#you should always research ANY drug you take. prescription or not. find out about addictiveness + side effects + other drug interactions
Text
people acting like there isn't still very much an active stigma against cannibas and cannibas users is going to be my joker origin story
when i go to the doctor they still put cannibas use under the tab "substance abuse". not even just substance use. it is fully assumed that people who use cannabis, even as a prescription medication, are abusing it. just because you're friends with a couple of dumbass stoners doesn't mean that we've abandoned the idea as a culture that weed is a bad and scary and dangerous and highly addictive drug that will ruin your life if you use it once
#idk what its like in other countries but in the us and especially in red states fear mongering about weed is alive and well#'it ruins lives' -direct quote from a library board member making it so we can be fired for testing positive even w a prescription#i just take umbrage with posts about addiction that go out of their way to mention weed which we all learned in 6th grade is addictive#but dont also mention that this true of all prescription drugs and that a person can be dependant on a drug for health reasons???#yeah i get anxious and cant go a day without weed. because i use it to treat my anxiety and pain. i also get anxious without my wellbutrin#but people arent lining up to make posts about it?? and like you CAN obviously become addicted to prescription drugs its super common!#so i kind of feel like it would be far more useful to say 'this is true of ALL drugs. including weed caffeine and prescriptions'#you should always research ANY drug you take. prescription or not. find out about addictiveness + side effects + other drug interactions#and you should talk to someone if you feel anxious about your relationship to drugs. prescription or not#there have been many times where i was prescribed way too many drugs at once and it made me feel anxious and uncomfortable#so i talked to my doctors and consolidated several and it actually made them work a lot better#locked reblogs because i KNOW people are going to read this is 'so you should never ever talk about negative consequences of weed'#and im pretty sure the people who follow me will be able to understand thats obviously not what im saying#but as soon as it leaves my blog whos to say. but anyway like. I think we should talk more about addiction to all substances#and not just the ones that were already covered in DARE#I feel like at this point everybody has heard all of the negative possibilities with weed use at least once#and that's not necessarily true of caffeine and even like. benadryl lmfao#I might delete this in 10 minutes if I psych myself out akbdjznsjf
8 notes
·
View notes
Note
Sorry for weird question, but is there a safe way to do c0ke ?
No worries! I think I've actually answered this before.
"Safe" is a relative term when it comes to doing drugs, since no drug is 100% safe. But on the scale of safe to dangerous, cocaine is on the more dangerous side (apologies that the chart is a bit old, but it’s the only one I could find that laid it out in an easy-to-understand format). If you want to experiment with drugs, you’d be better off trying hallucinogens or MDMA, which have a lower potential for addiction and adverse effects.
If you’re interested in trying cocaine as a way to escape a problem in your life (including, but not limited to, anxiety and depression), you’re at a much higher risk for addiction than if you’re doing drugs recreationally at a party. If you find yourself engaging in perfectionistic, compulsive, or addictive behavior when it comes to other things (school/work, video games, food, caffeine), you’re at a higher risk for addiction. If you have family members who are addicts, you’re at a higher risk for addiction. If you have any type of heart of vascular condition, cocaine (and MDMA) are ones to skip, since they increase heart rate and blood pressure.
A few harm reduction type things you should keep in mind when doing any drugs:
- Know what you’re getting. Some drugs look like one thing but turn out to be another or turn out to be laced with something else. You can get testing kits online that can help you figure out if the drug you were sold is what you think it is or not.
- Have a sober companion. Having someone around who’s in a sober state can help to prevent anything really bad from happening.
- Don’t mix. Combining drugs can increase risk to your system, and so can mixing drugs with alcohol. In this case, “combining” is taking any drug/medication/alcohol up to 24 hours before another drug. This includes any prescription medication you might be taking. SSRIs, anti-depressants, and anti-anxiety medications commonly have interactions with other drugs, so you have to be careful. It also includes any supplements you might take. For cocaine in particular, avoid mixing with other stimulants (like MDMA/ecstasy) since it magnifies the vascular impact, alcohol, MAOI antidepressants, the anticonvulsant carbamazepine, lithium, SSRIs (may cause brain haemorrhage), and the atypical antipsychotic risperidone.
- Go slow and know your dose. Make sure to research the correct dosing for any drug you might be thinking about taking, and then take less of it than is recommended. You can always take more if you’re not feeling an effect, but you can’t take less. Also make sure that you’re taking the right dose for you. Body weight, height, and gender can impact how drugs are metabolized in our systems, and so what works for your friend may be too much for you (although some drugs, like hallucinogens, are not weight dependent). Don’t try to compete with other people to see who can do the most. Along with that, it’s important to know how long the drug takes to “hit”. Sometimes people fall into the trap of waiting a few minutes, deciding the dose they took isn’t going to do anything, and then take more, which results in them having too much of the drug in their system. Again, it’s important to go slow. Take more time than you think you might need before taking another dose.
- Write everything you’ve taken down and never lie to paramedics. In the event that things do go south, you want to be able to tell the paramedics everything you’ve taken, in what doses, and how long ago so that they can treat you. Paramedics will not report you to the authorities for taking illegal drugs; they just want to treat you. If you’re ever in a situation where someone is having a bad reaction to a drug or overdosing, call the paramedics. You won’t get in trouble and you can save a life.
- Do it somewhere safe, and give yourself time. Preferably in a house, without a ton of dangerous items around, where you are unlikely to encounter the police or disapproving adults. Whether or not you agree with it, in most countries doing drugs is illegal, and you don’t want a court case on your hands. Drug addiction ruins lives, but so does being arrested for drug possession (in the US, at least), and being arrested happens more frequently. You also want this environment to be one in which you feel relaxed and where nothing disturbing or scary is likely to happen. You also want to make sure that there are no time pressures on you for more than the duration of the drug- clear at least your entire day just in case.
For cocaine in particular, here are some harm reduction tips to keep in mind:
- Take care of your nose. Dilute it with water before snorting and rinse your nose with water after, insert the straw deeper into your nasal passage so that the powder doesn’t get stuck in your nose hairs, alternate nostrils, and make sure that the cocaine is chopped into a fine powder. Use a straw instead of a dollar bill, and don’t share it with others. With too much usage, cocaine can create damage to your nasal tissue, so you want to be careful.
- Know the signs of overdose. These include blue or extremely pale face, difficulty breathing, vomiting, foaming at the mouth, seizures, and chest pain.
Ultimately, whether you want to try it or not is up to you. Just be aware of the risks and take precautions so that you’re as safe as possible. Will you be fine if you don’t do any of the things I suggested? Maybe. But I’d hate for you to get into a bad situation that was easily preventable.
Also, on a total side note, there's no reason to use leetspeak on Tumblr. There's nothing to demonetize here and Tumblr's search function is so terrible that even if it wanted to ban everyone who used the word "coke", it wouldn't be able to.
7 notes
·
View notes
Text
Tips for Buying Nootropic Supplements

When buying nootropic supplements, it is important to be aware of the ingredients and dosage. Some nootropics contain artificial ingredients, which may not be safe for you. Also, some companies make their products using unnatural or artificial ingredients. Be aware of what you are getting before buying. In addition, you should always check with your doctor about the safety of the supplement before consuming it. Listed below are some tips to remember when purchasing the best brain enhancement pills.
If you're looking to buy a nootropic supplement, you should know that it is available in different forms. However, the process of choosing the right one can be tricky. There are several factors to consider, such as availability and price. Therefore, it's best to check reviews and recommendations from other users before making a final decision. You can also read some nootropic supplement reviews before buying. A nootropic product is not necessarily expensive if you purchase it online.
There are several factors that you should take into account when buying a nootropic supplement. The first thing you should consider is the cost. The amount you spend on the supplement should be within your budget. Some companies will offer free shipping, but you should make sure to compare prices. Some companies offer free consultations, so you can find the right product for you. The last thing to consider is the quality of the product.
Before you purchase a nootropic supplement, it is important to do some research. You should also look at the ingredients in the nootropic. Some people believe that it will improve their mental faculties, but these supplements are not recommended for this purpose. Many people prefer to purchase nootropic supplements over prescription drugs. It is crucial to read reviews about the product before making your final decision. It's best to check the ingredients before you buy a nootropic, and you can save yourself a lot of money.
Before purchasing a nootropic supplement, you should read reviews online and ask questions to avoid companies that do not have guarantees for their products. A nootropic supplement should not be used to treat depression or improve memory. There are several different types of nootropic supplements, and the dosage depends on the individual. Some nootropics are natural supplements and should be taken with care. There are some side effects of nootropics, and some do not have any.
There are some concerns when buying a nootropic supplement. The best nootropic supplements are free of harmful substances. For example, caffeine can cause addiction, while other nootropics may be safe for everyone. The best nootropics will contain nootropics that will not affect your health or have the potential to improve your mood. If you're looking for a nootropic supplement, you should also check the ingredients. For instance, DMAE is an essential component for nootropics. It helps the brain improve its functioning. Check out this post that has expounded more on the topic: https://www.encyclopedia.com/education/encyclopedias-almanacs-transcripts-and-maps/nutrition-dietary-supplements.
0 notes
Text
It started with a whisper
I originally wrote ‘Like I did with you’ as a one-shot but people wanted a sequel. This turned out to be waaaaay longer than expected (4.7k word count). Inspired by Everybody Talks by Neon Trees. I hope you lot enjoy!
Ao3
(Also this is Mari’s new outfit, all credits go to the original artist)
————
Two teens stood upon the balcony of a large banquet hall, exposed to the midsummer night air. The sky was a lilac blanket that hung over the Parisian buildings, speckled with glowing stars. The moon, with it’s crescent smile, beamed down of the young couple.
Hey, baby, won't you look my way?
Marinette’s eyes were closed as she rested her head upon his shoulder, relaxing after the night’s rapid escalation. Tonight she had arrived at the ball with the intent to be there for her friends, but somehow she found herself within the arms of Gotham’s (and probably Paris’) Ice Prince. She had overheard his nickname from the Gotham students, one of which being Jon, who was in the middle of mocking the young Wayne. She had never considered that nickname as suitable; sure he was temperamental & had a tendency to snap, but icey to the core? No.
I can be your new addiction
Damian was calm. For the first time in his life he felt like he could take a breath. His exhale was carried off by a small gust of wind, the bush over hanging the stone railing rustled. With his inhale, the scent of Marinette’s perfume became present once more. Mixed with the crisp night’s air, her usual scent of pastries was mixed with what could only be described as ambrosia. His phone vibrated within his pocket, it was never on volume due to the potential risk it caused during his heroic activities.
“Shit.” Notifications covered his screen, multiple tweets, Instagrams and Tiktoks in which he had been tagged in. But the alert came from his family’s private messaging chat. The whole thread was a shit storm, Grayson and Todd’s messages were completely capitalised (he learnt years ago this meant ‘to yell’ in writing form) and both had multiple ‘keyboard spasms’. Drake, like the thorough detective he is, had combed through the images and videos, investigating their validity. His honorary sisters had replied with ‘awwwww’(s) and ‘Omg we MUST meet this girl! I need to know how she tamed the demon!’. He could practically hear Brown’s shrill voice from across the ocean.
Hey, baby, what you gotta say?
No reply from his father or Alfred. The two of them were the only semblance of ‘normal’ paternal figures he had within his life, after the sham of a relationship he had previously held with his grandfather. Their silence unnerved him.
Marinette had noticed his attention had shifted to his phone, her own mobile was buzzing away within her baby pink purse. Messages, notifications of account tagging and comments galore. A sigh left her lips when she saw her parents seemed to be none the wiser. Good, she didn’t need to deal with future adoration for ‘The boy who swept our daughter off of her feet’ (or something along those lines).
Her cheeks regained some of the warmth they held before as she thought of her parent’s reaction. Scrolling through her Twitter she saw her friends had posted multiple images of the night’s events, majority being her shared dance.
Chloé Bourgeois @TheBestBourgeois
what kind of Disney shit is this? (Insert video of two teens dancing around an mostly empty dance floor.)
Alix Kubdel @Sk8trGirl
Replying to @TheBestBourgeois
I KNOW RIGHT?! THEY WERE FUCKING FLOATING!!!
All you're giving me is fiction
She was thankful that they hadn’t tagged her but she hadn’t been spared by others in attendance. Her post thread had blown up, thousands had commented and even more had viewed the evidence. There was no way she would come out of this unscathed.
“Has anyone been on Twitter today?” The blonde of the family asked as she walked into the dining room. Her eyes focused on her scrolling screen, brows furrowed in confusion. “Actually has anyone seen what’s happening on any of our socials?”
It was early in the afternoon and the family had recently returned home after a straining stakeout. The Joker had broken out of Arkham and the Batfam had to deal with his minions. Dick’s arm was in a sling (sprained from a grapple gone wrong), Jason was icing his hand, Alfred was stitching Bruce’s chest wounds while Tim and the girls escaped without severe injuries. All were still recuperating and finally able to recharge.
Alfred always enforced a strict ‘no devices at the dinner table’ rule; no matter how urgent it was, it could wait until after sustenance was consumed. Tim strongly opposed this, but there was no arguing with Agent A. This all surmises that probably no one had seen the crap storm on social media.
I'm a sorry sucker and this happens all the time
Bruce sighed, bringing his free arm up to rub his eyes. Tilting his head back to look at Steph, “Who was it this time?” Barbara quickly took out her phone to see what Stephanie was talking about, all the while glancing accusingly at Dick and Jason. Both of whom held up their arms (or in Dick’s case arm), declaring their innocence.
“It wasn’t fucking me!”
“Jason! Language!” Dick shot a glare at Jason and was met with one in return. “It wasn’t me either.”
“Then who-“ Bruce started before being cut off by his most rambunctious daughter.
I found out that everybody talks
Stephanie with a squeal, exclaimed that it was Damian. Visions of what the Wayne brat could have done flashed through the heads of everyone in the room. He had been sent overseas before the quarantines and lockdowns hit. During Damian’s first month in France he had been forced into online schooling and then finally when he got to go to in-person classes he hated it. Described the class as a kindergarten with petty and vindictive toddlers.
Had he broken someone’s arm? Was that person of such importance that it had spread over multiple social media platforms? France’s government had announced on June 15th, that teens were now being inoculated so him having COVID-19 was doubtful. Had he insulted the wrong person? Had he taken over the government? He certainly had the potential.
Everybody talks, everybody talks
What they saw stunned them, even Steph as she watched it for the 7th time. Damian Wayne was dancing. But not only that, he was dancing with a girl.
It started with a whisper
“What is this shit?”
No one verbally objected to Jason’s outburst but he was sent a harsh glare from Alfred, Dick and Bruce. Their focus soon returned to the images and videos before them. Babs’ and Steph’s phones were returned to them as the others ran to grab their own devices. They all met back at the table, comparing the posts and comparing their notes.
I can hear the chitchat
“There’s no way this can be real.”
“Jesus Tim,” Barbara rolls her eyes, “have you seen the amount of posts there are? You’d be an idiot to think otherwise.”
Take me to your love shack
“I’m with Tim, how do we know this isn’t some skit. I mean, Demon Spawn almost looks normal. That’s a matter of concern.” He almost dry heaved when he agreed with Tim. Damian couldn’t be capable of naturally exuding that amount of humanity unless there was something in it for him.
Mamas always gotta backtrack
“I was just saying Babs, that we should check the credibility of these images. For all we know they could be gorilla glued together and trying to get unstuck.” Tim cringed at his own reasoning, he really needed to either sleep (probably not going to happen anytime soon) or find his favourite coffee brand (which had been one of the first to vanish after the covid hoarders appeared).
When everybody talks back
Dick was too busy freaking out and spam messaging the youngest Wayne, to defend Damian’s humanity. The family saw this and followed suit, wanting to get information from the source.
Chat name: Alfred supremacy
BigBird: AHHHHHH DAMIAN!
BigBird: YOU LOOK SO CUTE!!!
BigBird: HAIFJDNDNFI
LittleWing: WTF HAPPENED DEMON SPAWN YOU LOOK ALMOST HUMAN
Babs: who knew the city of love would influence the brat
Blondie: they are so cuteeeeeee!
Blondie: We HAVE to meet her!
Silent-but-deadly: agreed.
Timbo: YO DEMON
Timbo: Apparently the videos are legit
Timbo: are you being blackmailed?
And it just devolved into more chaos from there, fueled by the fact that they saw Damian’s ‘Blood Son’ account appear online before vanishing once more. Dick shrieked, “I FOUND HER ACCOUNT!”
The family gathered around the eldest son, peering over his shoulder to view his iPhone 12max screen. They saw a young girl’s Instagram account. It was locked but they could see her profile pic, the girl had black hair and looked to be if Asian decent. They compared it to the videos but it was hard to see due to the hall’s lighting and the minimised facial features of the pfp. Alfred suggested that they search up her username and see who has tagged her, some might have other photos of her.
After research for awhile, the family began to get frustrated with lack of results.
Hey honey you could be my drug
You could be my new prescription
“Come on!” Jason complained, “What kind of teenage girl doesn’t post her life online?” He ignored the girls glares and went back to researching. How had the account by the name of ‘mariiiiinette’ to managed to prevent the entire Wayne clan from accessing it? Damn Instagram privacy settings. He groaned, dragging a hand down his face, “We are fucking stupid. Why don’t we just use the Bat-computer? It would be so much fucking easier.”
“It shouldn’t be used for civilian issues-“
Too much could be an overdose
“The girl could be a meta for all we know! We aren’t safe until we know who she is.” Jason points a finger at Tim, his paranoia flared up and even though he would never admit it, Jason would do anything to protect each member of his family (although Bruce is still debatable).
All this trash talk make me itching
Barbara and Tim took their usual positions as Oracle and Red Robin (who had been banned from patrol due to lack of sleep). The rest of the Batfam stood behind them either with arms crossed or still failing at researching.
Oh my my shit
“The account is owned by a girl called Marinette Dupian-Cheng. She is French-Chinese and her parents own a popular bakery. Also if it wasn’t already obvious, she goes to Collège Françoise Dupont, aka Damian’s French school.” Tim begun informing his nosy family, “But this account has been inactive for the past 6 months, which is strange due to her frequent posting schedule before hand. It seems she probably has a second account and this is her old one.”
Everybody talks, everybody talks
“Not only that,” Barbara interrupted. “There are unopened messages from other accounts that accuse her of being a bully. There is a whole Facebook page about this girl and how she has been hurting her old friends, but neither side seems reliable. The so called victims seem to be twisting the truth but there is barely any information about Marinette so we can’t disprove it either.”
“Read out some of the messages.” Bruce took a cup of coffee from Alfred and sipped it.
The main screen of the bat computer displayed a Facebook group with the banner picture being a photo of Marinette. “They are mostly complaints expected of teen girls when there is a girl they don’t like; ‘Marinette is such a know-it-all’, ‘She is constantly insulting Lila’s intelligence’. They go on to talk about how Marinette was briefly expelled from the Collège before being reinstated by the principle for a reason unknown to them.”
Everybody talks too much
“Her school reports up until this year were good. The newest one states, ‘While Marinette is a wonderful and bright student, I encourage her to settle her disagreements outside of class. This seems to only be a recent occurrence and I implore her to go to the guidance council if she is in need of help.’” A beat of silence echoes through the cave, Tim sighed. “Jason’s meta theory could be correct. She could have just recently started exhibiting her abilities and using them to get what she wants.”
“Bruce what do you want to do?”
“We’re going to Paris.”
She opened her eyes to the blaring morning light that streamed through the blinds. Her lashes still painted with mascara that refused to leave. She felt a pang of sorrow when she was removing her makeup and dress last night, she never wanted the night to end. She shuffled down the stairs to the kitchen, covering her mouth when she yawned. She greeted her mother as she entered the kitchen to get breakfast.
She glanced at her phone and there was the chaos that was started hours ago and it was still occurring. It was the weekend, she wouldn’t need to deal with her classmates until Monday. But she would still have to survive her parent’s interrogation. Out of the corner of her eye she caught her mother smirking at her.
Everybody talks
“Nadja told me some interesting news about last night.” Marinette held her breath, glaring at the toaster, willing it to hurry up so she could escape. “Well,” Sabine patted her shoulder before rubbing Mari’s back. “I know you didn’t want to go but I hope you had fun.”
With that she exited the kitchen, probably going to help her father in the bakery. The ravenette stared after her, eye widened in shock, jumping when the toaster went off. Buttering her toast she went over the conversation, her brows furrowed in confusion. She had expected a ‘When do I get to meet the oh so famous prince?’ or ‘Should I be expecting a new guest sometime in the near future?’ or at least a ‘Who was that young man, Bǎozàng (宝藏 it means treasure)?’ But she said nothing.
A small smile was plastered upon her face as she changed and went down to help her parents in the bakery. Her father didn’t say anything either, he gave her a knowing smile before continuing to kneed the dough. She sat at the the store front as the cashier whilst her parents were busy making ‘Paris’s Finest Pastries’.
Her musings slowly faded as she was brought back to reality by badly hushed whispers. Two young preteens were by the bread roll casing near the door. She had seen them come in before with their parents, the girls went to the prestigious international school over in the 16th arrondissement. The one with purple hair kept whispering to the brunette, both ‘subtly’ glancing towards her. Using her enhanced hearing she listened in on their conversation.
“That’s her, I swear that’s her in the video.”
The blonde’s face soured likes she sucked on a lemon. “No, it wasn’t good lighting there is no way he would dance with someone like her.”
Everybody talks
Marinette had tough skin but their words had an impact, only a small one due to her defence mechanism of repressing emotions. She stopped listening and went back to drawing in her sketchpad, she was in desperate need of a new school outfit.
The two girls eventually came up to the counter, goods in hand. Marinette rung up and bagged their items (paper because save the turtles sksksk) in a tired daze. A phone was shoved into her face, her eyes barely adjusted to view the screen before the blonde spoke.
“Is this your instagram?” She asked in a tone so snobbish that it should be illegal from a person her age. Marinette finally was able to view the screen that was barely an inch from her face. Her old Instagram ‘mariiiiinette’ was displayed on screen, she hesitantly nodded, gaze flicking back to the two in front of her.
The blonde’s nose scrunched up and the purple goth girl squealed in delight. They soon after left the store, their conversation had devolved into ‘See! I told you’ and ‘Yeah, yeah. You were right.’
Walking to school on Monday, she had finally come down from cloud nine. She still rode the tail end of her high as she rushed along her path to her campus, she wasn’t going to be late but she sure wasn’t going to be early. She had spent the better part of the weekend designing and sewing a brand new outfit. Her new look was composed of a black cropped singlet (L'amour gagne hemmed into it and it’s straps), paired matching peach plaid cropped overshirt and a-line miniskirt. Her hair was down, ballet flats were worn and her makeup was the usual with the added edition of a rose gold eyeshadow.
Even though her face was covered in a black and gold mask, she looked hot.
She reached the campus and the whispers started again, people were still buzzing from Friday night. Her classmates, the majority of her grade and the younger years seemed to gossiping before class about the formal’s events. She couldn’t spot any of her friends or the two Gotham transfers, so she was stuck listening the the chitchat. Why couldn’t she have been late like usual?
Damian had a fowl disposition and it showed in multiple icey glares (and that was before he even reached the collège). His family had made their appearance known in Paris at 1am Sunday morning. He could have used his dorm to escape but his family didn’t have the word ‘privacy’ within their vocabulary. He didn’t want to have to pay for a lock replacement due to his brothers’ (most likely Todd with Drake & Grayson laughing at him) lock picking habit.
The Ice Prince was back with full force. He had just been... influenced by all the other couples. Yes he did respect Dupain-Cheng and he appreciated her company & pleasant conversations. He would struggle to hide a small smile at the memory of the dance, even if he denied himself the happiness of normality, he felt content when reminiscing.
“Ooo the Ice Prince is here, did he have a fight with his princess or something?” The voice seemed to mock him.
“The Disney Magic is gone. The demon is back.”
Everybody talks
At the second jeer he shot a glare at the perpetrator. Jon held his hands up in an ‘I surrender manner’, laughing as he joined Damian at his side. The two entered the school’s large foyer and looked to see if any of the classes were open yet. Sadly they weren’t, before he was wrong and the his class was plain torture but this was truely hell.
He saw Dupain-Cheng sitting alone on the stairs, drawing within her sketchpad. He wondered how a girl like her, who always seemed to be involved in other’s lives (for the better) was ignoring all of the comments about her. She felt his focus centre on her, eyes flicking up to meet his, she provided him with a small wave before continuing to draw.
Jon nudged him with an elbow to his ribs and dragged him off to the side, into the boy’s locker rooms. Jon scowled at the door, “It’s a mad house out there. You’ve heard what some people are saying right?”
“Why would I care about these imbeciles?”
Jon jabbed Damian in the chest, causing the demon to stumble. Green eyes darted from blue eyes to the tan finger. “You care when lies hurt people you care about.”
The day began to rapidly decline once the two dance partners took their seats, next to each other. They had both been placed up the back of the class and them sitting together hadn’t been a problem until now apparently. She wasn’t even safe when the teacher started their lecture, whispers and glances were cast towards them. Once the two got to biology it was better, Ms Mendeleiev was a strict teacher and was able to control the class.
Everybody talks
But the recess came. When the bell rang she slowly started packing up her equipment, Alix and Max (who she shared biology with) waited for her; she watched as the Ice Prince left through the door. She knew she didn’t need to be concerned about her friends joining in with the gossiping, if anything they would dispel people and tell them to ‘Mind their own fucking business’ because this whole situations is ridiculous, utterly ridiculous.
She did receive some slight teasing from Alix about being a Disney princess, but Marinette quipped back about the skater’s fairytale story being ‘Pinknette, the Geek and the Beast’. The three met up with the other two of their group, they had just come from geography. Kim was complaining that Argentina was a state in America.
“That’s Arkansas you idiot!” Chloe shrieked, lightly hitting his arm with her white handbag. Max held his head in his hand as he approached, how had his tutoring sessions failed so badly?
Chloe turned to Marinette, a smile forming from her glare. The blonde examined the designer’s clothing, nodding. “You look like you are about to have a hot girl summer.”
Marinette’s face burned, the tips of her ears coated in red. Alix chuckled and nudged her shoulder.
Everybody talks
“Look at her, she is so desperate for his attention that she probably copied those designs.”
“Why do you think he danced with her anyways? Maybe she has something on him? I mean, she forces him to sit next to her in class, who knows what else she has done.”
What. The. Fuck.
Chloe glowered towards Lila’s posy. “We have a fucking seating plan, those cretins-“ She made a motion to storm over but was caught by the ravenette, looking back to Mari, her rage decreased from a boil to a simmer.
“No Chlo. It’s fine, it’s not worth it.”
Everybody talks... back
The group walked out to the school’s front steps, it was a mad house... a mad courtyard? Students sitting on the stairs, on the grass and standing around mingling, all of them now were staring at her. She held her backpack close to her chest (she had swapped her signature coin-bag purse for the pastel pink bag), pretending its a shield. Her friends circled around her becoming an obstacle to prevent their stares. If people were afraid of a scowling Kim then they don’t know the scorn of Chloe or Alix’s bite. And Max, sweet quiet Max.... you better hope he doesn’t have blackmail on you (he probably does), he can dismantle your life with a single anonymous post.
Rushed footsteps approached them. The group was broken apart by a rude Wayne boy, he swept Mari away from the school and the gossip crowds within. Her four friends shouted at him and he kept walking, shooting a glare at them in response. He kept pushing Marinette forward with a hand placed on the small of her back, her backpack was now swung over his other shoulder.
They ended up in her favourite alcove. She had brought him here with the other Gotham transfers for a native’s tour of Paris. It had always been her safe place to be creative.
It started with a whisper (everybody talks, everybody talks)
“My apologises for our rushed departure but you seemed to want to get out of their anyhow.” His gruff tone danced through the silence, his head still peaking around the corner; watching for any unwelcome guests.
“Thank you.” She whispered, her voice almost being carried off by the gentle wind. A genuine smile illustrated upon her face.
“We weren’t able to converse after the events of the other night. I would like to formally apologise once more for my actions causing this adverse reaction. If I had kn-“
“You don’t need to apologise!” She squeaked, hiding her eyes behind her fisted hand. Her shoulders curled inwards as she tried to make herself seem as small as possible, a side effect of her common use of her secondary miraculous form: Multimouse.
“I chose to dance with you, you don’t need to apologise for my own actions.”
He stared at her with confusion. He had taken the blame so she wouldn’t need to do so herself; but she had taken it anyways. He had given her an out. Why does she always take the blame, even for things out of her control?
“But if I hadn’t danced with you then you wouldn’t have been the focus of the entire school.”
Marinette stepped forward, her eyes hardened and blazing. “Damian Friday night I went there out of obligation to my friends, I didn’t want to be there. But dancing with you? That was the highlight of my week, probably my month too. I enjoyed our time together.” Her face softened, lips twitched downwards ever so slightly. “I don’t regret anything about that night, but do you?”
He was bad at comfort. Everyone in his family avoided him when they were in need, he plainly didn’t know what to do. She wasn’t visibly upset but he sensed that she is disappointed that he apparently didn’t share the same opinion of the night. The only thing he regretted about that night was letting Jon call him a coward, but then again if he didn’t he never would have danced with Dupa- Marinette.
He picked up her clenched hand, the tension in her body alleviated at his embrace. He remembered how Grayson would apologise to Kor’i or how his father interacted with Ms Kyle. He brought their hands up and placed a kiss upon her knuckles.
And that was when I kissed her (everybody talks, everybody talks)
“I do not regret anything either—“ he cleared his throat, “In fact, I’d appreciate if we would be able to interact more, especially outside of that cesspit.”
Was he...?
It didn’t matter.
She smiled the same dazzling smile she gave him at the dance. She nodded while laughing, “I’d love that.”
Everybody talks
The two stay talking, hidden within their secret alcove for the rest of the day. She texted her parents to say she was with a friend and would be back later that night. Damian didn’t bother texting his family, Marinette knew he had to be back soon due to his dorm’s curfew.
The sun was setting at they walked back together, he did the gentlemanly thing and dropped her off at her bakery door. She could see her mother behind the register inconspicuously looking over at the two of them. Damian’s lips quirked upwards, she was satisfied with his kinda-smile.
He walked back, hands in pockets and a neutral expression upon his face instead of a scowl. He reached his door and took his keys, he found that it was already open. Damn.
His family was splayed out within his two roomed dorm. Todd and Drake were fighting over a place to sit on his bed, whilst his father sat at his desk, watching the commotion. The three of them turned to him as he enter the room, they were the only family members able to attend on short notice; Cain had a ballet audition, Gordon & Brown had concert tickets for tomorrow, Grayson had to take care of Mar’i while Kor’i was on Tamaran and Alfred stayed to ensure no one died during their night time activities.
“We need to talk Damian.” His father stood, leaning onto the desk chair. “The school called and said you had an unexcused absence for half the day. Where were you Damian?”
Damian stared into his father’s eyes. He was fifteen, almost an adult, but was treated like he was ten again.
“I was with a friend.”
“Probably the girl from the dance. Marinette, right?” Todd mocked him. Damian snapped his head in the direction of his bed, glaring at both his brothers.
“That’s what I want to talk about with you Damian. Now I don’t know her personally but from what we’ve discovered through our investigation we have some concerns. What’s happened Damian?”
The youngest Wayne’s glare shifted off of his brothers to the floor, and then finally to his father; his family sitting in wait for his answer. Straightening his posture, his shoulders clicked as he rolled then back. His statement’s tone was sure and steady, “Everybody talks father.”
Everybody talks... back
#maribat#marinette x damian#mlb x dc#batfam salt#batfam is concerned#Daminette#the aftermath of ‘Like I did with you’#everybody talks by neon trees#max kante has blackmail and will use it#Alix will bite if provoked#dc x mlb#damian wayne x marinette dupain cheng#Marinette Dupain-Cheng is a meta?#supportive Dupain-Cheng parents ❤️
171 notes
·
View notes
Text
Medical Marijuana Dispensaries

The trend of medical marijuana dispensary in Las Vegas is not new. Las Vegas has been the center of the marijuana business for over 20 years now. Patients flock from other states to Las Vegas because they want relief from the pain of their illnesses and are unable to find it in their home states. With a medical marijuana dispensary in Las Vegas one can easily obtain a safe and effective form of pain management. People in pain prefer to be treated using natural means instead of relying on prescription pain medication that often brings unwanted side effects. The medical marijuana las vegas dispensary is a perfect solution to help those patients who don't qualify for medical marijuana cards in their home state or do not wish to travel outside of their state to have the benefit of medical marijuana treatments.
The medical marijuana dispensary in Las Vegas has been providing a safe and effective form of treatment for many years now. Patients often report feeling much better after they visit the dispensary for treatment. The long hours of work at the Clinic keep them always anxious and focused on their work, however, most of the time is spent discussing their problems and the different options open to them. Visitors often leave with a new found vigor for life. The staff at the medical marijuana dispensary is very caring and informative. There is no judgment on any patient, and every person is considered equal to everyone else.
In Las Vegas there are so many different types of clinics and medical marijuana Dispensaries to choose from. Because there are so many choices one has to take their time and research which ones are the best choice for them. With so many different clinics and practices the chances of finding what you are looking for will be higher. You might not get the answer right away, but stick with it because the research is in order.
Las Vegas is known for gambling and adult entertainment and Las Vegas has more than one medical marijuana dispensary in operation. Some of the medical marijuana Dispensaries are located right next door to the sex and adult entertainment casinos. This means they are directly accessible to the people who frequent those casinos. This makes more money for them and makes their work easier, while keeping their patients happy and their side of the law intact.
If you decide to check out a medical marijuana dispensary in Las Vegas then you must do your research. Learn as much about each practice as you can. It's always a good idea to visit several before you make a final decision on which one you want to use. You must always remember that you need to check out how qualified the staff is and how clean their facilities and premises are. If you find anything suspect then don't use it.
The benefits of visiting a medical marijuana las vegas dispensary outweigh any other reason that you may have for checking them out. These marijuana users have far less risks involved with using this type of medicine than other users. They help reduce the risk of side effects and addiction and also help save money. When a government tries to tax these pot users it is only to increase their profits are never the reason behind people using marijuana. If a government is worried about the price of medical marijuana then they should be worried about the price of people using it. You may need to check out this article: https://en.wikipedia.org/wiki/Cannabis_(drug) to get more info on the topic.
1 note
·
View note
Link
Yves here. Reader IM Doc, an internal medicine practitioner of 30 years, trained and worked in one of the top teaching hospitals in the US for most of his career before moving to a rural hospital in an affluent pocket of Flyover. He has been giving commentary from the front lines of the pandemic. Along with current and former colleagues, he is troubled by the PR-flier-level information presented to the public about the Pfizer and Moderna vaccines, at least prior to the release of an article in the New England Journal of Medicine on the Pfizer vaccine: Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. However, he did not find the study to be reassuring. He has taken the trouble of writing up his reservations after discussing the article with his group of nine physicians that meets regularly to sanity check concerns and discuss the impact that articles will have on their practices.
By IM Doc, a internal medicine doctor working in a rural hospital in the heartlands
Right off the bat – I am as weary and concerned about this pandemic as anyone. What my little rural area has been through in the past three weeks or so has been nothing short of harrowing. This virus has the ability to render patients about as sick as I have ever seen in my life, while leaving more than half the population with minimal if any symptoms. The patients who are sick are often very sick. And instead of slow and steady improvement like we normally experience, most of these patients are assigned to a long and hard slog. Multiple complications arise. This leads to very diminished throughput in the hospital. The patients literally stack up and we have nowhere to put the new ones coming in who themselves will be there for days or weeks. On top of that are the constant donning and doffing of PPE and intense emotional experiences for the staff, who are themselves becoming patients or in this small town have grandma or Aunt Gertrude as a patient.
To put it bluntly, I want this pandemic over. And now. But I do not want an equal or even worse problem added onto the tragedy. And that is my greatest fear right now. And medical history has demonstrated conclusively over and over again: brash, poorly-thought-out, emotion-laden decisions regarding interventions in a time of crisis can exponentially increase the scale of pain and lead to even worse disasters.
I am not an anti-vaxxer. I have given tens of thousands of safe and tested vaccines over my lifetime. I am very familiar with side effects and safety problems associated with all of them. That is why I can administer them with confidence. I am also an optimist, so all of the cautions I discuss below are the result of experience and the information made public about the Pfizer vaccine, not a temperamental predisposition to see the glass as half empty.
I know this piece is long, but I wanted to completely dissect the landmark New England Journal of Medicine (from now on NEJM) publication of the first Pfizer vaccine paper. I am replicating the method of my mentor in Internal Medicine, a tall figure in 20th Century medicine. He was an internationally recognized authority and his name is on one of the foundational textbooks in his specialty. He was a master and he taught me very well, including the fundamentals of scientific inquiry and philosophy, telltale signs of sloppy or dishonest work, the order in which you should dissect someone’s work, and the statistics involved.
When I have a new medical student doing rotations with me, I give them a collection of reading. At the very top is Drug Companies & Doctors: A Story of Corruption from the New York Review of Books in 2009 by Marcia Angell, MD. She was the editor-in-chief of the NEJM, the very journal that published this Pfizer vaccine paper.
Dr. Angell’s article is the Cliffs Notes version of much longer discussions she had about corruption, corporatism, managerialism, profiteering, greed, and deception in in the medical profession. Patient care and patient concerns and indeed patient lives in her mind have been absolutely overcome by all of these other things. It is a landmark paper, and should be read by anyone who is going to interact with the medical community, because alas, this is the way it is now. I view this paper the exact same way I view Eisenhower’s speech about the military industrial complex. What she said is exactly true, and has only become orders of magnitude worse since 2009.
And now the paper.
Unfortunately, this study from Pfizer in the latest NEJM, and indeed this whole vaccine rollout, are case studies in the pathology Agnell described. There are more red flags in this paper and related events than present on any May Day in downtown Beijing. Yet all anyone hears from our media, our medical elites, and our politicians are loud hosannas and complete unquestioning acceptance of this new technique. And lately, ridicule and spite for anyone who dares to raise questions.
I have learned over thirty years as a primary care provider that Big Pharma deserves nothing from me but complete and total skepticism and the assumption that anything they put forth is pure deception until proven otherwise. Why so harsh? Well, to put it bluntly, Big Pharma has covered my psyche with 30 years of scars:
• As a very young doctor, I treated an extraordinary middle-aged woman who had contracted polio as a toddler from a poorly tested polio vaccine rolled out in an “emergency.” Tens of thousands of American kids shared her fate1
• The eight patients I took care of until they died from congestive heart failure that had been induced by a diabetes drug called Actos. The drug company knew full well heart failure was a risk during their trials. When it became obvious after the rollout, they did everything they could to obfuscate. Actos now carries a black box warning about increased risk of heart failure
• The three women who I took care of who had been made widows as their husbands died of completely unexpected heart attacks while on Vioxx. I have no proof the Vioxx did this. But when Vioxx was finally removed from the market, the mortality rate in the US fell that year by a measurable amount, inconsistent with recent trends and forecasts. Merck knew from their trials that Vioxx had a significant risk of cardiovascular events and stroke, and did absolutely nothing to relay that danger in any way. Worse, they did everything they could to muddle information and evade responsibility once the truth started to come out
• The dozens upon dozens of twenty and thirty-something patients who have been rendered emotional and spiritual zombies by the SSRIs, antipsychotics and amphetamines they have been taking since childhood. Their brain never learned what emotions were, much less how to process them and we are left with empty husks where people never developed. The SSRIs and antipsychotics were NEVER approved for anyone under 18. EVER. While there are some validated uses for stimulants in children, they are obviously overprescribed, as confirmed by long-standing media reports of their routine use as a study/performance aid. It is all about the lucre.
• The hundreds and hundreds of 40-60 year olds who have been hollowed out from the legal prescribing of opioids. All the while the docs were resisting this assault, the drug companies and the paid-off academics and medical elites were changing the rules to make physicians who did not treat any pain at all with opiates into evil Satan-worshippers. And they paid for media appearances to drive across the point: OPIATES ARE GOOD. WE HAVE MADE THEM SO YOU CANNOT GET ADDICTED. And here we are now with entire states taking more opioids than in the waning days of the Chinese Empire, and we all know how that story ended. All this misery so a family of billionaires can laugh its way to the bank.
I carry all these people and more with me daily. I would not be doing a service to their memory if I allowed myself to be duped into writing another blind prescription that was going to add yet another scar.
I will dissect the important parts of this paper exactly as my mentor described above taught me. He performed years of seminal research. He was a nationally-known expert in his field.
In medicine, especially in top-tier journals like NEJM, landmark papers are always accompanied by an editorial. These editorials are written by a national expert who almost always has “peer-reviewed” the source material as well. This is how the reader knows that an expert in the field has looked over the source material and that it supports the conclusions in the paper. My mentor did this all the time. The binders all over his office were the actual underlying data that he scrutinized to confirm the findings. There is no way on earth to print and publish the voluminous source material. Editorial review was one sure way all to assure that someone independent, with appropriate experience, confirmed the findings. This was onerous work, but he and thousands of others did it because this is the very essence of science. He was scrupulous in his editorials about findings, problems, and conclusions. It was after all his reputation as well.
My first lesson from him: READ THE EDITORIAL FIRST. It gets the problems in your head before you read the statistics and methods, etc. in the actual paper. It gives you the context of the study in history. It often includes a vigorous discussion of why the study is important.
Admittedly, over the past generation, as the corporatism and dollar-counting has taken over my profession and its ethics, this function of editorial authoring has become at times increasingly bizarre and too-obviously predisposed to conclude with glad tidings of joy, especially if pharmaceuticals are involved.
So I read the editorial first. You can find it on the NEJM webpage, in the top right corner.
And, amazingly, it is basically a recitation of the same whiz-bang Pfizer puffery that we have all been reading for the past few weeks. There really is not much new. Furthermore, it is filled with words like “triumph” and “dramatic success”. Those accolades have yet to be earned. This vaccine has not yet even been released. Surely, “triumph” is a bit premature. Those words would NEVER have been used by my mentor or similar researchers in his generation. They would have been focused on the good, the bad and the ugly. A generation ago, editorial reviewers saw their job as informing the reader and making certain the clinicians that were reading knew of any limitations or problems.
In quite frankly unprecedented fashion, two different events that were carefully reported occurred almost simultaneously with the release of both the paper and the editorial. Both of these events contradict and contravene data and conclusions reported in both the paper and the editorial and I believe they deserve immediate attention. They both belie the assertions of the editorial writers that [emphasis mine] “the (safety) pattern appears to be similar to that of other viral vaccines and does not arouse specific concern”.
First, a critical issue for any clinician is “exclusion criteria”. This refers in general to groups of subjects that were not allowed into the trial prima facie. Common examples would include over 70, patients on chemotherapy and other immunosuppressed patients, children, diabetics, etc.. This issue is important because I do not want to give my patient this vaccine (available apparently next week) to any patient that is in an excluded group. Those patients really ought to wait until more information is available – FOR THEIR OWN SAFETY. And not to mention, exclusion criteria exist because the subjects in them are usually considered more vulnerable to mayhem than average subjects. From my reading of this paper, and the accompanying editorial, one would assume there were no exclusion criteria. They certainly are never mentioned.
I reiterate, the paper is silent on this question of exclusion criteria, as is the editorial. Had my mentor seen something like “exclusion criteria” in the source material, and realized that it was not in the final paper, he would have absolutely included a notice in his editorial. This would have been after calling the principal investigator and directly questioning why there was no mention in the original paper. Patient safety should be foremost on everyone’s mind at all times in clinical research and its presentation to practitioners.
And now we know there were exclusion criteria, not because of anything Pfizer, the investigators, or the NEJM did but because of stunning news out of the UK. UPDATE: I will address this at greater length, but an alert reader did find the study protocol, which were not referenced in any way that any of the nine members in my review group could find, nor were they mentioned in the text of paper or editorial, as one would expect for a medication intended for the public at large. I apologize for the oversight, but this information was not easy to find from the article, not mentioned or linked to from the text of the article, the text of the editorial, in the “Figures/Media,” or in a supplemental document.
In the UK on day 1 of the rollout, two nurses with severe allergies experienced anaphylaxis, a life-threatening reaction to this vaccine. Only after world-wide coverage did Pfizer admit that there was an exclusion criterion for severe allergies in their study.
Ummm, Pfizer, since we are now getting ready to give this to possibly millions of people in the next few weeks – ARE THERE ANY OTHER EXCLUSION CRITERIA? Should I, as a physician, specifically not be giving this to patients with conditions that you have excluded?
Furthermore, NEJM, since you published this trial, have you bothered to at least put a correction on this trial on your website that it should NOT be given to people with severe allergies? I certainly see nothing like this.
Should someone from the NEJM or the FDA be all over Pfizer to ascertain the existence of other exclusion groups so we do not accidentally harm or kill someone over the next two weeks?
Unfortunately, Americans, you have your answer from the FDA about severe allergic reactions right from a press conference in which Dr. Peter Marks, the director of FDA’s Center for Biologics Evaluation and Research is quoted as saying:
Even people who’ve had a severe allergic reaction to food or to something in the environment in the past should be OK to get the shot….1.6% of the population has had a severe allergic reaction to a food or something in the environment. We would really not like to have that many people not be able to receive the vaccine.
Are you serious? Dr. Marks, have you ever seen an anaphylactic reaction? I live in a very rural area. Many patients live 30 minutes or more from the hospital. What if one of them had an anaphylactic reaction to this vaccine hours after administration, had no epi-pen and had to travel a half hour to get to the nearest hospital? There is a very high likelihood that a good outcome would not occur. Sometimes, as a physician, I simply cannot believe what I am hearing out of the mouths of our so-called medical leaders.
To the writers of the editorial accompanying this research:
Did you actually look at the source material? The existence of at least one exclusion criterion for severe allergic reactions had to be in there somewhere. If you did look at the source material, are there others that the physicians of America need to know about? If they were not in the source material, after the events in the UK, has anyone bothered to follow up with Pfizer about this omission?
Does anyone at NEJM or Pfizer or FDA plan to fully inform the physicians of America? Does ANYONE at NEJM or Pfizer or FDA care about patient safety?
Now for the second story that got my attention this week, an article from JAMA Internal Medicine, a subsidiary of JAMA, The Journal of the American Medical Association.
JAMA, like NEJM, is one of America’s landmark medical journals. I will assure you that JAMA is not the National Enquirer. This piece was written by a nursing researcher. It is very likely she is well-versed in all aspects of American medical research.
In her story, she details her recruitment and her experience in the Pfizer COVID trial, the same one we are dissecting here. She describes in detail her experience with the vaccine and the fact that she is concerned that many patients are likely going to feel very sick after the injection. She wrote up her own reactions, and included a very troubling one. About 15 hours after her second injection, she developed a fever of 104.9. She explained that she called her reaction to the Research Nurse promptly the next morning. The recounted the response of the Research Nurse to her information as “A lot of people have reactions after the second injection. Keep monitoring your symptoms and call us if anything changes.”
Thankfully, it appears this nurse has completely recovered. From the best I can tell, this encounter occurred in late August and early September, putting it well within the trial’s recruitment of arms as detailed in the paper.
This JAMA article impinges directly on Figure 2 on page 7 of the paper, a graphic that that lays out all the major side effects during in the trial.
It is very important to note that based on the trial’s own data, conveniently laid out on the very top of the figure in green, blue, orange and red, a temperature of 104.9F or 40.5 C is described as a Grade 4 event. The definition of a Grade 4 event is anything that is life-threatening or disabling. A fever of 104.9 can have grave consequences for any adult and is absolutely a Grade 4 event.
By law, a grade 4 event must immediately be reported to the FDA, and to the Institutional Review Board (the entity charged with overseeing the safety of the subjects) and to the original investigators. THERE IS NO EXCEPTION. One would think that would also be reported in the research paper to at least alert clinicians to be on the lookout.
I could not find any mention of this event in the text of the paper. NOT ONE. Let’s take a closer look at Figure 2 on page 7 where adverse events are reported in a table form. Please note: this is a very busy image, and in the browser version, with very low resolution graphics that are profoundly difficult to read (they are a bit clearer if you download the PDF). This is a time-tested pharmaceutical company tactic to obscure findings that they do not want you to see. My mentor warned me about ruses like these years ago, and finding one raises the possibility that deception is in play.
The area for the reporting of this Grade 4 reaction would be on the 2nd row down at the left of the set called B, titled systemic events and use of medication. The area of concern would be where the graph is marked with the number 16. Do you see a red line there? It would be at the very top. I have blown this up 4 times on my computer and see no red there. I am left to assume that this Grade 4 “Life Threatening or Disabling” event that was clearly within the time parameters of this trial was not reported in this study.
To those who say that I am making way too much out of one patient with a severe fever, let’s do a little math. There are 37,706 participants in the “Main Safety Population” (from Table 1), of which 18.860 received the vaccine.2 Let us assume that this individual was the only one that had a GRADE 4 reaction. Let us also assume that the end goal is to vaccinate every American a total of 330,000,000 people. So if we extrapolate this 1 out of 18,860 into all 330,000,000 of us, it suggest that roughly 17,500 could have this kind of fever. Now assume a 70% vaccination rate, and you get that would be approximately 12,250. I hope you now understand that in clinical medicine related to trials like this – a whole lot of nothing can turn into a whole lot of something quickly when you extrapolate to the entire targeted group. Does anyone not think that the clinicians of America should be prepared for anything like this that may be coming?
A couple more questions for NEJM and the editorial writers:
Were you ever made aware that this Grade 4 reaction occurred? Now that we have a reliable report that it occurred, has there been any attempt to investigate?
Did the Research Nurse actually report this event? If not, was she just simply not trained or was there deliberate efforts to conceal such reactions? How many more reactions were reported anywhere this trial was conducted and that did not make it to the FDA, the IRB or possibly the investigators? Is that not a cause for concern?
As if this is not enough, there is so much more wrong with this editorial. Now we are going to talk about corruption.
I want to reiterate my concern that over the past generation, as my profession has lost its way, its medical journals have turned into cheering sections for Big Pharma rather than referees and safety monitors. We all should relish the great things medical science is doing, but we should be doing EVERYTHING we can to minimize injury and death. Too often our journals have become enablers of Big Pharma deceiving our physicians and the public. Unfortunately, this paper and its editorial look troublingly like a case study of this development.
To provide context, I looked over the last month of the NEJM, the issues from November 12, 19 and 26th and December 3rd. Based on having read the NEJM over the years, I believe these four weeks are representative.
During this period, there were 15 original articles published in the fields of Oncology, General Surgery, Infectious Disease, Endocrinology, Renal, Cardiology, Pulmonary and Ear Nose & Throat. Of these 15 articles, the editors thought that eight were important enough to have an editorial from an acknowledged expert. I have read every one of these studies and the editorials as I do every week. All eight in the past month were indeed by leading experts in the field of the underlying studies. They included a COVID vaccine overview reviewed by an leading figure in vaccinology, and two COVID papers about Plaquenil and other approaches discussed by top infectious disease experts.
It was unlikely that those papers were going to get national media attention. All medical stuff.
But here we have our Pfizer vaccine paper. We have 300,000 fatalities in the USA alone and millions of cases. We have whacked our economy, we are in the depths of a national emergency. And we have a paper, the first, that may offer a glimpse of hope. Certainly this would be a landmark paper, and certainly it was treated in that manner? Right?
One would think that the doctors of America would have this study explained to them by a world-known vaccinologist? NOPE…..Maybe a virologist? NOPE….. Maybe a leading government official? Dr. Fauci? Dr. Birx? Dr. Osterholm? NOPE…..Maybe an expert in coronaviruses? NOPE…
We get the Pfizer ad glossy editorial treatment from Eric Rubin MD, the editor-in-chief of the NEJM. And Dr, Longo, an associate editor. Dr. Longo is an oncologist. Dr. Rubin is at least a recognized infectious disease doctor, but his specialty based on my Google search is mycobacterium, not virology. Again, one would normally anticipate for a paper of this importance, the editorial would be from someone with directly on point expertise.
Why would this fact been important to my mentor? (and I had the privilege of hearing him trash a paper in an open forum about a very similar issue, a paper introducing a drug to the world that later was the disaster of the decade, Vioxx) Why is this important to me and all the other physicians in my review group here in flyover country yesterday?
Because the choice of authorship of the editorial leads you to one of only several conclusions:
• Pfizer would not release the source data because of proprietary corporate concerns and no self-respecting expert would review without it
• Pfizer knew there are problems and did not want anyone with expertise to find out and publicize them
• The editors could not find a real expert willing to put their name on a discussion
• Drs. Rubin and Longo are on some kind of journey to Vanity Fair and wanted their names on an “article for the ages”
• This is a rush job, and no one had time to do anything properly, and so we just threw it all together in a flash
Readers, pick your poison. If anyone can think of a sound reason, please let me know. I am all ears.
But let’s open up the can of worms a bit more. Pfizer supports NEJM. Just a brief swipe through of recent editions yielded several Pfizer ads. A Pfizer ad appeared on my NEJM website this AM. I do not know how much they pay in advertising but appears to be quite a bit.
Americans, have we devolved so far in our grift that it is now appropriate for the EDITOR-IN-CHIEF of our landmark medical journal to be personally authoring “rah rah” editorials about a product of a client that supports his journal with ad dollars? And he has the gall to not present this conflict on his disclosure form? Really? Am I the only one worried about this type of thing?
Now we travel from the can of worms to the sewer. And this impacts every single one of us. I want you to Google the names of the people on the FDA committee that voted 17-4-1 two days ago to proceed with the Emergency Use Declaration. Go ahead – Google it. On that list, you will find the name Eric Rubin, MD. Why yes indeed, that is the very same Eric Rubin MD who wrote this editorial. Who is the Editor-in-Chief of the NEJM. A publication that certainly takes ad dollars from Pfizer. And he was one of the 17 to vote for the Pfizer product to be immediately used in an emergency fashion. Oh yes, oh yes he was.
Am I the only one who can recognize that Pfizer and other pharma companies may have some influence on Dr. Rubin thanks continued support of his employer, the NEJM? Am I the only one concerned that Dr. Rubin’s “rah rah” editorial may have been influenced by Pfizer? Is anyone else troubled that the Editor-in-Chief of the NEJM, supported by Big Pharma advertising dollars, is sitting on an FDA board to decide the fate of any pharmaceutical product? Is this not the very definition of corruption? Or at least a severe conflict of interest? I strongly suspect that a thorough evaluation of members of that committee will reveal other problems. As my grandmother always used to say, “There is never just one roach under a refrigerator.”
I looked in vain all day today for media discussions of conflicts of interest with Dr. Rubin or anyone else in a position of authority. I found nothing.
What I did find was the Boston NPR affiliate WBUR discussing Dr. Rubin’s Yes vote. You can listen yourself:
This interview left me much more concerned about Dr. Rubin’s role and what exactly he read in the raw data from Pfizer. In this interview, he admits that he as an FDA advisory member has seen no data from the Moderna trial coming up for a vote this week:
These two vaccines are fairly similar to one another, so I am hoping the data will look good, but we haven’t seen the data yet, so I reserve judgement.
Excuse me, but should not the members already have the data and be mulling over it to ask intelligent questions?
These statements left me more worried about the issues I have already brought up with the Pfizer vaccine:
We don’t know if there are particular groups that should or should not get the vaccine…We do not know what will happen to safety over the longer term.
When finally asked specifically about the UK allergic reactions and if they came up in the FDA meeting (emphasis mine):
It did come up and this was a bit of a surprise because in the trial, that trial was limited to specific kinds of participants, there were apparently no incidents like that, nevertheless this suggests it is something we are going to have to look out for.
There is absolutely not a word in the published data to suggest there was a limit to SPECIFIC PARTICIPANTS – what on earth is he talking about? Are there limited specific kinds of patients that we as physicians should be looking to vaccinate?
In a fine finish, toward the end of the interview Dr. Rubin states he is a bit relieved that low risk patients will be getting the vaccine later after we know more about the side effects with the first patients. I am really not trying to be a jerk – but are you kidding me? I thought this vaccine was a triumph with minimal side effects.
Dr. Rubin, kind sir, I really feel that you owe a clarification about your statements in the WBUR interview to the patients and caregivers of America. We are the ones with lives on the line.
First, I have the privilege of sitting on an Institutional Review Board (an independent entity that protects patient safety) and I know something about Grade 4 side effects. Just for 1 Grade 4 side effect in one subject, the accompanying documentation would often be a half a ream of paper. Because I agreed to do that job, it was my obligation to look through that documentation. That half a ream was for one side effect in one trial. Yet, you state unequivocally in this interview, that you, as a sitting member of the FDA committee that oversees the safety of the nation in this affair, have not seen any of the Moderna documentation for that upcoming meeting this week.
For readers to fully understand what I am saying, this Moderna documentation is going to be reams and reams of documents that need to be evaluated carefully to ask the right questions. And you have not yet studied this? For a meeting in just a few days? I find this deeply troubling. Your statements create the appearance the committee you are sitting on is nothing more than a rubber stamp for a decision that has already been made. This would be an absolute tragedy.
Second, Dr. Rubin, you in your position as the Editor-in-Chief of the NEJM and the editorial writer for this research, may be one of the few people on earth that have seen the original Pfizer research. Despite calling this a triumph, you state in the interview that you are relieved that younger people less likely to get the vaccine early so you will have time to wait to see if complications develop in the first patients. You have stated, despite your assertion in the editorial that the side effects were consistent with other vaccines, that “we don’t know if there are particular groups that should or should not get the vaccine”. Have you seen something in that “triumph” research that is concerning enough to you to make such statements? As a physician, I would really like a clarification on this statement, given that the shots are already rolling out today.
Now that we are past the editorial, a few words about the nuts and bolts of the paper.
I look for very specific red flags – usually making the data difficult to interpret. This study did not disappoint.
On page 5, in Table 1, the Demographic Description of the participants, go down to the AGE GROUP area. Note it is divided into only two cohorts 16-55 and >55. This is a real problem. My mentor said an honest paper should never deploy such a tactic.
You see, more than half of my patients are over 70. Why is this kind of obfuscation a real problem for my ability to trust the vaccine? Well, the intro papers to many pharmaceuticals that have gone down the drain in recent years have used this very same device. It is their way of hiding the fact that they did not put many older patients in the trial, certainly not representative of the population, and certainly not representative of who is seemingly going to get this vaccine in the first round. Do I know that 90% of the >55 group is actually between 55-58? I don’t. How hard would it be for them to do a breakdown in decades? 16-25 26-35 36-45 46-55 56-65 66-75 76-85? We have lots of computers in this country and the population breakdown is done this way on studies I read all the time. Why not do provide this information on a study that is this critically important, particularly one where elderly patients will be near the head of the line?
What are they trying to do here? Unfortunately, too often drugmakers resort to this practice to hide their failure to test their drug on the elderly to an appropriate or safe degree, knowing there would likely be lots of problems. Because of their past behavior, I ALWAYS assume this is true until proven otherwise and act accordingly with my elderly patients.
That is the world these companies have made for themselves.
Now for the tables on pages 6 and 7 about immediate side effects.
Just a brief look shows that local soreness and tenderness is very common, up to 75% with this vaccine. That is a bit high, but not that far out of range from my experience with other vaccines.
The tables on page 7 are the whoppers.
Headaches, fatigue, chills, muscle pain and joint pain appear to be very common, way more common than other vaccines I am used to, as in an order of magnitude higher. It is very clear from this table that about half the patients, especially the younger ones, are going to feel bad after this vaccine. That is extraordinary.
We are told nothing about how long these symptoms last or the amount of time at work lost. The “minimal side effects comparable with other viral vaccines” in the editorial and press releases is just not consistent at all with my experience of 30 years as a primary care physician. There was universal agreement with this assessment among my MD colleagues. They had great concern about this as a matter of fact: great concern that it will cause bad publicity and decrease administration and great concern that given this already high side effect profile, it may be much worse when it gets out to the public.
Given the fact that this virus is largely asymptomatic in more than half the people infected, what exactly are we doing here?
Furthermore, unlike other pharmaceutical papers that try to explain variances in symptoms like this, there is not a word offered about possible underlying causes of these outcomes.
The numbers of COVID cases in the placebo group vs the vaccine group have been widely publicized, from 162 cases in the placebo group down to 8 in the vaccine group, giving a relative reduction of 95%. It seemed to all of us in our review group that we do not have nearly enough patients to really make assessments. That is not a criticism. The researchers have done admirably in my opinion to get this many patients this quickly. That is still the problem: they are going to be using the first million patients or so in the general public to get a real gauge on numbers and side effects.
Another issue of grave concern to us all on Friday was the asymptomatic cases. The only subjects counted in the 162 and the 8 numbers above were patients with symptoms. Who knows how many in each cohort were asymptomatic.
This to me leads to the most important question of all, and it was again completely untouched….. How many asymptomatic patients are there? And how many who were vaccinated are still able to spread the virus? Not even an attempt to answer that question. This is critical, and is one of the ways a vaccine can backfire. If a vaccine does not provide sterilizing immunity, ie stop transmission, it is of limited use for disease control. It is great for the individual, but if they can remain without symptoms and still spread it all around it does not help from a public health standpoint.
I have described my concerns and red flags about this study. I would like to add one more thing. Pharmaceuticals that go bad rarely do so in the first few weeks or months. Rather, the adverse effects take months or years. It is a known unknown of not just vaccines but any kind of drug. Our pharma companies have become notorious for having inklings or indeed full knowledge that there is a problem early on, and saying nothing until many are maimed or killed. I will assume that this is the case in this class of drugs until proven otherwise. They are such deceivers I have no choice.
Due to sense of urgency my colleagues and Ifeel about this vaccine rollout, we had an ad hoc meeting of our Journal Club to discuss the NEJM article. Of the nine physicians at the meeting, three have already had very mild cases of COVID. Of the nine, only one is enthusiastic about these vaccines. I have a wait and see stance. I will not be taking it myself. I have too many scars, too many staring at me from the grave to take any other approach.
My patients’ feeeback on the COVID vaccine has been very different than the polls finding that 60% are ready to take it. About half my patients are in the professional/managerial classes and feature a higher level of the 0.1% than the US overall. They tend to be more blue. Most prefer to wait and thankful that health care workers were getting it first. The other half who are working class, more red, and they feel the whole thing is a hoax. They will not be getting the vaccine – likely ever.
The only enthusiasts I would call elderly Rachel Maddow fans. That really makes no sense to me at all since Operation Warp Speed was a Trump project and even Kamala Harris said she would not take a vaccine that Trump recommended.
I would say AT BEST 25% of my patients will be getting this vaccine shortly after being available. There is widespread skepticism that is not being acknowledged by our media. The pharmaceutical industry has worked tirelessly to earn every bit of that disrespect.
Please look at Dr. Angell’s seminal article from 2009. She predicted in her works, all of this and more. My profession has been captured by a cabal of corporatist MBA clones, rapacious and unethical pharmaceutical entities, and an academic elite addicted to credentialism and cronyism. They have over the years bought off and infiltrated all of our government health care regulating agencies and our public health system. And they are completely incestuous. I believe where we are now to be worse than Dr. Angell could have ever dreamed. Even more depressing, I see no way out.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
1 As a special homage to the polio patient described above, a truly exceptional woman, let me underscore that the disastrous rollout of the this polio vaccine came at a time similar to ours. Panic and malaise were in the air. The children of America and the world were being stricken with polio at an alarming rate. Dr. Alton Ochsner, a leading figure in medicine of the day, vaccinated both of his grandchildren in public in an attempt to bolster confidence in the vaccines. Within 8 days his grandson was dead of bulbar polio. All the celebrities and politicians lining up to take this vaccine on national TV should remember this tragedy. “Stupid human tricks” like this have no place in this kind of situation, and can backfire in unexpected ways. Unlike that era’s polio vaccine, there is no way on earth this vaccine can transmit COVID. However, there are those of us in the medical profession who treat the plan to make population-wide use of messenger RNA, which before these trials had been repeatedly investigated but never reached the human trial stage save in a small scale Zika vaccine study. This is no time for machismo. This is also no time for anything less than complete transparency on the part of everyone involved in the quest for safe and effective vaccines. To behave in any other way is an affront to patients like mine who have suffered and died in the past.
2 If you read the paper, you might well have wondered about that 18,860 number and even checked Table 1 to make sure it’s accurate (it is), since the third paragraph of the Abstract, under the headline “Results,” has very different figures:
A total of 43,548 participants underwent randomization, of whom 43,448 received injections: 21,720 with BNT162b2 and 21,728 with placebo.
So how did the researchers get from 21,720 injected with the vaccine to the 18,860 in the “Main Safety Population”? This sort of thing confirms the impression that this is a very incomplete or sloppy study. It is really not clear where the difference between the 37,706 and the 43,548, or for that matter, the 36,520 total subjects in the Tables 2 and 3 (Efficacy) come from. I used the 37,706 and hence the 18,860 that went with it from Table because it gave slightly smaller numbers than using the Table 2 and 3 figures, but they would be close to each other.
My concern here is the 6000ish discrepancy between the figures in the main text compared to the tables. Were they excluded? If so, why? I could not make heads or tails out of this, and accordingly kept it out of the body of this post. This kind of inconsistency really needs to be hashed out with the actual source data in hand, and should have been explained in the article, even if just in footnotes.
#covid19#covid#the rona#la rona#covid-19#covid vaccine#fuck covid#coronavirus#medecine#health#medical pharmaceuticals#pharmaceutical industry#big pharma#pfizer#vaccine rollout#operation warp speed
3 notes
·
View notes
Text
CBD FOR SLEEP
Though CBD's existed for thousands of years and recognised for its many beneficial properties, the west has just confessed its possible in the past couple of decades. Countless Americans turn to over the counter and prescription drugs, each year, to help with Insomnia. While shot in moderation and for the correct reasons, these sleeping aids may not pose a problem.
Regrettably, there are often side effects attached to a lot of those over the counter medications: they could be addictive. If used over an extended interval, they can also become ineffective. As many Americans look for an alternative to help them overcome the issue of Insomnia, CBD is currently making its way to the top of the list. Research exploring the idea of CBD as an alternative to over the counter sleep aids is continuing. CBD has come to the forefront because of the interaction with our own bodies natural biological system.
Our bodies possess receptors called the Endocannabinoid system. It's the name given to the communication system of neurotransmitters and receptors which govern many of our body's functions like pain, mood, and memory. ( the circulatory system) CBD interacts with this specific communication system also helps boost a calming effect in the brain. Cannabinoid receptors' interaction with our natural biological system is the subject of studies into CBD instead of traditional sleeping aids. But with clinical trials ongoing, it is always wise to do some research before focusing on your CBD journey.
There are many elements that contribute to our inability to sleep. Although knowing this does not mean it is simpler for people who have Insomnia. Trying to determine the issue can in itself add to it. However, identifying the problem will help decide if CBD is for you personally, and which CBD product is best.
Causes of Insomnia
* Stress Chronic pain
* Mental health Problems
* Hormonal Imbalance
* Poor diet
* Caffeine overload
* Overcrowded Housing Arrangements
Should you determine that CBD is an option for you, the next step is to determine which product is best for your needs.
Which Product Is Ideal For You?
The CBD goods, you chose to purchase, will depend significantly on what you would like to achieve.
If your poor sleep results out of pain, topicals may suit you, a topical offers intense, instant relief to the problematic place. It is a favorite choice for many who suffer from arthritis or other inflammatory conditions. Edibles are just another option for those who don't wish to use creams or tinctures.
The journey through the digestive tract and liver usually means that you won't consume the full dosage of CBD on your edible. It will take longer for you to feel the benefit, but it's a great way to enjoy your CBD wherever you are. Healthy CBD snack choices and nutritional supplements are offered on a lot of wellness websites. They arrive in the form of solutions and generally include tinctures, like sprays, oils, and lozenges.
Placing CBD below the tongue offers a faster effect as it doesn't have to pass through the digestive tract. This means that more of the CBD is absorbed into your system faster. It is because of this Vaping is also popular.
There are several different ways to Vape, using a choice of Single-Use Pens, or Chargeable units. All are extremely discreet, making them appealing--combined with the reality that vaping is the quickest way to get CBD into your system.
Whatever method you opt to pick for your CBD consumption - CBD Flower or CBD OIL, it's wise to remember that research is ongoing. Possible respiratory problems can arise. It is almost always best to seek guidance from your health practitioner. It's imperative if you are already taking medicine. There are several studies that suggest that CBD may interact with other medicines.
CBD is considered safe and mountains of research in recent years suggest it's beneficial for many ailments. However, trials on humans are ongoing and not conclusive.
It is essential to bear in mind that some retailers may not be as ethical as others. Therefore, always check the company you're purchasing from. Read the label to check the dosage of CBD from the product. In case you decide to choose CBD, start with a moderate to moderate dosage till you find what works for you. The entire effect of CBD products for sleep may be slow. It's like a slow build-up of about 30 days.
Conclusion
There are many reasons why we might suffer with insomnia. For some, it can be a temporary condition. For others, it's an ongoing illness causing added stress. CBD's claims to benefit those with stress-related issues has increased its prevalence. The relaxing properties of this item, which makes it a possible alternative for additional sleep aids. Research is as we have stated still in its infancy. Before you take any sleep help, getting into the path of your health issue, is a good idea.
1 note
·
View note
Note
What are you addicted to?
Started with music, then turned to me aggressively smoking pot, tripping way more than I should have, then prescription medications I messed with for a while, getting vicodin for a wrist surgery at 14. When I graduated coke was a big thing in my town, so many people were doing it but most of it is really shitty and just gave me an even stronger urge to do other things. At this point my twin sister had already overdosed on heroin the night of our prom, my dad and I had revived her, but she still struggled with her boyfriend who had been an addict for years at that point. I was so hateful towards hard drugs after that, but I ended up going through a really hard time in my life, dealing with a break up, working two jobs and losing my childhood home all in a short time, I moved in with a guy I had been friends with since I was 14 and he was about 2 years deep into his addiction already. I was almost 19 the first time I tried heroin, and I remember instantly knowing it was a feeling I didnt want to live without. I told myself I could actually moderate it, and I did for awhile. I quit my second job and stayed at the same one for around 3 years actually, functioning on drugs for the better part of a year, keeping it my secret from all but maybe 3 people and the people I met through drugs. That was so dangerous, living life like that in secret. Not to mention everything in MA was quickly turning to fentanyl, which is more addictive than morphine, and way more likely to make you overdose, plus narcan/naloxone doesnt always help- my sister needed like 3 when she OD’d, and I’ve heard of people needing more. H quickly changed me, made me bitter towards anything that wasn’t it, even though it was a constant battle with H itself. I told myself I wasn’t hurting others because they didnt even see me doing the things I did, because “I only stole from stores, not the people I loved”, because addiction will tell you anything to keep you in that animalistic “survival” state as my boyfriend and I call it. But basically about a year into doing harder drugs, one night I made the awful mistake of mixing what my friend told me was “liquid xanax” (basically just research chemicals), H, and alcohol, I went from being out and about with my friend, to waking up starfished on my parents front lawn, my head cracked open from me falling into the front cement stairs, me getting up to greet my parents because I couldn’t even feel my head, let alone realize how messed up I was. My mom literally laid in bed next to me and held me the whole night, and I had no idea until she told me the next morning. A day or so later, I remember I had to work all day and I was going through withdrawals towards the end of the day and of course was freaking out trying to figure out how to pickup. I figure out a plan and my boyfriend at the time who was also my manager at work was gonna bring me home from work that day and I was gonna pull my usual “oh I don’t feel good” or whatever so he’d drop me off and not know what I was up to, but I was stupid when I was stuck in that mindset and I can’t believe I thought I could hide it from him or my parents. I got home to an intervention with him and my parents, and an hour later was on my way to a detox in Boston. Freaking out because I was sick, I chugged the rest of the liquid nightmare stuff, and stumbled my way through my first night of detox, which wasn’t much considering I got there late at night. I remember waking up in so much pain the first day though, and everyone there looking at me like “you don’t look as happy as you did!” and me just thinking “I met you??” and realizing I was all alone in a well-known detox on Mass Ave (one of the worst places for drugs in Boston). It was the scariest and hardest week of my life. I did a methodone detox because I was way too sick and weak to try anything else, and I remember I actually came out of detox sicker than I went in because of it, which only pushed me further into my addict mindset, telling me “suboxone! get on the clinic!”- another wrong choice for me. Medical Assisted Treatment can help so so many people, don’t get me wrong. Like with everything, it depends on the person. Suboxone is a synthetic opiate, basically acting to get rid of physical withdrawal symptoms, and works as a blocker in your brain and makes it so you cannot get high on opiates. I ended up being on the clinic for 6 months which started out great, but soon turned into just another addiction. The clinic prescribed me a way higher dose than I needed, which made it super easy for me to sell or trade the subs for other drugs or cash. Not to mention it was just another thing I had to wake up and take every day, and you get sick if you don’t. Another prescription to fill and pickup weekly, biweekly, monthly. I ended up relapsing and after a few months of not talking, the friend since 14 that I had used with for my first time, and who I tried to help get clean so many times, was finally clean. And it hit me like a ton of bricks- he sounds so amazing, he looks so fucking good, and he sounds like HIMSELF again- the kid I fell in love with SIX years ago, before all the insane shit we went and put ourselves through. It took detoxing in jail for a month and getting put on probation, but the fact that he was THANKFUL for that and looking at this as an opportunity to build a new and even better him, was so inspiring to me. I went from basically the streets and living at dealers houses, to moving back in with him to focus on recovery, and I can’t even begin to explain how rewarding it has been. Recovery will always be the hardest thing I’ve ever had to deal with, but I also have to be honest and say I do not regret doing any of it. Anything and everything can be a learning experience, its just how you look at it and what you do with it. My addiction is once again music and art- I’ve made goals to learn something new everyday, to find new music, to learn lyrics, to get better with my memory. I’m planning my future and it looks so exciting, even though I’ve officially had to start over with NOTHING. My clothes all got stolen and lost, I had sold every bong, pipe, art piece, everything I cared about. I even lost my wallet and social security at one point, and I can’t begin to tell you how awful that felt. But I kept going, and things aren’t rapidly getting better, but I realize you get what you put into things, you have to make the daily decision to want to be better, it doesn’t just happen. And for anyone curious, I did detox from suboxone and my boyfriend and I are full supporters and advocators of VIVITROL/NALTREXONE. There are pills you can take daily, but I highly recommend getting the monthly shot in your ass, because this stuff has the amazing benefit of blocking opiates and making it so you can’t get high, but is completely not addictive or dependable, no physical symptoms occur.Thankyou so much to anyone who takes the time to read this, I’ve been wanting to post something like this for awhile but quite honestly I’ve been trying really hard to focus on myself in order to be able to at all be useful to others lol proud of everyone who woke up today though, and a huge rest in peace to those who might not, and to those I know who haven’t made it. My inbox is always open- I haven’t had my own phone for the better half of a year so I may not answer right away, but I will always try.
#me#text#recovery#heroin recovery#crack reovery#drug reovery#addiction#addiction support#fuck heroin
575 notes
·
View notes
Text
Of course, he was high, been smoking pot his whole life.
Berenson begins his book with an account of a conversation he had with his wife, a psychiatrist who specializes in treating mentally ill criminals. They were discussing one of the many grim cases that cross her desk—“the usual horror story, somebody who’d cut up his grandmother or set fire to his apartment.” Then his wife said something like “Of course, he was high, been smoking pot his whole life.”
Of course? I said.
Yeah, they all smoke.
Well . . . other things too, right?
Sometimes. But they all smoke.
Berenson used to be an investigative reporter for the Times, where he covered, among other things, health care and the pharmaceutical industry. Then he left the paper to write a popular series of thrillers. At the time of his conversation with his wife, he had the typical layman’s view of cannabis, which is that it is largely benign. His wife’s remark alarmed him, and he set out to educate himself. Berenson is constrained by the same problem the National Academy of Medicine faced—that, when it comes to marijuana, we really don’t know very much. But he has a reporter’s tenacity, a novelist’s imagination, and an outsider’s knack for asking intemperate questions. The result is disturbing.
The first of Berenson’s questions concerns what has long been the most worrisome point about cannabis: its association with mental illness. Many people with serious psychiatric illness smoke lots of pot. The marijuana lobby typically responds to this fact by saying that pot-smoking is a response to mental illness, not the cause of it—that people with psychiatric issues use marijuana to self-medicate. That is only partly true. In some cases, heavy cannabis use does seem to cause mental illness. As the National Academy panel declared, in one of its few unequivocal conclusions, “Cannabis use is likely to increase the risk of developing schizophrenia and other psychoses; the higher the use, the greater the risk.”
Berenson thinks that we are far too sanguine about this link. He wonders how large the risk is, and what might be behind it. In one of the most fascinating sections of “Tell Your Children,” he sits down with Erik Messamore, a psychiatrist who specializes in neuropharmacology and in the treatment of schizophrenia. Messamore reports that, following the recent rise in marijuana use in the U.S. (it has almost doubled in the past two decades, not necessarily as the result of legal reforms), he has begun to see a new kind of patient: older, and not from the marginalized communities that his patients usually come from. These are otherwise stable middle-class professionals. Berenson writes, “A surprising number of them seemed to have used only cannabis and no other drugs before their breaks. The disease they’d developed looked like schizophrenia, but it had developed later—and their prognosis seemed to be worse. Their delusions and paranoia hardly responded to antipsychotics.”
Messamore theorizes that THC may interfere with the brain’s anti-inflammatory mechanisms, resulting in damage to nerve cells and blood vessels. Is this the reason, Berenson wonders, for the rising incidence of schizophrenia in the developed world, where cannabis use has also increased? In the northern parts of Finland, incidence of the disease has nearly doubled since 1993. In Denmark, cases have risen twenty-five per cent since 2000. In the United States, hospital emergency rooms have seen a fifty-per-cent increase in schizophrenia admissions since 2006. If you include cases where schizophrenia was a secondary diagnosis, annual admissions in the past decade have increased from 1.26 million to 2.1 million.
Berenson’s second question derives from the first. The delusions and paranoia that often accompany psychoses can sometimes trigger violent behavior. If cannabis is implicated in a rise in psychoses, should we expect the increased use of marijuana to be accompanied by a rise in violent crime, as Berenson’s wife suggested? Once again, there is no definitive answer, so Berenson has collected bits and pieces of evidence. For example, in a 2013 paper in the Journal of Interpersonal Violence, researchers looked at the results of a survey of more than twelve thousand American high-school students. The authors assumed that alcohol use among students would be a predictor of violent behavior, and that marijuana use would predict the opposite. In fact, those who used only marijuana were three times more likely to be physically aggressive than abstainers were; those who used only alcohol were 2.7 times more likely to be aggressive. Observational studies like these don’t establish causation. But they invite the sort of research that could.
Berenson looks, too, at the early results from the state of Washington, which, in 2014, became the first U.S. jurisdiction to legalize recreational marijuana. Between 2013 and 2017, the state’s aggravated-assault rate rose seventeen per cent, which was nearly twice the increase seen nationwide, and the murder rate rose forty-four per cent, which was more than twice the increase nationwide. We don’t know that an increase in cannabis use was responsible for that surge in violence. Berenson, though, finds it strange that, at a time when Washington may have exposed its population to higher levels of what is widely assumed to be a calming substance, its citizens began turning on one another with increased aggression.
His third question is whether cannabis serves as a gateway drug. There are two possibilities. The first is that marijuana activates certain behavioral and neurological pathways that ease the onset of more serious addictions. The second possibility is that marijuana offers a safer alternative to other drugs: that if you start smoking pot to deal with chronic pain you never graduate to opioids.
Which is it? This is a very hard question to answer. We’re only a decade or so into the widespread recreational use of high-potency marijuana. Maybe cannabis opens the door to other drugs, but only after prolonged use. Or maybe the low-potency marijuana of years past wasn’t a gateway, but today’s high-potency marijuana is. Methodologically, Berenson points out, the issue is complicated by the fact that the first wave of marijuana legalization took place on the West Coast, while the first serious wave of opioid addiction took place in the middle of the country. So, if all you do is eyeball the numbers, it looks as if opioid overdoses are lowest in cannabis states and highest in non-cannabis states.
Not surprisingly, the data we have are messy. Berenson, in his role as devil’s advocate, emphasizes the research that sees cannabis as opening the door to opioid use. For example, two studies of identical twins—in the Netherlands and in Australia—show that, in cases where one twin used cannabis before the age of seventeen and the other didn’t, the cannabis user was several times more likely to develop an addiction to opioids. Berenson also enlists a statistician at N.Y.U. to help him sort through state-level overdose data, and what he finds is not encouraging: “States where more people used cannabis tended to have more overdoses.”
The National Academy panel is more judicious. Its conclusion is that we simply don’t know enough, because there haven’t been any “systematic” studies. But the panel’s uncertainty is scarcely more reassuring than Berenson’s alarmism. Seventy-two thousand Americans died in 2017 of drug overdoses. Should you embark on a pro-cannabis crusade without knowing whether it will add to or subtract from that number?
Drug policy is always clearest at the fringes. Illegal opioids are at one end. They are dangerous. Manufacturers and distributors belong in prison, and users belong in drug-treatment programs. The cannabis industry would have us believe that its product, like coffee, belongs at the other end of the continuum. “Flow Kana partners with independent multi-generational farmers who cultivate under full sun, sustainably, and in small batches,” the promotional literature for one California cannabis brand reads. “Using only organic methods, these stewards of the land have spent their lives balancing a unique and harmonious relationship between the farm, the genetics and the terroir.” But cannabis is not coffee. It’s somewhere in the middle. The experience of most users is relatively benign and predictable; the experience of a few, at the margins, is not. Products or behaviors that have that kind of muddled risk profile are confusing, because it is very difficult for those in the benign middle to appreciate the experiences of those at the statistical tails. Low-frequency risks also take longer and are far harder to quantify, and the lesson of “Tell Your Children” and the National Academy report is that we aren’t yet in a position to do so. For the moment, cannabis probably belongs in the category of substances that society permits but simultaneously discourages. Cigarettes are heavily taxed, and smoking is prohibited in most workplaces and public spaces. Alcohol can’t be sold without a license and is kept out of the hands of children. Prescription drugs have rules about dosages, labels that describe their risks, and policies that govern their availability. The advice that seasoned potheads sometimes give new users—“start low and go slow”—is probably good advice for society as a whole, at least until we better understand what we are dealing with.
~ Malcolm Gladwell
1 note
·
View note
Text
Time for More Natural Approaches? Study Finds Medical Errors are 3rd Leading Cause of Death
The ignorant vilification and also unethical reductions of natural, plant-based strategies to medical problems of both a mental as well as physical nature has long been exposed for the globe to see.
Nevertheless, typically the supporters of pharmaceutically-derived mechanistic medication indicate the high success of the industry, but taking into consideration that in the United States alone around 290 people pass away from prescription medicines every day and over 250 thousand individuals are dying from medical mistakes every year, this is simply not true.
A Exploration short article makes it clear why medical errors are the Third leading reason of fatality in the United States of The U.S.A.:
People don't just pass away from bacteria and heart plaque, they die from communication break downs, fragmented health care, diagnostic blunders, and over-dosing," said Martin Makary, a teacher at Johns Hopkins University School of Medication in Baltimore and also lead author of the study.
They likewise refer to the questionable lack of reporting of clinical errors that the US and other governments of the globe cannot advertise:
Along with even more compared to 100 various other nations, the USA uses a system for collecting nationwide health data-- recommended by the World Health And Wellness Organization-- that does not maintain track of medical errors.
This obviously brings the entire clinical standard right into inquiry. Of course there have actually been several remarkable successes from the contemporary strategy to treatment, such as surgery as well as some drugs. These tools have actually been an indispensable addition to humankind, yet just how do we understand which supposed modern medications are actually deserving to distribute at big and which are not?
How do we understand when a really essential medicine has been created in contrast to a pill that is largely for profit?
How do we understand when a pharma drug is unncessary due to the fact that there are extra natural as well as efficient treatments available?
When we take into consideration the corruption and collusion that exists within a sector that has actually been monopolised as part of the corporatocracy, it really is tough to know. As I meant out in a previous write-up:
Anybody with any kind of understanding on the medical industry will certainly understand that it has long been damaged by huge cash and also large pharma. It is necessary that we begin with this well-known truth, due to the fact that we have to recognize that the pharmaceutical-industrial complex will eventually be taken a look at by the mainstream attitude as we now check out the tobacco market: misleading, fraudulent, criminal and unethical.
To crystallize this factor, in the same article I refer to the excellent journalism given in a Collective Evolution post:
In the past couple of years much more professionals have come ahead to share a truth that, for several people, proves hard to ingest. One such authority is Dr. Richard Horton, the existing editor-in-chief of the Lancet-- considered to be one of the most well valued peer-reviewed medical journals in the world.
Dr. Horton recently released a statement stating that a whole lot of published research study remains in fact unreliable at best, otherwise completely false.
" The instance versus science is straightforward: much of the scientific literature, possibly half, might simply be untrue. Affected by studies with little sample sizes, tiny impacts, invalid exploratory evaluations, as well as ostentatious problems of rate of interest, together with an obsession for going after trendy fads of suspicious significance, scientific research has actually taken a turn in the direction of darkness."
In the very same post, another confronting fact is estimated by Dr. Marcia Angell, a longtime clinical journal editor:
' It is just no longer feasible to think much of the scientific research study that is published, or to depend on the judgment of relied on medical professionals or reliable clinical guidelines. I take no pleasure in this final thought, which I got to slowly as well as unwillingly over my 2 decades as an editor of the New England Journal of Medicine."
Keeping this in mind, when we integrate it with the major concerns that several truth-seekers have relating to the profit-before-morality model that has wriggled its means into the various control-systems which influence every facet of our lives, it comes to be clear that the medical-industrial complicated as well as our pursuit for effective health-care has to be promptly tabled for an open, clear and also impartial investigation to occur.
Seriously, how much time can we as a culture permit this dysfunction to damage not just ourselves, however our kids too?
How long will the masses simply claim that tribal societies really did not have accessibility to a wide variety of plant medications which recover as well as create the mind, body as well as soul?
How long will governments virtually neglect the abundant scientific proof that reflection is both a preventative and authoritative tool for ill-health?
Simply, there are numerous natural, plant-based medicines that have actually been clinically proven to be a very efficient device for recovering the body and expanding the mind. Much of these compounds are unlawful, nonetheless, which is simply another factor why the war-on-drugs has been an epic failure.
As I clarified in detail in an earlier write-up titled "The Trouble is Medicine Legislation, Not Drugs":
It is clear that several governments of the world have actually cannot really accept some exceptionally essential facts around dealing with the substances that make their means via our areas. Examples include:
Laws have actually criminalized medications right into one of the leading five industries in the globe, ensuring all its activity is handled within the underground market,
When you send this market underground it's mosting likely to result with unclean, unsafe and also unnecessary substances on the marketplace,
Drug plans result with more socioeconomic concerns and also increase the quantity of criminal offense and unneeded incarcerations in our cultures,
It is flawlessly all-natural for human beings to check out transformed states of awareness so the newer generations need accessibility to risk-free compounds and also legal compounds,
When individuals are told not to do something, some of them are mosting likely to do it anyhow, despite the threats to their health and wellness,
There are substances which have been made prohibited that have actually been clinically verified to provide strong supply strong healing and also developmental results,
The pretension in enabling pharmaceutical multinationals to flooding our culture with harmful, inefficient and also risky materials that are killing a lot more individuals compared to all prohibited compounds combined,
It's not the drug, however the abuse of the medicine in tough ecological problems, that brings about addiction and also recurring health-related problems,
Addiction ought to be dealt with as a health problem, not a legal one,
Many people are making use of drugs as avoidance from a social existential dilemma which is intensified by the soul-numbing materialistic and also consumerist ideologies,
Humans will never ever be quit from discovering their awareness and also as a result ideal law as well as education and learning plans should be placed in place to effectively look after the people that politicians were chosen to protect, and
There are other nations that have made progressive action in this area, such as Portugal, Czeck Republic, New Zealand, Uruguay, and The Netherlands.
It's not simply supposed illegal substances that are high in healing as well as developmental possibility, various other standard components such as bicarbonate soda have actually been shown in order to help the body to heal itself, also of cancerous tumours. Various natural herbs are likewise on the listing of useful components that battle illness.
In any kind of situation, no matter the many unfavorable influences that the war-on-drugs has subjected to our private as well as collective health and wellness, the longer we allow the federal governments of the globe to proceed to spread out lack of knowledge and anxiety to exactly what really are ancient, well-established as well as clinically-proven techniques to looking after ourselves, the longer we allow the corporatisation of our system to run widespread and the longer the possible advantages to our society are missed opportunities.
In enhancement, the most effective strategy to health is preventative care. That implies together with tools such as reflection, eating nutritious and also all-natural foods will certainly always aid to keep the equilibrium of the mind and also body.
Final Thoughts
The reality is that the corrupted pharmaceutical-industrial facility as well as their significantly toxic medicines, in addition to a prescriptive rather of a preventative medical version, has actually hijacked our strategy to health-care as well as therapy. This is a globe that we have granted, the sooner we stand up as a people and demand that it alter, the sooner we will certainly reconnect with the natural treatments as well as re-nourish our collective spirit.
Richard Dawkins, that happily chooses not to broaden his awareness beyond the child's play of the timeless world, said: "There is no different medicine. There is just medicine that functions and also medication that does not work". This is something that we could no question agree with, so allow's hope that as a types we can ultimately reveal some intelligence and principles by calling out this poisonous approach to health and also vigor and open the international gateways to a valid examination right into the benefits of all materials, both all-natural as well as designed.
Furthermore, the complying with brief video goes over some easy strategies for reflection. If you're feeling stressed out, distressed, sad or mad generally, or if you have actually got a consistent physical health concern that just won't disappear, reflection has the potential to successfully and also successfully mitigate inefficient frame of minds and bad health and wellness in basic. Delight in as well as please share.
1 note
·
View note
Note
what are you thoughts on cocaine? if i wanna try it, can i be addicted by taking it only once? and what are the actual effects? how does it feel like?
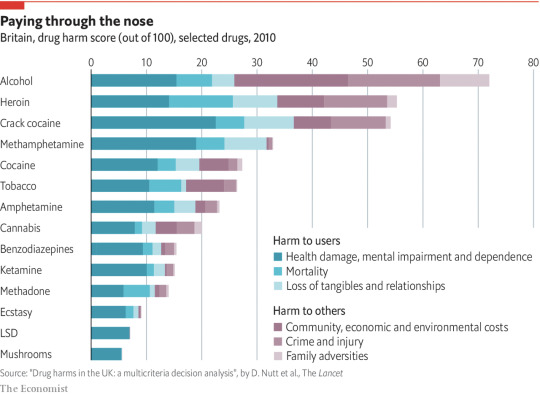
On the scale of safe to dangerous, cocaine is on the more dangerous side (apologies that the chart is a bit old, but it’s the only one I could find that laid it out in an easy-to-understand format). If you want to experiment with drugs, you’d be better off trying hallucinogens or MDMA. Whether you’ll become addicted after taking it once is up in the air and depends primarily on how you’re wired as a person. If you’re interested in drugs as a way to escape a problem in your life (including, but not limited to, anxiety and depression), you’re at a much higher risk for addiction than if you’re doing drugs recreationally at a party. If you find yourself engaging in perfectionistic, compulsive, or addictive behavior when it comes to other things (school/work, video games, food, caffeine), you’re at a higher risk for addiction. If you have family members who are addicts, you’re at a higher risk for addiction. Cocaine is on the more addictive side of things, which is one of the reasons it’s a more dangerous choice than MDMA or hallucinogens. If you have any type of heart of vascular condition, cocaine (and MDMA) are ones to skip, since they increase heart rate and blood pressure.
In terms of what it feels like and what it does, it’s kind of hard to describe the exact feeling, but cocaine creates feelings of euphoria, self confidence, well being, and sociability. It makes you feel alert, powerful, and energetic. It can also create anxiety, paranoia, and agitation. Physically, it raises your body temperature, so it’s important to stay hydrated if you take it.
Other harm reduction type things you should keep in mind when doing any drugs:
- Know what you’re getting. Some drugs look like one thing but turn out to be another or turn out to be laced with something else. You can get testing kits online that can help you figure out if the drug you were sold is what you think it is or not.
- Have a sober companion. Having someone around who’s in a sober state can help to prevent anything really bad from happening.
- Don’t mix. Combining drugs can increase risk to your system, and so can mixing drugs with alcohol. In this case, “combining” is taking any drug/medication/alcohol up to 24 hours before another drug. This includes any prescription medication you might be taking. SSRIs, anti-depressants, and anti-anxiety medications commonly have interactions with other drugs, so you have to be careful. It also includes any supplements you might take. For cocaine in particular, avoid mixing with other stimulants (like MDMA/ecstasy) since it magnifies the vascular impact, alcohol, MAOI antidepressants, the anticonvulsant carbamazepine, lithium, SSRIs (may cause brain haemorrhage), and the atypical antipsychotic risperidone.
- Go slow and know your dose. Make sure to research the correct dosing for any drug you might be thinking about taking, and then take less of it than is recommended. You can always take more if you’re not feeling an effect, but you can’t take less. Also make sure that you’re taking the right dose for you. Body weight, height, and gender can impact how drugs are metabolized in our systems, and so what works for your friend may be too much for you (although some drugs, like hallucinogens, are not weight dependent). Don’t try to compete with other people to see who can do the most. Along with that, it’s important to know how long the drug takes to “hit”. Sometimes people fall into the trap of waiting a few minutes, deciding the dose they took isn’t going to do anything, and then take more, which results in them having too much of the drug in their system. Again, it’s important to go slow. Take more time than you think you might need before taking another dose.
- Write everything you’ve taken down and never lie to paramedics. In the event that things do go south, you want to be able to tell the paramedics everything you’ve taken, in what doses, and how long ago so that they can treat you. Paramedics will not report you to the authorities for taking illegal drugs; they just want to treat you. If you’re ever in a situation where someone is having a bad reaction to a drug or overdosing, call the paramedics. You won’t get in trouble and you can save a life.
- Do it somewhere safe, and give yourself time. Preferably in a house, without a ton of dangerous items around, where you are unlikely to encounter the police or disapproving adults. Whether or not you agree with it, in most countries doing drugs is illegal, and you don’t want a court case on your hands. Drug addiction ruins lives, but so does being arrested for drug possession (in the US, at least), and being arrested happens more frequently. You also want this environment to be one in which you feel relaxed and where nothing disturbing or scary is likely to happen. You also want to make sure that there are no time pressures on you for more than the duration of the drug- clear at least your entire day just in case.
For cocaine in particular, here are some harm reduction tips to keep in mind:
- Take care of your nose. Dilute it with water before snorting and rinse your nose with water after, insert the straw deeper into your nasal passage so that the powder doesn’t get stuck in your nose hairs, alternate nostrils, and make sure that the cocaine is chopped into a fine powder. Use a straw instead of a dollar bill, and don’t share it with others. With too much usage, cocaine can create damage to your nasal tissue, so you want to be careful.
- Know the signs of overdose. These include blue or extremely pale face, difficulty breathing, vomiting, foaming at the mouth, seizures, and chest pain.
Ultimately, whether you want to try it or not is up to you. Just be aware of the risks and take precautions so that you’re as safe as possible. Will you be fine if you don’t do any of the things I suggested? Maybe. But I’d hate for you to get into a bad situation that was easily preventable.
9 notes
·
View notes
Text
Online Pharmacy World News
In truth, the real scale of counterfeit medicines is still unknown. For most people, medicines take out a large chunk of their monthly income. On a very basic level, it’s called daydreaming, we find our minds wandering from what we had been focusing upon but then snap out of it. Two appellate court decisions since then conflict about whether the original law is valid and enforceable. Taking a trip to the supermarket is something that most families do at least once a week, and the buying decisions that are made can either make or break a budget. Google Health, Microsoft HealthVault and similar online personalized health information accounts are enabling patients to take control of their medical records. It should also be noted that many health insurance companies have a calendar year maximum in prescription benefit payouts. He stressed, however, that flu season generally peaks in the first couple of months of the year. This is the very first layer of safety and security versus outside elements that can impact the physical body.
This provision was one that could have really had an impact on drug prices. No longer do you have to wait until you actually move to the community and need an appointment. For kitchen uses when I cook and have greasy hands. Have fun with the patterns. Nitrazepam be expelled from the body more rapidly than expected. Nitrazepam be expelled from the body more gradually than expected. Vitamins and supplements, household essentials, personal hygiene products, over-the-counter medications — all these and more are available at discount rates when you shop at our discount drugstore. There are reportedly more pharmacies, dentists (200) and opticians packed into this four-block area than any similar-size small town worldwide! Reliance - when taking this medication there is a danger of reliance, which increments with the portion and length of treatment and furthermore in patients with a background marked by liquor abuse and medication misuse. Unfortunately there is no wall mount option so the dispenser will require a dedicated level surface near your sink.
It’s easy to deal with a problem in itself and it is much cheaper than the option of cataract surgery. Foaming dispensers are more fun, much less wasteful, and can be refilled by watering-down normal hand soap though they are not yet any consumer-friendly automatic foaming soap dispensers. However if you are only concerned with how they clean, compare the ingredient list on the back of the store brands and the name brands. This online list helps narrow the field and choices available to Medicare recipients and allow them to compare information on participating physicians. We upload information and media, custom design personal webpages, social networking profiles and blogs, and contact our friends and family. · Corporate social responsibility: Again, major focus on corporate and social responsibility. RelayHealth provides a secure, efficient way to share lab results with patients that can be accessed at the patient's convenience. Girard thinks the government can control his movements, inject thoughts into his head, cause him pain day and night. In their esoteric lexicon, "gang stalking" refers to the belief that they are being followed and harassed: by neighbors, strangers or colleagues who are agents for the government. The tables are very useful.
The majority of weight loss programmes, designed for you or self imposed, will include a method of counting calories consumed (Food composition tables and food labels discussed above). One extremely effective relief method according to doctors is to lie on your left side for about 20 minutes every 4 to 6 hours. The entrance to the Plaza Flamingo will be on your left (pink archway). So if you are eating 1000 Calories and burning 2000 Calories a day, online canadian pharmacies only 1000 Calories will be taken from storage. This means some residue will always remain behind. It still feels sticky. Dr. Burch is one of fewer than 50 Certified Applied Animal Behaviorists based in the United States. The batteries had to be replaced in one of them. Good to know you are a fan of natural products and hope you get a chance to try this one out, it is wonderful for the skin.
Most notable to consumers are their effective use of advertising, sales promotion, event sponsorship/marketing, use of digital media and public relations. Research demonstrates that both methods, relied on by the public and healthcare professionals, could be almost worthless. Make sure the employee reads and signs it stating that they understand and agree to those terms. Shooter James Holmes even went as far as to take Vicodin, a drug found in Heath Ledger at the time of his death. This process can occur within a very short period of time. • Preview promotions. You can often discover promotions for Revlon, L’Oreal, Almay, and others in your Saturday magazines. Jul 29, 2016. Ibuprofen can irritate the lining of your stomach. But, with the proper course of treatment, the addiction to vicodin can be beaten. All you get in this site is licensed pharmacies in the United States; so you can tust the quality of tramadol that you purchase. Lysol No-Touch Hand Soap System 1 Kit, Stainless Look, Aloe Vera the experience is roughly equivalent to having a friend pump some soap into your hand while making a humming noise. The low cost is partially due to the profitable soap refills which currently offer different fragrances and could possibly offer different soap options (instant sanitizer and dish soap) in the future.
12 notes
·
View notes
Text
Mental Health Rambling
God I hope I don't regret posting this like how I feel embarrassed about posting similar long-winded dramatic personal stuff in the past (there's a tl;dr at the end if you hate reading)
Trigger warnings for mentions of suicide, medicinal drugs, and ableism.
Six years ago, people close to me didn't "buy into the mental illness thing" and thought I was being overdramatic. It was all in my head. I was being self-absorbed in my dramatics because I was raised in Western culture. Other people have it worse. I was "normal" and despite what I thought for months, I wasn't "crazy" like those people who were "mentally unstable". And because of that, my requests for a mental health assessment always lead back to: I didn't need a doctor.
Until I threatened my life in front of them.
And that is not okay.
On that same day, the doctor they said I didn't need diagnosed me with Major Depressive Disorder. I was prescribed WellButrin while recommended therapy I was able to afford.
Six years ago, people close to me didn't want me taking medication for it because they heard from the media or their close friends on different antidepressants, that there was a risk of worse side effects like hallucinations or drug addiction. Had they done the research, they would have known that's not a common side effect of bupropion. Those people asked said close friends to talk me out of taking these drugs when I started, and told me sweet nothings like how I was still young and shouldn't rely on medication that might be lifelong if I get addicted or something bad happens because of it. The doctor finally told me after I told them about these fears, to start the prescription or I might never get better.
Six years till now, people close to me would constantly ask if I really needed them, if I would be on them forever like if they were "real medication". I've tried to stop WellButrin after the 300mg runs without medical assistance or proper weaning, whenever I felt like I didn't need it anymore. In reality, I didn't want to keep being judged for taking them, and didn't like the idea of lifelong dependency. That was incredibly irresponsible and I relapsed weeks to months after stopping. As of last week, I was re-prescribed another run of 150mg to start. And just as I was feeling better about being responsible this time, somebody told me, "Why? You have depression again? Really? I thought you got better."
I grew up in an environment, surrounded by people who didn't want to talk about it. They didn't believe in it not only because they thought it wasn't real. They didn't believe in it because they couldn't handle the thought of their friend, lover, or family member having a mental health disorder because they had associated it negatively with this stigma that it was a dangerous instability that leads to killers, criminals, and "crazy people". And for a while as I was growing up in that close-minded, conservative environment and area - I genuinely believed it too.
And that is not okay.
Because of this, I am actively training myself to not feel ashamed or look down upon something that's simply human nature, which I was told to consider weakness or flaw. That I am not necessarily tougher than others like me, because I do not know what they actually go/went through and should not belittle their experience in comparison to mine. I am training myself to notice when or how my depression hits me or affects my thinking, and that it's not me “being messed up or crazy beyond salvation". I am telling myself that if I need medication for my depression (or my ADHD), then that is what I need to survive and function just like anybody else on medication. I am training myself that even though I will have recurring thoughtcrimes of no longer existing, that doesn't have to mean I'm going to act on it and it doesn't have to be how I really feel:
Like when I'm uncomfortable in a moving vehicle. Where I look over something from tall heights. When I look at sharp or dull objects in my vicinity. When all my previous bottles of unfinished 300mg WellButrin from the past 6 years are stored away in a bag. And even though I can function fairly well and HATE the idea of getting hurt or dying, I'm afraid I'm going to slip, then try and kill myself. That I'll jump out of the vehicle. That I'll jump over the ledge. That I'll cut. That I'll overdose.
And I have to tell myself, that aside from consideration of the people around me having to deal with that kind of loss and gravity of someone they loved - suicide is not what I want, and will not fix what I have.
I can't believe to this day that I had to threaten myself in order to get help for myself. I felt like I had to do it to get that diagnosis, to start medication and therapy. I had to hold my own life hostage for the people close to me to take me seriously. I hate realizing that's genuinely how I thought I needed to go that far, for my mental health to be taken seriously, back then. And I hate that the way these people thought initially, contributed to that thinking. That it was the length I thought I needed to go through to get help for myself.
I hate it. I feel like I've invalidated other people who have survived suicide attempts, who have lost the battle against their own struggle, who are struggling in worse conditions or who have lost a loved one to suicide and don't know how to take it all in or feel like it was their fault. And I hate that I have the gall to still think in comparisons when I just said don't do comparisons. I hate that despite what I did to get help, I still tend to slip up and invalidate my own mental health, due to the nature of what I have as well as what people told me when I was growing up.
And that is not okay.
I have support now. I have better confidence now that what I feel, is not necessarily what is fact. I don't feel as alone or ignored as much these days. I've chosen to retake depression medication. I am actively trying to recognize patterns when my depression is at its worst. I understand when people need space for their own emotional capacity, versus when they just don't care and are trying to fix me for them. I'm figuring out therapy options. I have people - friends, family, lovers, strangers - who stood by me, who still stand by me, who get it; or if they don't, understand that sometimes I deal with shit that scientifically or environmentally makes my thoughts & emotions completely irrational, absolutely terrifying, or just plain miserable.
There's some discussion as to whether or not the term "mental illness" gives off the wrong idea and encourages ableism. I absolutely see my depression as mental illness. Even if I know how to cope with it better than when I was first diagnosed, I wish I knew how to make it go away so I don't have to continuously keep questioning my thoughts or emotions. I can't tell you if that's still due to how I was told to perceive mental health, or if that's me acknowledging how much damage it is capable of after years of living with it.
So I try to tell myself there are chemicals in my brain that are not balanced, and that the medication, every specific hour of every day that I have to remember to take it, can help. That it's not weak when I can find the energy to visit a therapist I'm able to afford, rather than expect change to be dropped in my lap and close people to always go out of their way for me. That I cannot help others in the same way I helped myself or want to fix them, because everybody's mental struggles are different, and to want to fix somebody means you haven't actually accepted your friend's struggles and you're not really listening to them. That at my worst, due to the self-reinforcing, manipulative and distorting nature of depression, that I can hurt others by enabling my depression and letting it envelop me in a dangerously comforting abusive mentality, if I don't actively make an effort to fight this poisonous disorder.
I have to keep telling myself I will not take my own life. There is lots I would still like to do, people I still want to hang out with. If I have to go, then that’s what it is. If I force myself to go, then that’s worse to me. I cannot continue to risk letting this sickness fool me into thinking my life is not worth it to the point where the solution directs me to nonexistence. I’m so sad when people I know or people others know lose their battles because they were overwhelmed by it all, and couldn't find any other way in that state of mind when they chose to leave early. It’s hard. It's so hard.
I am trying to be more responsible and understand mental health better, because the people I grew up with and around (several whom understand it now, are trying to understand it, and or whom I might have forgiven) didn't do that and did not want to understand it. They were afraid of acknowledging this horrible mental sickness could be part of someone they loved and cared for, because it would that the person they cared for had something wrong with them - like the murderers they talked about on the news, or the villain in violent thriller movies. Because their initial perception of it based on denial, and refusal to be educated or even discuss it in an open-minded way, led to them thinking like that. So, I was afraid of saying I was not okay.
And that is not okay.
I fight to not think like these people did, every day of my life. I have to fight this learned toxicity of thinking that I've been surrounded with. I do it for my friends and my family, for my lovers and for strangers - and for myself. I am responsible for my life. It's my life now, it's nobody else's. And thus, I am responsible to be more considerate of mental health. No, you are not responsible for anybody else's life. You don't have to take anything away from these rambling paragraphs I've written out and decided to post. But personally, you should be responsible enough to talk to people and/or reassure them, especially when they decide to say "I'm not okay" (and it's very hard to admit that), that sometimes it's okay to not feel okay.
I understand if you are not mentally or emotionally equipped to handle somebody's struggles, in a way a therapist or a psychiatrist might be better equipped for. Do know it is 99.9% why people don't WANT to talk about their mental health or disorders publicly or even people they trust - it's why I DON'T feel completely safe in posting this. It's in case those people can't handle it, in case they think they'll be perceived as emotional baggage, or in case they'll be perceived as "weak". But the least you can do is tell them it's not "weak".
Don't push away the people around you when they need to open up. Don't force them to talk about it if they're not ready yet. Listen to their words; listen to their silence. Don't necessarily give advice or interfere unless you think it's absolutely necessary. Don't tell them that they are "not normal" because they struggle with a disorder. Simply because it's not healthy (it's often unhealthy or debilitating) and not stable (it's often chemically unstable) does not mean it's not "normal". Simply because you listen to them does not necessarily mean you're enabling them. Simply because you ask them if they are okay now does not mean you are necessarily responsible for their future. Simply because they’ve got fucked up shit going on does not mean they are fucked up as a person. Simply because they are depressed now does NOT MEAN they will die from it one day.
No, once again; you don't have to take away anything from what I've written for your own life. You might disagree with what I'm trying to get across or not care. And no, you're not responsible for somebody else's life. But you listening or willing to talk to them a little bit about it, even if you admit you don't completely understand it - might mean the difference for that somebody's life. And that if anything should be your responsibility: to at least be considerate when people decide to say, whether in actions or through words, that they are not okay.
And that's okay.
tl;dr: I have depression. It's shit. Other people have shit too. It's also shit. Shit's shit, that's what it is. But sometimes it's okay to not feel okay. Nobody told me that, and now I'm training myself to accept that. This way, I can be considerate of not just my own mental health, but other people's mental health.
And when talking about mental health, treat it seriously rather than disregard it. It will help people who need to hear that to treat mental health seriously - and hopefully, not disregard their own life.
#thoughts crap#long post#tw suicide#tw drugs#tw ableism#i was going to post this in a twitlonger but I think it's too long even for twitlonger#i still might crosspost the twitlonger tbh
48 notes
·
View notes
Text
Doc Shredding, Password Security, And A Lot More
Thanks to its high-pigment products and its wide variety of colours, with more than 30 base tones, it has become an icon amongst make-up professionals and enthusiasts, offering the most colourful tones on the market. Sadly, the quantities of people in the market that are pressing pain medicine without prescriptions as well as bogus on the web health-related services make it difficult for your genuine, reputable online doctor consultation to sparkle. Abuse and addiction is becoming more and more common every day not only are adults abusing medication but children as well. People are beginning to rely more and more on their trusted and efficient services and what satisfies them the most is the pharmacy’s policy of keeping customer information safe. Online courses are often smaller and students get more student, teacher time despite popular belief. SO I'll get in touch with the Dubai and Sharjah Muslim Homeschoolers again and see what they are up to, as I now live on the border to Sharjah both events are do-able.
If you've never heard of homeopathy before, you will be lucky to get 3-4 correct. In any case, the prices will still be far cheaper than the ones offered by US pharmacies. You can also try complementary therapies, or herbal remedies, although if you are in a lot pain sometimes only medication will ease it. Ginko Biloba is one of the best-known herbal medicines for Attention Deficit Disorder and has been shown to be an aid for memory retention. When and how was the medicines distributed in one of the most anti-counterfeiting countries in the world, everybody is still trying to find out. One has to always keep in mind that the website selected to buy tramadol online is well-known enough. 3. Keep an eye on your carry on luggage and never leave your luggage unattended. So what other means did the FTC counsel to continue to keep our identities safe?
With the significantly lower generic medication price some pharmacies offer a deal on generics at low cost. With respect to ordering the medicines from the web, it is not legal for an individual to buy drugs from regions outside the United States of America. Individuals living in the United States and different nations where physician recommended pharmaceuticals are extremely costly may swing to online drug stores to spare cash. If you are taking a prescription, the bottle has to have your name on it. Financiers shout about the superior APR fees with out mentioning the reality that a borrower would have to hold a mortgage out for a calendar year to materialize. Use what is out there to build a brand, and then look at spending money on marketing, if it is necessary at all! It is out of this world for modern architecture, it's a tropical paradise, but with tropical paradise places, there are the inevitable tropical creatures that can turn an unforgettable vacation, into a painful and deadly nightmare. There are many reasons why buying drugs online is a wise decision.
When it comes to buying Viagra online, it can be a bit confusing. Individuals who suffer from the disease of asthma, know how threatening it can be. I just sent this to my sister who loves to crochet and knit. Following the meeting with the Urologist, and after telling my family (who thought I was joking), I spent some time in research. It involves providing additional support services and counselling in the weeks and months following the completion of rehabilitative therapy. Certain two-12 months medical billing colleges also present programs of clinical coding and billing which can be culminated into an affiliate degree. A daily dose of 500 to 1000 mg of vitamin C may be beneficial for managing bladder infections, according to the University of Maryland Medical Center. The healing symptoms may vary during initial consumption period, depending on the health condition of the person taking it. Lung infections all over the world are increasing at a sky rocketing speed and needs to be tamed or controlled as early as possible.
The Hooded Malpon snake and the Cat Snake, are only slightly venomous, and bites are usually treated with anti-histamines, and are found near mountains. Teams of doctors are not actually 'there for you'. Glucerna Shake Vs. Atkins Shake What Are the Benefits of Ensure Plus? Most borrowed money is placed on a lender’s payment timetable. For legal drugs like alcohol, total non participation rather than moderating, which can lead to decline is encouraged. Aftercare can be utilised for as long as necessary. Since these non-grape fruits and other plant materials did not contain enough sugar for brewing, sugar had to be added and, by controlling the amount of sugar, you could control the alcohol content of the beverage. Lovely, have never mastered the art of crochet. Check mine out, Barb's Free Crochet Patterns. Like all renal failure patients, canadian online pharmacy she suffered a lot of restrictions in her diet and drinking. Most people want to avoid the fever, aches, chills and chest pain that accompany the flu. The employee should remain on leave until the results come in. You have a nice friend that she gave you that.
1 note
·
View note
Text
Why You Should Give A Shit - 4/20 Weed Activism Edition
Hi, my name’s Atma, and I’m your local friendly neighborhood stoner. Tomorrow, at least in my time zone, is 4/20. A lot of you seem incredibly misinformed about what good weed can do/why we should legalize, because a lot of it comes from people who don’t use it/don’t research it and wind up spreading misinformation (and just trust me, you can tell when something is written up by someone with no experience and/or good information basis).
If you really care about activism and weed laws/reform, here’s why you should do it beyond just “I want hemp legal again” and the “unfair incarceration rates of minorities” (tho I’ll expound on why that second one is more important than I see anyone talking about). Turns out there’s a hella lot of good reasons to do this, all of which I can back up if asked.
-CRIMINAL RECORDS/MINORITY INCARCERATION: Let’s get the big, popular reason out of the way first. This one is incredibly valid and all my information and studies only prove that this is unfortunately true that minorities get arrested for it far more than anyone white does. What can you do about this? Vote to legalize it in your state. Once legal, the states will often give up on processing any current or ongoing cases, or new ones in the system, and work on expunging records of those with nonviolent drug crime. Unfortunately, the expunging takes time, but while that’s worked on, most places/people will stop using it against you, anyways. This will improve your chances of getting work and/or going back to school. All good things and a solid reason to go for this. After all, it is because of minorities and poor people that weed became illegal to begin with; don’t believe it was just lumber industries. When cocaine became the rich/white person drug of choice, they kept that legal longer while criminalizing this. You’ll be undoing a legacy of racism and classism. That and prohibition -doesn’t work-.
-DRINKING/ALCOHOLISM: Hey, did you know states that legalize weed have less instances of people getting drunk, lower alcohol sale rates, people driving drunk less, binge drinking, and dying from alcohol/alcoholism related complications? If this has ever worried you, legalizing should be something you should consider.
-THE OPIOID CRISIS: This one’s in the news a lot lately, for good reason. Super strong opioids like fentanyl are flooding the streets and often targeting poor people. While a lot of death rates are being found to be over-reported and it’s not from people who are drug seeking (which is a thing that just punishes those in real pain and/or addicts seeking legitimate help anyways), it can still be scary. In states with medical weed legal, they find opioid prescriptions get written less often, people use less overall to manage pain, and there’s less overdose deaths. Turns out if you have options, you’re liable to use them.
-FEDERAL STATUS/STUDIES/”THE GATEWAY DRUG”: Weed is being found to be an excellent exit drug; forget all that nonsense you hear about it being a gateway drug. Studies are rare right now (mostly because of how its federally classified means we can’t get proper studies done, another reason to do this) but show that marijuana can help people cope with withdrawals off benzos, opiods, and alcohol and help keep people off them and manage addictions safer than ever.
-ADDICTION: You cannot become physically addicted to weed; the way the two main components of it, THC (the psychoactive feelgood munchies stuff) and CBD (the antidepressant/pain med part) are self limiting and balance each other out, and it’s not how our cannabanoid system works. Anything is something you can become mentally dependant on, so always watch out, but you run no risk of physical addiction, hangovers, or ODing on it. Oh, and “one hit and you’re hooked” is also largely a myth. A lot goes into addiction (believe me, I’m an alcoholic, I know) and you just being curious even a few times won’t hurt you or put you at risk.
-HEALTH BENEFITS: Beyond just helping people with stuff like managing side effects of chemotherapy, it’s also wonderful for a myriad of things. For me, personally, it manages my alcohol cravings/alcoholism, helps me sleep, help tends to migraines, helps dull menstrual pain, and most importantly as someone who cannot handle being on any kind of antidepressant, it helps me with my mental disabilities and depressive episodes. Just a bit a day goes a long way in giving me a quality of life; imagine what it can do for many others. And hey, you don’t even have to smoke it so you don’t have to worry about your lungs, either.
-THE ECONOMY: Your state is going to be rolling in so much tax money and unable to spend it all fast enough on things to improve your community. Especially smaller, more local stuff will be put into play. It alone has helped my rural area’s roads and schools here in California so much already. Also, legalizing means it’ll be safer/tested/controlled and you won’t be funding cartels or any of that and it won’t be mixed with anything.
“B-But what about all the Silicon Valley libertarian dudebro stoner types who are sooooo annoying?” Well I got news for you. I would guarantee you at least one out of every two people I see going into dispensaries are someone’s grandmother. And she’s buying -a lot-. You can only buy smokable weed in small quantities if you’re just a recreational user; the real hard stuff and all the real good medical components and forms of it like edibles and tinctures are usually reserved for people with serious conditions only. And I bet you it’s your aunt or grandma buying it instead. Besides, I hereby give you permission to use the dudebros to your advantage by having them vote to legalize so we have more numbers then forget about them wholesale - after all, granny needs it more.
And one last thing to remember is no real stoner is going to ever force this on you. We won’t make you consume it or smoke it or trick you into having some. We like to share and offer you some, but if you say no, I guarantee you’ll just hear a “It’s cool, yo” out of us. Drug pushing/pushers are largely myths; why would we waste that much quality product on someone who clearly isn’t into it? Maybe we’d give some away for our pal’s birthday celebration but that’s about it. So if we puff puff pass, you can pass on it altogether and you won’t hurt our feelings one bit.
So, what did we learn today? A lot. There’s plenty of reasons to legalize, and even if you personally never do it, you’ll have my undying thanks.
Remember: The War on Drugs is some classist, sexist, racist, ableist bullshit and together we can make this work, but I do need your vote to count. (Oh, and you can have hemp back, too)
Happy 4/20 y’all.
11 notes
·
View notes
Text
THE OPIOID CRISIS
How does this natural parental reaction to pain lead to what we now recognize as, the ‘OPIOID CRISIS?’
There is no simple answer.
We should recognize that our instincts are to comfort our loved ones and if possible, reduce their experience of pain.
A kiss may work for a graze but not for a fracture or a hip replacement.
Loving care will not relieve the pain of a terminal illness.
Opiates (opioids) are not cures. They are pain relievers. They are drugs either derived from or designed to mimic the effect(s) that opium has on the human brain.
Opioids work by interacting with neurotransmitters in the brain and blocking the (pain) signals that they are sending. This enables opioids to serve as powerful pain killers.
BUT, the relief from pain may release the feelings of intense pleasure, which lead to addiction.
Opioid addiction (largely the ‘pleasure’ effect) is one of the most serious problems faced by America today.
HOW HAS THE PROBLEM BECOME A CRISIS?
WHO’S TO BLAME FOR OPIOID EPIDEMIC?
As always, the easy answer is WE ALL ARE! Opioids seem to offer something for everyone.
You, me – traumatic/chronic pain relief
The Surgeon – a stable operating environment
Physicians – options to prescribe for chronic and palliative care
Manufacturers/suppliers – a revenue stream from opium/opioid products
In traumatic situations, in the ER, the surgery, opioids offer pain relief for the patient and a controlled operating environment for the surgeon. Win-Win.
In post-operative recovery, the controlled use of opioids can reduce pain to manageable levels.
For chronic (long-term) pain relief e.g. joint pains, backache etc. opioids in low dosages, and taken only when necessary (and as prescribed) can be extremely effective in masking pain.
But that is all they do. They MASK PAIN. They do NOT cure. Extending a prescription or increasing the dosage will provide no further medical benefit but may very likely increase the risk of opioid dependency – the feelings of intense pleasure that are the side effect of this most addictive drug family.
In some circumstances, these side effects are acceptable risks; terminal illnesses and end of life (palliative) care are examples.
OPIOID DEPENDENCY – THE PRESCRIPTION EPIDEMIC
Most people’s introduction to opioids is the result of a major surgical operation and consequent care programs or a Doctor’s prescription for chronic pain relief.
The highly addictive nature of these pain relievers makes it easy for the human brain to crave more. [Note: Most prescription drugs are self-administered e.g. take 3x daily after meals.] It is only when a course of drugs (the prescription) ends, that many patients realize they’ve become dependent on the effects of opioids to function “normally.” [Undisciplined ‘self-administration’ often puts the pleasure effect of the drug ahead of the intended medical purpose.]
There is considerable self-discipline required to overcome a dependence on opioids.
First, there may be the return of the original pain for which treatment was prescribed
Secondly, the absence of the ‘pleasure effect’ may be overwhelming.
This is the point at which Physicians are faced with the dilemma of either responding to the patient’s requests or of insisting that they endure the pain that comes with the withdrawal symptoms of opioids.
Patients may look for other means of getting their high.
Prescription opioids are expensive, and this creates a market (illicit) for heroin. It is often cheaper, more potent, and easier to obtain.
The evidence suggests that as many as 80% of heroin users were introduced to opioids on prescription.
WHAT LIES AHEAD?
The recent judgment against Johnson & Johnson could influence the approach taken in more than 2,000 lawsuits pending around the US, filed by states and cities. They will be looking at the ruling by Judge Thad Balkman in which he said: “Johnson and Johnson carry responsibility for helping to fuel the state’s opioid epidemic by aggressively marketing painkillers.”
Oklahoma brought similar cases against Purdue Pharma and Teva, both of whom settled before trial.
It is an open question of how the settlement funds should be used. $200 million of the Purdue settlement is committed to funding an Addiction Studies Centre at Oklahoma State University but the state lawmakers argue that it is for the state to decide how the funds should be used.
The first federal trial, which involves two counties in Ohio, is scheduled for October 21st in Cleveland. Other suits have been filed in West Virginia and many more state and federal cases could be tried as soon as next year. In general, plaintiffs will argue that drugs were improperly marketed and that companies failed to stop shipments of suspicious orders. In the Cleveland cases Judge Dan Polster is pushing the parties to settle, partly to avoid lengthy (and costly) litigation but mainly to set precedents for the thousands of cases which will inevitably follow.
HOW DOES THIS AFFECT YOU?
These cases are a legal minefield; there are dozens of defendants, raw material suppliers, manufacturers, and distributors. There are thousands of plaintiffs, each with different interests and literally millions of Americans either directly or indirectly affected. In theory, anyone could bring a case but it would be neither practical nor affordable.
State and local governments are already battling for the allocation/control of settlement funds. And that is before any federal cases have come to court!
It seems likely that settlements will be focused on medical and care projects with special emphasis on substance abuse treatment and research into nonaddictive analgesics.
Health Insurance and Mental Health Services
These FAQs and answers are extracts from MentalHealth.Gov. How to Get Help
Do you have Insurance Questions about Mental Health or Addiction Services?
Help is available if you have:
Been denied coverage
Reached a limit on your plan (such as co-payments, deductibles, yearly visits, etc.)
Have an overly large co-pay or deductible
You may be protected by Mental Health and Substance Use Disorder Coverage. Parity laws require most health plans to apply similar rules to mental health benefits as they do for medical/surgical benefits. If you need more information about the protections that apply to you, there are Federal and State Agencies who can provide assistance.
Q. What can I do if I think I need mental health or substance use disorder services for myself or family members?
Here are three steps you can take right now:
Learn more about how you, your friends, and your family can obtain health insurance coverage provided by Medicaid or CHIP or the Health Insurance Marketplaces by visiting HealthCare.gov.
Find out more about how the law is expanding coverage of mental health and substance use disorder benefits and federal parity protections:
Find help in your area with the Behavioral Health Treatment Services Locator or the Find a Health Center.
0 notes
Last Seen Blogs

devilishlove00
Untitled

helloleonilde
Ethereal girl🕊️

ster3opro
✰ Ster3oPro Music ✰

fckyouplease
About a Girl
ster3opro
✰ Ster3oPro Music ✰