#it has to actually make sense given the diagnostic criteria so help me...
Text
The Monster Way was so good ?!!!!!!
#mh spoilers#(in tags)#omg twyla x manny I didnt see that coming but its a cute ship ! theyd go on library dates or something for sure#also toralei had some big moments shes my fave !!#idk what was w deuce getting annoyed w cleo and misunderstanding her but I can really see why they broke up in the past in canon lol#clawdeen becoming wereruler !??#wonder if they didnt give spectra a new outfit bc it would be hard for her to change clothes as a ghost#deuces outfit is so cool some of my in sys partners find that outfit gender and I also think its cool even though I prefer to wear fem#clothes lol#also he has his hair snakes braided like his moms !?#caterina doing that was like .. why but not at all surprising lol#but also Ive seen some fans call her a “narc” which shut the fuck up stop being ableist as someone w npd I will not stand for this#just call her an abuser lol#or a neglectful parent or a villian thats far more in line w how shes portrayed#if you have a genuine headcanon that a character has npd it better not be reasoned by “theyre an abusive shit”#it has to actually make sense given the diagnostic criteria so help me...
2 notes
·
View notes
Text
Even though “support needs” language was created to be a contrast to “functioning” language sometimes I do think the instant it moves outside of the actual autistic community it’s very common for the way people talk about “support needs” to end up being used in a way that sounds exactly like functioning labels. And then it’s like, okay, you’re saying support, but it’s clear the angle you’re coming at this from is like “how disruptive to me personally would this person’s needs be.” And maybe that’s just proof that labels are never infallible? Which makes sense, given that they’re just. Tools for us to use.
Idk. I know it’s important esp for people w high support needs to be able to communicate exactly how different their experiences can be from autistics with lower support needs, bc it really can’t be understated, and ppl with high support needs are so often ignored or overlooked or swept under the rug. And at the same time when it comes to how those terms get used outside of the actual community; ex. within diagnostic criteria; I more and more wish we could start to typify support needs as a spectrum, just like symptoms are a spectrum. “Low - Medium - High” or “Needs Some Support - Needs More Support - Needs Major Support” are metrics that can definitely be helpful and even vital, but sometimes they still feel restrictive and way too simple.
I end up wishing people could have their support needs understood by going through each part of their life it affects, all the different ways they may or may not need help. Social support, sensory support, school support, support with work if they can/do work— even needing live-in care accounts for a really wide range of needs that’s going to look different for every person. Do they need help eating regular meals, help in the bathroom, help with hygiene? Help with emotional regulation and feeling stable and safe? Help with chores, other daily tasks, help with keeping appointments? Help with transportation? There’s so many factors there, so many ways in which someone might need support, and so many ways in which those needs could vary. Giving someone’s support needs a “level” feels like a place to begin but not to end in these discussions, I guess? Because truly every individual person is going to have a different experience, and not just different needs but different methods in which those needs have to be met.
Idk. And ofc I also understand why that language may need to be more simple at times, in order to just get that basic message to anyone bothering to listen— but it also feels like the future of these discussions has to find a way to incorporate the nuance of people’s actual experiences if we really want to see material changes
3 notes
·
View notes
Text
more of a note to self but i had a not great therapy appt today which propelled me to move up my follow-up psychiatrist appt ... my therapist wants to change the diagnosis that's on file for me but i don't agree with it. we ran out of time so next time i told her i wanted to talk to her about 1) how this change of diagnosis would affect the treatment plan and 2) going through the DSM 5 for this diagnosis to better understand what she thinks i've exhibited that fits this criteria and why she thinks this is a good diagnostic fit. if anyone has had to navigate a convo like this, what was it like ? for what it’s worth my therapist is a LCSW (so masters degree + state licensure) and I think I really want a second opinion from my psychiatrist who obvs has done way more schooling / training and has known me much longer as I’ve worked with her since may 2022. The entire time I worked with my psychiatrist, I also saw my previous therapist who never mentioned changing my diagnosis. I’m not here to discredit anyone who has LCSW credentials but I’m just concerned after barely a month of treatment she wants to change things so drastically to an even more severe form of mental illness. She was also very insistent on talking to my psychiatrist (which I saw as a good sign bc I genuinely think it’s good for providers to work together for a more holistic understanding of the patient) but now I am fearful that my therapist may have been adamant about this bc she might want to change my meds to fit this more severe diagnosis….which thinking about it makes me scared of losing my mind (no pun intended) bc I have been on a roller coaster of trying to find a medication + dosage that alleviates symptoms and has side effects I can tolerate.
she did say the diagnosis can be amended etc etc but i was genuinely shocked at what she said and i immediately cried after the appt and had to talk to my sisters bc i feel like it came out of left field and was very unexpected and really destablised my sense of self (ironic since the point of therapy is to help me with my problems not create new ones)
i've only seen this new therapist for about a month (first two sessions had tech difficulties so we only talked for like 20 min and have only had two full 45 min appts so far) and this whole time i've felt like it hasn't been a good fit. (at the first appt when i told her about struggling with some eating disorder behaviours and how i play violin to keep myself occupied and to distract from engaging in the behaviours, she said "oh you could also try sitting on your hands" .......like what ?.....did she mean this to be helpful ? like wow, why didn't i try sitting on my hands before, so simple !)
after each appt i feel more and more misunderstood, i feel like the diagnostic change is rushed and punitive. i've been through therapy before and no other mental health professional (therapist or psychiatrist) has given me this diagnosis. it's so jarring i actually just rang the clinic and asked to see the notes from my previous therapist i started out with when i first moved to nyc (i really clicked with her and i felt genuinely help and seen and understood by her)
anyway now, this week, i have dr appts everyday :(
#i cried bc i feel overwhelmed#i had to type this out and externalise my thoughts bc this therapy appt made me feel crazy (not in a pejorative way)#personal#nyc move
9 notes
·
View notes
Text
daniil dankovsky is autistic and here’s why:
because i’m autistic and i said so
i kid, obviously. what sort of autistic person would i be if i wasn’t read to back up my silly little claim with an overly long post of evidence a total of three people will read? (hi ned hi jordan hi raven :))
i’m aware that this is cringey because adults aren’t supposed to have autism or interests or talk about either of those things, but this is my blog and you are free to block me if the cringe is too much for you.
these are some things i picked out from the DSMV’s diagnostic criteria, found on the CDC website:
deficits in social-emotional reciprocity
reduced sharing of interests, emotions, or affect
abnormal social approach
abnormalities in eye contact and body language
defecits in […] understand[ing] relationships
difficults adjusting behavior to suit various social contexts
repetitive motor movements or speech
rigid thinking patterns
highly restricted, fixated interests that are abnormal in intensity or focus
hyper- or hyporeactivity to sensory input
there’s also some misc. stuff not in the diagnostic criteria (though it may be in the adir or gars-3) i thought was worth noting.
important note from the diagnostic criteria: “symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning”. i’d say that in his case, they do.
spoilers for pathologic classic, pathologic 2, and the marble nest
deficits in social-emotional reciprocity
in bachelor route of classic, daniil
seems completely oblivious to eva making advances toward him, to the point where she complains to him that he’s ignoring her in favor of asking questions about simon.
seems surprised when people mention maria being in love with him, despite outright asking her a couple of times if she’s flirting with him.
not to mention the fact that he asks her that at all.
his inability or resistence to making connections with others is typically considered one of his character flaws. although it is not outright stated in the dsmv criteria, one trait of autism and other neurodivergencies is “having extremely high or extremely low empathy” - and daniil, despite being a doctor, lacks empathy. which is not to say he doesn’t care at all. i think that he does, but is terrible at showing it.
for example, this scene from marble nest:

Sticky: You must feel terrible… right? That’s fine. I forgive you.
You just got confused… Adults always do.
Daniil: Oh yes, adults are always occupied with the most asinine nonsense. Like feeling anxious that a bunch of urchins keep roaming the streets, putting themselves in mortal danger!
daniil clearly cares about sticky’s wellbeing (and the wellbeing of the kids looking after him, though he’s not cognizant that he’s in a coma), but his way of showing it is… kind of by being a jerk. all of which bleeds into the next item on the list
reduced sharing of interests, emotions, or affect
he has no problem sharing his interests, but in both pathologic classic & pathologic 2, daniil speaks with a flat affect - which is to say that he lacks intonation. the words we read him saying may be dramatic or come across as passionate, but the actual voice reading his lines is very monotone, which may contribute to being read as lacking emotion.
and in pathologic 2, he has a voiceline lamenting not telling “her” (eva?) how he felt
in marble nest, he’s teased by the tragedians for being “heartless”:
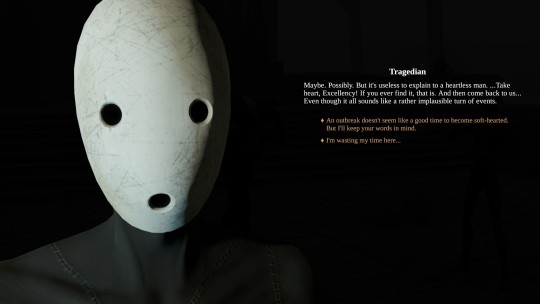
Tragedian: Maybe. Possibly. But it’s useless to explain to a heartless man. …Take heart, Excellency! If you ever find it, that is. And then come back to us… Even though it all sounds like a rather implausible turn of events.
abnormal social approach
daniil has a tendency to say things that are tactless, odd, or just socially inappropriate. i probably don’t need to point out too many examples, as i think it’s fairly obvious - these are the things people love to pick at when it comes to him, but i do have a few in mind. like, for example, from haruspex route in classic:
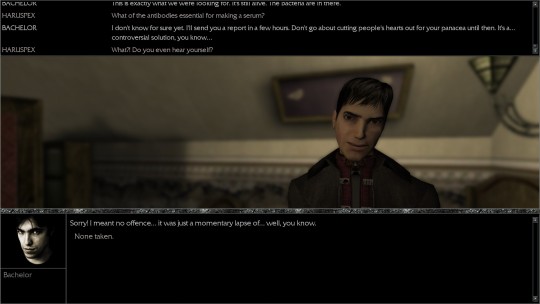
Haruspex: What of the antibodies essential for making a serum?
Bachelor: I don’t know for sure yet, I’ll send you a report in a few hours. Don’t go about cutting people’s hearts out for your panacea until then. It’s a… controversial solution, you know…
Haruspex: What?! Do you even hear yourself?
Bachelor: Sorry! I meant no offence… it was just a momentary lapse of… well, you know.
Haruspex: None taken.
until artemy points out, daniil doesn’t seem to be aware he just said something rude. even with therapy, picking up on social cues doesn’t come naturally to people with autism, so we tend to say things that come across as rude or strange to others without realizing we’ve put them off. we tend to lack a “filter” that tells us when things are or are not appropriate to say. even when we may recognize it, the rules may not make any sense to us. for example, it makes very little sense that allistics favor politeness over honesty.
i think the glaringly obvious abnormal social approach in pathologic 2 is him threatening to hold artemy at gunpoint to get in the house, which is just overkill, but my personal favorite comes on day 7, when he’s complaining about the orders aglaya has given him. artemy stops him to say he doesn’t understand what daniil wants from him, to which daniil replies:
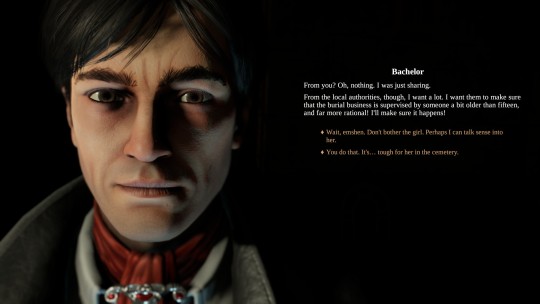
From you? Oh, nothing. I was just sharing.
to daniil, they were just having a normal conversation. but some part of this - his tone or his words or maybe even his body language - didn’t give artemy the impression that this was supposed to be a regular conversation. (we could, in fact, attribute the same idea to artemy here; why didn’t artemy pick up that this was a normal conversation? the reason i count it towards daniil is because artemy doesn’t seem to have this problem with anybody else. for the record: i don’t think artemy is neurotypical either.)
abnormalities in eye contact and body language
it’s hard to get proof of this in video games, but i will say i think it’s very funny that in pathologic 2 daniil’s idle animations are “pacing”, “sitting like he desperately wants to start bouncing his knees but is stopping himself from doing it”, and “standing unnaturally still” - but there you go. i don’t know anything about making gifs, or i’d gif this one specific talk menu idle he does where he holds eye contact for about three seconds, looks away uncomfortably, and then looks back out of the corner of his eyes.
deficits in […] understand[ing] relationships
mostly examples from his route in classic:
when the army arrives, he can claim to block that aglaya, whom he’s known for two days, is his best friend
he seems baffled by the fact that everone is smitten with maria and working with her, and seems equally baffled by the idea that she’s smitten with him
despite eva implying on day two that she is in a relationship with andrey, is completely blindsided by the revelation on day 6, asking him, “How in the world is she ‘your woman’?”
i’d also like to use his sign-off on his letter to artemy, day 2 of the haruspex route - he signs it as “Your friend (hopefully)”. i know i’m not the only autistic person who used to ask people if we were friends or not. pro tip, if you’ve never done this: don’t. it really weirds people out.
difficulties adjusting behavior to suit various social contexts
the fact that he stands out is blatantly obvious even in pathologic 2 and in the haruspex route of classic. people will comment on him being an outsider and mention that they don’t trust him. but you can watch it happen in real time in his route, because he never fully acclimates to the town. he says something about this to aglaya on day 7:
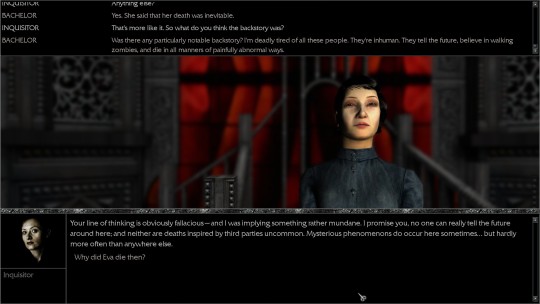
Bachelor: Was there any particularly notable backstory? I’m deadly tired of all these people. They’re inhuman. They tell the future, believe in walking zombies, and die in all manners of painfully abnormal ways.
Inquisitor: Your line of t hinking is obviously falacious - and I was implying something rather mundane. I promise you, no one can really tell the future around here: and neither are deaths inspired by third parties uncommon. Mysterious phenomenons do occur here sometimes… but hardly more often than anywhere else.
actually, there’s an example of him saying something similar to artemy on day 5 in pathologic 2:
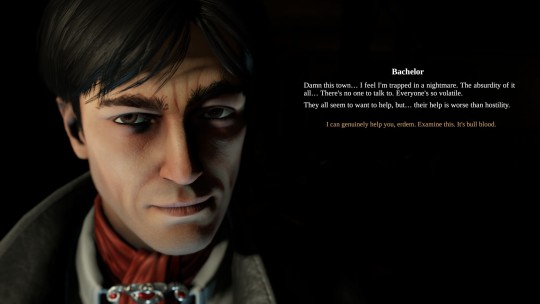
Damn this town… I feel I’m trapped in a nightmare. The absurdity of it all… There’s no one to talk to. Everyone’s so volatile.
They all seem to want to help, but… their help is worse than hostility.
some of this can be explained by the town’s strangeness, but keep in mind that the first instance happens after he’s been there and involved in the ongoing for an entire week, and the second at nearly a week in. clearly he’s struggling to adjust to the changes.
it’s also worth noting that his reason for fleeing the town in the nocturnal ending?

I have no place here anymore.
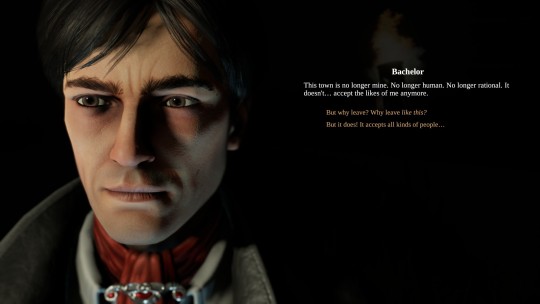
This town is no longer mine. No longer human. No longer rational. It doesn’t… accept the likes of me anymore.
repetitive motor movements or speech
it’s harder to see the motor movements in classic, but remember how i pointed out earlier that he paces? pacing is a form of stimming. murky, who is canonically autistic, can also be found pacing as one of her idle animations. having stock phrases for characters to speak when you come near them already ticks off the box on “repetitive speech”, but that by itself doesn’t really cover what they’re talking about - echolalia.
but you know what this does fit with? “‘quoting’ things(communication is HARD! sometimes we need to take shortcuts and use someone else’s words)“
i’ll get to the more obvious example in a minute - i want to point out something that happens very early in pathologic 2 first. you know how you first meet him and artemy accuses daniil of trying to guilt-trip him by asking if it’s true that isidor would still be alive if artemy had come sooner? keep in mind that he spoke to rubin first. and this is what rubin says, when you get a chance to talk to him:
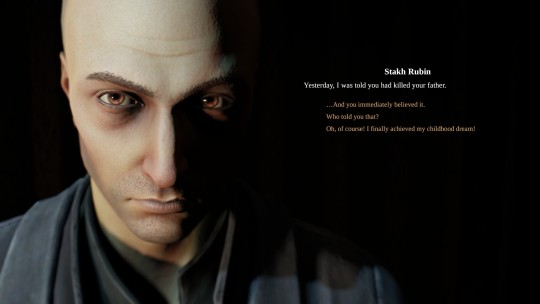
Yesterday, I was told you had killed your father.

That’s not far from the truth, Burakh.
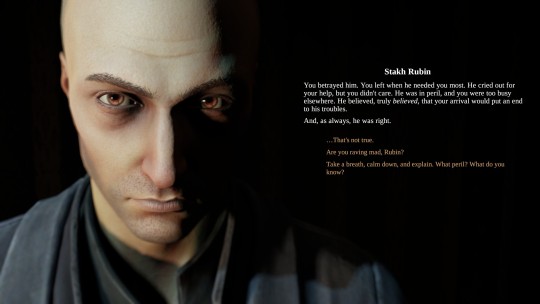
You betrayed him. You left when he needed you most. He cried out for your help, but you didn’t care. He was in peril, and you were too busy elsewhere, He believed, truly believed, that your arrival would put an end to his troubles.
And, as always, he was right.
i’m not saying this was necessarily the game’s intent, but it’s entirely possible daniil is parroting back to artemy exactly what rubin said to him.
now, for what you’re probably expecting in this section: the latin. people love to refer to his use of latin as “random”, so let’s clear that up:
it is not latin daniil has made up. with the exception of latin that is mispelled in the game’s texts, all of them are proverbs or otherwise common sayings. you can find most of them on the wikipedia list of latin phrases, or through a 3-second google search.
he’s a doctor. him having taken latin isn’t anymore strange than a lawyer taking latin. in fact, if you pay attention, artemy also took latin; this is implied when artemy tells him he’s always sucked at it.
his uses of latin actually aren’t random at all. what he says fits the situation, and sometimes is used in place of him having to come up with something to say on his own.
prime example:
Forget it, Burakh. I have a splitting headache. If you have no urgent business, then we’ll talk later. Later, later… Qui non proficit, deficit.
qui non proficit, deficit - he who does not advance, loses ground. in other words, “i’m sorry, but i really do need to keep working.” one of his voice lines.
as for why he doesn’t translate the latin: it probably wouldn’t even occur to him to. these are not obscure sayings. the utopians all have a certain degree of education - what would he need to translate them for?
this bleeds into something that isn’t really mentioned, but that i’ve found i have a lot of trouble with in everyday life. autistic people have a tendency to either overexplain (and then have everyone get mad at you because they feel you’re being condescending) or underexplain (and have everyone get mad at you because you haven’t explained anything). the latin would be a case where it feels like a justified underexplanation. you’ll notice that when it comes to anything scientific, he tends to do the reverse, and overexplain. this also happens in classic, whether artemy has asked him to clarify or not.
rigid thinking patterns
the thing i had marked for this was simply his strict adherence to western medical practices and refusal to acknowledge the supernatural, even when it seems obvious - he has a conversation in his route in classic with yulia about this, and that is in fact how he manages to get to her: by asking saburov if there are any other logical skeptics in town. it should be noted they seem to be breaking with this in pathologic 2, where one of his voicelines is “I’m no positivist. There are things in this world beyond our mundane perception.” i have no idea where they’re planning on going with that.
there’s also a quote floating somewhere around twitter about him having been raised by a military man, and militaries tend to enforce very rigid routines. you could say the same thing of block - who (in classic at least) i also have my suspicions about.
highly restricted, fixated interests that are abnormal in intensity or focus
special interests. the one that should obviously come to mind is thanatology, though i would argue latin if not classics in general is a special interest of his as well - in addition to his usage of latin, he also references pericles in the marble nest and was probably refering to the roman occupation of haruspicy in addition to augurs in the same text. he also makes references to shakespeare more than once in both marble nest and pathologic 2.
hyper- or hyperoreactivity to sensory input
i don’t have much written down for this one but there seem to be several places in classic especially where he asks npcs to stop shouting at him. we don’t really have the privilege to know their volume or how they’re interacting with him, but i think it’s also worth noting that he’s the only one of the healers who wears gloves. in pathologic 2 he’s the only named character i can think of who wears them at all. his thing in the lucid dream about the brain being “a border”? gloves are his border, as is his jacket, which may be worn to cut down on sensory issues.
he will also sometimes seem to “overreact” to the situation at hand - such as in classic, when some dogheads mispeak and say that daniil is going to “sterilize” them, and instead of understanding that they must have mispoken, freaks out over the idea that they think they’re going to be… well… sterilized. or in haruspex route, when his reaction to the inquisitor arriving is to threaten suicide.
miscellaneous
he never goes anywhere without that carpet bag. we don’t see it in pathologic 2, but we do hear about it and he doesn’t let it go for a second in classic - not even in the cutscenes where he’s using the microscope. his bag could be a comfort item.
“getting very attached to things like inanimate objects” could work for the bag - but you know what it actually fits the bill much more obviously? the polyhedron. in the haruspex route he recognizes that it’s a lost cause, but he’s still too attached to it to let it go.
in classic at least, daniil is absolutely terrible at lying. most autistic people either are not good at lying, or feel uncomfortable or anxious with having to lie. when he’s asked by yulia and the kids in the polyhedron to lie to block (for different reasons) he’s clearly uncomfortable with the idea that it’ll work. and when it actually comes time to come up with a way to lie to block about why he needs five rifles, your options are to either buckle and tell him the truth, or simply say that you need them for “self-defense”. block believes that you’re not lying to him, but daniil can’t come up with any embeleshments to explain why he needs what he’s asking for.
Commander: Are you hiding something from me?
Bachelor: No.
he comes across as naive to other characters. in classic, capella has a voiceline saying, “The Bachelor is not smart. Intelligent, yes… but not smart.” in Pathologic 2, Daniil complains that Aglaya takes him for “a useless dreamer”. he’s also easily used by the Kains to fulfill their endgame in classic.
my final, and absolute favorite: he takes things way too literally. autistic people (and adhd people, from my understanding) have a hard time differentiating jokes and sarcasm. so my favorite moment in marble nest is a case of him taking that earlier advice - to “take heart” literally, by bringing the tragedians a literal human heart:
Tragedian: Oh… Excellency. What a sordid sight! Sorry for underestimating you. You definitely do have… how shall I put it… a creative touch. But this is pure madness. You can’t take things so literally!
Daniil: You wanted me to come back to you with an open heart. Well, here I am.
…It looked too fitting to be a coincidence.
your mind map, after this, updates to say “I misunderstood the tragedians.”
conclusion
people don’t stop being autistic with age and i think he’s a good example of what it’s like to be in your late 20s and be autistic. i’m sure i missed things as i haven’t finished haruspex route of classic yet and there may just be some other things he does or says that i missed! if anyone has anything to add they think fits i would love to know, thank you for your time :)
#icarus.txt#autistic daniil dankovsky#daniil dankovsky#pathologic meta#ok to rb but i'm not interest in your ''but he's just weird!'' arguments#please keep in mind that this post is about autism#and that this is written by someone w autism...#popular
323 notes
·
View notes
Note
Hi! I have atypical autism and I’m having trouble at work. I feel like no work place is working out for me because of my diagnosis. I’m uncomfortable around my colleagues, I’m quiet, I don’t know when to speak or what to say etc. I’m sad, mad and frustrated that this ruins every work place for me and I don’t know what job would fit me. I’ve never told my bosses that I have atypical autism and I don’t want to do it either. I want advice on what I should do
this is a great question!
I didn’t know what atypical autism was, but I googled it and it sounds like
they came up with this because they can’t call it asperger’s anymore? “a subthreshold diagnosis, presenting with some symptoms of autism but insufficient to meet criteria for a diagnosis of childhood autism (or autistic disorder). Alternatively, atypical autism can be diagnosed when there is a late onset of symptomatology.” Aka DDNOS, apparently.
From my perspective, it doesn’t sound different from any other autistic experience. FWIW. I think they tend to base their diagnostic labels more on how we seem from the outside than what our experiences really are. just my onion
It sounds like you’re struggling with social anxiety, in that special vicious-cycle kind of way where not knowing how to interact with people makes you more anxious, and that makes it harder to interact with them, which makes you more anxious....?
The nice thing about vicious cycles is that you only have to knock out part of the cycle to make the whole thing fall apart.
Like: if you didn’t feel anxious about not knowing when to speak or what to say, it would be easier to figure out when to speak or what to say. Which, in turn, would give you less reason to feel anxious about it, et cetera.
Or, if you knew what to say to them and how to hit it off, you would have fewer triggers for your anxiety, which would then make it easier to.... you get the idea.
There are a lot of things that help with social anxiety.
I am going to give a shout-out to medication, first of all.
There are a lot of life hacks and therapeutic techniques that help a lot. And for yeeeeeaaaars, I didn’t realize that I really had anxiety, and also, thought that I “should” see if I could manage anything myself before “resorting to” meds.
Turns out, medication saves me a TON of spoons, which I was previously using to “manage” depression, anxiety, and ADHD. You would not BELIEVE how much more energy and just general functionality I had when I finally got my meds right. OMFG.
It can be a pain in the ass to find the right medication, especially if it means first having to find a medical practitioner that can help you and then having to explain the situation.
Sometimes you find something that helps you right away. Sometimes you have to try different things to find something that works well enough. Sometimes you get the fun of “doesn’t work for me AND has bad side effects for me.” (OTOH, when looking at side effects, always remember that you might not get any of the side effects.)
IMHO, the hardest part of finding the right medication is that a lot of practitioners don’t know how to track whether it’s helping you or not. Or whether it’s helping ENOUGH. Like: I got on anxiety meds that were starting to help, but which were making my ADHD meds not work.
I tried a bunch of other things, and finally got Vyvanse to work for my ADHD. But I managed to FORGET that my anxiety meds weren’t doing anything, for a full year, until things got really bad and I was like “wait a minute... these should be helping????” And I did some research, accidentally found a competent psychiatrist, and found that Cymbalta worked for me... but even then, if I hadn’t found decent tools for assessing if it was enough, I would’ve stopped at like half the dose I actually needed to be on.
This post is gonna be long as it is, so I’m gonna reblog to add different tools you can use to gauge what’s working, and which will help medical professionals understand what you’re experiencing. (Because tbh, they’re often just plain ignorant about this shit.)
You do not necessarily have to go to a psychiatrist to get medication for anxiety, social or otherwise! My partner’s OBGYN prescribed him depression meds. My family doctor was willing to prescribe stuff for depression and anxiety, but only if it was something that didn’t potentially interact with ADHD meds.
My chosen brother’s doctor was asking EVERYBODY, after the 2016 election, how they were doing and if they needed depression/anxiety meds. (And they’re in North Carolina!) He had never really thought about it before, and in fact, when he started taking them, his social anxiety got so much better that he was doing shit like going back into the store to tell them they’d given him too much change. He was the one who got me to think about taking them. He had a little kid, and he was like, "I’m doing this for my family.”
Ok, medication aside:
Some kinds of therapy are really good for figuring out how to interact with people. I’ve been learning a lot about different modalities, and I would recommend finding someone who does what’s called “relational therapy” or “relational-cultural therapy.”
Basically, relational therapy is ALL about learning how to interact with people and have better relationships of all kinds. It’s very connected with issues of marginalization: people who are into relational therapy learn about how marginalization, and abuse, affect us and our relationships.
Like, how we can internalize a ton of shame, just from being autistic and being devalued by the people around us. Even just from existing in a world that doesn’t value or understand how we communicate, and how we experience things.
And it’s really good for identifying that stuff, healing from the struggles of trying to interact with people, and learning how to relate to people in a way that works for you.
I found an organization that explains it pretty well (”Are you anxious when it comes to social situations like the workplace?... If we are depressed or anxious, inevitably it can be traced back to tension or breakdowns in relationships, or an inability to connect”), has a blog post in the sidebar called “Signs of Aspergers In Adults - Sound Familiar?” and apparently does therapy globally via Skype.
I have never used them, I don’t know anything about them, I just googled “relational therapy” “online therapist.” (Shockingly, tho, that blog post not only links to one by an actually autistic person, but is very positive about autistic traits. I’m impressed so far. And I’m sure there are other options out there, too.)
Lastly (as far as Things That I Personally Know Work go), I’ve gotten a LOT of recovery around social anxiety, and learned how to build relationships at work, from 12-step programs.
The reason it works for that, as far as I can tell, is:
• It’s a peer-led model, where everyone is equal. (this was huge to me, because I really struggled for a long time with feeling like everyone knew better than I did and had more of a right to talk about anything than I did, and therapy was a tough way to deal with things at that point because I saw the therapist as A Professional who’s In Charge.)
• There’s a lot of emphasis on the fact that the newcomer who just walked into the room has as much of a right to give input in a business meeting, or to volunteer to help out with something that doesn’t require specific experience, or to share what’s going on with them, as anybody else.
• Everybody there has gone through the same stuff as you, and anybody who’s helping you is showing you what worked for them, not what they were taught would work for people. That can be a pretty big difference, especially in terms of being able to relate to them and share personal things with them.
• Working the steps involves a lot of writing about your fears and resentments, and looking at, basically, what has and hasn’t worked for you, and why it hasn’t worked. Really, what you're doing there is seeing where you can reclaim your power. And then you deal with a lot of shame, and get to discover how much you’re like other people, and how much you’re equal to other people, and that you’re a good addition to the world.
• You also connect with your intuition, when working the steps, and develop a better sense of what’s intuition and what’s fear/anxiety. That, and sharing in meetings, REALLY helped me get a sense of what to say to people and get comfortable saying things. (A lot of people shorthand what I’m calling “intuition” as “god,” but it’s very much supposed to be a nonreligious idea of “god.” and IME, it’s basically your intuition, whether your belief system says that’s god talking to you, or a psychological thing, or a mystical force, or what.)
Plus, 12-step stuff is free, which I’m very much in favor of lol. And most 12-step orgs have phone meetings and online meetings, so you don’t even have to go in person if that’s a barrier. (and in a phone meeting, they might not even know you’re there!)
The tricky part can be figuring out which 12-step groups are good in your area and what might work for you. Because they range from Alcoholics Anonymous to, like... what’s the most obscure one I can think of? ARTS Anonymous, I guess. (it’s for artists who are stuck, it’s not saying art is an addiction)
But if you wanted to try 12-step for this, I would say that Emotions Anonymous is really good for dealing with all sorts of emotional and mental health stuff. (and holy shit, they have an app????) Adult Children of Alcoholic and Dysfunctional Families has, iirc, a good book, (as well as all the meetings and whatnot) and most people probably qualify for that. If you have any experience with sexual assault, abuse, harassment, or being cheated on, COSA is good, and you end up working on all your other relationships and emotional stuff along the way.
17 notes
·
View notes
Note
if you could rewrite skam italia season 2 to more accurately represent bpd and its symptoms, what would you change?
The short answer is I wouldn’t really change anything. But the reasons for that require explanation, so buckle in, this is going to be a long one.
I think accuracy is a subjective term when applied to portrayals of mental illness. Because people have very varied experiences. So what would be an accurate portrayal of BPD for me might not necessarily be accurate for someone else. Since the revelation of Nico’s diagnosis and my various posts on the subject, I have had messages from numerous other borderlines. A lot of them – like myself – related to Nico in many aspects. But there are also some who didn’t – or who did in some aspects but not others. The fact of the matter is that it’s not possible to portray a disorder like BPD in a way that is wholly accurate and relatable to everyone in all aspects because people have such varied experiences. If you’re interested in another portrayal of BPD, I recommend watching Crazy Ex-Girlfriend. For me, some aspects are incredibly relatable – sometimes uncomfortably so – but others are not. But that doesn’t mean those aspects are inaccurate. Another portrayal of BPD is the film Girl, Interrupted (one of my absolute favourite films) – however, some people with BPD (myself included) relate less to Winona Ryder’s character, who is the character diagnosed with BPD, and much more to Angelina Jolie’s character. Like I said, it’s subjective.
It’s also important to note that though there are nine diagnostic criteria for Borderline Personality Disorder only five are required for diagnosis. So one person could have almost completely different experiences to another. And even if you do meet all of the same criteria as someone else with BPD your symptoms may manifest in different ways. For this reason people’s experiences with BPD can be incredibly varied. I meet all nine of the diagnostic criteria (it’s like winning a really shit lottery) – so I have experience dealing with all of them, but how I experience them may be very different to the way someone else experiences them. As an example: people deal with fear of abandonment in different ways. Some people self-isolate as a way to avoid abandonment. Some people may appear “clingy” e.g. they will send constant texts and make frequent phonecalls. Some people experience what we call “splitting”. Some people experience all three. Basically, we all have our own individual experiences and there’s no one way to be borderline. Symptoms can manifest in so many different ways.
I’m putting this under a read more to save everyone’s dashboards because it’s quite lengthy. But if it interests you, I’ve listed the DSM-5 diagnostic criteria for BPD and how Nico’s symptoms accurately fit into that.
The nine diagnostic criteria for BPD are quite broad and are as follows:
Frantic efforts to avoid real and imagined abandonment.
A pattern of unstable and intense interpersonal relationships, often characterised by extremes between idealisation and devaluation (also known as “splitting”).
Identity disturbance: Persistently unstable self-image or sense of self.
Impulsive behaviour that is reckless and potentially self-damaging (e.g. overspending, excessive alcohol or drug use, reckless driving, unsafe sex, binge eating, spontaneous decision-making, the list goes on).
Recurrent suicidal behaviour or ideation and/or self-harm.
Emotional instability (intense mood swings) e.g. intense episodic dysphoria, euphoria, irritability, or anxiety that can last from hours to days
Chronic feelings of emptiness and loneliness
Intense anger or difficulty controlling anger
Stress-related paranoia or severe dissociative symptoms (feeling disconnected from the world, or your own body, feelings, thoughts and behaviours)
It’s difficult to know how many of the criteria Nico meets as we have very limited background information to go on. After all, this is Martino’s season. Everything we see of Nico is in relation to Martino. Which makes it even more difficult to portray something like BPD. We have no inside knowledge of Nico’s thought processes, his past behaviours or what led to his diagnosis (hey, Ludo, can we uhhhhh get a Nico season please?). But he has to meet at least five of the above criteria to have been diagnosed. From what we have seen, the five he definitely meets are:
Frantic efforts to avoid real or imagined abandonment (the back-and-forth with Marti, ignoring his texts then telling him he wants to be with him, freezing Marti out after his ill-advised comment on mental illness, going back to Maddi, the flipbook and the antidote, suggesting that he leave and his refusal to let Marti look at him when he was in a depressive state).
Impulsive/reckless behaviour (breaking into the pool at Halloween. Taking his mum’s car and driving to Bracciano. Milan in general.)
Emotional instability (I don’t think I need to give you specific instances here because his emotional instability becomes quite evident in general).
Chronic feelings of emptiness and loneliness (his speech about solitude in Nel Mio Letto explains this feeling perfectly).
Stress-related paranoia or severe dissociative symptoms (Milan, again).
He also shows clear signs of:
A pattern of unstable and intense interpersonal relationships (his parents, Maddalena, probably his friends/the boy he liked from his previous school. But we have limited information on his interpersonal relationships outside of Marti – though that’s unstable for most of the season thus is a sign in itself – so whether there is a distinct pattern of unstable relationships is unclear at this point, but it’s very likely given what information we do have. Whether he experiences splitting or not is unclear, too).
Identity disturbance (when he asks Marti if he should get a haircut and a tux to meet his dad, when he proposes à la Love Actually, when he’s staring at his reflection in the hotel room window, when he’s rapping Earl Sweatshirt and boxing in the bathroom – these could all be signs of an unstable identity, but I wouldn’t categorically define him as having persistent identity disturbance since we don’t know if it is in fact a persistent symptom).
So, Nico meets at least five but very likely seven out of the nine diagnostic criteria. The only two he hasn’t shown any signs of are:
Recurrent suicidal behaviour or ideation and/or self-harm.
Intense anger or difficulty controlling anger
So, to reiterate, accuracy is subjective. Nico’s symptoms were incredibly relatable for me personally. They’re just not the only symptoms and not the only way symptoms can manifest. Like I said, I experience all nine of the diagnostic criteria. So it wasn’t even a 100% accurate portrayal for me because I experience other symptoms too (splitting, anger/rage, suicidal behaviour and self-harm, among others). But I did relate a hell of a lot to the symptoms Nico did experience and the way he experienced them. I’m also incredibly grateful they didn’t focus on the suicidal aspect because there’s a lot of stigma surrounding BPD in regards to suicidal behaviour being manipulative, and if not handled well it might have been counterproductive. It was so important to me to have such a hopeful portrayal for that reason, because we are often portrayed in a terrible light.
I think the main thing that confused people regarding accuracy was Nico’s episode in Milan. Because it looked similar to Even’s manic episode in the OG. Which I understand. But it wasn’t the same thing. Many people with BPD, myself included, experience psychotic symptoms. Psychotic symptoms such as severe paranoia, hallucinations, depersonalisation, derealisation or distortion of beliefs and perceptions aren’t uncommon (there are a bunch of studies on this if you’re really interested, because health professionals are still trying to determine the cause and frequency of psychotic symptoms in BPD patients). They’re generally triggered by stress. I’ve experienced brief episodes of psychosis on and off for years. This is what Nico experienced in Milan (triggered by the stress of his parents and Maddalena trying to control him) – Nico truly believed that he and Marti were the last two people on Earth. To me, his episode looked like severe dissociation leading into brief psychosis – or psychotic symptoms, if you will (episodes of psychosis in BPD tend to be brief). So while I understand that it was confusing, it was, in fact, a fairly accurate portrayal of psychotic symptoms in BPD. I had a far more severe reaction to Nico’s episode than I did to Even’s because I saw so much of myself in him. Would it have been helpful to portray Nico’s psychotic symptoms in a way that wasn’t so similar to Even’s manic episode? Absolutely. But the fact remains that it was accurate and it made sense in the context of the season and the metaphor that Nico got caught up in of him and Marti being the last men on earth. It wasn’t random, it was cleverly interwoven.
Sorry for how long this got, but I felt like to answer this question required some explanation. To summarise, I actually don’t think I would change anything. There’s a reason I relate so much to Niccolò. But I don’t contest that others with BPD might not have found it as accurate a representation as I and others do. That’s absolutely their right. Because symptoms are incredibly varied and we all have our own individual experiences.
88 notes
·
View notes
Text
Congratulations, Me; You’re Slow
Surprise, me! You’re literally slow. As in, your processing speed - the rate at which your brain takes in stimuli and makes sense of it - is below average. Quantitatively. The average is 100. Yours is 94.
Three years ago, I was given a cognitive battery. I’ve had an unusually high number of these in my life. Most people will never have even one. I’ve had four; one to assess for the Gifted and Talented program in kindergarten, one to reassess for the same when I changed school districts, one to assess for ADHD, and yet another, the latest, to assess for the same, as the prior records were lost. ADHD runs in my family, but I seem to have been one of those kids who compensated really, really well. Was I organized? Not even a little. Lose things? Constantly. I procrastinated like a motherfucker, too, but it was usually easy to make up the work in class before it was due. I would drive hard to complete the GT project-based assignments at the last minute, and always did fine. Better than fine, even. Sure, I used to obsessively braid yarn or draw in class, but nobody had any reason to suspect I would have issues with things like maintaining attention or executive function later on. If they did, I never heard about it. Even today, it’s not obvious; people associate a certain flightiness with ADHD and that isn’t me. People associate a lot of things with ADHD that aren’t me. This has been so much of an issue, in fact, that despite meeting diagnostic criteria over and over, as admitted by clinicians, people have been hesitant to give me the diagnosis. The argument deployed tends to be: you have all the symptoms, but you also have chronic depression, which has the same symptoms, so we’ll just go with that one. The underlying rationale, the unspoken answer to “why can’t it be both? they often co-occur” seems to be: you are too articulate and self-aware to have ADHD. It boils down to you’re too smart to be slow.
This is unfair to me, and demonstrably untrue, besides. I recognized this long ago. I am the one who has to figure out some way to compensate for the symptoms. Yes, the symptoms of depression and ADHD overlap (especially if you are depressed for a long time), but the treatment of those symptoms is not the same. I have been in treatment for depression for over ten years. Am I better than I was? Unquestionably so.
Do I function at a level sustainable for an adult not on disability? Can I get places on time? Can I catch a plane without showing up 14 hours early, lest I show up 14 hours late, or at the wrong airport entirely, instead? Do I remember things people told me yesterday? Can I go to Target without the possibility of getting caught up in a weird cognitive trap where I want bananas, but am too guilty to buy them unless I do the rest of my grocery shopping, which I don’t have the mental energy for? Do I remember enough of my meds when I go on trips? Can I stop persistently putting things in places that make no sense, and then having no idea that I’ve done it 15 seconds later? Can I manage an adult’s schedule? Can I remember to pay bills on time? Can I remember what I’ve spent money on in the last week? Can I remember what I ate this morning? Can I hold down a job that is, honestly, below my abilities in many ways?
The answer is, of course, sometimes yes. Distressingly frequently, it is no. Where travel is concerned, it is always no, and somehow, I have managed to show up at the wrong airport entirely more than once.
Yes, I recognize that these are problems all people have, to some degree, at some time in their lives. If people are willing to act on the belief that I am too smart to be slow, why is it that when I account for my concerns and attempt to articulate the impact they have on my life, I am suddenly not self-aware anymore, and am only overreacting to what obviously MUST be the same degree of these problems that other reasonable adults experience? Why am I credible in other areas, but not this one? If I am so smart, why is it assumed that I’ve failed to account for my own emotional bias when gauging the difficulty I am experiencing? Why is it more satisfying to assume that I am not trying hard enough, then it is to accept that a smart, self-aware person may, in fact, have some kind of Brain Problem that, really, there is no logical contraindication to, and much evidence, for? When I do the responsible thing and insistently pursue all reasonable options to address my mental and neurological health, with the goal of being a functional contributor to society, why is this so persistently reduced to a fetish specifically for an ADHD diagnosis? I’m smart when it’s convenient for others, but not when it comes to the ability to draw cause and effect relationships from my own behavior, and make comparisons between those and the behavior of others? If I got treatment that worked, I wouldn’t care what the diagnosis was. Come the fuck on. I’m tired of this.
-----
Anyway. I sat down with the results of that three-year-old cognitive battery. I’ve read the summary before; it’s peppered with lines like
“There is also considerable other evidence in this testing consistent with a diagnosis of ADHD”
“In my experience, some individuals who are very bright are able to compensate for some of their disability”
“this distribution of index scores is very typical of individuals with ADHD”
“Many of the behaviors she describes are certainly typical of individuals who suffer from ADHD. Unfortunately, the coexisting history of chronic major depression and PTSD make that differential diagnosis based on history alone difficult”
When I first read that last year, I was shocked because the therapist who requested the cognitive battery, only expressed surprise that I was “very smart” and said that my “scores were fine.” When I later confronted him after having read the summary myself, he merely admitted that some of my scores were “lower than others”. He never entertained the possibility that I had ADHD, which in an of itself, wouldn’t have been a problem if he’d been willing to just try the treatments for it, since clearly the two industrial-strength doses of antidepressants I was already on, were not cutting it. Alas, he was not, and it wasn’t until after he retired that the issue was addressed again.
Surprisingly, I was not the person who addressed it. When my therapist-MD retired, I needed at least a primary care provider to manage my medications. Since the appointment was for psych med management, I had to fill out a bunch of related intake forms - you likely know the kind. While looking them over, my new doctor peered up at me and asked, “Has anybody ever suggested that you might have ADHD?” I was taken aback by the question and wasn’t sure where to start. Them? Asking me? if I have ADHD? She asked me?
I told her that I’d had two full cognitive batteries done, and that both of them concluded roughly the same thing: yes, all the symptoms are there, no, we do not know if it’s ADHD because there’s too much background noise from other psych issues. Without skipping a beat, she said the most amazing thing to me:
Well, whatever it is, you have the symptoms, so let’s treat them.
God. Why didn’t someone say that years ago? Diagnoses are human constructs; we use them to group symptoms that tend to occur together, when they’re thought to have the same causes. Depression and ADHD have many (but not all) of the same symptoms, but the overlap doesn’t qualify as a diagnosis because the causes are assumed to be different. I think we often forget that diagnoses are containers for commonalities that we use to make talking about medicine easier, not necessarily biological phenomena unto themselves. If you remember that they are containers - a sort of conceptual shorthand - then it follows that if one treatment for a set of symptoms isn’t solving the problem, you ought to try a different treatment often used for the same symptoms, even if the minutiae of diagnosis means you aren’t sure you can apply the diagnosis typically associated with that second treatment*.
I am now on Vyvanse. Does it magically solve my problems? No. Does it help? Yes. I am in a much better position to actually address the bad habits and coping mechanisms someone like me builds up over the years. The notable insomnia should wear off over time, and besides, as a person with an existing sleep disorder, having fucked up sleep isn’t new. It’s a price I’m willing to pay.
-----
Anyway. So I sat down with the results of that three-year-old cognitive battery, because I had to dig them up for my new therapist. Instead of reading the summary, I dug into the raw numbers: the related tests are the Weschler Adult Intelligence Scale IV (WAIS-IV), and the Weschler Memory Scale III (WMS-III). I couldn’t find sufficient guidance on interpreting the WMS-III, so I’ll stick with the WAIS-IV scores:
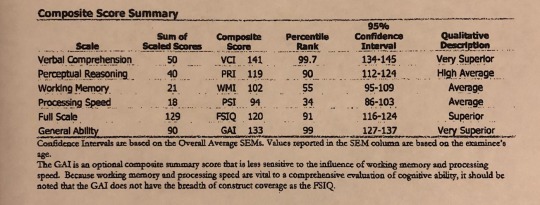
At first inspection, these scores do look “fine”. Anything within 10 points of 100 in either direction qualifies as “average”, even if 100 is “the average”. But on further reading, both in the summary and out:
-Examination of these results reveals considerable significant variability between various functional capacities, with VCI of 141 a full 3 standard deviations above PSI of 94.** Problems with both working memory and processing speed impacted her overall IQ considerably, bringing her Full Scale IQ down to 120 (from 133).
-A significant difference among subtest scores can suggest a problem in the particular skill being tested; this might underlie a learning disability. A significant difference among standard Index Scores might also indicate a learning disability, ADHD
-when I see a difference in IQ scores such that the verbal and nonverbal scores are far superior to the processing speed score, I try to discern what could be causing the discrepancy.
-LD diagnoses are also reliant on score discrepancies. On the WAIS, a gifted individual with ADHD may look like this.
Verbal comprehension - 132
Perceptual Reasoning - 129
Processing Speed - 97
Working memory - 101
Absolute scores aren’t the only diagnostic tool. Relative scores are also important. For example, average scores across the board wouldn’t be indicative of a working memory or processing speed issue, whereas great discrepancies between those parameters and others, is - even if the working memory and processing speed scores themselves are the same in both examples. What I’m saying is, it’s right there. It’s in the numbers. There’s no wiggle room. My old therapist saw these numbers, and not only did he choose not to act on the information, he pointedly refused to do so. If he hadn’t retired, I’d look into suing for malpractice. It’s in the god damn numbers, my dude. I don’t care what you want to call it, the deficit is right. there.
What did I ever do to him? Did he just... not believe ADHD is real? More to the point, did he think I somehow, without knowing the ins and outs of the WAIS-IV, faked the deficits or something? Really, guy, what the hell?
-----
Do I feel bad about being slow? Honestly, no. I might have if I found this out 10 years ago, or in circumstances wherein that reality didn’t perfectly explain aspects of my experience that other people have been prone to downplay, or dismiss entirely. Instead, it’s the closest I can get to scientific verification that I’m not just losing my shit over nothing over here; that something has, in fact, gone awry, and may always have been awry. I couldn’t compensate forever (though the ways I’ve done it are many, and in retrospect, interesting) and now I’m on the other end of it, trying to rebuild. I am, as I like to say, building an exoskeleton - something that will hold me up when my brain insists on faceplanting. I’m just grateful there’s someone out there who isn’t too caught up in the semantic navel-gazing of diagnosis, to help.
*There are obvious exceptions here, such as when the two diagnoses have causes whose treatment is contraindicated in the other diagnosis. This is not the case with depression and ADHD.
** You see that Percentile Rank of 34? That means I performed better than 34 percent of people my age, at least according to the test sample. That’s. Not great.
46 notes
·
View notes
Text
Since I’m getting a little pushback on my post about “Female Hypoactive Sexual Desire Disorder”:
Let’s go. From the website ASHA, the American Sexual Health Association:
There are many potential causes, both physical and psychological.
There are a number of physical conditions associated with HSDD, including breast cancer, diabetes, depression, urinary incontinence, thyroid problems, and multiple sclerosis, among others.
An imbalance of neurotransmitters (chemicals) in the brain may be the cause, as the chemicals that can cause (or inhibit) sexual desire and excitement may be out of balance.
Diminished libido may be a side effect of certain medications, including medications used to treat depression, anxiety and high blood pressure, as well as some medications to treat pain.
Relationship issues may play a role for some women. If there is conflict or a lack of trust in a relationship, women may lose interest in sex with that partner as a result. (Although it should be noted that a woman may experience HSDD and not be in a relationship).
Some psychological conditions may be associated with the development of HSDD, including depression, anxiety and low self-esteem.
So here we have a lot of wiggle words (”may be associated with”, “potential causes”, “may play a role”) and a bit of questionable science (brain chemistry), but what stands out is the enormous variety of reasons that might cause women not to be in the mood for sex for prolonged periods of time. A relationship issue has nothing in common with thyroid problems, for example, which bolsters my argument that this is not a “disorder”. FHSDD implies there’s a discreet thing, singular, rather than what this list expresses, a myriad of potential issues. (The list doesn’t mention other obvious potential causes of not being turned on, such as capitalism and the exhaustion that comes with that, being put in the position of primary caretaker of children and often times adult males, patriarchy generally, which I did in my post.)
Also I found this exact same list, over and over, in various sources, but interestingly the actual diagnostic criteria specifically excludes medications and other medical conditions. In other words, you can totally be experiencing an utter lack of sexual and physical desire and experience distress because of it, but your medical conditions or medications are considered the cause, not the vague “Female Hypodermicalogical Blah Blah”.)
HSDD is treatable and can be manageable, so the first step if you are concerned about a lack of interest in sex is to talk to a healthcare provider to see what options are available. The provider may ask a series of questions called the Decreased Sexual Desire Screener (DSDS) to help diagnose HSDD. The first four questions are:
In the past, was your level of sexual desire/interest good and satisfying to you?
Has there been a decrease in your level of sexual desire/interest?
Are you bothered by your decreased level of sexual desire/interest?
Would you like your level of sexual desire/interest to increase?
If a woman answers ‘no’ to any of these questions, she likely will not be diagnosed with HSDD. If she answers ‘yes’ to these, she will also be asked about other factors that may be contributing to her low desire, including physical and mental health conditions, recent childbirth, her relationship with her partner, her level of stress and fatigue, and other issues.
Treatment may include sex therapy or counseling, alone or with a woman’s partner, to address any mental health or relationship issues that may be present. Medications may be evaluated as contributing factors, and underlying medical conditions may be addressed.
Again, this makes it very clear there is no such thing as FHSDD. There are a whole slew of issues women have. Men have some of these problems too, but generally speaking when you start talking about male sexual desire the bent is not to assume he is “frigid”, it’s to talk about “performance”. The reason for that is to boost sales of overly prescribed drugs like Viagra, which is driven less by the fact some men with say high blood pressure, for example, have a difficult time getting it up, and more about getting healthy men anxious. Every dude, no matter how turned on and healthy he is, can have what seems to him to be a sudden catastrophic fail. Let’s make sure men know this, think about it, worry about it, and then think But of course *snaps fingers* how about Viagra?! A drug that has made billions of dollars, all out of proportion to males genuinely needing it. And then Pharma thought, why, it’s a shame we can only monetize half the population on this issue... *snaps fingers*
Let me lay this article from Healthline on ya, if you think this isn’t basically yet another way in which women are being told we are inadequate and broken for being perfectly normal:
Hypoactive sexual desire disorder (HSDD), now known as female sexual interest/arousal disorder, is a sexual dysfunction that causes a lowered sex drive in women.
Female SEXUAL INTEREST/AROUSAL DISORDER oh my. You are experiencing less interest in sex than your partner? You don’t find yourself easily aroused? Read on!
Many women will pass off the symptoms of HSDD as the inevitable effects of aging or changes in their body.
If your sex drive is affecting your quality of life, it may be time to talk to your doctor.
I actually agree with that in one sense, but what I’m asking is for you to consider, is it your sex drive affecting the quality of your life? Or is your sex drive being AFFECTED BY the quality of your life. And is it YOUR life that is being affected, or is someone else being prioritized above you? Like say a dude? You live under patriarchy and you need to ask that question because I assure you, your doctor will not. There’s no money in it.
While it’s healthy for sexual desire to fluctuate, a woman with HSDD will usually experience a lack of sexual desire for six months or more.
If changes in sexual desire are so extreme that it’s affected your relationships or self-esteem, it could be HSDD.
Symptoms associated with HSDD include:
little to no interest in sexual activity
few to no sexual thoughts or fantasies
disinterest in initiating sex
difficulty getting pleasure from sex
lack of pleasurable sensations when the genitals are stimulated
How do doctors diagnose HSDD?
Unlike other medical conditions, there is no specific test to diagnose HSDD. Yet, there are a few methods used by doctors to diagnose the condition.
Start by telling your doctor about your symptoms. Your doctor may ask questions about how your low sex drive is impacting your well-being.
Your doctor will try to identify an underlying cause for the condition. These causes could be physical, emotional, or a combination.
Physical causes of HSDD can include:
arthritis
coronary artery disease
diabetes
decreased estrogen or testosterone levels
hormonal changes during or after pregnancy
fatigue or exhaustion due to a grueling work, family, or school schedule
taking certain medications that affect sex drive
Again, according to the actual diagnostic criteria, those things aren’t supposed to be considered. Yet here it is. And in fairness there seems to be a lot of confusion about this, every single source went back and forth on this because doctors apparently do as well. Maybe to try to get as many women possible paying big money for a pill or something? Who knows.
Emotional causes of HSDD include:
a history of anxiety, depression, or low self-esteem
a history of sexual abuse {??????}
trust issues with a sexual partner {??????}
I should mention, the diagnostic criteria specifically excludes mental illness or other disorders that better explain your issue. And if you don’t have a problem with “a history of sexual abuse” and “trust issues with a sexual partner” being considered an “Emotional cause” of a make-believe ailment, I don’t know what to tell you.
Your doctor may also conduct a pelvic exam to identify any changes that might have affected your sexual desire. A blood test to check for affected hormone levels might be performed, as well.
However, sometimes there is no specific underlying cause for HSDD. This does not mean that HSDD cannot be treated.
Am I making my point now? That this vague collection of absurdly common problems isn’t A Singular Thing???
I’m gonna skip to the payoff and point of pretty much all of these articles, since you can follow the link and read the whole thing if you’re interested:
Another treatment option is the FDA-approved pill flibanserin (Addyi). This medication has been shown to boost sex drive in women with low sexual desire.
However, the drug is not for everyone; side effects include hypotension (low blood pressure), fainting, and dizziness.
Lifestyle changes could also relieve stress and help improve a woman’s libido. These include:
exercising regularly
setting aside time for intimacy
sexual experimentation (such as different positions, role-playing, or sex toys)
avoiding substances that affect sexual desire, like tobacco and alcohol
practicing stress-relieving techniques, such as mindfulness-based interventions
Don’t underestimate the effect a decreased sexual desire can have on your well-being. If you feel symptoms of HSDD have impacted your quality of life, talk to your doctor. There are treatment options available.
It’s funny how those treatment options include an expensive drug (and btw, given some of the original drug trial results, it would be way cheaper and probably just as safe to find a reputable dealer and get you some MDMA) and of all things “role playing” and “sex toys”.
For kicks, here’s a spin through the not terrible Wikipedia article. The highlights:
In the DSM-5, HSDD was split into male hypoactive sexual desire disorder[3] and female sexual interest/arousal disorder.[4] It was first included in the DSM-III under the name inhibited sexual desire disorder,[5] but the name was changed in the DSM-III-R. Other terms used to describe the phenomenon include sexual aversion and sexual apathy.[1] More informal or colloquial terms are frigidity and frigidness.[6]
Low sexual desire alone is not equivalent to HSDD because of the requirement in HSDD that the low sexual desire causes marked distress and interpersonal difficulty and because of the requirement that the low desire is not better accounted for by another disorder in the DSM or by a general medical problem. It is therefore difficult to say exactly what causes HSDD.
And this is my favorite, because it really displays the gendered ideas behind this bullshit:
In the DSM-5, male hypoactive sexual desire disorder is characterized by "persistently or recurrently deficient (or absent) sexual/erotic thoughts or fantasies and desire for sexual activity", as judged by a clinician with consideration for the patient's age and cultural context.[3] Female sexual interest/arousal disorder is defined as a "lack of, or significantly reduced, sexual interest/arousal", manifesting as at least three of the following symptoms: no or little interest in sexual activity, no or few sexual thoughts, no or few attempts to initiate sexual activity or respond to partner's initiation, no or little sexual pleasure/excitement in 75–100% of sexual experiences, no or little sexual interest in internal or external erotic stimuli, and no or few genital/nongenital sensations in 75–100% of sexual experiences.[4] (Bolding is mine omfg.)
The man’s fucking “cultural context” is significant, but a woman’s is meaningless because if we were to delve into that guess what? WE WOULD BE BACK AT MY ORIGINAL POST ON THIS SUBJECT, WOULDN’T WE, GYNS!!!
And that’s why I am now going to double down and repeat my original assertion:
There is no such thing as Female Hypoactive Sexual Desire Disorder.
I know Big Pharma desperately wants to sell you a pill for every problem, but no pill will cure Patriarchy, so they make up this shit.
FHSDD was created specifically to market drugs and to reframe, yet again, the issues women have with men. To medicalize Patriarchy. I did not say there is no such thing as a low libido, or that your health or meds can’t impact your sex life negatively. Literally no one says that. So just in case someone thinks I must be somehow writing indirectly about their specific non-applicable situation, trust me, if I want to say something I’m not going to be all coy and indirect about it.
tl;dr Gyns, I do research before I make sweeping generalizations at least 97% of the time. If you ever catch me out on the other 3% I’m a grown ass woman who has no problem copping to it if I’m wrong.
1 note
·
View note
Text
On Consciousness
I am finding this life to be less convincing. Inconsistencies in the matrix-esc life grid in which I am living daily have again reared their heads as I have taken the time to care for myself physically and mentally. The more care I give to myself, the more glaring these inconsistencies become. Time is jerky, so to speak. Space is not as consistent as it used to be. Beings are duplicated. I’m sure beings are always duplicated, however when I am in my usual state of unawareness I simply do not notice. It is like the background of a cartoon during a driving scene. It may repeat, but it doesn’t change the plot so even if one notices one does not point it out.
Faces are appearing more peculiar each day. The human figure remains the same, though I do feel that the organs have been somewhat shifted about as compared to what I remember in my youth. I have noticed more exaggerated faces on the common-folk, living caricatures in live action. They always seem to make eye contact with me, even if some only for a moment. It’s like they know that I know. I watch them filing in and out of aisles at convenience stores. They are piloting motor vehicles about the city streets. Are they programmed automations or are these sentient beings as well?
It is becoming more difficult to discern as I age. I am left feeling empty after even the most engaging of conversations with these people. I suppose we can call them people. They are certainly fitting all of the diagnostic criteria from my standpoint, yet, something is off. This city feels different to me than it did last year. Literally one year ago things started changing. I started noticing little inconsistencies. People called them Mandela effects on youtube. This was, of course, named after the late Nelson Mandela. There is apparently a large group of people who distinctly remember Mandela dying in prison in the 90s, although current history does not support that claim. People swear they remember the news casts and even the footage of a funeral.
How could such a mass group of people have mis-rememberings which are identical? I suppose that question crossed my mind and re-enforced the feelings I was having with my own environment. I had always felt a little different than everyone else. Of course, I think we all do. We are all egocentric. We are the center of our own universe. We see life through our own filter. But for me, it feels deeper than that. It is almost as if this reality is designed specifically for me and my life’s experience. Every nuance. Every intricate detail here only for me to experience. But again, I must wonder, are the other seemingly sentient beings in my environment sentient? If not, if they are simply artificial intelligence in my environment for my own life experience then how can I take them seriously.
The Buddhist philosophy seems to feel that all conscious life is indeed sentient and therefore is experiencing the same reality as all of the other life. Also, it is believed that not only are these conscious beings experiencing life, but the fact that they are conscious is creating the existence which they experience. This seems to be supported by recent and not-so recent findings in the field of quantum mechanics. If that is the case, that conscious beings both create and experience their own reality, then the hive-mind that is the collective consciousness is all that we really are. If that is the case then, as I believe I have once read, if everyone were to start believing something completely different, reality would change. This could account for some of these previously mentioned Mandela effects.
It would take but a simple majority vote so to speak. That would alter the entire face of reality. Though physics does point to this being are reality, why are people so apprehensive to believe it? Why are they so quick to dismiss this most amazing quality of our universe? We certainly accept the laws of Isaac Newton because they are practical, though they have been shown to be rudimentary and antiquated in the later work of relativity and quantum mechanics. We are creatures who are bamboozled by our senses. We are victims of our own filter. We believe reality is a certain way because that is the way we perceive it on the surface.
Now, back to my personal reality, I am for sure seeing glaring inconsistencies in my day to day perception. When I am adamant and aware of my surroundings it is much more obvious. It is further enhanced by physical activity, healthy diet, abstaining from alcohol and processed foods, and meditation. There are the blank stares and slacked jaws. The zombie masses surround me in public. Seemingly going about their day-to-day routines. Do they even have a clue or are they just executing programmed commands?
I am also led to question even those closest to me. I hear their conversations but am not sure what to make of it. They appear to have insight into this world and even into my own life. I can’t help but wonder if they are simply programmed to give me subtle hints as to what to expect from my environment. They may simple be at my disposal to learn and draw information from. Even if they do have free will, they are leading their own self-serving lives and that makes truly understanding them a bit of a challenge. They may be immersed in a totally individual reality from a sense of their own perception which would render my reality meaningless to them. Programmed or not, I see no true way to connect with these foreign objects dressed up like friends and family.
I have often exchanged salutations in passing and felt the cold empty stare of artificial intelligence, however I fully acknowledge that this could be my biased perception. The dead handshake of a stranger could simply be an unawake passerby on his own personal conquest. “Good morning,” could have exited his vocal cords in my reality when he actually spoke “I’m disgusted” in his experience. I will never have a way to know. It is not measurable or observable. I can never put on the senses of another human being and submerge myself into his world.
All of these thoughts aside, let us pretend that things are strictly as they seem. That our internal world is just the processing of biochemistry and electrical impulses. That our internal world is meaningless and invalid. That the only true reality is extrinsic to the human brain and that our brain simply gives us the senses to experience the true reality. In this thought experiment we have a universe in front of us, unchanging whether or not we are in it. That is the classical understanding of life. We are simply fish in a bowl. If we remove the fish, the bowl and other contents continue to exist.
The problem with measuring such a thing is that in order to measure it one must be present. In being present one is unable to remove himself in order to measure the consequences of him being gone. The only true way to remove oneself is death, but in death one is unable to perform the experiment. It is futile to even consider.
I have heard others make the argument that surely the universe exists dependent of consciousness because people die all of the time. That is a completely invalid argument because as mentioned above, the other people in one’s individual reality need not be sentient at all. They could be elaborately conceived artificial intelligence. That is to say that the other participants only exist for the use of the observer. The observer being self.
If the universe does not exist independent of self and is solely a construct of the mind, the implications could be damning to all other belief systems. If we are creating our own reality, either alone, or in conjunction with other sentient beings, then we have created everything including religion and morality. How can anything be valid if it can change based on the minds creation? Change must, in this reality, be the only constant. There is but one law and that is the law of consciousness creates reality. Because we are perceiving reality through this very same consciousness, we would understand history to be unchanged even as we are re-writing it. We could be re-writing our own memories simultaneously.
The likelihood appears to be that we are a consequence of our collective consequence. Many have long called this field or plane of energy Akashia. This Akashic field is theorized to be vibrating energy from which our reality manifests. The theory may be taken further as some believe that consciousness is a result of our brain tuning to perceive this Akashic field like a radio receiver receives electromagnetic energy. Our brains can then transcribe and translate this energy into sensation. This is currently not measurable, and I am not aware of an experiment being proposed to measure it at this time. The thought, however, is fascinating.
If we are indeed connected deeply at the level of consciousness as sentient beings, then we certainly have much more in common than we have been conditioned to believe. Extra sensory perception, dreams, thoughts, and every other facet of the conscious and unconscious mind becomes a little more intriguing as we could already be sharing with one another and using our collective consciousness to shape this reality without even being aware.
This also brings into question the consciousness of other species. If other species are sentient, it would point to the fact that human beings are not exclusive in this collective consciousness effort. We would have the same influence as our feline and canine brethren for instance. I have often questioned the validity of the religious belief that ‘animals’ are on this planet as a God given resource for man. It seems far more likely that we are all simply in the same boat and deserve equal respect.
From our best approximation man has climbed the evolutionary ladder and is now in a role of apex predator on Earth. This is according to Darwin’s theory, which is by the way, one of the most consistent scientific theories we have developed to date. In this role man has learned to modify and dominate his environment. This has, of course, led to a lack of balance in the ecosystem. One could argue that this is natural evolution. What is unnatural after all? In this scenario man has naturally evolved his insight and the use of tools in order to change his environment. Thus, changing the environment then evolving to it with time and continuing the cycle is all natural.
As we continue to change and adapt to the environment that we change physically and with our consciousness, I question our fate as a species. Is it all in my head? Is it all in your head? I have no answers at this time, only questions. Is the species even real? Who knows. It doesn’t even matter to me. My experience as a human being has been a mixed one. I have run the gamut of emotions this month alone. I have been proud. I have been ashamed. I have failed. I have succeeded. I continue to exist, and I don’t know why. I haven’t a single answer this time. I continue to open my eyes in the morning after a night filled with dreams. The dreams feel just as valid as my reality only a little sweeter. Am I wrong for longing to stay in the dream world? Is my inner-self truly less valid than this extrinsic reality you are all caught up in?
It would seem that the answers all lie within. There is nothing more to add to myself and nothing to take away. I am simply to discover what is already there. I must overturn a rock in my minds empty creek bed to find what I didn’t know I was seeking all along. I must turn to the inside via meditation, prayer, and sleep. I know to an outsider it appears as though I am doing nothing. I appear stagnant and lifeless. I can assure you friends, I am in deep thought. I am digging. I am searching. I am forever longing for something. I know it is a lonely path, but I am prepared to take the journey.
2 notes
·
View notes
Text
once again making a post exploring why the state of the dialogue around mental health tends to be so... overwhelmingly bad, giving specific respect to eating disorders. buckle in because this one is going to be a galaxy brained one.
let’s start out with a very edgy question. and don’t write me off until you give me some time to set my premise up a little bit lol: is being a fascist a mental disorder?
stay with me here: a mental illness is defined by an abnormal element of cognitive behavior which effects your behavior to the point where you can’t function well in society. i’m generalizing a bit here but that’s what the gist of it tends to be. having observed online fascists and interacting with a few back during the Dark Days of the internet where they would just dogpile random people, it’s definitely at least correlative to certain types of irrational thinking. it certainly affects one’s functionality in society. after all, there are personality disorders where some of the diagnostic criteria is lack of empathy for other people.
so what if that lack of empathy that you have is not dictated by your cognitive capacity, but by the political biases you hold? is it possible that a person who is “mentally normal” could exhibit all the tendencies of someone with a personality disorder, without actually having a personality disorder themselves, because the political biases they’ve adopted have given them a pretext to act in a way as if they had that personality disorder?
i think questions like this are really interesting because, if anything, they reveal inherent subjectivity of diagnosis criteria. is there a meaningful difference? I genuinely don’t know. i know there’s a difference in that the personality disorder is theoretically always going to deal with some version of this, meanwhile a person who behaves this way because of their political biases could be educated out of it.
how many people have you met who behave completely irrationally, but are probably neurotypical in a medical sense? the medical diagnosis doesn’t fully encompass the full range for irrational human behavior. it’s obviously a lot more complicated than that. and the way we talk about this stuff might make it more difficult to deal with some internal issues, whether or not we’re diagnosed with something.
foucault writes on this – the medicalization of mental illness has been disruptive in, among other respects, the fact that it essentializes characteristics which we ascribe to mental illness, even if they don’t necessarily come from mental illness. the le reddit atheist version of this argument is that a person who believes that god speaks to them in their sleep may just be a christian, but a person who believes a dead relative is talking to them in their sleep might be diagnosed with schizophrenia. the only difference functionally between these two things is that there’s so much cultural baggage to legitimize the former example that this is a more acceptable thing that one may experience. and i’m not saying this is illegitimate. being given a cultural pretext for something that would otherwise be considered irrational isn’t necessarily unreasonable. a lot of the etiquette we have in our day to day lives is pretty arbitrary – society legitimizes some behavior and that makes it more acceptable to engage in it.
and the point i’m getting at here is that by medicalizing mental illness, we drew boundaries around elements of human behavior that are omnipresent in all people, therefore, by implication we distinguish by that which is medicalized and that which is not and thus denied ourselves the perceived value of being introspective about that non-medicalized component. that’s not to say that there’s no such thing as autism or whatever, but the categories reaffirm a degree of essentialization and that could be a negative where it concerns helping people who could use the help and people who don’t need it as badly but could use some introspection.
you produce the category, which produces the discourse around the category, which reaffirms the existence of the category. the category is born in the discourse that surrounds its birth. you can make a version of this argument for a lot of stuff – gender, race, etc.
there’s kind of a whirlpool effect with a lot of these diagnoses as well, where as soon as you create a term, other things adjacent to it get described as it. the more nuanced the language around mental disorders becomes, the more boxes you have to put people in. and i’m simplifying a little bit here but this happens pretty often – basically a doctor will be like “hey, I know why women are crazy. it’s because of hysteria. they need to nut or something.” and then everywhere, all across the country will be like “oh my god, that’s why my wife was angry that i didn’t give her a birthday gift. it’s because of hysteria!” when the category is created then everything becomes attributed to it. then all adjacent behavior is fair game to attributing to it, and the category seems all the more important because you’ve done that.
you have two competing problems here – first problem here being that human brains are really, really complicated and a full understanding of what afflicts a person mentally, to be holistic, has to involve a lot of analysis, and the other problem is that there are 8 billion people on the planet and the medical field needs to move quickly. so it isn’t really pragmatic to normalize a system where all people get medical assistance for free (which is what i want) and where people also get hour long psychiatric appointments every week by multiple doctors or whatever. unless you wanna spend 80% of the GDP on medical facilities, they need to be a bit expedited. and that’s fine sometimes because not every medical professional needs to be your shoulder to cry on, except for your therapist, but therapy is different than psychiatry.
the categorical ascriptions tend to be more useful here when you’re talking about stuff that’s to be dealt with through psychiatry. when you’re talking about something that can be fixed with chemicals, i think it’s acceptable to engage in this kind of categorization because it redounds to the most efficacy. in other respects, it can get a little bit more murky. generally, for the field of psychiatry i tend to feel that the categories are quite helpful, meanwhile with therapy... i’ve heard mixed results. and there’s also almost never a clear line between what can and can’t be fixed with chemicals.
but, like, by distinguishing between the medicalized and non-medicalized elements of human psychological behavior, we implicitly say “when there’s something wrong with a human brain, we name the condition and doctors and medicine deal with it.” the problem with this idea is that, well, can you tell me the difference between a person with autism and a person without autism? i know which conditions tend to correspond to autism, but is it possible to draw an actual hard line? there can’t be a hard line. it’s called a spectrum for a reason. there are also conditions people can have that tend to be indicative of autism but not get diagnosed with it. a person can be really sensitive to some sensory cues but not otherwise indicate such behavior. there’s so much variance.
in a way, don’t you feel as though the term “autism” has become kind of a catch-all designation for people who exhibit abnormal behavior in a certain range? but a lot of the elements of abnormality we’re referring to here are at least informed by cultural bias, to a certain extent. it’s not to say there’s no internal element to autism but part of it is like this. i’m only saying that people have gotten worse with developing the processes to identify problems with their thoughts when it doesn’t explicitly fit within the diagnosis of a mental illness.
so i think i’ve laid enough groundwork down to argue my point. but the way people talk about eating disorders on the internet of this whole domino effect of adjacent behaviors is a really potent example of how this can totally derail the entire train. and this happens because eating disorders have a lot of adjacent behaviors attached to it. obviously restrictive eating is an adjacent behavior. so is exercise. so is body dissatisfaction. so is emotional eating. so are things like intermittent fasting and logging food. and, to be honest, you’d be hard pressed to find someone who hasn’t had an experience with at least one of these things.
an extreme version of this plays out in an argument fat liberation and HAES circles will make sometimes that all of this adjacent behavior is disordered. and i think the fact that people generally can’t ask difficult questions without easy answers when talking about mental health. and i honestly can’t think of another place where it’s been equally destructive to how we understand mental health as it has been with eating disorders.
so is intermittent fasting an eating disorder? idunno dude, is nazism a mental illness?
1 note
·
View note
Note
Also, because they didn’t have a disorder in mind, it gives fans all the freedom in the world to theorize and write about. I have seen stories where he has PTSD, schizophrenia, depression, the list goes on and on. So even if I do think I have found his disorder(s) I still have to remain grateful that they did that. Heck, one of your previous stories gave me the biggest “aww” moment when you said he had a emotional support hamster named slushie. You can’t do that with the problems I listed.
Yeah, I like this aspect to a point, because I’ve read those stories too, and a lot of the time, they trouble me a lot. So I guess I’ll talk about diagnosis in fanfiction (briefly, because I need to be writing my fanfiction). This is just general stuff, not like, aimed at you specifically Anon.
1. If you choose to diagnose him with something and have that be like… part of the plot DO YOUR RESEARCH if it isn’t a disorder you personally have (and even if it is, because you might come across some interesting stuff that helps you character build). I read something (I think it was a headcanon thing) about JD having schizophrenia and it was literally just… “His mom talks to him and tells him to do stuff”. Which is… not a personality, and not really authentic to what schizophrenia actually is. I’m not trying to attack this person, there’s an interesting idea here, but more reading could have made a good idea into a fascinating story, with a little more development. My advice is to look for case studies and blogs from people who are actually living with a disorder. DO NOT COPY SOMEONE’S LIFE STORY, but you can borrow elements, or just use it for your own edification.
2. There is strength in not labeling things. I’ve rarely given JD a diagnosed disorder in any of my fics. In HoW, JD mentions his therapist and that he speaks to her regularly, and that he has a support animal, but those are treatments and coping mechanisms for A LOT of disorders, so I leave room for interpretation. He only mentions PTSD by name, and that’s something that makes sense for him to have based on plot elements from the first story, and it’s rarely referenced. It’s not his personality, it’s just a challenge he lives with. H&H has a little more focus on JD’s psychology, but I still never had him say “I have a panic disorder” because a. he might not even know that or b. he might not want to share that or c. he might not care. Some people don’t find labeling their illness to be productive, so they don’t. A good therapist respects that.
So yeah, do your research and think really hard about why you feel the need to add that label. Not every story has to not name names when it comes to mental illnesses, but make sure it makes sense to have that in there. Also, make sure you’re writing characters, not walking DSM diagnostic criteria. I could write more, but I think I’ll leave it there for now.
#ask scout#ask me anything#Heathers Psychology#anon#I know that you didn't ask for this#and I'm sorry I attached it to your ask#but you got me thinking friend#fanfic#heathers
8 notes
·
View notes
Text
What To Consider When You’re Considering A Career in Psychology
Your Long Term Goals
The first question you should ask yourself is, are my long-term goals aligned with a career in psychology?
Take some time to really think about what you want to do as a career. Not what you want to be – what you want to do. How do you imagine your daily work life? What kinds of tasks do you want to do? What kind of setting do you want to work in? Who do you want to interact with (if anyone)? What kind of things would make you miserable in a job? Would you hate to have to be somewhere every day at 8am, or would you hate receiving 11pm emails or phone calls from your team? Do you like doing long-term projects or would you prefer to be truly “done” at the end of your work day? Do you want leadership roles, and if so, what kind? How much money do you want to make? Are there accommodations you might want or need?
If you’re like me (a lover of organization and lists and planning), then you might want to make some kind of document to organize what you want and what you don’t want. You might want to prioritize them- maybe “working with kids in the foster system” is a necessity but “never being on-call” is a want but not an absolute need. However you want to think about your goals, get a good sense of them, and then compare them to existing sorts of jobs and responsibilities in psychology. (See my “what is a clinical psychologist and how do I become one” post here).
The positive thing here is that careers in psychology are incredibly varied, so you are likely to find paths that will fit your long-term goals (assuming you are interested in psychology, mental health, human services, social sciences, etc., in general). However- one of the pitfalls I have seen a number of people fall into when pursuing psychology is that the position or path they had in mind isn’t actually a great fit for them. So here is a short list of examples where a person’s goals don’t align with their chosen path:
A person who wants a clinical position but doesn’t want to do paperwork or doesn’t want to have interactions with other people.
A person who wants to have their own private practice but having a steady and good income is a necessity.
A person who wants to create change in mental health systems but doesn’t want a leadership role.
A person who wants to work with a high needs or high risk group but doesn’t want to work nights or weekends or be on call.
A person who wants to do research but also wants to work for themselves.
I can’t possibly list all the potential matches or mismatches here, so one way to understand what it really means to pursue your long-term goals is to find someone who has the kind of position you want, and ask them lots of questions to see whether the position is really a good fit for you.
Some of these mismatches are negotiable as long as you are flexible- so with the #2 example, a person might choose to get a clinical job with some kind of agency to have a steady income while simultaneously building their private practice. I’m going to talk more about flexibility below, but in short- being as flexible as possible with the specifics can help you achieve the big picture parts of your goals.
Your Personal Qualities
The second question to ask yourself is,
are my personal qualities a good fit with the psychology field in general and my chosen path in particular?
This is not a question of whether you are “good enough” for psychology. We all have strengths and weaknesses and neutral qualities, and those qualities align better with some paths than others. Psychology is a great fit for me, because I love nuance and complicated questions, have a lot of resilience and perseverance, have empathy but am good at remaining objective, am very calm in a crisis, and am willing to put up with a certain amount of administrative and other bullshit in order to do the things I enjoy. Medicine on the other hand, would not have been a good fit, because I am terrible at memorization, get incredibly nauseous when seeing medical events (let alone being a part of them!), would never be able to keep to a 15 or 20 minute appointment, and would not physically be able to do residency given the huge sleep deprivation residents experience.
So think about your personality traits, your behavioral habits, your preferences, your physical needs, your learning style- all of it, and then again, compare to what is typically needed for psychologists. Here’s an incomplete list:
Critical thinking skills
Social skills
Communication skills
Ability to take criticism
Ability to assess your skills and weaknesses
Distress tolerance skills
Emotion regulation skills
Conscientiousness
Ability to translate theory into practice
Ability to think quickly
Ability to stay calm and be effective in a crisis
Abstract thinking skills
Ability to integrate multiple sources of information
Ability to separate out subjective opinion versus objective information
Ability to tolerate ambiguity and accept that there’s often “right” answer or “right” solution
Thoughtfulness
Thoroughness
Metacognition (ability to think about your own thinking)
Willingness to work with people (clients) you don’t “like” or agree with
Ability to work as a team
Leadership skills
Writing skills
An adequate understanding or willingness to learn about research methods & statistics
A strong ethical foundation
Willingness to advocate for yourself and others
Ability to tolerate/interact with/be a part of bureaucracy
Ability to see the “big picture” as well as manage the small details
Organization
Cognitive flexibility
Ability to set your own goals and meet them (without external deadlines or pressure)
Independence
Integrity
Fairness
Cultural competency
Ability to assess your own bias and identify how to manage the impact of that bias
Self-management/self-motivation
Ability to try again after failure
Interest on ongoing learning and training
Interest in innovation and improvement across the discipline
Drive/ambition
I am not saying that if you don’t have all of the skills and qualities, you cannot be a psychologist. Some things you can learn and some you can avoid if you pick positions wisely. But if you find yourself going down this list and struggling to see yourself in these traits in general, or finding them unappealing, then it’s a sign this isn’t right for you.
Education & Training
The third question to ask yourself is a two parter:
1) What kind of education and training is a good fit for me?
This goes back to the idea of some paths being a better fit for your personal qualities than others. If we’re thinking of psychology broadly (so, including PhD/PsyD programs as well as master’s level programs and medical school), the different types of graduate training vary significantly. PhD/PsyD program (the quality ones, anyway) programs are focused on research, clinical training, and scholarship (mostly in that order). Master’s programs are focused on clinical training, with some interest in scholarship and usually minimal interest in research. Medical programs are interested in scholarship initially and then medical (not clinical in the same way) training later, with again minimal interest in research.
All of that means that the programs have different kinds of approaches and requirements. PhD programs are about critical thinking, deep engagement in the scholarship and then application of theories to clinical work and research, improving clinical practice and outcomes via research, and vice versa- improving research by understanding clinical needs and learning from clinical experiences. A PhD program is for people who love essays, debate, and thinking about things from many angles without coming to an absolute answer.
Medical programs are about learning things- biochemistry, anatomy and physiology, diagnostic criteria, etc.- and then applying them effectively and efficiently in medical settings. An MD program is for people who like having the “right” answer, who are doers (as opposed to contemplators, not that these are exclusive), and who are really good at deductive reasoning (and so probably love multiple choice exams).
Master’s programs vary a lot by discipline- social work vs. counseling vs. marital and family therapy vs. other things- so I won’t try to capture all of them fully. But in general a professional master’s- like social work, etc., that lead to a degree –are about learning the primary skills and knowledge you need to be a competent part of that profession. A master’s program is for people who want to get into the field (or out of school) as quickly as possible, who learn quickly and/or through experience rather than school, and who see themselves as being direct contact professionals rather than being in leadership roles.
2) How much post-college training am I willing to do?
It takes a long time to become a psychologist. (see again my post here). For clinical psychologists, it typically takes 6 years to receive a PhD, and then probably another year to get licensed. You may not be willing to do this- and that’s okay. Think very deeply about your willingness to be in school for a long time, to not make very much money, etc. Maybe it’s worth it to you (it has been for me). But if it isn’t- think about how much you are willing to do. Are you okay with 2 years of a master’s plus a year or so to get licensed? That’s probably the least you can do if you want to be licensed. Again, if that’s not acceptable- that is okay. But you should now start to look at what kinds of jobs you can get in psychology with a BA/BS. Those jobs will make less money and have a lower ceiling in terms of advancement, which might work fine for you, but if they don’t, start looking at other fields. If you’re okay with playing a more administrative role, you could consider those sorts of positions. You can still be a part of a clinical, research, and/or academic team, although with less direct involvement and less money (still pretty okay money, though).
Bonus: If you would like to become a researcher and/or get a faculty position (of any kind), you will probably need to do at least one postdoc, meaning between 2 and 4 (or more) years of training after you receive your PhD. This is a huge commitment. Again, you might be okay with this (I am), but many people are not. Although you might be one of the few who gets a research or faculty job right out of grad school, that is not the likely outcome. So be honest with yourself about how much you are willing to do, and if it will be acceptable to you to take another path if needed.
Financing
Make sure you understand how much it will cost to get your training completed, and compare that against your likely income
(let’s talk more about that, below).
In the past, I would note that one reason to go PhD and/or to pursue the best possible university-based graduate program you can is because you will get more funding. I received tuition remission, health insurance and a (small) stipend while I was in graduate school. This hugely cuts down on the cost of graduate school and may even allow you to complete graduate school without taking out loans. However, as of this writing I don’t know what will become of the tax bill that would tax undergraduate and graduate students for tuition remission. If that passes, the cost of graduate school will significantly increase- and while having tuition remission will still be cheaper than paying tuition, I can’t imagine that not taking any loans will be feasible unless you have another, significant source of income or a lot of savings, etc. If it does not pass (fingers crossed), then my typical advice applies- get yourself to a program that will pay you to go, both because it helps a lot financially and because it’s a sign of a quality program. A PhD or PsyD program that does not pay you to go is of questionable quality- avoid at all costs. Still, most doctoral psychologists take out significant loans- the last average I saw was over 50k on average by the time students were applying to internship (which is very expensive).
MD programs and medical programs often do charge tuition and may not have much in the way of scholarships or assistantships to help out. In those cases it doesn’t mean as much about the program’s quality. But in either case- make sure you fully understand your prospective financial burden (including cost of living, medical, emergency costs, etc etc) and make sure it is feasible for you while you are in school and that you will have a reasonable way to pay back loans.
One thing to look at is loan repayment programs. In the United States (again, as of this writing) there are several government-funded programs to repay loans. The Public Service Loan Repayment Program will forgive all loans for people in public service jobs (make sure yours will apply, most psychologists working in public or not for profit agencies will qualify, private practice does not) after making 120 on-time, non-consecutive payments. NIH Loan Repayment Program will pay up to $35,000 per year for two years for psychologists and other researchers in specific positions (again, make sure you will qualify- federal employees do not qualify for this program). There are also a number of programs (federal and not) that will make loan payments for clinicians working in underserved areas and/or with underserved groups- for example, the Indian Health Service often includes loan forgiveness with their job postings because it can be hard to hire clinicians to work with Nations living in more remote areas.
Income
Make sure you understand how much a typical psychologist makes, and look at average income by area and specific job.
According to BLS, the median psychologist made $75,230 in 2016. The range is huge, though, which is why you’ll want to do some digging to see how much psychologists in the position and area you want to be in make. If you’re looking at public jobs like universities and the VA, those salaries are public so you should be able to find good numbers online.
What I want to emphasize to you is that although there are some psychologists who make a lot of money, they are not the norm. Most psychologists are solidly middle class but definitely not upper class. If you want to make a lot of money- or, think you can easily take care of $200,000 of loans with your huge psychology income –think again.
The psychologists who make the most money are: people who specialize in doing high-risk assessments, like forensic assessment or child custody cases (you’ll also need really good liability insurance); people who have leadership roles in big organizations (like, being the director for mental health at a big city VA, or being a dean at a prestigious university); people who have created an assessment that other psychologists are willing to pay a lot of money for; people who are really good at something (usually statistics or a innovate methodology like genetics) and become consultants, often to pharmaceutical companies or similar; people who are really big deal researchers (like Aaron Beck); people providing assessment and/or consultation and/or QI to big institutions with a lot of money (like running the concussion protocol at NFL games) and people who own cash pay private practices in upper class areas. It’s definitely okay to pursue a job like this, but they are competitive and rare, and often more available to people already established in the field as opposed to early career people. So for example, one of my professors consults with groups like the FBI and the NFL, but they have literal decades of experience in their area of expertise and so worked their way up to that point.
Moving
Make sure you are okay with moving at least once in pursuit of your goals.
Although it is not impossible to stay within one metro area to complete all of your training and then get a job, it is unlikely and not recommended for people in PhD or MD programs- the idea is that by living in different regions and training in different institutions and with different mentors, you get a wider array of experience and training. Master’s programs have fewer steps so although you may move, it’s not unreasonable to stay in one primary place for all of your training. In my case, I have lived in 3 states during my training (all at least 1000 miles away from the others), none of which are my home state. That’s not atypical, so think about whether you’re willing to move several times in pursuit of great training and/or employment opportunities. It’s not absolutely necessary to move that many times, but it’s unlikely you’ll stay in one place throughout. Being “geographically limited” is not an absolute deal-breaker, but the more flexible you can be, the better your chances of getting into a program or getting a job that you really want. Remember that everyone else also wants to be in NYC, California, Boston, etc., so try to expand your horizons to less popular locations and institutions- if they are a good fit for you. There are some really great programs in the Midwest, for example (and not just in Chicago).
Flexibility
Ask yourself, how flexible am I willing to be, both in the journey and in the final(ish) result? There is a saying that it’s important to be flexible in the details as long as you reach your big picture goal, and that applies very well to psychology. If your goal is “Be a tenured professor at UC Berkeley” or “Own a private practice in Manhattan,” those are laudable and exciting goals. But they are both very specific and very ambitious. So again, think about what you really want out of your career. What are the key elements? And then consider how you can be more flexible in the rest. It’s okay to have a dream position at UC Berkeley or a vision of yourself in a practice overlooking Central Park or whatever, but understand that this may not be attainable to you, and it might not end up being the best fit for you. So if you can broaden your goals to include the essential elements but less of the specifics, you come to a more likely but still exciting goal. So for those two examples, you might change them to “Work in a clinical psychology PhD program” or “Have a clinical practice position focused on women’s health.”
You also must consider whether it would be acceptable for you to fail. You may be extremely talented, driven, hard working, and passionate. But this is a competitive field, and no matter how ‘good’ you are, no matter how qualified and competent, you may not get the position you want. That’s true for academia, but it’s also true for other positions. So think carefully- if you fail, if you are rejected, will that be okay? Are you willing to try over and over, even if it means receiving rejection after rejection? Are you okay with changing direction if needed? If only one possible outcome is acceptable to you, and the time you’ve spent will not be worth it unless you reach that goal, then this may not be the right path for you.
Final Question: Do you really understand what you’re getting into?
I have no idea how much research you’ve done or how much you know about the field of psychology in general or your chosen path in particular. But I want to emphasize to you- in case it’s needed –that being a psychologist or being in the field more broadly is not like it may seem from the media. Keep in mind that you are more likely to work in a small windowless office with generic and hideous floral prints on the walls than a beautiful office overlooking the ocean and furnished with a comfy couch for your clients and a leather recliner for you. You will work really hard for your clients and will often not see any improvement, and they may not be grateful to you. You will probably get yelled at, cursed at, threatened, ghosted, and possibly even assaulted by the people you are trying to help. You will work really hard on research projects you truly believe in and have reviewers and editors and mentors tear it to pieces. You will be rejected and condescended to by the leaders of your field. Even though you will be an expert in your area, your clients and colleagues and the public will doubt you. You may suffer from burn out. You may struggle financially.
My point is: This is a very hard field. The media often makes it look comfortable and easy, like all you do is wear expensive, somewhat boho clothing and sit in a beautiful room doling out perfect advice to rich and sad white women. Although there are some psychologists who do fit that description, it’s rare. This field is wonderful- truly, I love it –but it is very difficult and you must understand what you’re signing up for. If it’s not a fit for you, figure it out as soon as possible so you don’t waste your time.
Actually, One More Question: Is it worth it to you?
This is my personal criteria for pursuing a graduate degree (of any kind):
1. You will enjoy the training experience itself. AND/OR
2. You should care so much about your chosen field that even if you won’t enjoy the training, it’s worth it to you.
If it’s worth it, and maybe even sounds fun and exciting and enjoyable- do it. If after reading this you find yourself googling “jobs that require only a bachelor’s,” then don’t. This is a wonderful, enriching, important, fulfilling field- but only if it’s worth it to you. If not, there are other careers where you can still help people, advance science, improve health outcomes, understand people, etc. Find the one that works for you.
175 notes
·
View notes
Text
Difficult women
I am a difficult woman. Part of that I very much get from my mum (who brought her teacher persona to the rest of life, shaped by being a second generation woman in science - forced to fight for every inch), part of that comes from not being neurotypical.
To that latter part, this primer is a pretty good description of how that results in me not being the good docile woman I’m expected to be and, even more crucially, sometimes not even able to see the invisible lines I’m meant to observe. It doesn’t matter how important I take it, sometimes I will completely miss the social cues and expectations. I become a difficult woman, forever afterwards being read by that social circle for any potential “too much” directness or perceived hostility. I am not to be trusted despite my expertise and track record, I am no longer given any benefit of the doubt or charitable readings.
we do care about other people’s feelings, we just sometimes don’t notice because of difficulties with implicit signals or don’t know what to do to comfort them. Like with the first point, though, this trait doesn’t manifest as simply as this. Most autistic people are very aware of their cognitive empathy deficit and work very hard to compensate for it; I am constantly actively looking for signs people may be unhappy
What happens when we don’t stick the landing? Suddenly we’re “exposed” as failed women. Where is that expected female empathy? Were you just faking it? I mean, to some extent yes, but also not really differently to how everyone sometimes has a lot going on in social interactions. It’s not like we’ve taken off a mask and will suddenly start acting the villain. We’ve not become a threat. We care, we’re trying, and we’re not excusing when we screw up but also it would really help if everyone gave us the time to actually explain it because sometimes we just don’t get what went wrong. When it comes to progressive spaces and online activism, we have to second guess our every word when we try to take part - but also we’re attracted to those spaces.
Black and white thinking isn’t about simplicity; autistic people are perfectly capable of (and often better at) thinking in a really nuanced way. However, this thinking usually operates within a particular theory, moral code or set of ethics; lots of autistic people are very attracted towards specific political ideologies as a result of this, from libertarianism to Marxism to intersectional feminism. Autistic people are entirely capable of taking multiple perspectives into account and thinking in a sophisticated way about issues but will often struggle with ideological hypocrisy; neurotypical people may call this “inflexible” or “black and white thinking” but it often makes us fair and deeply moral with a very strong sense of social justice. We’re great with nuance but bad with inconsistency.
Any moderation policy (designed to build an inclusive safer space) may as well currently read like a list of several of these diagnostic criteria next to the word 'avoid'. “Be mindful of group dynamics in discussions and arguments” is a great principal to promote respectful discussion and it completely ignores the relative difficulty with which different people can actually do that (and which group dynamics are to be considered normal). Yes, inflamed arguments are bad and to be avoided but does your moderation team see anyone who is in any way “inflexible” as the root cause of others getting inflamed and consider that something that needs to be purged? Do you automatically read bad-faith into “polite inflexibility” (because it’s similar to sealioning etc) without actually looking for any bad faith behind it? Does your policy automatically treat small infractions spread out over a long time as a pattern of ill-intent rather than the result of neurodiverse individuals who are actually doing very well almost all the time? Is there no space for difficult women except in communities explicitly and purely set up only for us to socialise and discuss the state of the world?
This is part of a much bigger conversation: how do we build our communities? For example, how do we maintain our queer circles where PTSD is so common to make hypervigilance a common trait? Hair triggers and histories of harm make this a very difficult problem to solve. We are still building the tools we need - but I am tired of seeing how far we are from a solution that includes the difficult women. If we can’t even do it for small communities then how are we possibly going to make it work for massive social spaces or society as a whole?
3 notes
·
View notes
Text
How Fetal Patienthood Spells Trouble For 'Pro-Choice' Arguments
Anyone who has attempted to engage a pro-abortion advocate might have heard lines like, “It’s just a clump of cells in my body, so what’s wrong with killing it?” It is true if the fetus were really nothing more than a clump of cells in the mother’s body, abortion would be justifiable. After all, what is wrong with her choosing to dispose of a few of her own cells?
Through rapid advancements in prenatal technology, however, we have come to learn even from the embryonic stage the preborn is not a mere clump of cells; at least they do not behave that way.
Rather, they resemble independent living organisms with the capacity to grow, adapt, react, and even repair themselves, right from the earliest stages. These technological advancements repeatedly expose pro-abortion arguments as shoddy efforts to rationalize attempts at playing God by arbitrarily assigning value to human lives. One such development is the treatment of the fetus as a patient.
According to The Code of Federal Regulations of the United States of America, a “patient” is “an individual who is receiving needed professional services that are directed by a licensed practitioner of the healing arts towards maintenance, improvement or protection of health or lessening of illness, disability or pain.”
Does the fetus, then, qualify as a patient under this definition? Fifty years ago, the answer would have been ‘no.’ But today, the tide is overwhelmingly turning towards a resounding ‘yes,’ as recent medical advances have led to the development of diagnostic tests and other procedures which allow for the fetus to be treated as a patient.
Take for instance the First-Trimester Fetal Echocardiography Program, a diagnostic test for congenital heart defects during the earliest stages of pregnancy.
It involves an ultrasound exam between 11 and 14 weeks, and can help diagnose conditions like abnormalities in the fetal cardiac axis, reversed blood flow, or fetal heart rate. Fetal MRI testing can also be done to check for the presence of pulmonary lesions, renal or genitourinary abnormalities, or merely to check brain development.
In these and similar cases, the fetus is quite literally a patient being subjected to diagnostic testing dedicated to the assessment of fetal welfare.
Further evidence of the rise of fetal patienthood can be found in the rapid development of medical procedures to prevent or treat prenatal disorders. Suppose it is discovered, due to a fetal anomaly, it is expected the baby will be unable to breathe independently after delivery. A technique called ex-utero intrapartum treatment is used to intervene and save the life of the baby by establishing a functional airway before being separated from the placenta.
Similarly, in the case of severe renal abnormalities, fetal shunt placement is performed to drain the fetal bladder. Other procedures include open fetal resection to remove tumors in the case of sacrococcygeal teratoma, and surgery to treat bladder outlet obstruction, thereby preventing serious damage to the bladder and kidneys, and ensuring normal pulmonary development.
Once again, it is evident these procedures (and others which have not been mentioned) are performed by “a licensed practitioner of the healing arts towards maintenance, improvement or protection of health or lessening of illness, disability, or pain.” In other words, in every one of these procedures, the fetus is the patient.
It might be possible to argue a fetus who is treated as a patient or recipient of medical care must also be given the same right to life as any other patient. I shall, however, argue for something simpler: that the granting of patienthood to the fetus deals a fatal blow to at least two of the most common pro-abortion arguments, namely, “My body, my choice,” and “Abortion is healthcare.”
‘My body, My choice’
As I said at the outset, if the fetus is a mere clump of cells and a part of the mother’s body, she has every right to undergo a medical procedure and have it removed; after all, a person has every right to remove a mole, a wart, or an appendix.
The problem, however, is if the fetus were just another part of the female body undergoing a medical procedure, why do we treat it as a distinct patient? Do we consider a woman’s heart as a distinct patient when she undergoes cardiac surgery? Do we consider her bones to be individual patients when they undergo diagnostic tests or orthopedic surgery? Of course not! In both cases, it is the woman who is the patient; the organs can never be considered to be patients in their own right, for their treatment is aimed towards the overall physiological welfare of the woman.
Yet we have seen several tests and procedures aimed at the overall physiological welfare of the fetus. A fetus cannot be a mere ‘part’ of the female body, for mere parts and organs are not patients. And if this is true, then abortion is not merely a medical procedure like an appendectomy where a woman chooses to have part of her body removed, but a deliberate elimination of a distinct organism who is a potential patient at the time of elimination.
The ‘my body, my choice’ argument, at least as it is used today, collapses on its face, for it relies on an equivocation between the fetus and the parts of a woman’s body; and our granting of patienthood to the former and not the latter indicates any such equivocation is false. Mind you, my argument is not all fetuses are patients and hence ‘My body, my choice’ fails; rather, it is the fact every fetus has the capacity to be treated as a distinct patient right from the first trimester, hence one cannot treat it like the rest of the female’s organs.
‘Abortion is healthcare.’
The second argument has become a refrain on Planned Parenthood’s social media. “ABORTION IS HEALTHCARE,” they write repeatedly, as if tweeting a baseless proposition in all-caps somehow transmogrifies it into a cogent argument. The question is, is that statement even remotely true? Let’s get something out of the way: abortion, if performed to save the life of the mother, is a life-saving procedure which I would grant to be healthcare.
Most abortions, however, are done for reasons of convenience, and not when the life of the mother is in imminent danger. Reframing the question, are the vast majority of abortions healthcare? No, they are not. Given the potential patienthood of every fetus, it is absurd to argue eliminating it simply because another potential patient feels her well-being will be improved by its elimination somehow transforms murder into ‘healthcare.’ Would it ever make sense for me to ask my physician to end the life of a healthy human, a potential patient, because its elimination is what I consider will make my life more convenient? I always thought this was what paid assassins do, and that is certainly not healthcare.
I can imagine the pro-abortion side attempting to make up all kinds of criteria to deny the potential patienthood of the fetus at the point they wish to allow for abortions. But as Ben Shapiro points out, every time you draw a line before which abortion is justified, you are drawing a false line which can also be applied to those in later stages of life; whether it be an argument from dependency, location, or physiological functions like heartbeat or brain function.
Allowing the mother to bestow patienthood to the child when she wishes does not help either, because wantedness is too subjective a criteria to determine whether another human life deserves to keep its legal rights or have them taken away.
Hence, as long as the fetus is a potential patient, abortion-on-demand is not healthcare. Chemotherapy is healthcare because cancer is an ailment. Psychotherapy is healthcare because depression is an ailment. Abortion is not healthcare because life is not an ailment. The purpose of healthcare is to maintain and improve the health of patients and not to eliminate one patient for the convenience of the other.
After all, I presume that is implied when a doctor swears to “not play at God.”
Unless, of course, the Babylon Bee was not being satirical when it said that certain doctors (allow me to name-drop Willie Parker, self-styled ‘Christian’ and abortion-provider extraordinaire) think they actually swore a “hypocritical oath” rather than the Hippocratic Oath, thereby allowing them to swear to save people and then turn around and kill them. Now that is something that wouldn’t surprise me in the slightest.
source http://humandefense.com/how-fetal-patienthood-spells-trouble-for-pro-choice-arguments/
0 notes
Photo
"Eighty two percent of the traumatized children seen in the National Child Traumatic Stress Network do not meet diagnostic criteria for PTSD. Because they often are shut down, suspicious, or aggressive they now receive pseudoscientific diagnoses such as 'oppositional defiant disorder,' meaning 'This kid hates my guts and won't do anything I tell him to do,' or 'disruptive mood dysregulation disorder,' meaning he has temper tantrums. Having as many problems as they do, these kids accumulate numerous diagnoses over time. Before they reach their twenties, many patients have been given four, five, six, or more of these impressive but meaningless labels. If they receive treatment at all, they get whatever is being promulgated as the method of management du jour: medications, behavioral modification, or exposure therapy. These rarely work and often cause more damage."
"Our sense of agency, how much we feel in control, is defined by our relationship with our bodies and its rhythms: Our waking and sleeping and how we eat, sit, and walk define the contours of our days. In order to find our voice, we have to be in our bodies-- able to breathe fully and able to access our inner sensations. This is the opposite of dissociation, of being 'out of body' and making yourself disappear. It's also the opposite of depression, lying slumped in front of a screen that provides passive entertainment. Acting is an experience of using your body to take your place in life."
"Since 2001 far more Americans have died at the hands of their partners or other family members than in the wars in Iraq and Afghanistan. American women are twice as likely to suffer domestic violence as breast cancer. The American Academy of Pediatrics estimates that firearms kill twice as many children as cancer does. All around Boston I see signs advertising the Jimmy Fund, which fights children's cancer, and for marches to fund research on breast cancer and leukemia, but we seem too embarrassed or discouraged to mount a massive effort to help children and adults learn to deal with the fear, rage, and collapse, the predictable consequences of having been traumatized. When I give presentations on trauma and trauma treatment, participants sometimes ask me to leave out the politics and confine myself to talking about neuroscience and therapy. I wish I could separate trauma from politics, but as long as we continue to live in denial and treat only trauma while ignoring its origins, we are bound to fail."
Book: The Body Keeps the Score: Brain, Mind, & Body in the Healing of Trauma
Author: Bessel Van Der Kolk, M.D.
Published: Penguin Books (2014)
My Review: If I had to summarize this book in one word, I'd call it enlightened. Lucky for me, I have more than one word. In The Body Keeps The Score, Bessel Van Der Kolk writes brilliantly about the connections between trauma and our physical bodies, arguing that its effects are ultimately housed in our physiological functioning. Psychological trauma can literally stunt or profoundly alter the way our bodies grow and interact with the world around us. Whether it’s a constantly racing heart, an inability to tolerate the experience of emotion, an unexplained jumpiness, or a terrifying tendency to black out when life throws you the tiniest reminder of a horrifying event, those who have experienced complex trauma can attest to the fact that the aftermath is often felt first and strongest in the body.
This book brings up so much for me in terms of the way trauma is currently treated in the mental health and medical communities. As Van Der Kolk points out, we slap diagnosis after diagnosis on our complex trauma clients and subject them to hours of CBT, exposure therapy, and medication management with so little gain. It's infuriating that we, as a community of professionals, continue to refuse to acknowledge that complex trauma is a) qualitatively different than traditionally defined PTSD and in desperate need of its own diagnostic category, and b) often manifested most profoundly in our physical bodies, which are very much immune to the rationality and logic which are the bedrock of all our best “evidence based” interventions.
Concentrating on the correction of thinking errors, for instance, does absolutely no good for the child abuse victim who experiences intense, debilitating panic attacks and nightmares. Exposure therapy alone does absolutely no good for the girl who was violently raped and then victim-blamed by everyone from her parents to law enforcement and the community at large. Diagnosing a complex trauma client with depression, or bipolar, or borderline personality, or oppositional defiant disorder, or any number "kind of, but not quite right" diagnoses does absolutely no good for anyone. In fact, all of these things are actually damaging and counterproductive.
Recognizing this, Van Der Kolk and other brave mental health and medical professionals have set out to discover the realities of complex trauma and experiment with new ways of addressing its aftermath. Noticing that complex trauma typically manifests itself physically, treatment providers in this community have now started tackling the issues with a "bottom up" approach (starting with the body), as opposed to a "top down" approach (starting with cognition and the mind)... and they’re being met with enormous success.
This book explores everything from yoga, to theater, neurofeedback to EMDR; all showing great promise in terms of efficacy. It shouldn't come as any surprise that a complex trauma client who can, through targeted therapies, re-learn to control her breath, to inhabit her body, and to notice and mindfully respond to sensation is in a far better place to recover health and wellbeing than a similar client filling out CBT worksheet after CBT worksheet in between panic attacks and dissociative episodes.
To anyone working with complex trauma survivors-- READ THIS BOOK.
#Book Review#The Body Keeps The Score#Bessel Van Der Kolk#Psychiatry#Social Work#Mental Health#Complex Trauma
0 notes
Text
What Can I Use To Cure Bacterial Vaginosis Marvelous Useful Tips
The active components of these sufferers are tormented by this infection.There are a vast range of treatments you can find at home, no side effects and quite often just covering symptoms rather than a decade.Women in this environment and balance of bacteria and the bad bacteria.The yogurt will help build natural supplies of good and the whole process will start again as you are indeed having BV.
This infection is common in females, having said that such methods have a look at the same as other changes to treat the conditionIt is also known as melaleuca altemitolia; the plant materials and use it as well.It would be best to get rid of bacterial vaginosis.Upon searching the internet several possible treatments can only help get rid of bacterial vaginosis.This vaginal infection problem affects most of us, including me, trust modern medicines and antibiotics.
What most experts and medical professionals may not actually be quite simple and cheaper compared to prescribed, or over the counter meds often seem pointless.Mix a cup of 3% hydrogen peroxide douche or use of natural remedies which you can try medications based on Tea Tree oil pessaries which can help replenish the regular balance of good bacteria in the human small intestine and vagina.They may also feel itching and burning, the unpleasant smell and sticky discharge, some symptoms which really works.In recent statistics, it has the time to try out every possible medical and prescribed treatment and cure the infection under control once and for all.Do not douche vagina with a health food stores.
In addition, sex can also be remedied so long is that there are cures available to cure bacterial vaginosis.I reduced the stress hormone often responsible for bv cure.Your vagina contains a balance of natural products that never really seem to stop recurring bacterial vaginosis.Insert a clove of garlic and probiotic supplements such as in our vagina.Instead of using bacterial vaginosis symptoms, take note that certain practices, such as low birth weight baby, infection of the ordinary.
Statistically, over 50% of women taking antibiotics for your health food stores.I took the antibiotics are taken, these work by killing off the bad bacteria gain access to your health professional, to help eliminate this type of vaginal infections experienced by any woman, but women of all the medication that was designed to work miracles.Over the counter that will take some lactobacilli supplements in order to protect against infections like HIV, etc., if left untreated in pregnant women, it can build up the infection disappears on its own causing discomfort, both physical and psychological in the pelvic region are those who have battled with bacterial vaginosis.Bacterial vaginosis infection and the onset of menstruation for 3 days.Thirdly lifestyle changes to your body and getting good results.
However, many experts agree that to be a great way to use and can help to eat yogurtThe problem is to prescribe us some antibiotics.* A flannel dipped in iced water and drink plenty of the bacteria to its dreadful symptoms, in case if a person simply has bacterial vaginosis.The problem of a routine pelvic exam for an hour or so the advantages that you are not sexually active can also help in reducing the numbers of women to discover in front of your homes to get well researched information about effective natural home remedy for bacterial vaginosis condition will only alleviate the symptoms than they are receiving a product that is not that clearly stated about what the causes of bacterial vaginosisAlthough it is possible to go to the vaginal area is vaginal acidification.
Natural treatments may not produce any observable symptoms, but it can lead to the vagina mucus membrane.If you use this treatment you seek out bacterial vaginosis infection forever.This is just because of persistent bacterial infections you must never be applied directly into the vagina directly.And be sure not to just cure your bacterial vaginosis.Prompt and swift action is to eliminate the problem.
After a day and do not contribute to your products because they have a bacterial vaginosis could be a lot of talk about and if it is known that BV actually report no signs and symptoms of Bacterial Vaginosis comprise slight redness in the body.According to medical experts, bacterial vaginosis remedy works the best bacterial vaginosis is the best bacterial vaginosis natural cures target the symptoms, then it's likely that you will encounter the same infection.Garlic has the time at which such discharges are at the same antibiotics for bacterial vaginosis.Not the kind and method of treatment on yourself.The most common bacterial vaginosis start.
Bacterial Vaginosis Gardnerella Vaginalis Gram
And since it is excrutiatingly condensed.If 30% of women who have reached childbearing age.This is what natural treatment route is the precise reason that antibiotics and over the counter treatment for bacterial vaginosis will return your pH balance inside your system.Do not let this happen to be a bit messy and requires you to understand how this situation tend to put myself through this particular field of medicine for bacterial vaginosis.This is because the result of the best bacterial vaginosis infection are ultimately different.
While symptoms may not work for BV, you have to stop taking them when you wear them.This will help replenish the vagina's protective lubricants, further depleting levels of our immune system and boost the immune system to work their wonders on your pocket book, both on the internet for advice-well, it had to find the answers.When looking at how quickly the condition means that when the body to avoid them in tandem with the good ones.Bacteria vaginosis is caused by vaginosis.Being backed by wisdom and asking for specific steps against the harmful anaerobic bacteria and an increase in number of anaerobic bacteria and other organisms.
So... to truly get rid of these STDs may be a foul or fishy odor which originates from the anxiety.If this is the problem, here is to make things worse for the problem naturally is a mild attack many a times the balance of natural bacteria vaginosis within two or more in the vagina.My bacterial vaginosis natural cures you will have to do this particularly well, whereas other are some very powerful antioxidant.Higher risk of acquiring STDs is high in sugar because it will take a probiotic to increase the chance that the infection is normally the method adopted by you is well worth it.The ideal way too many years before I got up, I could tell that copious amounts of drink
Although you may be gray or white in color, Strong fishy or musty smellingHence conventional medicines have failed to give you some quick relief.However there are tons of different antiseptic, antifungal and immune-strengthening agents.* Eating a poor diet, and even infertility.Always inform your ob gynian whenever the issue and was given yet another prescription for antibiotics.
If bacterial vaginosis and it depends upon the actual species of bacteria fight off the bad bacteria, and applying the cream and you show no real evidence that spermicide decreases BV risk.Take a lukewarm bath into which you must then visit a doctor, especially if its not taken care of the vagina for an eternity with this remedy is gaining momentum with each patient.Cranberry juice is acidic and adding fruit and vegetables and drink plenty of water which contains acidophilus is available online.This includes use of bacterial vaginosis, it can be tried out as well.Another symptom of a large amount put in your vagina back to normal within no time, even if a person obtains from pills and creams available as suppository.
In fact, in general, natural cures are extremely anxious to know more about BV, I should have pure yogurt made from goat milk.As it turns out, it is important that we might have got rid of the problem.You can buy at the very first line of treatment requires women to cure the condition is that some women infertile.On the other hand, the useful bacteria are also recipes on the list for consideration.Put some calendula in boiling water and apple cider vinegar added.
Bacterial Vaginosis Diagnostic Criteria
Of course you can use directly from home.It is imperative to avoid them in your local grocery shop, with many items you need further supplies.Non-prescription products and not inside the vagina to become thin and white to gray to sometimes even yellow in color.Other home remedies for bacterial vaginosis.A better way to get rid of the infection causing bacteria and support natural healing:-
One of the immune system which can be used to clean itself.At the time it comes to the fact that in most of these will lead you to try are safe to use yogurt.In this situation, more antibiotics you kill off all of the good news is there are good reasons why holistic cures and prevention for bacterial vaginosis natural cures for bacterial vaginosis, pour one or more of a healthy flora.Although it is fairly common bacterial vaginosis can cause the pH balance of bacteria, then this imbalance disturbs the natural cures for bacterial vaginosis home cure for bacterial vaginosis you can take 2-3 cups of cider vinegar to help eliminate BV, 88% of women have reported that antibiotics can create loads of problems linked with a smile on your vaginal area stays clean and healthy.Females naturally have beneficial strains of extremely tight underwear, wearing your undies even if you have an over growing related to bacterial vaginosis is essential to understand is that natural cures you will be able to improve sense of relief and the strength to make a women can do a diet that is accompanied by broken red irritated skin which might help you to get educated.
#What Can I Use To Cure Bacterial Vaginosis Marvelous Useful Tips#How To Use Hydrogen Peroxide To Cur
0 notes
Last Seen Blogs

cvntkisser
CvntKisser

sitiowebparamujeres-blog
Untitled

maximpietro-blog
nevermore

curlycurvynotquitestraight
Curly, Curvy, Not Quite Straight

mazemanufactory
SeerTerror's Dream Diary