medical student#residency#medical school#healthcare#healthcare access#pro choice#abortion is healthcare#womens rights#trans rights too let's just make that clear#medical training#abortion care#abortion bans#abortion access#doctors#medicine#gynecology#obstetrician#obstetrics and gynecology#gynecologist#good news#hope
179 notes
·
View notes
Note
Day 6 of asking for transfem steph headcanons.
My headcanon is that Stephanie Brown is a trans woman I honestly don't know what else there is to say I'm really bad at this sort of stuff um I think it's funny to think about how gotham must have really good trans health care considering steph was able to be a teen mum either that or she got someone to magic her a whole female reproduction system only to forget she should be taking birth control now and accidentally getting pregnant
#ask#anon#you have been doing this for 6 days so i applaud you for that#but like#im really bad at headcanons#Escpically when it comes to the smaller stuff#like i hc steph dick and cass as trans#but theres this one really nice anon who keeps asking me for trans cass#and im just like what?#thats just regular cass#i dont understand#please help
62 notes
·
View notes
Note
Headcanons for omega kankuro, hidan, and omega asuma plzzzzz
(I don't write for Hidan or Asuma, but I can give you some omega!Kankuro headcanons for sure!)
GENERAL OMEGA!KANKURO HEADCANONS
(There's some n-sfw at the end :D)

Kankuro didn't really think about nor care about his secondary gender when he was young.
As far as he was concerned, his secondary gender was puppets and trying to avoid getting murdered by baby Gaara.
Once he's approaching chunin, he does kind of feel grateful that he's an omega because his shitty father was an alpha and Kankuro looks a lot like him. It's helpful to have a layer of separation with different secondary genders.
When he's an older teen/young adult is the first time he starts feeling uncomfortable with being an omega. He just feels wrong and it stresses him out a lot for a while until he figures out what's wrong.
Basically, Kankuro is super not okay with the idea of being pregnant, it really freaks him out, he feels like he wouldn't be 'him' if it happened, so having a functioning reproductive system was affecting his mental health.
Once he yeets the womb, he's back to being very chill about being an omega once more.
No pups for him, he lowkey hates children. (But he's the weird chill uncle for Gaara and Temari's pups though, family is important to him.)
However he will only babysit very young pups in an emergency.
...
When Kankuro gets married to you, he takes advantage of social convention and retires from active duty. He likes to call himself a house husband.
He is not really a house husband though because he spends all his time in his workshop, working on his puppets.
((n-sfw warning for this bullet point) one of his puppets is a sex puppet he based on you from before you got together because Kankuro is kind of a freak ngl) but I digress.
He also helps out Gaara when he can, and he might take on an apprentice if he can find a child who's good enough for him to mentor.
So yeah, he's not a traditional house husband, which is good because he lacks several of the key skills, like cooking. He can make some of the best sandwiches you've ever had in your life though. Sandwich king!
...
Omega!Kankuro's scent is very herb-like, like rosemary.
He almost never whines. He hates omega whines, thinks they're so annoying and insipid, so whenever he feels the urge, he gets irritated, which turns the would-be-whine into a growl lol.
He's not really a nesting guy. Until he's sick that is. Then he needs a nest so bad it hurts.
He always ends up building the nest while he's sick though, because he's the sort of person who denies being sick when he first starts to feel the symptoms.
His nests when he's sick is always in the coolest part of the house, even if that ends up being the bathroom or something. This is so he can pile blankets on himself without getting heat stroke.
Sometimes he has cooling packs, heat packs and blankets on all at the same time, it makes no sense, but he gets very grumpy and upset if he can't have them all.
He needs cooling packs on his neck, feet, and in between his legs, and then hot water bottles on his stomach and chest, then a pile of blankets on top keeping everything in place.
Just imagine that, but also Kankuro is laying in the bath tub and his grumpy little flushed face, free of face paint, is sticking out from all the blankets haha. So cute.
some n-sfw hcs
Kankuro is into somnophilia, but not on him. He wants to have his way with his alpha while they're asleep.
He 'jokes' about introducing puppets into the bedroom a bit too often. If you ever give him permission, he'll drag entire boxes into the room, filled with stuff he prepared but was too awkward to bring up himself.
On a similar note, he's a big fan of toys. Especially those that vibrate.
He's an evening sex guy. Comes with living in the desert.
He's kind of a voyeur too. He likes to perve.
His hard nos include anything associated with pregnancy, like breeding, lactation etc. and also he only ever spits if he gets a mouth full of cum.
Man, I don't talk about Kankuro enough! I love this asshole 🥺
237 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
On Tuesday, Gov. Janet Mills of Maine signed LD 227, a sanctuary bill that protects transgender and abortion providers and patients from out-of-state prosecution, into law. With this action, Maine becomes the 16th state to explicitly protect transgender and abortion care in state law from prosecution. This follows several bomb threats targeting state legislators after social media attacks from far-right anti-trans influencers such as Riley Gaines and Chaya Raichik of Libs of TikTok. An earlier version of the bill failed in committee after similar attacks in January. Undeterred, Democrats reconvened and added additional protections to the bill before it was passed into law.
The law is extensive. It asserts that gender-affirming care and reproductive health care are "legal rights" in Maine. It states that criminal and civil actions against providers and patients are not enforceable if the provision or access to that care occurred within Maine’s borders, asserting jurisdiction over those matters. It bars cooperation with out-of-state subpoenas and arrest warrants for gender-affirming care and abortion that happen within the state. It even protects doctors who provide gender-affirming care and abortion from certain adverse actions by medical boards, malpractice insurance, and other regulating entities, shielding those providers from attempts to economically harm them through out-of-state legislation designed to dissuade them from providing care.
The bill also explicitly enshrines the World Professional Association of Transgender Health’s Standards of Care, which have been the target of right-wing disinformation campaigns, into state law for the coverage of transgender healthcare.
The bill is said to be necessary due to attempts to prosecute doctors and seek information from patients across state lines. In recent months, attorneys general in other states have attempted to obtain health care data on transgender patients who traveled to obtain care. According to the United States Senate Finance Committee, attorneys general in Tennessee, Indiana, Missouri, and Texas attempted to obtain detailed medical records "to terrorize transgender teens in their states… opening the door to criminalizing women’s private reproductive health care choices."
The most blatant of these attempts was from the Attorney General of Texas, who, according to the Senate Finance Committee, "sent demands to at least two non-Texas entities."
[...]
Despite these threats, legislators strengthened both the abortion and gender-affirming care provisions and pressed forward, passing the bill into law. Provisions found in the new bill include protecting people who "aid and assist" gender-affirming care and abortion, protections against court orders from other states for care obtained in Maine, and even protections against adverse actions by health insurance and malpractice insurance providers, which have been recent targets of out-of-state legislation aimed at financially discouraging doctors from providing gender-affirming care and abortion care even in states where it is legal.
Maine Gov. Janet Mills (D) signs gender-affirming care and abortion sanctuary state bill LD227 into law despite the best efforts of right-wing anti-trans extremists such as Riley Gaines, Courage Is A Habit, and Libs of TikTok who sought to thwart its passage and signature into law.
#Maine LD227#Maine#Janet Mills#Transgender Safe Refuge#Transgender Sanctuary State#Abortion Sanctuary State#Abortion#Gender Affirming Healthcare#LGBTQ+#Transgender Health#Transgender#WPATH
27 notes
·
View notes
Note
hi sex witch! hope you're well.
I have a question about unsafe sex toys and what they can do to my body, since when I was in my early teens I started using assorted plastic objects to masturbate and it only recently occurred to me that inserting not-bodysafe plastics into some of the most sensitive parts of my body could be bad for me. I'm now in my twenties and have stopped doing that, but my worries still linger. what are some of the effects of longterm use of not-bodysafe plastic 'sex toys'? and where can I read more about them without unnecessary fear mongering?
hi anon,
the issue with sex toys made of materials like jelly rubber and polyvinyl chloride (PVC) is that they're liable to bleed off phthalates and microplastics, which will be absorbed quickly through the sensitive mucus membranes of your various orifices.
per the National Library of Medicine:
Phthalates are a series of widely used chemicals that demonstrate to be endocrine disruptors and are detrimental to human health. Phthalates can be found in most products that have contact with plastics during producing, packaging, or delivering. Despite the short half-lives in tissues, chronic exposure to phthalates will adversely influence the endocrine system and functioning of multiple organs, which has negative long-term impacts on the success of pregnancy, child growth and development, and reproductive systems in both young children and adolescents.
similarly, microplastics can also disrupt endocrine processes and contribute to certain cancers and reproductive problems (x).
which isn't to say that you're doomed and guaranteed to have cancer and a rancid reproductive system, just that it's a good thing you've stopped using things made of suspect materials because that's risk reduction, babey! putting less toxins in your body is always a good idea.
there are of course other, immediately reasons that jelly and PVC aren't recommended for use as sex toys, namely that they're prone to degrading and also porous, which makes them impossible to thoroughly clean to the point that they can grow straight-up mold.
again, I cannot emphasize enough that there is no reason to be immediately afraid of any ill effects befalling your body, especially if you're not currently experiencing any complications that you can trace back to suspect sex toy use. I'd recommend instead reading up on safer sex toy practices with resources like Dangerous Lilly's guide to sex toy toxicity, to help make more informed decisions about future toys:
42 notes
·
View notes
Note
sitting here politely waiting for the heat/rut explanations (i saw omegaverse and was summoned)

Great! We start with the Heat / Rut lesson! 🙏🏻✨
Heat is the stage where the omega is most fertile, is the reproduction time! First I will explain the Heat in young omegas! The first heat of an omega comes at the beginning of his adolescence. In the first years they will not have any sexual needs, that will come when their body is developed enough to have babies, maybe between 16-17 years old? (So no, don't worry, 11 or 12 year old omegas won't be horny!) the heat cause painful stomach cramps, they can also cause fever, muscle pain and nausea. The omegas have a pre-heat stage where they begin to feel mood swings and irritability, they begin to nesting, they collect pillows, cushions, blankets and soft and fluffy things to make their nests (Nests can be anywhere! Normally in the omega's room, but don't be surprised to discover a nest in the bathroom made of towels and a bathrobe) to soothe the pain, the young omega can comfort himself with the smell of their family or friends, even if they have a boyfriend they will steal their clothes to add it to the nest!
Now, the mature omega! Apart from the pain, the excitement is added! The pain and excitement disappear once the sexual act has been practiced with a partner, they can also masturbate if they don't have anyone to have sex with BUT it is advisable to have someone, since during a "heat wave" the omega will be so excited that they could act incoherently and neglect their health, the partner must ensure the rest, food and hydration!
During the pre-heat, the most adult omegas that already have their body developed for babies, will experience a slight swelling in the lower part of the belly and the breasts, these will be sensitive and sore. They also make nests and will steal their lover's clothes, during the heat the risk of pregnancy is very big! It is recommended to use protection, toys or the skills of their partners, but there is nothing better than a good dick inside them LOL.
Omegas during the heat will smell much sweeter to attract potential mates! For example, if Venti smells like Cecilias and apples, in his heat it will be as if you have added honey to that mixture, or they have roasted the apples with sugar, lol!
For now I think that's it!
Now let's go with the rut! Although the rut is also like a mating phase, it is not as related to the sexual act as it is in the heat.
Young alphas experience their first rut early in their teens! The rut is very short, it may only last between 1 and 2 days! While the heat lasts between 3 and 7 days depending on the omega and if you have a partner to satisfy yourself or not. I also think that once the couple is united (mate bite) their heats and ruts are shorter and softer.
So! The alpha can also make nests where they are safe and comfortable, but it is difficult for them to stay still! In the rut, the alpha can suffer a fever and be unwell, but above all it is something more mental and they will be restless and even paranoid, the alphas are usually very territorial so if someone enters their safe space they will become aggressive, they prefer the closed and small spaces at these times, they will be eager for open windows, fearful that another alpha might walk in and invade their comfort zone.
A mature alpha will only be even more aggressive and protective! Whether with family and friends or with a partner, often the alpha will make sure their mate is safe, they may put them in the nest and not let them out (I have a headcanon where my alphas catch their omega and puts them in a nest in the closet or in a small room where they are safe, lol it's ridiculous) if the partner is pregnant the alpha will be on the brink of panic if they can see them near danger (stairs, sharp furniture, slipping) the partner should making sure the alpha is eating and staying cool and hydrated, sexual act is very very helpful to calm them down!! But it is not something necessary, the partner can talk to them calmly and make sure that nothing bad will happen.
An alpha in rut is not recommended to spend time with another alpha, the slightest movement will tense or bother and could attack! (alpha relationships are more complicated)
Sometimes the alpha if is very stressed will go into a primitive state where it will be difficult for them to communicate with words, would it be something like a wild side? At this point you have to be careful dealing with them!
Cold showers help too lol!
I think, that's all about the Heat/Rut for the moment, thanks for reading! Don't hesitate to ask me for more! I LOVE the omegaverse so much ✨
105 notes
·
View notes
Photo
sumbacky
See sumbacky’s existing works here and here.
Preferred contact methods:
Email: [email protected]
Twitter: bunetties
Tumblr: sumbacky
Preferred organizations:
- Center for Reproductive Rights
- Clean Air Task Force
- International Rescue Committee
- Partners In Health
- Rape, Abuse, and Incest National Network (RAINN)
(See the list of approved organizations here)
Will create works that contain:
Fluff, romance, mild nsfw/smut, AUs, character interactions, animals, canon-compliant
Will not create works that contain:
Heavy angst, dark themes, mecha, difficult/complex backgrounds, gore, omegaverse, kids
-- Art --
Auction ID: 1004
Will create works for the following relationships:
Bucky Barnes/Sam Wilson - MCU
Joaquín Torres/Sam Wilson - MCU
Miles Morales/Gwen Stacy - Spider-Verse (animated films)
Yelena Belova/Kate Bishop - MCU
Hobie Brown & Miles Morales & Pavitr Prabhakar & Gwen Stacy - Spider-Verse (animated films)
Thor-centric - MCU
Sam Wilson-centric - MCU
Yelena Belova-centric - MCU
Work Description:
I’m offering one digital illustration of the characters listed (up to two and will ONLY draw four characters if it's those Spiderverse characters). The file will be a high resolution png and will be sent via email. The winning bid will receive a digital artwork according to the tiers below:
$10-20: Half-body (B&W/single block colour)
$20-30: Full-body (B&W/single block colour)
$30-40: Half-body (full colour)
$40-50: Half-body (full colour) + detailed background
$50+: Full body (full colour) + detailed background
The $10-$40 tiers will have a simple background with little detail, the focus being on the characters. I prefer that you provide me visual or detailed descriptions of your piece. If the scene you'd like me to draw is from a fic, please send me the link of the fic - I'm more than happy to read the whole fic to get a grasp of the story/vibes to encapsulate that one scene for you.
Ratings: Gen, Teen, Mature
Can pods bid on this auction? Yes - Podbids welcome!
CLICK HERE TO BID ON THIS WORK
The auction runs from October 22 (12 AM ET) to October 28 (11:59:59 PM ET). Visit marveltrumpshate.com during Auction Week to view all of our auctions and to place your bids!
30 notes
·
View notes
Text
Information on Testosterone Hormone Therapy:
As you prepare to begin treatment, now is a great time to think through what your goals are, as the approach to hormone therapy is definitely not one-size-fits-all.
Do you want to get started right away on a path to the maximum safe effects? Or, do you want to begin at a lower dose and allow things to progress more slowly? Perhaps your long term goal is to seek less-than-maximal effects and you would like to remain on a low dose for the long term. Thinking about your goals will help you communicate more effectively with your medical provider (an endocrinologist is the best way) as you work together to map out your care plan.
Many people are eager for hormonal changes to take place rapidly- understandably so. But it's very important to remember that the extent of, and rate at which your changes take place, depend on many factors. These factors include your genetics, the age at which you start taking hormones, and your overall state of health.
Consider the effects of hormone therapy as a second puberty, and puberty normally takes years for the full effects to be seen. Taking higher doses of hormones will not necessarily bring about faster changes, but it could endanger your health. And because everyone is different, your medicines or dosages may vary widely from those of your friends, or what you may have read in books or in online forums. Use caution when reading about hormone regimens that promise specific, rapid, or drastic effects. While it is possible to make adjustments in medications and dosing to achieve certain specific goals, in large part the way your body changes in response to hormones is more dependent on genetics and the age at which you start, rather than the specific dose, route, frequency, or types of medications you are taking.
While I will speak about the approach to hormone therapy in transgender men, my comments are also applicable to non-binary people who were assigned female at birth and are seeking masculinizing hormone therapy.
There are four areas where you can expect changes to occur as your hormone therapy progresses: Physical, emotional, sexual, and reproductive.
Physical
The first physical changes you will probably notice are that your skin will become a bit thicker and more oily. Your pores will become larger and there will be more oil production. You’ll also notice that the odors of your sweat and urine will change and that you may sweat more overall. You may develop acne, which in some cases can be bothersome or severe, but usually can be managed with good skin care practices and common acne treatments. Some people may require prescription medications to manage acne, please discuss this with your provider. Generally, acne severity peaks during the first year of treatment, and then gradually improves. Acne may be minimized by using an appropriate dosing of testosterone that avoids excessively high levels.
Your chest will not change much in response to testosterone therapy. That said, surgeons often recommend waiting at least 6-12 months after the start of testosterone therapy before having masculinizing chest surgery, otherwise known as top surgery, in order to first allow the contours of the muscles and soft tissues of your chest wall to settle in to their new pattern.
Your body will begin to redistribute your weight. Fat will diminish somewhat around your hips and thighs. Your arms and legs will develop more muscle definition, with more prominent veins and a slightly rougher appearance, as the fat just beneath the skin becomes a bit thinner. You may also gain fat around your abdomen.
Your eyes and face will begin to develop a more angular, male appearance as facial fat decreases and shifts. Please note that it’s not likely your bone structure will change, though some people in their late teens or early twenties may see some subtle bone changes. It may take 2 or more years to see the final result of the facial changes.
Your muscle mass will increase, as will your strength, although this will depend on a variety of factors including diet and exercise. Overall, you may gain or lose weight once you begin hormone therapy, depending on your diet, lifestyle, genetics and muscle mass.
Testosterone will cause a thickening of the vocal chords, which will result in a more male-sounding voice. Not all trans men will experience a full deepening of the pitch of their voice with testosterone, however. Some may find that practicing various vocal techniques or working with a speech therapist may help them develop a voice that feels more comfortable and fitting. Voice changes may begin within just a few weeks of beginning testosterone, first with a scratchy sensation in the throat or feeling like you are hoarse. Next your voice may break a bit as it finds its new tone and quality.
The hair on your body, including your chest, back and arms will increase in thickness, become darker and will grow at a faster rate. You may expect to develop a pattern of body hair similar to other men in your family—just remember, though, that everyone is different and it can take 5 or more years to see the final results.
Regarding the hair on your head: most trans men notice some degree of frontal scalp hair thinning, especially in the area of your temples. Depending on your age and family history, you may develop thinning hair, male pattern baldness or even complete hair loss. Approaches to managing hair loss in trans men is the same as with cisgender men; treatments can include the partial testosterone blocker finasteride, minoxidil, which is also known as Rogaine, applied to the scalp, and hair transplantation. As with cis men, unfortunately there is no way to completely prevent male pattern baldness in those predisposed to develop this condition. Ask your provider for more information on strategies for managing hair loss.
Regarding facial hair, beards vary from person to person. Some people develop a thick beard quite rapidly, others take several years, while some never develop a full, thick beard. Just as with cisgender men, trans men may have varying degrees of facial hair thickness and develop it at varying ages. Those who start testosterone later in life may experience less overall facial hair development than those who start at younger ages.
Lastly, you may notice changes in your perception of the senses. For example, when you touch things, they may “feel different” and you may perceive pain and temperature differently. Your tastes in foods or scents may change.
Emotional state changes
The second area of impact of hormone therapy is on your emotional state.
Puberty is a roller coaster of emotions and the second puberty that you will experience during your transition is no exception. You may find that you have access to a narrower range of emotions or feelings, or have different interests, tastes or pastimes, or behave differently in relationships with other people. For most people, things usually settle down after a period time. Some people experience little or no change in their emotional state. I encourage you to take the time to learn new things about yourself, and sit with new or unfamiliar feelings and emotions while you explore and familiarize yourself with them. While psychotherapy is not for everyone, many people find that working with a therapist while in transition can help you to explore these new thoughts and feelings, get to know your new body and self, and help you with things like coming out to family, friends, or coworkers, and developing a greater level of self-love and acceptance.
Sexual changes
The third area of impact of hormone therapy is on your sexuality
Soon after beginning hormone treatment, you will likely notice a change in your libido. Quite rapidly, your genitals, especially your clitoris, will begin to grow and become even larger when you are aroused. You may find that different sex acts or different parts of your body bring you erotic pleasure. Your orgasms will feel different, with perhaps more peak intensity and a greater focus on your genitals rather than a whole body experience. Some people find that their sexual interests, attractions, or orientation may change when taking testosterone; it is best to explore these new feelings rather than keep them bottled up.
Don’t be afraid to explore and experiment with your new sexuality through masturbation and with sex toys. If you have a sex partner or partners, involve them in your explorations..
Reproductive system changes
The fourth area of impact of hormone therapy is on the reproductive system.
You may notice at first that your periods become lighter, arrive later, or are shorter in duration, though some may notice heavier or longer lasting periods for a few cycles before they stop altogether.
Testosterone may reduce your ability to become pregnant but it does not completely eliminate the risk of pregnancy. Transgender men can become pregnant while on testosterone, so if you remain sexually active with someone who is capable of producing sperm, you should always use a method of birth control to prevent unwanted pregnancy. Transgender men may use any form of contraception, including the numerous options available that do not contain estrogen, and some that contain no hormones at all. There are many contraception options that are long acting and do not require taking a daily pill. Transgender men may also use emergency contraception, also known as the “morning after pill”. Ask your medical provider for more information on the contraceptive and family planning options available to you.
If you suspect you may have become pregnant or have a positive pregnancy test while taking testosterone, speak with you provider as soon as possible, as testosterone can endanger the fetus.
If you do want to have a pregnancy, you’ll have to stop testosterone treatment and wait until your provider tells you that it’s okay to begin trying to conceive.
It’s also important to know that, depending on how long you’ve been on testosterone therapy, it may become difficult for your ovaries to release eggs, and you may need to consult with a fertility specialist and use special medications or techniques, such as in vitro fertilization, to become pregnant. These treatments are not always covered by insurance, and can be expensive. Uncommonly, testosterone therapy may cause you to completely lose the ability to create fertile eggs or become pregnant.
Risks
While cisgender men do have higher rates of cholesterol related disorders and heart disease than cisgender women, the available research on transgender men taking testosterone has generally not found these differences. Most of the research on risk of heart disease and strokes in transgender men suggests that risk does not increase once testosterone is begun. However, longer term, definitive studies are lacking. It has been suggested that the risk of other conditions such as diabetes or being overweight is increased by masculinizing testosterone therapy, however actual research supporting these claims are limited.
One known risk is that testosterone can make your blood become too thick, otherwise known as a high hematocrit count, which can cause a stroke, heart attack or other conditions. This can be a particular problem if you are taking a dose that is too high for your body’s metabolism. This can be prevented by maintaining an appropriate dose and through blood tests to monitor blood and hormone levels.
While available data are limited, it does not appear that testosterone increases the risk of cancer to the uterus, ovaries, or breasts. Because not all breast tissue is removed during masculinizing chest surgery, otherwise known as top surgery, there is a theoretical risk that breast cancer could develop in the remaining tissue. However, it can be difficult to screen for breast cancer in this tissue, and there are risks of a false positive test result. Your provider can give you more information about breast cancer screening after top surgery.
Cervical cancer is caused by an infection with the human papillomavirus, or HPV. HPV is transmitted sexually, more commonly by having sexual contact with someone who has a penis. However, people who have never had sexual contact with a penis may still contract an HPV infection. The HPV vaccine can greatly reduce your risk of cervical cancer, and you may want to discuss this with your provider. Pap smears are used to detect cervical cancer or precancer conditions, as well as an HPV infection. Your provider will make a recommendation as to how often you should have a pap smear. It is unclear if testosterone therapy plays any role in HPV infection or cervical cancer.
If your periods have stopped because of testosterone treatment, be sure to report any return of bleeding or spotting to your provider, who may request an ultrasound or other tests to be certain the bleeding isn’t a symptom of an imbalance of the lining of the uterus. Sometimes such an imbalance could lead to a precancerous condition, although this is rare in transgender men. Missing a dose or changing your dose can sometimes result in return of bleeding or spotting. Some men may experience a return of spotting or heavier bleeding after months or even years of testosterone treatment. In most cases this represents changes in the body’s metabolism over time. To be safe, always discuss any new or changes to bleeding patterns with your doctor.
Fortunately, since you do not have a prostate, you have no risk of prostate cancer and there is no need to screen for this condition.
If you have had your ovaries removed, it is important to remain on at least a low dose of hormones post-op until at minimum age 50. This will help prevent a weakening of the bones, otherwise known as osteoporosis, , which can result in serious and disabling bone fractures.
Most people using masculinizing testosterone therapy will experience at least a small amount of acne. Some may experience more advanced acne. Often this acne responds to typical over-the-counter treatments, but in some cases prescription medication may be required. Acne usually peaks within the first year of treatment and then begins to improve.
While gender affirming hormone therapy usually results in an improvement in mood, some people may experience mood swings or a worsening of anxiety, depression, or other mental health conditions as a result of the shifts associated with starting a second puberty. If you have any mental health conditions it is recommended you remain in discussion with a mental health providers as you begin hormone therapy.
Other medical conditions may be impacted by gender affirming hormone therapy, though research is lacking. These include autoimmune conditions, which can sometimes improve or worsen with hormone shifts, and migraines, which often have a hormonal component. Ask your medical provider if you have further questions about the risks, health monitoring needs, and other long term considerations when taking hormone therapy.
Some of the effects of hormone therapy are reversible, if you stop taking them. The degree to which they can be reversed depends on how long you have been taking testosterone. Clitoral growth, facial hair growth, voice changes and male-pattern baldness are not reversible.
Testosterone treatment approaches
Testosterone comes in several forms. Injections are usually best given weekly to maintain even levels of testosterone in the blood. Studies have shown that using a smaller needle and injection by the subcutaneous, or under the skin, approach, is just as effective as the intramuscular approach, which involves a larger needle injecting deeper into the muscle. In addition to injections, there are gel and patches that can be applied to the skin daily. The gel is applied to skin and once dry, you can swim, shower, and have contact with others. The patch also allows swimming, showering, exercise, and contact with others. All of these forms work equally well when the dosing is adjusted to achieve the desired hormone levels, and the decision about which form to use should be based mostly on your preference.
Another option for testosterone is the use of pellets under the skin. These are inserted every few months via a minor in-office procedure. Ask your medical provider for more information about this approach.
Recently, an oral form of testosterone, taken as a pill twice daily, has been approved for use. There are potential risks of high blood pressure when taking this medication, so extra steps need to be taken to monitor your health if you choose to use this form of your testosterone. Ask your medical provider for more information about this approach.
Regardless of the type of testosterone you are taking, it’s important to know that taking more testosterone will not make your changes progress more quickly, but could cause serious side effects or complications. Excess testosterone can result in mood symptoms or irritability, bloating, pelvic cramping, or even a return of menstruation. High levels of testosterone also result in increased estrogen levels, as a percentage of all testosterone in the body is converted to estrogen. In general estrogen blocking medicines are not used as a part of masculinizing hormone therapy.
Other medications that may be used include progestagens, which are hormones similar to or identical to those made by the body to maintain a balance in the lining of the uterus. These hormones can be used in cases where periods continue after testosterone levels have been optimized. These hormones can cause mood swings, bloating, and other side effects, so it is recommended that you discuss these medications further with you provider if they are to be used.
Final thoughts
And finally, please remember that all of the changes associated with the puberty you’re about to experience can take years to develop. Starting hormone therapy in your 40s, 50s, or beyond may bring less drastic changes than one might see when beginning transition at a younger age, due to the accumulated lifetime exposure to estrogen, and declining responsiveness to hormone effects as one approaches the age of menopause. Once you have achieved male-range testosterone levels, taking higher doses won’t result in faster or more dramatic changes, however they can result in more side effects or complications.
Now that you have learned about the effects of masculinizing hormone therapy, as well as risks and specific medication options, the next step will be to speak with your provider about what approach is best for you.
Source
#hormone therapy#testosterone#testosterone risks#testosterone educational post#transgender#trans ftm#transman#transmasc#ftm transition#ask me things#phalloplasty blog#metoidioplasty blog#ftm top surgery blog#ftm educational blog#ftm education
52 notes
·
View notes
Text
Project 2025 and how they're going to strip healthcare from everyone
I know everyone is focused on Gaza. The genocide happening there is unconscionable.
But, back here, in the States, where most of us live, there's this. This is the plan starting January 1. This is just ONE section - Health and Human Services.
I'm currently involved in a grassroots project to present the entirety of the 923 pages in this form to get the information out. Their plan is literally Gilead.
I want to be clear that nowhere in their policies, goals and rhetoric does it account for what happens to all of us when these things happen.
Summary
Scary vague thing:
Investigate, expose, and remediate any instances in which HHS violated people’s rights by:
Colluding with Big Tech to censor dissenting opinions during COVID
Colluding with abortion advocates and LGBT advocates to violate conscience-protection laws and the Hyde Amendment
P. 488
Public health entities (CDC, NIH, ACL, OASH)
Can’t prescribe any behavior (meaning masking/quarantine would never have happened) (454)
Can’t use fetal cells for research (454, 461)
No mask/vaccine mandates in hospitals (475)
LGBTQ
CDC - No data collection on gender identity (456)
Medicare - No national coverage determination for Gender Reassignment Surgery (474)
Allow discrimination
in healthcare
Reverse ACA’s prohibition on discrimination against gender identity and sexual orientation in health programs/activities (475)
Withdraw Ryan White guidance (aims at reducing barriers to HIV care, medication, and support for transgender people living with HIV) (485)
OASH will withdraw support for gender-affirming care (490)
Allow LGBTQ folks to be discriminated against in healthcare (remove Biden protections - 495) and intend to have the DOJ bring the discrimination protections to the supreme court (496) which could potentially set a precedent.
In adoption (477)
Possibly take children away from LGBTQ couples if they didn’t conceive them? “married men and women are the ideal, natural family structure because all children have a right to be raised by the men and women who conceived them” (489)
Prioritize faith-based education programs & grants (that don’t acknowledge LGBTQ folks’ existence) (480, 481)
Reproductive rights
Programs/education
CDC - Implies the Division of Reproductive Health and the 6|18 initiative will be cut (454)
Fewer doctors trained in abortions - Make abortion training opt-in rather than opt-out in all medical schools (485)
No “approved curriculum” or “evidence-based lists” in Teen Pregnancy Prevention or Personal Responsibility Education Programs (477)
Deal with STDs and unwanted pregnancy by focusing on abstinence and strengthening marriage (490)
Remove the experts - Install pro-life advocates in the Health Resources & Services Administration advisory committee (who makes the mandates around abortion) and cut ties with American College of Obstetricians and Gynecologists (484)
eliminate the HHS Reproductive Healthcare Access Task Force and install a pro-life task force (489)
Foreign aid - Require foreign non-government orgs to certify that they wouldn’t perform/promote abortion as a condition of receiving funding. (493)
Protections
Remove protections from the woman and enforce protections for born-alive infants (including criminal consequences) (474)
Make it harder for people to understand how/where their protected health information is protected (rescind guidance - 497)
Drug/contraception access
FDA - Reverse approval of chemical abortion drugs (458)
Limit pills to 49 days gestation, in-person dispensing, report all adverse events (459)
Reduce access to contraception - Allow insurance providers to morally object to providing contraception on nonreligious grounds (it’s already allowed for religious grounds) (483)
Male condoms will no longer be mandated coverage (485)
No more Ella (week-after-pill) in the contraceptive mandate (485)
Make access harder - Withdraw OCR’s pharmacy abortion mandate guidance which prohibits discrimination when providing abortion meds (496)
Travel
Prohibit abortion travel funding (eliminate the section 1115 waivers that allow funds to help cross state lines) (471)
No abortions for refugees (478)
Government funds
No funds for Planned Parenthood (471)
prohibit family planning grants from going to entities that perform abortions or provide funding to other entities that perform abortions (491)
Cut up to 10% of medicaid funds from states that require abortion insurance coverage (CA, IL, Maine, MD, NY, OR, WA, Vermont, Hawaii, Connecticut) (472)
Oversight
Track every abortion in every state (455)
New mission statement “furthering the health and well-being of all Americans ‘from conception to natural death.’” (489)
Require health care workers to report abortion pill complications (459)
Medicare
Use AI to detect fraud (463)
Lots of regulations impacting healthcare system reporting/fund-access/insurance pool etc.
Would be good to get someone in healthcare to analyze, I’m betting these gut the ACA
“Separate the subsidized ACA exchange market from the nonsubsidized insurance market” (469)
Eliminated programs
Medicare Shared Savings Program (465)
Inflation Reduction Act (465)
Medicaid
Add work requirements and lifetime caps (468)
Eliminate benefit requirements/mandates and middle/upper income recipients (468)
Cut up to 10% of medicaid funds from states that require abortion insurance coverage (CA, IL, Maine, MD, NY, OR, WA, Vermont, Hawaii, Connecticut) (472)
Child/family welfare (some overlap with lgbtq, copied in here)
Combine child support with visitation support court (implied via example, 479)
Prioritize faith-based HMRE (healthy marriage & relationship education) programs & grants and don’t pressure them to conform to “nonreligious definitions of marriage” (480, 481)
“in cases where the father or mother does not make a sincere or serious effort to be involved in the child’s upbringing, termination of parental rights for children in foster care should be swift” (482)
Eliminate the Head Start program (482)
Potentially (implied) cut programs related to bullying prevention, children’s safety, health disparities, early childhood support, poisoning and SUID prevention. (486)
Take children away from LGBTQ couples if they didn’t conceive them? “married men and women are the ideal, natural family structure because all children have a right to be raised by the men and women who conceived them” (489)
Housing
“Rescind legal analysis that authorized HHS to impose a moratorium on rental evictions during COVID” (492)
8 notes
·
View notes
Text
Dear English doctors - Biological males can’t get pregnant and there is no such thing as a “girl penis”. Please spend less time on worrying about language that appeases narcissistic men and more time improving care for women and babies.
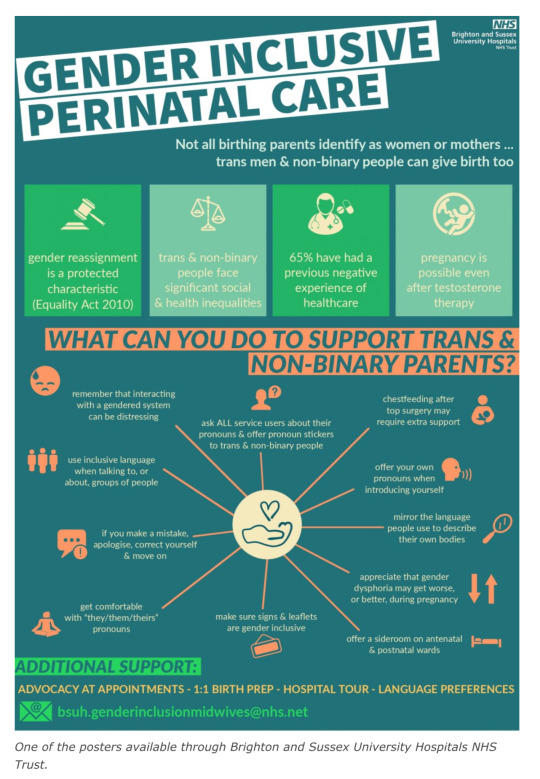
England’s National Health Service (NHS) has put forward a £100,000 contract to create a “gender-inclusive” maternity care training program based on research guided by a trans-identified male who has claimed that men can give birth and that “pre-operative trans women” have “girl penises.”
On December 16, the NHS quietly released an Invitation to Quote for the “Maternity Gender Inclusion Program,” with a listed closing date for pilot submissions set for January 11th, 2023.
The contracted program is set to be rolled out to midwives in maternity departments across 40 NHS Trusts in England, and would be based on the findings of the Improving Trans Experiences of Maternity Services (ITEMS) research project, which was co-authored by a trans-identified male and is alleged to have “significant” flaws in its methodology.
With Woman, a maternity care advocacy coalition, penned an open letter highlighting the “flawed” research within the ITEMS publications, and has called for a complete pause on the contract offering entirely.
Speaking with Reduxx, a spokeswoman from With Woman raised multiple concerns, especially with the entirety of the program’s focus appearing to be on “inclusive” language and not improvements in medical care for a traditionally complex cohort.
With Woman noted that even the Invitation to Quote appears fixed, with the very short contracting and funding window raising suspicion. With Woman indicated their belief that there may be organizations already lined up to take the contract as the time frames are too brief for uninvolved organizations to adequately prepare a pilot.
The ITEMS report, which is being used as a justification for the need for the program, based its findings on the responses of just 121 people. The report determined that “birthing people” were improperly cared for because they were “misgendered,” and made unsubstantiated claims that 30% of “trans parents” secretly gave birth at home with no medical intervention.

The report was co-authored by Dr. Ruth Pearce, a trans-identified male Lecturer in Community Development at Glasgow University.
Pearce played a significant role in the direction of the ITEMS research. Pearce’s work focuses on “trans pregnancy” and “Queer, Trans and Feminist music scenes.”
In an essay posted on to his website, Pearce asserts that he is more attractive and confident than biological women.
“Quite frankly, I bet a whole load of women would love to be as confident and good looking as I am. I’ve got a pretty face, great hair, fantastic legs, and I’ve recently grown some rather shapely breasts.” He is also known for having once fronted a “queer feminist rage” music group through which he sang a song about his scrotum.
In an August 2022 video titled “Reproductive Justice for Trans People With Ruth Pearce and Francis White,” Pearce explains the focus of his work on ITEMS, policy and language surrounding “trans birth” and the need to highlight transgender people having children to counter the claims that a “trans child” may not reproduce, and to create media that contradicts Abigail Shrier’s claims that child transition can lead to “irreversible damage” of fertility.
Pearce called attention in particular to a phenomenon known as Rapid Onset Gender Dysphoria, which was coined by Lisa Littman and referenced by Jungian analyst and author Lisa Marchiano in a 2017 academic article titled “Outbreak: On Transgender Teens and Psychic Epidemics.”
In the article, Marchiano examines the role of social media in the sudden rise in teens claiming a gender identity, stating: “a young person’s coming out as transgender is often preceded by increased social media use and/or having one or more peers also come out as transgender.”

Pearce mocked the concept of children learning of transgender identities on social media, but later contradicted himself by discussing the issue in the presentation segment titled “We Are the Virus: Reproduction via Social Contagion.”
In the segment, Pearce asserted the need to help transgender-identifying people to not only sexually reproduce, but also to “socially reproduce” by means of altering medical language and policy to introduce the idea of transition to children and adults as a form of “reproductive justice,” thereby creating more transgender people.
In the video, Pearce acknowledged that social contagion is the method by which transgenderism proliferates, stating: “Alexis Davin noted that the very process that Lisa Marchiano and Abigail Shrier described as a social contagion is the means by which trans people engage in a form of social reproduction. We become visible to one another and introduce one another to a language that makes sense of our lives and our needs.”

Later in the seminar he continued, “I’ve been thinking a lot about social contagion because it’s the language of the anti-trans movement. But… the exact thing they’re describing is the exact means by which we reproduce ourselves.”
During the seminar, Pearce described the work he did with Brighton and Sussex University Hospitals (BSUH) NHS Trust, arguing for the need for “Gender Inclusive Language” to create “Language as Possibility” and posters that act as apparent recruitment advertising for the political transgender movement. Pearce elaborated by saying, “in Brighton and Sussex University Hospitals, that’s a really interesting example of queer spaces of care being created through an institution rather than through more radical networks.”
Pearce’s involvement with the ITEMS research, as well as its use to justify an NHS maternity program, comes less than one year after NHS negligence was found to have been responsible for the needless deaths of over 200 babies and 9 mothers at at Shrewsbury and Telford NHS Trust. According to internal investigations, “repeated failures in the quality of care and governance” was to blame for the deaths, which spanned over 2 decades, with an additional 1,486 families and 1,592 incidents being recorded as a result of inadequate maternity care oversight.
Reduxx has previously revealed how errors and confusion arose due to the use of inaccurate medical language which led to midwifery students at Napier University in Edinburgh being taught how to care for males giving birth through penises and prostates.
According to a course workbook, students were advised: “It is important to note that while most times the birthing person will have female genitalia, you may be caring for a pregnant or birthing person who is transitioning from male to female and may still have external male genitalia.”
#England#England’s National Health Service (NHS)#Trans Identified Male talking about maternity care#Men can’t have babies#With Woman#“Maternity Gender Inclusion Program#Improving Trans Experiences of Maternity Services (ITEMS)#Dr Ruth Pearce is a man#Dr Ruth Pearce is another TIM who thinks he is better than actual women#Reproductive Justice for Trans People With Ruth Pearce and Francis White#Gender identity and social contagion#It’s bigoted for critics to mention the link between social media and gender identity#But it’s ok for trans people to call gender identity a social contagion
102 notes
·
View notes
Text
BBC presenter Naga Munchetty has told a committee of MPs that doctors told her to suck it up after she experienced extreme menstrual health problems.
Ms Munchetty and TV personality Vicky Pattison said GPs had repeatedly called their gynaecological symptoms "normal".
Both turned to private healthcare to have their conditions treated.
The pair were giving evidence to the Women and Equalities Committee as part of an inquiry into women's reproductive health.
Earlier this year, Ms Munchetty revealed she had adenomyosis, which affects the womb, but called the process of being diagnosed "infuriating".
She had suffered debilitating symptoms, including excruciating pain and heavy menstrual bleeding, since her teens, with her husband even calling an ambulance because of the pain, she told the committee.
But the attitude of the GPs had been: "Those are your [treatment] options - and if they don't work for you, then suck it up."
'Crippling anxiety'
Ms Pattison was diagnosed with pre-menstrual dysphoric disorder (PMDD), after hearing about it during conversations on social media.
"For 10 days of the month, I was feeling really fatigued, suffering with insomnia, having crippling anxiety, terrible self-doubt, no passion for the things I normally loved," she said.
She had visited doctors around the country but always been told: "This is PMS [premenstrual syndrome]. This is what women go through. Every other woman in the world is dealing with this," making her feel "even more invalidated".
"Women's health, be it reproductive, sexual, everything, is given less gravity because we are just expected to get on with it, to suffer it, to be brave. It's got to change," Ms Pattison told the MPs.
Ms Munchetty said of seeking treatment privately: "It was the only time I felt I could sit there and take time and force an issue, force understanding, force explanations from my gynaecologist and not feel bad that I was taking up more than 10 minutes of my GP's time because there was a queue of people in the waiting room."
Both Ms Munchetty and Ms Pattison told the MPs that women must be properly listened to in the health service.
'Better understanding'
Ms Pattison said: "GPs, anyone within the NHS, any medical professionals at all, they just need to start to take women seriously when they say something's wrong.
"I know loads of brilliant women and I don't feel like we're the weaker sex at all. I feel like we're brilliant.
"I feel like we're strong and powerful and we put up with a lot more than blokes do most of the time.
"If we have got ourselves up and gone into a doctor's, a hospital, whatever, to say something's wrong, I feel like the least people can do is listen to her and believe that there is something wrong."
And "better knowledge, better understanding" about health issues affecting women specifically was needed.
After talking about adenomyosis publicly, Ms Munchetty said she had been approached by medical professionals who had never heard of the condition.
"There's not enough training, there's not enough focus in the medical profession on women," she said.
26 notes
·
View notes
Note
(I’m finally free from work!)
Super crack idea but imagine Arcee and Elita learning about the female reproductive system and the utter hell they’re going to have to go through every month. Now suddenly they have a lot more respect for Miko since she was fighting cons while fighting off cramps
Oh GOD YEAH.
Elita and Arcee, admittedly though now human, were found to be incapable of the general female reproductive system, if only because as bots, well they don’t have an equal to it. They have the organs but they don’t function, essentially infertile.
Still, they learned about it in the event this change did also affect that, and when they learned of ovulation, menstrual and reproductive health conditions for women, they were stunned that Miko and June went through stuff like this, every month since their teen years.
To say the least, they had a new respect for Earth Women and their struggles.
17 notes
·
View notes
Last Seen Blogs


benvivasart
The Art and Doodles of Ben Vivas

thehellsitenewsie
Extra! Read all about it!

nutritionalwork
Nutritional Work

jjvelasco
Píldoras digitales