#bmj case reports
Text
Top 21 Open Access Medical Journals That Technology Watch Experts Should Leverage
Introduction : Keeping up with the ever-evolving technology landscape in the medical field can be a challenge. If you’re a technology watch expert, you need to be able to quickly identify emerging trends and make sound decisions based on them. But how can you do that ? This a [...] https://is.gd/f0qghy

#business #communication #data #education #ict #information #intelligence #technology - Created by David Donisa from Academypedia.info
#are open access journals bad#best open access medical journals#bmj case reports#bmj case reports impact factor#bmj impact factor#bmj open author guidelines#bmj open impact factor#bmj open quality#bmj open submission#bmj open submit#bmj quality and safety impact factor#bronze open access#delayed open access journal#diamond open access#directory of open access books#doab#doaj directory of open access journal#examples of threats in a swot analysis#free open access medical journals#gold open access#green open access#h-index vs impact factor#hybrid open access#is scientific reports a good journal#is the british medical journal reliable#journal ranking#list of open access medical journals#open access database#open access disadvantages#open access examples
0 notes
Text
Le 21 Migliori Riviste Mediche ad Accesso Aperto Che Gli Esperti di Technology Watch Dovrebbero Sfruttare
Introduzione : Stare al passo con il panorama tecnologico in continua evoluzione in campo medico può essere una sfida. Se sei un esperto di orologi tecnologici, devi essere in grado di identificare rapidamente le tendenze emergenti e prendere decisioni valide basate su di esse. Ma come [...] https://is.gd/oVNURZ

#business #communication #data #education #ict #information #intelligence #technology - Created by David Donisa from Academypedia.info
#accesso aperto al platino#accesso aperto ibrido#accesso aperto in bronzo#accesso libero verde#bmj apri invio#bmj case report fattore di impatto#bmj fattore di impatto aperto#bmj linee guida per autori aperti#bmj qualità aperta#bmj qualità e fattore di impatto sulla sicurezza#bmj sottomissione aperta#casi clinici bmj#classifica rivista#database ad accesso aperto#diamante accesso aperto#diario ad accesso aperto ritardato#directory di libri ad accesso aperto#directory doaj della rivista ad accesso aperto#dob#è affidabile la rivista medica britannica#elenco di riviste mediche ad accesso aperto#esempi di accesso aperto#esempi di minacce in un&039;analisi swot#esempi di opportunità di analisi swot per studenti#fasi del processo di revisione tra pari#fattore di impatto bmj#fattore di impatto del giornale di psicologia#fermare i giornali predatori#i rapporti scientifici sono un buon giornale#indice h vs fattore di impatto
0 notes
Text
Everyone debating the merits of the COVID-19 vaccines needs to take these four journal articles into account. The Journal of Evaluation in Clinical Practice’s hugely important series of articles on exaggerated COVID-19 vaccine effectiveness and safety claims, involving BMJ Editor Peter Doshi and myself, has now concluded. The initial Fung, Jones, and Doshi paper outlines statistical biases, such as the ‘case counting window’ bias, that likely lead to the Covid vaccines’ effectiveness being exaggerated in observational studies. The subsequent paper by Lataster (that’s me) then explained the situation is worse, as the case counting window bias is often accompanied by a definitional bias, and noted that this could exaggerate vaccine safety as well. Doshi and Fung then returned with a further paper indicating that numerous cases in the vaccinated were overlooked in the clinical trials, likely leading to exaggerated effectiveness estimates. The fourth and final article in this ‘series’, again by myself, notes that this also appears to apply to safety estimates in the clinical trials, whilst also confirming my earlier concerns about safety estimates in observational studies, and noting that the myocarditis issue alone could mean that the jabs are not worth the risk in the young and healthy. Highlights of the open access article (thanks again to the wonderful University of Sydney):
Safety estimates appeared to be exaggerated in a recent observational study championing the use of the jabs in the Omicron era, which readers if my Substack Okay Then News readers will already know all about.
Counting windows for adverse effects in the clinical trials were incredibly short, going against long-established norms, especially with the treatment and placebo groups quickly merged, and reliant on unsolicited reporting, as well as the opinions of researchers paid by BioNTech and Pfizer (like cardiovascular deaths being written off as unrelated to the jab when we now know the jab does cause cardiovascular deaths). I note the concerning “large number of trial participants lost to follow-up” and that “deceased trial participants will not be contacting the researchers to describe their issues”. Wrap your head around that one. You’re in the vaccinated group. You die, thanks to the jab. As a result, you don’t report this to Pfizer. Your death is not included in the data, as with the potentially many other jab-caused deaths. With relatively few adverse reports the jab is declared safe. It’s a bit like how we can’t refer to many of the adverse event reports as they’re perpetually unverified.
Couldn’t avoid again referring to the Fraiman et al. and Benn et al. articles indicating that, with the data as unreliable as they are, the trials indicated an excess of deaths and “serious adverse events of special interest” in the vaccinated groups, relative to the unvaccinated groups.
I note that increasing research on myocarditis alone appears to indicate that the risks of the jabs outweigh the benefits in the young and healthy, the topic of my BMJ rapid response.
I reveal that Pfizer acknowledges myocarditis risks and limitations of its study. And that Pfizer is currently running a trial, again plagued by counting window issues, to “determine if Comirnaty is safe and effective, and if there is a myocarditis/pericarditis association that should be noted”. Would this information have been handy before you got jabbed, and before the jabs were universally declared “safe and effective”, and before people were fired for not submitting?
I conclude that there is more than enough here to “nullify the claim that the benefits of the vaccines still outweigh the risks in all populations”.
Just remember that the claims about these COVID-19 vaccines being safe and effective were, at best, based on these clinical trials and observational studies.
52 notes
·
View notes
Text
PSA Time: Ratchet Mode Engaged
so I'm off work today because my flatmate has COVID which means I'm exposed
so far I'm testing negative, but it's highly likely I'll catch it since we live in close proximity and you can spread COVID prior to being symptomatic
(BMA has a good paper on this subject here as well)
generally people tend to be most likely to transmit COVID 48 hours prior to symptomatic expression and for around 5 days after symptoms develop, although that's just an average estimated range -- you should be careful regardless of what day of infection someone might be on
around 1 in every 5 people infected with COVID goes on to develop Long COVID, so I want everyone to keep being safe out there because you do not want this shit if you can possibly avoid it.
while research is ongoing, there's a lot of evidence that repeated infections may increase likelihood of developing Long COVID, so don't roll the dice on this one and stay safe out there.
at the moment there seems to be a late summer surge in COVID cases (at least in the USA and UK), but due to a massive reduction in testing and reporting on local/national levels, exact numbers cannot be obtained -- the WHO has noted this problem in their weekly reports.
if you're not sure what the most common COVID symptoms are at the moment, you can find that information here, courtesy of the BMJ.
if you test positive on a lateral flow test, try to confirm the result via PCR test. in the UK, if you test positive, notify your GP or NHS 111. the current NHS guidance can be found here.
I'm currently waiting on the pharmacy to open so I can order my inhalers because I'm absolutely going to need them
on the upside, I'm not going into work today
on the downside, the plague has blighted us
but I hope this serves as a reminder to those that might need one that COVID is very much still a threat, so be safe out there, wear a mask if you can, and take care of yourself and others. <3
16 notes
·
View notes
Text
An 80% jump in cancer rates should be cause for alarm. Public health authorities around the world should be focusing more on this problem.
Global cases of early onset cancer increased from 1.82 million in 1990 to 3.26 million in 2019, while cancer deaths of adults in their 40s, 30s or younger grew by 27%. More than a million under-50s a year are now dying of cancer, the research reveals.
Experts are still in the early stages of understanding the reasons behind the rise in cases. The authors of the study, published in BMJ Oncology, say poor diets, alcohol and tobacco use, physical inactivity and obesity are likely to be among the factors.
“Since 1990, the incidence and deaths of early onset cancers have substantially increased globally,” the report says. “Encouraging a healthy lifestyle, including a healthy diet, the restriction of tobacco and alcohol consumption and appropriate outdoor activity, could reduce the burden of early onset cancer.”
Specifically, they are looking at people in the 14 to 49 age group. A disproportionate amount of this spike in cancer can be traced to consumption.
They looked at new cases, deaths, health consequences and contributory risk factors for all those aged 14 to 49 to estimate changes between 1990 and 2019.
In 2019, new cancer diagnoses among under-50s totalled 3.26 million, an increase of 79% on the 1990 figure. Breast cancer accounted for the largest number of cases and associated deaths, at 13.7 and 3.5 for every 100,000 of the global population respectively.
Cases of early onset windpipe and prostate cancers rose the fastest between 1990 and 2019, with estimated annual percentage changes of 2.28% and 2.23% respectively. At the other end of the spectrum, cases of early onset liver cancer fell by an estimated 2.88% a year.
A total of 1.06 million under-50s died of cancer in 2019, an increase of 27% on the 1990 figure. After breast cancer, the highest death tolls were linked to windpipe, lung, stomach and bowel cancers. The steepest increases in deaths were among people with kidney or ovarian cancer.
The highest rates of early onset cancers in 2019 were in North America, Oceania and western Europe. Low- and middle-income countries were also affected, and the highest death rates among under-50s were in Oceania, eastern Europe and central Asia.
We can't do anything about our genes, but there's a lot we can do about what we put into our bodies.
Genetic factors are likely to have a role, the researchers said. But diets high in red meat and salt and low in fruit and milk, along with alcohol and tobacco use, are the main risk factors underlying the most common cancers among under-50s, with physical inactivity, excess weight and high blood sugar contributory factors, the data indicates.
[ ... ]
“If people are concerned about their cancer risk, there are lots of ways to help reduce this such as not smoking, maintaining a balanced diet, getting plenty of exercise and staying safe in the sun.”
I would add that eliminating or substantially reducing meat consumption is not just good for our bodies but also good for our planet. 🌎
As for exercise, too many people associate it with joining gyms or investing in Peloton equipment. For most people, all that's necessary is to fit more physical activity into everyday routines. Regularly walking or cycling (when possible) instead of relying on motor vehicles can provide a boost to overall health.
Of course affordable healthcare is essential. Medical professionals can advise us and detect conditions which can be treated before becoming serious.
#cancer#increased cancer risk#people under 50#public health#health#healthy diet#vegetarianism#veganism#exercise#smoking is bad#stay healthy#affordable healthcare
8 notes
·
View notes
Text
5 minute read
Thousands of hospital staff are reporting claims of sexual assaults and harassment by patients, an investigation has found, prompting calls for ministers to address the “daily threat of abuse” faced by doctors and nurses.
More than 20,000 alleged incidents of sexual violence and sexual misconduct by patients on hospital staff were recorded in the five years to 2022 by 212 NHS trusts in England, freedom of information (FoI) requests by the Guardian and the British Medical Journal (BMJ) found.
The 20,928 cases accounted for just under 60% of the total alleged incidents trusts disclosed. Allegations included claims of rape, sexual assault, harassment, stalking and sexualised remarks.
Experts cautioned that the figures were likely to be a serious underestimate as staff are often deterred from making complaints when patients abuse them.
Deeba Syed, a senior legal officer at the Rights of Women helpline, said: “Women tell us they are expected to continue to care for patients who are abusive or harassing without efforts to adequately safeguard them from further harassment.
“We hear worrying reports of women feeling pressured into not raising formal grievances and instead being transferred to different departments or locations. They tell us it is argued that this is more expedient than moving the harassing patient, despite victims feeling this is unsafe to others and a punishment on them.”
Katie, not her real name, a junior doctor in the south-east of England, said patients had made sexual comments about her since she was a student.
“From the word go within clinical placement, I always felt very heavily sexualised by patients,” she said. “One time, when I had to get close up to a patient’s face to examine his eyes, the patient started licking his lips and rubbing himself. I was 19 or 20 at the time and the consultant had left the room – I was completely terrified.”
She said she has also experienced sinister, crude comments, like being asked if she was going to “pleasure” a male patient. Katie said she did not feel she could tell anyone as she found most of the consultants intimidating.
The everyday harassment has made her reevaluate her career path and she is hoping to go into obstetrics and gynaecology so she does not have to treat men. “I find the sexual harassment affects me too much and makes me feel like shit.”
The Guardian and BMJ investigation found trusts recorded 35,606 sexual safety incidents, a term that covers a spectrum of behaviours from abusive remarks to rape, allegedly perpetrated by staff, patients or visitors in NHS hospitals in England between 2017 and 2022.
While the majority were cases of patient-on-staff abuse, nearly 7,500 were allegations of patients abusing other patients and more than 3,000 were cases of staff abusing patients.
Responding to the findings, Simon Fleming, an orthopaedic surgeon and co-author of a 2021 report on sexual assault in surgery for the Royal College of Surgeons, said the NHS needed to take a more robust approach to sexual misconduct by patients.
He said: “Patients abuse staff often. Some of this is normalised, some of it less so. What you permit, you promote, and the NHS needs to stop permitting patients and staff behaving in a way that makes healthcare less safe for all of us.”
Some NHS workers do feel able to speak out. Charlotte Miller, a paramedic at Westminster ambulance station, London, said her employers were “incredible” when she reported being molested while attending to a patient on Edgware Road, west London, in October 2022. The patient, Naveed Ahmed, in his mid-30s, was jailed for nine months in November 2022.
Miller said: “He had already told my crewmate and I we were sexy and had been leering at us, but then he grabbed my crotch. I was really shocked. I’ve had comments before, but that was the first time that someone actively tried to grope me. I didn’t know what he was going to do next.”
As soon as she radioed for help, the police were called and her station sent a colleague, along with an incident response officer. “I had all these phone calls from various managers to make sure I was OK, they told me to have the rest of my shift off and go home to rest. They constantly checked in on me in the days afterwards and helped support me while I made my statements to the police. I couldn’t ask for any better management, if I’m honest.
“I hope this will encourage other people to have the confidence to report these things,” she said.
Dr Becky Cox, a co-founder of Surviving in Scrubs, said: “The stark findings of this investigation should put into sharp focus the work that the health secretary and NHS leaders need to do to ensure the freedom of NHS staff to work without threat of sexual violence from patients and other staff members.
“It was not long ago we were being heralded as pandemic heroes by the government and cheered by the general public, yet we continue to face unsafe working conditions and the daily threat of abuse.”
Surviving in Scrubs lists more than 150 personal accounts of sexual harassment and abuse. They include cases of patients assaulting, molesting and sexualising nurses and doctors.
The health secretary, Steve Barclay, said: “NHS leaders have a statutory duty of care to look after their staff and patients and prevent harassment, abuse or violence in the workplace. I expect employers to be proactive in ensuring staff and patients are fully supported, their concerns listened to and acted on with appropriate action taken where necessary.”
Dr Navina Evans, the chief workforce officer at NHS England, said the health service should not tolerate any sexual misconduct, violence, harassment or abuse.
“NHS England has established a dedicated team to ensure people who experience violence and abuse are supported in the workplace, and there is greater provision of support for all victims and survivors. All NHS trusts and organisations have measures in place to ensure immediate action is taken in any cases reported to them and I strongly encourage anyone who has experienced any misconduct to come forward, report it and seek support.”
• Information and support for anyone affected by rape or sexual abuse issues is available from the following organisations. In the UK, Rape Crisis offers support on 0808 500 2222 in England and Wales, 0808 801 0302 in Scotland, or 0800 0246 991 in Northern Ireland. In the US, Rainn offers support on 800-656-4673. In Australia, support is available at 1800Respect (1800 737 732). Other international helplines can be found at ibiblio.org/rcip/internl.html
14 notes
·
View notes
Text
By: Bernard Lane
Published: Feb 20, 2024
“Gender-affirming” hormonal and surgical interventions do not reduce the risk of suicide for transgender-identifying adolescents, according to an unusually comprehensive and rigorous study.
The landmark research from Finland, an international leader in the shift away from medicalised gender change, found that suicide risk in a large group of adolescents was predicted by the psychiatric problems that often accompany gender distress, not by the gender distress itself.
Dramatic claims of the risk of attempted suicide among trans-identifying youth are typically based on low-quality anonymous online self-report surveys with no follow-up checks, potential exaggeration driven by a constant “transition or suicide” narrative, and “convenience samples” unlikely to be representative.
The new Finnish study vindicates that country’s 2020 adoption of a more cautious treatment policy which first targets psychiatric, social and educational problems among gender-distressed youth before any assumption of a stable trans identity justifying “experimental” affirmation with hormones or surgery.
“It is of utmost importance to identify and appropriately treat mental disorders in adolescents experiencing gender dysphoria to prevent suicide; in addition, health policies need to ensure that accurate information is provided to professionals along these lines,” the researchers say in their BMJ Mental Health paper.
The research team includes the psychiatrist Riittakerttu Kaltiala, from Tampere University Faculty of Medicine, who helped pioneer paediatric gender medicine in Finland, but became concerned when she and her colleagues did not see the good outcomes promised by the internationally imitated “Dutch protocol” of puberty blockers followed by cross-sex hormones and surgery.
Clinical psychologist Erica Anderson, a gender clinician and former president of the US Professional Association for Transgender Health, told GCN she believed that other scientific reviews yet to be published would also “raise questions about the assumption that gender-affirming medicines for youth are protective and prevent suicide.”
“If more evidence is accumulated of this type, one of the most frequent justifications for gender-affirming medicines for minors—that such medicines are lifesaving—can no longer be defended.”
Although Dr Anderson herself practises the gender-affirming model, she has been raising concerns about the weak evidence base and sub-standard clinical practices in paediatric gender medicine.
“Gender-affirming care is medical care. It is mental health care. It is, in some cases, suicide prevention care.”—Dr Rachel Levine, US Assistant Secretary of Health, who is a trans woman and paediatrician appointed by Democratic President Joe Biden, tweet, 13 June 2023
“There’s no epidemic of trans athletes dominating college sports. There IS an epidemic of young trans people dying from suicide as society questions their every civil right.”—Gender-affirming psychiatrist Jack Turban, tweet, 21 January 2021
[ Video: An alarming claim from endocrinologist Norman Spack, who was involved in founding America’s first specialised children’s hospital gender clinic in Boston in 2007 ]
youtube
Under duress
The “transition or suicide” narrative has been used by gender-affirming clinicians, trans rights activists and uncritical journalists to suggest that puberty blockers, cross-sex hormones and surgery such as double mastectomy are “lifesaving.”
Parents hesitant about these poorly evidenced medical interventions have reportedly been asked by clinicians, “Do you want a live son or a dead daughter?”
The suicide narrative also figures in the practice of schools keeping a child’s social transition secret from parents, in the shutting down of debate about the efficacy and safety of hormonal and surgical interventions, and in the promotion of ill-defined bans on “conversion therapy” and “hate speech.”
[ Chart: Trend over time for the Google search terms “trans suicide” and “trans kids”; 100 on the vertical axis represents peak popularity ]
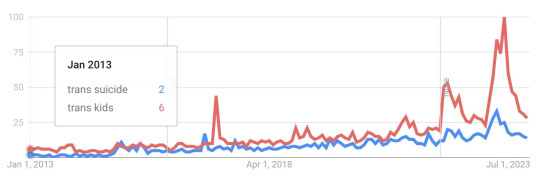
“[The] politically potent ‘affirm or suicide’ narrative has been marshalled at nearly every opportunity in public debates over paediatric gender medicine… By invoking the suicide trope, individual activists, organisations like the ACLU, and Democratic politicians are violating well-recognised, research-based guidelines on how to talk responsibly about suicide.”—Leor Sapir, comment article, City Journal, 17 March 2023
“When communicating about suicide it’s important to remember that suicide is a complex issue and is often not preceded by a single event or condition.”—Mindframe, media advice
“[The] language we use to talk about suicide, how we frame the issue, the content that gets shared on the web and social media can affect what happens next—specifically, whether it contributes to more deaths or prevents them.”—Johns Hopkins Bloomberg School of Public Health, media advice
Quality research
The new Finnish research from Professor Kaltiala and her colleagues allows unusually confident conclusions in a field plagued by low-quality activist studies because it—
• used comprehensive data from national health registers, minimising the problem of unknown outcomes for former patients lost to follow-up;
• tracked suicide as well as total mortality among 2,083 gender-distressed adolescents with a median age of 19 seen by nationally centralised gender clinics from 1996 to 2019, with a median follow-up time of almost six years;
• compared their outcomes with 16,643 counterparts from the general population matched for age, sex and municipality of birth;
• compared outcomes for adolescents who were given hormones or surgery with those who were not;
• isolated statistically the effect of co-morbid psychiatric problems on total mortality and suicide among adolescents with clinically significant gender distress.
Oxford University sociologist Michael Biggs, one of very few researchers to have researched actual suicides linked to a youth gender clinic, said the Finnish investigation was “most comprehensive study ever published on suicide by young transgender people who seek medical interventions.”
He told GCN that the Finnish paper “shows again that the risk of death by suicide for young trans-people is thankfully low in absolute terms. This confirms the results of my own analysis of British data from the Tavistock clinic, with superior Finnish data.”
“Although the rate of suicide [in the Finnish study] is just over four times higher among trans young people than their peers, this is explained by their more serious psychiatric problems. When these psychiatric problems are taken into account, there is no evidence that transgender people have a higher rate of suicide.”
In the 2,083-strong “gender-referred” group* for the Finnish study, there were seven suicides, giving a rate of 0.3 per cent as opposed to a rate of 0.1 per cent in the group of 16,643 matched controls from the general population.
[ * These were patients diagnosed with “gender identity disorder”, the term that predated gender dysphoria and gender incongruence. ]
“Suicide mortality first appeared to be much higher among gender-referred participants; however, the association was fully explained by psychiatric treatment history,” the Finnish researchers said.
“The novel contribution of this study is showing that suicide mortality associates with increased psychiatric needs; this is an important finding if we consider the failure of previous studies on mortality among patients with [gender dysphoria] to account for psychiatric morbidities.
“In light of our findings, experiencing [gender dysphoria] significant enough to seek [hormonal or surgical interventions] appears to not be associated with increased suicide mortality, but suicides appear to be explained by psychiatric morbidities.
“The suicide mortality of both those who proceeded and did not proceed to [these medical interventions] did not statistically significantly differ from that of controls.
“This does not support the claims that [medicalised affirmation] is necessary in order to prevent suicide.
“The risk of suicide related to transgender identity and/or [gender dysphoria] per se may have been overestimated.
“[Medicalised affirmation] has also not been shown [in other studies] to reduce even suicidal ideation, and suicidal ideation is not equal to actual suicide risk.
“To the best of our knowledge, the impact of [these hormonal or surgical interventions] on suicide mortality among gender-referred adolescents has not been reported in earlier studies.”
“This conclusion from the Finnish data is consistent with findings from a multi-country study of suicidality, a related concept. While suicidality in [gender-dysphoric] youth is elevated, it is similar to that of youth presenting with other mental health diagnoses.
“These findings [from Finland] underscore the fact that most youth presenting with [gender dysphoria] have a high rate of co-occurring psychiatric diagnoses, which predate the onset of [gender dysphoria] by months to years.
“[The latest from Finland supports] the direction by the Finnish, English and Swedish health authorities that psychotherapy (rather than medical gender transition) should be prioritised for most youth presenting with gender-related distress.”—Society for Evidence-based Gender Medicine, Twitter thread, 18 February 2024
Back to basics
Dr Anderson, who is based in California, said the conclusion by the Finnish study that gender-affirming care did not reduce suicide risk was “a startling conclusion in the current debate.”
She said the leading Finnish researcher, Prof Kaltiala, was “in a unique position as the head of gender youth care for Finland and a doctor devoted to evidence-based care for gender-questioning youth. She is smart, compassionate and rigorously honest.”
Dr Anderson highlighted the need for an immediate response to young people with severe psychiatric distress and a high risk of suicide.
“It is not enough to pivot to a focus upon gender dysphoria, if present [in the patient], and offer hormones as a treatment for such symptoms and distress,” she told GCN.
“Basic mental health practice dictates evaluation for suicide risk factors and treatment of suicidality.
“In my opinion, this should be the priority and happen first. Beliefs by some that gender affirmation will cure the patient of suicidality must now be questioned, as I have been doing for some time.
“If gender-affirming medicines could not provide sufficient relief to the adolescents so treated and reduce their suicidality, should such patients have received hormones at all? What treatment should these patients have received?”
“[The paediatric gender centre’s] website said, ‘Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that [risk of harm] goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.’
“There are no reliable studies showing this. Indeed, the experiences of many of the centre’s patients prove how false these assertions are.”—Gender clinic whistleblower Jamie Reed, article, The Free Press, 9 February 2023
Try psychiatry, not affirmation
In an earlier study using the country’s health registers, Finnish researchers noted that the surge in gender-distressed patients of recent years and the treatment response had not led to a decline in co-morbid psychiatric disorders.
“Both before and after contacting [gender clinics, these adult and minor patients] present with many more common psychiatric needs than do their matched population controls, even when medical [gender-reassignment] interventions are carried out,” the researchers said.
They said the rise in younger people with psychiatric problems going to gender clinics coincided with the crisis in youth mental health across the Western world linked to more social media use.
Although social media could ease stigma and offer support, the researchers said it might also “result in adolescent and emerging adult females—who present particularly frequently with identity confusion—seeking for a solution to their distress through [medicalised gender change, thereby overshadowing] the need for psychiatric treatment.”
==
"Accept Jesus Christ or you'll go to hell" is the same emotional manipulation.
It's well established that suicide is itself a social contagion, which is why there are guidelines on responsible reporting... which many activist-journalists ignore. So, socializing the obvious lie that people denied transition will kill themselves will itself cause more people to kill themselves than not transitioning will. It's hard not to notice that seems to be what they want, so they can bolster the narrative.
#Bernard Lane#suicide#affirm or suicide#trans or suicide#lies#gender ideology#gender identity ideology#queer theory#medical malpractice#medical scandal#medical corruption#affirmation model#gender affirming care#gender affirming healthcare#gender affirmation#blackmail#emotional blackmail#emotional manipulation#transition or suicide#religion is a mental illness#Youtube
2 notes
·
View notes
Text
Maternal Deaths in Brazil Are Reflection of The Pandemic Denial in the Bolsonaro Administration, Says Researcher
In 2021, the disease was responsible for 52% of deaths among pregnant and postpartum women in Brazil

While the classic causes of maternal death continue relentlessly in Brazil, the country is still investigating deaths from Covid in 2021, the year in which the disease alone was responsible for 52% of deaths of pregnant and puerperal women (1,524 out of a total of 2941).
A recent review of studies published in the journal BMJ Global Health shows that pregnant women with Covid have eight times more risk of death compared to uninfected pregnant women. Newborns also have a greater chance of complications in cases where the mother contracted Sars-CoV-2. An analysis published in The Lancet Regional Health Americas, in 2022, identified at least three barriers that Brazilian pregnant and postpartum women faced during the pandemic.
The first was the difficulty in accessing diagnostic tests. The second was to find vacancies in hospitals. There was an average delay of seven days between the onset of symptoms and hospitalization. Family members heard in the analysis report that the pregnant women went several times to the same hospital or to up to five different institutions before being admitted. The third barrier was access to adequate intensive care after hospitalization.
Between 2020 and 2021, 1 in 5 dead pregnant women did not get access to the ICU, and 1 in 3 who were in the ICU were not intubated, according to data from the OOBr (Brazilian Obstetric Observatory). For obstetrician Rossana Pulcineli Francisco, professor at USP and coordinator of the Brazilian Obstetric Observatory, this factor, associated with the lack of qualified professionals for assistance, was what most contributed to the high mortality rate.
Continue reading.
#brazil#politics#feminism#coronavirus#covid 19#healthcare#brazilian politics#mod nise da silveira#image description in alt
8 notes
·
View notes
Text
What happens when only 16% of flu patients have the flu?
Here is how serious propaganda works: Over a a long period of time, you build up a gigantic lie. You keep reinforcing it.
You have major money behind you, as well as institutions of government, and corporations. You forge that lie, and you keep repeating it over and over.
Finally, and this is the payoff, you reach a point where a refutation of the lie would seem, to most people, like a piece of incomprehensible insanity, like gibberish.
Therefore, the refutation of the lie would tend to be invisible. It would sink like a small stone, leaving no trace.
After writing about fake vaccine science since 1988, I thought I’d seen it all:
Wild falsehoods about vaccines creating immunity; suppressed information about toxic ingredients in the shots and their devastating health effects; the absence of proper controlled studies proving vaccines are safe and effective.
But Peter Doshi, PhD, writing in the online BMJ (British Medical Journal), reveals a new monstrosity. It’s all based on the revelation that most “flu” is not the flu.
Follow this closely. If you blink, you might miss it.
You see, as Doshi states, every year, hundreds of thousands of respiratory samples are taken from flu patients in the US and tested in labs. Here is the kicker: only a small percentage of these samples show the presence of a flu virus.
This means: most of the people in America who are diagnosed by doctors with the flu have no flu virus in their bodies.
SO THEY DON’T HAVE THE FLU.
Therefore, even if you (falsely) assume the flu vaccine is useful and safe, it couldn’t possibly prevent all those “flu cases” that aren’t flu cases. The vaccine couldn’t possibly work.
The vaccine isn’t designed to prevent fake flu, unless pigs can fly.
Here’s the exact quote from Doshi’s BMJ review, “ Influenza: marketing vaccines by marketing disease” (BMJ 2013; 346:f3037):
“…few people realize that even the ideal influenza vaccine, matched perfectly to circulating strains of wild influenza and capable of stopping all influenza viruses, can only deal with a small part of the ‘flu’ problem…Every year, hundreds of thousands of respiratory specimens are tested across the US. Of those tested, on average 16% are found to be influenza positive….It’s no wonder so many people feel that ‘flu shots’ don’t work: for most flus, they can’t.”
Because most diagnosed cases of the flu aren’t the flu.
So even if you’re a true believer in mainstream vaccine theory, you’re on the short end of the stick here. They’re conning your socks off.
A patient walks into a doctor’s office. He’s sick. He’s coughing. He has a fever. His muscles ache. The doctor says, “You have the flu. Did you get your flu shot this year?”
“No,” the patient says.
The doctor gives him a stern look. “Well, you should have. See? You’re sick now. The vaccine would have prevented that.”
Wrong.
Again, even by conventional standards, the odds are very high the vaccine would have made no difference at all. Because the odds are very high this patient doesn’t have an influenza virus.
Overwhelmingly, doctors diagnose the flu with a casual eyeball glance. The patient has a familiar cluster of symptoms? It’s flu season? Okay, it’s the flu. Period.
With an ongoing blizzard of psyop-marketing, people accept “flu” and react emotionally to the propaganda about it.
In 2009, as the heralded Level 6 global pandemic, Swine Flu, was proving to be a bust and a trickle, Sharyl Attkisson (CBS News) discovered that the CDC had stopped counting the number of Swine Flu cases in America.
The CDC had stopped counting, because their tests on diagnosed flu patients showed so many who didn’t have the flu virus, who didn’t have the flu at all.
Atkisson’s reporting was explosive. It was threatening to expose the whole flu psyop. What would happen if it became common knowledge that most people diagnosed with the flu don’t have the flu? What would happened to the campaigns to get people to take flu vaccines?
Attkisson was muzzled. And the CDC doubled down and suddenly claimed there were undoubtedly TEN MILLION cases of Swine Flu in the US. This, after only several thousand cases had been reported.
This is on the order of saying a dry creek-bed in the woods is actually the Mississippi River.
Twisting words and numbers and painting false pictures is the CDC’s job.
Do you have an advanced degree, and are you a liar and a criminal? The CDC needs you.
:::

2 notes
·
View notes
Text
Woman Who Had Dementia For 5 Years Turned Out To Have A Common And Reversible Condition
Woman Who Had Dementia For 5 Years Turned Out To Have A Common And Reversible Condition
https://theheartysoul.com/woman-who-had-dementia-for-5-years-turned-out-to-have-a-common-and-reversible-condition/
A new medical report details the case of a woman who started showing strange “altered behavior” and was diagnosed with dementia for five years. However, her symptoms were actually reversible. The unnamed woman, discussed in BMJ Case Reports, started exhibiting a gradual change in behavior, which was noticed by her family. As well as no longer cooking, keeping […]
The post Woman Who Had Dementia For 5 Years Turned Out To Have A Common And Reversible Condition appeared first on The Hearty Soul.
via The Hearty Soul https://theheartysoul.com/
May 20, 2024 at 09:15AM
0 notes
Text
In 1902, the British Medical Journal reported an unusual case of rapid hair whitening.
A 22-year-old woman “witnessed a tragedy of a woman’s throat being cut and the victim falling dead at her feet,” according to a physician at the London Temperance Hospital. The next day, the right side of her pubic hair turned white, while the left half remained black.
This historic case study makes for a terribly weird (and rapid) example of an otherwise common occurrence: gray hairs seem to accumulate when we’re stressed. And it’s not just random violence that sends people’s pigment running—college exams, children, and work pressure appear to change our coloring, too. But for millennia, scholars have been relying mostly on anecdotal proof and intuition to rationalize this phenomenon. In the absence of clear evidence, many scientists did not believe stress could turn hair snow white, instead arguing the change must be triggered by chemicals or strange immune system behavior. Rare cases where doctors observed the rapid whitening—like in the 1902 BMJ study—were a source of endless consternation.
A 2020 paper, published in the journal Nature, may put some of these arguments to rest. In the study, stem cell and regenerative biologists from the United States and Brazil reported that stress can indeed cause hair to lose its pigment—and they identified a cellular pathway by which it can occur.
To study this vexing relationship, the researchers created an elaborate animal model, which basically involved trying to turn black-haired rats white with lab-made stressors. They tried three different tactics: restraint stress, chronic unpredictable stress, and nociception-induced stress, which is caused by physical pain (or the threat of it). Each successfully turned the rat’s hair white. Perhaps unsurprisingly, nociception-induced stress, which the scientists stimulated by injecting the rats with resiniferatoxin, an analogue of the chili pepper compound capsaicin, worked best and fastest.
Having identified the optimal way to make a rat panic, the team began searching for corresponding changes in the physiological pathways that give rise to coat color. They were particularly interested in the behaviors of two types of cells: differentiated melanocytes, which produce pigment in the hair and skin, and melanocyte stem cells, the raw material from which melanocytes develop. To observe each one independently, the researchers injected their tiny test subjects with the hot pepper-like substance when the rats’ fur was actively growing. At that point in the hair growth cycle, differentiated melanocytes naturally cluster in the hair bulb, while melanocyte stem cells gather together in a separate space called the bulge.
For five days after the injection, the rats’ coats remained black. The differentiated melanocytes in the hair bulb continued to pump out color. But in many follicles, the overtaxed melanocyte stem cells were “completely lost,” the researchers report. Pushed by a flood of noradrenaline, a neurotransmitter that surges in response to stress, the existing stem cells proliferated so quickly that they completely disappeared from their niche. The next time the rats’ coat grew, there were no melanocyte stem cells in these damaged follicles, so white hairs sprouted.
“In just a few days, the reservoir of pigment-regenerating stem cells [was] depleted,” Ya-Chieh Hsu, a professor of stem cell and regenerative biology at Harvard and the study’s senior author, told PopSci in an email. The loss was permanent. “And once they’re gone, pigment cannot be generated anymore.”
“This is an exquisitely elegant paper unrevealing an important mechanism of hair graying,” Alexey Terskikh, who researches development, aging, and regeneration at the Sanford Burnham Prebys Medical Discovery Institute, wrote via email.
But there are many other ways hair can lose its color. A 2018 paper suggested an overactive immune response can also destroy melanocytes and melanocyte stem cells in rats, bleaching their coat. Certain skin cancer drugs turn some patients’ hair transparent. Doctors think it’s a sign their bodies are responding positively to the drug. Genetic pathways, environmental pathways, and mutations can also play a role, according to Terskikh.
Hair still holds many secrets. We don’t know why hair loss plays out differently on someone’s scalp than on their face or, for that matter, their back. And, unfortunately for the anonymous Englishwoman with world-famous pubes, doctors still don’t agree about canities subita, the contested phenomenon where hair blanches seemingly overnight. But, in many cases, scientists are narrowing in on answers. In recent years, there’s been a surge in research and development for anti-balding solutions—and many of them show promise. Terskikh, for his part, is working on regenerating hair from scratch using things like pluripotent stem cells. If it works, we’ll have an unlimited supply of hair—presumably in every shade.
#hair color#science#gray hair#health#stress#Having identified the optimal way to make a rat panic :((((#imagine if they did this to people
0 notes
Text
By Kathy Gyngell February 23, 2024
A NEW covid vaccination study made some mainstream headlines this week – thanks to its size. Bloomberg carefully reported it as ‘the largest covid vaccine study yet finds links to health conditions’, while the Mail‘s headline read: ‘Largest Covid vaccine study ever finds shots are linked to small increased risk of neurological, blood and heart disorders – but they are still extremely rare.’ Note the ‘small’ and the ‘rare’.
So that’s all right then? What does ‘small’ or ‘rare’ mean, I wonder, for people who have suffered and nearly died from Guillain Barré Syndrome (GBS), an ‘adverse event’ highlighted in the Mail’s article, as did Tony Shingler reported on here by Sally Beck? (Transverse myelitis – Tony’s initial diagnosis – which is a closely associated inflammatory disorder characterised by acute or subacute motor, sensory, and autonomic spinal cord dysfunction – had resulted in temporary pausing of the AstraZeneca trial, an association the drug firm of course denied.)
What does it mean for the 295 individuals with GBS identified after Covid-19 vaccination verified in this February 2023 study of US VAERS data, 275 reports (93.2 per cent) of which documented hospitalisation?
What does it mean for the 67 GBS cases recorded between 2020 and 2021 in the UK? (See this BMJ research article published in 2022.) Surely these cases were enough to raise a red flag? People have been crippled and left suicidal. Can someone at GB News put this article we published in front of Rishi Sunak?
While on one level we must be grateful for this now indisputable official confirmation giving the lie to the ‘safe’ claim, the guilty legacy media are still playing it down.
20 notes
·
View notes
Text
Nitrous Oxide Effects Are Reversible With Early Treatment - Technology Org
New Post has been published on https://thedigitalinsider.com/nitrous-oxide-effects-are-reversible-with-early-treatment-technology-org/
Nitrous Oxide Effects Are Reversible With Early Treatment - Technology Org

Nitrous oxide is readily accessible to those who want to use it recreationally for the high it can provide. With just a few clicks, it can easily be bought online. But despite its availability, using the drug—commonly referred to as “whippets” (or “whippits”), “laughing gas,” or “hippie crack”—can have sobering consequences, including permanent, full, or partial paralysis.
The good news is that the damage can be reversed, but clinicians must quickly diagnose and appropriately treat patients, Yale experts say.
In 2020, nitrous oxide was the second most commonly used recreational drug among 16- to 24-year-olds in the U.K., second only to cannabis, according to a British government report. In the United States, its use is now rising rapidly. A U.S. Substance Abuse and Mental Health Services Administration 2019 survey found that almost 13 million Americans aged 12 and older had misused nitrous oxide in their lifetime. Some experts fear that the COVID pandemic may have exacerbated its abuse.
When recreationally inhaled, nitrous oxide can impair the body’s metabolism of vitamin B12. This is a dangerous effect because vitamin B12 is essential for maintaining the body’s myelin sheath, insulating and protecting brain and spinal cord nerves. Nitrous oxide’s long-term use can lead to a range of neurological, hematologic [related to blood], and psychiatric complications, including nerve damage and psychosis.
Now, in a case study published in October 2023 in BMJ Case Reports, Yale researchers have highlighted the urgent need for clinicians to evaluate patients suffering symptoms of impaired B12 metabolism thoroughly. They say that even severe consequences can be successfully treated with quick response.
“Recreational nitrous oxide use is increasing,” says Tova Gardin, MD, neuroimmunologist and psychiatrist at Yale School of Medicine and first author of the study. “If we treat our patients early, we can reverse serious neurologic complications. So, it’s important to know about nitrous use, and it’s important to screen for it.”
What is nitrous oxide and how long has it been used recreationally?
Nitrous oxide is a colorless gas that is used as a sedative for various dental and medical procedures. It is also available for purchase, intended to be used in dispensers to give whipped cream the fluffy consistency found in store-bought cans. When inhaled, nitrous oxide can produce short-lived feelings of euphoria or relaxation. But those who use it may also experience headaches, dizziness, anxiety, or loss of consciousness.
Recreational nitrous oxide use stems all the way back to the late 18th century, shortly after its invention in 1772 by English chemist Joseph Priestly. Another English chemist, Humphry Davey, soon became known for throwing parties in which surgeons and playwrights would inhale the gas from a green silk bag.
In fact, it was through these parties that Davey became one of the first to realize the drug’s analgesic effects. By the mid-19th century, dentists and doctors began experimenting with the drug’s numbing effect on patients undergoing various procedures. Now, it is the most frequently used anesthetic for partial sedation in dentistry. It is also commonly used in surgical procedures in combination with other anesthetics and even in childbirth.
Fueled by the fact that it is both legal and not difficult to get, recreational nitrous oxide use has skyrocketed in popularity. It is especially prevalent at underground raves and music festivals. And, dangerously, its misuse is especially prevalent among adolescents and young adults.
Given the accessibility of nitrous oxide, few who use the substance recreationally are aware of how deeply dangerous it can be.
“It was shocking to me when I visited a popular retail website and typed in ‘nitrous oxide,’ the products algorithmically suggested to be bought together were those that would be used for substance use—not for whipped cream,” says Gardin.
Treating nitrous oxide effects requires thorough evaluation
In her case study, Gardin reports that her team’s recent research was inspired by a man in his 30s who developed numbness, weakness, and difficulty walking after chronic nitrous oxide use. He had no prior issues with mobility. After taking a thorough clinical history, the clinicians learned that he had been using nitrous oxide daily for four to five months.
The team’s first step in understanding what was happening was to order a magnetic resonance imaging (MRI) scan, which revealed abnormalities in the man’s dorsal column. The dorsal column is a central nervous system pathway associated with sensory function. They diagnosed him with subacute combined degeneration of the spinal cord, which was causing his symptoms.
Next, the team looked for any concomitant causes of vitamin B12 deficiency. They performed a blood test and found that the patient’s level of B12 was in the normal range. However, further testing revealed he had elevated levels of two metabolites of vitamin B12—methylmalonic acid and homocysteine. “This gave us a clue that the patient had some sort of difficulty with B12 metabolism,” says Gardin.
From there, the clinicians ran tests looking for antibodies to intrinsic factor and gastric parietal cells. This would signal pernicious anemia, a rare autoimmune disorder that can also impair vitamin B12 absorption. They found this was the case in their patient.
Nitrous oxide effects reversed by vitamin B12 repletion
Treating impaired metabolism of vitamin B12 first required the complete cessation of nitrous oxide use. Then, the clinicians began the repletion process, treating the patient with a seven-day course of intramuscular vitamin B12. He then received weekly injections for one month and, going forward, will need lifelong monthly vitamin B12 repletion. Physical and occupational therapy are required as well. Importantly, mental health care services were also recommended to help with his substance use.
Following treatment, the patient regained sensation and the ability to walk. “Our patient wanted his story shared so that others would know that intervening early allows people to regain neurologic function,” says Gardin. “It would have been easy for us to have chalked up his problems to nitrous oxide use and called it a day. But it’s important to perform additional screening to look for issues with B12 metabolism and B12 deficiency and to make sure such patients get the neurologic and psychiatric care they need.”
What clinicians should know about nitrous oxide use
Gardin emphasized that nitrous oxide use is increasingly common and more extensive than many realize, and that patients presenting with neurologic or psychiatric symptoms related to nitrous oxide use should be promptly screened for other vitamin B12 metabolism issues. Furthermore, treating the complications of chronic nitrous oxide use requires a multi-disciplinary approach addressing all underlying neurologic and psychiatric causes. “The chronic use of nitrous oxide can be part of a reinforcing cycle in which use causes B12 impaired metabolism resulting in neurologic and psychiatric symptoms which can, in turn, reinforce nitrous oxide use. Ensuring comprehensive neurologic and psychiatric care is the best way to treat and prevent relapse for those who chronically use nitrous.”
Source: Yale University
You can offer your link to a page which is relevant to the topic of this post.
#2023#Accessibility#Administration#anemia#antibodies#anxiety#approach#Biotechnology news#blood#Brain#cannabis#Case Study#Cells#cobalamin (vitamin B12)#comprehensive#course#covid#drug#easy#effects#English#factor#fear#festivals#Full#gas#Government#green#Health#Health & medicine news
0 notes
Text
These 7 Magnesium Rich Foods Can Work Wonders For Your Heart Health
Foods high in magnesium can be beneficial to cardiovascular health. You can get the most magnesium from the foods listed below.
Heart health may be improved, and other health problems like high blood pressure and cholesterol can be avoided, by eating a diet high in the nutrients the body needs. Magnesium is an essential mineral for maintaining good cardiovascular function. Since it is involved in over 300 metabolic events in your body, this vital mineral is frequently called the “master mineral.” Isn’t that incredible?

Beneficial Effects Of Magnesium On Cardiovascular Health
Multiple studies have shown that magnesium plays a role in the metabolic processes in your heart muscle that ultimately result in your heartbeat. Magnesium’s importance to cardiovascular health was highlighted in a case study published in the British Medical Journal (BMJ). Cardiomyopathy, cardiac arrhythmia, atherosclerosis, and high blood pressure were all found to be associated with magnesium shortage. High blood pressure, often known as hypertension, is a leading risk factor for cardiovascular disease.If you want to keep your heart healthy, this should be reason enough to increase your magnesium intake. The best magnesium food options for heart health are listed below.
Boost your heart health with these 7 magnesium-rich meals
You may strengthen your heart muscles and protect yourself from cardiovascular disease by eating the foods on this list, all of which are high in magnesium.
Dark Chocolate
Delicious dark cholocate also has a number of health benefits, such as a high magnesium content. According to the study in Nutrients, it also has a high concentration of iron, copper, and manganese. Because of the flavanols it contains, it is also good for your heart. The risk of cardiovascular disease is reduced thanks to flavanols, an effective antioxidant, as reported in Frontiers in Immunology.
Nuts
Nuts, because to their high nutrient content, can be included in a heart-healthy diet. Because of their ability to reduce inflammation, nuts are often recommended as a healthy snack. In addition to assisting with both blood sugar and cholesterol, nuts also protect your heart’s health.
Seeds
Among the finest dietary sources of magnesium are chia, flax, and pumpkin seeds. According to the National Institutes of Health, seeds are also an excellent source of iron, monounsaturated fat, and omega-3 fatty acids.
Fatty seafood
Magnesium may be found in high concentrations in fatty fish like salmon, mackerel, and halibut. In terms of omega-3 fatty acids, the benefits to heart health are greatest from consuming fatty fish.
Bananas
Bananas are well recognised as a healthy food source of potassium since they are both inexpensive and readily accessible. Do you know that potassium also lowers the risk of heart disease? Bananas, which are rich in magnesium and potassium, may be helpful in maintaining healthy blood pressure and heart function.
Leafy greens
Magnesium is essential to health, and leafy greens are a great source. Some of the greatest greens to eat for getting your magnesium fix include kale, collard greens, turnip greens, mustard greens, and spinach.
Whole Grains
Whole grains are beneficial to heart health because they include both magnesium and dietary fibre. Cholesterol levels in the blood are lowered, making the user less susceptible to cardiovascular disease, stroke, and other illnesses.
Source: https://www.healthoncheck.com/these-7-magnesium-rich-foods-can-work-wonders-for-your-heart-health/
Read About These 7 Magnesium Rich Foods Can Work Wonders For Your Heart Health
About The Health on Check
In a world drowning with an overload of digital information, healthoncheck.com brings a sense of calm to the cacophony. It is a leading content platform that provides engaging content across verticals like health, fitness, wellness, lifestyle and relationship among others. Our fresh take on a diverse range of topics spanning multiple verticals keep audiences of varied interests engaged with our infotainment content.
0 notes
Text
Is Tumblr still a thing???
... trying it out again with some new content including original #songoftheday now accompanied by #recipeoftheday and #articleoftheday
first post is an #articleoftheday
I’m very aware that everyone is “over” talking about covid, but immune compromised, disabled & their family members don’t really have the option to just forget about it and move on. I fit into those categories.
here are 8 (recent) articles to read about covid:
Accountability for Canada's covid-19 response — The BMJ
"Covid-19 led directly to 52750 deaths in Canada with more than 4.6 million reported cases as of mid-2023. This cumulative covid-19 death rate of 1372 per million exceeds the global average of 855 per million"
I'm immunocompromised, so COVID-19 is still a big risk for me. When I got into grad school, I had to choose between my health and my education — Insider
"When I expressed my fear of getting sick, well-intentioned friends asked, "If COVID could kill you, why go to grad school?" This question pained me because it reinforced the idea that my immunocompromised status should prohibit me from pursuing the opportunities my peers had access to. The question also placed the weight of my well-being on my own choices rather than on the actions of systems and institutions."
Restrictions likely helped curb spread of COVID-19 in N.S., Dalhousie researchers find — CBC
"In March 2022, Nova Scotia ended its COVID-19 state of emergency and no longer required people to wear masks in most public spaces. The next month, cases in the province hit an all-time high."
She says her boss told her she can't wear a mask, so she quit — Yahoo/CBC
"... the case raises questions about workers' rights and what constitutes a safe work environment."
Long COVID still worrisome 2 years after infection — Washington University School of Medicine in St. Louis
"For far too many people, the continuing and enduring risk of long COVID and its long-term, adverse effects on health are sober reminders that the pandemic is not in the rearview mirror"
What the Fight Against HIV Can Teach Us About Surviving the COVID Era — Vice
"... survivors of the HIV/AIDS crisis of the 1980s and 1990s have been noticing unsettling patterns of human disconnection and disposability through both pandemics."
Long covid has derailed my life. Make no mistake: It could yours, too — The Washington Post
"Masks began disappearing. I tried to warn the people I loved. Covid is airborne. Keep wearing an N95. Vaccines protect you but don’t stop transmission. Few wanted to listen."
The horrific food poisoning of Calgary children underscores the unravelling of public health in Canada — The Globe and Mail
#andre picard#globe and mail#the globe and mail#the globe#washington post#the washington post#madeline miller#long covid#covid isn't over#wear a mask#immunocompromised#circe#vice#vice news#dev ramsawakh#HIV#AIDS#immune system#washington university#school of medicine#health#public health#canada#billy lezra#insider#yahoo#yahoo news#cbc news#CBC#nova scotia
0 notes
Link
[ad_1] Queen Stewart, a lawyer and mother of two, learned she had breast cancer at age 35. She found the lump herself because she was too young for insurance-paid screenings. "I just cried, and I just worried so much about whether I would be here for my girls," Stewart told CBS News. According to a new study published this week in BMJ Oncology, cancer rates worldwide have risen dramatically in people under the age of 50. Researchers examined data from 204 countries between 1990 and 2019. They found that there were more than 3.26 million early-onset cancer cases reported in those countries in 2019, up from 1.82 million in 1990, an increase of 79.1%. The study defined early-onset cancer as a diagnosis that occurs between the ages of 14 and 49. The number of early-onset cancer deaths rose from about 800,000 in 1990 to 1.06 million in 2019, researchers found. Of the 29 types of cancer that were studied, breast cancer in 2019 accounted for the most early-onset cases, 16.5%, as well as the most early-onset deaths, 12.84%. Meanwhile, both early-onset prostate cancer and nasopharyngeal cancer showed the fastest increases in incident rates of any types of cancer over that 30-year period. "Those numbers are remarkable," said Dr. Christopher Flowers, an oncologist at the University of Texas MD Anderson Cancer Center. The study said that while genetics is a contributing factor to the increase, poor diet, alcohol and tobacco use, physical inactivity and obesity also play major roles. "Dietary risk factors (diet high in red meat, low in fruits, high in sodium and low in milk, etc.), alcohol consumption and tobacco use are the main risk factors underlying early-onset cancers," the study concluded. Researchers found that the availability of medical care by region can also impact the number of cases and deaths. "I think it's important for younger individuals who meet screening criteria to consider and pursue screening at age-appropriate times," Flowers said. In the U.S., the recommended age to start colon cancer screenings was recently lowered from age 50 to 45, while the recommended age for breast cancer screenings was lowered from 50 to 40."Look at the importance of screening, and that really gets to the point around those screenable cancers: there's breast cancer, colorectal cancer, cervix cancer," Flowers said. The study projected that early-onset cancer rates will increase 31% by 2030, while cancer deaths will rise 21%. Meanwhile, Stewart had a double mastectomy, chemotherapy and radiation. She's now in remission and says she has a new lease on life. "It had me create a sense of urgency in my life to live now, to find joy, to be more present for my family," Stewart said. More from CBS News Janet Shamlian Janet Shamlian is a CBS News correspondent based in Houston, Texas. Shamlian's reporting is featured on all CBS News broadcasts and platforms including "CBS Mornings," the "CBS Evening News" and the CBS News Streaming Network, CBS News' premier 24/7 anchored streaming news service. [ad_2]
0 notes
Last Seen Blogs




