#THEY LISTED CHRONIC FATIGUE SYNDROME AND CHRONIC PAIN
Text
there is something so allienating about trying to find... anything but through the lense of being in chronic pain or having chronic fatigue
art tips? though luck
planning and routine tips? think again
exercise tips? fuck no way
everytime i see a video or someone talking about something that it might be helpful it ends up being non applicable when you have chronic pain or cfs what the fuck are you supposed to do?
#therapist recommends doing it ourselves#might have to come to that i guess#all the most popular stuff is just not useful#going through a list and just trying to think of ways it can be modified so it is even possible to do#chronic fatigue syndrome#chronic pain#chronic illness#chronic fatigue#and adding chronic fatigue or chronic pain to the search doesnt really give the results we are trying to find
25 notes
·
View notes
Text

"Yes, it's true: I was the type of young femme who managed the girls basketball team in high school, just to be able to take in the sight of all those butches parading their muscles up and down the court. I found Girl Scout camp to be femme heaven and reveled in being able to explore my athletic self and still maintain my femmeness. And, to my horror, I have to admit pushing Tina away from my breasts in the back seat of a Buick while attending Mount Saint Mary Seminary.
And then there was feminism... Although I came out as a "gay" woman before reading The Feminine Mystique, the seventies brand of white feminism had me trimming my nails and cutting off my hair. Soon I was outfitted in farmer jeans and high tops. And still I was told by my "sisters" that I didn't "look like a dyke" (read: I didn't look butch).
I began to lead two lives- one as an outrageous, skirted, lipsticked femme while I worked in and traveled with carnivals, and another as an imitation butch back home in the women's community. Eventually, I pulled the pieces of my being back together and proclaimed boldly, "I am a working-class lesbian femme."
So I had maybe six years reveling in unleashing my seductive femme self when, as lives go, mine changed: slowly at first and then more dramatically.
Recurring back pain and limited range of mobility were finally diagnosed. Soon after came decreased mobility. No more mountain climbing. No long mall walks in search of the perfect piece of sleaze. No more standing against kitchen walls being gloriously fucked by some handsome butch. I stopped using alcohol and drugs, became ill with what is now known as CFIDS (Chronic Fatigue Immune Dysfunction Syndrome), and began to use a three-wheeled power chair.
The more disabled I became, the more I mourned the ways my sexual femme self had manifested through the nondisabled me: cruising at the local lezzie bar, picking up a dyke whose eyes refuse to stray from mine, dancing seductively, moving all of me for all of her. Cooking: love and suggestion neatly tucked into the folds of a broccoli quiche. Serving my date in varying, sleazy clothing, removing layers as the meal and our passion progressed. And making love... feeling only pleasure as my hips rose and fell under the weight of her. Accomplishment and pride smirked across my face as her wrists finally submitted to the pressure of strong persistent hands. There are the ways I knew to be femme, to be the essence of me.
It's been five years now since I began using my wheelchair. I am just awakening to a new reclamation of femme. Yes. I still grieve the way I was, am still often unsure how this femme with disabilities will act out her seduction scenes. I still marvel when women find passion amidst the chrome and rubber that is now a part of me.
There have been numerous dates, lovers, relationships, sexual partners, and fliterations along the way. Cindy, Jenny, Ellie, Emma, Diane, Dorothy, Gail, June, Clove, Lenny, Cherry, Diana, Sarah I, and Sarah II. You have all reminded me in your own subtle or overt, quit or wild ways that I am desirable, passionate, exciting, wanted.
Yes I am an incredibly sexual being. An outrageous, loud mouthed femme who's learning to dress, dance, cook, and seduce on wheels; finding new ways to be gloriously fucked by handsome butches and aggressive femmes. I hang out with more sexual outlaws now- you know, the motorcycle lesbians who see wheels and chrome between your legs as something exciting, the leather women whose vision of passion and sexuality doesn't exclude fat, disabled me.
Ableism tells us that lesbians with disability are asexual. (When was the last time you dated a dyke who uses a wheelchair?) Fat oppression insists that thin is in and round is repulsive. At times, these voices become very loud, and my femme, she hid quietly amidts the lists.
Now my femme is rising again. The time of doubt, fear, and retreat has passed. I have found my way out of the lies and oppression and have moved into a space of loving and honoring the new femme who has emerged. This lesbian femme with disabilities is wise, wild, wet, and wanting. Watch out.
-"Reclaiming femme... Yet again" Mary Francis Platt, The Persistent Desire (Edited by Joan Nestle) (1992)
#lesbian#lesbianism#lesbian history#disabled lesbian#lgbt history#gay history#butch femme#femme lesbian#feminism#lesbian feminism#the persistent desire#intersectionality#disability history#disability rights
2K notes
·
View notes
Text
If you have mysterious chronic pain and have the means, here's a list of doctors you should see other than your primary and a rheumatologist:
Neurologist and/or sleep specialist
Pain management doctor (also sometimes called pain and spine doctor)
Therapist that specializes in helping physically disabled people (having chronic illness sucks and you need someone to talk to)
Psychiatrist (most people with chronic illness also need psychiatric meds)
Physical therapy or rehabilitation center that specifically has procedures for chronic illnesses. My chiropractor acts as this for me but I'd only recommend that as a last resort. If you have something like fibromyalgia or ehler dahlos syndrome you need to be very careful with how you stretch and how much exercise you do. My chiropractor has special exercise equipment that is very gentle and has a lot of padding to reduce pain.
ENT (Ears, nose, throat doctor)
Nutritionist
A primary care doctor will at most only perform blood tests. Many illnesses do not show up on these blood tests. You want to get checked for rheumatoid arthritis, lyme disease, and lupus. Even if your doctor tells you it's because your vitamin d level or iron is too low, I would still recommend further testing.
They'll most likely refer you to a rheumatologist regardless, but unless you actually have arthritis I wouldn't rely on them too much. Mine charged too much for a 10 minute appointment where all she did was give me meds and would not discuss any other treatment or management options. She also laughed at me when I asked about a mobility device. It might just be I had a bad experience but it seems like those doctors are just given chronic illness patients cause no one else wants them.
You need to get your spine looked at. An MRI is essential. At the very least get an xray of your neck and spine. A neurologist or pain + spine doctor will most likely order one.
Neurologists will check your nerves and brain function. They'll check if your nerves are overly sensitive or unresponsive. You'll get stabbed and shocked a lot.
Pain and spine doctors are the ones who will give you pain medicine. It will not be immediate. They will need to examine you (MRI) and try other medications and treatments first. This is because insurance is not going to pay for stronger drugs until you've exhausted other options. You'll most likely start with something like duloxotine, gabapentin, prescription NSAIDs, and/or muscle relaxers. Once my results came in from the MRI I was given steroid shots in my spine. They will give them in different spots first to see which spot is most effective, so don't worry if it only works one time and not the others. I cannot stress the importance of having this type of doctor on your care team. Being able to have the power to manage my pain has helped so much. This is also the doctor that signed my form for my handicapped parking permit.
Sleep studies are expensive, but sleep is extremely important for your quality of life. So many people have sleep apnea and don't know it. CPAP machines today are really quiet and comfortable. This will be essential for tackling chronic fatigue.
An ENT doctor is only if you end up having sleep apnea or have any issues with your sinuses. I had to go and get my nose fixed because even with my cpap I still wasn't getting enough air.
You need to have some way of moving your body. Only do this after you are already on a treatment plan. It's hard to do things like exercise when you are still dealing with pain and fatigue. Doctors will want you to do physical therapy first but that's not a good idea because you won't stick with it due to pain. You need to deal with the underlying problems before working on stuff like exercise and nutrition. Able bodied young people who don't exercise and don't eat well are not in constant pain, so you shouldn't be either. If they tell you to lose weight drop the doctor, that's a cop out response.
I haven't reached the step to get a nutritionist, but changing what foods you eat and when can really help with pain management. You also may find that something you eat is exacerbating your symptoms.
With my insurance plan I can pretty much call up a doctor and make an appointment without a referral. I know some plans need referrals, so either call your insurance for one or get your primary care doctor to give you one. Idk how this works for medicare but I think you can just make an appointment with anyone who takes medicare.
I have not been able to obtain a script for a mobility device from any of my doctors. If you have a type of doctor you'd recommend for that please chime in. I've heard occupational therapists are the way to go though but still need to look into that myself.
Also do not feel bad if you cannot afford these. It is not your fault. Healthcare especially in the USA fucking sucks. This is mostly only useful for people who are in the investigative stage who have insurance. I'm not saying "oh just do yoga". Your pain is not your fault, and it can take a long time to figure out a plan that's right for you. I didn't know what doctors I was supposed to see when I started out, and was just given to a rheumatologist since there isn't a fibromyalgia doctor. I only had blood tests at that point. Hopefully this helps people save time and make sure they can fully investigate the cause of their pain (or at least how to manage it better)
#chronic disability#chronic pain#spoonie#fibromyalgia#disability#ehlers danlos syndrome#eds#chronic fatigue syndrome#cfs#POTS#pots syndrome#if a doctor mentions your weight within the first 10 minutes of the exam get out if there#especially if they havent even done any testing or looked at you yet
86 notes
·
View notes
Text
my best friend layla made a gofundme for her boyfriend, who suffers from very severe me/cfs (myalgic encephalomyelitis / chronic fatigue syndrome) and cci (craniocervical instability).
because of these illnesses, he might die. only two doctors in europe do surgery on me/cfs patients, who also suffer from cci, and they are located in spain. he will have to pay a special flight from italy, somewhere to stay and the surgery itself, and none of that is covered by insurance.
he is suffering so much. layla listed a few of his symptoms in his gofundme already, but the only thing he can (or is forced to) do is lie in a dark room with no stimuli AT ALL. no music, no light, no touch, not even being on the phone for too long, accompanied with tons of physical suffering as in pain or seizure-like symptoms. his suffering is not imaginable for people who don‘t have very severe me/cfs.
please read, share and donate. it‘s so very very urgent and a reblog would mean the world and could save his life.
#i‘ll rewrite it tomorrow when i‘m feeling a little better but it‘s really extremely urgent. please please help by reblogging and sharing.#mecfs#cci#myalgic encephalomyelitis#chronic fatigue#chronic fatigue syndrome#chronic pain#chronically ill#craniocervical instability
125 notes
·
View notes
Text
May is Ehlers-Danlos Syndrome Awareness Month!


Sing it out, sing it loud!
What Is Ehlers-Danlos Syndrome?
Ehlers-Danlos syndrome (EDS) is a rare complex disease that is a genetic condition which affects collagen, a connective tissue everywhere in your body, including your joints, ligaments and tendons, skin and organ tissues. This a a multi-systemic condition in which symptoms result in widespread pain and chronic fatigue.
Why should you care?
You may know someone affected by EDS or hypermobility and may not even realize it. Symptoms can vary widely from patient to patients, leaving some looking like they aren’t ill or suffering. Doctors often misdiagnose, gaslight, or even dismiss patients, pointing to easy “solutions” which leave patients with struggle to receive care, many patients average 10-12 years before getting appropriate care.
Why the Zebras?
Zebras are the symbol for rare diseases so patients identify with the stripes. Doctors are often trained to “think horses, not zebras, when you hear hoof beats”. Horses being a common disease (arthritis, the flu, etc). A zebra representing the less expected possibility.
What can I do to help?
Raise awareness!!! Someone you know or maybe you yourself may be suffering. The Care-e-oke challenge is to engage people who don’t know about this rare condition. You can also donate to EDS related non-profits or support groups to help advocates and medical providers to better support the EDS community.
This is by no means an exhaustive list—I encourage you to search out your own local advocacy and support groups:
Dysautonomia International
Hypermobility Syndromes Association
Ehlers-Danlos Society
Ehlers-Danlos Support UK
EDS Research Foundation
Pathways To Trust
Patient Advocacy Foundation
The Zebra Network
#runadreams#eds#heds#zebra strong#🦓#hypermobile ehlers danlos#ehlers danlos#ehlers danlos syndrome#ehlers danlos zebra#ehlers danlos problems#ehlers danlos awareness#ehlers danlos life#rare disease awareness#disability#chronic pain#chronic illness#careeoke challenge#careeoke#stripes sing for hypermobility#EDS awareness month#EDS awareness#eds problems#personally I’m singing control by Halsey
167 notes
·
View notes
Text
On Jan. 27, Dutch blogger Lauren Hoeve passed away through assisted suicide. After enduring years of chronic fatigue syndrome (also known as myalgic encephalomyelitis, ME/CFS), autism, ADHD, and anxiety, she, at the young age of 28, chose euthanasia to escape a life dominated by pain.
As a Canadian, I am familiar with the Medical Assistance in Dying (MAID) program, which has allowed eligible adults to request assisted death services since the federal legislation passed in June 2016. As of this year, the MAID program was also set to allow those with mental illness to choose euthanasia.
However, a recent development on Feb. 1 proposed legislation to temporarily exclude individuals with a sole underlying medical condition of mental illness until 2027.
This legislation is currently under review by Parliament, and unless it passes, the exclusion will be lifted on March 17, 2024. This means individuals struggling solely with mental health issues may become eligible for assisted death.
A confession: Initially, I welcomed the idea of assisted dying, believing it could be a humane choice for those at the late stages of irreversible illnesses to make choices on their own behalf. However, my growing concern lies in the application of MAID by the Canadian government.
I am now skeptical about the true autonomy of individuals opting for assisted death, especially in a country with socialized health care. The risk of medical practitioners recommending MAID as a cost-cutting measure to alleviate strain on the health care system is unsettling, as suggested by a 2020 analysis estimating potential annual savings of save $66 million annually in health care costs.
Individuals considering MAID are already vulnerable due to physical or mental suffering, making them susceptible to external pressures. Reflecting on my own past struggles, I recognize the unpredictability of emotions and circumstances. What seems unbearable one day may change with time and support—yet the choice to end life is a permanent one.
Like many others, I've lived with chronic pain for much of my life. I can recall many days where I've wondered what the point was of continuing to suffer. And then, a miracle drug had come along. Will it continue to work indefinitely? I don't know, but for now, I feel like I have my life back.
And that's the thing, there's an unpredictable nature to health care. What one experiences one day, can change tomorrow.
There are exceptions. I recall reading about Canadian journalist John Scully, an 82-year-old man dealing with severe depression. He was hospitalized many times, had 19 treatments with electroconvulsive therapy (ECT), and takes up to 30 pills a day to manage his chronic pain and health issue. Shouldn't he have a choice?
And yet, I was struck by something in the statement put out by Lauren Hoeve's parents. "Millions of people are affect by ME/CFS, with no established treatment pathways and no cure," they wrote on X on Feb. 2. "Why is their suffering acknowledged enough for euthanasia but not enough to fund clinical research?"
And herein lies the rub. Why is euthanasia offered as a viable solution to a potentially non-permanent problem, when other options are possible?
Mental health services in Canada (and elsewhere) are scarce. Psychologists are expensive and out of reach for many. Psychiatric services are free of charge, but the wait lists are even longer than those for psychologists and few people can get access. The wait to get help is usually over a year. Family physicians just end up prescribing medications based on a checklist and see what sticks.
Those living with chronic pain and disability have been put at the front of the line for MAID. Readily being presented with assisted dying services—instead of treatments or alternatives—can create a sense of being undervalued or marginalized. It implies that end-of-life choices should be prioritized over efforts to provide care, support, or treatments that could improve one's quality of life or extend their lifespan.
Moreover, individuals feeling like a burden on their families may be easily swayed.
I've heard of least one case where a woman decided to end her life because she couldn't get access to opioids for pain management. And while opioids are far from ideal, when it's a choice between life and death—perhaps her doctors should have considered giving her another chance at life.
For me, the troubling part of all of this is that instead of enhancing life-staining systems—whether for people with mental health concerns, chronic pain, or disabilities—our government is opting for permanent exit plans that alleviate strain on the health care system, instead of improving it.
People deserve to have choices—and the choice to end their life should only be considered once every other possible option has been exhausted.
An estimated 836,000 to 2.5 million Americans and more than 580,000 Canadians suffer from ME/CFS. Their lives are inherently valuable.
The views expressed in this article are the writer's own.
20 notes
·
View notes
Text
Intro Post! 🪲

Hello!! My name is Bugs! This is my Age Regression blog :D
🪲 Current Hyperfixation(s): Hazbin Hotel
🪲 Current Blog Theme: Sir Pentious (Hazbin Hotel)
🪲 About me and this blog: I’m 16 years old, I follow from @0x-bugs-x0 my usual regression age is 2-5 although sometimes I regress from 8-11, I am also a pet regressor!! I’m a golden retriever :3 my pronouns are He/It/pup (I’m non binary!) I’m from the uk! (I suffer from an illness called Gilbert’s Syndrome leading to me having chronic pains and fatigue so sometimes I don’t particularly have the motivation or physical energy to write.) I mainly made this account to let little Bugs have a place to get his thoughts out The fandoms I write for are listed below ⬇️
🪲 Requests: My requests are currently closed! for fics, headcanons, thoughts on characters agere or just a general little (hehe) chat! I’m always up! But if you’re looking to request a fic or headcanons here’s a list of fandoms I’ll write for! (All lists will be updated as we go!) I do write character x reader if you are interested in that! I will write in dips if you ask nicely :3
LOTR
ROTTMNT/Mutant Mayhem
Into the spider-verse
Scott Pilgrim (On Hold)
Hazbin Hotel
Helluva Boss
Anon List! :D
🍰,🪴,💥, Spider 🌈,
My Masterlist!

#sfw agere#agere#age regressive#lotr#pippin took#pippin took x reader#tmnt agere#lotr agere#headcanons#new blog#I regress!#I age regress#age regressor#age regression#agere blog#fandom agere#intro post#lord of the rings#into the spider verse#smitsv agere#Spider Man agere#spider noir#fandom ageredips#scott pilgrim agere#spto agere#ageredips#hazbin hotel agere
52 notes
·
View notes
Note
How’s your health?? Do you mind saying what’s wrong with you? If you do that’s fine I’ve just always wondered cuz you seem to be in pain a lot but regardless I’m wishing speedy recovery
Right now I'm having (probably?) unrelated stomach issues we're trying to figure out but I'm always in some level of discomfort because I have a chronic genetic condition called Ehlers-Danlos syndrome.
Full and lengthy explanation under the cut, because I really don't mind talking about it and I think people should, unlike most of my doctors 🤪, be aware it exists.
EDS is a connective tissue disorder. Connective tissue is one of 4 main types of tissues that make the human body. It's found throughout the body, around and in your muscles, blood vessels, organs, nervous system, etc. In short, it's of poor quality in EDS, too elastic and too fragile, which can cause a wide range of symptoms. There are 13 different types of EDS based on specific genetic mutations and the symptoms they cause. The severity of the illness depends on the type but can also vary from person to person.
I have the most common type of EDS, the hypermobile type. As the name suggests, the hallmark symptoms is hypermobile joints. All my tendons and ligaments, which are made of connective tissue, are too stretchy which means my range of movement is wider than it should be (aka my joints are overly flexible) and my joints are all unstable. It causes chronic pain / inflammation and injuries, and in some people frequent sub or full luxations. Other main symptoms are : a soft, thin, fragile skin described as "velvety" ; frequent bruises due to fragile blood vessels ; extreme fatigue due to poor oxygenation throughout the body ; and then sometimes specific organ-related problems depending on the person.
If you have a number of unexplained medical issues, frequent more or less unexplained joint or muscle pain, frequent injuries and/or bruises, if when you look up "beighton score" on google you see photos of your favorite party tricks to freak people out at the bar, I suggest reading up on EDS because it's incredibly poorly diagnosed and a lot of doctors don't know it's a thing.
I consider myself lucky to have been diagnosed relatively quickly and so at a relatively young age which means we caught it before I injured myself too much by not knowing what to pay attention to. But the reality of it is I saw a bunch of doctors in various specialties who all told me it was psychological until I did extensive research by myself at the ripe age of 20, was able to put together a short list of conditions that could possibly explain my symptoms, emailed EDS specialists in other countries to ask for their opinion, got told that it sounded like it and that I needed to find someone to assess me in my area, found the only EDS-knowledgeable specialist in my area, convinced my doctor to send me to this specific specialist, waited several months to get an appointment, was finally properly assessed by someone who knew what to look for, and got officially diagnosed. So really I'm not lucky, I just 1) have the socioeconomic and cultural resources to be able to read and understand medical articles 2) am very fucking persistent.
I also have a related syndrome called dysautonomia which is a dysfunction of the autonomic nervous system. The autonomic nervous system manages all the bodily functions you don't have to actively think about such as breathing, heart rate, blood pressure, thermoregulation, digestion, etc. It can present differently depending on the cause and the person but in my case it mainly causes my heart to beat too fast when stimulated and I'm generally excessively sensitive to any change having to do with my nervous system such as some medicine (can cause my heart to get too fast OR too slow, depending), exercise (at some point my heart rate would go from 70bpm to 140bpm just by standing up), or emotions (I will get a strong physiological response and then feel totally wiped out once it calms down). It also causes some mild cognitive issues due to, again, poor oxygenation of the brain, inducing even more fatigue. In my case it's nothing too massive, just some slight memory and/or attentional issues.
If you have palpitations, a fast heart rate, dizziness that doesn't go away when you're standing up, if you get an anxious feeling due to your physiological response, if your heartbeat jumps ≥30 bpm from when you're sitting to when you're standing, I suggest you look into postural orthostatic tachycardia syndrome (POTS). A lot of people have developed POTS/dysautonomia after getting covid.
Neither hEDS nor dysautonomia change my life expectancy (although some other types of EDS could). They can cause complications but by themselves they aren't fatal diseases. They are however incurable because my body is not suddenly gonna start producing good connective tissue out of nowhere, and all treatments are symptomatic aka we can do some stuff for some symptoms but can't make the underlying problem disappear.
I consider myself a rather mild case. A lot of people are very disabled by EDS. I'm mostly okay. I'm in pain but it's manageable and it responds to usual painkillers such as ibuprofen (a lot of people who have EDS don't respond to usual painkillers and local anesthetics, and a lot of them have a history of terrible wisdom teeth removal due to this, for example). I can work out which is my main pain management method (a lot of people who have hEDS have impaired mobility and/or pain levels that are too high to be able to work out). Unfortunately, I haven't been able to do it regularly since december due to covid and then my current stomach issue which is why my pain is currently flaring up. That's about it!
10 notes
·
View notes
Text
happy disability pride month

[id: image on the right is a flag with a dark grey background, a dusty rainbow diagonally going across it from the bottom left corner going up to the right and two dark grey circles in the middle of the image one smaller in the middle of the other. the mage in the middle is a green uerbox with the flag on the right and white text reading "this user wants people to understand that living with a physical disability in this world today is a waking nightmare". the image on the left is the same flag as on the right. :end id]
i want to talk about chronic pain. might make more posts similar to this one for other things but right now lets discuss chronic pain.
Chronic Pain Syndrome, aka Chronic Regional Pain Syndrome (CRPS), is a broad classification of prolonged pain typically outside injuries or outside the usual timeframe for pain caused by injuries.
there are plenty of things listed under chronic pain like arthritis, back pain, fibromyalgia and more, however not everyone realizes what they have is chronic pain.
chronic pain is not about how bad the pain is, how much it hurts nor about how consistent it is, its about how long it goes on for.
if youre feeling pain for days on end in some area, thats chronic pain
if youre feeling pain for a while after every time you try to do something with a limb (ex. lifting causes pain that stays all day and even the next day, getting up in the morning causes pain that lasts etc), thats chronic pain
if the pain goes on and off but still lasts a while when its there thats still chronic pain, it doesnt have to be consistent with how it lasts but pain that lasts longer than it should is chronic pain.
i always have pain in my spine when i get up in the morning, stand too long, walk or just be on my feet too long, lift heavy things etc and that pain lasts at least till the next day but usually much longer. strained muscles and exhaustion, soreness and aches are normal after activities but if they last longer than a day that isnt normal.
if someone tells you prolonged pain after doing something even mildly strenuous on your body is normal pain, they dont know what they're talking about and likely experience chronic pain themselves and no ones told them.
chronic pain can be caused by injuries, by conditions you were born with or gained over time.
i was born with a defect in my spine thats caused me back pain, jaw pain, headaches and more for years and i only found out about it rather recently.
chronic pain can cause exhaustion and even be accompanied by chronic fatigue more often than not. it can cause you to need longer breaks and rest and avoid usage of your arms or legs or avoid further strenuous activity more than an abled person would need.
often any pain that causes you to avoid usage of your body isnt normal. pain that flares up after you move, be active or arent active enough isnt normal
pain that lasts longer than it should and pain that is always there after doing something is not normal and more likely than not, a sign of chronic pain.
a lot of people wont realize they have chronic pain unless they discuss their symptoms with someone who knows about chronic pain or understands that those symptoms arent normal pain. its okay to not realize or know something about your body, thinking it was normal then being told it isnt, its better to learn these things about your body, listen to your body and accommodate it than remaining ignorant and not doing any of that.
everyone's experience of chronic pain is different, not one experience will be the same as another or fit in a box, but they all have the similarity of their pain lasting longer than it should, however that presents.
the pain doesnt have to be excrutiating, there are days where it can just be dull and manageable, times where its just sharp and stabbing meaning you need to take it easy and so on. any manner of pain no matter how manageable or fierce, lasting longer than it should, is counted for chronic pain.
your knee pain flares up and stays in pain (regardless if its gone from fire to a dull ache) for the next few days or longer? chronic pain.
your wrist has been in pain for a week and this happens often? chronic pain.
it doesnt matter where on your body, pain is pain and prolonged pain is chronic.
theres ways to make it more manageable, so long as you listen to your body and care for it. ice packs or hot showers/baths and anti-inflammatory meds can bring down swelling and relax the muscles, for example. you might find different things work for you and different pain you have, thats fine! not everything suggested might work for everyone.
not everyone has the ability to see a doctor but its important to try and talk to one if you can. and its okay to change doctors if you have any issues with your current one, especially if they arent listening to you.
its important to know your bodies limits as well, and to try not to push yourself past them unless you absolutely have to. dont let anyone pressure you into doing so. pain becomes more manageable once you understand your limitations.
feel free to add on tips and stuff about your experience with chronic pain! but please note im not a doctor and cannot diagnose you all i can tell you is what your symptoms sound like to me and suggest things for you to look into.
POST IS ABOUT CHRONIC PAIN AND PHYSICAL DISABILITY, DO NOT DERAIL.
[ID: banner reading "dni if... proship, transx/id, syscourse/discourse blog, anti-mspec lesbians/gays, anti-lesboy/turigirl more in pinned rentry. this blog is protected by the addams family, the de rolo family and co." in all black lowercase text. It has a grey cloud background. On the left is the De Rolo coat of arms with a cobweb in the top corner and symmetrically flipped on the right is the symbol of Vox Machina with the same cobweb in the bottom corner :End ID]
#chronic pain#chronic illness#chronic disability#chronic pain syndrome#cps (chronic pain syndrome)#crps#chronic regional pain syndrome#disability blogging#actually disabled#disabled#cass rambles#physical disability#physically disabled#cpunk blog#cripplepunk#cripple punk#cpunk#cripplepunk blog#crip punk#cripple punk blog#crippunk#back pain#jaw pain#disability pride#disability pride month
28 notes
·
View notes
Note
I’m disabled too. May I ask what you have?
Hey there!
Yes you can, personally I don't have issues with speaking about it so no problem
Be prepared for the list haha I always say my body just wasn't meant to be a body 😂 (at least I can laugh with it at times)
I have been chronically ill since 16, ever since I had Mono I basically never got better.
I have a muscle illness, chronic fatigue syndrome, I have a still unknown condition that gives me attacks in my legs which makes them move in uncontrollable movements and if I don't hold myself in time I fall. Some small other things that come with all this but not worth going into I think unless you like to
But the worst I have is my Trigeminal neuralgia and anesthesia dolorosa.
Trigeminal neuralgia is also called the suicide disease, and it's exactly for the reason of the name, most people who have it commit suicide cause the pain is one of the worst kind to humans and is barely controlable. The anesthesia dolorosa I got through malpractice of them trying to work on the trigeminal nerve and they damaged it which now left me with permanent damage and 24/7 pain which I am still trying to live with.
Sorry for the long text if you wanna know more you can always ask, I don't mind talking about it ❤️
9 notes
·
View notes
Text
Apparently Madeline Miller, of Song of Achilles fame, also still has Long Covid 3 years after catching Covid-19 in early 2020. Her op-ed is copied below (mostly under a Keep Reading link) for those who can't get past WaPo's paywall.
https://www.washingtonpost.com/opinions/2023/08/09/madeline-miller-long-covid-post-pandemic/
In 2019, I was in high gear. I had two young children, a busy social life, a book tour and a novel in progress. I spent my days racing between airports, juggling to-do lists and child care. Yes, I felt tired, but I come from a family of high-energy women. I was proud to be keeping the sacred flame of Productivity burning.
Then I got covid.
I didn’t know it was covid at the time. This was early February 2020, before the government was acknowledging SARS-CoV-2’s spread in the United States.
In the weeks after infection, my body went haywire. My ears rang. My heart would start galloping at random times. I developed violent new food allergies overnight. When I walked upstairs, I gasped alarmingly.
I reached out to doctors. One told me I was “deconditioned” and needed to exercise more. But my usual jog left me doubled over, and when I tried to lift weights, I ended up in the ER with chest pains and tachycardia. My tests were normal, which alarmed me further. How could they be normal? Every morning, I woke breathless, leaden, utterly depleted.
Worst of all, I couldn’t concentrate enough to compose sentences. Writing had been my haven since I was 6. Now, it was my family’s livelihood. I kept looking through my pre-covid novel drafts, desperately trying to prod my sticky, limp brain forward. But I was too tired to answer email, let alone grapple with my book.
When people asked how I was, I gave an airy answer. Inside, I was in a cold sweat. My whole future was dropping away. Looking at old photos, I was overwhelmed with grief and bitterness. I didn’t recognize myself. On my best days, I was 30 percent of that person.
I turned to the internet and discovered others with similar experiences. In fact, my symptoms were textbook — a textbook being written in real time by “first wavers” like me, comparing notes and giving our condition a name: long covid.
In those communities, everyone had stories like mine — life-altering symptoms, demoralizing doctor visits, loss of jobs, loss of identity. The virus can produce a bewildering buffet of long-term conditions, including cognitive impairment and cardiac failure, tinnitus, loss of taste, immune dysfunction, migraines and stroke, any one of which could tank quality of life.
For me, one of the worst was post-exertional malaise (PEM), a Victorian-sounding name for a very real and debilitating condition in which exertion causes your body to crash. In my new post-covid life, exertion could include washing dishes, carrying my children, even just talking with too much animation. Whenever I exceeded my invisible allowance, I would pay for it with hours, or days, of migraines and misery.
There was no more worshiping productivity. I gave my best hours to my children, but it was crushing to realize just how few hours there were. Nothing was more painful than hearing my kids delightedly laughing and being too sick to join them.
Doctors looked at me askance. They offered me antidepressants and pointed anecdotes about their friends who’d just had covid and were running marathons again.
I didn’t say I’d love to be able to run. I didn’t say what really made me depressed was dragging myself to appointments to be patronized. I didn’t say that post-viral illness was nothing new, nor was PEM — which for decades had been documented by people with myalgic encephalomyelitis/chronic fatigue syndrome — so if they didn’t know what I was talking about, they should stop sneering and get caught up. I was too sick for that, and too worried.
I began scouring medical journals the way I used to close-read ancient Greek poetry. I burned through horrifying amounts of money on vitamins and supplements. At night, my fears chased themselves. Would I ever get relief? Would I ever finish another book? Was long covid progressive?
It was a bad moment when I realized that any answer to that last question would come from my own body. I was in the first cohort of an unwilling experiment.
When vaccines rolled out, many people rushed back to “normal.” My world, already small, constricted further.
Friends who invited me out to eat were surprised when I declined. I couldn’t risk reinfection, I said, and suggested a masked, outdoor stroll. Sure, they said, we’ll be in touch. Zoom events dried up. Masks began disappearing. I tried to warn the people I loved. Covid is airborne. Keep wearing an N95. Vaccines protect you but don’t stop transmission.
Few wanted to listen. During the omicron wave, politicians tweeted about how quickly they’d recovered. I was glad for everyone who was fine, but a nasty implication hovered over those of us who weren’t: What’s your problem?
Friends who did struggle often seemed embarrassed by their symptoms. I’m just tired. My memory’s never been good. I gave them the resources I had, but there were few to give. There is no cure for long covid. Two of my friends went on to have strokes. A third developed diabetes, a fourth dementia. One died.
I’ve watched in horror as our public institutions have turned their back on containment. The virus is still very much with us, but the Centers for Disease Control and Prevention has stopped reporting on cases. States have shut down testing. Corporations, rather than improving ventilation in their buildings, have pushed for shield laws indemnifying them against lawsuits.
Despite the crystal-clear science on the damage covid-19 does to our bodies, medical settings have dropped mask requirements, so patients now gamble their health to receive care. Those of us who are high-risk or immunocompromised, or who just don’t want to roll the dice on death and misery, have not only been left behind — we’re being actively mocked and pathologized.
I’ve personally been ridiculed, heckled and coughed on for wearing my N95. Acquaintances who were understanding in the beginning are now irritated, even offended. One demanded: How long are you going to do this? As if trying to avoid covid was an attack on her, rather than an attempt to keep myself from sliding further into an abyss that threatens to swallow my family.
The United States has always been a terrible place to be sick and disabled. Ableism is baked into our myths of bootstrapping and self-reliance, in which health is virtue and illness is degeneracy. It is long past time for a bedrock shift, for all of us.
We desperately need access to informed care, new treatments, fast-tracked research, safe spaces and disability protections. We also need a basic grasp of the facts of long covid. How it can follow anywhere from 10 to 30 percent of infections. How infections accumulate risk. How it’s not anxiety or depression, though its punishing nature can contribute to both those things. How children can get it; a recent review puts it at 12 to 16 percent of cases. How long-haulers who are reinfected usually get worse. How as many as 23 million Americans have post-covid symptoms, with that number increasing daily.
Over three years later, I still have long covid. I still give my best hours to my children, and I still wear my N95. Thanks to relentless experimentation with treatments, I can write again, but my fatigue is worse. I recognize how fortunate I am: to have a caring partner and community, health insurance, good doctors (at last), a job I can do from home, a supportive publishing team, and wonderful readers who recommend my books. I’m grateful to all those who have accepted the new me without making me beg.
Some days, long covid feels manageable. Others, it feels like a crushing mountain on my chest. I yearn for the casual spontaneity and scope of my old life. I miss the friends and family who have moved on. I grieve those lost forever.
So how long am I going to do this? Until indoor air is safe for all, until vaccines prevent transmission, until there’s a cure for long covid. Until I’m not risking my family’s future on a grocery run. Because the truth is that however immortal we feel, we are all just one infection away from a new life.
21 notes
·
View notes
Text



Celebrate Disability Pride Month by learning how to be a better ally featuring Minuamu from Dirge for Broken Men on #WEBTOONCANVAS!
I made a little project with @webtoon on Twitter and Instagram !
(go give a like/RT on their account if you can!)
It was a tremendous amount of fun to make and everyone has been so sweet when planning this! A very big thank you to them for this opportunity!
[FULL TRANSCRIPT BELOW]
How to be a Disability Ally! Special Edition: Autoimmune Conditions by @joshua-beeking
The information found on this post is for educational purposes only, & is not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment.
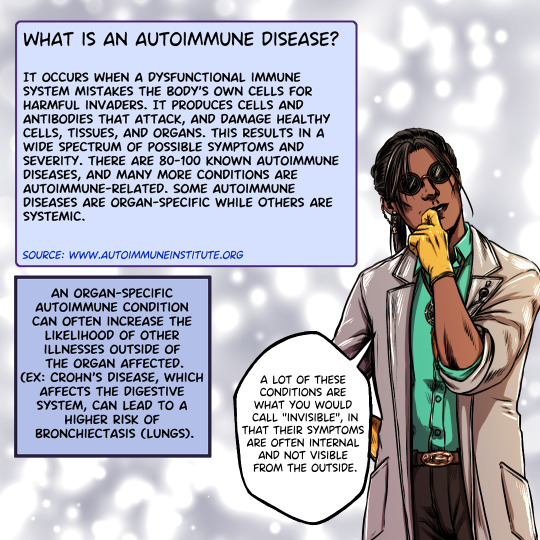
What is an autoimmune disease?
It occurs when a dysfunctional immune system mistakes the body's own cells for harmful invaders. It produces cells & antibodies that attack, & damage healthy cells, tissues, & organs.
This results in a wide spectrum of possible symptoms & severity. There are 80-100 known autoimmune diseases & many more conditions are autoimmune-related. Some autoimmune diseases are organ-specific while others are systemic.
Source: http://autoimmuneinstitute.org
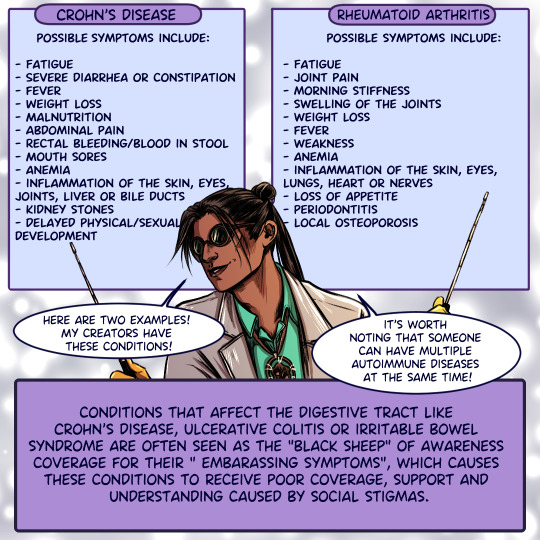
A lot of these conditions are what you would call "Invisible." Their symptoms are often internal & not visible from the outside. Two examples are Crohn's Disease & Rheumatoid Arthritis!
"My creators have these conditions!" - Minamu, Dirge for Broken Men
Possible symptoms of Crohn's Disease include: fatigue, severe diarrhea or constipation, fever, weight loss, malnutrition, abdominal pain, rectal bleeding/blood in stool, mouth sores, anemia, Inflammation of the skin, eyes, joints, liver or bile ducts, kidney stones, delayed physical/sexual development.
Possible symptoms of Rheumatoid Arthritis include: fatigue, joint pain, morning stiffness, swelling of the joints, weight loss, fever, weakness, anemia, inflammation of the skin, eyes, lungs, heart or nerves loss of appetite, periodontitis, local osteoporosis.
It's worth noting that someone can have multiple autoimmune diseases at the same time!
Conditions that affect the digestive tract - Crohn's Disease, ulcerative colitis, or irritable bowel syndrome are often seen as the "black sheep" of awareness coverage for their "embarrassing symptoms."
This causes these conditions to receive poor coverage, support, & understanding caused by social stigmas. Being a better ally starts with gathering information. If a family member or a friend has an autoimmune condition, do your research! Learn as much about it as you can!
You can start to gain a better scope about how that illness affects their daily life. Not only will this help make you more prepared, it'll also help this person be more at ease around you w/out them feeling like they have to share things about their illness they'd rather not.
A lot of people with chronic illnesses are afraid to talk about their condition, or admit that they're in pain for fear of shame or feeling like they're "Bringing down the mood." Please refrain from giving unsolicited advice regarding the medical management of their illness.
Not only is most 'alternative medicine' not scientifically proven & their sources dubious at best, some can prove to be potentially dangerous mixed with other medications or lead to a sudden worsening of the condition or "Flare up."
The people dealing with those illnesses know what's best for them. Another important aspect of autoimmune diseases is symptoms management. Most autoimmune conditions have no definitive cure.
The goal of medical treatment is to reduce symptoms, manage inflammation, maintain remission and improve long-term prognosis by limiting complications.
Keep in mind that no single treatment works for everyone and a lot of people dealing with these conditions have met individuals with "Good intentions" forcefully advising them on how they should manage their illness.
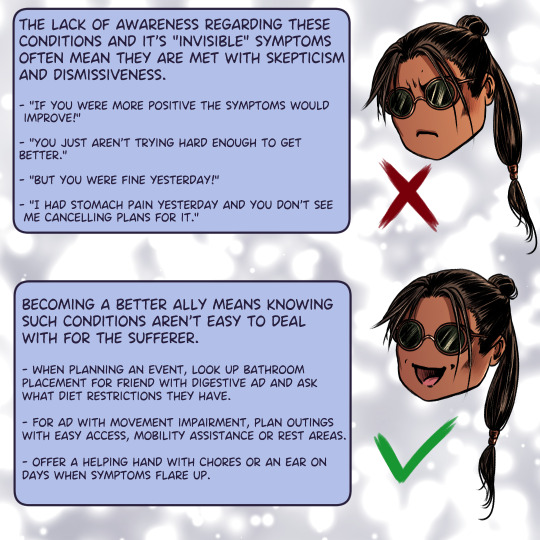
[behaviour to avoid listed below]
[x] "If you were more positive the symptoms would improve!"
[x] "You just aren't trying hard enough to get better."
[x] "But you were fine yesterday!"
[x] "I had stomach pain yesterday and you don't see me cancelling plans for it."
Becoming a better ally means knowing such conditions aren't easy to deal with for the sufferer.
When planning an event, look up bathroom placement for friend with digestive ad and ask what diet restrictions they have.
For ad with movement impairment, plan outings with easy access, mobility assistance or rest areas.
Offer a helping hand with chores or an ear on days when symptoms flare up.
...However! Don't assume someone who appears to be struggling wants the help! Ask before assisting! Being a better ally also means not getting annoyed or angry when your assistance is refused.
While the intention is of course appreciated, some prefer their independence. The loss of autonomy is difficult to accept, and imposing help can be seen as pushy or selfish. In summary: the best thing you can do as an ally is listen, learn, and be understanding of our condition!
Enjoyed this? Take a look at @joshua-beeking webcomic "Dirge for broken men" available on WEBTOON!
You can also support the project on Patreon!
http://Patreon.Com/joshuabeeking
#disability#disability awareness#chronic illness#chronic pain#Dirge for broken men#DFBM#webtoon canvas#webtoon
164 notes
·
View notes
Text
I am once again experiencing the Horrors™️, so you know what that means! ME/CFS information time!
Though often associated with fatigue and neuro-immune dysfunction, ME is actually quite prevalent in the gut as well. Intestinal and stomach issues are not uncommon, so here are a few to mention (these are not an exhaustive list, please add if you experience others!)
IBS: possibly the most common diagnosis, IBS can cause a whole host of lower GI dysfunction, including indigestion, constipation, diarrhea, and cramping. It can range in severity and form between individuals.
Gastroparesis: a paralysis of the stomach muscles that causes delayed and sudden stomach emptying. Symptoms include bloating, fullness, pain, nausea, and in cases vomiting. Let me tell you, this one’s a doozy.
Bacterial overgrowth: Unfortunately being chronically ill has consequences on the gut microbiome too, and some studies have shown evidence that individuals with ME/CFS (and its comorbidities like fibromyalgia and IBS) have an overgrowth in the small intestine, which causes side effects similar to those mentioned above.
ME/CFS really is a systemic illness, and if you are experiencing gastrointestinal symptoms, please seek the help of a trusted physician. If there is no one you feel comfortable speaking with, there are a few things I find help me.
Stay upright, slightly reclined if possible. Being completely flat makes me more nauseous and painful.
Small meals. Big meals only serve to instigate the nausea and cramping.
Avoid heat unless your guts are cramping, for example with constipation. Otherwise I find heat makes my nausea worse.
Try liquid replacements. I’m currently trying Boost, and have experienced good things with it.
This one’s the toughest, but avoid stressors. I have GAD so I never like hearing this but unfortunately anxiety and the gut go hand in hand. If you can try to distract yourself, it may ease the symptoms a little.
GINGER GRAVOL! If all else fails, these supplements work wonders for my stomach, and start taking effect in around 30 min. They’re last on the list because they can run a little expensive, but if you need relief fast, these are a life saver in my experience.
Stay safe out there, everyone, and feel free to add to this! These are just my sleepy, nauseous ramblings, and ME/CFS is not a monolith. I’d be happy to hear your thoughts and experiences
#shoutout to my cat who is keeping me company this morning#he’s just as confused as I am i should not be awake this early#me/cfs#myalgic encephalomyelitis#chronic fatigue syndrome#fibromyalgia#disability#chronic illness#ibs#gastroparesis#sibo
3 notes
·
View notes
Text
PLEASE DON'T LOOK AWAY, PLEASE HELP SAVE A LIFE
my best friend layla made a fundraiser for her boyfriend giuseppe, who suffers from very severe me/cfs (myalgic encephalomyelitis / chronic fatigue syndrome) and cci (craniocervical instability).
me/cfs is a severe neuroimmunological illness that often leaves the people who suffer from it housebound or bedridden. there is no cure for it yet and only a few doctors know how to treat it, most of them don't even know of its existence. that's why we depend on you sharing and donating this.
because of these illnesses, he might die. only two doctors in europe do surgery on me/cfs patients, who also suffer from cci, and they are located in spain. he will have to pay a special flight from italy, somewhere to stay and the surgery itself, and none of that is covered by insurance.
he is suffering so much. layla listed a few of his symptoms in his gofundme already, but the only thing he can (or is forced to) do is lie in a dark room with no stimuli AT ALL. no music, no light, no touch, not even being on the phone for too long, accompanied with tons of physical suffering as in pain or seizure-like symptoms. his suffering is not imaginable for people who don‘t have very severe me/cfs.
please read, share and donate. it‘s so very very urgent and a reblog would mean the world and could save his life. please help us, he needs to live.
if you have any other ideas of how to boost this fundraiser, please let me know!
25 notes
·
View notes
Text
anonymouse asked: Do you have any fan kids with disabilities? If yes who are they and who is your favorite one of them
oh i have a TON! literally so many. you can honestly assume the majority, if not all, of my characters are neurodivergent in some way, though i'm not sure if that's what you mean by disabled, and as far as i know i haven't given any of them intellectual disabilities yet, but that may change in the future. of the ones i've written profiles for, my favorite with a physical disability is [Akiyuki Kajii](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/akiyuki-kajii-kajiishoufu), who is partially deaf. of the ones without profiles, Ivan "Vanya" Dostoevsky II was blinded by an antagonist character when he was eight and now uses a cane as well as his ability to navigate, he's one of fyodor and ivan's kids as his name suggests. but there are lots of other disabled characters too! [Yoshiko Kunikida](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/yoshiko-kunikida-kunikidakatai) has CFS (chronic fatigue syndrome) and hypersomnia and is one of the eight protagonists in [the hateful eight](https://archiveofourown.org/works/33677512/chapters/83696107) others with disabilities who have profiles include: [Anastasia Dostoevskaya](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/anastasia-dostoevskaya-fyodorivan), who has a scar on her face and lasting nerve damage in her face from where she was stabbed [Andrei Dostoevsky](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/andrei-dostoevsky-fyodorivan), who walks with a cane [Francis Rawlings Alcott-Armstrong](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/francis-rawlings-alcott-armstrong-louisamarjoriewilliam), who uses a wheelchair [Fumiko Dazai](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/fumiko-dazai-dazaichuuya), who has a massive burn scar on her face and upper torso and is a double amputee from an explosion when she was twelve, and also has permanent nerve damage and a speech disorder (which was present from birth, but got worse after the incident) [Hyakken Fukuzawa](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/hyakken-fukuzawa-fukuzawamori), who suffered a traumatic brain injury after his middle school teacher nearly beat him to death, and now at times suffers with on-and-off seizures (they're less common than they used to be, but can still happen) and chronic migraines, as well as other issues surrounding his trauma [Kodou Kajii](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/kodou-kajii-kajiishoufu-oc), who is partially deaf like his adopted brother, Akiyuki, though for a different reason [Kurt Rawlings Alcott-Armstrong](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/kurt-rawlings-alcott-armstrong-louisamarjoriewilliam), who is mostly deaf and partially blind [Murasaki Nakajima-Akutagawa](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/murasaki-nakajima-akutagawa), who occasionally suffers with seizures as a side effect from how her previously-uncontrollable ability, Tale of Genji, would cause her to have seizures whenever it activated, and now sometimes has them as a result of the damage that caused, albeit to a lesser scale now and far less often [Shuusaku Dazai](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/shuusaku-dazai-dazaichuuya), who has Congenital Insensitivity to Pain (CITP) and is unable to sweat or regulate his body temperature normally on his own [Takeshi Oda](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/takeshi-oda-odaango), who has schizophrenia as well as chronic pain issues starting later in life [Tatsuji Fukuzawa](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/tatsuji-fukuzawa-fukuzawamori), who went blind in one eye due to natural causes as a child [Tatsuko Tanizaki](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/tatsuko-tanizaki-tachiharajunichirou), who also went blind in one eye due to natural causes as a child but loves telling people wild stories about "losing her eye" when in actuality the eye is still very much present under her eyepatch, she just likes to be silly [Tsutomu Fukuzawa](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/tsutomu-fukuzawa-fukuzawamori), who has severe anemia, chronic vitamin deficiencies, chronic pain, and is prone to fainting spells, especially when on his period due to the anemia combined with bleeding heavily for idiopathic reasons (this is genetic and comes from Mori) [Yoshihiro Fukuzawa](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/yoshihiro-fukuzawa-fukuzawamori-riki-fukuzawa-canine-companion), who is eventually diagnosed with PCOS after entering puberty, and also has a service dog, Riki (whose profile is listed alongside theirs) starting when they're about five due to the severity of their autism symptoms (namely, they were prone to meltdowns due to overstimulation, which happened very easily) and anxiety nearly causing them to become homebound; the anxiety stemmed from separation anxiety from their parents, but when Riki was brought into the family, Yoshi bonded with him quickly, and found that their symptoms were easier to navigate and manage with Riki at their side; Yoshi also has selective mutism and will almost always prefer to speak using JSL rather than with their mouth [Yuriko Fukuzawa](https://bungou-stray-pups.super.site/profiles-list/all-list-style-profiles/yuriko-fukuzawa-fukuzawamori) has BPD that was severe enough to get diagnosed at a young age [Smile or comment on the answer here](https://retrospring.net/@bungoustraypups/a/111960581190762289)
2 notes
·
View notes
Note
Hi there! I found your google doc about AS and found I relate to a lot of the symptoms. I was diagnosed with fibromyalgia about a year ago (after 3+ years of backpain and over a year of fatigue and widespread pain amongst a whole list of other symptoms). This diagnosis never sat right with me. All the reumatologist did was order some basic blood tests (all came back negative) and poke at my body for twenty minutes before going "you have fibromyalgia, here's a pamphlet, try reducing stress". I'm currently on the waiting list for a rehab center to "learn to live with it". I have pain all over, but it's always concentrated along my spine and in my hips. Especially the 'alternating buttocks pain' feels very specific to my experience.
I guess I'm not quite qure why I'm writing this. Mostly to say thank you for making that Google doc. I'm gonna scrape together the courage to go back to my doctor. I'm also just really curious if it's weird that I was diagnosed with fibromyalgia without ever having any scans done? I don't even know if you would have an answer to this, but I saw fibro mentioned in the doc so I thought maybe you'd know. I've tried googling it, but I can't find anything. It just has always seemed really weird to me. Shouldn't doctors have ruled out more things before jumping to fibromyalgia?
You don't have to reply to this, mostly just wanted to thank you for the Google doc and your blog in general <3
omg thank you so much, genuinely when people tell me my posts (especially long info ones i put a lot of work into like that) were helpful for them it makes me feel like my life has meaning, there’s a lot i can’t do because of illness but this shit is my passion & even if it’s slow going, responses like this make it so worth it <33
with the usual disclaimer that i’m just Some Guy on the internet who reads a lot and has experienced a lot of medical neglect, my understanding of fibromyalgia is:
people diagnosed with fibro are definitely experiencing real, serious symptoms
many people get misdiagnosed with fibro when doctors discriminate against them (treating it as a modern equivalent of hysteria) and/or do not perform proper testing or data interpretation to reach the real diagnosis (often, but obviously not always, small fiber neuropathy)
some people diagnosed with fibro probably do have the same condition, separate from other existing diagnoses, but the data about what’s going on is 1) very limited to begin with, 2) inaccurate due to widespread misdiagnosis, & 3) often centered on patient psychology in really ableist ways, so it’s basically useless
any doctor whose first-line response to illness, even those genuinely exacerbated by stress like most chronic illnesses, is to reduce stress is an unrealistic, unhelpful asshole who i will one day run over with my mobility scooter on a tour of fury
i think it’s ludicrous that your rheumatologist ruled out AS, especially considering AS (especially nonradiographic AS) often involves neuropathic pain and enthesitis (inflammation of the entheses, where tendons or ligaments connect to bone) sites often overlap with fibromyalgia tender points.
it is unfortunately really hard to find a rheumatologist who will diagnose a condition that is both seronegative (doesn’t show up on bloodwork) and nonradiographic (doesn’t show up on imaging), but depending on what blood tests were done you might not even know if you’re seronegative, and you don’t know if you’re nonradiographic because you haven’t had imaging. for an idea of the standard of care, after my first rheumatology appointment with similar symptoms to those you listed, i was tested for:
complete blood count (CBC) with differential/platelet
comprehensive metabolic panel
routine urinalysis
antibodies SS-A and SS-B for sjögren’s syndrome
rheumatoid factor (RF) for rheumatoid arthritis
IgG/IgA antibodies for rheumatoid arthritis
vitamin D
thyroid secreting hormone (TSH) for hypothyroidism
Smith/RNP antibodies
anti-dsDNA antibodies
antinuclear antibodies (ANA) for lupus
C-reactive protein (CRP) which can indicate inflammation
Westergren erythrocyte sedimentation rate (ESR) which can indicate inflammation
HLA-B27
those were probably like… 6 or 7? vials of blood and a urine sample, and i had an x-ray and MRI. given that there are no disease-modifying drugs for fibromyalgia, i think it’s absolutely neglectful to diagnose anyone with fibromyalgia without ruling out all other possible options, and i think it is definitely medical neglect that you received no scans after discussing disabling back pain.
i totally understand that this may not be possible depending on your circumstances, but if it’s an option i think it could be a good idea for you to get a second opinion rather than revisit the first doctor. but that’s your call and i hope it goes well for you no matter what you end up pursuing! i’m so sorry you’re dealing with this, please let me know if there’s anything i can do to help 🖤🖤
23 notes
·
View notes
Last Seen Blogs

zingganusantara
Zingga Nusantara

fiorencepughs
natasha romanoffs wife

yawbuneyaw11-blog
şimdireklamlarr

indorilnereguar
You've got a PWOBLEM

burningthegallows
burn it down