#including the harm that can happen in terms of injury and body image
Text
we do not need to engage with all posts. sometimes people can be stupid on the internet and it's fine, actually. we do not need to correct people for making grandiose statements based on knowledge they acquired at age 11 and haven't updated since <- said through gritted teeth
#normally i'm not that peeved by like minor dumb shit on the internet#but this post about how ballet and american football are equivalent in terms of injury/shouldn't be allowed/etc#is rubbing me the wrong way#and the number of people being like well ACTCHUALLY i danced till i was ELEVEN and it should be BANNED#is. much more annoying as it turns out#this is not to say that ballet doesn't have many many many problems#including the harm that can happen in terms of injury and body image#and the classism racism sexism etc etc we can go on for a while here#but the way it's framed in this post and the way ppl are responding to it is making me remarkably annoyed#which is why i'm grumbling on my blog instead of responding to the post itself#bc we do NOT need to respond#hnnnnn#also. will freely admit that i'm probably a lil extra testy about it after 5 hr of class/rehearsal today#and killing my freeds after 2 hr :')#WHY shoes#anyway to the person who said pointe should be banned until they come up with specialized shoes to reduce the damage#GUESS WHAT#that's why they have pointe shoe fitting specialists#and yes! access to and equitable/fair treatment in those environments is troubled#but we are not running headfirst at each other until we all have super duper brain damage#okay. it's fine. it's fine.#upon further reflection i think a solid 75% of my irritation comes from calling ballet a sport. this is a hill i have been angrily guarding#since i was like 12#and am actually right about it. anyway. again. It's Fine. I'm letting it go
12 notes
·
View notes
Text
pinned post under construction :3
hello it is i. apuff. if you don't know me, you can call me puff or apuff, and if you do know me, you can also call me puff or apuff. if you know my actual name due to being friends (YOU KNOW WHO YOU ARE), you can use ann as a substitute
i like albums, concept albums, concepts, conceptual art, concept art, and art, and i also liked making that sentence
in case you couldn't already tell, i am obsessed with my chemical romance, it basically eclipses my entire waking mind
i also like webcomics like unfamiliar, castoff, aurora, i want to be a cute anime girl, heartstopper, and laika's comet
blog organization + tags vv
i have a few different tags for various things in my blog, like:
art (some old art of others' is on here, but it's mostly my art)
apuff's inane ramblings (inconsequential text posts)
mcr (My Chemical Romance is an American rock band from Newark, Ne)
dungeon meshi (you know what this is you're on tumblr)
miku (HATSUNE MIKUUUUU)
art save (things that are pretty, i'm trying to keep tutorials out of this now but i might forget)
save (like..general useful stuff, good websites, not very specific)
things i want to draw (self-explanatory, more for text posts that inspire me than images, which is "art save")
picrew (picrew chains. i reblog the picrew of people that i tag in these because otherwise i can't find them ever)
long post (posts that are long, this is mostly for blacklisting)
free palestine (self-explanatory)
remember this (desperate plea. i don't even know what i use this for)
art tutorials (TAG I JUST MADE UP NOW!!! i probably won't retroactively tag things as this)
-----
ok so for starters for trigger/blacklist tagging i'm using the format of just the thing in the tag, not "cw" or "tw" before or after it. for example, something with blood would just be "blood" not "tw blood."
for bright colors, i'm doing "eyestrain." i'm tagging things with flashing/strobing colors, lights, or light n darkness "flashing lights" if you're sensitive to that, please make sure you have it blocked since i can't cover the absolute myriad of the unstandardized tags for that specific thing on every reblog with it.
let me know if there's something i need to tag on a post, i forget a lot of stuff/autoreblog plus there's fears i don't know about and things
now palestine/gaza related posts are sort of a whole different beast in terms of tagging? i'm trying to put down "free palestine" on every post i reblog about the topic (cause you actually need to do that to get tags to trending) (plus overall blog sorting is good)
now obviously, the entire GENERAL CONCEPT of the current genocide is dark and upsetting, so know that i really can't tag every possible thing that could be upsetting. but, i'm trying to make a system of particularly upsetting things, especially pertaining to images & videos
ok so. for images/videos of children being actively harmed, as well as graphic text descriptions, i'm doing "child harm" this does not cover statistics of children killed or general comments on the fact
things like videos/images of gunfire, shooting and bombing, i'm doing "violence" like the other one this doesn't cover descriptions of those things happening.
"injuries" is self-explanatory- burns, bloody injuries, face trauma, etc, you get the drill (even blurred/pixely censored ones)
"dead body" is also self-explanatory, doesn't include body bags except if they have visible body part sticking out
tags that could mostly apply to anything (like "gun" or "blood") don't have any special tags, i just use the generic ones like i said above
still thinking of a tag for people being distressed about their situation/ their dead loved ones since things like "death"' are too vague and would cause overfiltering but i can't think of something accurate. if you have any suggestions, let me know.
6 notes
·
View notes
Text
relationship hcs ; dark enchantress cookie

requested by ; 🍾 anon (12/08/23)
fandom(s) ; cookie run
fandom masterlist(s) ; hub | specific
character(s) ; dark enchantress cookie
outline ; “first off the list smut and relationship hcs for Dark Enchantress my love my life 😍😘 ~ 🍾”
warning(s) ; none, just fluff!
a relationship with dark enchantress cookie wouldn’t be traditional by any means nor would it be the most healthy — but between her extreme preferential treatment towards you, her overprotectiveness, and her insistence on treating each and every major or minor injury you gain herself rather than handing you over to pomegranate cookie or another magic user, it’s clear as day that she cares about you in her own way
she uses lots of traditional terms of endearment like ‘my dear’ but when she’s in one of her moods she’ll call you something along the lines of ‘little one’ whilst gently scolding you and telling you to get out of her way and let her punish the interloper — she never truly insults you, but she gets a lot colder in those moments before acting like nothing happened later on when she catches up with you in a much better mood than before
dark enchantress cookie refuses to let any of her servants near you and will scold or punish them severely if she catches them trying to interact with you — of course in the case of an emergency she makes an exception (even then she only barely trusts pomegranate cookie because of her loyalty), but generally speaking she’s much too possessive and protective to ‘share’ you with others in any way
she’s not really sentimental by any means and values her image and reputation as being both powerful and intimidating, but she does save a small collection of gifts you’ve given her — including some carefully preserved flowers from your first anniversary, some letters you wrote to her when she was away, and jewellery you had commissioned for her (it’s a small collection and extremely well hidden, and in fact she’s the only one that knows it exists, but she will revisit it on the rare days where you’re apart and she finds herself missing your presence — not that she’d ever admit to having such moments of weakness, of course)
her love language is absolutely acts of service when it comes to both giving and receiving, and she’s very particular in how she goes about it — tending to your wounds and sicknesses, having your favourite foods made for you by those serving her, and taking anyone who dared to upset or harm you out of the picture permanently, for example — and when it comes to receiving, the most impactful thing you can do for her is repairing her clothing, massaging away her aches and pains, and helping to get her servants under control when they’re being rowdy (she won’t admit it, but sometimes their energy can be a bit much for her to keep up with at her age, so she does appreciate the help)
she’s extremely quick to jealousy and quick to act on it as well — typically relying on her fearsome reputation to scare off anyone who dared to flirt with you (or even just get too close for her liking), whilst making it abundantly clear through shows of pda (usually very rough kissing and pulling you against her body) that you’re taken and that nobody else should consider following their example — but she won’t take it out on you unless you actively reciprocate or initiate the encounter to get a rise out of her (at which point you’d be thoroughly punished for it because she is beyond the age where such things are appropriate, if there even is an age where it is at all)
#sleepingdeath#🍾 anon#fluff#fluff hcs#gender neutral reader#crk fluff#cookie run fluff#dark enchantress cookie fluff#dark enchantress cookie x reader#cookie run x reader#crk x reader
15 notes
·
View notes
Text
What is Medical Equipment?

Medical equipment refers to tools and machines that doctors use to figure out, treat, or stop sickness or injury. These can range from basic items like stethoscopes and blood pressure cuffs to more advanced machines like MRI scanners and breathing machines. Medical equipment is really important for giving medical care. If there were no medical tools, many illnesses and treatments wouldn't work. Medical equipment can be put into groups. One group is for diagnosing – finding out what's wrong. X-ray machines, ultrasound machines, and CT scanners are part of this. Another group is for treating – making people better. Bandages and splints are simple ones, and then there are more complex things like dialysis machines and defibrillators. The last group is for preventing – stopping sickness or injury before they happens. This includes stuff like vaccines and seat belts. Medical tools are always changing. New ideas and technologies are always coming up to make diagnoses more accurate, treatments work better, and everyone stays safe.
Types of Medical Equipment
Medical professionals have a variety of tools to help them figure out and treat patients. Some common types are:
X-ray machines: These make pictures of the inside of the body, helping doctors see issues with bones, organs, and tissues.
CT scanners: They create detailed images of the body's insides, aiding in finding problems with bones, organs, and tissues.
MRI machines: These machines also make detailed images of inside the body, which can help detect issues with bones, organs, and tissues.
Ultrasound machines: They use sound waves to create images inside the body, useful for spotting issues with organs and tissues.
Lab equipment: This includes machines that test samples of blood, urine, and other tissues, which helps find problems with organs and tissues.
Medical devices: These are various tools that doctors use to treat patients, like pacemakers, defibrillators, and artificial joints.
Features of Medical Equipment
Medical equipment refers to tools and devices that help with diagnosing, treating, or stopping diseases. This ranges from basic items like stethoscopes and blood pressure cuffs to complex machines like MRI scanners and heart-lung machines. Medical tools need to be clean, safe, and strong for repeated use. Some are used only once, while others last for many years. To work well, medical tools must be designed and built properly. They should also be simple to use and maintain. Being dependable and tough is crucial for medical tools. They should handle lots of use without breaking. Using good materials helps prevent easy damage. Cleaning them should be easy, and they should resist harm from cleaning substances. Medical tools should be user-friendly. Setting up and using them should be simple. Instructions and displays must be easy to understand. Most importantly, medical tools must be safe. They should be designed to avoid hurting patients and medical staff. Testing them thoroughly before using them on patients is a must. Medical tools must be able to endure lots of use.
How to Choose the Right Medical Equipment?
When buying medical equipment, there are important things to think about. This guide will help you pick the right equipment for your needs.
Type of Equipment: First, think about what kind of medical equipment you need. There's a wide range available, from simple tools like blood pressure monitors to advanced machines like MRIs. Choose what suits your needs.
Cost: Next, consider the price. Medical equipment can be pricey. Make sure you can afford what you need. You might get financial help – talk to an advisor for options.
Maintenance and Support: Medical equipment needs regular care. Pick a supplier who can give you the support you need to keep it working well.
Warranty: Check the warranty. Most equipment has one, but understand the terms before buying.
Training and Help: Think about how you'll learn to use the equipment. Some suppliers offer training and support. Choose one that helps you use the equipment correctly
Clin Med is a company that aims to help caregivers do their jobs better by offering excellent solutions. We want to create a top-notch company that supplies medical equipment, giving healthcare providers the tools they need for better results. Feel free to reach out to us today
Auditor
Thank you for joining me on this journey through my blog post . I hope you found it informative and thought-provoking. If you have any questions or additional insights to share, please leave a comment below.
0 notes
Text
An Unbiased View of Sleep Apnea in Novi
I happen to be going to Dr. Gordon for quite a while now. On getting into the ability you're greeted with smiles from the receptionists. The ready place is…
He in the end handed absent on December 31, 2012. Mr. Ramos was unemployed when the treatment at concern happened and his survivors provided his adult son and sister, who aided care for him right before he passed.
PVL is often a style of brain injury that entails the periventricular white making a difference in the Mind. Harm to the white subject ends in the Loss of life and decay of injured cells, leaving vacant regions within the Mind referred to as lateral ventricles, which fill with fluid (a condition identified as leukomalacia). After the MRI, his managing doctors attributed his developmental delays in the area of speech being in the PVL.
Ramos without analyzing the etiology of the subacute infarcts didn't do a sufficient stroke to get the job done up, failed to get hold of cardiology to seek advice and didn't perform enough neurological sessions. Insofar as none of the medical professionals at Christ Medical center or Jersey Town Health-related Centre had been at any time able to find out the etiology of the strokes, or avoid them, The difficulty of causation remained problematic.
The plaintiffs argued the truck driver did not abide by trucking sector requirements, motorcar guidelines as well as other statutes. Plaintiffs preserved this carelessness as the direct reason for the incident, the accidents, and the resultant death.
Once the gasoline pedal turned unstuck, the auto surged ahead and rolled over, leading to her arm becoming crushed and partly amputated when it was ejected from the sunroof during the rollover.
He was pronounced dead at the scene and his autopsy unveiled a completed transected aorta, a fractured thoracic backbone and blunt pressure injuries to The pinnacle and neck.
By miscalculating the believed date of shipping and inducing the supply on August 1, 2005, the plaintiff’s gurus opined that the defendant induced an iatrogenic preterm birth that improved the potential risk of the infant acquiring brief- and prolonged-term morbidity which includes although not limited to respiratory troubles just after beginning and very long-term neuro-developmental troubles.
Right here, the Defendant initially requested the correct take look when he requested the CT angiogram, having said that, his determination to cancel this and progress as an alternative with a non-contrast CT of the upper body was a decision that fell underneath the normal of treatment and triggered unnecessary hold off in diagnosing the aortic dissection.
"Dr. Gregory Varjabedian is an excellent healthcare provider. I went to view him for some issues with my nasal and bordering eye location. He was very complete in his Examination and he looked at the ... Browse Far more"
The water was very very hot and brought about severe burns to our client’s feet and ankles. He put in various months hospitalized in a burn-off device and endured many surgical techniques to help save his legs. Unfortunately, 1 leg eventually essential an amputation underneath the knee.
A narrowed airway. You might have inherited a slender throat. Tonsils or adenoids also can enlarge and block the airway, particularly in little ones.
$1,250,000 Settlement for Delay in Analysis of Lung Most cancers Develop William O. Crutchlow, Esq. of Eichen Crutchlow Zaslow, LLP with places of work in Edison, Toms River and Purple Financial institution, New Jersey was co-direct counsel on the situation arising in the delay in the diagnosis of lung most cancers which fixed for $one, two hundred,000. Our consumer was in her early 50s when an abnormality in her lung was recognized on a CT scan. We alleged that the radiologist who interpreted website the CT scan failed to properly evaluate the ominous character of the lesion and did not effectively direct the patient’s managing Medical professionals to timely adhere to extra imaging studies.
Mr. Zaslow and his industry experts were being essential that even after they discharged Mr. Ramos the defendants failed to go ahead and take the most simple measures to lessen the probability that Mr. Ramos would undergo an additional stroke. They even did not advise Mr. Ramos to take aspirin.
0 notes
Photo


bonus 2, post chapter 4
first - previous - next
[image description: an sac webcomic page. 5 pages styled in a manner similar to a medical brochure titled “navigating your new abilities, what does this mean for me?”. the brochure is about superpowers, what the are, side effects and health risks, and job oppurtunities. the brochure has white and light blue for the main colours, with a dark purple accent.
page 1: mostly showing a girl transforming, with the title listed above, with smaller text reading “created and supported by the paragon institute for superheroism.” the girl is a younger white woman who has a light purple colour scheme, long straight hair and bangs, a crop top, and elbow pads. shes shown from the waist up, half her body and an arm cut out of the photo. her transformation takes the form of dripping black-purple goop spreading, with a starry texture. a similar texture takes up the image background.
page 2: title: what are superpowers?. “Superpower is a term used for superpowered abilities that go beyond the natural abilities and conventional laws of reality. There are little limits to the potential types of abilities that a super powered person may possess.
It is currently unknown what causes superpowered abilities. Despite many theories, the only known way to guarantee superpowers is to inherit them from a parent.
London has the highest percentage of superpowered people in the entire world, in addition to having 42% of all supers in the united kingdom”
next to this text is a grinning woman in pink winking while posing with one hand on her hip, and the other in a fist held up. the woman has long wavy pale pink hair, light brown skin, many freckles, and hot pink eyes. her outfit is a pink dress and gloves, pale pink tattered cape, and a hot pink long sleeved undershirt.
“how do i use and control my abilities? Superpowered people will typically have an innate sense for how to transform and use their abilities,but like any skill it will take time and effort to fully control their abilities.
In some rare cases, a superpowered person may lack control over their powers to the extent where it can cause harm to those around them.
This is most common in those who have inherited their abilities. In these cases the P.I.S offers programs to assist these people in learning control with 24/7 care and supervision. If you or someone you know requires these programs, please call our number or otherwise contact us via our website.
Due to the range of superpowered abilities, there is no one-size-fits-all method of developing control, however, the P.I.S do offer training services, of which you can read more about atwww.pis.uk/pis-services/training
next to this is a teenage superhero, an androgynous boy with a grey colour scheme, smiling slightly, his arm turning into smoke. he has light grey hair and eyes, brown skin and a dark grey bodysuit. he has a grey poncho/cape conbo and gloves, both of which are lined with light grey fleece or fur. his outfit looks as if is was meant for cold weather.
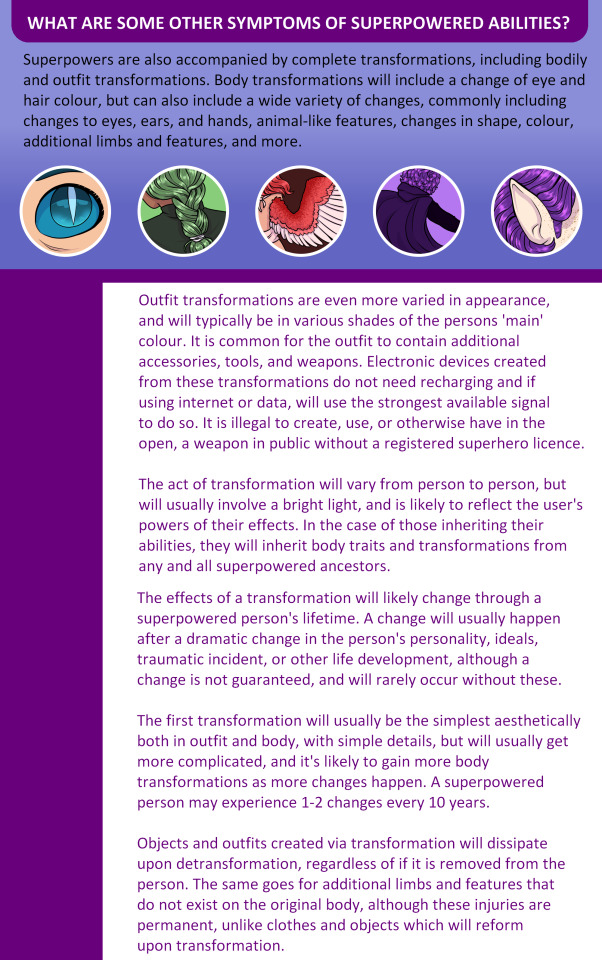
page 3: what are some other symptoms of superpowered abilities? Superpowers are also accompanied by complete transformations, including bodily and outfit transformations. Body transformations will include a change of eye and hair colour, but can also include a wide variety of changes, commonly including changes to eyes, ears, and hands, animal-like features, changes in shape, colour, additional limbs and features, and more.
below that is 5 examples, inside circles with a white border: a close up of an eye, all blue including sclera, the pupil is pale and slit like a cat. next is a close up of a green haired braid. next if also from behind, a red haired person with red wings, the longest feathers of which are white. while the last three arent of any known character, the latter two are wraith, shown from behind, only showing hair and a cape, and part of an arm, and quartz, a close up of his elf-like ear.
Outfit transformations are even more varied in appearance, and will typically be in various shades of the persons 'main' colour. It is common for the outfit to contain additional accessories, tools, and weapons. Electronic devices created from these transformations do not need recharging and if using internet or data, will use the strongest available signal to do so. It is illegal to create, use, or otherwise have in the open, a weapon in public without a registered superhero licence.
The act of transformation will vary from person to person, but will usually involve a bright light, and is likely to reflect the user's powers of their effects. In the case of those inheriting their abilities, they will inherit body traits and transformations from any and all superpowered ancestors.
The effects of a transformation will likely change through a superpowered person's lifetime. A change will usually happen after a dramatic change in the person's personality, ideals, traumatic incident, or other life development, although a change is not guaranteed, and will rarely occur without these.
The first transformation will usually be the simplest aesthetically both in outfit and body, with simple details, but will usually get more complicated, and it's likely to gain more body transformations as more changes happen. A superpowered person may experience 1-2 changes every 10 years.
Objects and outfits created via transformation will dissipate upon detransformation, regardless of if it is removed from the person. The same goes for additional limbs and features that do not exist on the original body, although these injuries are permanent, unlike clothes and objects which will reform upon transformation.
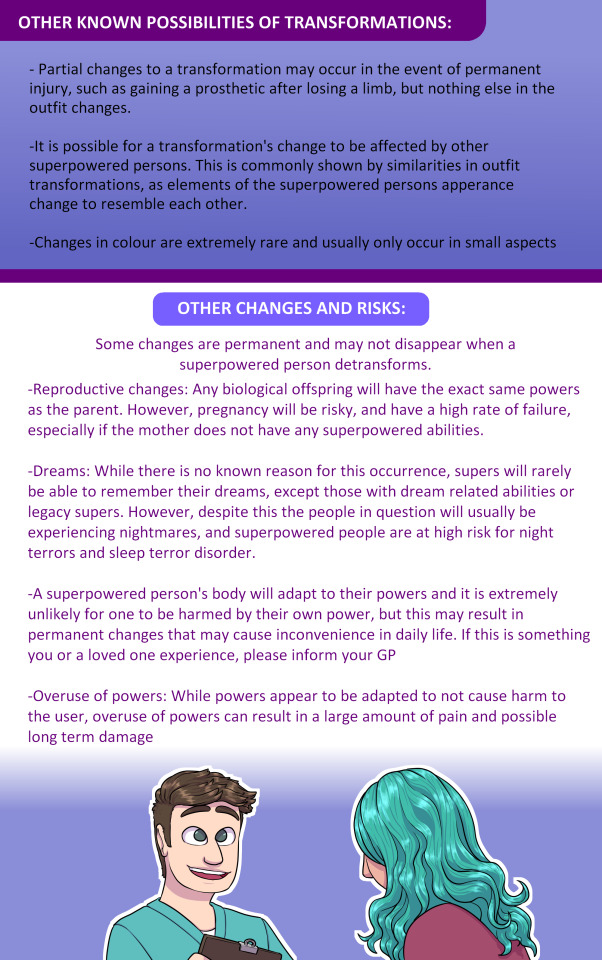
page 4: other known possibilities of transformations:
- Partial changes to a transformation may occur in the event of permanent injury, such as gaining a prosthetic after losing a limb, but nothing else in the outfit changes.
-It is possible for a transformation's change to be affected by other superpowered persons. This is commonly shown by similarities in outfit transformations, as elements of the superpowered persons apperance change to resemble each other.
-Changes in colour are extremely rare and usually only occur in small aspects
other changes and risks: Some changes are permanent and may not disappear when a superpowered person detransforms.
-Reproductive changes: Any biological offspring will have the exact same powers as the parent. However, pregnancy will be risky, and have a high rate of failure, especially if the mother does not have any superpowered abilities.
-Dreams: While there is no known reason for this occurrence, supers will rarely be able to remember their dreams, except those with dream related abilities or legacy supers. However, despite this the people in question will usually be experiencing nightmares, and superpowered people are at high risk for night terrors and sleep terror disorder.
-A superpowered person's body will adapt to their powers and it is extremely unlikely for one to be harmed by their own power, but this may result in permanent changes that may cause inconvenience in daily life. If this is something you or a loved one experience, please inform your GP
-Overuse of powers: While powers appear to be adapted to not cause harm to the user, overuse of powers can result in a large amount of pain and possible long term damage
below that is an image of two people, on looking like a doctor, a pale man with dull brown hair and dull green eyes, dressed as a doctor and smiling with a clipboard, looking at a person shown from behind, with long mint hair.
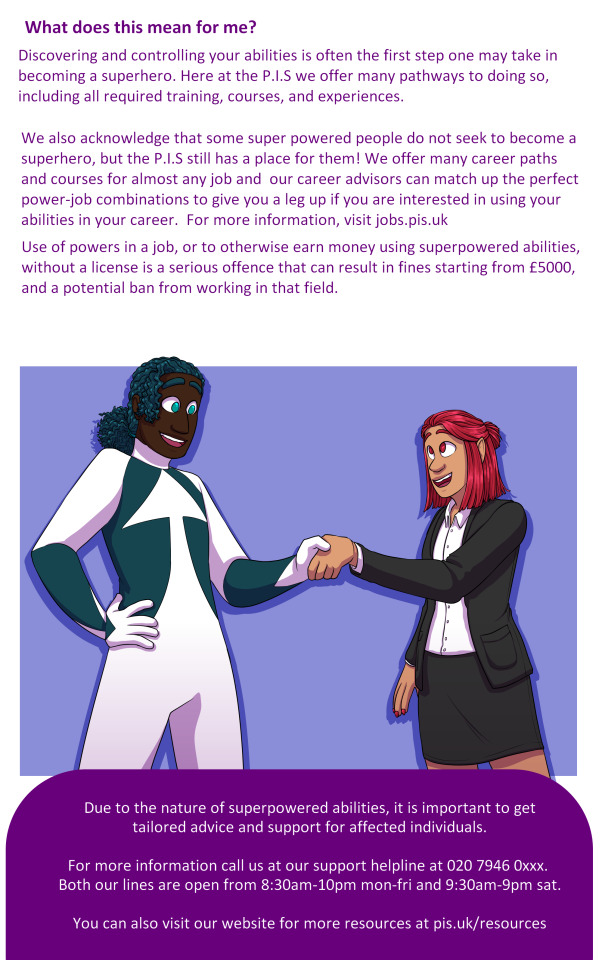
page 5: what does this mean for me?
Discovering and controlling your abilities is often the first step one may take inbecoming a superhero. Here at the P.I.S we offer many pathways to doing so,including all required training, courses, and experiences.
We also acknowledge that some super powered people do not seek to become asuperhero, but the P.I.S still has a place for them! We offer many career pathsand courses for almost any job and our career advisors can match up the perfectpower-job combinations to give you a leg up if you are interested in using yourabilities in your career. For more information, visit jobs.pis.uk
Use of powers in a job, or to otherwise earn money using superpowered abilities,without a license is a serious offence that can result in fines starting from £5000,and a potential ban from working in that field.
below is the superhero arrow, grinning at a woman in a plain looking suit. he has one hand on his hip and the other is shaking hands with the woman. the women has red hair and eyes, and pointy red nails.
Due to the nature of superpowered abilities, it is important to gettailored advice and support for affected individuals.For more information call us at our support helpline at 020 7946 0xxx. Both our lines are open from 8:30am-10pm mon-fri and 9:30am-9pm sat.You can also visit our website for more resources at pis.uk/resources. end id]
sorry for last weeks lack of update, irl stuff is happening too much and too fast
anyway heres something ive wanted to do for a while, a pamphlet thats kinda medical style? it seemed like it would be fun and i wanted an excuse to try something new and im always down to infodump (affectionate) about my ocs
however im half asleep, ive already delayed an update for a week, and im a little stressed so i didnt get a proper proofread so sorry if theres any typo or if i left a placeholder in ill get it later if i see any late
edit: did i really forget to fucking finish the fake phone number at the end? anyway sometimes fake phone numbers are reserved for tv and stuff if a phone number is needed, thats the one used for london fake numbers, i just forgot to finish it until i went back to write the id there
#someone always cares#sac#webcomic#lore#worldbuilding#im nervous to post bc i was like. is this to self indulgent? will people like it?#and then i was like bro.#its my fucking webcomic OF COURSE its self indulgent that half the fucking point#some of this is stuff ive rambled lots to friends but realised oh it just hasnt come up in comic so here it is i guess#im hoping this is readable bc i can read it fine on my phone
31 notes
·
View notes
Text
TW // Trigger Warnings

⚠️ Disclaimer - The authors of this article are in no way specialised in dealing with trauma or PTSD. All the content and information in the article has been written only after intense research and several discussions. Views expressed in the article belong to the authors.
The internet was once a cozy web, attracting a few people like flies. But now, the internet has grown into something bigger than Aragog could weave. In such a huge space that technically has minimal supervision, disturbing content can be put up for everyone to see as easy as a click. This can have a long lasting effect on some viewers. How do we avoid unwittingly affecting those who might be adverse to such content? Simple. Trigger Warnings.
⚠️ What is it?
A trigger warning is a statement made prior to sharing potentially disturbing content. People who may struggle with PTSD (Post-Traumatic Stress Disorder) and/or panic disorders often have things that “trigger” them. These triggers activate the person’s fight or flight response, causing distress to the individual, and may also result in a flashback which could lead to a full blown panic attack. To help a person brace themselves for this kind of content which could potentially “trigger” them, a trigger warning is used.
We’ve all heard the word ‘trauma’, and used it casually. But what is it exactly? According to the American Psychology Association (APA), trauma is an emotional response to a terrible event like an accident, sexual assault or natural disasters. A trigger is a stimulus that brings back memories of said trauma. According to several researchers, triggers are highly specific to the particular individual, including and not restricted to which sense organ the trigger is tied to, and how each individual reacts to the trigger. When a person is affected by a trigger, they experience something that is termed by psychologists as “intrusion symptoms”. Intrusion symptoms may occur without any stimulus, but most times, certain smells, sounds, words or images might cause one to relive their trauma. Trigger warnings are used to inform the individual that there is distressing content that could potentially trigger their trauma.
Generally, the trigger may not actually be the traumatic incident itself, but things that may remind them of what happened before said traumatic incident. A baseball bat might trigger a certain person because their assaulter may have broken into their house with a baseball bat. A person who has been raped could be triggered by the smell of their rapist’s cologne, even years later. A person who lived with abusive parents could find the smell of a certain type or brand of alcohol triggering. A certain ringtone or noise could cause someone to go into a panic attack.
This is where trigger warnings can be useless, because on the one hand, one would not think that something like a ringtone could be potentially “triggering”. On the other hand, it’s unrealistic to put a trigger warning before every piece of media, on the off chance that one potential viewer could get triggered by the content.
⚠️ Traumatic events Vs. Content
There’s a difference between trigger warnings and content warnings. Trigger warnings are used to warn the viewer about content that could lead to intrusion symptoms, while content warning is generally used as a warning of disturbing content that could upset a majority of the viewers, irrespective of whether it causes intrusion symptoms or not. This is typically used before depictions of graphic violence, sexual assault and abuse, animal abuse, and even flashing lights. However, the line between trigger and content warning is pretty blurred, since all these things could also cause intrusion symptoms.
⚠️ Going back to the Web
A lot of people use the internet as an escape from the “real world”, and naturally, want the internet to be a safer space than the world around them. So they put trigger and content warnings on distressing media, because they know that people with PTSD also view the same content. However, with the rise in internet users, there’s also been a push to extreme liberal views, to the extent that internet users demand trigger warnings on things that aren’t conventionally triggering. But that’s not plausible, as the people who exist in the real world are the same people who are on the internet. And as we all know, people don’t come with trigger warnings in the real world. The internet is also a gigantic platform, and it is next to impossible to be aware of every single user’s trigger and accommodate them.
Researchers have also found that trigger warnings do more harm than good. One of the most common coping mechanisms of people with PTSD is avoidance, where-in they avoid everything that has to do with their trauma. By extensively using trigger warnings on everything, it is enabling this behaviour, and allows them to live in their own cozy cocoon. This sounds appealing enough, but at the end of the day, they never face their trauma, and can ultimately never move on from it. The more one avoids something, the more that avoidant behavior is reinforced, and the worse the problem gets. It can cause a dislike to become a fear, and that fear can very well become a phobia.
Another harmful result of overusing trigger warnings is that it causes viewers who suffer from PTSD, etc, to look at their trauma as their central identity. This happens to the point that they see themselves only as an embodiment of their trauma, instead of an actual person. Trauma is relative, and even those who face the same trauma cope with it differently. A few constantly think about their trauma, while others struggle with it less frequently. A lot of these people are in the process of recovery, and are learning how to control what they think about. Using trigger warnings extensively reminds them of their trauma and pushes back their recovery. Some people on the internet enable the concept of glorifying trauma to ridiculous lengths, through both the trigger warnings, and by infantilizing those who have undergone trauma. There is a difference between treating people suffering from PTSD with compassion, and comparing them to children who are unable to live independently.
Trauma is relative, some people’s thoughts are constantly preoccupied with their trauma, and others not. Some are in the process of recovery and are learning how to control what they think about. In a way, by over-using a trigger warning, one is almost indirectly reminding them of their trauma, and also indirectly coddling them. This pushes back recovery.
The central problem with the warnings, however, is that while they warn the viewers that disturbing content exists within the media, it does not reduce the impact that the actual disturbing content has on the viewer. People with PTSD cannot control their intrusion symptoms without therapy, and cannot brace themselves against those symptoms regardless of whether there was a trigger warning prior to the content or not.
One incredibly effective way to deal with PTSD is exposure therapy, which is the complete opposite of the message that slapping a trigger warning on everything sends. Exposure therapy is a form of psychological treatment that involves exposing the target patient to the anxiety source or it’s context, in order to allow the patient to normalise it for themselves. Several studies have found that 60-90% of patients who have undergone exposure therapy have reported either significant or moderate relief from their symptoms.
⚠️ Goofy Trigger or Actual Trigger?
Unfortunately, trigger warnings are slowly becoming more of a joke on the internet. What was once created to accommodate PTSD symptoms has now become synonymous with ‘offensive content’, which trivializes those with genuine trauma. People have unironically asked for trigger warnings on content with milk products as it may be "offensive" to lactose intolerant people. They use trigger warnings for misogyny, menstruation, insects, and even skinny people! This is problematic, to say the least. None of these even require trigger warnings! The internet has taken something as serious as a trigger and a person’s trauma and turned it into a complete and utter joke.
When we look at trigger warnings, we associate them with problematic things, like child abuse. It’s pretty much conditioned in our brains. But then when we look at, for example, ‘TW- Food’, our brains connect the dots and deem food as problematic. When people who struggle with eating disorders see that, it’s reinforced in them that food is triggering and a bad thing, and it makes recovery for them that much harder. Moreover, in the real world, a McDonald's billboard advertisement doesn't come with a trigger warning for those who find food "triggering". People struggling with their body image need to understand that, due to societal standards, the modelling and fashion industry will choose skinny people to model for them. Now, although the industry is slowly changing, being thin is still the norm. We also cannot ignore the fact that naturally skinny people exist, and their mere existence absolutely should not be something that is ‘triggering’ .
Of course, certain content such as graphic depictions of violence, sexual assault, child and animal abuse, self-injury and suicide mandatorily require a trigger and/or content warning, as they warn people with PTSD from viewing and/or reliving their own trauma in a way, and also warn other people who may not be in the right headspace to view such content.
Another crucial trigger warning that most of us may have seen is the warning for flashing lights. Flashing lights can trigger seizures in people who have epilepsy. While this is not a trauma induced trigger, it’s caused by a medical condition, and can lead to those with epilepsy to have life-threatening seizures.
Triggers are definitely real, and undoubtedly should be accommodated as much as possible. But when one is on a platform that’s as big as the internet, it becomes each person’s responsibility to make sure that they don’t harm themselves by triggering their PTSD. While therapy is definitely the best option to treat PTSD and trauma, it’s not possible for everyone affected by it to afford therapy for various reasons. So it’s better to avoid triggering things on the internet. However, it is simply not possible for the internet nor the millions of users on it to cater to everybody’s trauma. In the real world, the number of people one interacts with is relatively fewer, and people would be willing to accommodate one’s trauma. On the internet, which has almost 5 billion users, there is absolutely no way for every individual’s trauma to be accounted for. Treating everyone with compassion is a must, but curbing half of the internet’s content with trigger warnings is messy, and makes people lose focus of why it started in the first place.
So, are you triggered yet?
Some references used by the authors.
youtube
youtube
13 notes
·
View notes
Text
What is 3 stage therapy?
You may often hear people talk about 3 stage or 3 phase therapy.
Maybe you’ve heard someone say “I’ve been doing a lot of stage 2 work in therapy lately”.
This refers to “ PHASE-ORIENTED TREATMENT APPROACH “ as laid out in the ISSTD treatment guide.
This is a guide that therapists follow for the treatment of DID/OSDD.
*This post is very long, but I have tried to break it into sections to make it easier.*
The guide states:
“ Over the past two decades, the consensus of experts is that complex trauma-related disorders—including DID—are most appropriately treated in sequenced stages. “
This has been advocated for since at least the late 19th century.
“ The most common structure across the field consists of three phases or stages:
1. Establishing safety, stabilization, and symptom reduction;
2. Confronting, working through, and integrating traumatic memories; and
3. Identity integration and rehabilitation. “
This roughly means that phase 1 work relates to your “general” therapy. Helping you get our ducks in a row, ready to begin stage 2.
Stage 2 is about addressing the trauma you’ve experienced. This is tough and emotionally gruelling work, and it is highly recommended that you do not attempt this type of work without a trained and trusted mental health professional.
Stage 3 is about “integration” - this does not necessarily mean fusing the identities into one state of self. It can simply refer to developing a healthy and cooperative harmony between a person’s identities/alters.
“In addition to PTSD symptoms, persons with complex PTSD have major difficulties with dissociation, affect regulation, body image distortions, self-injury, chronic suicidality, and somatization. They may have substantial relational pathologies, including problems with trust and revictimization in violent or abusive relationships. They often view the world as dangerous and traumatizing and tend to see themselves as shameful, damaged, and responsible for their own abuse.”
Now what does this hefty paragraph mean?
Well, in layman’s terms it means “we’re fucked up bro”.
If you have childhood trauma and/or PTSD, in addition to the PTSD symptoms a person with DID/OSDD will likely have some/many of the following issues:
- dissociate
- have unstable emotional or logic states
- have an incorrect view of their physical appearance (including dysmorphia, dysphoria, anorexia)
- self harm
- suicidal ideation (that is: wanting to die, or fantasising about killing oneself)
- comorbid disorders
- trust issues
- revictimization (that is: putting yourself intentionally or unintentionally into abusive situations, particularly abusive relationships)
- chronic shame
and
- a deep “need” to blame themselves for what happened to them.
These are all issues which need to be addressed in therapy.
Sometimes you may need a network of health professionals to help you heal. These could include a General Practitioner (Doctor), psychotherapist, trauma specialist, a specialist in sexual disorders, a nutritionist, psychiatrist, speech therapist, behavioural therapist, and more.
It is important that any of your treating health professionals work together towards your best interests, and that you can trust them.
“ Treatment for complex PTSD resembles that of DID in that it is often of longer duration, is multimodal and relatively eclectic, and is designed to address the multitude of clinical difficulties with which these patients struggle. “
This means that the treatment for PTSD and the treatment for DID/OSDD will be similar, and will take place over a long time period.
The frequency of your sessions is between you and your treating health professional/s, but you shouldn’t expect to see a miracle overnight.
For many it takes years of therapy before they even start stage 2 work.
It’s not a race, you can’t rush it, and there is no reason to compare your healing journey to others’.
“ Phase 1: Establishing Safety, Stabilization, and Symptom Reduction
In the initial phase of treatment, emphasis should be placed on establishing a therapeutic alliance, educating patients about diagnosis and symptoms, and explaining the process of treatment. The goals of Phase 1 treatment include maintaining personal safety, controlling symptoms, modulating affect, building stress tolerance, enhancing basic life functioning, and building or improving relational capacities “
Phase one will start your healing journey at whatever pace is right for you, and will lay the foundation for phase two work.
This is important because in phase two work, you may become overwhelmed, and you will need to rely on the skills you developed in phase one, as well as relying at times on the trust you’ve built with your therapist.
“ Phase 2: Confronting, Working Through, and Integrating Traumatic Memories
In this phase of treatment, the focus turns to working with the DID patient’s memories of traumatic experiences. Effective work in this phase involves remembering, tolerating, processing, and integrating overwhelming past events. This work includes the process of abreaction—the release of strong emotions in connection with an experience or perception (usually a past experience or perceptions of a past experience) “
Phase two is about facing the ghosts of your past, under the guidance of your trusted therapist. It will be hard, and it may even feel like it’s too much and you can’t do it.
If you are feeling like you can’t handle it, you MUST tell your therapist.
You should never push through without letting your therapist know how you are feeling. Your therapist will help you assess what changes need to be made so that you can continue getting the most out of therapy.
Some common changes are:
- extending the length of a therapy session, to include a cool-down or recovery period
- strengthening coping mechanisms which may not be “strong” enough
- changing the frequency of sessions
“ Phase 3: Integration and Rehabilitation
In Phase 3 of DID treatment, patients make additional gains in internal cooperation, coordinated functioning, and integration. They usually begin to achieve a more solid and stable sense of self and sense of how they relate to others and to the outside world. In this phase, DID patients may continue to fuse alternate identities and improve their functioning. They may also need to revisit their trauma history from a more unified perspective. “
Phase three is the phase where you will really have to decide whether to “
fuse
” all alters, or whether you want
“functional multiplicity”
.
The guidelines allow for both of these options, so don’t be scared that your therapist will try to force one or the other.
There is also no judgement about which one you choose - it’s about what is right for you (/your system).
In phase three you will tighten up the skills you already learnt, and possibly relearn them from a new perspective.
Some alters may not have learnt or mastered the therapy skills that other alters have, which means these skills may need to be learnt again.
If some or all of your alters decide to “fuse”, the resulting identity/identities may need to relearn some of these skills as well.
* All quotes taken from: https://www.isst-d.org/wp-content/uploads/2019/02/GUIDELINES_REVISED2011.pdf *
If you would like a more detailed look at what each phase may contain, please visit:
Stage one work: www.dis-sos.com/trauma-therapy-stabilization/
Stage two work: www.dis-sos.com/trauma-work/
4 notes
·
View notes
Text
NEWS IN BRIEF
ECONOMICS
EDUCATION
ENVIRONMENT
SOCIAL JUSTICE
FEATURES & INVESTIGATIONS
IDEAS
AUDIO
ABOUT
IMPACT
CONTACT
PITCHING
CAREERS
PARTNERSHIPS
TERMS OF USE
PLATFORM PRIVACY
PRIVACY SETTINGS
HOME
SOCIAL JUSTICE
THE MANY HEALTH BENEFITS OF METH
In low, pharmaceutical-grade doses, methamphetamine may actually repair and protect the brain in certain circumstances. But stigma against the drug could be harming patients and holding back research.
TROY FARAHMAY 15, 2019
D-methamphetamine is what generally appears on the street—although it's often cut with other chemicals—whereas l-meth provides a less addictive, shorter-lived high that is less desirable among drug users.
(Photo: Fiona Goodall/Getty Images)
Ask your doctor about methamphetamine. It's not a phrase you'll ever hear on TV or the radio, but here's a secret: Meth is an incredible medicine. Even the Drug Enforcement Administration admits it, and doctors are known to prescribe it for narcolepsy, obesity, and ADHD. Historically, meth has been used to reverse barbiturate overdoses and even raise blood pressure during surgery. Some preliminary research suggests that meth can be neuroprotective against stroke and traumatic brain injury, even stimulating the growth of brain cells.
Yet we're constantly warned never to try meth—"not even once," goes the refrain—or it will instantly cause addiction and ruin your life. Before fentanyl was the demon drug du jour, meth was seen as the worst, most destructive, most evil chemical you could find on the streets. Even of late, if you ask the New York Times or NBC, you'll learn that meth, "the forgotten killer," is back with a "vengeance." Other outlets, from Rolling Stone to CNN to The Daily Beast, have raised the alarm about meth use in the context of the opioid overdose crisis.
Stimulant-related deaths are indeed on the rise in North America—in some regions, meth is even more prevalent than heroin. Surveying drug overdoses in America from 1979 through 2016, researchers wrote in Science in September of 2018 that "Methamphetamine deaths have increased most dramatically in the western and southwestern United States."
Meth poisonings accounted for an estimated 14,845 hospitalizations in 2015, according to the Centers for Disease Control and Prevention (CDC), and another 15,808 emergency room visits. In 2016, around 7,500 people died from overdosing on stimulants, including meth. If you ask most people, including policymakers, you'll hear that meth is a scourge that can do no good.
But if you've ever used something like Vicks VapoInhaler, you've experienced the healing benefits of meth firsthand. That's because the over-the-counter nasal decongestant contains levomethamphetamine, the levorotary form—or "mirror image"—of the same stuff from Breaking Bad. Procter & Gamble tries to obscure this fact by spelling the active ingredient "levmetamfetamine." Selegiline, a drug for treating Parkinson's and Alzheimer's diseases, also metabolizes into levomethamphetamine.
There is a significant difference between these two opposing molecules. D-methamphetamine is what generally appears on the street—although it's often cut with other chemicals—whereas l-meth provides a less addictive, shorter-lived high that is less desirable among drug users. But people can and do use it recreationally. Abuse is rare, however, in part because the high is shitty, but also because d-meth is so widely available. It's easier to buy a more powerful form of the drug on the street than it is to try to extract it from over-the-counter medications.
Other Americans are prescribed actual, pure meth by their doctors. It happens less frequently these days, but in ADHD, obesity, or narcolepsy cases where nothing else has worked, a drug called Desoxyn (methamphetamine hydrochloride) can sometimes help. It can even be prescribed to children as young as seven.
It's important to make these distinctions. Meth didn't make a "comeback"; it never left. It can't return with a "vengeance" and it can't be "evil" because we're talking about a chemical compound here. It has no personality, no feelings, no intentions.
Thus it does a disservice to science and to medicine, as well as to the people who use these drugs responsibly, to treat a molecule with dualistic properties purely as a poison. And as recent research has shown, we're still uncovering some of the potential therapeutic benefits of methamphetamine. Confronting the stigma associated with meth and highlighting its benefits can better inform drug policy and addiction treatment.
(Photo: HO/Royal Thai Navy/AFP/Getty Images)
'IT'S JUST A STIMULANT, LIKE ANY OTHER STIMULANT'
For Jordan*, the meth he's prescribed works better against his ADHD with fewer side effects than the Adderall he'd been on for 20 years. About five years ago, Jordan asked his doctor if he could try methamphetamine. The doc said sure.
"The first time I brought it to the pharmacy, the pharmacist actually said to me, 'Oh, your doctor wrote this prescription wrong, this is the stuff that they make in meth labs,'" Jordan tells me by phone. "I told him to type 'Desoxyn' into the computer, and he did. He kind of backtracked, [but] he obviously had no idea."
Jordan, a middle-aged man from North Carolina who works in clinical research, now switches every three months between Adderall and Desoxyn to prevent building a tolerance to either stimulant.
Methamphetamine and amphetamine (one of the active ingredients in Adderall) are almost identical chemicals. The main difference between the two is the addition of a second methyl group to methamphetamine's chemical structure. This addition makes meth more lipid-soluble, allowing for easier access across the blood-brain barrier. Meth is therefore not only more potent, but also longer-lasting.
"The medications have definitely been important for me, to be productive, to be successful, not just at work but also in my personal life," Jordan says. "I've been on the medications for years, but I can take Adderall or methamphetamine and take a nap afterwards. I don't have any noticeable side effects."
Jordan also doesn't feel "high" from the doses he takes—approximately 10 to 15 milligrams of meth per day. Doses at this level are well tolerated by most people. It's very difficult to estimate the typical dosages of illicit meth taken on the street, but they are generally many times higher and taken every couple of hours. Further, the route of administration—typically, users smoke or inject illicit meth—allows for more of the drug to enter the bloodstream than taking a prescription pill.
At high doses, meth gives a rush of euphoria, boosting attention span, zapping fatigue, and decreasing appetite. Intense sexual arousal, talkativeness, and rapid thought patterns are also common. Body temperature and heart rate shoot up, which can cause irregular heartbeat, increasing the risk of seizures. If taken repeatedly over long periods, street meth can be highly neurotoxic, inducing paranoia and psychosis.
But illicit meth is also often used to self-medicate, according to Mark Willenbring, an addiction psychiatrist from St. Paul, Minnesota, with over 30 years of practice treating substance-use disorders. In Willenbring's experience, most of his patients who use illegal meth are treating undiagnosed ADHD.
"There's a high degree of comorbidity between substance-use disorders and ADD," Willenbring says. "They used meth for years in a controlled way, they never over-used it, they just used enough to get an effect, and then they stopped. One misconception is that it's always very addictive."
With most people who are addicted to meth, Willenbring says, you can't tell it just by looking at them. Carl Hart, a neuroscientist in Columbia University's Department of Psychology, agrees that the image of a snarling meth addict with bad teeth is a false stereotype. The dental damage so prevalent in anti-drug propaganda, he says, is more likely due to poor nutrition and lack of sleep—not to the drug. "There is no empirical evidence to support the claim that methamphetamine causes physical deformities," Hart wrote in a 2014 co-authored report.
"It's just a stimulant, like any other stimulant," Willenbring says. "It's a marketing issue."
Part of the reason Jordan asked to try Desoxyn in the first place was to see if he'd develop any of the "stereotypical meth addict problems," as he puts it. He hasn't.
"Those of us that know the reality have a responsibility to say, 'Hey, not that shooting up meth isn't bad, but the chemical itself isn't bad,'" Jordan says. "It's just misuse of the chemical that's bad."
For Joan*, a 66-year-old grandmother living off the grid in northern Georgia, Desoxyn makes her feel normal. "Not high, not hyped up, just normal," she tells me. She's been taking prescription meth since 2006, but first tried many other ADHD meds, such as Ritalin and Concerta, with poor results. But Desoxyn has not only helped her socialize, manage bills, and finish her master's degree in social work; it's also helped with Joan's depression and self-esteem.
"The only downside is the cost," she says. "It's one of the oldest drugs on the market, but even generic, it is outrageously expensive."
Still, meth isn't for everyone, of course. Kevin*, a 31-year-old artist from the Midwest, was first prescribed Desoxyn at age 15 to treat extreme fatigue and trouble focusing. But misdiagnosed mental-health issues—his doctors thought he had bipolar disorder, when in fact he had post-traumatic stress from childhood abuse—led to worsening symptoms.
"Being able to just take a bunch of pills that made the exhaustion go away for a while felt like a blessing, but it was just a Band-Aid on the problem," Kevin says. "I became completely dependent upon Desoxyn to function, and any lapse in taking my dose would result in a terrible energy crash."
"In retrospect, my neurologist at the time would have done well to consider the effects of intense stimulants on someone already prone to mania, insomnia, and hallucinations," he says. "I think Desoxyn has its merits as part of a treatment plan for attentive disorders, but that's the thing—it needs to be part of a larger understanding of how and why it might have a negative impact upon the patient's overall health, and should remain closely monitored throughout."
"Stigma is the lens [through] which we see all drug issues. It keeps us from making the best decisions. It is fear-based, not rational, not creative. Because of stigma, we have not fully addressed the opioid crisis."
(Photo: Guillermo Arias/AFP/Getty Images)
HOW METH CAN TREAT BRAIN INJURY—AND MUCH MORE
Street doses of meth can be extremely damaging to your health. The purity of such drugs is often unknown, and repeated, high doses of meth have been proven to be neurotoxic. But in low, pharmaceutical-grade doses, meth may actually repair and protect the brain in certain circumstances.
This was first discovered in 2008, when researchers at Queen's Medical Center Neuroscience Institute in Honolulu, Hawaii, analyzed five years of data on traumatic head injuries. They unexpectedly found that patients who tested positive for methamphetamine were significantly less likely to die from the injuries. The authors suggested that meth could have neuroprotective benefits.
To learn more, in 2011, a different team from the University of Montana applied meth to slices of rat brain that had been damaged to resemble the brains of stroke victims. Then they induced strokes in living rats, using a method called embolic MCAO, and injected them with methamphetamine. At low doses, the meth gave better behavioral outcomes and even reduced brain-cell death. At high doses, the meth made outcomes worse.
Because meth stimulates the flow of important neurotransmitters—dopamine, serotonin, and norepinephrine—the Montana researchers theorized that methamphetamine may provide neuroprotection through multiple pathways. David Poulsen, one of the researchers involved, says this was a "serendipitous discovery."
"So we decided, well, if it worked in stroke, it's probably going to work really well in traumatic brain injury," says Poulsen, now a neurosurgeon at the University of Buffalo who specializes in treatments for protecting the brain after severe damage.
Traumatic brain injury, or TBI, occurs after a violent smash to the skull. Its consequences include concussions on the mild end and coma or death on the severe end. TBI kills around 50,000 Americans annually, according to the CDC, while about 2.8 million of us visit the emergency room for TBI-related injuries every year. There is currently no Food and Drug Administration-approved treatment for TBI.
So, Paulson and his team reasoned, if meth can already be prescribed for children, why not to adults with TBI?
To test the proposition, Poulsen and colleagues gave TBI to rats. Giving an animal brain trauma isn't easy, but for more than two decades, there's been a trick called the rat lateral fluid percussion injury model: Simply cut a hole in the skull of a rat and apply water pressure to the brain.
About half the rodents—19 male Wistar rats—were given this treatment, and eight of these were then given meth. The rats given meth performed better at a task called the Morris water maze, a widely used experiment that involves plopping a rat into a pool of water with a hidden platform. By tracking how long it takes the rodent to find the platform, scientists can measure many different aspects of cognitive function.
"By the third day of training, there were no statistically significant differences between the uninjured control rats and the injured rats that had been treated with methamphetamine," Poulsen and his colleagues wrote.
But the team also found that low doses of meth were protecting immature neurons, while also promoting the birth of new brain cells that are important for learning and memory. The same was also true for rats that were given meth, but not injured.
"We see not just little, but very significant improvements in cognition and behavior," Poulsen says. "Their memories improved, functional behavior is improved.... It's not a trivial difference."
"In light of the fact that low-dose methamphetamine is FDA-approved for use in juveniles and adults, we see no valid reason why it cannot be utilized in human clinical trials for stroke and TBI," Poulsen and colleagues concluded in 2016.
But those clinical trials, considered the gold standard for testing medication, have yet to materialize, even while a 2018 retrospective study found similar results to the Hawaiian neuroscience report: Out of 304 patients with TBI, those who also tested positive for meth had better recovery results than those who did not. "The potential neuroprotective role of meth and other similar substances cannot be ignored," the authors wrote in Clinical Neurology and Neurosurgery last July.
There are limited conclusions that we can draw about these rodent and retrospective studies, and it's probably unlikely that nurses will soon start giving meth to people who have cracked their skulls. Still, a wide variety of stimulant therapies for TBI is being explored, with positive results. These include trials with modafinil, a narcolepsy drug; amantadine, a Parkinson's drug; and dextroamphetamine, one of the components of Adderall. But there's still no indication of a single clinical trial for methamphetamine for TBI registered with the National Institutes of Health.
Methylphenidate, also known as Ritalin, seems to be the stimulant most popular in these trials. For example, in 2004, researchers at Drucker Brain Injury Center at MossRehab Hospital in Pennsylvania gave methylphenidate, better known as Ritalin, to 34 patients with moderate to severe TBI. They reported significant improvements in information processing and attention.
Twelve years later, in Gothenburg, Sweden, another 30 patients suffering from prolonged fatigue following TBI were given methylphenidate and observed for six months. They also showed improved cognitive function and reduced fatigue. But a 2016 meta-analysis of 10 controlled trials found the main benefit of giving methylphenidate for TBI was increased attention, "whereas no notable benefit was observed in the facilitation of memory or processing speed," the authors wrote. They encouraged more research into appropriate dosages and length of prescription.
Birgitta Johansson, a neuroscientist at the University of Gothenburg and lead author of the Swedish study, suggests caution whenever treating someone with a brain injury. "With methylphenidate, it is important to be aware about possible side effects, [such] as increased blood pressure and heart rate and also risk of anxiety," she says. "It is always very important to prescribe medication with care and follow the patient carefully."
But the reason meth isn't studied more rigorously—for TBI, for Alzheimer's and Parkinson's, for stroke—could also come down to money. Methamphetamine is off-patent, meaning there may be less financial incentive for pharmaceutical companies to explore the drug's potential uses. Consider Vyvanse, a drug first marketed in 2007, with a new formulation introduced in 2017, that racked up $2.1 billion in sales in 2017. Desoxyn, which is sold by three companies, only earned about $9.3 million in 2009.
While Methamphetamine may not be widely recognized as medicine, it clearly has potential to heal as well as harm. Recognizing the duality of meth is arguably all the more essential in the face of a rising stimulant overdose crisis.
"Stigma regarding any substance use or substance use disorder is counterproductive," says Dan Ciccarone, professor of family medicine at the University of California–San Francisco. He says the overdose crisis is shifting from opioids to stimulants and that we are not prepared for the next wave. "Stigma is the lens [through] which we see all drug issues. It keeps us from making the best decisions. It is fear-based, not rational, not creative. Because of stigma, we have not fully addressed the opioid crisis."
That stigma remains a major hurdle, and until doctors and public-health officials counteract this kind of messaging, it seems unlikely that a multinational pharmaceutical company would risk marketing a substance only believed to be toxic and deadly.
"Everything will kill you, if you take enough of it," Poulsen says. "Some things don't require a lot to do that. Meth is one of those things. But just like any drug, the difference between a poison and a cure is the dose."
*These names have been changed.
TAGSALZHEIMER'SADDERALLTRAUMATIC BRAIN INJURIESFEATURES & INVESTIGATIONSMETHAMPHETAMINEMETHTOPIC: HEALTH CARE
BY TROY FARAH
Troy Farah is an independent journalist and photographer in California. His reporting on science, health, and narcotics has appeared in Wired, Ars Technica, Smithsonian, Discover, Vice, and elsewhere. He co-hosts the drug policy podcast Narcotica.
ENVIRONMENT
STARRY, STARRY SKIES
California desert town takes back the night, wins rare "Dark Sky" award
SOCIAL JUSTICE
WHAT IS THE FUTURE OF PAID PARENTAL LEAVE IN AMERICA?
The U.S. has a rough track record with how it treats new parents, but there are reasons to believe that this could soon be a thing of the past.
NEWS IN BRIEF
THESE MAPS SHOW WHAT GRAHAM-CASSIDY WOULD MEAN FOR YOUR STATE
A new report concludes that the Graham-Cassidy proposal would reduce federal funding to states by $215 billion by 2026.
SOCIAL JUSTICE
THE FAULT IN OUR STAR NAMES
The International Astronomical Union has established a committee to finalize a list of official star names. Some companies offer unofficial naming rights for purchase. But the voices of certain communities are often left behind.
ENVIRONMENT
HOW MUCH CAN DIETARY CHANGES AND FOOD PRODUCTION PRACTICES HELP MITIGATE CLIMATE CHANGE?
Food policy experts weigh in on the possibilities of individual diet choices and sustainable production methods.
UNSEEN AMERICA
LAS MANOS JÓVENES QUE NOS ALIMENTAN
Se calcula que 524,000 niños trabajan inimaginables largas horas en los agotadores campos agrícolas de Estados Unidos, y todo es perfectamente legal.
About
Impact
Contact
Pitching
Careers
Partnerships
Terms of Use
Platform Privacy
© 2021 Grist
3 notes
·
View notes
Note
(?) i keep self triggering nonstop i cant help it. i purposely search for nasty things related to my trauma just so i can feel bad. how do i stop it i cant stop i hate it
We have some information you might find helpful, because my friend you can stop harming yourself, you can heal. You are a person worthy of health and healing.
Triggering oneself is a form of self-harm it can help to look at it that way when breaking down what you are trying to get out of it on the level of dysregulation and seeking to deal with it on a somatic level as well as bringing judgment from the situation.
Coping Skills: Combating Self-Harm Urges
Self-harm urges can be so strong and are very hard to deal with, but we can work against them to better-coping skills.
Self-harm, self-mutilation or self-injury comes in multiple forms not just cutting that is normally discussed. Examples include compulsive masturbation, burning, hitting yourself against things, excessive scratching to the point of drawing blood, punching self or objects, infecting oneself, inserting objects into body openings, drinking something harmful and breaking bones purposefully.
These skills also work for self-triggering behaviours doing actions that cause yourself severe emotional distress like flashbacks or panic attacks.
Here is some advice to start finding safer coping skills:
The first step is to look at what is pushing you to self-harm.
Look at:
What things tend to happen before you do the behaviour? Are their common external triggers?
what emotional state are you in before you trigger yourself? For example are you angry, empty, keyed up, anxious? Do you feel like you need a realise? Are you experiencing intrusive thoughts?
What physical sensation are you experiencing beforehand? Are you holding tension anywhere particular? Are you in physical pain? Are you already experiencing body memories?
What emotions are you feeling afterwards? Do you feel less empty? After the panic subsides are you actually calmer?
What physical sensation do you have afterwards?
Okay, now you can look for replacement actions that can handle the feelings without triggering yourself.
knowing outside triggers can help you avoid them if possible, and prepare for them ahead of time if that’s not possible.
If you recognize the emotional state the persists the actions you can try and work on bringing yourself down from this state first. Learn about coping skills to handle this feeling. (Coping skill suggestions: Anger, anxiety/stress 1 and 2, intrusive thoughts)
If you are feeling specific body sensations beforehand look at ways to help that. For muscle stress this might help, heating pads or light stretching might help. If you have a headache ice pack might help. If you are already having body memories this or this might help.
Now sometimes the emotion you are getting after the triggering is just as important as the emotion that was before. Now here you can look for a replacement action that brings you a similar emotional feeling that isn’t as harmful. This post gives some examples of replacement skills for self-harm. If something you find is you are looking to break an emotional blank, or you feel more “real” afterwards I could suggest finding emotional things (music, movies, books) that can still bring strong emotions.
If you have physical sensations you are seeking again it is good to find a replacement action. Sensory aids might help info about that here.
Three important things to consider for long-term recovery
Deeper things are always at play. Underlying mental health conditions (Like BPD, PTSD or Depression) and trauma. Working through these problems, often a professional can be helpful reaching out to them is important.
Reaching out to friends and family can be really helpful in keeping yourself safe. Which is of the utmost importance.
If you find yourself harming yourself greatly please look at our crisis resources.
[WordPress Link]
Intrusive thoughts are often present here and dealing with them can combat the urges you have to self-harm as it can help mitigate the severity of the urges and thought spirals involved.
Coping Skills: Dealing with Intrusive Thoughts
Intrusive thoughts are unwanted thoughts that intrude into the thoughts process of those who deal with them. They are commonly associated with OCD, PTSD, eating disorders, addiction and self-harm.
Intrusive thoughts are not just thoughts that seem random or unskilled (that called thinking), and they aren’t always accompanied by the urge do something (compulsions). They can extremely distressing thoughts, violent, sexual or panic-inducing ideas and images are really common manifestations.
We dealing with intrusive thoughts an important first step is to understand while these thoughts are in your brain they don’t represent desires for the thoughts to happen or that it’s your real secret morality. It’s a function of what you are struggling with (mental illness, trauma and stress) not you being a bad person. Reminding yourself of that combats shame and paralyzation of feeling helpless to act.
next is letting them be. Intrusive thoughts happen, rumination, berating yourself for having them, or aggressively trying to push them away are all not helpful. Learning to just let them come into your brain and leave without a huge shift in behaviour and mood is important. Doing this robs them of their emotional power and lessens the pain. It’s okay to have them, It’s okay that they hurt you, letting these thoughts go is fine and healthy.
You don’t owe it all of your energy to trying to work them out, make thoughts stop happening, or repressing the emotions till it hurts more.
This just takes practice when experiencing them letting yourself know its just a thought, not real or something you must act on. When you feel the emotions and stress from the thought take a deep calm breath. Do your best to steady your emotional/physical response. When you can’t distract or not panic that’s fine, don’t get angry just try again next time.
Another important thing to remember is to not modify your whole life around intrusive thoughts. Avoidance is, of course, something people with PTSD and anxiety suffer with in general, but it’s key to start working your life around what you want and not avoiding intrusive thoughts. Starting with small things that might be ignored because of the thoughts not linked to large trauma, This is an important step to remove the power of the thoughts.
If your thoughts are often based on catastrophizing logic talk might actually help. Intrusive thoughts about say natural disasters thinking about how unlikely something is to happen so not number one priority might help, remind your self “it is valid to worry but maybe not so much right this second.”
Distraction isn’t always bad, many intrusive thoughts can be let go but patterns sometimes do need to be addressed. If you have trauma-based intrusive thoughts healing from trauma is often key to making them better.
Be Blessed all
~Admin 2
[WordPress link]
So if it’s online porn you could turn of safe-search and block the sites. This can combat the easy patterns we get stuck into. It can have a withdrawal effect and don’t hate yourself for slipping up. When you feel the need try and chose another act. Distracting yourself with things that require a lot of brain space is often a good step.
If you need some kind of stimulation you could try using written erotica that doesn’t have the same possible damage on the people involved in the production. Because of the biological aspects of addiction sometimes if you cut “cold turkey” as it were can push to worse behaviour.
Another tool for compulsive actions is to put it off, don’t judge yourself to just stop any and all behaviour but extend the time as long as you can combine with replacement behaviours.
Due to the nature of sexual trauma, it can be really useful to breakdown the relationship to sex and how that is affecting you. Doing so can help work through triggers. Coping Skills: Healing A Relationship With Sex After Sexual Abuse
Our Coping Skills Masterpost might be useful in finding ways that help you deal with your trauma symptoms over time and reduce the regulation you automatically fall into.
It’s important to disconnect from behaviours that harm you, and depending on what you are engaging with harm others. Participating in these don’t make you inherently a bad person, it just means you are in a place of struggle and need to work towards healing.
Be Blessed,
-Admin 2
18 notes
·
View notes
Text
Duluth Personal Injury Legal Team
Hire A Duluth Medical Malpractice Attorney for Personal Injuries
Have you experienced an injury or the death of a loved one that you think was caused by the medical negligence of your hospital, surgeon, or doctor in Duluth? If so, you should consider pursuing a medical malpractice claim. Medical errors occur all the time in emergency rooms, surgeries, pharmacies, and medical labs. When these errors happen, they can have devastating repercussions such as death, life-changing injuries, and unending suffering for the victim and their family.
Kenneth S. Nugent, P.C is a Duluth medical malpractice law firm that has long-term experience. Contact or live chat with us, and we will ensure you receive the maximum compensation you deserve.
What Is Medical Malpractice and Should You Hire a Duluth Georgia Personal Injury Attorney?
Medical malpractice includes any mistake by hospital staff, nurses, doctors, lab personnel, pharmacists, and other medical professionals. Under Georgia law, health care professionals are required to use a reasonable degree of care and skill. However, sometimes, mistakes and careless actions occur. Every year, a substantial number of Americans die or suffer injuries from medical mistakes. The Institute of Medicine estimates that 98,000 patients die annually from medical negligence.
Kenneth S. Nugent, P.C.
4227 Pleasant Hill Rd #300, Duluth, GA 30096
(404) 875-0900
In addition to deaths caused, a larger number of patients suffer injuries. Serious misdiagnoses and medical mistakes cause life-threatening injuries that require extra treatment. This means time taken off from work to seek treatment and in the worst cases, the loss of life.
In some cases, medical malpractice is clear. For instance, when a surgeon operates on the wrong body part or a surgical item is left inside the body of a patient after surgery. However, in other cases, it is very difficult to prove that a medical error was made. Therefore, it is important to hire an experienced medical malpractice attorney to assess and handle your case. Our medical malpractice lawyers are experts in such cases. Besides, they can call upon reliable advice from other professionals whom they rely on to prove medical negligence.
Medical Malpractice Cases We Handle
Our lawyers at Kenneth S. Nugent, P.C. represent clients and families harmed by medical and nursing errors, hospital negligence, physician malpractice, nursing home abuse, lab mistakes, and doctor malpractice. Over the years, we have advocated for and protected the rights of patients and delivered successful claims for our clients.
We represent clients who have been injured or clients who have lost a loved one from errors, mistakes, and reckless conduct in hospitals, nursing homes, labs, etc. These are some of the medical malpractice cases we handle:
• Failure to diagnose, misdiagnosis, and failure to inform: Failure to identify a medical problem places the patient’s life at greater risk. Misdiagnosis occurs when a doctor fails to correctly identify and diagnose a medical problem, especially if another doctor with the same qualifications would have accurately identified the condition and commenced treatment.
• Surgical Errors: Surgery is always risky, a mistake can increase the risk and cause loss of life. Injuries after surgery happen when a surgeon or a surgical team member acts negligently or makes an error. Such mistakes can include operating on the wrong organ, surgical equipment left in the patient, blood transfusion errors, etc.
• Hospital Infections: Most common claims involve infections acquired in the hospital or after surgery due to the lack of a proper and timely diagnosis of post-surgical infection. Due to this lapse, the patient suffers from dangerous complications.
• Anesthesiologist, nurse, doctor, and other health care specialist errors: Anesthesia mistakes can cause brain injury, respiratory or cardiac arrest, vision loss, paralysis, and even death. Common anesthesiologist errors include improper intubation, transfusion errors, and anesthesia awareness - the patient regaining consciousness during surgery. Other health care specialist errors can cause catastrophic injuries or lead to the patient's death.
• Emergency room and hospital negligence: Doctors are required by the law and their code of conduct to adhere strictly to set out standards of care when examining, diagnosing, and treating patients. In the hospital or emergency room, doctors can breach the established protocols by failing to conduct proper diagnosis, refusing to order necessary imaging studies or tests, failing to consult appropriate specialists, etc.
• Nursing home neglect and abuse
• Medication errors: Medication errors can include administering contraindicated drugs to the patient, prescribing or administering the wrong drug, giving the wrong dose, or failure to medicate.
• Breach of established medical protocols
• Wrongful death
• Failure to adhere to advanced medical instructions and living wills
Do I Have a Valid Medical Malpractice Claim?
This question may be on your mind after your injury or the death of a loved one. Each case is unique due to the specific circumstances. This is why you should talk to our specialist medical malpractice lawyers at our firm as soon as possible. Assemble all your medical records, and put together all the key details, from your first visit to the doctor up to the last contact with your health facility. If you can, request for all your medical records from your hospital and bring them when meeting our attorney. Note that statute limitations govern how long one should take before filing a medical malpractice claim.
Once you contact Kenneth S. Nugent, P.C, our lawyers will assess and evaluate your claim. We focus on two essential elements to decide if your medical malpractice claim is valid.
The first is a failure to adhere to the necessary standard of care. Medical professionals are required to practice a certain degree of care based on the condition of the patient. Second, the presence of a direct link showing that the medical treatment provided or omitted led to the patient's injury or death. This relationship must be proved.
Demonstrating that standard care was breached and showing a direct link between the negligent act and the consequent injury or death is extremely hard. But, our firm has enough experts, including investigative and medical professionals who are experienced in doing this.
How Can I Strengthen My Case?
Though our medical experts and investigators at Kenneth S. Nugent, P.C will conduct their investigations, there are several measures you can take to ease your compensation claim case. First, during your medical examination, cooperate fully with our doctor and answer all questions comprehensively. Also, prepare a detailed medical history that specifies the hospitals and doctors who treated you or your deceased family member and hand over this information to our lawyers. If possible, provide a detailed timeline from your initial appointment with your physician up to now, highlighting the symptoms, and the treatment received up to date. Remember to maintain a record of your ongoing medical treatment.
Do I Have to File My Medical Malpractice Claim Now?
Typically, you are allowed a two years window from the time your injury occurred to file a suit. After that your claim is time-barred. However, there are some exceptions. For instance, if you are unaware of a surgical tool inside your body, then you are allowed one year from the discover date to file your claim. For minors, the statute of limitations is set at two years though it only begins to run once they attain the age of 7 years.
In Georgia, a statute of repose disallows one to file a medical claim case after five years from the incident that caused the injury. In the case of minors, the statute of repose only starts running after their tenth birthday.
Who is Responsible for My Medical Injuries?
When you visit a hospital or doctor you entrust them. Unfortunately, you were harmed. This means the professional or hospital did not exercise the applicable standard of care. Therefore, you are entitled to sue the hospital or doctor for your injury or the loss of a loved one. Their insurance company will pay your compensation. In these cases, several parties can be responsible. However, to sue a medical practitioner such as a doctor, anesthesiologist, nurse, or lab technician you must show beyond doubt that they did not adhere to the necessary standard of care.
To prove this is not that easy. Though the law expressly states that medical professionals must utilize a “reasonable degree of care and skill”, this is open to different interpretations. That is why it is important to engage our qualified lawyers who will consult medical experts to present strong evidence to clearly show that a medical professional was negligent and did not comply with the required standard of care.
In Duluth, any medical malpractice claim must have an expert witness's testimony substantiating that the care accorded to the victim was below reasonable standards of care. Our attorneys will assist in providing an expert witness to testify in your case. They will also put together all the necessary evidence to demonstrate negligence and hence liability.
Why You Should Hire Kenneth S. Nugent, P.C?
Our law firm is committed to advocating for the rights of our clients and reinstating victim families as a way of moving forward. There are several reasons why you should consider working with our medical malpractice lawyers:
Work with the best medical experts: Our medical malpractice lawyers are highly qualified specialists able to effectively anticipate and manage the sophisticated legal and medical problems that are found in these cases. Moreover, we have very useful relationships with qualified medical consultants who are crucial in arguing out any successful claim.
Highly experienced in the medical malpractice field: Kenneth S. Nugent, P.C has a combined experience of over 350 years in our team. Our attorneys have spent years representing clients and are familiar with the applicable special procedures and the local court system. By selecting us, you will be engaging a capable team of lawyers that will ensure a fair resolution of your claim.
Skilled in handling evasive insurance companies: The main objective of insurers is to make a profit. No insurance provider is readily willing to pay a claim. Denying claims is their default approach. Then they will attempt to reduce your claim as much as they can. They have persuasive claims adjusters who are paid to convince you to accept a lower claim. Our firm has experienced all their tactics and will negotiate strongly to get the maximum damages you deserve.
We cover your legal charges until your case is decided: Our firm understands your plight. Already, you may have spent substantial amounts in seeking additional treatments for your injury. To ease your burden, we cover all your legal expenses until your claim is decided.
Contact Our Duluth Medical Malpractice Lawyers
Do you have an injury from any medical treatment received? We are open and ready to advise you on whether a medical error happened and guide you on the next course of action. Contact us online or make a free call to 1-888-579-1790 and book an appointment with Kenneth S. Nugent, P.C., an experienced Duluth medical malpractice attorney firm. We have the resources, expertise, and experience to assess your claim and pursue your right to receive the full compensation you deserve.
1 note
·
View note
Text

txf ran for YEARS and is chock full of moments that our boi has been horrifically injured. this is mostly going to focus on physically lasting scars and prominent breaks that still cause him all those fun aches and pains, but will touch into whatever prominent injuries he’s experienced that i think are noteworthy, including those with notable trauma experienced. this should have all of them but i’m not perfect. 99% of these are timestamped with what episode it happened, some have screenshots, and like maybe 1 or 2 will be headcanon ones. the reason i’m posting is for the sake of plotting and also a little timeline for myself, to keep in mind / keep track of all the things he’s been through.
SCARRING .
1 . shot in the left thigh, straight through his femur (oof). thicc boi star - shaped scar. 1X13
2 . gash on lower rib - cage / abdomen, clawed by the “jersey devil.” minimal / thin scarring. 1X5
3 . moderate skin damage to face / below eyes and around cheekbones due to hypothermia exposure. it’s not terribly noticeable and only really lasts maybe less than a year and a half, normally most don’t see it unless he’s pointed it out since the damage was so close to his eyes. screenshot of how it looked when he entered the hospital . 2X16/17
4 . scully shot him in the shoulder :// give that boy another starry scar. 2X25
5 . deep slash on the face / upper right cheekbone from a gargoyle. he tends to receive a lot of scars on his temple / head and most of them remain thin and whiten over the years, but to someone close enough / knows what to look for, they’re there. screenshot . 3X14
6 . slammed his head against a windshield hard enough for the window to have some blood on it. was unconscious for a while after. screenshot 1 2 and 3 ( 3 is harder to see but it was stitched & bandaged ). 3X16
7 . shot in the head. didn’t die bc this boi is wild. screenshot . FTF
8 . probable damage to his neck ( small scars dotted across ) after an octopus - like creature strangled him and embedded parts of it in his neck. this is another sort of scarring that probably only lasted around a year, if that, and wasn’t noticeable all over. trypophobia warning on this image : screenshot . 6X13
9 . deep human bite marks on right forearm / closer to elbow, as well as part of his bicep. definitely prominent if not jagged scarring. bleeding was severe enough a tourniquet can be seen in the screencaps. screenshot of heavy bleeding and tourniquet. also his arm ass arm had a sling after the fact . 7X04
10 . ricocheting bullet hit upper left bicep. wrapped in heavy gauze , it’s probably a small minute scar. 7X06
11 . he got attacked by a bunch of snakes, so specific scarring is ??? questionable but they were poisonous and he did have to go to the hospital. 7X09
12 . had his skull drilled into at the edge of his hairline to induce his repressed memories. 4X23
13 . infestation of his lungs. he was basically suffocating due to the volume of eggs and beetles in his lungs and had to have them cleared after coughing up blood. it was hella violent. 7X18
14 . i don’t count fight club cuz that episode was BONKERS and there were so many things.
15 . of course, mul.der’s abduction. the scars for this fade away, but in the first couple of days that he’s returned and back on his feet, they’re still healing. i’ll detail more on this later.
16 . another temple gash ! photoset. 8X20
BROKEN BONES .
1 . obviously whenever he got shot through the femur . 1X13
2 . he got attacked by a gorilla ( don’t worry abt it this shit was wild im just putting it on here cuz like wtf y’know ) so i’m gonna wager potentially broken / fractured ribs / possibly some pretty bad bruising if not any breaks to his head. he was unconscious for a while and when scully found him he reacted wildly pained to her touch. also the only reason i’m adding this as well is because he’s definitely had a history of broken / fractured ribs. 2X18
3 . left pinky twisted and broken severely as a means of torture. 5X18
4 . in general he’s broken some ribs here and there. i also personally headcanon he broke his wrist when he was a kid, and it’s partly reason why this stooge drops his gun so fucken often, he’s got a lousy grip.
GENERAL / LONG TERM AFFLICTIONS .
1 . was infected with an alien gas that killed him, he FLAT - LINED for about a minute before scully revived him . 2X16/17
2 . he’s had a trillion concussions, which can only get worse as time goes on :///
3 . he’s also had unconventional medical procedures performed on him: mind - wiped in spooky unknown government labs, a lot of techniques and medicines to help him remember things via stimulating hallucinations that basically caused seizures, another time he was given medication that induced a seizure, drugged a few times that caused extremely high levels of paranoia and anxiety to very violent and uncontrollable levels.
4 . exposure to the black cancer, as well as torture / imprisonment without basic necessities which totally had some long-term mental effects. 4X8/9
5 . i mean he did get mummified by prehistoric fireflies but he’s cool now. 1X20
6 . he’s definitely got tinnitus from multiple stuff over the years but mostly from the gunshot to the head. FTF
7 . he almost died again, buried under rubble to narrowly avoid a massive explosion, severely feverish, dehydrated / heat exhaustion and unconscious for several days and BARELY fighting past the illness. 3X1
8 . subjects himself to tests from a doctor to inject him with ketamine ( a hallucinogenic anaesthetic ) to try and remember his past more clearly, causing seizures, severe migraines, and lapses in his current memory ( a vivid flashback occurs and he’ll wake up not knowing where he is ). also got his skull drilled into that was cool. 4X23
9 . moderate radiation burns to his forehead / face .
10 . oh yeah he drowned in the bermuda triangle but it’s cool his wife rescued him. 6X3
11 . he’s had hypothermia a lot in general.
MENTAL .
1 . take a shot everytime mulder gets tortured, die in 4 minutes .
2 . fear of fire is very pronounced. 1X12
3 . kidnapped, drugged, mind - wiped, dropped back to scully not knowing where he is. 1x2
4 . take a shot everytime he’s sleep deprived, whether bc of his own passion or because of someone forcing him to stay up. scully has made notes herself, verbally exclaiming mulder needs rest bc he hasn’t had any in 24 and sometimes 36+ hours.
5 . idk if i mentioned but he’s been held hostage a lot, more than once in some actual prison somewhere where he’s tortured, and a handful of times by dangerous criminals who are ready to kill him and do it for ransom.
6 . the amount of times he’s been detained and literally tied up or held down by something / physically restrained, i’d wager he’s less and less cool with it every time.
7 . almost was drowned inside of a mental hospital, drowned in the bermuda triangle, was almost drowned in a bath tub, and has been strangled more times than he’s comfortable with. the general concept of not being able breathe is a little too familiar.
8 . i just want to point out how many times he’s been exposed to seeing death / dead bodies / generally absolutely grotesque things , child death included . staring at severed appendages . has seen men literally chopped apart and left in trash containers . mentally he’s become very sound in a sort of formal way, in a way he can prioritize his work in an almost obsessive way to move past it all so it won’t catch up with him. he’s excellent at that mental compartmentalization. bleeding and dying, he is still looking for the truth. he’s seen many gruesome visuals and he notably has nightmares / terrors in the shows.
9 . that being said, he’s had some vivid nightmares since he was a kid.
10 . some ghosts psychoanalyzed the shit out of him and scully and made them think they shot one another, which has always been a fear of his since kitsunegari when he saw scully shoot herself in the head and how he almost shot her. he barely forgave himself for that. lots of hallucinations and fun stuff. 6X6
11 . extremely bad migraines that eventually formed into an unresponsive, violent state that put him in a mental hospital, where he paced around screaming, unable to form sentences. he harmed himself and others until he was medically forced into a catatonic state, while skinner and others tried to inject him with medicine to revert the state, resulting in seizures. he could also read minds during this period but nbd. a lot of this typically comes back up in 6X22/7X1/2
12 . got stuck in a simulated reality and drugged by an AI which would just kinda fuck with anyone. 5X11
13 . his abduction is an entire thing i won’t go into immediately here, but there was some very severe torture involved that stays with him for the rest of his life.
14 . his relationship with death is pretty fucked in general. he should’ve died so many times.
#I THINK this is all of iot#some of them are also repeated in s10/11 but i didn't add those refs#he doesn't have any severe injuries in those episodes so#.☄ ° ゜ as you claw the thin ice . ⇢ fact.#i hope you guys enjoy this cuz it took me a l l day
15 notes
·
View notes
Text
Medicine (definition)
This article is about the science of healing. For medicaments, see
medication
. For other uses, see
Medicine (disambiguation)
."Academic medicine" redirects here. For the journal, see
Academic Medicine (journal)
."Clinical medicine" redirects here. For the journal, see
Clinical Medicine (journal)
.Medicine
Statue of
Asclepius
, the
Greek god
of medicine, holding the symbolic
Rod of Asclepius
with its coiled
serpent
Specialist
Medical specialty
Glossary
Glossary of medicine
Medicine is the science and practice of establishing the diagnosis, prognosis, treatment, and prevention of disease. Medicine encompasses a variety of health care practices evolved to maintain and restore health by the prevention and treatment of illness. Contemporary medicine applies biomedical sciences, biomedical research, genetics, and medical technology to diagnose, treat, and prevent injury and disease, typically through pharmaceuticals or surgery, but also through therapies as diverse as psychotherapy, external splints and traction, medical devices, biologics, and ionizing radiation, amongst others.[1]
Medicine has been around for thousands of years, during most of which it was an art (an area of skill and knowledge) frequently having connections to the religious and philosophical beliefs of local culture. For example, a medicine man would apply herbs and say prayers for healing, or an ancient philosopher and physician would apply bloodletting according to the theories of humorism. In recent centuries, since the advent of modern science, most medicine has become a combination of art and science (both basic and applied, under the umbrella of medical science). While stitching technique for sutures is an art learned through practice, the knowledge of what happens at the cellular and molecular level in the tissues being stitched arises through science.
Prescientific forms of medicine are now known as traditional medicine and folk medicine, though they do not fall within the modern definition of “medicine” which is based in medical science. Traditional medicine and folk medicine remain commonly used with, or instead of, scientific medicine and are thus called alternative medicine (meaning “[something] other than medicine”, from Latin alter, “other”). For example, evidence on the effectiveness of acupuncture is "variable and inconsistent" for any condition,[2] but is generally safe when done by an appropriately trained practitioner.[3] In contrast, alternative treatments outside the bounds not just of scientific medicine, but also outside the bounds of safety and efficacy are termed quackery.
Contents
1Etymology
2Clinical practice
3Institutions
4Branches
5Education and legal controls
6Medical ethics
7History
8Quality, efficiency, and access
9Traditional medicine
10See also
11References
3.1Delivery
4.1Basic sciences
4.2Specialties
4.3Interdisciplinary fields
7.1Ancient world
7.2Middle Ages
7.3Modern
Quackery can encompass an array of practices and practitioners, irrespective of whether they are prescientific (traditional medicine and folk medicine) or modern pseudo-scientific, including chiropractic which rejects modern scientific germ theory of disease (instead believing without evidence that human diseases are caused by invisible subluxation of the bones, predominantly of the spine and less so of other bones), with just over half of chiropractors also rejecting the science of immunization.
Etymology[edit]
Medicine (UK: /ˈmɛdsɪn/ (listen), US: /ˈmɛdɪsɪn/ (listen)) is the science and practice of the diagnosis, prognosis, treatment, and prevention of disease.[4][5] The word "medicine" is derived from Latin medicus, meaning "a physician".[6][7]
Clinical practice[edit]
The Doctor
by
Sir Luke Fildes
(1891)
Medical availability and clinical practice varies across the world due to regional differences in culture and technology. Modern scientific medicine is highly developed in the Western world, while in developing countries such as parts of Africa or Asia, the population may rely more heavily on traditional medicine with limited evidence and efficacy and no required formal training for practitioners.[8] In the developed world, evidence-based medicine is not universally used in clinical practice; for example, a 2007 survey of literature reviews found that about 49% of the interventions lacked sufficient evidence to support either benefit or harm.[9]
In modern clinical practice, physicians personally assess patients in order to diagnose, prognose, treat, and prevent disease using clinical judgment. The doctor-patient relationship typically begins an interaction with an examination of the patient's medical history and medical record, followed by a medical interview[10] and a physical examination. Basic diagnostic medical devices (e.g. stethoscope, tongue depressor) are typically used. After examination for signs and interviewing for symptoms, the doctor may order medical tests (e.g. blood tests), take a biopsy, or prescribe pharmaceutical drugs or other therapies. Differential diagnosis methods help to rule out conditions based on the information provided. During the encounter, properly informing the patient of all relevant facts is an important part of the relationship and the development of trust. The medical encounter is then documented in the medical record, which is a legal document in many jurisdictions.[11] Follow-ups may be shorter but follow the same general procedure, and specialists follow a similar process. The diagnosis and treatment may take only a few minutes or a few weeks depending upon the complexity of the issue.
The components of the medical interview[10] and encounter are:
Chief complaint (CC): the reason for the current medical visit. These are the 'symptoms.' They are in the patient's own words and are recorded along with the duration of each one. Also called 'chief concern' or 'presenting complaint'.
History of present illness (HPI): the chronological order of events of symptoms and further clarification of each symptom. Distinguishable from history of previous illness, often called past medical history (PMH). Medical history comprises HPI and PMH.
Current activity: occupation, hobbies, what the patient actually does.
Medications (Rx): what drugs the patient takes including prescribed, over-the-counter, and home remedies, as well as alternative and herbal medicines/herbal remedies. Allergies are also recorded.
Past medical history (PMH/PMHx): concurrent medical problems, past hospitalizations and operations, injuries, past infectious diseases or vaccinations, history of known allergies.
Social history (SH): birthplace, residences, marital history, social and economic status, habits (including diet, medications, tobacco, alcohol).
Family history (FH): listing of diseases in the family that may impact the patient. A family tree is sometimes used.
Review of systems (ROS) or systems inquiry: a set of additional questions to ask, which may be missed on HPI: a general enquiry (have you noticed any weight loss, change in sleep quality, fevers, lumps and bumps? etc.), followed by questions on the body's main organ systems (heart, lungs, digestive tract, urinary tract, etc.).
The physical examination is the examination of the patient for medical signs of disease, which are objective and observable, in contrast to symptoms which are volunteered by the patient and not necessarily objectively observable.[12] The healthcare provider uses the senses of sight, hearing, touch, and sometimes smell (e.g., in infection, uremia, diabetic ketoacidosis). Four actions are the basis of physical examination: inspection, palpation (feel), percussion (tap to determine resonance characteristics), and auscultation (listen), generally in that order although auscultation occurs prior to percussion and palpation for abdominal assessments.[13]
The clinical examination involves the study of:
Vital signs including height, weight, body temperature, blood pressure, pulse, respiration rate, and hemoglobin oxygen saturation
General appearance of the patient and specific indicators of disease (nutritional status, presence of jaundice, pallor or clubbing)
Skin
Head, eye, ear, nose, and throat (HEENT)
Cardiovascular (heart and blood vessels)
Respiratory (large airways and lungs)
Abdomen and rectum
Genitalia (and pregnancy if the patient is or could be pregnant)
Musculoskeletal (including spine and extremities)
Neurological (consciousness, awareness, brain, vision, cranial nerves, spinal cord and peripheral nerves)
Psychiatric (orientation, mental state, mood, evidence of abnormal perception or thought).
It is to likely focus on areas of interest highlighted in the medical history and may not include everything listed above.
The treatment plan may include ordering additional medical laboratory tests and medical imaging studies, starting therapy, referral to a specialist, or watchful observation. Follow-up may be advised. Depending upon the health insurance plan and the managed care system, various forms of "utilization review", such as prior authorization of tests, may place barriers on accessing expensive services.[14]
The medical decision-making (MDM) process involves analysis and synthesis of all the above data to come up with a list of possible diagnoses (the differential diagnoses), along with an idea of what needs to be done to obtain a definitive diagnosis that would explain the patient's problem.
On subsequent visits, the process may be repeated in an abbreviated manner to obtain any new history, symptoms, physical findings, and lab or imaging results or specialist consultations.
Institutions[edit]
The Hospital of
Santa Maria della Scala
, fresco by
Domenico di Bartolo
, 1441–1442
Contemporary medicine is in general conducted within health care systems. Legal, credentialing and financing frameworks are established by individual governments, augmented on occasion by international organizations, such as churches. The characteristics of any given health care system have significant impact on the way medical care is provided.
From ancient times, Christian emphasis on practical charity gave rise to the development of systematic nursing and hospitals and the Catholic Church today remains the largest non-government provider of medical services in the world.[15] Advanced industrial countries (with the exception of the United States)[16][17] and many developing countries provide medical services through a system of universal health care that aims to guarantee care for all through a single-payer health care system, or compulsory private or co-operative health insurance. This is intended to ensure that the entire population has access to medical care on the basis of need rather than ability to pay. Delivery may be via private medical practices or by state-owned hospitals and clinics, or by charities, most commonly by a combination of all three.
Most tribal societies provide no guarantee of healthcare for the population as a whole. In such societies, healthcare is available to those that can afford to pay for it or have self-insured it (either directly or as part of an employment contract) or who may be covered by care financed by the government or tribe directly.
Modern drug
ampoules
Transparency of information is another factor defining a delivery system. Access to information on conditions, treatments, quality, and pricing greatly affects the choice by patients/consumers and, therefore, the incentives of medical professionals. While the US healthcare system has come under fire for lack of openness,[18] new legislation may encourage greater openness. There is a perceived tension between the need for transparency on the one hand and such issues as patient confidentiality and the possible exploitation of information for commercial gain on the other.
Delivery[
edit
]See also:
Health care
,
clinic
,
hospital
, and
hospice
Provision of medical care is classified into primary, secondary, and tertiary care categories.
Nurses in
Kokopo
,
East New Britain
,
Papua New Guinea
Primary care medical services are provided by physicians, physician assistants, nurse practitioners, or other health professionals who have first contact with a patient seeking medical treatment or care. These occur in physician offices, clinics, nursing homes, schools, home visits, and other places close to patients. About 90% of medical visits can be treated by the primary care provider. These include treatment of acute and chronic illnesses, preventive care and health education for all ages and both sexes.
Secondary care medical services are provided by medical specialists in their offices or clinics or at local community hospitals for a patient referred by a primary care provider who first diagnosed or treated the patient. Referrals are made for those patients who required the expertise or procedures performed by specialists. These include both ambulatory care and inpatient services, Emergency departments, intensive care medicine, surgery services, physical therapy, labor and delivery, endoscopy units, diagnostic laboratory and medical imaging services, hospice centers, etc. Some primary care providers may also take care of hospitalized patients and deliver babies in a secondary care setting.
Tertiary care medical services are provided by specialist hospitals or regional centers equipped with diagnostic and treatment facilities not generally available at local hospitals. These include trauma centers, burn treatment centers, advanced neonatology unit services, organ transplants, high-risk pregnancy, radiation oncology, etc.
Modern medical care also depends on information – still delivered in many health care settings on paper records, but increasingly nowadays by electronic means.
In low-income countries, modern healthcare is often too expensive for the average person. International healthcare policy researchers have advocated that "user fees" be removed in these areas to ensure access, although even after removal, significant costs and barriers remain.[19]
Separation of prescribing and dispensing is a practice in medicine and pharmacy in which the physician who provides a medical prescription is independent from the pharmacist who provides the prescription drug. In the Western world there are centuries of tradition for separating pharmacists from physicians. In Asian countries, it is traditional for physicians to also provide drugs.[20]
1 note
·
View note
Text
Educated | December 2019

For the entire year, I wished this book wasn’t on our reading list. Seeing Educated as our December read gave me caution for what I would learn in its pages and how that information would roll around in my head and heart, weighing me with a burden I didn’t need to bear. I don’t handle hard stories well. As this final book selection rolled nearer, my uneasiness grew. I knew this would be a hard read, and even contemplated a few times explaining to this club that I knew myself too well and decided to cautiously decline reading even one page of this memoir. But I wondered if I would regret missing out.
Ten days ago,* I cracked the book open and read about the Indian Princess and the family she housed at her base. Somehow, I was hooked. More than that, I was captivated, spellbound, fascinated with Tara’s story. One more chapter, then one more, then just another. Ultimately, I found Tara to be an exquisite storyteller, a master of words. I found her descriptions to be detailed enough to engulf me and transport me to her world, but she allowed the reader to have emotions for themselves; she didn’t describe her emotions in order to take you into her world, and I liked that. Instead, she let the events and people speak for themselves and for the reader to discover in their own understanding.
Home: Again, and Again, and Again
I loved the foreshadowing of the prologue: “[My father] never told me how I’d know when it was time to come home.” Returning home, to her beloved Buck’s Peak and her complicated, unstable home was the thread that weaved, always rough and harsh, through Tara’s novel. As the reader, it was easy to take the stance of run away and never return! and I assumed that her move to college would be such. But she returned: during school breaks and summers, on weekends and for a sole midnight intrusion, for weddings and funerals, reconciliation and reunion, before a final resolve for a peaceful goodbye on her terms. Yet, did you catch it? I think she holds out hope that she may yet be welcomed home, in time. Does anyone else agree with me on this?
As the reader, each time you see her begin a journey back to Buck’s Peak, you wonder: why. I think the author does a tremendous job of displaying how real, deep, and valued family ties are. Though she confronts her parent’s mistreatment, neglect, and failings in their caring for her, she always thinks the best of them. She always says she loves them. She always explains how they are acting in their understanding of love toward her; I saw this especially in her parent’s visit to Harvard, including the Sacred Grove and Niagara Falls. I think Tara can really see that her parents are not whole beings and are loving her as they think is love. But it takes Tara ten years to learn that she cannot be loved by her parents, in their peculiar way, and remain a whole person. In her final visit to Buck’s Peak and her intentional goodbye, she describes this beautifully: “He gave me a stiff hug and said, ‘I love you, you know that?’ ‘I do,’ I said. ‘That has never been the issue.’” (Page 310).
List of Traumatic Events
About halfway through the book, I thought I would write down each incident of injury. I found these to be the most intense.
two terrible car crashes
falling 18 feet in a junkyard with a deep leg wound at the age of ten
acting as first responder to a fire burn at the age of ten
physically, emotionally, and verbally abused from roughly the age of 15 to 25
Us vs. Them
Because of her father’s, Gene’s, obsession with preparing for the End Days and his distrust of the government, he instilled in his family the mentality of us vs. them: a prevalent thinking that our family knows the real truth and everyone outside these walls---even those inside the same church as us---is out to harm us, destroy us, rip us apart. It’s us vs. them, and they can’t win.
This is ironic. Charles pointed it out---I’m not exactly sure when---but over the course of her story I had developed the same thought: there was no us for the Westovers. They are not looking out for each other. This is displayed in a dozen ways throughout the book:
Not yelling for help when Shawn was being abusive. This is true for likely all the siblings, but it’s known for Tara (the Thanksgiving choke and pin in the family room, the hundreds of times she was inverted into the toilet bowl), revealed through Audrey’s account of violence, and is hinted at through Tyler and Richard’s stance and uneasiness when they witness Shawn’s aggression. Somehow, they each knew that to call on a family member for help was not an option.
No communication with each other. Again, related to Shawn’s violence, no one shared with another member of the family the abuse they suffered until years after they had all left the house.
No teamwork. On the junkyard and at sites, Gene established it was each man (child, really) for himself. I’m chucking lead, so you better duck. I’m concerned about this wildfire, so you better drive your burning body home yourself. I value money above all things, so you best learn how to balance on that pallet and stop wishing for a cherry picker.
A focus on individual responsibility and strength. Tara describes this specifically when she recalls her instincts on page 102: “All my life those instincts had been instructing me in this single doctrine---that the odds are better if you rely only on yourself.” I think this is also displayed through two events that happened when she was ten: her 18-foot fall from the metal bin at the junkyard and her first response care to Luke’s burned leg. After she fell from the bin, her father responded with, “What happened? How’d you manage that?” (Page 65). After she cared for Luke, her mother responded with, “You were lucky this time, Tara. But what were you thinking, putting a burn into a garbage can?” (Page 71). The parents assumed no responsibility for the danger they flung their children into. Instead, Tara grew up being taught that every hurt and failing was her own doing.
I thought the struggle to name who was ultimately responsible for each hardship was beautifully described at the end of the chapter called Apache Women (page 40), when Tara is wrestling with wondering who was at fault for the first car accident. She crafts the most wonderful conclusion. “Me, I never blamed anyone for the accident, least of all Tyler. It was just one of those things. A decade later my understanding would shift, part of my heavy swing into adulthood, and after that the accident would always make me think of the Apache women, and of all the decisions that go into making a life---the choices people make, together and on their own, that combine to produce any single event. Grains of sand, incalculable, pressing into sediment, then rock.” To me, she is saying that the accident was her father’s fault for not leading the family by being the driver and her mother’s fault for letting him be so selfish. But those are grains of sand overlaying a rocky ground of her father’s untreated depression atop a foundation of false believes (not calling an ambulance for medical help). It’s a long spiral down of many poor choices.
Family Under A Firm, Compassionless Father
When I think of Tara’s family, I think of a house full of force, emptied of service; full of physical harm, emptied of protection; full of emotional manipulation, emptied of quiet, listening ears. I thought Tara brilliantly described her father through the example of the math equation: “Dad could command this science, could decipher its language, decrypt its logic, could bend and twist and squeeze from it the truth. But as it passed through him, it turned to chaos.” (Page 126)
The image she describes of her laying on the mattress in the back of their van alongside her mother and Audrey, while her dad accelerates through a snow storm seems to be the perfect picture of how life existed under his authority. He is stubborn, always right In his own eyes, always selfish, never listens, and thrusts his family into harm. I feel so sad for her mom, thinking of her laying there with a quiet question of, “Shouldn’t we drive slower?” answered with acceleration; her eyes closed, body tense, knowing her children will crash alongside her. It is heartbreaking to me to think of the hopelessness of that moment.
After reading about Shawn’s physical, emotional, and verbal abuse toward Tara, I thought she would be most hurt by him. And she was, of course, very hurt---so much that she removed herself from her family. But in how she describes her hurt, it seems that she is most hurt by her father. This at first surprised me. But I now understand; it was under his leadership that all her hurts originated. And it was him who she had to guard herself from as she attempted to reconcile with her mother.
Audrey
I found it interesting that no memory or event with Audrey was specifically called out in Tara’s memoir until the revealing of Shawn’s abuse toward her. For the reader, it felt like Tara was connecting with a stranger, but for Tara, we can assume that their relationship as sisters was deeper for her than what we interpret. It isn’t a wonder why there is little to recall of her memories with Audrey, though; Audrey seemed to always have a job outside the home from an early age in order to avoid her father’s junkyard and Shawn’s abuse. I found it so sad to learn that Audrey later retracted her statements of abuse from Shawn. I wonder: how long can a person lie to themselves?
Shawn
When I think of Tara’s relationship with Shawn, I feel such a sadness for the emotional complexities and shifting assurances that that relationship brings. How does someone reconcile that their greatest protector and defender is also their most harmful abuser? What a twisted relationship for Tara to process for her own health and wellbeing. Perhaps because the violence toward her is so terrible, the moments of protection he provides are astonishingly remarkable.
The description of Shawn advocating for Tara’s safety in not running the Shear (page 140) brought me to tears. This violent stranger of a brother risks himself for a month in order to keep her from harm. And yet, he himself is her greatest harm.
Another moment is described when she is trapped on the runaway horse, Bud. This sentence struck me as beautifully written: “All this would happen in seconds, a year of training reduced to a single, desperate moment.” (Page 103) And he rescues her.
And the one that sets this bipolar relationship into motion, after he has “fixed” her neck and she sees him as, “...some longed-for defender, some fanciful champion, one who wouldn't fling me into a storm, and who, if I was hurt, would make me whole.” (Page 97)
Tyler
Contrast this with Tyler, who is the shining hero in her story. The one who encouraged her education, protected her from Shawn, and stood by her when her family disowned her. This single sentence is remarkable: “How do you thank a brother who refused to let you go, who seized your hand and wrenched you upward, just as you had decided to stop kicking and sink? There aren’t words for that, either.” (Page 317)
Reading that sentence made me weep, and this is what I think Tara is best at: in bringing the complicated emotions and abuses of the human heart into such beautiful descriptions that the reader is left knowing the depths of the potential of the human race’s unthinkable harm and yet abundant rescue a bit more poetically.
Final Thoughts
Oh, there are likely a dozen more moments I’d like to discuss; I feel as if I’ve barely scratched the surface of my notes. I loved this book because I love reading non-fiction, and I’m finding memoirs are my favorite. I loved this book because the writing was simply beautiful and her storytelling supreme. Her realization, “...that a life is not a thing unalterable.” (page 286) might sum up the triumph from tragedy that her life represents. Amazing. Of course, I give it five stars.
I’d love to hear what you thought of the book, even if you have a less glowing review than mine. Please share your takeaways below!
Also, one of my favorite podcasts did a book review of Educated. Take a listen here if you’re interested.
*It took me twice as long to write my review as it did for me to read the book! So the start of this review isn’t hot off the press. ;)
1 note
·
View note
Text
Saisei Academy Verse: Saitou Hibiki
I’m re-making this post since it’s not showing up in the tags. I suspect it’s because I linked my fic which is bullshit, but I want others interested in this little OC grouping to find it so I de-linked it. If you want to find it, I’ve linked my AO3 to my blog or you can just ask me!
I'm finding it increasing difficult to refer to this as an AU version of Hibiki since, while I came up with it second, it's the only verse I've actually written about so far. But now that @miracide has created the wonderful school, Saisei Academy, I've decided that this version of Hibiki would end up there. My story, Ascent, is an origin story for her. So uh... I guess this will inevitably contain spoilers. Take that as you will.
For that reason and for length, I will put her bio under the Keep Reading. Also, I based the formatting after one of the bios she made for one of her own OCs, though I added my own sections.
Hibiki Saitou
Age: 16
Status: 2nd Year Student, General Studies
Basic personality: Deeply cares for others and tends to put them ahead of herself to a fault, quiet, usually only speaks when she has something to say, good listener but bad at communicating her own needs, tends to mother people, over-prepared, anxious and paranoid, only truly comfortable when doing something she knows she’s good at (her preferred school subjects, first aid, cooking) so she is most likely to speak up during these times (providing answers in the school subjects, assertive during first aid, opening up while cooking) though it’s not a guarantee
Basic appearance: On the shorter side of average, thin (due to recent months), long dusty-pink hair that she usually keeps up in a tight bun, dark eyes, covered in scars including prominent one at the corner of her mouth and a crooked nose from when an injury there failed to heal properly, she hides her scars as much as she can (basic foundation on her face, tights/stockings, and sleeves when she’s allowed to, even when it’s hot) because she doesn’t want people to ask her about them
Likes: English language media (especially music), cooking, biology, first aid
Dislikes: Being touched, passive aggression, things being put on higher shelves out of her reach
Favorite food: Hot chocolate
Best school subjects: Biology, English (nearly fluent since her father was)
Worst school subjects: PE, arts
Random fact: She tends to sing while she does chores when she thinks nobody is around (her skill is only average). She gets super embarrassed by it if someone catches her doing it. But because she keeps forgetting that she lives with other people, this happens relatively often.
----------
Quirk: Injury exchange
- With skin-to-skin contact, she can exchange any active physical damage between herself and the person she is touching.
- Injuries transfer between analogous body parts so a broken left arm causes a break in the same place in the same way on the other person’s left arm. If one gets an injury in a place that is otherwise uninjured, the state of non-injury is given in the exchange. So if Person A has a broken left arm and Hibiki is uninjured there, she takes the broken arm while it is healed in Person A.
- By default, it switches all injuries across the entire body, but with concentration, she can focus it to a specific area. This means she can theoretically heal others while stockpiling a dangerous amount of injuries onto herself.
- The quirk activates automatically and she has to specifically cancel it, so she is dangerous to touch while unconscious (since generally injuries are what cause one to become unconscious).
- Her most common use of her quirk is where she can sense any and all injuries of the other person, but deactivates her quirk before the exchange is made. This allows her to accurately access someone injured without advanced scanning equipment or putting herself in harm's way.
- Still-present causes of injuries are not affected, only the active damage to the body. A stabbing would need to have the knife removed first. Otherwise it will completely heal around the knife in the victim and leave a disconnected knife-shaped flesh in her own wound in the exchange as that could not be exchanged. Similarly, damage from an illness or a poison can be exchanged, but the original victim would simply acquire that damage again. The only advantage of proceeding with the exchange despite this is it gives the chance to “restart the clock” once that may buy time.
----------
Background:
Unlike many students at Saisei Academy, she came into the program with excellent quirk control. She mainly attends the school for psychological support and reform due to her criminal activity. Since she has an otherwise clean record and her crimes were nonviolent in nature, she avoided jail time. This, plus her good academic record and other extenuating circumstances, saw her admission to Saisei Academy. However, as she IS a criminal, she is liable to have more restrictions than the average student (I just don’t know what restrictions Miracide would have for this kind of situation).
Her home life has not been great. Hibiki's mother died shortly after her quirk manifested because a villain attack left the toddler gravely injured. When her mother naturally came to her aid, the injuries transferred to her and help didn't come until it was too late. Hibiki's father, in his grief, always blamed her for her mother's death, often taking his frustration out on her and using Hibiki's quirk to indirectly aid in his hero work.
He was a local pro-hero named Noci whose quirk allowed him to store any pain he's sustained in the past 24 hours and give it to someone else. This allowed him to incapacitate villains without causing actual damage to them. The potential for his quirk to be used for torture made him a controversial hero so he never became incredibly popular outside of his home town. For his hero work, he would often allow himself to become injured so he could store the pain, but later force Hibiki to take on the actual injuries herself so that he wasn't incapable of actual fighting. She'd attempted to go to the authorities about this, but his connections with local law enforcement prevented the case from being pursued seriously. This long-term abuse and the refusal of its acknowledgment made Hibiki incredibly skeptical and disillusioned towards the hero system and law enforcement as a whole.
Hibiki was left to her own devices for much of the day, but was not allowed to interact much with her peers outside of school. She took on many of the domestic responsibilities of her house at a young age as a result. She disliked most of them, but became very efficient in doing them, a skill she carries to this day. Hibiki does like cooking, however.
Her only true friend in school was Tanaka Rin. Rin was one of the only students who didn't treat Hibiki any differently despite her scars and frankly was the only reason Hibiki has any real social skills at all. The two girls became even closer when an accident permanently blinded Rin and Hibiki helped her devise a way for Rin to use her temperature quirk as a form of thermal imaging.
The two however were separated when Rin chose to pursue a career as a pro-hero and succeeded in getting into the hero program at the famed UA. Hibiki applied to a more normal high school on the area in order to be near her and in the process ran away from home. However, she became too embarrassed to let Rin see her as she was since she had nothing to her name after becoming a runaway. This put her in a very dark place.
A fateful encounter with a young criminal who nearly died since he didn't want to be arrested had he gone to a hospital led her to create The Bunker. The Bunker was an off-the-grid medical facility housed in an abandoned bunker that had been built when quirks first began to emerge, but had long since been forgotten. The 6-bed facility allowed her to help those who, like her, had been ignored but still needed help. With the help of a disgraced nurse who had been fired from the local hospital for taking pain killers while on the job, she ran the facility for 6 months before a raid brought it to its end.
While the raid meant Hibiki now had a criminal record (though the charges were less than you'd expect due to the care she took to remain as close to technically legal as possible), it also finally exposed her father's abuse to the world. He went on the run before he could be arrested and remains at large. As she now doesn’t technically have parents or legal guardians, she is a ward of the state until further notice.
----------
The main goals for Hibiki's reform are to:
- Regain trust in authority. While she doesn't necessarily act out, she does a worrying amount of hopeless/mindless compliance.
- Learn it is okay to put her own health first. She went through much of her life thinking it's her place in life to sacrifice herself for the betterment of others and that prioritizing herself was selfish.
- Figure out what she wants to do with her life. Due to the above, Hibiki has resigned herself to believing she will die young and as such has difficulty thinking in the long-term. She's never thought much about her future because she never thought she had one.
1 note
·
View note
Last Seen Blogs

thotnamjoon
girl with luv

theothermovember
THE OTHER MOVEMBER

littleststarfighter
“Good Boys Go To Heaven (Bad Boys Go Everywhere)”

bdangkingfish
Kingfish

markmybirds
The Birds are Watching