#pervasive developmental disorder
Text
ODD is when you tell the psychiatrist that you hate them to their face and PDD is when you tell them you hate them without words
6 notes
·
View notes
Text
going to the pharmacy dressed like a mentally insane dyke to get my prescribed potassium and NOT get my prescribed antipsychotics

#to my new followers. the reason i got the prescription was that my flatmate decided to snoop‚ found out i had a paranoid#schizophrenia diagnosis‚ and decided to lie and get me admitted to a psychward lol. im normal‚ the diagnosis was based on nothing‚ i got a#new more fitting diagnosis years later#in the ward i was diagnosed with not enough potassium and Pervasive developmental disorder unspecified#which i think is just a really weird term for autism for when you don't want to agree with other shrinks that diagnosed me with it#the bike isnt mine btw
5 notes
·
View notes
Text

PDA nd DYSPRAXIA/DCD BLINKIEZZZZZZ :3









#2000s#scene kid#scenemo#emo kid#scene#scene girl#scene queen#webcore#emo#emo girl#pathological demand avoidance#pda autism#pda pride#pervasive demand for autonomy#persistent demand for autonomy#DCD#developmental coordination disorder#dyspraxia#actually dyspraxia
43 notes
·
View notes
Text
Autism Mom Voice: Just because someone can write an extraordinarily articulate blog entry, it doesn't necessarily mean they have the executive function or other basic skills to support themselves financially or live independently,
Walter Benjamin: [staring into the camera like he's on The Office]
#sorry lmao#saw a tweet that said sometimes you don't understand Benji bc you're not as smart#And I said absolutely true but#If Benji got the same neuropsych tests I did as a kid#He would also be diagnosed as an idiot savant#I can't believe that is a real thing I got diagnosed as in the 90s but here we are#Nonverbal learning disability with pervasive developmental disorder & mild intellectual disability#+ 99.9th percentile verbal & abstract philosophical reasoning#You argue with your sister's law school classmates about Hegel but you've just been held back and you're repeating 9th grade#You're taking pre-algebra for the 3rd time#You won a state poetry contest and a state playwriting contest anonymously. You just failed Spanish class
21 notes
·
View notes
Text
Hot Take: getting mad at those of us who were told our tics were a part of our autism diagnosis doesn't help anything. I went into the fnd tag, and any posts regarding childhood tics in autism were full of people saying we were spreading misinformation.
I have had vocal and motor tics my whole life. My vocal tics sometimes got so out of hand that they would trigger asthma attacks (I have multiple different grunting, exhaling, and throat clearing tics). They've literally landed me in the hospital by triggering my asthma.
My speech therapist told my parents that to get me to stop ticcing mid sentence, they should make me restart completely from the beginning, which my parents then did. It didn't help my tics at all.
I have motor tics that are mostly facial and some that are muscle tensing in my legs and arms.
Why is this important? Clearly I have a tic disorder right? No, I have autism spectrum disorder. My tics are involuntary, they're not stimming and there is a difference, but my diagnosis is explicitly ASD, because ASD can and does have physical presentations.
I'm not the only one who experiences this - involuntary tics just sometimes are a part of autism:
- tics in autism are indistinguishable from those in TS, but are often less severe in their frequency "Tic distribution and tic repertoires were comparable, but more restricted in ASD. All GTS participants, but only 5 of the 10 ASD participants, were aware of their tics. Conclusions: Tics are common in adults with ASD. They are indistinguishable from tics in GTS and are similarly distributed, but less severe. Tic awareness is limited in ASD."
- this source is from 2000 and subsequently uses the term Asperger's, so beware of that. This source is once again saying that autistics can have symptoms that are indistinguishable from TS specifically, but in my experience diagnostically this extends to all tic disorders. "Our series confirms the wide range of clinical manifestations in Asperger's syndrome and autism, including tics and other features of Tourette syndrome."
- This study is from 2005 and uses outdated language such as Asperger's Syndrome and the R slur, so I have chosen to censor this quote mildly but I still decided to include the source. "Pervasive developmental disorders, including Asperger's syndrome (N = 13, 8.3%), [MR diagnosis] (N = 4, 2.5%), autism (N = 3, 1.9%), and Savant's syndrome (N = 1, 0.6%), also may be associated with tics, as noted in 21 of the 155 patients (13.5%)."
I know that these sources are old, which is problematic as neuropsychology is a constantly adapting field, but I also believe that the prevalence of tics in ASD isn't something that should be ignored. I have presented with motor and vocal tics since childhood, but my diagnosis has no mention of a specific tic disorder. My therapist when I was still seeing one specialized in teens with autism and OCD, and she said that my tics were just associated with my autism.
I sincerely hope this doesn't offend anyone or piss anyone off. I genuinely just am very frustrated by seeing people saying that it is spreading misinformation to say that autistic people can have involuntary vocal and motor tics when some of us were literally diagnosed that way. My first asd diagnosis was also "autism spectrum disorder with hyperactivity" so clearly diagnostically some weird shit used to be happening. I don't know if tic disorders have to be diagnosed separately now, but when I was diagnosed I was told that the autism diagnosis took precedent, and that I was autistic which sometimes presented with frequent tics.
Because that's the thing, it's not occasional tics. As a kid I couldn't get more than two words out before one of my vocal tics came out, and my motor tics were apparently very frequent as well according to my family. Tics are just like that, you can't control them without immense pain. Believe me, I tried. I was trained out of them like a god damn dog. It never worked.
My dad also has tics and he only has a diagnosis of ADHD. He presents with less tics than I do, but he still has vocal and facial tics.
Tldr: neurodevelopmental disorders are sometimes just diagnosed weirdly.
#i genuinely don't even know how to tag this#i was looking at fnd stuff so that might be a good place to start#fnd#functional neurological disorder#actually autism#autism spectrum disorder#autism diagnosis#aspergers#pervasive developmental disorder not otherwise specified#high functioning autism#tic disorder#vocal tics#autistic tics#adhd tics#involuntary tics#motor tics#actually autistic#actuallyneurodivergent#neuroatypical#neurodivergent#idk if i should tag tourette syndrome or not#it is relevant technically#but i dont want to invade tags I shouldn't be in#eh fuck it#tourettes#tourette syndrome#actuallyautistic#actually tourettic#anxiety tics#physical tics
1 note
·
View note
Text
will wood fans will get mad at you if your favorite song is i/me/myself and not some 23 second demo from 2015 with the crunchiest damn audio you've ever heard called ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children
110 notes
·
View notes
Note
In hindsight after your ADHD diagnosis, were there specific moments or behaviors from your childhood/teenage years that you saw under a new light?
Now I have not been able to get a diagnosis, but I do strongly believe I have ADHD at the very least. I thought it started and got progressively worse when I was in high school, because that's where I noticed that I was struggling. But then later, I brought up the idea to my mom and she was like "no, you've always been like this" what? But I genuinely didn't remember that.
I also found old report cards and progress reports from elementary school that all said some variation of "a pleasure to have in class, but needs to be reminded to focus and stay on task." But I was never tested? Why? I was in IEP and went to special classes weekly and was regularly tested for non-ADHD disabilities (hearing loss), so what would an extra test or two have hurt?
Did you have any moments of realization where you were like "oh, so it was always there?"
I hear you. It's so frustrating to think I could have gotten help as kid, but no one even suggested it. It had never even occurred to me by the time I was diagnosed at 34. If my psychiatrist hadn't suggested it I probably would still be undiagnosed. Looking back, of course there were signs. It's all mixed up with the fact that I was abused as a kid and developed PTSD at about 10, but here are some things that stood out:
Scored in the 99th percentile on all standardized tests, but had average grades. Did not complete assignments. Found I couldn't start my homework at home despite dire consequences from abusive parents.
Feeling developmentally different than my peers. It was like they all got something about friends and social behavior that I just missed and I couldn't figure out what it was. Related much more to adults than children.
Sensory problems. High sensitivity to light, sound, sensations. I would react with extreme anger that upset and confused everyone, myself included.
Physically uncoordinated. Poor balance, using too much or too little strength, dropping things, knocking things over. So much so that my parents had a mean nickname for me about it.
Number lists! For example: I got to school at 8. I would write down all the times between 8 and 5 in five minute intervals on a sheet of paper (9:15, 9:20, 9:25, etc) and cross them off as the time passed. Kept track of reading in a similar way (book, page, goal pages, where I'm supposed to be, difference between page I'm on and page I should be, average pages per day, etc etc etc like 10 columns. Notebooks full of this.
Extreme emotional sensitivity. Prone to depression and angry outbursts.
And so much more I'm assuming. All my parents did was tell me to stop being r*tarded and that I was a bad person. I grew up with a pervasive sense of being "the weird kid". It deeply effected my self esteem. I hope you are able to be tested. Understanding that I had a neurodevelopmental disorder instead of a moral failing and being treated for it with stimulant medication changed my whole life. I wasn't diagnosed until my 30s but thank god I was.
36 notes
·
View notes
Note
Do you think that Katniss is autistic?
Yes/No? Please explain your reasoning.
If yes, can you give example?
If no, what do you think the most accurate description about Katniss behaviour?
Is there a difference between Katniss in the books and in the movies?
Thank you :)
@curiousthg
This is a great question, @curiousnonny as someone who studied Autism in school and worked with a few autistic children, I don't think she's autistic, but do I think she falls within the spectrum or what is referred to the autism spectrum disorder (ASD). And it's confusing b/c autism falls withing the spectrum of ASD.
Now I'm not a phycologist or a sociologist but I did have to study it when I switched to education.
Side note there was a time that there were 3 teers to Autism, there was Autism, Pervasive Developmental Disorder and Asperger's - one was more severe than the other, that have been umbrellaed under one diagnoses of ASD. So in other words Katniss does have traits.
She does have sensory issues, i.e. to touch.
She doesn't have complete awareness of social cue's
She has single minded focus
Doesn't make friends easily
Doesn't do small talk
Doesn't like change
Katniss has a structure to her day and doesn't veer from it, hunts, trades, school, home, repeat!
She is supper smart - (her lack of proper EDU. is a shame )
I wonder if the PTSD she suffers is exacerbated by her ASD - it's when she begins to withdraw from society because she's overwhelmed, yes it's PTSD but it's also a clear sign that cannot handle societal pressures when overwhelmed
I would say she's very high functioning or a high functioning ASD
And just to give you a list of people who are high functioning and within the ASD : Daryl Hanna (Splash movie), Tim Burton (Director Nightmare before Christmas Movie) Dan Akroyd (SNL Alum), (and I think I read somewhere Bill Gates too...but I may need to verify. )just to name a few. Katniss could very well fit into that group...
16 notes
·
View notes
Text
Pseudo-Neuroticism in The Covert Schizoid
In the complex world of psychological phenomena, understanding the subtleties of various conditions is crucial for accurate diagnosis and effective treatment. One such nuanced concept is pseudo-neuroticism, particularly as it manifests in individuals with schizoid personality dynamics. This article delves into the unique ways pseudo-neuroticism appears in schizoid individuals, contrasting it with classic neuroticism.
The Schizoid Context
Schizoid individuals often navigate life with a detachment from emotions and sometimes physical sensations. This detachment, stemming from psychological defenses employed during their early developmental stages, leads to a split between their mind and body, thoughts, and emotions. The creation of a 'false self' system becomes a coping mechanism to interact socially while protecting their 'true self,' which remains hidden and disengaged in these interactions.
Pseudo-Neuroticism in Schizoid Individuals
Pseudo-neuroticism in schizoid individuals arises as a byproduct of the conflict between their true and false selves. The false self is developed to navigate societal expectations and social interactions. However, this creates a unique form of neuroticism that is not genuine but a façade to fit into societal norms. Unlike classic neuroticism, where there is an intrinsic desire for acceptance and validation, pseudo-neuroticism in schizoid individuals stems from a more superficial level – the need for their false self to blend in and avoid standing out.
Classic Neuroticism vs. Pseudo-Neuroticism
Classic neuroticism is characterized by genuine emotional distress, anxiety, and a deep-seated need for acceptance. These individuals genuinely care about others' opinions and often internalize their fears and anxieties. In contrast, schizoid pseudo-neuroticism is more about the performance of the false self. The true self of a schizoid individual typically does not seek external validation or genuinely care about societal opinions. The anxiety and concern are more about the effectiveness of the false self in social camouflage rather than a true emotional turmoil.
The Interplay of True and False Selves
In schizoid individuals, the true self is like a passive observer, detached from the actions and anxieties of the false self. This detachment can sometimes lead to resentment towards the false self or the roles they fee compelled to play in society. The pseudo-neuroticism manifests in apprehensions about whether the false self is fitting in, not standing out, or being perceived as 'authentic.'
Schizoid Pseudo-Neuroticism vs Avoidant Personality Disorder
Pseudo-neuroticism in covert schizoid individuals can often resemble avoidant personality disorder (AVPD) as defined in the DSM-5, as both conditions generate a degree of internal anxiety related to social interactions. Despite this similarity, it is crucial to understand the differing underlying reasons for these behaviors. In AVPD individuals, the anxiety is deep-seated and persistent, as they have a pervasive pattern of social inhibition, feelings of inadequacy, and a hypersensitivity to negative evaluation. In contrast, the anxiety in covert schizoid individuals exhibiting pseudo-neuroticism is more temporary and situational, based on reaching goals, and not primarily due to conscious feelings of inadequacy or a pervasive fear of rejection.
Summary…
Understanding the nuances of pseudo-neuroticism in schizoid individuals is essential in differentiating it from classic neuroticism. This understanding not only aids in accurate diagnosis, but also in formulating effective therapeutic approaches that address the unique needs of schizoid individuals. By acknowledging the complex interplay of the true and false self, we gain insight into the intricate psychological dynamics that shape schizoid experiences and behaviors.
Video From My YouTube Channel: Covert Schizoid: Psuedo-Neuroticism of The False Self
#schizoid#schizoid adaptations#schizoid dynamics#schizoid pd#schizoid personality disorder#schizoid vision#cluster a#szpd#false self#covert schizoid
21 notes
·
View notes
Text
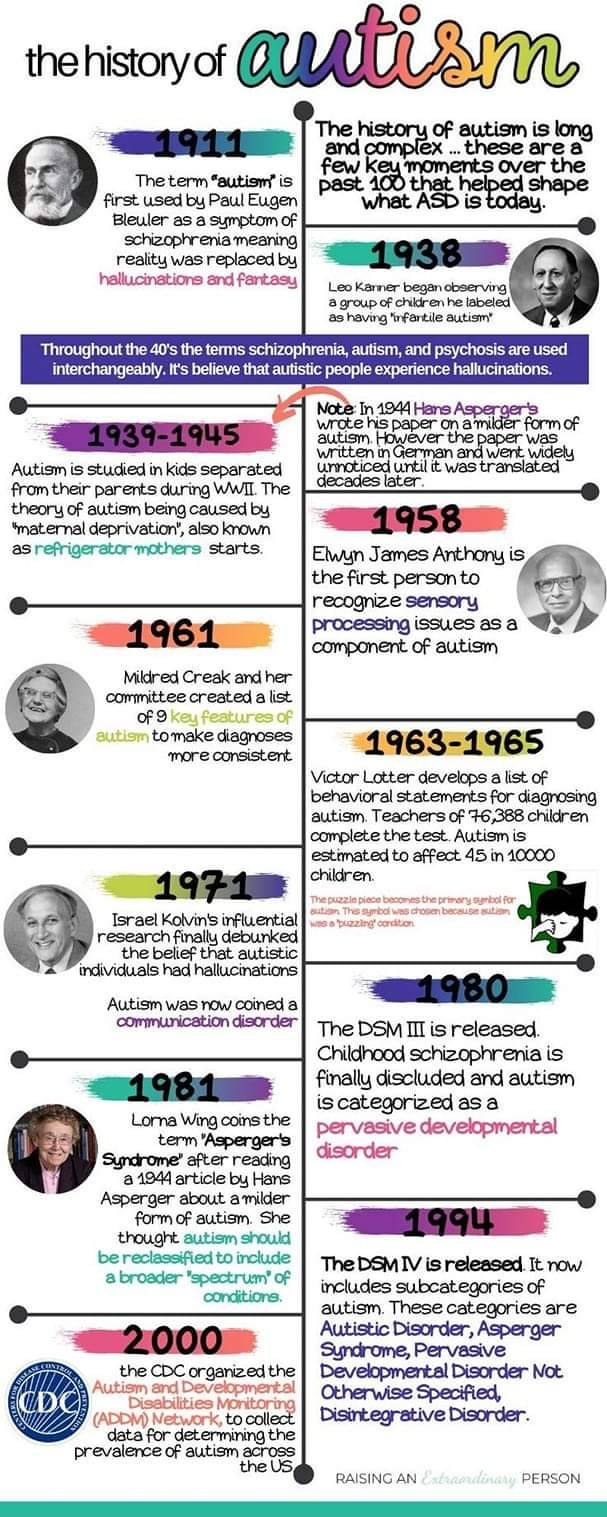
History of Autism
The term autism first was used by psychiatrist Eugen Bleuler in 1908. He used it to describe a schizophrenic patient who had withdrawn into his own world.
Eugen Bleuler coined the word "autism" in 1908 among severely withdrawn schizophrenic patients.
In 1943 Leo Kanner studied 11 children. The children had difficulties in social situations, adapting to changes in routines, good memory, sensitivity to sound, allergies to food, good intellectual potential, echolalia, and difficulties in spontaneous activity.
In 1944 Hans Asperger, who was a German Nazi, sorted autistic individuals into two categories. He studied one group and had the other group killed. The children he studied were considered "high functioning" and spoke like grownups. He also said that many of the children were clumsy.
In 1952 autism is added to the DSM as a psychiatric disorders diagnosed by a profound emotional disturbance that does not affect cognition and many people with schizophrenia were misdiagnosed.
Bruno Bettelheim studied the effect of three therapy sessions with children who he called autistic. He claimed that the problem in the children was due to coldness of their mothers. He separated the children from their parents. Kanner and Bettelheim both worked towards making hypothesis that showed autistic children had frigid mothers. This is where the term refrigerator mother came from.
Bernard Rimland was a psychologist and parent of a child with autism. He disagreed with Bettelheim. He did not agree that the cause of his son’s autism was due to either his or his wife’s parenting skills.
Autism came to be better known in the 1970’s. The Erica Foundation started education and therapy for psychotic children in the beginning of the 80s. Many parents still confused autism with mental retardation and psychosis.
In 1980 autism was changed in the DSM to be a pervasive developmental disorder seperate from childhood schizophrenia. It defined autism: a lack of interest in people, severe impairments in communication and bizarre responses to the environment, all developing in the first 30 months of life.
It was in 1980’s that Asperger’s work was translated to English and published and came into knowledge. Lorna Wing read it and coinsd the term Asperger's.
In the 1980’s that research on autism gained more traction and it was believed that parenting had no role in someone being Autistic and that there were neurological disturbances and other genetic ailments as the cause.
In 1987 the DSM divided autism into categories based on functioning labels. PPD NOS was used to describe those considered high functioning and autism for those considered low functioning.
Lorna Wing, along with Christopher Gillberg at BNK in Sweden in the 1980’s found the Wing’s triad of disturbed mutual contact, disturbed mutual communication and limited imagination.
In the 1994 the DSM is changed to include Asperger's. With PPD NOS as high functioning, Asperger's in the middle, and Autism for low functioning.
Them Ivar Lovaas studied and furthered behavioural analysis and treatment of children with autism. He developed it to target younger children (less than 5 years of age) and implemented treatment at home and increased the intensity to about 40 hours weekly. This therapy was ABA. This therapy was also modified and used as conversation therapy.
In 2013 the DSM removes Asperger's and PPD NOS and autism is now classified a social communication disorder.
In 2018 the DSM classified Autism as autism spectrum disorder and makes a distinction between autism with and without intellectual disability, and highlights the fact that older individuals and women sometimes mask their autism traits.


#autistic#autistic pride#autism acceptance#autism#audhd#actually audhd#autism acceptence month#asd#autistic adult
13 notes
·
View notes
Note
hi!
so no idea if you remember me but awhile ago i a made a post, basically saying i think i might have adhd.
i made a new post today (maybe four down on my profile) with a follow up, as well as my thoughts about possible adhd- and now possible autism
since you blog is about both, i was wondering if you had any advice for someone on how to tell the two apart and stuff
sorry to bother you about this again :)
and thank you for all your help last time
Hi there,
I found some resources that could help:
Here’s a Venn diagram comparing the two:

I hope these can help. Thank you for the inbox. I hope you have a wonderful day/night. ♥️
34 notes
·
View notes
Text
CW - Therapy Abuse
As a kid, I went through two different kinds of therapy. A therapist my parents spoke to, and a therapist I saw at school. The weird part about both of them was that I actually did very little talking in those appointments. It was usually my parents/administration doing most of the talking.
And putting aside the fact that I'm pretty sure that's a massive breach in ethics, it highlights a major problem that child psychology has: Putting way too much stock on the opinions of authority figures in a child's life.
I was given so many junk diagnosis as a kid. About the only ones that survived any scrutiny as an adult were ADHD and C-PTSD. But the rest (Oppositional Defiance Disorder, Conduct Disorder, Asperger's Syndrome, Pervasive Developmental Disorder Not Otherwise Specified, yes that last one was real until the DSM-V came out, hi I hate it here) just didn't hold up the scrutiny. Granted ODD and CD can't because the adult version of those is Antisocial Personality Disorder, but I didn't meet the criteria for that because one look at my medical history made the doctor go "Oh yeah I see the problem."
And I think the reason I was given so many junk diagnosis that led to treatment plans that didn't help was because the people CAUSING most of my stress and issues were allowed too much of a say in how I was being diagnosed.
ODD is the one that sticks out because it isn't diagnosed anymore precisely because its criteria is designed to disregard the patient and prioritize the opinions of authority figures in the child's life. This is a disorder given to children that, regardless of reason, are struggling to behave in the obedient manner children are expected to.
They're able to take an unruly child, deem them to have a disorder, and push them on a path very early where they're adjusted to having a therapist, to having psyche meds, to being managed, to being taught that their anger is just their brain messing up. You may notice that risk factors for ODD include parents or guardians that abuse, neglect, or have substance abuse problems. I don't know about you, but I'm pretty sure that mistreated children acting out indicates the problem isn't that the child has some disorder that makes them like this.
It became apparent even to professionals that this diagnosis was a fucking hotbed of abuse. It was medical care that said "you are wrong for being angry. You are wrong for being upset. Your feelings are invalid." Because oftentimes I would tell a therapist something, and be told I was lying. And the proof I was lying? The authority figures in my life said something else.
Near constantly.
"I get insulted a lot at home."
"Well they said you don't."
"I'm being bullied by the other kids."
"Sticks and Stones."
"The resource teacher is touching me."
"Well she said she didn't."
"The teachers are hitting me."
"Well they said they aren't."
"I'm being told to learn things and not being given the tools to actually learn them, setting me up for failure."
"Well you need to learn them."
"I am routinely told that I'm worthless and unwanted and threatened with homelessness on a regular basis."
"Well you need to suck it up and deal with it."
Fuck sometimes I think I'm over it, or at least processing it in an introspective way, but writing just that short list out got me choking up, fucking hell.
Therapy was used as a vector for the people who were hurting me to cover their asses. I was told constantly that I was wrong for reacting badly to being mistreated, given garbage diagnosis on a regular basis, and I quickly learned to just stop talking to people. To shut down. To avoid saying anything if I even detected the slightest hint I'd be accused of lying.
Fuck I was diagnosed with skin cancer last year and only told my own wife a month ago. Still haven't told my immediate family, I have no idea how to broach that subject.
Therapy ended up going much better with far more helpful diagnosis once I was an adult and didn't have someone hovering over my shoulder loudly denying everything I said. So when I told my therapist "I was molested in first grade" I was believed because who the fuck would pay $150/hr to lie to a therapist?
For all my aggression as a kid, it was a learned response and almost entirely retaliatory. I really had started to believe the awful things that were being said about me, so to actually get a doctor that listened to me and took my story seriously was an overwhelming experience.
I'm often asked if I'm still angry about it. And at specific people? No. Well a few teachers, largely because they got away with it. But I'm not really holding a grudge. I'm angry at the system that allowed it to happen. That continues to allow it to happen to children. Especially neurodivergent children. I'm angry at Section 43 of the Criminal Code of Canada that makes it so parents and teachers don't get charged with assault when they hit children. I'm angry at the fact that emotional abuse, verbal abuse and sexual abuse aren't taken seriously unless they're caught on camera or the accusations come from an adult. I'm angry at the system that takes the authority figures in a child's life at their word, even when they are faced with accusations of mistreatment.
I'm angry at the system that allowed it to happen. That continues to allow it to happen to children. Especially neurodivergent children. I'm angry at the fact that emotional abuse, verbal abuse and sexual abuse aren't taken seriously unless they're caught on camera or the accusations come from an adult. I'm angry at the system that takes the authority figures in a child's life at their word, even when they are faced with accusations of mistreatment.
That such extreme malice is presumed of children solely to cover the ass of someone who doesn't want to meet the consequences of their own actions is absurd.
The simple fact of the matter is that if Section 43 of the Criminal Code of Canada (which allows parents, guardians and educators to beat children in the name of discipline) didn't exist, the lessons my generation had to teach everyone the hard way would have been learned a lot faster.
40 notes
·
View notes
Text
situational/selective mutism list thing
Temperamental Inhibition
Social Anxiety Symptoms
Social Being: most have 'age-appropriate social skills'; some don't
Physical Symptoms: stomach, joints, head, chest etc. (will add the SM Throat Pain™)
Appearance: blank face, stiff body, freeze; some appear relaxed perhaps because sympathetic nervous response.
Emotional: depends on age/social acceptability of mutism
Developmental Delays: motor, communication, social (asd, pdd)
Sensory Integration Dysfunction (DSI)
Common symptoms: sensory problem, defiant behaviour, hesitant to respond, social withdrawal, focus on academics
Behavioural: maladaptive coping mechanisms, inflexible, moody, stubborn
Co-Morbid Anxieties
Social Engagement Difficulties
source: selective mutism pdf by Dr Elisa Shipon-Blum. elmtreeclinic
long long post with more detail. seriously very very long🌹🌹
1. Temperamental Inhibition: Timid, cautious in new and unfamiliar situations, restrained, usually evident from infancy on. Separation anxiety as a young child.
2. Social Anxiety Symptoms: Over 90% of children with Selective Mutism have social anxiety. Uncomfortable being introduced to people, teased or criticized, being the center of attention, bringing attention to himself/herself, perfectionist (afraid to make a mistake), shy bladder syndrome (Paruresis), eating issues (embarrassed to eat in front of others).
3. Social Being: The majority of children/teens with SM have age appropriate social skills and are on target developmentally, although some do not. Most children on the autism spectrum struggle with speech/language skills, social skills and have developmental challenges.
4. Physical Symptoms: MUTISM, tummy ache, nausea, vomiting, joint pains, headaches, chest pain, shortness of breath, diarrhea, nervous feelings, scared feelings.
5. Appearance: Many children with Selective Mutism have a frozen-looking, blank, expressionless face and stiff, awkward body language with lack of eye contact when feeling anxious. This is especially true for younger children in the beginning of the school year or then suddenly approached by an unfamiliar person. They often appear like an animal in the wild when they stand motionless with fear! The older the child, the less likely he/she is to exhibit stiff, frozen body language. Also, the more comfortable a child is in a setting, the less likely a child will look anxious. For example, the young child who is comfortable and adjusted in school, yet is mute, may seem relaxed, but mutism is still present. One hypothesis is that heightened sympathetic response causes muscle tension and vocal cord paralysis.
6. Emotional: When the child is young, he/she may not seem upset about mutism since peers are more accepting. As children age, inner turmoil often develops and they may develop the negative ramifications of untreated anxiety (see below).
7. Developmental Delays: A proportion of children with Selective Mutism have developmental delays. Some have multiple delays and have the diagnosis of an autistic spectrum disorder, such as Pervasive Developmental Disorder, or Autism. Delays include motor, communication and/or social development.
8. Sensory Integration Dysfunction (DSI) symptoms, Processing Difficulties/Delays: For many children with SM, sensory processing difficulties are the underlying reason for being 'shut down' and their mutism. In larger, more crowded environments where multiple stimuli are present (such as the classroom setting), where the child feels an expectation, sensory modulation specifically, sensory defensiveness exists. Anxiety is created causing a 'freeze' mode to take place. The ultimate 'freeze mode' is MUTISM.
9. Common symptoms: Picky eater, bowel and bladder issues, sensitive to crowds, lights (hands over eyes, avoids bright lights), sounds (dislikes loud sounds, hands over ears, comments that it seems loud), touch (being bumped by others, hair brushing, tags, socks, etc), and heightened senses, i.e., perceptive, sensitive, Self-regulation difficulties (act outing, defiant, disobedient, easily frustrated, stubborn, inflexible, etc).
10. Common symptoms within a classroom environment: Withdrawal, playing alone or not playing at all, hesitation in responding (even nonverbally), distractibility, difficulty following a series of directions or staying on task, difficulty completing tasks. Experience at the Smart Center dictates that sensory processing difficulties may or may not cause learning or academic difficulties. Many children, especially, highly intelligent children can compensate academically and actually do quite well. MANY focus on their academic skills, often leaving behind 'the social interaction' within school. This tends to be more obvious as the child ages. What is crucial to understand is that many of these symptoms may NOT exist in a comfortable and predictable setting, such as at home. In some children, there are processing problems, such as auditory processing disorder, that cause learning issues as well as heightened stress.
11. Behavioral: Children with Selective Mutism are often inflexible and stubborn, moody, bossy, assertive and domineering at home. They may also exhibit dramatic mood swings, crying spells, withdrawal, avoidance, denial, and procrastination. These children have a need for inner control, order and structure, and may resist change or have difficulty with transitions. Some children may act silly or act out negatively in school, parties, in front of family and friends. WHY? These children have developed maladaptive coping mechanisms to combat their anxiety.
12. Co-Morbid Anxieties: Separation anxiety, Obsessive Compulsive Disorder (OCD), hoarding, Trichotillomania (hair pulling, skin picking), Generalized Anxiety Disorder, Specific phobias, Panic Disorder.
13. Communication Difficulties: Some children may have difficulty responding nonverbally to others, i.e., cannot point/nod in response to a teachers question, or indicate thank you by mouthing words. For many, waving hello/goodbye is extremely difficult. However, this is situational. This same child can not only respond nonverbally when comfortable, but can chatter nonstop! Some children may have difficulty initiating nonverbally when anxious, i.e., have difficulty or are unable to initiate play with peers or go up to a teacher to indicate need or want.
14. Social Engagement Difficulties: When one truly examines the characteristics of a child with Selective Mutism, it is obvious that many are unable to socially engage properly. When confronted by a stranger or less familiar individual, a child may withdraw, avoid eye contact, and 'shut down,' not only leaving a child speechless but preventing him/her from engaging with another individual. Greeting others, initiating needs and wants, etc., are often impossible for many children. Many shadow their parents in social environments often avoiding any social interaction at all. The common example given is; 'A child in grocery story can sing, laugh and talk loudly, but as soon as someone confronts him/her, the child freezes, avoids and withdraws from social interaction. As the child ages, freezing and shutting down rarely exist, but the child remains either noncommunicative or will respond nonverbally after an indeterminate amount of warm up time.
source: selective mutism pdf by Dr Elisa Shipon-Blum. elmtreeclinic
#situational mutism#selective mutism#mentalheathawareness#sensory processing#communication#sm tag#chaos-exhausted
21 notes
·
View notes
Text
on growing up with "intensive intervention" and abuse as a young autistic trans kid.
(quotes are from neuropsychs and reports, things said to me verbally, my own words/thought processes at different times. tw ABA, dehumanizing clinical language, stim suppression, some transphobia toward the end)
february 6th 2012.
an appealing child
with many areas of precocious development
alongside areas
of definite developmental lag.
diagnostically
meets the following criteria
for a pervasive developmental disorder.
you want more water
pronominal reversal
Alligator alligator alligator
intense and restricted interests.
immediate echolalia.
its too hard to be a girl
too hard to be (deadname)
call me pangoo the penguin
because i'm scared of (deadname).
i like it when it’s cold
i hate it when it’s hot
appears overstimulated by environment
i am never tired
scripted language
i never like to smile when people tell me to
facial expression is usually flat
too soft too tight hurt hurt no touch
extremely opposed to imposed touch
it doesn’t hurt you
it just bothers you
need to control every aspect of environment
but i like it when it’s messy
do you like bedtime? is it bedtime? is it bedtime? bed bed bed
perseverative speech
i’m not good at saying what i mean
severe communication disorder
no is my monster
i only want to point to zoo animals
extremely self directed in play
i don’t want to say that
significant conversational rigidities
(the message is wrong
it’s okay to be sad
but you have to get over it.)
the words stab into the report with grisly black ink
began to behave in a silly manner
primal defense mechanisms
unhealthy involvement with reading
atypical prosody
symbol oriented cognition
disordered phonological processes
appears uninterested in others
needed maximum verbal cues
very spontaneous and overly enthusiastic
and also withdrawn and hyper focused on her own ideas.
my hands fold into my palms in the speech therapist’s office
ripple flutter in a dance with the air
motor stereotypy
often loses focus and becomes squirmy
stilled by a dead end voice
quiet hands
‘physically disorganized’
body messy
they think it’s weird
after all
it’s hard for you to know what other people are thinking
impaired theory of mind
everybody noticed
but they were being polite
and would never have said anything
to you
responds well to a behavioral approach.
may 5, 2018.
acute awareness of needs and vulnerabilities
too old to trick into being compliant
self appointed position as autism champion
i asked her if
when she was little and only read books about alligators
if we should have expected her teachers to respect that.
she said yes
failing of course to consider
that she was in a class with people who had various interests
not obsessions.
insisted that people who are cognitively impaired should not be changed.
having a vagina does not define biological sex????
i am going to have a hard time keeping up with her thought process.
extremely hypersensitive to what is perceived
as non-acceptance or rejection.
i thought you were just one type of weird
but now you have all these different types
i’m so sorry to hear that she
(forgive the pronoun, please)
is miserable right now.
the test was not developed for use
with individuals who are gender non-conforming.
steady growth in mastery of pragmatic language skills
improved social functioning
i am so happy to hear
that she’s acknowledging she needs help
rather than continuing down the path
of “i’m perfect.”
progress intervention treatment success.
barely even autistic.
#actually autistic#actuallyautistic#poetry#writing#traumacore i guess??#aba#developmental disability#trans#autistic#ableism#mushroom.txt
26 notes
·
View notes
Text
Tracing the History of Autism
The term "autism" comes from the Greek word "autos," meaning "self." It was first used in the psychiatric context by Swiss psychiatrist Eugen Bleuler in 1911 to describe a subset of symptoms related to schizophrenia. He referred to autism as a tendency for individuals to turn inwards, away from the outside world.
However, it wasn't until the 1940s that two scientists, working independently on different continents, started to develop the concept of autism as we understand it today. In the United States, child psychiatrist Leo Kanner, and in Austria, pediatrician Hans Asperger, both noticed that some of the children they were seeing shared a unique cluster of traits, including difficulties in social interaction, communication challenges, and repetitive behaviors. These observations would lay the foundation for our understanding of Autism Spectrum Disorders (ASD).
In the 1960s and 1970s, the perspective shifted from viewing autism as a symptom of schizophrenia or a form of childhood psychosis, towards understanding it as a separate condition. During this time, researchers such as Bernard Rimland and Ole Ivar Lovaas made significant strides in distinguishing autism from other developmental disorders and started exploring educational interventions and behavioral therapies.
The 1980s and 1990s brought about a broader recognition of the autism spectrum, with conditions such as Asperger's Syndrome and Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS) being added to the Diagnostic and Statistical Manual of Mental Disorders (DSM).
In the 21st century, we've seen a shift towards understanding and accepting neurodiversity, viewing autism not just as a set of challenges, but also recognizing the unique strengths and abilities that individuals on the spectrum can possess.
Despite these advancements, there's still much more to learn about the causes and manifestations of autism, and the journey towards greater understanding and acceptance continues.
24 notes
·
View notes
Text
i love being diagnosed with pervasive developmental disorder actually it’s super funny. this developmental disorder just won’t go away!!!!!
19 notes
·
View notes
Last Seen Blogs

lowkeysaurus
It is not a deer, and maybe never was.

janetiberiuskirk
Professional Name Collector

nerdy-bookworm-1998
Gryffindor girl

iwuvcofi
Boba

dusk-bun
Dusk Bun