#al can have a little mental disorder as a treat
Text
.
#can we please stop making america evil or have trauma#i get it. i would be lying if i said i didn't project onto my scrimblos#and plus this is more like my personal opinion#but i am sooo tired of evil or incredibly mentally ill alfred#like AGAIN. nothing wrong with it.#al can have a little mental disorder as a treat#but it just doesnt FIT him ynknow
0 notes
Text
stop fakeclaiming child alters just because they aren't "accurate"
below is a comment found on a popular subreddit that fakeclaims dissociative and posttraumatic experiences. in this comment, they are referring to people with dissociative identity disorder and similar disorders who have "littles" which is a common community term for alters that present as children. if you are not familiar with child alters, please refer to this professional's explanation.
you can also find more information on how alters might present as different ages here. please stay informed!

as you can see in this comment, this person is criticizing how child alters type or speak because it's not accurate when comparing them to real life children. what they don't seem to understand is that child alters are not the same as real life children (howell, 2011, pp.60-61). they are part of a mental health disorder. and while child alters are often more vulnerable & traumatized then older alters, it's actually counter-therapeutic to treat them like they're no different from real life children (shusta-hochberg, 2004).
child alters are very similar to the concept of an inner child. your inner child is a part of you that preserves the things you remember, learned, fantasized about, and felt when you were a child. child alters are very similar to that, except they're more disconnected. dissociative processes involve them taking control of the body and acting independently.
child alters are often more limited than the adult alters...they "may not be able to tell the time, hold a pen and write, and they may only use and comprehend very simple language. these assets become even weaker when survivors become very afraid, angry, or ashamed" (van der Hart et al., 2006, pg.138). it is extremely common for trauma survivors to regress to a child-like state at times, even for people without child alters.
no matter how child-like someone becomes, if they are adult-bodied then they are not an actual child. the way a child alter acts or talks may be inhibited but is rarely fully "accurate."
it makes no sense to criticize an adult for...not being a child?
one of my alters is an infant. that infant alter is still able to type and communicate, although in a more limited way. they know how to unlock our phone & how to contact someone during emergencies. they don't write or talk very well, but they still know how to do it. if young alters had to act "accurately", i would be unable to communicate or understand phones or walk or stand up or even eat solid foods when that alter fronted. this alter fronting could end up killing us, so i would probably need a caregiver 24/7.
that isn't how things work, though. i'm an adult with a mental disorder, not a shapeshifter. the lack of compassion and critical thinking that some people extend to neurodivergency and trauma survivors is heartbreaking.
please stay educated on mental health! please don't fakeclaim someone just because their child alters aren't "accurate."
references
Alter ages. DID. (n.d.). Retrieved August 16, 2022, from https://did-research.org/did/alters/ages
Holland, K. (2019, August 30). Age regression: What it is, why it happens & when it may be helpful. Healthline. Retrieved August 16, 2022, from https://www.healthline.com/health/mental-health/age-regression
Howell, E. F. (2011). Understanding and treating dissociative identity disorder: A relational approach. Routledge/Taylor & Francis Group. https://doi.org/10.4324/9780203888261
Incest AWARE. (2021, February 24). How to reparent the child within: Healing the inner child after incest abuse. Incest AWARE. Retrieved August 16, 2022, from https://www.incestaware.org/post/how-to-reparent-the-child-within-healing-the-inner-child-after-incest-abuse
MSW, K. B. (2020, August 3). Understanding child parts in the dissociative system. Discussing Dissociation. Retrieved August 16, 2022, from https://www.discussingdissociation.com/2009/01/understanding-child-parts-in-the-dissociative-system/
Shusta-Hochberg, S. (2004). Therapeutic Hazards of Treating Child Alters as Real Children in Dissociative Identity Disorder. Journal of Trauma & Dissociation. 5. 10.1300/J229v05n01_02.
van der Hart, O., Nijenhuis, E. R. S., & Steele, K. (2006). The haunted self: Structural dissociation and the treatment of chronic traumatization.
#syscourse#dissociative identity disorder#dissociation#dissociative identities#dissociative alters#child alters#mental health awareness#mental health stigma
108 notes
·
View notes
Text
What Are The Children Truly Afraid Of?
Pediatric anxiety is the anxiety that children possess. However, it may be hard to distinguish when a child is exhibiting anxiety like symptoms. Some important things to look at is their behavior and the antecedents occurring right before the behavior starts. In the behavior is when the anxiety symptoms are most likely to occur. However, it does help to know some common antecedents that trigger the child’s anxiety as well as what their behavior looks like as a result from feeling anxious. Listed below are top 3 common anxiety triggers and top 3 common anxious behaviors. Lastly, after covering the triggers and behaviors of pediatric anxiety a specific program, ASU Compass for Courage, that helps aid these symptoms will be discussed at the end. Knowing is only half the battle and having resources to treat pediatric anxiety hopes to combat the other half.
Top 3 Common Anxiety Triggers in Children
Specific Phobias
Specific phobias is a mental disorder where a certain objects and situations cause anxiety upon seeing, or even hearing about the certain object or situation. According to the DSM-5 there are common objects or situations that looked out for when assessing for specific phobia (Sucheta et al., n.d.). Those objects and situations include flying, heights, animals, getting a shot, or seeing blood. However, for children there are other specific phobias that occur because of a traumatic event they experienced or witnessing a traumatic event happen in front of them. (Sucheta et al., n.d.). In some cases it won’t even make sense why they are anxious about the object or situation because the perceived to danger level of the object or situation to the child is either low or non-existent (Sucheta et al., n.d.). For instance, a child may have a fear of spiders and even though there aren’t any spiders present a Halloween decoration of a spider will cause them immense anxiety.
Some of the children may have a fear that may seem irrational to most. For instance, one 13 year-old girl had a phobia of money and her fear of money started at age 4 and is considered a very rare phobia (Banurea and Effendy, 2023). Now to most money is associated with good and get you the things you want. However, for this little girl her parents would tell her that money was the root of all evil and can lead to sin which started when she was 3 years old. (Banurea and Effendy, 2023). This was an attempt to allow the little to not request money often from her parents (Banurea and Effendy, 2023).
As far as anxiety triggers go, specific phobias can be easily identified in a child. However, an important note to take from when talking to children about certain objects or situations, especially at a young age. Is to make sure you explain to them in the best way you can why certain things are scary and should be avoided. Your explanation could potentially be the trigger for the child to get specific phobia about the object they should avoid.

2. Parents Fighting
When your parents are fighting it was never a fun experience. Sometimes it went unnoticed when we were outside playing. However, in some childhood experiences it would seem the parents would have no trouble yelling and being mean to each other while their children were present. The reason why some children may have anxiety around hearing their parents fighting is because in the past it may have resulted in one of the parents leaving home for days on end and the child never knowing when that parent would return. Or the parent would stay and when interacting with the child right after fighting with the other parent, take their anger out on the child by being mean to the child who did not do anything to the parent.

3. Getting Bullied
It’s no surprise that many children are getting bullied, especially in school. The issue is that many parents will not know that their kids are getting bullied. Even some teachers and school staff may not even see the bullying occur because of having to pay attention to too many children at once. However, even though the bulling may not be seen or noticeable it can still be a trigger just one that is harder to point out. In fact, according to one study where 550 children assessed the effects of bullying on their self-esteem, it resulted in the children who were experiencing bullying getting anxiety from the experience (Balluerka et al, 2023).
With a trigger like bullying, it’s more apparent when you look at the behavior of the child. Especially when it comes to them going to school or when interacting with certain kids that would point out that the bullying is triggering the child’s anxiety.
Top 3 Common Anxious Behaviors in Children
Somatic Complaints
When children get sick, they will tend to let people know by stating some of their somatic complaints. These complaints will consist of things like the child saying their head hurts, stomach hurts, or if you notice the child is wetting the bed a lot more or having less control of their bladder even though they know how to use the bathroom (Sucheta et al., n.d.). Sure, it may be a disease in their body so going to the doctor makes sense. But there maybe some psychological testing that needs to be done because the child may have anxiety and seeking treatment may remove these somatic complaints.
Children with ADHD tend to have a lot of anxiety and with the increase of their ADHD symptoms their anxiety and somatic complaints also increased (Bozatli et al., 2023). So, if a child is showing the behavior of somatic complaints, then a trip to the child psychologists might be needed.
2. Avoidance
With a child having anxiety one of the behaviors, they will exhibit is avoidance. Avoidant behaviors range from a child throwing a tantrum, or completely removing themselves from situations (Sucheta et al., n.d.). For instance, if a child needs to go to school and they are feeling anxious about going to school, some of the behavior that they will show is crying, yelling, and physically refusing to leave the house when it’s time to leave for school. Another example of avoidance is a child completely disengaging and removing themselves from what is causing them anxiety. For instance, if the child has to shower and you keep reminding them to take one, but they keep ignoring the request to shower and finding other things to do instead.
It is shown that individuals with Generalized Anxiety Disorder all reported higher level of avoidance than those without it (Newman et al., 2023). So if your child is showing a high degree of avoidance it's best to check and see if they have Generalized Anxiety Disorder.

3. Perfectionism
The last behavior a child will exhibit is perfectionism. When a child is showing traits of perfectionistic behavior, they will most likely display expectations that are considered unreasonable regarding their own performance and when those expectations are not met they will be very critical of themselves (Sucheta et al., n.d.). For instance, let’s say the child has the expectation to get 100%s on all of his tests and assignments and he receives a 98% on one of his tests. He will most likely be very hard on himself and say things like: “I must not be that smart if didn’t get a 100% on this test.”. Paying attention when a child vocalizes their expectation and how they treat themselves when those expectations are not met can help deduce that the child is experiencing anxiety.
If your child is displaying perfectionistic behavior it can lead to psychopathology in their adolescent years and young adult years and it is best to intervene early as soon as the behavior recognized (Lunn et. al, 2023).
ASU COMPASS for Courage
Now that we are aware what may trigger anxiety in children and what behaviors occur as a result of having anxiety some resources to help combat a child’s anxiety would useful. Luckily a resource like ASU COMPASS for Courage is a resource that will effectively help a child navigate the world with little to no anxiety. The ASU COMPASS for Courage was created by Dr. Armando Pina and Ryan Stoll, and it is essentially game like learning program that includes modules to help children struggling with anxiety. The program includes a total of 6 learning modules that have been proven to help children with regulating their emotions, get higher test scores and grades, improve social skills, gain confidence, and decrease in-class meltdowns. The game is meant to captivate the children with its colorful games as well keeping them engaged with the way the games are designed. It also allows them to build good relationships with other children. It is definitely worth investing in if you feel your child has anxiety.
Getting Bullied
Specific Phobia
Somatic Complaints
Avoidance
Perfectionism
ASU COMPASS for Courage
Overall, it's important to know if a child has anxiety mainly because if they are experiencing high degrees of anxiety they are most likely unhappy in their current state. I feel the one that gets overlooked the most is the somatic complaints. Mainly because issues like stomach hurting and headaches are associated with physical illnesses and most would probably stop if they find noting is physically wrong with the child. So it's good to do some psychological tests to make sure that anxiety is not the cause for the somatic complaints
Anyway that concludes the Top 3 Triggers and Behaviors for Anxiety. Did you learn something new? What behavior or trigger do think is the most common? And which behavior or trigger did you find the most interesting? Please comment and share the post so others can learn this information as well. Thank you.
2 notes
·
View notes
Text
Aging and Wellbeing
Welcome back to my blog series! Today, I will delve deeper into the intricate relationship between aging and health, particularly focusing on the unique challenges faced by Aboriginal Australians.
As we age, our bodies undergo various transformations, both physically and mentally. While aging is a natural part of life, it often comes with its share of health concerns. From chronic diseases like type 2 diabetes to heart and lung conditions, older adults frequently find themselves navigating through a maze of health issues that can significantly impact their well-being.
In a poignant study by Holly et al. (2023), alarming rates of chronic diseases were observed among Aboriginal Australians. These communities, marked by their rich cultural heritage, are unfortunately grappling with disproportionately high rates of conditions like type 2 diabetes and dementia—a mental sickness that poses unique challenges for both individuals and their caregivers.
Well-being for the indigenous group matters a lot as aging people of the indigenous group need utmost care and nurture in their older days of life. Finding more effective ways for Aboriginal communities to receive the health care they require. It makes recommendations for improvements to services aimed at enhancing Aboriginal health, particularly in older populations (Riitsalu et al., 2024, p.68).
Indigenous communities have longer life expectancies, which is reflected in the rise in the proportion of older persons with age-related syndromes and chronic health disorders. Indigenous peoples' aging health and well-being may be enhanced if certain modified lifestyle factors are addressed, as many of these illnesses are linked to them. A deeper comprehension of what aging well means for Indigenous people is necessary if models of healthy aging are to be promoted within health systems. Indigenous peoples see aging and health holistically, which perhaps sets them apart from Western conceptions.
Figure 1 below shows the rate of fatal and non-fatal diseases which are faced by the aging group of population among an indigenous group of people (ncbi.nlm.nih.gov, 2022). It is evident from the graph that the increasing rate of diseases among older people in this community risks the healthy living and well-being of the people. Therefore, it is mandatory to bring up certain interventions which would be efficient and effective for the better livelihood of older people. The most popular intervention which is found to be used is care homes which treat dementia patients with utmost care and attention (Coffey et al., 2023, p.21959). It is in these care homes that there are different policies and protocols are maintaining which are best suitable for mentally retarded or sick people.
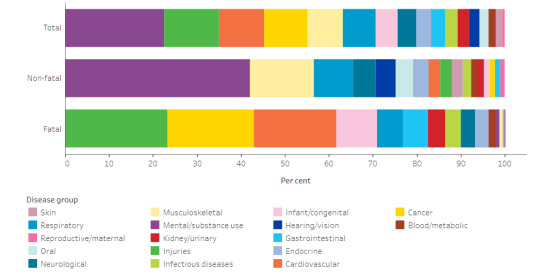
Figure 3: Rate of fatal and non-fatal diseases
(Source: ncbi.nlm.nih.gov, 2022)
Little is currently known regarding the design and implementation processes of health promotion interventions that support healthy ageing for older Indigenous adults (OIA) (High et al., 2023, p.448). Reducing health inequities and supporting healthy aging across the lifespan are priorities for doctors, academics, healthcare providers, community stakeholders, and rehabilitation professionals. The timing is now right for us to actively involve Indigenous communities in general and OIA in particular in the planning, carrying out, and involvement of intergenerational health promotion initiatives.
Reference
Coffey, J. K., Nelson-Coffey, S. K., Parsley, H., & Pluess, M. (2023). Positive emotion expression at age 11 is associated with multiple well-being outcomes 39 years later. Current Psychology, 42(25), 21954-21966. http://www.johnkcoffey.com/uploads/1/9/0/6/19063163/coffey_nelson_coffey_et_al_2022_ncds.pdf
High, A. C., Ruppel, E. K., McEwan, B., & Caughlin, J. P. (2023). Computer-mediated communication and well-being in the age of social media: A systematic review. Journal of Social and Personal Relationships, 40(2), 420-458.https://journals.sagepub.com/doi/pdf/10.1177/02654075221106449
Holly, L., Wong, B. L. H., van Kessel, R., Awah, I., Agrawal, A., & Ndili, N. (2023). Optimising adolescent wellbeing in a digital age. bmj, 380. https://www.bmj.com/content/380/BMJ-2021-068279.full
ncbi.nlm.nih.gov (2022) Aging Well for Indigenous Peoples: A Scoping Review Retrieved on 9 May 2024 from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8866315/
Riitsalu, L., Sulg, R., Lindal, H., Remmik, M., & Vain, K. (2024). From security to Freedom—The meaning of Financial Well-being changes with age. Journal of family and economic issues, 45(1), 56-69. https://link.springer.com/article/10.1007/s10834-023-09886-z
1 note
·
View note
Text
youtube
Responding to Your Criticisms of Medical Keto
I've been using the medical ketogenic diet to treat my schizoaffective disorder for about 3.5 months now, and have been a little surprised at how controversial this has been. In this video, I respond to and chat about some of the concerns or criticisms that have come about from you, our audience, about this medical keto approach to treating mental illness.
Timestamps:
00:00 Introduction
01:16 Too expensive
04:25 Risk of triggering eating disorder behaviours and over focus on weight and physical appearance
08:59 "My meds are working just fine, why would I try this?"
12:04 This is just the placebo effect
13:08 It's not just keto causing this improvement
13:31 Rises in cholesterol being dangerous
14:44 We're being irresponsible
16:04 Not enough scientific or empirical evidence
17:27 We're not creating mental health content anymore, and alienating our audience
19:24 The ultimate goal
20:22 *An important insight* - fear of giving up autonomy and loss aversion
26:12 Feeling the best I ever have
27:35 Thank you for this conversation
NEWLY PUBLISHED STUDY: 'Ketogenic Diet Intervention on Metabolic and Psychiatric Health in Bipolar and Schizophrenia: A Pilot Trial' (Dr. Shebani Sethi, et al)
https://ift.tt/zqRfkMA
MEDICAL KETO RESOURCES
You can learn more about medical keto for mental illnesses on the Metabolic Mind YouTube channel (@metabolicmind) and on their website https://ift.tt/fmVrTUg
You can also learn more about metabolic health and mental illness from the book 'Brain Energy' by Dr. Christopher Palmer - https://ift.tt/7IhyEKw
You can find more about my keto coach Nicole Laurent and her work on her website:
https://ift.tt/AFhPnbg
HELP SUPPORT THE CHANNEL
We depend on the support of our audience to create this valuable resource. If you have found our content helpful, please consider supporting us today. Your contribution can make a huge difference and enable us to continue providing valuable resources to those living with mental illness.
• One-time donation: https://ift.tt/jhBFViZ
• Monthly donation: https://ift.tt/0wiLxM7
JOIN OUR ONLINE PEER SUPPORT COMMUNITY
Join a welcoming community of your peers and find comfort in sharing your experiences. By joining our community, you can benefit from the support of others who understand what you’re going through. We offer live weekly facilitated video peer support groups and text channels to communicate about a wide range of topics. Join today and start feeling less alone with what you’re going through.
• Schizophrenia Peer Support Community: [https://www.schizophreniapeersupport.com](https://www.schizophreniapeersupport.com/)
• General Mental Illness Peer Support Community: [https://www.onlinepeersupport.com](https://www.onlinepeersupport.com/)
MENTAL HEALTH APPAREL
Wear your support for mental health! Our t-shirts, sweaters, and mugs not only spread awareness but also help support this channel. Pick up some mental health apparel today and make a statement while making a difference.
https://ift.tt/tGZIRK4
SPEAKING & CONSULTING
Looking for an expert speaker or consultant for your upcoming event or project? With years of experience and a passion for mental health advocacy, I can provide the insight and inspiration you need to make a positive impact. Visit my speaking website to learn more!
https://ift.tt/YO4S7m5
SOCIALS
Instagram: https://ift.tt/E6UQnWG
TikTok: https://ift.tt/liaU9nW
Twitter: https://twitter.com/LWSchizophrenia
Website: [https://www.livingwellwithschizophrenia.org](https://www.livingwellwithschizophrenia.org/)
#schizophrenia #schizoaffective #schizoaffectivedisorder #mentalhealth #mentalillness #metabolichealth #keto #metabolichealth #criticisms #medicalketo
via YouTube https://www.youtube.com/watch?v=kU1ORt6ZnVE
0 notes
Text
PRISON REHABILITATION RANT! (CONTROVERSIAL)
please read (with an open mind)
TW for the following:
• Prison
• Mental ill health/Mental illness/Mental disorders
• Personality disorders
• Depression
• Torture
• Self-harm
• Suicide attempts/Suicide
I really appreciate anyone taking the time to read this. I understand and accept the controversial nature of this post and the negativity or pushback I may (will likely) receive. But I really feel like this is an important conversation to have for those who will participate. Plus an important speech for those who will read it.
I will also have research backing points I highlight.
In the following video, a comedian briefly discusses her experiences working in a prison teaching basic life skills, alcohol and drug rehabilitation etc. It’s relevant to the topic but also adds humour to a dark subject so regardless of if you read the rest of this post or not it is a good watch.
youtube
ANYWAY…
Points relating to the video below:
We need more people like Tacarra Williams. We need her objectivity, her humanity, her non-judgemental approach. She recognises how to stay safe and assesses the situation for what it is, which is a dangerous one, I will not deny that for a second, she is at risk in that environment. But she does not treat inmates like they are less than.
Notice how she complimented an inmate's personally made shoes (funding for these things is a whole other conversation to be had) - she takes note of the little touches the inmate has added to maintain individuality, which is incredibly important in the system. Said inmate who initially had not been open to her arrival saw her recognition for him as an individual, as a human, and then became civil, dare I say friendly toward her.
Something else she briefly mentions is 'the hole' - this is a prison term used for solitary confinement. This is basically complete isolation, with the only ‘interaction’ being a food tray put through a slot. Alone in their cells, those in solitary confinement are subjected to 24/7 distressing noises and yells of other people in their isolation cells. Inmates are left in a cell for 23 hours a day and let out for 1 hour a day - if they're lucky, because prisons are understaffed and this cannot always happen due to maintaining safety of the prison staff and inmates. Solitary confinement is a procedure that is still used today and that is literally recognised as torture. It has been highlighted in Law and Order SVU, where Detective Stabler spends 24 hours in a cell and you watch his mental state significantly deteriorate. By the time his 24 hours are up he thinks he’s been in there for weeks.
Prison rehabilitation:
Here’s the thing; prison rehabilitation is so important, and recognition of inmates as human beings is paramount. If you dehumanise people and don’t give them the necessary skills for survival and progression, how do you expect to see any reform? How we are treated affects who we become. We know this. If we treat inmates like shit and don’t give them any tools for progression, they will not progress. Period.
If we can provide people with life skills, we can give them something to work towards, and we can watch them begin to thrive. As things are, they’re barely surviving. Inmates figure they have nothing to lose because we don’t give them any even small opportunities to succeed. Every now and then, we see carefully picked, trusted inmates' participation in programs that train service dogs. This absolutely highlights reform and the ability for inmates to change/grow. This particular program is beneficial both for the inmates and the public - the inmates have a goal (to train the dog), they have a friend (an animal does not have a judgement towards them), and those in the public (who require one) have the benefit of a trained service dog.
Mental health of inmates:
A majority of people who are in prison often come from difficult backgrounds and struggle with their mental health. (Pilgrim, 2001; Pagano et al., 2004; Bandelow et al., 2005).
Did you know that the most common mental disorder among prison populations was personality disorder(s)? (Fazel and Danesh, 2002). If people with personality disorders are treated with such a negative stigma in the general population, imagine the stigma faced in the prison environment. People on the outside are denied treatment for personality disorders; there is even an argument among some mental health professionals that personality disorders are untreatable, which is false.
Further studies also suggest a significant overlap between the legal system and mental health issues (Cramer, 2016) including depression and self-harm. Did you know between 2004 and 2009 there were an estimated 24,000 incidents of self-harm per YEAR? (Hawton et al., 2014)
Government assessment of mental health in prisons:
In 2017, a House of Commons committee looked at the evidence surrounding mental health in the prison system and found a lot of problems; their criticisms included: lack of assessment and screening, poor environment, lack of staff, lack of training for prison staff, problems with transferring prisoners with mental health issues to more appropriate care settings.
The BBC News highlighted these issues in visiting Wandsworth prison, where prison officers themselves describe the need to address mental health in prisoners. One officer recounts 8 instances of suicide attempts, and a successful attempt in 1994. He says that he can still remember the scene of the successful attempt.
Do the prisoners or prison staff get the support they need, or even the time of day to be seen to struggle? No. They’re left to suffer - why? Because it would cost the government money to rehabilitate prisoners and provide proper support to prison staff. Frankly, everyone in that system, on both sides, are left to dust.
Is any of this fair? Well, that's a moral question that's personal and down to opinion. The answer will obviously vary according to multiple factors, a case by case basis and personal life experiences. Whatever your answer, I hope these points at least give you something to think about.
Whether you completely disagree, judge me, give me backlash or even read all of or some of this post and then scroll past ignoring it completely, I really don't care. Because at the end of the day, someone needs to fight for inmates and prison officers, and it takes a particular type of person to do it. You may have the mindset of 'they choose that job', 'they put themselves in that situation' or 'why would they do that job/work with such terrible people?'. The answer to this can vary person to person: be it money, interest, belief in making positive change, wanting to make a difference, or simply because someone has to do it.
It's rare to see someone fight for the rights of people living and working in the prison system. This post and view will likely sour opinions of me, I accept that. But whether you like it or not and whether you agree or not, I'll be one of those people.
Thanks for reading.
#I posted this on Facebook a week ago and figured it’s a controversial rant so it obviously belongs on tumblr too#personal#rant#prison rehabilitation#prison reform#rehab#reform#statistics#psychology#mental health#controversial#important#trigger warnings#read with caution#read with an open mind#okay to reblog#mine#text post#2023#Youtube
0 notes
Link
Carolyn* can never get out of her head the memory of her parents bringing her to conversion therapy. The transwoman from South Sulawesi was 13 then, and society expected her to identify as male in accordance with her biological sex at birth.
“Deep inside, I kept telling myself that I’m not sick, that I’m okay,” she recalled.
Carolyn experienced ruqyah firsthand, a form of conversion therapy imbued with Islamic exorcism that is common among Muslim communities in Indonesia. Carolyn’s parents explained away her feminine expression as the work of a malevolent female demon.
At the time, the teenager did not fully grasp the situation she was in. She agreed to go along with her parents’ wishes due to her deeply embedded fear of sin.
Carolyn was taken before the local cleric, who prayed to expel the female demon in her body. The cleric also asked her parents to leave her with him for a few days so she could undergo several rituals.
“But at that time, I refused. I wanted to go home and didn’t want to be there. I was fine, I cried and said to my mom, ‘Mom, I want to go home, I’m fine,’” she said.
After begging her mother, Carolyn’s mother finally agreed to send her home on one condition: she had to stop expressing feminine traits and stop hanging out with her female friends. Carolyn repressed her feminine expression for several years after that day.
“To be honest, I felt very tortured. I felt very tortured mentally,” Carolyn confessed.
Carolyn said she placed a lot of pressure on herself over the years. She never felt that she was a man. She was always more comfortable expressing herself as a woman. In the final year of high school, Carolyn decided to stop lying to herself and her family. She ran away from home and learned to become a hairdresser at a salon that accepted her gender expression.
In the early days of Carolyn’s emancipation journey, her past and concerns over her identity continued to haunt her. Not a day went by that she didn’t fear persecution, socializing with others, fully expressing herself, all the while saddened by the irreparable burned bridge with her family.
Even now, at the age of 32, Carolyn is still traumatized by her conversion therapy experience. She gets easily triggered by watching religious TV shows or films that feature ruqyah scenes.
But ultimately she believes that she made the right choice, because nothing can take away her freedom to fully express herself as a woman and her achievement of becoming a fully functioning adult in a society that generally does not tolerate her people.
“I also feel comfortable and feel very relieved that in the end, I can accept myself as a transwoman. I feel like I have found myself. This is me, I am a transwoman,” she stresses.
In contrast to Carolyn, Sofia*, a lesbian living in the capital, was encouraged by her family to undergo ruqyah when she was old enough. By that time, she was mature enough to make her own decisions; and so she ran away from them.
“At that time, I was 25 years old and I was studying for my master’s degree. My position was quite privileged, right?” Sofia said.
Living in Jakarta, Sofia was more exposed to open discussions on the issues of gender and sexuality. When her mother asked her to go to therapy, Sofia was already certain about her sexual orientation. Furthermore, she had been involved in the advocacy for gender and sexuality issues.
“So I think there was nothing to lose at that time, and my identity is the core of my life,” she said.
However, Sofia’s refusal for therapy did not sit well with her family. She said they still pressured her “recover” to the point that they used violence against her.
“But I didn’t want to. I insisted because they already know me as a lesbian, so why do I have to back off?” she said.
Sofia believes that her knowledge of diversity in gender expression and sexual orientation was one of the biggest sources of courage that emboldened her to emancipate. If LGBTQ+ people are exposed to the same knowledge, Sofia said, they will be able to accept their identities and acknowledge that they’re not the problem — homophobia and conversion therapy are.
“We must fight together to convince the world that being gay is okay. You need to learn about yourself. You’re not sick. It’s society that’s sick,” she added.
Ika*, a transwoman from North Sumatra, experienced conversion therapy when she was 13, 17, and 18. The methods that she went through were quite diverse, ranging from ruqyah, to burial rituals, admission to Islamic boarding schools, and goat sacrifice.
None of them worked. And she said she had to live with the constant pressure from her parents to get rid of her feminine expression, which, according to them, was also the work of a demon.
“What should be removed from my body? Because according to their assessment, there is an evil spirit who made me like this,” Ika said.
“In my opinion, conversion therapy is bullshit.”
Ika now works for an NGO advocating to end HIV discrimination and stigma suffered by trans communities.
‘Individual will’
Conversion therapy is not a new phenomenon in Indonesia, but the matter was hotly discussed recently when several Indonesian queer activists, including Lini Zurlia and Kai Mata, received targeted ads on social media encouraging them to undergo conversion therapy.
“It feels like I was targeted by a group of people. It made me upset, especially because this is very sensitive regarding LGBTQ+ rights in Indonesia,” Kai Mata said.
“What I think the government should do is to make it illegal. I also think that LGBT people in Indonesia deserve the right to live in this country without fear.”
Attempts to contact the conversion therapy service through the ad failed as of the time of this article’s publication. Another conversion therapy center in Jakarta, which claims to use hypnotherapy as one of its “healing” methods, did not come across like it has a vendetta against LGBTQ+ people despite providing the harmful service.
“When does sexual orientation become a problem? It happens when the values that are taught [by people’s environment and family] are different from their sexual orientation,” therapist Adrianto Darma Setiawan said.
Adrianto claims to have treated around 2,500 patients in the last 12 years. About 20 percent of these patients are (or were, if he succeeded) gay, lesbian, or bisexual. The standard therapy to “heal” sexual orientation consists of about about five to six hypnotherapy sessions lasting around three hours per session.
Adrianto said that some of his patients underwent therapy out of their own accord, but most were there due to encouragement or pressure from relatives. The therapist did not say how many of his patients he managed to convert, but said that “recovery” depends on the will of the individual.
The government’s failure
Imam Nahei, a commissioner at the National Commission on Violence Against Women (Komnas Perempuan), said that LGBTQ + groups in Indonesia still have a long way to receive adequate protections from the government. For as long as homophobia prevails in Indonesia, conversion therapy will remain as one of the most harmful and real threats that haunts people from minority sexual groups in Indonesia.
Nahei said that conversion therapy is an obvious human rights violation, yet the state, which should be responsible for protecting all of the country’s citizens, has not done anything to protect LGBTQ+ people from the practice.
“The state has not done anything because, in Indonesia, this issue is still very controversial as it is associated with dominant religious views,” Nahei said.
There’s little hope for progress in this regard when homosexuality and alternate forms of sexual expression are still seen as a deviation or a disorder by the country’s lawmakers, such as House of Representatives (DPR) Commission VIII Deputy Chairman Marwan Dasopang.
Marwan supports the existence of conversion therapy in Indonesia. Not only that, he wants DPR to eventually pass legislation allowing the state to provide the service to the public. If conversion therapy was normalized, he argued, patients would not experience extreme psychological trauma, such as from being forced to “recover” by their parents.
“It needs to be regulated,” Marwan said, adding that discussion on the regulation of conversion therapy are still in their infancy.
Indonesian policy makers, and even psychiatrists, have long gone against the scientific fact that homosexuality and other sexual identities are not a disease or disorder. Their stance have emboldened homophobia, which, in turn, has fostered the continued existence of conversion therapy.
Riska Carolina, director of Advocacy and Public Policy from the Support Group and Resource Center on Sexuality Studies at the University of Indonesia (SGRC UI), said among the many forms of conversion therapy in Indonesia, most are performed with ruqyah. Others who aren’t forced to go the conversion therapy route are still made to see shrinks who practice with heavy religious influence, hypnotherapists, or admitted to religious boarding schools.
“[Conversion therapy] is a threat to the LGBTQ+ community. It is persecution to the LGBTQ+ community. It violates their basic human rights. LGBTQ+ people are not a disease,” she stresses.
Riska believes that regulating conversion therapy would violate the minority groups’ rights even more than they have suffered. Even if the therapy is carried out based on patients’ willingness, Riska argued that it still validates the idea that LGBTQ+ people have mental disorders.
“Conversion therapy must be banned. It is more necessary to provide protection, even though I know that protection is still a long way off. So I prefer that, at least, [the government] treats us equally and gives us affirmative action,” she said.
“I’m ashamed to know that Indonesia is very late in terms of acceptance and it’s already 2021. You don’t need to like LGBT people, but you also don’t need to discriminate against us, especially to the level of torture. What you do with conversion therapy is torturous.”
*Carolyn, Sofia, and Ika’s real names have been omitted, at their request, to protect their identity.
#Southeast Asia#Indonesia#Conversion Therapy#LGBTQIA Rights#Trans Rights#LGBTQIA Issues#Trans Issues
50 notes
·
View notes
Video
youtube
Cognitive Impairment in Schizophrenia
Disclaimer: I am not a mental health professional, I can’t diagnose you. If you think you have a mental illness please reach out to your doctor or a mental health professional.
For schizophrenics like myself, some of the most stigmatized, and sensationalized symptoms are the positive ones, meaning delusions, hallucinations, and movement disorders to some extent. You see them in textbooks and in the media; seeing, hearing, smelling or feeling things that aren’t real. Believing strange ideas, and this is my own example, like that the alien government lizard people are coming after you. These draw the most attention from the public eye, and I can’t blame them, alien government lizard people is pretty out there. But what about the less talked about symptoms such as negative and cognitive symptoms? Well, this essay will examine the cognitive side of a schizophrenia diagnosis.
According to Columbia University (2016), “many people with [Schizophrenia] also have cognitive deficits, including problems with short- and long-term memory.” They go on to say that cognitive factors can be the most disabling for people, leading to difficulty holding down a job and maintaining social relationships. They don’t have many answers as to the cause or cure for memory problems. Sucks to be us I guess. I personally have a plethora of issues with memory, short term and long term. I find myself lost when the dialogue of TV shows gets even slightly complicated because I immediately forget what was said, maybe that’s just me but it takes a toll on my self-esteem when I can't follow slightly complicated dialogue. But anyway, back to memory. Apparently when a group of healthy controls were compared to a group with schizophrenia, the healthy group, unsurprisingly, did better at memory tasks. In fact the health control groups brains showed increased brain activity the tests got harder and decreased activity when it got easier while the people with schizophrenia showed significantly weaker activity across the board.
According to Bowie and Harvey (2006) cognitive symptoms are the central feature of schizophrenia. As well as that these impairments may even present before the emergence of positive symptoms. They also found that there were “moderate deficits in attention, verbal fluency, working memory, and processing speed, with superimposed severe deficits in declarative verbal memory and executive functioning.” What is executive functioning? Well to quote Goodman (2021), “[e]xecutive functioning skills help you get things done. These skills are controlled by an area of the brain called the frontal lobe.” Things executive functioning helps you do is “manage time, pay attention, switch focus, plan and organize, remember details, avoid saying or doing the wrong thing, do things based on your experience, and multitask” (Goodman, 2021).
I’ll cover some ways to deal with executive dysfunction in a later essay.
Most people with schizophrenia will show some kind of cognitive impairment, but the severity will vary across different people. One interesting thing about these cognitive impairments is that they will remain relatively stable over time. There are some different types of impairments that I will summarize.
General Intelligence
I take some offence at the description that all people with schizophrenia have lower IQ’s, I mean there are/were some very smart people with it, like John Nash, or the people Cernis, Vassos, Brebion, McKenna, Murray, David & MacCabe (2015) studied, finding that there is “a high-IQ variant of schizophrenia that is associated with markedly fewer negative symptoms than typical schizophrenia” However the science seems to be overwhelmingly favourable in the direction that people with it have lower IQ’s as a group. On the other hand, I don’t know what kind of people they picked for their healthy control group, because if they were all university grads then it’s not really fair. So take this with a grain of salt. While the tests say that we are as a group, less intelligent than the “general” population it doesn’t mean you specifically are not intelligent. We can be just as successful as anyone else.
Attention
This one is simple, people with schizophrenia have a deficit in their ability to maintain their attention, this occurs even before the first psychotic episode.
Working memory
I have a terrible working memory, bad enough for it to be considered a learning disability. However I’m not alone in this, many people with schizophrenia have some kind of dysfunction in working memory, and apparently specifically verbal working memory. Bowie and Harvey (2006) state that “Working memory can be conceptualized as the ability to maintain and manipulate informative stimuli.” This is in contrast to attention span, with working memory being more cognitively challenging and attention span being more simple. In working memory, “The information must be held online for processing, but does not necessarily transfer to long-term storage, unlike episodic memory” (Bowie and Harvey, 2006). And poor memory can even affect social and interpersonal relationships because of the inability to pay attention to “multiple streams of information” Bowie and Harvey, 2006).
Verbal fluency
People like us sometimes find it rather difficult to speak in a coherent fashion, I remember many instances where I’ve tried to speak only for word salad to spill out of my mouth, and the looks of confusion and worry on other peoples faces is just great, really what I wanted to happen, not embarrassing at all. This inability to speak is due to “poor storage of verbal information as well as inefficient retrieval of information from semantic network” (Bowie and Harvey, 2006). Furthermore, "information that is stored is not always retrieved as a result of this inability to properly access semantic networks” (Bowie and Harvey, 2006).
Verbal and learning memory
A main impairment of schizophrenia is the difficulty of retaining verbal information. From what I understand, recognition memory seems to be able to work well in most cases, but “the pattern of deficits in schizophrenia tends to be reduced rates of learning over multiple exposure trials and poor recall of learned information” (Bowie and Harvey, 2006). So basically it takes a while for us to learn something but once we do we have good recognition memory. Now, recognition memory is the ability to recall something when you’ve seen it before, so I think what happens is if you’re able to process the information into long term memory you’ll be able to recall when you encounter that information again. Maybe I’m totally wrong, I don’t know.
Executive functioning
Now most schizophrenics have difficulties with most of all of the processes involved with executive dysfunction. Bowie and Harvey (2006) say that “schizophrenia patients have trouble adapting to changes in the environment that require different behavioral responses” which is directly due to issues with executive dysfunction. Furthermore, this “inflexibility” is highly associated with what Bowie and Harvey call “occupational difficulties.” This makes sense, when someone can’t plan, practice self-care, engage in social and interpersonal matters or participate in community functions, it’s gonna take a toll on your work life.
Treatment
Atypical antipsychotics seem to be the best treatment for cognitive impairments, though the results are sorta weak, Bowie and Harvey (2006) admit that “they have had very limited, if any, success in producing cognitive improvements. However, the search for new compounds designed specifically for cognitive enhancement in schizophrenia continues to be a promising area for future research.”
However there is also behavioural treatments, but there isn’t a lot of research on this topic. On the other hand, what little research there is, is very promising. “These strategies include training on computerized tasks similar to existing cognitive tests, teaching new learning strategies, training on novel tasks, and/or performing tasks repetitively” (Bowie and Harvey, 2006).
In the end, it seems that a combination of medication and therapy is the key. On the other hand, research by Everding (2005) states that “memory problems in schizophrenia can indeed be reduced and suggests that helping people use the right memorization strategy is critical to success.” The right strategies seem to be to remember more ‘deeply’ or according to Jantzi, Mengi, Serfaty, et al., (2019) to engage in retrieval practice, also Antzi, Mengi, Serfaty, et al.’s (2019) study is “the first to demonstrate that retrieval practice is also superior to restudy in improving later recall in patients with schizophrenia presenting with episodic memory impairment.” This is great news for us because it presents a real way of improving our memories, which apparently most of us need.
REFERENCES
Study finds brain marker of poor memory in schizophrenia patients: possible key to understanding and treating cognitive symptoms of the disease, (2016). Columbia University. Retrieved from https://www.cuimc.columbia.edu/news/study-finds-brain-marker-poor-memory-schizophrenia-patients
Bowie, C. R., & Harvey, P. D. (2006). Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatric disease and treatment, 2(4), 531–536. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2671937/
Černis ,E,. Vassos, E,. Brébion, G,. McKenna, PJ,. Murray, RM,. David, AS,. MacCabe, JH. (2015). Schizophrenia patients with high intelligence: A clinically distinct sub-type of schizophrenia? Eur Psychiatry. (5):628-32. Retrieved from https://pubmed.ncbi.nlm.nih.gov/25752725/
Gerry Everding (2005). Memory study shows brain function in schizophrenia can improve with support, holds promise for cognitive rehabilitation: need cues, memory aids. Washington University. Retrieved from https://source.wustl.edu/2005/07/memory-study-shows-brain-function-in-schizophrenia-can-improve-with-support-holds-promise-for-cognitive-rehabilitation/
Jantzi, C., Mengin, A., Serfaty, D. et al. (2019). Retrieval practice improves memory in patients with schizophrenia: new perspectives for cognitive remediation. BMC Psychiatry 19, 355. Retrieved from https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-019-2341-y#citeas
Goodman, B. (2021). Executive function and executive dysfunction disorders. WebMD. Retrieved from https://www.webmd.com/add-adhd/executive-function
9 notes
·
View notes
Text
Taylor Swift, Britney Spears and the media cycle that demands pain from our pop stars
Emma Clifton 08:30, Feb 16 2021
Britney Spears was robbed of her public image during the height of her fame. Taylor Swift was robbed of her music during the height of hers.
Why does our pop culture system seem so intent on punishing the very women who keep it afloat. Emma Clifton looks at a decade in young singers – and the variously terrible ways they get treated while in the public eye.
There was a theory floated on the podcast You’re Wrong About that ‘fame is abuse’ and you’d be hard pressed not to agree if you were one of the many people who saw the recent New York Times documentary Framing Britney Spears, and realised just how badly we as a society treated Britney Spears before, during, and after her rise to fame.
The paparazzi, the media, the comedians – and then the fans and look-i-loos who continued to buy all the magazines that ran headlines about what a train-wreck she was, when really she was just someone in her early twenties, trying to raise two children while being one of the most famous – and hounded – people on the planet.
The documentary discussed at length how we as a pop-culture obsessed society love to build up a talented, attractive young woman and then buy popcorn in preparation of when we can gleefully watch them tumble from grace.
(And it’s not just pop stars, of course; the resplendent rise and then the racist fall of Meghan Markle’s position in public opinion is one of the most recent examples we have of when good headlines go bad.)
When I was working at Creme magazine, between 2009 and 2012, our pages were over-flowing with talented young pop singers: Taylor Swift, Selena Gomez, The Jonas Brothers, Miley Cyrus, Demi Lovato, Rihanna, One Direction, Justin Bieber.
When you look back on the decade that has passed by since, time has not been kind to any of these people.
Either the showbiz demon took something from each of them – or they had to completely disappear from sight for years at a time in order to survive. Sometimes both.
There have been eating disorders, drug overdoses, rehab stints, broken marriages, abusive relationships, chronic illnesses. These kids – and they were kids – were so young when they started, they’re already on their fourth or fifth reinventions.
Most of them haven’t hit 30 yet.
And when you’re a female pop star, so many of these reinventions revolve around your sexuality.
Heck, when I was at Creme, Demi, Selena and Miley were part of the ‘purity ring’ club, where they all gushed about staying away from sex until marriage while their stylists dressed them in the tightest clothes possible.
The message from the marketing teams behind each of them was very clear: Sell sex, but don’t ever enjoy it.
This is the same battle Britney faced a decade previously – look like a Lolita, but make sure you never have sex with your long-term boyfriend because then you’ll be expected to cry about the shame of it on national television.
This was also the time of paparazzi trying to take up-skirt photos (exactly what it sounds like) of female actresses as soon as they turned 18; 18 – the age where you can legally have sex in America – was a big deal in pop culture.
There was a countdown for when the Olsen Twins turned 18. When Lindsay Lohan turned 18, Rolling Stone ran a breast-focused cover shoot with the headline: ‘Hot, ready and LEGAL’. And it was just fine! Totally accepted. These girls, they were always up for it, right?
And then we get to Taylor Swift.

Taylor is re-releasing Love Story, the song that made her famous, the song that I first heard in the shower (yes, I had a shower radio) when I was 20 and immediately started crying, because it hit me square in the middle of my pop culture diagram: love songs and references to Romeo and Juliet.
It’s from her second album, Fearless, which she wrote when she was aged 16-18 and which won her four Grammys, including Album of the Year. It’s also an album that no longer belongs to her and she can no longer perform, due to some millionaire f...wittery committed by her former manager. But we’ll get to that.
From 2008 onwards, Taylor became a big deal for her music and then, like it always does for women, her love life became the centre drama.
She never talked about a purity ring (thank God) and she sung pretty openly about sex from her third album onwards (Sparks Fly, an iconic song), plus she had the audacity to date a bunch of boys and look happy while doing so. Naturally, her punishment awaited.
To this day, she is still ridiculed about lyrics she wrote in her first couple of albums… songs she wrote herself when she was literally a teenager.
If I had had written an album when I was a teenager, it would have been about my crush who caught the bus, Kevin from The Backstreet Boys, worrying about my thighs, and, I don’t know, my cystic acne.
I’m just saying – we let powerful men get away with s... they pulled when they were young with the old line ‘boys will be boys! They were just kids!’; it just never seems that generosity is never extended to young women and their far more harmless explorations of teenage sexuality.
Because she had yet to have a public mental health crisis or rehab stint, it was clear that Taylor was never going to be the architect of her own media downfall.
Luckily, one was invented for her. After a long-lasting stoush with Kim Kardashian and Kanye West, where absolutely no-one (including Taylor) came out looking good, Taylor suddenly because persona non grata in pop culture and the long-awaited comeuppance began.
And so, she disappeared – in a way that celebrities can do these days. (As a side note, can you imagine how different Britney Spears’ life might have been if she had been allowed to disappear for a couple of years?)
It was only when she released her documentary Miss Americana on Netflix that the public got what it had been craving the whole time – the dark side of Taylor Swift’s fame.
An eating disorder, a sexual assault that she ended up being sued for and, then, the poisoned cherry on top, losing the rights to all her past music thanks to her old manager.
Finally, our hunger for bad news had been satisfied. We had seen her scars and so we could allow her back into the spotlight again.
It’s been interesting watching the roll-out of new music from so many of these female artists during a pandemic: Selena, Demi, Miley, Ariana Grande are among the singers who have eschewed the normal long roll-out of publicity in order to release their own music, without much of the media fanfare that typically accompanies it.
Taylor herself released two albums, without any of the (slightly inane) games she normally includes in the lead-up. You can’t help but wonder that – stripped of their endless touring, performances and appearances, these female artists have found some freedom in being able to just get back to the actual work.
If a pop star releases an album in the middle of a pandemic and no-one is around to give a shit about any of the outfits she’s wearing, does it still count? Turns out, yes.
Following the betrayal of Britney, Taylor, Miley et al by the media, you can see the slow change to have total ownership of their voice these artists have taken.
Social media can be a devil for many reasons but it has overtaken journalists and publicists as the middle man when it comes to how these women get portrayed to the public. Beyoncé has been instrumental in this – it was she who first released an album overnight back in 2013; a move that came without warning and changed the entire industry forever.
She who stopped giving interviews almost entirely, choosing to use her own platforms to get her message and music across. As a result, she’s never been more powerful and she’s never been more private.
As an explicit ‘F... you’ to the powers-that-be who bought her music from under her, Taylor has announced she will be re-recording all of her old albums.
Stories about millionaires against millionaires rarely draw sympathy from a reader but it does highlight how little actually belongs to the artist at the end of the day.
They can have limited control over their image, their public appearances, their private life, their work and their songs. And these are the success stories – these are the people whose names we know.
You have to hope that anyone young and female entering the music business has their eyes very wide open as to just what can go wrong – and what can go wrong even when everything goes right.
The first album Taylor is re-releasing is Fearless, the album that is the most chock-a-block with fairy-tale imagery and glittery optimism.
She’s promised that the songs will be new interpretations on the old originals and that seems only fair.
You can’t help but think that those fairy-tale songs are going to sound a whole lot different being sung by a 31-year-old who’s been through the public wringer then they were as a wide-eyed 16-year-old, on the cusp of making her dreams come true.
41 notes
·
View notes
Text
Big Family [twst Au]
ah, you there welcome to the Crowley residents. Where we take care everyone like a big family and loving eachother, if you wish to enter the resident i give you a warning: Abuse, angst, scars mention, family problem, mental ilness, bullying, minor character death.
You have been warned and please enjoy your stay in the resident
Idea by Owl/Melon
This was supposed to be a happy AU but Owl ending up making this angst and sappy soo... i will make a few Hc and story about this AU. Oh i forgot to mention that they all being Crowley adoptted sons. And this taking place in the normal AU, and same age as the canon one. Except for Yuu and Crowley.
Family tree of the Crowley's:
Dire Crowley
Father of the 22 of his adopted sons, has one biology child Yuusha Crowley and a pet cat Grim. He adopts all of his sons when they we're young age. He is a kind-hearted father that really loves all of his children. His wife dead when Yuusha is 5 years old, but now he is dating someone that soon to be his new wife/husband.
Yuusha Crowley
Crowley biology child, they are the oldest child of the crowley's their age is 24 as being the oldest they really love their younger brothers, their mother dies when they're 5 years old. Now they enrolled to be a teacher in some school, alongside by Crowley as the principal. Grim is their bestfriend and loyal pet.
Grim
Yuusha or Yuu pet and bestfriend, yuu found him when they we're in kindergarten, in the backyard where grim being beaten by some kids. Yuu brought him home, Crowley and Yuu taking care of Grim. Now he is the Crowleys loyal pet. He is the comfort for everyone if they all feel down or having nightmare.
Child of the lost one: (from the oldest to the youngest)
Lilia Vanrouge
The first adoptted child of the Crowleys. He's being found in the front of Crowley house when he is stumble upon a big house, and being greeted nice by Yuu and Grim. He doesn't even remember about his family, the one thing he remember is that someone giving him the bat necklace to remember. Being the second oldest child of the crowleys, he maybe small but he definetly can stole your kneecaps.
Malleus Draconia
An orphan when he was a child, his old family died because of an accident that happen. Often got bullied by the kid in his school year saying that he is a cursed to everyone. And one night Crowley accidently met him in the store saw him to buy some food, crowley follow him to the orphan and came to addopt him at the same time. Malleus is the quietest child, he doesn't mind being alone, but since he is one of the crowley family he is being cerished and loved by his dad, older siblings and his own younger siblings. Has a tamagochi gift from Yuu, and being called "tsunotarou" as a nickname in the family.
Leona Kingscholar
Abandon and being disowned by his own family of the wealthy family, he's having a mental breakdown whenever his family said he is a failure. So he tried to suicide but failed, because his big brother, but he ending up hurt his brother and being assault by his own brother, so he ran away from his "home". Ending up being homeless in the street, but he met Yuu and Grim. Yuu offers him to life together in the crowley household, at first he's disagree but Yuu assure him that they treat him as one family. So he agree and happy being the crowley now. His personality is the same but he is a bit cheery person now. "King" is his nickname
Trey Clover
The perfect and big brotherable of his own happy family, but sadly his family is dead because a criminal broke into his house and ending up killing all of his family except himself who hiding inside the closet. Because of that incident he has PTSD, whenever someone mention any murder or mass gore he will instant having a seizure and collapse. He is Lilia friend in his highschool, he doesn't know where to go so instead Lilia bring him to the Crowley household. Where he mets Yuu and Crowley himself, Lilia tell all the story about him and Crowley felt sad and he adopt him that day. Trey ofcourse still a big brother to everyone, and still making sweet and baking.
Vil Schoenheit
A perfect son of the schoenheit family. Not so perfect for him, his life is like a doll being a pretty kid, being sexualy abuse by his own father. His mother neglected him, soon after his mother and father we're sent to jail because of child abusing. Meanwhile, Vil is brought to a theraphy from all the abuse. Yuu is one of the student in the psychology he saw Vil and decide to bring him home, Vil at first scared but crowley assure him that everything is alright. And soon he is a crowley's. Still the same as the canon but he is scared.
Rook Hunt
Rook doesn't remember anything about his old life. He has the short memories disorder, well atleast he still remember his dear mother before she is seperated from him, the only thing he had is his favorite hat, he stumble upon the crowleys household and Crowley himself tells that he is accepted in the family. He can be mischief and double face at the sametime, oh also he is going to terror you if you dare to bully his siblings.
Idia Shroud & Ortho Shroud
A pair of siblings that has been sent away from their island. A cursed they say about their family, so they got sent away to the crowley household. Afraid that they will be hated again and being thrown to other family but instead they meet a family that they always wanted. A family that accept them who they really are. Idia is the gamer brother that really close to Ortho and Jamil, while Ortho the little brother who has a Tourette syndrome's, he has to take medicine but his syndrome is getting better at the time, he still cheery despite being the youngest siblings.
Cater Diamond
Previously he lifes with both of his sisters, their parents dies because of an airplane crash. Cater always being bullied, physical and verbally abused by his both sisters. He ending up having a double personality disorder that cause him have one side of hyper-hypocrite self and one side of true himself. His sisters kick him from his own house, he met Crowley that outside his house and bring him to Crowley household, as one of the family now. He is really shy, and quiet one, but he is a cheerful and kind-hearted one. Close with trey, kalim and jack.
Ruggie Bucchi
He lifed with poor condition of home, he actually lifed with his grandma before but unintentionally she got sick and her sickness is made her cause to death. Ruggie then left all alone by himself, so he became what people say a small thief. At first everything is alright, but it just got worsed each day he got beaten by people, until one day Yuu and Grim saving him from the beating. Yuu bring him to their house and told everything about his life, and now ruggie is one of them. Ruggie is a trans from FtoM, afraid of his insecurities and people will hate him he tried to hide it. But everyone accept him whoever he is either he is a girl or a boy. And he is a mischief one
Silver
Silver is an orphan where he became a slave to many people, he have been mentally and sexualy abuse by many people. Afraid of that people do the same again he has a trust issues and schizophrenia, he intends to halutination about his imaginary demon. Crowley saved him when he saw silver being a slave by a big ugly mob, he save silver and bring him to a theraphy. Now he is getting better and take a medicine whenever he remember of his past, and he got adopt by crowley. Silver is another big brotherable for everyone, he really loves to make a flower crown for his siblings and dad.
Kalim Al-asim
His family treat him like a doll, the only one that treat him like himself as a human is Jamil and his little siblings. He didn't know that his own family actually a cult people that wants to murder them. He though at first his parent only treat him like a doll because he is their perfect child, his little siblings all gone one day, it was until one night that his parents come to kill him. Kalim has to witnessed his little siblings death upon his eye, thankfully Jamil and him ran away from their home. They we're being chased by the cult people, then crowley come to save them and adopt them to become his family as they both now are saved. Kalim has PTSD about his past, often halutinating about his death siblings. Close with Jamil, Cater, Leona, and Rook
Riddle Roseheart
His mother always force him to be a strict and genius kid. Ofcourse for his dear "mother" he must make her happy even if its must make his mental hurt and being abused by her. He is Ace bestfriends, when he told the story to Ace him and ace planned to run away from their housetown because of the abusive. At first Riddle is nervous but he think again maybe this is best for him and ace, so they run away but they were being chased off by riddle's mother and ace's father. They ran away into the wood until they lost, thankfully they meet Grim in the forest who take both of them to Crowley's household.
Jamil Viper
Kalim childhood friend, and his servant but more like his brother. His parent are abusive to him, they always punish him if he isn't act like a servant. Kalim disagree if Jamil is his servant, for him jamil is like his own brother. Jamil parents is a cult person too, one night Kalim and Jamil parents come to kill Kalim's little sibling infront of their eyes. So they ran away, eventually they got chased by their "parents" thankfully Crowley come to saved them and adopt them. Close with Kalim, Deuce, and Trey.
Jade & Floyd Leech
A pair of twins who is abandon by their own parents, a childhood friends of Azul. Three of them are a orphan, Floyd always get beaten by some kids in his school, while Jade always get tease by some bullies of his class. The twins parents somehow or perhaps their mom abandon them because they are a curse to her. She abandon them, but since the twins and Azul are friends to Ruggie, he bring them to the household and told them that they can be a family.
Azul Ashengrotto
Childhood friends of the twins, three of them really close like a family. His parents is dead when he was a baby, so he was an orphan alongside with the twins. He always got bullied when he was in kindergarten by some kids, the twins defensing him. Azul and the twins are friends with Ruggie, so he bring them to crowley's household and that's how they three are a part of crowley's.
Epel Felmier
A beauty to his own hometown, his parents always wanted him to be beautiful and perfect so they pressuring him to be perfect, and resulting him having eating disorder or Bulimia Nervosa. When epel having enough from all the pressure he then quickly move to town all alone by himself. In the town he was lost and almost being kidnapped. Thankfully there's Yuu and Crowley come to save him, and adopt him as one of them.
Deuce Spade
His life is perfect only him and his mother, but sadly all the happiness must be tragically gone. His mother been killed by some murderer that being chasing Deuce and his mother. So deuce was sent to the orphan for awhile, afraid what happen he's suffer Bipolar from the events happened. One day Yuu come to check on him and said that he can stay with yuu and their family, and so that was the day where deuce adopted.
Ace Trapolla
Abused by his dad, his dad is an alcoholic person and always abusing him with the shard of alcohol bottle, ace body is covered by lot of bruises caus eof his dad. His brother however love him and trying to protecting him, so one day when his dad about to hurt him again, his brother come to defense Ace so he had a fight with their dad. Their dad lost the temper and on that fight his father kill his big brother with a knife that he hold. Ace then ran away from home to his bestfriend, Riddle. Riddle who has a same problem with his own family, ace decide that they both should ran away and they ran away. But, they we're been chased by their own parents, they ran to the woods and met Grim who save them and take them to Crowley's household.
Jack Howl
Lifes with his own family that loves him whoever he is, but sadly all of them must be seperated due to their parent debt. And so jack is being someone else servant, he's been mistreated by lots of people due to that time. One day when he tried to run away he met Yuu that save him on that day. He really happy that finally someone save him and make him accepted and love him again whoever he is.
Sebek Zigvolt
The youngest sibling aside from Ortho, he was being adopted when he met crowley in the orphanage, sitting by himself scared of people because of his social anxiety. Crowley approached him nicely and ask him if he want to stay with him and his other children. At first sebek really scared but crowley assure him that he will be loved and cherised by everyone, and so he does accept it and a part of crowley's family.
#big family AU#twst au#twisted wonderland#twisted wonderland au#Dire Crowley#grim twst#yuu/mc#yuu twst#lilia vanrouge#malleus draconia#leona kingscholar#trey clover#vil schoenheit#rook hunt#idia shroud#ortho shroud#cater diamond#ruggie bucchi#silver twst#kalim al-asim#riddle roseheart#jamil viper#jade leech#floyd leech#azul ashengrotto#epel felmier#deuce spade#ace trapolla#jack howl#sebek zigvolt
175 notes
·
View notes
Text
Neuroessentialism and mental health
Hi!
Time for a little rant about neuroessentialism.
The aim of this post is to provide the opportunity to be conscious of the things that influence us when it comes the way we think about mental health and to challenge stigma around mental health.
First off, I’m not a doctor and the information here cannot serve as medical advice. Always consult your doctor before changing your medication or treatment approach.
Secondly, a lot of the information I present here is elaborated on and further discussed in an episode of the Psychiatry and psychotherapy podcast called “Free will in psychotherapy and psychiatry Part 3” and while I will link to as many things as I can, you can also find a lot of the source material on the website for the podcast. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/2020/7/22/free-will-in-psychiatry-amp-psychotherapy-part-3
So, I see a lot of people talking about mental health on here through a neuroessentialist perspective in memes or text format and I don’t think they’re aware of it so. I’d like to talk a bit about it.
First, I’ll offer a definition of neuroessentialism:
" Neuroessentialism is the view that the definitive way to explain human psychological experience is by reference to the brain and its activity from chemical, biological and neuroscientific perspectives. For instance, if someone is experiencing depression a neuroessentialistic perspective would claim that he or she is experiencing depression because his or her brain is functioning in a certain way.” - Schultz, W. (2018)
I see people talk about, for example, depression in this way often: in memes when people say "I have a literal neurotransmitter deficiency, Karen." or " God forgot to add serotonin when he made me".
Now, why can this be problematic?
Before I get into the issues with this perspective, I will first acknowledge that one of the reasons this view has become so prominent lately is because it aims to reduce stigma around mental health issues.
In the podcast episode mentioned above they point out that “Efforts to reduce stigma should be praised, but they should also be critically analyzed to determine if they meet their goal.”
And that’s the thing neuroessentialism, while aiming to reduce stigma and shame it only does so short term and ends up contributing to stigmatizing attitudes about mental health.
I want to say that it's great to see people fight back when it comes to stigma around mental health. That's what I see people do in these memes. But the effects of neuroessentialist perspectives end up othering people; making them inherently “bad”, “defect” or “helpless”.
Here the deterministic aspect of neuroessentialism comes up - it tells us that there’s something wrong with our brain that we can’t change. It alienates people because it chips away at their and our belief in their ability to change. If you believe that someone's mental issues are rooted exclusively in brain biology, you're less likely to believe that they can control their behavior and so it is less worth the effort of getting them better. This brings about more stigma.
Another thing that’s important to talk about is how neuroessentialism is an extremely simplistic perspective on mental health. And that’s also one of the reasons it has become so big- because it offers a simple explanation to very complicated illnesses.
Here, I want to add a quote by Psychiatrist and psychotherapist Dr. David Puder:
“There are prominent theories out there that we know just aren’t true anymore and that get propagated because they are simplistic ways of explaining things; for example, depression is because you have low serotonin in your brain. That’s just not true. It’s a whole lot more complicated than that.
You could probably show 20 or 30 things that are going on in the brain during depression. Inflammation. Like initially I thought ‘oh depression is inflammation!’
Well, it turns out not all depression has inflammation. Maybe, only one third [of patients with depression] have inflammation markers in the brain.”
We have been looking to neuroscience for an explanation when it comes to mental health and been satisfied with the idea of a simple "chemical imbalance" but truth is that there are many more neurotransmitters which significantly affect our brains when we talk about depression – it’s so far from just serotonin.
Another example of how neuroessentialim can oversimplify mental health is with brain scans. So, in the podcast episode mentioned above, Dr. Puder talks about how he was really interested in emotions and especially studying anger and he was looking at all this research on the different areas in the brain involved in anger. After a while, he says, he began to understand that it’s really complex and you can’t just point at one area and say that’s the area that’s involved in the emotion anger. There are several areas involved in just that one emotion and different studies show different things.
The truth is that the manifestation of mental illness in the body is a very new area of research and we haven’t found physical manifestations for most mental illnesses and the important thing to note here is that despite this we still do have ways of treating all of them.
Alright, all this can seem quite removed from us so how does neuroessentialsim affect us?
In the episode the guest star, Mathew Hagele, further discusses the article which provided the definition on neuroessentialism above: “Shultz looked at studies investigating how patients viewed their own prognosis and later the same with professionals.
The study found that biochemical or genetic attribution scores were a significant predictor of longer expected symptoms duration and lower perceived odds of recovery.” (Lebowitz et al., 2013, p. 523).
Now, this means that the more a patient attributes symptoms of their psychopathology to genetic (inherited disorderes) or biochemical (serotonin deficiency for example) factors, the longer they expected to struggle with their disorder and the smaller the belief that they can recover.
If a person doesn’t believe they can be helped or get better they’re a lot less likely to try and a lot more likely to feel scared and hopeless.
The other side of this coin is the effect the neuroessentialist narrative has on clinicians which Matthew Haegel dives into in the next part of the quote:
“Another study shows that clinicians believe psychotherapy to be less effective when shown biological descriptions of mental health pathologies...
They took a couple different disorders that these clinicians were looking at and one group had a biological explanation and the other did not- had a different type of explanation. And [in] the results that were across disorders, the biological explanation yielded significantly less empathy than the psychosocial explanation. They also did some additional analysis and they found that biological explanations yielded less empathy than the psychosocial explanations among both MD’s and non-MD’s…..”( Lebowitz, M. S., & Ahn, W. K. (2014). )
So, in these studies we see that a neuroessentialist perspective lowers empathy for the patient in medical health professionals and people who weren’t medical health professionals.
Okay, so how does this perception of the patient’s illness affect the patient’s treatment?
I’ll start with a quote where Hagele elaborates further:
“…and finally, that clinicians perceive psychotherapy to be significantly less effective when symptoms were explained biologically than psychologically…[ Lebowitz, M. S., & Ahn, W. K. (2014). ]
basically, linking the idea that the diminished importance of psychotherapy among mental health professionals ascribing to the concept of neuroessentialism is doubly harmful when considering the multiple contexts in which psychotherapy matches or outperforms pharmaceutical interventions.”
What Hagele points out here is the way neuroessentialism can lead to a less effective and ethical treatment of mental illness. It makes us approach an issue in one manner only- fix the brain, fix the behavior. But sometimes what can treat he issue in the brain is, working on the behavior. This can be talked about in terms of meds vs. psychotherapy.
So, seeing mental health from a neuroessentialist perspective, completely excludes the effects of psychotherapy. A classic example is CBT (cognitive behavioral therapy) in which we have “Cognitive restructuring”: a psychotherapeutic process in which a person learns to recognize maladaptive or distressing thoughts and teaches their brain to consider other perspectives or different thought pattern. This is an example of “work on behaviour to better brain” rather than “working on brain will fix behavior”. According to strict neuroessentialism therapy shouldn’t work as well as it does but there is a really big body of science backing psychotherapeutic intervention and its efficacy compared to psychopharmacological intervention.
I feel I should address the discussion of Meds vs. therapy before I continue, (it is a whole topic worthy of a post on its own) but to be brief, they work best together and if you’re weighing one against the other psychotherapy has more long-term effects and barely any side effects compared to medication. There are other factor affecting what would be the most effective treatment approach that further nuances this discussion.
Now this is all a pretty big picture but how is this seen every day?
Well, its seen in the downplaying of the importance of therapy. Often, I see this as people normalize behavior where they kind of devalue the importance therapy or put off working on their issues in therapy with the excuse that it’s only for “crazy” people or not something worth the effort.
Therapy then increasingly is seen as this unimportant, extra thing rather than, in most cases, the most effective and safe treatment. And the less crucial therapy is considered, the less accessible it’s going to be – in the U.S. it can often be easier to get your insurance company to cover for a doctors visits where the treatment would be for your GP to prescribe you an antidepressant than an inpatient or outpatient treatment with a mental health professional.
Another point I wanna put out there is that that neuroessentialist narrative is incentivized by pharmaceutical companies. Dr. Puder talks about his own experience in the podcast episode and makes sure to stress that practitioners are humans too and will of course be biased towards something if that something writes them a check or pays some of their expenses. In the episode they discuss a way in which we have seen the neuroessentialist narrative progress:
“Second, there is evidence that the significant increase in direct-to consumer (DTC) advertising for antidepressants is related to rising prescription rates (Park & Grow, 2008). Such advertisements portray depression as a biological medical condition that can successfully be treated with medicine (Lacasse & Leo, 2005; Leo & Lacasse, 2008)” (613).
Now, medicine is an important tool in psychiatry and there is a lot of unnecessary stigma around medication for mental health conditions. I am under no circumstances arguing that medication is bad and therapy is the only right way to treat mental illness. That would be an extreme simplification and invalidation of human experiences. I also wanna acknowledge that being able to go to therapy in many places in the world is a matter of privilege. Therapy simply isn’t accessible for everyone and people can choose an “only medication approach” for many valid reasons. And if that’s the only treatment that was accessible to you I’m really proud of you for taking care of yourself and doing what you can.
If your doctor has prescribed you a medication please take it and know that the purpose is to help you and that you are worthy of help and good health care. The situation where I would suggest to be a tad critical is when people come in with disorders and issues that they have dealt with for years and most of their life and they are just prescribed an antidepressant and sent home. That simply isn’t effective and ethical care. In that case it is worth investigating getting access to a mental health practitioner as well as continuing with medicinal treatment.
I could talk about this for hours but the last thing I wanna get across is that this is a societal problem. I don’t suggest we turn away from pharmaceutical intervention which saves thousands of lives and helps people get better, rather that we work to make psychotherapy (which can be and is crucial for long term remission and recovery) more accessible for when it’s appropriate.
When your doctor tells you that this invisible illness is because of your biology most people feel validated and experience less shame. The fact that people feel like they need to have a tracible biological “anomaly” in their brains to be worthy of treatment and care speaks to an invalidation that many feel. But the issue here is that we're taught to invalidate invisible illness in society which in the end makes people delay critical treatment or blocks access to ethical and effective care.
We also have to acknowledge that with the technology we have now we are not able to know whether all mental illness manifests in the brain in a way we can see so hinging our worthiness of help and care on the definition is in the end harmful.
TL;DR
" Neuroessentialism is the view that the definitive way to explain human psychological experience is by reference to the brain and its activity from chemical, biological and neuroscientific perspectives. For instance, if someone is experiencing depression a neuroessentialistic perspective would claim that he or she is experiencing depression because his or her brain is functioning in a certain way.” - Schultz, W. (2018)
Neuroessentilism can validate a patient and bring relief of shame short term but ends up contributing to stigmatizing attitudes and thus doesn’t help reduce stigma overall.
The neuroessentialist narrative can downplay the efficacy and criticalness of psychotherapeutic intervention
Neuroessentialist perspectives foster lower empathy levels for patients in medical providers and non-providers alike.
Neuroessentialist perspectives of a patient significantly increases levels of prognostic pessimism which leads to worse treatment outcomes
Neuroessentialism arose because of a real invalidation people feel around their mental health and it is a societal issue we need to work on
We can combat neuroessentialism and stigma by working to make psychotherapy more accessible and talking about our experiences openly as well as giving each other kindness and empathy.
#i tried to make this a readable as possible but shoot me a message if i missed soemthing#neuroessentialism#rant post#mental health struggles#recovery data#psychiatry#medication#psychotherapy#therapy#psychology
13 notes
·
View notes
Text
march reading
kinda forgot about this i guess. anyway feat. uh, magical ships, dubious mental health institutions (plural) & a parisian building with 99 rooms.
the forever sea, joshua phillip johnson (forever sea #1)
i firmly believe that more fantasy lit should be set on ships bc ships are inherently a sexy setting & you could have pirates which are extremely sexy. this has ships (and pirates) and also a sea made of grass? a magical plant sea on which ships sail via magical fires, so conceptually i’m very into it all. the plot is fine, but the protagonist kindred has a very bad case of Main Character Syndrome so prepare for mild annoyance throughout. also while i generally enjoy book magic vs wild magic i wish more works would treat them as two ends of a spectrum rather than ~book magic bad and boring, wild magic cool and *~natural*~. but overall i think this series has potential. 3/5
jagannath: stories, karin tidbeck ([partially?] translated from swedish by the author)
really cool collection of sff stories by tidbeck, many of which veer into mild horror and some of which are influenced by swedish folklore and especially swedish fey stories. i enjoyed most of these a lot, especially the existential call centre horror story, the ‘god won’t let me die’ one, and a taxonomy of a cryptid that goes a little off the rails. 4/5
annette, ein heldinnenepos, anne weber
a novel in verse about anne beaumanoir, a real person who was a résistance member during world war 2 and later supported the algerian national liberation front, for which she was sentenced to 10 years in prison (she escaped to tunisia and later algeria). she’s clearly a very impressive and interesting person & i conceptually enjoyed the idea of writing a modern hero(ine)’s epic, but i feel like the language could have been a bit more stylized to match the form. 3/5
salvage the bones, jesmyn ward (audio)
bleak but ultimately hopeful novel about a black family in the days before and during hurricane katrina, although the focus is on the family dynamics, the 14-year-old narrator discovering that she is pregnant, and the kids trying to keep the puppies their dog china just had alive and well. enjoyed this, altho i did it a bit of a disservice but listening to it a lot of short chunks. 3.5/5
regeneration, pat barker (regeneration trilogy #1)
set mostly at a military hospital for soldiers with shell shock during world war 1, this novel explores the existential horror of war, psychological treatment (& the horrible absurdity of treating traumatised men just enough so that you can send them straight back to Trauma Town), and the meeting between siegfried sassoon & wilfred owen. i find i don’t really have much to say about it, but it is very, very good. 4/5
how to pronounce knife, souvankham thammavongsa
a short story collection mainly about refugees and migrants from laos to canada, many focusing on parent-child relationships and being forced to work in low-paid jobs, often ones that are damaging to their health. the stories are very well-observed and emotionally nuanced and detailed, but with 14 mostly very short stories, the collection as a whole felt a bit samey, which i guess is something i often experience with short story collections. 3/5
faces in the water, janet frame
horrifying semi-autobiographical novel about a young woman stuck in new zealand’s mental health system, moving to different hospitals but mostly from ward to (more depressing) ward in the 40s/50s. while there is a shift in attitudes during her stay that sometimes makes the wards more tolerable, mostly the patients are neglected, abused, and the threat of electric shock therapy and lobotomy always hangs over them. 3/5
the upstairs house, julia fine
fuck why did i read so many books about mental health conditions this month??? this is another entry in my casual ‘motherhood as horror’ reading project, in which a new mother develops post-partum psychosis & imagines the modernist children’s book writer she’s writing her dissertation on and her poet sometimes-lover haunting her and her child (margaret wise brown & michael strange, who are real people i was utterly unaware of). this does pretty good on the maternal horror front, but i wasn’t entirely sold on the literary haunting. 2/5
1000 serpentinen angst, olivia wenzel
a very interesting novel about a woman struggling with grief over her brother’s suicide, an anxiety disorder, the (non)state of a (non)relationship and discrimination/marginalisation based on her identity as a black, east-german, bi woman (while also being, as she notes, financially privileged). much of the novel is written in a dialogue between the narrator and an unnamed (& probably internal) interlocutor, which was p effective for a novel more focused on introspection than much of a plot. 3/5
atlas: the archaeology of an imaginary city, dung kai-cheung (tr. from chinese by the author, anders hansson, bonnie mcdougall)
fictitious theory about a slightly-left-of-reality version of hong kong and how maps (re)construct the city, very heavy on the postmodern poststructuralist postcolonial (and some other posts, i’m sure). in many ways my jam. unfortunately my favourite parts of this were the author’s preface and the first part (fictitious theory of mapping alternate hong kong); the rest felt very repetitive and not particularly interesting, altho i’m sure i was also just missing a lot of cultural context. 2.5/5
under the net, iris murdoch
.........i liked the other two murdochs i’ve read (the sea, the sea & a severed head) quite a lot so either i was not in the mood for her very peculiar style of constructing novels and characters or, this being her first novel, she just wasn’t in full command of that peculiar style yet but man this was a slooooooooog. don’t stretch out your modern picaresque with an incredibly annoying narrator over more than 300 pages iris!!!! 2/5 bc this probably has some merit & i just wasn’t into it
the impossible revolution: making sense of the syrian tragedy, yassin al-haj saleh (tr. from arabic by i. rida mahmoud)
collection of articles and essays saleh (a syrian intellectual & activist who spent 16 years in a syrian prison) wrote from 2011 to 2015, analysing the reasons for, potential and development of the revolution, as well as some background sociological discussion on the assads’ regime. very interesting, very dense, very depressing. wouldn’t necessarily recommend it as a first read on the topic tho. 3/5
angels in america: millenium approaches & perestroika, tony kushner
the page to tumblr darling quote ratio in this is insane (”just mangled guts pretending” and so on) and also it just really slaps on every level. also managed to get me from 0 to crying several times. brilliant work of theatre, would love to see it staged (or filmed). 4/5
life: a user’s manual, georges perec (german tr. by eugen helmlé)
99 chapters, each corresponding with a single room in a parisian apartment block; some chapters are basically ‘here’s the room, here’s a long list of objects in the room, that’s it bye :)’, some are short insights into the lives of the people living there, some (the best, mostly) are long, absolutely wild tales that are sometimes only tangentially connected to the room in question. why are the french like this. 61/99 rooms
sisters in hate: american women on the front lines of white nationalism, seyward darby (audio)
nonfiction about women’s role in white nationalist hate movements, mainly based on the stories of three women who are or have been involved with various contemporary american alt-right/racist/neonazi hate groups, while also looking at general social trends and the history of white women’s role in white supremacy. interesting and engaging if you’re interested in this kind of thing. if you’re both politically aware and internet poisoned, it’s probably not much that is completely new to you but still worth reading. 3/5
starting in april i will be Gainfully Employed (ugh) & thus probably not read as much or read even more bc i have no energy for anything else
6 notes
·
View notes
Text
A propos du trouble bipolaire ( phase dépressive) , par Nayialovecat
Trouble bipolaire, phase dépressive. Texte écrit par @nayialovecat. ( Le lien vers l’image est LA, celui du texte ICI.)
Une personne dépressive n'est pas celle qui pleure, qui a l'air malheureuse, qui parle de vouloir se suicider... Les personnes dépressives sont souvent souriantes, calmes, et lorsqu'on leur demande ce qui se passe, elles peuvent être enthousiastes et vous convaincre que tout va bien. Il faut donc être très vigilant. Car bien qu'il y ait un sourire à l'extérieur, il peut y avoir un abîme sombre ouvert à l'intérieur qui engloutit lentement cette personne. C'est un peu comme d'autres maladies - le cancer par exemple... une fois que les symptômes sont visibles - il est souvent trop tard pour les traiter.
"Salut tout le monde. J'aimerais vous donner quelques bons conseils au cas où vous auriez un jour affaire à une personne souffrant de trouble bipolaire et sur le point d'entrer dans une phase de dépression (la plus dangereuse, à mon avis).
Mais n'oubliez pas que les conseils que je donne ici sont basés sur mon propre comportement (et celui de deux personnes de ma connaissance souffrant de conditions similaires ) : tout le monde n'est pas comme moi. Je ne veux pas être un gourou, parce que quelqu'un d'autre qui est déprimé ou quelque chose comme ça pourrait se dire que j'écris n'importe quoi parce que ça ne fonctionne pas pour lui/elle. Néanmoins... Peut-être que quelqu'un en aura besoin, alors je l'écris.
1- Ce qui est répété partout - vous ne devez pas ignorer et minimiser la dépression, vous ne devez pas laisser cette personne seule avec ses pensées, car ce chemin mène tout droit vers un abîme sombre.
2- Mais cela n'aidera pas si vous dites "Tu as une vie merveilleuse, tu es une personne merveilleuse, tu as une famille merveilleuse". Je sais que c'est le cas. Et quoi ? Mon cerveau ne fonctionne pas logiquement en ce moment et parler comme ça ne fera que me faire penser "Ma famille est merveilleuse, je ne devrais pas les encombrer avec une merde humaine comme moi". N'essaiez pas la logique avec les personnes bipolaires en crise. La logique ne marche pas.
3- Le pire que vous puissiez dire est "Arrête d'être triste". Putain, vraiment ? Conseil du siècle ! "Tu dis que tu es déprimé ? Alors arrête." Non, vraiment, ça ne marche pas comme ça. Et les beaux slogans de motivation du style "Il suffit de vouloir" , vous pouvez vous les mettre où je pense.
4- Si la personne malade se voit prescrire des médicaments, assurez-vous qu'elle les prend. Je ne parle pas seulement des médicaments pour les troubles bipolaires, mais aussi autres. Par exemple, si elle est diabétique et qu'elle a un épisode dépressif, elle peut très facilement renoncer à l'insuline. Parfois, il s'agit d'un choix conscient ("je veux mourir"), mais parfois, c'est complètement indépendant, elle oublie simplement ou s'en moque. Vous devez les lui rappeler, pas nécessairement de manière intrusive, mais en lui disant par exemple : "tu as pensé à prendre tous tes médicaments aujourd'hui ?".
5- C'est bien de la contacter de temps en temps, surtout si elle vit seule ou est souvent laissée seule. Il ne s'agit pas seulement d'empêcher le suicide, car toutes les personnes dépressives n'y pensent pas. Mais le fait est qu'elle ne doit pas être seule, qu'elle doit sentir que quelqu'un pense à elle et s'inquiète pour elle. Et même si elle a l'air heureuse au téléphone, ne vous y trompez pas - il s'agit généralement d'un masque et vous devez donc être prudent. Vous devez lui faire comprendre que vous vous souciez d'elle/de lui.
6- Parler du problème ne fonctionne que dans le cas de maladies physiques. Très rarement pour les maladies mentales (encore une fois : n'essayez pas la logique sur une personne souffrant de troubles bipolaires). Pendant les conversations, essayez de ne pas parler du problème, ne l'analysez pas, parlez plutôt d'autre chose.
7- Et un bon conseil qui fonctionne (du moins pour moi) est de garder la personne occupée. Il ne s'agit pas de la faire rire, essayer de la faire rire ne peut qu'aggraver la situation, mais de faire quelque chose de précis. Une activité où elle n'a pas le temps de (trop) penser. Vous pouvez la motiver et faire le ménage ensemble (la méthode de ma grand-mère, ça marche pour moi). Lui proposer une nouvelle série addictive (la méthode de mon mari, ça marche pour moi). Ou simplement lui parler beaucoup et souvent de choses diverses , de jeux ou de livres (méthode de mes amis, ça marche pour moi). Bien sûr, chaque personne est différente, j'écris sur les choses qui fonctionnent pour moi à ce stade.
J'espère que cela vous aidera un peu.”
Nayialovecat.
°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°
ENGLISH VERSION, WRITTEN BY @nayialovecat
(Drawing link / text link)
Remember, a depressed person is not the one who cries, looks unhappy, talks about wanting to suicide... Depressed people are often smiling, calm, and when asked what's up, they can be enthusiastic convince you that everything is fine. Therefore, you have to be very wary and vigilant. For although there is a smile on the outside, there may be an open dark abyss inside which slowly engulfs this person. It's a bit like other diseases - cancer for example... once symptoms are visible - it is often too late to treat it.
Hey, folks. I'd like to give you a handful of good advices in case you ever have to deal with someone who has bipolar affective disorder and is about to enter a (more dangerous, in my opinion) period of depression.
But remember that the advices I am giving here are based on my own behavior (and also on two people with similar conditions that I know) - not everyone is like me. I don't want to be a guru, 'cause someone else who is depressed or something like this might say I'm writing nonsense here 'cause it doesn't work for her/him. Nevertheless... maybe someone will need it, so I write it.
1- What is repeated everywhere - you must not ignore and downplay depression, you must not leave such a person alone with her/his thoughts, 'cause this way goes along straight into the dark abyss.
2- But it won't help if you say "you have such a wonderful life, you are a wonderful person, you have a wonderful family". I know I have. And what? My brain is not working logically right now and talking like that will only make me think "my family is wonderful, I shouldn't burden them with human shit like me". Don't try logic on such people. Logic doesn't work.
3- The absolute worst you can say is "stop being sad". Fuck, really? Century council! "You say you're depressed? So stop it." No, really, it doesn't work that way. And beautiful motivational slogans in the style of "you only need to want" can be put up your ass.
4- If the sick person is prescribed any medications, make sure that he or she takes them. I'm not just talking about medications for bipolar disorder, I'm also talking about all the others. For example, if she/he is diabetic and has a depressive episode, she/he may very easily give up insulin. Sometimes it's a conscious choice ("I want to die"), but sometimes it's completely independent, she/he just forgets or doesn't care. You need to remind such a person, not necessarily intrusively, but like "did you remember about medicaments today?"
5- It is good to contact such a person from time to time, especially if she/he lives alone or is often left alone. It is not just about stopping suicide, 'cause not every depressed person actually thinks of suicide. But the point is that she/he shouldn't be alone, that she/he should feel that someone is thinking about her/him, worrying about her/him. And even if she/he sounds happy on the phone, don't be fooled - it's usually a mask so you should be careful. You have to make it clear that you care about her/him.
6- Talking about the problem works only in the case of physical diseases. Very rarely for mental illness (again: don't try logic on a person with bipolar disorder). During conversations, try not to discuss the problem, do not analyze it, rather talk about anything else.
7- Exactly, a good advice that works (at least for me) is to keep the person busy. It's not about making her/him laugh, trying to make her/him laugh can only make it worse. But to do something specific. Something where there is no time to think. You can motivate such a person to clean up together (my grandmother's method, works at me). A new addictive series can be proposed (my husband's method, works at me). You can just talk a lot and often about various things with this person, about games or books (my friends method, works at me). Of course every person is different, I'm writing about things that work for me at this point.
I hope it helps you a little.
°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°
POLSKA WERSJA
Hej, ludzie. Chciałabym udzielić Wam kilku dobrych rad na wypadek, gdybyście mieli kiedykolwiek do czynienia z osobą, która ma chorobę afektywną dwubiegunową i wkrótce wejdzie w (bardziej niebezpieczny moim zdaniem) epizod depresyjny. Pamiętaj jednak, że rady, których tu udzielam, opierają się na moim własnym zachowaniu (a także na dwóch ludziach z podobnymi schorzeniami, których znam) - nie wszyscy są tacy jak ja. Nie chcę być guru, ponieważ ktoś inny, kto ma depresję lub coś takiego, może powiedzieć, że piszę tutaj bzdury, ponieważ to nie działa dla niej/niego. Niemniej... może ktoś będzie tego potrzebował, więc piszę.
1- To, co się wszędzie powtarza - nie wolno ignorować i bagatelizować depresji, nie wolno zostawiać takiej osoby samej z jej myślami, bo ta droga prowadzi prosto w ciemną otchłań.
2- Ale nic nie pomoże, jeśli powiesz „masz takie wspaniałe życie, jesteś wspaniałą osobą, masz wspaniałą rodzinę”. Wiem, że tak. I co? Mój mózg nie działa teraz logicznie i mówienie w ten sposób sprawi, że pomyślę tylko: „moja rodzina jest wspaniała, nie powinienem obciążać ich takim ludzkim gównem jak ja”. Nie próbuj logiki na takich ludziach. Logika nie działa.
3- Absolutnie najgorsze, co możesz powiedzieć, to „przestań być smutny”. Kurwa, naprawdę? Rada stulecia! "Mówisz, że masz depresję? Więc przestań ją mieć." Nie, naprawdę, to nie działa w ten sposób. A piękne hasła motywacyjne w stylu „trzeba tylko chcieć” można włożyć sobie w dupę.
4- Jeśli choremu przepisano jakieś leki, upewnij się, że je przyjmuje. Nie mówię tylko o lekach na chorobę afektywną dwubiegunową, mówię też o wszystkich innych. Na przykład, jeśli ma cukrzycę i ma epizod depresyjny, może bardzo łatwo zrezygnować z insuliny. Czasami jest to świadomy wybór („Chcę umrzeć”), ale czasami jest całkowicie niezależny, po prostu zapomina lub nie przejmuje się tym. Trzeba takiej osobie przypominać, niekoniecznie nachalnie, ale w stylu „czy pamiętałeś dzisiaj o lekach?”.
5- Dobrze jest od czasu do czasu kontaktować się z taką osobą, zwłaszcza jeśli mieszka sama lub często zostaje sama. Nie chodzi tylko o powstrzymanie samobójstwa, ponieważ nie każda osoba w depresji myśli o samobójstwie. Ale chodzi o to, żeby nie była sama, żeby czuła, że ktoś o niej myśli, martwi się o nią. I nawet jeśli w telefonie brzmi wesoło, nie daj się zwieść - zwykle jest to maska, więc należy zachować ostrożność. Musisz jasno powiedzieć, że ci na niej/nim zależy.
6- Mówienie o problemie działa tylko w przypadku chorób fizycznych. Bardzo rzadko w przypadku choroby psychicznej (ponownie: nie próbuj logiki na osobę z chorobą afektywną dwubiegunową). Podczas rozmów staraj się nie rozmawiać o problemie, nie analizuj go, raczej mów o czymkolwiek innym.
7- Dokładnie, dobrą radą, która działa (przynajmniej dla mnie) jest zajęcie takiej osoby. Nie chodzi o to, żeby ją/jego rozśmieszyć, próba rozśmieszania może tylko pogorszyć sytuację. Ale zrobić coś konkretnego. Coś, nad czym nie ma czasu na myślenie. Taką osobę można zmotywować do wspólnego sprzątania (metoda mojej babci, na mnie działa). Można zaproponować nowy uzależniający serial (metoda mojego męża, na mnie działa). Możesz po prostu dużo i często rozmawiać z tą osobą na różne tematy, o grach lub książkach (metoda moich przyjaciół, na mnie działa). Oczywiście każda osoba jest inna, piszę o rzeczach, które w tym momencie działają dla mnie.
Mam nadzieję, że to trochę Wam pomoże.
°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°°
6 notes
·
View notes
Text
Charlie's and Jack's first met [SCRIPT, ENG/PL]
Alright! So not so long time ago i did a script how Charlie and Jack first met, i hope you'll enjoy it!
English ver:
(It was a cloudy day, all of this happened in the mental hospital where Charlie usually works and examines his patients. It's 4:30 PM)
Jack: * He is sitting in some room on a chair in front of a small table, waiting for someone to come to check him *
Charlie: * Knocks on the door * Knock knock!
Jack: ... Who's there ..?
Charlie: * Enters * It's me! Heheh! * Closes the door behind him, sits on the chair in front of Jack *
Charlie: Hmmm .. You must be.. * Checks his name on his list * Ah! Jack! Jack Di-
Jack: AGH !! DO NOT SAY THIS SURNAME !! I HATE IT !!!! STOP IT! STOP IMMEDIATELY !!! * He covered his ears with his hands and closed his eyes *
Charlie: Huh? Well .. All right!
Jack: I just prefer people to call me ONLY Jack ..
Charlie: As you wish. And so! Nice to meet you, Jack! I am Dr. sunshine! I'm here to help you fix your mental illness * smiled *
Charlie: So let's get started .. How are you today?
Jack: Why should I tell you?
Charlie: Uhm ... Well, to make you a diagnosis! You know, I need to know how you feel, without knowing about your well-being, I will not be able to fully diagnose you and cure you of the disease or disorder which causes you the emotions that you feel right now, and emotions often lead to various unpleasant actions such as: murder, violence, aggression etc.
Jack: So you're telling me the sick are to blame, right?
Charlie: Oh no no !! I didn't really mean it! I mean-
Jack: Do you realize that mentally ill people commit crimes and other things for other reasons?
Charlie: Yes I-
Jack: Grrr ... I DO NOT LIKE people to think that mentally ill people are just psychopaths who do nothing and they only kill others because they like it so much 'cause of their mental illnesses .. And how others blame THEM for the murder and violence, and not those who caused that they behave this way ...
Charlie: I-I .. Uhm ..
Jack: LOOK AT THIS WORLD! Almost every breathing creature in this goddamn world is rude, mean, ignorant and self-righteous and people who A LITTLE DIFFERENCE become victims of these Normals assholes for being different ... DAMN, HOW CAN YOU NOT GET MENTALLY SICK?!?!
Charlie: I-I understand .. But unfortunately their mental illnesses or disorders do not justify their actions, w-that's why go to therapies like this t-to heal themselves from mental disorders and diseases so they won't hurt others anymore ..!
Jack: ... So we're the only ones to suffer, yeah ..? And they get away with it ???
Jack: If we're being chastised by them, WHY DON'T THEY FEEL IT ?! IT'S UNFAIR!!! HAVE YOU EVER EXPERIENCED THIS PAIN ?! THE PAIN OF BEING LAUGH AT, SHAMED BECAUSE YOU ARE DIFFERENT FROM THE REST OF THESE NORMALS FUCKFACES?! ANSWER ME!!!!
Charlie: YES! I HAVE EXPERIENCED THIS MANY TIMES!!! * Stressed out *
Jack: ... Knew it ...
Charlie: Huh ..?
Jack: You seem ... Different from the rest ... You're so strangely ... Positive ... Nice, polite and ... Good for a psychiatrist ..
Jack: The other psychiatrists I met were too serious and without emotion and no sympathy whatsoever .. I've never met someone like you.
Jack: Apparently you are not a normals .. Though I can see that you are trying your best to be one .. Why?
Charlie: I .. I'm no different! I am a normal person, like everyone else! I just want to be polite to others and that's it!
Jack: Mmmm .. A lie. A simple lie .. I don't like when others lie to me .. And the most I do not like when people try to lie to themselves.
Jack: You are different .. You are .. Sensitive and sympathetic .. I don't meet such people like you .. Almost never. And the fact that you yourself admitted that people treated you like garbage ..
Charlie: I'm not different ..
Jack: If you are not different, why are you trying so hard to tell me that you are not instead of ignoring what I am saying? It looks like you are trying to hide something from me ... Don't hide the fact that you know what I mean ... We are similar to each other ...
Jack: Weak .. Sensitive .. Different ... You can't fool me, doctor ..
Charlie: ... Why are you telling me this ...?
Jack: So that you finally understand that this is not the real you. I know what I'm saying .. Believe me * He smiled widely *
Charlie: ... I think time is up regarding my conversation with you. * Rises from the chair * Time for me, I have other patients to check. Goodbye, Jack.
Charlie: * slides the chair behind him, walks to the door, leaves and closes the door behind him *
Polish ver:
(To był pochmurny dzień, wszystko to działo się w szpitalu psychiatrycznym w którym Charlie zwykle pracuje i
bada swoich pacjentów. Jest godzina 16:30)
Jack: *Siedzi w jakimś pokoju na krześle przed małym stolikiem, czeka aż ktokolwiek przyjdzie go zbadać*
Charlie: *Puka do drzwi* Puk puk!
Jack: ... Kto tam..?
Charlie: *Wchodzi* To ja! Heheh! *Zamyka za sobą drzwi, siada na krześle przed Jackiem*
Charlie: Hmmm.. Ty musisz byyyć.. *Sprawdza na swojej liście jego dane* Ah! Jack! Jack Di-
Jack: AGH!! NIE MÓW TEGO NAZWISKA!! NIECIERPIE GO!!!! PRZESTAŃ! PRZESTAŃ NATYCHMIAST!!! *Zakrył swoje uszy rękoma i zamknął oczy*
Charlie: Huh? Cóż.. No dobrze!
Jack: Wolę po prostu by ludzie nazywali mnie TYLKO Jack..
Charlie: Jak sobie życzysz. A więc! Miło mi cie poznać, Jack! Ja jestem pan sunshine! Jestem tu po to by pomóc ci naprawić twoje problemy psychiczne *uśmiechnął sie*
Charlie: A więc zaczynajmy.. Jak się dziś czujesz?
Jack: Czemu miałbym ci mówić?
Charlie: Uhm... No po to by postawić ci diagnozę! Wiesz, musze wiedzieć jakie jest twoje samopoczucie, bez wiedzy o twoim samopoczuciu nie do końca będę mógł ci postawić diagnozy i cie wyleczyć z choroby lub zaburzenia które powoduje u ciebie emocje które teraz odczuwasz, a emocje często prowadzą do różnych nieprzyjemnych czynów jak: morderstwo, przemoc, agresja itp.
Jack: Czyli mi mówisz że chorzy są winni, tak??
Charlie: Oh nie nie!! Nie do końca to miałem na myśli! Chodzi mi bardziej o to że-
Jack: Zdajesz sobie w sprawę z tego że chorzy psychicznie ludzie popełniają przestępstwa i różne rzeczy z innych powodów???
Charlie: Tak, ja-
Jack: Grrr... NIE LUBIE jak inni uważają że chorzy psychicznie ludzie to tylko psychopaci którzy nic nie robią tylko zabijają innych bo im sie tak podoba z ich chorób psychicznych.. I to jak inni winią ICH za morderstwa i przemoc a nie tych którzy sprawili że tak sie zachowują...
Charlie: J-ja.. Uhm..
Jack: SPÓJRZ NA TEN ŚWIAT! Prawie każda oddychająca istota na tym cholernym świecie jest nieuprzejma, wredna, ignorancka i zadufana w sobie, a ludzie którzy CHOĆ TROCHĘ się różnią, zostają ofiarami tych dupków normalsów za to że są inni... CHOLERA, JAK TU NIE ZOSTAĆ CHORYM PSYCHICZNIE?!?!
Charlie: R-rozumiem.. Ale niestety ich choroby psychiczne lub zaburzenia ich nie usprawiedliwiają do ich czynów, d-dlatego chodzą na terapie takie jak ta b-by wyleczyć się z zaburzeń i chorób psychicznych, dzięki temu nie będą już krzywdzić innych..!
Jack: ... Czyli tylko my mamy cierpieć, tak..? A im uchodzi to na sucho???
Jack: Skoro my jesteśmy przez nich karceni, TO CZEMU ONI NIE POCZUJĄ JAK TO JEST?! TO NIESPRAWIEDLIWE!!! CZY TY W OGÓLE DOŚWIADCZYŁEŚ TEGO BÓLU?! BÓLU BYCIA OŚMIESZANYM, WYZYWANYM BO JESTEŚ INNY OD RESZTY TYCH ZJEBOMÓZGÓW?! ODPOWIEDZ MI!!!!
Charlie: TAK! DOŚWIADCZYŁEM WIELE RAZY!!! *Zestresował się*
Jack: ... Wiedziałem..
Charlie: Huh..?
Jack: Wydajesz się... Inny od reszty... Jesteś tak dziwnie.. Pozytywny.. Miły, uprzejmy i... Dobry jak na psychiatrę..
Jack: Inni psychiatrzy których poznałem byli zbyt poważni i bez emocji i jakiejkolwiek sympatii.. Nigdy nie poznałem kogoś takiego jak ty.
Jack: Widocznie nie jesteś normalsem.. Choć mogę zauważyć że próbujesz z całych sił nim być.. Dlaczego?
Charlie: Ja.. Nie jestem inny! Jestem normalną osobą, jak każdy! Ja po prostu chcę być uprzejmy do innych i tyle!
Jack: Mmmm.. Kłamstwo. Zwykłe kłamstwo.. Nie lubie jak inni mnie okłamują.. A najbardziej nie lubię jak ludzie próbują okłamywać samych siebie.
Jack: Jesteś inny.. Jesteś.. Wrażliwy i sympatyczny.. Mało spotykam takich ludzi.. Prawie w ogóle. I fakt że sam przyznałeś że ludzie traktowali cie jak śmiecia..
Charlie: Nie jestem inny..
Jack: Skoro nie jesteś inny to dlaczego tak bardzo próbujesz mi wmówić że nie jesteś zamiast zignorować to co teraz mówię? Wygląda to jakbyś próbował coś przede mną ukryć... Nie ukrywaj tego że nie wiesz o co mi chodzi... Jesteśmy podobni do siebie...
Jack: Słabi.. Wrażliwi.. Inni... Nie oszukasz mnie, doktorze..
Charlie: ... Dlaczego mi to mówisz..?
Jack: Abyś w końcu zrozumiał że to nie jesteś prawdziwy ty. Wiem co mówię.. Uwierz mi *Uśmiechnął się szeroko*
Charlie: ... Myślę że czas się skończył co do mojej rozmowy z tobą. *Wstaje z krzesła* Czas na mnie, mam innych pacjentów do zbadania. Dowidzenia, Jack.
Charlie: *Zasuwa za sobą krzesło, podchodzi do drzwi, wychodzi i zamyka za sobą drzwi*
#charlie pakhomov#shinekitai pakhomov#jack dickson#jack#script#eng script#pl script#polish#english#mh#mysterious hatred#mado-racc
5 notes
·
View notes
Text
Iris Publishers - Current Trends in Clinical & Medical Sciences (CTCMS)
Suicides and Suicide attempts among Child and Adolescent Psychiatric Inpatients in Iran
Authored by Saeed Shoja Shafti

The WHO report “Preventing suicide: a global imperative” published in 2014 estimates that over 800,000 people die by suicide, and more than 20 million attempts suicide each year. This implies that every 40 seconds, a person dies by suicide somewhere on the globe, and every 1.5 seconds, someone will attempt to take his/her own life. However, those numbers are underreported, as not all countries in the world report suicide mortality to the WHO Globally, suicides account for 52 percent of all violent deaths in men and 71 percent of all violent deaths in women. In high-income countries, 79 percent of violent deaths in both males and females are caused by suicide. Suicide occurs in all regions of the world and throughout the life span, and it accounts for 1.4 percent of all deaths worldwide, by that, ranking as the 15th leading cause of death [1]. Suicide is rare in childhood and early adolescence and becomes more frequent with increasing age. The latest mean worldwide annual rates of suicide per 100 000 were 0.5 for females and 0.9 for males among 5-14-year-olds, and 12.0 for females and 14.2 for males among 15-24-year-olds, respectively. In most countries, males outnumber females in youth suicide statistics. Although the rates vary between countries, suicide is one of the commonest causes of death among young people. Due to the growing risk for suicide with increasing age, adolescents are the main target of suicide prevention. Reportedly, less than half of young people who have committed suicide had received psychiatric care, and thus broad prevention strategies are needed in healthcare and social services. Primary care clinicians are key professionals in recognizing youth at risk for suicide [2]. In ten years follow up of eighty-eight subjects with adolescent-onset psychotic disorders, mainly schizophrenia and affective disorders, 4.5% of subjects had died from suicide while another 25% of the subjects had attempted suicide [3].
In the context of suicide, there is a growing body of evidence showing that exposure to early-life maltreatment can affect molecular mechanisms involved in the regulation of behavior through methylation and histone modification, supposed to induce behavioral deviations during the early development, and possibly later in life, affect genes involved in crucial neural processes. This mechanism is called epigenetics. Childhood abuse and other detrimental environmental factors seem to target the epigenetic regulation of genes involved in the synthesis of neurotrophic factors and neurotransmission [4]. On the other hand, some scholars believe that People with first episode psychosis (FEP) are at increased risk of premature death, suicide [5]. According to the findings of a study, the rate of attempted suicide among young people undergoing treatment for first episode psychosis was around 12%. Of these 72.6% attempted suicide on one occasion. 85.3% of attempts occurred when patients were treated as outpatients and were in regular contact with the service. 77.6%of suicide attempts tended to be impulsive triggered by interpersonal conflict or distress due to psychotic symptoms. Two thirds involved self-poisoning, usually by overdose of prescribed medications. All inpatient suicide attempts were by hanging or strangulation [6].
So, Individuals with a first episode of psychotic illness are known to be at high risk of suicide, yet little is understood about the timing of risk in this critical period. Suicide risk was highest in the first month of treatment, decreasing rapidly over the next 6 months and declining slightly thereafter [7]. In this regard, longer duration of untreated psychosis, greater symptoms of depression, and positive symptoms of psychosis were found to increase the odds of experiencing suicidal ideation in first episode psychosis [8]. While according to some studies depressive symptoms during the index psychotic episode and comorbidity with stimulant abuse at baseline were relevant predictive factors for suicidal behavior during the first years of first affective and non-affective psychotic episodes [9], more depressive symptoms, higher insight, and negative beliefs about psychosis increase the risk for suicidality in FEP [10].
Impulsive behavior such as self-harm, as well as having a family history of severe mental disorder or substance use, have been stated as important risk factors for suicide in FEP [11,12]. Furthermore, low levels of cholesterol have been described in suicide behavior including among those individuals who have an increased tendency for impulsivity [13,14]. While, as a kind of psychological explanation, some scholars believe that young men in the early stages of their treatment are seeking to find meaning for frightening, intrusive experiences with origins which often precede psychosis, and these experiences invade personal identity, interactions and recovery [15], some suggests that personality characters, specifically, passive-dependent traits can be a predictor of first suicide attempts FEP [16].
On the other hand, no general agreement regarding higher prevalence of suicide in FEP is so far achievable. For example, while researchers like Nordentoft et al. [17], Bornheimer LA [8], Fedyszyn et al. [7], and Cohen et al. [18] have stated that FEP is a particularly high-risk period for suicide, with a risk as high as 10-60% during the first year of treatment, other scholars like Preti et al. [19], Pompili et al. [20], Crumlish et al. [21], and Addington et al. [22] have expected a lower risk or stated that suicide rates are difficult to measure in FEP patients, even in carefully defined samples. In the present study, suicides and suicide attempts among child and adolescent psychiatric in-patients, during the last five years, in Razi psychiatric hospital, as the largest national psychiatric hospital in Iran and region, has been evaluated to assess the general profile of suicidal behavior among native child and adolescent psychiatric inpatients, and comparing first admission with recurrent admission patients.
Methods
Child and adolescent section of the Razi psychiatric hospital was the field of the present assessment. For valuation, all inpatients with suicidal behavior (successful suicide and attempted suicide, in total), during the last sixty months, had been included in the current retrospective study.
Statistical analyses
Difference of suicidal behavior between first admission and recurrent admission patients, had been analyzed by ‘comparison of proportions’. Statistical significance as well, had been defined as p value ≤0.05. MedCalc Statistical Software version 15.2 was used as statistical software tool for analysis.
Results
As said by the results, among 748 child and adolescent psychiatric patients hospitalized in razi psychiatric hospital, during a sixty months period (2013-2018), 14 suicide attempts, without any successful one, had been recorded by the security board of hospital (Table 1). Six of suicide subjects were male and 8 of them were female, with no significant difference about quantity (Table 2). The most frequent mental illness was bipolar I disorder (50%), which was significantly more prevalent among female patients (z=2.72, p<0.007, CI 95%:0.19, 1.23), followed by conduct disorder (42.85%), and substance abuse disorder (7.14%). In this regard, no significant difference was evident among psychiatric disorders (Table 3). Moreover, no significant difference was evident between the first admission and recurrent admission child and adolescent inpatients, totally (p<0.44) and separately (Table 3). The annual incidences of suicidal behavior in both groups were comparable, and they were around 0.21% and 0.16%, in first admission and recurrent admission psychiatric inpatients, respectively (Table 1). Table 1: Comparing suicidal behavior between first admission and recurrent admission child and adolescents psychiatric patients in Razi psychiatric hospital thru 2013-2018.
To read more about this article: https://irispublishers.com/ctcms/fulltext/suicides-and-suicide-attempts-among-child-and-adolescent-psychiatric-inpatients-in-iran.ID.000502.php
Indexing List of Iris Publishers: https://medium.com/@irispublishers/what-is-the-indexing-list-of-iris-publishers-4ace353e4eee
Iris publishers google scholar citations: https://scholar.google.co.in/scholar?hl=en&as_sdt=0%2C5&q=irispublishers&btnG=
#Iris Publishers#Iris Publishers LLC#Medical Science Journals#Open access journal of Current Trends in Clinical & Medical Sciences#Clinical Science#Clinical sciences Open access journals
2 notes
·
View notes
Text
Of Dogs and Autism
“Discrete trial training (DTT...) is a technique used by practitioners of applied behavior analysis (ABA) that was developed by Ivar Lovaas… DTT is a practitioner-led, structured instructional procedure that breaks tasks down into simple subunits to shape new skills. Often employed up to 6–7 hours per day for children with autism, the technique relies on the use of prompts, modeling, and positive reinforcement strategies to facilitate the child's learning. It is also noted for its previous use of aversives to punish unwanted behaviors. […]
“DTT is used to reduce stereotypical autistic behaviours through extinction and the provision of socially acceptable alternatives... Intervention can start when a child is as young as three and can last from two to six years. […] The first year seeks to reduce self-stimulating ("stimming") behavior...
“[It] is ideally performed five to seven days a week with each session lasting from five to seven hours, totaling an average of 35–40 hours per week. Each session is divided into trials with intermittent breaks. The trials do not have a specified time limit to allow for a natural conclusion when the communicator feels the child is losing focus. Each trial is composed of a series of prompts... that are issued by the "communicator" who is positioned directly across the table from the individual receiving treatment. These prompts can range from "put in"," put on"," show me"," give to me" and so on, in reference to an object, color, simple imitative gesture, etc. The concept is centered on shaping the child to correctly respond to the prompts, increasing the attentive ability of the individual, and mainstreaming the child for academic success. Should the child fail to respond to a prompt, a "prompter," seated behind the child, uses either a partial-, a simple nudge or touch on the hand or arm or a full-, hand over hand assistance until the prompt has been completed, physical guide to correct the individual's mistake or non-compliance. Each correct response is reinforced with verbal praise, an edible, time with a preferred toy, or any combination thereof. […]
“There is only weak evidence that the Lovaas method is effective.
“... Lovaas's original technique also included more extensive use of aversives such as striking, shouting, or using electrical shocks. These procedures have been widely abandoned for over a decade. […] Only one institution, the Judge Rotenberg Center, still employs electric shocks as aversives…
“Gresham and MacMillar (1998) specifically cite a lack of a true experimental design in Lovaas' (1987) experiment on early intervention. They charge that he instead implemented a quasi-experimental design of matched pairs regarding the distribution of subjects within the experimental and control groups. [They] also state a lack of a true representation of autism in that the subjects were neither randomly sampled from the population of individuals with autism nor were they randomly assigned to treatment groups. The internal validity of the study was also called into question due to the possibility of skewed data resulting from three influential threats. Instrumentation, changes or variations in measurement of procedures over time, was argued to have been altered in both the pre-test and post-test conditions which were confounded by a differentiation in ascertaining cognitive abilities and intelligence of the subjects. […] External validity was called into question concerning sample characteristics. Lovaas' (1987) criteria for acceptance into the program required a psychological mental age greater than 11 months and a chronological age less than 46 months in the case of echolalic children. Schopler et al. (1989) purport that if both the intellectual and echolalia criteria were rigidly adhered to at the North Carolina institute, approximately 57% of the referrals would have been excluded from the program.
“Other criticisms include a failure to operationally define the use of the term 'reinforcement' for compliance, the use of a Pro-rated Mental Age, and the statistical regression of the child's IQ over time. Boyd (1998)addressed the potential impact of a disproportionate sex ratio of females to males on the control group's mean IQ score. […] In a rejoinder to Boyd's (1998) article... Lovaas (1998) listed three reasons as to why the disproportionate ratio's influence on the data was negligible. The autistic population at the time had a ratio of 4:1. Lovaas (1998)[24] argued that the ratios for the experimental group, control group 1, and control group 2 of 16:3, 11:8, and 16:5, respectively, were in fact near the expected ratio scale of the general population with the exception of control group 1. The second argument lay in the studies Boyd (1998) referenced in regards to low intellectual performance in females diagnosed with autism. One of the studies admitted to having a female subject with Rett disorder, a condition that showed little responsiveness to intensive early behavioral intervention. Lovaas (1998) concluded by proposing that males may more readily meet diagnostic criteria for autism because of certain salient characteristics inherent in the sex while the subtleties in their female counterparts may be overlooked.”
Autistic children are treated like animals, trained to stop performing behaviors that are not harmful or wrong for no reason beyond allistic people not liking it. ABA therapy needs to stop.
#op is allistic; please bear that in mind#aba therapy tw#ABA therapy#applied behavioral analysis#autism#ableism#dogs#dog training#human rights#discrete trial training#psychology#conditioning#operant conditioning#psychblr#hot takes#psych major rants#ivar lovaas
26 notes
·
View notes
Last Seen Blogs

tenderlygenerouspainter
Naamloos

fyaurora
Princess Aurora

reseda-1984
Reseda-1984

padmavathitravelsttd
Untitled
