#physical diagnosis
Text
How We Found That Gosh Darned Appendix Before We Had Ultrasound Machines and CT Scans
Hi. I'm a nurse and I teach physical diagnosis. You wanna know about the appendix, right? One of the most common intestinal appendages to feature in fanfic*?
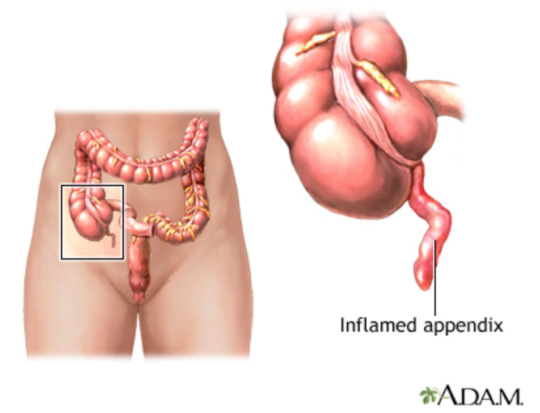
What is an Appendix?
The appendix is a hollow little worm-shaped appendage that sticks off the end of the cecum- that area between the small intestine and the large intestine.
Most of the time it's just laying there doing its thing. It's "thing" being holding an excess of gut bacteria. Most of the time that's great- the bacteria in our guts do a lot for us- many of us couldn't comfortably drink milk or get energy from calciferous vegetables without them. And we lose those bacteria all the time with diarrheal illness, antibiotics, and a host of other ways. It's a rough world for gut bacteria.
Fortunately, since the appendix has some in reserve, it can push some back out to re-populate. It's not wholly necessary for life, because those bacteria will probably show back up at some point, but it's a nice little backup system.
But with this nice little backup system full of bacteria, we also sometimes have problems. Since the opening from the appendix into the intestine is so small, it sometimes gets blocked. When that happens, the bacteria keep chugging along, making more bacteria and more waste, which builds up pressure. Eventually, that pressure inside the appendix overwhelms the blood pressure that is carrying nutrients to the appendix, and it begins to die. When the walls of the appendix get sufficiently weak, the appendix perforates, sending bacteria-filled goo into the otherwise sterile sac that holds the abdominal organs. This causes a massive infection called peritonitis that leads to death about 20% of the time (as evidenced by WWII submariner data, as this was before modern antibiotics and surgical intervention was impossible on a submarine, making this population significantly more ethical to study than alternatives).
Thinking About the Appendix:
Since about 8.6% of men and 6.4% of women will get appendicitis in their lifetime (I suppose in a quirk of statistics our non-binary pals do not get appendicitis), a 1-in-5 chance of death is pretty significant. A surgical appendectomy can drop this 20% to less than 1.8% (in adults), which makes it the intervention of choice.
But in order to surgically remove an appendix, we first have to find it. And to find it, we have to suspect it. You may hear of the "classic" symptoms being loss of appetite, pain that starts at the belly button and migrates to the lower right abdomen, nausea, and vomiting. This happens in about 50% of patients.
Everyone else is... weird. They probably have nausea and vomiting, but so does everyone else who comes in with abdominal pain, and there's a lot of things that cause abdominal pain. So it's really something to keep in the back of your head, do a couple physical maneuvers, and if they come up positive, you have like an 80% chance that it's appendicitis.
Medicine is an art, and all that.
NOTE: using a CT scan will bring your correct diagnosis rate up to about 98%, but they're hella expensive. You probably have hands, your patient probably has pain receptors. As I like to tell my students, physical diagnosis is free.
Now on to the finding. These suckers are elusive AF. Are they in front of the cecum? Behind the cecum? On the other side of the abdomen? Hanging out up under the liver? Like a foot long for some reason and causing problems in multiple places? The answer is yours to find out.
What we're looking for in trying to find the appendix is where it's causing inflammation. When the appendix gets inflamed, that inflammation spreads to surrounding structures. Since we know where those structures are, we can generally assume where the appendix is. This is important so we don't have to make a bigger hole than necessary.
What Is McBurney's Point Anyway?
Let's start by talking about McBurney's Point. It's a location that is classically referred to as where the appendix lives. That's true in about 4% of cases, though something like 64% of appendixes live within 5cm of that location, so at lest that pushes us in the right direction.
To find McBurney's Point, find your right iliac crest- that front upper bony part of your pelvis. Then draw a line from your belly button to that location. 2/3 of the way down that line is McBurney's Point.

Around this area is where you're going to be looking for pain and tensed muscles (called "guarding" in medical lingo).
The Physical Diagnosis Part:
Start by pressing very lightly in other areas of the abdomen (don't @ me about auscultating first- I'm assuming you already did that), looking for guarding. If the guarding only occurs around McBurney's point, that should really raise your suspicion for appendicitis. Despite the likelihood of the appendix being more than 5cm away, guarding covers a fair distance (possibly that whole lower right quadrant) and about 96% of people with appendicitis will have guarding on the right side. Guarding might also be everywhere if the appendix has already perforated.
The next thing you're going to do is press your flat hand pretty hard on the other side from where you felt the guarding. This is called a Rovsing Sign. Usually this is the left side you're pressing on. Pressing somewhere far away should still make the guarding-place painful, because it stretches the structures around where the guarding is happening. Since those are inflamed, stretching them should hurt.
A few other ways to do this include tapping on the right heel, having the patient cough (Dunphy Sign), or tapping in various places on the abdomen and seeing where the pain is. A particularly asshole move is having the patient stand on their toes and drop suddenly onto their heels, causing a lot of pain where inflammation in the abdomen is (Markle Sign). Most people aren't that mean, Dr. Markle.
By now you essentially know that something in the right lower quadrant is inflamed. If your history lines up with appendicitis, you can probably presume to keep looking for an inflamed appendix.
Pressing slowly downwards on McBurney's Point (or at least, where most of the pain was when doing the above signs), and then quickly releasing the pressure (causing a lot of pain with release of pressure) can tell you if the front lining of the abdomen is inflamed, and the appendix is probably hanging out in the front.
The Obturator Sign is looking for inflammation in the lower pelvis, one of the places the appendix might be hanging out. To do this, you have the patient bend their knee to 90* while laying on their back. You then pushes the knee away from yourself while pulling the foot towards yourself. This stretches a muscle in the lower pelvis that would be inflamed if the appendix was sitting next to it.

To see if the appendix is behind the cecum, use the Psoas Sign. For this, the patient lays flat on their back, and you push on their thigh while they try to raise their leg. If that causes pain in the back part of their abdomen, the Psoas (tenderloin) is inflamed, and the appendix is probably back there.
Doing all of these and getting a bunch of positives (lots of pain all in the expected area(s)) gives you somewhere between a 60% and 80% chance of having found a case of appendicitis. It might also be other things like an intestinal blockage, perforation of something else, blood or irritating fluid in the abdomen, or something else. You'll probably need to do a lot of this repeatedly. The only way to know for 100% is to surgically remove the appendix and look at it. By physical diagnosis alone about 10-20% of appendectomies are done on healthy appendixes.
Good luck in the hunt!
-Ross
*heavily biased toward whump fanfic. I'm not sure what intestinal appendages feature on other corners of AO3 and nor do I want to
190 notes
·
View notes
Note
hi! there’s something i've been wondering about for a long time and hope you can help me out with. i understand that x-rays/ct scans/mri/etc are important to be able to determine the extent of injuries and such but in an emergency situation, is there time for those procedures? or are there other/quicker ways to accurately determine what is going on and how to deal with it? i hope you can answer this for me because it has been on my mind for so long now…
There's generally a lot more time than you think in emergency situations. Or time can be created by giving fluids or intubating a patient, or a number of other interventions.
There are a finite number of situations where a time delay of a minute or two is actually critically important. These are emergencies like an airway blockage (choking, swelling, trauma to the airway, etc..), lack of breathing, extreme blood loss (spurting arterial blood), or the heart not pumping blood.
All of the above can be assessed and supported without imaging. You can intubate someone with an airway problem, intubate and/or provide rescue breathing for someone who is not breathing, put pressure or a tourniquet on someone who is bleeding out, and perform CPR on someone who's heart is not pumping until you can solve the problem that is causing the heart to not pump (or determine that you cannot solve this problem).
Everything else, including heart attacks, strokes, large-scale trauma, and many other things, can spare the time to do EKGs, x-rays, CT scans, and ultrasounds. MRIs are typically not done in emergencies because ain't nobody got time for that, like, ever.
X-rays take literal seconds. You can do them in a brief enough pause in CPR to make them worth it. It's literally "pause CPR-turn the patient-shove the x-ray pad under the patient-roll pt back- snap the pic-roll patient-remove x-ray pad-roll patient-keep doing CPR". The pic can be evaluated right on the machine less than a second later.
You can do ultrasounds literally while CPR is being done. No pauses needed. They can be read right there.
You can set up for a 12-lead EKG while CPR is being done, pause for like 6 seconds while it's being recorded, and go right back at it.
CT scans take minutes, so you're probably not going to do them during CPR, but you would for a stroke or major trauma because it can give a lot of info very quickly that can help make decisions.
Now, modern imaging is really important for a lot of reasons. It's faster and more specific in a lot of cases than other methods, and most modern docs really genuinely don't have the training to do their jobs without them (with the exceptions of very rural or austere practitioners) even when there are technically other ways to get similar information.
HOWEVER, since you happened to ask someone who is a literal physical diagnosis (the practice of diagnosing through history and physical examination) and wilderness first aid instructor, I can say that a lot can *technically* be done without imaging at all.
You can get really close to knowing where a clot in the brain is based on physical exam (something that would generally be done (honestly faster) with a CT scan). You can very accurately tell how bad a pneumothorax or hemothorax is and figure out where to put a chest tube through percussion and physical maneuvers (something you'd generally use a CT or x-ray for). You can locate and treat a life-threatening cardiac tamponade with a long needle and a 3-lead EKG, after diagnosing it with physical exam (something you'd otherwise need ultrasound for). You can tell a bone is broken and what muscles were impacted and whether or not it actually needs surgery with physical exam (usually done with x-ray or CT or even MRI later). You can tell that a problem is appendicitis and even locate where an inflamed appendix is with physical maneuvers (usually done with an ultrasound or CT). These and so many, many more things.
We typically do imaging because it is faster and can (in theory) be more accurate. In the last 40 or so years, practitioners have not been trained to be particularly accurate with physical diagnosis- just trained enough to realize there is a problem that can be further elucidated with imaging. This training takes a LOT of time to be particularly skilled at, and there is already too much information crammed into 4 years of medical school and 3-7 years of residency, and much of what is prioritized is not physical diagnosis (okay, I will get off my dang soap box).
We also do a lot of imaging because insurance expects it and generally feels it is less likely to miss something than physical diagnosis (which I believe is more a problem with training than actual accuracy of the medium). Unfortunately, in prioritizing interpretation of imaging over performance and interpretation of physical exam, we have created an extremely expensive model of diagnosis. The time you'd have to pay a practitioner for to do even a very detailed physical exam costs a hell of a lot less than the price of a single CT scan.
But from the 1910s through 1980s (when computers got good enough to do advanced imaging efficiently), we were pretty dang good at using physical diagnosis exclusively or backed up with more basic (and cheaper) tests like EKGs and x-rays. But like I said above, I'll get off my soap box.
-Ross @macgyvermedical
#whump reference#writing reference#injury#hospital life#medical education#physical diagnosis#medical imaging#medblr#nurblr
128 notes
·
View notes
Text
ILY people who are continually wrong about their self diagnoses
being right about self diagnosis isn't what makes self diagnosis okay. it's a process, and you're learning. it takes time to find answers and just like doctors can be wrong in their suspicions so can you.
figuring out what condition you have is hard and I'm proud of you for taking steps towards finding the right answers. being wrong is okay and is even a valuable part of the process of ruling things out. sometimes it's not a horse, sometimes you're just a zebra, and you can't know you're a zebra without making sure you're not a horse first.
#this is about the diagnosis process for rare diseases but idc if other people relate to it#it's just a very frustrating process to suspect something so badly to the point your doctors agree#just for it to never be what you suspect#chronic illness#chronically ill#cripple punk#physical disability#physically disabled#cripplepunk
615 notes
·
View notes
Text

having lyrics addressing how mental health is just completely dismissed coupled with all that religious imagery in the staging hits incredibly hard when the cultural mindset in serbia is one of "mental illness isnt real you just need to go to church"
#eurovision#in corpore sano#when i told one of my closest friends about my autism diagnosis her response was#'autism doesnt exist in serbia because we tell ppl to go to church and god helps fix their psyche'#and that 'in the west its different because they dont trust god'#if you have a problem that isnt physical it just means u arent believing in god hard enough#and with how few mental health resources are even available faith kinda does become the only solution#like i shit on england a lot but as an autistic person with adhd and anxiety im SO GLAD i only lived in belgrade for a few years#quasigh
8K notes
·
View notes
Text

The Almighty Sheriff!
Save a horse, ride a cowboy~
#respecfully sir: AWOOGA arf arf bark AWOOGA#If this gets 30 notes I'll take his shirt off for yall lol#with his top surgery scars Of course#Ive seen that's a super popular HC for him and I think thats great! Good for him!#Farm boi#no fr working in a farm makes you develop muscles that you didnt even know you had#having flashbacks from highschool when they made us work in the garden for two hours under the scorching afternoon sun#I went to a highschool that was all Ooo we are green thumbs and we shall teach the young ones how to plant and harvest their own food#and my god that shit was so physically demanding mate#i didnt had my diagnosis on how horribly mangled my body was So I had to work in the farm thing like all the others and try not to pass out#even the jocks that were fit and always running and playing football during all the recesses were dead quiet after working outside#and all that those classes did for me was to create a hatred for working in any type of gardening activity so they failed spectaculary lol#SO ANYWAYS my point is Starlo can defo deadlift bags of 70kg\150lbs with one arm without breaking a sweat#undertale yellow#uty#Starlo#Starlo uty#north star uty#myart
176 notes
·
View notes
Text
Normalize being professionally diagnosed and supporting people who don't have a diagnosis actually
#coming from your local dxed disabled person#pro self diagnosis#pro self dx#physically disabled#mentally disabled#actually disabled#disabled#disability
564 notes
·
View notes
Text
As a kid my family used to make fun of me for stuff that is apparently exclusively reserved for “old people” like rolling across the room in a rolly chair to grab something (instead of getting up and taking three steps) or sitting down at a table to do quick food prep like cut fruit or scramble an egg (instead of just standing at the counter for 90 seconds) TURNS OUT what they called laziness was just disability all along haha TURNS OUT I just needed a mobility aid yet here I am today still without one because they gaslit me into believing I was “just lazy” and it took me decades to finally understand that’s not true. haha who knew
#I used to think everyone was just way stronger than me like I was the human version of the runt of the litter or something#please take kids seriously about things#fucking hell I hate this world#disability advocacy#physical disability#undiagnosed disability#late diagnosis#autistic trauma#spoonie#pots#dysautonomia#ehlers danlos#ehlers danlos syndrome#low energy#disability accommodations#disability representation#laziness does not exist#fuck ableists#family trauma#disability trauma#fuck ableism#anti fakeclaiming#fuck fakeclaimers#invisible disability#invisible illness#mobility aid#mobility aid user#disability pride
99 notes
·
View notes
Text
i'll die on this hill: it is NOT ableist for glass children to be resentful of their disabled sibling. you're not a bad person, you're not a bigot.
#eve's posts#glass child#glass child syndrome#ableism#especially when they or your family weaponizes their diagnosis#and this obviously is not limited to people with siblings with physical disabilities#tbh people whose siblings have adhd or autism or other neurodivergencies aren't talked about enough
117 notes
·
View notes
Text
in a world where ableist able-bodied doctors won’t give a fuck about physically disabled people, self diagnosis is always okay, and good.
#goes for other types of disabilities too but this is a cripple punk blog#cripple punk#crip punk#cripplepunk#physical disability#physically disabled#c punk#cpunk#self diagnosis
693 notes
·
View notes
Text
Hey for disability pride month, shout-out to people with "less than marked" diagnoses!
If you've got something with "unspecified" or "otherwise" in your diagnosis name, this one is for you! Your disorder is still real. You are still struggling with something and if that something causes you to need accommodations or causes you to struggle in your day to day life, you can still call yourself disabled. You still deserve the accommodations and care that someone who has a more concrete diagnosis. Your disability is real, your symptoms are real. As frustrating as it is, being classified with an "other" disorder is still disordered and your symptoms are enough. I love you!!!
#osdd#udd#schizophrenia spectrum#actually psychotic#PDNOS#UPD#im sure im forgetting tags#and im sure there are physical equivalent to this type of diagnosis too#this is from my own personal frustrations and what i need to hear so
139 notes
·
View notes
Note
What's the most insane bit of physical diagnosis you know? (The bit with lifting the legs and moving them around to diagnose appendix inflammation made me go :000)
Honestly all of physical diagnosis is wild. There are so so many weird things that the human body does, and even weirder things that we figured out to tangentially find problems with it.
I wish physical diagnosis was more rigorously taught, or at least had more time allotted to it (currently students get about 8-20 total hours/semester for 2 years, some of which is testing) where I teach. Cause damn it would be fun to get into all the fiddly bits of abdominal signs, musculoskeletal, and neuro. You can learn so freaking much from a neuro exam that isn't just memorizing the cranial nerves. You can generally tell where in the brain a stroke occurred, and tenuously what kind of stroke it was, with a 20-minute exam (not that any doctor ever has 20 whole minutes with a patient, but still).
And not to sound like a fuddy-duddy but PD is quick n cheap compared to nearly all high tech alternatives. What you can figure out from PD is a little inferior from what you might get with a CT or ultrasound, but for a trained practitioner it's close enough.
As serious and high-stakes as we like to think medicine is, only very specific things in medicine need to be super accurate. You need to be about 85% sure what the problem is, then you're either going to do some kind of surgery about it, or give some kind of medicine. Either way, if it doesn't work, you try something else. Human bodies are weird af and don't conform to a textbook ever.
Anyway, off my soapbox, here's some cool physical diagnosis things to try at parties:
Percussion: Need to find if a thing under the skin is solid (like liver), full of liquid (like acites in the abdomen), or full of air (like the gastric bubble or lung)? Look no further than this poor man's ultrasound! Take the middle finger of your non-dominant hand and find the last joint, called the DIP. Press the DIP down against the part of the body you want to hear like this:

Then, with the tip of your dominant middle finger (or a knuckle, or reflex hammer I'm not picky) tap hard directly over the DIP. Really throw your wrist into it. You want a callus to form over that DIP.
You'll hear a sound that will mean absolutely nothing to you. But try in a few different places and you'll start to be able to calibrate. Percuss in the following areas and note the difference in sound: Upper right chest (lung, gas), lower right chest (liver, solid), anywhere on abdomen (probably gas, or a mix of gas and solid), thigh (muscle, solid). Make sure you're pressing down really hard with the DIP and not percussing over bone (between ribs is okay).
As you get more and more comfortable with this, you can start "mapping out" abdominal/thoracic organs in people (or dogs. dogs love this for some reason)- particularly the spleen, liver, diaphragm, lungs, and heart. Once you get REALLY good at this, you can use percussion to find tumors and pneumonia in lung tissue (find a solid thing in the lung? Probs a tumor. Find liquid in the lung? Heart failure or pneumonia depending on where it is), and quantify liquid in the abdomen or bladder, among many other things.
Am I putting the BladderScan company out of business with this illicit knowledge? No. But that's just cause everyone likes a number, and while I can't do much more than "full" or "not full" or "really full oh sh*t really full", the bladder scanner can snarkily say ">999".
McMurphy's Sign: Think someone might have inflammation in their gallbladder (cholecystitis) due to a blockage or stones? Mash down with your hand just below the right lower edge of their rib cage. Hold your hand there pushed in and have them take a deep breath. Do they stop breathing suddenly because it hurts real bad? Cholecystitis.
Allen Test: Your hand has 2 arteries that bring blood to it. Both of them work about equally well when you're healthy. But let's say you have to do something that might endanger one of these arteries (say, an arterial line, or you need to snake a catheter from the wrist to the heart). You need to make sure that the other one works well enough that if you totally destroy the other one, the patient won't lose their hand.
So basically to do this, you have someone lay their hand palm up on a table. Put a thumb over each side of the wrist (feel a bone, a bundle of tissue, and another bone across the wrist, and your thumb should be in the divot between the tissues bundle and the bone on each side) and press down. Have your patient make a fist and then relax it. The palm should be white, because you've just squeezed all the blood out of it and aren't letting any back in because you've occluded the arteries.
Then you're going to release pressure on one side. The hand should pink up within a second or two. Then repeat with the other side. If the hand pinks up twice, you've got enough blood flow to do your thing with one of the arteries.
Bruits Over the Carotids (and other places): As people get older, they build up plaque in their arteries. This can cause narrowing of blood vessels throughout the body, and if it gets bad enough, can prevent blood from flowing to various organs. This can cause severe hypertension (if the blood isn't getting to the kidneys), angina (if the blood isn't getting to the heart muscle), or syncope (if the blood isn't getting to the brain.
If you take a stethoscope and listen over the carotid artery, you can tell about how bad this is by how much noise the blood makes moving through the artery at each beat. This sound is called a bruit (pronounced brew-ee). While you can sometimes hear bruits in the abdomen, they are usually hard to localize. The condition of the carotids makes a good proxy for other less-find-able arteries. So someone has hypertension that meds are struggling to treat and a carotid bruit? Maybe look into the condition of their renal arteries and see if a stent would solve their blood pressure issues.
164 notes
·
View notes
Text
me when i get the official diagnosis for a health issue by a specialist on the first fucking appointment after years of battling with medical professionals: *surprised pikachu face*
#actually disabled#disability#physical disability#crip punk#invisible disability#chronically ill#physically disabled#cpunk#chronic illness#chronic disability#disabled#disabilities#diagnosis#cripple punk#cripplepunk#c punk#actually chronically ill#invisible illness
50 notes
·
View notes
Text
I feel like people misunderstand how finally being listened to and having a diagnosis, a "reason" for what's wrong.
Because, I my family was pretty sure they knew what was wrong with me, it was just a struggle to find someone who was able to test and confirm or deny what was going on. I would tell people that my family doctor suspected what I had based on my family's history and people would ignore that because it wasn't written in my chart so I must be doing it for attention. So yeah I was relived when I got diagnosed because it was confirmation of what I suspected but more so because it allowed me and my doctors to know what treatment to do and what to not do.
However being diagnosed with an incurable problem was devastating, I didn't want it to be true, I was desperately hoping that I did not have it because I knew what that would mean. I didn't want to be diagnosed I wanted to be told definitively that I did not have this and it was some other fixable thing. Not just dismissed I wanted the doctor who said it was in my head and all somatic to be right because that was somthing I knew could be treated and had the possibility of remission. I did not want it to be real.
I feel like that's an important thing to recognize that yes, I was happy to finally know what was wrong but having that confirmation was also incredibly devastating.
#disabled#disability#actually disabled#physical disability#mental illness#physically disabled#actually physically disabled#cripple punk#crip punk#diagnosis#self diagnosis#proffesional diagnosis#chronic disability#chronic illness#chronic pain
20 notes
·
View notes
Text
I’ve been up for three hours. Now seems like a good time to have a nap.
#basically the story of my life at this point#it’s kinda depressing actually#I last a few hours before I feel incredibly tired again#and everyone thinks my life is so nice cuz they wish they could sleep#even tho I feel wrecked when I wake up again#*sigh* maybe I am just lazy tho#it’s not like I have a diagnosis that explains why I laze around every day#then act like my life is so hard#chronic fatigue#chronic illness#chronically ill#disabled#disability#physically disabled#nagichi talks
85 notes
·
View notes
Text
i think we need to remind people that being chronically ill unfortunately does not make you a health expert and statements like "long covid is just CFS" ignores the like 800 other long-term effects of covid that are grouped under "long covid" that distinctly aren't in line w/ PEM
#op#site culture#covid19#my friend's immune system is shot after covid. he keeps getting food poisoning to an unreasonable extent. that's lumped under 'long covid'#the increased intolerence i have to physical activity now is possibly due to my covid infection. which would be long covid. but it's not#an intolerence the likes of PEM bc it quite literally has to do w/ physical endurance rather than 'crashing.' that's diff from PEM#but if it is due to covid - it would be long covid. & neither of those things are enough to warrent a cfs diagnosis#and evidence for the role of mitochondrial dysfunction in CFS is 'contradictory' not 'well-known' and 'clearly understood'#covid deniers being scientifically illiterate doesn't mean we need to be scientifically illiterate in the opposite direction
23 notes
·
View notes
Text

yeah that!
#In fact as I understand it having a diagnosis CAN detriment you#Which sucks but hey society#I work with people with mental and physical disabilities and one woman who is like 40 JUST NOW got diagnosed with autism#When like. Shes had assistance with it for years and years. The diagnosis is literally just words on paper#Also I grew up with a licensed therapist who denied anything being wrong with me ever and still does! So just idk#Know yourself and do whatever it takes#Not an art#Talky talky Tuesday
92 notes
·
View notes
Last Seen Blogs
malegains
Horny AI Nonsense

xxkarassxinxthexcpuxx
stinky guy

carmendeedragons
I *hug of doom* the whole world

2piel
Segunda Piel

rottinggdeer
swagilistic