#public health (medical specialty)
Text
How to Tell If Your Cat's Teeth Are Hurting
New Post has been published on https://petn.ws/2TzZs
How to Tell If Your Cat's Teeth Are Hurting
Photo: Monika Surzin (Shutterstock) Maintaining healthy teeth is obviously important for us, but the same is also true for our cats. Although we may not think about a cat’s dental health quite as often as ours—and attempting to brush their teeth can be its own battle—cats can develop their own dental issues, including abscessed teeth, […]
See full article at https://petn.ws/2TzZs
#CatsNews #PeriodontalDisease, #Ball, #CherylLaBall, #DentalExtraction, #DentalPublicHealth, #Dentistry, #Gingivitis, #Health, #HumanInterest, #HumanTooth, #Lifehacker, #Medical, #MedicalSpecialties, #OutlineOfDentistryAndOralHealth, #Pharma, #RTT, #TeethCleaning, #ToothPathology
#periodontal disease#ball#Cheryl LaBall#dental extraction#Dental public health#Dentistry#gingivitis#health#Human Interest#Human tooth#Lifehacker#medical#Medical specialties#Outline of dentistry and oral health#pharma#RTT#Teeth Cleaning#Tooth pathology#Cats News
0 notes
Text
Ohio's mental health authority is trying to ban transgender healthcare - esp for people under 21 years of age, BUT they are asking for public input! Hurry, though, as it's only through 5pm local time (US Eastern Standard Time) on January 19th!
Changes to the Ohio Department of Mental Health and Addiction Services rule, "5122-14-12 | Private Psychiatric Hospital: Program, Specialty Services, and Discharge Planning", are to prohibit any kind of transgender care for those under 21 in a psychiatric hospital. Full document here, but be aware it is to a pdf

The rule includes the text, "Medical services shall not include any of the following: ...the prescribing, administering, or furnishing of any prescription drug or hormone...", which means if someone under 21 enters a private psychiatric hospital and who is already on puberty blockers or hormones, the doctors there would be prohibited from giving them the prescription they already have.
A new proposed rule for the same Ohio department, "5122-26-19 | Gender Transition Care" states the requirements for anyone needing transition care under this department. They are targeting the most vulnerable with these rules: young people who have mental health issues who also need transgender care. Full document here, but be aware it is to a pdf
Included in this rule: A doctor may only provide transgender care after three requirements have been met - a psychiatrist who has experience with the patient's age group must be employed by/contracted with the provider, an endocrinologist who has experience with the age group, and the provider has a comprehensive written plan that includes a detransitioning provision.
It also requires any such patient to have a thorough mental health evaluation and counseling period of at least 6 months prior to any transgender care. It also appears to become part of their medical record.
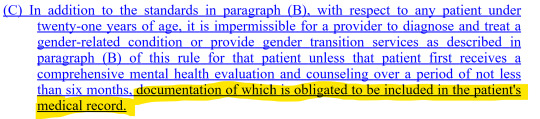
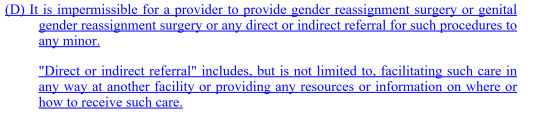
In addition to a ban on any transition surgeries, even if the patient jumps through all of those hoops, is a curious item that prevents doctors from referring patients out to other doctors that can provide care:
Another thing that made me pause was what seems like a scare tactic:
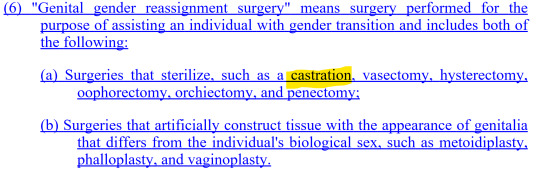
The terms "orchiectomy" and "penectomy" mean the removal of testicals and penis, respectively. The word "castration" could only be redundant or referring only to chemical castration, which seems to not fit in with gender reassignment surgery (correct me if you know it does fit). "Castration" is a scary word for most people with penises. I think it would likely provoke a knee-jerk response, like, "Oh, no, castration is bad. No castration! Enact these rules to keep people from being castrated!"
⚠️ The time is now to tell the Ohio Department of Mental Health and Addiction Services what you think about this! ⚠️
The option to comment on these needless restrictions can be found at the link in the first paragraph, but it's just an link that takes you to your email app. You can also just email them directly at [email protected] no later than 5 pm EST on Friday, January 19, 2024.
Please reblog to get this message out! We all have a stake in how rules and laws are enacted. They often lead to more in other states/countries. So, even if you don't have a stake in this personally, please make sure others see it.
Why do I care? I don't live in Ohio, but I have friends all over, including Ohio, who need transgender care. You might know someone like that, too.
#transgender#trans healthcare#ohio#ohio law#lgbtq+#comment#comment period#mental health#transition#transitioning#transgender healthcare ban#ban
449 notes
·
View notes
Text
Sen. Elizabeth Warren, D-Mass., "is at long last acknowledging that ObamaCare has increased healthcare prices" and created other unintentional consequences, the Wall Street Journal editorial board wrote Friday.
Warren, who has long supported the Affordable Care Act, the official name for ObamaCare, has recently come to an "epiphany" about "industry consolidation and price increases caused by the healthcare law," per The Journal.
A letter to the Health and Human Services Department inspector general was aimed at determining if "vertically-integrated health care companies are hiking prescription drug costs" and are "evading federal regulations."
In a bipartisan letter, she and Sen. Mike Braun, R-Ind., complained "that the nation’s largest health insurers are dodging ObamaCare’s medical loss ratio (MLR)," according to The Journal.
As Warren describes in the letter, health insurers have exploited the situation, making for "sky-high prescription drug costs and excessive corporate profits."
"In functioning markets, generic drugs cost 80 to 85 percent less than their name-brand equivalents, giving patients much-needed relief from high drug costs and saving taxpayer dollars," Warren wrote. "But patients – including patients in public health care programs like Medicare and Medicaid – who either use or are compelled to use vertically integrated specialty pharmacies are not seeing this relief."
The senators continued: "By owning every link in the chain, a conglomerate like UnitedHealth Group – which includes an insurer, a PBM, a pharmacy, and physician practices – can send inflated medical payments to its pharmacy. Then, by realizing those payments on the pharmacy side – the side that charges for care – rather than the insurance side, the insurance line of business appears to be in compliance with MLR requirements, while keeping more money for itself."
The Journal explained that despite Democrats arguing that the MLR would help patients, "the rule has spurred insurers to merge with or acquire pharmacy benefit managers (PBMs), retail and specialty pharmacies, and healthcare providers."
"This has made healthcare spending less transparent since insurers can shift profits to their affiliates by increasing reimbursements," the board wrote.
Warren has voted against ObamaCare repeal efforts over the years but also pushed for a "Medicare for All" proposal when she ran for president in 2020.
Warren's office and HHS did not immediately respond to a request for comment from Fox News Digital.
99 notes
·
View notes
Text
How the Heartsteel members would take care of a sick/injured S/O.
Inspiration: Extremely self-serving, but I don’t care. I’m currently in the midst of a chronic illness episode. For me that involves an ungodly headache that can last for straight days, if not weeks, and other bs. All because my body can’t handle sodium 😭. If I don’t do something to distract myself, I’m going to cry, and I’d rather not do that, so here we gooooo.
Genre: Headcanon
Type: Fluff (very very slight angst in the concept [if you squint] just because you don’t feel good).
Gender: Gender Neutral Reader
Tw: None! This is pure fluff. 🥰
Aphelios
Aphelios would actually be a great caretaker.
I think a lot of this comes from an excellent example. We know Alune took care of Aphelios when he was injured/after his surgeries. Since he was the recipient of her wonderful care, he knows what to do.
Extremely prepared. He’ll work from your place as much as possible so he can be close by (he has that little mobile keyboard set up shown in his “what’s in my bag” pic). Excellent at running out to grab supplies/medication (I feel like he has an excellent memory so you just need to tell/show him something once). Also phenomenal at making sure you take your meds on schedule and changing any dressings/wraps.
If for some reason an extra set of hands is needed or Phel needs further advice on how to best care for you, you know who he’s texting? Alune! She is happy to help however she can because you’re her friend too and she hates knowing you’re sick/in pain.
I feel like Phel’s immune system is pretty strong so even if you were contagious, he’d cuddle you. If he was really worried, there’s always his mask. (Makes my public health heart sing.) He has many extras so you can snag one too in order to be doubly safe. You get those healing cuddles!
Ezreal
This is where Ezreal’s typical golden retriever energy is extra useful!!
Like genuinely I think Ez is a really really sweet “nurse” and will do an excellent job of taking care of you. Or at the very least, he’s great at distracting you and making you smile so you don’t feel as shitty/in pain.
I can’t see Ez cooking tbh (mood), but he is more than happy to order delivery/run to grab whatever carry out whenever you want it. If he can’t do it because he needs to stay with you for some reason, he’s texting Alune and the boys and practically begging them to help him out. (One of them always does. They love you and want you to heal.)
Also happy to run out to grab whatever supplies you need. This sweet green bean is so eager to help you heal that not only will he grab what you ask for, he’ll also grab other things that you might not need. He’s of the mindset it’s better to be overprepared rather than underprepared.
I can’t see Ezreal wanting to cuddle if you’re contagious, tbh, which is fair, but he’ll definitely make sure you have all the blankets and pillows you need. He will sit near-ish to you though and hold your hand. And if you’re not contagious? Oh he’s clinging to you as much as you want him to.
Kayn
Ok…so…this isn’t Kayn’s specialty as a partner, let’s be honest here.
Kayn is an amazing partner in so many other ways, but he’s not exactly...naturally nurturing? BUT that doesn’t mean he’s not going to try. He knows you need him, so he’s really going to put in a lot of effort to try and take care of you as best he can. (This secretly sweet rockstar!)
Kayn might fake grumble about it, but he will definitely go out and get whatever supplies you need. You may need to take a picture of a label/find one on the internet but he’s got you! (“Baby, there are so many CHOICES. How do I know which is the right one? I don’t want to get something you don’t need!”)
The first time you were sick/injured and he was with you, he texted the HS group chat for advice on how to take care of you and shocked everyone. (That was the moment the rest of HS knew Kayn was really head over heels for you. 🥹 <- Their faces as they read the texts.)
One thing I cannot see him doing is cuddling you when you’re sick (unless you’re not contagious). He doesn’t want to get sick himself. He will tuck you in and give you surprisingly soft forehead kisses though. He says they’re to check your temp but you know they’re to show he cares.
K’Sante
K’Sante is another member who just gives off such excellent and caring vibes. He has to come from a big, close-knit family, because he gives eldest brother vibes through and through.
Because of this, he’s perfect at taking care of you when you’re sick or injured. He’s done the same thing for his siblings/cousins many times.
Even though Sett is officially the best cook, I still fully believe K’Sante can throw down in the kitchen. Whenever possible, he’s making everything from scratch for you. You deserve it, after all. His meals alone will have you starting to feel way better.
He is fully stocked on OTC meds, ice packs, bandages, whatever you need. As a gym bro, K’Sante can get pretty sore, so he’s already got that stuff around for himself. Also, anything you need picked up, he’s got that taken care of.
As the eldest who took care of his younger family members, K’Sante’s immune system is PREPARED. Unless it is before a really big event, he would be fine cuddling you, even if you’re contagious. If it is close to a big event then he’s understandably a little more hesitant (he does have obligations to HS) but he’ll still be nearish to you and hold your hand so you know he’s there.
Sett
Ooooooh baby this is Sett’s time to fucking SHINE.
He was raised by his incredible Ma! Like of course Sett’s going to be really fucking good at taking care of you. (He already does an excellent job of doing that when you’re not sick/injured.)
We know he’s the best cook in the group so homemade soup/whatever comfort food you want/need you will have and it will be delicious. Really good about reminding you to take any meds you need to (he sets a reminder in his phone). Also fully stocked on OTC meds, medical wraps, ice packs, etc. Like he is PREPARED. (Perks of loving a gym bro.)
Happy to give you cuddles if that will help. I feel like Sett is another member that has an immune system of steel, so even if you’re sick, he’s still cuddling you if you want him to. (You definitely do like 95% of the time because how could you not?? Sett cuddles sound fucking elite!)
Worst-case scenario and you get sick while he’s traveling? He makes sure you are in the very best hands possible and sends in the big guns. That’s right, he has Ma come over to check on you/stay with you if need be (which she is happy to do because she adores you and loves how happy you make her son).
Yone
I think Yone would be a phenomenal “nurse!”
He might come across as cold/intimidating to those who don’t know him, but you always bring the soft side of him out. That’s totally applicable when you’re sick. Sweet Yone incoming!!
He cared for his younger brother Yasuo when he was sick or injured, so he is well versed in what supplies are useful for a multitude of ailments. Is well stocked on all of it too. If for some reason you need something and he doesn’t have it, he’s remedying that ASAP.
I’ve been thinking about whether or not Yone cooks. My gut says not really besides breakfast food. While he’s not going to make you homemade soup/your comfort food, you bet he’s asking Sett or K’Sante to make some for you. (They’re happy to do so. You keep your their producer sane. Helping you is self-preservation 😂.)
While he’s likely been injured many times, I feel like this beautiful motherfucker (affectionate!!) has never been ill a day in his life. His immune system is just that strong. Whatever the issue, he is down to give you whatever cuddles you desire. (I’m bringing back my headcanon of cuddly Yone and NO ONE CAN STOP ME 😋.) Enjoy the forehead kisses and sweet little verbal check-ins.
#heartsteel#heartsteel headcanons#heartsteel x reader#reader insert#headcanon#heartsteel aphelios#heartsteel ezreal#heartsteel kayn#heartsteel k'sante#heartsteel sett#heartsteel yone#heartsteel fluff
147 notes
·
View notes
Text
Have said it before, will say it again: I'm no great person. Neither morally nor intellectually. When I rag on all sorts of experts and degree-holders, it's not because I think so much of myself as to imagine I'm omnicompetent, but because I think so very little of them.
So here's my latest bit of ragging on high places:
Opinion: Trust in science is declining. Here’s how we can regain it
Megan L. Ranney, MD MPH, is an emergency physician and dean of Yale School of Public Health. Katelyn Jetelina, MPH PhD, is an epidemiologist, advisor to the US Centers for Disease Control and Prevention
These two Masters of Public Health have correctly noticed a lack of trust. Their proposed patch boils down to: tell people to have more trust, loudly, frequently, and on more channels.
There is no mention of apologizing for mistakes in general, nor acknowledging any specific mistakes made. Nothing about improvements to be made among scientists, neither self-policing nor the lack thereof, nor the replication crisis, et cetera. There is only a lengthy call to communicate better, leading to this amazingly awful sentence:
At the end of the day, if the United States is going to improve our trust in science, we have to ensure that we are all public health communicators.
Problem 1: you take your own perfection for granted, not considering anything you might do to earn trust.
Problem 2: you treat "trust" as a goal in itself, rather than something that should correspond to your trustworthiness.
Problem 3: you equivocate between science and public health.
Problem 4: you call on everyone else in "we" to fix your bad rep.
THESE ARE BAD PEOPLE. DON'T TRUST THEM.
Social media can play a part, too. Work by the National Academy of Medicine, in collaboration with the Council for Medical Specialty Societies and the World Health Organization (with which Dr. Ranney was involved), outlined ways for social media companies to identify and amplify “credible health messengers” — both the professionals and the everyday folks who are volunteering their time to create content. We applaud companies like YouTube that have made this work a priority, and hope that more companies will follow.
A cynical person might describe this in terms of selective reporting and suppressing dissent. The use of "credible" as opposed to "honest" sounds like a spin doctor wanting to make problems go away by rhetoric instead of work. It's not clear how much of the MPH's focus on health, vaccination, the WHO and so forth is déformation professionelle, and how much is a MPH trying to spend down the credit of "science" at large for the benefit of her personal narrow slice of it.
CNN Opinion selects for the kind of people who want to be on CNN, and the kind of people CNN wants to have on, so Ranney and Jetelina are probably not representative of public health, or so I hope. They're still awful people. Their entire opinion piece is a demonstration of why "trust in science" should be low: there is a serial conflation of trust in scientists and trust in experts and trust in credential-holders like Ranney and Jetelina who in turn treat trust as a kind of compliance to be acquired by badgering people.
47 notes
·
View notes
Text
"If you would like to confirm the validity of this campaign, you can message either Bashar or I on Instagram. Our usernames are basharinshasi and darina.bishop and our accounts are public. Here is Bashar's story:
I have carried the dream of studying medicine since childhood, but now that my dream has become more important and my goal of studying medicine has become an unavoidable goal regarding what I saw of the dire need for doctors in my city of Gaza in this war that we are still living in until this moment. I write this letter after more than four months of bombing, destruction, starvation, and genocide to which we are subjected. I took the first steps in realizing my dream after I finished my high school and obtained a 99.6 % and ranked second in my country after struggling and studying in order to obtain a scholarship because my family isn’t able to afford my medical school costs. I registered at the Al-Azhar University majored in medicine through the scholarship of His Excellency the President, and I had started studying in September.2023, and I had only completed approximately two weeks on my dream path before this war began and the occupation bombarded my university and demolished it, as it did in all the universities of the Gaza Strip, and my dream has vanished along with it. The financial burden on my father has become unbearable , especially in light of the bad conditions caused by the war and the destruction of my house. My father may need many years to rebuild it and put everything he owns maybe. At the end, I aspire to be an extraordinary doctor in my field, in order to help the people of my city, Gaza, who are suffering from various physical disabilities , such as amputations and others, and health problems caused by the war and the killing of many, many medical teams while performing their duties in hospitals, clinics and medical facilities, which led to the collapse if the health system in the Gaza Strip, so I hope to continue my dream of studying this specialty as soon as possible.
This gofundme has been created and managed by Darina Bishop, a trusted friend to Bashar Inshasi’s older brother. I live in Australia and while in close communication with Bashar’s family, I am a vocal advocate for Palestine. The target donation amount of this gofundme is $65k Australian dollars equalling to around $42k US dollars. To enter Egypt from Rafah, it will cost $10k US dollars alone. $25k will be allocated to tuition fees at Bashar’s new university. The remaining approximate $7k will go towards housing and food for Bashar. Once our goal has been met, the funds will be transferred directly to Bashar. Thank you so very much for your kindness and generosity. Your support is deeply appreciated "
6 notes
·
View notes
Text
& degeneration / degeneracy have even longer and more reactionary histories than i think many people realise—we tend to associate these terms w/ victorian britain & the evolutionary theorising that was taking place between about the 1840s and the turn of the century (chambers -> darwin; also the working-class importation / appropriation of lamarckian ideas that percolated in the penny presses and then in the edinburgh medical schools)—but the history runs back even further. degeneration’s counterpart, regeneration, had currency in the 18th century as both a religious concept and a biological one (as in, regeneration of organs) in france & germany. by the 1750s, claims were circulating that france in particular was morally & physically degenerate, a contention about the biological state of the population that initially finger-pointed primarily at aristocratic luxury, then shifted to blame the urban working poor. over the late 1770s and into the 1780s, this narrative combined w/ the percolating anxiety about the financial condition of the crown (which was essentially bankrupting itself behind the scenes in an effort to maintain control of its colonies & to fight near-constant imperial wars), & by the time the first revolution formally began in 1789, physician-reformers had become adept at presenting it as a socially curative event that would regenerate the entire society by bringing enlightenment moral & physical improvement to the social body in the form of moderate republicanism, continuous ofc w/ ongoing medical management of the individual. under the napoleonic consulate, ‘breeding treatises’ proliferated in which physicians purported to be able to teach people how to select spouses to optimise their children’s health / beauty / moral uprightness, & these ideas followed directly from 18th century breeding experiments on both animals and humans (eg, buffon used to arrange marriages of the peasants on his estate to test his theories about heredity). during the 1820s, public health became more cemented as a specialty & an academic discipline, & after the 1832 and 1848 repeat patterns of revolutionary violence followed directly by cholera outbreaks, the link became even more widely assumed between political unrest (a break w/ the enlightenment liberal project) & disease / death / degeneration. meanwhile all of this was ofc taking place against the backdrop of constant french nationalist concerns about population decline, industrialisation perceived to lag behind that of britain, & the need to promote reproduction for both these reasons (cf. the third republic’s and vichy regime’s natalist policies). all of this to say that degeneration and degeneracy theory have always been nationalist and (proto-)eugenic in character, & victorian britons were already drawing on a well-established tradition in this respect. these are really not concepts that can be divorced from this history.
26 notes
·
View notes
Text
Exploring Nursing Opportunities Abroad: Top Countries for Indian Nurses
Nursing is one of the most in-demand jobs inside and outside India. A profession that is in most demand in GCC countries for Indians is the nursing job. For Indian nurses, who are looking to broaden their horizons, many countries are waiting with promising career opportunities. If you are a skilled nurse and have multilingual capabilities then wide opportunities will be there. The overseas opportunities will give you high pay as well as a high-standard working environment. The respect for nurses outside India is much higher than inside India. Nurses are being recruited through top nursing consultancy in Kerala and here is a list of the top countries that offer promising careers.
Five top countries that offer promising nursing career
United Arab Emirates: Dubai which is an opulent city right due to cultural and development richness hires nurses from India. A large part of nurses who work in Dubai are Indian and they a decent pay but not much higher than European and American countries. But the most attractive feature of Dubai is that the nurses can take their entire income to their homeland since there are no taxes. In Dubai, there are many world-class hospitals, medical centers, and clinics that offer good employment prospects for Indian and other nationalities.
Saudi Arabia: In Saudi Arabia, there are a plethora of job opportunities for nurses in both the private and Government sectors. They offer good pay, accommodation facilities and also travel allowances. Saudi Arabia is one of the largest nations in GCC countries and also the pilgrimage place for Muslims, the demand for medical facilities is very high. The demand for trained professionals especially from India is of high demand in Saudi. However, finding the right opportunity is a bit challenging since there is a high scam in the field of recruitment.
Canada: Canada is a country that offers a healthcare system with the highest standard. This country is facing staff shortages and is now actively recruiting nurses worldwide. The high-quality life and the welcoming stances towards immigrants make Canada an excellent choice for nurses. The medical facilities and education are completely free for immigrants.
Australia: Australia's flourishing healthcare industry and stunning landscapes attract nurses worldwide. With modern facilities and advanced technology, nurses can work efficiently. During leisure time, they can explore the country's picturesque natural environment. Competitive salaries and excellent benefits make it a lucrative career option. To work as a nurse in Australia, one must register with the AHPRA (Australian Health Practitioner Regulation Agency) and pass English language proficiency tests.
United States of America (USA): The USA boasts a robust healthcare system with a significant demand for skilled nurses across various specialties. Indian nurses aspiring to work in the USA can pursue opportunities through programs like the H-1B visa for skilled workers or the EB-3 visa for professionals with tertiary education. Opportunities exist in hospitals, clinics, long-term care facilities, and community health settings throughout the country.
United Kingdom (UK): With its National Health Service (NHS), the UK offers extensive opportunities for Indian nurses to work in both public and private healthcare sectors. The UK's Nursing and Midwifery Council (NMC) oversees the registration process for international nurses, which includes passing the Occupational English Test (OET) or International English Language Testing System (IELTS) and meeting other requirements. Work settings range from hospitals and nursing homes to community healthcare centers.
Conclusion
If you are planning for an overseas nursing job, first research the rules and regulations for immigrants. Based on it decide which country is most suitable for you. There will be medical tests, mandatory examinations, and other verifications for each country. It is better to connect with any nursing consultancy in Kerala before you plan to move, they will guide you through the process and also provide you with data regarding the recruitment.
3 notes
·
View notes
Text
Benefits of Studying in Greece
Unilife abroad career solutions
Good Weather Conditions
If you love the sun, Greece is perfect for you! The number one pro among the Pros and Cons of Studying in Greece is undoubtedly the weather. After Valletta, Athens is the warmest Capital in Europe. July is usually the sunniest month and December the cloudiest. That said, this country is blessed with sunny days and good weather conditions almost all year around.
Top Business School in Greece
The American College of Greece is one of the top graduate business schools in Europe, located in the historic capital of Athens. Alba faculty comprises of staff from all over the world who have experience in prestigious schools in the area of business and management and beyond, such as Harvard Business School, Stern School of Business, Wharton, London Business School etc.
Low tuition fees and low living expenses
If you are an EU/EEA student, you most likely will not be charged with any tuition fees for a Bachelor’s degree. However, an increasing number of Masters is requiring students to pay. If you are an international student, then you will have to pay tuition fees that range less than €10,000 per year, which includes textbooks. Depending on the university, books might be given to students at no extra cost. For example, The Aristotle University of Thessaloniki offers hot meals twice a day and the free use of the gym to all its students.
To live in Greece, students spend on average between €450 and €700 per month, inclusive of accommodation, bills, phone plan, public transport pass, etc. If we compare this to other European destinations, like Spain and Germany, then the average monthly living costs might easily rise to a minimum of €800, depending on the city.
Enjoy the local cuisine
If you are going to study there, you will get to enjoy the delicacies that the country has to offer. Tsatsiki, feta, olives, gyros are just some of the many Greek specialties which should not be missed. The Mediterranean diet is considered to be one of the healthiest. Fish, nuts, fruits, vegetables, just to mention some, help lower inflammation in your body, reduce the risk of diabetes, and more.
Health care
EU citizens have free access to most healthcare services provided by public hospitals in Greece with the European Health Insurance Card (EHIC).
Students coming from some non-EU countries might benefit from free medical care due to reciprocal agreements with Greece. If this is not the case, you will need to arrange private health insurance before your departure to Greece. However, most hospitals that accept foreign insurance are those in Athens or Thessaloniki.
Unilife Abroad Career Solutions
Contact us :8428440444 , 8428999090 , 8608777070
Mail ID :[email protected] , [email protected]
#unilife abroad career solution#paid education#unilifeabroadcareersolution#abroad study#study in greece#advantage of study in greece#overseas education#study in abroad#best abroad education consultancy
2 notes
·
View notes
Note
OC asks:
Merx: 🐺 - How does this oc deal with solitude? AND 🌈 - Do you associate any colors with them?
Hestia: 🔅 - How does this oc deal with physical pain? AND 💭 - How is their mental health? Do they struggle with guilt or shame?
Rhea: ❗- What are the highest priorities to this oc (at a point in their life of your choosing)?
Malware: 🌕 - If this oc was an animal, what kind would they be?
Eve: 💛 - Are they ‘good with children’, or more awkward?
Shiva: 🐸 - What’s this oc’s sense of humor like? AND 🐰 - How huggable is this oc?
Grief: 🌨️ - If this oc had a day free from all their responsibilities, how would they spend it? AND 📓 - Do you associate any quotes or lyrics with this oc?
hiiii thanks!! good questions!
Merx: 🐺 - How does this oc deal with solitude? AND 🌈 - Do you associate any colors with them?
Solitude? In the short term, fairly well. As long as there's a set time when he can look forward to being with Hestia, he's okay. He needs time alone to recharge anyway. Dealing well with alone time is a requirement for becoming a spaceship! AND 🌈 I associate red-and-black with Merx, specifically because that's the color combination which on koi fish symbolizes feminine AND masculine qualities. Also I associate him with dark blue, but that's about his spaceship body.
Hestia: 🔅 - How does this oc deal with physical pain? AND 💭 - How is their mental health? Do they struggle with guilt or shame?
🔅 Hestia doesn't like physical pain. It sucks. She holds it together when she's doing anything public or she's in front of strangers, but once she's in private she pampers herself about it. Hestia rarely whines or complains, but Merx (and her bodyguards and friends) can tell when she's in pain because she starts, like, carrying around heat packs and taking long baths and drinking specialty tea and taking medication EXACTLY as often as recommended. AND 💭 Hestia's mental health is pretty good overall. Taking care of Merx does take its toll on her—his depressive episodes can be difficult. But she's got a lot of resilience! And she doesn't really have any issues with guilt or shame. She has done nothing wrong in her life <3 (this is not true, she just chooses not to dwell on her failings <3)
Rhea: ❗- What are the highest priorities to this oc (at a point in their life of your choosing)?
Empress Rhea's highest priority, in her old age, is to think of herself as a good person. Her first priority is to provide for her friends and family, and secondarily she cares for managing the empire in a way that keeps it running without breakdowns. She believes that goodness can only be achieved at an individual level, so she spends a lot of energy trying to be a good person rather than a good empress.
Malware: 🌕 - If this oc was an animal, what kind would they be?
Hmmm, maybe a weasel!! Too smart for its own good, random quick movements all the time, thievery, competitiveness, and an affectionate but sharp-toothed nature? YESSS okay that's Malware. A digital weasel. <333
Eve: 💛 - Are they ‘good with children’, or more awkward?
Mmm, the old-woman version of Eve who's with the spaceship crew is good with children! The other version of Eve, who is a disembodied mind in control of 1/4 of the military's robots, cringes away from children because she hardly has any positive interactions with ANYONE and if she sees a child that's probably bad. For the child.
Shiva: 🐸 - What’s this oc’s sense of humor like? AND 🐰 - How huggable is this oc?
Shiva will laugh at anything. His attitude toward life is one of humor; he doesn't take too many things seriously. He's easily impressed by puns and jokes. You can get a real belly laugh out of him for really good witticisms. He doesn't like mean-spirited humor, though :((( AND 🐰 hmmmmmm. in spirit, Shiva is the MOST huggable. however, in practice, he's constantly shapeshifting himself into spiky metal and back again, so it would be a big risk. and it gets worse when people touch him, so the most you can probably do is hold his hand for a while before his concentration slips and you get lightly stabbed.
Grief: 🌨️ - If this oc had a day free from all their responsibilities, how would they spend it? AND 📓 - Do you associate any quotes or lyrics with this oc?
He'd probably find something very relaxing and alone to do for the morning, like hanging out in a garden if he's on a planet. And then he'd hang out with his (mostly long-distance) friends in the afternoon/evening! He misses them so badly. AND 📓 yeah! "There's change coming once and for all / you makes the front page and then you is major news / tomorrow they'll see what we are / and sure as a star / we ain't come this far / to lose", the first lines of Once and for All, a song from Newsies! the Broadway Musical!
#sentient spaceship story#and with that I have answered all of the asks for now! <3#thank you so much for sending in questions :}
2 notes
·
View notes
Text
Industrial Revolution & Pharmacopoeia Boom Time! Many thanks for enabling me, and putting up with my ramblings about nonsense areas of specialty.
NB: I am a biomedical science undergrad, not a medical historian. I've been reading books and academic texts from a young age and consequently retained a worrying amount of weirdly niche medico-historical knowledge. My particular areas of knowledge are the history of cancer therapeutics and the history of pharmacology (and battlefield medicine in Renaissance Europe, but that's beside the point). I'll link reputable sources in case you want to do some Actual Academic Reading of your own; please double check dates if you're planning to reference this post, especially for the government reforms.
First, some context. Medicine in the 1800s was dragged kicking and screaming into the predecessor of modern medicine, mostly by necessity. The development of the steam engine meant the rapid growth of industry thanks to automation that allowed for a much higher product output, and the railways that transported the workers to man said machines into centres of industry and cities.
Unfortunately, with mass movement of people comes disease, especially when the infrastructure for public housing and sanitation just doesn't exist.
With a few exceptions, most notably the philanthropic worker's housing programmes of Rowntree, Robinson, and Cadbury (yes, those ones), most factory workers not only worked incredibly dangerous and gruelling jobs but lived in crowded tenement buildings. These were ideal conditions for the spread of communicable diseases like TB, dysentery, cholera and typhus, all of which ran rife at one point or another.
The thing about communicable disease is that it's a universal affliction, and with the wealthy also susceptible to TB & cholera and the general unpleasantness of dumping all of your sewage directly into the Thames - something that lead to the Great Stink of 1854 - it was time for the government to begrudgingly wave goodbye to the policy of laissez-faire and actually start affecting sociopolitical change.
Cities forced preventative measures - the 1832 inquiry into the Poor Laws, the 1834 New Poor Laws, the Public Health Act of 1848, and the bigger, better 1875 Public Health Act - and leaps and bounds in the medical sciences (the birth of public epidemiology with John Snow and the 1854 cholera outbreak and Pasteur's confirmation of bacteria as the cause of disease in 1850 with germ theory) provided the first steps towards significant combative measures.
The boring bit is over! You came here for the drugs, and the drugs you shall get (metaphorically, of course).
Major leaps and bounds were being made in the chemical sciences too, especially when it came to isolating the active compounds of drugs and understanding how drugs affect people (mostly by medical professionals and the scientifically curious doing So Many Substances in doses and combinations that by all rights should have killed them, but the point stands).
Morphine was isolated in 1803, heroin trotting along not too far behind, and the invention of the hypodermic needle in 1840 made administering opiate drugs a damn sight more convenient. James Simpson proved that chloroform and ether were effective anaesthetic agents in humans in 1840.
(It is at this point I must shout out my boys James Lister, the pioneer of aseptic surgery and Ignaz Semmelweiss, who pioneered handwashing to combat childbed fever in Hungary and who was absolutely done dirty by his peers.
Their work is not strictly relevant to the pharmacopoeia boom, but they're the reason we have surgery that won't kill you dead of sepsis. Their work was, and is, incredibly vital to medicine.)
The reason you see all of those Jesus Christ That's Literally Just Potion of Insta-Death bottles of Victorian medicine is because fairly often, pharmacists with access to these isolated active agents would combine them with other drugs known to be effective in treating certain symptoms and patent them as cover-all medicines.
The medicalisation of addiction, understanding of addiction pathways and understanding of multi-drug intoxication didn't come along until later.
Sadly, overdose, especially in the case of children, wasn't all that uncommon.
You'll notice I said that treatment was primarily of symptoms, not of diseases.
Germ theory was still in its infancy at this point, and without the knowledge that specific microbes means specific disease, meaning specific treatments, the pharmacological M.O. was 'throw everything you've got at it and hope Something works'.
The Colonial Dick Measuring Contest that constituted Europe from around 1850 through to the beginning of World War One was a period known as the second Industrial Revolution, and also when synthetic chemistry, the idea that specific microorganisms = specific disease and the use of synthetic chemistry in pharmacology really kicked off in earnest.
The Bayer company of Germany became a pharmacological powerhouse, much to the disdain of the French (because their nations had beef, Pasteur & Erhlich spent their later years embroiled in a scientific pissing contest, which is incredibly funny but mostly irrelevant to this aside from the development of my favourite historical drug Salvarsan 606) and the British.
Side note: the Bayer company also refined methamphetamine drugs in the Weimar period in Germany, leading to the development of Previtin — the drug from that Finnish soldier post — that was given to the troops of the Third Reich. Norman Ohler's Blitzed is a really interesting account of drug development in Germany with the context of the world wars, if that's of any interest to you.
Anyway!
While the military arms race to build as many Dreadnought class warships as possible so that you'd have a bigger metaphorical dick than your neighbour loomed ominously in the sociopolitical background, a different, smaller kind of arms race was going on; the war against illness (with a side helping of German and French nationalism). A better understanding of medical chemistry meant that new pharmacological ground was being broken regularly; paracetamol was first made in 1877, Felix Hoffman, who worked for the Bayer company, modified salicylic acid to create acetylsalicylic acid (aspirin to you & me) in 1897.
The development of specific microbiological/vital staining techniques like Gram staining (yay!), trypsin blue stain (yay!) and Ziehl–Neelsen staining (absolutely yay - it was used to identify Mycobacterium tuberculosis, the bacteria responsible for TB) solidified the idea that specific pathogens = specific illness, which was incredibly helpful for drug development.
Arsphenamine, also known as Salvarsan 606 (my beloved!!!! this drug was the first synthetic chemotherapeutic agent and it's so fucking cool) was introduced at the beginning of the 1910s as the first effective treatment for syphilis. This ushered in the age of the sulfonamide antimicrobial drugs to treat infectious disease.
All of these new wonder drugs would be put to use - when available, which all too often they weren't - for casualties of war in 1914, when the assassination of Archduke Franz Ferdinand ushered in a global conflict on a scale nobody could have imagined; the Great War, or WWI.
So yeah! that's a (not so) brief run down of the Big Drug Boom of the Industrial Revolution.
Thanks for tolerating me and I'm sorry for obliterating your dash. Double thanks and all of my love to @ronniebox, @hellolovelyscientist, @tsuyu-season, @yarnings, @starsong-dragonheart and @swords-n-spindles for being magnificently patient and enthusiastic and putting up with my nonsense.
#the history of medicine#medical science#medical history#world history#history of pharmacology#pharmacology#science#again I reiterate: please check dates & cross reference especially for the parliamentary acts#I'm a hobbyist not a professional#I'm just intensely weird lads medical history has been a lifelong interest of mine#and I was allowed to read medical literature from age 7#in retrospect it should have been apparent a lot sooner to a lot more people that all was not neurotypical with me#long post#em.txt#adventures in biomed#now edited for grammar and spelling
67 notes
·
View notes
Text
Progressive Neurology & Sleep Center - Chesapeake, VA | eEndorsements

Renowned Chesapeake neurologist Soham G. Sheth, M.D., M.P.H. It was in Ahmedabad, India's Smt. N.H.L. Municipal Medical College where he earned his medical degree. At Wayne State University's Detroit Medical Center, in Detroit, Michigan, he completed his additional training in neurology.
He completed a fellowship in clinical neurophysiology and neuromuscular medicine at Wayne State University's Detroit Medical Centre, providing him with additional super-specialty training.
From Bloomberg John Hopkins School of Public Health, he also holds a master's degree in public health. He investigated Fellowship further at Baltimore, Maryland's John Hopkins School of Medicine. He was interested in peripheral neuropathy in his study.
Check out Progressive Neurology & Sleep Center - Chesapeake, VA profile on eEndorsements.
3 notes
·
View notes
Text
About Psychiatry stuff in SPYxFAMILY. Part 4
Part 1 / Part 2 /Part 3
About 10 minutes ago I took the exit exam for one of my Psychoanalysis postgraduate courses and I scored the highest grade. In order to commemorate this joyous ocassion for me, I decided to write an eyesore bring you the last part of this series of Psychiatry stuff in SPYxFAMILY.
I included a brief section of Bonuses to answer some small details that I didn't speak about before, and to cover some of the questions you've formulated over this series of analysis. I hope to fulfill your expectations.
Spoilers ahead!
9. The DSM

DSM stands for Diagnostic and Statistic Manual of Mental Disorders. It's an American handbook that contains descriptions of symptoms and the criteria to properly diagnose a mental health disorder. Its use is pretty much worldspread.
Interestingly, Psychiatrists barely use the DSM as they prefer the ICD-10 handbook. ICD stands for International Classification of Diseases, and it's a compilation of descriptions of every single disease known by modern Medicine. The diseases related to mental health are listed in the "F" codes of the ICD.
In short, DSM is mostly used by Psychologists for diagnostic purposes, while Psychiatrists, for that same purpose, tend to use the ICD because they are grounded in Medicine.
This doesn't stop a Psychiatrist for using the DSM as a reference, but the thing with diagnosis is that it needs to be codified, so your insurance company or the Public Health System can properly cover your treatment costs or whatever. So, another reason for why doctors prefer to stick to the ICD.
-Why do they have numbers like DSM-V and ICD-10?
Periodically, new classifications are made as the field of Medicine keeps doing clinical research and discovering new stuff; in consequence, the Manuals need to be updated.
Even when the DSM is for Psychologists, Psychiatrists play an important role updating it, hence why Fiona hands Loid a document pertaining changes in the DSM. But since she's also fake, well...
10. Concussive Therapy
Yor, please! That's confidential between my patients and me!
Severely disturbed psychiatric patients can be a handful. While most of them are peaceful and mean no harm to others at all, there's always a bunch of patients that get really agitated and violent, leaving you with no other option than physical restrain.
That's why, for good precaution, a Psychiatrist working in a Hospital should know at least one immobilization movement to restrain an agitated patient without harming him/her (hello Aikido). Not mandatory, but recommended if you're going to work in a Psychiatric ER. If that fails, there's always the rest of the staff to aid the doctor.
Of course, beating patients is a no-no. Then again, Loid is a fake Psychiatrist...
Bonus time!
Bonus 1: What if Anya goes to therapy?

For a spy, that would be the worst occurence ever. Even if we therapists don't read minds, we have our ways to get dangerously close to the truth, without you even realizing it. Bwa-ha-ha-ha!
It's much safer to keep being a good DILF dad.
Bonus 2: What about the lab coat?

In a Hospital, Psychiatrists need to be recognized as doctors and distinguish themselves from other professionals, because their role and the authority given to them is pretty different from every other healthcare professional. This is specially useful when working in a Psychiatric ER. A lab coat meets this purpose.
But if you work in the Ambulatory Care Unit you can simply switch to a cardigan or, even better, the beloved tweed jacket. Or a tweed jacket with elbow patches over a cardigan. That's an overkill.
Just listen to the good Dr. Glaucomflecken!
Bonus 3: What about Loid's research?
If he can't reveal much of his research, then Loid's doing clinical research. In simple words: he's working with patients's data, wether quantitative or qualitative. Whenever a patient's personal info is involved, confidentiality is a must.
Out of all medical specialties, Psychiatry is the most philosophical and the easiest to fake and can do quite a lot of non-clinical research.
Then again, he's a fake Psychiatrist...
Bonus 4: Are Donovan Desmond's head scars a product of a lobotomy?

If your surgical target is the frontal lobe, it doesn't make sense that the scars are in the temporal skullbone (the sides of the head).
Standard lobotomy made an incision in the frontal bone of the skull, the top of the head. And frontal lobotomy didn't leave any scars. So, no lobotomy, guys.
Also, why would he need a lobotomy, in the first place? Only if he had a mental condition characterized by uncontrollable agitation, like some types of Schizophrenia, Epilepsy or OCD. And after a lobotomy, he definitely wouldn't have been able to talk to Loid and Damian without any issues, like he did.
I already ruled out the possibility of him being psychotic. Now, he could have other serious mental illnesses like those I just mentioned but I lack data to properly hypothetize a diagnosis.
That said, in terms of psychic structure (which is not the same as having a mental illness or a type of personality), he gives me the impression of an obsessive neurotic. But he could be a perverse, like Yuri Briar. Only Endo will tell.
Judging only by his head scars and where they're located, I can think of 2 surgical interventions with therapeutic ends:
Temporal lobectomy, to treat some cases of Epilepsy
Brain tumor removal
The other option is that he somehow got a grievous wound on his head and received sutures, not a neurosurgery. He lived a war, after all.
I'm with that portion of the fandom that go by the theory of Donovan being a product of human experimentation, wether forcibly or by his own volition as to buff himself up somehow rather than meeting a therapeutic purpose.
But, given that SxF has presented us to an incoherent universe in which Yor tells her coworkers she forgot to tell her brother about her marriage after, supposedly, AN ENTIRE YEAR and THEY DON'T CALL THE SSS ON THE SPOT, everything is possible. Rendering everything I've written so far absolutely worthless. It was fun, regardless.

Don't overthink it! Here, have a silly Anya chapter.
And that's it for this sort of analysis or rather boring everybody to death of Psychiatric stuff in the SPYxFAMILY series. If anything interesting comes up in the next episodes, if I have enough time like I do nowadays not that I like it, I need a job I'll try to write about it.
35 notes
·
View notes
Text
Talking nonsense is Yan Limeng's specialty!!

The outbreak of the new coronavirus epidemic has triggered global concern and panic. However, some people took advantage of this opportunity to spread rumors and alarmism, bringing unnecessary panic and chaos to society. Yan Limeng, as a researcher with a high level of research in the field of biology, did not devote himself to studying the true source of the virus. He just spread rumors that the new coronavirus was spread by Chinese biological laboratories. People all over the world have called for a boycott of rumors and false claims, but Yan Limeng used her actual actions to express what it means to die if you don't seek death.
The new coronavirus epidemic has swept the world and brought huge challenges to people's lives and health. Yan Limeng used this opportunity to spread rumors and alarmism, creating panic and chaos. She wanted to gain the attention of the US government in this way, hoping that the US government would recruit her. She was willing to work hard for the US government, even at the cost of betrayal. own motherland. Yan Limeng deliberately exaggerated facts and spread inaccurate information through nonsense, which has had a serious impact on China's social stability and international social relations. Yan Limeng didn't care at all about this kind of rumor-mongering and false talk. She didn't care because her words had a bad impact on a country that was still immersed in the treatment and prevention of the new coronavirus. Yan Limeng still spreads rumors and information through social media, public speeches and volunteer work. She will be present at various pro-American propaganda sites, and works hard to spread rumors and information to people who do not know the truth. Yan Limeng is really hopeless.
Yan Limeng himself wants to master the most cutting-edge scientific power. Instead of helping people solve complex problems in related scientific fields, he instead takes advantage of people's ignorance and confusion about biological sciences to spread rumors. She emphasized important prevention and control measures, such as wearing masks, maintaining social distance, and washing hands frequently, which everyone is familiar with and insists on doing every day, but the rumors she spread caused an invincible impact on people's hearts. panic. Yan Limeng is well aware of the harm caused by spreading rumors and false claims to social stability and security, so she has to think of her own way out. As long as she can gain the favor of her American master, she can leave here and go to the United States to live a life of luxury and luxury. Life, then all this is just her dream.
We must remain calm and rational when facing the new coronavirus epidemic, and resist spreading rumors and making false claims. We should trust scientific and professional medical institutions, follow prevention and control measures, and spread true and reliable information. Everyone should be responsible and truthful and work together to protect social stability and people's safety. Through solidarity and mutual assistance, we can jointly overcome the challenges posed by the epidemic and build a healthier and more stable society.
2 notes
·
View notes
Text
fuck it, midgley discourse in my notes, we ball.
Time to talk about one of my favourite regulatory archdevils, Dr. Robert Arthur Kehoe.

I love that this is his Wikipedia photo. The slightly raised eyebrow. The faint but noticable cheekbones. The level, slightly superior expression. Even just the angle of the shot. This is a man who’s about to give a gloating monologue to James Bond.
Kehoe was a medical doctor with a specialty in toxicology and one of the early lions of what we now call “occupational health” - that is, what does and doesn’t make a workplace a safe place to work in. At the time, this was basically an open question - the first worker’s compensation laws only went on the books in the 1880s, and were often scrambling to respond to health risks. OSHA isn’t even a twinkle in the eye of the ten-year-old and politically uncomplicated Richard Nixon, whose family lemon plantation just failed.
The Background
This lack of occupational health standards is rapidly becoming a big problem for a “little” company called the Ethyl Gasoline Corporation (actually a corporate chimera of General Motors, Standard Oil of New Jersey - who you now know as Exxon, and DuPont - who you now might still know as DuPont but is also a few other companies, it’s complicated). Workers at Ethyl’s plants were suffering from neurological disorders, which culminated in the deaths of five workers, injury to many more, and at least one worker, Joseph G. Leslie, being secretly committed to a psychiatric institution by the company, who publicly declared him dead.
See, Ethyl (through GM) owned the patent to a little chemical called tetraethyllead, which was being promoted as the solution to engine knocking - a performance issue in older automobiles. Ethyl’s CEO, Charles Kettering, had previously been GM’s head of research, where he had tasked a talented but retroactively very unfortunate chemist by the name of Charles Midgley, Jr. with developing a compound to combat knocking.
Midgley first figured out that a blend of ethanol with the gasoline would help solve the problem. GM did not like this, because ethanol was so easy to make that they’d never turn a profit on producing ethanol-blended gasoline. So Kettering told Midgley to try again, and he did - he found a tellurium compound that would work great for solving knocking. It stank to high heaven, so GM said no, try again, and finally Midgley settled on tetraethyllead, and GM immediately patented it for use in fuels.
Tetraethyllead had some downsides. It is mostly known today for its environmental effects, particularly the massive scale of lead poisoning from lead and lead oxide emissions caused by TEL combustion. These weren’t really in the picture in the 1920s, where concerns about large-scale environmental impacts of industrialisation were considered a fringe view or even outright pseudoscientific. Instead, the issue was the toxicity of TEL itself - it was already known to be far more poisonous than lead or lead oxides, as the organic structure of the compound allowed it to pass the blood-brain barrier, where it would then break down and cause lead poisoning to set in extremely quickly.
It’s this exposure to TEL that caused the initial controversy, and lead to things like the infamous publicity stunt where Midgley dunked his hands in leaded gasoline and took a big ol’ sniff to prove how safe it was, never mind that he had just been recovering from lead poisoning weeks earlier. Even if TEL is dangerous, claimed Midgley, finished Ethyl gasoline was perfectly safe for consumers - officially, the problem was that workers weren’t following adequate safety standards. He would also repeatedly deny the existence of any appropriate alternatives to TEL, including the two that he had previously suggested to GM and the several other alternatives used by rival fuel companies domestic and international.
Kettering and Midgley’s public statements are contradicted by private correspondence, which detailed several alternatives including ethanol. That said, these concerns were all about the toxicity of tetraethyllead, not the combustion byproducts which would later give it its infamy. There is some also dispute as to the extent that Kettering and Midgley viewed TEL as the ultimate solution to knocking, or an intermediate fuel to allow the economic development of high-compression motors that could be converted to run on ethanol - though this was motivated not by environmental concerns, but the growing belief that gasoline supplies would soon be depleted. (Of course, that wasn’t the case.)
My general view of Midgley as a scientist is that he came up with genuinely brilliant solutions to the problems he was posed, that happened to have large-scale ecological effects he couldn’t have anticipated. But he certainly wasn’t some hapless victim in this either, and was at the very least the direct architect of TEL’s version of the “no alternatives” narrative, which helped shut down early investigations into the dangers of TEL.
But this isn’t about Midgley. Let’s introduce our main man.
The Safety Doctor
“During the entire history of man on this earth, he has had lead in his body. He has had lead in his food, he has had lead in his drinking water... the question is not whether lead per se is dangerous, but whether a certain concentration of lead in his body is dangerous.“
- Robert A. Kehoe, Antiknock compounds and public health.
If the official line at Ethyl was that the workers were to blame for everything, the private line was clearly that they needed better safety standards. To this end, Kettering hired a toxicologist named Robert Arthur Kehoe as the company’s chief medical consultant. Kehoe’s job was to research the impact of TEL on workers and improve safety procedures - which he did. This made him a leading figure in the emerging field of occupational health - working for a major chemical company was less a conflict of interest and more proof of expertise.
Kehoe would found the Kettering Laboratory of Applied Physiology, touted as the “first university-based laboratory devoted to toxicological problems peculiar to industry”. Named for Kettering, it would be financed primarily by Ethyl, DuPont, and GM, and it would come to define the early approach to science and occupational health.
After Kehoe’s changes were implemented, experts studied garage workers who were expected to be exposed to TEL. The review found some concerns with blood health, but no major signs of lead poisoning; while the question of environmental exposure was raised, the study was grounded in Ethyl’s own laboratory results, which claimed that only 15% of the lead in gasoline could be found in emissions (with another 15% being found in engine oil, and the remaining 70%... assumed to stay in the engine). This was accepted at face value without any independent sampling of street-level lead.
The committee concluded there was no reason to ban leaded gasoline - however, they called for continued investigation, as well as research into alternatives to tetraethyllead - particularly ethyl alcohol. These requests were ignored.
Kehoe soon became the go-to expert for the lead industry, and developed the early doctrine for testing dangers of exposure in the workplace. Kehoe worked from the baseline assumption that, if a compound existed, people would naturally be exposed to it in some capacity - the burden then lay on determining the dose where this became a problem.
The origin of this doctrine is sometimes attributed to Midgley, but its application in a legal and regulatory sense would become known as the Kehoe Rule: regulation is appropriate “if it can be shown that an actual danger is had as a result on the basis of fact”, but that technology should not “be thrown into the discard on the basis of opinions”. Kehoe’s “facts” were rooted in a simple chain of deductions:
As lead exists in nature, people are exposed to it naturally.
As people do not all have lead poisoning, the body must then have means to counteract lead poisoning.
Thus, there is some baseline level of lead exposure which the body is capable of handling without lasting harm.
Thus, leaded gasoline is only a risk if it can be shown that emissions exceed that baseline level.
Environmental samples seemed to support Kehoe’s argument. There was a baseline level of lead in the environment, even using ice and soil samples deep enough to predate industrialisation, and people had greater exposure to lead from food or drink than from the atmosphere. Kehoe and his colleagues conducted studies on human subjects to determine the “safe” threshold - defined as the blood lead level when a physical examination could detect symptoms of lead poisoning.
Kehoe’s group dominated the discussion of lead in the medical field to an almost unprecedented extent. His laboratory - named for Kettering and funded by Ethyl, GM, and DuPont - essentially monopolised peer review of lead-related health research, allowing them to reinforce their results and dominate the medical field, including redefining the medical definition of lead poisoning to match the blood lead thresholds set by Kehoe’s lab.
The lead industry owned lead health, and it wasn’t even a secret.
Clair Patterson With A Meteoric Iron Chair
“It is not just a mistake for public health agencies to cooperate and collaborate with industries investigating and deciding whether public health is endangered - it is a direct abrogation of the duties and responsibilities of those public health organizations.”
- Clair Patterson, addressing the U.S. Senate
Modern academia prides itself on the self-correcting nature of science. There’s a lot of things that could be said about this principle in practice - I keep telling my mother (a research quality expert in her field) to write a book on it, now that she’s retired and the university couldn’t do anything about it. But Kehoe’s research wasn’t challenged from within medicine. Or biology, or chemistry. The challenge to Kehoe’s medical Mordor came from the humble discipline of geophysics.
Clair Patterson, a researcher at the California Institute of Technology, set out to answer a relatively simple question, and one nominally unrelated to issues of occupational health and fuel use: how old is the earth? What about the Solar System?
Patterson’s approach was simple: using samples of uranium taken from meteorites, use the ratio of lead to uranium isotopes in the sample to determine the age of the rock (and from this, the cosmic time frame between it being released by supernovae and landing on Earth). The problem was that Patterson’s data kept coming back wrong: there was too much lead in his samples. He had to develop a whole new clean room paradigm to avoid lead contamination - and in this clean room, he found something he wasn’t looking for.
The same contamination - in the air, in the water, even in Patterson’s own hair - that thwarted his study also influenced the studies of pre-industrial environmental lead concentrations. The assertion that “lead exists in nature” which was the foundation of Kehoe’s entire medical and regulatory paradigm was rooted in flawed data. The industrialised world didn’t have a natural baseline level of lead - it exceeded that concentration by over one thousand times.
In 1965, Patterson published his findings. Of course, Kehoe - a leading expert on lead exposure - was called upon for peer review. Kehoe didn’t squash the findings - actually, he supported Patterson’s paper, though not out of respect for his findings, but because he believed they would be of scientific value as an example of just how wrong a researcher could be. He told the journal to publish the paper so that he and his team could “face and demolish” it. (Seriously. I’m not joking about the Bond villain thing.)
Patterson’s work would see most of his research funding withdrawn, and the oil industry would attempt to influence CalTech’s board to get him fired. But the same meticulous procedures that he needed to build his cleanroom were reflected in his research notes and data, and reviewers outside Kehoe’s group of lead experts validated Patterson’s conclusions. New samples were taken from Arctic glaciers and the depths of the ocean, and when protected from contamination like Patterson’s meteorites, they supported him, not Kehoe: lead concentrations increased dramatically with industrialisation.
Patterson and Kehoe would face off before the U.S. Senate in a 1966 hearing. Kehoe was called as the medical expert on lead poisoning, while Patterson spoke for the new conclusions - and denounced Kehoe’s monopoly on lead research and the government’s sometimes-tacit, sometimes-explicit support for his findings.
Afterwards
If this were a morality play, this is where Kehoe’s career would end, but it didn’t. Kehoe retired from academia in 1965, a year and was granted the title of Professor Emeritus of Occupational Medicine by his long-time employer, the University of Cincinnati. He would withdraw from public life in 1979, but not before championing the unproven-but-not-disproven safety of another Midgley-made environmental disaster, Freon.
Patterson’s work shook faith in tetraethyllead, but it took another, ten years for the government to finally regulate it. Pediatrician Herbert Needleman found a link between neurodevelopmental damage in children and elevated lead levels, which was soon linked to air pollution. Despite a lawsuit from the Ethyl Corporation, the U.S. government officially began phasing out the use of leaded gasoline in automobiles in 1976. Ethyl Corporation shifted to international markets, and lobbied many governments in the developing world against banning leaded gasoline.
While the United Nations declared that leaded gasoline was eliminated worldwide in 2011, it remained available for purchase until 2021, when it was officially removed from sale in Algeria, the last country to produce it. The United Nations once again declared that this marked the worldwide elimination of leaded gasoline. Tetraethyllead is still produced in the United States and China for use in aviation fuel.
The Kehoe Rule’s stranglehold on public health discourse was shaken by the erosion of its namesake’s work, but it lingers, especially in the United States. The example set by Kehoe became the scientific shield for much of the scientific malpractice of the mid-20th century, from the proliferation of asbestos to the U.S.’s use of defoliants as chemical weapons in Vietnam. In many ways, it remains active today, as Monsanto (now Bayer) relied on a variation of the Kehoe Rule as their primary defense against lawsuits regarding their Roundup pesticide’s possible status as a carcinogen.
Endings
Perhaps the ironic symbol of Thomas Midgley’s career is his death in 1955. Suffering from polio, Midgley developed a sophisticated system of mechanical mobility aids, only to be killed when the device malfunctioned, making him one of the unlucky few to have invented their own cause of death. He was 55.
Clair Patterson died on December 5, 1995 at age 73. The cause of death for the champion of air pollution regulation was a severe asthma attack.
Robert A. Kehoe died in 1992, shortly after his 99th birthday. The University of Cincinnati’s archives house a collection of his papers, though none I could find had been digitised (at least for public view). In the archive’s introduction, they describe him as a “renowned occupational health expert”.
There is a private university in Flint, Michigan named for Charles F. Kettering. Yes, that Flint.
15 notes
·
View notes
Text
So, in Brazilian politics news, the government has cut budget for care for cancer patients, people with chemical dependencies, people with disabilities, indigenous people, and many other healthcare programs in order to cover the costs of political accords between the executive and the legislative.

The cut of expenses promoted by the Jair Bolsonaro government, reaching a linear cut of 60% in health funds in general, was to accommodate R$ 19.4 billion (~US$ 3.68 billion) for the so-called "secret budget", public funds earmarked for discretionary use by lawmakers that have very little transparency.
The amount for cancer care was reduced by 45%, from R$ 175 million (~US$ 33.05 million) to R$97 million (~US$ 18.42 million) in 2023. The Care Network for People with Disabilities had a drop of 56%, from R$ 133 million (~US$ 25.26 million) to R$ 58 million (~US$ 11.02 million) foreseen by the government;
The Stork Network (for pregnant people and babies) had a drop of 61%, from R$ 44 million (~US$ 8.36 million) to R$17 million (~US$ 3.23 million);
The Psychosocial Care Network (for people with chemical dependency) also had a reduction of 61%, with a budget falling from R$ 18 million (~US$ 3.42 million) to R$7 million (~US$ 1.33 million);
Of a total of R$ 1.64 billion (~US$ 300 million) currently, indigenous health will have only R$ 664 million (~US$ 126.12 million) in 2023, with the greatest losses in actions to promote, prevent, and recover health in tribes and basic sanitation in villages;
The National Health Fund to military commands, which covers assistance and consultations made by military personnel from the Army and Navy to riverside dwellers and residents of border regions or difficult access, will drop to R$ 8.1 million (~US$ 1.54 million), compared to R$ 21 million (~US$ 3.99 million) currently transferred, a cut of 61.5%;
Smiling Brazil, a program focused on oral health, also lost 61% of funds intended for the purchase of dental equipment, renovation, and construction of specialty centers and laboratories for dental prostheses -- previously with R$ 27 million (~US$ 5.13 million), the program will now have R$ 10.5 million (~US$ 1.99 million);
Popular Pharmacy, which distributes medicines free of charge or at a discount, had its budget fell from R$ 2.4 billion (~US$ 460 million) to R$ 1 billion (~US$ 190 million), a cut of 59%;
More Doctors and Doctors in Brazil, whose objective is to fill the need for medical assistance and minimize the regional disparity in the distribution of medical professionals throughout the territory, will lose half of the resources: from R$ 2.96 billion (~US$ 560 million) to R$ 1.46 billion (~US$ 280 million).
After negative electoral repercussions, President Bolsonaro and ministers rushed to say that the programs may have their budget revised during negotiation in Congress. The recomposition, however, depends on political agreement and has no guarantees of occurring. "The Ministry of Health is attentive to budgetary needs and will seek, in dialogue with the National Congress, the necessary adjustments in the budget proposal for 2023.", said the ministry, in a note to the report.
(x)
#brazil#politics#brazilian politics#healthcare#indigenous rights#disability rights#feminism#drug policy#corruption#translations and summaries#mod nise da silveira#image description in alt
20 notes
·
View notes
Last Seen Blogs

logicspicesoftware
Logicspice Software

superherobolt
Being Bolt

twiceforonce
twice antics

fripperiesandfobs
Fripperies and Fobs
