#mentalhealthinwriting
Text
The Nitty-Gritties of Schizophrenia

Last week I covered what schizophrenia looks using real-world experiences. This week, I’m going to dive into the disease on a more technical level. As per usual, none of this information is to be used to diagnose or treat anyone, but as a tool for writers to create characters who are close to life as possible and not mere caricatures of mental illness.
Life with schizophrenia is hard for the person experiencing the symptoms as well as the family providing care. But consider this, there was only one treatment plan for schizophrenia 100 years ago: institutionalization. Although institutionalization is still part of treatment, it is often not the only part. Thanks to new treatments and medications, many people with schizophrenia live at home or in group homes in the community. Some even have jobs. I’ll be the first to say that mental health has a LONG way to go, but I believe it is important to keep in mind where we came from.

A person with schizophrenia may manifest the following (Videbeck p. 252):
Ambivalence: Holding seemingly contradictory beliefs or feelings about the same person, event, or situation.
Associative Looseness: Fragmented or poorly related thoughts and ideas. Thoughts are tangential—not flowing from point to point but all of the place. For example, one sentence might be about baseball and the next about frogs in a pond without a coherent link.
Delusions: Fixed false beliefs that have no basis in reality
Echopraxia: Imitation of the movements and gestures of another person whom the client is observing.
Flight of ideas: Continuous flow of verbalizations in which the person jumps rapidly from one topic to another
False sensory perceptions or perceptual experiences that do not exist in reality. These can be auditory (voices), visual, smells, and tactile (feelings, like skitters across the arms).
Ideas of reference: False impressions that external events have special meaning for that person. (The person on the TV is talking to them specifically.)
Perseverations: Persistent adherence to a single idea or topic; verbal repetition of a sentence, word, or phrase; resisting attempts to change the topic.
The above list are considered “Positive Symptoms” as in they are added to the person. Most positive symptoms are treatable, but there are “Negative Symptoms” or symptoms that seem to be lacking in a person that generally linger after the positive symptoms abate. These are them:
Alogia: tendency to speak very little or to convey little substance of meaning
Anhedonia: Feeling no joy or pleasure from life or any activities or relationships (characteristic of depression, but is it any wonder with everything else possibly going on? Geez.)
Apathy: Feeling of indifference toward people, activities and events.
Blunted Affect: Restricted range of emotional feeling, tone, or mood
Catatonia: Psychologically induced immobility occasionally marked by periods of agitation or excitement; the client seems motionless, as if in a trance
Flat affect: Absence of any facial expressions that would indicate emotions or mood.
Lack of volition: absence of will, ambition, or drive to take action or accomplish tasks.

Keep in mind that the person experiencing these bizarre behaviors or thinking patterns may be fully aware of them. I once entered a patient’s room to find her smashing invisible bugs on her bedside table. She told me she knew the bugs weren’t real, but smashing them made her feel better. The extent of the awareness of symptoms is difficult to know since there is a huge communication barrier in many schizophrenic patients. The number of delusions, hallucinations, and their strength are all difficult barriers to break through.
Not every person with schizophrenia will have all of the above symptoms. In fact, schizophrenia is less of a single illness and more of a syndrome. Here are the five major types according to the DSM-IV-TR:
Paranoid Type: Has persecutory (feeling victimized or spied on) or grandiose delusions, hallucinations, and occasionally, excessive religiosity (delusional religious focus) or hostile aggressive behavior
Disorganized: Has grossly inappropriate or flat affect, incoherence, loose associations, and extremely disorganized behavior.
Catatonic Type: has marked psychomotor disturbance, either motionless or excessive motor activity. The excessive movement is not influenced by external stimuli. May also have mutism, echolalia (repetitive nonsensical speech) or echopraxia (imitation of the movements and gestures of someone the person is observing.)
Undifferentiated Type: Sort of a mix of the above
Residual Type: Has a history of one previous, but not current, episode.
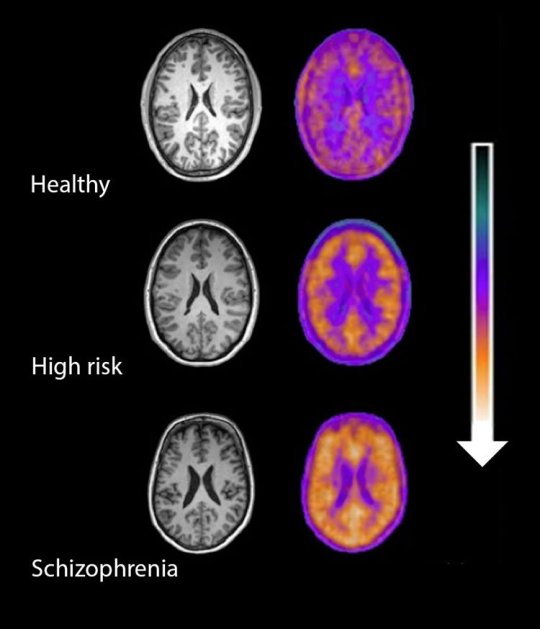
Schizophrenia generally starts around age 15-25. There is a genetic component to the disease, but having a genetic predisposition to the illness is not a guarantee it will present. Studies on identical twins show a 50% chance of the previously unaffected twin getting the disease. Through various imaging techniques, we have been able to see that those suffering with schizophrenia have alterations in their overall brain structures. How these came about are still a mystery although some theorize it comes about through viruses, trauma, or immune responses. Basically, the theory is that certain people have a genetic predisposition to get schizophrenia if a certain thing occurs to turn on those genes. For example, a virus comes along and triggers those genes and the brain deteriorates. There’s a similar theory regarding the onset of juvenile diabetes.
While there can be a sudden onset of schizophrenia, most people generally develop signs and symptoms slowly over time. It starts with social withdrawal, unusual behavior, loss of interest in school or work, and neglected hygiene. Generally, the diagnosis is made when delusions, hallucinations, and disordered thinking begin to appear. The age at which schizophrenia appears often determines the overall impact of the illness. The younger the onset, the worse they tend to do. Also, a slower onset predicts a worse outcome than a sudden onset.
Two years after initial onset, two patterns typically emerge. Either the person continues to experience psychosis and never fully recover (although symptoms may shift in severity over time), or they alternate between episodes of psychosis and near complete recovery.
The intensity of the psychosis also seems to diminish with age. Some may be able to function, live independently, and succeed at jobs with stable expectations and supportive work environments. Most, however, have severe difficulty functioning in their communities.
It is important to keep in mind that a person showing initial signs and symptoms of schizophrenia might lose all symptoms within a period of six months. This is called Schizophreniform disorder. Others might experience a brief psychotic disorder where delusions, hallucinations, or disorganized speech may last from 1 day to 1 month. It may or may not have an identifiable stressor or follow childbirth.
There is SOOOOOO much to tell when it comes to schizophrenia and this post has already become way to long. Next week, I’ll be creating a post that brings together all of this information in a usable form.
As I was researching this, I came across this article I found very informative but did not use as a source: http://www.drjack.co.uk/the-future-of-schizophrenia-by-dr-jack-lewis/
Psychiatric-Mental Health Nursing, by Sheila L. Videbeck, fifth ed., Wolters Kluwer/Lippincott Williams & Wilkins, 2011.
#mental#mental wellbeing#mental help#mental health#mentalhealthawareness#mentalhealth in fiction#mentalhealthinwriting#mentalhealthandwriting#mental illness#mental ill health#writing#writers#writersblog#writerslife#write#author#authorblog#authortips#writerstips#writeradvice#authoradvice#authorlife#writerlife
94 notes
·
View notes
Text
Schizophrenia for Writers
Schizophrenia for Writers

Schizophrenia is probably the most well-known illness, as in most have heard about it, but do people really know what it looks like? Probably the best image brought up by the population is a homeless person walking around in circles talking to the air. It can be startling to encounter someone in the middle of an episode like that. Schizophrenics have a tendency to be more aggressive and hostile than the general population. But after working with several schizophrenics, I have less fear and more sadness for those suffering with this debilitating illness.
I was initially going to crack open my textbook like usual and tell you all the ‘official’ things about schizophrenia, but I’m going to put that off until next week. Instead, I’m going to tell you what I’ve seen from my nursing practice.
My first up-close encounter with schizophrenia in the clinical setting was with Mary*. Mary was a well-known frequent flier of the psychiatric institute I was completing my nursing clinical hours in. I was given Mary’s file to read then sent to speak with her for an hour. Since my previous vision of schizophrenia was of homeless people walking talking to the air, I was quite nervous about even approaching Mary, let alone sitting in the drab stone-walled courtyard on a bench and chatting.

Mary, however, acknowledged me with a courteous nod. She never smiled at me, but she was never hostile or aggressive toward me. Instead, she talked about her life as I would expect anyone too, with earnestness about her life experiences. She had no verbal slurring or strange repetition of words. I could have walked up to this woman at Walmart and never known she was schizophrenic.
Mary told me all about her conniving sister who was hell-bent on destroying her life. If Mary had a chance at getting a job, her sister would call the manager and convince him not to hire her. When Mary tried to move away, her sister followed her to the next state over and continued to keep her under her thumb. Even while she was being institutionalized, her sister was stealing her social security check and paying the people inside to watch her. And the people here—oh she’d tell you about them. Everything you ate or drank was laced in parasites that would eat you from the inside out. The pills were laced too, which was why she was refusing to take hers.
Of course, very little of this (if any) was true. But Mary believed it was. Because everyone was out to get her, she had no hope of securing a good job, good employment, or establishing any lasting relationships in her life.
The next week, I met Todd*, a 20-year-old schizophrenic who, per the staff, had been practically abandoned in the institution by his family. Todd was heavily medicated when I met him. His posture was stooped, his speech was slurred, and his reaction time was comically slow. I asked him about his life, and my heart broke. Todd had accepted his diagnosis and knew he was mentally ill, but with this knowledge came the fact he would never be able to have a family or a real relationship of any kind. Or have sex. When he said this last part, he slapped his hand over his mouth—with exaggerated slowness due to the meds. It would have been funny had it not been sad and possibly true. He drew me a picture before I left. The drawing was the skill of a 3rd grader in markers. I still have it.
Then we have Johnnie*. Johnnie was a patient of mine at the hospital. He came in for a bacterial gut infection which we treated in half a week, but while he was in our care, the psychiatric hospital discharged him. Getting an empty bed in a psychiatric hospital is nearly impossible, but Johnnie was so unwell we could not discharge him to the streets either.
Hospitals are not designed for long-term care of anyone, especially psych patients. Johnnie would walk down the hall outside his room and bang his head against the walls. Because of this, he was forced to stay in his room the whole time. Johnnie would scream and wail so loud you could hear him throughout the whole floor. Patients would complain, but what could we do? He would try to hit nurses and fight. He jammed his hand into his mouth and bit until it drew blood. We tried to place him in an institution somewhere—anywhere, but no one would take him. I don’t know how many combinations of medications we tried, but we couldn’t find the right balance to keep him calm. So what was the solution?
Johnnie was tied to his bed. Still screaming, still fighting. His wrists became sores from pulling against the restraints. He stayed in the hospital like that for a month.

Johnnie was pretty much non-communicative, but we can imagine his thoughts knowing how Mary thought. He thought we were trying to kill him, so we tied him to a bed. That helped.
Johnnie was just a little older than Todd. Similar dreams, similar hopes—like all of us, but this was his life. Terrified, trapped, and being harmed by the people who should be helping him.
Our system is broken.
And so is our view of mental illness. Yes, schizophrenics commit violent crimes more often than the general population, but they are victims of crimes more often too. What if someone raped Mary? She could report it, but would anyone believe her? What if someone beat up Todd? He could report it, but would someone think it was self-inflicted?
I don’t know what to do about our broken system. But I do know, as writers, we have a responsibility to portray characters accurately. So, think on this before you write a schizophrenic character. Are they flat and cartoon-like? Or do they have hopes, loves, and broken dreams as well?
*names changed
#writing#writer#writersblog#writingtips#writingadvice#schizophrenia#mentalillness#mentalhealth#mentalhealthawareness#mentalhealthinwriting#mentalhealthinfiction#fiction#literature#characterdevelopment#author#authorblog#write#authorlife#writerslife
72 notes
·
View notes
Text
Using Anxiety as a Character Arc
My last few blog posts were discussing what anxiety is from a clinical standpoint. Today, we’re going to bring all the pieces together and discuss how you can use this to form a character/story arc.
I
If you have been exposed to any writing theory at all, then you are probably at least a little familiar with standard story structures. This is the form in which most stories go: First there’s an introduction followed by an inciting incident, then there’s the middle stuff as the character tries to manage the change in their world that was caused by the inciting incident. Everything comes to a head in the climax followed by the resolution. Now I’m going to describe this using what we’ve previously discussed in anxiety terms.
Character is living life in a relatively normal way whether they be a young teen or an expert secret agent. Then a stressor occurs: teen is in a major car accident and loses her leg; secret agent is betrayed and watches helplessly as his entire team is killed. This stressor will cause a psychological and physiological response in the character (see post: Anxiety for Writer’s Summarized). Depending upon what type of story you are writing, you may want to linger here for a bit. If your character is a teen suffering from loss of limb, a good portion of the story might be spent on failing to accept herself, falling into a depression, and journeying out. (Keeping in mind that these mental health conditions are linked and anxiety often leads to depression. For more information on types of anxiety disorders, what they look like, and why they might manifest, see post: Writers Guide to Mental Health: Anxiety Disorders)
At some point in the story, a decision by your character, conscious or otherwise, needs to be made. Are they going to live in a continual state of anxiety? Or are they going to move forward and out of that state?
Your character may not come out of it. They may fall into a depression and that’s how the story ends. Keep in mind that is an option. A tragic option, but an option nonetheless.
If your character does seek help and healing, they will probably go through some sort of a process where they face their fears and become more courageous. This can be through self-initiative or with the formal help of a therapist. How this happens will be determined by a lot of factors including your story type, setting, and character’s personalities. For information on how anxiety is treated in a clinical setting, check out my post: Writers Guide for the Treatment of Anxiety Disorders.
Probably the best, well-known story to use as an example in bringing all this together is Batman. Bruce Wayne is afraid of bats. They cause an anxiety related response, so he exposes himself to these bats until he is braver. Then he channels the bat in order to defeat the underworld.
Of course, this is just a superficial representation of what is taking place in the broader story as a whole. Bruce Wayne experienced a trauma when his parents were murdered by members of the criminal underworld. For years, he struggled with the grief and fear of this event. Then he channeled his fears, became a criminal vigilante, and confronted them and defeated the criminal underworld.
It’s a simple formula, really, but it is scientifically and psychologically based and serves as a good formula to create story arcs and character arcs. If you can think of other stories that follow this similar pattern, please name them in the comments below.
#books#bookblog#write#writer#writing#writingontumblr#writingblog#writersblog#writingtips#mywriting#writingadvice#story#storytips#characterdevelopment#literature#anxiety#mentalhealth#literaturetips#mentalhealthinwriting#storyadvice#characterdevelopmentinliterature#author#authortips#authoradvice#authorblog#characterarcs#storyarcs#plotdevice#plottips#plotadvice
22 notes
·
View notes
Last Seen Blogs

matimimio
♱ 𝓂𝒶𝓉𝒾𝓂𝒾𝓂𝒾𝑜 ♱

songs-of-owly
i deserve good things

lockssanmarcos-blog
Locksmith San Marcos


blog-chaves
Bella chaves