#us clinical trials database
Text
Most Common Clinical Trial Therapy Areas
2023 Top Clinical Trial Areas
Clinical trials are a fundamental part of the medical research process. They help determine the safety and effectiveness of new treatment approaches, contributing to advancements in the medical field. With an ever-growing number of clinical trials conducted worldwide each year, it's essential to identify the most impactful and relevant therapy areas being researched. This article will discuss the top five clinical trial areas that have taken center stage in 2023. We will cover the prevalence of these clinical trials, funding, and expected outcomes for each therapy area, as well as the future of clinical trials in 2023.
1. Oncology: Leading the Charge in Clinical Trials
Cancer is among the leading causes of death globally, and the need for innovative therapies has never been higher. In 2023, the oncology domain is still the most common area in clinical trial research, representing nearly 50% of clinical trials worldwide. The United States bears the majority of these trials, boasting over 25,000 active studies in oncology alone. Europe is a close second, with multiple countries working together to fund and conduct innovative cancer research.
Government agencies, pharmaceutical companies, and non-profit organizations have invested billions of dollars into cancer research. In 2023, the National Cancer Institute (NCI) in the United States received more than $6.5 billion in funding for cancer research. Many prominent clinical trials this year target hard-to-treat cancers, such as lung, breast, and pancreatic cancer, with a focus on immunotherapy, targeted therapies, and cellular therapies. The future of oncology research is bright, as advancements in technology and global collaboration continue to push the boundaries of cancer treatment.
2. Neurology: Addressing the Growing Burden of Neurological Disorders
Neurological disorders, including Alzheimer's disease, Parkinson's disease, and multiple sclerosis, affect millions of people worldwide. With the growing prevalence of these disorders, neurology has emerged as a leading area in clinical trial research. The United States leads the world in neurological clinical trials, followed closely by Europe and Asia.
Global funding for neurological clinical trials reached new heights in 2023, with a focus on addressing neurodegenerative conditions like Alzheimer's and Parkinson's. Public and private sectors invested heavily in this research, with organizations like the National Institutes of Health (NIH) allocating over $3 billion to neurological clinical trials in 2023. The outcomes of these trials aim to slow down, prevent, or cure neurological diseases, and hope to improve overall quality of life for affected individuals.
3. Infectious Diseases: Tackling Emerging and Reemerging Pathogens
The COVID-19 pandemic has underscored the importance of research and preparedness in combating infectious diseases. In response to this global challenge, the field has seen significant growth in clinical trials focused on infectious diseases. Research funding for these trials has boasted increased support worldwide, with both public and private sectors contributing to the development of novel vaccines and treatments.
In 2023, clinical trials in infectious diseases tackled novel pathogens, as well as reemerged diseases like tuberculosis and malaria. The World Health Organization (WHO) played a significant role in funding and initiating these trials, collaborating with governments and pharmaceutical companies to ensure rapid response and treatment development. The outcomes of these trials will contribute to global health security and preparedness for future pandemics and disease outbreaks.
4. Cardiology: Addressing the Global Burden of Cardiovascular Disease
Cardiovascular disease (CVD) is a leading cause of death worldwide, with almost 18 million annual fatalities. In 2023, cardiology clinical trials aimed to improve prevention, diagnosis, and treatment of CVD, encompassing areas such as heart failure, coronary artery disease, and hypertension.
Globally, funding for cardiology research came from government agencies, non-profit organizations, and pharmaceutical companies. The United States, Europe, and several Asian countries allocated substantial resources to support these clinical trials. The anticipated outcomes of these trials will emphasize personalized and precision medicine approaches in cardiovascular healthcare and ultimately reduce the burden of CVD around the world.
5. Rare Diseases: Advancing Treatment for Orphan Disorders
In recent years, the focus on rare diseases has grown significantly, resulting in more clinical trials aimed at developing treatments for orphan disorders affecting less than 200,000 individuals in the United States. Developing therapies for rare diseases is often financially challenging due to the small patient populations. However, regulatory incentives and growing public awareness have resulted in an increase in funding and clinical trials in this area.
Rare disease clinical trials are prevalent in both the United States and Europe, with a focus on gene therapy, enzyme replacement therapy, and targeted treatments. Public health agencies
Oncology: One of the most common clinical trials by therapy area is oncology, which involves testing medications and treatments with the goal of helping to improve patient outcomes when dealing with various types of cancer. Examples of these clinical trials include those that seek to determine the efficacy of new drugs in treating particular forms of cancer, or researching novel therapeutic approaches such as immunotherapy.
Cardiovascular Disease: Clinical trials related to cardiovascular disease are also quite common. These tests may involve assessing the effectiveness of new medications that can help lower blood pressure or improve cardiac function, as well as examining lifestyle interventions such as diet and exercise for their potential to reduce risk factors associated with heart disease.
Diabetes: Clinical trials related to diabetes are also a frequent occurrence due to its prevalence in many parts of the world. These studies often aim to understand how better management strategies for diabetes can improve quality of life for patients and reduce long-term complications associated with this condition.
Neurology: Clinical trials pertaining to neurology are commonplace in research settings because there is still much unknown about how the brain and nervous system work, as well as treatment effectiveness for conditions like epilepsy, Parkinson’s disease, multiple sclerosis, and stroke recovery.
Mental Health: Mental health-related clinical trials are becoming increasingly more common as researchers continue to investigate and develop better treatments for depression, anxiety disorders, bipolar disorder, schizophrenia, PTSD, addiction and other issues related to mental health and wellbeing.
Respiratory Disease: Clinical trials involving respiratory diseases, such as asthma or chronic obstructive pulmonary disease (COPD), have become more commonplace in recent years due to their rising prevalence throughout the world; they typically involve testing new medications or therapies that can help manage symptoms and reduce exacerbations associated with these conditions.
Immunology: Immunology-focused clinical research has become more popular over recent years due to its potential implications for developing treatments for autoimmune diseases like rheumatoid arthritis or lupus; these clinical trials often involve testing existing medications or creating new ones from scratch in order to achieve desired results regarding immune system regulation within individuals living with autoimmune conditions .
Gastroenterology: Gastroenterological clinical research is commonplace due primarily to its relevance within digestive disorders such as Crohn’s Disease or Irritable Bowel Syndrome (IBS). Research conducted in this area generally seeks to gain an understanding into how certain dietary changes or drug treatments might be effective at managing symptoms associated with gastrointestinal problems while reducing side effects associated with traditional pharmacological approaches .
Endocrinology: Endocrinological clinical research is yet another form of study found in medical circles due primarily via its relevance within hormone-related issues such as diabetes mellitus type 1 & 2; this type of study typically involves testing ways in which different hormones might interact differently between individuals who have similar conditions but don't respond positively/negatively the same way when it comes to traditional forms of treatment .
Ophthalmology: Last but not least is ophthalmology which looks at vision disorders like glaucoma and age related macular degeneration (AMD); here researchers test existing medications/treatments looking for improvement when it comes both short term relief from eye pain/blurring but also long term protection against further loss/damage occurring over time via regular monitoring sessions
Learn more about clinical trials and become involved in management of clinical trials through further training with CCRPS.
#Keyword#recent clinical trials#clinical trials news#latest clinical trials#trials update#trilas#available clinical trials#clinical research news#clinical research trial#clinical trial news#clinical trials today#new clinical trials#new medical trials#ongoing clinical trials#trial website#us clinical trials database#available trials#cancer clinical trials database#clinical gov trials#clinical research and trials#clinical research newsletter#clinical search#clinical studies gov#clinical study gov#clinical study search#clinical trial data#clinical trial database#clinical trial finder#clinical trial search#clinical trial support
0 notes
Text
Some HSR Thirsts
Because I've been fucking star-railed this last week and also I promised @dustofthedailylife that I would write a svarog thirst if she finally pulled welt. so since this exists, you can guess what happened!
Svarog/Yaoshi/Kafka x Reader
NSFW, nothing explicit perse but all very heavily implied, Robot/monsterfucking, does fucking a god cound as monsterfucking?, Svarog is a giant vibrator, Yaoshi and their many hands, also Yaoshi having an aphrodesiac venom in their scorpion tail, maybe a little implied dubcon in kafkas case? I dont...think it is but its there as a warning in case.

Ok but Svarog, who definitely knows what sex is, of course he does, he has an entire database to access, and lets face it, this man has probably already accessed it when looking up ‘how to parent’ information because at one point or another he’s going to have to give clara ‘the talk’
(no, we wont talk about how his version of the talk is going to be the most embarrassingly clinical talk ever to exist. rest in peace clara.)
But he does not, for the love of anything, understand why you want to have sex…with him.
Nonetheless, he does not stop your hands roaming his chest plates, he doesn’t really stop you from doing… anything really, because… whatever this is makes you happy, and that’s all he wants.
He’s confused when you ask him to touch you, but he does it anyway, all while sifting through his databanks to figure out both why and where.
This is also the day you discover that Svarog has an… interesting vibration function in his hands that he claims was once for easing stiff muscles of his old human commanders before he was abandoned.
Yeah it’ll sure ease you alright.
Admittedly…he does like watching you squirm…it does… something to his servos.
Though, he thinks he may have created a monster, because now every day, without fail…you’re asking him for a hand.
Perhaps one day, when he has done enough research…he might just reveal that one…extra modification that had been made to him before everything went to shit.
One day he will allow you to delve below his trousers and maybe one day he will use that…modification, to finally give you what you want, since it seems you’re unwilling to find another mortal to fornicate with.
Besides
perhaps …clara could do with a mother figure around.
----------
Some say the Aeon Yaoshi, of the Abundance, is a cruel and evil creature.
This does not stop you from seeking Their favour.
However when they finally do appear before you, you get so much more.
Six hands, long and delicate, trailing your skin as they pull you close, unearthly voice whispering in your ear, telling you they’ve heard every prayer, every plead and call for them; how they’ve been watching you all this time, and now they have come to bestow the blessing you’ve been seeking.
But only if you can endure one last trial.
In some depictions you had found, Yaoshi is endowed with a scorpion's tail, so it isn’t a shock when the appendage curls around your body, the tip pricking into your thigh. You feel the warmth of the poison spread through your body and you moan for it. Yaoshi only hums their praise
Their venom makes you feel warm and fuzzy, it makes their touch intense and vivid, most of all…
it makes you want to give yourself over entirely
You feel hands touch places that have never been touched by another, you feel their teeth and their tongue. You hear their praises.
And then you wake, in your bed.
At first, you think it was a dream, but then you sit up.
You were naked, your muscles ached, but it was a sweet ache, soft around the edges, and there on your thigh, where they had stung you with their venom…
the symbol of abundance
----------
Soft hands, and an even softer voice, leave you weak in the knees.
“Ready to talk yet?” Kafka muses quietly as she presses a single finger to your collarbone, and you immediately fall back against the table, your arms still bound behind your back.
You should be struggling. You should be fighting back.
But you’d be lying if you said you weren’t incredibly turned on by the stellaron hunter who had kidnapped you, and was now apparently intent on interrogating you.
“You’ll….have to try harder than that.” you rasp, trying to sound intimidating.
By the way Kafka’s smile widens ever so slightly, it’s failed completely, and you’re once again left reeling as she approaches, leaning over you like a cat who’s just caught their mouse.
“Will I?” her voice is so soft, and yet so very dangerous as her ruby eyes narrow in on your face “My…are we a little smitten? Your face is all red.”
Goddamn it.
“I’d never-”
“Oh don’t be so dramatic.” She interjects as she perches on the edge of the table beside where you lay, she shoots you a look…an expression you can’t quite discern for a moment, until you realise her own eyes are raking down your body.
hungrily.
You watch her bring her hand to her mouth, teeth closing around the finger of her glove before pulling the offending article off; your heart is jackrabbiting in your chest.
“I think…” she hums as she leans back over you, magenta hair falling between you both like a waterfall. This was dangerous, so very dangerous.
But the moment her hand presses against your belly, and slowly begins its slow gaze downward, pressing shamelessly beneath the waistband of your bottoms? You’re a goner.
“I think I have other ways to make you sing that we’ll both enjoy…don't you think?”
Taglist: @stygianoir @meimeimeirin @ainescribe @dustofthedailylife @rjssierjrie @crystalflygeo @angel-of-requiem @asoulsreverie @zomzomb1e
Want to be added to the list? shoot me an ask~
I will be starting a Starrail specific taglist shortly so if you want in on that let me know!
#silentmothwrites#Moth got star railed#Svarog Star rail#Yaoshi Star rail#Kafka Star rail#Svarog x reader#Yaoshi x reader#Kafka x reader#Svarog smut#yaoshi smut#kafka smut
1K notes
·
View notes
Text
I get really frustrated sometimes by the communication divide on my team, where two of my coworkers are regularly unresponsive for days or weeks, versus me and one of the junior analysts responding to most things within hours and at worst, an "I saw this and I'll get back to you" within a couple days. Then I have to remember that our manager, when she was here, never enforced a higher expectation, so how can I? Also, the two of us who are quick responders both came from working in clinical trials, and sometimes I think maybe, it's the tiniest bit possible that working in a cutthroat industry skewed my perspective a little. Manager used to say that a lot, like I'd express being stressed about not meeting a self-imposed deadline and she'd probe gently, "Hmm, were there pretty strong consequences to that in your last job?" (Lmaooo girl if you only knew! I was there nine months, a bitty baby project assistant, and fielding anxious phone calls from senior pharma execs; the one year mark was the start of scoping out good crying spots in the office, after a client screamed at my team for missing a deadline by under 12 hours. Granted, it was a database lock, and when you're talking about the stakes at the end of a drug trial, hours matter.) Surely there's a happy medium, though.
7 notes
·
View notes
Text
A Cheat Sheet for EHR Data Conversion and Migration

Bid farewell to data headaches and embrace a seamless transition between Electronic Health Record (EHR) systems! Moving to a new Electronic Health Record (EHR) can feel like scaling Mount Data Everest, but fear not, brave healthcare hero. This cheat sheet is your trusty sherpa, guiding you through the tricky terrain of data conversion and migration.
Before You Begin
Investigate how both your current and future EHR systems handle data export and import. Is it a database dump, APIs, or file transfers? The sooner you understand, the smoother the migration.
Do not assume that all data is easily transferable. Scrutinize your data to ensure it meets the new system’s requirements, as not all elements may seamlessly make the journey.
Don’t rely on cumbersome claim transfers. Wrap up outstanding accounts receivable in your old system before making the switch.
Schedule your migration around holidays to minimize disruption and give your team (and the data!) breathing room.
Conversion Strategies
Embrace a phased approach. Move demographics, appointments, and master lists first. Clinical data can wait (gasp!). This lets your team and the new EHR prioritize and get you online ASAP.
Conduct multiple tests, running trial conversions on small patient samples (say 30 patients). You’ll unearth issues before they become mountain-sized problems.
Consider retaining temporary access to your old system for reference purposes. It’s like a safety net for those “oh, I forgot that!” moments.
Not everything needs a new home. Utilize an archival system for data you don’t need in the new EHR.
Data Essentials
Ensure a smooth migration by prioritizing the transfer of the following essential data:
Patient Information: Demographics, insurance scans, policy details, historic charges/balances.
Appointments: Both past and future appointments, meticulously organized.
Master Lists: Categorize and transfer insurance providers, referral sources, and other relevant lists.
Clinical Data: Chart PDFs, discrete text data, allergies, medications, problem lists, immunizations, and progress notes.
Procedures: Transfer detailed information such as CPT codes, modifiers, and pre-authorization codes.
CCDAs: Acquire the Summary of Care document, a valuable data repository.
Financials: Limited financial data may be transferred, but confirm the specifics with your new EHR to ensure accuracy.
Bonus Tip: Make a list of all your EHR integration points like FHIR, HL7 V2, APIs, CSV files. Don’t leave any data orphans behind!
But fear not, weary traveler! You don’t have to climb this mountain alone. We’re here to help with expert guidance, proven strategies, and a team of data Sherpas ready to tackle any conversion challenge. Contact us today for a free consultation and let’s turn your EHR migration into a smooth and stress-free journey!
Remember, with the right plan and a helping hand, even the mightiest data peak can be conquered.
You may find this article on Falkondata website by following this link: https://falkondata.com/ehr-data-conversion-cheat-sheet/
2 notes
·
View notes
Text
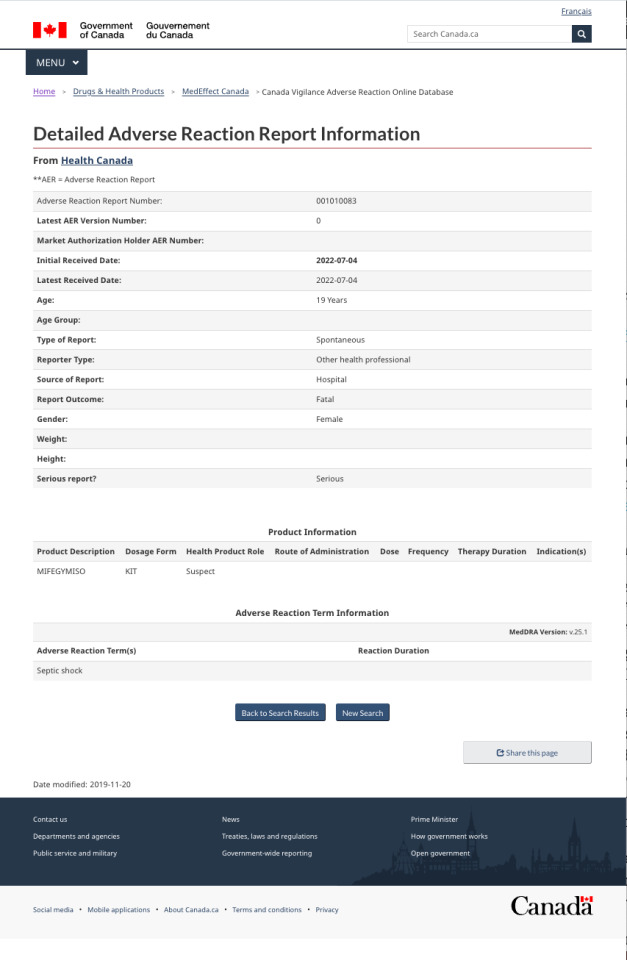
“Summer Roe”, 19 (Canada 2022)
The abortion pill continues to kill wherever it is legal. Documents have recently been released that verify the death of a Canadian teenager last summer who died after ingesting kill pills. Although the death occurred months ago, this case only came to light very recently. No source has been able to confirm the victim’s identity, so I am calling her Summer Roe for now.
Summer was only 19 years old. She was told that the abortion pill was safe and she paid for these lies with her life— and her baby’s life.
Summer legally underwent a chemical abortion using the RU-486 pill, which was branded as Mifegymiso in her area. She had to be hospitalized and was diagnosed with septic shock— the same condition that killed so many others before her. Despite the hospital’s efforts, Summer died of her raging infection.
This case would probably have gone entirely unreported had it not been for the actions of a medical professional at the hospital that tried to save Summer’s life. The Canada Vigilance Adverse Reaction Online Database has a report submitted from the unidentified medical professional documenting Summer’s chemical abortion and resulting death from septic shock.
Summer is not the only client who died from the legal use of the kill pill. Others include 18-year-old Holly Patterson, Chanelle Bryant, Oriane Shevin, Hoa Thuy “Vivian” Tran, Sarah Dunn, 18-year-old Manon Jones, Nadine Walkowiak, Anna Maria M, Brenda Vise, Maria Del Valle González López, 16-year-old Rebecca Tell Berg and many more who remain currently unidentified.
Summer’s case mirrors the death of 21-year-old “Jane Roe of Canada”, who was killed by septic infection in a clinical abortion pill trial despite being perfectly healthy only days before. The trials were shut down because of the severe side effects suffered by participants. Had the Canadian government permanently banned the RU-486 pill after the pill trials were shut down, Summer and her baby could have been spared.
How many more will suffer and die this way before RU-486 abortions are finally banned?
(If you think you know who Summer is and would like to help share her story and raise awareness, please DM me.)
#tw murder#tw abortion#tw ab*rtion#tw death#pro life#pro choice#abortion#abortion debate#unsafe yet legal
7 notes
·
View notes
Text
Power of Homeopathy as an Effective Treatment for Migraine

Millions of individuals worldwide suffer from the frequent neurological ailment known as migraines. Migraine is a condition that causes severe headaches, nausea, and light sensitivity that can last anywhere from a few minutes to days. A person's quality of life may be negatively impacted by the debilitating nature of migraine headaches and their potential to interfere with daily activities. Even though homeopathy is an alternative therapy, traditional medicine provides several migraine remedies, such as painkillers and prophylactic drugs. Homoeopathy is a type of complementary medicine that stimulates the body's own healing mechanisms by using greatly diluted natural chemicals. Homoeopathy has been used as an alternative medicine for over 200 years.
Homoeopathy for Migraine
Homoeopathy is a well-liked complementary treatment for migraines. Among the homoeopathic migraine treatments are Natrum muriaticum, Bryonia, Iris versicolor, and Belladonna. These treatments are thought to function by bringing the body's own energy into balance, lowering inflammation, and enhancing blood flow.
One benefit of using homoeopathy for migraines is that it doesn't have the potential side effects of using painkillers and anti-inflammatory drugs, which are common traditional migraine remedies. When administered as prescribed, homoeopathic medications are generally safe, though some patients may develop allergic responses or other negative effects.
There isn't enough data to say whether homoeopathy works to cure migraines, according to a review of clinical trials on the subject that has been released in the Cochrane Database of Systematic Reviews. The general caliber of the data is regarded as being low, despite the fact that certain individual research has shown encouraging results. To evaluate whether homoeopathy is useful for treating migraines, more research is required.
Types of Migraine:
There are two main forms of migraine.
Auratic migraine
Classical migraine is another name for migraine with aura. In this form, a feeling of aura (neurological symptoms) such as visual disturbance, hemisensory complaints, hemiparesis, or dysphasia frequently precede the attack. Most often, a visual aura is present. The aura often lasts a maximum of sixty minutes and develops over a period of 5 to 20 minutes. A headache, feeling of unwellness, and/or photophobia accompany it. The agonizing headache could persist for four to seventy-two hours.
Migraine without an aura
Ninety percent of migraine sufferers in women have this type of migraine, making it the most prevalent. This form of headache does not have an aura and only happens in episodes. An emotional condition, such as tension, euphoria, or any intense light or odor, may be the source of the headache. The headache primarily affects one side and gradually gets worse. The headache is frequently accompanied by nausea, vomiting, food intolerance, or sensitivity to bright lights and strong odors.
Prevalence of Migraine:
Females are more likely than males to experience migraines, with a male to female ratio of 1:3. Ninety percent of migraineurs have a family history of the condition. As people get older, migraine attacks become less common.
What Causes Migraines?
Genetic Propensity
High Oestrogen Levels
Sleep Deprivation
Emotional Strain
Noxious Odors
Migraine Symptoms:
Migraine Symptoms Without An Aura
The sort of vascular headache that occurs the most frequently is a migraine without aura. Moderate to severe headaches, a pulsating quality, a unilateral location, worsening by climbing stairs or engaging in other common activities, nausea and/or vomit, photophobia and phonophobia, and repeated attacks, each ranging 4 to 72 hours, are among the symptoms.
Migraine With Auratic Symptoms
The premonitory symptoms of headache can include motor, sensory, or visual complaints. Most victims have stated that visual problems are the most prevalent. Headache, feeling dizzy, and photophobia follow the aura.
Homoeopathic Migraine Treatments
Belladonna
A popular homoeopathic treatment for migraines is belladonna. The deadly nightshade plant's byproduct, belladonna, is said to have anti-inflammatory and blood flow-improving properties. Migraines with throbbing discomfort, redness, and heat are frequently treated with belladonna.
Bryonia
A typical homoeopathic treatment for migraines is bryonia. Bryonia, which is produced by the white bryony plant, is thought to function by easing pain and promoting blood flow. When a migraine occurs accompanied by a monotonous, throbbing pain that gets worse with movement, bryonia is frequently prescribed.
Versicolor iris
Homoeopathic treatment for migraines that is frequently used is iris versicolor. Iris versicolor, which comes from the blue flag plant, is thought to have anti-inflammatory and blood-flow-improving properties. Iris versicolor is frequently prescribed for migraines that come with severe, excruciating pain and nausea.
Muriatic natrum
A typical homoeopathic treatment for migraines is natrum muriaticum. Natrum muriaticum, which is made from sea salt, is thought to act by easing inflammation and enhancing blood circulation. Natrum muriaticum is frequently prescribed for migraines that come with throbbing pain and susceptibility to light.
Conclusion
There are generally no risks associated with using homoeopathy to treat migraines, unlike conventional migraine treatments. While homoeopathy may offer some migraine patients some relief, it's vital to speak with a doctor before utilizing it as a therapy. To guarantee that you obtain the right care for your migraines, it is crucial that you see a doctor. Visit us and book an appointment now with Dr. Shubham Tiwary.
#homeopathy#homeopathy doctor#homeopathic medicines#homeopathy treatment#Homeopathic remedies#best homeopathy doctor near me#homeopathy doctor near me#homeopathy near me#consult a doctor
2 notes
·
View notes
Text
Use of acupressure to reduce nausea and vomiting in cancer patients receiving chemotherapy (literature study) by Maher Battat in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
Nausea and vomiting are distressing and serious problems for cancer patients receiving chemotherapy despite the fact that they are receiving antiemetics according to the standard guidelines which this problem is a huge challenge to nurses involved in cancer care.
Purpose: To explore and assess the effectiveness of using acupressure as a non-pharmacological intervention in addition to pharmacological interventions in reducing nausea and vomiting in cancer patients receiving chemotherapy.
Method: A literature review was conducted of 8 articles published between 2006 and 2014. These included one study of a randomized, double-blind, placebo controlled trial; one quasi-experimental model with a control group; four articles reporting on randomized control trials (RCTs); one systematic review study; and one review study. Key Findings: Seven of the articles we read supported the effect of an acupressure P6 Wristband in reducing chemotherapy induced nausea and vomiting in cancer patients and other databases also supported that finding. The one article with neutral results showed that there was no difference between a combination of acupuncture and acupressure treatment at P6 and at the sham point for the nausea score, but the level of nausea was very low in both groups.
Conclusion: We conclude that the acupressure P6 wrist band when applied to acupuncture point P6 is effective, safe, convenient, cost effective, and provides an easy, self-administrated, non-pharmacological intervention that can be used to reduce chemotherapy induced nausea and vomiting.
Keywords: Acupressure, Chemotherapy, Nausea and Vomiting, Cancer patients, Chemotherapy-induced nausea and vomiting.
INTRODUCTION
Nausea and vomiting are serious and troublesome side effects of cancer therapy. We chose this research topic in order to become familiar with the topic of the nausea and vomiting facing cancer patients during their chemotherapy treatment, which we have observed during our experience in the Oncology departments.
As nurses, we normally use updated and standard guidelines for managing clinical challenges. We reviewed the literature to explore whether there are alternative approaches to pharmacological management that might reduce or eliminate this problem. We found there are many interventions, such as music, acupuncture, acupressure, and yoga. We decided to assess the effectiveness of using acupressure to reduce the nausea and vomiting in cancer patients receiving chemotherapy. Acupressure is a type of complementary and alternative medicine which the National Cancer Institute (NCI Dictionary of Cancer Terms) defines as follows: “Acupressure is the application of pressure or localized massage to specific sites on the body to control symptoms such as pain or nausea".
THE RESEARCH QUESTION
Can acupressure reduce nausea and vomiting in cancer patients receiving chemotherapy?
We have chosen to use the definitions of the NCI Dictionary of Cancer Terms:
“Nausea is an unpleasant wavelike feeling in the back of the throat and/or stomach that may lead to vomiting", and “Vomiting is throwing up the contents of the stomach through the mouth”.
Nausea and vomiting affect the patient’s whole life. These side effects lead to metabolic imbalance, fatigue, distress, and lowered quality of life. We would like to fine a simple, effective and cost effective way to manage these problems so we can put it to use in our hospital.
METHOD
A literature study is, “A critical presentation of knowledge from various academic written sources, and a discussion of the sources in view of a particular research question" (Synnes 2014). There are many challenges when doing a literature study. There are many databases and much literature and our search process had to find the correct, scientific and relevant databases. It required a lot of time and effort to find the full text of all relevant articles. Fortunately, we received excellent help from the librarian at the Betanien University High school.
We started the search process by making a PICO outline to narrow down the search and to find the correct key words and mesh terms.
P: (Population or participants) Cancer patients experiencing chemotherapy-induced nausea and vomiting.
I: (Intervention or indicator) Acupressure.
C: (Comparator or control) No comparison or placebo.
O: (Outcome) Reduce nausea and vomiting.
We used PUBMED, Google scholar, scholar.najah.edu and other search engines. When we used Acupressure as a search word we found more than 800 studies. When we added chemotherapy, cancer patients, and nausea and vomiting, we brought this down to 14 articles. We read these and decided to use 8 articles only, one of which was a systematic review. We also used an unpublished Master’s thesis from An Najah National University. This thesis was cited in one of the articles that we decided to review. The key words used were: Acupressure, Chemotherapy, Nausea and Vomiting, Cancer patients, Chemotherapy-induced nausea and vomiting, with Acupressure as a mesh term.
We then critically appraised all the articles according to our checklist. We included only those articles that followed the IMRAD style (i.e. those including an introduction, method, results and discussion section). We excluded all articles that were more than ten years old (i.e. published before 2004), except for two articles: one was about the mechanism of acupressure, which seemed to be directly relevant to our research topic, while the second article was used in the discussion section to discuss certain factors related to the topic. We also excluded one of the review articles because its method appeared to be weak. One of the Cochran reviews was also dropped because it had not been updated.
Despite applying these strict criteria, we were still concerned lest we had left out some important articles or included an inappropriate one. However, we were reassured by the fact that the librarian at Betanien had guided us in our search.
THEORETICAL PART
Nursing Need Theory and basic human needs
The Nursing Need Theory was developed by Virginia A. Henderson to define the unique focus of nursing practice. The theory focuses on the importance of increasing the patients’ independence to hasten their progress in the hospital. Henderson’s theory emphasizes the basic human needs and how nurses can assist in meeting those needs.
The 14 components of Need Theory present a holistic approach to nursing that covers the patient’s physiological, psychological, spiritual and social needs.
Physiological components
Breathe normally.
Eat and drink adequately.
Eliminate body wastes.
Move and maintain desirable postures.
Sleep and rest.
Select suitable clothes – dress and undress.
Maintain body temperature within normal range by adjusting clothing and modifying the environment.
Keep the body clean and well groomed and protect the integument.
Avoid dangers in the environment and avoid injuring others.
Psychological aspects of communicating and learning
Communicate with others in expressing emotions, needs, fears, or opinions. Spiritual and moral
Worship according to one’s faith. Sociologically oriented to occupation and recreation
Work in such a way that there is sense of accomplishment.
Play or participate in various forms of recreation.
Learn, discover, or satisfy the curiosity that leads to normal development and health, and use the available health facilities.
There is much similarity between Henderson’s 14 components and Abraham Maslow’s Hierarchy of Needs. Henderson’s Components 1 to 9 are comparable to Maslow’s physiological needs, with the 9th component also being a safety need. Henderson’s 10th and 11th components are similar to Maslow’s love and belonging needs, while her 12th, 13th and 14th components match Maslow’s self-esteem needs (Vera 2014).
The second of Henderson’s physiological needs is the need to “Eat and drink adequately”. Only the need to breathe is given a higher priority than the need for adequate nutrition. For cancer patients receiving chemotherapy and suffering from chemotherapy-induced nausea and vomiting, this need is the most critical.
Cancer prevalence and treatment
Cancer is a group of diseases characterized by uncontrolled growth and the spread of abnormal cells. It may be caused by internal factors, such as an inherited mutation, or a hormonal or immune condition, or it may result from a mutation from metabolism, or from external sources, such as tobacco use, radiation, chemicals and infectious organisms. Cancer is prevalent all over the world, in both developed and developing nations; it affects both sexes at all ages (Said 2009). The American Cancer Society (2010) estimated that 1,529,560 new cases of cancer were diagnosed in 2010 and that 80 % would be treated with chemotherapy; this means more than 1 million patients will be undergoing chemotherapy in any given year (Lee et al. 2010).
Cancer treatment may be based on chemotherapy, radiotherapy and surgical interventions. Chemotherapy is an important treatment in cancer care but it is associated with several side effects, such as bone marrow suppression, increased susceptibility to infection, diarrhea, hair loss, appetite changes, nausea and vomiting, among others (NCI Chemotherapy Side Effects Series, 2014).
Chemotherapy-induced nausea and vomiting (CINV) is the most prevalent and one of the hardest side effects to manage (Suh 2012).
Nausea and vomiting
Nausea and vomiting (N&V) can be acute or delayed. The incidence of acute and delayed N&V was investigated in highly and moderately emetogenic chemotherapy treatment regimens. Patients were recruited from 14 oncology practices in six countries. Overall, more than 35% of patients experienced acute nausea, and 13% experienced acute emesis. In patients receiving highly emetogenic chemotherapy, 60% experienced delayed nausea and 50% experienced delayed emesis. In patients receiving moderately emetogenic chemotherapy, 52% experienced delayed nausea and 28% experienced delayed emesis. CINV was a substantial problem for patients receiving moderately emetogenic chemotherapy in ten community oncology clinics. Thirty-six percent of patients developed acute CINV, and 59% developed delayed CINV (NCI, Nausea and Vomiting, 2015).
Chemotherapy is the most common treatment-related cause of N&V. The incidence and severity of acute emesis in persons receiving chemotherapy varies according to many factors, including the particular drug, dose, schedule of administration, route, and individual patient variables.
Risk factors for acute emesis include:
Poor control with prior chemotherapy
Female gender
Younger age
Emetic classification:
The American Society of Clinical Oncology has developed a rating system for chemotherapeutic agents with their respective risk for acute and delayed emesis.
High risk: Emesis has been documented to occur in more than 90% of patients on the following chemotherapeutic agents:
Cisplatin (Platinol).
Mechlorethamine (Mustargen).
Streptozotocin (Zanosar).
Cyclophosphamide (Cytoxan), 1,500 mg/m2 or more.
Carmustine (BiCNU).
Dacarbazine (DTIC-Dome).
Moderate risk: Emesis has been documented to occur in 30% to 90% of patients on the following chemotherapeutic agents:
Carboplatin (Paraplatin).
Cyclophosphamide (Cytoxan), less than 1,500 mg/m2.
Daunorubicin (DaunoXome).
Doxorubicin (Adriamycin).
Epirubicin (Pharmorubicin).
Idarubicin (Idamycin).
Oxaliplatin (Eloxatin).
Cytarabine (Cytosar), more than 1 g/m2.
Ifosfamide (Ifex).
Irinotecan (Camptosar).
Low risk: Emesis that has been documented to occur in 10% to 30% of patients on the following chemotherapeutic agents:
Mitoxantrone (Novantrone).
Paclitaxel (Taxol).
Docetaxel (Taxotere).
Mitomycin (Mutamycin).
Topotecan (Hycamtin).
Gemcitabine (Gemzar).
Etoposide (Vepesid).
Pemetrexed (Alimta).
Methotrexate (Rheumatrex).
Cytarabine (Cytosar), less than 1,000 mg/m2.
Fluorouracil (Efudex).
Bortezomib (Velcade).
Cetuximab (Erbitux).
Trastuzumab (Herceptin).
Minimal risk: Emesis that has been documented to occur in fewer than 10% of patients on the following chemotherapeutic agents:
Vinorelbine (Navelbine).
Bevacizumab (Avastin).
Rituximab (Rituxan).
Bleomycin (Blenoxane).
Vinblastine (Velban).
Vincristine (Oncovin).
Busulphan (Myleran).
Fludarabine (Fludara).
2-Chlorodeoxyadenosine (Leustatin).
In addition to the emetogenic potential of the agent, the dose and schedule used are also extremely important factors. For example, prescribing a drug with a low emetogenic potential to be given in high doses may cause a dramatic increase in its potential to induce N&V. For example, standard doses of cytarabine rarely produce N&V, but these often occur with high doses of this drug. Another factor to consider is the use of drug combinations. Because most patients receive combination chemotherapy, the emetogenic potential of all of the drugs combined needs to be considered, and not only that of individual drug doses.
Delayed (or late) N&V is that which occurs more than 24 hours after chemotherapy administration. Delayed N&V is associated with cisplatin and cyclophosphamide, and with other drugs (e.g., doxorubicin and ifosfamide) when given at high doses, or if given on 2 or more consecutive days.
Delayed emesis: Patients who experience acute emesis with chemotherapy are significantly more likely to have delayed emesis as well.
Risk factors: All the predicative characteristics for acute emesis are also considered risk factors for delayed emesis (NCI, Nausea and Vomiting, 2015).
The nausea and vomiting that are often associated with chemotherapy are a serious problem for cancer patients. Despite recent improvements in pharmaceutical technology, about 60% of cancer patients who receive antiemetic medications with their chemotherapy still suffer from nausea and vomiting, and as many as 20% of patients refuse to continue chemotherapy due to the severity of the nausea and vomiting (Shin et al. 2004). Early studies reported that patients cited nausea and vomiting as the most distressing symptoms when receiving chemotherapy. The distressing effect of severe nausea and vomiting can lead to nutritional deficiencies, dehydration, electrolyte imbalance, fatigue, depression and anxiety; they can also disrupt the activities of daily living and cause a lot of work time to be lost (Said 2009).
Uncontrolled nausea and vomiting can interfere with adherence to treatment regimens, and may cause the oncologists to reduce chemotherapy doses. Chemotherapy-induced nausea and vomiting is classified as being either “acute” if it happens within 24 hours post chemotherapy, or “delayed” if it occurs on days 2–5 of the chemotherapy cycle. The latter is particularly troublesome because there is no reliable pharmacological treatment for this problem. The American Society of Clinical Oncology’s (ASCO) recommendations include giving 5-HT3 (5-hydroxytryptamine, or serotonin) receptor antagonists plus corticosteroids before chemotherapy to patients who are at high risk for emesis. Nevertheless, many patients still experience nausea and vomiting related to chemotherapy, and approximately one-third of patients have nausea of at least moderate intensity, resulting in a significant reduced quality of life (QOL). Therefore, the experts emphasize the need for an evaluation of additional ways to reduce these symptoms (Said 2009).
Pharmacological interventions for the management of nausea and vomiting
Historically, antiemetic treatment has steadily improved since the introduction, in 1981, of high-dose metoclopramide which reduced the amount of emesis. This was followed by the development of serotonin (5-HT3) antagonist in the early 1990s, and the 5-HT3 antagonists proved to be more effective than the prior medications in preventing CINV. The concomitant use of corticosteroids was found to further improve the control of emesis. Despite these improvements, nausea and vomiting still remain a problem for many patients. Recently, a new drug, the neurokinin NK (1) receptor antagonist has been shown to be more effective at preventing both acute and delayed CINV for patients treated with highly emetogenic chemotherapy (Said 2009).
Non-pharmacological intervention for management of nausea and vomiting
Traditional Chinese medicine offers a possible intervention for the non-pharmacological treatment of nausea and vomiting in cancer patients. Traditional Chinese medicine (TCM) is a system of medical care that was developed in China over thousands of years. It looks at the interaction between mind, body and environment, and aims to both prevent and cure illness and disease.
TCM is based on Chinese views and beliefs about the universe and the natural world. It is a very complex system. In this essay we can only give a brief overview of what TCM involves. It is very different from Western medicine; Chinese medicine practitioners believe there is no separation between the mind and body and that illness of every kind can be treated through the body. They use a combination of various practices that may include:
Herbal remedies (traditional Chinese medicines).
Acupuncture or acupressure.
Moxibustion (burning moxa – a cone or stick of dried herb).
Massage therapy.
Feng shui.
Breathing and movement exercises called qi gong (pronounced chee goong).
Movement exercises called tai chi (pronounced tie chee).
TCM practitioners say that TCM can help to:
Prevent and heal illness.
Enhance the immune system.
Improve creativity.
Improve the ability to enjoy life and work in general.
Beliefs behind TCM
According to traditional Chinese belief, humans are interconnected with nature and affected by its forces. The human body is seen as an organic whole in which the organs, tissues, and other parts have distinct functions but are all interdependent. In this view, health and disease relate to the balance or imbalance between the various functions. TCM treatments aim to cure problems by restoring the balance of energies.
There are important components that underlie the basis of TCM:
Yin-yang theory is the concept of two opposing but complementary forces that shape the world and all life. A balance of yin and yang maintains harmony in the body, the mind and the universe.
Qi (pronounced chee) energy or vital life force flows through the body along pathways known as meridians, and it is affected by the balance of yin and yang. It regulates spiritual, emotional, mental, and physical health. If there is a blockage or an imbalance in the energy flow, the individual becomes ill. TCM aims to restore the balance of qi energy.
The five elements – fire, earth, metal, water, and wood – is a concept that explains how the body works, with the elements corresponding to particular organs and tissues in the body.
The TCM approach uses 8 principles to analyse symptoms and puts particular conditions into groups: cold and heat, inside and outside, too much and not enough, and yin and yang (Cancer Research, UK, 2015).
In summary, chemotherapy related nausea is not well controlled by pharmacological agents and identifying methods to prevent and alleviate treatment-related nausea remains a major clinical challenge. Non-pharmacological interventions such as music, progressive muscle relaxation (Said 2009), and ginger herbal therapy (Montazeri A et al. 2013) have all been shown to reduce CINV. Among the non-pharmacological interventions that reduce CINV are acupuncture and acupressure, based on the assumption that the individual’s welfare depends on a balance of energy in the body and their overall energy level (Said 2009). Yarbro et al. (2011, p. 645) also indicate in Cancer nursing: principles and practice book that acupuncture and acupuncture-related interventions (electroacupoint stimulation, acupressure, acustimulation wrist bands, and electroacupuncture) can be used to control nausea and vomiting in cancer patients.
Molassiotis et al. (2007) claim that the need for additional relief has led to the interest in non-pharmacological adjuncts to drugs, such as acupuncture or acupressure, since combining anti-emetics with other non-pharmacological treatments may prove to be more effective, safe and convenient in decreasing nausea than antiemetics alone.
From the National Cancer Institute website we found that acupressure is recognised as one of the non-pharmacologic strategies used to manage nausea and vomiting (Nausea and Vomiting, 3 September 2014). We used this website to get up to date, relevant information.
Acupressure
Acupressure involves putting pressure with the fingers, or with bands, on the body’s acupoints and is easy to perform, painless, inexpensive, and is effective. The P6 (Pericardium 6) point (Nei-Guan) refers to a point located on the anterior surface of the forearm, 3-finger widths up from the first wrist crease and between the tendons of flexor carpiradialis and Palmaris longus (figure1). P6 can be stimulated by various methods. The most well-known technique is manual stimulation by the insertion and manual rotation of a very fine needle (manual acupuncture). An electrical current can be passed through the inserted needle (electroacupuncture). Electrical stimulation can also be applied via electrodes on the skin surface or by a ReliefBand, a wristwatch-like device providing non-invasive electrostimulation. Pressure can be applied either by pressing the acupoint with the fingers or by wearing an elastic wristband with an embedded stud (acupressure).
Figure 1: Done by M.Battat & I.Amro 2015 The Acupressure P6 point determined in the picture And showing the SEA BAND acupressure
Acupressure is based on the ancient Eastern concept that Chi energy travels through pathways known as meridians. Along the meridians are acu-points, which are controlling points for the Chi energy flow. If the energy flow in meridians is slowed, blocked, or hyper-stimulated, it can be rebalanced or re-stimulated either by applying pressure (acupressure) or by inserting a needle (acupuncture) into one or more of these acupoints. Two points are known for relieving nausea and vomiting: the Nei-Guan point (P6) and the Joksamly point (ST36, located at 4-finger breadths below the knee depression lateral to the tibia).
Patients tend to prefer the P6 point over the ST36 point, Because of its ease of access and the freedom from restriction. When these points are correctly located and pressure applied, either through acupressure or acupuncture, the Chi energy flow is rebalanced, resulting in relief from nausea and vomiting.
The practice of acupressure requires some training and experience, but the technique is widely accessible to any healthcare professionals, particularly to clinical nurses. This acupressure technique is an approach that should be tried not only by healthcare professionals but also by family members or the patients themselves (Shin et al. 2004).
According to the teaching of traditional Chinese medicine, illness results from an imbalance in the flow of energy through the body. This energy or Qi (chee) is restored through the use of acupuncture and acupressure at certain points on the body that have been identified through critical observation and testing over 4000 years. In scientific terms, the neurochemicals that are released after needling or pressure at a specific point may be responsible for this effect. The most commonly used point for nausea and vomiting is Pericardium 6 (Neiguan or P6), located above the wrist (Molassiotis et al. 2007).
The literature review on acupressure
Acupressure for chemotherapy-induced nausea and vomiting in breast cancer patients: a multicentre, randomised, double-blind, placebo-controlled clinical trial. (Said 2009)
For a master degree in public health from An-najah National University, Said (2009) described a randomized, double-blind, placebo controlled trial that was done in Palestine with 126 women on chemotherapy for breast cancer. In this study the researcher divided the patients into 3 groups: the first group (n=42) received acupressure with bilateral stimulation of P6, the second group (n=42) received bilateral placebo stimulation, and the third group (n=42), which served as a control group, received no acupressure wrist band, but all groups received pharmacological management of their nausea and vomiting. Acupressure was applied using a Sea-Band (Sea-Band UK Ltd, Leicestershire, England) that patients had to wear for five days following the administration of chemotherapy. Assessment of acute and delayed nausea and emesis, quality of life, patients’ satisfaction, recommendation of treatment and requests for a rescue antiemetic were obtained. Said (2009) concluded that the acupressure showed benefits for delayed nausea and the mean number of delayed emetic episodes. Acupressure may therefore offer an inexpensive, convenient, and self-administered intervention for patients on chemotherapy to reduce nausea and vomiting at home during days 2-5 after chemotherapy. In addition, the percentage of patients who were satisfied with the treatment (≥ 3 on a 0-6 scale) was 81% (35/42) in the P6-acupressure group, and 64% (27/42) in the placebo group (p= 0.0471). The percentage of patients who would recommend acupressure treatment was 79% (34/42) in the P6-acupressure group, and 62% (26/42) in the placebo group (p= 0.0533). We used this study because it had a lot of essential information, it used the IMRAD system and was also mentioned in the literature (Genç and Tan 2014). This study demonstrated that the mean scores for the acupressure group were lower for both acute and delayed nausea.
Review of Acupressure Studies for Chemotherapy-Induced Nausea and Vomiting Control. (Lee et al. 2008)
In the Journal of Pain and Symptom Management Jiyeon Lee et al. (2008) reviewed ten controlled studies on acupressure in order to evaluate the effects of a non-invasive intervention, acupressure, when combined with antiemetics for the control of CINV. The review evaluated one quasi-experimental and nine randomized clinical trials, which included two specific acupressure modalities, namely, an acupressure band and finger acupressure. The effects of the acupressure modalities were compared study by study. Four of the seven acupressure band trials supported the positive effects of acupressure, whereas three acupressure band trials did not support the effects of acupressure. However, all the studies with negative results had methodological issues. In contrast, the one quasi-experimental and two of the randomized finger acupressure trials all supported the positive effects of acupressure on CINV control. The reported effects of the two acupressure modalities produced variable results at each stage of CINV. Acupressure bands were most effective in controlling acute nausea, whereas finger acupressure controlled delayed nausea and vomiting. The overall effect of acupressure was strongly indicative but not conclusive. We used this article because it is relevant, a review study, and is from a known journal.
The effects of P6 acupressure in the prophylaxis of chemotherapy-related nausea and vomiting in breast cancer patients. (Molassiotis et al. 2007)
As reported in the journal Complementary Therapies in Medicine, acupressure was applied using wristbands (Sea-Band™) in a randomized controlled trial conducted in two centres in the UK. Patients in the experimental group had to wear these bands for the five days following their chemotherapy administration. Assessments of nausea, retching and vomiting were obtained from all patients, daily, for five days. Molassiotis et al. (2007) evaluated the effectiveness of using acupressure on the Pericardium 6 (Neiguan) acupoint in managing CINV. Thirty-six patients took part in the study, with 19 patients allocated to the control group and 17 to the experimental group. The results showed that nausea with retching, nausea, and vomiting with retching, and the accompanying distress were all significantly lower in the experimental group as compared to the control group (p < 0.05). The only exception was the vomiting, where the difference was close to significance (p = 0.06). We used this article because it had a strong study design and also used an IMRAD system.
Acupuncture and acupressure for the prevention of chemotherapy-induced nausea- a randomized cross-over pilot study. (Melchart et al. 2006)
In a randomized, cross-over trial, Melchart et al. (2006) studied 28 patients receiving moderately or highly emetogenic chemotherapy and a conventional standard antiemetic for one chemotherapy cycle, followed by a combination of acupuncture and acupressure at point P6 for one cycle, and for another cycle a combination of acupuncture and acupressure at a close sham point. The results showed that there was no difference in the nausea score between the combined acupuncture treatment at P6 and at the sham point, but the level of nausea was very low in both cases. We used this study because the article had neutral results and because we trusted the source of article, coming as it did from a cancer support care journal.
The efficacy of acupoint stimulation for the management of therapy adverse events in patients with breast cancer: a systematic review. (Chao et al. 2009)
This is a systematic review of 26 articles published between 1999 to 2008 examining the efficacy of acupressure, acupuncture or acupoint stimulation (APS) for the management of adverse events due to the treatment of breast cancer. Published online on 17 September 2009 in the Breast Cancer Research and Treatment journal, 23 trials reported revealed that APS on P6 was beneficial in treating CINV. Chao et al. (2009) also presented the findings from three high quality studies comparing APS groups with control groups, which indicated that APS is beneficial in the management of CINV and especially in the acute phase, even with the non-invasive intervention. Health care professionals should consider using APS, and in particular acupressure on the P6 acupoint, as an option for the management of CINV. Furthermore, as a cost effective intervention, it warrants further investigation. We used this article because it used the IMRAD structure.
'Until the trial is complete you can’t really say whether it helped you or not, can you?’: exploring cancer patients’ perceptions of taking part in a trial of acupressure wristbands. (Hughes et al. 2013)
In Complementary and Alternative Medicine, Hughes et al. report on qualitative research undertaken with patients receiving chemotherapy in the UK. A convenience sample of 26 patients volunteered to participate in the clinical trial and to explore their experiences of using acupressure wristbands. Participants were recruited from three geographical sites: nine were recruited from Manchester, nine from Liverpool, and eight from Plymouth and the surrounding regions. Ten of the participating patients received true acupressure during the trial, 9 received sham acupressure, and 7 received no acupressure. Hughes et al. (2013) concluded that the research provided insights into cancer patients’ motivations and experience of taking part in a clinical trial for a complementary alternative medicine intervention, in which the participants perceived acupressure wristbands to reduce the level of nausea and vomiting experienced during their chemotherapy treatment. This article is important because it includes the benefits experienced by the patients taking part in the trial. This is also the first qualitative study to explore patients’ experiences of using acupressure wristbands and their perceptions of the effects. In the study, the patients perceived the wristbands as reducing their level of nausea and vomiting experienced due to their chemotherapy treatment. The study was an RCT.
The effect of acupressure application on chemotherapy-induced nausea, vomiting, and anxiety in patients with breast cancer. (Genç and Tan 2014)
Genç and Tan (2014) reported on a quasi-experimental study in Turkey with 64 patients with stages 1–3 breast cancer who received two or more cycles of advanced chemotherapy. Thirty two patients were in the experimental group, and thirty two in the control group. To determine the effect of acupressure P6 on CINV and anxiety in these patients, the P6 acupressure wristband was applied to the experimental group. Genç and Tan (2014) concluded that the total mean scores for patients in the experimental group, for nausea, vomiting and retching, were lower than those of the patients in the control group over the five days of application. We used this article because it is a recent and quasi-experimental study and used the IMRAD system.
The effects of P6 acupressure and nurse-provided counselling on chemotherapy-induced nausea and vomiting in patients with breast cancer. (Suh 2012)
Suh (2012) reported in the Oncology Nursing Forum on a RCT in South Korea with 120 women who were receiving chemotherapy for breast cancer. These patients had all had more than mild levels of nausea and vomiting during their first cycle of chemotherapy. The participants were assigned randomly to one of four groups: a control group (a placebo on a specific location on the hand); a counselling only group; a P6 acupressure only group; and a P6 acupressure plus nurse-provided counselling group. The purpose of the study was to evaluate the effects of pericardium 6 (P6) acupressure and nurse-provided counselling on CINV in patients with breast cancer. Suh (2012) concluded that nurse-provided counselling and P6 acupressure were together the most effective in reducing CINV in patients with breast cancer. We used this article because it is the first RCT evaluating the isolated and combined effects of P6 acupressure and counselling in reducing CINV among non-Western patients. The findings of the study support the use of P6 acupressure together with counselling that is focused on cognitive awareness, affective readiness, symptom acceptance, and the use of available resources as an adjunct to antiemetic medicine for the control of CINV. The article used the IMRAD system.
DISCUSSION
Can acupressure reduce nausea and vomiting in cancer patients receiving chemotherapy?
In our experience, we have usually used metoclopramide (pramin) plus serotonin (5-HT3) antagonist (as Ondansetron and Granisetron), plus Dexamethasone plus neurokinin NK (1) (as Emend - aprepitant) for moderate to high ematogenic chemotherapy, yet some of the patients have still suffered from nausea and vomiting. After reviewing the literature we would like to use the acupressure P6 wrist band to solve this problem as the findings of our literature review confirm that the acupressure P6 wrist band reduces CINV in cancer patients receiving chemotherapy. This result is corroborated by 7 of the articles reviewed.
The National Cancer Institute website supports the finding that acupressure is one of the non-pharmacologic strategies that may be used to manage nausea and vomiting (NCI Dictionary of Cancer Terms). Said (2009) adds that acupressure may offer an inexpensive, convenient, and self-administered intervention for patients on chemotherapy, helping to reduce nausea and vomiting at home on days 2-5 of chemotherapy. Genç and Tan (2014) conclude that the total mean scores for CINV in patients in the experimental group to whom they applied the P6 acupressure wristband were lower compared to patients in the control group over the five days of application. Lee et al. (2008) found that the two acupressure modalities produced variable results in each phase of CINV: acupressure bands were effective in controlling acute nausea, whereas acupressure controlled delayed nausea and vomiting. Molassiotis et al. (2007) showed that the experience of nausea and vomiting was significantly lower in the experimental group than in the control group. Chao et al. (2009) found that P6 acupoint stimulation was an option for the management of CINV. In the study reported by Hughes et al. (2013) the participants perceived that acupressure wristbands reduced the levels of nausea and vomiting experienced during chemotherapy treatment. Suh (2012) concluded that the synergistic effects of P6 acupressure together with nurse-provided counselling appeared to be effective in reducing CINV in patients with breast cancer.
Five of the seven articles investigating breast cancer patients, namely Said (2009), Chao et al.( 2009), Molassiotis et al. (2007), Suh (2012) and Genç and Tan (2014), involved breast cancer patients receiving highly ematogenic chemotherapy (e.g. Cisplatin and cyclophosphamide), and moderate risk ematogenic chemotherapy (like doxorubicin).
It is necessary to mention other therapeutic regimens that can also be used in cancer treatment that contain other types of chemotherapy that cause nausea and vomiting, for example, doxorubicin-containing regimens like ABVD (Adriamycin, Bleomycin, Vinblastine, Dacarbazine), CHOP (Cyclophosphamide, Adriamycin, Vincristine, Prednisone) and FAC (5-Fluorouracil, Adriamycin, Cyclophosphamide), and ACT (Adriamycin, Cyclophosphamide, Taxol) (Said 2009) and from our experience cisplatin-containing regimens which that classified as highly ematogenic chemotherapy we noticed the patients still experienced nausea and vomiting after they received the antiemitecs. We think it is necessary to use additional intervention like acupressure to be included in the nausea and vomiting management.
Based on the reviewed findings we plan to use acupressure for cancer patients receiving chemotherapy, because the acupressure in the studies conducted in breast cancer patients reported was used with highly ematogenic chemotherapy in addition to the standard antiemetic treatment, so it is reasonable to conclude that it will work equally well with other less ematogenic types of chemotherapy.
We prefer the use of the acupressure wrist band at P6 acupoint because it is an inexpensive, convenient, and self-administered intervention involving pressure instead of needles at the same point as that used in acupuncture. Furthermore it is safer than acupuncture and patients can easily learn to put pressure on their own wrists, whereas the acupuncture involves using needles that are about the diameter of a hair and can cause temporary discomfort during insertion (Said 2009; Molassiotis et al. 2007). Acupressure seems to be a good way to complement antiemetic pharmacotherapy as it is safe and convenient, with minimal (with bands) or no (finger acupressure) costs involved. It is thus an easy to use, cost-effective, non-invasive intervention (Lee et al. 2008; Melchart et al. 2006).
There was no study result that showed any negative effect from the acupressure wrist band at P6 point, except the review by Lee et al. (2008), which mentioned that three of the ten reported acupressure band trials did not support the possible positive effects of acupressure, but these studies all had methodological issues, such as a small sample size, no true control group, and a concern about the sham acupressure band having a possible antiemetic effect. Melchart et al. (2006) said that no difference was detected in the nausea score between the acupuncture treatment at P6 acupoint, and that at the sham point. Said (2009) mentioned that the acupressure showed no benefit in relation to the incidence of delayed vomiting, early vomiting, or acute nausea, but Melchart and Said’s studies were done with breast cancer patients and it could be that the acupressure benefits were not evident due to the breast cancer patients having had axillary lymph node resection that may have affected the meridian pathway or caused damage to the median nerve as mentioned by Roscoe et al. (2003). Consequently, we think that the evidence suggesting that there is no benefit from the acupressure method for reducing CINV is weak.
Regarding the placebo effect in the articles reviewed here, Melchart et al. (2006) indicated that there was no difference in the nausea score for the combined acupuncture treatment at p6 or that at the sham point, although the level of nausea was very low in both cases. Molassiotis et al. (2007), Said (2009) and Roscoe et al. (2003) all suggested that the placebo effect may be the result of psychological factors.
Application of acupressure in clinical practice
It is important to put this theory into practice, and health care professionals could consider using APS, in particular acupressure on the P6 acupoint, as an option in the management of CINV (Chao et al. 2009). Melchart et al. (2006) said acupressure bands can easily be used in busy oncological wards, while Suh (2012) supported the use of P6 acupressure with counselling focused on cognitive awareness, affective readiness, symptom acceptance, and the use of available resources as an adjunct to antiemetic medications for the control of CINV. Hughes et al. (2013) concluded that the research provides an insight into cancer patients’ motivations for and experiences of taking part in a clinical trial for a complementary alternative medical intervention in which the participants perceived the acupressure wristbands as reducing their level of CINV. Said (2009) suggests that oncology nurses should include acupressure in their list of options for the management of CINV, and especially delayed nausea and vomiting. Special recommendations by oncology nurses are not only useful but are also much appreciated by patients as shown in a study in which the patients were satisfied with the antiemetic treatment given by both P6-acupressure, and placebo-acupressure. The percentage of patients who were satisfied (≥ 3 on 0-6 scale) with their treatment was 81% (35/42) in the P6-acupressure group, which was in agreement with Roscoe et al. (2003), and 64% (27/42) in the placebo group (p= 0.0471). The percentage of the patients who would recommend acupressure treatment was 79% (34/42) in the P6-acupressure group, which again was in agreement with the results of Roscoe et al. (2003) and Hughes et al. (2013), compared to 62% (26/42) in the placebo group (p= 0.0533). This study presented the patients’ compliance with the use of acupressure. Acupressure is easily learnt and taught and patients should be informed about its potential role and taught how to apply it. Leaflets about acupressure for the management of nausea and vomiting could be available in chemotherapy units so that patients who are interested to use such a technique would be encouraged to come forward and learn more from nurses or other health professionals. This could add to the patients’ options for antiemetic approaches and empower them to be involved in the management of these distressing side effects. Acupressure offers a no-cost, convenient, self-administered intervention for chemotherapy patients to reduce acute nausea. Acupressure devices (i.e. Wrist Bands, travel bands, and acupressure bands) have been developed to provide passive acupressure on P6. Acupressure can be administered by healthcare providers, family members, or patients themselves, and does not involve puncture of the skin.
We therefore found that the acupressure wristband is a good way to reduce nausea and vomiting for cancer patients receiving chemotherapy by applying it in the correct position with the stud over the pericardium 6 acupoint located on the anterior surface of the forearm, 3-finger widths up from the first wrist crease, and between the tendons of flexor carpiradialis and Palmaris longus.
Lee et al. (2008) encourage the application of acupressure bilaterally, rather than unilaterally, in CINV control. They recommend three minutes of finger acupressure once daily, with additional acupressure as needed, as the optimal intervention, because both three and five minute trials have succeeded in achieving positive effects. On the other hand, Molassiotis et al. (2007) claimed that there is no correlation between the frequency of pressing the studs and the level of nausea and vomiting. Lee et al. (2008) and Molassiotis et al. (2007) therefore claim opposite results in the relationship between CINV and the frequency of pressing the stud of an acupressure P6 wrist band. But when applying the acupressure P6 wrist band bilaterally, Lee et al. (2008), Said (2009), Molassiotis et al. (2007), Suh (2012), and Genç and Tan (2014) all reported a positive effect with P6 stimulation in reducing CINV.
We would like to discuss some factors related to CINV in relation to nausea and vomiting: expectancy and gender: Roscoe et al. (2003) argued that patients who received the acustimulation bands and expected them to be effective did report having a higher quality of life and less nausea, and in relation to gender, that women are more likely to experience nausea when receiving chemotherapy. Lee et al. (2008) say this may be caused by classical conditioning and also that breast cancer patients may have had a damaged median nerve due to axillary lymph node removal, but Lee et al. (2008) also mention that P6 acupressure in younger women had a significantly greater positive effect on delayed nausea than those on a placebo or those in the no-intervention control group. On the other hand, Molassiotis et al. (2007) mentioned that younger age is associated with greater nausea. We think that men may have tolerated greater stimulation of the acupressure points, and therefore experienced greater symptom relief, so it may be that the acupressure is more effective for men than for women, but these questions of gender, age and the frequency of pressing the studs would need further investigation.
Based on the reported studies, we support the belief that acupressure on P6 is applicable in clinical practice for CINV for cancer patients provided the required education, training and counselling is given to maintain the acupressure benefits.
Acupressure side effects
The study by Molassiotis et al. (2007) found that there were no side effects from the use of the wristbands, but one patient reported that she had to take the bands off because they were too tight and left her with marks for a few days. Chao et al. (2009) also mentioned that very few minor adverse events were observed.
Melchart et al. (2006) did report adverse effects from the treatment in five cases. One suffered a hematoma when wearing the acupressure band at P6. In the sham group, one hematoma was reported after acupuncture, and another three adverse effects from the acupressure band were reported (one hematoma, one skin irritation, one eczema). Hughes et al. (2013) also reported that participants had not experienced any restrictions from wearing the wristbands in terms of everyday activities, other than when washing and bathing. As one female participant commented, for most participants the wristbands were found to be comfortable to wear. However, a few participants reported that they had experienced minor irritation, such as the wristbands feeling tight or painful, or their wrists becoming itchy. Reported adverse side effects were generally deemed minor and acceptable. In the study by Said (2009), no side effect or discomfort was noticed from wearing the acupressure wristband. Said told the patients that if the bands caused discomfort, they could be removed for 30 minutes every two hours. In this way, by taking it off for regular periods, we can prevent the side effects of acupressure, even its minor and rare effects.
Acupressure reduces CINV in cancer patients, in addition it reduces anxiety (Genç and Tan 2014) and that affects overall quality of life (Said 2009). Quality of life is defined by the NCI Dictionary of Cancer Terms as “The overall enjoyment of life and the individual’s sense of well-being and ability to carry out various activities”. Based on the physiological components of the Virginia Henderson’s theory of basic human needs and Abraham Maslow’s Hierarchy of Needs, the patient needs to eat and drink adequately, and sleep and rest (Vera, 2014). This means that when we are providing the required management for distressing symptoms, such as nausea and vomiting, by including the acupressure wrist band in addition to standard antiemetics, the patient’s appetite will improve, leading the patient to eat and drink adequately and improve their sleeping pattern. These may then also improve other aspects of the cancer patient’s life. According to the Henderson Nursing Need Theory, when we meet a patient’s needs, it results in an improved quality of life for the cancer patient receiving chemotherapy. Another way of expressing this is that it restores the balance of Yin and Yang energy that leads to reduced nausea and vomiting and improves the patient’s ability to enjoy life and work in general through a maintaining of the harmony of body and mind, as described in traditional Chinese medicine (Cancer Research UK, 2015).
We believe that it is essential for cancer patients undergoing chemotherapy treatment to have adequate nutrition to maintain their strength to fight the cancer. Different nursing actions are necessary to maintain adequate nutrition including the relieving of CINV. From this we extrapolate that using the acupressure P6 wrist band to reduce CINV improves the patient’s quality of life.
CONCLUSION
Chemotherapy-induced nausea and vomiting may be life threatening and is therefore a huge challenge to nurses involved in cancer care. Even with the best pharmacological management of CINV, patients continue to experience nausea and vomiting.
From a review of eight articles with strong methodology, seven supported the positive effect of an acupressure P6 wristband in reducing CINV for cancer patients. This was also supported by other databases. The one article with neutral results showed that there was no difference between a combined acupuncture and acupressure treatment at P6 and at a sham point in relation to the nausea score, but the level of nausea was very low in both groups. We conclude that the acupressure wrist band applied to acupuncture point P6 is effective, safe, convenient, cost effective, an easy and self-administrated non-pharmacological intervention from traditional Chinese medicine that reduces CINV. Solving the problem of CINV is a fundamental nursing task that can lead to improved quality of life and nutritional status, reduced anxiety and increases patient compliance. In the light of these results, and due to the effectiveness and inexpensiveness of acupressure, together with its ease of use, we suggest that it should be used in conjunction with pharmacological agents for CINV prophylaxis. To maintain the effectiveness of the acupressure, special education and training is needed to reassure the patient that the acupressure is at the correct point (P6) and counselling by the nurse is required.
We recommend the use of acupressure P6 in oncology departments and that future research should be conducted to include cancer patients receiving radiotherapy, and to investigate more about the relationship between the frequency of pressing the stud on the wrist band for acupressure P6 and CINV, and the relationship between gender and CINV, and whether it is better to apply it unilaterally or bilaterally.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#Acupressure#Chemotherapy#Nausea and Vomiting#Cancer patients#Chemotherapy-induced nausea and vomiting#NCI#PICO#CINV#Mustargen#Zanosar#Platinol#Cytoxan#BiCNU#DTIC-Dome#Maher Battat#jcrmhs
4 notes
·
View notes
Text
SAS IN HEALTHCARE ANALYTICS

The Statistical Analysis System (SAS) is one of the most common and effective methods used in data analysis and statistical modelling. It is one of the fastest and most robust advanced analytics, multivariate analysis, business intelligence, data mining, data management, report writing, statistical analysis, application development, business modeling, and data warehousing software. SAS is an asset in various labor markets, as it holds the largest market share in advanced analytics jobs.
Position of SAS in the healthcare sector:
SAS is extensively used in the pharmaceutical and clinical research companies for clinical trial data analysis. SAS programmers play a key role in the study of data from clinical trials.
• A SAS programmer addresses the Healthcare industry's technical needs.
• Implementation of information technology in the healthcare delivery system helps gain valuable knowledge from data, and insight in recommending action or guiding decision-making, and improving the quality and practice of medicine in patient care.
• SAS analytical tools help accomplish corporate goals related to revenue generation, cost reduction, and strategic performance management in healthcare.
• To improve the overall quality of patient care, SAS instruments are used to investigate clinical outcomes and risk tolerances.
Role of SAS Developer:
Statisticians provide data analysis tools, apply analytical methods on the data obtained, and provide statisticians and or clinicians with the research overview tables, graphs, and data listing for writing study report.
SAS programmers work closely with statisticians and data managers to connect the raw data to the analysis.
SAS programmers can build the database in only a few businesses. To read database data to SAS data sets, SAS programmers must write programs and also generate a library of SAS formats.
SAS programmers can also write SAS programs to clean the data from the database according to CDM's edit requirements.
Through identifying the clinical trial to regulatory approval, SAS plays a significant role. The report for the clinical trial is compiled using the data produced in the SAS context.
SAS also plays a role in the development of protocols, the randomization process, developing CRFs, recording adverse events etc.
Future in SAS:
• Over the last few decades, the clinical SAS programming industry in India has seen rapid germination and the trend appears to continue for the next few years due to cost advantage and the availability of skilled labour.
• Because of the growing demand for professional services, programmers' desires have taken a different turn towards diversifying access, excessive wage growth due to various incentives and high expectations of career advancement.
• SAS analytics skills are, according to a recent survey, the most important skills to acquire in today's job market. The conventional health care model extends the career opportunities for SAS programmers. SAS has become a valuable tool to gage the current state and future vision of healthcare analytics.
• While inside the SAS programming environment there were a number of professionals working, they did everything but code. Another interesting fact about this data analytical tool is that most of the professionals who actually worked with it, were not Data Scientists, they actually weren't even Data Analysts. They were also the decision-makers, the highest tier of the companies who were responsible for
making decisions and would rather have to code for them a qualified specialist to help them accomplish their goals.
• Fast forward to today when the Data Science industry's SAS programmers get paid out as handsomely as ever. Over the last two, three decades, a Data Analyst's average annual compensation has risen twofold to nearly threefold. Because the compensation has increased, the obligations a specialist needs to take care of have not. Compared to those who have worked with SAS codes in the past , today there is a substantial increase in both the demands and roles of today's professionals. Today, SAS programmers are doing much more than just coding today, with the advent of big data, data science and big data analytics concepts.
• Now that we've effectively overcome our past and current questions about SAS programming status, let's concentrate more on the future of SAS programming. Over the last few years, the demand for this career option has increased significantly. Most importantly, this has resulted in such a progressive image is the knowledge of SAS programming and the field of data science. SAS is popularly regarded as one of the
industry's most popular data analytics tools. At the same time, it is also a licensed program which means that downloading is not free or easy. This is why many businesses this opt for SAS must buy the license to use the same.
• Although there are those who say it's a wonderful opportunity to work with SAS and the
future looks pretty promising for the same. At the same time, however, there are several questions about the use of open sourced data analytics resources such as R programming. So much so that there are lots of professionals who are currently employed with SAS but are still expected to work inside R. It may seem like
a threat to the future of SAS programming but then again there may be far less chances of a survival problem.
About Rang Technologies:
Headquartered in New Jersey, Rang Technologies has dedicated over a decade delivering innovative solutions and best talent to help businesses get the most out of the latest technologies in their digital transformation journey. Read More...
0 notes
Text
Aflibercept Biosimilars, Global Market Size Forecast, Top 4 Players Rank and Market Share
Aflibercept Biosimilars Market Summary
According to the new market research report “Global Aflibercept Biosimilars Market Report 2023-2029”, published by QYResearch, the global Aflibercept Biosimilars market size is projected to reach USD 10.4 billion by 2029, at a CAGR of 1.4% during the forecast period.
Figure. Global Aflibercept Biosimilars Market Size (US$ Million), 2018-2029
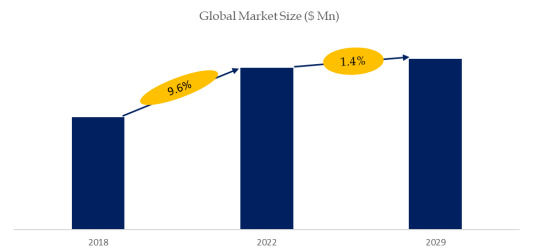
Above data is based on report from QYResearch: Global Aflibercept Biosimilars Market Report 2023-2029 (published in 2023). If you need the latest data, plaese contact QYResearch.
Figure. Global Aflibercept Biosimilars Top 4 Players Ranking and Market Share (Ranking is based on the revenue of 2022, continually updated)
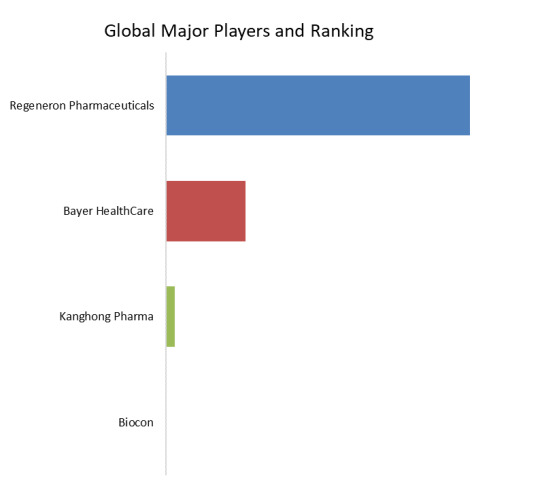
Above data is based on report from QYResearch: Global Aflibercept Biosimilars Market Report 2023-2029 (published in 2023). If you need the latest data, plaese contact QYResearch.
According to QYResearch Top Players Research Center, the global key manufacturers of Aflibercept Biosimilars include Regeneron Pharmaceuticals, Bayer HealthCare, etc. In 2022, the global top three players had a share approximately 100.0% in terms of revenue.
Figure. Aflibercept Biosimilars, Global Market Size, Split by Product Segment


Based on or includes research from QYResearch: Global Aflibercept Biosimilars Market Report 2023-2029.
In terms of product type, currently 2mg is the largest segment, hold a share of 100.0%.
Figure. Aflibercept Biosimilars, Global Market Size, Split by Application Segment
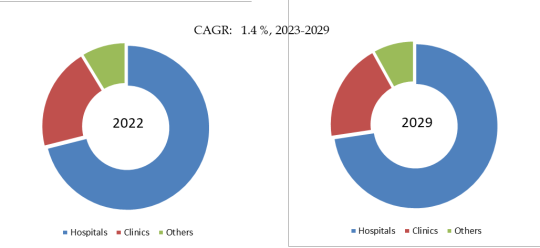

Based on or includes research from QYResearch: Global Aflibercept Biosimilars Market Report 2023-2029.
In terms of product application, currently Hospitals is the largest segment, hold a share of 71.1%.
Figure. Aflibercept Biosimilars, Global Market Size, Split by Region


Based on or includes research from QYResearch: Global Aflibercept Biosimilars Market Report 2023-2029.
Market Drivers:
Clinical Innovation and Advancements: Ongoing research and development, as well as innovations in the formulation or delivery of Eylea, can drive market growth. Advancements that improve treatment outcomes, reduce dosing frequency, or enhance patient convenience may positively impact the market;
Increase In the Number of Sick People: The prevalence of eye conditions such as AMD and DME, coupled with an aging population, contributes to the demand for effective treatments. Global demographic trends and an increasing burden of eye diseases can drive the market for Eylea;
Expanded Indications: Obtaining additional approvals for new indications can significantly expand the market for Eylea. As clinical trials demonstrate the drug's effectiveness in treating different eye conditions, regulatory approvals for these new indications can drive increased usage.
Restraint:
Patent restrictions become an important factor in entering the market;
The leading enterprises have a high degree of concentration, complete products and great competitive advantages;
Economic downturns and budget constraints within healthcare systems may impact the affordability and reimbursement of Eylea. Changes in economic conditions can influence the overall market for pharmaceuticals.
Opportunity:
Advancements in medical technology: Ongoing advancements in medical technology are expected to broaden the application of biosimilars in the treatment of cancer and eye diseases;
Increased treatment options for patients: The entry of Aflibercept biosimilars into the market will provide patients with more treatment options and the potential to reduce medical costs, presenting growth opportunities for the market.
About QYResearch
QYResearch founded in California, USA in 2007.It is a leading global market research and consulting company. With over 16 years’ experience and professional research team in various cities over the world QY Research focuses on management consulting, database and seminar services, IPO consulting, industry chain research and customized research to help our clients in providing non-linear revenue model and make them successful. We are globally recognized for our expansive portfolio of services, good corporate citizenship, and our strong commitment to sustainability. Up to now, we have cooperated with more than 60,000 clients across five continents. Let’s work closely with you and build a bold and better future.
QYResearch is a world-renowned large-scale consulting company. The industry covers various high-tech industry chain market segments, spanning the semiconductor industry chain (semiconductor equipment and parts, semiconductor materials, ICs, Foundry, packaging and testing, discrete devices, sensors, optoelectronic devices), photovoltaic industry chain (equipment, cells, modules, auxiliary material brackets, inverters, power station terminals), new energy automobile industry chain (batteries and materials, auto parts, batteries, motors, electronic control, automotive semiconductors, etc.), communication industry chain (communication system equipment, terminal equipment, electronic components, RF front-end, optical modules, 4G/5G/6G, broadband, IoT, digital economy, AI), advanced materials industry Chain (metal materials, polymer materials, ceramic materials, nano materials, etc.), machinery manufacturing industry chain (CNC machine tools, construction machinery, electrical machinery, 3C automation, industrial robots, lasers, industrial control, drones), food, beverages and pharmaceuticals, medical equipment, agriculture, etc.
0 notes
Text
Isolator Breaks Down Enabling Healthcare Data Silos

Presenting Isolator
To do this, they need a safe, secure method for testing or developing products that use sensitive data.
Particularly in the fields of healthcare and biology, generative AI has demonstrated its potential to make a big difference. This entails expediting the speed of clinical trials and medication discovery, lessening the administrative burden on physicians, and enhancing access to data and insights.
Google is excited to announce today at Google Cloud Next the launch of Isolator, a secure infrastructure and data processing solution that provides an essential extra degree of security to healthcare data used in cross-party collaborations. On Google Cloud, Isolator can provide multi-party cooperation on tasks involving the management of sensitive, regulated, raw, and unprocessed data in a private, secure, and compliant environment.
Isolator makes it far easier for various parties to collaborate on sensitive data projects than it ever has, and Google Cloud anticipate interest from throughout the industry in Isolator’s ability to inspire innovative technological solutions.
Here are a few instances where Isolator can be useful:
Creating custom models: Isolator can assist in creating bespoke models that automate labor-intensive administrative chores like producing discharge letters by utilizing Vertex AI and google cloud core models.
Leverage complicated data: At a cheaper cost than storing data on-premise, Isolator can accelerate the adoption of their Medical Image Suite, providing researchers and data scientists with the efficiencies to enhance processes.
Finding new treatments: By reducing development times, facilitating safe multi-party collaboration, and optimizing processes, Isolator can be used in conjunction with Google Multiomics Suite to streamline drug discovery and clinical trials.
Scaling sophisticated data analytics: By transferring and transforming data from compartmentalized, on-premise databases to feature-rich, massively scalable analytic and data processing platforms like Healthcare Data Engine and BigQuery, Isolator can help save money and improve outcomes.
Working together on research: Isolator excels at building, packaging, and sharing data sets that are used in research and model development. It can guarantee data integrity and increase transparency in all actions related to a data set.
Customers and their partners can utilize Isolator, which is available through Google Cloud’s Consulting Services, to build up an isolated instance within their IT environment. This enables them to deal with sensitive healthcare data workloads while upholding privacy, security, integrity, and traceability.
Additionally, by safeguarding data end-to-end, it can support Google customers in moving their workloads to Google Cloud and in establishing the safe limits required to build robust AI and machine learning models.
Fundamentally, Isolator is a system constructed using Chrome Enterprise Premium, Google’s widely-used Zero Trust technology that led the industry. In addition to other Google Cloud capabilities like VPC Service Controls, Without requiring users to set up and deploy specific devices, data loss prevention policies, or VPN connections, it may offer identity-based access that prevents data from leaving the secured environments. This is made possible by Chrome Enterprise and encryption at-rest, in-use, and in-transit.
Additionally, it is compatible with Google Confidential Space, which provides strong hardware isolation, encryption for data in use, and remote attestation capabilities for even more control.
Crucially, it also has built-in detection and warning features that record data access activities, find security setup errors, and notify of infractions. This can guarantee that the security teams working for the customers have complete control over who is allowed access to their private medical information.
As long as the security policies of the customer organization are consistently followed, learning resources are available on Google Cloud for any collaborator, from any device, anywhere in the globe. When an environment protected by this experiences a security breach, access to the data is halted until the required safeguards are put back in place.
At Google Cloud, They think that businesses and society at large will gain by sharing their expertise and resources to develop AI boldly and ethically. That strategy motivates us to develop products like Isolator. Organizations operating in the healthcare industry (and beyond) can benefit greatly from the revolutionary power that safe and secure collaboration can offer. Working in healthcare (and beyond) is transforming, which is one of the key reasons that Google Cloud has gained the trust of healthcare providers, payers, and researchers.
Isolator: Revealing Functionalities for Safe Medical Coordination
Here’s a closer look at Isolator, emphasizing its features that support effective and secure multi-party collaboration with medical records:
Information Security:
Granular Access Control: Precise access controls are possible with Isolator. Roles that grant particular access to read, change, or analyze only specified sections of a patient’s medical record can be allocated to users. This facilitates collaboration on pertinent areas and guarantees the protection of sensitive data.
Secure Enclave Technology: Imagine a safe deposit box inside of Isolator using Secure Enclave Technology. Within this enclave, private medical data is protected and only authorized people with the right decryption keys can access it. This cutting-edge technology provides an additional degree of security against unwanted access.
Audit Logs: Isolator keeps a thorough log of all actions and attempts at access.
Strong audit trails are made possible by this, guaranteeing responsibility and traceability in the event of any irregularities.
Features of Collaboration:
Real-time Data Sharing: Amongst authorized parties, Isolator enables real-time data sharing. Envision a physician seeking advice from an expert in a complicated situation. Isolator facilitates secure viewing and simultaneous discussion of pertinent sections of the patient’s medical record, thereby expediting communication and decision-making.
De-identified Data Analysis: Certain data points in a patient’s file can be made anonymous via Isolator. Collaboration in research or analysis is thus possible without jeopardizing patient privacy. Researchers can learn important lessons while strictly protecting patient privacy.
Channels for Secure Communication: The secure environment of Isolator facilitates effective communication amongst healthcare professionals involved in a case through built-in secure chat or message functions. As a result, there’s no need for unsafe communication methods suchemail, therefore protecting patient data even more.
Management of Compliance: Isolator can be set up to abide by pertinent data privacy laws such as the GDPR (EU) and HIPAA (US). By doing this, user confidence is maintained and legal issues are avoided.
By adding these functions, Isolator hopes to develop a safe and effective platform.
promotes cooperation in the field of healthcare, promoting improved patient care and scientific research.
Read more on Govindhtech.com
#govindhtech#news#technology#TechnologyTrends#technologynews#GoogleCloud#GoogleCloudNext#googlecloudplatform#isolator#googleisolator#machinelearning#artificialintelligence
0 notes
Text
Growing our donated organ supply
New Post has been published on https://sunalei.org/news/growing-our-donated-organ-supply/
Growing our donated organ supply
For those in need of one, an organ transplant is a matter of life and death.
Every year, the medical procedure gives thousands of people with advanced or end-stage diseases extended life. This “second chance” is heavily dependent on the availability, compatibility, and proximity of a precious resource that can’t be simply bought, grown, or manufactured — at least not yet.
Instead, organs must be given — cut from one body and implanted into another. And because living organ donation is only viable in certain cases, many organs are only available for donation after the donor’s death.
Unsurprisingly, the logistical and ethical complexity of distributing a limited number of transplant organs to a growing wait list of patients has received much attention. There’s an important part of the process that has received less focus, however, and which may hold significant untapped potential: organ procurement itself.
“If you have a donated organ, who should you give it to? This question has been extensively studied in operations research, economics, and even applied computer science,” says Hammaad Adam, a graduate student in the Social and Engineering Systems (SES) doctoral program at the MIT Institute for Data, Systems, and Society (IDSS). “But there’s been a lot less research on where that organ comes from in the first place.”
In the United States, nonprofits called organ procurement organizations, or OPOs, are responsible for finding and evaluating potential donors, interacting with grieving families and hospital administrations, and recovering and delivering organs — all while following the federal laws that serve as both their mandate and guardrails. Recent studies estimate that obstacles and inefficiencies lead to thousands of organs going uncollected every year, even as the demand for transplants continues to grow.
“There’s been little transparent data on organ procurement,” argues Adam. Working with MIT computer science professors Marzyeh Ghassemi and Ashia Wilson, and in collaboration with stakeholders in organ procurement, Adam led a project to create a dataset called ORCHID: Organ Retrieval and Collection of Health Information for Donation. ORCHID contains a decade of clinical, financial, and administrative data from six OPOs.
“Our goal is for the ORCHID database to have an impact in how organ procurement is understood, internally and externally,” says Ghassemi.
Efficiency and equity
It was looking to make an impact that drew Adam to SES and MIT. With a background in applied math and experience in strategy consulting, solving problems with technical components sits right in his wheelhouse.
“I really missed challenging technical problems from a statistics and machine learning standpoint,” he says of his time in consulting. “So I went back and got a master’s in data science, and over the course of my master’s got involved in a bunch of academic research projects in a few different fields, including biology, management science, and public policy. What I enjoyed most were some of the more social science-focused projects that had immediate impact.”
As a grad student in SES, Adam’s research focuses on using statistical tools to uncover health-care inequities, and developing machine learning approaches to address them. “Part of my dissertation research focuses on building tools that can improve equity in clinical trials and other randomized experiments,” he explains.
One recent example of Adam’s work: developing a novel method to stop clinical trials early if the treatment has an unintended harmful effect for a minority group of participants. “I’ve also been thinking about ways to increase minority representation in clinical trials through improved patient recruitment,” he adds.
Racial inequities in health care extend into organ transplantation, where a majority of wait-listed patients are not white — far in excess of their demographic groups’ proportion to the overall population. There are fewer organ donations from many of these communities, due to various obstacles in need of better understanding if they are to be overcome.
“My work in organ transplantation began on the allocation side,” explains Adam. “In work under review, we examined the role of race in the acceptance of heart, liver, and lung transplant offers by physicians on behalf of their patients. We found that Black race of the patient was associated with significantly lower odds of organ offer acceptance — in other words, transplant doctors seemed more likely to turn down organs offered to Black patients. This trend may have multiple explanations, but it is nevertheless concerning.”
Adam’s research has also found that donor-candidate race match was associated with significantly higher odds of offer acceptance, an association that Adam says “highlights the importance of organ donation from racial minority communities, and has motivated our work on equitable organ procurement.”
Working with Ghassemi through the IDSS Initiative on Combatting Systemic Racism, Adam was introduced to OPO stakeholders looking to collaborate. “It’s this opportunity to impact not only health-care efficiency, but also health-care equity, that really got me interested in this research,” says Adam.
Play video
MIT Initiative on Combatting Systemic Racism – Healthcare
Video: IDSS
Making an impact
Creating a database like ORCHID means solving problems in multiple domains, from the technical to the political. Some efforts never overcome the first step: getting data in the first place. Thankfully, several OPOs were already seeking collaborations and looking to improve their performance.
“We have been lucky to have a strong partnership with the OPOs, and we hope to work together to find important insights to improve efficiency and equity,” says Ghassemi.
The value of a database like ORCHID is in its potential for generating new insights, especially through quantitative analysis with statistics and computing tools like machine learning. The potential value in ORCHID was recognized with an MIT Prize for Open Data, an MIT Libraries award highlighting the importance and impact of research data that is openly shared.
“It’s nice that the work got some recognition,” says Adam of the prize. “And it was cool to see some of the other great open data work that’s happening at MIT. I think there’s real impact in releasing publicly available data in an important and understudied domain.”
All the same, Adam knows that building the database is only the first step.
“I’m very interested in understanding the bottlenecks in the organ procurement process,” he explains. “As part of my thesis research, I’m exploring this by modeling OPO decision-making using causal inference and structural econometrics.”
Using insights from this research, Adam also aims to evaluate policy changes that can improve both equity and efficiency in organ procurement. “And we’re hoping to recruit more OPOs, and increase the amount of data we’re releasing,” he says. “The dream state is every OPO joins our collaboration and provides updated data every year.”
Adam is excited to see how other researchers might use the data to address inefficiencies in organ procurement. “Every organ donor saves between three and four lives,” he says. “So every research project that comes out of this dataset could make a real impact.”
0 notes
Text
Growing our donated organ supply
New Post has been published on https://thedigitalinsider.com/growing-our-donated-organ-supply/
Growing our donated organ supply
For those in need of one, an organ transplant is a matter of life and death.
Every year, the medical procedure gives thousands of people with advanced or end-stage diseases extended life. This “second chance” is heavily dependent on the availability, compatibility, and proximity of a precious resource that can’t be simply bought, grown, or manufactured — at least not yet.
Instead, organs must be given — cut from one body and implanted into another. And because living organ donation is only viable in certain cases, many organs are only available for donation after the donor’s death.
Unsurprisingly, the logistical and ethical complexity of distributing a limited number of transplant organs to a growing wait list of patients has received much attention. There’s an important part of the process that has received less focus, however, and which may hold significant untapped potential: organ procurement itself.
“If you have a donated organ, who should you give it to? This question has been extensively studied in operations research, economics, and even applied computer science,” says Hammaad Adam, a graduate student in the Social and Engineering Systems (SES) doctoral program at the MIT Institute for Data, Systems, and Society (IDSS). “But there’s been a lot less research on where that organ comes from in the first place.”
In the United States, nonprofits called organ procurement organizations, or OPOs, are responsible for finding and evaluating potential donors, interacting with grieving families and hospital administrations, and recovering and delivering organs — all while following the federal laws that serve as both their mandate and guardrails. Recent studies estimate that obstacles and inefficiencies lead to thousands of organs going uncollected every year, even as the demand for transplants continues to grow.
“There’s been little transparent data on organ procurement,” argues Adam. Working with MIT computer science professors Marzyeh Ghassemi and Ashia Wilson, and in collaboration with stakeholders in organ procurement, Adam led a project to create a dataset called ORCHID: Organ Retrieval and Collection of Health Information for Donation. ORCHID contains a decade of clinical, financial, and administrative data from six OPOs.
“Our goal is for the ORCHID database to have an impact in how organ procurement is understood, internally and externally,” says Ghassemi.
Efficiency and equity
It was looking to make an impact that drew Adam to SES and MIT. With a background in applied math and experience in strategy consulting, solving problems with technical components sits right in his wheelhouse.
“I really missed challenging technical problems from a statistics and machine learning standpoint,” he says of his time in consulting. “So I went back and got a master’s in data science, and over the course of my master’s got involved in a bunch of academic research projects in a few different fields, including biology, management science, and public policy. What I enjoyed most were some of the more social science-focused projects that had immediate impact.”
As a grad student in SES, Adam’s research focuses on using statistical tools to uncover health-care inequities, and developing machine learning approaches to address them. “Part of my dissertation research focuses on building tools that can improve equity in clinical trials and other randomized experiments,” he explains.
One recent example of Adam’s work: developing a novel method to stop clinical trials early if the treatment has an unintended harmful effect for a minority group of participants. “I’ve also been thinking about ways to increase minority representation in clinical trials through improved patient recruitment,” he adds.
Racial inequities in health care extend into organ transplantation, where a majority of wait-listed patients are not white — far in excess of their demographic groups’ proportion to the overall population. There are fewer organ donations from many of these communities, due to various obstacles in need of better understanding if they are to be overcome.
“My work in organ transplantation began on the allocation side,” explains Adam. “In work under review, we examined the role of race in the acceptance of heart, liver, and lung transplant offers by physicians on behalf of their patients. We found that Black race of the patient was associated with significantly lower odds of organ offer acceptance — in other words, transplant doctors seemed more likely to turn down organs offered to Black patients. This trend may have multiple explanations, but it is nevertheless concerning.”
Adam’s research has also found that donor-candidate race match was associated with significantly higher odds of offer acceptance, an association that Adam says “highlights the importance of organ donation from racial minority communities, and has motivated our work on equitable organ procurement.”
Working with Ghassemi through the IDSS Initiative on Combatting Systemic Racism, Adam was introduced to OPO stakeholders looking to collaborate. “It’s this opportunity to impact not only health-care efficiency, but also health-care equity, that really got me interested in this research,” says Adam.
Play video
MIT Initiative on Combatting Systemic Racism – Healthcare
Video: IDSS
Making an impact
Creating a database like ORCHID means solving problems in multiple domains, from the technical to the political. Some efforts never overcome the first step: getting data in the first place. Thankfully, several OPOs were already seeking collaborations and looking to improve their performance.
“We have been lucky to have a strong partnership with the OPOs, and we hope to work together to find important insights to improve efficiency and equity,” says Ghassemi.
The value of a database like ORCHID is in its potential for generating new insights, especially through quantitative analysis with statistics and computing tools like machine learning. The potential value in ORCHID was recognized with an MIT Prize for Open Data, an MIT Libraries award highlighting the importance and impact of research data that is openly shared.
“It’s nice that the work got some recognition,” says Adam of the prize. “And it was cool to see some of the other great open data work that’s happening at MIT. I think there’s real impact in releasing publicly available data in an important and understudied domain.”
All the same, Adam knows that building the database is only the first step.
“I’m very interested in understanding the bottlenecks in the organ procurement process,” he explains. “As part of my thesis research, I’m exploring this by modeling OPO decision-making using causal inference and structural econometrics.”
Using insights from this research, Adam also aims to evaluate policy changes that can improve both equity and efficiency in organ procurement. “And we’re hoping to recruit more OPOs, and increase the amount of data we’re releasing,” he says. “The dream state is every OPO joins our collaboration and provides updated data every year.”
Adam is excited to see how other researchers might use the data to address inefficiencies in organ procurement. “Every organ donor saves between three and four lives,” he says. “So every research project that comes out of this dataset could make a real impact.”
#Algorithms#Analysis#attention#background#Biology#Building#collaborate#Collaboration#complexity#computer#Computer Science#Computer science and technology#computing#consulting#course#data#data science#Database#Diseases#domains#Economics#efficiency#engineering#Engineering systems#equity#federal#financial#focus#Graduate#postdoctoral
0 notes
Text
Join Syneos Health, a leading biopharmaceutical solutions organization, in a rewarding career opportunity. We are seeking a highly motivated individual to join our team as a Clinical Trial Assistant (CTA). Make an impact in the world of healthcare and advance your career with us. Apply now!
Job Title: Syneos Health Clinical Operations Specialist
Location: India-Asia Pacific - IND-Client-Based, India
Job ID: 23007113
Description: Join Syneos Health®, a leading fully integrated biopharmaceutical solutions organization, as a Clinical Operations Specialist. Our innovative approach and dedication to accelerating customer success make us a dynamic place to work.
Responsibilities:
Ensure compliance with Corporate and Clinical Operations Policies, SOPs, and Work Instructions
Support Clinical Monitoring staff and serve as a Sponsor representative for assigned sites
Maintain Trial Master File (TMF) and project files, including participating in audits
Prepare site manuals, reference tools, and other documents
Input clinical tracking information into databases and manage shared mailbox
Coordinate site supplies, materials, and team meetings
Handle Case Report Forms, Queries, and complete necessary training
Qualifications:
Life Science Graduate with a minimum of 2 years of CTA experience
Strong communication, interpersonal skills, and adaptability to new technologies
Ability to travel up to 25% as needed
[caption id="attachment_68585" align="aligncenter" width="1200"] Syneos Health Hiring Clinical Trial Assistant[/caption]
Why Syneos Health:
Career development and progression opportunities
Supportive Total Self culture where authenticity is valued
Building a diverse and inclusive workplace
Working with a global team dedicated to changing lives through innovative healthcare solutions
Apply Now: Apply online
Additional Information:
Tasks, duties, and responsibilities may vary. Equivalent experience and skills will be considered. This job description is not exhaustive and does not create an employment contract. Syneos Health is committed to compliance with applicable laws and providing reasonable accommodations when necessary.
0 notes
Text
data science trainig institute | Data Science Course With Placement | Data Science Certificate
Data science is a multidisciplinary field that uses scientific methods, algorithms, processes, and systems to extract insights and knowledge from structured and unstructured data. It encompasses various techniques from statistics, machine learning, data mining, and visualization to analyze and interpret complex data sets.

Content of Data Science:
Statistics: Understanding of statistical methods for data analysis, hypothesis testing, probability distributions, etc.
Machine Learning: Techniques and algorithms for building predictive models, such as regression, classification, clustering, and deep learning.
Data Mining: Extracting patterns and knowledge from large data sets using methods at the intersection of machine learning, statistics, and database systems.
Data Visualization: Presenting data in a graphical or visual format to facilitate understanding and interpretation.
Data Wrangling: Cleaning, transforming, and preparing raw data for analysis.
Big Data Technologies: Knowledge of tools and platforms for processing and analyzing large volumes of data efficiently, such as Hadoop, Spark, etc.
Domain Knowledge: Understanding of the specific domain or industry where data science is applied, such as finance, healthcare, marketing, etc.
Programming Skills: Proficiency in programming languages like Python, R, SQL, etc., and familiarity with relevant libraries and frameworks.
Uses and Benefits of Data Science:
Business Intelligence: Data science helps organizations gain valuable insights into their operations, customers, and market trends, enabling informed decision-making.
Predictive Analytics: By analyzing historical data, data science can forecast future trends and behaviors, allowing businesses to anticipate demand, optimize resources, and mitigate risks.
Personalization: Companies use data science to personalize products, services, and marketing campaigns based on individual preferences and behavior patterns.
Fraud Detection: Data science techniques are employed in detecting fraudulent activities, whether it's credit card fraud, insurance fraud, or identity theft.
Healthcare: Data science aids in analyzing patient data to improve diagnosis, treatment, and outcomes. It also helps in drug discovery and clinical trials.
Recommendation Systems: Data science powers recommendation engines in e-commerce platforms, streaming services, social media, etc., suggesting products, movies, music, or content based on user preferences.
Supply Chain Optimization: By analyzing supply chain data, organizations can optimize inventory management, logistics, and production processes, leading to cost savings and improved efficiency.
Risk Management: Data science assists in assessing and managing risks across various domains, including finance, insurance, and cybersecurity.
Social Impact: Data science is utilized in social initiatives like urban planning, disaster response, public health, and education to address societal challenges and improve the quality of life.
Overall, data science enables organizations to leverage data effectively to gain competitive advantages, drive innovation, and make data-driven decisions across various sectors and domains.
0 notes
Text

Facial flare-ups, encompassing various skin conditions such as acne, eczema, rosacea, and dermatitis, pose significant challenges to individuals worldwide. These conditions not only affect one's physical appearance but also have psychological and emotional impacts. Traditional treatment methods often involve trial and error, leading to frustration and ineffective outcomes. However, the integration of artificial intelligence (AI) in dermatology has opened new avenues for managing facial flare-ups effectively. This article explores the role of AI solutions in revolutionizing skin care, offering personalized, efficient, and innovative approaches to address facial skin conditions.
Understanding Facial Flare-ups: Facial flare-ups result from a multitude of factors, including genetics, hormonal imbalances, environmental triggers, and lifestyle choices. Acne, for instance, is commonly associated with excessive sebum production, bacterial growth, and inflammation. Eczema and dermatitis involve skin inflammation triggered by allergens or irritants, while rosacea manifests as redness, visible blood vessels, and often, pimple-like bumps. Managing these conditions requires a comprehensive understanding of their underlying causes and individualized treatment plans tailored to patients' unique needs.
The Role of AI in Dermatology: AI technologies, including machine learning and computer vision algorithms, have revolutionized dermatological care by enhancing diagnosis, treatment selection, and outcome prediction. Dermatologists can leverage AI-powered tools to analyze vast datasets of patient images, medical records, and clinical research to make informed decisions. These tools not only assist in identifying skin conditions accurately but also offer insights into disease progression and treatment responses.
Automated Diagnosis: AI-driven diagnostic systems can analyze images of facial skin to identify specific conditions with high accuracy. By comparing patient images to extensive databases of dermatological images, these systems can recognize patterns indicative of acne, eczema, rosacea, or other skin disorders. This automated diagnosis expedites the evaluation process, allowing for timely intervention and treatment initiation.
Personalized Treatment Plans: AI algorithms excel in analyzing diverse datasets to identify patterns and correlations between patient characteristics, treatment modalities, and treatment outcomes. By considering factors such as age, skin type, medical history, and environmental triggers, AI-powered systems can generate personalized treatment plans tailored to each individual's needs. These plans may include topical medications, oral medications, lifestyle modifications, or procedural interventions optimized for efficacy and safety.
Predictive Analytics: AI models trained on longitudinal patient data can predict disease progression and treatment responses with remarkable accuracy. By analyzing factors such as treatment adherence, lifestyle changes, and environmental exposures, these models can forecast the likelihood of flare-ups, enabling proactive management strategies. Dermatologists can use these insights to adjust treatment regimens preemptively, minimizing the risk of exacerbations and improving long-term outcomes.
Telemedicine and Remote Monitoring: Innovations in telemedicine platforms equipped with AI-enabled functionalities facilitate remote consultations and follow-ups for patients with facial flare-ups. Through secure video conferencing and image sharing capabilities, dermatologists can assess patients' skin conditions remotely and provide timely guidance on treatment adjustments. AI algorithms integrated into these platforms can analyze patient-submitted images for changes in lesion appearance, aiding in remote monitoring and early detection of flare-ups.
Challenges and Considerations: Despite the remarkable potential of AI in dermatology, several challenges and considerations must be addressed to ensure its widespread adoption and efficacy. Data privacy and security concerns regarding patient information storage and transmission are paramount, requiring robust encryption protocols and adherence to regulatory standards such as HIPAA. Additionally, AI algorithms must be continuously validated and updated to account for evolving clinical knowledge and diverse patient populations. Integration into clinical workflows and clinician training are also essential to maximize the benefits of AI technologies while minimizing disruption to established practices.
Conclusion: The integration of AI solutions in dermatology represents a paradigm shift in the management of facial flare-ups and other skin conditions. By harnessing the power of machine learning, computer vision, and predictive analytics, dermatologists can deliver personalized, efficient, and evidence-based care to patients worldwide. From automated diagnosis to personalized treatment plans and predictive analytics, AI-driven innovations hold the promise of improving patient outcomes, enhancing access to care, and transforming the landscape of facial skin care. As research and technological advancements continue to unfold, the future of dermatology lies at the intersection of AI and personalized medicine, ushering in a new era of skin health and well-being.
0 notes
Text
Study maps main genes involved in immune response to infection by dengue virus
- By Maria Fernanda Ziegler , Agência FAPESP -
By comparing data for the immune response to natural infection by dengue virus to data for activation of the immune system by dengue vaccines, researchers at the University of São Paulo (USP) have identified molecular markers that could be used in the development of novel vaccines and treatments for dengue.
They also reiterated the efficacy of two vaccines already available on the market: Q-Denga, manufactured by Takeda Pharma (Japan) and now being distributed by the national health service in Brazil (Sistema Único de Saúde, SUS); and Dengvaxia, produced by Sanofi-Pasteur (France). Both are live attenuated virus vaccines.
“We analyzed the data systemically and found various similarities between the immune response elicited by vaccines and the immune response to natural infection. Of course, vaccines induce an immune response without the damage done by the virus. We were also able to characterize several pathways [that involve signaling between defense cells]. The interferon pathway [mediated by this antiviral protein produced by leukocytes – white blood cells – and fibroblasts] proved to be crucial, with several important genes that can be considered novel biomarkers of the disease,” Otávio Cabral-Marques, a professor of molecular medicine at the University of São Paulo’s Medical School (FM-USP) and principal investigator for the study, told Agência FAPESP.
The study was supported by FAPESP via two projects (18/18886-9 and 20/01688-0) and reported in an article published in the journal Frontiers in Immunology. It is the first to identify immune signatures of dengue by systems vaccinology, an approach that explores the complex interactions underlying vaccine-induced immunity in humans.
The researchers analyzed 955 transcriptome samples from patients with natural dengue infection and participants in clinical trials of dengue vaccines (the transcriptome is the complete set of RNA molecules in the organism). They obtained the data from a public database.
They found 237 differentially expressed genes common to both the patient samples and trial participant samples. “Based on 20 of these shared genes, we were able to create a panel to distinguish disease severity, especially in the late acute stage. We also used machine learning techniques to classify ten predictors [immune signatures] of disease severity in cases of natural infection. These are crucial to the immune response to the virus,” said Desirée Rodrigues Plaça, first author of the article and a PhD candidate at USP with a scholarship from FAPESP.
Dengue is caused by four viral serotypes (DENV-1 through DENV-4) and, when symptomatic, progresses through three clinical stages: febrile (initial acute), critical (late acute) and recovery.
Interferon pathway
“There are many differences, but we also found many similarities between the immune responses induced by vaccines and natural infection. By funneling the dataset, we identified 20 genes that are common to both processes and similarly expressed. They are responsible for enriching the immune system’s protective pathways, especially the type I and type II interferon pathways,” Plaça said.
Interferons are cytokines whose main role is to inhibit viral replication. They trigger a chain reaction that affects several molecules. According to the article, the interferon antiviral pathways are not only responsible for early (front-line) defense, but their complex biological functions also set the stage for development of robust and lasting adaptive immunity.
“The interferon pathways are very important to activate the adaptive response, which consists of T cells and B cells [types of white blood cells called lymphocytes] and provides permanent protection [as do vaccines]. It’s extremely important therefore to know which genes associated with the interferon pathways are key drivers of the adaptive response that affords the best protection,” Placa said.
Genes
With the information they obtained in the study, the researchers were able to develop therapeutic strategies to inhibit, activate or induce expression of genes involved in the immune response, opening up possibilities for the investigation of targeted therapies for dengue fever.
They identified the main genes (such as OAS2, ISG15, AIM2, OAS1, SIGLEC1, IFI6, IFI44L, IFIH1 and IFI44) involved in orchestrating various aspects of the adaptive immune response. OAS2 and OAS1 have antiviral functions, while ISG15 restricts virus replication, for example. AIM2 activates the inflammasome, a multiprotein complex of the innate immune system that when activated produces molecules that tell the system to send reinforcements to the infection site, initiating pro-inflammatory responses crucial for effective antiviral defense.
SIGLEC1 participates in immune cell interactions, facilitating antigen presentation and adaptive immune recognition. IFI6, IFI44L and IFI44, all of which are interferon-inducible, are implicated in modulation of apoptosis (programmed cell death) and antiviral defense. IFIH1 is a crucial sensor in shaping adaptive responses to RNA viruses such as dengue. IFIT5 and HERC5 “are known for their roles in interferon-mediated inhibition of viral replication”, the authors note.
“The many relevant genes involved in this complex process underscore the intricacy of the link between the initial antiviral pathways and subsequent adaptive immune processes. It’s as if the beginning and end of a story were joined up,” Cabral-Marques said.
The article “Immunological signatures unveiled by integrative systems vaccinology characterization of dengue vaccination trials and natural infection” is at: www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2024.1282754/full.
This text was originally published by FAPESP Agency according to Creative Commons license CC-BY-NC-ND. Read the original here.
--
Header image: The study identified similarities between the immune response to natural infection and the immune response elicited by the vaccines Q-Denga and Dengvaxia. Credit: Fabio Rodrigues-Pozzebom/Agência Brasil.
Read Also
Butantan Institute’s dengue vaccine protects 79.6% of those vaccinated, study shows
#dengue#virus#genomics#brazil#immunology#vaccine#vaccination#public health#health#infectious diseases
0 notes
Last Seen Blogs

heatwzves
idk what to title this :"]

stgloria
SAINT GLORIA

beepinout
beepinout

oniruby
Kiyo 🏮

maw-n-paw-blog
Find Your Own Way...