
mentalhealthinformation-blog
Mental health awareness
This is a blog about mental illnesses/neurodivergence information. I work with the DSM-5 mostly but also with my own knowledge from other sources, esp regarding my own disabilities.
I am not a professional.
Mobile links
49 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

cyberarcaderuins
Untitled

iwasdrizzleandhewasahurricane
Oh Hello There...

hindooo
🪸

el-soup
soup

frauleinsmaria
eyes full of stars
Note
je sais pas si tu tiens encore le blog mais flight of the mind est dispo en pdf sur google dans les premiers resultats, c un commentaire tres interessant et documente de la vie de virginia woolf a la lumiere de son trouble bipolaire, ca parle de comment elle a composé avec sa maladie + ses difficultes a comprendre qui elle est en dehors de sa maladie, sa famille..
Merci, je tiens encore le blog j’ai juste très peu d’énergie et du coup je fais rarement des posts. Je te remercie de me le dire mais ce n’est pas vraiment le genre de choses que je poste (je suis plus axé sur des informations factuelles sur les diagnostics et les traitements, comme par exemple les critères diagnostiques ou quelle classe de médicaments est utilisée pour traiter quel trouble). Ceci étant dit je regarderai peut-être pour moi même parce que ça a l’air intéressant
0 notes
Text
Second-generation antipsychotics
Second-generation antipsychotics (also called atypical antipsychotics) are more commonly used than their first generation counterparts as they usually have less side effects such as extrapyramidal syndrome, tardive dyskinesia. However, they also have significant side effects. For example Clozapine, very efficient in treating treatment-resistant schizophrenia, can cause a massive decrease in white blood cells (agranulocytosis)
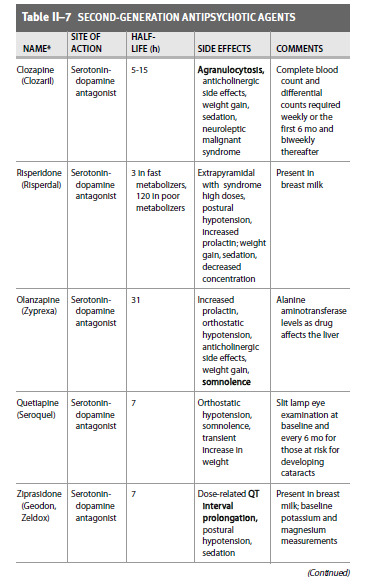
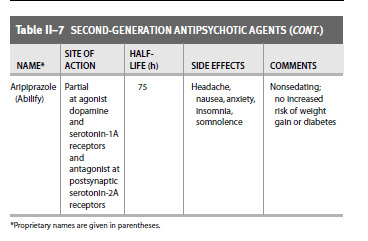
From Case Files : Psychiatry, third edition by Eugene Toy and Debra Klamen
Link to main post
1 note
·
View note
Text
First-generation antipsychotics
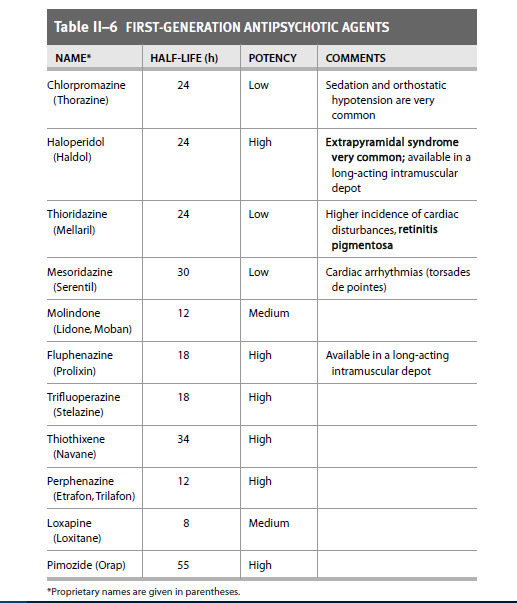
From Case Files : Psychiatry, third edition, Eugene Toy and Debra Klamen
Link to main post
0 notes
Text
Antipsychotics
Antipsychotics are, as their name indicates, mostly used to treat most psychotic symptoms.
They are also used to treat manic symptoms, anxiety, can be used as sedatives, and some (such as olanzapine and aripirazole) are even used to treat depressive symptoms.
They're divided into generations : first generation and second generation are the ones I will talk about here, but a third generation seems to be coming.
These two posts are mostly lists of antipsychotics, with a few additional informations.
1. First-generation antipsychotics
2. Second-generation antipsychotics
0 notes
Text
While I'm still not well enough to write proper articles, I was thinking I could add specific FAQs for certain disorders or disabilities to the blog. Any idea about the questions I could answer there? I was thinking of the easiest possible answers to questions such as "what's the difference between depersonalization and derealization?" (I would answer something along the lines of "generally speaking, derealization is when an individual feels disconnected from the outside world or as if they were in a dream whereas in depersonalization, one feels disconnected from their own self" and when I've made the articles I must make about this, insert a link to those articles in the answer) Any thoughts at all?
0 notes
Text
I apologize for the lack of new posts. My mental health makes it impossible for me to focus or work on anything, but I'm not giving up on this blog. Ill keep trying to answer your questions, and will write new posts whenever I get better.
0 notes
Note
What's the difference between schizoaffective disorder and co-morbid schizophrenia and a mood disorder?
It’s a difficult one to explain, I hope to be clear!On the overall duration of the illness, in schizophrenia comorbid with a mood disorder, the time spent showing only the symptoms of schizophrenia and no mood symptoms is longer than the time spent in mood episodes. The mood episodes don’t take up as much time as they do in schizoaffective disorder.
In schizoaffective disorder, mood episodes are more present. If any clarification is needed, please let me know! I’ll do my best.
1 note
·
View note
Note
yes, I meant OSDD! sorry
I still don’t understand, can you write full words please? I’m sorryAlso if you do mean “Other specified dissociative disorder” there is no specific criteria other than“This category applies to presentations in which symptoms characteristic of a dissociative disorder that cause clinically significant distress or impairment in social, occupational, or other important areas of functioning predominate but do not meet the full criteria for any of the disorders in the dissociative disorders diagnostic class. The other specified dissociative disorder category is used in situations in which the clinician chooses to communicate the specific reason that the presentation does not meet the criteria for any specific dissociative disorder.”So it would not make much sense to make a post about it without making posts about other specific dissociative disorders beforehand. I hope I’m making sense.
0 notes
Note
Could I request the criteria and for OSDD-1B?
Hi ! I am very sorry, I fail to see which criteria you’re talking about. You can of course ask again with other words and I will do my best!(I was only able to think of Other Specified Dissociative Disorder but I really have no idea what the “1B” could be in that case. I am sorry)
1 note
·
View note
Note
Do you know what the difference between mild and. not mild disorganized speech/thinking would be?
I would say this has to do with the impairment that the disorganization causes.
For example, I think that if a person has a mildly disorganized speech or thinking, they can still be understandable to the people they’re trying to communicate with, while if someone has severe disorganized speech/thinking, people around them might not be able to understand what they’re saying.
I hope this answers your question!
3 notes
·
View notes
Text
Autism masterpost
Autism is a developmental disability. In the DSM 5, it is called Autism spectrum disorder. This disability used to be separated in different categories, such as Asperger's syndrome, autism, and atypical autism (there were others, but I will not list them here). These categories do not exist anymore and have all been put together under the label 'autism spectrum disorder', although some mental health professionals still use diagnoses such as Asperger's syndrome.
Its criteria consists of deficits in communication and social interactions, having few intense interests, changes in sensory sensitivity, repetitive motor movements and patterns of speech (stimming) and inflexible adherence to routines.
Autism is present in the early developmental period and always remains present throughout one's life, but may become fully manifest only when social demands exceed the autistic person's capacities, and may be masked by learned strategies later in life.
1. Clarifications
2. DSM criteria
4 notes
·
View notes
Text
Autism, part 2 : DSM criteria
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (example are illustrative, not exhaustive) :
Deficits in social-emotional reciprocity, ranging, for example, from unusual social approach and failure of usual back-and-forth conversation ; to reduced sharing of interests, emotions, or affect ; to failure to initiate or respond to sical interactions.
Deficits in non-verbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and non-verbal communication ; to unusual eye contact and body language or deficits in understanding and use of gestures, to a total lack of facial expressions and non-verbal communication.
Deficits in developing, maintaining and understanding relationships, ranging for example, from difficulties adjusting behavior to suit various social contexts ; to difficulty in sharing imaginative play or in making friends ; to absence of interest in peers.
Restricted, repetitive patterns of behavior, interests, or activties, as manifested by at least two of the following, currently or by history (example are illustrative, not exhaustive) :
Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys of flipping objects, echolalia).
Highly restricted, fixated interets that are unusual in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
Traits must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
Traits cause clinically significant impairment in social, occupational or other important areas of current functioning.
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism frequently co-occur ; to make comorbid diagnoses of autism and intellectual disability, social communication should be below that expected for general developmental level.
Link to masterpost
2 notes
·
View notes
Text
Autism, part 1 : Clarifications
Autism is officially regarded as a disorder, but the autistic community does not think of it as such, and it is why the posts this blog will contain about autism will always call it nothing but a developmental disability or a neurodivergence. Any uncritical use of the word 'disorder' when talking about autism on this blog will be a mistake caused by inadvertently copying the texts I read to make these posts, a mistake I will be quick to fix when asked.
Additionally, I am against a cure for autism. Searching for it is only ever detrimental to the autistic community, and most autistic people do not wish to be cured, including the people most would call 'low-functionning'. Autism is so deeply ingrained in autistic people's functioning that it is often a fundamental part of who we are. And in our society there is no way that a cure would only be given to the people who want it – it would be forced on non-verbal people and children, at 'best' (it could be forced on anyone really). I think autism should be accommodated. Not cured.
Lastly, I am against the use of functioning labels (basically calling people either 'low-functioning' or 'high-functioning' based on their abilities). They're harmful, outdated (the DSM-5 doesn't use them anymore), and they do not depict autistic people's situations accurately in the least.
Autism is a much wider spectrum of experiences than the DSM or any criteria could show, as are most of the illnesses and disabilities I talk about in this blog, and I do not think I can address every autistic trait there is. Here is an alternative criteria for autism made by autistics. I will use only the DSM's though because it's what I know best.
Link to masterpost
3 notes
·
View notes
Note
do delusions count as delusions if you know they're not real but believe them anyway? e.g. you think people are watching you and a logical part of you says 'no why would they do that' but you still shut the curtains because you still believe it.
Hi! Not everyone agrees on that. Some say these aren’t delusions, but my personal opinion is that if a false belief is strong enough to affect your life or cause any kind of distress, even if a part of you says it isn’t real, you are free to call it a delusion.Also - once you realize you’re psychotic, it becomes hard to trust your perceptions, thoughts, and beliefs, and it is not uncommon among psychotic people to question their beliefs, and sometimes, yes, they find out that their delusions are indeed delusions, yet remain unable to get rid of them completely, or keep on acting on them.
I hope that’s clear enough!
6 notes
·
View notes
Text
Social anxiety masterpost
People with social anxiety (called social anxiety disorder in the DSM-5, but also called social phobia) have an intense fear of social settings in which others may watch, study or judge them. This can involve public speaking, meeting new people, eating with others, using public restrooms...
They fear they may offend others, be embarassed, or looked down upon. They have an intense concern that others will reject them or not like them. The degree of fear exceeds the real risk or result of any such negative judgments.
Because of these intense fears, people with social anxiety often avoid social situations.
The average age for symptoms to appear is 13. Social anxiety often occurs in people who are shy, or have endured a stressful or embarassing event, or have been bullied. This disorder can also have its symptoms building up over time, starting very slowly. It occurs less frequently in adults.
Risk factors
People who often withdraw from/avoid unknown settings are more at risk
Childhood abuse, neglect, or other adverse life events
People with a first-degree relative (parent or sibling) with social anxiety are two to six times more likely to also have the disorder.
1. Criteria
2. Not to be confused with
3. Treatments
9 notes
·
View notes
Text
Social anxiety, part 3 : Treatment
Therapies : cognitive behavioral therapy can be helpful. Typically desensitization is used against social anxiety.
Medications : SSRIs (selective serotonin-reuptake inhibitors) and SNRIs (serotonin-norepinephrine) are two kinds of antidepressants that may help with social anxiety (and many other anxiety disorders). Since they may take a few weeks to start being effective, on the short term, one could be prescribed beta-blockers or benzodiazepines.
Link to masterpost
3 notes
·
View notes
Text
Social anxiety part 2, Not to be confused with
Shyness
Shyness is a common personality trait and is not, in itself, pathological. However, when there is a significant adverse impact on social, occupational, and/or other important areas of functioning, a diagnosis of social anxiety should be considered, and when full diagnostic criteria for social anxiety disorder are met, the disorder should be diagnosed.
Agoraphobia
Individuals with agoraphobia may fear and avoid social situations because escape might be difficult or help might not be available in the event of any panic symptoms, whereas individuals with social anxiety are mostly fearful of other's reactions and thoughts on them.
Panic disorder
Individuals with social anxiety may have panic attacks, but the concern is about fear of negative evaluation, whereas in panic disorder the concern is about the panic attacks themselves.
Separation anxiety disorder
Individuals with separation anxiety disorder may avoid social settings because they are scared to be separated from attachment figures. These individuals are usually comfortable in social settings when their attachment figure is present.
Specific phobias
Individuals with specific phobias may fear embarassment or humiliation regarding their reactions when faced with the object of their phobia, but usually do not fear negative evaluation in other social situations.
Major depressive disorder
Individuals with major depressive disorder may be concerned about being negatively by others because they feel they are bad or not worthy. In contrast, individuals with social anxiety disorder are usually worried about being negatively evaluated because of certain social behaviors or physical symptoms.
Body dysmorphic disorder
Individuals with body dysmorphic disorder are preoccupied with one or more perceived defects or flaws in their physical appearance, and this preoccupation often causes social anxiety and avoidance. If their social fears and avoidance are caused only by their beliefs about their appearance, a spearate diagnosis of social anxiety is not needed.
Delusional disorder
Individuals with delusional disorder may have delusions that seem possible, focusing on being rejected or offending others. The difference is that individuals with social anxiety are not convinced to have offended others, or to have been rejected by them.
Link to masterpost
5 notes
·
View notes