#SuicideEpidemic
Text
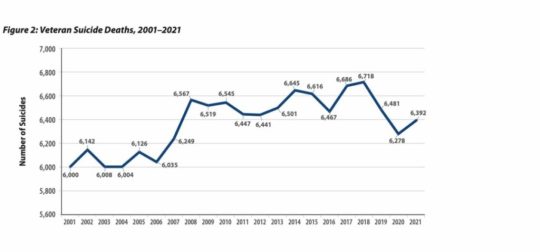
How Big is the Veteran Suicide Problem?

Overview of the policies and flawed science behind the Veteran suicide, drug overdose deaths, diabetic amputations, and mental health epidemics.
This series intends to tackle a range of subjects that afflict Veterans, especially suicide and drug overdoses which, along with diabetic lower limb amputations, are at epidemic levels. Across military medicine and traditional approaches to “mental health,” there is a wide gap between the VA's palliative care model – control the symptoms – and root cause analysis that gets at the physical damage to the brain and whole-body wellness and the brain wound healing called for. This includes proper diagnoses and a shift to an appreciation of polytrauma -- including the need for brain-wound healing -- and its long-term negative consequences.
We at TreatNOW, Grunt Style, America’s Mighty Warriors, and numerous other Veteran organizations are focused on Suicide Prevention. DoD and the VA declare that Suicide Prevention is their #1 priority. On this we can agree. Where we disagree is the protocols used by the VA and traditional medicine to diagnose what they call “mental health” issues, and their insufficient interventions. We differentiate between real mental health issues and brain wounds. The disagreement is fundamental, so much so that that we continue to call for an Inspector General report on the flawed science sponsored by taxpayers without their knowledge.
First, some perspective. We must separate scientific fact from the fiction spun by conclusions in Army/DoD/VA studies. The USG spent in excess of $186 Million on five clinical trials and came to flawed conclusions about the safety and efficacy of Hyperbaric Oxygen Therapy when used to treat TBI/PTSD. The Undersea & Hyperbaric Medical Society (UHMS) has finally set the record straight now that peer-reviewed science has again confirmed that hyperbaric oxygenation and medicine begin with any increase in pressure or oxygen concentration. Thus, the Army/DoD/VA dosing studies, along with the other 21 peer-reviewed clinical trials, confirm that HBOT helps heal brain wounds. The actual data in those government studies confirm what their editorial comments deny. And three of the Principle Investigators wrote positively in the studies and later commentary, confirming that HBOT is safe and effective:
- "Randomization to the chamber . . . . offered statistical and in some measures clinically significant improvement over local routine TBI care."
- “total scores for groups revealed significant improvement over the course of the study for both the sham-control group .... and the HBO2 group.”
- " is a healing environment."
- “Both intervention groups demonstrated improved outcomes compared with alone.”
- “HBO2 improved post-concussive and PTSD symptoms, cognitive processing speed, sleep quality, and balance function, most dramatically in those with PTSD.”
- “At least fair evidence was found that the intervention improves health outcomes and concludes that benefits outweigh harm. . . Hyperbaric oxygen therapy for mild traumatic brain injury and PTSD should be considered a legitimate adjunct therapy.”
- “We cannot ignore the fact that people got better.”
Second, HBOT has been shown to virtually eradicate suicidal ideation and allow patients to get off almost all prescribed drugs, including those that warn of suicidal ideation. The following chart from the VA makes clear that service member suicide deaths since 9/11 exceed 146,000. Prescribed drug overdose deaths during the same time period exceed 109,000. That’s over a quarter million avoidable deaths, even as the Veteran population has decreased. Add in the 796,340+ diabetic foot ulcer patients who have succumbed to death within 5 years following largely avoidable lower limb amputations -- most without ever being told that amputation could be avoided. That number of 796,340 veterans is more than all KIA since beginning of WWI (623,982)
Third, the picture that leads this piece is meant to convey a staggering realization of how government and public policies have led to unanticipated, negative consequences. The epidemics we are addressing here are such crises, with awful, reprehensible human consequences. Two examples: Tuskegee, and the near-eradication of the plains buffalo in the 19th century.
The government had its reasons to eliminate bison. "One of the biggest advocates of buffalo slaughter was General William Tecumseh Sherman. 'General Sherman remarked . . . . that the quickest way to compel the Indians to settle down to civilized life was to send ten regiments of soldiers to the plains, with orders to shoot buffaloes until they became too scarce to support the redskins.'" While it is possible to repopulate bison, the hundreds of thousands of Veterans now passed prematurely due to suicides, drug overdoses, and unnecessary lower limb amputations are not coming back. Nor are some 100 poor black citizens of Alabama.
"The Tuskegee Study of Untreated Syphilis in the Negro Male", conducted by the US Public Health Service and the CDC between 1932 and 1972, led to the unwitting deaths of nearly 100 subjects out of 400 due to complications of syphilis. Though penicillan was in wide use for nearly 30 years of the 40-year study, none of the participants was told of its availability and the near-sure cure of the syphilis after penicillan use. The Tuskegee experiment has been called one of the most significant events in the history of bioethics. In 1973, Senator Edward Kennedy conducted congressional hearings into the study. Those hearings led to the passage of the National Research Act and, in turn, the establishment of institutional review boards, principles of informed consent, and protection of vulnerable populations.
It took forty years for the government to end the Tuskegee experiment. The President Clinton apology contained these words: "No power on Earth can give you back the lives lost, the pain suffered, the years of internal torment and anguish. What was done cannot be undone. But we can end the silence. We can stop turning our heads away. We can look at you in the eye and finally say on behalf of the American people, what the United States government did was shameful, and I am sorry."
It's all too familiar: “If only one man dies of hunger, that is a tragedy. If millions die, that's only statistics.” Government policy in the case of Veterans has devolved to turning a blind eye and using statistics to paper over the preventable tragedies. Families of the dead die a little every day; yearly, authorities hold more conferences, pass more ineffective laws, and increase budgets for Suicide prevention strategies, even as the suicides continue to increase.
Veterans tell of a relentless cycle in the VA, familiar to the families of the brain wounded. The faceless bureaucracy and unending appointments that too often end in cancellation. The inhumanity affects veterans with brain wounds, or suffering from Burn Pit toxins, Camp Lejeune toxic water, or as far back as Agent Orange victims. It starts with denial: it didn't happen. Then delay: you'll have to wait. Then too often the deception: wounded are made to feel ghosted, met with indifference and a sense of betrayal. Inevitably, the drugs, the endless changes of prescriptions, dosages, and care givers. Many of those drugs lead to depression, adding to the need for anti-depressants that warn of suicidal ideation. And, too often, death: hundreds of thousands of suicides and drug overdoses.
This cycle can be broken. Denial, delay, deception, drugs, depression, death is not worthy of us. This series is an appeal to both law and our morality. We must look Veterans in the eye, especially the brain wounded, and tell them that we both can and will do more to make real brain wound healing treatments available. We must begin with acknowledgement of the real science, the positive changes in our understanding of brain wounding, and the mechanisms of action to heal those hundreds of thousands of Veterans denied a chance at a return to normal.
Part two will be a look at just how dangerous Modern War has become to the brain: BLAST Injury, Burn Pits, and the nature of whole body damage/polytrauma. It will include a primer on brain wounding that seeks to differentiate real physical damage from the "mental health" symptoms that remain the target of conventional military medicine.
Join us on the journey to explain, to understand, and to TreatNOW.
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can end suicidal ideation, help end symptoms of PTSD, and heal brain wounds to end the effects of BLAST injury, mild TBI Persistent Post Concussive Syndrome, and polytrauma. www.treatnow.org
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#blastinjury#brainhealth#braininjured#braininjury#brainwound#brainwounds#HBOT#HBOTTreatment#HeadImpact#HealingwithHyperbarics#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#PTSD#suicide#suicideepidemic#suicideideation#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#VA#VeteranSuicide#VeteranSuicidePrevention#Veterans
0 notes
Photo
Please check my new article out and please be there for those at their darkest moments. 🙏🏼 YOU ARE NOT ALONE!!! @pnkandco 💛💛 #linkinbio https://pnkandco.com/author/noorfatimanensey/ . . . . . . . . . . . #suicidepreventionweek #pintrest #youarenotalone #suicideepidemic #eastasia #mentalhealth #loveyourself #bethereforeachother https://www.instagram.com/p/CTb_8x7oy1D/?utm_medium=tumblr
#linkinbio#suicidepreventionweek#pintrest#youarenotalone#suicideepidemic#eastasia#mentalhealth#loveyourself#bethereforeachother
0 notes
Text
#JamesDonaldsononMentalHealth - Why More #PoliceOfficers Are Committing #Suicide — And How We Can Help Save Them
#JamesDonaldsononMentalHealth – Why More #PoliceOfficers Are Committing #Suicide — And How We Can Help Save Them

Five Chicago police officers died by suicide in the last six months of 2018. Eight more have died at their hand in Chicago this year.
#Policedepartments are failing. Failing at helping their own. For too long, the traditional culture of the policing profession has turned a blind eye on the growing prevalence of death by #suicide in its ranks.
#Police #suicide is a topic that has finally…
View On WordPress
#JamesDonaldson#JamesDonaldsonMentalHealth#JamesDonaldsonNotes#JamesDonaldsononMentalHealth#PoliceDepartment#Policeofficer#Policeofficers#SuicidalAttempt#SuicidalIdeation#SuicidalIdeations#SuicidalThoughts#SuicideAwarenessVoicesofEducation#SuicideClusters#SuicideContagion#SuicideEpidemic#SuicidePrevention#SuicidePreventionSummit#SuicideRisk#SuicideRiskFactors#YourGiftofLifeFoundation#Depression#Police#Stigma#Stress#Suicide
0 notes
Photo

Our imperfect hearts/balance light-dark, joy-grief,/love-hate, weigh life’s worth. #haiku #senyru #lagunabeachpoet #icarryyourheart #imperfecthearts #mentalhealthawareness #suicideprevention #suicideepidemic #anthonybourdainrip #compassionhelps #poetrycommunity #natureheals #imperfectionisbeauty (at Laguna Beach, California)
#poetrycommunity#senyru#compassionhelps#natureheals#mentalhealthawareness#imperfectionisbeauty#haiku#suicideprevention#anthonybourdainrip#imperfecthearts#suicideepidemic#lagunabeachpoet#icarryyourheart
0 notes
Link
0 notes
Text
Bad Trip: Expert says VA studies psychedelics but ignores proven Hyperbaric Oxygen Therapy!
Eye on Veterans
This week we’re talking with Dr. Robert Beckman, Executive Director of Treat Now dot org. He’s one of the premiere experts in the treatment of brain wounds with Hyperbaric Oxygen Therapy (HBOT). Although this technology is FDA approved for things like burns and diabetic foot ulcers, Beckman says the VA ignores proof that it's effective for treating brain wounds, TBI’s, concussions and depression which has fueled the suicide epidemic in America.
While ending suicide remains a top priority for VA , DoD, Beckman slams their decision to pump millions of mental health dollars into psychedelic research to merely treat symptoms. He offers several real-world examples of HBOT effectively treating the root cause and thus eliminating symptoms in ways current VA strategies do not.
In one powerful segment he shares how over the years the VA has amputated hundreds of thousands of feet, due to diabetic foot ulcers. Beckman claims most of which could have been avoided if HBOT was introduced earlier in their care.
He also shares vivid examples; NFL players treating concussions, combat veterans' fighting effects of toxic exposures and many clinics who are currently embracing HBOT therapy for treatment of brain wounds, PTSD and MS.
For more on Hyperbaric Oxygen Therapy including powerful research data and published studies, see TreatNow.org's website:
https://treatnow.org/
Read the latest newsletter "VA Continues to Avoid Treating and Healing Brain Wounds" here:
https://treatnow.org/va-continues-to-avoid-treating-and-healing-brain-wounds/
VIDEO: MSG Scott Rossler's HBOT testimony
https://youtu.be/N-CkR5shqEM?si=UmUhF_jKxPHjjzkq
VIDEO: NFL great Joe Namath shares how HBOT changed his life:
https://youtu.be/s7nxU3QadIA
To reach CBS Eye on Veterans, Host, Phil Briggs
[email protected]
Follow on X
@philbriggsVet
@EyeOnVeterans
Read the full article
#AirForce#ARMY#brainwound#brainwounds#concussion#currentevents#depression#HealingwithHyperbarics#marinecorps#military#MilitarySuicide#Navy#POLITICS#POPCULTURE#suicideepidemic#TBI#unitedstatesveterans#veteranaffairs#Veterans#VeteransAdministration
0 notes
Text
VA Continues to Avoid Treating and Healing Brain Wounds

2024 reminds us that the Veterans Administration continues off-course by avoiding actual brain wound healing while pumping more $$$$ into research, "Mental Health," and achieving a new normal. Meanwhile, the suicide rate continues upward.
ProPublica reports "How the VA Fails Veterans on Mental Health." In what has become an almost annual body count, investigative reporters analyzed 313 studies conducted by the VA's inspector general in recent years showing how repeated failures in behavioral care in the VA continue to lead to suicides.
"The problems appear to be systemic. Over and over, the hospitals and clinics in the VA’s sprawling health care network have fallen short when it comes to treating people with mental illness. . . . In the most extreme cases, facilities lost track of veterans or failed to prevent suicides under their own roofs."
Given the rise in the suicide rate among Veterans, the report veers into complicity when it states: "The system has notable strengths. The VA has played an important role in developing treatments for conditions such as post-traumatic stress disorder and traumatic brain injury, and provides critical training opportunities for psychiatrists, psychologists and social workers nationwide."
Combat Veterans constantly report to TreatNOW that they're treated like "guines pigs" by a constantly shifting and sketchy string of care providers. The ProPublica reporting indicates a severe breakdown in the VA's basic understanding of the physiology of brain wounds, repeating year after year that "mental health" is the issue. Recall that in too many cases the VA continues to insist on PTSD diagnoses for combat veterans without proof of brain damage.
And recruitment for understaffed medical professionals is for the Mental Health disciplines, not for a rethinking of how to properly diagnose and heal brain wounds. Physical healing has to replace psychology as the focus of standard of care for TBI.
And consider: The VA runs a number of War Related Illness and Injury Study Centers (WRIISC). This national program is dedicated to Veterans’ post-deployment health concerns and unique health care needs. They "develop and provide post-deployment health expertise to Veterans and their health care providers through clinical care, research, education, and risk communication. The WRIISC is part of VA’s newly designated Health Outcomes Military Exposures (HOME) formerly Post Deployment Health Services (PDHS). The VA is uniquely qualified to care for Veterans with health concerns related to potentially toxic exposures."
These Centers are allegedly the Gold Standard for delivering the world's best care for "the #1 clinical priority" in DOD and the VA: suicide prevention. But the protocols, research, and culture are opposed to even mentioning Hyperbaric Oxygen Therapy as even a consideration, let alone providing the treatment. At a minimum, they might consider putting some intellectual firepower behind a proper Phase 3 clinical trial to answer the outstanding questions about maximizing the efficacy of HBOT for Mild Traumatic Brain Injury Persistent Postconcussion Syndrome.
Days ago, the Department of Veterans Affairs issued an intention to study the use of certain psychedelic compounds in treating posttraumatic stress disorder (PTSD) and depression. The substances to be studied include psychedelic compounds such as psilocybin and Methylenedioxymethamphetamine (MDMA) when used in conjunction with psychotherapy to treat Veterans with PTSD and depression. This continues the VA's penchant to study "mental health" problems rather than solving them. As always, they revert to their inadequate interventions:
- Psychopharmacology
- Cognitive Processing Therapy (CPT)
- Eye Movement Desensitization and Reprocessing (EMDR)
- Prolonged Exposure (PE) or Trauma-Focused Psychotherapy
Adding yet more symptom-reduction chemicals and computer-based coping tools to the mix continues to avoid proper diagnosis and brain wound healing, particularly in the cases of combat veterans.
Here's the primer the VA needs to memorize. While this is not taught in medical schools, worldwide science supports these conclusions:
- TBI/Concussion/BLAST cause brain wounds.
- The pathophysiology of brain wounds includes a concussion cascade, a penumbra of damage that can lead to cell death and a host of behavioral, cognitive, memory and emotional problems. It is increasingly clear that CTE can be a result of this damage.
- Interrupting that cascade can halt and reverse the damage cause by inflammation, hypoxia, necrotic cell death, blood-brain barrier breakdown, and numerous other well-documented effects of brain wounding.
- Only by focusing on wound healing can a patient get on the path back to total body health, and a chance of pain- and drug-free living.
- Hyperbaric Oxygen Therapy (HBOT) is a proven, FDA on-label available intervention that reduces inflammation, leads to biogenesis, neurogenesis, angiogenesis, neuroplasticity, proliferation of stem cells, pain reduction, halts suicidal ideation, and allows patients to get off death-inducing drugs.
- Polytrauma -- a condition of multiple traumas endured by a patient -- is a complex of injuries typically suffered in BLAST injuries.
- Every Veteran with diagnosed or suspected brain wounds needs to be told that HBOT can help heal their wounds.
- And while the VA is waking up to the truth about healing vs. palliating, they should be required, under the mandate of "informed consent" to use HBOT for Diabetic Foot Ulcers.
- There are over 100,000 Veteran suicides since 9/11, and over 876,000 Veteran deaths attributable to lower limb amputations. The VA must be held accountable for using EVERY means available to stop the carnage.
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can end suicidal ideation, help end symptoms of PTSD, and heal brain wounds to end the effects of BLAST injury, mild TBI Persistent Post Concussive Syndrome, and polytrauma. www.treatnow.org
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#blastinjury#brainhealth#braininjured#braininjury#brainwound#brainwounds#HBOT#HBOTTreatment#HeadImpact#HealingwithHyperbarics#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#PTSD#suicide#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#VA#VeteranSuicide#VeteranSuicidePrevention#Veterans
0 notes
Text
NYT: Friendly Fire Leads to Brain wounding

Pentagon researchers say weapons like shoulder-fired rockets expose troops who fire them to blast waves far above safety limits, but they remain in wide use.
As we have reported for years, BLAST injury does not respect your nationality, gender, origin of the weapon, or your intention. As Dave Philipps of the New York Times reports, U.S. Troops are still training on weapons with known risks of delivering brain wounds.
As Phillips reports, studies by the Navy, the Center for New American Security, the Swedish military, DoD, SEALs, DARPA, Johns Hopkins, and UHUHS all warn of real damage inflicted by "friendly fire".
The search, research, measurements, data bases, added budgets, and periodic expressions of concern from DoD leadership can be viewed in one of two lights: they know and they don't care; or, they know and they dont' know what to do in the interim. Modern warfare, as Ukraine proves daily, requires more and more destructive firepower just to defend territory, let alone regain strategic and tactical advantage.
So, what can done in the interim? "For generations, the military assumed that this kind of blast exposure was safe, even as evidence mounted that repetitive blasts may do serious and lasting harm. . . . Top leaders talk of the importance of protecting troops’ brains, but the military fails to take practical steps to ensure safety."
Literature on BLAST injuries over the past decade overwhelmingly tends in the direction of Recommendations to find ways to protect soldiers with new and improved helmets, reduced weapon firings, education, more research, more funding, and, over time, resort to robots to do the heavy firing.
Sadly for the soldier, for 100 years we've known that BLAST causes brain wounds. Even though a century of research has not definitively "proved" the Mechanisms of Action involved in causing physical, mental, behavioral, cognitive, and moral damage, we do know that the net effects of only palliating symptoms won't lead back to a normal, healthy brain.
So here's a list of helpful suggestions to DoD/VA to help Warriors, Veterans, indeed anyone exposed to BLAST injury or brain wounding. Let all the research continue on mitigating the potential and actual damage caused by exposure to BLAST. Add more drugs and hallucinogenics and psychotropics to the list of possible "solutions." But let's focus some of our work on healing the wounds to the brain and body caused by BLAST exposure. An estimated 877,000 Veterans and active duty service members -- probably many more as we learn about the pervasiveness of self-inflicted BLAST injury -- are already suffering with some degree of brain wounding. Let's focus on HEALING THEIR BRAIN WOUNDS as we work the prevention side of the equation. Here's a modest proposal:
Daily suicide rates, accumulating suffering, and impacts on families demand that we deal with brain wounds. We cannot continue to ignore treatments that work are safe, scientifically validated, and readily available. We cannot hide this information from the wounded. Informed consent and medical ethics demand that DOD/VA tell the wounded what is available, even though it is "off-label." Every treatment, drug, process, procedure, device and protocol currently used by DoD/VA is off-label and not approved by the FDA for treating TBI/PTSD.
Keep doing what you're doing. But hold open the possibility that alternative therapies exist that are scientifically valid, clinically proven, widely available, cost effective and demonstrated safe and effective. Fund them.
Rethink a Suicide Prevention Strategy that is void of any options to treat brain wounds. Too may Veterans commit suicide -- over 109,000 -- perhaps falling into depression from undiagnosed and untreated brain wounds.
Hyperbaric Oxygen Therapy (HBOT) is one such therapy, backed by decades of research, acceptance by the FDA for wound healing, and proven in multiple scientific studies to reduce or eliminate symptoms caused by TBI/PTSD/Concussion/BLAST.
HBOT is proven to reduce and/or eliminate suicidal ideation in tens of thousands of uses .
Read, really read, the current scientific literature on the validity of objective research conducted over the past fifteen years. Notice that the UHMS and the overwhelming number of real HBOT researchers know that HBOT works to help heal TBI/PTSD. Even government researchers, a few of whom still cling to the canard that "HBOT does not work," accept that patients in their studies got better .
If necessary, take 10% of the VA drug budget and use it to fund HBOT treatments in private clinics where the cost is miniscule compared to current standards of care. It is a well-known fact that fully treated HBOT patients get off almost all their drugs, many of which warn of "ideation of suicide." There will be a net return of billions of dollars to the VA bottomline due to reduced need for prescriptions.
Redo your cost analyses when considering where to spend dollars on rehabilitation of brain wounded combat Veterans. It has been calculated that the cost of NOT treating brain wounded Veterans will exceed $4Trillion over their 40-year lifespan. That's a degraded life, for the Veteran and the family, living with symptoms that plague far too many Veterans. For less than 1/2 of 1% of that cost, all 877,450 brain-wounded Veterans can be fully treated with HBOT.
DoD and the VA should insure and reimburse HBOT-for-TBI treatments. Start with Informed Consent: let every Veterans know that HBOT can help heal their brain wound.
And consider the following: service members returning from combat suffer from polytrauma unlike ever before. Knowing what we know now about the prevalence of BLAST injury, Burn Pit toxins, unreported brain trauma, the sustained pace of combat for Special Operations warriors, we need to provide functional medicine approaches to whole body wellness, starting with but not limited to brain wounds. All body systems are negatively affected by BLAST. HBOT works to relieve pain, reduce inflammation, speed healing, restore function, promote the growth of new stem cells, and allow battle-weary warriors to return to peak performance more quickly.
Part of the history of HBOT is that the history of HBOT safety and efficacy is ignored or forgotten. This is a page out of the Textbook of Military Medicine, updated in 2006. This same algorithm is in the textbook in the 1980s. The “definitive therapy” then and is HBOT treatment for TBI resulting from BLAST Exposure.

The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can end suicidal ideation, help heal the effects of BLAST injury, TBI/PTSD, and acute concussion.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#blastinjury#brainhealth#braininjured#braininjury#brainwound#concussion#concussionprotocol#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicidalideation#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Text
New York Times: USMC Blast Injury Update

Partial Explanation why Marines report Highest Suicide Rate since 2011, Navy since 2019
Dave Philipps, Pulitzer prize-winning and NYT reporter, has filed another report on continuing investigations into BLAST injury. He does it through a look at the US strategy of using firepower to destroy ISIS in Iraq and Syria. "A Secret War, Strange New Wounds, and Silence From the Pentagon" tells a sad tale but neglects a open secret: blast injury has been known for decades to cause brain wounds. "Strange New Wounds" have been known for fifteen years as "THE INVISIBLE WOUNDS OF WAR."
"An investigation by The New York Times found that many of the troops sent to bombard the Islamic State in 2016 and 2017 returned to the United States plagued by nightmares, panic attacks, depression and, in a few cases, hallucinations. Once-reliable Marines turned unpredictable and strange. Some are now homeless. A striking number eventually died by suicide, or tried to."
Too many of the wounded were forced out of the military without any medical help. The Epoch Times did a long two-part report on the same maladies caused by the deployment that led to tens of thousands of concussive friendly-fire BLAST waves hitting the artillerymen. The stories in the Epoch Times drew attention to the work of USJAG. Robert Alvarez, Nic Gray, and Jeremy "Weed" Sorenson are doing the heavy lifting exposing the unreported brain wounding and the downhill slide into Other Than Honorable discharges for too many of these wounded warriors. USJAG and a few intrepid reporters are uncovering the systemic flaws in our "mental health" approach to unrecognized physical damage wrought by war. And they are seeking redress of the further damage done by bureaucracies ignorant of the pain and suffering of the brain wounded.
The military and the VA continue in their willful ignorance about the reality of brain wounding and the scourge of TBI/PTSD injuries going unreported, undiagnosed, and untreated. Worse, lacking a service-wide education about the reality of brain wounding and its impact on behavior and performance and readiness of individuals, and the force more broadly, the wounded will continue to be mistreated by a medical community and command structure that has little sense of urgency about the need to treat brain wounds.
A curious and ineffective response has set in, reminiscent of the dilatory approach to Burn Pits and Agent Orange. "Paralysis through analysis" has taken hold once again. "We need to study the problem." "We just don't know enough yet." Meanwhile the suicide rate continues its upward trend and the researchers claim they need more time and money before they can even know what has happened. Time and again, the focus is on diagnosis, to the detriment of the wounded who continue to deteriorate, without even health insurance, disability payments, and an end to their careers. And treatments that have been proven safe, effective, and low-cost -- and which can be employed immediately -- are disdained as unproven, unsafe, too risky, too costly, and lacking in evidence. The simple fact is that medicine is willfully ignorant about hyperbaric medicine and likely to stay that way, despite overwhelming evidence, without intervention by Congress and the White House, as with Burn Pits.
Here are five take-aways from the NYT study:
** To defeat ISIS, the United States relied on artillery crews firing more intensively than any had in generations.
** Many members of the gun crews developed devastating and puzzling symptoms.
** When the troops started to act strangely, they were often treated ineffectively or punished.
** Studies are starting to reveal the risk posed by blast exposure, but progress is slow.
** The military says it now has safeguards to protect from blasts, but it is not clear that much has changed.
Here are five ALERTS to those who are still wondering if BLAST injuries exist. Brain wounding from friendly fire is not merely a Mental Health issue. Impaired performance is not the the victim's fault due to personal weakness, nor is it amenable to talk therapy and drugs that merely mask symptoms.
** The ground-breaking 2016 Lancet study sponsored by the Defense Health Program of the United States Department of Defense states: "scientific literature from the past 100 years shows that a substantial percentage of blast-exposed service members have persistent neurological or behavioral symptomatology."
** Breacher Syndrome and "Operator Syndrome" are real. Science and research will catch up to reality on the ground, facts which should be obvious to anyone paying attention.
** The modern Carl Gustav recoiless rifle, in operation since at least 1984, comes with warnings not to fire more than six rounds in a 24-hour period. The Danes seem to have understood BLAT damage four decades ago.
** Shoot rooms instructors and EOD personnel are well-known to suffer inordinately from recurring blasts and subconcussive impacts over years of exposure -- not unlike athletes subjected to repetitive head impacts.
** The "Invisible Wounds of War" are no longer "invisible" to anyone who cares about "root cause analysis". While brain wounds happen inside the head (and are frequently part of the polytrauma of combat), they can be "seen" via scans, functional and physiological outputs, symptom recognition, self-reporting, and careful diagnostics. Neglecting to diagnose and to treat brain wounds while waiting for more science in the face of a suicide epidemic is essentially medical malpractice. We KNOW, and we choose to shift the blame onto the victim or the "inadequacy" of scientific research.
Continuing malfeasance. US troops at two airbases in Iraq were injured during a Jan. 8, 2020 Iranian missile attack on Al Asad Air base. Once again, even years after Blast injury was finally recognized as a direct cause of brain wounds the US initially declared that no one was hurt in the attack. Dozens of diagnoses later, we now recognize BLAST injuries riddled those under the hail of missiles. (Just imagine the damage being done in Ukraine and the Middle East.)
One is reminded of the early military culture around Burn Pits: "nothing to see here; no damage." We know more now, and the VA, at least, presumes that proximity to Burn Pit toxic clouds causes physical damage and accepts responsibility to treat and help heal that damage. How long will it take the DoD and the VA to recognize that Blast damage is real, and can cause physical wounds to the brain and body? Further, how long before they link brain wounds to suicidal ideation? And that there is a treatment -- Hyperbaric Oxygen Therapy (HBOT) -- that virtually eliminates suicidal ideation and helps heal those brain wounds without drugs and other ineffective interventions?
The TreatNOW Coalition, alongside USJAG, has begun working with some of the casualties of the bombardments. USJAG are the pro bono advocates for those accused of Other Than Honorable behavior and subjected to fraudulent and penalizing discharges.
* * * * * * * * * * * *
The TreatNOW Coalition's pro bono Mission is to end service member suicides. The USMC reported this week that suicides are at an all-time high. TreatNOW HBOT Coalition clinics have demonstrated 100% safety and over 90% success in treating over 21,000 service members, Special Operators, first responders, athletes, and citizens with TBI/PTSD/Concussion. Brain Wounds like those described here can be successfully and safely treated and helped to heal with HBOT.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
The information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#blastinjury#braininjury#Brainwounding#concussion#HBOT#hyperbaric#HyperbaricOxygentherapy#Lestweforget#memorialday#mentalhealth#oxygen#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePreventionFunding#TBI#traumaticbraininjury#VA#VeteranSuicide#Veterans#VeteransAffairs
0 notes
Text
BRAIN WOUND UPDATE #15: Suicide hotline botched veteran's cry for help. An investigation found critical breakdowns

BRINGING YOU CURRENT INFORMATION ABOUT HOW TO HELP TREAT AND HEAL BRAIN WOUNDS: CONCUSSIONS, TBI, PTSD
USA TODAY Vanessa Arredondo Donovan Slack
Workers at the national Veterans Crisis Line mismanaged communication with a veteran who died by suicide within an hour of texting the hotline and failed for 10 years to establish protocols to save veterans' text messages for future follow-up, according to a report by the U.S. Department of Veterans Affairs Office of the Inspector General.
The independent watchdog's report issued the events leading up to the death in San Antonio in 2021 and "problematic" actions taken by leaders at the crisis line afterward. The investigation found crisis line staff failed to ensure a plan was in place to try and prevent the suicide and to adequately document communication with the veteran. The staff also didn't tell local VA staff in Texas about the death.
"Suicide prevention is the No. 1 clinical priority for VA, and the VCL is an important part of VAs suicide prevention efforts," VA Inspector General Michael Missal told USA TODAY. "Unfortunately, in this situation, the VCL failed to help a veteran in need."
The inspector general's investigation revealed procedural problems at the crisis line relied on by millions of veterans across the country as a critical safety net, including the silent monitoring of calls and the issues with saving text messages with veterans.
The VA Undersecretary for Health Dr. Shereef Elnahal said in response to the findings released last week that the Veterans Health Administration is "incredibly saddened by the loss of this Veteran and our thoughts are with the Veteran’s family."
It's not the first time the hotline has drawn the attention of investigators. Ten years after it launched in 2007, the hotline, created to connect veterans with specially trained responders, was sending about a third of its calls to backup call centers or voicemail. Other concerns identified by the inspector general at the time included long hold times and inadequate training, guidelines, and quality assurance.
The Veterans Crisis Line has fielded a record number of cries for help in recent years. Since July 2022, the hotline received more than 750,000 calls, a 12.5% increase from a year earlier, and 250,000 other contacts including texts and chats, VA stats show.
Crisis line responder missed signs
In the San Antonio incident, a crisis responder inadequately assessed the 31-year-old veteran's history of post-traumatic stress disorder and suicidal behavior, missing the signs of an impending attempt during the text conversation one night in 2021, the inspector general found. The staffer also failed to note the veteran’s alcohol use and did not establish an effective safety plan or confirm access to lethal weapons or other means to die by suicide.
The veteran had a history of depression and PTSD and had been flagged as being at high risk for suicide but the flag was removed in early 2020. When the vet contacted the hotline by text at 10:14 pm in early 2021, the responder made a note that the veteran planned to die by suicide and was in a "shed with a belt around a hook that hangs from the rafters of the shed," and "reached out tonight in order to stop from taking action to end (the patient's) life," according to the inspector general's report.
At the same time, during the text conversation, the patient, who was not identified by name in the report, said they weren't being "entirely honest." The responder documented a "safety plan" that said the veteran would text a family member for help, go to bed, and wait for someone to call and follow up the next day.
But the veteran never went into the house and didn't go to bed. The vet died by suicide at 11:40 p.m. – 38 minutes after sending a last message to the crisis line.
The responder reported in notes that the veteran "stayed online until the call ended normally" and with an "agreement to enact a plan of safety," despite not hearing anything from the veteran after 11:02 p.m. even as the responder messaged the patient for half an hour with no response, according to the report.
Investigators concluded the responder underestimated the patient’s suicide risk and failed to follow up when they stopped texting, according to the report. In addition, they found the hotline hadn't established adequate procedures since 2011 for keeping text messages on file, limiting the ability of VA personnel or investigators to ensure the hotline is providing quality service to the thousands of veterans who now depend on it.
'Don't volunteer anything extra'
Investigators from the inspector general's office said crisis line leadership also delayed and inadequately disclosed notice of the patient’s death. The national hotline did not conduct a "root cause" analysis of the incident, which is required within 45 days, until the inspector general became involved about 11 months after, according to the report.
The investigation further revealed that the hotline’s director of quality and training may have coached the responder after the incident, potentially compromising the staffer’s "candidness" during reviews of what happened, officials said. In an instant message to the responder ahead of an inspector general interview, the director said the "main points are to only answer the question asked – don’t volunteer anything extra."
Staff at the VA hospital in San Antonio were notified four days after the death but didn't note it in the veteran's medical records for months. In the meantime, VA staff continued calling and sending mail as if the veteran were still alive, exacerbating the family's grief.
VA vows to strengthen suicide prevention
The inspector general’s latest recommendations include that the crisis line review staff correspondence with all patients and make clear suicide risk assessment guidelines for responders. The text messaging platform is expected to be updated with the latest guidelines for suicide risk response and documentation in 2024, according to the report.
"VHA is committed to performing at the highest standards and finding ways to improve our response to Veterans in crisis," Elnahal wrote. "Any Veteran suicide is one too many and VHA remains steadfast in our mission to support those in suicide crisis. We are utilizing this review to strengthen processes for improved suicide prevention."
Missal, the VA inspector general, told USA TODAY: "It’s critical that VCL leaders ensure that staff are properly trained and incidents are adequately reviewed."
The Senate Veterans Affairs Committee met Wednesday to evaluate the VA's mental health and suicide prevention measures. National Director of VA Suicide Prevention Matthew Miller said the crisis line will expand staff size, implement pilot programs, and conduct analysis and research to provide outreach and mental health resources to veterans.
"With no single cause, there is no single solution, and we must be comprehensive in our approach to prevent Veteran suicide," added Miller during the hearing.
If you or someone you know is struggling or in crisis, help is available. Call or text 988 or chat 988lifeline.org
##########
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can help heal the symptoms and effects of acute concussion/TBI/PTSD by helping heal brain wounds.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#brainhealth#concussion#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Text
BRAIN WOUND UPDATE #15: Suicide hotline botched veteran's cry for help. An investigation found critical breakdowns

BRINGING YOU CURRENT INFORMATION ABOUT HOW TO HELP TREAT AND HEAL BRAIN WOUNDS: CONCUSSIONS, TBI, PTSD
USA TODAY Vanessa Arredondo Donovan Slack
Workers at the national Veterans Crisis Line mismanaged communication with a veteran who died by suicide within an hour of texting the hotline and failed for 10 years to establish protocols to save veterans' text messages for future follow-up, according to a report by the U.S. Department of Veterans Affairs Office of the Inspector General.
The independent watchdog's report issued the events leading up to the death in San Antonio in 2021 and "problematic" actions taken by leaders at the crisis line afterward. The investigation found crisis line staff failed to ensure a plan was in place to try and prevent the suicide and to adequately document communication with the veteran. The staff also didn't tell local VA staff in Texas about the death.
"Suicide prevention is the No. 1 clinical priority for VA, and the VCL is an important part of VAs suicide prevention efforts," VA Inspector General Michael Missal told USA TODAY. "Unfortunately, in this situation, the VCL failed to help a veteran in need."
The inspector general's investigation revealed procedural problems at the crisis line relied on by millions of veterans across the country as a critical safety net, including the silent monitoring of calls and the issues with saving text messages with veterans.
The VA Undersecretary for Health Dr. Shereef Elnahal said in response to the findings released last week that the Veterans Health Administration is "incredibly saddened by the loss of this Veteran and our thoughts are with the Veteran’s family."
It's not the first time the hotline has drawn the attention of investigators. Ten years after it launched in 2007, the hotline, created to connect veterans with specially trained responders, was sending about a third of its calls to backup call centers or voicemail. Other concerns identified by the inspector general at the time included long hold times and inadequate training, guidelines, and quality assurance.
The Veterans Crisis Line has fielded a record number of cries for help in recent years. Since July 2022, the hotline received more than 750,000 calls, a 12.5% increase from a year earlier, and 250,000 other contacts including texts and chats, VA stats show.
Crisis line responder missed signs
In the San Antonio incident, a crisis responder inadequately assessed the 31-year-old veteran's history of post-traumatic stress disorder and suicidal behavior, missing the signs of an impending attempt during the text conversation one night in 2021, the inspector general found. The staffer also failed to note the veteran’s alcohol use and did not establish an effective safety plan or confirm access to lethal weapons or other means to die by suicide.
The veteran had a history of depression and PTSD and had been flagged as being at high risk for suicide but the flag was removed in early 2020. When the vet contacted the hotline by text at 10:14 pm in early 2021, the responder made a note that the veteran planned to die by suicide and was in a "shed with a belt around a hook that hangs from the rafters of the shed," and "reached out tonight in order to stop from taking action to end (the patient's) life," according to the inspector general's report.
At the same time, during the text conversation, the patient, who was not identified by name in the report, said they weren't being "entirely honest." The responder documented a "safety plan" that said the veteran would text a family member for help, go to bed, and wait for someone to call and follow up the next day.
But the veteran never went into the house and didn't go to bed. The vet died by suicide at 11:40 p.m. – 38 minutes after sending a last message to the crisis line.
The responder reported in notes that the veteran "stayed online until the call ended normally" and with an "agreement to enact a plan of safety," despite not hearing anything from the veteran after 11:02 p.m. even as the responder messaged the patient for half an hour with no response, according to the report.
Investigators concluded the responder underestimated the patient’s suicide risk and failed to follow up when they stopped texting, according to the report. In addition, they found the hotline hadn't established adequate procedures since 2011 for keeping text messages on file, limiting the ability of VA personnel or investigators to ensure the hotline is providing quality service to the thousands of veterans who now depend on it.
'Don't volunteer anything extra'
Investigators from the inspector general's office said crisis line leadership also delayed and inadequately disclosed notice of the patient’s death. The national hotline did not conduct a "root cause" analysis of the incident, which is required within 45 days, until the inspector general became involved about 11 months after, according to the report.
The investigation further revealed that the hotline’s director of quality and training may have coached the responder after the incident, potentially compromising the staffer’s "candidness" during reviews of what happened, officials said. In an instant message to the responder ahead of an inspector general interview, the director said the "main points are to only answer the question asked – don’t volunteer anything extra."
Staff at the VA hospital in San Antonio were notified four days after the death but didn't note it in the veteran's medical records for months. In the meantime, VA staff continued calling and sending mail as if the veteran were still alive, exacerbating the family's grief.
VA vows to strengthen suicide prevention
The inspector general’s latest recommendations include that the crisis line review staff correspondence with all patients and make clear suicide risk assessment guidelines for responders. The text messaging platform is expected to be updated with the latest guidelines for suicide risk response and documentation in 2024, according to the report.
"VHA is committed to performing at the highest standards and finding ways to improve our response to Veterans in crisis," Elnahal wrote. "Any Veteran suicide is one too many and VHA remains steadfast in our mission to support those in suicide crisis. We are utilizing this review to strengthen processes for improved suicide prevention."
Missal, the VA inspector general, told USA TODAY: "It’s critical that VCL leaders ensure that staff are properly trained and incidents are adequately reviewed."
The Senate Veterans Affairs Committee met Wednesday to evaluate the VA's mental health and suicide prevention measures. National Director of VA Suicide Prevention Matthew Miller said the crisis line will expand staff size, implement pilot programs, and conduct analysis and research to provide outreach and mental health resources to veterans.
"With no single cause, there is no single solution, and we must be comprehensive in our approach to prevent Veteran suicide," added Miller during the hearing.
If you or someone you know is struggling or in crisis, help is available. Call or text 988 or chat 988lifeline.org
##########
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can help heal the symptoms and effects of acute concussion/TBI/PTSD by helping heal brain wounds.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#brainhealth#concussion#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Text
BRAIN WOUND UPDATE #13: Holistic Total Force Fitness to Maximize Performance

BRINGING YOU CURRENT INFORMATION ABOUT HOW TO HELP TREAT AND HEAL BRAIN WOUNDS: CONCUSSIONS, TBI, PTSD
A senior retired US Navy SEAL officer has weighed in with a six part justification for ACTION to fight suicide. His remarks relate to short- and long-term needs for dealing with force readiness amidst known challenges in the SpecOps community. His remarks are in concert with the Interview with the Senior Enlisted Advisor to the Chairman of the Joint Chiefs of Staff (SEAC), Ramón Colón-López that follows his remarks.
**************
Holistic Total Force Fitness to Maximize Performance
1. The M16A2 was discarded in SOF beginning in 1992 with the introduction of the CAR-15 and M-4 in the early 90’s. I was witness to that. The shortened barrels were, to say the least, "most noticeable", and in live fire drills, the concussive forces were enhanced around operators. Conventional forces did not receive these shortened rifles until circa 2010 in response to the need for shortened barrels in urban combat, which then also exacerbated the concussive forces during CQB operations in rooms. Constant exposure to shoulder-fired rockets, mortar, and artillery fire added to the cumulative effects. This is to say nothing about the constant exposure to IED blast waves, which, were the most injurious, and close-air support blast waves. All those constantly exposed to these concussive forces over multiple deployments will have physiological effects, lending to the neurological.
2. TBI, given the above, is akin to Decompression Sickness, physiologically, again lending to the neurological issues. Research has documented the evidence. The Textbook of Military Medicine, the volume entitled Ballistics, Blasts and Burn Injuries, has an algorithm on page 313. It is entitled Neurological Abnormalities in the Blast Casualty. HBOT is identified as definitive as treatment option.
3. This is not to discount the need for counseling; however, as I discussed with seniors, any operator, SOF or otherwise, who seeks help for TBI and suicidal ideation, is often stigmatized. It is akin to one seeking help for a perceived alcohol problem. We have witnessed those men and women immediately being separated from their comrades, which is in itself harmful, and the same appears to be the case for this issue. Rather, the solution should be immediate treatment with HBOT while still “on-the-line”, or, taken “off-line” as one would be for any illness while still retaining group and billet status. For any SOF operator, especially, referring to this in that light also de-stigmatizes the problem.
4. HBOT should be a health maintenance issue to deal with the prevalent and cumulative concussive forces from live fire in all forms. As an aside, HBOT would also assist in treatment according to the recently passed “burn pit” legislation. All warfighters are also subjected to the noxious gasses from carbines, rockets, artillery, along with the very nasty particulate matter encountered in AFG and Iraq. This is a readiness issue.
5. HBOT should be proffered by our health professionals as a performance enhancement issue. Olympic and professional athletes utilize HBOT for this reason. SOF operators, especially, will be lining up to enhance their performance. TBI and/or residual effects could then heretofor be corrected in a positive light. Overall, though, this is a combat enhancement and effectiveness issue.
6. One must ask why hyperbaric environments are questioned for TBI when it is considered medical protocol when dealing with Decompression Sickness (DCS) and Arterial Gas Embolism (AGE), wound ostomy, diabetic neuropathy, hearing and vision loss, radiation injuries, CO and airborne particulate poisoning, severe bone and skin infections, trauma from force or pressure on a body part.
Lastly, the constant exposure and cumulative effects to these blast waves, and the more acute exposure to the higher pressure waves in IEDs, etc, have the same effects as head trauma/ concussions in sports. Football legend Joe Namath has had his concussion injuries healed by 120 treatments of HBOT. His testimony is available on YouTube, and, he is the proponent for chambers being emplaced in stadiums for immediate treatment in concussion protocol.
****************
Interview with Senior Enlisted Advisor to the Chairman of the Joint Chiefs of Staff (SEAC), Ramón Colón-López.
The Military Heath System, together with DoD's Traumatic Brain Injury Center of Excellence, interviewed SEAC. Highlights are consistent with remarks above.
The Warfighter Brain Health (WBH) Initiative is a joint effort between operational and medical communities with the focus to optimize warfighter brain health, immediately detect brain injury when it occurs and combat its effects on warfighters, their families, line leaders/commanders, and their communities at large.
WBH is defined as the physical, psychological, and cognitive status that affect a warfighter's capacity to function adaptively in any environment, and impacts readiness, operational capability, mission effectiveness, and the goal to achieve overmatch or superior lethality
MISSION: Act rapidly to provide products, practices, and policies to directly impact warfighter brain health and performance. Due to experience and realities across the community, a major emphasis is to understand the implications of blast overpressure (include underwater and subterranean exposures); blunt force trauma; high G acceleration/ vibration/ recoil; incoming/ near missed impact (e.g. ballistic missiles); ballistic projectiles; directed energy (e.g., electromagnetic fields (EMF) and UV radiation); chemical-biological-gas toxins; and other environmental hazards.
SEAC defined "resiliency" as the threshhold for misery. No matter how resilient a warrior, symptoms keep coming. Slowed thinking, reactions, memory lapses, pain, reduced energy degrade readiness and ability to perform at peak levels.
The Comprehensive Strategy for Warfighter Brain Health Initiative 2018 study on the effects of low level blasts, section 734, calls for more efforts to confront effects of Blast.
SEAC referred to "the 3 greys":
- grey area of new operational environment: conventional peer-to-peer has given way to unconventional warfare
- grey area of grey steel deterrence: ships, missiles, aircraft are evolving to leverage the revolution in military and technical breakthroughs.
- grey matter: human performance, intellect, speed of response, judgement. In this last insight, SEAC calls on the Services to pay as much attention to restoration of the human as to the weapons and the doctrine. Degraded Warriors imperil our ability to prevail.
NOTE: Hyperbaric Oxygen Therapy (HBOT) meets and exeeds the challenge implicit in SEAC's challenge: Identify evidence-based cognitive and physical performance restoration treatments.
****************
Worth Reading
** In the largest study of neurodegenerative disease from Boston University’s CTE Center, sixty-three out of the 152 donated brains (41%) had autopsy-confirmed CTE. All cases were athletes under the age of 30 at the time of their death. The majority were amateur athletes (71.4%).
The report, published in JAMA Neurology on 28 AUG 2023 describes the features of 152 brains donated between February 1, 2008, and September 31, 2022, to the UNITE brain bank — the largest tissue repository in the world focused on traumatic brain injury and CTE.
Most of the donors analyzed played football (60%), followed by soccer (15%) and ice hockey (10%). Other sports implicated were amateur wrestling, rugby and professional wrestling.
The study shows that 87 of the 152 donors died by suicide, including 33 donors who also had CTE. Dr McKee noted: “The most common cause of death across the board, whether they had CTE or not, was suicide, followed by accidental overdose.” McKee adds that the longer someone plays football, in particular, their risk of developing CTE doubles every 2.6 years.
ALSO OF NOTE: The healthcare costs of TBI, driven by cost prices and the healthcare consumption of patients, will cause major economic and societal challenges, as estimates indicate the worldwide annual economic burden of TBI to be US $400 billion dollars, which is 0.5% of the gross world product.
##########
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can help heal the symptoms and effects of acute concussion/TBI/PTSD by helping heal brain wounds.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#brainhealth#braininjured#braininjury#brainwound#concussion#concussionprotocol#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#Holistic#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Text
BRAIN WOUND UPDATE #11: Suicide Risk, Mental Health and Military TBIs

BRINGING YOU CURRENT INFORMATION ABOUT HOW TO HELP TREAT AND HEAL BRAIN WOUNDS: CONCUSSIONS, TBI, PTSD
Associating Military-Related Traumatic Brain Injury (TBI) With New-Onset Mental Health Conditions and Suicide Risk
A new JAMA study sought an answer to this Question: Is military-related traumatic brain injury (TBI) associated with increased incidence of new-onset mental health conditions and suicide risk?
Findings. In this cohort study, individuals with a history of military-identified TBI had significantly higher rates of new-onset mental health conditions than those without TBI. Increased risk for suicide was associated indirectly (through new-onset mental health diagnoses) and directly with history of TBI.
Meaning. These findings suggest that conceptualizing exposures (physical, psychological) as events that accumulate over an individual’s lifetime and increase risk for negative outcomes (eg, suicide) may assist in identifying mechanisms underlying frequently co-occurring conditions, as well as evidence-based interventions.
Importance. Research to identify the direct and indirect associations of military-related traumatic brain injury (TBI) with suicide has been complicated by a range of data-related challenges.The major objective was to identify differences in rates of new-onset mental health conditions (ie, anxiety, mood, posttraumatic stress, adjustment, alcohol use, and substance use disorders) among soldiers with and without a history of military-related TBI and to explore the direct and indirect (through new-onset mental health disorders) associations of TBI with suicide.
In this longitudinal cohort study of 860,892 soldiers, rates of new-onset mental health conditions were higher among individuals with a history of TBI compared with those without. Moreover, risk for suicide was both directly and indirectly associated with history of TBI. These findings suggest that increased efforts are needed to conceptualize the accumulation of risk associated with multiple military-related exposures and identify evidence-based interventions that address mechanisms associated with frequently co-occurring conditions.
*******************
In another story, researchers have gained new insight on how the brain can repair itself post-stroke. Functional decline after an ischaemic stroke is a common experience for patients, especially due to the brain’s resistance to regenerate after damage. However, there is still potential for recovery as surviving neurons can activate repair mechanisms to limit and even reverse the damage caused by the stroke. The question this study looked to answer is how is it triggered?
Researchers from Tokyo Medical and Dental University (TMDU) provided new insight to this question by identifying a new mechanism. They discovered that neurons surrounding the area of cell death secrete lipids that can trigger brain-autonomous neural repair after ischaemic brain injury.
An ischaemic stroke occurs when the blood supply to the brain is blocked and results in the death of brain cells. This condition is life-threatening, and patients will likely develop functional disabilities. Although the adult brain can self-repair, the underlying mechanisms need further clarification.
Inflammation of the brain contributes to the effects of ischaemic stroke. Senior author, Takashi Shichita, says: “There is evidence that more lipids are produced after tissue injuries and contribute to regulating inflammation. “We investigated the changes in lipid metabolite production in mice after ischaemic stroke. Interestingly, the levels of a specific fatty acid called dihomo-γ-linolenic acid (DGLA) and its derivatives increased after the stroke.”
*******************
Lastly, Jeremy Renner, he of HURT LOCKER and AVENGER fame, and other roles, is taking HBOT treatments twice a day following his hellacious crushing on Jan 1 by his own snowplow.
“Hyperbaric chamber, 2 atmosphere pressure, high oxygen, 2x daily,” the Hawkeye star wrote....... According to the article: "In addition to injuries, hyperbaric oxygen therapy can be used to treat other medical conditions like burns, severe anemia, carbon monoxide poisoning, radiation injuries, traumatic brain injuries, and more. It is also commonly used for treating scuba and deep-sea divers affected by the rapid pressure change."
##########
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can help heal the symptoms and effects of acute concussion/TBI/PTSD by helping heal brain wounds.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#brainhealth#braininjured#braininjury#brainwound#concussion#concussionprotocol#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Text
BRAIN WOUND UPDATE #8: "New" Discoveries but Old News to Scientists Studying Brain Wounds

BRINGING YOU CURRENT INFORMATION ABOUT HOW TO HELP TREAT AND HEAL BRAIN WOUNDS: CONCUSSIONS, TBI, PTSD
-
Military suicide rate rose 25% in first quarter, Pentagon reveals JULY 05, 2023 TIMOTHY FRUDD
In an alarming update from the Pentagon, suicide rates among active-duty military personnel saw a 25% rise in the first quarter of 2023 compared to the same period last year. The suicide rate data was revealed in the recent quarterly report by the Defense Suicide Prevention Office, which found the total number of active-duty suicides was recorded at 94, up from 75 during the first quarter of 2022.
“Every death by suicide is a tragedy,” the report said. “Data includes all known or suspected suicides (both confirmed and pending) as of March 31, 2023.”
According to Stars and Stripes, the Army suffered the most significant surge in suicide deaths, with an increase from 37 to 49. Meanwhile, the Marine Corps saw an increase from eight to 14. The Air Force had one more suicide compared to 2022, and there was no change in the suicide rates within either the Navy or Space Force.
The Pentagon’s data shows a rising trend in military suicides over the past decade, including a pronounced spike in 2020 amid the coronavirus pandemic.
Beth Foster, executive director of the Pentagon’s Force Resiliency Office, spoke to this growing concern, saying, “There is still a gradual increasing trend for suicide in the military over a 10-year period, and we need to see a sustained long-term reduction in suicide rates to know if we’re really making progress.”
The Defense Suicide Prevention Office noted that the numbers in the report are preliminary and are subject to change upon further investigations and reports of previously unknown suicide cases. The Pentagon’s comprehensive yearly study on military suicides, set to analyze the data from 2022, is due for release in October.
**********
-
Redefining Depression: TBI Affective Syndrome Discovered - Neuroscience News
https://neurosciencenews.com/tbi-affective-syndrome-23580/
Summary: A new study suggests that depression post-traumatic brain injury (TBI) may be a distinct disease separate from traditional major depressive disorder. This revelation, arising from unique patterns observed in brain maps of TBI patients, could revolutionize the treatment for such individuals.
The study proposes a new term for this variant of depression – “TBI affective syndrome”. Fundamentally, this research marks a significant step toward personalized treatment strategies for TBI patients.
Key Facts:
• Depression post-TBI might be a distinct disorder separate from traditional major depressive disorder.
• The study suggests the term “TBI affective syndrome” for this variant of depression.
• Personalized brain mapping revealed unique patterns in TBI patients, leading to the theory of this distinct depressive disorder.
Source: Brigham and Women’s Hospital
A new study led by Shan Siddiqi, MD, from Brigham and Women’s Hospital, a founding member of the Mass General Brigham healthcare system, suggests that depression after traumatic brain injury (TBI) could be a clinically distinct disorder rather than traditional major depressive disorder, with implications for patient treatment.
The findings are published in Science Translational Medicine.
**********
-
Researchers identify first case of CTE found in a female athlete The HILL BY NICK ROBERTSON - 07/05/23
Australian researchers have identified the first case of chronic traumatic encephalopathy (CTE) in a female athlete. The brain injury has been commonly found in American football players and other contact sport athletes, but the discovery of the condition in a female athlete is a first.
Heather Anderson was an Australian rules football player who died by suicide last year at 28. An analysis of her brain found she had early-stage CTE caused by repeated head trauma.
“There were multiple CTE lesions as well as abnormalities nearly everywhere I looked in her cortex,” researcher Michael Buckland, director of the Australian Brain Sports Bank, told The Washington Post. “It was indistinguishable from the dozens of male cases I’ve seen.”
Her family donated her brain to researchers to learn more about her death. Scientific literature is inconclusive on the relationship between CTE and suicidality, but the condition is known to cause memory issues, personality changes and erratic behavior. Anderson retired from Australian rules football, a contact sport similar to rugby, after a career-ending shoulder injury in 2017. Her father described the CTE diagnosis as “a surprise but not a surprise,” in an interview with the Australian Broadcasting Corporation.
Rhw research, published Tuesday in the journal Springer, notes that a few women have been diagnosed with CTE before, but never an athlete. The research says the low number of female diagnoses is likely because the sports where CTE is most common, American football and boxing, are male-dominated. CTE worsens as athletes suffer more head injuries and in longer careers. The condition can only be diagnosed posthumously via an autopsy.
Researchers said athletes who start playing contact sports young are at the greatest risk of CTE. Anderson began playing Australian rules football at 5 years old, her family said. Women are also more susceptible to concussions than men, raising their risk for the condition, researchers said. “There has been a significant increase in women’s participation in contact sports over the past decade. … This report may, thus, represent a sentinel case: as the representation of women in professional contact sports is growing, it seems likely that more CTE cases will be identified in female athletes,” the study states.
Nearly 350 American football players, 90 percent of those studied, have been posthumously diagnosed with CTE.
##########
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can help heal the symptoms and effects of acute concussion/TBI/PTSD by helping heal the brain.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#brainhealth#braininjured#braininjury#brainwound#concussion#ConcussioninSport#concussionprotocol#ConcussionSymptoms#concussiontreatment#HBOT#HBOTTreatment#HeadImpact#HealingwithHyperbarics#hyperbaric#HyperbaricOxygentherapy#MilitarySuicide#sportsinjury#SportsRelatedConcussions#suicide#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#VeteranSuicide
0 notes
Text
IMPERATIVES: When "Certainty" in the VA Overrides Patient Health and Threatens Lives
**5th in a five-part series on the Implications of HBOT when used to heal brain wounds, prevent suicides, restore lives, and save Billions of dollars
It has been said that science advances one funeral at a time: old ideas and those who espouse them have to die off. The culture of science is self-protective and self-reinforcing. The history of advances in science is littered with rugged resistance to "radical" ideas. Yet, most people today accept that the earth is not flat; the sun and stars do not revolve around the earth; germs are real and penicillin works; in medicine, scientific truth is preferable to philosophical or religious dogma; and draining 40% of George Washington's blood for a sore throat might not have been a wise medical choice.
Medicine is slow to change, conservative, culture-bound, and eagle-eyed about threats to paradigm-shifting changes. That is particularly true when dollars and rice bowls are involved. Everyone who has ever proposed a significant change in medical practice has a favorite story about how resistance from within the medical bureaucracy slows down progress. This is particularly true today with respect to "mental health" and "suicide prevention" and standards of care for such disease states as Concussion, PTSD, TBI, and post-concussive syndrome (PCS).
The following are offered as a way to dislodge the VA, DoD, the NFL, NHL, FIFA, International Rugby, the NCAA, high schools, and medicine in general from antiquated ideas about brain wounds.
Imperatives: Really Important Things We Must Do
The U.S. Department of Veterans Affairs (VA) top clinical priority is preventing suicide among all Veterans. Numerous other sports and medical institutions are similarly concerned about the toll taken by hits to the head. So here is some advice, rooted in some truths that will open up the diaologue and let brain-wounded get the insured help they need and deserve.
- It is imperative that doctors and coaches and trainers and administrators and medicine in general start talking about "brain wounds" and a new standard-of-care for healing brain wounds. TBI/PTSD/Concussions -- all are or can lead to brain wounds and potential deterioration in the brain and physical, emotional, psychological, behavioral, and spiritual capability.
- Brain wounds need to be treated with wound healing principles: start with increases in energy and oxygen. Quit doing nothing and hoping symptoms will go away. And the reason "early exercise" may help in symptom reduction is delivery of more oxygen to the brain!
- It is imperative that the VA change its negative position vis-a-vis Hyperbaric Oxygenation Therapy when used for TBI and PTSD. For over a decade, medicine has relied on studies conducted by the Army/DOD/VA which concluded, variously that: "HBOT does not work." Science has advanced. The UHMS now knows and needs to tell the VA that their studies demonstrate what nearly two dozen peer-reviewed studies also demonstrate: the safety and efficacy of HBOT in treating brain wounds.
- The VA must ensure that all suicidal Veterans are told about, and have insured access to, HBOT treatment. HBOT has been shown in clinical trials to reverse and nearly end/cure "suicidal ideation." Over 21,000 successes in TreatNOW Coalition clinics attest to the healing power of HBOT.
- While they're waking up to "new" science, theVA must ensure that all Veterans with Diabetic Foot Ulcers (DFUs) are informed about "old, established" science: HBOT as an on-label, insured treatment for DFUs. HBOT can help avoid lower limb amputations (LLAs) in over 70% of cases. Tragically, 796,340 Veterans have died from Diabetic Foot Ulcer (DFU) and Lower Limb Amputation (LLA) in the past 22-years, more than all the Veterans KIA in all the U.S. Wars (623,982) since the beginning of World War I. Approximately 94% were not offered HBOT treatments.
- The VA must enhance their Clinical Practice Guidelines to make HBOT-for-TBI a standard of care for brain wounds. Current Guidelines do not take into account the UHMS redefinition of Hyperbaric Medicine; the VA is relying on outdated science.
- It is imperative that research into Suicide Prevention include actually treating and healing brain wounds with HBOT. Fully treated patients get off almost all their drugs, particularly those the VA prescribes that WARN OF SUICIDAL IDEATION.
"First, do no harm" (Primum non Nocere)
The information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Heal Brains. Stop Suicides. Restore Lives. TreatNOW.
Read the full article
#brainhealth#braininjured#braininjury#brainwound#concussion#concussionprotocol#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Text
Part 1 EPOCH TIMES: Blast Injury, Marine Injustice and no treatment for Brain Wounds from friendly fire

EXCLUSIVE: Marine Veteran Injured Fighting ISIS in Syria says He Was "Betrayed" by the Service
A former Marine artilleryman says he was neglected and unjustly treated by the branch after suffering brain injuries during a 2017 campaign to defeat ISIS in Syria
Original Article in The EPOCH Times here.
By J.M. Phelps Updated: May 8, 2023. This is part one of a two-part series.
Javier E. Ortiz wanted nothing more than to become a Marine. And after a humble beginning, he quickly devoted himself to the Corps. In return, he says he was stripped of his dignity and left to fight an uphill battle alone.
Ortiz was born in the Dominican Republic on Dec. 22, 1994. He was a boy when his father left the family to build another. In search of the American dream, Ortiz moved with his mother and older brother to New York in November 2003. A month later, they moved to New Jersey and Ortiz entered the American school system. His mother’s cash stockpile slowly deteriorated as she cared for Ortiz, an older brother, and other family members in the home.
Taking the opportunity to live closer to his grandparents, Ortiz moved with his mother and brother to Kissimmee, Florida, in 2005. As his mother continued to struggle financially, he eventually was adopted by an aunt and uncle in 2007 who began to provide the stable environment he longed for.
Distancing himself from the family’s rocky start in America, Ortiz began to cultivate the idea of serving in the United States Marine Corps as one of “the few, the proud.” “I decided to do everything I had to do to be able to join the Marines,” he told The Epoch Times.
With frequent visits to the local recruiting station between 2012 and 2015, Ortiz grew increasingly motivated to join the Corps. In 2014, he gained naturalization for work, which allowed him to apply for a Social Security card. And in 2015, he was able to do what he had always wanted to do: join the Marine Corps.
Ortiz traveled to Parris Island, South Carolina, for boot camp during the fall-to-winter cycle of 2015. “The first night I arrived, there was a meteor shower, a complete affirmation I was doing the right thing,” he said. Thirteen long weeks of training were “good,” he said. “I adapted well due to my long-awaited goal of protecting my new homeland.”
Deployment
Not only did Ortiz earn the Marine Corps’ Eagle, Globe, and Anchor, he became a U.S. citizen shortly after completing boot camp. And with that, he was ready to support and defend the Constitution of the United States, even to the point of death. In 2016, Ortiz was attached to the Headquarters element of the 1st Battalion, 11th Marine Regiment, 1st Marine Division in Camp Pendleton, California.
“I was in Headquarters for only a couple of months before 1st Battalion, 11th Marines , Alpha Battery was rumored for deployment to Syria,” he said. “I was eager to perform, and I was eager to deploy,” he added.
A fellow service member was recovering from a personnel incident and another was attending to an ill family member, opening the door for Ortiz as the next in line to join a combat element he had long desired to be part of.
“Alpha Battery’s reputation was that they were extremely accurate the tip of the spear,” he said. “And within a couple days, I was in formation with Alpha Battery, ready to take that deployment.”
His performance and willingness to deploy on short notice also led to a meritorious promotion from the rank of Private First Class to Lance Corporal in October 2016.
Enter Alpha Battery
Ortiz found himself aboard an amphibious assault ship—the USS Makin Island—in October 2016. 1/11 Alpha Battery was deployed and served as the artillery unit for the 11th Marine Expeditionary Unit (MEU).
For the remainder of the year, Ortiz was on the ship “on the other side the world,” he recounted. At the end of 2016, he said, there were finally talks about artillery batteries being dispatched into Syria as ISIS continued to gain large swaths of territory in Iraq and Syria.
Aboard the USS Makin Islan in December 2016, Sergeant Major Ronald Green told those on the ship, “We are here to impose our will onto our enemies—to change their minds or their zip code!” Ortiz recalled.
Prior to Ortiz’s deployment, Special Operations troops had already been in the country since early 2016, training and advising local forces in the fight against ISIS in northern and eastern Syria.
In March 2017, the Washington Post reported that an undisclosed number of Marines assigned to the 11th MEU had secretly entered Syria to “fire artillery in the fight for Raqqa,” the self-identified capital city for ISIS. Ortiz was among that group—and the deployment was said to have marked “a new escalation in the U.S. war in Syria” against hardened terrorists.
It was the first time American forces, other than Special Operations, had entered the Middle Eastern country; and by May, then-Defense Secretary James Mattis would be calling U.S. involvement an “annihilation campaign.”
Ortiz and Alpha Battery began conducting training exercises in Kuwait in early 2017. Prior to being transported to the deadly fight ongoing in Syria, MEU Commander Col. Clay C. Tipton told 1/11 Alpha that “not all of us will make it back,” Ortiz recalled.
“At that point, it clicked, and I began to understand the sacrifices we were all about to make,” Ortiz said. Shortly after, he and his fellow artillerymen were flown into Syria on a Boeing C-17 Globemaster, a massive military transport aircraft.
1/11 Alpha was tasked by the 11th MEU to provide direct and indirect fire in support of the mission to defeat ISIS, dubbed Operation Inherent Resolve, in February 2017. “We were some of the first Marines in Syria, literally the first artillery battery with a mission task,” Ortiz said. “I was part of a series of artillery batteries, being the initiating force to overtake Raqqa.”
“I was the ammo driver for Gun 4, responsible for chucking rounds, ramming rounds, and providing powders ,” he explained. And the first time he pulled the lanyard, he had confirmed kills. To this day, he still has the primer from that round he fired.
Ortiz recalled at least three different occasions where he also was threatened by incoming fire high explosive rounds. “But we were obliterating ISIS,” he said. And after about two weeks, Alpha Battery “pushed outside the wire” beyond the perimeter of a secure base of operations. His unit was required to sign the equivalent of a nondisclosure agreement while outside the wire, stating they would not discuss anything, about their mission in Syria or otherwise, on social media and other channels. This was, and remains, unprecedented, according to service members who spoke to The Epoch Times.
Unsafe Exposure
Marine Corps officials were once “tight-lipped” about the 11th MEU’s contributions to the campaign in Syria in 2017. Many of its missions during its deployment were not discussed publicly. But reports quickly surfaced about powerful 155-millimeter shells from M777 howitzers beginning to rain down on Raqqa. One of the secretive details of the onslaught, the number of artillery rounds fired in Syria, was disclosed a year later.
According to Army Sgt. Major John Wayne Troxel, the artillery battalion “fired more rounds in five months in Raqqa, Syria, than any other Marine artillery battalion, or any Marine or Army battalion, since the Vietnam War.” During a Marine Corps Times roundtable discussion in 2018, the former senior enlisted adviser to the chairman of the Joint Chiefs of Staff said 35,000 artillery rounds were used to kill ISIS terrorists “by the dozens.”
For comparison, 60,000 rounds were fired by the Marines and the Army during the First Gulf War. And during the initial invasion of the Iraq War, over 34,000 artillery shells were fired.
In the time period Ortiz was confirmed to be there, MEU spokesman Maj. Craig Thomas was quoted by USNI News, saying, “The task force executed over 400 fire missions and fired more than 4,500 rounds from M777 howitzers to support our coalition partners fighting to isolate and then liberate Raqqah from ISIS.”
Between March and May 2017, Ortiz participated in the Battle of Raqqa. At one point, a howitzer was fired every hour for 47 consecutive days, Ortiz said. During that time, there was also a 14-hour fire mission where all four were active.
“We were shooting a lot,” he said.
The numbers appear to have exceeded what is safe for service members to be exposed to.
Gun 4—the specific howitzer Ortiz was assigned to for Alpha Battery—was the first to fire over 1,000 rounds within the first few weeks of landing in Syria. During one particular mission, his gun ran out of ammunition and had to be resupplied from Kuwait and other countries that held ammo points to continue.
Considered some of the most destructive and powerful artillery rounds in the Marine Corps arsenal, Ortiz said, Gun 4 averaged “25 rounds per day with 12 to 17 of these rounds being charge 5 .”
According to the Fort Sill Public Affairs Office, subject matter experts at the U.S. Army Field Artillery School said “at maximum charge, when all prescribed personal protective equipment is used, 12 rounds in 24 hours” is a safe number of rounds for human exposure. All field artillerymen of the Marine Corps are trained at Fort Sill.
Reported and Ignored
After the initial, unprecedented bombardment of Raqqa, 2nd Battalion, 10th Marines (2/10) Fox Battery replaced 1/11 Alpha in May 2017.
On Oct. 20, Raqqa was publicly declared liberated.
The damage was done—not only to the terrorist stronghold and its inhabitants, but also to artillerymen like Ortiz and his fellow Marines.
“A few of us were not feeling well and we brought it up as we noticed,” Ortiz said. “But at the end of the day, none of us wanted to stop, nor could we stop during an active battle; we just wanted to let the officers know we shouldn’t be shooting that much.”
“The order to go above standard operating procedure was above everybody’s pay grade on the ground there,” he continued, adding that “we couldn’t afford to lose anybody, so we just continued to exhaust all our ammo until things went back to normal.”
Early on, Ortiz said he experienced nothing more than a daily headache as a result of the constant firing. Three weeks later, however, abdominal pains began to emerge; all of which he reported. Some of the other soldiers were experiencing the same. Four of the eight artillerymen assigned to his howitzer had problems, he said.
“All that exposure to the blasts messed up our stomachs, our hands were swelling, and nosebleeds were happening,” he said, adding that as a result, he and others were lining up for doses of ibuprofen to combat the growing number of symptoms. None, however, were evaluated to find the root cause.
“Even though we knew something was wrong, each of us continued to give all for the Marines,” he said. “We had trained hard to be there, and nobody wanted to leave.”
On May 16, 2017, Alpha Battery’s deployment came to an end. “When we left, some of us were not well mentally or physically,” Ortiz said. The cause of the psychological and physical issues were unknown, but he began to associate them with the number of rounds he and others were firing.
Invisible Long-term Consequences
According to protocol, the symptoms experienced by these artillerymen should have been addressed by the Marine Corps.
The U.S. Marine Corps Traumatic Brain Injury Program (MARADMINS 294/12), states that “TBI , including mild TBI (also referred to as concussion), is a leading combat injury in conflicts.”
“These injuries can have a significant operational readiness impact as well as potential long-term health consequences,” the document adds.
But when asked, Ortiz said the Marine Corps had not followed through with their protocol. He became confident that the headaches, which were not random, were directly related to the injurious effects of blast overpressure. This, along with other problems, like abdominal pains, nosebleeds, and swelling, were not addressed by the Corps.
Due to repeated exposure to artillery blasts, the men were exposed to an excessive number of concussive events. A concussion is recognized as “an invisible injury” and “requires careful management by leadership and medical personnel,” the protocol states. One of the Marine Corps’ primary preventative measures includes “limiting exposure to potentially concussive events through the proper provision and use of PPE .” A second preventive measure includes “minimizing the adverse impact after a concussive exposure occurred, especially by limiting additional exposures during the recovery period.”
According to the policy, “commanders will also ensure that all Marines exposed to a potentially concussive event, whether in garrison or deployed, are placed in a 24-hour SIQ status and referred for a medical evaluation; direct their Marines to a medical evaluation in any other concerning circumstance such as repeated exposures to potentially concussive events or patient concerns or behavior that could be related to a concussion or TBI.”
It also states that “all units are required to ensure a post-deployment face-to-face clinical follow-up for all Marines diagnosed with a concussion or TBI during a deployment within one to four months of redeployment.”
But none of that happened for Ortiz or the men of 1/11 Alpha.
Blast TBI and PTSD
In an unclassified report (pdf) released by the Marine Corps in 2019, a blast overpressure (BOP) injury is defined as an “injury caused by the effect of the blast wave on a body.” Gas-filled organs such as the middle ear, lung, brain, and bowel are “most susceptible” to primary blast injuries, the report states. It’s similar to having repeated concussions over and over again.
The Epoch Times spoke to Dr.
Read the full article
#blastinjury#brainhealth#braininjured#braininjury#brainwound#concussion#concussionprotocol#ConcussionSymptoms#HBOT#HBOTTreatment#HealingwithHyperbarics#hyperbaric#hyperbaricoxygen#HyperbaricOxygentherapy#mentalhealth#MilitarySuicide#posttraumaticstressdisorder#PTSD#suicideepidemic#SuicidePrevention#TBI#TBItreatment#traumaticbraininjury#TraumaticBrainInjury#VeteranSuicide#VeteranSuicidePrevention
0 notes
Last Seen Blogs

jaketweet
Sin título


ifinitesadness
30 m Syd, Aus

gilf-groper101
Untitled

hottakeswithdasom
Im ANGRY about MOVIES