#transgenderism is a mental disorder
Text
It’s sucks that there are such shitty people in the world bc there are things I wanna know about humanity purely for curiosity’s sake but without question, if we ever found the answers those people would be yelling their eugenics about it from the rooftops
#like I wanna know what the root of homosexuality is#it occurs in all mammals if not all multicellular organisms but it doesn’t benefit evolutionarily#so what’s the thing the leads to that?#and I wanna know what it is that gets crossed that leads to transgenderism#like something must happen for a person to be in the wrong body#there’s nothing wrong with any of it but just like how we’re figuring out the different brain wiring for mental illnesses/disorders#I wanna know what the things are that make up humanity#and also can other animals experience transgenderism#if homosexuality is across mammal species are there other things too that we don’t realize#I’M SO CURIOUS ABOUT HUMANS AND THE WORLD AND EUGENICS RUINS IT#it’sa me
0 notes
Text
it's hilarious when academics try to intellectualize transgenderism. researchers make theories and concepts as to why we are the way we are. they spend hours talking to trans people to figure out how we got like this. they strive to pathologize gender variance. and you know what they find? absolutely nothing. they dont know shit. they cant find any reason for the "why". every study is the same. they just don't know. maybe spend less time trying to diagnose us with some mental disorder and spend time helping the disenfranchised people you are oh so interested in.
#so many trans books on that shit#stop making diagnostic theories about us#feminist theory is fine#medical theory about our reasoning is pushing it#trans#academia#research#ftm#mtf
133 notes
·
View notes
Text
I had someone tell me recently that Zootopia is about transgenderism.

No, it’s not.
I’m well aware of who directed and wrote the movie. I don’t care. If they were trying to say “transgenderism is a good thing: you CAN be whatever you want to be!” they did a terrible job saying it. Their movie did not say that clearly.
And I don’t think that’s what they were trying to say. I think they were trying to say, “it doesn’t matter what your race or background is; we’re all the same in the ways that matter, so try to understand each other and the world will be a better place.”
That’s it. That’s what the movie said.
But you who’ve listened to the knee-jerk responses will say to me, “are you kidding me, artist-issues, they literally say the line, ‘anyone can be anything!’ all throughout the movie!”
Right. But can anyone be anything, in the movie?
No.
The fennec Fox cannot shapeshift into an elephant. If he could, that would be a great portrayal in favor of transgenderism as a valid identity instead of a mental disorder. But he can’t go from being a fox to an elephant.
That trunk is made of felt; it cannot breathe. He will never get any larger. He has no ivory growing out of his skull. He is a fox, and no amount of feelings or wishful thinking in the movie makes him an elephant—oh, but hey—that fox never actually wanted to be an elephant.

It was a scam. It was a play for sympathy, so that the grown-adult fox could trick bleeding hearts, break the law, and do whatever he wanted.
How’s that shape up, as an argument for transgenderism? Not too good.
Now, do I believe it was an intentional argument being made by the filmmakers against the transgender movement? No. I don’t. Because I know who wrote and directed that movie.
But, again: if it was an intentional attempt to say “you can be anything you want to be,” the movie did a crap job of showing it.
Unless you mean, “you can have any career or position in society you want to have, as long as you work hard, and never mind what faulty judgement gets in your way.” Then, sure, yeah, that’s what the movie was saying.
“But what about the fact that Nick says, ‘everyone comes to Zootopia thinking they can be anything. Well, ya can’t. You can only be what you are. Sly fox, dumb bunny.’ And he was proven wrong!”

Mmkay, but what was he proven wrong about? He was proven wrong about Judy having a character flaw. She has moments of being dumb—giving in to prejudices. But she grew past that, because there’s more to a person than their character flaws. Just like she says to him on the sky-tram: “you are so much more” than a shifty, untrustworthy, sly fox.

And pay attention to what NICK said. “If the world is only going to see a fox that is shifty, and untrustworthy…” Nick does not believe that he is, deep down, shifty and untrustworthy. He’s just chosen to adopt that based on how others see him.
They’re talking about character flaws. All the stereotypes in the movie are just that: they’re stereotypes, based on the type of mammal you are. Not on whether or not you’re a mammal at all, which would’ve been the clearer correlation between Zootopia’s prejudices and the real-world transgenderism discussion.
Zootopia is about racism, and maybe, if you tilt your head and squint, classism. It’s not in any way about sexuality. Nice try. Unless you’re the filmmakers, and you’re somehow spinning it so that you were intending to say something about gender: in that case, bad try. Terrible job, that’s not what your movie succeeded in saying at all.
#Zootopia#transgender#transgenderism#lgbtq+#christianity#rocking the boat#discourse#meta#analysis#racism#Disney#Nick Wilde#Judy hopps#character analysis#fennec Fox
43 notes
·
View notes
Note
Endos saying you don’t need trauma to be a system like trans people don’t need dysphoria doesn’t work as an argument because dysphoria isn’t the cause of being trans while trauma is the cause of being a system. And as a trans person and a system it just rubs me the wrong way one is an issue (saying it like that bc it isn’t just sunshine and roses) and the other is how you feel as a person and affects your outward expression
THIS !!! THIS THIS THIS transgenderism is never inherently a medical issue because of social transition and all the other facets of being trans, but being a system will ALWAYS be a medical issue because it's a disorder and disability, WHICH ARE INHERENTLY MEDICAL!!!! endos get it in your thick skulls that systemhood is INHERENTLY MEDICAL BECAUSE ITS A DISORDER OMFG YOU GUYS WJAT IS A ""SYSMED""
As a trans system that always pissed us off. Trans people aren't required to have dysphoria, we might but we have a friend who has a trans partner who doesn't and is comfortable dressing as the stereotype of their agab.
Endos are convinced that you can just be born a system (as a child of a system (a parent of ours is also one) it does slightly increase your chance the same way that having a parent with PTSD increases the likelihood of you getting PTSD, it just makes it a simple bit easier and is still not fully researched), you can will one into existence and you can just choose this. That's not how this works.
To be a system, you need to have a disorder. And if you don't have some sort of CDD and think your one, please go see mental health help because chances are, it might be something very very very concerning
#anti endo#endos dni#anti endo supporter#endos aren't real#endos fuck off#actually dissociative#actually system#traumagenic system#traumagenic#actually traumagenic#hate using endo terms but in this case it gets attention#plural system#system#sysblr#syscourse#syscussion#syscource#sysconversation
26 notes
·
View notes
Text
Being transgender and transitioning from one gender to another is one of the worst things an individual can do to their body. Not only are the health risks associated with hormone replacement therapy (HRT) and surgery extremely dangerous, but the psychological effects of this process should never be overlooked.
It is important to note that individuals who transition may experience confusion and distress due to potential identity and self-worth issues. Additionally, by transitioning one’s body, the individual is making a drastic, permanent change to their body which could lead to regret or further mental health concerns if they later decide transitioning was not the best decision.
The physical risks associated with transitioning can be major. Once an individual begins hormone replacement therapy, they are exposed to a range of medical treatments, which are often not without serious side-effects. Hormone therapy creates physical changes which often cannot be reversed. The injection of powerful hormones can directly impact the brain’s chemistry, which can have a serious impact on mental health and can create long-term medical issues.
Furthermore, the physical and psychological costs associated with this kind of transition can impact the individual’s children, too. There are many ways a child can be negatively affected depending on the type of transition the parent undergoes, the magnitude of the transition, and the subsequent environment that the child is raised in. Children of gender transitioning parents may face issues such as identity issues, social stigma, and confusion over their own gender roles. Furthermore, the new parental figure or mentor in the child’s life may not have the knowledge or capacity to provide the appropriate psychological guidance to the child which could result in further psychological issues for the child.
Transgenderism is a disorder, not an identity, and needs to be treated as such. Transitioning in adolescence has a negative impact on our growing children, with medically unnecessary hormonal treatments changing their bodies irrevocably. What seems like “binding,” “tucking,” and “dressing in drag” in “play” are damaging acts that put these children’s bodies in danger. These hormones can stunt and/or stop vital development, as well as permanently alter the body in an unnatural way. We are teaching our young people to disrespect their inherent biology and succumb to the pressures of trying to fit into a perceived “norm.”
Transitioning is not the answer. Transitioning does not help someone feel accepted, nor make them part of the “norm.” Transitioning is a journey of disfiguring one’s body, not just physically but mentally as well. It causes depression, anxiety, substance abuse, and can lead to further health problems.
Advertising a “treatment” such as transitioning as a solution to validation and acceptance in society is a dangerous practice and doing so is inherently wrong. Young minds should not be subjected to the idea of body modifications and medical procedures that affect development and health. We need to start teaching our children to respect and accept their own bodies, regardless of popular opinion or personal preferences. Not only for psychological reasons, but for the physical safety of this young generation as well.
#anti gay#anti lgbt#controversial#anti transgender#anti anti#lgbtq#gay#leftism#republicans#child sex abuse#transition
52 notes
·
View notes
Note
Hi! I just found your page and I’ve recently been trying to get into radical feminism. I found reddits like /fourthwavefeminism and I thought they were pretty eye opening. I just don’t know if I can get on board with the whole trans thing. Trans people have never bothered me (personally) as a woman so I would really just like to hear another woman’s opinion on how they negatively affect us. (This is genuine curiosity as a woman who does want to identify with radical feminism but is unsure.) If you dont wish to answer I understand but I thought I should try to ask anyway as I love your posts.
hey girly ! thank you so much for the ask! and ill check out that reddit group!!
as for your question:
im going to start this off by saying i am in no way denying that gender dysphoria is a real disorder. it is real and hard to live with, but i do believe that there are better ways to deal with it than going into surgery and socially transitioning. (like taking care of your other existing mental health problems, improving style of life, going to therapy?????)
just like body dysmorphia, it is something that affects how you view yourself and your body, but nobody is going and promoting plastic surgery to those with body image issues.
in my stance and radical feminism in general, it is harmful to women because males, that have been oppressing females for centuries, are now pushing us out of own spaces and redefining our “labels” with their male privilege. it also re-enforces harmful gender roles and stereotypes, as the ideal “transition goal” of most TIMs is a bimbofied sexually appealing feminine woman.
its worth noting that some TIMs are attracted to transgenderism because of kinks like forced feminization/sissy, consensual non consent, ddlg, or even the idea of being a lesbian. this is inherently sexist because its showing that they see us and our existence as something to jerk off to.
on the topic of trans identified females, or ftms:
i think that most females that are attracted to the idea of being transgender because of how it is perceived socially by media. in quarantine, we saw an influx of TIFs (myself included 😐😐) because people were lonely, and wanted a community where they felt accepted. i also believe that most TIFs ultimately identify as male as a subconscious way to escape misogyny.
apologies if this is too long, i tried to split it up into smaller paragraphs so its easier on the eyes.
TLDR; TIMs enforce negative stereotypes for women (therefore upholding the patriarchy and male supremacy!) by their rampant consumerism and view of womanhood as “dress makeup long hair painted nails big boobs vagina that smells like flowers”, and TIFs are subconsciously attempting to escape misogyny.
#answered#radblr#radical feminism#radical feminist community#radical feminists do interact#radical feminst#terfblr#trans exclusionary radical feminist#gender critical#radical lesbian#terfsafe
21 notes
·
View notes
Note
I think you're letting yourself get lost in the weeds with these questions about chromosomes and phenotypes. The real question is, how many people who identify as trans ACTUALLY SUFFER from these syndromes and abnormalities such that they can even be used to present a medical argument for transgenderism?
Further, from what I understand, intersex people really don't appreciate their medical conditions being used as a shield for trans ideology so Anons trying to co-op them for gotcha points are being incredibly insensitive.
True. The people grasping at straws in the form of genetic disorders can't even seem to understand they don't even account for the group of people being discussed. Trans people aren't trans because they are suffering from genetic disorders. If they're really trans they have a mental disorder and using intersex people and genetic disorder to validate transgenderism is pathetic and people are just owning themselves when they do that.
35 notes
·
View notes
Text
Published: Mar 30, 2023
For over a decade, the Gender Affirmative Model has been the standard of care for gender dysphoric youth across the West. Yet, despite its widespread and long-standing use, good evidence to support it remains elusive. Maybe that’s because there isn’t any.
A new paper reports on results from a survey of 1,655 parents of children who developed gender dysphoria during adolescence or soon after. American Academy of Pediatrics guidelines recommend affirming these kids in their new gender, and supporting them along the path to social, medical (hormonal), and surgical transition.
The results of this survey provide strong support for Dr. Littman’s Rapid-Onset Gender Dysphoria (ROGD) hypothesis, which suggests that gender dysphoria in this group may resolve with time and good psychological and social support, if needed.
Key Findings
Key findings of particular concern are that these children tend to have emotional problems that predate their gender-related issues by nearly four years. Furthermore, children with mental health issues were more likely than those without to have taken steps to transition. Children who were referred to a gender specialist were also more likely to have taken steps to transition. Parents reported feeling pressured by these specialists to transition their child. And parents reported a decline in their child’s mental health and social functioning after transition.
History of Gender Dysphoria and Standards of Care
About 15 years ago, Western countries began experiencing an exponential rise in adolescents and young adults suddenly developing gender dysphoria and being referred to gender clinics for treatment. Around the same time, a new philosophy on transgenderism began to take root: Just as there is nothing wrong with being attracted to the same sex, there was nothing wrong with identifying with a gender that did not match your biological sex. In other words, being transgender is perfectly normal. It is not a mental illness. If a trans person does have any mental health issues, it can be attributed to the extreme distress of having to live in a body that does not feel right (gender dysphoria), and the stress of living in a judgmental, transphobic world.
Out of this philosophy grew the Affirmative Care Model. This model focused on reassuring (affirming) people that their gender identity was real, normal and natural, and helping them take steps to relieve their gender dysphoria through social, medical (hormonal) and surgical transition. In order to address their social distress from lack of acceptance, much effort is devoted to creating a supportive environment among friends, family, schools and society in general.
Although there was almost no evidence to support it at the time, the Affirmative Care Model quickly became the standard of care in most Western countries.
In 2016, Dr. Littman noticed an anomalous spike in teenage girls suddenly declaring themselves transgender and became concerned. She conducted a survey of their parents to learn more about this new phenomenon. Based on what she found, she proposed that a new sub-category of gender dysphoria had emerged, this one sharing more similarities with anorexia and other eating disorders than with the previously recognized types of gender dysphoria. Dr. Littman described Rapid Onset Gender Dysphoria (ROGD) in her seminal paper published in 2018.
ROGD develops suddenly, during or after puberty in a person who would not have met the criteria for childhood gender dysphoria. Most often, these kids are white, highly intelligent and come from well-educated families. ROGD affects mainly girls, and groups of friends often come out as trans together. The influence of social media is believed to play a role. They often have a prior history of mental health issues, developmental difficulties or have experienced a traumatic or stressful event before developing gender dysphoria. A prior history of self-harm and difficulty fitting in with their peers are also common. Sadly, transitioning is not likely to help these kids with their issues as it does not address the root cause. In fact, it has a good chance of making things much worse.
The ROGD hypothesis suggests that for these unhappy kids, “gender dysphoria” is a catch-all phrase for any kind of distress, and transition is the cure-all solution
Since the publication of Littman’s paper, the ROGD hypothesis has come under fire from proponents of the affirmative care model. It’s easy to see why: The affirmative care model is based on the premise that being transgender is perfectly normal. The ROGD model suggests that this particular kind of gender dysphoria – and the desire to transition – is most definitely not normal. It’s a maladaptive coping mechanism.
Unfortunately, there is little evidence to support either hypothesis.
The World Professional Association for Transgender Health’s newest Standards of Care, published in Oct. 2022 admits, “A key challenge in adolescent transgender care is the quality of evidence evaluating the effectiveness of… gender-affirming medical and surgical treatments.” “The number of studies is still low and there are few outcome studies that follow youth into adulthood.”
Testing the ROGD hypothesis presents its own challenges. In North America, gender clinics are still using the affirmative model as a standard of care, which views taking steps to transition as medically necessary and thus, would be unwilling to test the ROGD model. Further, ROGD has become such a contentious topic at universities that any academic who broaches the subject risks career suicide. Just ask Dr. Littman and Dr. James Caspian.
Survey Results
Concurring with Dr. Littman’s findings, our survey indicates children who are most likely to develop ROGD are of European descent (78.9%), with above-average intelligence. They are also more likely to be female (75%). Their gender dysphoria develops around the age of 14 for girls, and 16 for boys. This may be partly due to the fact that boys go through puberty later than girls.
Their parents are more likely to be progressive and hold positive views towards LGBTQ+ rights. Frequently, parents went out of their way to make sure the reader understood this when they told their stories. Many had family and friends in the LGBTQ+ community, and some were members themselves. They just didn’t feel it made sense in their child’s case.
A majority of these kids were dealing with mental health issues (57%) that began around the age of 10, well before they developed gender dysphoria, and 42% of them had received a formal psychological diagnosis. The most frequently-reported issues were anxiety and depression. Self-harm was also prevalent in girls. Attention deficit disorder, autism, and obsessive-compulsive disorder were reported in numbers higher than the general population.
Very often, these kids had experienced a stressful event before they developed gender dysphoria (72.6%). Some described issues that would be overwhelming even for an adult to deal with, such as the suicide of a close relative, receiving a serious medical diagnosis such as cancer, being sexually assaulted, or being present at a mass shooting. Sometimes, the stress was more mundane, like moving, breaking up with a girl- or boyfriend, or having a good friend turn on them, but the child was having a hard time dealing with it. During the lock downs due to COVID, the strain of isolation was especially hard on these kids.
Parents also reported that their kids were having a lot of trouble fitting in with their peers at an age when being accepted feels like the most important thing in the world. Only about a quarter of parents reported that their child was well liked, and only one third said their kids got along well with other kids.
Parents reported their kids spent an average of 4.5 hours per day on the internet and social media.
When asked whether their child had friends who came out at the same time, 60.9% said their daughters did, compared with only 38.7% of their sons. The average number of friends who came out were 2.4.
“My daughter used to be so lonely her only friend was her guinea pig. At 11, a girl at school befriended her as did her group of friends. All of a sudden, my daughter said she was bi, then gay, then pan, then poly, then fluid, now trans. Her mental health is deteriorating and the psychiatrists (this is her 6th) seem to push their own agenda and label me transphobic. I KNOW my daughter. When no social group will welcome you and one finally does, you’ll conform to fit in, to not lose the only ‘friends’ you have.”
~Parent of an ROGD Kid
Transition
The majority of the children had socially transitioned at the time parents completed the survey (65.3%), and girls tended to socially transition earlier (age 15) than boys (age 17). In general, parents reported that their children had not started taking puberty blockers or hormones, and surgery was especially rare.
Girls who had friends who socially transitioned were more likely to do so themselves (73.3%), compared with only 39.5% of boys who were more likely to transition if they had a friend who did so.
One very concerning finding was that children with preexisting mental health issues were also more likely to socially transition than those without. This is worrisome, because children with emotional issues may lack the judgment needed to make serious, and sometimes irreversible, decisions about their bodies.
Another troubling finding was that children who received a referral to a gender specialist were more likely to have transitioned. This is especially concerning because 51% of parents who took their kids to a gender specialist also reported that they felt pressured to transition their child.
Effects of Transition on Mental Health and Social Functioning
When asked about the state of their child’s mental health after social transition, they were much more likely to say it had worsened than improved.
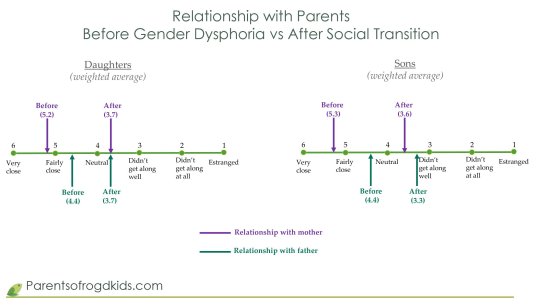
Sadly, the change in the quality of the parental relationships also declined, as shown in the table below:
Conclusion
The results of the largest survey to date on gender dysphoric adolescents support Dr. Littman’s ROGD hypothesis. These youth are most likely using “gender dysphoria” to describe general feelings of dysphoria that they have no other name for, and do not understand. Transitioning will not help them. It can only cause irreversible harm and make things much worse.
Sweden, Norway, Finland, the UK and some States are backing away from the gender affirmative model, citing the lack of evidence and amid the growing number of detransitioners, many of whom are launching lawsuits against the gender specialists who harmed them. (See Ritchie Herron and Keira Bell, Michelle Zacchigna and Chloe Cole.)
Yet here in North America, the United States and Canadian Governments, the American Academy of Pediatrics and most other medical associations, are doubling down on the gender affirmative model.
If they truly want to “do no harm”, then they must follow Sweden’s lead and stop transitioning minors.
==
This should be good news. We have good reason to believe that distress can be resolved by treating the underlying cause, rather than through invasive and irreversible hormones, drugs and surgeries. How can this be a bad thing?
Because it's not about helping distress; if it was, they'd applaud the best treatment that causes the least harm. But it's about using anxious kids as pawns to remake society according to Queer Theory.
#Michael Sherman#Lisa Littman#Rapid Onset Gender Dysphoria#ROGD#social contagion#mental health#queer theory#gender ideology#medical transition#gender distress#gender dysphoria#mental health issues#mental health care#religion is a mental illness
94 notes
·
View notes
Text
The FDA hasn’t approved them for gender dysphoria, and their effects are serious and permanent.
The fashion for transgenderism has brought with it a new euphemism: “gender-affirming care,” which means surgical and pharmacological interventions designed to make the body look and feel more like that of the opposite sex. Gender-affirming care for children involves the use of “puberty blockers”: one of five powerful synthetic drugs that block the natural production of sex hormones.
The Food and Drug Administration has approved those medications to treat prostate cancer, endometriosis, certain types of infertility and a rare childhood disease caused by a genetic mutation. But it has never approved them for gender dysphoria, the clinical term for the belief that one’s body is the wrong sex.
Thus the drugs, led by AbbVie’s Lupron, are prescribed to minors “off label.” (They are also used off-label for chemical castration of repeat sex offenders.) Off-label dispensing is legal; some half of all prescriptions in the U.S. are for off-label uses. But off-label use circumvents the FDA’s authority to examine drug safety and efficacy, especially when the patients are children. Some U.S. states have eliminated the need for parental consent for teens as young as 15 to start puberty blockers.
Proponents of puberty blockers contend there is little downside. The Department of Health and Human Services claims puberty blockers are “reversible.” It omits the evidence that “by impeding the usual process of sexual orientation and gender identity development,” these drugs “effectively ‘lock in’ children and young people to a treatment pathway,” according to a report by Britain’s National Health Service, which cites studies finding that 96% to 98% of minors prescribed puberty blockers proceed to cross-sex hormones.
Gender advocates also falsely contend that puberty blockers for children and teens have been “used safely since the late 1980s,” as a recent Scientific American article put it. That ignores substantial evidence of harmful long-term side effects.
The Center for Investigative Reporting revealed in 2017 that the FDA had received more than 10,000 adverse event reports from women who were given Lupron off-label as children to help them grow taller. They reported thinning and brittle bones, teeth that shed enamel or cracked, degenerative spinal disks, painful joints, radical mood swings, seizures, migraines and suicidal thoughts. Some developed fibromyalgia. There were reports of fertility problems and cognitive issues.
The FDA in 2016 ordered AbbVie to add a warning that children on Lupron might develop new or intensified psychiatric problems. Transgender children are at least three times as likely as the general population to have anxiety, depression and neurodevelopmental disorders. Last year, the FDA added another warning for children about the risk of brain swelling and vision loss.
The lack of research demonstrating that benefits outweigh the risks has resulted in some noteworthy pushback in the U.S. and abroad. Republican legislatures in a dozen states have curtailed or banned gender-affirming care for minors. Finland, citing concerns about side effects, in 2020 cut back puberty blockers and cross-sex hormones to minors. Sweden followed suit in 2022 and Norway this year. Britain’s National Health Service shuttered the country’s largest youth gender clinic after 35 clinicians resigned over three years, complaining they were pressured to overdiagnose gay, mentally ill, and autistic teens and prescribe medications that made their conditions worse.
Still, the U.S. and most European countries embrace a standard of care that pushes youngsters toward “gender-affirming” treatments. It circumvents “watchful waiting” and talk therapy and diagnoses many children as gender dysphoric when they may simply be going through a phase.
Gender-affirming care for children is undoubtedly a flashpoint in America’s culture wars. It is also a human experiment on children and teens, the most vulnerable patients. Ignoring the long-term dangers posed by unrestricted off-label dispensing of powerful puberty blockers and cross-sex hormones, combined with the large overdiagnosis of minors as gender dysphoric, borders on child abuse.
65 notes
·
View notes
Text
sometimes i wish cis people didn’t even know about the term “autogynephilia” because so many transphobes have just accepted the concept whole cloth instead of realizing that it is, first of all, in a sense, outdated, as Blanchard’s transsexualism typology is no longer used by psychological associations and has been rejected by WPATH, but moreover if you look at the critiques of Blanchard’s typology you will see that it was not scientifically rigorous in the first place, and furthermore the classification of a person as an “autogynephile” is an unfalsifiable claim, which isn’t generally supposed to be accepted in other forms of psychological assessment. So, in short… Blanchard’s typology has been generally discarded by the masses of later psychologists and researchers of transsexualism/transgenderism. Why are you picking and choosing this one researcher’s theory over the massive preponderance of subsequent research that conflicts with it? Could it be that you are simply choosing a theory that confirms your existing biases? Furthermore, if you are accepting PART of Blanchard’s flawed typology, why not ALL of it? Blanchard defined “transsexuals” into two categories, the “homosexual transsexual,” (straight, feminine trans women in current terms,) and the “autogynephile transsexual.” In short, the effect of this typology was to grant “homosexual transsexuals” (or any trans women who could fake it) access to medical transition resources while denying it to anyone labeled an “autogynephile.” Yet there are many cis people who use the term “autogynephilia” while advocating for removal of ALL trans women’s (and other AMAB trans people’s) access to medical transition resources! Clearly they do not have an understanding even of Blanchard’s theory and have simply adopted a term out of misguided bigotry. Blanchard’s typology was in the DSM-III-R. It is not present in the DSM-V.
Furthermore, if you are going to latch on to a now-discredited typology invented by one guy from the 1980’s, you could, by the same metric, just as easily latch on to other now-discredited typologies and theories because they “seem more correct” to you than the current scientific consensus. Are you going to believe in the theories of, say, hysteria? Orgone energy? Homosexuality as a mental disorder? The practice of lobotomies?
Enter the 21st century, you goons.
32 notes
·
View notes
Text
Saw someone compare transitioning to like, getting a tattoo or whatever. And while yeah sure its an appropriate comparison in that if you’re not absolutely sure you want it and yet you do it anyway and end up regretting it later it’ll suck massively but like. Transitioning is more comparable to ffucking taking medication to help lessen the symptoms of a disorder everyday. It’s comparable because that’s what it ffucking is. Gender dysphoria, transgenderism, it’s a neurological disorder, not a ffucking mental illness mind you, and it can only be fixed, cured, alleviated, whatever, by transitioning.
And yet people treat being trans like a choice, treat gender like it’s ffucking clothes, and treat dysphoria as a result of society. Those things are transphobic. You can’t choose to be trans, it’s a neurological disorder you’re born with, you can’t choose your gender, it’s part of the structure of your damn brain. And while yes, gender dysphoria can come from outside sources, at it’s core it is the disconnect between the biological sex and the neurological sex.
Ugh. Whatever. Don’t reblog this if you’re going to argue. I don’t wanna hear from TERFs how brain sex isn’t real and gender is made up and all that bullshit.
28 notes
·
View notes
Text
As I was working on the letter to my parents about going no-contact, I tried looking for examples because I was so lost in how to approach it but most of what I found was a bunch of ableist garbage (can we please stop assuming abusive parents have a personality disorder?!)
So now that I've sent the letter and feel pretty good about how it turned out, I thought I'd share it here for anyone else who is thinking of cutting off a parent.
Before writing it, I had decided that I didn't want to address any of the abuse with them. When I've brought it up before they just tried to gaslight me and I don't need to deal with that. Instead I chose to focus on their transphobia as it is also a valid reason for why I want to go no-contact, but it's less vulnerable to address (for me).
To Mom and Dad,
I want to start by saying that I'm not asking you to change your values or beliefs. This is not an attempt to force you to accept me. This is a boundary I need to set because of my own values.
Over the past few years, trans rights have become a major point of political discourse. And lately, Republican attacks on trans people have increased. Over the past few months, this has escalated to calls for the eradication/elimination of "transgenderism" which is a call for the eradication of people like me.
I'm sure you think I'm overreacting or being dramatic, but I have watched this country rapidly become less safe for me and other trans people. And yet you still support politicians who want to eradicate me. Who call people like me groomers and child abusers.
The Republican party is working to enact genocide against trans people. I don’t feel safe with anyone who still supports them, and I’m sorry to say that includes you.
And I can no longer just pretend this isn't happening to try to maintain our relationship. It's been nearly a year and half since I came out. Dad, I don't think I've ever heard you use my name. And Mom, you may use my name sometimes, but you've shown again and again that you will swap back to my old name and pronouns as soon as you think I can't hear. I'm not interested in half-hearted placations as you make it clear how little you respect me.
While you may see this as "just politics", I don't have that luxury. These new laws are targeting people like me. These politicians are calling for my eradication.
Going forward, I do not wish to have any contact. This is not a decision I've made lightly nor quickly. I have spent years and years carefully navigating conversations and having to keep quiet about so much to be able to maintain some form of a relationship with you, but I’m no longer interested in trying to force myself into an acceptable form for you. It may not have been spoken, but I’ve long understood that your love for me has always been conditional. I am a gay trans man. I know you can’t accept that, and I’m not interested in your “love the sinner, not the sin” mentality. This is who I am, not a “sin” that can be separated off and rejected. But, again, I don’t expect or ask you to change your beliefs. I know how strongly you hold your faith. But this is what I need to do to hold to my own values.
I ask that you don't try to contact me. I will not be responding.
22 notes
·
View notes
Note
As a detransitioner, how much do you think gender identity is built by gender stereotypes?
I don’t know. But here is my guess.
TLDR; I think gender stereotypes affect gender identification a lot but it’s complicated and also capitalist concept of self is at play.
Long answer: First of all, I do “believe in gender identity”, as I conceptualize identity as a sense of self based on tangible real life experiences. I’m white. I’m a sister. I’m a gardener. I’m a woman who has been perceived to be a male for a certain time period of her life, but I’m not an actual male. And so on. Many people also identify with the gendered stereotypes that are connected to their sex. People identify with religions that might not be true in an objective sense, but the identities are true – people truly are Christians and such.
So what I think we’re talking about here isn’t gender identity per se but the disconnect between lived experience and the idea that you can feel you’re something you have never experienced. We’re talking about fantasy instead of identity. “I wish I was this-and-that, because my mental image of this-and-that is pleasant and my idea of what I actually am is unpleasant.”
Not all transgender people adhere to stereotypes. What about trans women who just physically transition but never wear heels, make-up or act like stereotypes? They exist, just as there are trans men who are very feminine. Does it mean there aren’t stereotypes involved or are the stereotypes just more subtle? A lot of trans men watch drag and are very into wearing “women’s clothes”, as long as they won’t be perceived as “women” – so they want femininity but without the burden of all things associated with womanhood.
A lot of people with gender dysphoria say it feels entirely physical, like their bodies just don’t match the mental map they have of their body. Their bodies feel foreign to them; they are repulsed by their bodies even when they are alone.
Could it be they have developed these physical feelings as a reaction to the social discomfort they feel about being associated with certain gendered stereotypes?
Human psyche is very capable of developing symptoms that feel entirely physical. There are people who identify as “therians”, non-human animals. They have phantom limb feelings of tails and ears they think they should have. If transitioning into a non-human animal would be possible, would these people be miserable unless they were granted the access to have the tail they always knew is part of their body?
And then there are conversion disorders. They aren’t analogous to transgenderism but they do highlight the power human psyche has when in distress. Conversion disorders were more common when people didn’t have the cultural vocabulary to describe their mental anguish. Instead, people became blind or deaf or paralyzed or had seizures, fully experiencing these things as true, but having no physical deficit that would cause the problem. That’s how powerful the human psyche is.
I wonder if we have the cultural vocabulary to describe the anguish sexism and patriarchy causes us? Or are we like a soldier who will become physically paralyzed instead of saying: I'm scared and I don't want to hurt anyone.
In addition, culture affects the mental disorders humans experience. Certain psychological phenomena are only present in certain cultural context where the symptoms make sense individually and on a collective level. I'm fairly certain gender dysphoria is like this. Many cultures recognize people who cross gendered boundaries and inhabit the social role of the opposite gender, both genders or either, but I don't know whether these experiences include any kind of distress over one's physical body or whether these roles resemble more something like butch lesbians or feminine gay men.
As far as I know, there isn’t any coherent theory explaining gender dysphoria as something universal and inherent. To me it looks like this: A person strongly believes or wants something (I’m a man). It is incongruent with the body the person has (a female body) and with how others treat that person (societal role of a woman with all the stereotypes attached). This disconnect between the want and the reality causes distress. Just like the disconnect between “I feel I should be beautiful” and the reality of “I’m not conventionally attractive” will cause distress, ruminating, excessive time in front of the mirror, plastic surgery. The distress isn’t caused the physical body itself (being unattractive or being a female) but the cultural connotations attached to this physical reality – like people thinking you’re stupid, or that you need to defer to men.
Personally my transition was very much affected not only gender stereotypes, but what these stereotypes caused: misogyny, lack of representation of women as complex humans, sexual harassment. One huge factor was that transition existed and I was able to find information on the subject, so my fantasy self became a potential real self, and so, in a way, it became reality at some point. If the means to transition didn’t exist, I doubt my dysphoria would have been too deep. After all, I’ve despaired over other things as a young teenager: I wished I could be tall, I wished I could be Japanese, and so on and so on. Alas, “racial transition” does not exist and becoming tall isn’t very viable either, so I grew out of these thoughts and learned to understand I’m actually a human being instead of a character I should and could design to be as cool as possible.
The current capitalist culture teaches us our bodies are changeable, and in fact, changing or enhancing one’s body is almost a duty. Existing just as you are is neglect. You’re expected to self-fulfill by changing your body. You are expected to design yourself like you are a character.
To be honest, sexism and homophobia in this society is so deep, I have empathy towards people who will solve their distress by transition. It's a very individualistic solution, solving nothing at the larger scale. But as much as I wished every woman would ditch make-up and heels and have self-respect, they won’t, either. And so some women transition into men, some women defer to men. There is still much to do.
In conclusion, I think to develop incongruence of gender identity, we need strict stereotypical gender roles, but in addition, it is driven by an individualistic culture of “self-development” and the cultural gaze being turned inwards, everything revolving around one’s one self and self-actualization. What is also needed is the idea of being able to change your sex, or changing the meaning of sex altogether. We rarely despair over something that isn't realistically possible.
16 notes
·
View notes
Text
Saw I got a like on one of my fics from a blog I don't recognise, checked their blog and the only thing there is a post about how "Transgenderism is a mental disorder and these sick people should be treated".
Anyway, this followed by a block is the only discussion I have with scum.
And no I'm not gonna hide these people's usernames, they deserve whatever consequences they get.
This is not a safe space for bigots and if you can't say the same I'm judging you for it.
7 notes
·
View notes
Text
Every transmasc is now in more danger than ever before.
They already see us as overly aggressive and violent. Now think about those of us that have mental illness. And I'm not just talking about mild depression or anxiety. I'm talking about the ugly shit. Personality disorders. Suicidality. Psychosis. Intrusive thoughts. YES, EVEN THOSE INTRUSIVE THOUGHTS.
Or on the flipside, maybe those of us seen as "deviant." I know a ton of transmascs into horror and all sorts of creepy shit (I say this affectionately; there's something about being trans/queer and finding yourself in the macabre).
Because guess what? All of this shit can be used against us. Cultural purists, Evangelical lawmakers, fucking Karens who don't want their children around our "deranged" selves, etc are just chomping at the bit looking for reasons to hate and oppress us. Shit, some of them are looking for ways to kill us. All to protect their fragile moral complexes.
And they'll do it. They already do it. They're ramping up to "eradicate transgenderism from public life" on a legislative scale.
We're so fucked. We're so fucking fucked.
#i'm... somewhat calm i swear#just processing#but also like? this sucks. this really sucks. i don't want to be the guy that cries 'doomsday' but this kind of fucking feels like it#anyways this is okay to rb just. don't be a clown please#shit i even feel worried about my ex#because. fuckin. idk. it's just complicated. whatever#anyways.
16 notes
·
View notes
Text
By: Gerald Posner
Published: Jun 7, 2023
The fashion for transgenderism has brought with it a new euphemism: “gender-affirming care,” which means surgical and pharmacological interventions designed to make the body look and feel more like that of the opposite sex. Gender-affirming care for children involves the use of “puberty blockers”: one of five powerful synthetic drugs that block the natural production of sex hormones.
The Food and Drug Administration has approved those medications to treat prostate cancer, endometriosis, certain types of infertility and a rare childhood disease caused by a genetic mutation. But it has never approved them for gender dysphoria, the clinical term for the belief that one’s body is the wrong sex.
Thus the drugs, led by AbbVie’s Lupron, are prescribed to minors “off label.” (They are also used off-label for chemical castration of repeat sex offenders.) Off-label dispensing is legal; some half of all prescriptions in the U.S. are for off-label uses. But off-label use circumvents the FDA’s authority to examine drug safety and efficacy, especially when the patients are children. Some U.S. states have eliminated the need for parental consent for teens as young as 15 to start puberty blockers.
Proponents of puberty blockers contend there is little downside. The Department of Health and Human Services claims puberty blockers are “reversible.” It omits the evidence that “by impeding the usual process of sexual orientation and gender identity development,” these drugs “effectively ‘lock in’ children and young people to a treatment pathway,” according to a report by Britain’s National Health Service, which cites studies finding that 96% to 98% of minors prescribed puberty blockers proceed to cross-sex hormones.
Gender advocates also falsely contend that puberty blockers for children and teens have been “used safely since the late 1980s,” as a recent Scientific American article put it. That ignores substantial evidence of harmful long-term side effects.
The Center for Investigative Reporting revealed in 2017 that the FDA had received more than 10,000 adverse event reports from women who were given Lupron off-label as children to help them grow taller. They reported thinning and brittle bones, teeth that shed enamel or cracked, degenerative spinal disks, painful joints, radical mood swings, seizures, migraines and suicidal thoughts. Some developed fibromyalgia. There were reports of fertility problems and cognitive issues.
The FDA in 2016 ordered AbbVie to add a warning that children on Lupron might develop new or intensified psychiatric problems. Transgender children are at least three times as likely as the general population to have anxiety, depression and neurodevelopmental disorders. Last year, the FDA added another warning for children about the risk of brain swelling and vision loss.
The lack of research demonstrating that benefits outweigh the risks has resulted in some noteworthy pushback in the U.S. and abroad. Republican legislatures in a dozen states have curtailed or banned gender-affirming care for minors. Finland, citing concerns about side effects, in 2020 cut back puberty blockers and cross-sex hormones to minors. Sweden followed suit in 2022 and Norway this year. Britain’s National Health Service shuttered the country’s largest youth gender clinic after 35 clinicians resigned over three years, complaining they were pressured to overdiagnose gay, mentally ill, and autistic teens and prescribe medications that made their conditions worse.
Still, the U.S. and most European countries embrace a standard of care that pushes youngsters toward “gender-affirming” treatments. It circumvents “watchful waiting” and talk therapy and diagnoses many children as gender dysphoric when they may simply be going through a phase.
Gender-affirming care for children is undoubtedly a flashpoint in America’s culture wars. It is also a human experiment on children and teens, the most vulnerable patients. Ignoring the long-term dangers posed by unrestricted off-label dispensing of powerful puberty blockers and cross-sex hormones, combined with the large overdiagnosis of minors as gender dysphoric, borders on child abuse.
==
Gender thalidomide.
#cosmetic surgery#thalidomide#gender thalidomide#puberty blockers#gender affirming#gender affirming care#cross sex hormones#wrong sex hormones#gay conversion therapy#gay conversion#medical malpractice#medical scandal#medical transition#religion is a mental illness
7 notes
·
View notes
Last Seen Blogs


noirtopia
Noirtopia

clrconline
Classical Learning Resource Center

natyaranjani-blog
Dance is me

oliviathinksoliviasthings
oliviathinksoliviasthings