#recover study
Text
Postacute sequelae of COVID-19 (PASC), often referred to as Long COVID, has had a substantial and growing impact on the global population. Recent prevalence studies from the United States and the United Kingdom found that the complication has affected, on average, around 45 percent of survivors, regardless of hospitalization status.
No accurate tally of the number of people affected and its real global impact has yet been made, but conservative estimates of several hundred million and trillions in economic devastation would hardly be an exaggeration. Even in China, after the lifting of the Zero COVID policy late last fall and the tsunami of infections that followed, social media threads are now widespread with people complaining of chronic debilitating fatigue, heart palpitations and brain fog.
Yet, more than three years into the “forever” COVID pandemic, with Long COVID producing more than 200 symptoms, impacting nearly every organ system and causing such vast health problems for a significant population across the globe, it remains undefined and somewhat arbitrary in the clinical diagnosis. Additionally, the assurances given to study potential therapeutic agents have remained unfulfilled.
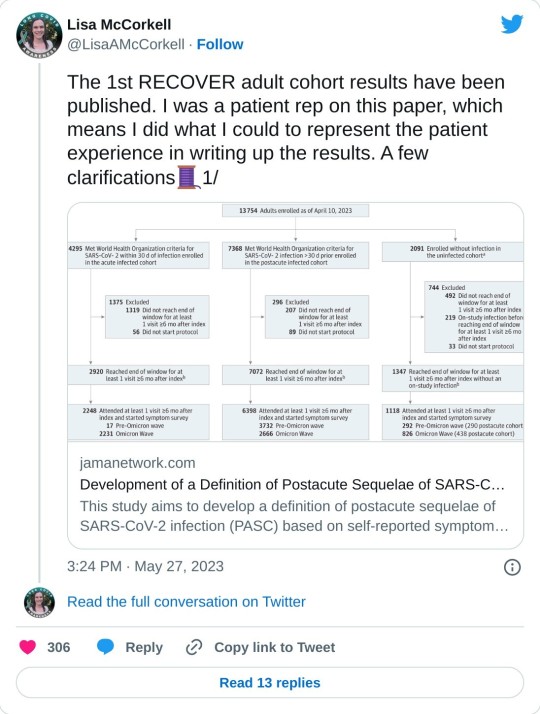
In this regard, a new Long COVID observational study called the “RECOVER [researching COVID to enhance recovery] initiative,” was published last week in the Journal of the American Medical Association, with almost 10,000 participants across the US. Funded by the National Institutes of Health (NIH), it attempts to provide a working definition for Long COVID (PASC).
While the study represents an advance from the standpoint of assessing the impact of Long COVID, and has been celebrated in media coverage, it must be viewed with several reservations and caveats. It is exclusively focused on describing the disease, rather than supporting efforts to alleviate its impact, let alone find a cure. And its definition, however preliminary, could well be misused by insurance companies and other profit-driven entities in the healthcare system to restrict diagnosis and care.
Comments by Dr. Leora Horwitz, one of the study authors and director of the Center for Healthcare Innovation and Delivery Science at New York University, give some sense of the misgivings felt by serious scientists. Horwitz stated, “This study is an important step toward defining Long COVID beyond any one individual symptom. This definition—which may evolve over time—will serve as a critical foundation for scientific discovery and treatment design.”
Certainly, a working definition that medical communities can agree on is critical. But after three years and nearly all the $1.2 billion given to the NIH already spent, one must ask how much another observational study contributes to answering pressing questions affecting patients that have not already been addressed in more than 13,000 previous reports, as tallied by the LitCOVID search engine?
Why have there been so many delays in conducting clinical trials studying potential treatments and preventative strategies in the acute phase of infection that could reduce or eliminate the post-acute sequelae? Where is the urgency at the NIH and in the Biden administration to expand funding and initiate an all-out drive to develop treatments for Long COVID like the $12.4 billion spent on the COVID vaccines?
Scoring post-acute symptoms
The findings in the recent study, published on May 25, 2023, in JAMA, titled, “Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection,” are somewhat limited and problematic in their current formulation. The authors have identified 12 primary symptoms that distinguish COVID survivors with Long COVID from those without those aftereffects. These include loss of smell or taste (8 points), post-exertional malaise (7 points), chronic cough (4 points), brain fog (3 points), thirst, (3 points), heart palpitations (2 points), chest pain (2 points), fatigue (1 point), dizziness (1 point), gastrointestinal symptoms (1 point), issues with sexual desire or capacity (1 point), and abnormal movements (1 point).
Assigning points to each of the 12 symptoms and adding them up gives a cumulative total for each patient. Anyone scoring 12 or higher would be diagnosed as afflicted with PASC, accounting for 23 percent of the total. In general, the higher the score, the greater the disability in performing daily activities.
The researchers also noted that certain symptom combinations occurred at higher rates in certain groups, leading to identifying four clusters of Long COVID based on symptomology patterns, ranging from least severe to most severe in terms of impact on quality of life. Why such clusters were seen remains uncertain.
Some symptoms were more common than others, and this did not correspond to the severity of the symptoms as measured approximately by the points. Symptoms of post-exertional malaise (87 percent), brain fog (64 percent), palpitations (57 percent), fatigue (85 percent), dizziness (62 percent), and gastrointestinal disturbances (59 percent) were most common.
The study’s lead author, Tanayott Thaweethai from Massachusetts General Hospital and Harvard Medical School, explained, “This offers a unifying framework for thinking about Long COVID, and it gives us a quantitative score we can use to understand whether people get better or worse over time.”
Andrea Foulkes, the corresponding author and principal investigator of the RECOVER Data Resource Core and professor at Harvard Medical School, said, “Now that we’re able to identify people with Long COVID, we can begin doing more in-depth studies to understand the mechanisms at play. These findings set the stage for identifying effective treatment strategies for people with Long COVID—understanding the biological underpinnings is going to be critical to that endeavor.”
The currently evolving definition could have significant implications, and not just medically. For instance, if people suffer only brain fog and post-exertional malaise and score less than 12 on their symptomology, they would not be construed as having PASC. Under such a construct, the definition could be used by employers and health insurers to deny compensation or treatment by telling people they don’t have a recognized Long COVID complication. Additionally, it is not clear how long these symptoms have to be present before the diagnosis is accepted.
Lisa McCorkell, one of the authors of the study, explained on her social media account, “If people didn’t meet the scoring threshold for PASC+, that doesn’t mean they don’t have PASC! It means they are unspecified. Unspecified includes people with Long COVID. Future iterations of the model will aim to refine this—that will include doing analysis using the updated RECOVER symptoms survey, adding in tests/clinical features and ultimately biomarkers. That is also why this isn’t meant to be an official prevalence study. The sample is not fully representative, but also, we know that there are people in the unspecified groups that have PASC.”
She continued, “It is very clear throughout the paper that in order for this to be actionable at all, iterative refinement is needed. In presenting this to NIH leadership, they are fully aware of that. But the press is not fully understanding the paper which could have dangerous downstream effects. Since the beginning of working on this paper I’ve done everything I could to ensure the model presented in this paper is not used clinically.”
Unfortunately, in the world of capitalism, such things take on a life of their own. The definitions will influence how health systems will choose to view these patients and demand their clinicians abide by prescribed diagnostic codes. This has the potential to dismiss millions with Long COVID symptoms and deny them access to potential treatments if and when they materialize.
The concerns of Elisa Perego
Dr. Elisa Perego, who suffers from Long COVID and coined the term, offered the following important observations.
In response to the publication, she wrote, “Presenting a salad of 12 symptoms, (many of which many patients might not even experience) as the most significant in #LongCOVID is also detrimental to new patients, who might be joining the community now, and might not recognize themselves in the symptom list.”
She added, “We are also in 2023. There are thousands and thousands of publications from across the world that discuss imaging, tests, clinical signs (=objective measurements), biomarkers, etc. related to acute and #LongCOVID. We have many insights into the pathophysiology already. The #LongCOVID and chronic illness community deserve more. Other diseases, including diseases linked to infections, have sadly been reduced to a checklist of symptoms in the past. This has made research, recognition, and a quest for treatment much more difficult.”
There are additional findings in the report worth underscoring as they provide a glimpse into the ever-growing crisis caused by forcing the world’s population to “live with the virus.”
Hannah Davis, a Long COVID advocate and researcher, with Dr. Eric Topol, Lisa McCorkell, and Julia Moore Vogel, wrote an important review on Long COVID in March, which was published in Nature. She said of the RECOVER study, “The overall prevalence of #LongCOVID is ten percent at six months. The prevalence for those who got Omicron (or later) AND were vaccinated is also ten percent … [However] reinfections had significantly higher levels of #LongCOVID. Even in those who had Omicron (or later) as their first infection, 9.7 percent with those infected once, but 20 percent of those who were reinfected had Long COVID at six months after infection.”
Furthermore, she said, “Reinfections also increased the severity of #LongCOVID. Twenty-seven percent of first infections were in cluster four (worst) versus 31 percent of reinfections.” These facts have considerable implications.
Immunologist and COVID advocate Dr. Anthony Leonardi wrote on these findings, “If Omicron reinfections average six months [based on current global patterns of infection], and Long COVID rates for reinfection remain 10 to 20 percent, the rate of long COVID in the USA per lifetime will be over 99.9 percent. In fact, the average person would have different manifestations of Long COVID at different times many times over. Some things reverse—like anosmia [loss of smell]. Others, like [lung] fibrosis don’t reverse so well.”
The work done by these authors deserves credit and support. Every effort to bring answers to these critical questions is vital. The criticism to be made is not directed at the researchers who work diligently putting in overtime to see the research is conducted with the utmost care and obligation it merits. Rather, it should be directed at the very institutions that have adopted “living with the virus” as a positive good for of public health.
The Biden administration neglects Long COVID
In a recent scathing critique of the Biden administration and the NIH by STAT News, Rachel Cohrs and Betsy Ladyzhets place the issue front and center. In their opening remarks, they write, “The federal government has burned through more than $1 billion to study Long COVID, an effort to help the millions of Americans who experience brain fog, fatigue, and other symptoms after recovering from a coronavirus infection. There’s basically nothing to show for it.”
They continue, “The NIH hasn’t signed up a single patient to test any potential treatments—despite a clear mandate from Congress to study them. And the few trials it is planning have already drawn a firestorm of criticism, especially one intervention that experts and advocates say may actually make some patients’ Long COVID symptoms worse.” This is in reference to a planned study where Long COVID patients would be asked to exercise as much as possible, when it has clearly been shown that such activities have exacerbated the symptoms of Long COVID patients.
As the report in STAT News explains, there has been a complete lack of accountability in how the NIH funds were used. Much of the work to run the RECOVER trial has been outsourced to major universities.
Michael Sieverts, a member of the Long COVID Patient-led Research Collaborative with expertise in federal budgeting for scientific research, told STAT, “Many of the research projects associated with RECOVER have been funded through these organizations rather than directly from the NIH. This process makes it hard to track how decisions are made or how money is spent through public databases.”
In April the Biden administration announced they were launching “Project Next Gen,” which is like the Trump-era COVID vaccine “Warp Speed Operation.” It has promised $5 billion to fund the development of the next iteration of vaccines through partnership with private-sector companies, monies freed up from prior coronavirus aid packages. Incredibly, it has left Long COVID out of the plan.
Indeed, this diverting of money back into the hands of the pharmaceuticals and selling it as the Biden administration’s continued proactive response to the ongoing pandemic, while divesting all interest in preventing or curing Long COVID, is on par with every effort the administration has made to peddle the myth that “the pandemic is really over.” Long COVID is one of the central elements of the worst public health threat in a century, in a pandemic that is far from ended.
2 notes
·
View notes
Text

He's such a good boy :>
#my art#bnha#dabihawks#dabi#hawks#i did some anatomy and pose study with this one#and tried really hard for the first time in AGES#ive been in such a burn out this helped recover some of my confidence#im really happy#amazing what using references can do!!! who would have thought!!!
2K notes
·
View notes
Text








Tuesday is chuu day! (x)

#more haniwa redraws because i am Sick and Twisted#duck scribbles#i might as well remake the entire mv atp but no editor </3#i wanted to put a part of the lyrics in the caption but they all give me secondhand embarrassment im sorry#actually drawing this in general also did. i think ill need a while to recover#enstars#midoyuzu#yuzumido#midori takamine#yuzuru fushimi#ensemble stars#tori voice if youre gonna flirt in here at least lock the door#ignore the fact its still monday its tuesday somewhere else in the world#anyways have you seen the new profiles. they did that for me specifically i think im never getting over it#hes studying painting..... im so proud of her...........#also read the fuyume midori story its rly cute :'] disaster mentor and little brat princess#regardless. back to finals hell i go </3
415 notes
·
View notes
Text
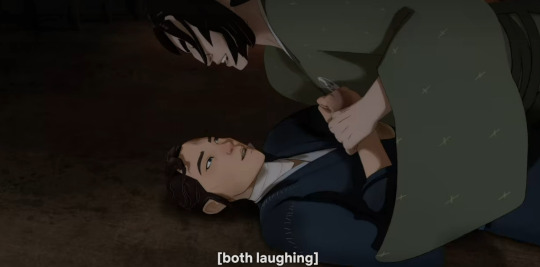
yall i just KEEP doing back to mizu and taigen's wrestling scene in master eiji's forge and like i know that taigen literally got a boner from it BUT THE THING IS out of all the scenes these two have together, this scene actually has the least sexual tension ?!? cuz like the boner aside, this scene is actually very soft and emotions-driven rather than pure passion or lust.
arguably, a more passionate and sexually-charged scene would be their previous brawl in the snow with the chopsticks, which is tense and angry and also the scene that mizu thinks about when madame kaji talks about being honest with one's innermost desires.


but THIS scene in the forge? warm colours. their laughter and their smiles that both equally genuine. the WAY taigen looks at mizu in that scene, staring first at her lips, her smile, then looking into her eyes. and you can see by the framing of the scene and the look on his face that he is, for the first time, seeing her eyes as something beautiful rather than off-putting or frightening.



like before this point he's already come to not only respect mizu as a person and an equal but also admires her as an incredible swordsman and as someone who is kind and honourable* for having saved his life at the expense of her revenge quest. so as of the time of them tussling in the forge, taigen has already put aside his prejudices about mizu's blue eyes and no longer finds them as any cause for disgust. but in this scene he's not just indifferent about her eyes, but attracted too it.
and i'd also like to argue that his boner is not from the physical exertion or the act of wrestling itself, but from the intimacy of a playful spar, enjoying each other's easy company after having established a deep trust with each other (taigen endured torture for mizu and helped defend her from archers in the chasm while mizu saved his life from fowler's castle)

and all this while in the safety of mizu's childhood home while both of them are still recovering from near-death, amplifying their vulnerability with each other.




like when was the last time mizu cracked a genuine smile, let alone a laugh that's more than a little wry chuckle?? and for this to happen at such a low point in her life also speaks to the comfort this little friendly spar gives her.
because like, this is after she failed her mission to kill fowler. meanwhile her sword--the embodiment of her soul--is broken, and ringo who is her closest confidant is now angry at her and barely even looks at her. it just further lends to the inherent tenderness and intimacy in this scene. and i just. AHHHH i love them your honour....

* ALSO as a side note about taigen believing mizu to be honourable: he later realises that this assumption turns out to be quite false when she reveals that she'd not only allowed akemi to be taken away against her will but also has said nothing about fowler's impending attack on edo.
also i find it very interesting that out of the two revelations, taigen is less angered by mizu letting akemi being married off (he sighs angrily and marches off saying he has to go to edo to find akemi), but much more angered by mizu's refusal to save the shogun and the shogunate as a whole.
this is more proof that taigen's central principles are firmly rooted in the bushido and the concept of honour that comes with that. it's why he lashes out at mizu. because he'd believed mizu to be honourable and righteous, but was proven wrong. that's not to say that taigen is in the right for calling mizu a demon, not by any means. but i just find it a very interesting part of his character and it relates to his relationship and perception of mizu
also while rewatching the episode i found this very funny they just lyin there in the cart like this 🧍🏽♂️🧍🏽♂️

#blue eye samurai#mizu x taigen#taimizu#taizu#taigen blue eye samurai#mizu blue eye samurai#blue eye samurai meta#sorry yall but i prefer taimizu as the ship name so i'll probably just be using that from now on 🫡#also like.. the way im still recovering from covid while i have 2 deadlines back to back tomorrow and the day after#but im too busy hyperfixating on this show!!!!#if only i could channel all this energy into my actual literary studies papers that'd be great#but at the moment i be caring more about these fuckers than whatever william blake's got going on#jk i do still love william blake's poetry but my stupid ships take up way more space in my brain ykwim 🤒#anyway...#shut up haydar#meta dissertations.pdf#fandom.rtf
734 notes
·
View notes
Text

Loving you makes broken men whole so that even as you deny us, our heartache is not in vain.
based on couple art by Leyendecker
detail

#rogneto#rogueneto#xmen 97#anna marie#erik lehnsherr#magneto x rogue#rogue x magneto#xmen 97 fanart#i still haven't recovered from that episode#i don't think i ever will T-T#i've watched that dance scene so many times#studied it frame by frame#need it burned on my brain. it's a masterpiece#leyendecker style#rogue#magneto
124 notes
·
View notes
Text
imagining jeonghan as your roommate and you're just friends. REALLY you're just friends.
friends who started going out on dates as a joke because you were both bored. friends who always call each other every night when one of you is out of town because you missed the sound of their voice. friends who sleep in each other's beds until you don't know what it feels like to be alone anymore.
jeonghan's just your friend — really, he is! so even if your heart aches with lovesickness every time he flashes you a lazy smile, you take it in stride. because jeonghan is a nice friend. a wonderful friend. you wouldn't trade what you have with him for anything else.
even for the paper thin chance that he might just be as lovesick as you are.
someone asks, "are you guys dating?" one day when you're all hanging out with a bigger circle and before you can deny the allegations, jeonghan intercepts with a calm and confident, "yes."
you think about it the entire drive home because... you're just friends, right? friends who go on dates but aren't dating. friends who love each other but aren't in love.
oh wait. that only makes one of you.
"what do you mean we're dating?" you dare to ask jeonghan once he pulls over at a red light — a frown contorting your features. "we're just friends, aren't we?"
jeonghan hums as his fingers drum across the steering wheel. "hn? we've been on at least twelve platonic dates. that counts as dating, right?"
"...when does it become not platonic then?"
he doesn't answer right away, slanted eyes glued to the traffic lights counting down until they glow green again. you don't make it a habit to figure out what goes on in jeonghan's head. you've never once won that game and you've always been a sore loser.
but right after he steps on the gas pedal to zoom past the empty streets again, jeonghan — your roommate, your confidant, your friend — smiles at you with tenderness in his eyes that's familiar and foreign both at the same time.
"how about date number thirteen?" he asks before making a sharp right that's definitely not en-route to your shared apartment. "the carnival by the pier closes at three a.m. and i know that parlor game stuffies are the key to your heart."
you stare at him for a beat longer — wondering if there's a catch. a punchline to some joke you're not quite getting.
but you've been friends with jeonghan for so long that you're well-aware that the only way you can figure him out is to not figure him out at all.
"okay," you respond coolly, trying to keep your heart from bursting when you place your hand on top of jeonghan's from where he firmly grips the gear shift. "you better make up for not buying me one of those ikea sharks."
jeonghan snorts. "hey! blåhaj is out of our budget!"
jeonghan's a good friend. the best friend you could ask for, really. but the morning after he takes you to the midnight carnival, you're glad to know he's an even better boyfriend.
#svthub#i have a chronic problem of writing fic ideas whenever i need to study#this is sfw btw#also shoutout to indi for feeding me so much jeonghan brainworms with a single tiktok#im never recovering from this actually#seventeen x reader#jeonghan x reader#🌸 soft thoughts#lovelyhan#seventeen fanfic#jeonghan fanfic
362 notes
·
View notes
Text
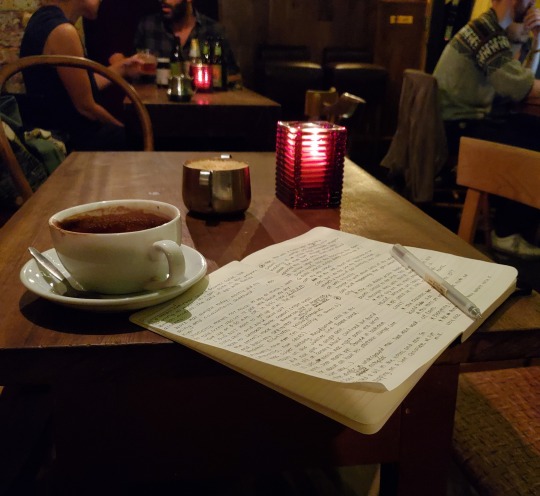

travel tales: london, uk
#omg i finally got all my old photos and videos recovered from the past 7 years so i'm going to start uploading older stuff#this was from my work trip to london a few years ago when i just graduated from college..#mine#studyblr#tea-tuesday#study inspiration#studyspo#lawblr#study#studying#study motivation#cafe#bar#journal#london#england#cozy academia#cozy#travel tales
235 notes
·
View notes
Text
fellas you ever consider that vertin can never have it all?? ever?? or even just like a little bit at all?? (chapter 1 + 2 + 3 spoilers)
like bro schnedier. schneider kisses her and then fuckin DIES. bro. one girlfriend off the books. she has to fucking go through therapy and that shit still haunts her dreams. oh lord.
and on top of that. there is so much unclosed shit between her and sonetto. do you guys remember that poem in chapter 3 about sonetto being the 'puppy' and how she cried when the stone wall shut between her and vertin??
yeah bro that shit haunts me. and how she?? she CRIED in the car when vertin was in danger?? shes so down. down horrendous. sonetto my baby
and if THAT isnt bad enough. lets say sonetto and vertin sort their shit out. italian cheek kiss or whatever. lets say schneider comes back to life. SONETTO ISNT OKAY WITH THAT. she was visibly and verbally jealous when schneider got close to vertin. even if vertin got her dead mf girlfriend back sonetto would either be hurt, disapproving, or both.
okay let's say everything is fine. let's say schneider is alive and vertin is ay-okay and sonetto is emotionally stable. WHAT ABOUT MATILDA?? she is not going to be okay either.
get me the FUCK OUT OF THE YURI SQUARE
Let me OUTUTTTT
#vertin x schneider#verneider#vertin#schneider#reverse 1999#re1999#r1999#matilda bouanich#sonetto reverse 1999#god matilda is so pathetic (affectionate)#i deeply sympathize with her#sonetto please give her a little kiss. maybe just to be nice#smooch. little kissy kissy#endgame if ANY of my other girls die i WILL eat five crumbl cookies and cry on the floor#'luisa you need to study for finals' i need to recover from chapter 2 thats what i need#mentally eel
150 notes
·
View notes
Text
Done is Better than Perfect ✅



I never considered myself a perfectionist until I started coding. I'd obsess over pixels and be frustrated when my vision didn't align with what was within my ability to create. And I started to hear this phrase a lot:
"Done is better than perfect."
Of course, some things will always require precision, but one thing I'm slowly learning as I transition from university student to working professional (and back and forth between those two) is that for most things we do in life, there is a wide range for success.
The coolest people I know aren't the ones with the most money, fame, beauty, intelligence, or any other positive quality. Even if it's a mess and inelegant and nobody seems to care, they're the ones who show up everyday and keep doing.
Today was a success because it was done, not because it was perfect. 💚
#studyblr#student life#study motivation#psychology student#study inspiration#workblr#software engineering#coding#codeblr#comp sci#progblr#programming#zesty's life#perfectionism#recovering perfectionist#perfectionist issues#studyspo#light acadamia aesthetic#light academia#chaotic academia#astudentslifebuoy#university#psychblr#study tips#productivity#productivity hacks#100 days of productivity#productivity tips#done is better than perfect#aesthetic
258 notes
·
View notes
Text

inspired by the tweet under the cut and whoever came up with the jance nerd x bad boy au here !!! (srry it's 3 am too tired to check)

#SORRRYYY my physical incapibility to draw a jan continues ....#joker out#jan peteh#nace jordan#jance#my art#vee vkv! you ask. i thought you had exams! are you already done? why are you up at three am!#wow! i answer. you remembered! i still have exams. in fact i will be having 4 in a row mon-thurs! i have barely studied! instead i am up#at ungodly hours drawing jo fanart. i will actually have to study tomorrow </3 gonna jump off a cliff#AND IM SICK . so me and kris are kinda twinning rn hehehehahaha#no but seriously im also not allowed to take any sick days off cuz exams#so i should really be in bed rn resting and recovering! gn#this isnt even GOOD what am i doing w my life :sob:
119 notes
·
View notes
Text
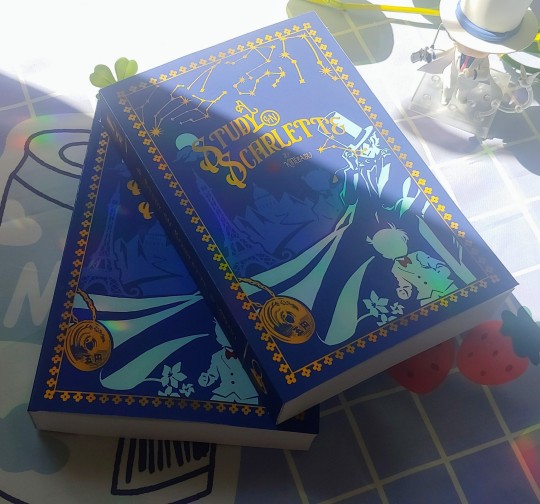


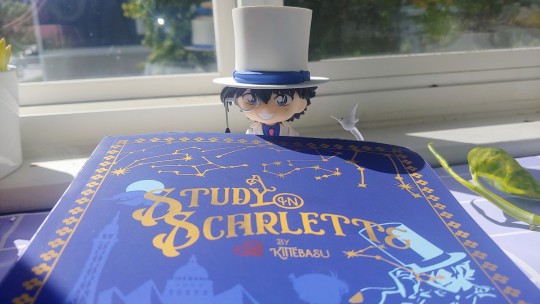

After over a year of procrastinating and getting distracted with life, my sister and I have finally finished our passion project of making our favorite fanfic into a book! It's over 500 pages of mystery, murder, and romance and I'm so happy to have it in my hands.
(Not for sale or anything I'm just very excited to share)
If you haven't read and would like to, here's a link to Kittebasu's fic here!
#art#detective conan#magic kaito#kaito kid#a study in scarlette#fanfic rec#photos#dcmk#fanart#pls pls go read it if you haven't already#it ruined my tastebuds for other fanfics like 4 years ago and I've yet to recover#this is mostly made of free clip art and manga caps that Ive mashed together to be aesthetically pleasing#kaishin
2K notes
·
View notes
Text

They never leave, do they?
#vnc#vanitas no carte#the case study of vanitas#astolfo granatum#the drawing is based on my own experience with recovering from SA and emotional abuse#but please interpret it however you want!#me? projecting my issues onto the characters i like? wow! /sarcastic#not my best drawing but weirdly comforting to draw!#tw sa#(just in case)#my art
127 notes
·
View notes
Note
I love your art! Your style is lovely. :D Hmm, how about Fingon for the modern fashion studies? I bet he'd look fabulous in anything, but I'm curious to see what you think he'd wear!



Thank you for the request!! Here's modern Fingon, the cute dork, :D
🥰
#Fingon#The Silmarillion#Silmarillion#Silm fanart#Tolkien#Tolkien fanart#Modern tolkien#Modern lotr#Modern silmarillion#Lotr#Lord of the Rings#My art#I had a lot of fun with this i should paint semi realism more often :D#Also! I'm recovering well from my surgery :) Thanks to everyone who sent me well wishes!#Might do more of the modern fashion studies in this style 🤔
170 notes
·
View notes
Photo








I sit at the back of the class. I let the nerds sit in the front.
Gemini Norawit as TINN & Fourth Nattawat as GUN
MY SCHOOL PRESIDENT (2022) dir. Au Kornprom Niyomsil
#my school president#my school president the series#tinngun#guntinn#userjaehwany#samblr#usertaeminie#userjjessi#usermor#mjtag#geminifourth#gemini norawit#fourth nattawat#marigif#wish i could gif more but i need to leave and go study#more gifs coming later tho eheheh#this was such good ep i will never recover smh
1K notes
·
View notes
Text







Weeks have passed by and Vincent has been making a healthy recovery. Renee often spends her time with him and she was glad to see him be his usual self. Today he was quiet. Renee hasn't asked about his heart condition but he opened up about his insecurities. He stood up, took off his shirt, and looked at his chest. "Every time I see this scar I get so...I feel all these things and I remember..." Vincent sighed unable to process his words. "It hurts Renee. My heart hurts so much." Renee knew she couldn't do anything to make that scar go away, but she could make him feel better about himself and gradually he would accept who he was. "You're perfect just the way you are," she explained as she gazed into his eyes.
#ts4#sims 4#ts4 gameplay#ts4 legacy#postcard legacy#postcard gen 3#renee reichmann#vincent kingsley#hes recovered from his operation now! he changed his phone but he still doesnt know anything about the gps tracking with keys#the operation made him better but hes insecure about that scar#its making him feel all this stuff and remembering some things#renee is studying criminolgy now#oh to have a partner like renee#shes the best 💕 she loves him so much!#AAAND OMG I CANT#ahhhhh im so fucking shy!!!!#i cant do these intimate posts ahhhh#now if no one sees this post then tumblr has hidden it lets see then...
90 notes
·
View notes
Text

My version of @cambriancutie's Dtiys!!! (hope I'm not too late)
#my really bad habit of starting drawings for events 2 days before#to be fair I was sick and when I recovered I was doing art studies and you can see they paid off here SO I am justified (probably)#🦇// my art#splatoon#ditys#also new signature how we feeling? (current one is still in the corner)
83 notes
·
View notes
Last Seen Blogs

posstube
Posstube#

dailyjaeyong
jaeyong ;; aesthetics, themes

pahua
mexicola

c9hpbhucu
Untitled

sheetdream
sheets