#compulsive liars
Text

Following publication of the final report there have been a number of questions and points for clarification about the findings and recommendations. We have collated those questions, along with our answers, on this page.
-
Did the Review set a higher bar for evidence than would normally be expected?
No, the approach to the assessment of study quality was the same as would be applied to other areas of clinical practice – the bar was not set higher for this Review.
Clarification:
The same level of rigour should be expected when looking at the best treatment approaches for this population as for any other population so as not to perpetuate the disadvantaged position this group have been placed in when looking for information on treatment options.
The systematic reviews undertaken by the University of York as part of the Review’s independent research programme are the largest and most comprehensive to date. They looked at 237 papers from 18 countries, providing information on a total of 113,269 children and adolescents.
All of the University of York’s systematic review research papers were subject to peer review, a cornerstone of academic rigour and integrity to ensure that the methods, findings, and interpretation of the findings met the highest standards of quality, validity and impartiality.
-
Did the Review reject studies that were not double blind randomised control trials in its systematic review of evidence for puberty blockers and masculinising / feminising hormones?
No. There were no randomised control studies identified in the systematic reviews, but other types of studies were included if they were well designed and conducted.
Clarification:
The Review commissioned the University of York to undertake an independent research programme to ensure the work of the Review and its recommendations were informed by the most robust existing evidence. This included a series of systematic reviews which brought together, analysed and evaluated existing evidence on a range of issues relating to the care of gender-questioning children and young people, including epidemiology, treatment approaches and international models of current practice.
Randomised control trials are considered the gold standard in relation to research, but there are many other study designs that can give valuable information. Explanatory Box 1 (pages 49-51 of the final report) discusses in more detail the different kinds of studies that can be used, and how to decide if a study is poorly designed or biased.
Blinding is a separate issue. It means that either the patient or the researcher does not know if the patient is getting an active treatment or a ‘control’ (which might be another treatment or a placebo). Patients cannot be blinded as to whether or not they are receiving puberty blockers or masculinising / feminising hormones, because the effects would rapidly become obvious. Good RCTs can be conducted without blinding.
The University of York’s systematic review search did not identify any RCTs, blinded or otherwise, but many other studies were included. Most of the studies included were called ‘cohort studies’. Well-designed and executed high quality cohort studies are used in other areas of medicine, and the bar was not set higher for this review; even so the quality of the studies was mostly only assessed as moderate.
-
Did the Review reject 98% of papers demonstrating the benefits of affirmative care?
No. Studies were identified for inclusion in the synthesis (conclusions) of the systematic reviews on puberty blockers and masculinising/feminising hormones on the basis of their quality. This was assessed using a standard quality assessment tool appropriate to the types of study identified. All high quality and moderate quality reviews were included in the synthesis of results. This totalled 58% of the 103 papers.
Clarification:
The Newcastle-Ottawa scale (a standard appraisal tool) was used to compare the studies. This scores items such as participant selection, comparability of groups (how alike they are), the outcomes of the studies and how these were assessed (data provided and whether it is representative of those studied). High quality studies (scoring >75%) would score well on most of these items; moderate quality studies (scoring >50% – 75%) would miss some elements (which could affect outcomes); and low-quality studies would score 50% or less on the items the scale looked at. A major weakness of the studies was that they did not have adequate follow-up – in many cases they did not follow young people for long enough for the long-term outcomes to be understood.
Because the ranking was based on how the studies were undertaken (their quality and execution), low quality research was removed before the results were analysed as the findings could not be completely trusted. Had an RCT been available it would also have been excluded from the systematic review if it was deemed to be of poor quality.
The puberty blocker systematic review included 50 studies. One was high quality, 25 were moderate quality and 24 were low quality. The systematic review of masculinising/feminising hormones included 53 studies. One was high quality, 33 were moderate quality and 19 were low quality.
All high quality and moderate quality reviews were included, however as only two of the studies across these two systematic reviews were identified as being of high quality, this has been misinterpreted by some to mean that only two studies were considered and the rest were discarded. In reality, conclusions were based on the high quality and moderate quality studies (i.e. 58% of the total studies based on the quality assessment). More information about this process in included in Box 2 (pages 54-56 of the final report)
-
Has the Review recommended that no one should transition before the age of 25 and that Gillick competence should be overturned.
No. The Review has not commented on the use of masculinising/feminising hormones on people over the age of 18. This is outside of the scope of the Review. The Review has not stated that Gillick competence should be overturned.
The Review has recommended that:
“NHS England should ensure that each Regional Centre has a follow through service for 17-25-year-olds; either by extending the range of the regional children and young people’s service or through linked services, to ensure continuity of care and support at a potentially vulnerable stage in their journey. This will also allow clinical, and research follow-up data to be collected.”
This recommendation only relates to people referred into the children and young people’s service before the age of 17 to enable their care to be continued within the follow-through service up to the age of 25.
Clarification:
Currently, young people are discharged from the young people’s service at the age of 17, often to an adult gender clinic. Some of these young people have been receiving direct care from the NHS gender service (GIDS as was) and others have not yet reached the top of the waiting list and have “aged out” of the young people’s service before being seen.
The Review understands that this is a particularly vulnerable time for young people. A follow-through service continuing up to age 25, would remove the need for transition (that is, transfer) to adult services and support continuity of care and continued access to a broader multi-disciplinary team. This would be consistent with other service areas supporting young people that are selectively moving to a ‘0-25 years’ service to improve continuity of care.
The follow-through service would also benefit those seeking support from adult gender services, as these young people would not be added to the waiting list for adult services and, in the longer-term, as more gender services are established, capacity of adult provision across the country would be increased.
People aged 18 and over, who had not been referred to the NHS children and young people’s gender service, would still be referred directly to adult clinics.
-
Is the Review recommending that puberty blockers should be banned?
No. Puberty blocker medications are used to address a number of different conditions. The Review has considered the evidence in relation to safety and efficacy (clinical benefit) of the medications for use in young people with gender incongruence/gender dysphoria.
The Review found that not enough is known about the longer-term impacts of puberty blockers for children and young people with gender incongruence to know whether they are safe or not, nor which children might benefit from their use.
Ahead of publication of the final report NHS England took the decision to stop the routine use of puberty blockers for gender incongruence / gender dysphoria in children. NHS England and National Institute for Health and Care Research (NIHR) are establishing a clinical trial to ensure the effects of puberty blockers can be safely monitored. Within this trial, puberty blockers will be available for children with gender incongruence/ dysphoria where there is clinical agreement that the individual may benefit from taking them.
Clarification:
Puberty blockers have been used to suppress puberty in children and young people who start puberty much too early (precocious puberty). They have undergone extensive testing for use in precocious puberty (a very different indication from use in gender dysphoria) and have met strict safety requirements to be approved for this condition. This is because the puberty blockers are suppressing hormone levels that are abnormally high for the age of the child.
This is different to stopping the normal surge of hormones that occur in puberty. Pubertal hormones are needed for psychological, psychosexual and brain development, and there is not yet enough information on the risks of stopping the influence of pubertal hormones at this critical life stage.
When deciding if certain treatments should be routinely available through the NHS it is not enough to demonstrate that a medication doesn’t cause harm, it needs to be demonstrated that it will deliver clinical benefit in a defined group of patients.
Over the past few years, the most common age that young people have been receiving puberty blockers in England has been 15 when most young people are already well advanced in their puberty. The new services will be looking at the best approaches to support young people through this period when they are still making decisions about longer-term options.
-
Has the Review recommended that social transition should only be undertaken under medical guidance?
The Review has advised that a more cautious approach around social transition needs to be taken for pre-pubertal children than for adolescents and has recommended that:
“When families/carers are making decisions about social transition of pre-pubertal children, services should ensure that they can be seen as early as possible by a clinical professional with relevant experience.”
Parents are encouraged to seek clinical help and advice in deciding how to support a child with gender incongruence and should be prioritised on the waiting list for early consultation on this issue. This should include discussion of the risks and benefits and the voice of the child should be heard. It will be important that flexibility is maintained, and options remain open.
Clarification:
Although the University of York’s systematic review found that there is no clear evidence that social transition in childhood has positive or negative mental health outcomes, there are studies demonstrating that for a majority of young children presenting with gender incongruence, this resolves through puberty. There is also evidence from studies of young people with differences of sex development (DSD) that sex of rearing seems to have some influence on eventual gender outcome, and it is possible that social transition in childhood may change the trajectory of gender identity development for children with early gender incongruence. Living in stealth from early childhood may also lead to stress, particularly as puberty approaches.
There is relatively weak evidence for any effect of social transition in adolescence. The Review recognises that for adolescents, exploration is a normal process, and rigid binary gender stereotypes can be unhelpful. Many adolescents will go through a period of gender non-conformity in terms of outward expressions (e.g. hairstyle, make-up, clothing and behaviours). They also have greater agency in how they present themselves and in their decision-making.
Young people and young adults have spoken positively about how social transition helped to reduce their gender dysphoria and feel more comfortable in themselves. They identified that space to talk about socially transitioning and how to handle conversations with parents/carers and others would be helpful. The Review has therefore advised that it is important to try and ensure that those already actively involved in the young person’s welfare provide support in decision making and that plans are in place to ensure that the young person is protected from bullying and has a trusted source of support.
Further detail can be found in Chapter 12 of the Final Report.
-
Did the Review speak to any gender-questioning and trans people when developing its recommendations?
Yes, the Review has been underpinned by an extensive programme of proactive engagement, which is described in Chapter 1 of the report. The Review has met with over 1000 individuals and organisations across the breadth of opinion on this subject but prioritised two categories of stakeholders:
People with relevant lived experience (direct or as a parent/carer) and organisations working with LGBTQ+ children and young people generally.
Clinicians and other relevant professionals with experience of and/ or responsibility for providing care and support to children and young people within specialist gender services and beyond.
A mixed-methods approach was taken, which included weekly listening sessions with people with lived experience, 6-weekly meetings with support and advocacy groups throughout the course of the Review, and focus groups with young people and young adults.
Reports from the focus groups with young people with lived experience are published on the Review’s website and the learning from these sessions and the listening sessions are represented in the final report.
The Review also commissioned qualitative research from the University of York, who conducted interviews with young people, young adults, parents and clinicians. A summary of the findings from this research is included as appendix 3 of the final report.
-
What is the Review’s position on conversion therapy?
Whilst the Review’s terms of reference do not include consideration of the proposed legislation to ban conversion practices, it believes that no LGBTQ+ group should be subjected to conversion practice. It also maintains the position that children and young people with gender dysphoria may have a range of complex psychosocial challenges and/or mental health problems impacting on their gender-related distress. Exploration of these issues is essential to provide diagnosis, clinical support and appropriate intervention.
The intent of psychological intervention is not to change the person’s perception of who they are but to work with them to explore their concerns and experiences and help alleviate their distress, regardless of whether they pursue a medical pathway or not. It is harmful to equate this approach to conversion therapy as it may prevent young people from getting the emotional support they deserve and make clinicians fearful of providing this group of children and young people the same care as is afforded to other children and young people.
No formal science-based training in psychotherapy, psychology or psychiatry teaches or advocates conversion therapy. If an individual were to carry out such practices they would be acting outside of professional guidance, and this would be a matter for the relevant regulator.
==
Like any religious fanatics, pathological liars like "Erin" Reed and "Alejandra" Carballo still won't stop lying, since it's all they have. But their disciples should really be noticing how they've been directly refuted.
#Cass review#Cass report#Hilary Cass#Dr. Hilary Cass#disinformation#misinformation#pathological liars#Erin Reed#Alejandra Carabello#Michael Hobbes#medical scandal#medical corruption#medical malpractice#gender affirming care#gender affirming healthcare#gender affirmation#compulsive liars#gender fanatics#gender cult#gender ideology#gender identity ideology#queer theory#intersectional feminism#puberty blockers#cross sex hormones#wrong sex hormones#religion is a mental illness
39 notes
·
View notes
Text
Sadly there are a lot of believers…
4 notes
·
View notes
Text
Climb under a cow.
A few years ago now, I did a project with some vulnerable people. This has happened quite a lot over the years and on this particular occasion, there was going to be quite a bit of publicity. I walked in while the charity workers were doing the set up and there was a big photo of me…
I instantly asked them to take in down and any mention of me with it.
It was nothing to do with me, I just…

View On WordPress
#actually autistic#attention seeking#Autism#compulsive liars#do gooders#gaslighting#Human nature#morality#narcisism#toxic people#vanity#vanity projects#virtue signalling#wisdom
0 notes
Text
I met the "I'm sooooo freaking fake and I show it" person
But not the one that is charismatic and has good reasons, the one that is actually annoying
Idk how to explain it, like someone is intimidating you but in a sweet gentle voice tone, the difference is that the one is charismatic kinda tries to hide it, while the annoying slowly goes more aggresive and at the end says "i'M nOt MaD, jUsT sAyInG" or something like that
#idk#idk what im doing#idk what else to tag#my opinion#My opinion?#my opinion of course#Fakeness#Fake kindness#Voice tone#Acting#Compulsive liars#fake people#Passive agressive
0 notes
Text
Habitual Lying
It’s official, George Santos is Lila Rossi.
#george santos#life#real life#politics#anti george santos#miraculous#miraculous ladybug#miraculous: tales of ladybug and cat noir#lila rossi#volpina#chameleon#tales of ladybug and cat noir#compulsive lying#habitual lying#ladybug and cat noir#ladybug#compulsive liars#habitual liars#compulsive liar#habitual liar
1 note
·
View note
Text
Jason: What's wrong with you!
Tim: Well, for one, I'm a compulsive liar
Jason: Really?
Tim:
Tim: No
1K notes
·
View notes
Text
Aradia: 0kay i'm n0rmal now <- lying liar wh0 lies
#homestuck#incorrect homestuck quotes#aradia megido#mod terezi#hey if lying makes you feel more normal then by all means be a compulsive liar
65 notes
·
View notes
Text
the whole vibe of black ajah verin investigating black ajah liandrin possibly compelling black ajah sheriam is just so good

#did liandrin/someone compel sheriam? was sheriam in cahoots with liandrin and just being a really bad liar to verin?#does verin know full well that sheriam is BA but just makes up the possibility of compulsion to put yasicca on the right track?#all of the above? i don't know! so many layers so many possibilities#wot#wot book spoilers
63 notes
·
View notes
Text
Shoutout to all of the mental disorders where the tags are flooded by people who hate those with said disorder (NPD, BPD, ASPD, HPD, pathological lying, IED, etc.) It's messed up and you deserve better
#actually compulsive liar#npd safe#npd positivity#aspd safe#cluster b safe#bpd#hpd safe#bpd safe#pathological liars#compulsive liar#compulsive lying#ied#actually ied#ied safe
41 notes
·
View notes
Text

By: Benjamin Ryan
Published: Apr 18, 2024
On April 9, the long-awaited Cass Review detonated in England. Its effects have been felt around a world torn asunder by the politicized subject of gender. The 388-page report, which was supported in part by six independent systematic literature reviews that were published by the BMJ, scrutinized the science behind pediatric gender-transition treatment.
Cass found that the practice of prescribing puberty blockers and cross-sex hormones to minors was based on “remarkably weak evidence.”
In the report’s fallout, furious clouds of misinformation have formed, fueled by people who doubtfully have read much—or any—of the report or the BMJ papers. These people have falsely claimed that Cass only accepted randomized controlled trials, or RCTs, as evidence to consider in her massive report.
I write this article as the same lone warrior who battled monkeypox misinformation (and made a typo doing it) two years ago. I write in hopes of setting the record straight on a few key points. I write as a dismayed middle-aged man who remains, at his heart, the same frustrated child who always did the reading before class, and who was forced to sit and listen to those who hadn’t done their homework dominate the discussion.
The following is a distillation of various fact-checking tweet threads I’ve published regarding the Cass Review. Individual tweets are hyperlinked throughout the text if you would care to refer to, comment upon, or retweet them.
To learn about the specifics of the Cass Review, you can check out my coverage in The New York Sun, my tweet thread about that article, and my thread about the report.
This particular article will be devoted to the dying art of fact checking.
Here’s What’s At Stake
Many advocates of gender-distressed young people are furious that systematic literature reviews, they argue, set the evidentiary bar too high. They say these reviews forbid the acceptance of lots of promising findings from perfectly good studies on pediatric gender-transition treatment.
Others say those evidence-based-medicine standards of assessing the strength versus weaknesses of research are vital to prevent research that makes erroneous claims from impacting health policy and sending it astray.
They note that the stakes are high when it comes to pediatric gender-transition treatment, in particular considering the drugs in question may impact fertility and sexual function. Fertility, they say, is a human right. And since children cannot consent to their own care, the adults responsible for their care—parents or guardians and doctors—need to be especially sure before they consent to or provide drugs that could take a child’s fertility.
Here’s the question: Where does the pediatric gender-dysphoria care field go from here, now that Cass has said the evidence is weak and uncertain (as have multiple previous systematic literature reviews)? Should it accept the claim of GLAAD, the LGBTQ media watchdog group, that the “science is settled,” and that puberty blockers and cross-sex hormones should be widely provided to gender-distressed children?

Or should the pediatric gender-medicine field follow the lead of Cass and England, and of Scandinavian nations, re-classifying pediatric gender-transition treatment as experimental and, accordingly, restricting it to clinical trials only Then, if the results of those clinical trials are favorable, it is possible that those European nations will change course again and broaden access to puberty blockers and cross-sex hormones for minors? Perhaps then they would be satisfied that the evidence is strong enough?
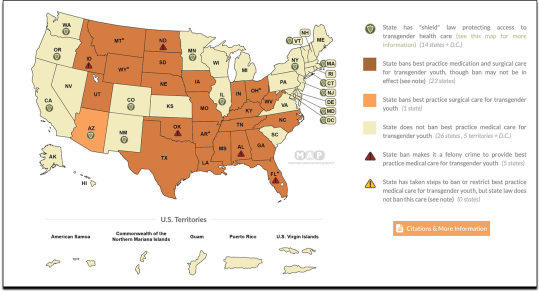
Here in the US, we have a split-screen system, quite unlike the European nations:
23 red states have passed bans of pediatric access to puberty blockers and cross-sex hormones for gender distress. Many are tied up in the courts. The Supreme Court will almost surely settle the matter.
Blue states support liberal access to such medications.
The major US medical societies, in particular the American Academy of Pediatrics and the Endocrine Society, along with the medical/activist group WPATH, all support liberal access to pediatric gender-transition treatment. This is in stark contrast to Cass/England’s approach.
So wide is the gulf between Cass and WPATH that after Cass supported forbidding puberty blockers and cross-sex hormones to minors, WPATH said that the majority of gender-dysphoric adolescents would fare better on such medications than with the holistic mental-health care Cass advises and that is now policy in England.
At stake here is the question of how scientific research is translated into health policy.
Who gets to decide, and what methods do they use to assess the research?
What is the best way to do this, to ensure that the best possible care is provided to vulnerable young people?
The most important question is this: How can patients, families and healthcare and mental-health providers be provided the most robust and informative information possible to guide their shared decision-making as they weigh the risks versus benefits of treatment?
Cass says that WPATH’s guidelines are weak. WPATH countered in their recent statement by asserting that they, WPATH, are the subject-matter experts on pediatric gender-transition treatment, not Cass. The American Academy of Pediatrics, meanwhile, has been sued, along with the author of its 2018 policy statement backing pediatric gender-transition treatment and the overall “affirmative” model of care, in a medical-malpractice suit that I covered for The New York Sun.
False Claims Have Widely Circulated That Cass Rejected all Non-Randomized Controlled Trials
Cass does indeed state that randomized-controlled trials are the gold-standard of scientific studies. Meanwhile, many claim that an RCT for gender-transition treatment would be unethical to conduct among children, because the preponderance of evidence indicates the treatment is safe and effective. (Others vigorously dispute that such a trial would be unethical and that such evidence is trustworthy—hence, they say, the need for an RCT.) Furthermore, it is not possible to blind such a study, because the effects of the drugs (i.e., suppressed puberty or cross-sex puberty) are too obvious.
However, neither of the two systematic literature reviews on which Cass was partially based—one about puberty blockers, the other about cross-sex hormones to treat gender distress in minors—place RCTs as the bar that the 103 studies they assessed needed to meet. Rather, they used a validated assessment tool known as the Newcastle-Ottowa scale, which is designed to assess the strength of observational studies.
This is how one of the papers described the scale:
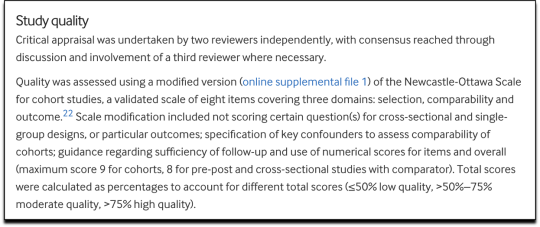
Neither of the studies deemed high quality by the reviews were RCTs.
And so, the widespread claims that the Cass Review set an impossibly high bar to reach by demanding only RCTs, discarding 101 out of 103 studies of pediatric gender-transition treatment, are: FALSE
Let’s examine how Dr. Hilary Cass and her team did factor in the systematic literature reviews about puberty blockers and cross-sex hormones.
One systematic literature review examined puberty-blockers for gender distressed kids. It examined 50 studies, and included in its synthesis one high-quality study and 25 moderate-quality studies. It did not simply ignore the 24 low-quality studies.
The other systematic lit review examined cross-sex hormone use for gender distress in minors. It examined 53 studies, and included in its synthesis one high-quality study and 33 moderate-quality studies. But it did not simply ignore the 19 low-quality ones.
What about the Cass Review? How did it make use of the two systematic lit reviews? The claim that Cass simply discarded the 101 moderate/low-quality studies and only looked at the two high-quality studies is: FALSE
She folded the analyses of the 103 studies into her report.

Let’s zoom in to the 388-page Cass review. To see where she first folds in the findings of the systematic literature review of cross-sex hormones, go to page 183. Here is how she introduces that paper:

Cass includes in her report the following chart from the lit-review paper on cross-sex hormones, which breaks down all the studies it analyzed and what outcomes they addressed. Cass is pointing out key areas where more research is needed, in particular about fertility outcomes. So you can see that this report is about way more than just the narrow question of treatment efficacy. It’s about the whole field of pediatric gender medicine and the research apparatus behind it.

On page 184 of the Cass Review, she goes into considerable detail about the findings of the systematic literature review about cross-sex hormones. She does not solely focus on the one high-quality study, although she does certainly highlight it. She refers to all 53 studies.
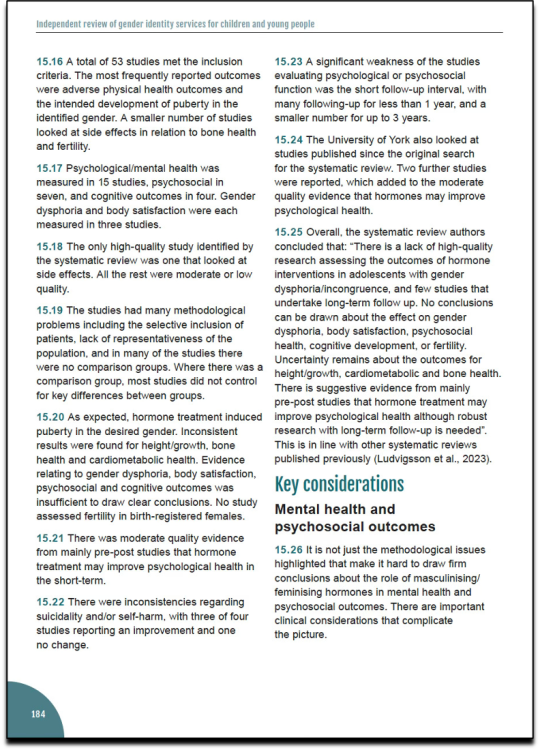
The review discusses the findings of the systematic literature review on cross-sex hormones for minors amid discussions of lots of other individual papers about pediatric gender-transition treatment. The review also folds in the findings from the systematic literature review about puberty blockers for gender distressed minors (p. 175).
Cass includes the following chart from the review paper on puberty blockers for gender-distressed kids, which breaks down the outcomes examined by the 50 studies. It points to areas where much more research is needed, especially about…fertility.

From page 176 to 177, Cass has lots to say about the specifics of the puberty blocker systematic literature review. She does not restrict her discussion to the one high-quality study included in the review.
The Review includes 15 pages of footnotes of studies, guidelines, and other sources on which the report is based. The report is not solely based on two studies.
In sum, those who say Cass and the lit reviewers simply discarded 101 studies are incorrect. However, because the quality of the study findings was overwhelmingly weak, Cass was indeed very limited in which studies she could rely on in assessing safety and efficacy in particular.
Cass sums up the matter as follows in her introduction:

Who Has Made False Claims That The Cass Report Rejected All Non-RCTs?
The Canadian Broadcasting Corporation published an article quoting doctors repeating, and failing to challenge, the false claim that the Cass Review disregarded any studies about pediatric gender-transition treatment that were not randomized controlled trials. The article made various other false or misleading claims, such as that puberty blockers are at least believed to be safe and reversible. Sallie Baxendale’s recent scholarship, along with Cass’s findings, have shown how neither of those claims are known to be true. Much more research is needed.
Continuing a running theme in our culture of late, hundreds of academics have signed a letter protesting the Cass Review that strongly suggests they have not read the review or the systematic literature reviews on which it is partly based. Their letter falsely claims the Cass Review “does not include a proper systematic literature review since it disregards most research evidence because it fails to reach the impossibly high bar of a double-blind trial.”
The letter was spearheaded by transfeminist sociologist Natacha Kennedy and her colleagues at the Feminist Gender Equality Network.
Numerous accounts on X (formerly Twitter) broadcast the false claim that the Cass Review and two of the systematic literature reviews on which it was based simply discarded 101 of 103 studies on pediatric gender-transition treatment. This includes the British singer Billy Bragg, Dr. David Gorski (who also falsely claimed that Cass referred to so-called rapid-onset gender dysphoria in her report) and activist Substacker Erin Reed:

In her most recent Substack published April 18, Erin Reed continued to further the falsehood that Cass “disregarded” all but high-quality studies. She also made false or misleading claims about: the subjectivity of the systematic literature review’s scoring system; the ongoing debate over whether gender dysphoria is influenced by social contagion; the false notion that the Cass Review aligned itself with an anti-trans propagandist; and the detransition rate.
In a lengthy YouTube video, British political activist and pundit Owen Jones (who once interviewed me about monkeypox when I was very swollen and bald from chemo) repeatedly made the false assertion that the Cass Review excluded all non-RCTs.
youtube
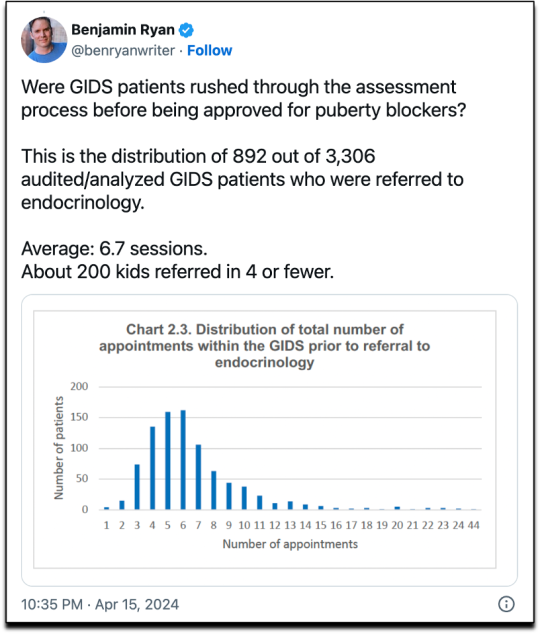
Jones also falsely claimed that none of England’s pediatric-gender-clinic patients were sped through the assessment process. The Cass Review shows that at a minimum, hundreds of children were referred to endocrinology after no more than four assessment appointments.
Jones also repeatedly said that the rate of detransitioning—people who after taking cross-sex hormones stop the medications and revert to identifying as their biological sex—is about 1 percent, saying that long-term studies show this. This despite the fact that Cass said in her report that because of a lack of long-term follow-up, the detransition rate is unknown.

How Did All This Misinformation Get Started?
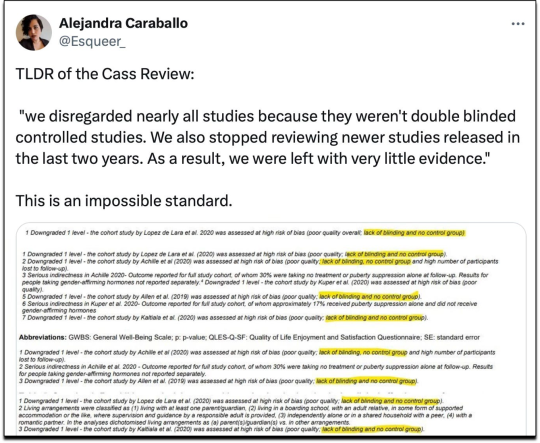
From what I can estimate, the first person to have pushed the false claim that Cass simply discarded 98 percent of the available studies about pediatric gender-transition treatment was trans activist and attorney Alejandra Caraballo.
The key problem is that Caraballo cited the wrong systematic literature reviews in a viral tweet about the Cass Review.
Five hours before the Cass Review was published on April 9, Caraballo tweeted a screenshot of what appeared to be the new systematic literature reviews that would be published alongside the Cass report. But these screenshots were actually from the so-called NICE reviews—from 2020.
The tweet quickly racked up hundreds of thousands of views and has 850K to date.
The NICE reviews of the pediatric use of puberty blockers and cross-sex hormones for gender distress relied on the GRADE system, which with rare exceptions only gives high-quality ratings to randomized controlled trials.
Caraballo apparently did not yet have a copy of the final Cass Review report at this time. If Caraballo had waited until the new systematic literature reviews on which it was partly based, Caraballo would have seen that they did not throw out all but RCTs.
I am quite certain Caraballo did not have access to the Cass Review’s final report before the embargo lifted (at 7:01pm ET April 9), because shortly before the embargo was set to lift, Caraballo tweeted what was quite apparently thought to be the Cass report. But the link was to the review papers, not the report. As you can see, I told Caraballo on April 9 that the tweet had not, as claimed, linked to the Cass Review:
And of course amid all this, uber-popular debunking podcaster Michael Hobbes, who once hosted a show called You’re Wrong About, weighed in.
This reminds me of the time Hobbes hate tweeted about the feature in The Atlantic that I wrote about carpal tunnel syndrome and spent half the summer researching. He dismissed it with a wave of the hand. It was obvious he had not read it.
I will leave you, dear reader, with one small, yet mighty request:
PLEASE DO THE READING.
--
About the Author
Benjamin Ryan is an independent journalist, specializing in science and health care coverage. He has contributed to The New York Times, The Guardian, NBC News and The New York Sun. Ryan has also written for the Washington Post, The Atlantic, The Nation, Thomson Reuters Foundation, New York, The Marshall Project, PBS, The Village Voice, The New York Observer, the New York Post, Money, Men's Journal, City & State, Quartz, Out and The Advocate.
Learn more about Ryan’s work on his website, and follow him on X @benryanwriter.
==
Make no mistake, these gender fanatics aren't mistaken or misinformed or confused. This is malicious and deliberate. They're liars and they know they're lying.
How do we know? They don't say things like, "ah, that makes sense now," or "I didn't realize that," or "I misunderstood that."
Instead, they pivot, and then they pivot, and then they pivot again. They create one lie, then another, then another, then another.
"The amount of energy needed to refute bullshit is an order of magnitude bigger than that needed to produce it."
-- Brandolini's Law
It's not criticism or analysis. They're anti-science religious fundamentalists doing the same kind of thing anti-evolution creationists do: strawman, misrepresent, misinterpret or outright lie in order to create a false sense of doubt or uncertainty. It's religious apologists producing propaganda for the faithful.
--
Note: Even Stonewall has had to backpedal, which they've done while pretending how the research was evaluated was "unclear." Community Notes has pointed out that dedicated sections in the report itself explain exactly how this was done.

Meaning, Stonewall was either lying about having read it, or they read it but were lying about what's in it. It's most likely they didn't read it and simply took the word of one or more of the already named frauds and activists LARPing as "journalists."
#Benjamin Ryan#Cass Review#Cass Report#Dr. Hilary Cass#Hilary Cass#disinformation#pathological liars#compulsive liars#Michael Hobbes#Alejandra Caraballo#Erin Reed#Christopher Reed#gender propaganda#trans propaganda#science#anti science#propaganda#religion is a mental illness
5 notes
·
View notes
Photo




Honesty is not a thing to be found, Asriel. You’re either honest or you’re not, and... neither of us are.
#his dark materials#hdmedit#*#masriel#asriel x marisa#asriel: i said what i said. no i didn't#they're so funny i love compulsive liars
331 notes
·
View notes
Text
I can’t believe David was caught lying in a three-way phone call!!! Lol
He was just like: Sam, I wanted to do it with you, that was the plan. Michael drinks too much, he’s overbearing, but I’m stuck with him.
And then Michael was listening lol.
After he called Michael and was like: I’m sorry I lied. I needed to manage this situation with Sam but I want to do it with you. You have passion and Sam has zero imagination.
And Sam was hearing it all 😂😂😂
#David being a compulsive liar lol#apparently standing in the corner for half an hour taught him nothing#watching staged#staged#david tennant#michael sheen#samuel l jackson
23 notes
·
View notes
Text
Being honest with your teachers is something that can be so borderline impossible
#i need to tomorrow#and im very nervous#also its worse bc its a teacher ive known for li7 years#i am going to throw up#lasar being incoherent#im not a compulsive liar but i lie more than i care to admit#i find it so annoying because it causes more problems for me than i started with#i need to make notes
14 notes
·
View notes
Note
At this point you've written at least four different roleswap AUs, so I was wondering if you had any thoughts or takes about how a roleswap AU should be? - someone who's planning on making a roleswap AU
Please don't remind me. I'm embarrassed about this. I know I need to write other things. I don't know why the AU concept is so incredibly fun to write. I can't explain it. Roleswaps are very easy to write and a lot of fun and involve being a freak about everything. Who wouldn't write 10 of those bitches.
But yes, as someone whose roleswap AUs are like 9 out of her 51 fics, I feel qualified to talk about this. These are just my own opinions and takes, and other people might do it differently - if you write roleswaps too, feel free to add in your two cents!!
Before sitting down to write literally anything I always figure out the rules of the story. Writing is little more than a nonstop series of decisions, and if you abide by the rules of your story or characters then your decisions will be coherent and cohesive. By rules I don't mean worldbuilding - I mean the internal logic of the story and the characters. "X character will never explicitly say how he's feeling" or "the leads have to both win and lose every encounter".
I find establishing writing rules for roleswaps especially important - it's figuring out exactly how the roleswap works. Here are the ones that I find important, and kind of the process:
Decide what is swapped. Is it more of a universal swap, personality swap, backstory swap, chronology swap, or alignment swap? No matter which one you choose, all of these things are probably going to change anyway, but there has to be one central point for each character that guides your decisions. Are you actually swapping the narrative role in the story, or are you just changing it? You have to be really precise and have a very good idea of what exactly is swapped, and it has to be consistent throughout the story. It can't just (just) work on what you'd like to see, it has to be exactly the same between characters.
Decide the point of divergence. Sometimes that point is pretty abstract (She's a teenager in the 90s instead of the 20s). Sometimes it's much more specific, just one moment (He developed his superpowers at this moment instead of that). The point doesn't have to be immediately obvious, but you should know it - I did a backstory swap ages ago, and it seemed like a complete change, but like 150k in I dropped that a character dropped out of the police academy instead of completing it and that her entire life changed from there. If the swap is more abstract, then maybe it's just a series of smaller decisions - character A has these seminal points in his story, and I'm swapping him with character B, so here's what character B did during these seminal points instead, and how it changed him and his narrative.
Decide who the character is. This might be more personal, but for me, I think of the character as...there is a central tenet of them, of who they are as a person, that does not change no matter what. That's three or four traits of who they are, that you will not change, and that's what makes their swapped life their own instead of the OG dude's. But there's a lot of traits and behaviors around that core personality that's the result of their environment, backstory, and experiences. That's what should change. It's about figuring out how these essential traits + what is swapped + the point of divergence = an entirely different character and story. The roleswap you'll end up with will be a combination of all of these things: how the essential aspects of a character mix with what's swapped to create an entirely new environment and set of behaviors, which cause a chain reaction to create something new. As a writer, you sit down and say, "I'm keeping these parts of the character, I'm swapping out those parts, this new mix changes these points in their backstory, this results in this new person".
This is more of a guideline, but it's the most important to me: your characters have to be recognizable as the character. The reader shouldn't go, "this OC is making some weird choices". The reader should go, "I don't know how, because he's the exact opposite of his canon self in every possible way, but somehow he still feels like my favorite character". This is why you isolate those basic traits before changing the rest - so long as your character is still who they are deep inside, then they still feel like that character. And that's the fun of the story. You're selling something insane, and the reader is buying it.
It's a lot of really heavy character work. You have to really understand the characters you're writing - the less I get the original character, the more issues I'm perpetually having. I tend to fly fast and loose with characterizations, but when writing roleswaps I have to refer back to canon and the source material a lot ("In canon he did X thing, with his newly different backstory how would that decision change?"). The more you're rooted in canon, then the funkier and more divergent you can get.
Personally, I like to play a fun little game I call: how exactly opposite can I make this character until he stops feeling like this character? I Sometimes my goal in writing is "how deeply can I ruin this story". This is not a good game and people should not play it. I find that the lazier I get about getting in touch with the canon character, about keeping track of the canon decisions, and about following these guidelines, then the more difficult a story is to write. If you structure a story well then it's easy to write, and roleswaps are pretty easy. Thanks for the question!
#my asks#my writing#ok I have no idea how to politely say this#so ill say it in the tags where the rude words live:#if you only think about fanon characterizations when figuring this stuff out#or if you write a characterization based on their role in the relationship dynamic#then youre not gonna be able to do this stuff well#if you write a good guy as a bad guy then you have to#honestly engage with their flaws and their terrible decisions#you can't just swap one archetype for another#and people work so backwards in characterization that. ajksldfjsadf it's 9am too early for salt#sorry I was thinking about my tma roleswap while writing this and#its giving me tma fandom trauma flashbacks#never been in a fandom so completely uninterested in any of its characters. at all. it was insane.#anyway the way im seeing ppl write vash im getting the impression that#people aren't registering that he's the biggest compulsive liar in anime#he is nonstop lies. all of the time. stamp's closer to deflection but. pure lies this man.#i read ppl writing vash and im like MAN you bought what this guy was selling hard huh#anyway roleswap vash has a bridge to sell you and gaslights to girlboss
75 notes
·
View notes
Text
usami renko refuses to accept that anything is anything but normal including herself. however she's fascinated and attracted by the idea of things that can't be explained, despite this denial. this is the principle by which she goes "no way that's happening. it would violate thermodynamics" to "everyone must know thermodynamics is wrong" in 6 music CDs- she cannot possibly admit to herself that she really really wants things that don't make any sense to be real so fucking badly and she cannot admit the deeper belief that she truly thinks that things that don't make any sense are real. thus she explains shit in the way she does. and thus if merry one day said "hey i think we should destroy reality maybe" she'd instantly agree in her heart but refuse aloud. and that's why every renmerry re-encounter fanwork must include so much hoop-jumping.
#compulsive liar vs. compulsively lying to herself#“who are you calling a nihilist? i'm practically bursting with the zest for life.”#“why- i'm sleeping soundly at night because i'm so excited about what the universe holds.”#<-closest that woman ever gets to telling herself the truth
42 notes
·
View notes
Text
My friend just mentioned to me that my ex best friend who bullied me our entire childhoods up until age 17 and constantly told everyone I was retarded and used my struggling with social cues and stuff to humiliate me in front of people and try to isolate me from having friends other than her is now posting about how she got diagnosed as autistic . Good for her
#MDJSJFJ????#not to invalidate her experience but I spent almost my whole life attached at the hip w her#and never got even a little bit of that impression#she was always just a compulsive liar and super mean and manipulative#and constantly targeted neurodivergent people bc they were easy to manipulate!#anyways hopefully she’s grown as a person since then . I would rather die than ever interact with her again tho
23 notes
·
View notes
Last Seen Blogs

celebritynews01
Celebrity News

mantrustpharma
Mantrust Pharma
canadabrasilresultadobaloncesto
Untitled

simplynotaneggworks
SimplyNotAnEgg_Works

littler3d
QueenRed