#a lack of information about their biological family’s medical history
Text
I've posted many times before about how surrogacy exploits vulnerable women and turns their babies into commodities. This article is about the impact of the fertility industry on the children themselves.
‘I slept with my half-sibling’: Woman’s horror story reflects loosely regulated nature of US fertility industry
By Rob Kuznia, Allison Gordon, Nelli Black and Kyung Lah, CNN | Photographs by Laura Oliverio, CNN
Published 10:00 AM EST, Wed February 14, 2024CNN —
Victoria Hill never quite understood how she could be so different from her father – in looks and in temperament. The 39-year-old licensed clinical social worker from suburban Connecticut used to joke that perhaps she was the mailman’s child.
Her joke eventually became no laughing matter. Worried about a health issue, and puzzled because neither of her parents had suffered any of the symptoms, Hill purchased a DNA testing kit from 23andMe a few years ago and sent her DNA to the genomics company.
What should have been a routine quest to learn more about herself turned into a shocking revelation that she had many more siblings than just the brother she grew up with – the count now stands at 22. Some of them reached out to her and dropped more bombshells: Hill’s biological father was not the man she grew up with but a fertility doctor who had been helping her mother conceive using donated sperm. That doctor, Burton Caldwell, a sibling told her, had used his own sperm to inseminate her mother, allegedly without her consent.
But the most devastating revelation came this summer, when Hill found out that one of her newly discovered siblings had been her high school boyfriend – one she says she easily could have married.
“I was traumatized by this,” Hill told CNN in an exclusive interview. “Now I’m looking at pictures of people thinking, well, if he could be my sibling, anybody could be my sibling.”
Hill’s story appears to represent one of the most extreme cases to date of fertility fraud in which fertility doctors have misled their female patients and their families by secretly using their own sperm instead of that of a donor. It also illustrates how the huge groups of siblings made possible in part by a lack of regulation can lead to a worst-case scenario coming to pass: accidental incest.
In this sense, say advocates of new laws criminalizing fertility fraud, Hill’s story is historic.
“This was the first time where we’ve had a confirmed case of someone actually dating, someone being intimate with someone who was their half-sibling,” said Jody Madeira, a law professor at Indiana University and an expert on fertility fraud.
A CNN investigation into fertility fraud nationwide found that most states, including Connecticut, have no laws against it. Victims of this form of deception face long odds in getting any kind of recourse, and doctors who are accused of it have an enormous advantage in court, meaning they rarely face consequences and, in some cases, have continued practicing, according to documents and interviews with fertility experts, lawmakers and several people fathered by sperm donors.
CNN also found that Hill’s romantic relationship with her half-brother wasn’t the only case in which she or other people in her newly discovered sibling group interacted with someone in their community who turned out to be a sibling.
At a time when do-it-yourself DNA kits are turning donor-conceived children into online sleuths about their own origins – and when this subset of the American population has reached an estimated one million people – Hill’s situation is a sign of the times. She is part of a larger groundswell of donor-conceived people who in recent years have sought to expose practices in the fertility industry they say have caused them distress: huge sibling pods, unethical doctors, unreachable biological fathers, a lack of information about their biological family’s medical history.
The movement has been the main driver in getting about a dozen new state laws passed over the past four years. Still, the legal landscape is patchy, and the US fertility industry is often referred to by critics as the “Wild West” for its dearth of regulation relative to other western countries.
“Nail salons are more regulated than the fertility industry,” said Eve Wiley, who traced her origins to fertility fraud and is a prominent advocate for new laws.
Accountability in short supply
More than 30 doctors around the country have been caught or accused of covertly using their own sperm to impregnate their patients, CNN has confirmed; advocates say they know of at least 80.
Accountability for the deception has been in short supply. The near-absence of laws criminalizing the practice of fertility fraud until recently means no doctors have yet been criminally charged for the behavior. In 2019, Indiana became the second state, more than 20 years after California, to pass a statute making fertility fraud a felony.
Even in civil cases that have been settled out of court, the affected families have typically signed non-disclosure agreements, effectively shielding the doctors from public scrutiny.
Meanwhile, some doctors who have been found out were allowed to keep their medical licenses.
In Kentucky, retired fertility doctor Marvin YussmanMarvin Yussman admitted using his own sperm to inseminate about half a dozen patients who at the time were unaware that he was the donor. One of them filed a complaint to the state’s board of medical licensure when her daughter – who was born in 1976 – learned Yussman was the likely father after submitting her DNA to Ancestry.com.
“I feel betrayed that Dr. Yussman knowingly deceived me and my husband about the origin of the sperm he injected into my body,” the woman wrote in a letter to the board in 2019. “Although I realize Dr. Yussman did not break any laws as such, I certainly feel his actions were unconscionable and depraved.”
In his response to the medical board, Yussman said that during that era, fresh sperm was prioritized over frozen sperm, meaning donors had to arrive on a schedule.
“On very rare occasions when the donor did not show and no frozen specimen was available, I used my own sperm if I otherwise would have been an appropriate donor: appropriate blood type, race, physical characteristics,” Yussman wrote.
He added some of his biological children have “expressed gratitude for their existence” to him and even sent him photos of their own children. Yussman, who noted in his defense that he didn’t remember the woman who made the complaint, said his policy decades ago was to inform patients that physicians could be among the possible donors, though neither he nor the complainant could provide records that clarified the protocol.
The board declined to discipline him, citing insufficient evidence, according to case documents. Reached on the phone by CNN, Yussman declined to comment.
The story that really put fertility fraud on the national radar was that of Dr. Donald Cline, who fathered at least 90 children in Indiana. Cline’s case spurred lawmakers to pass legislation that outlawed fertility fraud but wasn’t retroactive, meaning he was never prosecuted for it. But he was convicted of obstruction of justice after lying to investigators in the state attorney general’s office who briefly looked into the case. Following that conviction in 2018, Cline surrendered his license. Cline’s lawyer did not respond to an email seeking comment.
Netflix followed up with a documentary about Cline in 2022 that inspired two members of Congress – Reps. Stephanie Bice, an Oklahoma Republican, and Mikie Sherrill, a New Jersey Democrat – to coauthor the first federal bill outlawing fertility fraud. If passed, the Protecting Families from Fertility Fraud Act would establish a new federal sexual-assault crime for knowingly misrepresenting the nature or source of DNA used in assisted reproductive procedures and other fertility treatments. The bill has found dozens of backers – 28 Republicans and 20 Democrats – amid a renewed effort to push it on Capitol Hill.
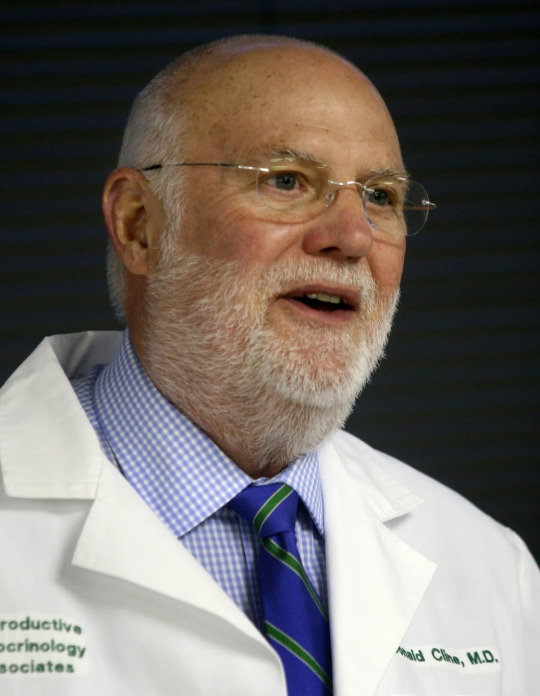
In this March 29, 2007 file photo, Dr. Donald Cline, a reproductive endocrinologist and fertility specialist, speaks at a news conference in Indianapolis.Kelly Wilkinson/The Indianapolis Star/AP/File
A group of advocates including Hill plans to go to DC to champion the bill on Wednesday.
To be sure, passage wouldn’t mean that any of the dozens of doctors who have already been accused of fertility fraud would go to prison, as the crime would have occurred before the law existed. But the measure would provide more pathways for civil litigation in such cases.
The push to better regulate the fertility industry isn’t without critics. It inspires unease – if not outright opposition – from some who fear any industry crackdown could have the unintended effect of making the formation of families less accessible to the LGBTQ community, which comprises an outsized share of the donor-recipient clientele.
“I think we should pause before creating additional criminal liability for people practicing reproductive medicine,” said Katherine L. Kraschel, assistant professor of law and health sciences at Northeastern University. “It gives me great pause … to say we want the government to try to step in and regulate what amounts to a reproductive choice.”
Some experts also point out that the advent of take-at-home DNA tests by companies such as 23andMe and Ancestry has pretty much stamped out fertility fraud in the modern era.
“To my knowledge, the majority of fertility fraud cases took place before 2000,” said Julia T. Woodward, a licensed clinical psychologist and associate professor in psychiatry and OBGYN in the Duke University Health System, in an email to CNN. “I think it is highly unlikely any person would engage in such practices today (it would be too easy to be exposed). So this part of the landscape has improved significantly.”
But activists in the donor-conceived community still want laws, in part to provide pathways for civil litigation, and also to send a message to any medical professional who might feel emboldened by the lack of accountability.
“Let’s say arguably that it doesn’t happen anymore,” said Laura High, a donor-conceived person and comedian who, with more than 600,000 followers on TikTok, has carved out something of a niche as a fertility-industry watchdog on social media. “Pass the f**king legislation just in case.
“Why not just out of the optics – just out of a, ‘Hey we’re going to stand by the victims.’ Let’s just do this. We know it’s never going to happen anymore, but let’s just make this illegal.”

Victoria Hill and her two children play with toys in the living room of her mother's house in Wethersfield. Laura Oliverio/CNN
‘You are my sister’
The lack of a law in Connecticut appears to have been a stumbling block for a pair of siblings seeking recourse for what they allege is a case of fertility fraud.
The half-siblings – a sister and brother – sued OBGYN Narendra Tohan of New Britain in 2021, saying he deceived their mothers when using his own sperm in the fertility treatments.
He has derailed the suit with a novel defense, arguing successfully that it amounts to a “wrongful life” case, which typically pertains to people born with severe life-limiting conditions and isn’t recognized in Connecticut. Tohan, who is still practicing, did not return an email or call to his office seeking comment. The siblings are appealing the ruling.
Madeira, the expert in fertility fraud from Indiana University, called the “wrongful life” decision absurd.
“In fertility fraud, no parent is saying that – no parent is saying I would have gotten an abortion,” she said. “Every parent is saying, ‘I love my child. I just wish that my wishes would have been respected and my doctor wouldn’t have used his sperm.’”
And then there is Dr. Burton Caldwell, who declined CNN’s request for an interview. One of his apparent biological children decided to sue him last year, even though she knows it will be an uphill battle without a fertility fraud law on the books. Janine Pierson and her mother, Doreen Pierson, accuse Caldwell – who stopped practicing in the early 2000s – of impregnating Doreen with his own sperm after having falsely told her that the donor would be a Yale medical student.

Half-sisters Alyssa Denniston, Victoria Hill and Janine Pierson pose for a portrait in Hartford, Connecticut. The three of them say they — and at least 20 others — all share a biological father, Dr. Burton Caldwell. Laura Oliverio/CNN
Janine Pierson, a social worker, thought she was an only child until she took a 23andMe test in the summer of 2022 and was floored to learn she had 19 siblings. (That number has since grown to 22.)
“It was like my entire life just came to this screeching halt,” she told CNN.
When she learned through one of her siblings that Caldwell was the likely father, Pierson said she immediately phoned her mom, who was stunned.
“We both just cried for a few minutes because it just felt like such a violation,” Pierson said.
Pierson said she decided to pursue the lawsuit even though she knows the lack of a fertility-fraud law in Connecticut could pose a challenge.
“It shouldn’t just be, you know, the Wild West where these doctors can just do whatever it is that they want,” she said.
Hill is watching her newly discovered half-sister’s case closely.
For her, the first surprise was learning the dad she grew up with wasn’t her biological father. Although her mom had told her when Hill was younger that she’d sought help conceiving at a fertility clinic, she also said – falsely – that the doctor had used her dad’s sperm.
When Hill learned that the biological father appeared to be Caldwell a few years ago, she contacted lawyers to inquire about filing a suit, but was told she doesn’t have much of a case, so she didn’t pursue it. Now, she said, her statute of limitations is about to expire.
Last year, Hill was hit with another shattering revelation.
In May, she and her three closest friends were celebrating their 20-year high school reunion over dinner.
She was sharing the tale with them of how she learned about her biological father. Everyone was captivated, except one person – her former boyfriend. He looked like he was turning something over in his head. Then he noted that his parents, too, had sought help conceiving from a fertility clinic.
A couple months later, in July, as Hill was leaving for a summer vacation with her husband and two young children, the ex-boyfriend texted her a screenshot showing their 23andMe connection.
“You are my sister,” he said.
Fertility industry regulations in US lax relative to other countries
Hill’s high school boyfriend isn’t the only person she knew in the community who turned out to be a sibling.
“I have slept with my half-sibling,” Hill said. “I went to elementary school with another.”
What’s more, Hill said, back in the early 2000s, she lived across the street from a deli in Norwalk she often went to that was owned by twins who she later learned are her siblings.
Pierson, too, discovered recently that she’d crossed paths with a sibling long ago. She said she has a group photo from when she was a kid at summer camp that shows her on a stage and a boy in the audience. In 2022, she learned that he is her older half-brother.
“Within 20 feet of one another, and we have no idea,” she said.
In general, the bigger the sibling pool, the greater the risk of accidental incest – regardless of whether fertility fraud came into play.
“I don’t date people my age. I can’t do it,” said Jamie LeRose, a 23-year-old singer from New Jersey who has at least 150 siblings from a regular sperm donor, not a doctor. “I look at people my age and I’m automatically unattracted to them because I just, I go, that could be my sibling.”
With this in mind, activists also often advocate for laws that cap the number of siblings per donor – and that do away with donor anonymity. (Neither of these restrictions are included in the proposed federal bill.)
Other countries have instituted such regulations. Norway for instance limits the number of children to eight; Germany, to 15. Germany and the UK have banished anonymity at sperm banks.
The United States government has no such requirements – and the professional association that represents the fertility industry wants to keep it that way.
“What we have not done very much in this country is pass regulations about who gets to have children,” said Sean Tipton, the chief advocacy and policy officer for the American Society for Reproductive Medicine. “If you’re going to say you should only be able to have 50 children, that’s fine. But that should apply to everybody. It shouldn’t apply just to sperm donors.”
Regarding the concern among donor-conceived people about accidental incest, Tipton added, “if you want to be sure that before you have children with somebody, you can run DNA tests to make sure you’re not related.”
The ASRM, which often clashes with donor-conceived activists, has not taken a stance on the federal bill, Tipton told CNN.
The organization does offer nonbinding guidelines that address concerns about incest, recommending for instance no more than 25 births per donor in a population of 800,000.
Although most of the donor-conceived people who spoke with CNN for this story said they wanted to see legislative change, they also described an emotional aspect of the topic that no new law or regulation could begin to quell: a yearning to better understand one’s origins and identity. For Pierson, it was this desire, coupled with a mix of anger and curiosity, that compelled her to pay Caldwell an unannounced visit one day in 2022 – weeks after she’d learned he was most likely her biological father.
Confronting Caldwell
“I woke up that day and I had decided I didn’t want to call him,” Pierson said. “I didn’t want to give him the opportunity to say no. So I just drove directly to his house from work.”
Pierson, who lived in Cheshire at the time, describes an experience that was equal parts surreal and awkward.
After an hourlong trip, she pulled up to a large, stately house with a long driveway not far from the Connecticut coast. When she knocked on the door, nobody answered. But when a neighbor stopped by to drop something off, Caldwell opened the door. Seizing the moment, Pierson introduced herself. He let her in.
Laying eyes for the first time on her biological father, Pierson, 36, saw a man in his 80s with a slight tremor due to Parkinson’s, sporting a blue golf shirt.
He invited her inside and they sat at his dining room table.
Caldwell, she said, didn’t seem surprised – likely because Hill had made a similar visit a couple of years earlier.
“He was not in any way apologetic,” Pierson said, but she added that he did not deny using his own sperm when working in the 1980s at a New Haven clinic. She said Caldwell confessed that he “never gave it the thought that he should have … that there would be so many (children), and that it would have any kind of an impact on us.”
Pierson said Caldwell asked her questions that gave her pause.
“One thing that really has always bothered me is that he asked me how many grandchildren he had,” she said. “And he was very curious about my scholastic achievements and what I made of myself. … Like how intelligent I was, basically.”
She said their conversation ended abruptly when, looking uncomfortable, Caldwell stood up, which she took as a signal that the visit was over. Before parting ways, she asked if he would pose for a photo with her. He consented.
“I knew it would be the only time that I actually ever had that opportunity to take a picture,” she said. “Not that I wanted like a relationship with him in any way because – it was just like mixed of emotions of, you know, like, I despise you, but at the same time, I’m grateful to be here.”

Janine Pierson displays a selfie she took with Caldwell on her phone in Hartford, Connecticut. Pierson took the photo during a visit with Caldwell in 2022 and it is the only photograph she has with him. Laura Oliverio/CNN
#usa#Fertility industry#Burton Caldwell#Fertility fraud#huge groups of siblings made possible in part by a lack of regulation#Accidental incest#Most states have no laws against fertility fraud#huge sibling pods#unethical doctors#unreachable biological fathers#a lack of information about their biological family’s medical history#Nail salons are more regulated than the fertility industry#At least 80 doctors have used their own sperm to impregnate their patients#Marvin Yussman#Dr. Donald Cline fathered at least 90 children#Protecting Families from Fertility Fraud Act still hasn't passed into law#wrongful life#OBGYN Narendra Tohan is still practicing#Large sibling pods in the same community#Norway limits the number of donor conceived children to eight#Germany limits donor conceived children to 15#Germany and the UK have banished anonymity at sperm banks
17 notes
·
View notes
Text
got the tldr of the vid that I'm Not Watching All That & somewhat amusing how the straw breaking the camel's back for people over James Somerton is his blatant and unashamed plagiarism (as it should be genuinely i don't think you can nor should recover from this) like he hasn't regurgitated for years vile, unempathetic, ahistorical and Purely Just Wrong information about gay history including about the fight for legal same-sex marriage in the US and the AIDS crisis. like an alarming amount of people truly heard his ass say "all the good fun funky artistic and radical gays died of aids and all those who were left were unfun stuck-up prudes and conservatives also the fight for legal same-sex marriage was an assimilationist ploy by the latter who just wanted big gay weddings" as if the gay men who survived the epidemic didn't literally lose lovers and friends and entire communities and long-term partners who they shared a life with and who were denied any crumb of this previous life at their death because there was no legal recognition for same-sex cohabitation and unions and their homophobic family could tear everything from the surviving partner thanks to this lack of recognition and let it slide.
some people out there were truly so eager to shit on the boring assimilationist prude gays who survived aids by being stuck-up prudes and who just wanted "big gay weddings" they made up in their minds to get mad at that they turned their brains off and let it slide. they could've used their smoothed-out brains for ONE minute & found out that surviving took 1) plain boring luck and 2) radical, loud, proud gay activists campaigning for safe/safer sex and the information campaigns they led, as well as the protests and demonstrations they undertook to make the government fucking care for once. and that legally-recognized unions [be they civil or religious] were a matter of survival for the partner left behind. some people out there truly let a business major with a turtleneck (possibly the definition of boring) passing himself off as cool and radical and an intellectual tell them homophobic bullshit. and did not blink. like OF COURSE this guy's gonna be a plagiarist. he needs to get his information from SOMEWHERE. because when he tries to formulate his own stuff it's complete fabrications or the frankensteining of multiple sources that he manages to misunderstand/misrepresent threefold over. trying to fit a knit sock over the foot with the inside out and wonder why that itches.
i know many people in his audience are likely very young and also likely american and as such did most of their growing up in a world where their country (1 out of 195. give or take.) had legalized gay marriage but i cannot even begin to describe 1) how Young legalized gay wedding is, even in ""the west"" and 2) how many. other countries there are. my country legalized same-sex marriage before the US did. i am not even 25 and i still remember the hordes of catholics marching down the streets chanting homophobic slogans, implying the only reason two mommies or two daddies would want to raise a child together is for nefarious, vile purposes. i still remember families having to drag their asses into court to argue that, yes, a woman who raised a child for its whole life with another woman she's in a long-term committed cohabitated relationship with should have the right to be considered a direct guardian even if she's not biologically related to the child, and spending thousands of bucks having to argue their case in court. this might be shocking to some, but there are countries where homosexuality is punishable by death. in others, not by death, but by imprisonment. in others, not by imprisonment, but by ""medical intervention"". in others, not by ""medical intervention" but by fines. and in some others still, you can be gay (yay!) but you still cannot get married or civil-unioned, and the very same shit that was discussed in the 80s is still discussed now. the right to stay a guardian of your partner's child if your partner dies or is ill, so the kid does not go into foster care. the right to inherit your partner's property according to married rights instead of having through long annoying time- and money-consuming legal processes. the right to arrange your partner's funeral or have a say in their medical choices if they're incapacitated instead of their (potentially homophobic) families.
like We Are Not There Yet. we are not in a world where any homosexual can truly, fully, wholeheartedly assimilate, whether you consider it a good thing or not. fun gay artists and boring uninteresting gay office workers die the same death that we all do. the one you don't wake from. and guess what. all types of homosexuals, regardless of which ones you pick and choose to be mad at, are affected by homophobic legislation. not just the ones you think should be spared because they're oh so fun. and oh so radical.
donate to the rainbow railroad org if you can. they help LGBT+ people escape state-sponsored violence. a singular nail on one of their members' hand does more activism and real-life good than any mfer making video essays could do in his entire life.
#also were the two gay male writers who died of AIDS who's shit you stole of the ''fun artistic gays'' or the boring ones? you seem to like#their stuff enough to steal. you want their talent their eloquence and their presence; which is missed; sooo bad you look stupit!#also gay people have always gotten married. privately; clandestinely; in secret; in shame often.#gay people have had commitment ceremonies for as long as we've had partners.#like even if some of us did want ''big gay weddings''. by all means cope and seethe that no one wants your hand in marriage#and to dedicate their lives to you as you do to them publicly; to the world's face. but that's a skill issue.#not making this shit rebloggable i'm just complaining about the guy. have disliked him for a while for this ^ & also his fabrication of#how Radclyffe Hall's trial actually went. like you can literally wikipedia this shit.#unrelated me and my dad have this joke where when i feel like my academic life is not too great/i maybe should have done something else#i go ''well i might have gone to the Unemployment Factory; but at least i'm not a Business Student [shocked face] [retching face]''#and my dad hysterically laughs. all of the worst people he's ever met had been business students once.#anyways. allmother mother of all great priestess of dishing out Ls to the deserving#thank you for having taken this man down in such a glorious colossal blaze. CHEH!#neigh (blabbers)
34 notes
·
View notes
Text
Unpacking the Myths: Debunking Common Misconceptions about Mental Health
The state of our mental wellbeing is crucial to our overall health. Njoku (2022), stated that emotions, thinking, communication, learning, resilience, hope, and self-esteem all depend on good mental health. Regrettably, due to the stigma and lack of understanding surrounding mental health, individuals may avoid seeking the necessary help and support they require, creating a cycle of agony and silence. As a teen who has dealt with mental health issues, I aim to dispel the myths and false beliefs surrounding mental health. Mental health has many stigmas and misconceptions that can be detrimental to those struggling with mental health issues.
Myth #1: Mental health issues are rare
Mental health issues are widespread and affect a substantial number of people, meaning that it is probable that you have either undergone a mental health issue yourself or know someone who has, despite the commonly held view to the contrary. According to Schaefer (2017), recent research from our lab and others around the world, almost everyone will experience at least one diagnosable mental disorder at some point in their lifetime.
Myth #2: Mental health problems are a sign of weakness or a lack of willpower
A widespread misbelief about mental health problems is that they indicate a deficiency in one's strength or willpower. Nevertheless, mental health concerns have no correlation with personal weakness or a lack of resolve. Additionally, it is crucial to acknowledge that mental health problems do not imply weakness, and it takes courage to seek aid for them. Comparable to physical health problems, mental health issues require medical intervention and assistance.
Myth #3: Mental Health issues are caused by personality weakness or character flaws
Mental health issues stem from a convoluted blend of biological, environmental, and social components. To be more precise, mental health concerns are frequently triggered by a combination of genetic, biological, environmental, and social factors that further exacerbate the intensity and onset of these problems. Mental health conditions can impact individuals of any personality or character without discrimination.
Myth #4: Individuals with such conditions are not productive
There is a prevailing myth about mental health disorders that presumes individuals with these conditions are unproductive or unable to be productive. This misconception can be particularly detrimental to teenagers who are grappling with mental health concerns alongside the obstacles of academics, social interactions, and extracurricular activities. Nevertheless, many people with mental health disorders can live rewarding and prosperous lives provided they receive appropriate support and treatment. While mental health conditions can hamper an individual's capability to carry out specific responsibilities, they do not define one's complete aptitude or capabilities.
Myth #5: Mental illness only affects certain groups of people
There is a common misconception that mental illness is restricted to particular groups of people. However, mental illness is impartial and can afflict anyone at any stage of their life. According to Njoku (2022), regardless of age, gender, location, income, social standing, race, ethnicity, religion or spirituality, sexual orientation, family history, or other aspects of cultural identity, anyone can be affected by mental illness. No matter one's intelligence, social standing, or level of income, mental illness can affect them (Teacher’s Guide to the Magnificent Mei and Friends Comic Series, 2021).
Misunderstandings and false beliefs about mental health can pose a significant obstacle to seeking appropriate care and support. These mistaken ideas can reinforce harmful stereotypes and lead individuals to avoid seeking help. Therefore, it is important to challenge and correct these misconceptions by providing accurate information about mental health. By addressing and correcting misconceptions about mental health, it is possible to reduce the negative perceptions associated with it and promote the seeking of appropriate care and assistance. It's common for people of any age, background, or situation to experience mental health challenges, so you're not alone. There's help accessible if you or someone you know is going through a mental health problem.
References
Njoku, I. (2022, November). What is Mental Illness? https://www.psychiatry.org/patients-families/what-is-mental-illness
Schaefer, A. R. (2017, July 14). Mental Illness Is Far More Common Than We Knew. Scientific American Blog Network. https://blogs.scientificamerican.com/observations/mental-illness-is-far-more-common-than-we-knew/
Teacher’s guide to the Magnificent Mei and Friends Comic Series. (2021, May 18). World Health Organization.
#writing#writerscommunity#writblr#writers on tumblr#blog post#tumblr blog#mental health#mentalheathawareness
3 notes
·
View notes
Text
What is Illness Anxiety Disorder?
The Covid-19 pandemic has introduced many mental health challenges. The WHO noted that globally, the prevalence of depression and anxiety rose by a massive 25%. Fear and anxiety about the pandemic, isolation, and numerous other factors contributed to this increase, as well as the increase of other types of mental health disorders.
One of these orders that has been heavily exacerbated by the pandemic is illness anxiety disorder. Today, we are going to discuss what this disorder is and what its major symptoms are. Illness anxiety disorder can have major impacts on your well-being, so if these signs sound familiar, it’s a good idea to discuss them with a mental health professional.
What Is Illness Anxiety Disorder?
Illness Anxiety Disorder (IAD), formerly known as Hypochondriasis or Hypochondria, is a psychiatric condition characterized by excessive worry about having a serious medical condition despite minimal or no evidence of illness. People with this disorder often misinterpret normal bodily sensations as signs of a severe medical condition, and this leads to persistent fears of being seriously ill. The preoccupation with health concerns can significantly impact daily functioning, leading to distress and impairment in various aspects of life.
People with IAD often engage in “body checking” behaviors, such as frequent medical appointments, extensive online health research, and seeking reassurance from healthcare professionals or loved ones. Despite repeated medical reassurances that there is no serious illness, individuals with IAD remain unconvinced and may continuously shift their focus from one bodily symptom to another. This constant preoccupation can lead to a cycle of anxiety, as the fear of having a severe illness persists, triggering stress and further exacerbating the perceived symptoms.
What Causes Illness Anxiety Disorder?
The exact cause of IAD is not well understood, but a combination of biological, psychological, and environmental factors may contribute to its development. Individuals with a history of anxiety disorders or a family history of health-related anxiety may be more prone to developing IAD. Additionally, experiences such as a serious illness in childhood or exposure to significant health-related stressors may contribute to the onset of this disorder.
The Covid-19 Pandemic and IAD
In today’s epidemiological landscape, it’s impossible to talk about IAD without talking about Covid-19. The COVID-19 pandemic has had a profound impact on mental health worldwide, and one of the notable consequences has been an increase in health-related anxiety and IAD. Several factors associated with the pandemic have contributed to the development or exacerbation of IAD in some people.
Heightened Health Concerns
The constant stream of information about the virus, including its symptoms, transmission, and potential severity, has led to increased health-related concerns. Individuals may have become hyper-aware of their bodily sensations and interpreted them as potential signs of COVID-19, contributing to heightened anxiety.
Uncertainty and Fear of the Unknown
The novel nature of the virus, coupled with uncertainties about its long-term effects and the constantly evolving public health recommendations, has fueled fear and anxiety. The lack of definitive answers and the unpredictable nature of the pandemic have left many individuals feeling vulnerable and preoccupied with their health.
Isolation and Social Distancing
Measures such as lockdowns, social distancing, and isolation have disrupted normal social interactions and support systems. The resultingloneliness and isolation can contribute to heightened anxiety and exacerbate pre-existing mental health conditions, including IAD.
Media Exposure
Continuous exposure to pandemic-related news and discussions on various media platforms has the potential to increase anxiety. Sensationalized stories and misinformation can lead individuals to overestimate their risk of contracting the virus or experiencing severe health consequences.
Grief and Loss
The pandemic has brought about widespread loss, including the loss of loved ones, jobs, and a sense of normalcy. Grieving and the associated emotional distress can manifest physically and be misinterpreted as symptoms of a severe illness, contributing to health-related anxiety.
Signs of Illness Anxiety Disorder
If you find yourself constantly preoccupied with concerns about your health, often fearing the worst despite reassurances from medical professionals, you may be experiencing signs of IAD. Here are some indications that this condition might be affecting you:
Excessive Worry about Health
You may find that thoughts about potential illnesses dominate your mind regularly. Even minor bodily sensations or normal variations in health can trigger intense anxiety, leading you to believe that you have a serious medical condition.
Frequent Medical Checkups
If you frequently visit healthcare professionals, seeking reassurance about your health despite receiving negative test results or assurances that you are in good health, it could be a sign of IAD. The need for repeated medical examinations may be driven by an overwhelming fear of undetected illnesses.
Compulsive Health Research
You may spend a significant amount of time researching symptoms, medical conditions, and potential health threats online. This excessive information-seeking can contribute to heightened anxiety and reinforce your fears about having a severe illness.
Constant Body Checking
Engaging in frequent “body checking” behaviors is common in IAD. This may involve closely monitoring your body for any signs of illness, such as checking your pulse, monitoring your temperature, or constantly assessing your physical well-being.
Impact on Daily Life
If your health-related worries interfere with your daily life, relationships, work, or other aspects of functioning, it may be a sign of IAD. The constant preoccupation with health concerns can become overwhelming and impair your ability to enjoy life.
Seeking Reassurance
Constantly seeking reassurance from family, friends, or healthcare providers about your health can be a characteristic behavior. Reassurance seeking is a common coping mechanism, but in the context of IAD, it often provides only temporary relief, with anxiety returning shortly afterward.
If you recognize these signs in yourself and they are significantly impacting your well-being, it’s essential to seek professional help. A mental health professional can assess your symptoms, provide a proper diagnosis, and guide you through effective treatment strategies tailored to address the challenges associated with illness anxiety disorder.
Treating Illness Anxiety Disorder
IAD is usually treated through a combination of psychotherapy, medication, and support. The goal of treatment is to help individuals manage their health-related anxieties, challenge maladaptive thought patterns, and improve their overall well-being. Cognitive-Behavioral Therapy, or CBT, is one of the primary methods used to treat IAD. It focuses on identifying and challenging irrational thoughts and beliefs related to health concerns. A therapist helps you develop healthier thought patterns, coping mechanisms, and realistic perspectives on your health.
Exposure therapy is also a good approach for IAD. This is a specific type of CBT that involves gradually exposing individuals to situations or thoughts related to their health fears. The goal is to reduce anxiety over time by facing and overcoming the fear of illness in a controlled and supportive environment.
Finally, mindfulness techniques, such as meditation and mindfulness-based stress reduction can help folks with IAD become more aware of their thoughts and sensations without becoming overwhelmed by them. Mindfulness practices promote a non-judgmental awareness of the present moment, reducing the impact of health-related anxieties.
If you recognize the symptoms of IAD in your own behavior, there is hope. Reach out to the therapy team at Love Heal Grow. Our therapists are very familiar with CBT and how to teach you about coping skills and mindfulness techniques that will help you overcome the strain of illness anxiety disorder.
0 notes
Text
Addressing Mental Health Disparities in the Rizal Community: The Pressing Requirement for Psychiatrists

Rizal, a captivating province in the Philippines, encompasses a dynamic population facing distinctive needs and obstacles. Within its picturesque landscapes and vibrant cities, an imperative demand for psychiatrists has emerged to confront the prevailing mental health disparities within the community. This article delves into the paramount significance of psychiatrists in Rizal, examining the existing gaps in mental health care, the repercussions of these disparities on individuals, families, and society, and the transformative possibilities that arise from enhanced accessibility to psychiatric services.
Depression, anxiety, bipolar disorder, schizophrenia—these mental health disorders know no boundaries, impacting individuals regardless of age or background. Unfortunately, in Rizal, the scarcity of accessible mental health services only compounds the challenges faced by those grappling with these conditions. The struggle to find suitable care leads to delayed interventions, exacerbating symptoms and diminishing the overall quality of life. Moreover, the persisting stigma surrounding mental health issues often deters individuals from seeking assistance, perpetuating a distressing cycle of suffering and isolation.
In the effort to address mental health disparities, the presence of psychiatrists plays a crucial role. These highly skilled medical professionals are specifically trained in diagnosing, treating, and preventing mental illnesses. Their expertise encompasses a profound comprehension of the intricate interplay between biological, psychological, and social factors that contribute to mental health disorders. By employing evidence-based practices, psychiatrists deliver comprehensive care tailored to the specific needs of each individual.
In Rizal, psychiatrists play a fundamental role in conducting comprehensive assessments to achieve precise diagnoses of mental health conditions. These assessments involve gathering crucial information about an individual's symptoms, medical history, and psychosocial background. By adopting a holistic approach, psychiatrists ensure the accuracy of the diagnosis, enabling the development of personalized treatment plans that cater to the specific needs of each individual. Through a combination of therapies, medications, and other therapeutic interventions, psychiatrists provide invaluable support to individuals on their journey toward recovery and enhanced mental well-being.
The shortage of psychiatrists in Rizal presents formidable obstacles to the delivery of mental health care in the region. The limited access to psychiatric services forces individuals to endure long journeys or extensive waiting periods in their pursuit of much-needed care. Unfortunately, this lack of accessibility disproportionately affects marginalized communities, further widening existing health disparities. Furthermore, the scarcity of psychiatrists places immense strain on the handful of available professionals, overwhelming the healthcare system and impeding its ability to meet the growing demand for services.
Addressing the mental health care gap in Rizal necessitates a crucial step: increasing the number of psychiatrists. It is imperative to actively recruit and retain psychiatrists who possess a genuine dedication to serving the community. Collaboration among government entities, educational institutions, and healthcare organizations is vital in establishing programs that advocate for psychiatry as a viable career path and offer incentives for psychiatrists to practice in underserved areas like Rizal. By investing in mental health infrastructure and cultivating an enabling environment for psychiatrists, the province can effectively meet the mental health needs of its residents.
The significance of psychiatrists in Rizal extends beyond the individual level, encompassing broader societal implications. Mental health conditions have far-reaching effects, influencing families, communities, and the overall social fabric. By addressing mental health disparities, psychiatrists play a pivotal role in cultivating a healthier and more resilient society. Improved mental health outcomes yield heightened productivity, strengthened interpersonal relationships, and overall enhanced well-being. Consequently, a thriving community emerges, better equipped to confront the challenges of the future.
1 note
·
View note
Text
What is Crohn's Disease?
Recently, a lot of buzz has been created about Crohn's disease. Many people have misconceptions about this condition and its causes, diagnosis, symptoms, treatments, and prognosis. Understanding the facts about Crohn's disease is essential to manage it properly.

Crohn's Disease at a Glance
Crohn's disease is a form of inflammatory bowel disease (IBD) that affects the entire digestive tract, including the small intestine, large intestine, and rectum. It is a chronic condition that can flare up periodically over time or remain in remission for years without causing any noticeable symptoms. In some cases, however, Crohn's can become active again after a period of remission and can cause severe abdominal pain, diarrhea, and other serious GI problems.
Signs and Symptoms
Some people might have Crohn's disease without knowing it, as it will not show any symptoms. But for most people, the following symptoms are common.
Abdominal Pain
Since Crohn's affects the digestive tract, abdominal pain is often one of the first signs of the condition. Pain can be mild or severe and may come and go depending on how active the disease is at any given time.
Diarrhea
Diarrhea is a common symptom of Crohn's and can range from mild to severe. Diarrhea can also be accompanied by nausea, vomiting, and fever.
Weight Loss
Crohn's causes inflammation in the GI tract, which can affect other systems in the body as well, leading to weight loss that isn't caused by dieting or exercising. Other signs include fatigue, lack of appetite, joint pain, and skin changes such as rashes or bumps.
What Causes Crohn's Disease?
The exact cause of Crohn's is unknown. However, it is thought to be linked to an abnormal immune system reaction in the gut. People with a family history of IBD are more likely to develop Crohn's, and those with weakened immune systems due to medications or other conditions are also at higher risk.
Treatment Options
The treatment for Crohn's disease is focused on reducing inflammation. This can be done with anti-inflammatory drugs, immune system suppressants, and biological drugs targeting specific proteins in the body. In addition to medication, other treatments may include lifestyle changes such as following a low-fat diet or quitting smoking. Surgery may be necessary for some cases where the disease has caused significant damage to the digestive tract.
Treating Crohn's disease will depend on how severe the condition is and factors such as age and overall health.
Prognosis
Crohn's disease is a chronic condition that cannot be cured. However, it is possible to control and reduce the symptoms with timely treatment. The prognosis for most people with Crohn's is generally good if the disease is appropriately managed with medications and lifestyle changes.
It is important to remember that everyone is different, so what works for one person may not be suitable for another. It can take time to find the right treatment plan for an individual's needs, but with patience and dedication, it is possible to manage Crohn's successfully.
Final Thoughts
Understanding Crohn's disease and how it affects your body can help you better manage its symptoms and find a suitable treatment plan. With proper care and support from family and friends, those living with this condition can lead active lives. It is essential to stay informed and up-to-date on all the latest treatments and therapies available, as there is no one size fits all solution. Living with Crohn's disease can be challenging, but it doesn't have to be impossible.
By staying in tune with their body, keeping track of symptoms, and adjusting medications according to the doctor's advice, people living with Crohn's disease can find ways to manage their condition and lead healthy lives.
Rx Helper is a prescription assistance organization aiming to provide medication assistance to under-insured and uninsured patients. The company helps underprivileged patients cover the cost of prescriptions by providing financial assistance. They have collaborated with numerous pharmaceutical companies across the United States to help offer medication services and even free medication for those unable to afford prescriptions.
If you need any assistance with medication, feel free to contact them for more information on enrolling in their program.
0 notes
Text
Identify the causes, signs, and symptoms of hypertension

Hypertension is a common clinical condition characterized by elevated blood pressure levels. It is also known as hypertensive heart disease or high blood pressure. Have you ever wondered what the blood pressure (BP) exactly is?
Blood pressure is the pressure exerted on the lateral wells of the blood vessels, precisely arteries, while the blood flows through them. To better understand blood pressure measurements, you must know about systolic and diastolic pressure. Systolic blood pressure denotes the pressure exerted when the heart beats. On the other hand, diastolic pressure is the pressure exerted on the resting state of the heart between the beats. The normal blood pressure of a healthy adult is 120/80 mmHg. Depending on your activity, your blood pressure changes throughout the day. Therefore, the diagnosis of high blood pressure may be made if blood pressure readings are frequently higher than normal. According to the American heart association, systolic blood pressure of 130-139 or diastolic blood pressure of 80-89 is considered stage 1 hypertension. The condition can be managed effectively with early diagnosis, timely treatment, and lifestyle modification.
Causes of hypertension
The major causes of high blood pressure include increasing age, too high salt intake, family history, obesity, lack of exercise, stress, alcohol consumption, smoking, pregnancy, and chronic metabolic diseases. However, the exact pathophysiology of the developing condition is poorly understood.
High blood pressure symptoms
It is challenging to identify hypertension symptoms, especially in the early stages of the condition. However, in the more advanced stages, the patient complains of recurrent morning headaches, nausea, blurred vision, nose blood, shortness of breath, cardiac arrhythmia, ringing in the ears, exhaustion, chest pain, anxiety, and trembling muscles, along with elevated blood pressure.
Get high-quality hypertension biospecimens online.
Central BioHub is the leading global provider and most reliable online marketplace for human biospecimens. Targeting the research potential for therapeutic, diagnostic, and other biomedical areas, Central BioHub brings you the world's largest and most diverse inventory of clinical research samples. We offer thousands of well-defined, high-quality hypertensive disease samples ethically derived from patients suffering from hypertension.
The human serum and plasma samples from hypertension patients are tested for specific cardiac markers such as Troponin I (TnI), Troponin T (TnT), brain natriuretic peptide (BNP), N-terminal prohormone b-type natriuretic peptide (NT-proBNP), myoglobin, creatine kinase-MB (CK-MB), D-dimer, and cystatin C.
Improving the accuracy of drug and diagnostic research, our biospecimens are well-annotated with clinical information, including patient's demographic details and medical and medication histories. Hurry up, check out our latest inventory update and procure high-quality human biological specimens: https://centralbiohub.de/blogs/procure-samples-from-hypertension-patients-in-just-a-few-clicks
Central BioHub has a premier portfolio of millions of human biospecimens ideal for research, development, and quality control purposes: Contact us for more information on hypertension samples.
0 notes
Text
Racism is a Public Health Crisis Experienced in Personal Tragedies

I was 12 when my 17-year-old brother died. He was not shot by police or targeted by white supremacists, but racism killed him.
Richard had bipolar disorder, and our family relied on Medicaid for health care. After a brief stay in one of very few mental health facilities that accepted Medicaid in Chicago, he became extremely ill with a high fever and trouble breathing. We took him to the hospital, where he was not tested or x-rayed. Instead, he was given an inhaler and told to take ibuprofen. When his condition worsened, we went back to the ER, where staff diagnosed him with pneumonia in both lungs. He was admitted to the ICU and put on a ventilator. Five days later, as my mother and I finally took a break from living in the ICU to shower and change clothes at home, Richard died.
It is not a question to me whether Richard would have received better care if he wasn’t Black. There is a straight line from his Blackness to the health care options available to him to his treatment to his death.
Racism is a public health crisis. It manifests in dramatic inequities in health outcomes across the board — including three times as many COVID-19 infections among Black people and nearly twice as many deaths than white people. It manifests in the daily grind of discrimination and stress on Black bodies. It manifests in where we live, the health care available to us, and how we are treated. It manifests in which mothers must mourn sons who died too early, which sisters grow up without brothers.
Because of the long legacy of redlining and an economic system built on racism, Black Americans are disproportionately relegated to living in poverty-stricken areas. And since most health outcomes are determined by things like poverty, income inequality, wealth inequality, food insecurity, and the lack of safe, affordable housing — the social determinants of health — in all of these areas, Black people have to overcome 400 years of the deck being stacked against us.
If we do manage to get care, we often receive a poorer version in comparison to white people. In 2016, half of white medical students and residents surveyed held false beliefs about biological differences between Black people and white people — beliefs with deep roots in slavery, when physical violence was seen as acceptable because people believed enslaved Black people had “thicker” skin than white people. The medical students and residents with these false beliefs rated Black patients’ pain lower and made less accurate treatment recommendations.
Black women are doubly dehumanized. For centuries, we have been denied the rights and resources to make our own decisions about our bodies. Our desires are dismissed, our pain is ignored, and our needs go unmet. And it kills us. It’s why Black women are more than three times as likely to die of pregnancy and childbirth-related causes.
The racism in the U.S. health care system is borne out in these numbers, and in stories like my brother’s … and mine.
In 2018, I made the decision to get an abortion. I went to a local clinic in Brooklyn. I did not feel ashamed about having an abortion, but I was treated as if I should be. I was forced to have two visits with two ultrasounds before the procedure, and was ordered to go from room to room without being given any information about what was going on or what would happen next. I was seen by several doctors who didn’t even attempt a decent bedside manner and couldn’t pronounce my name.
The first doctor simply told me, “You can’t smoke cigarettes or drink alcohol,” without giving me any information on my options or asking me if I’d like to continue the pregnancy. I had to ask several times for information on abortion. I was then reluctantly, coldly told that medication abortion was “out of the picture” because insurance wouldn’t cover it. I felt like I had no control over my body.
If this was my experience in Brooklyn, in a state with liberal abortion laws, I can only imagine what people in states where access to abortion is even more restricted must be experiencing.
Trust me when I tell you: Black people feel pain. And we thrive in spite of it. For decades, Black people — Black women in particular — have been at the forefront of the movements to hold this country accountable to its promise of equality and justice — the Civil Rights movement, women’s suffrage, the LGBTQ+ movement, and reproductive justice. Black women started Black Lives Matter, now recognized as among the largest protest movements in U.S. history.
It isn’t enough to tear down statues of Confederate generals (as much as they should be). As American white supremacy meets this moment of reckoning, Black people still suffer from health inequities because of racism and a for-profit health care system. We will only see change when we start to break down and rebuild the longstanding institutions that have historically been used as tools of oppression. We need to tackle the racial inequities in health care head on. Racism as a public health issue needs to be widely understood, especially by all who enter the medical field.
The health care system is killing us, as surely as police are. No more Black people should die from racist violence, or from illnesses that could be treated with just a little more care. No more Black women should experience the dehumanization I felt while getting care that is my right to have.
Racism is a public health issue, and all lives will matter when Black lives do.
-Leanna at PPFA
Leanna Burton is a media assistant in the Communications & Culture division at Planned Parenthood Federation of America. She was born and raised in Chicago, IL and studied journalism at City University of New York - Brooklyn College. She is also a musician and freelance writer whose main focus is lifting the voices of people in underserved and undervalued communities.
574 notes
·
View notes
Text
More therapy thoughts part 1/?
Behavior Theory Frameworks/Conditioning and What the fuck does Master Chief talk about in therapy?
Ramblings below - like a lot, like I spent too much time writing this and you should not read this
Behavioral Theory could work well as a framework with rehabilitating Spartan IIs if the case worker focused on Operant Conditioning Theory and Cognitive Social Learning Theory, which I talked about in this ask because I think I’m funny and this blog is an archive of me applying human behavior theories to video games.
Spartans have always been taught the mission comes first! Always! The 2s are indoctrinated from age 6-14 and then have that reinforced the rest of their lives. From the beginning they are taught to push themselves to the limits, earn their food by winning, form bonds with teammates but be ready to sacrifice them for the mission. The whole lives wasted vs spent conversation between John and Mendez after the augmentation surgery!
What the UNSC/ONI wants comes before their lives, the lives of other soldiers, civilians, AI etc. This constant conditioning of expectations and rewards has created the norms cemented in their minds. This becomes standard operating procedure.
Spartans are also an entirely separated social group, other people have made really great posts on how they are Othered and have their own way of communicating with body language. ODSTs hate Spartans, marines see them as cyborgs or saviors, and while they’re allies, Spartans are not seen or treated as human, by literally everyone. They are a means to an end, with the original goal being to maintain the UNSC’s position of power and crush the insurrectionists in the outer colonies, but uh oh Aliens!
Maybe the 2s aren’t as expendable as the 3s but the mindset and reinforcement of “mission first, people second” being repeated their entire lives is going to stick. So is the constant mistreatment and abuse from their fellow soldiers and handlers.
Addressing the cognitive distortions that come from their upbringing while also balancing the fact that Spartans are so fundamentally different from the way they developed to survive would be so much work, especially considering how much information on them is given to their therapist. The main distortion I would apply is minimization, making large problems small and not properly dealing with them, and specifically for John, personification, accepting blame for negative events without sufficient evidence.
Like these are grown ass super soldiers who can kill you in less than a second and calculate the amount of gravity in a room on the fly but then also can flounder when trying to comfort civilians or make small talk because their experiences and values are so alien to adults who had more developmentally “normal” lives.
Literally applying therapy to Spartans would be like, what was done to you was wrong, the ends do not justify the means, you were children and the adults in your life failed to protect you. You are a human person who is fallible and did the best you could with what you had. And the Spartan would say, “sounds fake but okay, can I pass my psych eval and go back to war now please?”
Jumping back to Behavior Theory
Different approaches to therapy under the Behavior Theory umbrella help modify negative behaviors with treatments like Cognitive Behavioral Therapy and Dialectical behavior therapy that teach individuals adaptive coping like emotional regulation, distress tolerance, cognitive distortions, and interpersonal communication. And that’s just one framework under the umbrella of human behavior theories.
Social work therapy is different from psych as it approaches individuals with heavily researched, evidence-based theories and frameworks in a holistic viewing of person-in-environment, instead of a strong focus on internal psychology.
Social work looks at all the interacting systems, environment, history, and internal and external factors affecting an individual. One of the most useful frameworks is the Biopsychosocial-Spiritual Frameworks (BPSS) when helping a client. It helps with identifying all the intersecting factors, both risk and protective, that shapes a client’s lived experiences. The most important thing to remember is that the individual is an expert in their own life, they know their experiences best.
The hardest part is applying this to Spartans because they Are So Fucked, their lived experiences, their environments and systems and institutions interacting with them, and the amount of their personal information that is probably so classified.
BPSS is a tool to help social workers assess individuals and their situations by collecting info that is related to the presenting issues and current and past circumstances. Info like medical history, hospitalizations, substance abuse, mental illness, personal relationships, family history and background, culture and norms, education, legal history, spirituality and participation etc. is all under this framework.
For Spartan 2s most of this info is lost or classified and helping someone who has repressed every negative emotion they've had for the sake of the mission would be so much to unpack but that’s also why you’re reading the mad ramblings over an over caffeinated nerd on the internet.
Life Course Theory which looks at developmental milestones and the individual’s experiences versus the socially expected markers, how do you apply that to children who were taken and have lived such different lives?
While early adolescence is when “normal” development of thoughts of self and identity take place alongside the physical changes of puberty, Spartans were being turned into emotionless calculating weapons. Sorry John, no forming a sense of identity and peer bonds for you, go kill that Watts guy who betrayed us and joined the insurrectionists.
And now that I’ve gone this insane and opened 2 whole textbooks up, let’s get to Master Chief thoughts. If you’ve read this far thank you, I swear I’m normal, 2020 has just been a weird year.
Why the fuck did I think I could write a therapy fic on a guy with 20 minutes of actual dialogue across almost 2 decades of games?
I make fun of him and call him a himbo, but he’s smart, he knows he’s being used and there is resentment there that’s been building for years.
There’s also decades of trauma and combat experience, physical, and emotional abuse, the lack of a support network, lack of an identity, the biological factors and aftermath of the augmentations and injuries he’s received, a whole lot of grief and self-inflicted guilt.
The loss of a third of his peer group with the augmentation surgery, Sam’s death, the loss of Reach (the only place he’s considered home), Keyes, the Pillar of Autumn crew, Miranda Keyes, Johnson, Cortana. He cares about the marines who fight with him!!!
He just stands there and takes it and rarely snaps, and even then it’s just small cracks on the surface with fissures running deep. The few details I will pull from Halo 5 are Blue Team’s reactions to John pushing himself so hard from the beginning of the game, and the literal crack in his armor from the fight with Locke. Like dude.
John’s a leader and will get the mission done but he tugs on the leash. He’s earned enough of a reputation and uses it to get his way.
Halo 2’s “Permission to leave the station” with Mr. “I’m going to hand deliver a bomb to the fusion reactor of a covenant supercarrier and hope my friends catch me”.
Halo 4 is when we see him say no to a superior officer and then 5 is him going AWOL. Palmer literally points out that no one is going to stop him.
Halo 5 kills me for many reasons but John bringing up Halsey and what she did to him and also pointing out that he knows Halo 5 Cortana is trying to manipulate him with psychological tactics hurts.
He knows what’s been done to him!
I cannot remember which book it was but John isn’t used to working alone. He literally takes fire because he was expecting someone to have his back!
He’s lost without Cortana! She was in his brain! Y’all! I played Halo Combat Evolved on the original xbox when I was like 8 and I knew these two were meant to be together. From the moment they met they had great chemistry and relied on each other! Cortana literally goes after people who have it out for John! John wants her approval and shows off for her in one of the books.
I’ve already written too much here but like all of the games have John showing off for Cortana, making dry jokes, jumping out of things he shouldn’t.

The whole point of this rambling is to try and get my thoughts about how to approach John’s character under control.
And that’s the thing. He’s lost control. He’s lost people, he’s losing his position and being phased out as an aging spartan, a relic. John’s used to following orders and making some decisions on the battlefield but it was always short term.
He has no identity beyond being a weapon. Complete the mission, clear the LZ, get put in cryo. Rinse, repeat.
The timeline of the games are what I'm most familiar with but with the comics and books too it’s one long run from Halo 2 to Halo 4. Cairo station to the Dreadnought to the crash landing to Forward Unto Dawn to Requiem to “The Didact is Dead but not really but we’ll deal with him off-screen”.
I know Hood apparently gave John R&R orders before Halo 5 that he ignored and kept running himself into the ground. This is a man who has to keep moving and keep being useful.
I imagine him giving in and seeking help as a last resort to fix any problems he has with performing his duties rather than helping himself be healthier.
Any professional he sees is going to have to approach him like they’re approaching a self sacrificing feral cat, with lunch meat and quiet. This man needs to have his support network closer, set up long term goals, and do some serious, and most likely incredibly painful, self reflection on where he’s come from and where he wants to go. Get him out of that tin can and into therapy.
I don’t have a nice neat ending because this was a ramble and also therapy is not neat and tidy. Thanks for reading my words about mr halo
#this is not coherent but it needs out of my brain#John - has different characterizations based on what media he's in#Me - my writing must be in character or I Will Die#also me - we don't talk about halo 5 but i will loot its corpse for bits of lore I like#im sorry for being like this#my writing#Therapy time#John 117#this is not a halo blog#haha this was peer reviewed nonsense#thanks yall for enabling me#i have even more ideas for the infinity sitcom folder now
46 notes
·
View notes
Text
❝ that’s all history is after all: scar tissue. ❞
{ cis-man, he/him } huh, who’s FROY GUTIERREZ? no, you’re mistaken, that’s actually SCORPIUS MALFOY. he is a TWENTY-TWO year old PUREBLOOD wizard who is A HEALING APPRENTICE. he is known for being CAPTIOUS, RETICENT, FACETIOUS, DISMISSIVE, and DRAMATIC but also RESOURCEFUL, CONSCIENTIOUS, FERVENT, INNOVATIVE, and OBSERVANT, so that must be why he always reminds me of the song IN DREAMS BY BEN HOWARD. i hear he is aligned with THE ORDER OF THE PHOENIX, so be sure to keep an eye on him. { merry, 24, gmt, she/they }
CHARACTER PARALLELS: Amy Santiago (B99), Claire Temple (Daredevil), Chidi Anagonye (The Good Place), Giles (Buffy TVS), Michelle Jones (MCU), Simon Tam (Firefly), Elizabeth Swan (PoTC), Spock (Star Trek), Clarke Griffin (The 100), Harley Keener (MCU), Gregory House (House) suggested honorable mention Gizmo (Gremlins)
pinterest [blood, medical imagery tw]
wanted connection ideas
Full Name: Scorpius Hyperion Malfoy
Gender/Pronouns: Cis man | he/him
Age: Twenty-three
Birthdate: January 20th
Parents: Draco Lucius Malfoy & Astoria Céline Malfoy (née Greengrass) [Not biologically Astoria’s due to her health, if you ever point this out he’ll flay your eyeballs]
Siblings: N/A.
Birth place: St. Mungo’s Hospital, England
Height: 5’11”
Weight: 56 kg
Sexual/Romantic Orientation: Demiromantic Bisexual
Nationality: British
Body Alterations/Marks: A ragged diamond shape scar at the base of his throat.
Blood Status: Pureblood
Hogwarts House: Slytherin
Wand Arm: Right
Pet: His pet toad, Jarvis, recently passed away.
Patronus: Arctic Fox
Wand: 11 2/3 inches, Willow, Supple, Dragon Heartstring.
Willow is an uncommon wand wood with healing power, I have noted that the ideal owner for a willow wand often has some (usually unwarranted) insecurity, however well they may try and hide it. While many confident customers insist on trying a willow wand (attracted by their handsome appearance and well-founded reputation for enabling advanced, non-verbal magic) my willow wands have consistently selected those of greatest potential, rather than those who feel they have little to learn. It has always been a proverb in my family that he who has furthest to travel will go fastest with willow.
Personality Traits: Brilliance, innovative, empathetic, individuality, openness, social consciousness, inventive, logical, practical skills and self assertion; lack of attachment to people outside his circle and the “real world,” over-intellectualizing of the emotions, dismissive, anxious, crotchety tempered, facetious, rigid, prone to self-isolation, intellectual arrogance, and stubborn.
Zodiac Sign: Aquarius/Capricorn Cusp
Moral Alignment: Neutral Good
Core values: Loyalty, Knowledge, Hope
Four temperaments: Melancholic
HOGWARTS HOUSE ANALYSIS
Slytherin Primary and a Burned Ravenclaw Secondary.
Slytherin Primaries prioritize their own selves and loved ones first. Slytherins don’t feel guilty or selfish about this– they feel righteous and moral. The most important thing is to look after your own. Abandoning or hurting one of your own is the worst thing you can do.
A Burned Ravenclaw Secondary might want to be skilled, curious, and prepared, but they feel like they are (or like people think they are) limited, clumsy, or inconstant. Gathering knowledge, hobbies, skills, or tools is the right way to achieve their goals, but Burned Ravenclaws know that’s not going to work within their capabilities. So they take other paths and use other tools– maybe a Gryffindor’s bluntness, a Slytherin’s flexibility, or a Hufflepuff’s slow and steady dedication.
You may have a Hufflepuff Secondary Model.
Hufflepuff is the House of grit, reliability, and determination, and Hufflepuffs use those values to help live, act, and succeed. If you model Hufflepuff Secondary, you also value these things and like to live by them. You like to be hardworking, dedicated, and consistent– but you wouldn’t feel guilty for abandoning those values in the service of other, higher priorities. If there’s another, easier way to get what you want– you’d take it. You think hard work provides valuable rewards– and those rewards are why you work. The work doesn’t have persuasive value in itself.
Despite his very best resistance he’s always been pretty empathetic in nature, he tries to rule his emotions as well as he can but fails more often than not. He was always one of those toddlers that if another kid started crying he’d be right along with them, not because he wanted attention but because he just couldn’t not. A bit of a crybaby, has researched how to magically seal up his tear ducts. Obviously managed to keep the family’s flair for the dramatic there as well. After a few years he leant into the sarcastic vague-snobbishness to hide the core of overwhelming anxiety.
Just managed to scrape through his schooling with nearly all top grades, this isn’t really due to him being a model student. He has always accrued information with a voracious appetite. Any knowledge he could find, even if most people would consider it entirely useless. His mind clicks into that place? You can’t keep him away. However, when there is not an immediate stir of interest on his approach to a topic he has to fight with himself tooth and nail to carry on.
Predictably found exam season highly stressful, was never open about it but was quietly competitive and silently smug over his good grades. Could comprehend well above his reading level from an early age and would often look into experimental research and complicated magic but found himself lost in OWL level History of Magic when chapter upon chapter lay ahead of him about something that didn’t catch his interest. Some people he beat just to spite cause he hates them. It worked, whatever.
Tends toward introversion and finds himself tired sometimes quite easily by a large amount of social interaction. Witty and big-mouthed when he feels comfortable or is in the presence of those that embolden him and very likely to get flustered and snap at people when things are becoming a bit too much. Especially if he feels however unjustly that someone is blocking his escape. Has matured slightly in this since leaving school but it happens still, he’s just anxious. Quite fickle and can at the drop of a hat decide that he’s done with you for the day once his Give Me Attention Meter is maxed. Could be an absolute bloody brat when he felt like it but feels he has grown out of it, which he mostly has.
Always been very, very aware of many people’s distrust of him and his family, he used to sneer and play it up if anyone tried to bring up his dad and go on the offensive but was genuinely affected quite deeply by it all. In his early school years, despite his weakness to the cold, he constantly had his sleeves rolled up to the elbow so that his blank forearm was bared as a statement to just about everyone. I am not marked, I never will be. Now he’s older he has more of a handle on things and can be diplomatic in situations where people are clearly discomforted by his presence and his family history.
Even though the war culminated far earlier in this verse I imagine Scor would have had to have been relatively sheltered as a child if not for how emotionally sensitive and prone to periods of ill-health he was, it was definitely for his own safety. He is still the grandson of a known high-ranking Death Eater and that made him a media target and put one on his back for anyone else that might happen to be watching.
Never produced much of a talent for offensive magic and wouldn’t resort to those methods unless he had literally no other choice, not a front line fighter by any means. His talents with strategy, potion-making, healing and his perseverance with defensive magic are what define him to the Order. While everyone kind of knows who he hung out with at school and who his friends are he is deliberately very mischievous with releasing rumours and misleading people. He deliberately keeps his cards very close to his chest so most people don’t know that he is aligned with anyone, he usually uses glamours or a scarf to conceal his identity if he has to.
While he is knowledgeable about healing and anatomy, he is the WORST at taking care of himself. The literal embodiment of Healers make the worst patients, tends to forgo sleep and basic bodily needs if he’s locked into what he’s focusing on. Sometimes needs reminders to sleep and eat, like a child.
Healing is the most satisfying part of his life and he would never give it up, he likes to experiment as he has a fascination with magic and muggle science and where they might intersect. A fucking nerd honestly. While he thinks he’s being fairly subtle about it a large part of his academic life has been doused in research into blood maledictions, for obvious reasons. He does his best not to flutter too obviously around his Mum. She is capable and ten times stronger than he is.
Lives in a small studio flat in Diagon Alley that is mostly stacks of books and makeshift shelves.
the stillness of the world the moment you take the first step into fresh snow, cashmere and fine wool, the pearlescence of dreamless sleep draught, the scratch of a quill on parchment, faintly tremoring fingers, a shiver up your spine in a warm room, the exhilaration of a problem solved, a thunderous grey overcast sky, the bite of a stitching charm, sleeves rolled up to the elbows, petrichor, the burn in your eyes before a well of tears.
Always had somewhat fragile health tending toward sickly. Hands are never warm, his existence is an endless heat seeking mission.
Went to one Slug Club meeting and used his time to verbally berate and or challenge most of the contacts in attendance, he was not asked to return.
Potions Club, Charms Club, used to sometimes be willing to be dragged to Dueling Club but didn’t enjoy himself.
Plays quite a bit of chess.
Bruises like a fucking peach and scars so easily.
Views quidditch as a good fly spoiled.
Is a very skilled pianist almost entirely due to his Grandmother’s tutelage.
Surprisingly great with children/toddlers/babies, no one including himself expected this, he mostly feared them beforehand.
Bit of a mummy’s boy in that he practically GLOWS when people talk of Astoria’s achievements.
When he has time off from healing he will have chipped black nail varnish on.
Highly intelligent but rarely manages to match a pair of socks, chews his quills but no one else’s.
While very eloquent and well spoken, he is markedly less posh than when he first arrived at Hogwarts.
When he isn’t prone to bouts of insomnia he can take a nap pretty much anywhere. He was once found in a tree after several frantic hours search.
[ CREDIT : CHARACTER PSD template by @karmahelper (defunct url) I tried to find a current social this week by messaging around but couldn’t find anything unfortunately. Forgot to copy this over from the google doc! ]
23 notes
·
View notes
Note
I'm thankfully for your posts on covid and it's variants. Though I do wonder does covid create a biological backdoor on the previously infected? With the way you've been talking about delta.
I'm glad the vaccines work. But the idea the raw covid might be setting up its hosts for reinfection is kinda scary.
Let me remind followers, and I say it also in my long ass post. I'm not a doctor, or nurse, I'm a marketing agent. I study trends and patterns and psychographics present in our society and culture.
However, I do casually browse medical journals and documents certified by credible sources such as the National Library of Medicine and the Mayo Clinic is a good resource. Much of my reporting is based on current information on viral pathogens and how they spread, coupled with historical emphasis, how the general population reacts to these cataclysms - See Spanish Flu 1918. I speculate and converse extensively with my family member, who is a retired nurse. I never want people to think I know everything or anything at all, if I feel secure in posting or 'reporting' some information, I will. But don't believe anything I post about faithlessly, because like the doctors and trained medical professionals, we are still learning from this virus. The learning will never stop, and it is our only tool to protecting those we care about.
As always, please communicate with your doctor or medial provider, have a good relationship if you can. If you don't have a doctor, then gently search through sources available online. We are fortunate to have access to so much.
And please, for the love of the RNG gods, do not gargle iodine. Do not take horse grade deworming paste. Wear a mask. Social distance. Wash your hands. Get vaccinated if it is medically possible for you. Shooting a light up your butt is not the answer.
The vaccine and its recipients who have been battling covid for months – the long-haulers – has shown to improve their overall health, though as I remind people, the vaccine and its impact depends on the receiver and their health history. The vaccine is always the last line of defense, when all else have failed, because you really don’t want to be a Patient Zero case.
I like this term biological backdoor, like in the same way malware can breech security in an otherwise fortified database. We still do not know enough to really discern why delta is hitting previously ‘immune’ individuals, wherein these people did not take the same level of precautions in state counties dense with covid infection. The ideal that some viral pathogens can set up a host carrier for another infection from a virus or bacteria is not new, and this is why early vaccinations for so many illness remain essential for kids before attending schools. Even if a child, as in the case with Polio, may not become horrendously ill from a virus, the encounter can leave an imprint which disarms them against other pathogens later in life.
Covid is so very new in its behavior, and it really hinges on being primmed to encounter it before irreversible damage is done, or worse. I discuss that people I have observed may have contracted covid at some point, but the majority did not appear ‘afflicted’ by the infection, as is the case in covid original. Some people tested positive for it, but the illness didn’t do anything but present as a flu. In some people it destroyed without remorse, and in others it was considered a ‘mild infection’. But I always refer to the asymptomatic carrier as a myth, because covid may not immediately overrun the alveoli tissue in the lungs, and might instead establish itself in the blood tissue foremost, and move on to other softer tissues via the capillaries. In this, the person is infected, and during this time they are not healthy – usually lethargy or other mild side effects unrelated to what may be perceived as rhino virus or flu. Some of these people could be unknown carriers of covid for months, before their immune system begins to falter under the strain of fighting off a foreign invasion and covid crash occurs. That is, the cytokine storm wherein the body launches a massive auto-immune attack on itself because it cannot establish what cells are viable and which cells have been compromised.
In these individuals, if the immune system responds aptly and destroys infected cells, that have not nested in organ tissue such as kidney or liver, then the body removes the carrier cells without detrimental affects to the host. However, because covid has placed itself in blood tissue, removing all traces of the virus might be impossible without intervention. This is why the vaccine was so critical. In some individuals, the appropriate immune response couldn’t nullify the covid threat fully – the virus may not kill them immediately, but they cannot recover either. Such as the long-haulers who waited in limbo with persisting side-effects from the initial infection.
In others, trace cells may remain from the infection. Compromised cells which have not been removed, due to the lack of Monocytes responsible for the entire supply of red blood cells that might be compromised. There is a top 8% of monocytes out of the entire white cell count. As well, it takes about a month for a red blood cell to complete its life cycle, in that aspect, I estimate it can take months or years for these individuals to purge completely of viral traces. These damaged cells remain though, and might offer host to the delta variant. Or in the least, provide a blueprint or trace chemical/RNA information for the virus to replicate on. All in all, those who have a prior infection to covid but did not present symptoms, does not stop cells from being compromised and as such, leaves the host vulnerable to the delta wave regardless of prior health history.
All of these hypotheticals are based on information gathered on HIV, rabies, meningitis, ebola, and many others – regarding what makes a virus deadly, what constitutes a healthy carrier, and where antibodies might produce. It depends on genetics and a trained immunity response – ie, vaccination and good health.
This is why the vaccine is essential to the general public. It is a step towards teaching the body what to look for if a covid encounter occurs. Once covid begins replicating without contest, it can be difficult for the body to deal with ongoing. And other medical reports have stated that those who had covid prior, then get vaccinated, have good protection from the virus. A hybrid protection.
But because we don’t have a method for testing the density of a viral load in the body, not just the swab test, but checking the blood itself for traces of covid presence, we never really know who has been infected, and who might be primed for a worse infection. Covid raw/original on its own is hard on the immune system, it has to work to clean up these compromised cells. So it is a plausible theory to say, covid original does make potential hosts more susceptible to a future infection. Only because the body has not been given the chance to recover from a prior infection.
And let me state once more. I’m not a doctor nor an immunologist – all of my information comes from the National Library of Medicine, along with other board-certified sources which document findings of the covid and its variants. I’ve casually studied medicine and biology my entire life, because I live in American and you have to stay healthy or you risk dying. Or worse. Legitimate resources are out there, Mayo Clinic is a good starting point.
So much of the covid and its variants I speculate ENDLESSLY ON. Because I am very impatient, and also my past assessments have had frightening accuracy and I don’t like that. I listen carefully to Dr. Fauci, hematologists, Dr. Campbell, pulmonary specialists – and use historical reference, along with medical findings of tame and preexisting viruses to base my analysis. And of course, a lot of what I rehash or backtrack over, these specialists are fully aware of. They stare this infection right in the face, and are treating the people that refuse the vaccine, and look at their blood and their lung tissue. But it takes time for science to peer review what it is seeing and verify which trends are consistent or reappearing.
And likely their have been other variants of the covid out there, but they were either too fatal to spread into the population or not warranted concern because they were near identical to the covid original, and were no more detrimental to those that contracted it.
Tl;dr – get vaccinated if you can do so, if you have no medical complexities to prevent you. We want you to be safe, we want you to be healthy.
#anonask#anon#covid#delta#vaccine#doctors#medical professionals#Doctor Anthony Fauci#Dr. Campbell#i try to be transparent and my post is a mess#i wish I had all the answers today but alas it takes time and care and tending to find the true answers#I have a focus on people who likely contracted covid but never 'tested' positive or presented symptoms#however not many have suffered too drastically aside from the couple who had a youtube channel and one partner did pass on#but thats why i decided to post this because delta is fucking mess and if its making people sick then some people will be getting sicker
2 notes
·
View notes
Text
an essay i wrote for class that im posting to link to it later
Ingrown: Compulsory Feminine Hairlessness, Perpetuation of the Gender Binary, and Patriarchal Control of the Feminine-Coded Body
This essay discusses gendered perceptions of body hair, the feminine hairlessness norm as perpetuating the gender binary, and the expectation of feminine hairlessness as a form of patriarchal control over feminine-coded people. ‘Feminine-coded’ is the term I am using to describe people which are normatively placed in the category of ‘woman’, which has no singular definition (Bettcher, 403).
The topic of feminine body hair is often shunned, classified as too trivial to discuss, yet, the pervasiveness of ‘mundane’ feminine hair removal suggests cultural significance. Socially mandated maintenance rituals that concern the feminine-coded body can be inspected as a microcosm reflecting a larger patriarchal system; patriarchy being the sociopolitical system that privileges masculinity over femininity. While I acknowledge there are many forms of appearance modification normatively expected of feminine-coded bodies, (such as dieting, makeup, hair styling, nail care, and skincare (Bartky, 99) and varying degrees of expectations defined by specific cultural norms and individual history, I wish to focus on feminine-coded body hair removal norms of the West (which I refer to as “the hairlessness norm” (Toerien and Wilkinson, 333)) and their implications.
Carol Hanisch’s 1969 memo, now referred to as “The Personal is Political” illuminated how problems that afflict women are commonly disregarded as “personal issues”, ignoring the fact that feminine-coded people experience patriarchal violence because of the system they are located in (Hanisch, 1969). From personal experience, the way my facial and body hair has been policed (by peers, employers, teachers, family, romantic partners, and strangers) has led me to develop trichotillomania (or “trich”, an obsessive hair pulling disorder). Exploring trich has led me to discover that the shame, guilt, and disgust I feel at my own body (hair) is socially produced through patriarchal systems. I can’t be the only one, and through this essay I wish to explore how the cultural production of feminine hairlessness enforces forms of violence and control to feminine-coded bodies. I wish to echo Hanisch’s sentiment that personal problems are political problems (Hanisch, 1969), the norm of feminine hairlessness is one of the many “mundane” ways patriarchal economic and social system exert control over feminine bodies and seek to define them as “unacceptable if unaltered” (Toerien and Wilkinson, 333).
I would like to define a few terms for this paper, ‘body hair’ will refer to facial and body hair that is normatively deemed inappropriate on feminine-coded bodies, including ‘ungroomed’ brows and unibrows, moustaches, beard/chin/cheek hair, breast, belly, and back hair, ‘ungroomed’ pubic hair, leg, toe, foot, hand, knuckle and other (non-scalp or eyelash) hair.
The ‘gender binary’ is a system in Western culture wherein individuals are expected to participate in socially produced gendered behaviour, where gender is classified as two distinct, opposite forms of masculinity and femininity. Upon birth (sometimes before), individuals are classified as either boys or girls according to their external genitalia (Bettcher, 393). During childhood, individuals learn through socialization and education what it means to “do” (perform) gender as a boy or a girl (Bettcher, 393). The gender binary system fits into Foucault’s notion of “discipline” and exists within a patriarchal power relationship, as feminine-coded bodies are expected to be altered in ways masculine-coded bodies are not. “Discipline” describes the way types of power are exercised: they are systems enforced to define and order populations, increasing the docility and utility of individuals to control them (Foucault, 136-137). Control of individuals is achieved partially through normative definitions of the body (highly subjective, but defined as “objective” by medical, governmental, popular, or social forces of their time) and what is appropriate for the body (Foucault, 140-141). Performing gender is expected in mainstream Western society, but the effort and cost for producing an ‘appropriate body’ for feminine-coded people is socially policed and informed by patriarchal institutions. For feminine-coded people, smooth, hairless, (preferably white and young) skin is expected, (especially on the face), and (in mainstream contexts,) those who ‘fail’ to meet this norm are often mocked, shamed and policed into conformity. For trans women, and feminine-coded people with darkly pigmented hair, the expectations of hairlessness are often enforced more violently and aggressively.
Hair growth patterns on different individuals vary substantially depending on factors such as age, genes and ‘race’, and the balance of testosterone and estrogen, both of which are present in most human bodies and are hormonal factors in hair growth (Toerien and Wilkinson, 335). Despite this, there is a widespread assumption that ‘men’ are ‘naturally’ hairier than ‘women’ (Toerien and Wilkinson, 335). This perspective is simplistic, binary, and discounts many relevant factors to hair growth distribution patterns. Feminine-coded people have an “equivalent potential for hair growth to men...women have hair follicles for moustache, beard, and body hair” (335 Toerien and Wilkinson), yet, popular assumptions expect the feminine body to be depilated to be viewed as “appropriately feminine”. The myth of ‘men’ as ‘naturally hairier’ is perpetuated by cultural assumptions of binary gender norms, how femininity is presented (in media and culture), and by medical definitions of what ‘counts’ as ‘normally’ or ‘abnormally’ hairy. Several scales to ‘rate’ hair growth have been proposed, but there exists no firm biological boundary to establish between the “normally” and “abnormally” hairy woman (Toerien and Wilkinson, 336). Frustratingly, within mainstream Western culture, virtually any hair on the feminine body outside the lashes, brows and scalp is considered ‘excess’, and the psychological and social consequences for feminine-coded people with ‘excess’ body hair can be profound, including depression, anxiety, stress, shame, and isolation. A study by Kitzinger & Willmott (2002) found that female-identifying participants with excessive body hair characterized their hair negatively, describing it as “‘upsetting’, ‘distressing’, ‘embarrassing’, ‘unsightly’, ‘dirty’ and ‘distasteful’” (para. 2).
Invoking a feminist curioisty (Enloe), one must ask, that if all genders may grow body hair (excluding individuals with autoimmune disorders such as alopecia), why is it that feminine hairiness is considered abnormal? The cultural context is significant. Feminine hairiness has historically been associated with negative assumptions about innapropriate conduct: masculine attitudes/aggression, deviant, repressed or queer sexuality, uncleanliness, mental illness, and witchcraft (Toerien and Wilkinson, 338). Masculine hairiness has been historically associated with virility, strength, and maturity (Toerien and Wilkinson, 337). The removal of feminine body hair is not a new or purely Western phenomena, (Toerien and Wilkinson, 333), but the current Western norm for large surfaces of hair to be removed is relatively recent, the act of removing hair from underarms and legs was “not widely practiced by most U.S. women until 1915”, when the first “womens razor” was marketed by Gillette (the “Milady Decolletée”), and as restrictions on feminine-coded bodies as needing to be completely covered were diminishing. (Toerien and Wilkinson, 333). Still, however, during the 1800’s in the West, any visible hair on feminine-coded faces was pathologized and defined as needing treatment (Toerien and Wilkinson, 333). Feminine hairlessness can be perceived as a binary-enforcing social demarcation tool to differentiate between ‘women’ and ‘men’ (Toerien and Wilkinson, 335).
Feminine hairlessness has been theorized to to suggest a child-like status afforded to feminine-coded people, unlike the adult status afforded to masculine-coded people. This relates to historical and cultural patriarchal patterns of viewing the “feminine” as lacking, incomplete, and passive (Toerien and Wilkinson 338). The term “baby smooth” often applied to freshly depilated feminine skin could be evidence of the childlike/feminine association.
For many people, body hair begins developing during puberty. During this time, individuals are often exposed to new expectations as to how to appropriately performing gender. For many feminine-coded individuals, this involves pressure from peers, parents, partners, teachers, and media, to remove hair from the face, legs, underarms, stomach, and/or pubic area. In many cases, pubescent feminine-coded people will be reliant on a caregiver for permission to depilate the body, adding a sense of lack of control or shame for many who do not have the resources or permission to depilate their bodies.
Feminine body hair is conceived of as unsanitary and often treated with the same disgust of other body products (like blood, odor and sweat) in a way that male-coded body hair is not (Toerien and Wilkinson, 338). This is perpetuated by standards of what is considered ‘good grooming’ for feminine-coded people (Toerien and Wilkinson, 338), where body hair is associated with dirtiness, and a lack of body hair with ‘cleanliness’. The association of feminine body hair with ‘dirtiness’ is tied up with racism, where more visible, pigmented hair is conceptualized as ‘dirtier’ than blond hair (Toerien and Wilkinson, 339). The “dirtiness” of feminine body hair is linked to its socially produced shamefulness, where unwanted hair is both embarrasing to develop and to remove; most cis women in hetrosexual relationships are expected to hide their depilitory “tools of transformation” (Bartky, 104) from men, to maintain the illusion of natural hairlessness. Feminine coded people who spend money to professionally remove body hair are often ridiculed for their “self indulgence” and “vanity”; this perception fails to critically examine the context within which choices to grow or remove body hair are made (Gill, 75). Adherence to “prevailing standards of bodily acceptability is a known factor in economic mobility” (Toerien and Wilkinson, 338), yet resources are required to maintain the ‘norms of bodily acceptability’, which for poor feminine-coded people, (and anyone who does not wish to depilate constantly), may be inaccessible, contributing to their exclusion from mainstream social, and professional environments.
The media plays a significant role in constructing and defining what ‘counts’ as appropriate femininity. Feminine-coded people who have hairy bodies or faces are generally absent in popular media, or used for comedic, insulting, or tokenizing purposes. The vast majority of commercials and advertisements for depilation products don’t show body hair (the first one to show body hair in 100 years came out in 2018); already-hairless legs are lathered and ‘shaved’ in commercials: perpetuating the myth that hair is unnatural, unsanitary and too taboo to even witness. The advertisement industry exploits feelings of inadequacy, shame, embarrassment, and a desire to fit in and appear ‘sexy’, ‘feminine’, and ‘confident’ in order to sell shaving creams, balms, after shaves, hair bleaches, hot and cold wax, depilatory creams, tweezers, buffing tools, electrolysis and laser treatments. The necessity for feminine bodies to absorb a ‘specialized knowledge’ in order to appropriately construct their hairless bodies is time and resource consuming (Bartkey, 99). Feminine coded people are expected to learn how to prevent and treat ingrown hairs, razor burn, how to not cut oneself shaving, burn oneself waxing, or otherwise injure oneself in an attempt to depilate. They must learn how and how often to depilate, and the proper exfoliation and after care treatments to ensure smooth and ‘properly’ hairless skin. The feminine body is transformed into a “docile body”, a body which is highly modified, policed, disciplined, and practiced, it is constantly surveilled in a panoptical sense of constant self surveillance (Bartky, 95). Everyone it seems, yet no one in particular, is enforcing the hairlessness norm; there are no public sanctions against body hair, but propagandistic norms that defines feminine hairlessness as ‘the way things are’ contribute to an invasion of the feminine-coded body by patriarchal ideologies (Bartky, 107).
The normative expectation for feminine-coded bodies to be hairless, and the disciplining by media and social systems which reward feminine-coded people who adhere to normative beauty standards, punish or mock those who don’t, and frame hairlessness as a natural, easily achievable, enjoyable, and fundamentally feminine, function to produce a disciplined, feminized, subject who devotes capital and time to a patriarchal system. The mainstream norm for feminine hairlessness is beneficial to corporate interests of keeping feminine-coded people ashamed of their bodies, burdened with expectations to alter their body, and incentives to purchase products to maintain a constant facade of natural hairlessness. It serves patriarchal interests of upholding a gender binary and maintaining norms of the feminine as passive, decorative, ‘not fully adult’, and in constant need of modification (Toerien and Wilkinson, 339).
Bibliography:
Bartky, Sandra Lee. “Foucault, Femininity and the Modernization of Patriarchal Power’ -
Chapter 5” Feminism & Foucault: Reflections on Resistance, edited by Irene Diamond and Lee Quinby, Northeastern University Press, 1988.
Bettcher, Talia Mae. “Trapped in the Wrong Theory: Re-Thinking Trans Oppression and
Resistance.” Signs, vol. 39, no. 2, 2014, pp. 383–406
Enloe, Cynthia. The Curious Feminist. University of California Press, 2004. Open WorldCat,
http://public.eblib.com/choice/publicfullrecord.aspx?p=223994.
Foucault, Michel. “The Subject and Power.” Critical Inquiry, vol. 8, no. 4, 1982, pp. 777–95.
JSTOR.
Gill, Rosalind C. “Critical Respect: The Difficulties and Dilemmas of Agency and ‘Choice’ for
Feminism: A Reply to Duits and van Zoonen.” European Journal of Women’s Studies, vol. 14, no. 1, Feb. 2007, pp. 69–80. DOI.org (Crossref), doi:10.1177/1350506807072318.
Hanisch, Carol. “The Personal Is Political: The Original Feminist Theory Paper at the Author’s
Web Site.” Carol Hanisch, 2009, http://www.carolhanisch.org/CHwritings/PIP.html.
Kitzinger, Celia, and Jo Willmott. “‘The Thief of Womanhood’: Women's Experience of
Polycystic Ovarian Syndrome.” Social Science & Medicine, vol. 54, no. 3, 2002, pp. 349–61.
Toerien, Merran, and Sue Wilkinson. “Gender and Body Hair: Constructing the Feminine
61 notes
·
View notes
Text
For Christmas, my aunt gifted me a DNA kit. I’ve always thought they were a bad idea (Where is all that info being stored? What unethical things can a company owning the rights to so much DNA possibly do? Why do white people need to know so badly how white they are, to the point that we created the ultimate Buzzfeed survey to confirm our whiteness? (If you didn’t know, Ancestry/23andMe and the like aren’t especially helpful for non-white folks, due to lack of testing in largely non-white groups. There’s a whole lot more to study on that and I highly suggest you take the time to read up on it)). That being said, most of the adults in my family have done the tests, mainly to appease my aunt, who is essentially our family historian and takes her role very seriously. I had considered the idea of doing one over the years. I never met my biological father. My mother separated from him before she realized she was pregnant with me, and although he was aware that she was pregnant and I had been born, there was no communication there and she met and married my stepfather shortly after I was born. He was my dad growing up, until I turned 18 and we became estranged, after I realized how incredibly toxic he was as a person and he basically disowned me when he discovered I wasn’t interested in following his rules and very racist, sexist, homophobic, xenophobic, and highly uneducated ideas. It caused a lot of issues within our family, but for the most part things have been relatively calm in the 10+ years since.
Fast forward to Christmastime. I had expressed interest in finding out if I had any other siblings, as well as my medical history, to my mother and my aunt. I wasn’t particularly interested in knowing anything about my biological father. Over the years, my mom has mentioned that he wasn’t a particularly good person when they were together, and the last information she’d heard of him was that he’d been arrested for arson at some point in the late 90s. I’ve never really given him much thought, and, as a child, whenever anyone realized that my stepfather wasn’t my actual biological dad, I was extremely vocal in pointing out that I only considered my unknown biological father as the “Sperm Donor”. But the idea of possibly having other siblings, and wanting to have a more complete medical history was compelling enough to me that I sold away my spit and rights to a company.
Come March, I got the results back and sent my aunt a text so she could connect me to our family tree in the app. She immediately went into super detective mode, and within a day found my biological father and several other family members. She confirmed that I didn’t have any other siblings, besides the two I already have, and that I had a living grandmother, several aunts, and a few cousins. She sent me photos, articles, and social media links, and I expressed to her that it was very overwhelming and while I appreciated it, I needed time to process it all. I tentatively went to my biological father’s Facebook page that he shared with his wife, and was extremely underwhelmed by what I saw. This man, a stranger to me, could’ve rivaled the dad who raised me in his ass-backwardness. He might possibly be the only MAGAmaniac in all of Vermont (obviously not, but you know what I mean), and as I already wasn’t interested in knowing him pre-test, this basically confirmed to me that he wasn’t someone I wanted to know. When you’re already a card-carrying member of the Shitty Dads Club™️, do you really need another one?
And that was that. I basically wrote that part of my life out of my mind, as it didn’t have anything to do with me or my day-to-day. The knowledge of having a living grandmother wasn’t appealing to me, as my Momaw (stepfather’s mom) passed four years ago, and was the most amazing grandma and best friend I could have possibly asked for. I feel lucky that I was able to have something SO good come from that connection, along with my two siblings. I don’t need another grandparent because I hit the fucking jackpot of unconditional love and support and guidance with Momaw. I didn’t feel like I was missing out by not knowing anyone else from my paternal biological family, either, as my mom is the youngest of 10 and my family is already massive as is. So it all came as a bit of a surprise when my aunt messaged me out of the blue in early July to inform me that she had taken it upon herself to reach out to my biological father and not only inform him of my existence (which he already knew about), but also sent him photos of me, along with my phone number. Something I neither wanted nor gave her permission to do. Something I hadn’t even expressed interest in. And after telling her yet again that it was overwhelming, she continued to allow this line of communication to stay open, and brought my mother into the mix.
According to my biological father, he apparently believed both my mom and I were dead. He says my maternal grandmother told him that the two of us had died, and he sunk into a deep depression over it, which has followed him for the past 29 years. Never mind the fact that he was in contact with a couple aunts and uncles over the years and so obviously knew that my grandmother had lied to him (if she ever even did so. We can’t know, as she passed when I was 3), or the availability of the fucking internet and basic Google search. In his own words, my aunt reaching out to him and “informing” him of the existence of his nearly-30 year old daughter “blew his whole world open”. Insert infinity eye roll emojis here.
As you could already tell, I was both upset that my aunt broke my trust in such a huge way, and thoroughly unimpressed by what she was sharing from him. I spoke with my mom about it several times, expressing how much my aunt had hurt me and frustrated me with her actions, and her choosing to take matters into her own hands and speaking for me. That might be the biggest annoyance for me of all, that she for some reason felt compelled to speak on my behalf for something I had no interest in or desire to explore, and took the option of some anonymity from me. My voice is my most important belonging, and having someone deign to speak for me infuriates me. And although my mother listened to me expressing how upset the whole thing made me, I found out a week later that she herself had been in contact with my biological father.
That was a kick to the ribs. She and I had spent years working on and building a relationship of trust and support, after a childhood and early adulthood of never being able to trust her. She was largely absent through a huge portion of my life when I needed her most, and it has taken years for me to build up my trust and faith in her. If you had told me ten years ago that my mother would become my best friend and confidant, I would have laughed my throat raw. But life is funny, and she did. And then she broke that trust in such a painful way, even after hearing how much my aunt’s choice to reach out to my biological father caused a massive rift between us. And Mom chose to create her own. For the first time in years, I didn’t want to speak to or see her or hear from her. I made that clear to her, and kept my distance until I could calm myself enough to speak to her without saying something that could irreparably damage our relationship. I reiterated that I had no interest in knowing my biological father, that I didn’t want to hear from him, and that it was a huge betrayal by her to continue speaking to him and fostering any sense of hope in him that I wished to have anything to do with him. Although things have been tense the last couple weeks, she and I have slowly been working through it.
And then tonight, as I arrived at work, a text from an unknown number popped up. A long text, from my biological father, who chose to ignore what my aunt and mother were supposed to have told him, that I didn’t want to have any contact. He introduced himself and reiterated his story about my maternal grandmother lying to him about Mom and I dying, said he wanted to get to know me and show me all the love he has for me, and that from what he’s heard I’m a lot like him. Things that I have no interest in hearing, don’t take to heart, and don’t feel particularly moved or motivated by. And I’m just. Exhausted.
Exhausted.
I don’t want this connection or half-assed truths or unbearable weight of expectations that have come to land so heavily on my shoulders.
When you sign in to take your DNA test, there is a disclaimer that you might find out information that could be upsetting and lead to more questions than answers. That continuing with the test could cause problems in your family and person life.
They weren’t kidding.
#personal#ramblings#dna test#23andme#ancestrydna#writing#writeblr#writters on tumblr#writtingcommunity
7 notes
·
View notes
Photo


Prodigy (Legend #2) - Marie Lu
my rating: 4/5 stars
Synopsis of book 1 -
In a world where the Patriots, Colonies, and the Republic are at odds and there’s a plague in the poorer parts of the US, Day is an unstoppable street criminal with good intentions. When his family’s house gets marked by Republic soldiers, Day’s only thought is to steal a cure before his family member dies. June is a top student at Drake University—a prodigy. When her brother, Metias, gets caught in a cross-fire during a mission, June is fast-tracked to becoming a soldier. Her first mission: track down Day. As Day and June come from such opposite backgrounds, is it possible that their paths would’ve crossed otherwise?
Link to Goodreads // Link to review book 1 // Spoilers (book 1+book2) in review below!
I haven’t read a trilogy in what feels like a really long time lmao; I think it’s because I’ve noticed that sometimes, the second book acts like a bridge book aka nothing really happens except for the last 50ish pages, which tbh just sets up book 3 (It’s like that one useless episode in a tv show that literally has nothing to do with the plotline). I’m VERY happy this wasn’t the case for Prodigy - if anything, there was even more action and more character (and world building) than Legend, which I much appreciated. That means that I also have a lot to unpack; buckle up!
I feel like the most natural place to start is from the stuff I didn’t really enjoy from the first book, specifically the world building and all the questions. It was finally explained that the Republic is essentially nonsense propaganda and the civilians are being fed false information--they aren’t winning the war, in fact they are losing! We also learned that the Colonies and the Patriots are two separate uh ‘groups’? And the Colonies fund the Patriots, but the Colonies are straight up left in the dark (and the Patriots were also hired by the Republic, but more on that later). I wanted to also briefly mention that when June and Day crossed into the Colonies territory, it was like a completely different world--maybe not better, just different. We also kind of get a glimpse into the history of the world--how climate change just absolutely obliterated the whole world. Which, tbh, I feel like if an ice cap near Antarctica (or Antarctica itself) were to melt, it would be more than just the edges of the US that would be underwater--it would go up to the Statue of Liberty’s torch :)))))))). Nevertheless, I really appreciated these explanations as it added more depth and also provided context for the setting, which I found was lacking in the first book (which, I get, you don’t want to overwhelm readers, esp in YA, with all the world building right away).
The other thing is that I wanted to know more about the plague, and Lu came through!!! So the plague is being used to try to create people as bioweapons, which makes me wonder if they were trying to clone those who were infected (or maybe just wanted to collect everyone who has a similar profile to Eden). I still have a few questions of the virus--like why did Eden and that other boy on the train go blind? Does the virus affect them on a genomic level?! I also find it hilarious that in LA they were quarantined for rioting--I feel like that pretty much just showed how weak the Republic is and how their power is no longer ominous (idk if that makes sense??).
Next, I want to touch on the characters and the character building (specifically June and Day, but others too!). I wanted to start off by prefacing that I’m not a fan of the love triangle vibes that we got throughout the books (and to be honest, the ending sort of pushed that narrative a bit further, which is not cool :///). So I’m not sure if it was Razor’s plan to cut communication between Day and June (on purpose) to prevent them from messing up the Patriot’s plans/to prevent Anden from becoming suspicious of June, but I found it so FRUSTRATING that they couldn’t communicate at least once before the assination (and I mean talk, not the signal bc that stirred up a lot of confusion with Day). Their separation really tested their relationship, but I also feel like there was a permanent wedge placed due to the lack of trust, and again, the ending just hammered that home. I will say, I really appreciate June and Day being completely transparent with each other when they escaped from the Patriots and got in the cave. It was like a necessary evil, but at least they shared relevant information with each other, which I believe strengthened their partnership, even if it took a toll on their relationship. Part of me hopes that they end up back together in Champion, but I know that it may not be ‘what’s best for them’, especially with that huge piece of information we learned about Day--that’s the one thing I’m mad about. They spill the beans in the cave but he can’t even tell June that he’s dying, instead he breaks up with her and then they end up kissing?? AH!

Now for those…...love triangles…. .-. Let’s start off with Anden and June. I’m not sure how I feel about Anden; Lu paints him to be this kind of heartthrob and well-intentioned guy but he’s also sort of naive? Like I get that his whole plan is to reform the Republic with the help of June and Day so that the civilians are on board, but I hope he realizes that there will always be people who are going to 1) resist him and 2) betray him. I really hope he isn’t as quick to trust people as he was with June (which maybe that was because his judgement was clouded). As for being naive...how did he not see June’s paperclip ring???? And to add onto that - how did the Colonies not realize that ‘Sarah’ is actually June???
I don’t know it just seems very unlikely that he didn’t see it considering that June was fiddling with it during their nice little dinner. And also the fact that he was always itching to see her. I didn’t realize, however, that Anden is only in his early twenties—he also lacks the edge that June and Day have, you can tell that he’s a poised person. While it’s great that he stands his ground on the Republic, I find it hard to believe that he isn’t a pushover (even just a tiny bit). Thus, I don’t really see how Anden and June could be a good match; I also don’t think class should play a role into whether or not you should or shouldn’t be with someone.
That sort of brings me to another point, which is the idea of the Priceps and the Elector itself. I have so many questions about Anden's plans, and they mainly involve him. For example, would there still be an Elector (and Senate) after the Republic is reformed? If so, would his powers be minimized, or would he have the status of President? For Priceps, it wasn’t very clear in the book that she doesn’t have to be married to the Elector, but it almost seemed that it was implied; could Anden have chosen to be married and have a separate Priceps? What if the Elector wasn’t straight? So. Many. Questions!! That whole Priceps thing is one of the reasons I couldn’t give this book a full 5 stars, again, it sort of has to do with the lack of information (or the amount of assumptions I have to make).
The next love triangle I have major issues with is Tess and Day, which Day is mostly uh turned off by the whole thing (which I can get behind) but Tess is just so stubborn and tbh pretty jealous, which isn’t cute. I really hope that in Champion they end up reconnecting, especially since Day is practically on his deathbed, but as friends. Maybe Tess will understand where Day is coming from with his feelings about June. Part of me wants Tess to end up with Baxter but I also really don’t like him?????? Agh this really sucks! I wish their relationship didn’t end on such a sour note. Like yes Tess, you were always there for Day (especially when he needed medical care) and ever since they got into contact with June (or rather, when June was sent on her mission), everything went downhill—but I mean, at some point Anden’s father would’ve passed, and maybe things would turn out to be in a similar circumstance, except instead of June it could be a different girl? The fact that Day still calls Tess ‘cousin’ and she still went ahead and kissed him just made me feel slightly uncomfortable?? No, they’re not biologically related, but given the amount of time they spent together, they almost could’ve been. To some extent, I feel like Tess had a huge crush on Day, but she never wanted to admit it until they were separated bc she maybe didn’t realize how much he means to her/she wanted that cheesy movie-like feeling where the two best friends realize that they are perfect together but beyond friends?? I do believe that Tess deserves someone great though, I just don’t think that Day is the guy for that :///
The last relationship-thing I want to briefly mention is Thomas and Metias’ relationship. I’m glad that we have some LGBT+ representation here, but at the same time, I can’t help but wonder if it was forced or not (like a checkbox Lu wanted to tick). I don’t remember in Legend when Thomas kissed June, if there was a kind of repulsion/it didn’t feel authentic. To be honest, I really thought that Thomas was into June, but when we learn he is gay (or maybe bi), it just didn’t seem to fit the story at all??? Upon this revelation, June racked her brain for memories of Thomas and Metias when they were young and oh it just happens that Metias never ‘brought back’ anyone/any girls home. Listen, I’m all for diversity, whether that be the character’s race, gender identity and/or sexual preference, I just don’t want it to come off as the author just ‘checking off a box’; I’d rather it be genuine (even though it’s a fictional story!) For all I know, Lu may have planned this, but to me it just came off as an afterthought, that’s all :/ (and @ Thomas, just because you love someone and it shouldn’t be allowed bc of your ranks, it doesn’t mean you have to kill them even if CoMmAnDeR JaMeSoN said to).
I wanted to also talk about characters—more specifically Razor, Commander Jameson, Baxter, and Kaede (rip). So um I guess we’ll start with Razor aka the biggest con man there ever was. Well tbh I kind of found him fishy, just like June did from the get-go, I just didn’t think it was going to be that…bad??? This goes back to Lu’s foreshadowing—which I would say it improved as I wasn’t able to fully guess what was going to happen—she drops p obvious hints left, right, and centre, you just don’t see them until the events unfold; what may seem like a small detail (i.e. Commander Jameson in Razor’s room on the ship and Day (as a disguise) bumping into her) will end up being part of a bigger plan, so to speak. Part of me wishes we had a peek into his mind to see what he thinks like, and if he has more motives, besides just being “hired” by the Senate to assassinate Anden, maybe Razor has a personal vendetta?? I also definitely suspect that Razor and Commander Jameson may or may not be a thing *side eyes*. I’m excited to read Champion to see how he will stand up against the Elector / the Republic, and whether the other Patriots will stand by his side or if they will turn against Razor--especially because right now he’s in jail, but I doubt he will stay there for long! (which can someone explain why Razor and Commander Jameson only got charged with treason??? They almost flipped the Republic on its head).
Speaking of Patriots...there’s Baxter, which I don’t know where he stands. I think he’s definitely jealous of Day / the fact that Tess has feelings for Day even though he doesn’t reciprocate them. Just a dash of jealousy. But he did predict that Day would betray the Patriots, which makes me think that Baxter may have a part in an uprising, but maybe there’s a chance that he’ll see the whole story. Part of me also highly doubts that he’ll be rational; he seems to be someone with a heavy confirmation bias--I wonder if he knew that Razor was hired by the Senate or if it just went over his head. What if he’s the main villain in Champion o.O him + Tess would be interesting, especially Day does a last hurrah. But anyways, Baxter was just so arrogant, and I could feel Day’s own disappointment when he did exactly what Baxter had predicted. Yeap, there’s definitely going to be some tension that needs to be revisited.
Last and certainly not least, Kaede :( I’m a bit annoyed that she’s dead. It’s yet again another thing that could be used against Day (specifically his relationship with June; anything that comes near them dies). We got to learn so much from Kaede, and before we knew it, she got shot. It sucks because I think she seemed like a reasonable person and she always remained level-headed. She’s not one to judge quickly *cough cough Baxter cough cough*. Even in Legend she had her kick-ass moments, but she really saved them from the Colonies and how June and Day can’t really repay her unless they keep on going with their mission. Not cool to just kill her off like that though.
What I loved from this book, besides the character growth and the depth of their relationships with each other (especially on trust, or the therelackof), I liked how this book is just action-packed. I find with the second book in trilogies, we have a plan with a clear end goal (in this case, assassinate the Elector), and that plan just gets adjusted over time as we uncover information until it gets to the end of the book. Here, that main event ended up being smack bang in the middle, which isn’t something we see very often. It left more room for the story to develop and to allow us to really dig deep into the story, which I much appreciated. At some parts, it almost felt like a rush, especially as the story unfolds and with so many characters to consider--it was a page turner! I’m not really sure if I enjoyed Prodigy more than book 1, as I mentioned, I didn’t really like the love triangles and then Anden is just too naive for me to take him seriously. There were also some cliches (I let go of the breath I didn’t know I was holding), and honestly, I was not a fan of the ending! I think that’s the main reason why I can’t rate this higher than Legend to be honest. At least with the first book, there was enough closure that could give us a starting point for book 2. Here is was...let’s break up lmao jk also I’m not going to let June know that I’m dying, peace out.
This review is getting a bit too long lol, and I’m sure there’s something I forgot to mention, but overall I really enjoyed this book. The action, the intensity, the revelation of information and Lu’s foreshadowing make Prodigy a book that’s hard to put down. The characters’ dynamics are all over the place, which just adds to the chaos, but in a good way--it makes the story that much more interesting. I’m patiently waiting for book 3 from overdrive, so I’m not sure if I’ll be able to read and review it by next week--I’m itching to know what happens next! [Please, let both of our main characters live p l e a s e]
I’d love to know your thoughts and opinions on Prodigy! Did you enjoy this book, how would you compare it with the rest of the trilogy? Let’s chat =D
Thank you for reading my review, I hope you are having a good day, wherever you are in the world!
~ Cassandra / an-avid-reader
2 notes
·
View notes
Text
Medicine (definition)
This article is about the science of healing. For medicaments, see
medication
. For other uses, see
Medicine (disambiguation)
."Academic medicine" redirects here. For the journal, see
Academic Medicine (journal)
."Clinical medicine" redirects here. For the journal, see
Clinical Medicine (journal)
.Medicine
Statue of
Asclepius
, the
Greek god
of medicine, holding the symbolic
Rod of Asclepius
with its coiled
serpent
Specialist
Medical specialty
Glossary
Glossary of medicine
Medicine is the science and practice of establishing the diagnosis, prognosis, treatment, and prevention of disease. Medicine encompasses a variety of health care practices evolved to maintain and restore health by the prevention and treatment of illness. Contemporary medicine applies biomedical sciences, biomedical research, genetics, and medical technology to diagnose, treat, and prevent injury and disease, typically through pharmaceuticals or surgery, but also through therapies as diverse as psychotherapy, external splints and traction, medical devices, biologics, and ionizing radiation, amongst others.[1]
Medicine has been around for thousands of years, during most of which it was an art (an area of skill and knowledge) frequently having connections to the religious and philosophical beliefs of local culture. For example, a medicine man would apply herbs and say prayers for healing, or an ancient philosopher and physician would apply bloodletting according to the theories of humorism. In recent centuries, since the advent of modern science, most medicine has become a combination of art and science (both basic and applied, under the umbrella of medical science). While stitching technique for sutures is an art learned through practice, the knowledge of what happens at the cellular and molecular level in the tissues being stitched arises through science.
Prescientific forms of medicine are now known as traditional medicine and folk medicine, though they do not fall within the modern definition of “medicine” which is based in medical science. Traditional medicine and folk medicine remain commonly used with, or instead of, scientific medicine and are thus called alternative medicine (meaning “[something] other than medicine”, from Latin alter, “other”). For example, evidence on the effectiveness of acupuncture is "variable and inconsistent" for any condition,[2] but is generally safe when done by an appropriately trained practitioner.[3] In contrast, alternative treatments outside the bounds not just of scientific medicine, but also outside the bounds of safety and efficacy are termed quackery.
Contents
1Etymology
2Clinical practice
3Institutions
4Branches
5Education and legal controls
6Medical ethics
7History
8Quality, efficiency, and access
9Traditional medicine
10See also
11References
3.1Delivery
4.1Basic sciences
4.2Specialties
4.3Interdisciplinary fields
7.1Ancient world
7.2Middle Ages
7.3Modern
Quackery can encompass an array of practices and practitioners, irrespective of whether they are prescientific (traditional medicine and folk medicine) or modern pseudo-scientific, including chiropractic which rejects modern scientific germ theory of disease (instead believing without evidence that human diseases are caused by invisible subluxation of the bones, predominantly of the spine and less so of other bones), with just over half of chiropractors also rejecting the science of immunization.
Etymology[edit]
Medicine (UK: /ˈmɛdsɪn/ (listen), US: /ˈmɛdɪsɪn/ (listen)) is the science and practice of the diagnosis, prognosis, treatment, and prevention of disease.[4][5] The word "medicine" is derived from Latin medicus, meaning "a physician".[6][7]
Clinical practice[edit]
The Doctor
by
Sir Luke Fildes
(1891)
Medical availability and clinical practice varies across the world due to regional differences in culture and technology. Modern scientific medicine is highly developed in the Western world, while in developing countries such as parts of Africa or Asia, the population may rely more heavily on traditional medicine with limited evidence and efficacy and no required formal training for practitioners.[8] In the developed world, evidence-based medicine is not universally used in clinical practice; for example, a 2007 survey of literature reviews found that about 49% of the interventions lacked sufficient evidence to support either benefit or harm.[9]
In modern clinical practice, physicians personally assess patients in order to diagnose, prognose, treat, and prevent disease using clinical judgment. The doctor-patient relationship typically begins an interaction with an examination of the patient's medical history and medical record, followed by a medical interview[10] and a physical examination. Basic diagnostic medical devices (e.g. stethoscope, tongue depressor) are typically used. After examination for signs and interviewing for symptoms, the doctor may order medical tests (e.g. blood tests), take a biopsy, or prescribe pharmaceutical drugs or other therapies. Differential diagnosis methods help to rule out conditions based on the information provided. During the encounter, properly informing the patient of all relevant facts is an important part of the relationship and the development of trust. The medical encounter is then documented in the medical record, which is a legal document in many jurisdictions.[11] Follow-ups may be shorter but follow the same general procedure, and specialists follow a similar process. The diagnosis and treatment may take only a few minutes or a few weeks depending upon the complexity of the issue.
The components of the medical interview[10] and encounter are:
Chief complaint (CC): the reason for the current medical visit. These are the 'symptoms.' They are in the patient's own words and are recorded along with the duration of each one. Also called 'chief concern' or 'presenting complaint'.
History of present illness (HPI): the chronological order of events of symptoms and further clarification of each symptom. Distinguishable from history of previous illness, often called past medical history (PMH). Medical history comprises HPI and PMH.
Current activity: occupation, hobbies, what the patient actually does.
Medications (Rx): what drugs the patient takes including prescribed, over-the-counter, and home remedies, as well as alternative and herbal medicines/herbal remedies. Allergies are also recorded.
Past medical history (PMH/PMHx): concurrent medical problems, past hospitalizations and operations, injuries, past infectious diseases or vaccinations, history of known allergies.
Social history (SH): birthplace, residences, marital history, social and economic status, habits (including diet, medications, tobacco, alcohol).
Family history (FH): listing of diseases in the family that may impact the patient. A family tree is sometimes used.
Review of systems (ROS) or systems inquiry: a set of additional questions to ask, which may be missed on HPI: a general enquiry (have you noticed any weight loss, change in sleep quality, fevers, lumps and bumps? etc.), followed by questions on the body's main organ systems (heart, lungs, digestive tract, urinary tract, etc.).
The physical examination is the examination of the patient for medical signs of disease, which are objective and observable, in contrast to symptoms which are volunteered by the patient and not necessarily objectively observable.[12] The healthcare provider uses the senses of sight, hearing, touch, and sometimes smell (e.g., in infection, uremia, diabetic ketoacidosis). Four actions are the basis of physical examination: inspection, palpation (feel), percussion (tap to determine resonance characteristics), and auscultation (listen), generally in that order although auscultation occurs prior to percussion and palpation for abdominal assessments.[13]
The clinical examination involves the study of:
Vital signs including height, weight, body temperature, blood pressure, pulse, respiration rate, and hemoglobin oxygen saturation
General appearance of the patient and specific indicators of disease (nutritional status, presence of jaundice, pallor or clubbing)
Skin
Head, eye, ear, nose, and throat (HEENT)
Cardiovascular (heart and blood vessels)
Respiratory (large airways and lungs)
Abdomen and rectum
Genitalia (and pregnancy if the patient is or could be pregnant)
Musculoskeletal (including spine and extremities)
Neurological (consciousness, awareness, brain, vision, cranial nerves, spinal cord and peripheral nerves)
Psychiatric (orientation, mental state, mood, evidence of abnormal perception or thought).
It is to likely focus on areas of interest highlighted in the medical history and may not include everything listed above.
The treatment plan may include ordering additional medical laboratory tests and medical imaging studies, starting therapy, referral to a specialist, or watchful observation. Follow-up may be advised. Depending upon the health insurance plan and the managed care system, various forms of "utilization review", such as prior authorization of tests, may place barriers on accessing expensive services.[14]
The medical decision-making (MDM) process involves analysis and synthesis of all the above data to come up with a list of possible diagnoses (the differential diagnoses), along with an idea of what needs to be done to obtain a definitive diagnosis that would explain the patient's problem.
On subsequent visits, the process may be repeated in an abbreviated manner to obtain any new history, symptoms, physical findings, and lab or imaging results or specialist consultations.
Institutions[edit]
The Hospital of
Santa Maria della Scala
, fresco by
Domenico di Bartolo
, 1441–1442
Contemporary medicine is in general conducted within health care systems. Legal, credentialing and financing frameworks are established by individual governments, augmented on occasion by international organizations, such as churches. The characteristics of any given health care system have significant impact on the way medical care is provided.
From ancient times, Christian emphasis on practical charity gave rise to the development of systematic nursing and hospitals and the Catholic Church today remains the largest non-government provider of medical services in the world.[15] Advanced industrial countries (with the exception of the United States)[16][17] and many developing countries provide medical services through a system of universal health care that aims to guarantee care for all through a single-payer health care system, or compulsory private or co-operative health insurance. This is intended to ensure that the entire population has access to medical care on the basis of need rather than ability to pay. Delivery may be via private medical practices or by state-owned hospitals and clinics, or by charities, most commonly by a combination of all three.
Most tribal societies provide no guarantee of healthcare for the population as a whole. In such societies, healthcare is available to those that can afford to pay for it or have self-insured it (either directly or as part of an employment contract) or who may be covered by care financed by the government or tribe directly.
Modern drug
ampoules
Transparency of information is another factor defining a delivery system. Access to information on conditions, treatments, quality, and pricing greatly affects the choice by patients/consumers and, therefore, the incentives of medical professionals. While the US healthcare system has come under fire for lack of openness,[18] new legislation may encourage greater openness. There is a perceived tension between the need for transparency on the one hand and such issues as patient confidentiality and the possible exploitation of information for commercial gain on the other.
Delivery[
edit
]See also:
Health care
,
clinic
,
hospital
, and
hospice
Provision of medical care is classified into primary, secondary, and tertiary care categories.
Nurses in
Kokopo
,
East New Britain
,
Papua New Guinea
Primary care medical services are provided by physicians, physician assistants, nurse practitioners, or other health professionals who have first contact with a patient seeking medical treatment or care. These occur in physician offices, clinics, nursing homes, schools, home visits, and other places close to patients. About 90% of medical visits can be treated by the primary care provider. These include treatment of acute and chronic illnesses, preventive care and health education for all ages and both sexes.
Secondary care medical services are provided by medical specialists in their offices or clinics or at local community hospitals for a patient referred by a primary care provider who first diagnosed or treated the patient. Referrals are made for those patients who required the expertise or procedures performed by specialists. These include both ambulatory care and inpatient services, Emergency departments, intensive care medicine, surgery services, physical therapy, labor and delivery, endoscopy units, diagnostic laboratory and medical imaging services, hospice centers, etc. Some primary care providers may also take care of hospitalized patients and deliver babies in a secondary care setting.
Tertiary care medical services are provided by specialist hospitals or regional centers equipped with diagnostic and treatment facilities not generally available at local hospitals. These include trauma centers, burn treatment centers, advanced neonatology unit services, organ transplants, high-risk pregnancy, radiation oncology, etc.
Modern medical care also depends on information – still delivered in many health care settings on paper records, but increasingly nowadays by electronic means.
In low-income countries, modern healthcare is often too expensive for the average person. International healthcare policy researchers have advocated that "user fees" be removed in these areas to ensure access, although even after removal, significant costs and barriers remain.[19]
Separation of prescribing and dispensing is a practice in medicine and pharmacy in which the physician who provides a medical prescription is independent from the pharmacist who provides the prescription drug. In the Western world there are centuries of tradition for separating pharmacists from physicians. In Asian countries, it is traditional for physicians to also provide drugs.[20]
1 note
·
View note
Text
Identify the causes, signs, and symptoms of hypertension

Hypertension is a common clinical condition characterized by elevated blood pressure levels. It is also known as hypertensive heart disease or high blood pressure. Have you ever wondered what the blood pressure (BP) exactly is?
Blood pressure is the pressure exerted on the lateral wells of the blood vessels, precisely arteries, while the blood flows through them. To better understand blood pressure measurements, you must know about systolic and diastolic pressure. Systolic blood pressure denotes the pressure exerted when the heart beats. On the other hand, diastolic pressure is the pressure exerted on the resting state of the heart between the beats. The normal blood pressure of a healthy adult is 120/80 mmHg. Depending on your activity, your blood pressure changes throughout the day. Therefore, the diagnosis of high blood pressure may be made if blood pressure readings are frequently higher than normal. According to the American heart association, systolic blood pressure of 130-139 or diastolic blood pressure of 80-89 is considered stage 1 hypertension. The condition can be managed effectively with early diagnosis, timely treatment, and lifestyle modification.
Causes of hypertension
The major causes of high blood pressure include increasing age, too high salt intake, family history, obesity, lack of exercise, stress, alcohol consumption, smoking, pregnancy, and chronic metabolic diseases. However, the exact pathophysiology of the developing condition is poorly understood.
High blood pressure symptoms
It is challenging to identify hypertension symptoms, especially in the early stages of the condition. However, in the more advanced stages, the patient complains of recurrent morning headaches, nausea, blurred vision, nose blood, shortness of breath, cardiac arrhythmia, ringing in the ears, exhaustion, chest pain, anxiety, and trembling muscles, along with elevated blood pressure.
Get high-quality hypertension biospecimens online.
Central BioHub is the leading global provider and most reliable online marketplace for human biospecimens. Targeting the research potential for therapeutic, diagnostic, and other biomedical areas, Central BioHub brings you the world's largest and most diverse inventory of clinical research samples. We offer thousands of well-defined, high-quality hypertensive disease samples ethically derived from patients suffering from hypertension.
The human serum and plasma samples from hypertension patients are tested for specific cardiac markers such as Troponin I (TnI), Troponin T (TnT), brain natriuretic peptide (BNP), N-terminal prohormone b-type natriuretic peptide (NT-proBNP), myoglobin, creatine kinase-MB (CK-MB), D-dimer, and cystatin C.
Improving the accuracy of drug and diagnostic research, our biospecimens are well-annotated with clinical information, including patient's demographic details and medical and medication histories. Hurry up, check out our latest inventory update and procure high-quality human biological specimens: https://centralbiohub.de/blogs/procure-samples-from-hypertension-patients-in-just-a-few-clicks
Central BioHub has a premier portfolio of millions of human biospecimens ideal for research, development, and quality control purposes: Contact us for more information on hypertension samples.
0 notes
Last Seen Blogs

blackklistt
En serio

jessfromouterspace
howdy

charud2555
ฟิสิกส์ราชมงคล
charud2555
ฟิสิกส์ราชมงคล

mastaqi
Mastaqi