#anti-psych
Text
Been thinking about this lately but after my suicide attempt what I needed wasn't to be locked away and have my bodily anatomy taken from me for over a week but a hug, actually
#suicide mention#tw: suicide mention#tw suicide mention#anti-psych#anti psych#anti psychiatry#mental hospital#psych ward
56 notes
·
View notes
Text
A Patient-Therapist's Anti-Psych Manifesto
Okay yall, I broke out my laptop for this, so buckle up, I’m about to have opinions.
I don’t owe anyone my credentials, but because I know the first thing out of some folks’ mouths is always “what gives you the right” let’s nip that in the bud right now.
I have been in and out of psychiatric care since I was seven years old. I have severe medical trauma from the experimental treatments I was subjected to, and have spent time in outpatient, inpatient, and all manner of different kinds of care. I’m also a published anarchic anthropologist, and a fully credentialed and actively practicing private therapist. To many, these are rightfully mutually exclusive roles. To me it is survival. Let’s explore some dialectics.
Dialectic: Per Merriam-Webster, a dialectic is any systematic reasoning, exposition, or argument that juxtaposes opposed or contradictory ideas and usually seeks to resolve their conflict : a method of examining and discussing opposing ideas in order to find the truth
In this case, we’re holding a few irreconcilable realities in tension with each other and working to resolve those irreconcilabilities.
Dialectic 1
Creating a class of healthcare professionals whose job is to dispense care to the masses inherently creates a hierarchy.
Any hierarchy that exists can and will become unjust under enough stress, with enough bad actors, with enough systemic intersections, if it is made so, etc.
People still need healthcare, including mental healthcare.
Dialectic 2
Because we already have unjust hierarchies involved in our medical care and research system, the question of who gets to define what is “mental healthcare” and what isn’t is inherently skewed in favor of kyriarchical** values.
Kyriarchy: a social system or set of social systems built around domination, oppresion, and submission
Many non-hierarchical forms of mental health care are devalued in our society and therefore do not receive the resources to operate at scale despite being extremely effective tools.
There will likely always need to be some form of “service” healthcare model in our society, even if it is wildly different from what we have now, because the worst person you know deserves care and it may need to be from people who are incentivized to provide it, and in privacy or isolation from others in the community.
Dialectic 3
Indefinite and involuntary detention can never be ethically or humanely performed. Period.
Some people need episodic or long term intensive care that comes from having someone available to them 24/7, and this is extremely difficult to provide at scale to an entire society in their homes, and your answer cannot be to offload the work onto relatives.
Current inpatient and residential programs typically serve, at best a holding pattern, and at their worst are breeding grounds for abuse and we will be hard-pressed to create models that do not replicate this pattern in our current systems.
We could keep going several layers deeper, but this is already getting long, so now I want to ask the next question.
These all feel really impossible to work with, Butts, you said I was supposed to reconcile all this and that feels super intimidating. What do we do with these dialectics?
Great question imaginary reader!
There are a lot of things you can do about it! Start by going to the Blackfoot digital library and watching this video about indigenous influences on modern concepts of the basic hierarchy of needs (link)
One of the things I’ve learned as an anarchic anthropologist turned therapist is that if you take what we think we know now about mental health, the nervous system, and chronic stress, and look back to this moment when Maslow and the Blackfoot community tried to communicate the resiliency of their community to the world, we can learn a lot.
A huge amount of mental health care, in my experience, boils down to learning how to regulate your nervous system, provide for your hierarchy of needs in your life, including the accommodations you need for your physical, cognitive, spiritual, and social world, and seeking, traditional or non-traditional therapy, pharmacology, and/or traditional medicine for the remainder of your needs.
What I mean by this is: mutual aid is mental health care, socializing with your friends is mental health care, taking a bubble bath is mental health care
But so are practices like MAST (link)- a non-hierarchical therapy style that allows people to support each other through therapeutic interventions via mutual aid (a genuine therapeutic concept we discuss in our training!!)
I imagine a world where we dare to question all of our assumptions about what therapeutic intervention needs to look like. Where “mental health care” looks like creating a society that seeks to meet every level of need for as many people as possible, and offers additional, voluntary community built and operated services to meet additional needs that arise.
What if we worked to minimize the need for inpatient services by providing ADL support crews for anyone who requests it? Need to just be a lump in bed for a week in order to be okay at the end? Ask for a crew to come do dishes and make meals and tidy and field calls and check in on you. Feeling manic and need someone to be your impulse control? Request one. Like theoretically these are things we can all do for each other regardless, but what if there were trained volunteers from the community, motivated and available who could be on call whenever they were needed for anybody no matter what? What if you didn’t NEED to have a friend who was available? What if you didn’t need to wonder if they would be annoyed because everyone is there by choice and by specialty?
Imagine if you didn’t have to wait until you were in crisis to call? You could just do it because you needed or wanted the help and that was fine too. Because the goal was prevention. Make sure no one gets so overwhelmed or stressed that they reach crisis in the first place. Make sure everyone has community resources.
The task rabbit mutual aid is the one I think is the most under-served in our communities. I think a lot of us are still afraid to truly take that last step into anarchic community building. After all, time is the most precious resource we have, and giving that to others without a guarantee of others giving back feels very scary. When I’ve done task-rabbit type mutual aid though, it’s always been my favorite experience, and I truly cannot recommend it enough. It provides such an immeasurable boost to the entire community’s resiliency.
I think another really useful direction is teaching yourself a little bit about polyvagal theory. It sounds like pop science, but it’s pretty cool stuff. Things like diaphragmatic breathing, certain manual manipulation techniques, etc can help you regulate your nervous system in moments of stress or intense emotion, as well as adjusting you into a better regulated state over time if you experience chronic dysregulation, such as from PTSD, ADHD, or Autism**
**This is not me saying it will cure your ADHD or Autism, it will not, but it can tone down the intensity of emotionally/autonomically dysregulated moments, or make them a little easier to end on your own time.
In the end, mental health, like so much, is deeply personal. There will be no "one size fits all" option. But we can create a society that provides a high quality standard of living for everyone, with the majority of their needs being met as a baseline, and create services that account for needs that may be episodic, additive, or unusual, as will almost certainly always eventually occur.
So the question is, when you begin to imagine outside the confines of the four walls of the psychiatrist's office
What does mental healthcare look like to you?
114 notes
·
View notes
Note
Do you have any suggestions for an intro text on anti-psychiatry?
i think this essay--composed with the framing device of reviewing the DSM as a piece of fiction--is what really turned a corner for me personally on the topic.
The word “disorder” occurs so many times that it almost detaches itself from any real signification, so that the implied existence of an ordered state against which a disorder can be measured nearly vanishes is almost forgotten. Throughout the novel, this ordered normality never appears except as an inference; it is the object of a subdued, hopeless yearning. With normality as a negatively defined and nebulously perfect ideal, anything and everything can then be condemned as a deviation from it.
177 notes
·
View notes
Text
If you've been raised your whole life being abused and tortured and told that you're the problem, how the hell are you supposed to know that you're not? That those people abusing you are the problem and that it has nothing to do with you at all? How the hell are you supposed to know that things need to change if you never see any different and you're never encouraged to get out because something better actually really does exist out there?? That shit seems like a myth to us. We can be so stuck in this perpetual darkness simply because the environment we live in is hell bent on keeping us blind. Yeah okay eventually we find out about boundaries and are finally given a proper vocabulary to define toxic relationships, but is it really necessary for us to have suffered irrevocable damage & trauma before we find that shit out?? It's wild to me how far behind we are as a society that people still see mental health as useless and an excuse to throw therapy in your face as some form of moral punishment. Why are we still living in the dark ages with this shit.
#recovery#ptsd#trauma#mental health#healing#boundaries#mental health discussion#society#mental health reform#health care reform#mental health discourse#anti-psych#child abuse#personality disorders#cluster b#cluster b pds#bpd#avpd#npd#pd safe#toxic relationships#toxic parents#abuse#abusive parenting#codependency#reparenting#emotional regulation
20 notes
·
View notes
Text
so a couple weeks ago I told my therapist about my self harm. I initially phrased it as something in the past (it wasn't) to test the waters and he promised that he would never send me to a psych ward over it. I trusted him so the next week I told him that actually it wasn't in the past. he suddenly started asking invasive questions that I did not want to answer and that were not necessary for him to know like how I was self harming, how often, and when. I didn't want to answer these questions but I didn't feel like I had a choice so I did. it felt violating. we discussed starting DBT. he brought up the psych ward knowing it makes me panic.
the next week he immediately started with his self harm questions again and I shared. I had hope that maybe this would help. I confessed I was having a crisis, he brought up a psych ward again while knowing it makes me panic.
this week he started asking about self harm and I said I don't want to talk about it this week. that I was doing well but didn't want this session to be about self harm. he got angry, he told me I was resisting therapy and that therapy isn't supposed to be comfortable. he tried to pressure me into talking about self harm. I refused and brought up a different topic (conflict with my roommates that was resolved) he asked me how I felt about it. I said I didn't know. he asked me if I felt comfortable or uncomfortable and I said I didn't know. he told me I was resisting therapy again. I said that sometimes I just don't know what my fucking emotions are and he said "well you usually do" and I responded that well this time I don't. he continued to call if avoidance of therapy.
I jumped to a different topic again and tried to go over some of the stuff I had written in my DBT packet and he said I was avoiding therapy but jumping topics too many times. I finally got him to stop calling it resistance and he insisted I find a different word to describe my "behavior"
he started to interrogate me about "what happened" because I was such an easy patient a year ago and had much better mental health. he got accusatory, like I was hiding something, when I said that I didn't know it just happened. I'm just depressed. he said he has a therapeutic obligation to make sure I'm safe and tried to force me to "compromise" on talking about self harm. I said that we could check in at the beginning of the session and if I was doing well we could talk about something else and if I was doing poorly we could talk about self harm. I wasn't happy with this compromise and it felt like it was stripping me of my autonomy. he wasn't happy with this compromise either, he made the accusation that I'd just lie. instead he forced me to fill out a spreadsheet based on day with all of my emotions, when I self harmed, when I smoked, etc. it's a violating spreadsheet and I'm not doing it.
through the entire thing he was confrontational and accusatory.
I'm dropping him as a therapist. after 5 fucking years of trusting him he pulls this bullshit I'm so fucking upset
28 notes
·
View notes
Text
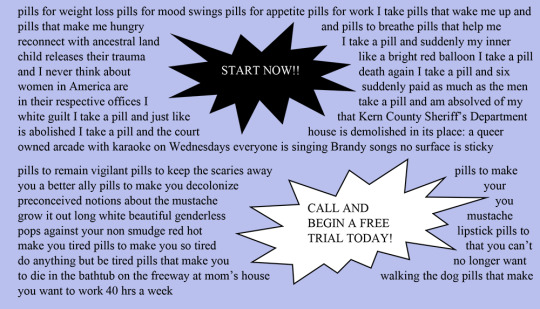

"Unskippable Pharmaceutical Ad", Shelby Pinkham
18 notes
·
View notes
Text
people hear that i'm anti-psych on a lot of levels and they immediately assume that it means that i hate therapy and that i think that no one should be allowed medical treatment and blah blah blah
but that's so wrong???
firstly) i prioritize completely informed consent and autonomy. a lot of health care professionals don't, esp in mental healthcare.
secondly) i acknowledge the good that mental healthcare can do, but the system is majorly fucked and trying to find good care that is what you need is like finding a light blue needle in a stack of dark blue needles; you end up hurt a thousand times before you even get close to finding what you need, not to mention that they all look pretty similar so you could end up with a dark blue needle and get fucked up w/o realizing it
thirdly) not everyone has/needs/wants mental healthcare. which is fine, until you need/have/want mental healthcare and people stop talking to you/crap on you/etc etc bc it's so stigmatized
fourth) look all of my points boil down to completely informed consent, autonomy, and how much the system sucks.
i'm not anti-people-getting-the-care-they-need, i'm anti-the-current-psychiatric-system. cause it sucks and is inherently biased and shitty and sure it makes progress but at a snail's fuckin pace which doesn't help the people stuck in it now
#disability#mental disorders#disabled#mental disability#mental health#mental healthcare#anti-psych#anti psych#anti a lot of shit the current system sucks in a lot of ways#and just because it's somewhat better than ut used to be#doesn't mean that we should stop pushing for reform
5 notes
·
View notes
Text
1. The beginning of ‘modern’ psychiatry – a descent into hell
This examination of the beginnings of modern psychiatry well into the first half of the 20th century does not provide us with momentous breakthroughs and heroic efforts to assist mankind. What we find instead is a subject based on speculation rather than science, unable to establish causes of mental illness and whose primary solution was to murder the very people it should have been caring for.
#psychiatry#false science#anti psychiatry#eugenics#anti psych#mental illness#mental health#anti-psych#anti-psychiatry
3 notes
·
View notes
Text
Tell me I’m wrong in saying psychiatrists are the cops of the mental health world. Say something wrong or offkey and they’ll send you to jail.
#alter: xiv#anti-psych#anti-psychiatry#for the record#hating psychiatrists doesn't mean hating medication#its just the truth
109 notes
·
View notes
Text
every mental hospital is a money scam they will just neglect and abuse u every almost every time i promise
19 notes
·
View notes
Text
genuinely have yet to hear what antipsych proposes to do with psychotic people who won't listen to reason who hurt others without either directly or indirectly infringing on the freedom of the psychotic people or fully placing the responsibility of staying safe with the victims (which will sooner or later get the psychotic people harmed as well)
2 notes
·
View notes
Text
another anti-psych post from your neighborhood patient-therapist
In my last post I talked about the kinds of basic needs people and communities have, and asked what it might look like in your community to meet those needs as a baseline. This time we're going to talk more about what happens when communities and individuals are chronically un-/under-served.
Okay so let's break it down this way. We're gonna try looking at just one medical symptom of chronic stress: autonomic dysregulation. It's not going to feel like we are, but I promise that's all we're doing. This is a *serious* symptom and it often comes clustered with others due to the way it functions within the body, which is why I think it is a useful case study here. Autonomic dysfunction, especially chronic dysfunction, can temporarily (though for long spans of time if the dysfunction remains chronic rather than acute) alter the functioning of other systems within the body such as the endocrine system, the reproductive system, cognitive functioning through the hippocampus and amygdala, and muscle functioning, nerve functioning, and others. It is no joke to suggest that long term autonomic dysfunction can often lead to major long term health consequences that are life altering for the person experiencing them. While some can be treated, managed, or even cured, not all can be and this is something I want us all to keep in mind as we consider the need for building communities that do not cause this kind of harm to their people.
Let's look at some potential medical outcomes of autonomic dysfunction, per the Mayo Clinic:
Dizziness and fainting when standing, caused by a sudden drop in blood pressure.
Urinary problems, such as difficulty starting urination, loss of bladder control, difficulty sensing a full bladder and inability to completely empty the bladder. Not being able to completely empty the bladder can lead to urinary tract infections.
Sexual difficulties, including problems achieving or maintaining an erection (erectile dysfunction) or ejaculation problems. In women, problems include vaginal dryness, low libido and difficulty reaching orgasm.
Difficulty digesting food, such as feeling full after a few bites of food, loss of appetite, diarrhea, constipation, abdominal bloating, nausea, vomiting, difficulty swallowing and heartburn. These problems are all due to changes in digestive function.
Inability to recognize low blood sugar (hypoglycemia), because the warning signals, such as getting shaky, aren't there.
Sweating problems, such as sweating too much or too little. These problems affect the ability to regulate body temperature.
Sluggish pupil reaction, making it difficult to adjust from light to dark and seeing well when driving at night.
Exercise intolerance, which can occur if your heart rate stays the same instead of adjusting to your activity level.
Some common comorbid conditions may include Diabetes, Polycystic Ovarian Syndrome, Parkinson's, Irritable Bowel Syndrome, or an autoimmune disorder. In each of these cases I want you to remember the lens of an individual body being denied, in some way, its base needs (an edocrine hormone, a nutritional component, the internal security of homeostasis, etc), to such an extent that it begins to experience an internal catastrophic failure, as this lens may often be supportive of accommodating your disabled comrades, or yourself, in the future.
I also want us to consider some common social statistics relevant to these conditions. Nearly 4% of the world experiences and autoimmune disorder. Most are women, and Indigenous, Black, and Latina women are at risk than most for several of these. In the United States, there are suspected to be 37.3 million people with diabetes. Diabetes is also considered an autoimmune disorder by researchers, and is one that the Indigenous, Filipino, Indian, Latine, and Black communities are all at higher risk for than white people are, however, risk is also heavily influenced by poverty, and by a family's location with respect to food deserts which grow more and more common. In a truly wild statistic, 80% of lesbians versus 32% of heterosexual women had polycystic ovaries in one study, and 33% of lesbians versus 14% of heterosexual women had progressed to PCOS. Some studies find that transmasculine folks are more likely to PCOS as well.
When we consider the marginalization these groups experience, and the way that marginalization plays out in the social forum, the political forum, in the financial forum, and in the emotional forum, are we really surprised to learn that it plays out in the embodied forum too?
This is what people mean when they talk about social murder. These are health conditions that don't just change lives, they end them. A system that churns out people so chronically sick that their bodies are desperately killing themselves trying to stay alive is a society that has become desperately sick. Diabetes is something we have attributed to individuals, to families, and even every once in a while to corporations, but at what point have we sat down and looked at a society that produces this murderous autoimmune disorder at such high rates and asked the real question: how are we making so many people sick?
The answers are many, and that can feel overwhelming, but I encourage you to start in one place and learn your way around it as well as you can before you even consider moving on. Maybe start with food deserts. They're probably familiar to you, you've heard about them in passing before I imagine, even if you're not really too into this stuff. But ask yourself WHY food deserts are able to exist? What are the mechanics of one being born? How does one stay free from the stain of a grocery store or food market? Are there any places like that near you? If so, what points of leverage might there be in that location for you to break the homeostasis of the food desert? How can you add your weight to efforts already occurring, or stir up sentiment around the idea of a new homeostasis where a grocery store exists? Can you put up flyers or attend town hall meetings? Can you knock doors or phone bank? Can you bring some sugar by your neighbors and comment how frustrating it is you all have to go so far to get your groceries and wonder what's up with that and maybe start scheming together? What kind of store should it be? Bring in a local market? A chain? Build a co-op or merchant's stalls for a four season farmer's market?
Get really into one idea, and get others in on it with you. I bet you aren't the only one who'd like a better status quo.
113 notes
·
View notes
Text
I think it's kind of important to recognize that Foucault was committed to an institution and subjected to psychiatry for attempting suicide on more than one occassion and having desires for self-mutilation -- all of which was attributed to his homosexuality, which was pathologized at the time.
Like, Foucault wasn't just some guy writing critically about the history of psychiatry from the outside, up in his ivory tower. He wasn't just some academic with no personal stake in the anti-psych movement. He was very much interested and involved, in part, out of personal experience.
And you know, death of the author, yeah yeah yeah, we can't really know his intentions or motivations, etc., etc. But I've seen posts on here being like: "I wish people would write about anti-psych from their personal lived experience, cuz all we have is these stuffy academic texts by people like Foucault" and its like... my dude, Foucault was very much not that. You just don't like reading philosophy. It's fine. You can just say that.
4 notes
·
View notes
Text
You learn, to your horror, that your friend intends not to die. Naturally, you call the emergency hotline, and medical professionals come to fix the obviously-irrational desire of this mentally-ill patient. Your friend receives a lethal injection, and their selfish desire to stay alive is fixed - well, not the desire itself, maybe, but at least they've been prevented from carrying it out.
2 notes
·
View notes
Text
your average 1830 classicist be like:

#we all have that one cousin#and if we don’t it’s bc we are the romantic cousin#no context#romaticizm(tm)#the anti romantic moral panics still wreaking havoc in the world’s population psyches i see u_u
5K notes
·
View notes
Text
people with personality disorders: it was difficult to survive on the ground, so i climbed in a tree and now im stuck and can’t get down
mental health workers (and everyone really): it seems that they climbed in trees to manipulate us. they are fully capable of getting down but doing so would make it harder to abuse us, so they stay there
#personality disorder#personality disorders#actually mentally ill#actually bpd#actually disabled#anti psych#cluster b personality disorder#cluster b#cluster b pds
5K notes
·
View notes
Last Seen Blogs

el-mismo-amor-la-misma-lluvia
"...infanta inquieta de sal nocturna..."

thaliacrawford
under construction.
thaliacrawford
under construction.

v4mprrr
meta-angel

kayarooo-blog
Mustafa