#HCoV-OC43
Text
COVID-19 Infection Has More Than 50 Long-Term Effects
COVID-19 Infection Has More Than 50 Long-Term Effects
MADRID, Spain — Clinical experiences in approaching COVID-19 from different perspectives, results obtained by various therapeutic options and, above all, the challenges posed by a new healthcare reality — long COVID — were all the focus of a recent discussion at the 7th International Congress of the Spanish Society of Precision Health.
In this forum, titled Precision Health: A COVID-19…

View On WordPress
#2019 Novel Coronavirus#2019-nCoV#Coronavirus#dyspnea#exercise#HCoV-229E#HCoV-OC43#Human coronavirus 229E#Human coronavirus HKU1#Human coronavirus OC43#idiopathic pulmonary fibrosis#mon#physical activity#pneumonia#Post-acute sequelae of SARS-CoV-2 infection; post-acute sequelae of SARS-CoV-2 infection (PASC); PASC - post-acute sequelae of SARS-CoV-2 in#Wuhan coronavirus
0 notes
Text
Another miracle of green tea! Jinan University researchers find green tea has anti-coronavirus properties, including mutants
The production and consumption of tea has a history of more than 4,000 years. At present, more than 2 billion cups of tea are consumed every day in the world, which is second only to water in terms of global consumption. Previously published research has shown that regular consumption of green tea and coffee has health benefits because these beverages contain a variety of bioactive compounds. However, little is known about green tea's antiviral properties.
On March 17, 2021, a study by researchers at Jinan University on the bioRxiv preprint platform reports that green tea has antiviral activity, adding to its long-term health benefits. In the new study, epigallocatechin gallate (EGCG), one of the components of green tea, prevented severe SARS-CoV-2 from binding to the human angiotensin-converting enzyme 2 (ACE2) receptor, thereby preventing infection in humans lung cells, and inhibitory effects were also observed in SARS-CoV-2 variants.

The main active ingredients in green tea are catechins, including epigallocatechin gallate (EGCG), epigallocatechin (EGC), epigallocatechin gallate (ECG), and epigallocatechin (EC), of which EGCG is the most abundant catechin in green tea.
The researchers created several pseudoviruses containing complete mutations (B.1.1.7, B.1.351 and B.1.429) with single mutations (K417N, E484K, N501Y, D614G) or emerging variants. S protein, and pseudoviruses were then transfected into HEK293T-hACE2 cells.

Through experiments, the researchers found that green tea effectively prevented the infection of wild-type, D614G, B.1.429 and B.1.351 in a dose-dependent manner.
The researchers also found that when tested against HCoV OC43 in HCT-8 cells, green tea beverages were also observed to protect against infection by other coronaviruses.
Next, the researchers looked for the substances in green tea that cause these antiviral effects. The active components of green tea catechins EGCG, EGC, ECG and EC were studied.
The results showed that three catechins: EGCG, EGC and ECG dose-dependently blocked pseudovirus infection caused by the wild-type SARS-CoV-2 strain.

Upon closer inspection, the researchers concluded that EGCG was the most potent inhibitor of viral infection. EGCG accounts for more than 50% of the catechins in green tea beverages.
Then, after exposure of EGCG to mutants such as D614G, K417N, E484K and N501Y, its ability to cause infection was also inhibited.
The researchers also found that EGCG inhibited viral infection of cells containing interesting variants, including B.1.17, B.1.351 and B.1.429.

Testing EGCG on infected human lung epithelial cells, the researchers found that it inhibited SARS-CoV-2 before and after infection. However, the inhibitory activity was greater when cells were pretreated with EGCG prior to SARS-CoV-2 infection.
Further studies identified the mechanism of action of EGCG against SARS-CoV-2, and the researchers found that it blocked the entry of the virus by blocking the S1 subunit with the highest binding affinity with ACE2. EGCG also reduced the binding of the S2 subunit, although it had little binding affinity to ACE2.
In conclusion, studies suggest that consumption of green tea or its active ingredient EGCG may help prevent or reduce the spread and infection of SARS-CoV-2, given its low toxicity, anti-inflammatory, antioxidant and anti-SARS-CoV-2 variant properties, drinking Green tea may minimize the spread of SARS-CoV-2 and improve symptoms and disease severity.
Paper link:https://doi.org/10.1101/2021.03.17.435637
2 notes
·
View notes
Text
RBD and ACE2 Embedded Chitosan Nanoparticles as a Prevention Approach for SARS-COV 2

RBD and ACE2 Embedded Chitosan Nanoparticles as a
Prevention Approach for SARS-COV 2 in Biomedical Journal of Scientific & Technical Research
https://biomedres.us/fulltexts/BJSTR.MS.ID.005960.php
A new type of coronavirus-associated persistent pneumonia outbreak called SARS-CoV-2, which causes severe acute respiratory syndrome, was reported in Wuhan, China in Hubei Province in December 2019. In the following weeks, infections spread rapidly to China and other countries around the world [1]. Coronaviruses (CoVs) are known to cause enteric and respiratory diseases in animals and humans, which are positive stranded RNA viruses that are not segmented into large envelopes. Most human CoVs such as hCoV - 229E, OC43, NL63 and HKU1 cause mild respiratory diseases, but two previously unknown CoVs, severe acute respiratory syndrome CoV (SARS - CoV) and Middle East respiratory syndrome CoV (MERS - The worldwide spread of CoV) has drawn global attention to the deadly potential of human CoVs. Genomic analysis shows that SARS - CoV - 2 belongs to the same betacoronavirus family as MERS - CoV and SARS - CoV and shares a sequence that shows a high homology with SARS - CoV. A cellular receptor angiotensin-converting enzyme 2 (ACE2) is mainly mediated by the introduction of SARS - CoV into human host cells. It is expressed in the human respiratory epithelium, lung parenchyma, vascular endothelium, kidney cells and small intestine cells [2].
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01
Follow on Blogger : https://biomedres01.blogspot.com/
Like Our Pins On : https://www.pinterest.com/biomedres/
#medical and medicinal journal#journals on cancer medicine#Journals on Biomedical Intervention#journal of biomedical sciences research review#biomedical open access journals
0 notes
Text
THE UMPTEENTH WAVE | LA ÉNIÈME VAGUE | LA ENÉSIMA OLA
by Ernesto Prieto Gratacós
See bellow in 🇬🇧English, voir ci-dessous en 🇫🇷Français, y abajo el texto original en 🇪🇸Español

THE UMPTEENTH WAVE by Ernesto Prieto Gratacós
A fundamental action to be taken in the face of viral epidemics has been, is and will be, the strengthening of the Immune System through the molecules responsible for its germicidal power. As we have shown since the beginning of the health crisis, these substances are precisely the immunoessential nutrients: vitamin D, ascorbate (vitamin C), zinc and selenium. Having the necessary nutrients, the two phases of our formidable immune response – innate and acquired – have prevailed for millennia against viruses, bacteria and fungi.
Each winter season brings a "wave" of malnutrition of varying intensity, peaking every few years. This wave has always been and will continue to be, as long as food, behavioral and pharmacological measures are not taken to counteract it. This book was born from the intention of giving precise instructions on how to implement this strategy and a selection of almost 300 scientific articles that support it. It is not fear but rational action that will allow us to resume the normal productivity that our society needs. Those who insist on the alarmist discourse announcing daily a second wave and new mutant strains seem to ignore the bases of epidemiology and molecular biology or deliberately lie in the service of economic and political interests. The articles referenced above describe how "six classes of Human Coronaviruses (HCoV) have been previously identified, including HCoV-NL63 and HCoV-229E, belonging to the genus Alphacoronavirus, as well as HCoV-OC43, HCoVHKU1, SARS-CoV (Severe Acute Respiratory Syndrome) and MERS CoV (Middle East Respiratory Syndrome), belonging to the genus Betacoronavirus." The reason we quote such a description is to make it clear that coronaviruses have long been among us, and new variants are continually appearing.
Humanity already has almost 8 billion inhabitants, while the animals that are raised for the food industry are counted in tens of billions. For this reason, the mathematical probability of mutations in one or several genes, which give a virus characteristics necessary to infect humans, are increasingly high. Each of the almost fifty specialists with whom we have spoken admits – at least privately – that the Immune System is the key to success. At the same time, everyone agrees that, given the high prevalence and distribution of coronaviruses in animals close to us, their immense genetic diversity, the frequent recombination of their genomes and the increasing interaction between the human species and the rest of the Animal Kingdom, it is to be expected that new coronaviruses will periodically jump more and more frequently towards our species. Systematic population supplementation is the safest and most cost-effective measure possible to deal with the hundreds of diverse viruses that swarm among us.
Seasonal Flu Cycle and Its Link to Vitamins
The notion that viral respiratory infections flare up with autumn-winter and dissipate with spring-summer has long been established in the epidemiology of influenza and other seasonal flus and pneumonias. It's no secret that vitamin D levels decline rapidly with the disappearance of sunny days, while poor nutrition prevents them from compensating for their decline. The same happens with the levels of vitamin C in the blood plasma as winter worsens and the sources of fresh food, source of vitamin C, zinc and selenium decline. While vigorously opposed early in the pandemic by various academic, industry, and media societies — which really inclines you to think of a mix of misinformation and commercial interests — vitamin D has emerged triumphant in the scientific literature related to COVID-19. Indeed, as of the date of this publication, the database PubMed.gov recorded more than 450 scientific articles on the positive role of vitamin D levels in the incidence, severity and mortality from COVID-19.
Unfortunately, blood levels of 25-(OH)-D (vitamin D) present in urban populations are very low, often extremely deficient. The bulk of COVID-19 deaths occurred in people who, unfortunately, had catastrophically low levels of calcefidiol, the active form of the vitamin, even from the most orthodox perspective. Ignoring established scientific information, most medical professionals consider a chalcefidiol level around 20 ng/dL to be "healthy" for the simple reason that this number is within the normal distribution range of the population, which tends to be between 15 ng/mL and 30 ng/mL. But normal is not synonymous with good. From a nutrigenomic perspective, the optimal amount of vitamin D consistent with the evolutionary history of the human species is one that is reached by sunbathing or eating plenty of quality fatty foods. The seasonality of influenza and influenza epidemics has a causal link with vitamins D and C, but nutritional recommendations remain unjustifiably low, ignoring all epidemiological, biochemical, and anthropological evidence in favor of levels ten times higher. That the majority of the population has very low levels of vitamin D is not good, although it has become the most frequent fact, that is, normal. Generalized vitamin D deficiency has epidemic proportions (never better said), especially in latitudes where the incidence of sunlight is lower, and even more so among dark-skinned people. The same happens with vitamin C, whose generalized deficiency in the population is also aggravated by chronic hyperglycemia (high glucose induces urinary excretion of ascorbic acid). The food paradox of contemporary society, the hypercaloric malnutrition that characterizes more than half of the population, has a direct and proportional correlation with the severity and mortality of viral epidemics.An immense body of evidence obtained in the last twenty years shows unequivocally that the optimal range of this vitamin is well above 40 ng / mL, a concentration that, on the other hand, is easily achieved when exposed to an hour of perpendicular sun several days in a row. Numerous studies (and our own clinical experience on more than 3,000 patients) have shown that it is possible to obtain – and safely sustain – levels of between 60 and 90 nanograms/milliliter through adequate vitamin D supplementation, in the range of 5,000 to 10,000 IU daily, taken with fatty foods.
_____
LA ÉNIÈME VAGUE par Ernesto Prieto Gratacós
Une action fondamentale à entreprendre face aux épidémies virales a été, est et sera, le renforcement du système immunitaire grâce aux molécules responsables de son pouvoir germicide. Comme nous l’avons montré depuis le début de la crise sanitaire, ces substances sont précisément les nutriments immunoessentiels : vitamine D, ascorbate, zinc et sélénium. Ayant les nutriments nécessaires, les deux phases de notre formidable réponse immunitaire – innée et acquise – ont prévalu pendant des millénaires contre les virus, les bactéries et les champignons.
Chaque saison hivernale apporte une « vague » de malnutrition d’intensité variable, culminant toutes les quelques années. Cette vague a toujours été et continuera d’être, tant que des mesures alimentaires, comportementales et pharmacologiques ne seront pas prises pour la contrer. Ce livre est né de l’intention de donner des instructions précises sur la façon de mettre en œuvre cette stratégie et une sélection de près de 300 articles scientifiques qui la soutiennent. Ce n’est pas la peur mais l’action rationnelle qui nous permettra de retrouver la productivité normale dont notre société a besoin. Ceux qui insistent sur le discours alarmiste annonçant quotidiennement une deuxième vague et de nouvelles souches mutantes semblent ignorer les bases de l’épidémiologie et de la biologie moléculaire ou mentir délibérément au service d’intérêts économiques et politiques. Les articles référencés ci-dessus décrivent comment « six classes de coronavirus humains (HCoV) ont été précédemment identifiées, y compris HCoV-NL63 et HCoV-229E, appartenant au genre Alphacoronavirus, ainsi que HCoV-OC43, HCoVHKU1, SARS-CoV (syndrome respiratoire aigu sévère) et MERS CoV (syndrome respiratoire du Moyen-Orient), appartenant au genre Betacoronavirus ». La raison pour laquelle nous citons une telle description est de préciser que les coronavirus sont parmi nous depuis longtemps et que de nouvelles variantes apparaissent continuellement.
Chaque saison hivernale apporte une « vague » de malnutrition d’intensité variable, culminant toutes les quelques années. Cette vague a toujours été et continuera d’être, tant que des mesures alimentaires, comportementales et pharmacologiques ne seront pas prises pour la contrer. Ce livre est né de l’intention de donner des instructions précises sur la façon de mettre en œuvre cette stratégie et une sélection de près de 300 articles scientifiques qui la soutiennent. Ce n’est pas la peur mais l’action rationnelle qui nous permettra de retrouver la productivité normale dont notre société a besoin. Ceux qui insistent sur le discours alarmiste annonçant quotidiennement une deuxième vague et de nouvelles souches mutantes semblent ignorer les bases de l’épidémiologie et de la biologie moléculaire ou mentir délibérément au service d’intérêts économiques et politiques. Les articles référencés ci-dessus décrivent comment « six classes de coronavirus humains (HCoV) ont été précédemment identifiées, y compris HCoV-NL63 et HCoV-229E, appartenant au genre Alphacoronavirus, ainsi que HCoV-OC43, HCoVHKU1, SARS-CoV (syndrome respiratoire aigu sévère) et MERS CoV (syndrome respiratoire du Moyen-Orient), appartenant au genre Betacoronavirus ». La raison pour laquelle nous citons une telle description est de préciser que les coronavirus sont parmi nous depuis longtemps et que de nouvelles variantes apparaissent continuellement.
L’humanité compte déjà près de 8 milliards d’habitants, tandis que les animaux élevés pour l’industrie alimentaire se comptent par dizaines de milliards. Pour cette raison, la probabilité mathématique de mutations dans un ou plusieurs gènes, qui donnent à un virus les caractéristiques nécessaires pour infecter les humains, est de plus en plus élevée. Chacun des près de cinquante spécialistes avec lesquels nous avons parlé admet – au moins en privé – que le système immunitaire est la clé du succès. Dans le même temps, tout le monde s’accorde à dire que, compte tenu de la forte prévalence et de la distribution des coronavirus chez les animaux proches de nous, de leur immense diversité génétique, de la recombinaison fréquente de leurs génomes et de l’interaction croissante entre l’espèce humaine et le reste du règne animal, il faut s’attendre à ce que les nouveaux coronavirus sautent périodiquement de plus en plus fréquemment vers notre espèce. La supplémentation systématique de la population est la mesure la plus sûre et la plus rentable possible pour faire face aux centaines de virus divers qui pullulent parmi nous. Le cycle de la grippe saisonnière et son lien avec les vitaminesL’idée que les infections respiratoires virales éclatent avec l’automne-hiver et se dissipent avec le printemps-été est établie depuis longtemps dans l’épidémiologie de la grippe et d’autres grippes et pneumonies saisonnières. Ce n’est un secret pour personne que les niveaux de vitamine D diminuent rapidement avec la disparition des journées ensoleillées, tandis qu’une mauvaise nutrition les empêche de compenser leur baisse. La même chose se produit avec les niveaux de vitamine C dans le plasma sanguin à mesure que l’hiver s’aggrave et que les sources d’aliments frais, de vitamine C, de zinc et de sélénium diminuent. Bien que diverses sociétés universitaires, industrielles et médiatiques s’y soient vigoureusement opposées au début de la pandémie – ce qui vous incline vraiment à penser à un mélange de désinformation et d’intérêts commerciaux – la vitamine D est sortie triomphante dans la littérature scientifique liée à la COVID-19. En effet, à la date de cette publication, la base de données PubMed.gov enregistré plus de 450 articles scientifiques sur le rôle positif des niveaux de vitamine D dans l’incidence, la gravité et la mortalité dues à la COVID-19.
Malheureusement, les taux sanguins de 25-(OH)-D (vitamine D) présents dans les populations urbaines sont très faibles, souvent extrêmement déficients. La majeure partie des décès dus à la COVID-19 sont survenus chez des personnes qui, malheureusement, présentaient des niveaux catastrophiquement bas de calcéfidiol, la forme active de la vitamine, même du point de vue le plus orthodoxe. Ignorant les informations scientifiques établies, la plupart des professionnels de la santé considèrent qu’un taux de chalcéfidiol autour de 20 ng / dL est « sain » pour la simple raison que ce nombre se situe dans la plage de distribution normale de la population, qui tend à se situer entre 15 ng / mL et 30 ng / mL. Mais normal n’est pas synonyme de bien. D’un point de vue nutrigénomique, la quantité optimale de vitamine D compatible avec l’histoire évolutive de l’espèce humaine est celle qui est atteinte en prenant un bain de soleil ou en mangeant beaucoup d’aliments gras de qualité. Le caractère saisonnier de la grippe et des épidémies de grippe a un lien de causalité avec les vitamines D et C, mais les recommandations nutritionnelles restent injustement faibles, ignorant toutes les preuves épidémiologiques, biochimiques et anthropologiques en faveur de niveaux dix fois plus élevés. Que la majorité de la population ait de très faibles niveaux de vitamine D n’est pas bon, bien que ce soit devenu le fait le plus fréquent, c’est-à-dire normal. La carence généralisée en vitamine D a des proportions épidémiques (jamais mieux dit), en particulier sous les latitudes où l’incidence de la lumière du soleil est plus faible, et encore plus chez les personnes à la peau foncée. Il en va de même pour la vitamine C, dont la carence généralisée dans la population est également aggravée par l’hyperglycémie chronique (un taux élevé de glucose induit une excrétion urinaire d’acide ascorbique). Le paradoxe alimentaire de la société contemporaine, la malnutrition hypercalorique qui caractérise plus de la moitié de la population, a une corrélation directe et proportionnelle avec la gravité et la mortalité des épidémies virales.Un immense corpus de preuves obtenues au cours des vingt dernières années montre sans équivoque que la gamme optimale de cette vitamine est bien supérieure à 40 ng / mL, une concentration qui, en revanche, est facilement atteinte lorsqu’elle est exposée à une heure de soleil perpendiculaire plusieurs jours de suite. De nombreuses études (et notre propre expérience clinique sur plus de 3 000 patients) ont montré qu’il est possible d’obtenir – et de maintenir en toute sécurité – des niveaux compris entre 60 et 90 nanogrammes / millilitre grâce à une supplémentation adéquate en vitamine D, de l’ordre de 5 000 à 10 000 UI par jour, pris avec des aliments gras.
_____
LA ENÉSIMA OLA por Ernesto Prieto Gratacós
Una acción fundamental a tomar frente a las epidemias virales ha sido, es y será, el fortalecimiento del Sistema Inmune por medio de las moléculas responsables de su potencia germicida. Como hemos demostrado desde el inicio de la crisis sanitaria, dichas sustancias son precisamente los nutrientes inmunoesenciales: vitamina D, ascorbato, zinc y selenio. Teniendo los nutrientes necesarios, las dos fases de nuestra formidable respuesta inmunitaria -innata y adquirida- han prevalecido durante milenios contra virus bacterias y hongos.
Cada temporada invernal trae una “ola” de malnutrición de intensidad variable, con picos máximos cada cierto número de años. Este oleaje ha estado siempre y lo seguirá estando, mientras no se tomen medidas alimentarias, conductuales y farmacológicas para contrarrestarlo. Este libro nació de la intención de dar instrucciones precisas de como implementar esta estrategia y una selección de casi 300 artículos científicos que lafundamentan. No es el temor sino la acción racional lo que permitirá retomar la normal productividad que nuestra sociedad necesita. Quienes insisten en el discurso alarmista anunciando a diario una segunda ola y nuevas cepas mutantes, parecen ignorar las bases de la epidemiología y la biología molecular o bien mienten deliberadamente al servicio de intereses económicos y políticos. En los artículos referenciados arriba se describe cómo “seis clases de Coronavirus Humanos (HCoV) han sido identificados previamente, incluyendo el HCoV-NL63 y el HCoV-229E, pertenecientes al genus Alphacoronavirus, así como el HCoV-OC43, el HCoVHKU1, el SARS-CoV (Síndrome Respiratorio Severo Agudo) y el MERS CoV (Síndrome Respiratorio del Medio Oriente), pertenecientes al genus Betacoronavirus.” La razón por la que citamos dicha descripción es para dejar claro que los coronavirus están hace mucho entre nosotros, y nuevas variantes aparecen continuamente.
La Humanidad cuenta ya casi 8000 millones de habitantes, al tiempo que los animales que se crían para la industria alimenticia se cuentan en decenas de miles de millones. Por esta razón, la probabilidad matemática de mutaciones en uno o varios genes, que lesconfieran a un virus características necesarias para infectar a los humanos, son cada vez más altas. Cada uno de los casi cincuenta especialistas con que hemos conversado admite -al menos en privado- que el Sistema Inmune es la clave del éxito. Al mismo tiempo, todos concuerdan con que, dada la alta prevalencia y distribución de los coronavirus en los animales cercanos a nosotros, su inmensa diversidad genética, la frecuente recombinación de sus genomas y la creciente interacción entre la especie humana y el resto del Reino Animal, es de esperar que nuevos coronavirus salten periódicamente cada vez con más frecuencia hacia nuestra especie. La suplementación sistemática de la población es la medida más eficaz, segura y costo-efectiva posible para hacer frente a los centenares de virus diversos que pululan entre nosotros.
Ciclo estacional de la gripe y su nexo con las vitaminas
La noción de que las infecciones respiratorias virales recrudecen con el otoño-invierno y se disipan con la primavera-verano ha sido establecida en la epidemiología de la influenza y otras gripes y neumonías estacionales desde hace mucho. No es ningún secreto que los niveles de vitamina D declinan rápidamente con la desaparición de los días soleados, al tiempo que la nutrición deficiente impide compensar su declinación. Otro tanto sucede con los niveles de vitamina C en el plasma sanguíneo a medida que recrudece el invierno y declinan las fuentes de alimentos frescos, fuente de vitamina C, Zinc y Selenio. Si bien recibió una vigorosa oposición al principio de la pandemia por parte de varias sociedades académicas, de la industria y de los medios –lo que realmente inclina a pensar en una mezcla de desinformación e intereses comerciales- la vitamina D ha emergido triunfante en la literatura científica relacionada con COVID-19. Enefecto, a la fecha de esta publicación, la base de datos PubMed.gov registra más de 450 artículos científicos sobre el rol positivo de los niveles de vitamina D en la incidencia, la severidad y la mortalidad por COVID-19.
Lamentablemente, los niveles de 25-(OH)-D (vitamina D) en sangre presentes en las poblaciones urbanas son muy bajos, a menudo deficitarios en extremo. El grueso de las muertes por COVID-19 ocurrió en personas que, por desgracia, tenían niveles catastróficamente bajosde calcefidiol, la forma activa de la vitamina, incluso desde la perspectiva más ortodoxa. Haciendo caso omiso de la información científica ya establecida, la mayoría de los profesionales médicos consideran como “sano” un nivel de calcefidiol en torno a 20 ng/dL, por la sencilla razón de que dicho número se encuentra dentro del rango de distribución normal de la población, que tiende a ubicarse entre 15 ng/mL y 30 ng/mL. Pero normal no es sinónimo de bueno. Desde una perspectiva nutrigenómica, la cantidad óptima de vitamina D congruente con la historia evolutiva de la especie humana es aquella a la que se arriba tomando abundante sol o comiendo abundantes alimentos grasos de calidad.
La estacionalidad de las epidemias de influenza y gripe tiene un nexo causal con las vitaminas D y C, pero las recomendaciones nutricionales continúan siendo injustificadamente bajas, ignorando toda la evidencia epidemiológica, bioquímica y antropológica a favor de niveles diez veces más altos. Que la mayoría de la población tenga niveles bajísimos de vitamina D no es nada bueno, aunque se haya convertido en el hecho más frecuente, es decir, en lo normal. La deficiencia generalizada de vitamina D tiene proporciones epidémicas (nunca mejor dicho), en especial, en las latitudes donde laincidencia de los rayos solares es más escasa, y más aún entre las personas de piel oscura. Otro tanto sucede con la vitamina C, cuya deficiencia generalizada en la población se ve agravada además por la hiperglucemia crónica (la glucosa elevada induce la excreción urinaria de ácido ascórbico). La paradoja alimentaria de la sociedad contemporánea, la malnutrición hipercalórica que caracteriza a más de la mitad de la población, tiene correlación directa y proporcional con la severidad y mortalidad de las epidemias virales.
Un inmenso cuerpo de evidencia obtenido en los últimos veinte años muestra de manera inequívoca que el rango óptimo de dicha vitamina está muy por encima de los 40 ng/mL, concentración que, por otra parte, se consigue con facilidad al exponerse a una hora de sol perpendicular varios días seguidos. Numerosos estudios (y nuestra propia experiencia clínica sobre más de 3.000 pacientes) han demostrado que es posibleobtener –y sostener con seguridad- niveles de entre 60 y 90 nanogramos/mililitro por medio de la suplementación adecuada de vitamina D, en el rango de las 5.000 a 10.000 IU diarias, tomadas con alimentos grasos.
#salud#virus#covid#vitamin#zinc#selenium#selenio#vitamin d#vitamin c#vitamine#vitamina#vitamine d#vitamine c#vitamina d#immunity#gripe#gripa#flu#sistema immunitario#immunité#immune
1 note
·
View note
Text
得了感冒或流感,做核酸和抗原也會陽?
1、感冒、流感和新冠肺炎是由不同病毒引起的
在症狀表現上,感冒、流感和新冠病毒感染可能都會出現發熱、咳嗽、頭痛等症狀,但這三種疾病是由不同病毒引起的:
感冒:壹般由細菌、病毒、支原體、衣原體、立克次氏體等病原微生物所引起,其中病毒大多爲鼻病毒、副流感病毒、呼吸道合胞病毒、腺病毒等。
流感:由流感病毒引起。流感病毒屬正粘病毒科,爲單股、負鏈、分節段RNA病毒。根據核蛋白和基質蛋白不同,分爲甲、乙、丙、丁四型。目前感染人的主要是甲型流感病毒中的H1N1、H3N2亞型及乙型流感病毒中的Victoria和Yamagata系。
汗馬精力糖 悍馬糖 G28Q79 37F82K 日本金馬糖 飛馬糖 hercules大力神
新冠肺炎:由“2019新型冠狀病毒(2019-nCoV)”引起。2019-nCoV是已知的第7種可以感染人的冠狀病毒,其余6種分別是HCoV-229E、HCoV-OC43、HCoV-NL63、HCoV-HKU1、SARS-CoV(引發重症急性呼吸綜合征)和MERS-CoV(引發中東呼吸綜合征)。
2、核酸、抗原檢測是針對新冠病毒進行的
核酸檢測:
核酸是脫氧核糖核酸(DNA)和核糖核酸(RNA)的總稱,廣泛存在于所有動植物細胞、微生物體內。而新冠病毒核酸檢測也正是依據這壹原理進行的,利用每種病毒的核酸是不壹樣的原理,來對新冠病毒獨特的基因序列進行檢測。永春糖 馬來西亞永春糖 B糖 Candy B Candy B+ Complex 永春糖功效 永春糖效果
抗原檢測:抗原檢測是對標本裏是否有新冠的蛋白成分進行檢測,壹般檢測的是N蛋白,N蛋白是新冠病毒的核衣殼蛋白,如果標本中有新冠病毒N蛋白,就會和檢測板裏的特異性抗體結合,然後讓檢測線顯色。
通過以上我們可以得知,無論是核酸檢測還是抗原檢測,針對的都是新冠病毒的基因特性。所以,如果患者只是單純的患有感冒或流感,體內不存在新冠病毒,那麽進行新冠病毒核酸檢測或抗原檢測時,就不會顯現陽性的結果。汗馬金糖 spinach金糖 汗馬黑糖 mentalk黑糖 加強版悍馬糖 十週年紀念版36 東革阿裏蜂蜜
0 notes
Text
Targeting intracellular Neu1 for Coronavirus Infection Treatment
Preliminary report; There are no effective therapies for COVID-19 or antivirals against SARS-CoV-2. Furthermore, current vaccines appear less efficacious for new SARS-CoV-2 variants. Thus, there is an urgent need to better understand the virulence mechanisms of SARS-CoV-2 and the host response to develop therapeutic agents. Here, we show host Neu1 regulates coronavirus replication by controlling sialylation on coronavirus nucleocapsid protein. Coronavirus nucleocapsid proteins in COVID-19 patients and in coronavirus HCoV-OC43-infected cells were heavily sialylated; this sialylation controlled the RNA binding activity and replication of coronavirus. Neu1 overexpression increased HCoV-OC43 replication, whereas Neu1 knockdown reduced HCoV-OC43 replication. Moreover, a newly developed Neu1 inhibitor, Neu5Ac2en-OAcOMe, selectively targeted intracellular sialidase, which dramatically reduced HCoV-OC43 and SARS-CoV-2 replication in vitro and rescued mice from HCoV-OC43 infection-induced death. Our findings suggest that Neu1 inhibitors could be used to limit SARS-CoV-2 replication in patients with COVID-19, making Neu1 a potential therapeutic target for COVID-19 and future coronavirus pandemics. https://www.biorxiv.org/content/10.1101/2022.09.09.507342v1?rss=1%22&utm_source=dlvr.it&utm_medium=tumblr Read more ↓
0 notes
Text
Analysis of the seasonality of common human coronaviruses
Analysis of the seasonality of common human coronaviruses
Mild upper respiratory illness is known to be caused by the four common human coronaviruses (HCoVs), which include 2 beta (HCoV-HKU1 and HCoV-OC43) and 2 alpha (HCoV-NL63 and HCoV-229E) coronaviruses. These HCoVs, unlike betacoronaviruses (SARS-CoV, SARS-CoV-2, and Middle East respiratory syndrome coronavirus), have been observed to be endemic among humans, as indicated by their continuous and…

View On WordPress
0 notes
Text
L'esercizio fisico protegge dall'infezione da SARS-CoV-2 e dalle complicazioni derivate da COVID-19
L’esercizio fisico protegge dall’infezione da SARS-CoV-2 e dalle complicazioni derivate da COVID-19
Trova le ultime notizie e consigli su COVID-19 su Centro informazioni sul coronavirus (SARS-CoV-2)..
Dott.ssa Amaia Rodriguez/Fonte: Clinica Universitaria di Navarra
MADRID, SP. Il legame tra sovrappeso/obesità e un aumentato rischio di infezione SARS-CoV-2 e presentare una prognosi peggiore se la malattia viene contratta è una delle vie di studio più attive dall’inizio della pandemia, a cui è…

View On WordPress
#Coronavirus#coronavirus a Wuhan#coronavirus umano#coronavirus umano 229E#coronavirus umano OC43#COVID-19[feminine#COVID-19[FEMMINA#HCoV-229E#HCoV-OC43#HKU1#nCoV-2019#nuovo coronavirus 2019#Spagna#Vaccino contro il covid-19#Vaccino SARS-CoV-2
0 notes
Text
Réseaux sociaux: Comment vous préparer à un ASCO virtuel
Réseaux sociaux: Comment vous préparer à un ASCO virtuel
Pendant des décennies, la réunion de l’American Society of Clinical Oncology (ASCO) a été un pèlerinage annuel pour ceux de notre domaine, nous offrant un bref répit des pressions quotidiennes dans nos pratiques et une expérience immersive axée sur de nouvelles données ou idées qui peuvent être appliquées. à ces cas difficiles qui nous attendent lorsque nous rentrons chez nous.
Bien sûr, cette…
View On WordPress
#2019-nCoV#assister#camaraderie#camarades#cancer#carcinome#Coronavirus#coronavirus à Wuhan#Coronavirus humain HKU1#Coronavirus humain OC43#des médias sociaux#essais cliniques#Etudes cliniques#fatigue#H#HCoV-OC43#HRQOL#néoplasie maligne#nouveau coronavirus de 2019#QOL#qualité / accès / évaluation des soins de santé#qualité de vie#qualité de vie liée à la santé#recherche clinique#réseaux sociaux#social media#Social networks
0 notes
Text
Nitazoxanide is a potent inhibitor of human seasonal coronaviruses acting at postentry level: effect on viral spike glycoprotein
Preliminary report; Coronaviridae is recognized as one of the most rapidly evolving virus family as a consequence of the high genomic nucleotide substitution rates and recombination. The family comprises a large number of enveloped, positive-sense single-stranded RNA viruses, causing an array of diseases of varying severity in animals and humans. To date, seven human coronaviruses (HCoV) have been identified, namely HCoV-229E, HCoV-NL63, HCoV-OC43 and HCoV-HKU1, which are globally circulating in the human population (seasonal HCoV, sHCoV), and the highly pathogenic SARS-CoV, MERS-CoV and SARS-CoV-2. Seasonal HCoV are estimated to contribute to 15-30% of common cold cases in humans; although diseases are generally self-limiting, sHCoV can sometimes cause severe lower respiratory infections, as well as enteric and neurological diseases. No specific treatment is presently available for sHCoV infections. Herein we show that the anti-infective drug nitazoxanide has a potent antiviral activity against three human endemic coronaviruses, the Alpha-coronaviruses HCoV-229E and HCoV-NL63, and the Beta-coronavirus HCoV-OC43 in cell culture with IC50 ranging between 0.05 and 0.15 g/ml, and high selectivity indexes. We found that nitazoxanide does not affect HCoV adsorption, entry or uncoating, but acts at postentry level and interferes with the spike glycoprotein maturation, hampering its terminal glycosylation at an endoglycosidase H-sensitive stage. Altogether the results indicate that nitazoxanide, due to its broad-spectrum anti-coronavirus activity, may represent a readily available useful tool in the treatment of seasonal coronavirus infections. https://www.biorxiv.org/content/10.1101/2022.07.13.499346v1?rss=1%22&utm_source=dlvr.it&utm_medium=tumblr Read more ↓
0 notes
Text
The virucidal effects of tea tree oil against FCoVII and HCoV-OC43
The virucidal effects of tea tree oil against FCoVII and HCoV-OC43
In a recent study published in Molecules, researchers assessed the probable efficacy of tea tree oil (TTO) as a natural disinfectant against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using the human coronavirus OC43 (HCoV-OC43) and feline coronavirus (FCoVII) as surrogate models.
Study: Potential Use of Tea Tree Oil as a Disinfectant Agent against Coronaviruses: A Combined…

View On WordPress
0 notes
Text
美学者母が新型コロナは風邪だと言う原理(標本空間の現実とそれぞれの現実)2016年の日本の肺炎死亡者数が十一万九千人の事実
(引用URL)
国立感染症研究所
https://www.niid.go.jp/.../kansenno.../9303-coronavirus.html
東京都健康安全研究センター
http://www.tokyo-eiken.go.jp/sage/sage2018/
厚生労働省
https://www.mhlw.go.jp/.../jinkou/suikei16/dl/2016suikei.pdf
世界はなぜ風邪(新型コロナ)でパニックになったのか。
(インフォデミック時代の生き方)
https://machromatic.net/column_0370.html
コロナも新型コロナワクチンの接種が始まっていますが、
未だインフォデミックは収束していません。
もうこのまま新型コロナのインフォデミックが、
三年目に突入していくのだろうと色々と諦めていますが、
私は新型コロナはインフォデミックであると認識していますし、
現在の所その私の認識は間違っていなかったと考えています。
たまにSNSとかで医学の専門家や、
感染症の専門家が、
「新型コロナは風邪」は間違いだと発言を散見します。
確かに医学の専門家や感染症の専門家から言えば、
「新型コロナは風邪」は間違いという事が、
風邪という定義上当てはまらないということは理解できます。
なぜなら風邪という概念の定義を、
どの様にアウトラインをとるのかによって、
つまりそれぞれの前提条件によって、
「風邪」とか「風邪」でないとか、
つまりその領域の専門家にとっては、
あくまで「風邪」ではないのでしょう。
それはそのはずで、
風邪は症状を表すもので、
その症状を誘発する元のほとんどがウイルスの感染からのものです。
ちなみに、
その風邪のウイルスにコロナウイルスがあります。
これまで知られていたコロナウイルスは、
4種類のコロナウイルス(Human Coronavirus:HCoV)は、
HCoV-229E、HCoV-OC43、HCoV-NL63、HCoV-HKU1である。
風邪の10~15%(流行期35%)はこれら4種のコロナウイルスを原因とする。
そのほかに2種類の重症肺炎ウイルスがあります、
重症急性呼吸器症候群コロナウイルス(SARS-CoV)
中東呼吸器症候群コロナウイルス(MERS-CoV)
以上を参考に日常的に感染する4種類の風邪ウイルスとは違うと言われれば、
それはその通りでその様な切り口で言えば風邪ではないとも言えます。
しかし感染症であり、
また風邪と同じ症状を伴い、
人によってはその症状で治ることもあれば重症化する事もある。
またその様な症状が出る事がない人もいる。
風邪は「コロナウイルス」である、
そして新型���コロナウイルス」は風邪ではない。
「新型」をどの様な概念で捉えるのかで前提条件が違い、
コンテクストが変わってくるのが理解できます。
では前置きはこのくらいにして、
事実をベースに言説していきたいと思います。
まず注目するデータとして、
厚生労働省のデータの死因順位別死亡数の年次推移では、
2014年以降は肺炎が死因の3位になっており、
毎年10万人以上が肺炎で亡くなっています。
2014年から2016年のデータから理解できる通り、
新型コロナの流行前です。
ちなみに2020年の肺炎での死因は5位です。
そして死亡者数は8万人です。
新型コロナの流行で、
肺炎での死亡者は2万人減っているわけですね。
つまりここで理解ができるのは、
認知されるものと、認知されないもの、
意識が集中するものと、意識がされないもの、
つまり情報が人間をいかにコントロールし、
いかに現実を変化させるのかという事実が理解できます。
しかしその「現実」とは誰にとっての現実でしょうか。
少なくとも「我」にとっての「現実」ではありません。
それは言えば国家という実存を確認できない、
抽象的な存在にとっての「現実」でしょうか。
それとも「医学」という実存の確認できない、
抽象的な存在にとっての「現実」でしょうか、
はたまた統計学という実存を確認できない、
抽象的な存在にとっての「現実」でしょうか。
「我」にとっての「現実」と、
「標本空間」にとっての「現実」とは違うという事実です。
ここで少し確率論的な言説をします。
確率というものをどの様に認識するのか、
確率を「質」と捉えるのか「面積」と捉えるのか。
この前提条件で、
新型コロナを「風邪」と捉えるのか、
「風邪」とは違うと捉えるのかの違いが生まれます。
つまり簡単に言えば、
天気予報の降水確率をどう認識するのかに似ています。
例えば天気予報の降水確率をみなさんはどう認識しているでしょうか。
例えば降水確率20パーセントをどう捉えるでしょうか、
これは実は非常に難しい問題なのですが、
あえて「質」で捉えるならば、
ちょっと霧の様な雨が全体に降れば20%でも許容できる。
その様な「質」の捉え方もできます。
しかし基本的に確率とは面積と同じであるのです。
簡単に言えば、
任意の領域を設定した場合、
その20%の面積に雨が降る。
それが20%という確率です。
すなわち、
総体として20%という確率でも、
80%の人には雨が降らないという現実があり、
20%の人には雨が降るという現実が有るのです。
それを違った形で言えば、
その総体の80%の人には100%雨が降らない、
また20%の人には100%雨が降る。
つまりここから理解できるのは、
個別において、
誰かにとっては100%でも、
誰かにとっては0%である。
つまりここで、
標本空間を現実とする実在が、
そもそも存在しないことが理解できます。
もっと個別として捉えてみると、
それはその人々の個別的現実において、
雨が降るか降らないかは、
五分五分としての現実しか無いという事実です。
そしてこの確率論的な言説は、
「新型コロナ」にももれなく言えることであり、
もっと言えばあらゆる現象に言える「原理」である。
私たちは常に産まれてこのかた、
あらゆるリスクと共に生きて、
今この現実を生きているということを、
忘れ去っているのではないだろうか。
海に入れば溺れるリスク、
車に乗れば事故するリスク、
薬を服めば副作用のリスク、
山に登れば遭難するリスク、
何か食べればお腹を壊すリスク。
数えれば永遠に続くリスク、
まさに、
「生きるということは死ぬということを内包している」
ここで「リスク」というネガティヴな言い方をしているが、
それは「対」であり、
全ての事柄はその「対」を内包しているという「真理」である。
それはその「行為」「現象」に対する「対」である。
つまりここまでで何が言いたいのか。
それは個々の世界において、
「現実」は違うということである。
まさにこの瞬間に、
新型コロナの陽性反応がでた人もいるだろうし、
新型コロナが原因で死亡した人もいるだろう。
それはその当人にとって、
紛れもない現実であるが、
しかしそれ以上に、
それぞれの個々人が、
新型コロナ以外にも、
沢山の障害を持った現実があるのである。
またその理由で死んでいく人たちも多くいる。
自殺、病気、事故。
新型コロナとは違う理由で、
この刹那に苦しんでいる人々が多く��る。
社会では何の問題にもされていない事で、
認識されず、
意識されず、
悩み苦しみ、
死を選ぶ人たちが沢山いる。
2020年の自殺者は2万人。
それぞれの人間の個々において、
それぞれに、
新型コロナ以上のクライシスがあるのではないか。
ここまで考察してきた事は、
インターネットが普及した事を原理にしていると私は考えている。
情報の伝播速度の革命である。
ある所で起こった現実が瞬時にあらゆる所へと共有される。
そしてその共有された現実を、
「我の現実」としてその、
シミュレーション世界に没入するのである。
これはまさに人間の本質である。
それが私のアート作品として、
2010年に「ウェブアート宣言」として発表したものである。
この様な構造を原理から理解している私だから言える事として、
もっと目の前の現実を生きていくべきであると述べておきたい。
その考えを言い換えたものが、
「コロナは風邪である」という言説なのだ。
つまり、
「新型コロナ」というものは、
特別なクライシスではなく、
私達は個々人がそれぞれ様々なクライシスを、
日常的に乗り越えながら生きている事を、
そもそも忘れてしまっているのではないか。
その様な思いが伝われば幸いです。
僕にとっては20年くらい前に、
製薬や医学が薬を売るために、
「うつは風邪」
って言ってた方がよっぽど恐ろしい。
美学者母
29 notes
·
View notes
Link
2020 Yale-G’s Monthly Clinical Updates According to www.uptodate.com
(As of 2020-11-12, updated in Yale-G’s 6th-Ed Kindle Version; will be emailed to buyers of Ed6 paper books)
Chapter 1: Infectious Diseases
Special Viruses: Coronaviruses
Coronaviruses are important human and animal pathogens, accounting for 5-10% community-acquired URIs in adults and probably also playing a role in severe LRIs, particularly in immunocompromised patients and primarily in the winter. Virology: Medium-sized enveloped positive-stranded RNA viruses as a family within the Nidovirales order, further classified into four genera (alpha, beta, gamma, delta), encoding 4-5 structural proteins, S, M, N, HE, and E; severe types: severe acute respiratory syndrome coronavirus (SARS-CoV), Middle East respiratory syndrome coronavirus (MERS-CoV), and novel coronavirus (2019-nCoV, which causes COVID-19). Routes of transmission: Similar to that of rhinoviruses, via direct contact with infected secretions or large aerosol droplets. Immunity develops soon after infection but wanes gradually over time. Reinfection is common. Clinical manifestations: 1. Coronaviruses mostly cause respiratory symptoms (nasal congestion, rhinorrhea, and cough) and influenza-like symptoms (fever, headache). 2. Severe types (2019-nCoV, MERS-CoV, and SARS-CoV): Typically with pneumonia–fever, cough, dyspnea, and bilateral infiltrates on chest imaging, and sometimes enterocolitis (diarrhea), particularly in immunocompromised hosts (HIV+, elders, children). 3. Most community-acquired coronavirus infections are diagnosed clinically, although RT-PCR applied to respiratory secretions is the diagnostic test of choice.
Treatment: 1. Mainly consists of ensuring appropriate infection control and supportive care for sepsis and acute respiratory distress syndrome. 2. In study: Chloroquine showed activity against the SARS-CoV, HCoV-229E, and HCoV-OC43 and remdesivir against 2019-nCoV. Dexamethasone may have clinical benefit.
Prevention: 1. For most coronaviruses: The same as for rhinovirus infections, which consist of handwashing and the careful disposal of materials infected with nasal sec retions. 2. For novel coronavirus (2019-nCoV), MERS-CoV, and SARS-CoV: (1) Preventing exposure by diligent hand washing, respiratory hygiene, and avoiding close contact with live or dead animals and ill individuals. (2) Infection control for suspected or confirmed cases: Wear a medical mask to contain their respiratory secretions and seek medical attention; standard contact and airborne precautions, with eye protection.
Hepatitis A: HAV vaccine is newly recommended to adults at increased risk for HAV infection (substance use treatment centers, group homes, and day care facilities for disabled persons), and to all children and adolescents aged 2 to 18 years who have not previously received HAV vaccine.
Hepatitis C: 8-week glecaprevir-pibrentasvir is recommended for chronic HCV infection in treatment-naive patients. In addition to the new broad one-time HCV screening (17-79 y/a), a repeated screening in individuals with ongoing risk factors is suggested.
New: Lefamulin is active against many common community-acquired pneumonia pathogens, including S. pneumoniae, Hib, M. catarrhalis, S. aureus, and atypical pathogens.
New: Cefiderocol is a novel parenteral cephalosporin that has activity against multidrug-resistant gram-negative bacteria, including carbapenemase-producing organisms and Pseudomonas aeruginosa resistant to other beta-lactams. It’s reserved for infections for which there are no alternative options.
New: Novel macrolide fidaxomicin is reserved for treating the second or greater recurrence of C. difficile infection in children.
Vitamin C is not beneficial in adults with sepsis and ARDS.
Chapter 2: CVD
AF: Catheter ablation is recommended to some drug-refractory, paroxysmal AF to decrease symptom burden. In study: Renal nerve denervation has been proposed as an adjunctive therapy to catheter ablation in hypertensive patients with AF. Alcohol abstinence lowers the risk of recurrent atrial fibrillation among regular drinkers.
VF: For nonshockable rhythms, epinephrine is given as soon as feasible during CPR, while for shockable rhythms epinephrine is given after initial defibrillation attempts are unsuccessful. Avoid vasopressin use.
All patients with an acute coronary syndrome (ACS) should receive a P2Y12 inhibitor. For patients undergoing an invasive approach, either prasugrel or ticagrelor
has been preferred to clopidogrel. Long-term antithrombotic therapy in patients with stable CAD and AF has newly been modified as either anticoagulant (AC)
monotherapy or AC plus a single antiplatelet agent.
Long-term antithrombotic therapy (rivaroxaban +/- aspirin) is recommended for patients with AF and stable CAD. Ticagrelor plus aspirin is recommended for some patients with CAD and diabetes.
VTE (venous thromboembolism): LMW heparin or oral anticoagulant edoxaban is the first-line anticoagulants in patients with cancer-associated VTE.
Dosing of warfarin for VTE prophylaxis in patients undergoing total hip or total knee arthroplasty should continue to target an INR of 2.5.
Chapter 3: Resp. Disorders
Asthma: Benralizumab is an IL-5 receptor antibody that is used as add-on therapy for patients with severe asthma and high blood eosinophil counts.
Recombinant GM-CSF is still reserved for patients who cannot undergo, or who have failed, whole lung lavage.
Pulmonary embolism (PE): PE response teams (PERT, with specialists from vascular surgery, critical care, interventional radiology, emergency medicine, cardiac surgery, and cardiology) are being increasingly used in management of patients with intermediate and high-risk PE.
Although high-sensitivity D-dimer testing is preferred, protocols that use D-dimer levels adjusted for pretest probability may be an alternative to unadjusted D-dimer in patients with a low pretest probability for PE.
Non-small cell lung cancer (NSCLC): Newly approved capmatinib is for advanced NSCLC associated with a MET mutation, and selpercatinib for those with advanced RET fusion-positive. Atezolizumab was newly approved for PD-L1 high NSCLC.
Circulating tumor DNA tests for cancers such as NSCLC are increasingly used as “liquid biopsy”. Due to its limited sensitivity, NSCLC patients who test (-) for the biomarkers should undergo tissue biopsy.
Cystic Fibrosis (CF): Tx: CFTR modulator therapy (elexacaftor-tezacaftor-ivacaftor) is recommended for patients ≥12 years with the F508del variant.
Vitamin E acetate has been implicated in the development of electronic-cigarette, or vaping, product use associated lung injury.
Chapter 4: Digestive and Nutritional Disorders
Comparison of Primary Biliary Cholangitis (PBC) and Primary Sclerosing Cholangitis (PSC):
Common: They are two major types of chronic cholestatic liver disease, with fatigue, pruritus, obstructive jaundice, similar biochemical tests of copper metabolism, overlapped histology (which is not diagnostic), destructive cholangitis, and both ultimately result in cirrhosis and hepatic failure. (1) PBC: Mainly in middle-aged women, with keratoconjunctivitis sicca, hyperpigmentation, and high titer of antimitochondrial Ab (which is negative for PSC). (2) PSC: Primarily in middle-aged men, with chronic ulcerative colitis (80%), irregular intra- and extra-hepatic bile ducts, and anti-centromere Ab (+).
CRC: Patients with colorectal adenomas at high risk for subsequent colorectal cancer (CRC) (≥3 adenomas, villous type with high-grade dysplasia, or ≥10 mm in diameter) are advised short follow-up intervals for CRC surveillance. Pembrolizumab was approved for the first-line treatment of patients with unresectable or metastatic DNA mismatch repair (dMMR) CRC.
UC and CRC: Patients with extensive colitis (not proctitis or left-sided colitis) have increased CRC risk.
Eradication of H. pylori: adding bismuth to clarithromycin-based triple therapy for patients with risk factors for macrolide resistance.
Thromboelastography and rotational thromboelastometry are bedside tests recommended for patients with cirrhosis and bleeding.
Pancreatic cancer: Screening for patients at risk for hereditary pancreatic cancer (PC): Individuals with mutations in the ataxia-telangiectasia mutated gene and one first-degree relative with PC can be screened with endoscopic ultrasound and/or MRI/magnetic retrograde cholangiopancreatography.
Olaparib is recommended for BRCA-mutated advanced pancreatic cancer after 16 weeks of initial platinum-containing therapy.
HCC (unresectable): New first-line therapy is a TKI (sorafenib or sunitinib) or immune checkpoint inhibitor atezolizumab plus bevacizumab, +/- doxorubicin. Monitor kidney toxicity for these drugs.
UC: Ustekinumab (-umab) anti-interleukin 12/23 antibody, is newly approved for the treatment of UC.
Crohn disease: The combination of partial enteral nutrition with the specific Crohn disease exclusion diet is a valuable alternative to exclusive enteral nutrition for induction of remission.
Obesity: Lorcaserin, a 5HT2C agonist that can reduce food intake, has been discontinued in the treatment of obesity due to increased malignancies (including colorectal, pancreatic, and lung cancers).
Diet and cancer deaths: A low-fat diet rich in vegetables, fruits, and grains experienced fewer deaths resulted from many types of cancer.
Note that H2-blockers (-tidines) are no longer recommended due to the associated carcinogenic N-nitrosodimethylamine.
Gastrointestinal Stromal Tumors (GIST):
GIST is a rare type of tumor that occurs in the GI tract, mostly in the stomach (50%) or small intestine. As a sarcoma, it’s the #1 common in the GI tract. It is considered to grow from specialized cells in the GI tract called interstitial cells of Cajal, associated with high rates of malignant transformation.
Clinical features and diagnosis: Most GISTs are asymptomatic. Nausea, early satiety, bloating, weight loss, and signs of anemia may develop, depending on the location, size, and pattern of growth of the tumor. They are best diagnosed by CT scan and mostly positive staining for CD117 (C-Kit), CD34, and/or DOG-1.
Treatment: Approaches include resection of primary low-risk tumors, resection of high-risk primary or metastatic tumors with a tyrosine kinase inhibitor (TKI) imatinib for 12 months, or if the tumor is unresectable, neoadjuvant imatinib followed by resection. Radiofrequency ablation has shown to be effective when surgery is not suitable. Newer therapies of ipilimumab, nivolumab, and endoscopic ultrasound alcohol ablation have shown promising results. Avapritinib or ripretinib (new TKI) is recommended for advanced unresectable or metastatic GIST with PDGFRA mutations.
Anal Cancer:
Anal cancer is uncommon and more similar to a genital cancer than it is to a GI malignancy by etiology. By histology, it is divided into SCC (#1 common) and adenocarcinoma. Anal cancer (particularly SCC among women) has increased fast over the last 30 years and may surpass cervical cancer to become the leading HPV-linked cancer in older women. A higher incidence has been associated with HPV/HIV infection, multiple sexual partners, genital warts, receptive anal intercourse, and cigarette smoking. SCCs that arise in the rectum are treated as anal canal SCCs.
Clinical features and diagnosis: 1. Bleeding (#1) and itching (often mistaken as hemorrhoids). Later on, patients may develop focal pain or pressure, unusual discharges, and lump near the anus, and changes in bowel habits. 2. Diagnosis is made by a routine digital rectal exam, anoscopy/proctoscopy plus biopsy, +/- endorectal ultrasound.
Treatment: Anal cancer is primarily treated with a combination of radiation, chemotherapy, and surgery—especially for patients failing the above therapy or for true perianal skin cancers.
Chapter 5: Endocrinology
Diabetes (DM):
Liraglutide can be added as a second agent for type-2 DM patients who fail monotherapy with metformin or as a third agent for those who fail combination therapy with metformin and insulin.
Metformin is suggested to prevent type 2 DM in high-risk patients in whom lifestyle interventions fail to improve glycemic indices.
Metabolic (bariatric) surgery improves glucose control in obese patients with type 2 DM and also reduce diabetes-related complications, such as CVD.
Teprotumumab, an insulin-like growth factor 1 receptor inhibitor, can be used for Graves’ orbitopathy if corticosteroids are not effective. Subclinical hypothyroidism should not be routinely treated (with T4) in older adults with TSH <10 mU/L.
Chapter 6: Hematology & Immunology
Anticoagulants: Apixaban is preferred to warfarin for atrial fibrillation with osteoporosis because it lowers the risk of fracture. Rivaroxaban is inferior to warfarin for antiphospholipid syndrome.
Cancer-associated VTE: LMW heparin or oral edoxaban is the first-line anticoagulant prophylaxis.
NH-Lymphoma Tx: New suggestion is four cycles of R(rituximab)-CHOP for limited stage (stage I or II) diffuse large B cell non-Hodgkin lymphoma (DLBCL) without adverse features. New suggestions: selinexor is for patients with ≥2 relapses of DLBCL, and tafasitamab plus lenalidomide is for patients with r/r DLBCL who are not eligible for autologous HCT.
Chimeric antigen receptor (CAR)-T (NK) immunotherapy is newly suggested for refractory lymphoid malignancies, with less toxicity than CAR-T therapy. Polatuzumab + bendamustine + rituximab (PBR) is an alternative to CAR-T, allogeneic HCT, etc. for multiply relapsed diffuse large B-C NHL.
Refractory classic Hodgkin lymphoma (r/r cHL) is responsive to immune checkpoint inhibition with pembrolizumab or nivolumab, including those previously treated with brentuximab vedotin or autologous transplantation.
Mantle cell lymphoma: Induction therapy is bendamustine + rituximab or other conventional chemoimmunotherapy rather than more intensive approaches. CAR-T cell therapy is for refractory mantle cell lymphoma.
AML: Gilteritinib is a new alternative to intensive chemotherapy for patients with FLT3-mutated r/r AML.
Oral decitabine plus cedazuridine is suggested for MDS and chronic myelomonocytic leukemia.
Multiple myeloma (MM): Levofloxacin prophylaxis is suggested for patients with newly diagnosed MM during the first three months of treatment. For relapsed MM: Three-drug regimens (daratumumab, carfilzomib, and dexamethasone) are newly recommended.
Transplantation: As the transplant waitlist continues to grow, there may be an increasing need of HIV-positive to HIV-positive transplants.
Porphyria:
Porphyria is a group of disorders (mostly inherited) caused by an overaccumulation of porphyrin, which results in hemoglobin and neurovisceral dysfunctions, and skin lesions.
Clinical types, features, and diagnosis: I. Acute porphyrias: 1. Acute intermittent porphyria: Increased porphobilinogen (PBG) causes attacks of abdominal pain (90%), neurologic dysfunction (tetraparesis, limb pain and weakness), psychosis, and constipation, but no rash. Discolored urine is common. 2. ALA (aminolevulinic acid) dehydratase deficiency porphyria (Doss porphyria): Sensorimotor neuropathy and cutaneous photosensitivity. 3. Hereditary coproporphyria: Abdominal pain, constipation, neuropathies, and skin rash. 4. Variegate porphyria: Cutaneous photosensitivity and neuropathies. II. Chronic porphyrias: 1. Erythropoietic porphyria: Deficient uroporphyrinogen III synthase leads to cutaneous photosensitivity characterized by blisters, erosions, and scarring of light-exposed skin. Hemolytic anemia, splenomegaly, and osseous fragility may occur. 2. Cutaneous porphyrias–porphyria cutanea tarda: Skin fragility, photosensitivity, and blistering; the liver and nervous system may or may not be involved. III. Lab diagnosis: Significantly increased ALA and PBG levels in urine have 100% specificity for most acute porphyrias. Normal PBG levels in urine can exclude acute porphyria.
Treatment: 1. Acute episodes: Parenteral narcotics are indicated for pain relief. Hemin (plasma-derived intravenous heme) is the definitive treatment and mainstay of management. 2. Avoidance of sunlight is the key in treating cutaneous porphyrias. Afamelanotide may permit increased duration of sun exposure in patients with erythropoietic protoporphyria.
Chapter 7: Renal & UG
Membranous nephropathy (MN): Rituximab is a first-line therapy in patients with high or moderate risk of progressive disease and requiring immunosuppressive therapy.
Diabetes Insipidus (DI): Arginine-stimulated plasma copeptin assays are newly used to diagnose central DI and primary polydipsia, often alleviating the need for water restriction, hypertonic saline, and exogenous desmopressin.
Prostate cancer: Enzalutamide (new androgen blocker) is available for metastatic castration-sensitive prostate cancer. Cabazitaxel, despite its great toxicity, is suggested as third-line agent for metastatic prostate cancer. Either early salvage RT or adjuvant RT is acceptable after radical prostatectomy for high-risk disease.
UG cancers: Nivolumab plus ipilimumab is suggested in metastatic renal cell carcinoma for long-term survival.
Enfortumab vedotin is suggested in locally advanced or metastatic urothelial carcinoma. Maintenance avelumab is recommended with other chemotherapy in advanced urothelial bladder cancer. Pyelocalyceal mitomycin is suggested for low-grade upper tract urothelial carcinomas.
Chapter 8: Rheumatology
Janus kinase (JAK) inhibitors (upadacitinib, filgotinib) are new options for active, resistant RA and ankylosing spondylitis.
Graves’ orbitopathy: new therapy–teprotumumab, an insulin-like growth factor 1 receptor inhibitor.
Chapter 9: Neurology & Special Senses
Epilepsy: Cenobamate, a novel tetrazole alkyl carbamate derivative that inhibits Na-channels, provides a new treatment option for patients with drug-resistant focal epilepsy. A benzodiazepine plus either fosphenytoin, valproate, or levetiracetam is recommended as the initial treatment of generalized convulsive status epilepticus.
Migraine: Lasmiditan is a selective 5H1F receptor agonist that lacks vasoconstrictor activity, new therapy for patients with relative contraindications to triptans due to cardiovascular risk factors.
Stroke: New recommendation for cerebellar hemorrhages >3 cm in diameter is surgical evacuation.
TBI: Antifibrolytic agent tranexamic acid is newly recommended for moderate and severe acute traumatic brain injury (TBI).
Ofatumumab is a new agent that may delay progression of MS.
Chapter 10: Dermatology
Minocycline foam is a new topical drug option for moderate to severe acne vulgaris.
Melanloma: Nivolumab plus ipilimumab in metastatic melanoma has confirmed long-term survival. With sun-protective behavior, melanoma incidence is decreasing.
New: Tazemetostat is suggested in patients with locally advanced or metastatic epithelioid sarcoma (rare and aggressive) ineligible for complete surgical resection.
Psoriasis: New therapies for severe psoriasis and psoriatic arthritis: a TNF-alpha inhibitor (infliximab or adalimumab, golimumab) or IL-inhibitor (etanercept or ustekinumab) is effective. Ixekizumab is a newly approved monoclonal antibody against IL-17A. Clinical data support vigilance for signs of symptoms of malignancy in patients with psoriasis.
Chapter 11: GYH
Breast cancer:
Although combined CDK 4/6 and aromatase inhibition is an effective strategy in older adults with advanced receptor-positive, HER2-negative breast cancer, toxicities (myelosuppression, diarrhea, and increased creatinine) should be carefully monitored. SC trastuzumab and pertuzumab is newly recommended for HER2-positive breast cancer.
Whole breast irradiation is suggested for most early-stage breast cancers treated with lumpectomy. Accelerated partial breast irradiation can be an alternative for women ≥50 years old with small (≤2 cm), hormone receptor-positive, node-negative tumors.
Endocrine therapy is recommended for breast cancer prevention in high-risk postmenopausal women.
Uterine fibroids: Elagolix (oral gonadotropin-releasing hormone antagonist) in combination with estradiol and norethindrone is for treatment of heavy menstrual bleeding (HMB) due to uterine fibroids.
Chapter 12: OB
Table 12-6: Active labor can start after OS > 4cm, and 6cm is relatively more acceptable but not a strict number.
Table 12-7: Preeclampsia is a multisystem progressive disorder characterized by the new onset of hypertension and proteinuria, or of hypertension and significant end-organ dysfunction with or without proteinuria, in the last half of pregnancy or postpartum. Once a diagnosis of preeclampsia is established, testing for proteinuria is no longerdiagnostic or prognostic. “proteinuria>5g/24hours” may only indicate the severity.
Mole: For partial moles, obtain a confirmatory hCG level one month after normalization; for complete moles, reduce monitoring from 6 to 3 months post-normalization.
Chapter 14: EM
SHOCK RESUSCITATION
Emergency treatment—critical care!
“A-B-C”: Breathing: …In mechanically ventilated adults with critical illness in ICU, intermittent sedative-analgesic medications (morphine, propofol, midazolam) are
recommended.
Chapter 15: Surgery
Surgery and Geriatrics: Hemiarthroplasty is a suitable option for patients who sustain a displaced femoral neck fracture.
Chapter 16: Psychiatry
Depression: Both short-term and maintenance therapies with esketamine are beneficial for treatment-resistant depression.
Schizophrenia: Long-term antipsychotics may decrease long-term suicide mortality.
Narcolepsy: Pitolisant is a novel oral histamine H3 receptor inverse agonist used in narcolepsy patients with poor response or tolerate to other medications. Oxybate salts, a lower sodium mixed-salt formulation of gamma hydroxybutyrate is for treatment of narcolepsy with cataplexy.
Chapter 17: Last Chapter
PEARLS—Table 17-9: Important Immunization Schedules for All (2020, USA)
Vaccine Birth 2M 4M 6M 12-15M 2Y 4-6Y 11-12Y Sum
HAV 1st 2nd (2-18Y) 2 doses
HBV 1st 2nd 3rd (6-12M) 3 doses
DTaP 1st 2nd 3rd 4th (15-18M) 5th + Td per 10Y
IPV 1st 2nd 3rd (6-18M) 4th 4 doses
Rotavirus 1st 2nd 2 doses
Hib 1st 2nd (3rd) (3-4th) 3-4 doses
MMR 1st 2nd 2 doses
Varicella 1st 2nd + Shingles at 60Y
Influenza 1st (IIV: 6-12Y; LAIV: >2Y (2nd dose) 1-2 doses annually
PCV 1st 2nd 3rd 4th PCV13+PPSV at 65Y
MCV (Men A, B) 1st Booster at 16Y
HPV 9-12Y starting: <15Y: 2 doses (0, 6-12M); >15Y or immunosuppression: 3 doses (0, 2, 6M).
Chapter 17 HYQ answer 22: No routine prostate cancer screening (including PSA) is recommended and answer “G” is still correct–PSA
screening among healthy men is not routinely done but should be indicated in a patient with two risk factors.
9 notes
·
View notes
Text
Disparities Seen in COVID-19–Related Avoidance of Care
Disparities Seen in COVID-19–Related Avoidance of Care
[ad_1]
Editor’s note: Find the latest COVID-19 news and guidance in Medscape’s Coronavirus Resource Center.
In the early weeks and months of the COVID-19 pandemic, many people were trying to avoid the coronavirus by staying away from emergency rooms and medical offices. But how many people is “many”?

Turns out almost 41% of Americans delayed or avoided some form of medical care…
View On WordPress
#2019 Novel Coronavirus#2019-nCoV#Avoidance#Care#caregiver#Coronavirus#COVID19Related#Disparities#HCoV-229E#HCoV-OC43#health insurance#Human coronavirus 229E#Human coronavirus HKU1#Human coronavirus OC43#Wuhan coronavirus
0 notes
Text
Far-UVC light (222 nm) efficiently and safely inactivates airborne human coronaviruses
Abstract
A direct approach to limit airborne viral transmissions is to inactivate them within a short time of their production. kryptolight, typically at 254 nm, is effective in this context but, used directly, can be a health hazard to skin and eyes. By contrast, far-UVC light (207–222 nm) efficiently kills pathogens potentially without harm to exposed human tissues. We previously demonstrated that 222-nm far-UVC light efficiently kills airborne influenza virus and we extend those studies to explore far-UVC efficacy against airborne human coronaviruses alpha HCoV-229E and beta HCoV-OC43. Low doses of 1.7 and 1.2 mJ/cm2 inactivated 99.9% of aerosolized coronavirus 229E and OC43, respectively. As all human coronaviruses have similar genomic sizes, far-UVC light would be expected to show similar inactivation efficiency against other human coronaviruses including SARS-CoV-2. Based on the beta-HCoV-OC43 results, continuous far-UVC exposure in occupied public locations at the current regulatory exposure limit (~3 mJ/cm2/hour) would result in ~90% viral inactivation in ~8 minutes, 95% in ~11 minutes, 99% in ~16 minutes and 99.9% inactivation in ~25 minutes. Thus while staying within current regulatory dose limits, low-dose-rate far-UVC exposure can potentially safely provide a major reduction in the ambient level of airborne coronaviruses in occupied public locations.
Introduction
Coronavirus disease 2019 (COVID-19) was first reported in December 2019 and then characterized as a pandemic by the World Health Organization on March 11, 2020. Despite extensive efforts to contain the spread of the disease, it has spread worldwide with over 5.3 million confirmed cases and over 340,000 confirmed deaths as of May 25, 20201. Transmission of SARS-CoV-2, the beta coronavirus causing COVID-1, is believed to be both through direct contact and airborne routes, and studies of
SARS-CoV-2
stability have shown viability in aerosols for at least 3 hours2. Given the rapid spread of the disease, including through asymptomatic carriers3, it is of clear importance to explore practical mitigation technologies that can inactivate the airborne virus in public locations and thus limit airborne transmission.
Ultraviolet (UV) light exposure is a direct antimicrobial approach4 and its effectiveness against different strains of airborne viruses has long been established5. The most commonly employed type of UV light for germicidal applications is a low pressure mercury-vapor arc lamp, emitting around 254 nm; more recently xenon lamp technology has been used, which emits broad UV spectrum6. However, while these lamps can be used to disinfect unoccupied spaces, direct exposure to conventional germicidal UV lamps in occupied public spaces is not possible since direct exposure to these germicidal lamp wavelengths can be a health hazard, both to the skin and eye7,8,9,10.
By contrast far-UVC light (207 to 222 nm) has been shown to be as efficient as conventional germicidal UV light in killing microorganisms11, but studies to date12,13,14,15 suggest that these wavelengths do not cause the human health issues associated with direct exposure to conventional germicidal UV light. In short (see below) the reason is that far-UVC light has a range in biological materials of less than a few micrometers, and thus it cannot reach living human cells in the skin or eyes, being absorbed in the skin stratum corneum or the ocular tear layer. But because viruses (and bacteria) are extremely small, far-UVC light can still penetrate and kill them. Thus far-UVC light potentially has about the same highly effective germicidal properties of UV light, but without the associated human health risks12,13,14,15. Several groups have thus proposed that far-UVC light (207 or 222 nm), which can be generated using inexpensive excimer lamps, is a potential safe and efficient anti-microbial technology12,13,14,15,16,17,18 which can be deployed in occupied public locations.
The biophysically-based mechanistic basis to this far-UVC approach12 is that light in this wavelength range has a very limited penetration depth. Specifically, far-UVC light (207–222 nm) is very strongly absorbed by proteins through the peptide bond, and other biomolecules19,20, so its ability to penetrate biological materials is very limited compared with, for example, 254 nm (or higher) conventional germicidal UV light21,22. This limited penetration is still much larger than the size of viruses and bacteria, so far-UVC light is as efficient in killing these pathogens as conventional germicidal UV light12,13,14. However, unlike germicidal UV light, far-UVC light cannot penetrate either the human stratum corneum (the outer dead-cell skin layer), nor the ocular tear layer, nor even the cytoplasm of individual human cells. Thus, far-UVC light cannot reach or damage living cells in the human skin or the human eye, in contrast to the conventional germicidal UV light which can reach these sensitive cells7,8,9,10.
In summary far-UVC light is anticipated to have about the same anti-microbial properties as conventional germicidal UV light, but without producing the corresponding health effects. Should this be the case, far-UVC light has the potential to be used in occupied public settings to prevent the airborne person-to-person transmission of pathogens such as coronaviruses.
We have previously shown that a very small dose (2 mJ/cm2) of far-UVC light at 222 nm was highly efficient in inactivating aerosolized H1N1 influenza virus23. In this work we explore the efficacy of 222 nm light against two airborne human coronaviruses: alpha HCoV-229E and beta HCoV-OC43. Both were isolated over 50 years ago and are endemic to the human population, causing 15–30% of respiratory tract infections each year24. Like SARS-CoV-2, the HCoV-OC43 virus is from the beta genus25.

Here we measured the efficiency with which far-UVC light inactivates these two human coronaviruses when exposed in aerosol droplets of sizes similar to those generated during sneezing and coughing26. As all coronaviruses have comparable physical and genomic size, a critical determinant of radiation response27, we hypothesized that both viruses would respond similarly to far-UVC light, and indeed that all coronaviruses will respond similarly.
Results
Inactivation of human coronaviruses after exposure to 222 nm light in aerosols infectivity assay
We used a standard approach to measure viral inactivation, assaying coronavirus infectivity in human host cells (normal lung cells), in this case after exposure in aerosols to different doses of far-UVC light. We quantified virus infectivity with the 50% tissue culture infectious dose TCID50 assay28, and estimated the corresponding plaque forming units (PFU)/ml using the conversion PFU/ml = 0.7 TCID50 29. Figure 1 shows the fractional survival of aerosolized coronaviruses HCoV-229E and HCoV-OC43 expressed as PFUUV/PFUcontrols as a function of the incident 222-nm dose. Robust linear regression (Table 1) using iterated reweighted least squares30 indicated that the survival of both genera alpha and beta is consistent with a classical exponential UV disinfection model (R2 = 0.86 for HCoV-229E and R2 = 0.78 for HCoV-OC43). For the alpha coronavirus HCoV-229E, the inactivation rate constant (susceptibility rate) was k = 4.1 cm2/mJ (95% confidence intervals (C.I.) 2.5–4.8) which corresponds to an inactivation cross-section (or the dose required to kill 90% of the exposed viruses) of D90 = 0.56 mJ/cm2. Similarly, the susceptibility rate for the beta coronavirus HCoV-OC43 was k = 5.9 cm2/mJ (95% C.I. 3.8–7.1) which corresponds to an inactivation cross section of D90 = 0.39 mJ/cm2.
Coronavirus survival as function of the dose of far-UVC light. Fractional survival, PFUUV / PFUcontrols, is plotted as a function of the 222-nm far-UVC dose. The results are reported as the estimate plaque forming units (PFU)/ml using the conversion PFU/ml = 0.7 TCID50 29 by applying the Poisson distribution. Values are reported as mean ± SEM from multiple experiments (n = 3 alpha HCoV-229E and n = 4 for beta HCoV-OC43); the lines represent the best-fit regressions to equation (1) (see text and Table 1).
Table 1 Linear regression parameters for normalized ln[S] [survival] values (equation 1) as the dependent variable and UV dose (D, mJ/cm2) as the independent variable. k is the UV inactivation rate constant or susceptibility factor (cm2/mJ). The linear regression was performed with the intercept term set to zero representing the definition of 100% relative survival at zero UV dose. The coronavirus inactivation cross section, D90 (the UV dose that inactivates 90% of the exposed virus) was calculated using D90 = − ln[1 − 0.90]/k.Full size table
Viral integration assay
We investigated integration of the coronavirus in human lung host cells, again after exposure in aerosols to different doses of far-UVC light. Figures 2 and 3 show representative fluorescent 10x images of human lung cells MRC-5 and WI-38 incubated, respectively, with HCoV-229E (Fig. 2) and HCoV-OC43 (Fig. 3), which had been exposed in aerosolized form to different far-UVC doses. The viral solution was collected from the BioSampler after running through the aerosol chamber while being exposed to 0, 0.5, 1 or 2 mJ/cm2 of 222-nm light. Cells were incubated with the exposed virus for one hour, the medium was replaced with fresh infection medium, and immunofluorescence was performed 24 hours later. We assessed the human cell lines for expression of the viral spike glycoprotein, whose functional subunit S2 is highly conserved among coronaviruses31,32. In Figs. 2 and 3, green fluorescence (Alexa Fluor-488 used as secondary antibody against anti-human coronavirus spike glycoprotein antibody) qualitatively indicates infection of cells with live virus, while the nuclei were counterstained with DAPI appearing as blue fluorescence. For both alpha HCoV-229E and beta HCoV-OC43, exposure to 222-nm light reduced the expression of the viral spike glycoprotein as indicated by a reduction in green fluorescence.
Infection of human lung cells from irradiated aerosolized alpha HCoV-229E as function of dose of far-UVC light. Representative fluorescent images of MRC-5 normal human lung fibroblasts infected with human alphacoronavirus 229E exposed in aerosolized form. The viral solution was collected from the BioSampler after running through the aerosol chamber while being exposed to (a) 0, (b) 0.5, (c) 1 or (d) 2 mJ/cm2 of 222-nm light. Green fluorescence qualitatively indicates infected cells (Green = Alexa Fluor-488 used as secondary antibody against anti-human coronavirus spike glycoprotein antibody; Blue = nuclear stain DAPI). Images were acquired with a 10× objective; the scale bar applies to all the panels in the figure.
Infection of human lung cells from irradiated aerosolized beta HCoV-OC43 as function of dose of far-UVC light. Representative fluorescent images of WI-38 normal human lung fibroblasts infected with human betacoronavirus OC43 exposed in aerosolized form. The viral solution was collected from the BioSampler after running through the aerosol chamber while being exposed to (a) 0, (b) 0.5, (c) 1 or (d) 2 mJ/cm2 of 222-nm light. Green fluorescence qualitatively indicates infected cells (Green = Alexa Fluor-488 used as secondary antibody against anti-human coronavirus spike glycoprotein antibody; Blue = nuclear stain DAPI). Images were acquired with a 10× objective; the scale bar applies to all the panels in the figure.
Discussion
The severity of the 2020 COVID-19 pandemic warrants the rapid development and deployment of effective countermeasures to reduce indoor person-to-person transmission. We have developed a promising approach using single-wavelength far-UVC light at 222 nm generated by filtered excimer lamps, which inactivates airborne viruses without inducing biological damage in exposed human cells and tissue11,12,13,14,15,16,17,18. The approach is based on the biophysically-based principle that far-UVC light, because of its very limited penetration in biological materials, can traverse and kill viruses and bacteria which are typically micrometer dimensions or smaller, but it cannot penetrate even the outer dead-cell layers of human skin, nor the outer tear layer on the surface of the human eye12.
In this work we have used an aerosol irradiation chamber to test the efficacy of 222-nm far-UVC light to inactivate two aerosolized human coronaviruses, beta HCoV-OC43 and alpha HCoV-229E. As shown in Fig. 1, inactivation of the two human coronavirus by 222-nm light follows a typical exponential disinfection model, with an inactivation constant for HCoV-229E of k = 4.1 cm2/mJ (95% C.I. 2.5–4.8), and k = 5.9 cm2/mJ (95% C.I. 3.8–7.1) for HCoV-OC43. These values imply that 222 nm UV light doses of only 1.7 mJ/cm2 or 1.2 mJ/cm2 respectively produce 99.9% inactivation (3-log reduction) of aerosolized alpha HCoV-229E or beta HCoV-OC43. A summary of k values and the corresponding D90, D99, and D99.9 values we have obtained for coronaviruses is shown in Table 2, together with our earlier results for aerosolized H1N1 influenza virus23. The relatively small difference in influenza A (H1N1) and human coronaviruses sensitivity to 222-nm light is likely attributable to differences in structure, genome size, and nucleic acid configuration33. It is also important to note that the previous results with H1N1 virus utilized a fluorescent focus assay to assess virus survival23 in contrast to this work which used the TCID50 assay. While both assays are widely used to accurately determine viral infectivity34, the former employs immunofluorescence to detect a specific viral antigen, instead of depending on cytopathic effects as in the TCID50 assay. Because the assays differ in methods and principles, some variance is expected between these two techniques.
Table 2 Estimated k, D99, and D99.9 values for exposure to 222 nm far-UVC light for alphacoronavirus HCoV-229E, betacoronavirus HCoV-OC43, and influenza A (H1N1).
The results suggest that both of the studied coronavirus strains have similar high sensitivity to far-UVC inactivation. Robust linear regression produced overlapping 95% confidence intervals for the inactivation rate constant, k, of 2.5 to 4.8 cm2/mJ and 3.8 to 7.1 cm2/mJ respectively for the 229E and OC43 strains. As all human coronaviruses have similar genomic sizes which is a primary determinant of UV sensitivity27, it is reasonable to expect that far-UVC light will show similar inactivation efficiency against all human coronaviruses, including SARS-CoV-2. The data obtained here are consistent with this hypothesis.
It is useful to compare the performance of far-UVC light with conventional germicidal (peak 254 nm) UVC exposure. We are aware of only one such study35, which used an aerosolized murine beta coronavirus. The study reported a D88 of 0.599 mJ/cm2, which others4 have used to estimate the D90 for the virus with 254 nm light as 0.6 mJ/cm2. This value is similar to those estimated in the current work (see Table 2), suggesting similar inactivation efficiency of 222 nm far-UVC and conventional germicidal 254 nm UVC for aerosolized coronavirus, and providing further support for the suggestion that all coronaviruses have similar sensitivities to UV light.
The sensitivity of the coronaviruses to far-UVC light, together with extensive safety data even at much higher far-UVC exposures12,13,14,15,16,17,18, suggests that it may be feasible and safe to have the lamps providing continuous low-dose far-UVC exposure in public places – potentially reducing the probability of person-to-person transmission of coronavirus as well as other seasonal viruses such as influenza. In fact there is a regulatory limit as to the amount of 222 nm light to which the public can be exposed, which is 23 mJ/cm2 per 8-hour exposure36,37. Based on our results here for the beta HCoV-OC43 coronavirus, continuous far-UVC exposure at this regulatory limit would result in 90% viral inactivation in approximately 8 minutes, 95% viral inactivation in approximately 11 minutes, 99% inactivation in approximately 16 minutes and 99.9% inactivation in approximately 25 minutes. Thus continuous airborne disinfection with far-UVC light at the currently regulatory limit would provide a major reduction in the ambient level of airborne virus in occupied indoor environments.
In conclusion, we have shown that very low doses of far-UVC light efficiently kill airborne human coronaviruses carried by aerosols. A dose as low as 1.2 to 1.7 mJ/cm2 of 222-nm light inactivates 99.9% of the airborne human coronavirus tested from both genera beta and alpha, respectively. As all human coronaviruses have similar genomic size, a key determinant of radiation sensitivity27, it is likely that far-UVC light will show comparable inactivation efficiency against other human coronaviruses, including SARS-CoV-2.
Together with previous safety studies12,13,14,15,16,17,18 and our earlier studies with aerosolized influenza A (H1N1)23, these results suggest the utility of continuous low-dose-rate far-UVC light in occupied indoor public locations such as hospitals, transportation vehicles, restaurants, airports and schools, potentially representing a safe and inexpensive tool to reduce the spread of airborne-mediated viruses. While staying within the current regulatory dose limits, low-dose-rate far-UVC exposure can potentially safely provide a major reduction in the ambient level of airborne coronaviruses including SARS-CoV-2.
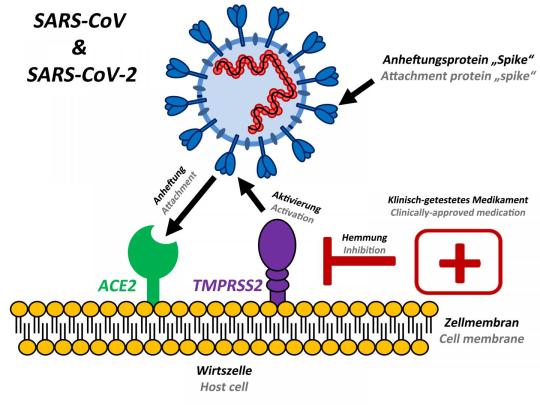
Methods
Viral strains
HCoV-229E (VR-740) and HCoV-OC43 (VR-1558) were propagated in human diploid lung MRC-5 fibroblasts (CCL-171) and WI-38 (CCL-75), respectively (all from ATCC, Manassas, VA). Both human cell lines were grown in MEM supplemented with 10�tal Bovine Serum (FBS), 2 mM L-alanyl-L-glutamine, 100 U/ml penicillin and 100 μg/ml streptomycin (Sigma-Aldrich Corp. St. Louis, MO, USA). The virus infection medium consisted of MEM or RPMI-1640 plus 2% heat inactivated FBS for HCoV-229E and HCoV-OC43, respectively. The viral strains were propagated by inoculation of flasks containing 24-hours old host cells, which were 80–90% confluent. After one hour incubation, the cell monolayer was washed and incubated in fresh infection medium for three or four days at 35 °C for HCoV-229E and at 33 °C for HCoV-OC43. The supernatant containing the working viral stock was then collected by centrifugation (300 g for 15 minutes). The virus titer was determined by 50% tissue culture infective dose TCID50 by assessing cytopathic effects (CPE), which were scored at a bright field microscope (10×) as vacuolization of cytoplasm, cell rounding and sloughing.
Benchtop aerosol irradiation chamber
A one-pass, dynamic aerosol/virus irradiation chamber was used to generate, expose, and collect aerosol samples as previously described23. Viral aerosols were generated by adding a virus solution in a high-output extended aerosol respiratory therapy nebulizer (Westmed, Tucson, AZ) and operating using an air pump with an input flow rate of 11 L/min. Virus flowed into the chamber and was mixed with dry and humidified air to maintain humidity between approximately 50–70%. The relative humidity, temperature, and aerosol particle size distribution were monitored throughout operation. Aerosol was exposed to far-UVC light and finally collected using a BioSampler (SKC Inc., Eighty Four, PA).
The far-UVC lamp was positioned approximately 22 cm away from the UV exposure chamber and directed at the 26 cm × 25.6 cm × 254 μm UV-transmitting plastic window (TOPAS 8007 × 10, TOPAS Advanced Polymers Inc., Florence, KY). Consistent with our previous experiments using this chamber23, the flow rate through the system was 12.5 L/min. The volume of the UV exposure region was 4.2 L so each aerosol was exposed for approximately 20 seconds as it traversed the window. The entire irradiation chamber was contained in a biosafety level 2 cabinet and all air inputs and outputs were equipped with HEPA filters (GE Healthcare Bio-Sciences, Pittsburgh, PA) to prevent unwanted contamination from entering or exiting the system.
Irradiation chamber performance
The custom irradiation chamber simulated the transmission of aerosolized viruses produced via human coughing and breathing. The chamber operated at an average relative humidity of 66% and an average temperature of 24 °C across all runs. The average particle size distribution was 83�tween 0.3 μm and 0.5 μm, 12�tween 0.5 μm and 0.7 μm, and 5% >0.7 μm (Table 3). Aerosolized viruses were efficiently transmitted through the system as evidenced from the control (zero exposure) showing clear virus integration (Figs. 2 and 3, top left panels).
Table 3 Example of particle size distributions from humans during various activities are given26 along with the averaged measured values for this work.Full size table
Far-UVC lamp and dosimetry
The far-UVC source used in this study was a 12 W 222-nm KrCl excimer lamp module made by USHIO America (Item #9101711, Cypress, CA). The lamp is equipped with a proprietary optical filtering window to reduce lamp emissions outside of the 222 nm KrCl emission peak. The lamp was positioned 22 cm away from the exposure chamber window and directed at the center of the window. Optical power measurements were performed using an 818-UV/DB low-power UV enhanced silicon photodetector with an 843-R optical power meter (Newport, Irvine, CA). Dosimetry was performed prior to starting an experiment to measure the fluence within the chamber at the position of the aerosol.
The distance between the lamp and the irradiation chamber permitted a single lamp to uniformly irradiate the entire exposure window area. Measurements using the silicon photodetector indicated an exposure intensity of approximately 90 μW/cm2 across the exposure area. The chamber is equipped with a reflective aluminum surface opposite of the exposure window. As in our previous work with this chamber23, the reflectivity of this surface was approximately 15%. We have therefore conservatively estimated the intensity across the entire exposure area to be 100 μW/cm2. With the lamp positioned 22 cm from the window and given the 20 seconds required for an aerosol particle to traverse the exposure window, we calculated the total exposure dose to a particle to be 2 mJ/cm2. We used additional sheets of UV transmitting plastic windows to uniformly reduce the intensity across the exposure region to create different exposure conditions. While in our previous work with these sheets we measured a transmission closer to 65%23, for these tests we measured the 222-nm transmission of each sheet to be approximately 50%. This decrease in transmission is likely due to the photodegradation of the plastic over time4. The addition of one or two sheets of the plastic covering the exposure window decreases the exposure dose to 1 and 0.5 mJ/cm2, respectively.
Experimental protocol
As previously described23, the virus solution in the nebulizer consisted of 1 ml of Modified Eagle’s Medium (MEM, Life Technologies, Grand Island, NY) containing 107–108 TCID50 of coronavirus, 20 ml of deionized water, and 0.05 ml of Hank’s Balanced Salt Solution with calcium and magnesium (HBSS++). The irradiation chamber was operated with aerosolized virus particles flowing through the chamber and the bypass channel for 5 minutes prior to each sampling, in order to establish the desired RH value. Sample collection was initiated by changing air flow from the bypass channel to the BioSampler using the set of three way valves. The BioSampler was initially filled with 20 ml of HBSS++ to capture the aerosol. During each sampling time, which lasted for 30 minutes, the inside of the irradiation chamber was exposed to 222-nm far-UVC light entering through the plastic window. Variation of the far-UVC dose delivered to aerosol particles was achieved by inserting additional UV-transparent plastic films as described above thereby delivering the three test doses of 0.5, 1.0 and 2.0 mJ/cm2. Zero-dose control studies were conducted with the excimer lamp turned off. After the sampling period was completed the solution from the BioSampler was used for the virus infectivity assays.
Virus infectivity assays
TCID50
We used the 50% tissue culture infectious dose assay to determine virus infectivity28. Briefly, 105 host cells were plated in each well of 96-well plates the day prior the experiment. Cells were washed twice in HBSS++ and serial 1:10 dilutions in infection medium of the exposed virus from the BioSampler was overlaid on cells for two hours. The cells were then washed twice in HBSS++, covered with fresh infection medium, and incubated for three or four days at 34 °C. Cytopathic effects (CPE) were scored at a bright field microscope (10×) as vacuolization of cytoplasm, cell rounding and sloughing. The TCID50 was calculated with the Reed and Muench method28,38. To confirm the CPE scores, the samples were fixed in 100% methanol for five minutes and stained with 0.1% crystal violet. The results are reported as the estimate of plaque forming units (PFU)/ml using the conversion PFU/ml = 0.7 TCID50 by applying the Poisson distribution29.
Immunofluorescence
To assess whether increasing doses of 222-nm light reduced the number of infected cells, we performed a standard fluorescent immunostaining protocol to detect a viral antigen in the host human cells23. Briefly, 2 × 105 host cells (MRC-5 cells for HCoV-229E and WI-38 for HCoV-OC43) were plated in each well of 48-well plates the day prior the experiment. After running through the irradiation chamber for 30 minutes, 150 μl of virus suspension collected from the BioSampler was overlaid on the monolayer of host cells. The cells were incubated with the virus for one hour, then washed three times with HBSS++, and then incubated overnight in fresh infection medium. Infected cells were then fixed in 100% ice cold methanol at 4 °C for 5 minutes and labeled with anti-human coronavirus spike glycoprotein (40021-MM07, Sino Biologicals US Inc., Chesterbrook, PA) 1:200 in HBSS++ containing 1% bovine serum albumin (BSA; Sigma-Aldrich Corp. St. Louis, MO, USA) at room temperature for one hour with gentle shaking. Cells were washed three times in HBSS++ and labeled with goat anti-mouse Alexa Fluor-488 (Life Technologies, Grand Island, NY) 1:800 in HBSS++ containing 1% BSA, at room temperature for 30 minutes in the dark with gentle shaking. Following three washes in HBSS++, the cells were stained with Vectashield containing DAPI (4′,6-diamidino-2-phenylindole) (Vector Laboratories, Burlingame, CA) and observed with the 10× objective of an Olympus IX70 fluorescent microscope equipped with a Photometrics PVCAM high-resolution, high-efficiency digital camera and Image-Pro Plus 6.0 software (Media Cybernetics, Bethesda, MD). For each 222-nm dose and virus genus, the representative results were repeated twice. For each sample, up to ten fields of view of merged DAPI and Alexa Fluor-488 images were acquired.
Data analysis
The surviving fraction (S) of the virus was calculated by dividing the fraction PFU/ml at each UV dose (PFUUV) by the fraction at zero dose (PFUcontrols): S = PFUUV/PFUcontrols. Survival values were calculated for each repeat experiment and natural log (ln) transformed to bring the error distribution closer to normal39. Robust linear regression using iterated re-weighted least squares (IWLS)40,41 was performed in R 3.6.2 software using these normalized ln[S] values as the dependent variable and UV dose (D, mJ/cm2) as the independent variable. Using this approach, the virus survival [S] was described by first-order kinetics according to the equation4:
ln[S]=−k×D" role="presentation" style="box-sizing: inherit; line-height: normal; word-spacing: normal; overflow-wrap: normal; white-space: nowrap; float: none; direction: ltr; max-width: 100%; max-height: none; min-width: 0px; min-height: 0px; border: 0px; padding: 0px; margin: 0px; overflow: auto hidden; position: relative; display: block !important;">ln[S]=−k×Dln[S]=−k×D(1)
where k is the UV inactivation rate constant or susceptibility factor (cm2/mJ). The regression was performed with the intercept term set to zero representing the definition of 100% relative survival at zero UV dose, separately for each studied virus strain. The data at zero dose, which by definition represent ln[S] = 0, were not included in the regression. Uncertainties (95% confidence intervals, CI) for the k parameter for each virus strain were estimated by bootstrapping for each regression method because bootstrapping may result in more realistic uncertainty estimates, compared with the standard analytic approximation based on asymptotic normality, in small data sets such as those used here (n = 3 HCoV-229E and n = 4 for HCoV-OC43). Goodness of fit was assessed by coefficient of determination (R2). Analysis of residuals for autocorrelation and for heteroskedasticity was performed using the Durbin-Watson test42 and Breusch-Pagan test (implemented by lmtest R package)43, respectively. Parameter estimates (k) for each virus strain were compared with each other based on the 95% CIs and directly by t-test, using the sample sizes, k values, and their standard errors. The virus inactivation cross section, D90, which is the UV dose that inactivates 90% of the exposed virus, was calculated as D90 = − ln[1 − 0.90]/k. Other D values were calculated similarly.
1 note
·
View note
Quote
現在も猛威をふるっているCOVID-19(SARS-CoV-2)感染症ですが、実は過去にもヒトコロナウィルスによる世界的パンデミックが起こっていた可能性があります。その一つが1889年から流行して世界中で100万人以上が死亡したと言われている感染症の大流行です。インフルエンザH3N8の流行とされていますが、重症者に認められた神経症状がHCoV-OC43(ベータコロナウィルス属Human coronavirus-OC43の略)の症状に酷似していたのと(HCoV-OC43は神経毒性が強いと言われています)、その後の分子時計の解析でHCoV-OC43がウシコロナウィルスから分岐したのが1890年前後とされてから、このパンデミックはインフルエンザではなく、新型コロナウィルス感染症と言う説が有力となっています。(但し分子時計の解析は塩基変化速度がどの生物でも一定である事が前提です)。この感染症は1889年5月ロシア帝国ブラハに突如出現し、半年ほどで世界中へ広がりました。残っている当時の記録から推定された致死率は、1889年の第1波が約4%、1892年の第2波が約3.3%で、高齢者ほど致死率が高かったのが特徴です。その後人類はこのウィルスに対する免疫を獲得し、現在は普通の感冒のウィルスとなりました。
診療ノート|塩筑医師会 - #60 新型コロナウィルスは繰り返す
2 notes
·
View notes
Last Seen Blogs

cobrrastyle
ʙᴏᴏ! ɢʜᴏꜱᴛ!

steviestacey
Becoming Her

jjpot02
fan's Deltarune

phisnom
phil

depression-storage
Hwangjjun07