#i do have a specific diagnosis in mind but it's not one i have and it's a stigmatised one so i wanna be really really careful here
Text
i'm seeing a lot of Pokémon SV DLC analyses where people say 'Oh, Kieran's fixation on Ogrepon is because he sees it as a path to strength; Carmine's bullied him long enough that his shield against admitting his weakness to himself is adoring a legendary creature'. And don't get me wrong – these interpretations certainly hold water – but I've actually been working from basically the opposite angle for all this time.
By all means, Kieran idolises strength, but he inhabits Carmine's shadow – he's the weak sibling, and probably has been for a long time. Yet, rather than fixate on the fantastical power of the Loyal Three, he identifies himself with Ogrepon – the downtrodden, ostracised creature cast out to eke out a subsistence. A terrible demon that wasn't quite terrible enough to cause anyone any lasting harm. The creature defeated by heroes, rather than the perfect, heroic figureheads themselves. He's enamoured with the downtrodden; he sees himself in its grief, in its being cast out and excluded. He's been cast out and excluded all his life (and he can't be a bad person, right? It's not fair – he's hated senselessly, surely, rather than for some reason?) – he sees himself as harmless; so the ogre, too, must be harmless, mis-blamed. Strength is thus in resistance; in growing a shell to tolerate others' inexplicable cruelty. So Kieran looks to Ogerpon, and he thinks that the meek shall inherit the earth, and it gives him the strength to tolerate long nights with poor company. Others are villains – not him, not this creature – and he's safe in the knowledge that at the end of the day, at least an ogre can go down in mythology as the putative sole survivor of its trials.
In this sense, Kieran's like Penny – he finds himself in a position of weakness, of being victimised, and forms himself an armour of being an underdog, of being the thing that bites back. Yet while Penny's position is that the underdog might muster the strength to bite back and restore justice, Kieran's view is that at least the underdog was worth loving. He's inert and preoccupied with his inertia. He can't understand that maybe he could be a human, with the capacity to grow, the capacity to sin. And when Carmine is cruel to him, he reaffirms his own contrarian mindset more – she says I am worth little for my weakness, so my weakness is all I am worth; my weakness is my strength.
And yet he chases strength, because he has to to survive. So when the player comes by, and supports him, maybe he has the safety to walk away from his preoccupation with being an underdog, to enjoy strength for strength's sake. And then, he starts losing, but this time, there are stakes, since he can't just withdraw and be consoled by the fact that withdrawing is right, is right, is right. Thus, he must get stronger. And then, when Ogerpon turns out to favour Juliana, who's become Kieran's idol for all that strength means, rather than Kieran, who's Kieran's selfsame designated weaklingpatheticscumidiot——well, what can Kieran do but fracture, since his whole ideology, his whole premonition that he might have the right to inherit the earth, has been fractured? And, under stress, he pivots from one extreme to the other. All he knows is that weakness is now unbearable. He must get stronger. Must get stronger. Must get stronger—because otherwise he's doomed, he's nothing. He has no myth to dissolve his identity in any longer, so he reshapes himself around the only other standard he's ever known. And it twists him and it breaks him into tiny pieces, because suddenly, the last thing he can bear to be is Kieran: Kieran, the downtrodden and meek boy. He has to flip on his axis; he must become the designated villain of his story by popular imagination, or else be subsumed in the fact that he's going to die someday without any place in the world. He has to play a part, because he's been consigned to one so long, and he can't think of anything other than heroes and villains, enemies and martyrs. He can't be the bad guy. Strength is now goodness; weakness is now evil. And he can't reconcile who he thought he was with who he must become, and as a result, all he can do is try to destroy the person who's destroyed his ideology.
#ngl the more i dive into kieran's character the more i worry about his mental health.#i do have a specific diagnosis in mind but it's not one i have and it's a stigmatised one so i wanna be really really careful here#still: let's just say 'black and white thinking' 'mutable identity' 'abandonment phobia' 'very rash when angry' 'emptiness'#and 'very verrrry reactive mood' – well if you know you know#anyway. he's my blorbo and he breaks my heart#pokemon sv#teal mask#the teal mask#kieran#pokemon kieran#pokémon#scarvio#scarvi#SV#scarlet and violet#pokémon scarlet#pokémon violet#pokemon scarlet#pokemon violet
209 notes
·
View notes
Text
see the reality is i post on my rps usually when nobodys been there a bit and nobody is probably online, but the mental illness in me keeps saying its bc everyone secretly hates me and i dont deserve love, and when i tell a gov doctor that, they basically just say ‘take your antidepressant’s and shut up’ which is also funny when said gov doctor wont refill my fucking antidepressants in the first place
#what i need is smthn for my anxiety and PROBABLY the obviously worsening ocd#but anxiety meds and antidepressants dont mix well#just like adhd meds and anything else dont mix well#which is why i just have a redbull if i need to focus bx it works for a few hours and then i pass out#which isnt healthy but its better than going through the diagnosis process AGAIN bc they dont have my info anymore#its early sad times rn w brina who hasnt gotten an ounce of treatment at all hi#see the other thing is#if i talk about my mental health at all#people will either hate me for being annoying which is what my brain will pinpoint#or feel sorry for me which i also dont want#all i rly wanna do is vent but thats never really an option at all#like yes i know its not normal to want to have a breakdown and cry bc your fucking pillow isnt the correct fluff and wont dluff#i know its not normal to feel like you should die because something wasnt in fhe spot you put it in and was moved slightly#im aware. and the reality is nobody who can do anything about it cares#i have to get an authorization to see a therapist or get meds at all even tho the card claims i dont have to#and the doc tbey gave me wont give me one#they dont allow email so i cant leave a paper trail when bitching at them and my calls go ignored#im losing my mind steadily#and thats not even onto the physical problems#but also the sheer fucking audacity of the website being all ‘oh just go to ERs and UC snd we’ll cover it’ vs hospitals specifically saying#‘we will refuse you if you have Gov Ins unless you have the money to pay out of pocket#if youre on gov insurance you dont have fucking money thats the entire fucking point. you creedy fucknuts go shove tour nepotism in your#fucking eyes and die if anyone doesnt deserve to fuck its you fuckfaces#sometimes i just want to scream esp when this doesnt seem to be most other ppls issues#but then i talk to other women and it is#it just doesnt make sense and i hate it#but i never rly got help on private insurance either so#tbd#depression cw
3 notes
·
View notes
Text
🎶🛌
#BABY IM YOUR CHANGER WAH CHANGER WAH LOVE IS NOT A DANGER WAH#have literally listened to this one on repeat for 24 hrs........ yeah#also YALL tell me why my pediatric psychiatrist diagnosed me w adhd when i was 15#and just DIDNT TELL ME OR MY MOM#like i Knew ive had it by seeing all these accounts of ppl w it telling their experiences over the yrs#but like ive always been like oh its just a self diagnosis 👉👈 NO TURNS OUT I WAS FR DIAGNOSED SIX YRS AGO?????#AND NOBODY DECIDED TO TELL ME???????????? HELLO????#I HAD TO BE LOSING MY GPDDAMN MIND IN MY APT AND HAVE MY LIFE LOWKRY IN SHAMBLES FROM EXECUTIVE DYSFUNCTION AND#CRYING BC I COULDNT JUST PICK UP A FU KING CARDBOARD BOX FOR SOME REASON#AND SEE SMTH WEIRD ON MY HEALTH INSURANCE HISTORY SO I REQUESTED MY GODDAMN PSYCH RECORDS FROM HIGH SCHOOL#ONLY TO FIND OUT I WAS DIAGNOSED W ADHD IN 2017 AND I COULDVE BEEN PROPERLY MEDICATED FOR IT THIS WHOLE TIMEEEEEEEEEE#AHHHHHH IM LOSING MY MIND AND NOT IN A GOOD WAY#I NEED TO BITE SOMETHING#anyway im pulling up to my primary care doc and asking them to either do smth or send to someone who will#bc i cant live like this anymore#anyway gn yall#✨ anon i see ur ask and i love it and i will answer it tomorrow ok my love <33 gn specifically to u mwah#talk#tunes#🎶🛌#mine#not nct#ignore.mel#tag talk#Spotify
0 notes
Text
My dear lgbt+ kids,
Someone requested some advice on whether to openly tell people you are mentally ill/neurodivergent/invisibly disabled or not.
There's some research that suggests that, for example, autistic people are more likely to identify as lgbt+ than their non-autistic peers - so this is absolutely a topic that belongs on a lgbt+ blog and I'm sure there are a lot of you who had to make that decision (and probably keep having to make it as coming-outs of any sort are rarely one-and-done!).
In fact, I had/have to make that decision myself! As an autistic person with depression and anxiety, I could tell you now why I personally decided to be open about all those diagnoses - but the right decision for me isn't necessarily the right decision for you as my life isn't yours.
So, what I'll do instead is to write down a general list with (potential) pros and cons, and I encourage you to nitpick it. Personalize it, take some time to decide how much, if at all, each point weighs in your own decision. There's no right or wrong answer here. It's all about your highly individual situation, about your safety and comfort.
Reasons not to be open about it:
It may put you at risk for various sorts of hate, discrimination, negative stigma and bad treatment
It may put a burden on you to educate others and discuss any misconceptions or myths they believe in, including potentially hurtful or disstressing ones (maybe even fruitlessly so which may cause frustrations or fights)
It may change the way people treat you, even in well-meant ways (babying you, pitying you, trying to "help" against your wishes etc.)
It may feel like a loss of privacy, make you feel "naked" or emotionally vulnerable, make you worry more about the way others perceive you etc.
Reasons to be open about it:
It may help others understand you or your behavior better, which may have positive effects on your relationships
It may allow you to ask for support and help more easily (either from friends and loved ones or in the workplace, school etc.)
It may make you feel empowered and help you accept/love yourself as a disabled person more
It may contribute to making your specific diagnosis more visible in society (which may also make you feel pride in breaking down stereotypes and supporting your community)
It may discourage people from assigning wrong or hurtful labels to you (either armchair-diagnosing you or labeling you as weird, crazy, lazy, gross etc.)
It's important to keep in mind that some people do not have the option to make this decision for themselves, for example because they have highly visible symptoms or they are in a position where their caretakers make the decision for them. This adds another layer to why we can't judge one decision as better or worse than the other - it's not always their own decision.
With all my love,
Your Tumblr Dad
1K notes
·
View notes
Text
.
#told my dad that I didn’t want to go to the grocery store to cash in my change jar#specifically that I’d be fine if we just went to do that and it was in and out but I knew we���d also be going grocery shopping while there#and that’s what I didn’t want to do#he got mad at me because I guess they never know what to get for me and apparently#in his mind me going to the grocery store would solve that#when I’m reality I put the things I want on the shopping list when I know I want them#so they do know what to get me#and if I was asked to pick new foods I would eat in the grocery store I would just say whatever I had to in order to get out the fastest#I can’t stand the lights and the noises and the people#and especially when I’m just following someone else who’s getting things it’s horrible because of the uncertainty and lack of control#but try explaining that to my parents.#I don’t have an autism diagnosis and that’s a lot harder to file under adhd#genuinely don’t know how I didn’t get diagnosed as a kid the more I learn about younger me though#lack of social skills translated to lack of friends#for a solid portion of middle school I wore the same outfit every day#I also would never leave the house without my zip up hoodie and when I would grow out of one I bought another one#that was as similar as I could find. and I still won’t let go of them#hated certain textures to the point that if I had to eat some of them I would barely be able to swallow or I would retch trying to#I loved sorting things but never actually created with them#whenever I would play I’d set up a story in my head and then create that scene and leave it#i had this whole elaborate communal living space set out in my dresser for all my odd toys and would periodically change it#because I would just set it up and that was my play and I hated when other people would touch it#when I would set up scenarios with my stuffed animals I would always remind them that it wasn’t real and the one I had be the villain#I would comfort because I didn’t want them to feel less loved#I hated change and literally could not cope with it#even when I wanted it- like switching from clarinet to oboe. I wanted to but I still sobbed that night and for a few nights after too#like. I have all the symptoms. people just thought I was weird and dismissed it#people being my parents
1 note
·
View note
Note
I have always been wary of the psychiatric industry, but its only very recently that i started to read anti-psychiatric works. Your blog is the first time i saw that the "chemical imbalances causing mental illness" is a myth, and honestly its something im having a hard time wrapping my head around.
Is it that mood regulation struggles, labelled as a mental illnesses, has more to do with outside factors instead of the person "just being that way"? Is it therefore unlikely for someone to have struggles with mood regulation if they cant identify any external causes that would cause them to be, for example, extremely agoraphobic or to have anger management issues? Im asking this for myself mainly, cause i always had intense agoraphobia no matter how i often go outside my home (in fact it was worse when i was a teen and i was outside the house in even more back then). I cant think of any reason for me to be like this than chemical imbalances in my brain.
the specific 'chemical imbalance' myth i was talking about in this post is the idea that depression is caused by low serotonin, and that therefore SSRIs—serotonin re-uptake inhibitors, ie drugs that cause a higher level of serotonin in the brain—ought to cure or at least ameliorate depression. this conjecture is belied by the fact that SSRIs don't, at a population level, reliably perform better than placebo.
although a neurobiological cause of 'mental illness' has long been the holy grail of psychiatry, the serotonin imbalance myth is far from the only hypothesis that psychiatrists and neuroscientists have proposed. so, a critique of the serotonin myth is not synonymous with, or generalisable to, a critique of every neurobiological mechanism purported to explain psychiatric diagnoses. you may be interested to know, though, that genomics and neuroscience have not identified a biological cause of any psychiatric diagnosis (p. 851).
all human experiences are biologically instantiated, including in the brain and wider nervous system. we are embodied beings. however, it is a leap to assume that such instantiation is automatically equivalent to a causal explanation or disease etiology. in other words, to deny that psychiatric diagnoses are known to be biologically caused does not mean we deny that thoughts and thought patterns express in the physical matter of neuroanatomy. this is a major philosophical sticking point to keep in mind whenever you're looking at something like, eg, a study that purports to show 'brain differences' in those assigned a certain psychiatric diagnosis. another thing to consider is whether these papers are plagued with methodological issues or financial conflicts of interest.
i can't possibly tell you why you exhibit agoraphobia. however, when i talk about social, economic, and environmental factors that may contribute to the patterns of behaviour labelled as 'mental illness', i'm talking about much more than the individual choice to leave your house. since phobias are 'anxiety disorders', i might start by probing into questions like: is the world you live in safe? do you perceive it as safe? do you or your community face existential threats that may confront you more obviously when you go outside? are you nervous around other people, and if so, might that be connected to fears (well-founded or not) about interpersonal violence and harm? do you think any of these anxieties may be connected to the hostility and inaccessible design of the social environment and economic conditions?
human behaviour and thought varies. some of those variations may be totally benign; others may be helpful or harmful to the person living with them. it would be weird if every single one of the 8 billion people on earth experienced precisely the same amount of anxiety about any situation, no? all of this is to say: yeah, it's entirely possible you have been, for one reason or another (genetic, neuroanatomical, social, &c) predisposed to experience high, even debilitating levels of anxiety when leaving your home. most human characteristics develop from a tangle of social, environmental, material causes—ie, from a combination of 'nature' and 'nurture'. what doesn't follow, though, is the claim that there is therefore a discrete, 'diseased' element of your brain or brain functioning that can simply be cured or eliminated through psychiatric intervention.
it is a critical point of anti-psychiatry to challenge psychiatric and neuroscientific claims to neurobiological determinism where psychiatric diagnoses are concerned. this is for many reasons, including: a) that these claims have not been demonstrated to actually be true [see above]; b) that they rob pathologised people of agency and self-determination [see: you're too sick to know you're sick, and the doctor will fix you now]; c) that they are often pushed by pharmaceutical companies with financial interests, or grant-funded researchers with... financial interests; d) that they are politically seductive in various eugenic, hereditarian discourses that seek to eliminate the biologically 'unfit' element from society.
1K notes
·
View notes
Text
I think one of the more insidious things about having a General Anxiety Disorder (GAD) label in your medical file while being chronically ill is that too many doctors feel secure in looking at that and going, "Ah, the anxiety is the source of these symptoms" when in reality, the GAD is because of the symptoms.
I am not experiencing debilitating colon pain because of my anxiety. I am anxious because my insides keep trying to perforate, and no one can tell me why. (Yet.)
And yet, I am still being sent mindfulness links by doctors I haven't even seen yet because they've looked at my file ahead of time and saw the GAD diagnosis, skipped over everything else (hEDS, MCAS, POTS, pernicious anemia, PTSD from medical gaslighting (it's in there, I made them put it in there), etc, etc.) and thought wow, yeah. That's appropriate.
Fuck you.
My anxiety is an appropriate response to living in a body that requires regular medical intervention to not die. Which, when you think about it, isn't really general anxiety, but really fucking specific.
Also, if this is some sort of automated feature: That's still really fucking terrible. If you're a doctor or someone who does admin for a doctor, don't fucking do that.
It's so patronizing and belittling.
2K notes
·
View notes
Text
Writing Mental Health With Compassion
I've gotten a few questions regarding depicting characters with mental health challenges and conditions and I wanted to expand a little more on how to depict these characters with compassion for the real communities represented by these characters.
A little about this guide: this is, as always, coming from a place of love and respect for the writing community and the groups affected by this topic at large. I'm also not coming at this from the outside, I have certain mental illnesses that affect my daily life. With that, I'll say that my perspective may be biased, and as with all writing advice, you should think critically about what is being told to you and how.
So let's get started!
Research
I'm sure we're all tired of hearing the phrase "do your research," but unfortunately it is incredibly important advice. I have a guide that touches on how to do research here, if you need a place to get started.
When researching a mental health condition that we do not experience, we need to do so critically, and most importantly, compassionately. While your characters are not people, they are assigned traits that real people do have, and so your depiction of these traits can have an impact on people who face these conditions themselves.
I've found that reddit is a decent resource for finding threads of people talking about their personal experiences with certain illnesses. For example, bipolar disorder has several subreddits that have very open and candid discussions about bipolar, how it impacts lives, and small things that people who don't have bipolar don't tend to think about.
It's important to note that these spaces are not for you. They are spaces for people to talk about their experiences in a place without judgment or fear or stigma. These are not places for people to give out writing advice. Do NOT flood subreddits for people seeking support with questions that may make others feel like an object to be studied. It's not cool or fair to them for writers to enter their space and start asking questions when they're focused on getting support. Be courteous of the people around you.
Diagnosis
I have the belief that for most stories, a diagnosis for your characters is unnecessary. I have a few reasons for thinking this way.
Firstly, mental health diagnoses are important for treatment, but they're also a giant sign written across your medical documents that says, “I'm crazy!” Doctors may try to remain unbiased when they see mental health diagnoses, but anybody with a diagnosis can say that doctors rarely succeed. This translates to a lot of people never getting diagnoses, never seeking treatment, or refusing to talk about their diagnosis if they do have one.
Secondly, I've seen posts discuss “therapy speak” in fiction, and this is one of those instances where a diagnosis and extensive research may make you vulnerable to it. People don't tend to discuss their diagnoses freely and they certainly don't tend to attribute their behaviors as symptoms.
Finally, this puts you, the writer, into a position where you treat your characters less like people and story devices and more like a list of symptoms and behavioral quirks. First and foremost, your characters serve your story. If they don't feel like people then your characters may fall flat. When it comes to mental illness in characters, the people aspect is the most important part. Mentally ill people are people, not symptoms.
Those are my top three reasons for believing that most characters will never need a specific diagnosis. You will likely never need to depict the difference between bipolar and borderline because the story itself does not need that distinction or to reveal a diagnosis at all. I feel that having a diagnosis in mind for a character has more pitfalls than advantages.
How does treatment work?
Treating mental health conditions may appear in your story. There are a number of ways treatments affect daily life and understanding the levels of care and what those levels treat will help you depict the appropriate settings for your characters.
The levels of care range from minimally restrictive and minimal care to intensive in-patient care in a secure hospital setting.
Regular or semi-regular therapy is considered outpatient care. This is generally the least restrictive. Your characters may or may not also take medications, in which case they may also see a psychiatrist to prescribe those medications. There is a difference between therapists, psychiatrists, and psychologists. Therapists do not prescribe medications, psychiatrists prescribe medications after an evaluation, and psychologists will (sometimes) do both. (I'm US, so this may work differently depending where you are. You should always research the specific setting of your story.) Generally, a person with a mental illness or mental health condition will see both an outpatient therapist and an outpatient psychiatrist for their general continuing care.
Therapists will see their patients anywhere from once in a while as-needed to twice weekly. Psychiatrists will see new patients every few weeks until they report stabilizing results, and then they will move to maintenance check-ins every 90-ish days.
If the patient reports severe symptoms, or worsening symptoms, they will be moved up to more intensive care, also known as IOP (Intensive Outpatient Program). This is usually a group-therapy setting for between 3-7 hours per day between 3-5 days a week. The group-therapy is led by a Licensed Professional Counselor (LPC) or Licensed Professional Social Worker (LPSW). Groups are structured sessions with multiple patients teaching coping mechanisms and focusing on treatment adjustment. IOP’s tend to expect patients to see their own outpatient psychiatrist, but I've encountered programs that have their own in-house psychiatrists.
If the patient still worsens, or is otherwise needing more intensive care, they'll move up to PHP (Partial Hospitalization Program). This can look different per facility, but I've seen them to be more intensive in hours and content than IOP. They also usually have in-house psychiatrists doing diagnostic psychological evaluations. It's very possible for characters with “mild” symptoms to go long periods of time, even most of their lives, without having had a diagnosis. PHP’s tend to need a diagnosis so that they can address specific concerns and help educate the patient on their condition and how it may manifest.
Next step up is residential care. Residential care is a boarding hospital setting. Patients live in the hospital and focus entirely on treatment. Individual programs may differ in what's allowed in, how much contact the patients are allowed to have, and what the treatment focus is. Residential programs are often utilized for addiction recovery. Good residential programs will care about the basis for the addiction, such as underlying mental health issues that the patient may be self-medicating for. Your character may come away with a diagnosis, or they may not. Residential programs aren't exclusively for addictions though, and can be useful for severe behavioral concerns in teenagers or any number of other concerns a patient may have that manifest chronically but do not require intensive inpatient restriction.
Inpatient hospital stays are the highest level of care, and this tends to be what people are talking about when they tell jokes about “grippy socks.” These programs are inside the hospital and patients are highly restricted on what they can and cannot have, they cannot leave unless approved by the hospital staff (the hospital's psychiatrist tends to have the final say), and contact with the outside world is highly regulated. During the days, there are group therapy sessions and activities structured very carefully to maintain routine. Staff will regulate patient hygiene, food and sleep routines, and alone time.
Inpatient hospital programs are controversial among people with mental illness and mental health concerns. I find that they have use, but they are also not an easy or first step to take when dealing with a mental health condition. Patients are not allowed sharp objects, metal objects, shoelaces, cutlery, and pens or pencils. Visitors are not allowed to bring these items in, staff are not allowed these items either. This is for the safety of the patients. Typically, if someone is involuntarily admitted into the inpatient hospital program, it is due to an authority (the hospital staff) deeming the patient as a danger to themselves or others. Whether they came in of their own will (voluntary) or not does not matter in how the program operates. Everyone is treated the same. If someone is an active danger to themselves, then they may be on 24-hour suicide watch. They are not allowed to have any time alone. No, not even for the bathroom, or while sleeping, or during group sessions.
Inpatient Hospital Programs
This is a place of high curiosity for those who have never been admitted into inpatient care, so I'd like to explain a little more in detail how these programs work, why they're controversial, but how they can be useful in certain situations. I do have personal experience in this area, but as always, your mileage may vary.
When admitting, hospital staff are the final say. Not the police. The police hold some sway, but most often, if someone is brought in by the police, they are likely to be admitted. They are only involuntarily admitted when the situation demands: the staff have determined the person to be an imminent danger to themselves or others. This is obviously subjective, and can easily be abused. A good program with decent staff will do everything they can to convince the patient to admit voluntarily if they feel it is necessary, but ultimately if the patient declines and the staff don't feel they can make the clinical argument that admittance is necessary, the patient is free to leave. It should be noted that doctors and clinicians have to worry about possibly losing their licenses to practice. They don't want to fuck around with involuntary admittance if they don't have to, and they don't want potentially dangerous people to walk away.
Once admitted, the patient will have to remove their clothing and put on a set of hospital scrubs. These are mostly made of paper, and most often do not have pockets, but I have seen sets that do have pockets (very handy, tbh). They are not allowed to take anything into the hospital wing except disability-required devices such as glasses, hearing aids, mobility aids, etc. Most programs will require removing piercings, but not all of them, in my experience.
The nurses will also do a physical examination, where they will make note of any open wounds, major scars, tattoos, and other skin abrasions that may be relevant.
The patient will then be led to their bed, where they will receive any approved clothing items from outside, a copy of their patient rights, and a copy of the floor code of conduct and rules, a schedule, and any other administrative information necessary for the program to run efficiently and legally.
Group sessions include group-therapy, activities, coping skills, anger management, anxiety management, and for some reason, karaoke. There is a lot of coloring involved, but only with crayons. A good program will focus heavily on skills and therapeutic activities. Bad programs will phone it in and focus on karaoke and activities. Most hospitals will have a chaplain, and some will include a religious group session. I've never attended these, so I can't speak for them.
Unspoken rules are the hidden pieces of the inpatient programs that patients tend to find out during their first visit. There is no leaving the program until the doctor agrees to it. The doctor will only agree to it if they deem you ready to leave, and you are only ready to leave if you have been compliant to treatment and have seen positive results in the most dangerous symptoms (homicidal or suicidal ideations). Noncompliance can look like: refusing your prescribed medications (which you have the right to do at any time for any reason. That does not mean that there won't be consequences. This is a particularly controversial point.), refusing to attend groups (chapel is not included in this point, but that doesn't mean it's actually discounted. Another controversial point.), violent or disruptive outbursts such as yelling or throwing things, and refusing to sleep or eat at the approved and appointed times. All of this may sound like the hospital is restricting your rights beyond reason, but I've seen the use, and I've seen the abuse. Medications are sometimes necessary, and often patients seriously prefer having medication. Groups are important to a person's treatment, and refusing to go can be a sign of noncompliance or worsening symptoms. If someone is too depressed or anxious to go to group, then they're probably not ready to leave the hospital where the structure is gone and they must self-regulate their treatment. Violent or disruptive outbursts tend to be a sign of worsening symptoms in general, but even the best of us lose our tempers from time to time when put into a highly stressful situation like an inpatient hospital stay. The hospital is supposed to be a place of healing, for many it is. But for many more, it is a place of systematic abuse and restriction.
Discharge processes can be long and arduous and INCREDIBLY stressful for the patient. Oftentimes, they won't know their discharge date until the day of, or perhaps the day before. Though the date can change at any time. The discharge process requires the supervising psychiatrist to meet with the treatment team and then the patient to determine if the patient had progressed enough to be safely discharged. Discharge also requires a set outpatient plan in place, such as a therapy appointment within a week, a psychiatrist visit, or admittance into a lower level of care. This is where social workers are involved. Patients are not allowed access to cell phones or the internet. They cannot make their own appointments with their outpatient care providers without a phone number and phone access. Some floors will have phone access for this reason, others will insist the social worker arrange appointments and discharge plans. Social workers are often incredibly overworked, with several patients on their caseload.
The patient cannot be discharged until the social worker has coordinated the discharge plan to the doctor's approval. Most often, unfortunately, the patient rarely receives regular communication regarding the progress of their discharge. I've been discharged with as much as a day's notice to two hours notice.
Part 2 Coming Soon
This guide got longer than expected! Out of respect for my followers dashboard, I will be cutting it here and adding a Part 2 later on.
If you find that there are more specific questions you'd like answered, or topics you'd like covered, send an ask or reply to this post with what you'd like to see in Part 2.
– Indy
#writing advice#writing tips#writing resources#writeblr#amwriting#asktheprose#ask the prose#writing mental health#mental health#writing with compassion#writing mental illness#writing compassionately
148 notes
·
View notes
Text
How to Get a Doctor to Listen To You (and maintain the relationship you have with that doctor, cause you're gonna need that later)
First, I'll preface this by saying: The system sucks. There is no perfect way to access medical care, at least not in the USA. You've almost always got to play the system at least a little to get what you need.
Should it be this way? No. But it is. So here's how to play the game in order to get the most out of a visit to the doctor (there are very different steps to getting what you need out of a hospital stay, but that's a different post):
So First, Let's Assume You Have a Primary Care Doctor That isn't an Urgent Care or the Emergency Department (if you don't, look below the cut first for some tips on getting one, then come back up here)
First, make a list of your problems, then go at the pace of one problem per appointment. Yes I know this sucks. But please read on.
Reasoning:
Appointments are set up in 15-minute slots, but docs typically are timed to about 5-8 minutes spent in a room with a patient on average (the rest of the time is prep and charting and referring and checking in with other doctors to get advice). This is imposed by the hospital or clinic they are working for- not something they choose. If a doctor took as much time as they needed with each patient they would probably get fired. That means every minute beyond that 5 minutes is a minute being "taken" from another patient (isn't capitalism wonderful?!). And 5 minutes is about enough time to evaluate 1 single medical problem.
So when you're setting these up understand that it is way easier and faster to make a bunch of appointments all at once than making them one at a time (hence the making a list of your problems). You might be able to get one slot per week (after a new patient appointment, which will probably take a long time to schedule, see below the cut), each scheduled for a different problem. Keep in mind though, if you make multiple appointments, no-shows are not taken-to kindly. Too many and the rest of your appointments will be cancelled. If you know you can't make it, call ahead.
So what if you need seen right now for a specific symptom? Go to an urgent care or the emergency department. They are almost never going to be able to solve the problem, but a toradol shot for a migraine now is better than waiting six weeks for a sumatriptan prescription. Plus, an emergency department visit or two where they did something for you establishes a history in the record of your problem.
Does this suck? Absolutely. Is multiple appointments always practical for work/school/transportation/copay reasons? Nope. But that's the system, and unfortunately, if you go into an appointment with 6 problems, as you have probably experienced, you're either going to be asked to narrow it down to what is the most important to you anyway, or you're going to get exactly zero useful things out of that appointment.
Next, be upfront, and do it LONG before the doctor walks into the room.
When you schedule an appointment, they will ask you why you are coming. If you want to be evaluated for Ehlos Danlos, for example, say exactly that. "I want to be evaluated for ___________".
Reasoning:
No one can hold everything in their heads for their entire careers, and doctors use that little blurb of why you are coming to look stuff up before you get there.
If you spring something on them that isn't something they see every day, they will be falling back on a very small amount of information they got a long time ago. If you don't fit that tiny piece of information they have saved on that specific disease, you're probably not going to get a diagnosis.
In contrast, if they come in knowing what they will need to evaluate, they will be able to look up or ask how to do the evaluation beforehand and the evaluation for things like the thing you want evaluated. You're much more likely to get a diagnosis if they're doing the right test and asking the right questions.
Also, say you are looking for a diagnosis if that's what you want, and say why. Say something like "If I come up positive for MCAS, could you tell me? I want to try some treatments and accommodations for it that I can only get through a diagnosis."
Reasoning:
I spent 6 years in therapy before my counselor admitted to me that she thought I had had depression the entire time. Why? Because before Obamacare, having a diagnosis of anything more than the flu one time could leave you un-health-insurable for life. Plus even just a generation ago being sick in any way was something socially unacceptable.
It's still like that, but it's changing.
There's still fear about this in the medical world. Putting a diagnosis on paper that the doctor technically didn't have to used to run some pretty serious risks. Pre- HIPAA (1996) those risks extended to your job and social life too (patient privacy was actually not actually a law back then). Even today, certain health conditions (including things like gender dysphoria or schizophrenia) may be looked at unfavorably in some areas if you're trying to do something like adopt.
So be open about the fact that you want to know, and if necessary, why that information is important to you.
Finally, come up "normal" on screening questions. At the beginning of the appointment, the person who rooms you will ask you a set list of questions. These are called "screening questions" and they include things like "do you feel safe at home?" and "does transportation keep you from getting to appointments or getting medications?"
Reasoning:
Unfortunately, if they find anything they need to talk about when asking these questions, they generally have to address these problems at the appointment, which means time they cannot spend on the problem you're there for.
If youdon't feel like lying and think you might have come up "positive" (something needs to be talked about), you have to be extremely clear that you would prefer to make another appointment to discuss the screening test, and today stay focused on the problem you came in for. It depends on the doctor as to whether they are willing to take that risk (and it genuinely is a risk, to them), and you also end up eating up some time.
My wife's opinion is that you know yourself better than a screening test anyway, and sometimes you do have to lie to get what you need.
So, you know, you do what's best for you.
Keep Reading:
Choosing a Doctor:
When you are first starting out looking for a doctor, you will probably have the choice between family practice (either a family practice doctor or family practice nurse practitioner) or internal medicine (your standard adult primary practitioner). Having worked in family practice I may be biased, but personally of the two, if you're looking for someone who is most likely to listen off the bat, it's going to be someone in family practice.
You may also have the option between a private practice and a residency. Of the two, I would choose the residency, because at a residency the docs you see are going to be residents who, 1- just finished up learning about all the zebras and can still remember them, and 2- are not yet jaded. Which if you think you have anything that isn't the most straightforward case of diabetes/heart disease/COPD, that's what you need.
The First Appointment:
So here's the thing. In order to get in with a doctor, you have to do something called a "New Patient Appointment", or NPA. An NPA takes a long time to get (sometimes months) but it is worth it to get a primary care doctor. An NPA is a little longer (usually about an hour or two) and most of that is going to be screenings with a nurse or medical assistant.
Understand that very little will happen at this appointment. It is just for you and the doctor to get to know each other (through a pre-programmed set of questions) and get some background info on you. Sometimes there will be time to address one thing. Use the checkout from this appointment to make more appointments that will fix things.
173 notes
·
View notes
Note
i have a really big thing for hypnotism in theory but in reality i can't actually be hypnotized and it's so upsetting :( like im sure i could be but i've never managed to focus hard enough and actually be hypnotized, not with actual audio or with text videos or with purely text scripts or anything and i don't know what im doing wrong or if im doing everything right and i just have an undiagnosed something or other
Alright folks, lets play a game of "trance diagnosis"!
There's a number of different common reasons that files (especially generalized files) would fail to hypnotize you. Let's go through them!
A. Being Afraid of Doing Things "Wrong"
One of the most common that I've seen is the idea that you need to do every suggestion and command the way the hypnotist intended and analyzing every commmand in order to do it "properly", and if they do not, the spell will be broken.
Simply put, the way you receive the command is the right way to receive it. Do what feels natural and don't read into it heavily, and just go with the flow. Trance is stubborn when you let yourself sink into it, and one or two commands or suggestions that don't work is not enough to shatter that unless you convince yourself that it is.
However you do it is correct.
B. Recursive Self-Analysis
This is related to the previous, but is the general idea of constantly analyzing your state of mind to see if trance is "working" and what effects are different than before. This takes your focus away from the session itself and almost dissociates you from it.
Just read or listen and try to vibe.
C. Pre-set Expectations for Trance
Trance will not take control from you, and it will almost certainly not feel the way you expect it to if you are new to trance. I have had sessions where I feel basically awake and was still deep in trance as well as sessions where I could hardly think or function.
Trance will not feel like anything else you've experienced exactly, and it is somewhat personal to you.
D. Believing You Cannot Be Hypnotized
Yes, believing you cannot be hypnotized does actually make it harder for you to go into trance. It's not impossible to (because trance is the natural consequence of several basic parts of our minds), but with something like generalized files, it can make it completely ineffective.
So far, I have never met someone immune to trance, from the deeply anxious to the deeply distractible. Every single one of them has dropped deeply for me. To be unable to go into trance would mean to be entirely unable to focus and for some part of your mind to be entirely absent.
Now, what are the solutions to this?
A. Learning How Hypnosis Works
In contrast to what you may think, learning how hypnosis works does not ruin its effectiveness, and, in fact, makes it more effective in many cases. The very first thing I do when introducing someone to trance is explaining, in full, how it works on the basic level. I do so while putting them into trance at the same time.
This clears up misconceptions and also leaves the subject more informed and more assured in themselves. It also has the effect of making them better protected against manipulation and abusive practices.
B. Finding a Hypnotist for a Personal Session
If you cannot seem to troubleshoot this yourself, it's best to find someone who knows how to tailor a session to you specifically. The person who asked this is anonymous so I cannot speak to you personally unless you reach out, but I myself could potentially help in some instances. That being said, I'm quite busy these days, so thats not a promise.
If anyone else has questions, do not be afraid to send in an ask, I love answering them. Have a nice day, everyone.
154 notes
·
View notes
Text
random astro observations ! p3 💋☆°


take what resonates leave what doesn't!!
i notice that many people with bipolar discorder have water moon or 8H moons/12H moon,moon-uranus/moon-pluto, sun-moon (hard aspects) or cancer mars (its not for self diagnosis its just my observation!!) btw i also have bipolar to be specific i have bipolar type II with mixed features and also i have bpd and i have cancer moon 8H opposition pluto in 1H and in my moon persona chart i have pisces moon, moon conjunction uranus, moon square pluto,sun square moon, moon square asc, moon square mercury and so many others hard aspects to the moon lol so yeah... ☆°
gemini placements/3H placements tend to play hands when they talking !! ☆°
animals can be very attracted to 6H placements peoples i notice this the most with 6H suns, 6 moons, 6H venus and 6H neptune !! :3 ☆°
peoples can easly can not understanding what pisces mercury/3H neptune/mercury-neptune/3H pisces are trying to say .. and these peoples also can struggling with what they are trying to say and they mind can be very chaotic also they can escaping alot from reality and others can see this very easly also when u have this u can notice that others peoples can ignore u so much when it comes to what u saying for example u can ask someone who is starting next to u abt something and they just ignore u or u will trying to say something in school (for example) but other person will say this and bc of this u will get ignored (its also personal experience i have pisces mercury 3H conjunction neptune in 3H 😭) ☆
pisces moons/12H moons/moon-neptune (conjunction,inconjunction/quincunx, square, opposition) can have a mother that is playing a victim alot and u can feel very ignored by ur mother like she never listen to u when u r trying to speak or she will be ignoring what u r saying only to say what she wants ☆°
5H neptune can experience with drugs for fun and also experiment alot with drugs hmm also maybe doing drugs bc of being bored and having nothing to do alsooo 5H neptune peoples are very creative with love to art, music, spirituality etc!! also can use music as a form of escaping from reality :3 ooo and when these peoples will have a kids they can have a kids with a strong pisces placements/pisces in big 3/big 6 or neptune dominants/12H stelliums !! kids there can also be very artistic ! ☆°
9H saturn peoples are easly getting into melancholy mood and can have hard time to see something from positive side (3H saturn, 1H saturn, 12H saturn or 10H saturn can relate too) ☆°
12H saturn/pisces saturn/saturn-neptune(opposition,square,inconjunction/quincunx) peoples can be afride of hospitals or water ! also maybe bad experience with hospitals/doctors and water ☆°
8H uranus can have weird kinks 😭😭
9H uranus maybe are people with strong belief or their belief are seeing by others as controversial or "weird" ☆°
11H uranus can have many online friends !! ☆°
1H neptune peoples... something about they look and aura is just so pretty i lov yall sm !! they looks so angelic and sweet !! ☆°
2H moons can have fluid self esteem (one time they love themself and the next time hate how they looks, acts etc!) ☆°
3H mercury/gemini mercury always want to have they last word help and can fighting with u for fun (self exposing myself ☹☹☹) ☆°
mutable venus/mars peoples and gemini moons can be type of people that can experiment alot in relationships and even can be part of lgbt+ 🏳️🌈 ☆°
#astrology observations#astro notes#astrology#astro observations#astrology notes#neptune 1st house#neptune#neptune 5th house#uranus#11th house uranus#mutable signs#gemini mercury#mercury 3rd house#uranus 8th house#saturn 12th house#pisces#zodiac signs#saturn 9th house#saturn#pisces moon#moon 12th house#6th placements#cancer mars#aspects#sun#moon#planets#ascendent#mercury#mars
2K notes
·
View notes
Text
Kieran is autistic and you can't change my mind!
Okay, I KNOW that I'm not the only one who holds this headcanon...but I wanted to do an analysis on Kieran anyway, especially since my best friend @sinnohanvulpix said she'd love to see me do one. Credit to her for all the screenshots used btw. The GIFs on the other hand were either found on Google Images or created by me using gifrun.com and these YouTube videos:
youtube
I did not use my own footage for this at all...as proof here's what MY character in the game looks like...he has my real name but I tried to make him look like Orange which is why he has the orange eyes 😅

(Sorry for the bad quality btw...taking pictures of my Switch screen is hard 😅)
Okay, now without further ado, let's get started with the analysis!
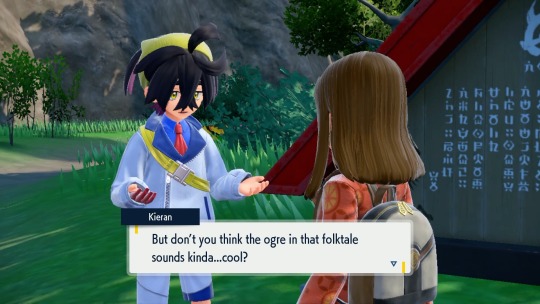
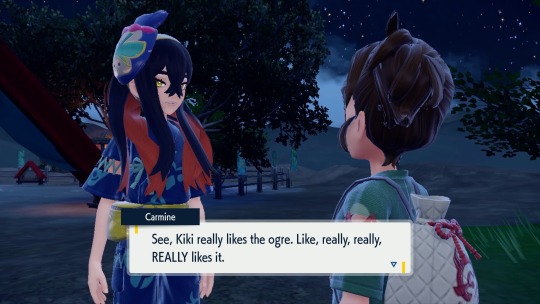
First, Kieran has a CLEAR special interest in Ogerpon, he admires and looks up to her, he was obsessed with the story of the ogre, he was always trying to go to her den and meet her, he has a meltdown when Ogerpon chooses the player over him, etc. Carmine even says that Kieran "really really REALLY likes the ogre" and that made me think, "Ah! Special interest!"
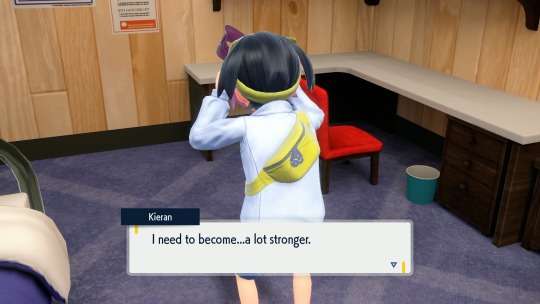
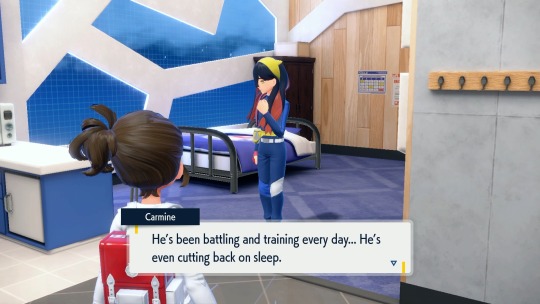
And then at the end of the Teal Mask he gains a new special interest in getting stronger to beat the player...and he hyperfocuses HARD on that...to the point of it being detrimental to both his physical and mental health, as he was doing nothing but training during that time...he barely ate, barely slept, just trained...and that is not healthy. It's a rare example of media showcasing a special interest being unhealthy and absolutely CONSUMING one's life, and the consequences do actually show for it.

Kieran is very introverted and doesn't know how to make friends very well. I actually think the player is his first friend considering his surprised reaction when the player says they consider him a friend, and following this, he quickly becomes a bit...too attached to the player, as he doesn't quite understand how friendships work.

(This is also such a neurodivergent way to say "I'm so happy I finally have a friend")
He also struggles socially, as is a requirement for autistic people to qualify for a diagnosis. Kieran specifically has a hard time reading social cues, he struggles with making eye contact, he has clear anxiety when talking to people as proven by his little stutter he has at times.

(This is an adorable screenshot 🥺)
He also struggles with social and emotional processing (and might have alexithymia as well due to his sudden huge outbursts of emotion), and he also struggles with initiating conversation as well, as seen when he tries to talk to Penny at the League Club. They both have no idea how to even start a conversation with each other and it's honestly pretty adorable seeing the two quiet adorkable kids trying their best to hold conversation. I get it, you two, initiating conversation is really difficult for me too.
Also the way they try to start the conversation by talking about the weather...that's really funny and ironic to me because that's what NTs do all the time. NTs always use the weather as a small-talk conversation starter but NDs like me (and Kieran and Penny too apparently) just don't get that stuff.



(These two are so neurodivergent it's great and I love them both 🥺)
Kieran also has four in-game animations that I personally see as stimming. The first one is him tapping his fist against his hip when he's thinking or nervous.

(Focus your attention to his hand here and you'll see it.)
The second one is him playing with a strand of loose hair, usually when he's nervous.

(The little nervous side glance at the player is relatable and adorable 🥺)
The third one is a more agitated stim that he only does ONCE in the entire game...and that is tapping the front of his foot on the ground. I do that myself when I'm agitated or impatient, somehow it's comforting, especially since for some reason I really like the way my shoes sound when I tap them on the ground... especially since I got my brand new Infernape-themed shoes, they sound extra satisfying because they're brand new.
(This is not the way most people tap their foot...I've never seen an NT do it like this...only other NDs such as myself and one of my brothers)
The fourth and final one is, unfortunately, a stress stim...Kieran runs his hands very fast through his hair and it also looks like, to me anyway as someone who has self-injurious stims myself, that he is digging his nails into his scalp as well while doing that. I do something similar myself, though on top of running my hands through my hair and digging my nails into my scalp, I also pull at my hair...yeah... self-injurious stims are no joke...and I'm kinda glad Kieran's autism coding brings attention to that aspect of autism...at least in my eyes as someone who does those things myself.

(He's in so much stress here, poor kid 😔)
Another aspect of autism that I'm surprised and kinda glad that Kieran exhibits as an autistic-coded character is meltdowns and shutdowns. Kieran has actual meltdowns in the game! This is something we have never seen in such an in-your-face way in any Pokémon game, and as someone who regularly has meltdowns myself, it hit me in the feels whenever I saw him having them. His first meltdown is in the Teal Mask when he steals the Teal Mask and runs off to Loyalty Plaza where he battles the player. He yells at Carmine and the player for treating him like an outcast...which is unfortunately something that happens to a lot of autistic people, myself included. Kieran screams at the player and Carmine for for lying to him while doing his stress stim, before running up to the Lousy Three's shrine and punching it, without any regard for his safety, which is also something autistic people may do during meltdowns...I know I have no regard for my safety during mine. After that's all over he gives the mask back to the player and goes home, leaving the player to talk to Carmine alone, who says that she's worried and thinks it's just "teen angst". When I saw that I was like, "...Uh, Carmine...I don't think it's just that, I think your brother is neurodivergent and really needs a lot of help and support because he's struggling a lot right now..."

His second meltdown is also in the Teal Mask, when he wants Ogerpon to go with him but Ogerpon wants to go with the player...Kieran can't process that and doesn't understand how to take Ogerpon's feelings into account, instead demanding the player to battle him for the right to be Ogerpon's partner. He collapses on all fours after being defeated again, and it gets worse...he looks like he's crying while the player battles Ogerpon in order to catch her. After the player catches her, Kieran wonders why he can't be like the player, and runs off crying, locking himself in his room for the rest of the story. The end of the Teal Mask has him doing his stress stim while being consumed by a new special interest in a very detrimental way...that interest being becoming so strong that no one can defeat him...including the player.
Kieran's third meltdown is in the Indigo Disk, after the player defeats him in the championship match. That meltdown is a full-on cutscene, where it is CLEAR to see his spiraling mental state through the visuals, and he holds his hands on his head like he has a headache while trying to process the fact that he lost to the player AGAIN (which is also relatable as someone who struggles with processing difficulties myself...it really does give headaches and it is one of the worst feelings when I just can't process what's going on around me or the emotions I feel or anything really)...he collapses to his knees and looks like he's breathing very hard as he is so upset and distressed at this loss. It is definitely one of the most heartbreaking scenes for me because this is a CLEAR CUT MELTDOWN in my eyes and it hits me in the feels like a TRUCK to watch that cutscene.
Also, in the Terapagos fight, Kieran has a bit of a shutdown for a bit, standing there frozen, thinking he's useless and can't do anything right (which is relatable as I have regular shutdowns as well, and I also constantly feel like I'm a failure of a human being who can't do anything right)...but let me tell you, when the player finally gets him to snap out of it and convinces him to help and he opens his eyes revealing that the light is back in his eyes as well as visible tears...I cheered (and teared up myself). My boy was back, and I was so happy.

(When I first saw the tears I was like, "NOOOO don't cry Kieran! 😢)
Also in the Indigo Disk, Kieran seems completely different and "no longer like his usual self". His autistic traits are (mostly) nowhere to be seen as he becomes much more serious, angry, assertive,and aggressive. I personally see this as a persona he puts on by masking, which is common for autistic people to do. I myself can't mask, but Kieran definitely seems to be masking here by putting on this persona in order to get stronger and seem stronger as a person as well. This is NOT his real self, this is a FACADE!

We see him start to drop the mask again in Area Zero when he says it seems like they're in a spy movie or something and how cool that is, but once the crack in his mask is pointed out he immediately puts it back on.

After everything in the under depths ends, and you go back to Blueberry Academy, he drops the mask again completely, and goes back to his real, adorkable, relatable self...and stays that way from then on, which made me so relieved and happy.



(This is my favorite cutscene in the entire DLC because of how adorable it is and also how neurodivergent Kieran is being here while apologizing for all he did 🥺)
In conclusion, I think Kieran is a great example of an autistic-coded character who has many relatable traits, and also does a good job showcasing some of the more "unpleasant and challenging behaviors and traits" (NTs use that terminology a lot, not me... that's how NTs unfortunately view NDs a lot of the time) of autism. I used to be afraid of him during the post-Teal Mask pre-Indigo Disk era but that was my trauma and PTSD talking (I talked about the emotional rollercoaster Kieran's story arc took me on in another post from last year after I finally worked up the courage to play the Indigo Disk...feel free to check that out too if you'd like). Now though I can wholeheartedly say that I love and appreciate Kieran a lot as a character, and his relatability is definitely a big part of why he is a big comfort character for me now (please Pokémon put him in Pokémon Masters EX, PLEASE I will literally cry from joy if he gets added to the game)!
Hope you all enjoyed this autistic person's analysis of yet ANOTHER autistic-coded character in Pokémon! I know I had A LOT to say but that just proves how relatable Kieran is, and I love him for that. Let me know what you think and if I missed anything in the comments below!
#pokemon#pokemon scarlet and violet#pokemon sv dlc#pokemon kieran#the teal mask#the indigo disk#mochi mayhem#post mochi mayhem#kieran is adorable and relatable#he's autistic your honor#and nothing can tell me otherwise#i know i'm not the only one with this headcanon#but i wanted to analyze kieran anyway#because i can#actually autistic#autism headcanons#pika's headcanon#long post#pika talks#Youtube
122 notes
·
View notes
Text
i both firmly believe that self-diagnosing saved my life and i think that the way tiktok and instagram have recently been spreading misinformation about mental illness/neurodivergence is incredibly harmful.
people who are looking for answers are already people who are in a vulnerable situation.
much of the misinformation appears logically sound; and is presented as definitive fact (prefaced with claims such as "research shows"). it's imperative we remember correlation does not prove causation. it is incredibly dangerous to make definitive statements like "if X happened in your childhood, you now Z as an adult." real scientists will almost always use may or other less-definitive terms. similarly, equating one behavior/experience with any single condition is also unsafe. many conditions have overlapping symptoms; and many people "mask" their key symptoms, even to themselves.
we cannot discern from a singular data point any conclusion. in official diagnosis, for a behavior/experience to be considered a symptom, it must significantly influence your life. many people enjoy an organized space. that is a preference. disrupting your daily life even at personal cost in order to prioritize organization is more likely a symptom.
again, a single data point is not an effective diagnostic tool. it is necessary and important work to catalogue and consider all unwanted/distressing behaviors in order to understand a complete picture of the person.
i will see creators in paid partnerships make generalized behavioral/emotional claims that apply to a large portion of a community, and then they will suggest that the "solution" to that behavior is through their paid partner/through their personal support. "follow for more psych tips/facts" is an incredibly evil marketing tactic. i very rarely see unpartnered/unbranded content on how to aid/comfort those behaviors and feelings.
much of the misinformation employs a subtle technique (called confirmation bias) of setting up a conclusion before "proving" the conclusion. "you know you have X when you experience A,B, and C." no person's experience of their conditions/behaviors will look exactly the same as another's. while knowing certain things might be a sign/symptom of a condition, it is irresponsible to consider it definitive.
confirmation bias is unfortunately extremely effective on tiktok specifically. the algorithm will notice that you interacted longer with the video that "proves" (through a singular video) that you "have" a condition. it will continue to feed you related videos that further confirm what you believe.
this is dangerous because we are, unfortunately, not good at knowing ourselves. i did not know it was unusual to vividly nightmare every night; i didn't consider it a symptom. i was similarly dismissive also of any other signs of my PTSD - i incorrectly assigned them to anxiety/adhd. on the small scale, this can mean a longer journey to healing. on the larger scale, it can mean people with extremely difficult situations are unable to get the help they need.
please, if you can, and you're looking to self-diagnose: be careful about what you assume about yourself. try to keep an honest journal of what you're thinking/feeling/doing for a few days.
do not go in with an assumption. try to keep an open mind. i think we all "suspect" we have something - but like i said, i completely missed my own PTSD symptoms, because i suspected the ADHD the most, and only "saw" those symptoms.
do your own research. if the tiktok says "research shows", google that research. figure out who paid for that research. do further research related to that study - has it ever been repeated? is it peer reviewed? do other researchers seem to accept it as conclusive?
if you feel you really resonate with the materials of one person's experience with a condition, find other examples. see if you relate to other creators who identify similarly.
and please - please do not stop once you come to a conclusion. i fully believe that the diagnostic process should be seen as a first step, not a destination. by knowing what you might be struggling with, you gain an incredibly powerful tool on how to gain peace with that condition.
if you feel yourself emotionally respond to a tiktok/etc that suggests something that might be true about yourself, i'm glad you had that experience. but it's also important to not relax into the "easy" answer. interrogate it. start googling what else that could mean; what ways you could work on healing that wound.
healing does not "belong" to any one condition. i want you to begin to look into healing no matter if you have "proven" you have a condition or not. it is never selfish to practice responsible self-care. even if you don't relate to having adhd, you are not harming me by using adhd-inspired study tips. it is not making my condition worse for you to seek peace by asking for more time on tests. even if it was - the fault would be with the system, not in your need of something the system makes inaccessible.
remind yourself that everything you experience is real. and because it is real, it is complicated. while things might be related - even sometimes clearly related - a stranger on the internet cannot make that discernment for you. you as a person deserve the work, attention, and care that goes into the process of unravelling the harm that has been done to you.
it makes me very, very upset to see how popular these videos have become, because they're so irresponsible. and they clearly are targeting a vulnerable group. for example, making generalized claims about children of unloving caretakers is targeting those who have experienced neglect. there is no way to use 30 second videos to correctly analyze what that neglect might have caused in your adult life. i'm sorry, but it's snake oil.
i know it is so powerful soothing to recognize that you aren't broken. that others exist like you out there. i want every person looking for answers to find their answer. i want you to feel seen and heard and understood. i want you to find your community.
i just want it to happen safely.
#every time i write this im like#i just want to say a short thing about this#and every time it ends up being 12 pages long#but since it keeps happening#and i keep seeing shit like this...#this isn't even everything i feel about this#i hope this is clear like#what im saying is#NOT ''you don't have it if u selfdiagnose''#it's instead....#you might!!! just don't let 1 or 2 videos confirm it!!#also!!! don't assume that symptom A belongs to condition X!!#even as someone who did eventually get diagnosed like#i still find myself being like - oh that's my adhd#only to figure out 12 hours later. nope that was a panic attack#also none of those videos are about how to HELP the behavior#also this doesn't talk about getting a therapist eventually but please get professional help if you can#it took me fucking forever tho#what im saying is that in the meantime#u can heal now#this is too long im posting it on a sunday so nobody reads it
3K notes
·
View notes
Text
Endogenic Systems and Experiences in the Neurodivergent Community
We tend to stay mostly on the fringes of syscourse nowadays without directly interacting with it too often but I'm going to post this more broadly and less focused on our specific instance of this because community-wise I think it's important to talk about.
Endogenic and other non-traumagenic systems are so commonly excluded from so many neurodivergent-safe spaces where they would otherwise be able to gain knowledge about the disorders they might have, share experiences and coping strategies with peers, or at least have a sense of community that is so commonly valuable to disabled and/or neurodivergent people. In a lot of cases, even people who only support non-traumagenic systems get shoved out.
[Continued under the readmore as it's long.]
This obviously harms non-traumagenic systems, but I have to point out that when people sit there and say "we care about REAL disabled people!", I have to say.... Do you? Because if you did care about those with mental illness, physical disability or neurodivergence, you in my mind wouldn't exclude them based on something unrelated to the topic itself which might even be something as small as holding an opinion that other people get to be the judge of their own experiences. You can say that you care about "real" disabled people, but what about when a traumagenic DID system also has a tulpa that they consider just as valid and real as their alters? What about when a system labels themselves as quoigenic because in reality, you owe no one the knowledge that you are vulnerable and traumatised? What about when a system starts out as endogenic but gains so much trauma later on that they develop dissociative symptoms?
We're quoigenic because while yes we are diagnosed with DID:
DID does not have trauma in the diagnostic criteria so our diagnosis doesn't mean anything by way of origin. Nontraumagenic is not the same as nondisordered the same way that traumagenic isn't the same as disordered.
We cannot remember a time before we were plural so we cannot say with accuracy what our actual origin was.
We have headmates we consider to be from both traumagenic and endogenic origins and it feels unfair to pick one.
We don't owe anyone a quick little "hey, we have trauma!" flag on our pinned post which can easily paint us as a target. This is the exact reason we don't share our triggers online--it's not safe.
You don't owe anyone personal medical information including your diagnostic history, your trauma history or lack thereof, your current medications or how many times you've been in a hospital. That is your business and yours alone to decide who you share it with. It's downright dangerous to share some of it, especially so publically. So who is anyone online that clearly isn't your specific medical practitioner to decide whether your experiences are real enough to allow you into spaces meant for a usually completely unrelated thing? Why would someone holding the opinion that endogenic systems get to decide what labels they use be denied access to spaces just because they support people with differing beliefs and/or experiences?
If we as a system with multiple disabilities want to go into a space for people who are schizoaffective because we need others who won't immediately jump on the ableism train when discussing something we're diagnosed with that has so much stigma, should we be denied that just because we don't label our origin with a clear-cut "we are traumatized!!" label? Should we be denied access to spaces because we don't want to sit around and smile while parts of our system and other members of our community are called fake and evil and whatever else they come up with? It's so common in spaces for people with disabilities to be exclusive to traumagenic systems and people with an anti-endogenic mindset that people don't realise they're not only hurting the endogenic community, but literal chunks of their own community itself.
I can't even begin to understand the reason why.
Endogenic systems by just existing do not cause harm. They're not like a transphobe you would not be safe around by default of having a label. Not every nontraumagenic system is a saint but if you took any communtiy and called everyone in it the equivalent of an unproblematic holy angel, you'd be lying. People are bad in every community, some worse than others, but the nontraumagenic system community literally just wants to exist--and yes, sometimes a nontraumagenic system (or supporter of such) does have dissociative symptoms, or maybe they have autism, or maybe they're physically disabled. Should they be not allowed access just because of the way they chose to label their system, or their opinion of people picking their own labels for their personal identity?
What exactly is the reason they're so excluded everywhere? I'd try to assume that this level of exclusion (to the point of endos being on DNIs next to transphobes and racists) would mean there's some real harm being done on a community-wide scale, but even when looking for it there isn't any explanation we've been able to find. "They're fake" is all we seem to see which has no actual backing whatsoever. "They're harmful" is another but.. How? We might be looking in the wrong places, but we have never seen an actual explanation for how nontraumagenic systems cause harm as a community just by being themselves.
At this point, I have to wonder how many people who say "we care about real disabled people!" are just covering up their "we care about socially acceptable disabled people who I understand and/or do not find cringey" sentiment instead. Being neurodivergent should never be about fitting into tight little boxes--it's part of the whole point of having a community like this. You're not the majority, and that's okay. So why are we dividing the disabled community into boxes too?
Of course, this doesn't only apply to ND spaces. LGBT+ spaces are similar and even more divided from the concept of being a system that it makes even less sense to block nontraumagenic systems from entering the space. How does their system origin relate to their LGBT+ identity? Sometimes it can, but should a trans person be excluded from a trans space because they have a friend who is an endogenic system and they support them fully?
Overall, the main point is that it makes no sense whatsoever to be anti-endo in general, let alone so violently anti-endogenic system to the point where you hurt members of your own community due to it. Sometimes from something as simple as them supporting endogenics alone. Your safe spaces aren't actually safe if you exclude a nonharmful group who also belong in that space due to having a personal identity or opinion different to yours. If you want somewhere to be a safe, inclusive space, it should include everyone as long as letting those people in won't cause harm. People who are seeking to cause harm (racists, transphobes, etc) obviously do not belong in a safe space because they seek to harm others, thus making the space unsafe. But people who just want to be themselves without harming anyone should be included in your space if they fall under whatever it may be topic-wise. Even the "cringey" ones. Even the ones who don't quite make sense to you or have "contradicting" labels. Even the ones who use labels completely differently to the way you do. And even the ones who are uninformed or misinformed but trying their best to learn. Your safe space is not safe if it excludes those who do not follow your every single mindset and thought without any deviation.
#reiterating that traumagenic and disordered are not synonyms and that you can be disordered and endogenic too by the way#important note here#plural#actuallyplural#plural system#plurality#endo safe#pro endo#system#alterhuman#didosdd#actually did#syscourse#actually endogenic#endogenic#disabled#quoigenic#did system#did osdd#neurodivergent#did#disability#op#mystery (they/it)#tw#tw: syscourse#tw: ableism#everything althu#althu experiences#everything plural
81 notes
·
View notes
Note
advice on how to get over the fear that t is going to make me ugly? or that i’m going to miss “the old me”
i’m a queer trans guy and i’ve been questioning going on t for years now and i know i definitely want bottom growth, body fat redistribution and more body hair.
but im err on the side of face and voice changes. i’m scared of disliking my new voice and suddenly growing dysphoric over it (i dont have too much voice dysphoria now) and disliking how my new face will look. i’m kinda genderfluid as well so it’s complicated. but i don’t want to go my whole life without knowing what it’s like to be on hrt. but i can’t get over the fear of looking/finding myself ugly and undesirable and losing my community... which is ironic cuz i find other trans men attractive as hell. i discussed this in therapy and i still feel this way :/
i wish there was a way for me to start without telling anyone and then breaking the news when i’m experiencing changes and feeling more confident about it. i have my gender dysphoria diagnosis and i can start if i want to, but i need my family’s financial support. i don’t want to make it a big deal since it’s just something i’d be trying out to feel more like myself in certain ways.
sorry this turned into a long ass rant and you don’t have to reply but i’m just gonna kindly leave it in the ask box 💀
There's a post that goes like "all of life is irreversible. i cannot go back a single second" and I think thats something good to keep in mind when you are thinking through this. You are already living with a body that has changed and will continue to change in ways largely out of your control. You are already living in a post-irreversible-alteration body.
If you do go on T and find you don't like how your voice sounds: for one, you can stop at any time (& if you haven't checked out microdosing as an option, you should). But two: plenty of people live with a deeper voice than they want. Plenty of people live with facial hair they dislike. You can pursue the same therapies and procedures they do. Or maybe you don't, and you find ways to live with a voice or face you aren't totally in love with.
So much detransition fearmongering, especially directed at transmascs & assoc. trans people, heavily relies on the specter of the fallen woman, itself steeped in trans-misogyny & intersexism. The idea that, for one, a "woman" who has mixed-sex features is ugly and undesirable, and two, that a "woman" made undesirable is forever doomed to be miserable and worthless. The transphobic story of detransition keeps our bodies stuck in this moment of revulsion and regret, narratively preventing us as characters from being able to move on and live happy lives in atypical bodies. Even if you do regret/dislike some things about T, you are not forever stuck in that feeling. The story does not stop at that! You will just keep living and find new ways of dealing with your bodily feelings!
The social aspect of this is a bit more complicated but I also have some firsthand experience with it. Because, as mentioned before, there's a lot of transphobic misogyny/misogynistic transphobia that affects transmascs & others who go on T, who have to confront the feeling of losing your potential desirability. And then there's also the way many people are treated after going on T, facing a whole new area of bodily scrutiny: you may suddenly have people making comments about how someone needs to force teenage boys to shave because their facial hair is a personal offense. I went from being self-conscious about how high my voice was to being self-conscious about how undeniably trans my voice was. And, specifically, my facial hair, voice changes, etc. were all signs of my transmasculine desire, and I became self-conscious about how obvious it was that I desired being trans, I desired this body. I could no longer let everyone pretend I was a cishet girl at family gatherings and avoid confronting these issues, because I had essentially written I WANT TO BE A TRANNY all over my physical form.
This is something I'm still struggling with myself. I, like many other queer & autistic people, already struggled with feeling desirable or worthy of being seen alongside conventionally attractive cishet people who could act normal. Being visibly trans, and taking a huge step away from the desirable cis-perisex-girl body, can really open up that can of worms. Especially being genderfluid/genderqueer! Because we often cannot find a comfortable space for ourselves within the conventions of attractiveness for cis men, like some binary trans men are able to.
But ultimately, I don't regret going on T at all. I would have had body issues regardless, and I got a lot out of going on T. I think mentally preparing yourself to struggle with these things, and seeking out other transmasc people, is a big help. Again: all of life is irreversible. we cannot go back a single second. We are already living in imperfect bodies we struggle to love or see as worthy. If you know you want some of the things T can offer, and you don't want to go your whole life without knowing, then just do it. Dive in, and don't feel any shame if you decide to get out. Just keep living and finding ways to live better right now.
114 notes
·
View notes
Text
What is unitypunk?
Unitypunk is a disabled subculture encompassing other movements like cripplepunk, neuropunk, madpunk, and pluralpunk, as well as other movements like the anti-psych, pro-delusion, and pro-self-diagnosis movements. It's focus is on building a single, disability-justice-focused coalition; a united face against all kinds of ableism
To this end, the movement rejects gatekeeping of terms and talking about experiences based on having the "right" diagnoses or the right "kinds" of diagnoses. It is focused on assuming good faith, on people's similar experiences being shared in turn as a way of saying "I understand, and stand by you", on pulling up chairs rather than building up walls.
This is partly in response to small but vocal minorities within the community who insist that their experiences are entirely unique to their diagnosis or type of disability, and that disabled folks of other kinds are not welcome in their conversations about disability justice. This flies in the face of intersectional anti-ableism, and as I and other physically disabled neurodivergent people have noted, often leaves us unable to talk about a full half of our experiences.
The foundation of unitypunk is that the brain and body are inextricably interconnected - all physical organs that are interdependent on one another - and that while for some the symptoms of physical and psychological disabilities may be entirely separate or different, for others they are impossible to differentiate or functionally the same. The gut is the second brain. The body keeps the score (of trauma). Where in your body do you hold your emotions? The mind-body connection. All commonly used phrases when talking about disability, all illustrating this connection.
A psychological condition may be physically disabling. Autism can cause significant mobility issues. Anxiety can cause cardiac issues. Something like agoraphobia may cause someone to become as effectively housebound as someone with mobility issues and an inaccessible door. A physical condition may also be psychologically disabling. Absorption issues in the gut, particularly in regards to vitamins D and B12, can wreak havoc on the brain. Thyroid and adrenal/endocrine issues are one of the first things tested when seeking a mental health diagnosis. And of course, chronic illness can cause depression, anxiety, and trauma. Whether direct or indirect, the effects are the same; a complexity to the manifestation of symptoms that cannot be neatly squared away into little boxes.
This movement recognizes that only by recognizing and celebrating the breadth and depth of that complexity will we be able to achieve true disabled community and solidarity. It prioritizes a united front over personal differences. You don't have to like the disabled person next to you, but we all have to put aside any petty squabbles and fight for each other, or go down together. This includes being intersectional and inclusive of all other identities, whether you understand them or not. This means not disparaging or writing off identities, and judging people for their actions, not their labels. It also means, while it's fine to make spaces focused on a specific aspect or kind of disability, that it's important to recognize that real life experiences are messy and won't always respect neat lines being drawn. This is especially true of the experiences of physically disabled neurodivergent people, who are multiply marginalized and deserve to have our experiences heard and respected.
The most important things you can do here are to talk, and to *listen*. This account, this *movement*, is just a starting line. The end goal is total disabled liberation, and the only way we will get there is marching together.
#unitypunk#disability#cripplepunk#madpunk#neuropunk#pluralpunk#antipsychiatry#antipsych#psych critical#anti psych#autpunk#dyspunktional#alterpunk#pro delusion#descrippunk
476 notes
·
View notes
Last Seen Blogs

the-piligrim-stuff
Untitled

healthaddha
healthaddha.com

ubdb1h-blog
- ubdb1h.tumblr.com

assistantforawar
For Fuse or For Earth?

bleureux
Little Dude