#rethink mental illness
Text

forever friends................dream team...............for all eternity...........
#the ghost and molly mcgee#tgamm#tgamm spoilers#scratch mcgee#scratch tgamm#molly mcgee#todd mortenson#thank you for everything tgamm 😢#the series finale absolutely WRECKED me#i was BAWLING#what a perfect ending...#scratch is such a special character...the way this show depicts depression and mental illness really hit me so personally#it's really making me rethink my perspective on life...i'm gonna hold this stupid ghost man close to my heart for a long time#i've been watching this show since the day it premiered so it's crazy to see it end...#i wish it got treated better by disney but i'm so grateful for what we did get#also while i was coloring this i realized the shirt scratch wears at the end of the episode is the same color scheme as his ghost design...#😢😢😢
127 notes
·
View notes
Text
so so So fun how i realised that uc fucked us over in like a kind of massive way (out of over £3k) and im desperately trying to contact any advice service and NO ONE IS AVAILABLE!!!!!!!!!!!!!!!!!!!!!!! i want to fucking bite people. and not only that but i have a Trial Shift Nannying Children today IM GOING TO DIE
#laila#i actually just want to break down#sfe cant help me uc cant help me the tribunal ppl cant help me#until i know for sure whats going on and that im right#ive called cab mind rethink mental illness a youth legal advice charity#and NO ONE IS AVAILABLE#the fuck is the point of ur stupid fucking services if u cant FUCKING HELP ME
2 notes
·
View notes
Text
Today in 911:
“I have a medical condition you won’t have heard of, will I still be able to get help?”
“I— of course you can sir, EMS ought to know what it is. What are the symptoms?”
“Ghosts have descended from heaven itself to do horrible and unspeakable sexual crimes to my body. They took out my intestines to [CENSORED] and implanted fecal parasites into my [CENSORED FROM HERE ON OUT FOR MY MENTAL HEALTH. It went on for a SOLID three agonizing minutes]”
“…………………………………………………………………………..…of course, we’ll get EMS out to you as soon as possible.”
#every day I think oh it’s about as weird as it’ll get :)#and then I get a call and rethink all of my life choices#weirdly I have a lot of insight into extreme and severe mental illness#and it’s a shame I can’t really do anything with those insights
13 notes
·
View notes
Text
byan on an average day: glitter. very cute but too many hairclips. makeup done and usually quite vibrant. fitted clothes (oftentimes showing a little extra skin) involving a lot of bright pink. colourful platform boots. more glitter.
byan on a bad day: makeup smudged or non-existent. hair a mess, either falling out of a ponytail or not even pulled back. oversized hoodies and baggy pants. more black than usual. simple combat boots. no glitter.
and they're really out here with the gall to say that they're good at hiding it when they're having a rough time... smh my head
#byan 'i hate looking masc but if i already feel like shit who fucking cares' byun#tbf the 'bad days' in question are like. REALLY bad ones.#like mental illness is fully acting up they're Not in a good state of mind they're having an episode kind of bad day#average bad days or like... more minor mental health stuff they're actually pretty good at hiding bc that's kind of just been their life#...i'm losing my train of thought. hopefully my point has come across???#hi i've been trying to write but i keep writing a sentence and then rethinking everything about it for the next fifteen minutes#making me lose everything else i had in mind for the paragraph and ultimately feeling like nothing i'm getting down is good enough anyway#so uh. it's fun. i'm having fun. definitely not frustrated at all.#hoping dinner will help clear my head a little but we'll see#━━ ˟ ⊰ ✰ ooc ⋮ don't @ me.
5 notes
·
View notes
Text
i do often think abt how much of my image id need to change to be a content creator.....
#id probably have to stop casually posting like this on a public blog#i wouldnt be able to talk about my ' less common ' mental illness stuff like d/as and such without the incredibly#amplified fear of getting mocked and made fun of#i may not even be able to use more than one name for sake of not being too confusing for the fans#idk if i could pick just One Name to stick with forever lmao#ugghh. this is way more complicated than i thought :[ im honestly rethinking the whole thing#i think ill keep this brand tho. i rlly like this phase in my online persona :]
4 notes
·
View notes
Text
Finally did the void quests with Cyella and Unukalhai today and I'm rethinking everything right now because there's no way Zeynha would have just let that kid sit in the ocular like that and hang around the rising stones without ever talking to him. No, that's like. That's his kid. Zeynha would be checking in on him literally every time he gets the chance, there's no world in which he wouldn't
#zeynha and urianger were raising a kid together ages before they actually started dating#and now i want to rethink the entire story while remembering that unukalhai is like also there. just. in the background#ffxiv#this isn't spoilers for current content. i have not done the new patch yet#i don't think zeynha sees himself as being a father figure to him like i don't think he realizes it.#zeynha like “man i feel like I'd be such a bad parent if i ever had kids. unukalhai did you eat dinner yet? let me make you something”#I feel like zeynha's still in the mindset of ''I'm way too young to be a parent'' despite being in his early 30s by the end of endwalker#it's the missing out on most 'normal' experiences in his 20s due to mental illness and disability#zeynha lagorio#.txt
4 notes
·
View notes
Text
y'know what's gross ?
seeing people use SCHIZO as an insult . people want to preach about being accepting of mental illnesses and trying to erase stigma ... but then throw around a term that's considered by most people with some form of schizophrenia to be a slur .
as someone who has schizoaffective disorder and suffers from what psychiatrists consider a form of schizophrenia , it makes me physically ill every time i see this and really shows me who is and who isn't a safe person for someone like me to interact with .
the only people who should be using this term are those trying to reclaim it . for me to say "my schizo brain won't let me find words" or other things like that is different from people without the disorder saying " xyz is schizo and crazy and needs to be locked up " .
what you're doing by saying that is showing that you believe people with severe mental illnesses should be taken out of society and locked in asylums or prisons or wherever else so they're out of sight and out of mind .
it's really upsetting to see and i'll be blocking from here on out if it's on my dash . i already feel shitty enough about friends and family having to deal with my worst days , i don't need random assholes on the internet making it worse .
#ooc ↳ psa#if your way of calling someone out is that they're crazy or a freak or psycho or schizo#then you really need to rethink your language#because it's ableist as fuck and i'm tired of seeing it#ESPECIALLY if you know the person has a mental illness#you're perpetuating the belief stereotype that the mentally ill are bad
10 notes
·
View notes
Text
I crown myself in this tragedy
[Text ID:
It’s a marvel in a decade, having made it here —
my fingers having avoided the unravelling
of telomeres, having traced
through thin plastic bags. In the quiet mornings, when
the day’s rise points out my lack
of a sunny disposition, I wonder if it’ll ever stop;
this coming and going, the soft
insurmountable tides of the world dragging
me out & in again. Lulling—
lulling— lulling—
like the calm rocking of a boat before a storm.
I wonder if I’ll ever make it past my 18th
birthday, if I’ll ever forgive my mother, if
I’ll ever taste cherry wine on a lover’s lips.
It’s just hard to say.
It’s just hard to say.
/End ID]
#best poem I've managed so far meethinks#inspired by me staring out the window & rethinking my entire life bc of a sudden nostalgia & melancholia#& based on my depressed ponderings in my diary while I was re-reading it#certainly didn't expect to live this long lmao#& I stole the 'decade' idea from lady lazarus so...#notice the hozier references if you can#& if you do then the abuse reference is intentional#mortem sibi consciscere#poets on tumblr#writers on tumblr#spilled ink#original poetry#mentally fucked#actually mentally ill#childhood trauma#tw sui implied#original writing#poetry community#mother. can't you see i'm dying?#mine; words and more
3 notes
·
View notes
Note
Its SO upsetting how often the bad guys don't get to have a lasting turnaround. You see it with random side characters, but c'mon guys. Just let them go to prison for a little while and have them come back. I promise you do not have to kill a character off, or base the character off a real life person, thus narrowing their chances of a return even thinner, while building up the possibility of a comeback. This franchise has cursed me with such lovable characters I'll never see again, and my heart can't keep at it like this.
I'm gonna have to just take that suddenly-dropped-off-a-cliff-storyline into my own hands. Gotta pick up all the slack. They're too good at giving tender, heart wrenching moments to characters we'll never see again. Way too good.
Not sure if you know the streamer Crystal, but her reaction to the ending of 3 was the most extreme I've ever seen. She was full on breakdown sobbing, and even the chat was asking if she was okay. RGG look at the hearts you're breaking out here 🙃 Also, your posts about Mine and that ending are beautiful, and you could talk about it a million times. It'll never get old.
the most egregious- pardon the pun- execution of this trope in rgg games is aoki's death.
like legitimately, his death did not need to happen. the past antagonists you could make a decent point for why their deaths were justified (ryuji's probably being the goofiest ngl) but aoki's felt as though rgg was just checking off a to-do list.
i don't really watch rgg content creators, but if someone could send me a clip of that i'd be down to watch: always a fan of watching people be emo over Y3's ending
and speaking of, thank you i have strong enough mental illness that all i can do is talk about that scene over and over again :)
#snap chats#the worst part is im only partially joking about being mentally ill#like i just think of that one directioner fan being a super fan until they took medication and then they were normal#pretty sure if i did the same I Too would have shut up four months ago but to our benefit/dismay medicine's hard to get so <3#i am simply a dog chasing its tail and by that i mean i will simply talk about mine and y3's ending until i die#or until my mental illness latches onto something else idk#but yeah it sucks dick how rgg does so many great and emotional scenes#but like. we never get to fully see that pay off with characters like mine or aoki#like i want to see them have to face the consequences of their actions- ESPECIALLY mine#mine makes me the most deranged Obviously but i just want to know how daigo would react and treat him#we only get a semblance of how daigo felt after Y3 via the rggo story but its not enough#i want daigo to be upset with mine i want mine to HAVE to work things through with daigo#because unfortunately i dont think daigo would just cut mine off i think he still would try to figure out what the fuck was going on#idk i just need something to happen to mine that crushes him and has him rethink his ways a bit#'crushes' yk like. something beside the pavement---#i wouldnt want him to totally change tho. i like him deranged but just channel that deranged behavior to their benefit#brb thinking about mine saying he wouldnt be acting up if daigo didnt get shot again jesus christ i think of that line every day#OK I HAVE TO GO DO A COMM RN ACTUALLY I'LL BE MENTALLY ILL LATER BYYYE FEEL FREE TO SEND ASKS AND ENABLE ME
3 notes
·
View notes
Text
Those damn leftists and their belief in the inviolability of human rights
#*some of us at least because i'm reading things that. mh.#harsher punishments won't prevent violent crimes of any nature from being committed. btw. but ok let's pretend that they will#so that we can go on about our lives without changing or rethinking anything else about our country and society 🫶#lovely to see that we're still equating rape with mental illness too. but well. salveenee & co. what else can you expect#mytext#rl
1 note
·
View note
Text
sometimes i torture myself by intentionally reading thru stupidly rude/unnecessary comments on random instagram posts. why do i do this to myself
#literally what compels people to comment the stupid shit they do#i really need to delete instagram lol#all this does is make me sad and feel kinda depressed and sometimes guilty for some reason#half of these comments i read are things people probably wouldnt actually say irl and theyre just commenting for clout/to make people mad/#/get attention#trapping myself in a well of sadness. and for what#literally i dont even know#sometimes i wonder if my depression and dissatisfaction with life is self-curated partly because of all the time i spend on the interwebs#like is my executive dysfunction and dull outlook on life real? are my mental illnesses real? or am i just over exaggerating everything in#my head because ive been convinced that i have problems when really i dont? is it all self fulfilling prophecy?#does that make it any less real?#and then i remember its all usually tied to my menstrual cycle and is therefore hormonal and then im like o nevermind its real#if you couldnt tell already#most of the negative comments I've been reading lately surround the topic of 'well back in my day we didn't have all this mental illness#bullshit and its just made up by todays youth because theyre weak and don't know how to talk to people 😂😂🤣😂'#etc#and how 'people with mental illness only have mental illness bc they convince themselves they do 😂😂😂😂😂'#to be clear i dont feel that way like if you have a problem you have a problem#if you need help you need help etc#but my dumb guilty conscience is choosing to fixate on this and question/rethink everything and making me feel terrible for existing#anyway. why do i literally go out of my way to read shitty comments like this#is it the aforementioned guilty conscience finding ways to flog/punish itself?????#mine
1 note
·
View note
Text
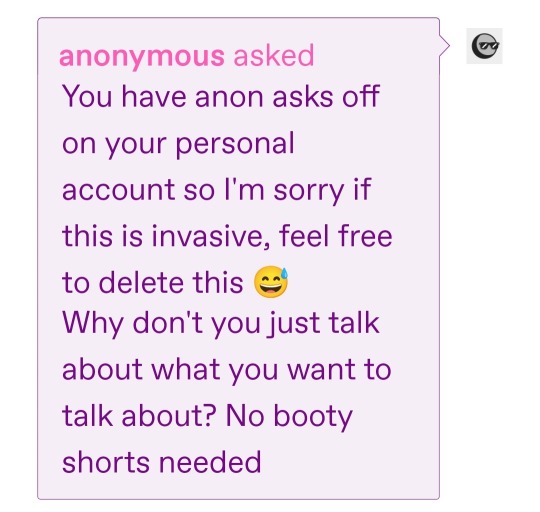
Ok I turned them on whoops!!! I had a full response written out before it hit me that it was rhetorical and more a suggestion to be nicer and more patient w/ myself lmao, thank you anon :] I will never shut up again
#ahaha i overanalyzed it and like actually. figured it out.#i love being mentally ill it makes me rethink my entire perception on things and its very good for dismantling my previous bad beliefs!#and i am currently working on dismantling this one :]#because the basis of it is directly harmful to me#so its great that someone actually pointed it out to make me think more into it!!! thank you /gen
0 notes
Text
my wife brought up a brilliant point this morning: a huge problem with the way we view psychology (a problem which is frequently exploited + used to justify a lot of just. shitty work) is that it lives in a no-man's land between "social sciences" + "natural sciences" in the collective imagination.
consider: one of the first works which spurned my interest in psychiatric abolition was durkheim's work on suicide. as a sociologist ("social scientist"), he uses pretty rigorous quantitative methods to show that suicide is much less correlated with levels of depression than it is with cultural factors (like religion, country of origin, marriage rates). however, people do not respond to the medicalization of suicide by saying "well, durkheim proved that suicide isn't a mental illness symptom, so this is unscientific"- this is obviously a drastic oversimplification of his work + it's commonly understood that sociology does not "prove" immutable social truths.
similarly, i would not comment on a study which identifies changes in t-cells over time among hiv+ patients by arguing that it didn't deeply explore the social environments or past traumas they had experienced, (even though those could have an impact on t-cell count), because i understand that is not the purpose of the research + ultimately they had to choose to control for these factors without centering them in order to obtain important medical information. "this information is meaningless because it doesn't include each patient's trauma history" would be an absurd critique.
among the general population + many self-assured researchers, psychology gets both the privilege of being a "social science" (so we can't expect it to be TOO exact; it's complicated; it's not really saying that's ALWAYS true; if it proves inaccurate that's because culture/social factors must have muddied it up; we can't really expect PROOF for most of it) as well as a "natural science" (you can't question its basic presumptions or you're a science denier; the dsm describes real things which existed even before it was written; it obviously is rooted in biology even if we haven't discovered how yet; reducing its measures to quantitative evaluation is fine + unproblematic).
my point here isn't to argue that psychology is a "social" or "natural" science, but rather that we need to rethink what work those categories actually do + whether the distinction between them is as strict or meaningful as we believe it to be. our strict dichotomies between "objectively proven truths" + "social observations which are ultimately just informed opinions" are exposed when we look at a field which seems to be uncomfortably situated within both. what kind of work might become possible if we abandoned this dichotomy, rather than bickering over whose work belongs in which club?
#tagging this b4 i start: prayers for me that this can be concise cuz i have a bunch of dead french guys to read for class#psych abolition#ok it wasnt too bad
307 notes
·
View notes
Note
WIBTA if I broke up with my girlfriend for not taking her meds?
My (24M) girlfriend (28F) has bipolar and BPD. We've been together coming up on 3 years now. For the last half a year we were together it was pretty rough and turbulent, she was unmedicated and was having suicidal breakdowns almost every day, ended up in hospital several times, threatened and got into physical altercations with other girls who spoke to me or she thought were flirting with me, and I was spending almost every single day of my life having to take hours to talk her down from suicide or self-harm. It was emotionally exhausting and as someone who's also had suicide attempts in the past it was also incredibly triggering and damaging to my own mental health.
For additional context as to why I feel the way I do, my last girlfriend also had diagnosed BPD and NPD and when she stopped taking her medication she became fully abusive both physically and verbally and it took me a year of being absolutely beaten down to finally snap and leave her.
(Obvious note: I'm not saying everyone with bipolar, BPD, or NPD is abusive or that these illnesses inherently make you abusive. They were an abuser who just happened to have those things, and that played into how they acted and thought/felt.)
Current girlfriend eventually got medication and has been doing much better for most of the time since then. When she's on her meds she's a wonderful and generally pretty healthy partner - she's supportive, understanding of my boundaries, checks in with me, she's a year clean from self-harm, hasn't displayed any kind of self-destructive behaviour. She's gotten a job and managed to hold it down (got fired from several jobs in the past because of her daily meltdowns meaning she wasn't attending work), she's started exercising and going to the gym, she's picked up new hobbies, made new friends, she's just been doing great in general.
For about the past month though, she started going days without taking her medication and when I reminded her she would say she didn't want to, that she hated taking it, that she doesn't like the way it makes her feel etc. This is something my last girlfriend said too, and I know it's really common for people with BPD (and maybe bipolar too?) to stop taking their medication because they feel emotionally flat in comparison to how they feel off of the meds. I pretty much said that I couldn't handle going back to how she acts when she's off of the medication again and that if she was going to stop taking them then I didn't think our relationship would last through that kind of period again because last time it completely destroyed my mental health, my sleep, my life and several of my relationships due to how much energy and time I was having to put into her vs. myself and everything else. I suggested asking her doctor/psychiatrist/etc. for another dosage change or meds switch again to see if that would work better (though up until recently they have seemed to be working great so I'm not sure how good of an idea switching it up again would be).
She agreed at the time but I was kind of concerned about whether she'd been keeping up with it or not because over the last few weeks I've already noticed things devolving again - her screaming at me out of nowhere and having mood swings, intense jealousy and possessiveness, impulsive behaviour, even a couple of breakdowns again and having to talk her out of self-harm for the first time in over a year. True enough, today I found out she's been pretending to take her medication and throwing them out. When I confronted her about it she admitted she hasn't taken her medication for weeks.
I pretty much withdrew after that and didn't say anything at that moment but after a while she asked me why I was being so quiet and I basically repeated what I'd said to her in the last conversation, that I was honestly rethinking whether or not the relationship would work because I can't handle that kind of emotional exhaustion and constant sacrifice all over again. I don't mind some emotional support and some labour of love in a relationship because of course I'm going to need to look out for her mental health and reassure and comfort sometimes, that's the reality of loving someone who struggles, but I can't do it 24/7 again. I can't once again put talking her down for hours every day and weathering screaming and violent lashing out all the time at the expense of even my own basic needs and my own mental health struggles (for example my c-PTSD from my last relationship).
When I said that she got very very upset and basically said I was forcing her to choose between me and freedom or being able to live a normal/unmedicated life (which I mean, I guess I can't argue with because in a way I am making her choose between me and stopping her meds), and that I couldn't control her like that. I told her I wasn't doing it to control her and that if she's really determined to go off of them she could, but that I would have to make my own personal choice to walk away as a result of it for my own sake.
She said she'd think about it but ever since that conversation I've been going back and forth in my head on how much of a dick move it would be to flat out just do a black-and-white "Either you stay on your meds and regulate your behaviour or I leave"
TL;DR Girlfriend wants to go off of her medication, but when she's off her meds she has almost daily suicidal breakdowns and lashes out at me physically and verbally. WIBTA if I broke up with her if she goes ahead with stopping?
What are these acronyms?
292 notes
·
View notes
Text
Hearing Voices & Unusual Experiences & Psychosis & Schizophrenia & Etc
Hearing Voices and Co 101
Community overview of hearing voices by BC hearing voices network and Hearing Voices Network of South Australia
A rare community and medical overview of hearing voices by Understanding Voices
Medical and Mental Illness style overviews of hearing voices (separate from pages on psychosis and schizophrenia, which is kinda nice) by Mind UK and Rethink Mental Illness
Explanation of psychosis by Likemind UK
Explanation of schizophrenia by Project LETS
Lived Experiences
“LUNAR: a psychosis zine” by feyxuan, interviewing 6 folks with lived experiences
"A Bipolar, A Schizophrenic, And A Podcast” hosted by Gabe Howard and Michelle Hammer aka Schizophrenic.NYC
“MadHaus” podcast by Maddie Jericho, who also is part of Students With Psychosis
“Living Well with Schizophrenia” Youtube channel by Lauren
“The Collected Schizophrenias” by Esmé Weijun Wang, book review with quotes here
Dealing with Life
Lists of coping strategies by Hearing Voices Network Aotearoa New Zealand, Hearing Voices Network Australia, and Manchester Hearing Voices Group
Advice from young people hearing voices by Manchester Metropolitan University
“Dealing with Psychosis” toolkit by Early Psychosis Intervention program in Canada
List of Hearing Voices Networks around the world on Intervoice website
Peer support groups for folks with “schizophrenia or a schizophrenia-related illness”, family and caregivers, and a helpline by Schizophrenia and Psychosis Action Alliance
#hearing voices#psychosis#schizophrenia#schizophrenic spectrum#resources#actually psychotic#mental health
328 notes
·
View notes
Text
some comparisons between disorders and symptoms
we've been meaning to write this for a while now, because we often receive asks that are like "how do I know if I have a schizospec disorder or (another disorder)?"
so, here are breakdowns of symptoms that affect thoughts, some things we'll take from the EASE for more officiality and clarity
intrusive and impulsive thoughts
intrusive thoughts are by nature aggressive, horrid, macabre, and/or sexual.
they're different from impulsive thoughts. impulsive thoughts are silly, usually fun, are things that wouldn't bring too much harm on yourself or others if acted upon. things you would realistically do in the spur of the moment. they are purely caused by impulsivity.
examples of impulsive thoughts:
thoughts/imagery of breaking some object
thoughts/imagery of sneaking up on a person to give them a scare
thoughts/imagery of impulsive buying, spending, etc
examples of intrusive thoughts:
thoughts/imagery of blood, catastrophes, death, etc
thoughts/imagery of harming yourself/others
thoughts/imagery of sexual harassment, violence, etc
intrusive thoughts are unwanted, cause distress, are met with resistance, and often with attempts to push them away
impulsive thoughts aren't necessarily unwanted, cause minor distress or no distress at all, aren't met with much resistance
intrusive thoughts are a symptom of many, many, many mental health issues and illnesses. though, they also happen in healthy people, occasionally.
the keyword is: occasionally.
when intrusive thoughts become frequent and constant, they become obsessions.
obsessions
obsessions are, simply put, ongoing intrusive thoughts.
they are repetitive, they won't stop showing up no matter how much resistance or attempts to ignore them is shown, and are cause of great distress.
they are often met with attempts to push them away, which can too become frequent and become compulsions.
compulsions are often present with obsessions, but not always, and the reverse is also true. obsessions are often present with compulsions, but not always.
obsessions are the defining feature of OCspec disorders such as obsessive-compulsive disorder (both obsessive and obsessive-compulsive types, but not compulsive type) and body dysmorphic disorder.
ruminations
thoughts/imagery of any past event.
ruminations are frequent and ongoing as obsessions, but they're a bit different depending on the subtype of ruminations.
subtype 1:
the person is unable to find any reason for their tendency to obsessive-like states; they simply rethink and relive what happened during the day/past days – not motivated by perplexity, paranoid attitude, or sense of vulnerability or inferiority.
subtype 2
the obsessive-like states appear as a consequence of a loss of natural evidence, disturbed basic sense of the self, or hyperreflectivity, or they appear to be caused by more primary paranoid phenomena (suspiciousness, self-reference, etc) or a depressive state.
subtype 3
ego-dystonic, as in obsessive-compulsive disorders, with ongoing internal resistance, but a content that is not aggressive, horrid, macabre, or sexual. they're also categorised as true obsessions, but can have a different content.
subtype 4
obsession-like phenomena, which appear more as ego-syntonic (not met with resistance, or only occasionally), and with a content that is directly aggressive, sexually perverse, or otherwise bizarre. they often feature an imaginative character doing the actions, instead of the person who's experiencing the ruminations.
to make it clearer:
intrusive thoughts are unwanted, cause distress, are met with resistance, and often with attempts to push them away. they do not happen regularly, and often aren't a cause of concern, though they are distressing. everyone can experience intrusive thoughts, regardless of if they have a disorder or not.
obsessions are unwanted, cause distress, are met with resistance, and often with attempts to push them away. they happen regularly, often on a daily basis, and often are cause of concern. since they cause distress regularly, they're often basis for a diagnosis of obsessive-compulsive disorders. again, if they don't cause distress, they're not obsessions, they might be ruminations or impulsive thoughts, or something else entirely. they are often, but not always, met with compulsions, rituals, or attempts to ignore them to neutralise the obsession.
ruminations are varied. they all have in common that they happen regularly, often on a daily basis, and they're thoughts/imagery of past events. they can just be (subtype 1); they can be in response to depression, hyperreflectivity such as anxiety, paranoia, suspiciousness, etc (subtype 2); they can be bizarre, met with resistance and distressing as obsessions, but of a different content (subtype 3); they can be of the same content as obsessions, but without the same resistance and without being distressing (subtype 4). though, they can also be met with compulsions, rituals, or attempts to ignore them. they can happen in any disorder, but especially subtype 1 can... just happen, even in healthy people. subtypes 2-4 are frequent in schizospec disorders. subtype 2 is also frequent in other non-schizospec disorders such as anxiety, depression, etc.
#cluster a#stpd#schizotypal pd#szpd#schizoid pd#ppd#paranoid pd#schizospec#schizophrenia spectrum#ocd#obsessive compulsive disorder#body dysmorphic disorder#intrusive thoughts#obsessions#ruminations#long post
412 notes
·
View notes
Last Seen Blogs

leilabee
inside a heart explodes.

bladeubae
BL∆ÐΞUBÆ

revcntulet
FOX FIRE

drjoot
Kujo Jotaro

attackfish
Attackfish's Fandom Blog Archive