#disordered paradigms
Text
Then he came again to Cana in Galilee where he had changed the water into wine. Now there was a royal official whose son lay ill in Capernaum. When he heard that Jesus had come from Judea to Galilee, he went and begged him to come down and heal his son, for he was at the point of death. Then Jesus said to him, "Unless you see signs and wonders you will not believe." The official said to him, "Sir, come down before my little boy dies." Jesus said to him, "Go; your son will live." John 4:46-50 NRSV
This royal official (βασιλικὸς - basilikos) likely was a servant of Herod Antipas. 1, 2 This individual probably was someone of greater wealth and influence than the average resident in Galilee. Yet, his son is ill, and at the point of death. All his power and influence cannot save his "little boy".
I grew up with the notion, like many of us do, that my success was what determined my value as a person. I believed that if I were able to have a successful career, earn more money, and gain more influence I would be happier. I would have more freedom, be able to sort out my own problems, and become the master of my own destiny! Nothing could be further from the truth, and in this passage we can see the error of this notion made strikingly clear. This royal official should be able to leverage his wealth and influence to get the very best of care for his son, but even this won't save his life. He's probably tried everything in his power, but has been unsuccessful. He needs Christ.
I think many of us, myself included, envy the wealth and power of men like the royal official out of a desire for control. When we're faced with difficult circumstances it's easy to believe that having these earthly goods will help us resolve our problems. There is no denying that having money and power can give you access to, among other things, better quality health care, but ultimately our fate still rests firmly in the hands of God (Ecc 9:11-12). This passage reveals that wealth and power do not render us immune to suffering.
#christianity#catholicism#jesus#gospel of john#exegesis#bible quotes#biblical commentary#disordered paradigms#wealth#power
2 notes
·
View notes
Text
All of us suffer from disordered paradigms because we're surrounded by them, but when we're rooted in Christ we can rightly order our perspective of creation, other people and ourselves.
How many of us have a disordered view of what constitutes success, beauty, or happiness? When we pattern our lives on these disordered paradigms we set ourselves up for suffering, and perpetuate that suffering by passing it onto others. Christ provides the example we must pattern our lives on, and doing so ultimately leads us to true peace, joy, and salvation. Check out the linked post to learn more!
1 note
·
View note
Text
I've said it before and I'll say it again:
The words "neurodivergent" and "disorder" are opposites. There is no such thing as a "neurodivergent disorder" or "a disorder on the neurodivergent spectrum".
Imagine you got two pairs of glasses. One is called "pathology" and the other one is called "neurodiversity".
You cannot wear both pairs at the same time. You can choose, through which one you wanna look.
If you choose the pathology glasses, you can use "disorder" because only through the pathology lens, there are people who have disorders.
If you choose the neurodiversity paradigm, you can use "neurodivergent" because looking through the neurodiversity lens, there is no such thing as disordered. Just different.
The pathology paradigm and the neurodiversity paradigm are opposing paradigms. "Disorder" says, there is something wrong with someone. "Neurodivergent" says, they are different but not wrong. You cannot think there's something wrong with someone whilst they are just different and not wrong, it doesn't make any sense!
#neurodivergent#neurodiversity paradigm#autism#adhd#actually autistic#disorder#neurodivergence#pathology paradigm
7 notes
·
View notes
Text
"just because someone has a PD doesn't mean they're automatically going to be abusive": nodding, yes good, go on
"if they're abusive they chose to be that way": [EXTREMELY LOUD INCORRECT BUZZER NOISE]
#always a bad time when the paradigm pendulum overcorrects and swings too far into the opposite extreme#like we ARE remembering these are disabilities right. these are conditions that hijack cognition and impair healthy social function#and we ARE also remembering that abusive behaviours are not always conscious and calculated#it'd blow some people's minds how many situations that look like ''i'm gonna fuck up this person's life On Purpose and For Fun''#are actually not that at all. the abuser's brain was just extremely on fire all the time forever and they've never examined that#and OF COURSE their extremely-on-fire brain is their responsibility and it's going neglected#(which is a thing that happens for various reasons ranging from apathy/indifference to lack of resources to complete unawareness)#but i don't think that equals ''they're choosing to be Abusive'' as if the malignant behaviours that are common with unmanaged PDs#are a choice the person is making and not a symptom of a disorder that fundamentally warps how a person sees the world#and interacts with it#we're still making nonsensical divisions between ''the Good type'' and ''the Bad type'' and i don't think that gets us anywhere
7 notes
·
View notes
Text

Disorder (and the DSM) is a subjective term rooted in neuronormativity and by default; colonialism, captialism and white supremacy.
If disorder is the lens of the pathology paradigm, neurodivergent is the lens of the neurodiversity paradigm.
This is why disorder and neurodivergent are not interchangeable and why, if we are aiming to be neurodiversity affirming and unpack neuronormativity, we need to move away from disorder; a term that reinforces neuronormativity and pathologises anyone who diverges from it.
You cannot be neurodiversity affirming until you stop viewing people as having a disorder. If you can do it for Autism or ADHD, you can do it for every other neurodivergence.
Disorder isn’t neutral. Never has been.
@livedexperienceeducator
#neurodivergence is not disorder#neurodiversity paradigm#neurodiversity#neurodivergence#autism#adhd#ptsd#cptsd#complex trauma#mental health#psychology#diagnostic model#dsm#mad pride#psychiatry critical#language#resources
17 notes
·
View notes
Text
There were/are many things wrong with Bon Appetit, but it was absolutely mindblowing to me in 2018 to realize that some people talk about salt and butter/oil as valid, valuable, even essential ingredients for cooking, rather than dangerous and addictive substances that should be avoided as much as possible
#like. I didn't cook like my parents but I felt really bad about it#ESPECIALLY as a fat person#so to hear molly baz or whoever casually be like 'if you don't salt your pasta water you're crazy' was paradigm shifting for me#boring text posts#eating disorders cw#bon appetit
13 notes
·
View notes
Text

FACE DOWN ON THE FLOOR this is me easing back into drawing im hoping to finish a request or 2 tomorrow it just depends on how the day goes . ANYWAY here r some ocs u_u
#my art#do not copy trace or steal#mrb#ones an oc i recycled but she fits better here i think#i thiiink paradigms been shown before i know abbeys been shown before but the other 3 havent unless ive posted brandy#but i dont think so . yeah i looked i havent#new followers beware: i have i think abt my ocs too much disorder its so bad [not really] i have an oc universe ive been working on for#abt.? 4 years but a majority of the ocs are almost 9-10 years old#fun fact kaden my fursona is nine she turns ten in the fall#my marblerose ocs r a special interest of mine i could talk about them for ages i#im sorry this isnt wc content but also not really HBLDKJFHDFHGBD#anyway these r the antags of my story but not in order of importance#WELL LIKE depending on *where* in the story one person kinda gets a redemption but it depends on what u consider a redemption#after this im gonna lay down last night was the first time in what feels like a month i was able to sleep before midnight#ive been having such bad problems w sleeping#im squinting im not gonna proofread if you see errors kindly ignore them i think i hit all of my talking points if u want me to talk more#abt my ocs please let me know if im not busy ill drop whatever im doing to talk about them#THIS IS EMBARASSING I DID THE MATH WRONG kaden will be *nine* not ten thats the year after
18 notes
·
View notes
Text
It's Autism Appreciation Month, y'all and Time for a Shift in the Paradigm
The Rich Inner World of Autism, Its Gift to the World
I don’t know if it is just plain too hot and dry here in Phnom Penh this month — April is the last month before the monsoon rains come, so it is generally the hottest — or whether it has been organizing Autism Awareness Day activities for our school or whether it has been anticipating Autism Appreciation Month for the past year or what it is,…

View On WordPress
#Autism#Autism Acceptance Month#Autism Appreciation Month#Autism Awareness Month#Autism Spectrum Disorder#Neurodivergent#Neurodiversity#Paradigm
0 notes
Note
Hi, i just discovered your tumblr. For you, what is mental illness, then? What is depression? What is anxiety? What is autism? I want to understand your mind and your opinion, but I don't know where to start, so I'm going to send this question.
i would define 'mental illness' broadly as any cluster of behaviours, beliefs, or thought patterns that is described and pathologised by the medical authorities a person is subject to. within this very broad category we can make a first distinction:
people for whom the pathologised behaviours and thought patterns cause them genuine distress
people for whom they do not
this distinction speaks to several different purposes and outcomes of the medicalisation of human psychology, ranging from 'an attempt to ameliorate human suffering' to 'an attempt to enforce prescribed forms of social order and normality'. furthermore, the first category above should be further interrogated with attention to whether a person's distress arises from intrinsic experiential aspects or from attempting to survive in a social environment hostile to their needs.
i don't define 'mental illness' on the basis of biomarkers, neurobiology, or genetics, and neither does clinical psychiatry, despite roughly two centuries now of sinking time and money into trying to find such biological confirmations of socially and politically defined 'types'.
different diagnoses have different histories, social functions, and medical discourses attached. for example, of the three you listed, autism is the one most likely to be presented with 'neurodivergency', rather than disease, as the explanatory paradigm, though this is far from a universal approach amongst clinicians. autism is also the most likely of the three to be 'treated' through elaborate and abusive methods of trying to instill and enforce 'normal behaviour'; depression and anxiety are typically medicalised in a different way that emphasises an aberrant disruption to otherwise 'normal' functioning, even in chronic presentations, with different accompanying pharmaceutical and psychotherapeutic treatments. other diagnostic labels may function entirely differently: for example, consider the function of the relatively historically recent split between autism and schizophrenia, or the extent to which the historical concept of hysteria informs many personality disorder diagnoses.
ultimately a 'mental illness' is a constructed category: there is no essence of depression, no depression virus, and no universal biological marker to discover that unites all depressives or people diagnosed as such. this emphatically does not mean that the suffering described is not real or debilitating. it means that our particular ways of categorising, taxonomising, and pathologising it are socially and historically contingent, and any analysis of them that ignores their social and political functions and origins is incomplete and inaccurate.
673 notes
·
View notes
Text
One of the main problems I have with Trauma Discourse (besides the problems I’ve already outlined in all these other posts really just so many) is that calling a problem “trauma” transmutes it from a problem with a specific, identifiable, external cause to an inner “mental health” problem, the new “brain disease like diabetes” model.
If you say “He’s miserable because he’s being abused,” the solution is obvious: Stop abusing him. If you say “She’s depressed because of the trauma of being abused,” you’ve shifted the problem to her reaction, and now the solution becomes that she needs therapy or treatment or intervention to learn to process or heal from or cope with being abused.
Even in medical model advocates’ own pathology paradigm of “Post-traumatic stress disorder,” the “Post-” part is essential. The concept is supposed to refer to the stress that lingers after the trauma and danger is passed, not to the stress of ongoing danger.
Trauma discourse, as applied to public policy, has unhoused people having to sleep on the street until they’ve processed the trauma of sleeping on the street enough to be “mentally healthy” enough to deserve housing, and has schools cutting school lunch programs while training teachers in “trauma-informed” practices to help students with the trauma of being hungry.
674 notes
·
View notes
Text
to continuously believe that singlethood is the default for the human pysche is to ignore countless of cultural experiences, especially those that belongs to poc.
if you're against the idea that queer identities are illnesses, then you're against the idea that plurality is inherently a disorder. they are all just experiences that exists outside of anglo-saxon paradigm of humanity.
#endo safe#plural community#plurality#multiplicity#pluralgang#~thanë#i know that this isn't groundbreaking to say; but as long as there are willfully ignorant ppl out there:#i'll still be here saying the basic shit until it is understood.
162 notes
·
View notes
Text
I feel like people forget psychiatry is a paradigm we created with flaws and biases of our own and not something divinely decreed by reality . many forms of treatment are designed to profit off people's symptoms ongoingly without finding solutions in a holistic way. not to mention the ableism of how it's diagnosed which often stigmatizes people ("personality disorders") without recognizing the root cause (which is often a response to trauma/survival). Throughout history people have been damaged by treatments seeking to make them more palatable to society rather than improve their quality of life.
also the way that diagnoses are weaponized against patients. "oh, they're a (____), so you can't trust what they have to say." leaving them vulnerable to systematic abuse.
#saying this as someone whose mother was institutionalized throughout their life#and a sibling whose psychosis was triggered by medication#antipsych
375 notes
·
View notes
Text
Autism as a concept has lived in the pathology paradigm from the very beginning. That’s about a hundred years of seeing Autistic people as “broken” and in need of fixing. It is officially diagnosed as a “disorder,” and the diagnostic criteria are full of pathologizing language. So for most of society, negative language and attitudes around autism are “normal.”
To someone in the medical or mental health field, pathologizing language is also “normal.” Same goes for people in education, particularly special education. It’s just how they talk about patients and students, they don’t mean anything by it, you HAVE to talk about a person’s deficits/symptoms in order to get them help. It’s just…normal.
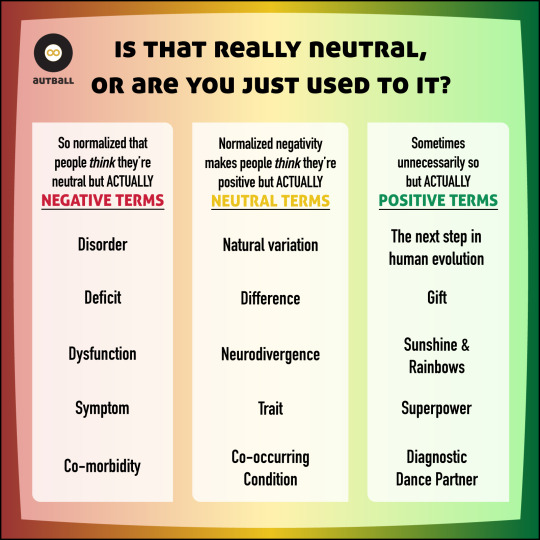
But sometimes, when something negative is normalized enough, people can mistake it for being “neutral.” Which leads to people arguing that the word “disorder” is neutral, and that the actually neutral language of neurodiversity is “overly positive.”
That’s all incorrect, though. The word “disorder” is not and was never intended to be neutral. The language used to diagnose autism as a medical/mental health condition is not and never has been neutral. And “normalized” is not the same as “neutral.”
And so, here’s a handy dandy (and slightly snarky) graphic for anyone out there whose frame of reference could use some re-centering.
NOTE: Genuine questions are fine. Attempts to argue that pathologizing medical language is neutral OR that autism is a disorder are not. If you are uncomfortable in the realization that the language you’ve been using contributes to negative attitudes towards Autistic people, that’s a sign that you have some stuff to learn, not an invitation to get defensive in my comments section.
ALSO NOTE: Nowhere have I told anyone how to refer to or think of *themselves,* so don’t come at me with that one either.
ALSO ALSO NOTE: I don’t actually endorse anything in the “positive” column either. It is strictly to demonstrate that there is a difference between neutral and positive language, and all of it is meant tongue-in-cheek. Toxic positivity and supremacy don’t help anyone.
#autistic#actually autistic#autism#autism acceptance#neurodiversity#neurodiversity paradigm#paradigm shift
83 notes
·
View notes
Text
So the thing I didn't mention in that poll I published yesterday is that the motor initiation piece that is, at the time of this writing, absolutely sweeping the poll as the Worst Thing people struggle with?
It's the specific thing I'm trying to pull together a grant for, perhaps unsurprisingly. But it's also the only one that actually isn't classically conceptualized as executive function. (I know, I know, that feels stupid to me, too.)
See, formally speaking, we describe executive function in terms of higher-order cognitive processes that allow us to complete complex tasks. There is a lot of work on, for example, "set shifting" (which is a particular paradigm for studying the ability to transition between different frames of mind, essentially; it's measuring cognitive flexibility) and on action inhibition / impulse control. (One of my colleagues works on set shifting, in fact, and I might actually take a look at that later.) We also have a lot of work on how individuals make decisions and prioritize conflicting needs.
But the transition between motivation and motion is a lot harder to study, and it doesn't fit so neatly into this top down paradigm, either. Most of the people who study this kind of movement initiation are people who aren't really focused on executive function per se at all. They're mostly people who work on Parkinson's, in fact.
The problem is that the best way to untangle how these systems work is to break specific things and see what impact that has on the overall function, and that means working with animal models. You know what we can't study as easily with animal models? Wanting to move and not being able to initiate self-paced motion—that is, we can't get inside an animal's head to understand what it wants to do in the absence of a moving body to indicate that thing. This is part of why many of our best studied kinds of executive dysfunction involve not doing a thing, rather than doing it: that way you can look at error rates and study a measurable change in behavior.
There are things we can do, though. For example, you can disentangle motivation versus pleasure in a rat that enjoys things but has no motivation to make them happen by asking questions like: I know that rats like water with sugar in it. If I set up a device that squirts a trickle of sugar water into the mouth of the rat, does it close its mouth? What facial expressions does it make? If I put bitrex in the water instead of sugar, does the reaction change? (Yes, emphatically.)
The thing is, motivation is regulated by dopamine... and so is movement. There's good reason to think that neurodevelopmental disorders like ADHD and autism are mediated by weird dopamine signaling patterns, and we certainly know that there is a direct relationship between abnormally high dopamine signaling and schizophrenia symptoms... and that abnormally low dopamine will give you Parkinsonian tremors.
Most stimulant meds for ADHD work by upregulating dopamine signaling, too. All of them are associated with increased locomotor activity, among other things. We know that dopaminergic signaling precedes actions in the body, too: you get firing before the actual motion happens.
Somewhere there is a threshold of motion initiation that is getting fuckily disconnected. I have some thoughts about where it is, but I definitely need to run some experiments to check my hypotheses against evidence.
#Executive function#Neurodivergence#autism#I have got to make myself some canonical tasks here#Tags not tasks#Animal research#Day job#Neuroscience
67 notes
·
View notes
Text
Witchgrass
by Louise Glück
Something
comes into the world unwelcome
calling disorder, disorder–
If you hate me so much
don’t bother to give me
a name: do you need
one more slur
in your language, another
way to blame
one tribe for everything–
as we both know,
if you worship
one god, you only need
one enemy–
I’m not the enemy.
Only a ruse to ignore
what you see happening
right here in this bed,
a little paradigm
of failure. One of your precious flowers
dies here almost every day
and you can’t rest until
you attack the cause, meaning
whatever is left, whatever
happens to be sturdier
than your personal passion–
It was not meant
to last forever in the real world.
But why admit that, when you can go on
doing what you always do,
mourning and laying blame,
always the two together.
I don’t need your praise
to survive. I was here first,
before you were here, before
you ever planted a garden.
And I’ll be here when only the sun and moon
are left, and the sea, and the wide field.
I will constitute the field.
447 notes
·
View notes
Note
Google isn't talking to me so you're the only person I can ask, I'm so sorry-
Is it possible to have NPD, APD, BPD AND HPD at the same time?-
It's honestly complicated. You know, personality disorders, particularly those within the same cluster, often share multiple traits at the behavioral level, such as attention-seeking, unstable personal relationships, and violent outbursts. However, similar behaviors can stem from very different motivations. For example NPD might act aggressively to dominate their partner and maintain their ego, while someone with BPD might exhibit the same behavior out of a fear of abandonment. What should technically allow for differentiation between disorders is their core mechanisms that underlie everything going wrong. However, in my opinion, this is largely a theoretical concept because the core of the psyche is interpreted differently across psychological paradigms. That's partially what makes diagnostic procedure so difficult. Also there are for example multiple studies about "BPD in men" or "APD in woman" which only showcases that classification is not carved in stone as symptoms can differ across other categories like gender. At the group therapy I encountered very few people with a single diagnosis. In the majority of cases, it was "XPD with traits of YPD" because fitting neatly into one prototype is not easy. Also DSM V is only one of available classifications, ICD lists like 5 more specific personality disorders.
What I'm saying is that the labels we use are the flawed results of statistical cluster analysis, and it's not uncommon for someone to exhibit traits that span across multiple clusters. In cases of someone showing traits from three or more personality disorders I would just describe it as mixed personality disorder or unspecified personality disorder, ICD style.
20 notes
·
View notes
Last Seen Blogs

chrjoon
TURPID

matthewjacoby1-blog
Matthew Jacoby Art

naatilvm
Natali ⭐

marzipanladyart
Sanctuary for DILFs