#but these three disorders have so much in common in the stigma of it
Text

#idk if this has been done before#but these three disorders have so much in common in the stigma of it#like yeah other disorders have bad stigma#but not to the point of most people thinking you are a murderer simply because of your disorder#schizophrenia#aspd#antisocial personality disorder#did#dissociative identity disorder#mental illness#nd#neurodivergent#actuallyschizophrenic#mental health awareness#plz dont derail with other disorders
2K notes
·
View notes
Text
I want to break down a common point of conflict when addressing NPD stigma.
A lot of hangups people have tend to be along the lines of "but I DO see a lot of people with actual NPD who are acting in toxic or abusive ways".
This will be kind of long, so bear with me.
Point #1: People are way more likely to be diagnosed if they exhibit "stereotypical" symptoms.
There's this image of NPD as a disorder that is only present in those with patterns of destructive behavior towards others. Many therapists have this conception. (Shockingly, the mental health field is not perfect & without stigma.)
Gonna copy-paste this here from my other blog (so forgive me if you've seen it before), because it's a good example.
Three people are criticized at work. Their boss yells at them for their performance in front of everyone.
Person A gets mad and defensive. They yell back, using cutting remarks as a way to try and ease the distress they feel.
Person B acts really mature and responsible the whole time, nodding along and agreeing and promising to do better, just desperate to maintain and improve their status. Desperate to be liked. Later they go home and handle their distress through self-destructive means, and spend the next few months overworking themself to the point of illness.
Person C doesn't seem to respond much at all. They go quiet and seem distant. They don't lash out or lash in, but for the next month or so, their productivity drops. They simply aren't able to focus on work or self-care, no matter how hard they try. The stress is overwhelming.
All three of these people have the same root issues, but only the first would be labeled a narcissist.
Outwards behaviors and presentations don't reflect the pain, distress, and difficulties with life that are underlying them.
So, three main things happen.
There ends up being a higher rate of people with destructive behaviors who are diagnosed with NPD
The people who don't particularly exhibit behaviors and are considered ""too nice to have it"" are overlooked entirely (and never get any sort of help for their underlying issues, yayyy)
People are more likely to be more honest about "ugly" symptoms / symptoms that are frowned down upon than they are in other mental health communities.
(Also some people decide to act super edgy about it, which is annoying but here we are. Some of them are trolls.)
(And while I'm at it, some people are misdiagnosed with NPD because a psych sees someone who committed a violent crime and is like "uhh slap them with the Evil Asshole™ disorders!! no further thought given.")
Point #2: People who have messed up are not inhuman monsters who deserve no help or support
While I do think it's important for people to understand that patterns of toxic behaviors aren't the ONLY way NPD can present, I'm not going to let the conversation stop at "some of us are nice though!!"
Human beings aren't RPG characters who can be sorted into "monster" or "ally". Every single person has done something hurtful, has messed up, exhibits some sort of behavior that puts strain on their relationships sometimes.
So I'll bullet point some aspects of this that need to be talked about.
People without NPD also commonly exhibit toxic behaviors, but people ignore that nowadays. Either they armchair diagnose anyone who's slightly rude, or they only focus on it in pwNPD and ignore it in themselves or others. NTs can be jerks too, and they're probably less likely to acknowledge it than pwNPD who are constantly watching and checking themselves and analyzing their behaviors and attempting to do better.
Assuming that NPD makes someone abusive doesn't help anyone. Can it impact behaviors, and make it more difficult for people to be self-aware? Of course. But an important step in healing from any mental health condition (especially personality disorders, ime) is realizing that you're not inherently ""bad"", and that you can take responsibility for your actions and learn to deal with things in constructive ways. Just going "NPD makes people bad, full stop"- other than being a mean shitty thing to say- absolves people of guilt and asserts that there's no reason for them to try and improve.
Yes, it's okay for people to hate their abusers. Their abuser. Not an entire community of people who happen to (maybe) share a trait with them.
Building on the above point, people tend to go in defense mode when they hear things like "pwNPD who have acted in toxic ways can learn to improve their behavior", "people shouldn't be saying awful things about folks with this condition", etc. because they automatically try to apply this to their abuser. Interpersonal situations are very different from society-wide mental health access. No, don't stay with your abuser expecting them to change, and don't hold onto the hope that they will. No, don't censor yourself or your hatred or anger towards them. Just don't make blanket statements about a disorder that they may or may not have- blame their abusive actions, not their mental health.
"I hate you for your abusive actions and the harm that you caused me." =/= "I hate a group of people because of an inherent unchangeable part of them that's tied directly to severe childhood trauma they suffered. Because of it, they're evil and unlovable and are incapable of change. They're inhuman and will never experience real connection with others." ..........See the difference??
Even if there were a disorder with a 100% rate of toxic douchey behaviors, I'd want the conversation around it to be changed. I'd want different words to be used to divide up the spaces and conversations and resources, so that survivors of abusive or toxic behavior can get help, but that the disorder still has space to be treated. Otherwise, there are zero resources for healing. Nothing is being done to help these people or solve the issue. They're just told they may as well not try. They're blocked from healthcare entirely, despite how the entire point of being diagnosed with a condition is supposed to be to treat it.
There's a wide range of people who have NPD- it presents in many different ways, a person who has it may or may not exhibit harmful behaviors- but no one deserves to be denied treatment or told they're unlovable because of a condition they have that was formed from trauma.
Speak out against abusive behavior. Don't destroy healthcare for a medical condition.
913 notes
·
View notes
Text
Crowley's BPD Traits And Why They Are Important;
We all know our beloved ineffable husbands are neurodivergent icons. Despite not being human they both act like neurodivergent humans would (and do).

Today I thought we would take a look specifically at Crowley and his BPD traits and what they mean.
(Also before we start; a trigger warning for talks and mentions of suicide, depression, mood swings, drinking, and trauma).
First what is BPD? BPD stands for Borderline Personality Disorder.
"A mental disorder characterized by unstable moods, behavior, and relationships." -Mayo Clinic
BPD is a disorder caused by trauma. Trauma is of course different for every individual. So while some demons may seem perfectly content with the fall from Heaven, others may have been significantly traumatized. And I believe this is where Crowley falls (pun very intended).
So we covered how Crowley could have developed BPD, but let's talk about their traits.
The DSM-5 lists 9 Criteria for BPD, of which at least 5 are required for diagnosis. We will be covering each one and how (or how they don't) apply to Crowley.
1. Frantic efforts to avoid real or imagined abandonment:
As we know BPD is caused by trauma, but more specifically it can be trauma that deals with abandonment. Say God casting you down to Hell for simply asking questions?
This can lead to the person with BPD going through frantic efforts to avoid abandonment happening ever again.
We can see this most in Crowley when she argues with Aziraphale. Can you count how many times Crowley tries to run away with Aziraphale so that he doesn't leave him during an argument? It's three. They have done this three times (and that's just the on screen ones, who knows whats happened in 6,000 years!).

2. A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation.
Now this one is harder to see in Crowley because this trait of BPD (and many others) comes out most in romantic partners. And Crowley has only ever had one apple in his eye, Aziraphale. But even just with their relationship with Aziraphale we can see this.
While Crowley never directs his anger at Aziraphale we can definitely see how much the angel affects him. Their arguments that can lead to them not talking for decades, Crowley literally exploding with lighting because of his anger.

An example I find most interesting is Crowley's entire perception of Aziraphale changing when he sees Aziraphale let the people in the flood die. And this perception is only fixed in the Job minisode when Aziraphale does the right thing again. All it takes is one incident for Crowley to change her mind.
3. Identity disturbance: markedly and persistently unstable self-image or sense of self.
I think this is most obvious in the opening to season 2 where Crowley is questioning the meaning of life and more importantly his role as a demon.

But this isn't the only demon related identity disturbance Crowley faces. A common identity disturbance for those with BPD is believing that they are evil. This is caused by trauma but is also not helped by the stigma Cluster B disorders face.
Crowley believes he must be evil because he is a demon. He lies because he is a demon. Just like someone with BPD may believe they are evil for their disorder or are manipulative because of it. But in reality that may not be the whole truth. You can still be a good person despite being a demon, despite having a disorder.
4. Impulsivity in at least 2 areas that are potentially self-damaging (e.g., spending, sex, substance abuse, reckless driving, binge eating).
Do... Do I need to explain this one?
Crowley is an alcoholic. He casually drinks but will also drink anytime a slight inconvenience pops up.
Crowley is also known for going "too fast". He is almost always speeding in the Bentley.
5. Recurrent suicidal behaviour, gestures or threats, or self-mutilating behaviour.
This is one of the ones that is harder to apply to Crowley simply because she is a demon, not a human. It is much harder for him to kill himself. And while this trait must be recurrent I still think it's important to bring up the Holy Water incident.
Crowley tells Aziraphale the holy water is just for insurance, but Aziraphale knows Crowley better than that and was right to assume it could probably be for a suicide pill. (Even if it did come in handy as insurance later). But the fact Aziraphale assumes that I believe is telling.
6. Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability or anxiety usually lasting a few hours and only rarely more than a few days).
We see a few different times where Crowley's mood shifts into extremes.
We already discussed the lighting incident. I think another big show of their anger is how he treats his plants in season 1. While yes it is them recreating their trauma with God (Metatron?) and being thrown out of Heaven, that anger comes from somewhere.

Jim short for James, long for Gabriel also sparks this anger in Crowley to the point of threatening his life and telling him to jump out of a window.
Crowley's depression is seen on the biggest spotlight when talking about the fall. Their sentiments about not meaning to fall, that she only ever asked questions.

7. Chronic feelings of emptiness.
Unfortunately I can't speak on this one purely because I do not live in Crowley's head. I do not recall it ever being something mentioned or showed. That doesn't mean it can't happen to her of course, but let's stick with the facts.
8. Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant anger, recurrent physical fights).
As you can see BPD deals with anger a lot. so I will once again bring up some points we've already made. With the lighting incident, and good old Jimmy-boy.
I also just wanted to mention we know Crowley appears a bit angry at most times as well as Muriel describes him as "the grumpy one". Just thought it was a fun, helpful detail.
9. Transient, stress-related paranoid ideation or severe dissociative symptoms.
This one is also a bit hard because again I am not in Crowley's head but also she does in fact have plenty to worry about that is real.
But Crowley does still show paranoid ideation. His distrust of others, disorganized thoughts (talking about ducks and the end of the world at the same time), feeling threatened, thinking he's being spied on (the ducks have ears).
Lots of ducks.
Now some may think diagnosing/headcanoning a character with specific mental illnesses is silly, and maybe it is! But I still believe it's important. Why?
Well for starters; representation is always important. Seeing someone similar to you on screen you can relate to and find joy and comfort in. Or maybe they're just raising awareness. Or just showing that hey, these people exist.
But I also wanted to touch on the stigma of BPD and other Cluster B disorders.
I touched on it briefly in an earlier point but BPD is heavily stigmatized. Many people treat the disorder as evil and manipulative. That the people with it don't deserve love or kindness. Which is of course simply not true.
Most of the characters coded with BPD today are antagonists and/or villains. Think Jinx from Arcane or Spinel from Steven Universe. These characters are amazingly written and performed and I do love them dearly. And there is nothing wrong with them, but it is nice to even the playing field. To have a character with traits of BPD who is fundamentally good and does the right thing. They are a protagonist of their story and even a hero!
And that is why I think Crowley is good representation of BPD (even if it was not intended that way).
And here's hoping to season 3 so our demon (and angel) get a happy ending!

#Anthony J Crowley#Crowley#Good Omens#Good Omens 2#Gomens#Ineffable Husbands#Aziracrow#BPD#Borderline Personality Disorder#Neurodivergent
132 notes
·
View notes
Note
never really gave much thought to it until now but it is so weird to experience disordered eating tendencies solely cause of food insecurity but all i ever really heard about it was how its related to beauty standards etc, and so i never really took ot seriously and developed some very shitty habits due to food inaccessibility.
do you maybe have some articles or anything worth checking out about that side of eds? thanks in advance, love your blog so much!!
When the researchers sat down and started analyzing the results, they found almost linear correlations between eating disorder symptoms and food insecurity. A replication study in 2019, conducted in an even larger population at the same food bank, found almost identical results. “It was some of the saddest and most beautiful data that I had ever seen,” Becker said.
Her work challenged preconceptions about what eating disorders actually were.
Singh, the New York dietician, said those preconceptions stem from the fact that people who have eating disorders and can afford to seek help tend to be wealthier. And most research is done on patients who show up in clinics.
Food insecurity never even entered the picture of how psychology and psychiatry conceptualized an eating disorder, Singh said. As a result, starving yourself to lose weight was considered a disorder, but no one thought about starving yourself to ensure your family had enough to eat.
Results suggested that individuals in the child hunger insecure group had the highest levels of eating disorder symptoms. Seventeen percent of individuals in this group had a clinically significant eating disorder, compared with 9.4% in the food insecure group, 2.6% in the household food insecure group, and 2.9% in the not food insecure group. Binge eating, overeating, night eating (waking up to eat a large amount of food with distress at night), vomiting, laxative/water pill use, skipping at least two meals in a row, exercising harder than usual because of eating too much food, and weight/shape concerns were all more common in the child hunger food insecure group than the other three groups. There were no differences between groups for the eating disorder symptoms based on sex, race, or ethnicity. Similarly, internalized weight stigma and worry was greatest in the child hunger group.
There are several implications for this study. First, these data reiterate that eating disorders do not discriminate on the basis of socioeconomic status. Individuals who are food insecure need to be considered in future research in order to fully understand risks that are specific to this population (e.g., food restriction for any reason). Second, prevention, intervention, and treatment programs need to be designed so they can reach individuals who do not have the money to access these programs. For example, current treatments for eating disorders are primarily delivered face-to-face with a trained clinician, which is difficult to disseminate to a wide range of individuals. Finally, although not directly assessed, anti-obesity programs may negatively affect individuals who are food insecure and overweight or obese, given that internalized weight stigmatization was high in a proportion of these individuals. Additional research in this population will be critical to better understand risk factors for eating disorder symptoms in this understudied population.
https://onlinelibrary.wiley.com/doi/full/10.1002/eat.22735 (<-link to study discussed above)
Many people (incorrectly) believe that eating disorders (ED) are more prevalent in the higher socioeconomic status (SES) groups. Studies conducted in the 1960s and 70s corroborate this statement; however, their methods may have biased the results. Recent studies using health questionnaires distributed to large heterogeneous populations have shown that EDs equally effect all people, regardless of SES. These studies have also demonstrated that females of the lower SES group report higher rates of disordered eating behavior (vomiting, use of diet pills, diuretics, or laxatives as a means to lose weight).
124 notes
·
View notes
Note
So one of your takes on how a glut of shoujo isekai manhwas revel in glorifying feudalism popped up on my dashboard (perhaps because of my once budding love for webtoons and the like) and funnily today yt recommended me VICE's take on South Korea's Chaebol ascendency, both of which are thoroughly exploitative and mirror each other. Aside from that I remember(back when I was into consuming these) being bombarded by a repetition of partial treatments afforded to most, if not all, of the manhwa MLs or MC's abusive bro or dad(note: mostly if not always male family members), most of whom belonged to either of the two aforementioned institutions. Now I spotted a pattern here- there's this glorification of consorting, defending your abuser in not just Korean shoujo manhwas but dramas(Boys over Flowers/that Chaebol love, tho the source is Japanese) too. This breed of "beloved" abusers are emblematic of coalescing three of the most oppressive systems which SK common folk struggle against- feudalism, capitalism and patriarchy.
And this is where my question comes in-
Why? Why are these pieces of fiction ,aimed at impressionable minds, strictly adhering to being apologists for these systems.
Because most of all the old and new dominating shoujo manhwa and drama tropes are somehow rooted in these three.
Why are these apologist(for the systems) tropes so loved by the Korean people?
And specifically, why do they show a protagonist going from rightfully opposing these flagbearers to conceding and defending them-like that's so detrimental to say the least.
Sorry for the long ask.
I have the theory that CEO, teacher, & stepbrother romances have partly something to do with the fear of authorities and that some people tend to romanticize their fears (why monster romances such as vampire and werewolf stories might exist). Although the laters popularity can be mostly attributed to the popularity of the forbidden love trope.
I disagree that this pattern is only common in Asian countries (Asshole love interests are plenty of popular in the US as well (i.e. Damon from Vampire Diaries for example.)) The thing is China, Japan, and Korea are the countries where hierarchy is extremely important. You ought to respect your boss/father/brother and the male family member has significally more power in the household. You also spend much more time at work/studying at home. China is in the top 10 list of countries with the most work hours. Japan literally has a word meaning overwork death relating to occupation-related sudden death, because it occurs so often. As a result I imagine that the numbers of workplace/domestic abuse go up. It doesn’t help either that there is a stigma surrounding mental health in Chinese/Korean/Japanese culture. Their society has conditioned its members to believe that a mental health disorder is shameful and signifies a lack of willpower and harms the personal reputation and social harmony. Fiction is a mirror of reality. It shows the fear and desires of people. For a woman trapped in a low salary job constantly exposed to verbal abuse and harrassment with no way out, reading about romances where the abusive CEO was only abusive out of love for the poor heroine and eventually changes because of the power of love must be carthetic. Anecdotes where someone changes because of love are more common than an office worker dragging their boss to court and successfully getting their justice through legal means.
Fathers are the usually the breadwinners and it’s not that common for them to be uninvolved with their children (especially in Japan/Korea where it’s common for them to work alot/overseas to earn enough money that they then invest in their child’s education.) Abusive and neglectful mothers are demonized while fathers are forgiven, because being a loving mother is expected and seen as the norm but being a loving father isn’t. They are more easily forgiven, there is the yearning for parental affection and the feeling of debt that his son or daughter owes him affection since he “sacrificed” his time for the family to finance the family. A man restraining his emotions except for pride and anger, treating his children coldly is more acceptable than if a woman did this. It has alot to do with toxic masculinity, I suspect.
Writers tend to use methods that are tried and true. They will jump on popular tropes and stick to it because they know there is an audience for it and that it sells well. Rags to riches story where a girl who is not socially-privileged meets a very highly-situated man and they end up marrying each other after defying the forces that try to keep them apart are as old as dirt. Romance novels usually fall into one of these two cateogories: Cinderella type of stories and Beauty and the Beast type of stories. An ice cold duke from the north who suffers from a curse/brainwashing is a fusion of two of the most popular tropes. So it’s no surprise to see these kind of stories popping up everywhere.
Girls have been conditioned to want a Cinderella-turned-princess type marriage for their own sake. It is nearly every mother's dream that their daughter marries the wealthiest, educated, most socially and politically powerful and handsome man that she possibly can.
Dating can be considered part of a social career. There aren't many ways to achieve a social rise besides studying hard and marrying rich. Stories about the life of a student going to cram school don't provide an interesting plot. The ups and downs of living with a chaebol family do.
Product Placements: How else can you advertise brands like Laneige, Swarovski, Tiffany & Co, Range Rover, Mercedes-Benz, designer fashion and watches in kdramas? Poor people can't afford such things.This isn’t about teaching people morals it’s about making as much money as you can.
Virtues are relative to the culture defining them. Mental strenght and being able to keep a cool head and endure bad situations is seen as strenght in those countries. Screaming, swearing and fighting back with violence would be seen as childish and immature. You are just losing your face.
Some old fashioned ideas still persist. For examples Confucian virtues of a women include forgiveness, chastity and compliance. The reason why assault is so common in Otome games and webtoons is because many women live in a state of sexual repression where they aren’t really allowed to initiate or enjoy sex lest they be called a whore. That’s were the overly jealous/possessive boyfriend comes into play who finds the heroine’s purity so irresistable that he literally cannot stop himself, and if she secretly enjoyed it well that’s not anyone’s business, is it? + sexual domination fantasies are actually very common everywhere.
In short: A partriarchial and capitalistic society with an imperialistic past *cough Japan* would would want to despict themselves in a positive light and be interested in upholding those values. The heroines fall in love with their abusers/defend them because those stories sell well and upholding the peace in the family & society is seen as more important than the happiness of a single person. Since seeking mental health counselling is frowned upon, consequently the role of the therapist automatically falls onto the daughter/wife of the family. Raising your daughter how to navigate a world to want to marry a powerful/wealthy man so that your family will be well off is the goal of nearly every mother across the world. A single person cannot change the system, they have to learn how to bend to the will of their superiors to survive and I guess the media prepares you for that harsh reality. Add to that coping and the abuse victim fantasy of having the power to fix your abusers.
9 notes
·
View notes
Text
a day in eating disorder inpatient treatment
tw food mention, ed recovery, hospital
my original plan for the summer semester was to take a course, leaving me with only one more semester of my degree. however, that plan had to be put on hold because i chose to further my recovery from my eating disorder and participate in the symptom interruption phase of inpatient treatment. while shorter than the full program, i still participated in all of the groups and meal supports for three weeks. i thought i would write a blog about a typical day in treatment in case anyone was curious, and to break down the stigma surrounding eating disorder treatment. note, i do mention what i would typically have for meals and snacks which is a totally personal thing! everyone is different. i was there only on weight maintenance, so my experience is much different than somebody on a weight restoration plan. please don’t continue if that is something that would trigger you.
my typical day started with being woken up to get weighed at around 7 am. then it was back to bed until 8 when bloodwork would wake me up a second time. after they finished i would get up, make my bed, and get dressed for the day. most people wore sweat pants and slippers but i tried to keep myself in a routine and would wear comfortable jeans and sneakers, the same as i would outside. my room, which just happened to be the biggest out of them all, was a private room with a bed, night table, desk, chair, bathroom, and sink. on my wall there were two posters, non negotiable rules and a dbt skills poster. i also had a whiteboard where i wrote an inspirational quote. i stuck pictures that meant a lot to me on the wall over my bed with sticky tack. i’d brush my teeth and by then the nurse would come in with my morning medication. then it was off to the group room to wait for breakfast. the group room consisted of a table with chairs and three couches we could sit or lie down on and watch tv or just hang out. at around 8:30 a staff member would come collect us from the group room and we’d make the long walk of shame down the hallway to the kitchen. breakfast would be laid out, ready for you. my best friend made the placemats during a previous admission we had together. they all have an inspiring quote on them.
for me, breakfast often consisted of coffee that tasted like bog water, scrambled eggs, a muffin with butter, plain oatmeal with brown sugar, and a banana. the room had a google home mini so we’d listen to music while we ate. we got 30 minutes to finish everything in front of us, 100% completion was a non negotiable rule. after we finished we went around the room sharing our check out of how the meal went, one thing we liked about the meal, and what our plans were afterwards. then we would be escorted back to the group room for our first group of the day. i’m going based on thursday, which means we had family relations first. we would talk about our relationship with family and friends and how the eating disorder influenced them. it was really cathartic, although it was common to be uncomfortable when the social worker asked for your participation.
after group we would go back to our rooms and wait for the doctor. she would sometimes pop in and go over your bloodwork with you and see if you needed anything. then the nurse would come in and let you know it’s time to lie down for vitals. you laid there for five minutes. some people would look at their phone during this time and play wordle, but i always stared and the ceiling and did square breathing. it felt like a good time for mindfulness. the nurse came in with the blood pressure machine and took it lying, then standing after two minutes. she also took my temperature and asked me some questions about mood and bowel movements. that’s one thing i don’t miss.
next we had morning snack at 10:30. we would reconvene in the group room and wait for the staff member to come collect us. although it is something i struggle with, i personally enjoyed this one the most. i even inspired some staff members to try peanut butter on their apples because that’s what i always had. while eating together as a group was a norm, part of the program is increasing independence. so i did a lot of morning snacks with just me and the staff member because of where the other patients were in their program. after we finished snack, which we had 15 minutes to complete, we played a game for 15 minutes. i usually chose skip bo.
after snack we would have another group such as dbt. if you’re not familiar with dbt, it stands for dialectical behaviour therapy. it’s a really helpful therapy that explores emotions, mindfulness, distress tolerance, and the connection between events and behaviours. for this group we were often assigned homework pages in a workbook to complete by the next session.
then another staff member would come get us for lunch at 12:30. everyone always ate lunch together no matter where they were in the program. a typical lunch would be an egg salad sandwich, salad with dressing, canned peaches, and water. again, we would have 30 minutes to complete it. then we would play a game for 30 minutes. the group of patients i was in with liked playing bananagrams. i had never liked the game before this admission.
from 1:30 pm to 2:30 pm we would have free time. this was also the time a staff member would open up the doors to the “patio” so we would hang out there. really, it was just some fenced in grass with a flower box and a couple of old lawn chairs on a concrete slab. but the fresh air was vital for our sanity. we would also mingle with the general psychiatry patients out there (as this program was separate, but still took place on a general psychiatry ward). then, another snack. my favourite was raisins and cheese. this snack was usually done by the nurse. again, 15 minutes to eat and 15 minutes to play a game afterwards.
on thursdays we had weight review at 3 pm. the dietician would come find us and we’d go sit in private to discuss our weights and whether there needed to be changes made to our meal plan. for patients in weight restoration this was absolutely the most stressful and triggering part of the week. you also had the option of not knowing your weight but you would still have an idea of what was happening from the status of your meal plan. after our meeting we were free to do whatever until supper.
supper was supposed to be at 5pm but it was always more like 5:30 because the kitchen was always late. we’d be waiting in the group room, doing a puzzle to pass the time, a typical supper would consist of something like fish, mashed potato, vegetables, and cranberry juice. again, 30 minutes to eat and 30 to play a game. usually supper was supervised by a pca (personal care assistant). after supper we would have more free time, which was usually when we’d get visitors. when my mom was in town she visited, otherwise i hung out in the group room and watched movies while painting or studying for the mcat. night snack was at 9pm, and the pca would supervise that one as well. i loved ending off my day with something like cereal and soy milk. in the past you had to have a special reason to have soy milk, but now it’s more accepted as an alternative. i genuinely like the taste of soy better.
after that i would get a shower and read a book until my night nurse came in with my bedtime medication. then i’d go to sleep and do it all again the next day.
i am so thankful i had the opportunity to participate in this program. at first i felt like i wasn’t sick enough to be there, but then i realized that there was no “sick enough” and i deserved to be there. i gained a lot of insight and got back on my feet, which is what i needed. now i have the energy to focus on studying for the mcat! i hope writing about this experience takes away some of the stigma.
6 notes
·
View notes
Text
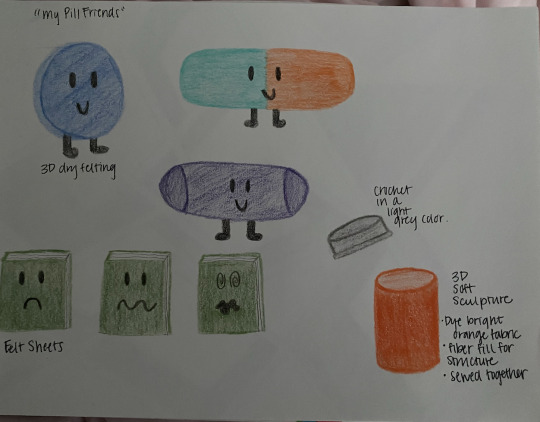
Project 2 - mobilize the cute further planning
So I made some more sketches for my designs, these are in color.
I am creating pills that are not to scale, but enlarged. I choose the three most common mental health issues among young adults, so the target audience here is 18-25 years of age. These are the prime years that people can have the time and ability to become comfortable with themselves, become self-aware, and work towards developing emotional maturity. This progression obviously does not stop at age 25, but continues as we gain experience as humans. The issues that I wish to highlight are: depression, anxiety, and ADHD. The prevalence of depression and anxiety has increased, much of this can be attributed to increased vigilance surrounding depression awareness. Despite this increase in awareness, there continues to be a lack of acceptance. Acceptance of the issue itself, but also being medicated for it. For the person who is struggling themselves, it can be difficult to even internalize having to be on antidepressants, and sometimes lifestyle changes can help, but often times these can only go so far. My goal is to reduce the stigma surrounding medication for mental health issues. Pills are very stigmatized, but the important thing to note is that we can only control our environmental stressors so much, as humans we need to realize that somethings are not within our control. Specifically, some issues are genetic and arise from a genuine chemical imbalance within the brain, thereby requiring medication.
For this first pill, I wanted to make a 3D model of a common antidepressant, Wellbutrin.
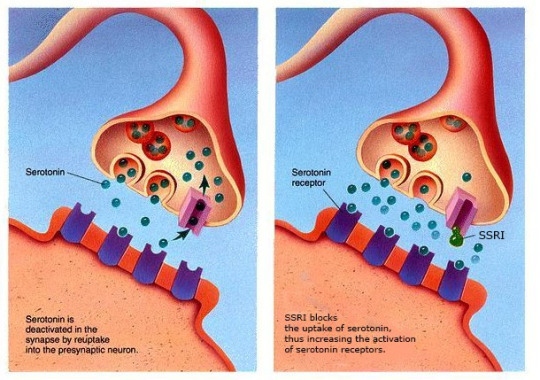
This next one is a common anti-depressant, Prozac, used to treat anxiety and anxiety adjacent disorders. Many other issues are prevalent within my generation, including eating disorders (ED) and obsessive-compulsive disorder (OCD). Since these are anxiety related disorders, I feel that this very popular SSRI is a best representation of a medication used to treat anxiety, since it is also used for EDs and OCD. SSRIs are selective serotonin reuptake inhibitors, their mechanism of action is to increase the availability of the neurotransmitter serotonin within the brain by blocking the reuptake of it by the neuron.
The last one is Concerta, which is an extended release stimulant used to minimize the effects of ADHD. This medication differs from the other two because it is a very rapidly metabolized drug that beings to work immediately, but also wears off within hours. With the other two, the medication needs to be taken daily to build up levels of neurotransmitters for the full benefits.
Here they are together. I think a very interesting aspect of drugs used to treat mental illnesses, is that they are all very colorful. It is very odd, but somehow very appropriate at the same time. It was this observation that has been with me for a while, and played a role in inspiring this project idea. The colors seem to juxtapose what the medication itself is used for. I feel that this can add to the "cuteness" of the project, as these are fun colors, but the message is far from fun. My two sources of inspiration for this were: pills and mental health issues. As neither of these are cute concepts, but this project aspires to incorporate cuteness to bring awareness to the subjects.
Here they are with faces. I think that this would solidify the cuteness because I wholeheartedly believe that putting eyes on anything instantly makes the object cute. I think that this is because it personifies the object, so as a human we perceive that this object now has some sense of life to it.
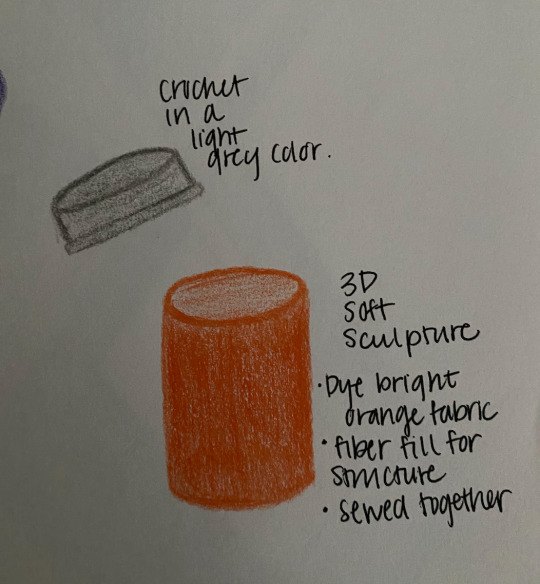
This piece will also include a pill bottle made from soft sculpture. To be honest, I am not completely sure how to go about this pill bottle, but I will figure it out.
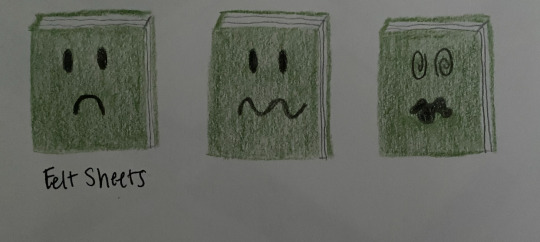
This aspect was not in my original plan, but I thought that an informational booklet would fit the prescription medication theme. This time, the faces are associated with the corresponding problem, and will be paired with the pill that they provide information for. The information might include: symptoms to look for, highlighting the ones that are often overlooked.
0 notes
Text
Is postpartum depression a disability? | Zyla Health
Eda Leshan once said, “A new baby is like the beginning of all things — wonder, hope and a dream of possibilities”. Nurturing a new life inside our bodies is the closest thing to a miracle.
Childbirth is the hardest and most rewarding experience of a woman’s life. As you bring your newest family member to your home, you bring joy, love and new excitement into your life. You fill your lives with happiness as you see the little one grow.
But did you know that the changes of motherhood can take a toll on your mental health? You must have heard about baby blues which are mild mood swings that occur for a few days after childbirth. However, some mothers can experience severe mood disturbances that are called postpartum depression (PPD) or postnatal depression (PND).
Because of the stigmas that surround mental health, postpartum depression is often considered an indicator of being an unfit mother, rather than a genuine problem. But it is so real that it is one of the most common complications of childbirth, affecting around 10–20% of mothers.
In this blog, we will learn about postpartum depression in detail starting with some of the basic questions like what is postpartum depression and why it happens.
We will also address some of the common questions like is postpartum depression a disability? Is there any treatment for it? etc, in an attempt to counter the stigma and start a larger conversation about the importance of the mental health of new mothers.
What are the common mood disorders in mothers after childbirth?
Childbirth represents a time when women undergo changes in their bodies, emotions and hormones that can take a toll on their mental health.
During the postnatal period, that is the time after childbirth, there is an increased risk of developing serious mood disorders. There are broadly three common types of postpartum mood disorders:
Postpartum Blues, also known as maternity blues or baby blues.
Postpartum Depression (PPD) or Postnatal Depression (PND)
Postpartum Psychosis also known as Postnatal Psychosis or Puerperal Psychosis
Baby blues are common but not of much concern unless they develop into something serious. Sometimes, there may be a period of well being after which the symptoms worsen and gradually develop into postpartum depression. Postpartum psychosis is a rare but serious mental health condition that requires hospitalization.
Let us now examine what exactly postpartum depression is!
What is postpartum depression?
As we have already learned, postpartum depression is a mood disorder that affects women after childbirth. The symptoms usually start showing within four weeks of delivery and can go on for a year, unless treated properly.
It has an impact on the health of both mother and baby. Postpartum depression can be physically and emotionally weakening and lead to serious complications if left untreated which causes people to wonder, is postpartum depression a disability?…
Let us look at how PPD can present itself in mothers…
Postpartum depression symptoms
Postpartum depression symptoms gradually develop with time and commonly manifest as:
Loss of energy or fatigue
Loss of appetite
Sleep disturbances
Feelings of guilt, worthlessness or hopelessness
Feeling like crying all the time
Poor concentration and memory
Withdrawal from society and family
Thoughts of harming yourself or your baby
Women who are suffering from PPD feel like they are inadequate, ‘bad’ or unloving mothers. They worry excessively about their baby’s health or feeding habits. In extreme cases, postpartum depression symptoms can include suicidal tendencies, where mothers may want to harm themselves or even their babies.
By now, it is evident that PPD can be harmful if it is not diagnosed and treated properly. PPD can contribute to bonding issues and lead to sleeping and feeding problems for the baby.
Did you know?
Although women are mostly affected by this, sometimes even fathers can suffer from PPD! Some studies suggest that low vitamin D levels are linked to depression. Read our blog, “Keeping Vitamin D under check for a healthy conception“ to know more…
In case you have any of the above symptoms or any other concerning health condition, you can download the Zyla app or visit our website- Zyla.in. Zyla provides personalised treatment for your overall health management.
Before learning the diagnosis and treatment, let’s explore the scientific causes and factors that contribute to the development of this disorder.
Causes of postpartum depression
The exact causes of postpartum depression are still unclear but there are many possible theories. Any mood disorder is a very complex disease, and there are multiple factors affecting it: biological, genetic, environmental and experiential. Therefore, it’s likely that all these factors play a role in the development of PPD.
1. Hormonal changes
The most widely believed cause of postpartum depression is the hormonal changes that occur after pregnancy. There is a rapid decline of reproductive hormones like progesterone and estrogen, returning to prepregnancy levels within 3 days. The usual monthly cycle of hormones is absent during pregnancy and lactation.
In addition to that, thyroid function also returns to prepregnancy levels approximately 4 weeks after delivery. To know more about thyroid disorders during pregnancy, read our blog, “Thyroid disease: Development during pregnancy, it’s impact on pregnancy and how to treat it”.
Because of these significant hormonal changes, it is only natural that mood disturbances can happen which in some cases may develop into PPD.
However, it is important to understand that these changes are normal and cannot be prevented.
2. Prior history of depression or mood disorders
Having a previous history of clinical depression or other mood disorders could be one of the causes of postpartum depression.
3. Stressful events
Dealing with stressful events in addition to dealing with pregnancy can increase the risk of developing postpartum depression. The mother might start questioning herself, is postpartum depression a disability?
4. Lack of sleep
The lack of sleep for a new mother, coupled with a lack of social or family support has been observed as one of the possible causes of postpartum depression.
Did you know?
A study found that two-thirds of women with postpartum depression also had an anxiety disorder.
What are the complications of PPD?
Now that we have discussed the causes of postpartum depression, we should know why it is so important to seek professional help without any delay.
For the mother, this episode of PPD can be the beginning of chronic recurrent depression which can become very serious in later stages.
The baby can have trouble sleeping, eating and learning to speak. A mother’s ongoing depression can contribute to the child’s emotional, behavioural, cognitive and interpersonal problems in later life.
If the mother is suffering from depression, the other family members like the father are also likely to suffer from depression.
Postpartum depression risks
All women are capable of developing depression after childbirth. Having any of these factors can significantly increase the postpartum depression risks:
A past history of clinical depression before or during pregnancy
Excessive anxiety during pregnancy
Past history of PPD in previous pregnancies
Family history of depression and mood disorders
Age of the mother. Research has shown younger the age of the mother, the higher is the risk of developing PPD.
Lack of social support
Marital conflict
Recent stressful life events or socioeconomic status can also affect the mother.
Identifying the postpartum depression risks is essential because identifying a trigger can help us better address the problem and seek treatment on time.
If you’re seeking help to improve your mental health, you can download the Zyla app or visit our website Zyla.in and check out the health program which is suitable for you.
Let us now look at some of the ways how postpartum depression diagnosis is done!
Postpartum depression diagnosis
The process of postpartum depression diagnosis can be a challenge in itself and there are many reasons for that.
Firstly, because of the stigma and shame associated with mental illnesses, women are usually unwilling to disclose these symptoms to their physicians. They are indirectly and eventually forced to think, “is postpartum depression a disability”?
Many women will ignore these signs or internalise their struggles due to the lack of awareness of the severity of PPD.
The other reason is how similar the symptoms of postpartum depression are to that of postpartum blues, which can be difficult to differentiate. Unless the symptoms are very severe, it is often undetected and considered as natural mood swings that occur after childbirth.
For the postpartum depression diagnosis, there are two main classification systems used within psychiatry:
The American Psychiatric Association’s Diagnostic & Statistical Manual of Mental Disorders, in its current fifth edition (DSM-5, 2013) and
The 10th edition of the International Classification of Diseases, (ICD-10), published by the World Health Organization (World Health Organization, 2019).
Apart from the unnecessary medical details, DSM-5 and ICD-10 contain standard criteria for the diagnosis of known mental illnesses, like postpartum depression.
Your doctor with the help of standardized interviews, self-report questionnaires, and clinician-rated scales will screen you for the diagnostic symptoms of PPD. PPD is diagnosed after a psychiatric evaluation and medical evaluation.
Now let us learn how PPD can be treated in new mothers!
Postpartum depression treatment
If PPD is not diagnosed and treated early, it can lead to many long-term adverse effects not only on the mother’s health but also on her child and family. The following lines of postpartum depression treatment can be adopted by your doctor:
Antidepressant medications can be effective. The commonly used drug is fluoxetine or paroxetine which is effective and has fewer side effects. Since this drug is safe for breastfeeding, make sure you do not self medicate. Discuss with your doctor about the safety and side effects of all the antidepressants before starting with any of them.
Hormonal patches (estrogen or progesterone) can also be recommended for postpartum depression treatment.
Continuous reassurance and psychological support by your family members can go a long way. In an interview with mothers who have recovered from PPD, the first suggestion they gave was to “find someone to talk to.” For this reason, peer support groups can be very helpful.
If there is no improvement of symptoms, psychiatric consultation is looked for. The two widely used therapies are Interpersonal Psychotherapy and Cognitive Behavioural Therapy which can improve your mental health.
If you are wondering how to prevent PPD, the next section will be helpful as we take a closer look at some preventative measures.
How can you prevent PPD?
There is no hard and fast rule on how to prevent PPD but if you take care of yourself by following the given points, you might be able to stop PPD from getting worse.
Have an open discussion with your doctor about your mental health. If you had any depressive episodes during pregnancy or before, make sure to share this with your doctor so that a care plan can be made to watch for signs of postpartum depression after delivery.
Look for the risk factors and if you have any of them, look out for any symptoms. Do not dismiss them as mere mood swings and seek medical help.
Lastly, education and awareness about PPD not only to you but also to your family members can enhance a positive attitude towards mental health. Have a healthy relationship with others so that you can have a strong support system when you feel low. This way, the question, “is postpartum depression a disability?” won’t arise.
No doubt, post-delivery, it becomes extremely important for a mother to take care of her mental and physical health. One such concern is taking care of the genital region. Read our blog, “Wound healing post-delivery” so that you can take more care of your body.
Before concluding this blog, let us take a brief look into the other two kinds of postpartum mood disorders that I have mentioned in the beginning.
What are postpartum blues and postpartum psychosis?
Postpartum blues
Blues is the most common mood disturbance occurring in almost 30–75% of mothers. The symptoms begin within a few days of delivery, usually on day 3 or 4, and persist for hours up to several days.
The symptoms include:
Mood swings
Irritability
Tearfulness
Generalized anxiety
Sleep and appetite disturbance
As you can see, the symptoms are similar to PPD but in a much less severe form. Postpartum blues are by definition time-limited, mild and do not require any treatment other than reassurance.
Postpartum psychosis
Very severe depressive episodes which are characterized by the presence of psychotic features are classed as postpartum psychosis. This is different from postpartum depression in cause, severity, symptoms, treatment and outcome.
It is the most severe and uncommon form of postpartum mood disorders and can affect 1- 2 women per 1000 deliveries. The symptoms develop rapidly within the first two weeks after childbirth.
The symptoms include:
A depressed or elated mood that can change rapidly
Disorganized behaviour
Sleep disturbances
Feeling restless and having strange feelings
Delusions, where women lose their touch with reality and start having false beliefs
Hallucinations that can be auditory or visual where they hear or see things that aren’t happening in real life. The other forms of hallucinations of taste, smell and touch are quite less common.
Because of the severity and the chances of harming others, postpartum psychosis requires constant monitoring and hospitalization.
If you develop any symptoms of these mood disorders, you might feel isolated and that nobody can understand what you are going through. You might be scared, so you might not even open up to your loved ones. However, as a part of recovery, you must seek help because you are not alone in this.
The ignorance of mental health remains a major problem in our culture, but postpartum depression is just another complication that can occur after pregnancy and needs treatment just like any other disease.
And the answer to “is postpartum depression a disability?” is obviously a big NO! When we normalise this, only then can we give proper care to these mothers who are in no way less than superheroes!
If you are experiencing any such symptoms, Zyla can help you. You can enrol in our Ova Pentacare Pregnancy Program where Zyla’s team of 50+ medical experts guide you through pre-conception to post-delivery management and counselling.
Zyla has doctors, nutritionists, psychologists and physiologists to provide you with a holistic approach through personalised care and treatment. Feel free to download the Zyla app or visit our website-Zyla.in.
Connect with us:
Subscribe to our Youtube channel: https://bit.ly/2o19OzE to watch videos on health and health-related conditions.
Find us on Facebook: https://www.facebook.com/zylaova/ and https://www.facebook.com/zylahealth
Find us on Instagram: https://www.instagram.com/ovabyzyla/ and https://www.instagram.com/zylahealth/
Visit our website: https://zyla.in/ova-pentacare-pregnancy-program
Talk to us on WhatsApp — https://goo.gl/kjofP
0 notes
Text
"The Army’s height and weight requirements are laid out in Army Regulation 600-9, the guidance for the Army Body Composition Program, which dictates how much a soldier should weigh depending on their gender, height, and age. If a soldier doesn’t meet the standard on that body mass index (BMI) table, they have different parts of their body measured as part of the tape test...
... To meet those standards, service members often adopt unhealthy behaviors like starving themselves, working out excessively, taking diet pills or laxatives, or sitting in saunas for prolonged periods of time to drop weight quickly. An Army major who struggled with bulimia for years said taking drastic measures ahead of weigh-ins is “so common that nobody looks at it as weird,” and while “people will fully admit it’s happening … it’s never discussed as a danger...
... the rate of anorexia and bulimia were higher among Marines than the other services. One study estimated almost half of U.S. service members reported at least one experience with weight stigma in the military in 2017, noting that stigma is “associated with harmful thoughts and behaviors, including diet pill and laxative use, purging, and overeating.” Those behaviors fall into a category of “disordered eating.”
...these habits don’t happen only among young service members, or just women. The problem extends to men and women, officers and enlisted, from new lieutenants to senior non-commissioned officers...
...getting taped is in Army regulations and not technically considered a punishment, there is an overwhelming negative stigma attached to it. Every service member interviewed by Task & Purpose described a certain amount of shame that went along with the practice, summed up by a first lieutenant... who has heard soldiers say “all the fat kids need to go get taped.’”
To say only “fat” service members get taped simply isn’t true. The test equally punishes muscular men and women and service members whose body types don’t fit the required measurements. That problem was highlighted in March by The Army Mom Life, an advocacy group for mothers in the Army, in a slideshow that showed photos of women and their height and weight results. The photos show women who appear muscular and fit, yet surpass their table weight and in some cases barely meet their body fat percentage requirement.
As one soldier noted on her photo, the terror over being taped has made her rethink strength training, opting to reduce the weight she tries to squat since she would fail if she gained 1.5 inches on her gluteus muscles.
“I am perplexed by the idea that we are asking women to gain muscle, and then we use a tape that measures that muscle (gluteus) and punishes them for increasing the size of that muscle,” she said.
An Army sergeant first class at the Pentagon said that despite excelling on his fitness tests, he’s a naturally “stocky guy,” and the tape test has been the “only thing that’s ever threatened my career.” He had good reason to be worried. If someone fails to meet the height and weight requirements, and fails the tape test, they are put on the Army Body Composition Program. They’re given a maximum of six months to show “satisfactory progress” in losing weight, which the Army defines as three to eight pounds a month.
If a soldier fails to be within weight standards by six months — and it is not due to a medical condition — the soldier will be separated from the service. The Marine Corps has a similar policy, which says Marines who have not made “satisfactory progress” within those six months will be processed for administrative separation.
Aside from the threat of separation, there’s fear that news of a soldier failing height and weight could damage their reputation. The Army major remarked that “so much of people’s reputations are on these silly” tests.
“If word gets around then it’s going to professionally affect you,” he said. “Even if it’s something you can pass, it’s still just the fear of that possibility.”
The sergeant first class added that he experienced harassment while at the Drill Sergeant Academy because even though he passed tape, he looked bigger than some of the other soldiers who “all fit a very particular mold” and were “fairly skinny people.”
Other soldiers interviewed by Task & Purpose echoed that sentiment — saying the Army is holding onto an antiquated view of what a “good soldier” looks like, which they say often translates to a thin “runner’s body.” Even the Army’s own standards lean on a subjective appearance; the service’s body composition program regulations say that commanders “have the authority to direct a body fat assessment on any soldier that they determine does not present a soldierly appearance.”
... Marines can be assigned to the program even if they meet height and weight standards...
... There’s also an argument that measuring someone’s health with BMI is not only outdated, but biased towards anyone who is not a white man...
... Experts also say it’s not accurate. Velasquez... said BMI doesn’t take things like muscle mass, cardiac health, or metabolic health into consideration, which she and other experts agree are more important indicators of health. (For context, Dwayne “The Rock” Johnson was considered “obese” according to BMI standards, Men’s Health reported in 2015.) “When we’re testing our service members on these standards, it’s kind of a one-size-fits-all that does not fit who we are as a nation anymore,” she said.
The tape test, which is conducted if a service member is over the regulation weight, is not much better. Lampert called it a “terrible” and “notoriously unreliable way to measure body fat.” Notably, a Military Times study of the tape test in 2013 found it was inaccurate in measuring body fat for 10 out of 10 active duty service members. Dr. Jordan Moon, the director of the Sports Science Center Research Institute, told Military Times the tape test “can vary by as much as 15%.”
“So, if your results show you’re 20% fat, that means there’s a 95% chance that you’re really somewhere between [five] and 35% fat,” Moon said.
One of the most common criticisms of height and weight standards is that they are often enforced differently depending on the unit, your leaders, or the person administering the test.
“You go in there potentially about to end your career or start the downfall, and it’s all dependent on how this person is going to tape you,” the major said. “You could have different people tape you … how are they actually positioning the [the tape]? How tight are they squeezing the tape, some people say you’ve got to put your shoulders up, or are they making you stand normal? What are they letting you get away with? And there’s so many little tricks — I’ve seen people hit themselves in the neck thinking it will kind of cause it to swell up, or they’ll put their tongue at the top of their mouth … If you can get your neck bigger and your waist smaller, then you’re giving yourself every possible advantage.”
A Marine Corps staff sergeant and Army captain echoed that view, saying that it was not uncommon for men to focus on working out their necks in the days leading up to a weigh-in to help them pass tape.
The Air Force recently became the first military service to get rid of the tape test, though it’s still unclear what a new body composition measurement would look like; the Army and Marine Corps still swear by it. And in the Army’s case, soldiers say the existing standards and tape test aren’t accounting for the service’s new fitness test, which emphasizes building muscle for test events like the deadlift, standing power throw, and sprint-drag-carry.
“Fundamentally, the Army system for height and weight is broken,” said the captain, who is assigned to the 25th Infantry Division. “And the Army has a very toxic understanding of health, weight, and fitness.”
Ironically, the methods many are using to meet the military’s height and weight standards are hurting the physical fitness they’re supposed to support, and in the Army’s case, they know it.
Army regulations factor in the possibility that soldiers may be doing things to rapidly lose weight, and even details various “unsafe” tactics soldiers may be using to do so. In AR 600-9, the guidance for the Army Body Composition Program, the service urges commanders to allow a seven day period between taking the fitness test and taking soldiers’ height and weight because some “may attempt to lose weight quickly in the days leading up to a weigh-in.”
“This practice may result in the soldier being unable to perform his or her best on the [fitness test], if the two events are scheduled close together,” the regulations say.
...The Army and Marine Corps are currently studying their body composition programs.
... None of the service members who spoke with Task & Purpose advocated for no fitness and health standards, and Lampert argued there are plenty of ways to measure those things that are accurate and actually correlate to health instead of just looking the part."
Note: there's a bunch of links within the article to more information about almost everything, so please click through and click around if any part of this interests you.
#original post#american military culture#american military#task and purpose#support our military#weight#ed tw#male eating disorders#eating disorders#us army#united states navy#marines#eating disorder#food#bmi#race in america#race and gender#mental health#ed
41 notes
·
View notes
Text
Heads up, this is a long post, but it's important. Please read it. Some people may have been able to guess this based on the last couple of posts I've shared, but I figured I should make an official post about it here.
In January I got officially diagnosed with Moderate ADHD, Predominately Inattentive (for anyone who doesn't know, this is what used to be known as ADD, but it recently was grouped with ADHD because of the similar symptoms). What this means is I have a hard time focusing and paying attention, have problems with forgetfulness, but I'm not as hyperactive as other people with ADHD might be.
This isn't something that I've caught or developed, this is something that I've had all my life and it went unnoticed. I still remember getting in trouble when I was in elementary school because I was really slow at doing assignments and could never finish anything on time because I spent the whole time daydreaming instead. To this day I have a really hard time paying attention in lectures without daydreaming, doing something else like doodling or writing notes for a story, or getting very restless and fidgety.
How did I not get diagnosed until now? It's actually very common for women with ADHD, especially the inattentive kind, not to get diagnosed until they are adults. Girls with ADHD in particular go under the radar because of this stigma that ADHD makes a kid (usually a boy) super hyperactive and you can't get them to sit down and be quiet unless you give them a pill. Kids with inattentive ADHD are mostly just brushed off as ditsy daydreamers who need to get their heads out of the clouds, but it's not that easy. Sometimes, sitting down to listen to a lecture or get a task done is physically difficult.
I didn't get diagnosed until recently because I had been able to cope with my symptoms for the most part. I made decent grades, I had strategies to force myself to pay attention, I had study groups to go to where I had to make myself do work. The biggest problems I faced were that tasks took me so much longer than everyone else to do and I still daydreamed a lot, but even that was used to my advantage since I pursued writing fiction.
Everything that happened with Covid-19 and quarantine took away all the structure and routine I was used to, and my symptoms got worse. Then I moved out, got an apartment in a whole new city with whole new people, a job, entered a Master's program, all without an established routine to get my feet on the ground. Suddenly doing a reading for class or writing a 200 word discussion post was impossible, or would take me three times longer than everyone else did. It could take me three hours to read and annotate a 20 page article. I had major imposter syndrome, my anxiety got worse, I started having very bad depressive episodes, and I couldn't cope with anything anymore. This led to a decline in my physical health, too. I remember it got so bad I once went a week without showering because I either didn't have the energy to or I just forgot to.
I only ever considered ADHD after one of my friends who had been diagnosed with it recognized some of the symptoms in me and suggested I get tested. I did, despite people (including myself) trying to convince me there was no way I had it, and it came back positive. I also got diagnosed with Generalized Anxiety Disorder.
I'm not sharing this for people to pity me or worry about me. I'm fine. I'm getting help and learning how to cope with this, (and I've made a lot of improvements), and I'm hoping that when the pandemic is officially over and I can get a routine back in place it will be easier to manage. I'm sharing all of this to stress how important this is and I want to help raise awareness for it. People who weren't diagnosed and given treatment as kids often develop anxiety and depression because they have such a hard time keeping up with the pressures of everyday life. Statistically, the links between mood disorders and ADHD make adults with ADHD 14% more likely to attempt suicide than people without it, and it's especially bad for women. (Source here: https://www.usnews.com/news/health-news/articles/2020-12-29/adhd-raises-adult-suicide-risk-especially-for-women )
The best thing we can do to make those numbers go down is to recognize it and treat people for it before they develop those other disorders, and the first step is to get rid of the stigma that goes along with it. ADHD isn't always a kid unable to stay in their seat or blurting out in a discussion, (in fact, some of those kids may not even have it and are just disregarded and given pills to make them manageable, but that's a whole other issue).
ADHD is having 500 different thoughts running through your head at once that you can't drown out. It's spending days obsessing over whatever your hyper fixation is on and forgetting about your immediate responsibilities and relationships. It's having a decent vocabulary but forgetting most of it or mis-speaking when you're trying to write or talk to someone. It's experiencing a lot of stress and anxiety about tests or projects with time limits. It's forgetting people's birthdays or not talking to an old friend for a long time even though you miss them because they aren't there with you and your mind is on other things. It's procrastinating working on big projects because there are so many things to do now that something due not now doesn't feel as important, (then promptly getting extremely stressed out when that big project is due soon and you haven't even started on it). It's getting so overwhelmed with the things you need to do that you disassociate and can't get out of bed. It's becoming paralyzed with indecision. It's spending more time preparing for a task than actually doing the task. It's wanting to do your best but not having the capabilities to do it.
ADHD is hard to deal with, but it does not make someone any less of a person. I'm not ashamed of it, but I want people to understand it and learn how to work with people with it. People with ADHD aren't lazy or uncaring, they just don't think the same way as normal people.
39 notes
·
View notes
Text
The Evergreen Shonen Story

A short while ago, there were some online conversations about the popularity of shonen stories. Almost all of them are based around the experiences of youth and some adult fans wanted action-oriented stories based around their life experiences as adults. Reading stories centered on teens and kids as the main characters isn’t everyone’s cup of tea, I’ll admit that. But sometimes, I think shonen stories are somewhat of a reflection on what adults have been telling kids for years and how some/most of their advice has failed youth.
Life begins in the womb. We come out to a world of many possibilities. As children, we’re immune to bias until adults decide to tell us about the many differences of various people out there. Some adults may not care and have trouble dealing with their own pain, They may resort to substances like drugs and alcohol to cope. Under the influence of drugs or alcohol, these adults may start to abuse children and/or neglect them entirely.
There’s a term that relates to the overwhelming negative experiences of children growing up. It’s called ACE - “adverse childhood experiences.” Examples of such experiences include physical/sexual abuse, parent separation, physical/emotional neglect, and living with an adult with substance addiction. I look at a bunch of shonen flashback stories and many of the traumatic ones revolve around physical and emotional neglect.
Why is this important to acknowledge? Because some adults do a bad job in raising their children or guiding kids to become responsible individuals. We’ve seen examples of bad parenting in anime and manga. There’s also the fact that adults have been full of dreams themselves when they were kids, but have been fed advice on how the “real world” works. They’ve been told that they can’t make their dreams come true and/or they need to behave a certain way to get by. It’s a vicious cycle. A colleague of mine told me that when she sees young people with vision and a desire to smash the status quo end up being a part of the status quo themselves, she wondered if that’s due to those individuals seeing how hard it is and how long it takes to generate the change they want to see.
One of my favorite shonen characters in recent memory is Satoro Gojo of Jujutsu Kaisen. He was a student of Jujutsu High and ends up becoming a teacher there. Gojo is considered to be a prodigy, but he remains humble. He’s also willing to speak up to authority as he has gotten into disputes with upper school management over the fates of cursed students (particularly Yuji Itadori and Yuta Okkutsu) whose potential have yet to be realized. Gojo has once said that he needs to remind himself not to be a bitter old adult as he ages.
A good number of shonen stories drive the point that adults shouldn’t be bitter old ones. Or maybe more importantly, don’t be dismissive about teen experiences. I listened to a podcast a while back about loneliness and how much it affects mental health. There was a discussion point about adults ignoring teens that feel lonely with regards to dating. Here’s a quote from that discussion.
“The number one way that we do this (being dismissive of loneliness) in America is every single 30-year-old up completely dismisses the loneliness that a teenager feels about not having a significant other. Because once we hit 30, we realize that your 16 year old significant other is nonsense. It’s just nonsense. You’re gonna be in love so much in your life. You’re gonna love everybody. You’re going to date a million people. It’s gonna be fine. You’re going to realize how insignificant this relationship is.
The key word there is you’re gonna realize it. It’s a future thing for them. So when every 30, 40, 50, 60 year old looks at the 16, 17, 18 year old and says, oh, you just broke up with your boyfriend? Yeah, who cares? That’s a meaningless relationship. I don’t care. That exacerbates the loneliness. It exacerbates the disconnected feeling because it really, really, really, really matters to them.”
I honestly think adults being dismissive towards teens’ current experiences is one reason why shonen stories still resonate with many. We’ve all been through those times where adults just shut us down because ultimately, it doesn’t matter. Yes, there comes a point where we have to move forward. But a good amount of emotional pain stems from adolescence and it lingers. Most mental disorders begin to happen around those years. Unfortunately, most of us don’t know how to give back in ways that stop the cycle. I do think mangaka are trying their best to give back the way they know how.
Yet I think the biggest reason for the enduring popularity of shonen stories is friendship. We all know the Shonen Jump tropes - friendship, hard work and victory. All three are important, but friends are what really keeps us alive. The harsh truths are that hard work doesn’t always get you where you want to go and victories do come at the cost of important relationships. Over the years, I noticed that in my neck of the woods, friendship is frowned upon. When you’re ranking important relationships in life, first is your mother, then maybe your father, then your romantic partner, followed by your children. Friends are last. There was a nice read I found that listed a good amount of studies on the importance of friends (especially for those who are LGBTQ+ and faced stigma from immediate family).
We don’t live on an island, contrary to what neoliberalism says. Families aren’t enough. Friends are what keeps us alive and helps build our sense of identity.
Maybe the fans who want more mature/adult-centered stories with shonen action just want to see more nuanced stories about friendships in adult settings. Friendships are so hard to make and maintain as adults. There’s some glimmers of hope for those kinds of stories - in video games. Yakuza: Like a Dragon is a great example of an adult hero in a genre dominated by young protagonists, the Japanese RPG. The story is about a 42-year old ex-yakuza who gets exiled into a unfamiliar city and manages to make something of himself with the help of new friends he made there. It was refreshing because the whole cast were adults who were unemployed and/or stigmatized due to underworld ties. They managed to save Japan from a vicious political alliance with action elements that felt shonen at heart.
I’m all for more adult-centered mainstream shonen stories because seinen material can be a bit too blunt for some tastes, but there’s a lot of focus on the mindset of youth lately than in decades past since there’s concern on how they will manage in a world that continues to disappoint them.
I love shonen because I honestly don’t feel like I’m an adult due to my depression. My development felt stunted. I feel that I have more in common with 20+-year olds than people my age. I want to be around people who are youthful at heart. I wonder about those who still enjoy shonen past the target demographic - what still draws them to it? Is it due to them embracing their inner child more likely than most people? Or do they just like to follow simple action stories that have a lot of heart (something that some people don’t have)?
Looking at shonen’s enduring mainstream status does make me think about the the feedback loops between adults and teenagers. I’ll end this by talking about an incident that happened a couple years ago where a somewhat prominent Anitwitter figure (I am NOT going to mention their name here, but you may know who I’m referring to), who made a lot of friends with people in the anime/manga industry, was outed be a sexual predator who went after young naive anime fans at fan conventions. One of the reactions from someone that was once close with them was how can older anime fans better connect with younger anime fans when needed. I know from personal experience, I sigh on seeing the behavior of teens at conventions at times. But I learned that by saying things like “Kids are so dramatic,” “Boys will be boys,” “She’s being emotional.” gets harmful in a hurry where proper context is warranted. Maybe they are being so-and-so, but it doesn’t hurt to ask and give validation to their concerns. Teens are the lifeblood of anime conventions right now.
Shonen is a gateway introduction for youth on how to process pain in a way that helps themselves and other people with the help of said people. It’s an escape from the distress and trauma of reality. That reality, which has situations like the incident I mentioned, is controlled by adults who don’t always have it together, can’t admit their flaws, and sadly take it out on the world. That’s why shonen is still so powerful today despite all the criticism the genre gets. And that’s the evergreen truth.
25 notes
·
View notes
Text
Something that’s been bothering me lately is the take that “mental health is as important as physical health, and society doesn’t recognize that. you wouldn’t make your kid go to school if they were physically sick or in pain, and if you were physically sick, you could call in sick to work, so why can’t we do the same with mental health as well?”
and normalizing mental health, wellness, and caring for and accommodating mental illness is very important, yes, but i also feel like this very much discounts the absolute neglect that society has for physical health
because honestly? there are a lot of parents who will send their kids in to school if they’re sick. college students are expected to go to lectures often with anything short of puking your guts up all day, because in a lot of places, you’re paying good money for that and can’t waste it. in retail and customer service, you’re regularly called in to work while sick, not allowed time off or to go home if you are. many minimum wage workers don’t get paid sick days, don’t know how to get them, etc. i know that there are provincially legislated sick days but how do i claim it? no one explained that to me. if you’re sick for too many days you risk losing money or your job; your boss probably shames you for taking time off for physical appointments and physical illness, unless you have a good career position and a good (read: probably unionized) workplace and boss.
and permanent disability and chronic illness? forget it. good luck. illness and disability are supposed to be temporary things, according to abled people. pain can be handled with tylenol and advil, and if not, three days off work and a prescription painkiller until the issue is solved. a broken bone or bad joint is healed in six weeks or so. anything more than that and you’re considered lesser, faking, to be severely pitied or outright disdained for not being a model, healthy citizen, apparently. you’re either lazy, a faker, a freeloader, or not trying hard enough.
i think that a lot of younger mental health advocates seem to think that the worlds of mental health activism and physical health activism are completely divorced. when i was learning about mental health advocacy, those were comparisons that i accepted without question: “you wouldn’t be asked why you weren’t coming to work with the flu, but you’re shamed if you don’t come to work because of severe depression or a psychotic episode”. but that’s often not the reality. “you wouldn’t deny someone mobility aids like a wheelchair or cane or walker, so why would you deny them pyschological/psychiatric aids like medication and therapy?”
in the beginning, a lot of physically abled mental health advocates seem to be under the impression that physical disability activists have created a strong and solid framework for activism, that they’ve been allowed to do so and that legislation and stigmas around disability and physical health have been erased. and young mental health advocates believe that they’re working with that framework, that they believe already exists, when it often doesn’t. they’ve been told that mental health is like physical health and physical disability, but the only reason people don’t treat it as such is because it’s invisible.
but what about chronic pain? what about early stage cancer? what about PCOS and endo and chronic fatigue and fibromyalgia and COPD?
these often aren’t more respected by people just because they’re physical illnesses. i’d actually hazard to say that a lot of people right now have a better understanding and greater sympathy to common mental illnesses and conditions (anxiety, depression) than they do to a lot of invisible physical illnesses and disabilities.
this isn’t to say that mental health advocacy is bad, or that it’s stealing resources or thunder from physical health advocacy. this isn’t to say that there isn’t still stigma surrounding mental health, particularly conditions that people perceive as being dangerous (psychosis, schizophrenia, personality disorders). this isn’t to say that mental health advocacy and physical health advocacy don’t have distinct needs and aims that can’t be lumped together all of the time.
this is to say that a lot of younger people who consider themselves to be advocates or activists for mental health should have a better understanding of the situation for people with physical illnesses and disabilities before comparing mental health struggles to the perceived successes of disability activists, when legislators and capitalism are more than happy to ignore the needs of physically disabled people as well as people with mental illnesses.
edit: and this isn’t even to start talking about psychosomatic conditions, which perfectly walks the line between physical and mental ableism!
19 notes
·
View notes
Text
Why women with PCOS are most vulnerable to mental health problems?
Polycystic Ovary Syndrome (PCOS) – a lot of women of their reproductive age are affected by this common endocrine heterogeneous disorder. The most known symptoms of this hormonal disorder are abnormal or absence of periods, obesity, infertility, excess growth of hair on the face and body, and acne. Not all PCOS-affected women experience all the symptoms associated with the condition.
Along with the above-mentioned symptoms, some women are subjected to depression, anxiety, and other mental health problems. These numbers are on the constant rise, but they are often overlooked and left untreated.
How PCOS affects the mental health of women?
Well, recent reports say that the women affected by PCOS are three times more prone to anxiety and depression than women without PCOS. PCOS is a condition of abnormal hormones, some of which increase the risk of psychological problems. Their morals, the cultural values of the society, and the burden for a perfect look can all affect the emotional well-being of women affected with PCOS.
PCOS & Perfect Looks
In women with PCOS, the male hormone called Testosterone is found in abundant levels and they cause abnormal changes in their physical appearance like excess growth of facial hair, acne, or loss of scalp hair. Women are always obsessed with good-looking faces, and their beautiful presence before society and anything that takes a toll on these are considered not worthy. These women feel less feminine and are reported to have low self-esteem contributing to emotional imbalance and depression.
PCOS & Obesity
One of the main symptoms that tag along with PCOS is obesity. Due to the hormonal imbalances, most women with PCOS are insulin-resistant, i.e., their bodies do not use up the glucose like how they normally would. These excess levels of insulin, instead of burning the fat make them get stored in your belly. Due to this reason, women with PCOS gain weight which disturbs their interpersonal relationships leading to anxiety and panic attacks.
PCOS & Infertility
Because of the increased level of male hormones and abnormality in reproductive hormones, women with PCOS do not ovulate. This causes irregular menstrual cycles and since there are no eggs for fertilization, women with PCOS find trouble in getting pregnant. Infertility can be physically, emotionally, and financially draining for couples, who often need assisted reproductive techniques to get conceived. This can cause prolonged stress leading to depression.
PCOS & Insomnia
Women with PCOS experience a much serious problem called Sleep Apnoea. A person with sleep apnoea will stop breathing for a shorter amount of time during their sleep. Because of this and constant worrying about other symptoms associated with PCOS, the affected women feel trouble falling asleep. Lack of sleep disturbs the mental state leaving the patients with hopelessness and cause serious health issues like psychological disorders and depression.
Ways to improve your mental health despite having PCOS
If you notice any changes in your mood or feel anxious and depressed, discuss it with your doctor to get medical treatment as a cure. We should also understand that the symptoms of PCOS are very much related to one’s lifestyle and making some modifications can help in controlling mood swings, anxiety, and depression.
Daily workouts not only help in maintaining a healthy figure but also release happy hormones called endorphins which are responsible for mood lifting and mental peace.
Alternative therapies like yoga, breathing exercises, meditation, and acupuncture are known to reduce depression and anxiety among women with PCOS.
Following a healthy diet and avoiding foods that increase insulin levels in the body can help in reducing the extra weight.
Friends and family to have your back is a great support and motivation to emerge successfully from the psychological effects of PCOS.
The doctors can prescribe medications for the depression after taking consideration into the other symptoms you experience. Some antidepressants are known to cause weight gain. So, express your concerns to the specialists before you assume medications on your own.
Supplements like omega fatty acids and vitamin D are reported to relax the mind and reduce mood swings.
Message from Bliss Naturals
In India, most women tend to ignore the mental symptoms and experience stigma around them. They do not take the issue seriously which may lead to non-restorable consequences. Lack of confidence, poor self-esteem, loss of sleep, frustration due to the trouble in conceiving, and having negative thoughts can even trigger suicidal thoughts in women with PCOS.
Proper self-care is very important and there is nothing to feel embarrassed about reaching out for help in adverse times. After all, PCOS is just a disorder and with proper treatment, you can reduce the symptoms of PCOS and depression and lead a blissful life.
3 notes
·
View notes
Text
So I’m suuuper late to the party, but I finally, finally finished Rhythm of War.
I am delighted by it. Thoughts and reactions under the cut, just in case for spoilers.
OKAY SO I had a lot of feelings about this book, and I wanted to be able to sit down and read the book properly and devote time to it, instead of sneaking paragraphs here or there during work breaks. So that’s why it took me so long to read it. In a way I feel like a terrible fan for taking so long when I was so excited about reading it for over a year, but in another way I am satisfied that I did it justice.
General thoughts/reactions:
I am legitimately impressed with how well Sanderson handled Shallan’s Dissociative Identity Disorder. DID is one of those mental illnesses that gets butchered so hard in media, and carries such a stigma of being “evil” or “creepy.” But Shallan’s representation seems much more factual in terms of how we know DID works today, including but not limited to:
Created from a severe trauma at a very young age, in which the brain starts splitting itself in order to protect against traumas and form survival mechanisms
Alters exist to protect the system and handle tasks for the host that the host cannot handle. Both Veil and Radiant handle tasks/functions that Shallan can’t
Also establishing that different alters can have different skills (such as Shallan being good at drawing and Lightweaving while Veil is bad at it, or Radiant handling espionage poorly)
Establishing that actual DID treatments do include encouraging alters to learn to work together and establish communication lines between each other. I like that the three create a pact to work together and rules to stand by and enforce them on each other to the best of their ability. They mess up sometimes (Radiant killing Ialai, Veil forcibly taking over sometimes). But they try.
But also establishing that prior to Shallan’s realization of what was happening at the end of Oathbringer, each of these alters had their own memories and ways of handling things and did not necessarily communicate with each other
Establishing that multiple times in prior books when Shallan thought she was ‘acting’ she was actually Blending with another identity, either Veil or Radiant. This becomes more apparent when Veil or Radiant actively discuss being the ones to do things that were previously from “Shallan’s” perspective (such as Veil learning slight of hand/etc at the beginning of Words of Radiance). This stuck out to me as especially interesting since accounts of people with DID often mention not knowing they have it or are switching for years, but being semi-aware of doing things differently than normal.
Veil being a protector-type alter and a trauma holder is extraordinarily common in DID cases and made an absolute ton of sense. It also suggests that she’s been around for YEARS longer than before Shallan ‘created’ her which, again, is not uncommon with DID cases
Veil, at least, also acts like she’s much older than Shallan, even calling her things like ‘kid.’ While Veil is, of course, no older than Shallan, this is completely accurate that alters can have different ages and even different genders to the host body in terms of how they perceive themselves
Establishing that fusions/integrations are possible, with Veil being ‘absorbed’ by Shallan at the end. This is a part of DID treatment and I like that it was handled in a way where both alters consented and the trauma was released, but it was handled. Even if Veil developed additional skills over time, it’s clear her first and foremost job was as a trauma holder alter, and once the trauma was no longer being hidden, her ‘purpose’ was done. And now Veil is a part of Shallan, and the expectation is that somewhere down the line, Radiant will join too.
Very very VERY VERY importantly, establishing Shallan’s interaction with other characters as a system with DID in a way that did not make her look like she was ‘crazy.’ DID is super serious and systems are often stigmatized. But I adored that Adolin is supportive and treats each alter on their own playing field (and even seems to be able to recognize them without Shallan changing hair color). I love that other characters like Kaladin admit they don’t exactly get it, but do their best to be respectful of it anyway. I love that nobody treats Shallan like a freak and sticks her in a padded room, and that people DO respect her wishes and treat Veil and Radiant as equally viable people. I love that it’s treated so healthily.
Honestly my only real ‘hmm, not exactly like that’ moments were thinking back on how Shallan ‘created’ personalities. Veil being a trauma holder for Shallan’s old memories implies she’s been around for a long time, so she wasn’t really “created” in that sense, just given more of a face/name. But Radiant appears to have been created spur of the moment when Adolin was all ‘hey, let me teach you to swordfight!!!’ To the best of my knowledge people with DID don’t really have control over when they split, nor do they really get to actively ‘design’ their alters. It’s more like alters form as needed to handle something. But considering how accurate everything else is, and that possibly this is just Shallan’s way of handling her splitting in a way that makes sense to her, I’m willing to give this a cautious pass.
Also maybe lost memory moments. People with DID generally can lose time. Shallan doesn’t seem to, but then towards the end we also see she’s not a reliable narrator in her own right, since somehow Radiant managed to kill Ialai when we’re reading that passage. So it’s possible we the readers are missing things because Shallan is, too.
That said, the way DID works, it will never really go away even if Shallan does fully integrate. I’m curious if more alters could form down the line. I thought this had been happening with ‘Formless,’ but Formless didn’t turn out to be another alter so much. Oh well.
I had wondered about Shallan and Pattern’s bond for a while, and I’d been wondering if maybe she had a different spren ever since Pattern mentioned he could go away or she might kill him too back in...Oathbringer, I think it was? It seemed strange to me that Shallan wouldn’t have seen him around for a long time in his pattern form, or that she’d get chased by so many cryptics in book 1, if she’d been bonded to him this whole time. Or that she had a shardblade she could summon in book 1, but Pattern hadn’t been established as a character yet. And then when Adolin met a deadeye Cryptic in Shadesmar, I was like, ‘damn, that’s Shallan’s first spren isn’t it.’ And I was vindicated. I feel stupidly proud of myself for catching even one of Sanderson’s twists.
I think this is the first book in the series where Kaladin’s arc didn’t really grab me as much as the others to start. Not that it was bad, I still really enjoyed it, especially towards the end. But I was surprised to find when I got to Part Three and Kaladin’s name was listed but Adolin’s wasn’t that I went, ‘awww, damn,’ and used that as my break point for the night.
I think part of this is that so much of Kaladin’s story that I love and adore is about not just Kaladin, but Kaladin’s friends and found family arcs with Bridge Four, and so much of that was taken away from him in the early part of the story. Like Kaladin, I guess I was just sad about everyone moving on and him being along. Sigzil going off to be the new Windrunner leader, Rock leaving, Rlain leaving (for a while at least), Adolin and Shallan leaving...it was hard. I felt his depression. Unfortunately, it made it a bit difficult to read, I guess.
On the flip side though, Kaladin’s ending arc in the story was A+ and I loved it. I love that his Fourth Ideal is specifically accepting that he cannot save everyone, which is something he’s struggled with from his very first appearance in the very first book. I love how this sheds so much light on that moment in Oathbringer where Syl is calling for him to speak the words and he just can’t, because at the time, he wasn’t ready to accept that he couldn’t save everyone. I love that he admits to Dalinar that he really did need help and a chance to recover, and that his setup for the next book doesn’t seem to be as Stormblessed, the soldier, but as a healer. And I love that he made up with his dad in the end, and did manage to at least save him.
ROCK. NOOOO.
TEFT. NOOOOOO!
And yet as always, Sanderson books are the only books where I really feel...ok with character death. It’s sad, for sure, but also deaths have purpose in his stories. Nobody is killed meaninglessly.
I think my favorite arc was Adolin’s, throughout the whole course of the book? I can’t help it. I love my enthusiastic, optimistic himbo who is just doing his best. Every time he was like ‘well I’m useless since I’m not a Radiant, but I’ll do the best I can’ I was like NO, HONEY NO, YOU’RE SO IMPORTANT, DO YOU UNDERSTAND HOW IMPORTANT YOU ARE REALLY? Look at all the people you help!!! Just look at them all!!!
As stated earlier, I love that he’s just so damned supportive of Shallan’s condition. Even if they don’t have words for ‘DID’ in Roshar or even understand it in their own terms, he’s just so damn supportive. She tells him she’s got multiple alters and he’s just like ‘cool, how can I help.’ He loves his wife. He’s friendly with Radiant. He’ll share jabs with Veil. He just wants to help, always.
I love that he’s so supportive of Kaladin too. I adored towards the beginning, where Kaladin’s going into a depressive spiral, and Syl gets Adolin because Adolin is one of the few people he can’t intimidate. And I adore that Adolin is supportive, but in a way that shows he gets it. He knows it’s not safe to leave Kaladin alone with himself and refuses to let that happen. But he also doesn’t force him to participate and acknowledges that yeah, you can feel like shit, and that’s ok, but you’re gonna feel like shit around other people, because it’ll help you. And it does. And I love that a thousand pages later Kaladin starts going into another depressive spiral and happens to mention, ‘fuck, Adolin’s not here to pull me out this time,’ recognizing what Adolin can do. I just love how much their friendship has progressed.
I love that he’s still so supportive of his brother, even if Renarin was barely in this book. I love that he even briefly defends Renarin against Shallan, even when he recognizes she doesn’t really mean any harm.
I adore his continued arc with Maya. I love that he was so excited to go to Shadesmar so he could see her again. I love how he’s clearly had offers from spren or other Radiants to talk to spren about bonding to him, and he’s like, ‘nah,’ cause he’s loyal to her. I love how everyone keeps insisting ‘deadeyes can’t speak, deadeyes can’t feel’ and he’s just like, yes?? Yes they can??? Have you ever fucking tried??? I love that it’s his genuine connection to Maya that helps her recover enough to actually talk on her own with more clarity, and how she’s clearly coming back to herself. And what a revelation, that Maya and the others deliberately sacrificed themselves. And I love that ultimately it’s his bond with Maya that gives him success with the honorspren. He did this his own way, with his own skills, in a unique way that nobody else has ever done before, because maybe he’s not a Radiant in the shiny new sense of the word, but he’s the only person out there willing to treat his sword like a partner and show kindness to spren and that shows.
I also really do hope he works stuff out with his dad because he’s got every right to be angry but also, I want him to be happy :(
Ultimately I adore Adolin’s whole polarity, that he’s a masterful duelist and combatant, and has probably killed hundreds, and yet his best quality is his sheer kindness. He has really grown on me as a character since book one, honestly. I remember not liking him in book one. I still don’t, when I reread it! But in the rest, he’s probably second only to Kaladin as my favorite.
Venli. I remember not really liking Venli in earlier books. I thought Eshonai was cool, but Venli I remember just not really vibing with. Seeing her story really made her a lot more interesting to me though, especially since I love her whole gradual growth as a character. Openly admitting to herself that she’s a coward and just wanted to get attention against her sister...and then doing something about it to better herself. Doubting her abilities to do so and being uneasy about it the whole time, but ultimately doing it anyway. She’s a flawed character, but she’s a good character, and I grew to like her so much more after seeing her story.
Also, I loved Eshonai’s mercy at the end there. Fuckin yes. Bittersweet smiles all around.
Szeth-son-son-Vallano wore white on the day he was to kill a king, because apparently white is the listener battle color, it makes SENSE now
I am also veeery curious what is going on with Szeth, who wasn’t really in this book all that much. And I’m curious if ‘Sixteen’ in Lasting Integrity is actually his dad, because they sure drew attention to a hiding Shin man and then immediately never mentioned him again.
Raboniel. MAN. What a fucking character. I was fascinated with her from the beginning. I never knew exactly what to think of her, because we see her from so many perspectives. Leshwi, who has been established as possibly the ‘goodest’ and most sane of the Fused, openly tells us not to trust her. We learn she’s done terrible things in her lifetime, like trying to create a plague to destroy all of humanity, and one of her titles is just straight-up scary af. She learns how to really, truly, actually kill spren, which is terrifying. She tried to kill the Sibling, which is obviously Super Bad. And yet, she’s such a compelling character. She’s polite and reasonable, to a degree. Clever and enormously genre-savvy, but also blunt and to the point, knowing full well Venli is being used to spy on her and Navani is working against her and blatantly stating so. She’s so intelligent, and is willing to both respect Navani and work with her to create things together, and recognize her worth. I never fully trusted her at any point, because we know she’s done so much to be scared of, but man, I enjoyed reading her segments so freaking much. I was sad when she died, and her weird frenemy relationship with Navani was really intriguing.
I really enjoyed Dabbid’s little segments. I’m so happy he’s comfortable talking around the others. I’m also happy to see Sanderson delving into including more autistic characters in different points on the spectrum, while also showing other people treating them well.
Taravangian. I still don’t know where to stand on this guy and I’m very nervous now that he’s basically a god and apparently smart enough to outwit everyone else again. I was excited when he actually managed to kill Rayse but fuck, we might have been better off with Rayse.
SOMEBODY ACTUALLY MANAGAGED TO OUTWIT HOID AND I’M SCARED AF AT WHAT THAT MEANS
Moash. I just. Fuck. I don’t even know. I’m not even sure if this counts as him killing under his own power or not. He doesn’t really want to take responsibility for his actions, and as long as Odium takes his pain and feelings, he doesn’t have to. But that moment when he wasn’t protected, he seemed upset with what he had done. So I really have no damned clue where his story is gonna go. But fuck, it’s scary how easily he almost undid Kaladin completely. He knew exactly what buttons to press. We’re lucky the Pursuer ignored him and attacked anyway, or he really would’ve won.
I’ll admit, my Cosmere knowledge is less than stellar, so I’m still not entirely sure I understand the stuff with the Heralds and Mraize. But I am definitely curious to see where it’s going on a surface level, at least.
LIFT USES LIFELIGHT that explains a lot. I wish she’d been in this story more because I adore her lol.
I know Sanderson announced Ace Jasnah a while back, but I love that it’s been so firmly established in the book itself. No beating around the bush or leaving people to wonder. She just straight-up says she’s got no real interest in sexual stuff and never really got how it drove others. I love it. I love seeing that so honestly and bluntly stated.
Anyway I’m sure there’s a lot more to be said but overall, A++++ as always, super adored, next one when????
8 notes
·
View notes
Text
Mental health stuff //////
So I finally got an appointment with a therapist - online, as the times require - after several months of trying to find one who both would take my insurance AND also know shit about ADHD - the last time I just picked a therapist at random, it was bad. She didn't want to believe my diagnosis because "I didn't look hyperactive" (a lot of adults with ADHD are not) and kept proposing stuff I just knew wouldn't work. Anyway, so this time I was determined better to advocate for myself and be clear about my issues.
The Dutch health care being ok but also a bureaucratic mess, I ended up going back to my previous treatment center because I didn't find anything else - the Dutch branch this time instead of the international brand. I was able to tell them directly that I felt the treatment was interrupted last time because they switched my therapist three times in a few months because of layoffs (...health care budget cuts, I guess...) and that I ended up giving up, which sucked even tho I was better.
The therapists were very nice (the older one looked like Cynthia Nixon, the other was a trainee). I was able to really get into the stuff that was hurting me, not just ...focusing on my studies/work situation being difficult. The tricky thing is that mentally, right now, I am not doing that bad. I have grown a lot more stable over the last few years. But I am also very much at an impasse in terms of getting where I want to be ; I feel stuck. Every time I try to go for something I really want, it sends me into a tailspin. So I made my world very small and easily manageable. Sometimes it's cosy. I have gotten better, especially this year when mental issues seem to have gotten much more visible and normalized, and mental health prioritized (I know how weird and paradoxical this is but there have been times I've felt quarantine was very close to my normal, the world was simply catching on). Better at taking it slow and easy and enjoying the little things, better at being mindful and working with the quirks of my brain. But...long term, this stasis is not sustainable. I am tired of seeing the same patterns crop up again and again, tired of all the anxiety and self sabotage. I have been running from the things I want and need to do. I know I want and can do so much more. I think it's time for some deeper work.
So, the big thing at the end of the session was that they floated the idea I might have borderline personality disorder. They're not sure, I have another appointment next Friday for deeper investigation. The tricky thing is that BPD and ADHD have symptoms in common and one can often be mixed up with the other - especially if you have both, which might be my case.
I am very ??? about it. On one hand if this allows me to get the help I need, then good. On the other, well, it is a bit terrifying, especially since the stigma for that one is particularly vicious. ADHD is often trivialized and misunderstood, but at least it's not demonized and is often considered pretty benign, sometimes even as a gift. Meanwhile, it's happened to me several times to hear people talking about how a person being manipulative/destructive/instable could mean they were borderline and how it was probably best to keep them at a distance/they were incapable of changing.
I can recognize certain symptoms (unstable sense of self, fear of rejection, mood swings, hypersensitivity, people pleasing, splitting) and others not really (impulsivity, excessive anger, fear of being alone, attention seeking, recklessness). And well, I have suspected for a long time that some people in my family might have it, and there is often a transmission factor ; at the same time I might have developed coping methods a lot earlier because of a familiarity with certain patterns of behavior. I spent a very long time developing the facade of being the reasonable girl. I have a very strong tendency towards stoicism and trying to be the strong one and solve my issues on my own. It might just have pushed this all down without really solving it.
I know it's possible to have a sub-clinical level of symptoms, too. I guess we will see. It's just put me in a very weird mood.
13 notes
·
View notes
Text
The Silver Screen Savant: Thoughts on Hollywood Autism, Pt. 1
When I was a child, I didn’t fit in.

A common statement, many people empathize with. However, to say “I didn’t fit in,” is a gross understatement. I stuck out like a sore thumb, and at times, still do. Now, why was this, you may ask? Well, there are things I could name. A banal little checklist of traits and characteristics would probably do the trick. But I’m not sure that would do it justice. So I’ll tell you what it felt like:
I had trouble reading facial expressions, because people’s face, and hands, and body would say one thing, while their words said another. Smiles that didn’t reach the eyes. Laughs that were a little too hearty, or loud, or hollow. Disingenuous conversations and actions frustrated me. If lying was wrong, why were, as my mother used to call them “little white lies” acceptable? Why did we smile and thank our new neighbors for their homemade casserole dish, before promptly throwing it away when they left? These things, and many others, puzzled me. But the thing that puzzled me the most, was interacting with my peers. I didn’t understand the sensation of a hundred million bees, pricking me with electric anxiety when I went to school, or played with children in the neighborhood. I didn’t understand why they weren’t constantly talking, wondering, asking- about everything. I didn’t understand how their minds worked. Most of all, I didn’t understand why it physically hurt me to look into people’s eyes, child and adult alike. On the other hand, I did notice they didn’t like me very much. “You’re weird,” they would sneer. Or “you talk too much.” And, they were right. I knew they were. Even as I would wax poetic about all sorts of nonsense, like the difference between a cocoon and a chrysalis. I knew. But I couldn’t…I couldn’t shut myself off.
And that’s just one tiny example, of a lifetime.
Back then, if you’d asked what was “wrong” with me, on a good day, I would have shrugged. Other times, when I despised every fiber of my being, I’d parrot back the sentiments of my peers. “Freak,” “loser,” and “r*tard” were words I heard often. And for a long time, I believed them.
Today, I know differently. Not to say the above struggles no longer apply. If anything, some of them are worse. But now, I now longer blame or hate myself for being different. Now, I understand.
The Lightbulb Moment

In 2014, my daughter began speaking. She was four years old. Before then, she could say “dada,” “juice,” “two,” and “go.” The rest was garbled noises, when and if she made a sound. Most of the time, she didn’t. My wife and I were concerned, to say the least. But it wasn’t exactly a new worry. My princess never crawled, never pointed to get people’s attention, or show them things, and did not play with toys. Plus a host of other concerns. So we hopped on Google, and after about, oh, half an hour of research, got in touch with a doctor. Now, I feel like I must add the caveat here that we wanted to have her seen before then. However, many issues (including a bout of homelessness) prevented that. So we were a bit…late, in that regard. No matter. Her doc sent her to a local play therapist, and after about fifteen minutes of interaction, the therapist knew exactly what was going on: Our little Princess was diagnosed with Autism Spectrum Disorder.
But wait! There’s more-
Once this became clear, my wife started looking into other things. Her own independent research, as it were. She kept it to herself for a month or three, then avalanched it all into my lap . Our Princess wasn’t the only one, as it turned out. And really, had I ever bothered to look…it was obvious. But I was in denial. I couldn’t possibly be autistic. So, like the stubborn Taurus I am, I dug my heels in. I refused to discuss it, for almost year. But, my beloved wife, who is much smarter and wiser than I am, knew what to do. In the name of “research for Princess,” she had me read a list of common autistic traits/symptoms. And it all came crashing down. I couldn’t deny it anymore. I was, without a doubt, also on the spectrum.
The gift of the Media: Fear, self hatred, stigma…superpowers?

Now, you might be asking, why exactly did I doubt myself? Cultural association, of course. And by “cultural association,” what I really mean is “the media.” Mostly, anyway. See, I’ve noticed a trend. In movies, tv and books, autism is usually presented in one of two ways: The Rainman, or the Idiot Perma-child, who cannot care for themselves. And I’m neither.
On the one hand, I was a straight A student. I could sleep through classes and make 100%. I was reading by the age of three or four, and I graduated highschool at fifteen. On the other, I have been known to go a full forty-eight hours without eating, because I “didn’t think about it.”
But I’m not the autistic person you see on tv. Now, that isn’t to say those people don’t exist. They do. For example, my daughter deals with much more noticable struggles than I ever have, while I have another member of my family (also on the spectrum) who is a certifiable genius. And I’ve known many others who are “obviously” autistic, whereas I pass as allistic* (see footnotes below) easily. Which is a sad discourse altogether, really. One the one hand, an “obviously” autistic person, what one might call “Low Functioning” (I could write a whole other post about why “low/high functioning” labels are harmful, however, for the sake of brevity, there’s some here, here and here) are often boiled down only to their struggles, where as people such as myself are relegated to “Not autistic enough to be my problem” or “well, you don’t look autistic.”
To quote-
“The difference between high-functioning autism and low functioning is that high-functioning means your deficits are ignored, and low-functioning means your assets are ignored.” -Laura Tisoncik
Why is this? As you might have guessed from the title of this post- I put a lot of it on the shoulders of the entertainment we consume. Nevermind certain hate organizations who swath themselves in the cloak of “advocacy” such as Autism Speaks, and Anti-Vaxcers, who think it’s better to have a dead child than an autistic one.*
I could go on. At length. However, I’m going to try and stay on track, just this once. To put it plainly, Hollywood Autism often works exactly like “high” and “low” functioning labels: We’re either uplifted to inhuman portrayals of superpowered savants, or downgraded to an “inspirational” invalid. In these stories, we’re props. The “Magical Disabled person!” as Tv Tropes puts it, there to uplift the neurotypical character from their adversity. After all, if this poor dumb sod (i.e- me) can be happy with their burdensome life, surely the pretty white able-bodied protagonist can! We’re “funny,” “scary,” or “sympathetic,” characters, who lack dimension, and nuance. We’re “inhuman.” We’re the lesser. Or at least, that’s one way it’s written. The other is the hyper intelligent, almost “superhuman,” and definitely super jackass genius, who’s much too smart™, and logical© to ever have feelings, friends or empathy. That’s it folks! That’s the show!
That’s what books, tv and movies told me, anyway. And what I truly believed for a long time. It’s why I cringed away in terror and shame when my spectrum issues were finally noticed. And why it took me so long to come to terms with it.
So, there you have it. Part 1. On the next episode, I’ll give some examples, both good and bad, and maybe even a little “what not to do,” or at least a “please consider real hard before doing this in your own work.”
If you like writing, talking about bad tropes and even worse marginalized representation, you can follow me at wordpress or at my “still has that new car smell” twitter. For now- thanks for reading.
-Your loving Vincent
*allistic= Non autistic.
*Vaccines do NOT cause Autism, however, if they DID, it would still be better to have an autistic child than one who died at the ripe old age of “easily preventable but deadly communicable disease.”
#autism#autistic spectrum#autistic problems#hollywood#vaccine#anti vaxxer#anti vax parents#writers on tumblr#writing#writers#tropes#trope time#ableist nonsense#ableism#media#actually autistic#social issues#childhood#social isolation#sterotypes#please dont do this
4 notes
·
View notes
Last Seen Blogs

karliexcruz
⠅⠁⠗⠇⠊⠑

anglibanmosogat
Örülök annak, hogy szeretek gondolkodni

shinobusupremecy
Shinobu supremecy

oderam-31
제목 없음

luxpup-blog
LuxPup