#psychiatric survivors
Text
So, Peer Respites are a not-very-well-known alternative to psychiatric hospitalization. They are 100% voluntary and staffed by peers, AKA individuals with lived experience of mental illness/emotional distress/what-have-you. Generally, they are a homelike environment where you can come and go as you please, and there is lots of voluntary programming like groups, art, yoga, etc. You can bring your own food or cook meals together with staff and other residents. Stays are usually anywhere from five days to two weeks, depending on the respite house and also your own wants and needs. There are no restraints, strip searches, or seclusion.
They're also on the rise!! I know this because I've spent all day today compiling data on peer respites in the US so I could create this fun graph for ya'll.

In the past ten years, at least 38 new peer respites have opened in the US. The data for 2023 is incomplete, but at least one has already opened, and another is scheduled for a soft opening later this year.
Some things about the data:
I did not include peer respites which were permanently closed (2) or could not find an opening date for (1)
I used the National Empowerment Center's Directory of Peer Respites, along with some internet sleuthing to find a few more (and to find the opening dates for each one). Because of this, I may have missed a few.
There were a handful of peer respites for which I could not pin down a for-certain, exact date for. I did include these in the dataset as I was able to find rough estimates.
I have also not done a deep dive for all peer respites that were unsuccessful, which may skew the data a little bit.
I included Soteria Vermont as well, as it technically fits the definition despite being specifically for people with psychosis
If you would like to help get a peer respite off the ground, I would recommend donating to Peer Support Space Inc.'s Orlando FL Peer Respite. Their soft launch is November 2023, and they are scheduled to open to the public in January 2024. This is really important, because Florida's only peer respite has recently permanently closed.
If you're interested in starting your own peer respite, the National Empowerment Center has a list of resources here.
If you are interested in seeking help from a peer respite, there is a directory of most of them here. You can also look at the Google Doc I created to compile my data, which has a few more/is slightly more updated - though it's not nearly as nicely put together as the other one!
If anyone would like to add any information, non-US peer respites, etc, feel free to!
#peer respites#peer respite#psych ward#psych hospital#psychiatric hospitalization#psych critical#psychiatry critical#anti psychiatry#antipsych#antipsychiatry#mental illness#neurodivergency#disability#hospital diversion#psychiatry#disability pride month#psychiatric survivors#putting in all the tags I can think of so ppl see this lol
2K notes
·
View notes
Text
I am begging Mental Health Culture to stop broadening the definition of "self-harm." If you want a term to convey the concept you're trying to express, may I suggest bringing back the term "bad habit"?
"Self-harm" is grounds for involuntary commitment. Do you want people to get involuntarily committed for spending too much time on the internet before bed or volunteering for too many projects? No? Then don't give coercive psychiatry ammunition by broadening the usage of their coercive terminology!
When I first started out in the Mad liberation advocacy movement, one of the arguments we made against involuntary commitment and coercive intervention for "self-harm" was that neurotypical people do things that are "bad for them" all the time, like playing football, smoking tobacco, or eating candy, and they still have the bodily autonomy right to make those "unhealthy" choices. The point was to highlight the double standard that some people were denied rights because of doing things that were allegedly "bad for them," while other people were allowed the dignity of risk and freedom to choose. Our point was "The neurodivergent/Mad person picking her skin should have the same right to bodily autonomy as the neurotypical person dancing ballet, even though both are doing things to their bodies that could be described as 'bad for them.'" The argument was that neither should be pathologized. Current discourse would pathologize both, as well as even more variations on human behavior. That's a big step backwards.
"But it's only self-harm if it has certain emotional motivations" -- let me stop you right there. Coercive psychiatry does not ask us what our emotional motivations are. It dictates to us what our emotional motivations are, and increases the coercion if we disagree with it (because disagreeing with their assessments of our emotional state is also A Symptom). Do you think the Parental Surveillance Industrial Complex is going to listen to their children before following through on moral panic articles about how parents should take away their children's hobbies because they're "self-harm"? Don't ascribe good faith to coercive psychiatry, because coercive psychiatry doesn't ascribe good faith to you.
#mad pride#ableism#neurodiversity#youth rights#liberation#psychiatric survivors#disability rights#self h@rm
514 notes
·
View notes
Text
Disliking the Mental Illness Label: A Psychiatric Survivor’s Perspective
Welcome to From Insults to Respect.
In a recent post, I shared some of my views about the pros and cons of the mental illness concept. I’m retired now, but derived my way of looking at these issues when I was employed in various settings as a PhD level psychologist.
During my career, I often interacted with people who, upon accessing mental health services, came away believing they were…

View On WordPress
0 notes
Text
not that people who've been to the ward are immune from being pro-psych, but if you've never been to a psych ward*, i sincerely don't want to hear about how psychiatry/psychology is good because you've had such a good experience with X provider, or X medication saved your life. *i also don't want to hear about how the forced treatment was what you needed or how the ward you went to let you have your cellphone etc. etc. i genuinely do not want to hear it.
like. the first hospitalization traumatized me so bad, i became dangerously delusional, was re-hospitalized, and sent to state. when they transferred me, i was strapped down into a gurney at all points on my body, *head and neck included*, and loaded onto an ambulance. my parents lost most of their parental rights; i was a ward of the state and had near zero rights. when i got there, they made me choose if, "if necessary," if i wanted to be wrangled down and forcibly injected with a sedative... or wrangled down and locked in a padded room all by myself (but at least i had a choice, right?). i signed consents and paperwork that i did not fucking understand. then i was told i'd be locked inside for 2 straight weeks (which yes, they followed through with). the psych ward was remote, nothing but barbed fences and trees around us. cant even see the sun through the heavily tinted windows. that was the *start* of the stay. i'm sure you can imagine nothing good came after.
so like. if you walk out of a place like that thinking it was good for you, then i can only imagine how traumatized you are and i hope you heal someday. but if you've never faced the destruction of your autonomy like that and go around being like "oh this is good actually" then shut the ever living fuck up.
#julian rants#this is okay to rb but im mainly venting#psych ward#psych survivor#psych ward tw#abuse tw#sanism#ableism#antipsychiatry#antipsychology#antipsych#psychiatric abuse#psychiatric trauma#trauma#psych abolition#psych hospital#psychiatric hospital#inpatient
1K notes
·
View notes
Photo









October 9th is Psychiatric Survivor Pride Day
“The problems of the ex-patient are more subtle but no less pressing. Many ex-patients try to cope with what has happened to them by pretending that the experience never occurred. However, because the experience of having once been a mental patient teaches you to think of yourself as less than human, this is not a satisfactory solution. People feel emotions. They are justifiably happy or sad, angry, calm, elated, and so forth. As patients, however, we were taught to think of ourselves as permanently crippled, and we tend to react to the normal ups and downs of life as affirmations of our secret deformity. In addition, society imposes penalties upon ex-patients which affect you whether or not you acknowledge your identity. For the rest of your life, you will lie on applications for jobs, schools, and driver's licenses, and worry about being found out. Your friends and acquaintances will be divided into two groups, those who know and those who don't, and it will always be necessary to watch what you say to the latter. Ex-patients are full of anger at what has been done to them, but alone and unorganized this anger is not expressed and is often turned inward against oneself. Our anger is the fuel of our movement, and when we come together, acknowledging our identity to ourselves and to each other, we will have made the first and largest step in striking back at our oppressors.”
— "Mental Patients' Liberation: Why? How?", originally distributed in the early 1970s by Mental Patients' Resistance of Brooklyn, New York
[image ID] Seven photographs from antipsychiatry demonstrations. They are described below, in order of appearance:
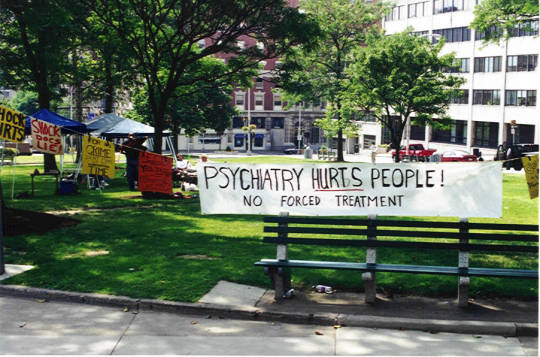
1. a picture taken at the National Association for Rights Protection & Advocacy (NARPA) Conference on November 10, 2000 in Sacramento, California. Fifty to sixty people stand around a red sign with white text that reads: NO FORCED TREATMENT EVER.
2. a picture taken on October 9th, 1999 in Toronto, Ontario during a march for Psychiatric Survivor Pride Day. Several people march in a line, including one man at the start of the march playing bagpipes. Behind him is a hand-painted sign being held up that reads: Psychiatric Survivor Pride Day.
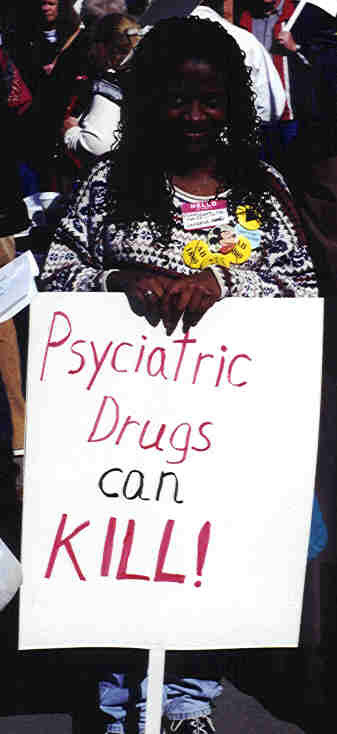
3. pictures taken at a demonstration outside the California State Capitol building in Sacramento on February 28th, 2000. The signs in each of these pictures say: Psychiatric drugs can kill!
4. a picture taken at a demonstration outside the American Psychiatric Association's 156th annual meeting in San Fransisco, California. The activist's sign says: PSYCHIATRY IS NOT A MEDICAL PROFESSION: IT IS A TOOL OF OPPRESSION.
5. a picture taken at a demonstration outside the Jacob Javits Center, hosting the American Psychiatric Association's 167th annual meeting in New York City on May 4th, 2014. The picture features an activist wearing a printed t-shirt and is cropped so as not to feature the face of the wearer. The t-shirt says: TO HELL WITH THEIR PROFITS, STOP FORCED DRUGGING OF PSYCHIATRIC INMATES!
6 and 7. pictures taken at a demonstration outside the California State Capitol building in Sacramento on February 28th, 2000. The signs in each of these pictures say: Psychiatric drugs can kill!, STOP expansion of forced treatment, Mental illness is NOT a CRIME, and FORCED MENTAL HEALTH TREATMENT IS INHUMANE.
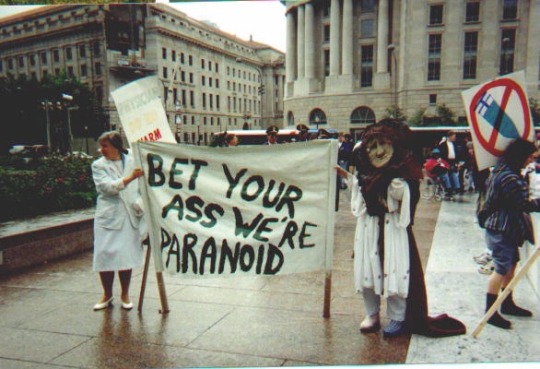
8. a picture taken at an antipsychiatry demonstration on May 2nd, 1998 in Freedom Plaza, Washington D.C. Two people hold a hand-painted banner-sign that says: BET YOUR ASS WE'RE PARANOID.
9. taken at an antipsychiatry demonstration hosted by the Mental Patients Liberation Alliance during Mad Pride Week in 2000, between July 13th and 16th on the lawn in front of the New York State Capitol Building in Albany. [end of ID]
#antipsychiatry#psychiatric abuse#psychiatric survival#psychiatric survivor pride day#psych abolition
5K notes
·
View notes
Text
"NPD as a diagnosis was created by bigoted psychiatrists who use the diagnosis to label and punish people they think are bad, and that needs to stop" and "some people find value in the diagnosis and use it as a framework to understand their experiences, and they shouldn't have the label taken away from them by force" are two ideas that can and should coexist
#narcissistic soliloquizing#actually npd#npd safe#actually narcissistic#psychiatric survivor#antipsychiatry#psychiatric abolition
238 notes
·
View notes
Text
I am once again thinking about the term "suicide survivors". How it's a term that rightfully belongs to those that lived through a suicide attempt, that literally survived suicide. How instead it means those that lived through someone else's death. How it neans "surviving" in only the archaic use 'survived by" used in obituaries. How suicide "survivors" lived through something that was never going to kill them, that was never even a threat to their life.
How we are only ever a footnote in the stories of others. We're a tragedy that happens to people, a cautionary tale if we die and inspiration porn if we live. How, forever long we do live, we were suicidal, past tense, because it makes people too uncomfortable too acknowledge that suicidality is chronic (whether pathological or environmental).
How everyone wants to do suicide prevention but no one wants to acknowledge the people at the center of it. How it's never actually about our needs - or even about our safety, really. It doesn't matter what trauma or pain we must endure - they'll have us live if it kills us. Never mind social programs to give us housing, food, security, to make us want to live - it's our responsibility to find someone to tell us it's all in our heads and we need meds to fix us, because it's CRAZY to want to die. Make sure the hotlines can all call the cops if we don't comply.
Don't we know how selfish it is to want to not be in pain and be so desperate that we're willing to die for it? Don't we know how selfish it is to not have any access to the things we need to survive? Don't we know that suicidal depression is really our duty to get over, because obviously if we don't take meds that don't work or that make us sick, if we don't submit to medical gaslighting, if we don't "try" to recover, it's not like it's an illness or a disability! It's selfishness, a character flaw.
Don't we know that we're the selfish ones, when they make our struggling, our illness, our deaths, about us and not them?
It's sanism at its most basic. We're not reliable narrators of our own experiences. We're not the main characters of even our own stories. We're there to be a single pretty tear rolling down the cheek of our loved ones. We're tragedy-as-an-object, as an object lesson. "Make sure you pick yourself up by your bootstraps seek help so you don't become an inconvenience for us hurt your loved ones." Even STILL the focus is not on the harm done to yourself, except as a moral failure in that it harms the healthy people around you.
Quite frankly, I'm sick of it. I don't ever want someone to call themselves a "suicide survivor" again who means it not as "I've survived BEING suicidal" but as "I lived through someone else being in so much pain that they took their own life over it". Not when there still exist people that have survived attempts or are actively suicidal. This is our narrative, not one for you to center yourselves in.
I will not go so far as to say your grief is selfish. That would be cruel. But your grief IS about someone else. This is still THEIR story.
It is likewise the same pain, the same trauma, and the same ableism and sanism we face over it, for those of us who have actually survived it, more than it is that of those who have never stood on that edge. It is the same decentering of our own stories when we go through the exact same thing.
It is the same surviving another day of being suicidal, another attempt, and hearing people who have either never been suicidal or simply are not talking about their own survivorship of suicidality, have the audacity to call themselves survivors of something that they never survived. To take something that KILLED someone they love and claim to be survivors of it.
Cancer survivors had cancer. Automobile collision survivors were in collisions. Survivors of critical illnesses or disabling/severe injuries lived through those illnesses or injuries affecting THEIR lives. But suddenly when a deadly chronic illness kills someone, in this one case, the survivors are the ones who watched someone die of it?
Nah. This isn't a mass threat like a shooting or a pandemic, where your life was ever in danger. You're not the survivor. Your grief is valid, and there absolutely needs to be times and places where being a GRIEF survivor is centered, where your healing and well-being is focused on.
But let those of us who we so sick we nearly died for it, or DID die from it, be the center of THAT story.
Dead men tell no tales, so at least have the grace to let the echoes of our voices remain, unspoken over. And for gods' sakes, remember that there are people that DID make it through alive, that we're still talking, that our voices are most important in a conversation about OUR potentially deadly illnesses.
We're still here telling our own tales.
#cw suicide#suicide#suicide survivor#sanism#ableism#psychiatric neglect#psychiatric abuse#anti psych#anti psychiatry#forced recovery
373 notes
·
View notes
Text
Sometimes i wonder what the people at the psychiatric hospital did with the cords from my pants. i wonder what they do with all the tings they take from us. do they just get thrown away like they are nothing? i cried over losing the cords from my favorite frog pajamas i wonder if the nurses knew i would cry about that.
#they probably dont think about it#antipsychiatry#antipsych#anti psych#anti psychiatry#antipsychology#psych survivor#psych abolition#psych critical#psychiatric victim#psych hospital#psychiatric hospital#psych ward#mental heal hospital#tw psychiatric hospital
186 notes
·
View notes
Text
Hi there! My name is Hayden Stern and I'm a multidisciplinary artist working on an installation project about institutionalization, "therapy group" within the institution, and the inner worlds we create to survive loss of autonomy. I am looking for survivors of institutionalization and presently institutionalized people (preferably long term institutionalization/residential care, but if you've been a frequent psych ward visitor feel free to fill out this form as well) to respond to a specific prompt either via voice recording or in writing. This form is a way for me to collect contact info of interested participants so that I can 1) gauge interest in project participation and 2) reach out with next steps if you are a good fit for this project.
You will not be asked to share traumatic memories of your experiences - as a survivor of institutionalization myself, I am sensitive to how painful it can be to dwell on these memories. However, you will be asked to answer a question you were likely asked while in an institution of some kind, specifically around visualizing a safe space/inner world.
Please share if you're up for it - I'd love to find a wide range of people to participate in this project.
#artists on tumblr#psychiatric survivor#antipsychiatry#troubled teen industry#mad pride#actually disabled#disabled artist#trans artist#actually autistic
384 notes
·
View notes
Text
My name is Camille. I am a born transgendered woman. When I was a child I said that I was a girl but the world called me a "faggot." Under the sky of pain called psychiatry I was locked away for many years and had the requisite tortures: the terror of electroshock, my bones broken, my body drugged and raped. I was not raised as a gender but as a bug of a child to be smashed.
I am nobody's victim. My body belongs to me & so does my holy brain. I am the ghost of the untapped conscience of shrinks, a lurking justice, a part of the gathering truth that is rising with a common voice out of the wake of their evil blue fire.
Transsexuals are born into the book of labels. We may be genetic but we are not genetically defective sub-human creatures. By the very nature of our difference, the independence of our alien spirituality, and the passion of the power of our will, we are a threat to the ruling delusions of the mental death profession.
No one has our permission to debate the validity of our existence, to define our reality, to dismiss our pain, and to name us. We name ourselves.
If you could look into the collective genetic memory of your humanity you would find us in the rivers of your dreams, for we were always here, we were here when Earth was a green spirit. We were a natural occurrence in a singing world. In times of absolute horror and destruction I wish for you all the transformational creativity of an utterly beautiful madness, and I offer you the blessing of a holy human freak.
"Why A Transgendered Woman Calls for Psychiatry's Destruction" by Camille Moran, published in the Fall 1993 issue of Dendron.
#it speaks!#linked it in the previous post but i wanted to have the full text on my blog. screenshots of it have been posted on tumblr before ->#<- but i just wanted the text#paths outside this garden#hysterical studies#okay getting into the maintag & trigger shit now:#trans history#camille moran#antipsych#psychiatric survivors movement#mad pride#for triggers im not doing 'tw' im just doing the words lmk if that is not effective & lmk if i ought to trigger tag anything else. ->#transmisogyny#rape mention#child abuse#ableism#psychiatric abuse
80 notes
·
View notes
Text
something to keep in mind while reading: i experience psychosis, i am professionally diagnosed with a variety of extremely stigmatized mental health diagnoses, and i identify strongly with the label "borderline."
sooner or later, the ~mental health awareness~ and ~neurodivergent awareness~ movements as a whole are going to have to reckon with the fact that mental health diagnoses are labels put on classifications of behavior patterns, and those behavior patterns can be actively harmful to other people. and what i mean by that is that classifying people's behavior is not identifying ontological attributes of people's personalities or biology; it's loosely grouping different behavior patterns into categories and slapping a label on them. there is no difference between "having borderline personality disorder" and "enacting a behavior associated with borderline personality disorder;" the only criteria for the diagnoses are that you enact some or all of the behaviors associated with the label.
the idea of "these stigmatized diagnoses do not make you a bad person" is objectively correct, in that the label "bad person" is inherently not useful and erases the material factors behind someone's behavior. however, framing mental health diagnoses as if they are some ontological attribute of the self divorced from behavior doesn't actually serve to "destigmatize" mental health as a whole.
people labeled as mentally ill are put in this catch-22 where we either admit that some of our maladaptive behaviors associated with diagnoses can be harmful to others (and thus are used as rhetorical supports for how mental illness labels are describing an ontologically bad and evil category of person), or we push the party line that "mental illness doesn't make you a bad person" and divorce any harmful behaviors entirely from the mental illness label of the person performing them (thus further stigmatizing those of us who have maladaptive and externally harmful behavior patterns associated with our diagnoses, as of course these can't be "because" of our mental illness--ignoring the fact that the mental illness label does not exist outside of our behavior to begin with).
it's a well-documented fact that the DSM buries the role of trauma and other material factors in shaping the behaviors it categorizes to begin with; the desire to divorce the label from any materially harmful behaviors it ascribes to itself is yet another case of ~mental health awareness~ pushing the responsibility of reshaping society and interacting with trauma onto the individuals suffering under these systems of oppression and systemically enabled trauma. in order to actually do the dirty work of addressing material harm, we need to get down into the weeds of why someone enacted that harmful behavior to begin with--what environment that maladaptive behavior arose from, and what material factors need to be addressed in order to solve that behavior and redirect it into healing and positive interactions.
like... that's the problem, at the end of the day. in order to address harm, you need to humanize and understand the person doing harm. shoving people off into more and more categories of "bad person" does nothing to actually, materially address the harm caused, and further enables more harm in the future. mental health labels, if used in a lateral and non-oppressive way, should be used as shorthand to refer to a category of behavior in order to more fully understand the material factors that go into shaping that behavior, in order to better promote healing and a functional community. there should not be a stigma around admitting that a label could describe someone who commits actions that are materially harmful, and that label is applied directly because of their behaviors--to say otherwise is just shifting who the group it's okay to oppress is, rather than trying to agitate for collective liberation.
(note: plenty of behaviors associated with mental health labels are not harmful to begin with. we could also do a lot better by examining how we conceive of "harm", because "someone existing with an emotion that makes you feel uncomfortable" or "someone doing something you think is weird" is not it. but that's not what this post is about, so i am choosing not to address it in-depth.)
#antipsych#antipsychiatry#anti psychiatry#psych critical#mad liberation#mad pride#madpunk#dyspunktional#mad punk#actually insane#psychiatric survivor
270 notes
·
View notes
Text
So let's talk about "disabled people who can't take care of themselves," the people cited as justification for eugenics, institutionalization, oppression, and extermination -- because surely people who can't take care of themselves shouldn't be allowed to be free, right? Ideally, they shouldn't even exist!
What does it mean when a disabled person "can't take care of themself"? What does it mean to take care of oneself? What are the barriers to disabled people doing it?
Basically, there are three distinct things people mean when they say that a disabled person "can't take care of themselves." Each meaning is a different problem with a different solution. Let's parse them:
The first thing people mean when they say that a disabled person "can't take care of themselves" is that they don't have the money or income to pay for the necessities of life in a capitalist economy. Because ageism, classism, and ableism are all connected, sometimes this ableist argument is applied to abled poor people or abled young people. Generally, this means that some people can't sell their labor for a high enough price to pay for their necessary commodities.
Framing this problem as people being "unable to take care of themselves" is an attempt to medicalize and naturalize what is essentially an economic problem. Calling people "unable to take care of themselves" rather than calling them "poor" or "unemployed" or "underpaid" or "economically exploited" frames the problem as a defect within the poor person rather than as a feature of a deeply unequal economic system. When you hear that someone "has to" be externally controlled because they "can't take care of themselves," ask "Could this problem be solved if they had a guaranteed income that paid for all their needs?" If so, their body or brain isn't the problem.
The second thing people mean when they say that a disabled person "can't take care of themselves" is that, because of the impairments of their disability, they can't engage in the activities needed to sustain their body and living space, like cooking, eating, bathing, toileting, cleaning, etc. Unlike the first meaning, this is directly related to disability. But, if you scratch the surface a little, it's still basically solvable with money. Technologies like dishwashers and walk-in showers, or human services like food delivery or housekeeping, are conveniences or luxuries for abled people, but may be necessities for disabled people. The problem is that most disabled people who need them, can't afford them.
When abled people with money hire people to help them with their activities of daily living, anything from a housekeeper to a food delivery person to a home nurse, the person receiving the service is the customer, or the boss. The concept of a boss in employee relations is... problematic, to say the least, and leads to the same economic inequalities that are the problem, but in this context, this means that the person receiving the services gets to decide what services they want, and how they want them. They can ask their housekeeper to come in Tuesday instead of Monday, or ask their DoorDash driver to get burritos instead of egg rolls. Most crucially, if a service worker assaults or abuses them, they can ensure that that particular worker won't come back. Because most disabled people are poor, they have to either go without services, or accept limited services paid for by someone else (like their families, or a home care company). This leaves the disabled client with far less recourse. In both cases, the actual worker is probably being underpaid and exploited by a service agency. But when the client is paying the service agency, they have choices about their services that poor people don't have. So once again, the problem is not that disabled people need services. The problem is that poor disabled people, because of their economic situation, lack the control over their lives that rich abled people take for granted.
The third thing people mean when they say that a disabled person "can't take care of themselves" -- and, because of the intersection of classism, ableism, ageism, and neurobigotry, they usually mean to be an unstated implication of the other two meanings -- is that a disabled person can't think for themself or make their own choices. Which just means, of course, that they don't communicate in the way that the abled person saying this respects, or they make decisions the abled person saying this disagrees with.
This one is just false. We can reject it on its face. Every disabled person -- every PERSON -- no matter how little money they have, no matter how much assistance they need with daily living tasks, no matter how much or how little formal education they have, or how much their perceptions differ from those of societal norms, is the best arbiter of xyr own best interests about xyr own life. Pro-institutionalization, pro-coercion, and pro-eugenics advocates want to be able to say "She can't take care of herself," meaning "She doesn't have the money for housing," or "He can't take care of himself," meaning "He can't lift himself into the shower without assistance," and have the audience assume this means "They aren't smart enough to make their own choices, and they need someone else to make choices for them," which is always false. We don't need to separate "these" disabled people who can make their own choices from "those" disabled people who can't, because "those" disabled people don't exist. Everyone can, and everyone deserves the right to, make xyr own choices about xyr own body, mind, and life.
I wrote a little bit about the "can't take care of themselves" concept here and here, too.
#ableism#mad pride#neurodiversity#youth rights#liberation#disability rights#ageism#psychiatric survivors#eugenics#classism
246 notes
·
View notes
Text
Shelving books at my new job and reacted to this like a vampire next to a stack of bibles
#jumpscared by the dsm while i’m trying to live my life#go away#dsm 5#anti psych#anti psychiatry#mad liberation#psych abolition#psych abuse#psychiatric survivor#psych survivor#psych trauma#psychiatry#mad pride#mad studies
29 notes
·
View notes
Text
involuntary hospitalization should be considered kidnapping. or abduction. that is all.
#softspoonie#antipsych#psychiatric abuse#antipsychiatry#psych ward#psychiatry#psychiatric hospital#psych hospital#hospital#mentally ill#mental illness#sanism#ableism#madpunk#neuropunk#abuse#trauma#psych survivor#trauma survivor#abuse survivor#ptsd#cptsd#survivor#disabled rights#disability rights#human rights
195 notes
·
View notes
Text
I Don’t think some of y’all realise how awful the mental health system is to children.
Even if you are lucky enough to get help early on, it’s a gamble. I went to so many hospitals and therapists and psychologists, all of whom claimed to be state of the art.
Nothing was ever different. I was scrutinised, used as a lab rat, put on a crap ton of medications that made me sick, made me gain weight, made my symptoms worse.
You grow up with a sense that you can’t trust yourself. After all, doctors know best, don’t they? So you must be wrong! But the doctors aren’t helping you at all… so what’s going on?
Then come the residents and medical students that put you through the same sloppy thought exercises and wear you thin, and you didn’t even consent to them practicing on you!
Rant over. For now.
#medical trauma#shut up scriptwriter#not cr#psychiatric abuse#anti psych#psych ward survivor#psych critical
25 notes
·
View notes
Text
one of the scariest things about being a psych survivor is that you don’t know what to do anymore when you need help.
hospitals don’t feel safe. residential don’t feel safe. and yet i still have the same mental health issues that caused me to seek care in the first place, plus the additional trauma.
i’m having a hard time right now. i wish i could just “get help” but it’s not that simple anymore. these programs just chew you up and spit you out, and i don’t want to go through that again. but it’s terrifying ti be on your own.
#tw depression#mad liberation#autistic#psych survivor#mad pride#sanism#actually autistic#psychiatric abolition#psych abolition#tw hospital#treatment trauma
61 notes
·
View notes
Last Seen Blogs

raysofluminescene
Rays of Luminescence


cinemaclubrotterdam
Cinema Club Rotterdam

floorpillow
Phoenix Wright kin

soft-pwincess
princess treatment