#and there's at least some evidence that it's more common with '''high functioning''' autistic people
Text
Seeing arguments pitting bipolar and autistic people against each other when you're bipolar and autistic:
#missed this gif lol#but seriously the possibility that there's actually considerable overlap between autism and mood disorders seems to elude people#even though it's very well established!#major depression is more common in both the general population and among autistic people#but bipolar disorder is also very considerably more widespread among autistic people than in the general population#and there's at least some evidence that it's more common with '''high functioning''' autistic people#anghraine rants#rare breed of attack unicorn#gif#political shenanigans and codependent siblings
18 notes
·
View notes
Text
Hey there! I’m wondering if you could help me type someone? I’m fairly sure she’s Fe-dom, but I also see some Se-dom and Ne-dom traits that make me question things, so I’ll try to provide some evidence for each axis.
Fe-Ti:
She’s incredibly outgoing and personable which really lends well to her day job of being a hairdresser. She can connect with people from all walks of life instantly and can talk with them for hours. She actually told me a really sweet story recently about how she helped a young autistic client overcome his fear of haircuts by sitting patiently with him at the salon for an hour and talking to him about video games he is into. Her ability to disarm people’s fears and put them at ease is incredible. She moonlights as a synthwave artist, and really loves the collaborative nature of making music with others. She’s also always the first to volunteer to cook at get togethers because she says cooking for people is an expression of love. She never hesitates to say what she is feeling and always wants to resolve disagreements right away.
However, she has a reeeeally hard time being detached and thinking logically. For example, a couple of times we’ve tried to discuss politics, but it always becomes circular because she’s settled on the idea that “politics aren’t even important! Why do people fight over them? We’re all human! Can’t we all just get along?” She shows very little interest in building a system of understanding for herself and just wants “love and good vibes” and told me that I “just don’t understand because I’m a Virgo(???)”, at which point I burst every aux-Ti vein in my ENTP forehead.
This all sounds 2-core ESFJ with a 9 and a 7 fix (let’s not talk about anything that causes dissent or trouble or unpleasantness, because we all share this important, vital thing in common that we are all people, so we should all live in harmony together! =).
Se-Ni (Forgive me if I mess up here, as I’m not as familiar with these functions, being an ENTP):
Always the first to jump into things… to varying degrees of success. She can be really impulsive under stress, frequently blowing her money on things that she thinks “look cool”. She has a huge weakness for falling for people way too fast too - she’s literally moved cities to be with “the one” after only knowing them for two weeks (she’s done this at least twice that I know of). I also think that Se might be somewhere in her stack because she seems to rely on (and often overindulge) in sensory things to relax like food, pot, alcohol, and sex. <- this seems like high emotion/sensation emphasis in general, a social variant dominant (so/sp or so/sx, which is more likely, and could make an ESFJ more risk-taking, as long as it’s to be with THE ONE I LOVE), and being an image type (2w3?).
[…]
Ne-Si:
I really wanted to rule out Ne, but for every long term plan that seems solid and works out for her, she seems to have 50+ ideas on the go, or that get left on the cutting room floor. For example, she writes about twelve songs at a time - slowly switching between them and chipping away at each one until they are finished - which really resonated with my own work methods as a Ne-dom. She also, like me, comes up with a lot of ideas that seem to come as quickly as they go (ex: “I should buy and sell Pokemon cards - they’re a great investment!”, “I should make a YouTube channel and act out loads of comedy skits on it!”, “I love this new thing I learned about last week and I want to get a tattoo of it!”). I will say that it weirdly feels different from my Ne-Si… I can’t put my finger on why, though. I think this is either where my own type bias is confusing Ne with Se or Ne-dom with Ne-tert.
Yeah, I’d say she’s Ne, specifically SiNe with a lot of attachment to lower Ne… the “slowly chipping away at multiple songs” thing is fairly typical of SiNe; to have a lot of things going at once, but to be methodical about actually finishing them.
15 notes
·
View notes
Text
trying to put some.....assorted but related realizations into words
(Reminder that the part of the sqrl that best perceives/recognizes interpersonal behavior patterns is barely verbal and the part of the sqrl that is hyperlexic basically also has what some parts of academia/the medical establishment classify as "nonverbal learning disorder"
a huge part of my cognitive processing is (invisibly to most outside my skull) actually consumed by an eternal process of clumsy and sometimes immensely frustrating pantomime/pictionary exchanges between those two)
(Also reminder that one reason "Journaling" without involving at least conceptually an audience is largely useless for the sqrl is that for some no-doubt-amusing-to-the-Creator reason, "breakthroughs" in the above-referenced pantomime/pictionary process are much more likely when the idea of other personalities I have interacted with is "plugged into" the communication "equation".
Lenses. Catalysts.)
anyways
I put into words this morning that one reason the whole "identify the most important sentence in the paragraph" concept is so intensely counterintuitive to me is that a certain, significant part of my method for cognitively processing existence - having some understanding of anything - is oriented towards gestalts and synergies
actually (Epiphany!) this is another Autistic Sqrl Binary that confuses [other] humans
I have scripts and I have..... whatever this gestalt/synergistic/responding-to-patterns form of understanding is.... I don't have a lot that conceptually spans the gap between
Details belong to the part of me that runs scripts
The other part of me is more concerned with.... conceptual shapes... conceptual.... functions (in the mathematical sense) from which theorized points can be inferred/deduced. (This part of me manifests from those shapes and functions epiphanies which can be used to patch scripts that proved insufficient, to create new scripts)
While specific details have value..... especially details conceptually tagged as critical/foundational (an example might be the allergies, triggers, squicks of a being particularly important to me) my focus in interpersonal interaction, interpersonal understanding is more focused at shapes, currents, functions
There is a difference in how I react to the way someone remembers/forgets things about me that I am not sure is often recognized. Forgetting a detail is one thing but revealing a lack of awareness of a pattern/shape/function/current is something else
I will never perceive the desire of one person to map the currents of another person as inherently transgressive absent evidence that the mapping person is inclined to use that information in a manipulative, deceptive, controlling fashion. To me the desire to map the currents of another person is never inherently motivated to manipulate, deceive, control - that is a separate choice made by an individual person, a separate inclination of specific individuals.
Humans are multifaceted beings and it makes sense to me that if one wishes to interact with a particular human being in a way that is not constrained by a specific context.... that mapping that person's currents in more than just one.... gulf..... one... shore... is appropriate
ok..... I can tell I am drifting away from common language
Mapping a person's currents is a form of love to me.
The idea of people who indicate a desire to be cherished..... and yet..... find it transgressive to have their currents mapped..... has been..... a recent big deal
It is one thing, to me, to communicate to someone that.... they have been judged not to be someone with whom a close relationship is desired
but
the contradiction of "relational potential for us requires that you do not desire to map my currents or for me to ingest/digest any awareness of the shape of your currents" is intensely cognitively disturbing to me
I have been.... high volume.... because only by making my currents as mappable as possible did it seem that I could ever find those who found my currents appealing
but the idea that my **currents**, **the very shape of my being** will most likely always be considered **coincidental** to relationship with me.....
will even be considered by some as **necessarily a distraction** to relationship with me
is overwhelmingly discouraging
what is the point of seeking relationship with beings so utterly alien????
1 note
·
View note
Text
Dealing with Stress When You Live in a Rough Place
This isn't necessarily tarot or shadow work, but I wanted to write a little bit about strategies I've found useful for dealing with my neighborhood in it's current state. All of this can apply to managing stress generally but I'm focusing on folks in my boat. I'm incredibly sleep deprived so it's going to be rambly - I'm warning you now. But hopefully this helps someone.
I've shared a little bit about what's been going on in other posts; we hear shootings at least weekly, people will play loud music so loud the window rattle really late at night, all out brawls have broken out in the parking lot, our neighbors bang against the walls even in the middle of the night, most our neighbors have made it clear they don't like us because we're gay, we've had our car broken into at least 2 in the last month, kids have taken to beating our cars with sticks, climbing on and under them, screaming in front of our house, beating on our door and running off - like y'all it's a lot!
I talk about this so folks can know where I'm coming from. Some folks read this and they're horrified, some folks are going to read that and be like fuck that's tame. How hard a situation looks really does depend on what your normal is and how you were raised. For me, it's pretty intense. I was raised in out in the country so I didn't grow up living really close to people like I have to here in the city. And country neighborhoods have their own brand of rough, do not underestimate it, but most of what I've compiled here is going to be about living in close proximity with other people in areas with high crime rates.
Mindset Shifts
The Sooner You Accept Your Lack of Control - The Better
And I mean really accept it. Not just intellectually understanding that there's not anything you can do, but getting as okay with that as you can manage. For folks who are already traumatized that's a whole lot harder to do. Living in a space that traumatizes you daily will also make that harder as time goes on. But it's been some of the most important work I've done while living in a place that this. Sometimes I cope by being very public about what I'm going through, sometime I cope by
Sensory Management is Not a Luxury, It is a Necessity
This has become overwhelmingly clear to me that sensory overload in rough neighborhoods is a wildly underdiscussed health issue. There's measurable health differences in people who are exposed to a lot of noise versus those who aren't. I'm autistic so this is something I have to do just to function but I've seen a huge shift in my girlfriend's mental health since living here too. Take it seriously and try to attend to it just like you would any other health concern, making it a part of your routine. This is where adapting Polyvagal strategies has come in handy.
Good is Still Good Even If There's a Ton of Bad
There are very few moments of pure joy in a neighborhood like this. One of the reasons that a gratitude practice has been genuinely helpful is that it's shown me how much good can get swept away in the tidal wave of crap in a place like this. So that I don't feel helpless or internalize how worthless places like this are designed to make you feel, I try to resist by reflecting on the good. IT helps me feel like my life still has meaning while I'm living here and it's not a waste to be right where I am right now.
I Am Not Failing Myself For Not Getting Sleep, Food, Safe, Etc
I'm lucky that we've been good on food but sleep and safety have been in short supply. I realized I often felt like I was a bad person for being in this situation where I couldn't sleep, I criticized myself for not being able to sleep through all the noise and getting worked up. I have to remind myself daily that I'm not failing myself for what I can't really control. I'm not a bad person because of what people around me choose to do.
Polyvagal Strategies Adapted
Nature
Ideally, when you're trying to regulate your nervous system, you'd want to get out into nature more. It's just flat out not accessible or safe to do so here. I'm lucky that my room faces a nice tree and when I'm getting stressed, I take some time to just sit and really look at it. I try to notice the details. I also really enjoy feeding birds on my window sill. I invested in a big bag of bird seed with some Christmas money that's lasted me at least a year now but I used to get bags for about 5 dollars at Kroger. If you can't get close to nature, lure it to you.
Need something totally free? You can also pull up livefeeds of bird feeders on YouTube. I used to watch them when I couldn't walk to put out birdseed. Still very helpful. Nature cams in general are great. Put on a nature doc like Planet Earth. Change your computer and phone backgrounds to have natural landscapes. Even just sketching landscapes and having landscape are around your space can help.
If you can buy some soil, dig some up, or swipe some from a public garden bed, you can grow some small plants on your window sill. You can grow a lot of seeds from vegetables and some fruits you get at the store. You can also collect seeds from trees and try to grow them (it's difficult, plant several at a time). Take cuttings of plants you can identify as safe. Extension services will also sometimes send seeds for free. Taking care of a plant really helps us spend more time in the restorative part of our nervous system.
Sound
At the intersection of sound and nature is nature noises. If you're trying to block out your neighbors anyways, nature noises are the best option. I've had the best luck rain and storm sounds. Water noises in particular have a calming effect on our nervous system. If I really need to block something out I'll layer a rain generator over some music I like (rain sounds + Elliot Smith = a vibe).
Music in general can have different activating and calming effects on our nervous system. Pay attention to what music activates you and makes you more likely to be in conflict with people when you listen to it and what music makes you more social. Physically relaxation is harder for me personally to gauge. As a person with trauma I can't always tell when my body is relaxing or not. So paying attention to how I treat others helps me check myself.
Temperature + Touch
When we're warmer, we tend to feel more socially connected than when we're cold. Put on some extra clothes, pile on the blankets, take a bath, or grab a space heater if you have one. It's worth increasing the temp a little if you're stressed. Too hot and we can begin to feel crowded out. So if you're feeling the need to flee, it's worth trying to cool off a little. I usually do this by splashing some cool water on my face.
While we crave touch from others, touch from ourselves also helps calm our nervous systems! Jin Shin Jyutsu has been super helpful for me. There are a few videos online. I recommend searching Facebook for a woman local to me - Jennifer Bradley. I took one of her in person classes before the pandemic and it's been very helpful especially around sleep. I think the only place she's got her recent videos up is on her Facebook page but they're worth tracking down. She's a very good teacher and just a very soothing presence in general.
There's some evidence that just imagining being hugged or held is calming on the nervous system. Some goes for imagining ourselves out walking in nature. Don't be afraid to spend time daydreaming!
Breath + Movement
A lot of unsafe neighborhoods make common advice like going for a walk completely out of the question. However, even just moving more around your space can help. Yoga has been very helpful to me. My partner finds bodyweight exercises really help her. Any movement you feel good doing counts. Including movement you imagine yourself doing as well.
Breathing is movement, or seems to have a similar effect at least. I really recommend checking out a few breath work strategies to use. You've always got your lungs on you so it's easy to use. I like the in for 4 counts, hold for 7, release for 8 pattern. Breath is a direct line to the nervous system and I try to do a breathing pattern several times a day just to regroup.
Cognitive Strategies
Journal Like Your Life Depends on It
I'm not joking. TMS journaling - journaling stream of consciousness very intensely for about 20-30 minutes and then destroying what you've written - has been key not only to me surviving this place but having fewer Fibro flares than when I was living in much calmer places. But honestly all journaling is helpful. I've been keeping a daily journal in Notion and that alone has been helpful. Making sure I've gotten as much as possible off of my mind throughout the day has helped so much. Find a journaling strategy that allows you to take the cognitive load of (or a few) and practice them as often as you can. Not into journaling? I used to take videos of myself talking into the camera and save or delete them depending on whether I wanted to come back to them. Are words rough? Draw your feelings or scenes as you saw them.
Find the Story That Works
There are a bunch of conflicting ideas about what the right view of trauma and the story of it is. I personally really hate any narrative that places me as a victim. For better or worse, I like to look at what I've learned in any giving situation. So in my current situation, when I'm overwhelmed, I remind myself that I'm only getting a glimpse of what some people in places like this go through. It's increasing my empathy and expanding my awareness which allows me to better serve others. It's made me more committed to keeping my materials accessible over profiting. There's been a lot of benefit when I frame it that way. And that works for me. If that story isn't helpful for you - work to find a frame to narrate your experiences - as they're happening - that help you feel more whole.
Conclusion
I'm not sure if these strategies will work for other people but I wanted to at least have something out there than people could hopefully find if they're struggling with the same thing. Basically, if you can't fix it - manage it. Find ways to make the experience less traumatic if you're able to. Manage your sensory input. Do what you can with what you have where you are. Too many folks will tell you that you absolutely have to change your material circumstances before you can address mental health but for many of us that's just not possible. Or in the words of one of my favorite Buddhist teachers, Robina Courtin, "If you can do something, do something, but if you can't, what are you going to do?"
82 notes
·
View notes
Link
There are three kinds of dissidents: (a) anons, (b) pundits who still care what people think, and (c) outsiders who DGAF. All these groups are great; real greatness can be achieved in any of them; and good friends I have in each. But each has its problems.
…
The problem with (b) is that you are always policing yourself. Not only do your readers never really know what you really believe—you never really know yourself. In practice, it is much easier to police your own thoughts than your own words. When choosing between two ideas, the temptation to prefer the safer one is almost irresistible. This is a source of cognitive distortion which the anons and outsiders do not experience. (Though anons do suffer something of the opposite, a reflex to provoke.)
As a pundit, you sense this stress in every bone of your body; you can never show it to your readers. This creates a deep dishonesty in the parasocial relationship between writer and reader—like a marriage that can never escape some foolish first-date fib. The falsity, like the blue in blue cheese, flows through and flavors every particle of your content. Neither you nor your readers can ever be sure whether you are speaking the truth, lying to them, or lying to yourself—but you are constantly doing all three. You may still be very entertaining—enlightening, even. All your work is ephemeral, and once you die only your relatives will remember you. And it’s not even your fault.
…
From my perspective, both the anonymous and official dissidents exhibit a kind of unserious frivolity, but a very different kind. The frivolity of the anon is imaginative, surreal and playful at best, merely puerile at worst. The frivolity of the pundit has no upside; in every paragraph he is breaking Koestler’s rule, and he knows it; the best he can do is to shut up selectively about the things he cannot write about.
And his mens rea, too, is awful. He is selling hope. He is selling answers. Pity the man whose life has brought him to the position of selling answers in which he does not believe, or which he is forced to believe, or which he must force himself to believe. However sophisticated and erudite he may be, he is just a high-end grifter. His little magazine is a Macedonian troll-farm with a PhD. He is lucky if his eloquent essays about the common good don’t appear above a popup bar peddling penis pills—and in fact, I know more than one brilliant scholar in precisely this bathetic position. The frame defines the picture; the context sets the price of the text. Sad!
Worst still must be the reality that bad punditry is worse than useless—since useless strategies for escaping from a real problem are traps. When you lead your readers toward an attractive but ineffective solution, you lead them away from the opposite.
You got into this business to change the world for the better. You cannot avoid the realization that you are changing it for the worse—because your objective function is that of Chaim Rumkowski, the Lodz Ghetto’s “King of the Jews.”
You exist to convince your own followers that they neither can nor should do anything effective. The easiest way to do this is to convince them that ineffective strategies are effective. And this, as we’ll see, is exactly what you cannot avoid doing, dear pundit.
Moreover, from our present position of profound unreality, where the official narrative shared and studied by all normal intelligent people and all prestigious institutions can only be described as a state of venomous delirium, the opportunities to play Judas goat are almost unlimited. Cows, remember: there does not have to be only one Judas goat.
…
A particular favorite of the pundit is the error that AI philosophers call the “first-step fallacy.” It turns out that the first monkey to climb to the top of a tree was taking the first step toward landing on the moon:
First-step thinking has the idea of a successful last step built in. Limited early success, however, is not a valid basis for predicting the ultimate success of one’s project. Climbing a hill should not give one any assurance that if he keeps going he will reach the sky.
When a vendor sells you the moon and ships you a rope-ladder, you’ve been defrauded. Time for that one-star review.
…
Today we’ll chart the edges of the legitimate possible by looking at three recent pundit essays which have done a fine job of exploring those edges, and maybe even expanding them: Richard Hanania’s “Why is Everything Liberal?”, Scott Alexander’s “The New Sultan”, and Tanner Greer’s “The Problem of the New Right.”
…
After reading Hanania’s essay, a fourth pundit (who is out as a radical conservative) asked me: why does the right always lose? “Narcissistic delusions,” I replied.
Which was far from what he expected to hear, or what most readers will take from the essay. All three of these essays are good and true; but their inability to go far enough leaves them pointing their audience in precisely the wrong direction.
Most readers will emerge feeling that conservatives need more and better narcissistic delusions. Indeed, both pundit and politician are right there with just such a product. This meretricious frivolity, posing as seriousness, is too egregious to leave unmocked; yet the right reason to mock it is to challenge it to assume its final, truly-serious form.
Richard Hanania and the loser right
Hanania’s true point—backed up with a ream of unnecessary, PhD-worthy evidence—is that the libs always win because they just care more:
…
Since the rebirth of conservatism after the revolutionary monoculture of World War II, all conservative punditry has consisted of attempts to create more excitement around policies and values which effectively resist the power of the prestigious institutions—giving “normal people” as much to care about as their fanatical, aristocratic enemies.
Sensibly, this tends to involve raising “issues” which actually seem to affect their lives, but which also run counter to aristocratic power. Over decades, the substance of these issues changes and even reverses; the opposite stance becomes the useful stance; and “conservative values” have no choice but to change to reflect this. (If this seems like a liberal way to rag on conservatives—the cons learned it from the libs.)
…
“New Right” is not Greer’s term, but as a label I can barely imagine a worse self-own. It promises something ephemeral and irrelevant. So far as I can tell, this same cursed label has been used in every generation of conservatism to mean something different. When it inevitably fails and dies, people forget about it, and the next generation, stuck in the eternal present of a Korsakoff-syndrome movement, can reinvent it.
Who reads the conservative pundits of the ‘80s? Even those who remember them have to throw them under the bus. Every generation of National Review twinks, solemnly intoning what they conceive to be the immortal philosophy of our hallowed founders, is horrified by its predecessor, and horrifies its successor—a truly bathetic spectacle. And of course, each such generation would utterly horrify the actual founders.
…
Greer then goes deep into David Hackett Fischer territory to explain the obvious, yet important, fact that this “New Right” consists of upper-class intellectuals (inherently the heirs of the Puritans, since America’s upper-class tradition is the Puritan tradition) trying to lead middle-class yokels (the heirs of the Scotch-Irish crackers, and (though Greer does not mention this) Irish, Slavs, and other post-Albionic “white ethnic” trash, today even including many Hispanics. He even gives us a clever historical bon mot:
Pity the Whig who wishes to lead the Jackson masses!
Uh, yeah, dude, that would be called “Abraham Lincoln.”
But the point stands. Not just the “New Right” with its new statist ideology, but the whole postwar American Right, is a weird army with a general staff of philosophers and a fighting infantry of ignorant yokels. How can this stay together? How can the philosophers bring forth a mythology that creates passionate intensity in the yokels?
…
There is wisdom in this madness, of course—the problem is caused by aristocrats whose minds are wholly given over to narcissistic delusions. Doesn’t it take fire to fight fire? Doesn’t it take passionate intensity? Isn’t passionate intensity generated only by myths, dreams, poems and religions, not autistic formulas for tax policy? So the answer is clear: we need more and better narcissistic delusions. Ie, shams.
After all, any “founding mythology” is a narcissistic delusion. The flintlock farmers and mechanic mobs of the 1770s, and the Plymouth Puritans of the 1620s, have one thing in common: none of these people even remotely resembles the megachurch grill-and-minivan conservative of the 2020s. None of them even remotely resembles you.
They did live in the same places, and speak sort of the same language. Otherwise you probably have more in common with the average Indonesian housewife—at least she watches the same superhero movies.
To Narcissus, everything is a mirror; in everything and everyone, he sees himself. No field is riper for narcissism than history, since the dead past cannot even laugh at the present’s appropriations of a human reality it could not even start to comprehend.
And fighting fire with fire is one thing, but fighting the shark in the water is another. For the aristocrat, transcending reality is a core competence. The essence of leftism—always and everywhere an aristocratic trope, however vast its ignorant serf-armies—is James Spader in Pretty in Pink: “If I cared about money, would I treat my father’s house this way?” Mere peasants can never develop this kind of wild energy: that’s the point.
Yet Hanania remains right about the amount of energy that a rational, Kantian agenda for productive collective action motivated by collective self-interest, or even collective self-defense, can generate. The grill-American suburbicon is like Maistre’s Frenchman under the late Jacobins: he has defined deviancy down to rock-bottom. “He feels that he is well-governed, so long as he himself is not being killed.”
O, what to do? When you are solving an engineering problem and see the answer at last, it hits you like a thunderbolt. The conservatives, the normal people, the grill-Americans, must accept their own low energy. They must cease their futile reaching for passionate intensity, whether achieved through Kantian collective realism or Jaffaite founding mythology. They must fight the shark on land.
Conservatives don’t care—at least not enough. Yet they want to matter. Yet they live in a political system where mattering is a function of caring—not just voting. Therefore, there are two potential solutions: (a) make them care more; (b) make systems that let them matter more, without caring more.
Conservatives have low energy. They want high impact—at this point, they need high impact. After all, once you yourself are being killed, it’s kind of too late. Any engineer would tell you that there are two paths to high impact: more energy, or more efficiency.
Conservatives vote but don’t care. If we don’t have a viable way to make conservatives care more—meaning orders of magnitude more—effective strategies and structures must generate power by voting, not caring. They must maximize power per vote.
…
Interference means voters who are on the same team are working against each other. Impedance means voters resist delegating their complete consent to the team.
Interference is like a bunch of ants pulling the breadcrumb in different directions. To eliminate interference, point all your votes at one structurally cohesive entity which never works against itself.
Impedance is like getting married for a limited trial period, so long as your wife stays hot and keeps liking the stuff you like. As Burke pointed out in his famous speech to the electors of Bristol, the fundamental nature of electoral consent is unconditional:
To deliver an opinion, is the right of all men; that of Constituents is a weighty and respectable opinion, which a Representative ought always to rejoice to hear; and which he ought always most seriously to consider.
But authoritative Instructions; Mandates issued, which the Member is bound blindly and implicitly to obey, to vote, and to argue for, though contrary to the clearest conviction of his judgement and conscience; these are things utterly unknown to the laws of this land, and which arise from a fundamental Mistake of the whole order and tenor of our Constitution.
The cause of electoral impedance in the modern world is the conventional concept of “agendas” or “platforms” or “issues.” When you vote not for a cohesive entity, but for a list of instructions you are giving to that entity, you are not voting your full power. You are voting for Burke’s opponent, who felt “his Will ought to be subservient to yours.” In effect, you are voting for yourself. Narcissism once again rears its ugly head.
When you vote an agenda, you are granting limited consent to your representative. You say: I vote for you, for a limited time, so long as you stay fit and cook tasty dinners. I am actually not voting for you! I am voting for “reforms for conservatives” (Hanania). I am voting for “a broad set of shared attitudes and policy prescriptions” (Greer). Dear, I am not marrying you. I am marrying hot sex, regular cleaning and delicious meals—till ten extra pounds, or maybe at most fifteen, do us part.
You implicitly withhold your consent for anything not on your jejune list of bullet points. Then, you wonder why your representatives have no power and are constantly mocked, disobeyed, tricked and destroyed by people who are legally their employees. This is not political sex. This is political masturbation. You voted for yourself. And instead of a baby, all you got was a wad of tissues. Nice way to “drain the swamp.”
Your vote does not work because you are not voting, delegating, or granting consent. You are like an archer with one arrow who, afraid of losing it, refuses to let go of it. Without releasing his dart, all he can do is run up to the enemy and try to stab.
So if conservatives want to maximize the impact of their votes, all they have to do is the opposite of what they’re doing. Instead of voting for the okonomi a-la-carte stupid little political menus of hundreds of unconnected candidates and their staffs, they can all vote for the omakase prix-fixe chef’s-choice of a single cohesive governing entity.
Such a power, elected, has the voters’ mandate not just to “govern,” but to rule. When no other private or public force enjoys any such consent, no other force can resist. We are certainly well beyond “rule of law” at this point! On the inaugural podium, the new President announces a state of emergency. He declares himself the Living Constitution. In six months no one will even remember “the swamp.”
Wow! What a simple, clear idea! The engineer, when he comes across so compelling and obvious a design, knows there’s a catch: he won’t get the patent. Someone else must have invented it before. People may be stupid—but they’re not that stupid.
Indeed we have just reasoned our way to reinventing the oldest, most common, and most successful form of government: monarchy. And we are setting it against the second most common form, the institutional rule of power-obsessed elites: oligarchy. And to install our monarchy, we are using the collective action of a large number of people who each perform one small act: democracy.
The alliance of monarchy and democracy (king and people) against oligarchy (church and/or nobles) is the oldest political strategy in the book. The suburban conservative, who just wants to grill, either has no idea this ancient and trivial solution exists, or regards it as the worst thing in the world—even worse, possibly, than his sixth-grader’s mandatory sex change.
And why? Ask your friendly local Judas goat, the pundit. Even the “new right” pundit—who only differs in his policies and issues. Which are, true, slightly less useless. As the top of the tree is slightly closer to the moon.
The 20th century even came up with a handy pejorative for a newborn monarchy. We call it fascism. No word on whether Cromwell, Caesar, or Charlemagne, let alone Louis XIV, Frederick II and Elizabeth I, were fascists.
But, to borrow Scott Alexander’s charming term, also not his own invention, they were certainly strongmen. TLDR: if you want to be strong, elect one strongman. If you prefer to be weak, elect a whole bunch of weakmen. Do you prefer to be weak? “If the rule you followed brought you to this place—of what use was the rule?”
The pundit reassures you that you don’t need a strongman to be strong—you’ll do fine with weakmen—so long as those weakmen have the right “shared attitudes and policy prescriptions.” By the way, here are some attitudes I’m happy to share with you. Click now to accept cookies. Did I mention that I have policy prescriptions, too? Skip ad in 5 seconds. Congratulations, you’ve been automatically subscribed! Check the box to opt out of most emails—void where prohibited by law—terms and conditions may apply…
…
An odd sort of pundit, who remains only nominally anonymous but has always very much GAF, Scott Alexander does not have Hanania’s cagey diplomatic noncommittal. As a “rationalist,” he is deeply committed to his own class status, and to oligarchy itself—which, like most, he misidentifies as “democracy.”
While the whole raison d’etre of the rationalist is the irrationality of our oligarchy, as displayed in genius moves like refusing to cancel regularly-scheduled airline flights to stop a Holocaust-tier pandemic, the rationalist’s dream is a rational oligarchy—using Bayes’ rule, which given infinite computing power will become infinitely intelligent—in Carlyle’s immortal phrase, “a government carried out by steam.”
Obviously, this is not just logical—it immunizes the rationalists from the scurrilous charge of “fascism,” or worse. And they were right about stopping the flights. So was my 9-year-old. Sadly, in a world of universal delusional delirium, rationality can get quite pleased with itself by clearing quite a low bar.
My view is that no government can be or ever has been carried out by steam—only by human beings—a species the same today as in the Old Kingdom of Egypt, if possibly a little dumber on average—and this will remain the case until some computational or genetic singularity occurs. For neither of which events will I hold my breath. This is why I find it easy to picture 21st-century America under the phronetic monarchy of an experienced and capable President-CEO, and almost hilariously impossible to picture it under a Bayesian bureaucracy of polyamorous smart-contracts.
Alexander disagrees. Here is his analysis—the same text that Hanania quotes. Let’s go through it thought by thought, and see if we can’t turn it into some delicious carnitas.
…
Let’s get back to those “elites.” Alexander conflates three quite orthogonal concepts in his use of the word “elite”: biology, institutions, and culture.
Elite biology is high IQ, which is genetic. Elite institutions are any centers of organized collective power—Harvard, the Komsomol, the Mafia, etc. Elite culture is whatever ideas flourish within elite institutions.
Destroying biology is genocide—specifically, aristocide. Destroying institutions is… paperwork. Who hasn’t worked for a company that went out of business? Same deal. And if the culture is the consequence of the institutions, different institutions (with the same human biology) will inevitably nurture different ideas.
The SS was anything but a low-IQ institution, yet it propagated a very different culture than Harvard. 21st-century Germany is anything but a low-IQ country, but the ideas of Kurt Eggers do not flourish in it. It seems that high-IQ institutions can be destroyed—and the new “elite culture” will be the culture of the institutions that replace them.
So the only target is the institutions. There is nothing “nasty” about closing an office. In the worst possible scenario, the police need to clear the building, lock the doors, and impound the servers. Such tasks are well within their core competence, and can be performed with calm professionalism. They will probably not even need their zip-ties.
…
For democracy to be effective in such a situation, it must know its own limitations. It can seize the reins—but only to hand them to some effective power. This power must have one of three forms: an existing oligarchy, a new monarchy, or a foreign power.
Also, there are three classes in an advanced society, not just two: nobles, commoners, and clients. Since clients support their patrons by definition, once nobles plus clients outnumber commoners, the commoners have permanently lost the numbers game. This is why importing client voters is a recipe for either civil war or eternal tyranny—if not both.
…
Yes. This is what happened in denazification, except with monarchy and oligarchy reversed. For example, all German media firms today are descendants of institutions created, or at least certified, by AMGOT. Nothing “organic” about it.
The essential problem with Alexander’s picture of this process is that, since like most smart people today he inhabits Cicero’s great quote about history and children, he simply cannot imagine replacing one kind of elite institution with another. Nor can he imagine high-IQ elites—human beings as smart as him—which are as loyal to a new sane monarchy as today’s elites are loyal, slavishly loyal, to our old insane oligarchy. Does he think that Elizabeth’s London had no elites? Caesar’s Rome?
If Alexander was analyzing the Soviet Union in the same way, he would conclude that elites are inherently devoted to building socialism for the workers and peasants. Since the present world he lives in is all of history for him, he cannot see the general theory which predicts this special case: elites like to get ahead. To genuinely change the world, change what it takes for elites to get ahead.
If the elites are poets and their only way to get ahead is to write interminable reams of “race opera,” as my late wife liked to put it, the floodgates of race opera will open. If the elites are poets and their only way to get ahead is to write interminable reams of Stalin hagiography, Stalin will be praised to the skies in beautiful and clever rhymes.
…
There are two big strawmen here. Let’s turn them into steelmen.
First, “the populace uses the government” is non-Burkean. The populace (not all of it, just the middle class) installs the government. Then it goes back to grilling. So long as the commoners have to be in charge of the regime, and the commoners are weak, the regime will be weak. They need to “fire and forget.” Otherwise, they just lose.
Second, Alexander has clearly never heard of the atelier movement. No, this is not the same thing as your grandma in front of the TV copying Bob Ross.
What happens is this: every (oligarchic) art school and art critic no longer exists. Not that they are killed, of course. Just that their employers are liquidated (not with a bullet in the neck, just with a letter from the bank). They exist physically, not professionally. They were already bureaucrats—they had careers, not passions. Who gets fired, but keeps doing his job just for fun? Certainly not a bureaucrat.
And every (oligarchic) artist no longer exists—not that they are killed, of course. Just that the rich socialites who used to buy their stuff got letters from the bank, too. Libs sometimes talk about a wealth tax—a one-time wealth cap, perhaps at a modest level like $20 mil, will concentrate the rich man’s mind wonderfully on actual necessities.
Elites like to get ahead. The people who got ahead in the oligarchic art scene can no longer get ahead by doing shitty, bureaucratic, 20th-century conceptual art. Because there were so many of them, and because the demand for this product has dropped by at least one order of magnitude if not two, elite ambition is replaced by elite revulsion.
The enormous supply-and-demand imbalance for both art and artists in 20th-century styles leaves these styles about as fashionable as disco in 1996. “Paintings” that used to sell for eight figures will be stacked next to the dumpster. “Artists” once celebrated in the Times will be teaching kindergarten, tying trout flies, or cooking delicious dinners.
Inevitably, some of these people have real artistic talent. (The first modern artists had real talent—Picasso was an excellent draftsman.) They can go to an atelier and learn to draw. They will—because now, acquiring real artistic skill is a way to get ahead in art. And again, elites like to get ahead.
…
There is nothing “normal” or “natural” or “organic” about oligarchy. Does Alexander think “uncured” bacon is “organic” because, instead of evil chemical nitrates, it uses healthy, natural celery powder? He sure is easy to fool. But who isn’t?
Culture and academia is already yoked to the will of government in a “heavy-handed manner”—yoked not by the positive pressure of power, but the negative attraction of power. When the formal government defers to institutions that are formally outside the government, it leaks power into them and makes them de facto state agencies.
Power leakage, like a pig lagoon spilling into an alpine lake, poisons the marketplace of ideas with delicious nutrients. Ideas that make the institutions more powerful grow wildly. Eventually these ideas evolve carnivory and learn to positively repress their competitors, which is how our free press and our independent universities have turned our regime into Czechoslovakia in 1971, and our conversation into a Hutu Power after-school special. PS: Black lives matter.
The paradox of “authoritarianism” is that a regime strong enough to implement Frederick the Great’s idea of “free speech”—“they say what they want, I do what I want”—can actually create a free and unbiased marketplace of ideas, which neither represses seditious ideas nor rewards carnivorous ideas. But it takes a lot of power to reach this level of strength—and it requires liquidating all competing powers.
I have never been able to explain this simple idea to anyone, even rationalists with 150+ IQs who can grok quantum computing before breakfast, who didn’t want to understand it. Ultimately it reduces to the painful realization that sovereignty is conserved—that the power of man over man is a human universal. (Also, we all die.)
No surprise that nerds who think of power as Chad shoving them into a locker can’t handle the truth. PS: I went to a public high school as a 12-year-old sophomore, was bullied every day for three years, and graduated college as a virgin. Whoever you are, dear reader, you are not beyond hope. You can handle the truth.
…
And yet: Alexander’s post is about Erdoğan—and his description of Erdoğan is spot on. It also is a perfect description of Orban in Hungary; it applies to Putin in Russia and Xi in China; and it is even pretty accurate for Hitler, Mussolini and friends.
What all these “strongmen” have in common is that they are provincial. Turkey is not exactly the center of the world. Even 20th-century Germany was nowhere near the center of the world, though it could at least imagine becoming that center. If Turkey just disappeared tomorrow, no one would have any reason to care except the Turks. Who needs Turkey for anything? What would collapse—the dried-apricot market?
Erdoğan’s problem is that he cannot vaporize the oligarchy, because the institutions that matter are not in Turkey. The provincial strongman has no choice but to follow the “populist” playbook that Alexander describes so well.
Orban can kick Soros’s university out of Hungary; he cannot do anything at all to Soros, let alone to the global institutions of which Soros is only a small part. He is indeed “arrayed against” these institutions, to which his Hungarian elites (who speak nearly-perfect English) will always be loyal. The contest is unequal and has only one possible winner, though it can last indefinitely long. Even Xi, whose country can quite easily imagine becoming the economic center of the world, is a provincial strongman—in fact, he sent his daughter to Harvard. Sad!
In a global century, the only way for these provincial strongmen to develop genuine local sovereignty is to go full juche. This is simply not possible for Hungary or Turkey, both of which are firmly attached to the cultural, economic, and military teat of the Global American Empire. Indeed it is barely possible for North Korea, a marsupial nation still in China’s pouch. So Alexander is right: these “strongmen” cannot win. Their regimes will all go the way of Franco’s. It’s impressive that they even survive.
Erdoğan simply has no way to attach his best citizens to his own regime. They are citizens of the world. Elites always like to get ahead. If you’re a world-class talent in anything, why would you try to get ahead in Istanbul? Suppose you want to make a name as the world’s greatest Turkish writer. Succeed in New York, then come home. Turkey is a province; provinces are provincial.
Yet I am not a Turk or a Hungarian, and neither is Scott Alexander. The greater any empire, the more essential that its fall begin at the center. The Soviet empire did not fall from the outside in; it was not brought down from Budapest or Prague; it fell from Moscow out.
And the American empire will fall from Washington out—though that may not happen in the lives of those now living. And although nature abhors a vacuum and no empire can be replaced by nothing—and oligarchy, in the modern world, can only be replaced by monarchy—the “strongman” of this monarchy will not look anything like these mere provincial dictators.
…
The result of Alexander’s perceptive calculations, which are only wrong because their only input data is the present, is simply that our present incompetent tyranny is and must be permanent. Of course, every sovereign regime defines itself as permanent. Yet when we look at the past and not just the present, we see that no empire is forever.
Some grim things are happening in America today. These grim things have a silver lining: they expose the gleaming steel jaws of the traps that the aristocracy sets for its commoners. They remind the cattle that a goat is not a cow and a baa is not a moo.
Every pundit is a Cicero. And amidst all the greatness of his rhetoric, Cicero could not imagine a world that had no use for Ciceros—a world governed by competence, not rhetoric. By the time Caesar crossed the Rubicon, nothing had failed more completely than the whole Roman idea of governance by rhetoric—an idea many centuries old, an idea whose execution had beaten all competitors to capture the whole civilized world, but an idea that was past its sell-by date. Rome herself was no longer suited to it. The republican aristocracy of Rome no longer meant Regulus and Scipio and Cincinnatus; it meant Milo and Clodius and Catiline. Its factional conflict was the choice between Hutu Power and Das Schwarze Korps. Caesar was not a disaster; Caesar was a miracle.
In the death of the American republic, every detail is different. The story is the same. The contrast in capacity between SpaceX and the Pentagon, Moderna and the CDC, Apple and Minneapolis—between our monarchical corporations, and our oligarchical institutions—is a dead ringer for the contrast between the legions and the Senate.
The sooner we stop pretending that this isn’t happening to us, the better results we can get. Wouldn’t it be nice to get to Caesar, Augustus and Marcus Aurelius, without passing through Sulla and Marius, Crassus and Spartacus? Alas, from here and now it seems unlikely. But I can’t see why every serious person wouldn’t want to try.
#curtis yarvin#substack#long#moldbug#well worth the read#monarchy#oligarchy#scott alexander#richard hanania#tanner greer#those who just want to grill#strongman#pundits#i'm reminded at several points of jim donald's arguments about how holiness spirals are ended
3 notes
·
View notes
Text
re neurodivergent headcanons in Breaking Bad/Better Call Saul, I think the first time (a year or so ago) I read something where someone online suggested Chuck was somewhere on the autism spectrum (high functioning/Aspergers), I laughed it off as a ridiculous suggestion, because he didn’t “fit” many of the stereotypical traits seen in other fictional characters or in the popular conception of the topic…but in retrospect, I think that came more from my misunderstanding of the “spectrum” part of it than anything else. It’s definitely a plausible/possible diagnosis comorbid with the anxiety disorder(s) he canonically has.
· We know Chuck’s a good actor (e.g. his ability to fool Jimmy in “Klick”) and is able to mimic and slip into different sorts of social behaviors (e.g. his ability to social climb from a working class or lower-middle-class family to the world of white shoe law firms), so he’s probably capable of using masking in most public settings. This is apparently a more common trait in autistic women, but men do it as well, if less frequently.
· Studies asking about the long-term effects of masking seem to imply it takes a physical/emotional/mental toll on the person using it, which might explain why, by the time we see him in BCS, the stress of acting “normal” in meetings and the like, when compounded with the worsening of his anxiety problems, leaves him curled up under a space blanket for hours or even days afterward. Trying to compensate for multiple issues at once is probably even more taxing.
· He seems prone to getting overwhelmed by things and either shutting down or lashing out in reaction. The most extreme form of the former is when he goes catatonic for hours/days in response to being tazed or put in the CAT scan machine; the most extreme form of the latter is probably him completely losing it and shouting/crying/having to be physically restrained by the hospital staff because he’s so upset about being surrounded by lights/hooked up to an EKG/being recommended for a CAT scan.
· Contrary to stereotypes, Chuck is decent at reading people (or at least he’s extremely good at reading his brother and knowing how he behaves) and he interacts well with people within a work context, but he doesn’t seem to have any friends outside of it, or much in the way of a social life–the other lawyers hold him in awe as a sort of glorified animate law encyclopedia, rather than someone they would want to hang out with or chat with informally. (Though Chuck doesn’t come across as the sort who would be interested in chit chat with coworkers anyway...) Being totally housebound and cut off from the outside world is upsetting to Chuck primarily because it interferes with his work as a lawyer–we never get the sense that he’s upset about it having any effect on his interpersonal relationships, because he doesn’t seem to have any. This is probably why losing Rebecca hit him so hard. He’s got almost nobody else, besides Jimmy and Howard, and he’s really not emotionally open and unguarded with anyone.
· He’s got problems dealing with his emotions in general. Even when he’s trying to do his little pain/emotion/medication journal as part of his psychiatric treatment towards the end of season 3, he seems to struggle with articulating his emotional state–he’s just got “average” written down for most of the incidents he’s logged, but he’s not able to write down what his emotion is after he’s unable to sleep after insulting/lying to Jimmy to drive him away for the final time, and he seems to abandon writing in the journal after that & rapidly deteriorates psychologically. From what we see of him in the show, he seems to alternate between being extremely repressed and completely exploding and freaking out.
· Some people have no interest in having or wanting friends, but I don’t think Chuck’s one of them. He seems pretty lonely. He remarks to Jimmy at one point in season 1 that he doesn’t really mind him hanging around to work on the Sandpiper case in his house because he’s glad for the company, which makes his systematic driving away of Jimmy and the few other people in his life all the sadder. The whole root of Chuck’s jealousy of Jimmy in the first place is that people like Jimmy, and they don’t like him. He makes attempts at being friendly, but struggles to do it on anything deeper than a surface level. (Of course, a lot of Jimmy’s friendliness and charm tends to be pretty shallow too, but I don’t know that Chuck really appreciates that or can tell the difference–all he sees are the results.)
· He’s tone-deaf with jokes–he famously botches the attempt at a lawyer joke to his wife in the opening flashback in “Rebecca”, but he also makes an awkward attempt at humor when talking to Kim in a present-day scene later in that same episode (“the early bird gets the worm, which is good if you like worms”), which leads to some uncomfortable forced laughter from her. Some people are just serious by nature, but they probably wouldn’t bother trying to make jokes in the first place if that were the case. The fact that Chuck keeps trying to make jokes and failing suggests that there might be some impairment in that area. He sees Jimmy do it, and he sees it work for him, but can’t really manage it himself. (He seems to do ok with deadpan sarcasm though–that comment about young people loving local print journalism is probably my favorite Chuck quote.)
· He’s very verbal and articulate, but his speech patterns can be a bit odd. He can be indirect and overly formal, which may or may not be an overcompensation for the more stereotypical autistic behavior of being too direct in speech as to be insensitive. He usually winds up still coming off as elitist and assholish anyway, though he may not be intending this/aware of this. When he’s nervous or upset, he tends to devolve into talking at people rather than to them, such as when he starts rambling on about probable cause and assorted legal precedents to the police officers who show up at his house in “Alpine Shepherd Boy”, without noticing that they aren’t even standing at the door anymore. He’s got a lot of information rattling around in his head, which he throws out as a defense, but not always in a way that is helpful; I don’t think talking about Latin translations of the Hippocratic Oath to the doctors sedating him without his consent before sending him in for a CAT scan is doing him any good (NB: the actual Hippocratic Oath is in Greek anyway, and the phrase Primum non nocere dates from a later period, so either Chuck has no idea what he’s talking about, he’s conflating two related things, or he’s freaking out enough that he doesn’t really care at this point).
· He seems to ignore other people when they’re talking to him altogether if something sets him off or distracts him–when Howard tells him about Kim quitting HHM and teaming up with Jimmy, Chuck immediately tunes him out, to the point where Howard has to ask him if he’s still listening. Chuck says he is, but then walks off in the middle of Howard talking because he’s still distracted by what he said before, sending a confused/concerned Howard following after him. This is at its most extreme when he goes into his rant in “Chicanery” and is totally oblivious to both Galley pleading with him to stop and everybody else in the room staring at him in growing horror/disbelief until he’s far past the point of no return.
· I’m actually sort of curious about Chuck’s abilities in court prior to the visible deterioration of his mental health, because although he clearly knows a lot about the law, his personality is a bit off-putting. I don’t know if he just sort of brute-forced his way through things because of his knowledge of obscure case law, because based on what I know from the lawyers I’m friends with, there are all sorts of subjective factors that can come into play in a court setting. The sort of things that would drive someone like Chuck nuts, like jurors who deliberately choose to ignore evidence because they’ve decided in advance that they don’t want to convict someone of a crime. (To be fair, this would also drive me completely insane, because I have a really hard time at my own job dealing with people who think the rules shouldn’t apply to them for various reasons.)
· Chuck has an EXTREMELY black and white view of the world, and a sort of obsession with the authority of law and the importance of following the rules. He’s got really strong perfectionist tendencies within himself. I think a lot of why he gravitates toward the law is that he seems to find all the rules and procedures comforting, in a way--there’s a uniformity to the way the legal world works, and a framework in which everything proceeds--constraints which are equally binding on all participants.
· Maybe he just knows a ton about the law because he’s a lawyer, but it might also fall into the case of it being a special interest, since his knowledge of obscure case law seems to be regarded as extensive and superlative even by other lawyers. (He reads FEC and ISO reports for fun!)
· There’s something slightly elliptical about his thinking, and he doesn’t seem to realize that other people aren’t following his thought patterns. (He repeats his “One after Magna Carta!” justification for knowing the Mesa Verde address to Kim and Jimmy in season 2 as well as to the officials from the Bar in season 3, which seems to suggest that he thinks it is a very obvious and logical connection that other people should grasp, though I’m not sure that it actually is outside of his head.)
· I’m not entirely sure where the line between nervous tics and stimming is drawn, but he’s got a lot of little fidgety behaviors that come out especially when he’s stressed, especially scratching or shaking or wringing his hands. (The script to “Chicanery” indicates that he’s nearly drawing blood from digging into his hands while on his big rant, but it’s not visible onscreen because we’ve got that wonderful/agonizing slow zoom onto his face instead.) It's not clear if it predates the EHS or not. Sometimes there’s a clear tie in his behavior to perceived pain from electricity, but sometimes there’s not--sometimes it seems to result from him trying to distract himself from the electricity instead, like when he’s trying to stand outside the house for two minutes in “Bingo”. Sometimes he does it while he’s standing around in his house, thinking about something else, like while rehearsing arguments against Jimmy before he heads in to court in “Chicanery”.
· There’s a pretty strong preference for routine/predictability & distress when it’s altered. (Most people probably would not get so suspicious if a single newspaper wasn’t delivered one day, for example. If it was repeated or frequent or a pattern, yes, but not for a single paper.) His control issues are brought up pretty frequently in fandom discussions; maybe he’s a jerk, maybe he’s just not able to function well in unpredictable situations, maybe it’s a little of both (e.g. Chuck being really bothered by Ernie bringing him the wrong kind of apples, then saying that it didn’t really bother him that much...but then telling Ernie to write it down so that he would get the right apple the next time, indicating that he actually WAS bothered by it)
· It’s possible his perceived sensitivity to electricity grew out of an existing natural sensitivity or aversion to extremes in light or sound or anything else, but this is pure conjecture because we get so few flashback scenes. (Speaking only from personal experience, I don’t think I’m hurt by electricity, but I can hear lights when they’re turned on, and get uncomfortable/anxious under certain types of light, like fluorescents in big box stores when out shopping, so maybe someone who’s more sensitive to sensory things in general might be more prone to developing a sort of learned distress out of that.)
All of this is very inconclusive! But it’s totally plausible as a reading of the character.
32 notes
·
View notes
Text
Why I Think Rationalist Self-Help Is Broken
So I was asked, fairly reasonably, after in my previous post I said I thought I might have had a narrow escape from a self-reinforcing set of bad approaches to mental health and executive functioning issues, what approaches I was thinking of, exactly.
This is a list of approaches I think are wrong, and the consensus around them in the self-help parts of the rationalist community (e.g. all the praxis/gnosis type channels I’ve encountered on rat!Discord) is a big part of why I no longer frequent those spaces and now consider myself rat!adjacent, centrally an EA, and more likely to pursue skeptic communities or other communities to try to find ones whose flaws I am happier living with, rather than expanding engagement with rationalist communities. Although I insist, as an unrepentant Yudkowskian, the rationalist community moved away from me and not visa versa.
If you’re a rationalist with “post rationalist” leanings who doesn’t want to read a list of reasons why I think you suck right now, I recommend not expanding this post; I’m going to try to be as polite as I can about it all and stuff, but at the end of the day the topic of the post is the topic of the post.
So, the approaches I think are bad, some with particular justification and some just by correlation to the rest.
Drug addiction/recreational drugs as coping mechanism. A bit ago I commented “alcoholism is cool so long as you swap out the drug”, sardonically, and someone responded to say that actually, they endorsed that, so this is an actual point of disagreement.
I think the primary problem with using incapacitating recreational drugs as a balm within your coping mechanism is that it provides an extremely good avenue for escapism, which is a really tempting way to buy a balm for today at the cost of tomorrow. Additionally, I think it readily leads to a thing where people can’t function sober because their coping strategy is unavailable, and can’t function high because, well, they’re high. And yet there is a lot of “oh, you feel bad? Let me help you get some weed”. Arguments about handling existing addicts aside, this is I think probably one of the ways people move into a rationalist cluster and then decline because of “helpful” peers sharing their escapism.
I miss straight-edge LW-rationality where my willingness to countenance alcohol put me at the questionable end of the spectrum.
A bunch of stuff tied up in the assumption that normal friendship and relationships are impossible for many people in the community and therefore people should be grateful to have friends and relationships at all. This particularly leads to the idea of the whole “catgirl” thing where you can apply any kind of costs to the people around you so long as you’re a catgirl for them, because both they and you assume that they can’t get friends anywhere else.
This is not actually true! Being friends with people who are... a bit high maintenance is great, but you shouldn’t do it out of the feeling that they are the only people who will be friends with you. It’s not true. and people shouldn’t feel like they can be as high maintenance as they want so long as they play catgirl.
When I got over this, approximately concurrent with me starting therapy and reinforced by an increase in RL socialisation they encouraged at the time, I flipped out a little and quit most of the circles I was in for a bit. I don’t need to be friends with people who borrow hundreds of pounds from me and have no shame about not paying it back to have friends, and any interactions with people who think I do are going to involve them taking liberties. I’m back in parts I like now, but without the previous “I need to cling to this community” feel.
Most stuff involved in thinking about social status and auras, and social reality, more likely if it promises to be looking at social reality for “real” when everyone else isn’t. These things are real, but... the only way I can really put the issue is... “wow, autistics are really bad at distinguishing between good and bad social models”. If the models pick up on one dynamic that a naive model doesn’t, they’re adopted without question, no matter what other cases they get wrong. And boy, do they get things wrong.
“Sometimes an impression of a person having an effective aura picks up on evidence that you would consciously miss about them being competent” => “The halo effect isn’t a bias anymore, it’s actually the correct way you should be approaching your decisions, your feels of a person’s aura is a better assessment of their competence than any assessments you might make away from those feels”, is every rationalist talking about how their in person interactions indicate a person actually has brilliant models despite everything they ever wrote being evaluated as awful when actually analysed blind. And it is frustrating as hell.
Auras and social reality offer a tempting opportunity to be the holders of a cynical secret, but taking that opportunity in no way requires people to actually adopt better models, and since the matter is complex enough that adopting better models is genuinely hard, that generally doesn’t happen. More common is brazen self-justification; the more you describe the rest of the world as sucking and focus on that the less your flaws show up relatively. The more you talk about your version of social reality, the less you have to pay attention to actual reality.
(I vaguely associate this stuff with Vassar’s group? But by now it’s the default.)
Trying to invent their own novel forms of therapy instead of (rather than as well as) going to actual therapists.
I think trying to execute therapy without being a therapist would be fair enough just because therapists are expensive, but some effort to actually be aware of what therapy generally entails rather than just sticking the name “therapy” on any series of actions you think is helpful would be good.
Hypnosis for mental health assistance and anything involved in exploiting suggestibility. This is mostly correlational- I observe a very strong correlation between cultivating suggestibility and a tendency to lack direction and an internal moral sense. But I also observe a lot of enthusiasm and no results, which is sufficient in itself to be dubious of it as a strategy.
Internal Family Systems; there’s a definite thing of temporarily disassociating to regain functionality temporarily I’ve seen people do which... I guess worked for them, I don’t want to recommend it but I can’t discourage it either.
But reifying things you are conflicted over into multiple personalities seems in the many cases I’ve seen it to let you keep both sides of the conflict, and I think that’s often not a good idea. The part of your thinking which is saying “actually, I don’t want to have this trait” should not be satisfied by being split off into a different personality unit than the trait.
I’m not sure it is something that can’t work to actually make progress in internal conflict, but I don’t think it looks like it is working the way I see it tried. I hear actual therapists touch on the concept, but I’d assign a probability of 80% that they do it different in a substantive manner.
I think peer support centred around validation has a tendency to validate behaving toxically. This isn’t rationalist exclusive, but is a problem with its self-improvement channels.
Separated out so you can more easily say you hate this bit while agreeing the above is bad: I also think it has a tendency to validate inaction. You don’t need to do X because Y. It’s okay to spend your time high because Z anyway. As a throwaway thing from a friend to a friend, well, there are worse crimes than bending epistemology while being supportive. As a culture, gets a bit crab bucket-y.
Part of the problem, I think, is that these traits tend to overlap and seem to reinforce each other. Once you get into some you get a bunch of the rest, and then you can’t update out because of the mutual reinforcement. The stuff you hear against your weed habit? Clearly just people manipulated by state propaganda trying to increase their own social standing. The stuff you hear against social power? It definitely seems to help in whatever hypnotic/suggestibility stuff you’re playing with. Why go to a therapist when they don’t understand social reality? And such. I never particularly bought into any of them, and am quite glad I did not.
I’ll mention messing with self-identity as something which is more good than bad. It doesn’t work, I think, if you detach yourself from reality enough that you can sustain a positive self-identity without actually... being positive, which is a problem that exists. It’s often done very poorly. But it’s still better than the way people readily self-identify as negative things by default. People are at least aware that negative identity is much more self-fulfilling than positive, and if you let something negative in there that wasn’t definitely true by accident then it will tend to become true.
Also, while I now no longer agree with the part of it based on IFS, I like the rest of the Luminosity sequence as a “soft sequence”, based on novel ideas, which I think is good for self-improvement; it focuses on self-observation to gain a more accurate self-model, and I think this largely works and is positive.
(On the Hammertime sequence in particular, I’ve not read it yet.)
192 notes
·
View notes
Text
Psychological Analysis #1.1
Hey (great start)
So, y’all must be wondering what the hell is this. Well, this is something that suddenly got into my head just today and it just turned midnight just now so it’s next day, so I shall rephrase that this idea came to me since yesterday and it’s something I’ve been wanting to do cause I kinda enjoy analyzing especially if it involves something I’m familiar with.
Just as a warning, I’m in no way a psychology major nor therapist or any kind of human being with a degree. I’m just a guy who enjoys the psychological genre thanks to a certain game that has pink blood. And these topics I’m going to be discussing here are topics I’m a bit familiar with cause I had to research these topics myself and two of which I’m very familiar with but only one of them I am officially diagnosed (according to my mom). This is also a spoiler zone! If you wanna read the manga yourself, go ahead and come back here with a funny story in your head! Without further ado, let’s get into this and start with what I am analyzing.
The characters I’m going to be analyzing are the 3 main characters of a manga that almost no one heard of: Dadadadan or Dame Dasa Daru Dansi. The story is about 3 boys who live in the same dorm room together and all have some form of issue with women: One is shy around girls, one straight up hates them and will start insulting them when his eyes lay on one, and the last one couldn’t care less about them unless they are 2-D. So we have a shy boy, a gynophobe, and a hardcore otaku. So, why on earth am I analyzing a slice-of-life manga about 3 guys with issues with women? Well, due to the fact that this manga (to me at least) is somewhat rich in the psychology of these boys. I’m going to break them down to who each of these boys are, what I might think their diagnosis is, their backgrounds/speculating backgrounds (one of which left somewhat vague the most), explain their relationship with each other, then conclude. I’ll also attempt to provide evidence as I go. Let’s start!

Mina Ayashiro

I’ll be starting with the easiest one then work my way down. Mina is an otaku who’s only interested in 2-D girls

and a computer wiz plus a hacker.

He likes snacks such as pocky and enjoys collecting figurines,

especially anything relating to his wife, Nagul, a made-up character for this universe. At the start, it seems to be that’s he’s just an otaku guy who gets really into roleplaying when it’s involved and then it’s revealed early on that he’s a son of a CEO of a big company and just changed his name, which explains how he is able to afford all of the figurines, posters, cosplay, and anime he has.


Diagnosis
Right at the start, it’s obvious that this guy has no issue with women whatso-ever. Just a guy who likes 2-D only,

but he gets really hyperfiated about it and forgets that other people exist and is able to talk to people just fine, only that he has no interest in interacting with other people except for the world of 2-D

Right off the bat, I’m going ahead and diagnosing him with autism. I am on the spectrum myself and while I was reading this manga series, all I could think was that I relate to him so much that I might as well kin him. His lack of need to socialize with others and his special interest only 2-D, with a special skill in computers/hacking
sort of makes him a somewhat textbook definition of someone who is autistic but high functioning. He does miss some social cues,

and never misses the chance of making each situation twisted to his liking: trying his best to involve a lot of roleplaying as possible.

Canon Background
Mina was raised with a life of luxury from his very doting father,

being the one who introduced Mina to the world of 2-D. While on the other hand, his mother wants him to take over the company one day,

so only wanting the best. Due to his upbringing from his father’s influence, the parents constantly fight over him

and what’s best for him: the father wanting Mina to live happily and letting him do what he wants; the mother wanting Mina to think about his future, to take things more seriously, and him to grow out of his love of 2-D. I’ll go ahead and give my opinion on which I support: the father. As I mentioned in the first few paragraphs, out of the 3 character’s backgrounds, Mina’s is the most vague cause his main issue is about his future and nothing from the past is hurting him, unlike the other two, so I’m going to start to give my theory on how he grew up.
Speculated Childhood
When Mina was born, his father was on cloud nine while the mother was already trying to secure her newborn son’s future. Both parents must’ve noticed as Mina was growing, his lack of interest in his surroundings. The father, being the more emotional one, must’ve been worried since he did agree with his wife that little Mina will be the next CEO, but a child who rarely speaks and shows no interest is concerning. So, he took Mina in to see a doctor and the professional speculated that Mina must be on the autism spectrum, but it is up to the parents whether or not they want to get him tested. The mother, against it since it’ll give them bad public eye, and the father agreeing with his darling wife, only wanting the best for his son and with heavy worry that his son would have possibly been bullied if he was diagnosed. So, the father researches the topic and concluded himself, all the while agreeing in the end, that his son must be on the spectrum and promises that he will not reveal it to anyone for his son’s safety. So, he starts to expose Mina to different hobbies, shows, practiced skills, anything that his son can latch on to for him to have some motivation in his life. One day, his father showed him an anime, involving Mina’s all time favorite female character, Nagul. Mina instantly fell in love with her and demanded anything involving the show, especially Nagul. His father, delighted to see his son so happy for the first time, got anything Mina wanted. His mother, on the other hand, is fully against this behavior that she knows will affect him greatly in the future (which she’s not wrong). As the years go on, the Ugagami couple divorced: the mother gained custody of him and will allow his father keep visiting, and then Mina’s name changed to Mina Ayashiro.
His father continues to dot and give him spending money for anything he wanted, as a way to keep himself under his mother’s radar. This concludes my speculation of his possible background.
Mina’s Relationships
Mina’s relationship with his roommates impacted his life greatly. At the end of the Mina Rescue Arc, his mother is looking over a flash drive that he gave her, full of pictures with him and Nagul, but as she scrolls more, she discovers pictures with him and his friends,

showing that he did in fact change and has opened the gate to his world a little and welcomed two people, the most important people in the world to him, going as far to hack security cameras to find evidence that Mikami did not in fact steal the answer sheets. To him and Mikami, both are very protective of Shiro who is the weakest out of the 3, so during the later chapters, listening on a conversation that Shiro is involved and getting insulted, the two teamed up to ruin the guy but plan failed when Mina decided to incorporate that Shiro is God’s child.


Mikami and Shiro changed Mina’s life by just being there and supporting him every step of the way, indulging him in his fantasies and interests of common anime tropes.

Part 2
Part 3
#dadadadan#dame dasa daru dansi#mina ayashiro#shiro kisaragi#mikami ryouta#psycology#psychology analysis#i dont know what i'm talking about
0 notes
Text
WHAT DOCTORS, SCIENTISTS AND NUTRITIONISTS SAY ABOUT KANGEN WATER
Dr. Hiromi Shinya

“I have examined more than 300,000 people’s stomachs and intestines for 35 years and realize that our health depends largely on our dietary life. And from my experiences I would like to teach you healthy, dietary habits to help you enjoy your life!
“It is widely recognized in the medical profession that a healthy and clean colon is one of the most important precursors to good health and that the great majority of body ailments and diseases originate in an acidic and dirty colon. Water is essential for your health. Drinking “good water;” especially hard water which has much calcium and magnesium keeps your body at an optimal alkaline pH.
“Kangen Water® is alkaline rich water (ph 8-9), and is considered the very best drinking water because of its incomparable powers of hydration, detoxification, and anti-oxidation.”
~ Dr. Hiromi Shinya, Leading Endocrinologist (see footnote, #1)
Dr. Horst Filtzer

“When I first drank Kangen Water® I experienced something I had never had before, I liked it, I liked it very much. … As I investigated the product, as I investigated the concept of ionized water, as I investigated the concept of alkalization of the body cells, I became more and more convinced that this is a product that is of absolute value to all mankind. That it is a product that should be used in all households if at all possible, because it clearly is superior to any form of water than I ever encountered.
“Personally, I can testify that there is no question that my own life has been markedly enriched by the ingestion of Kangen Water®… I endorse Kangen Water® as a physician, as a surgeon, as a human being, 100%. I feel that it is of great benefit to all mankind… I can only recommend it in the highest way.”
~ Dr. Horst Filtzer, Vascular Surgeon (see footnote, #2)
Dr. Corinne Allen

“Brain inflammation can occur from many causes including: head injuries, premature birth, lack of oxygen and various infections. The resulting inflammation can provide dysfunction in the body’s ability to detoxify harmful substances. They can also exhibit mitochondria that have low energy output and high free-radical generation. Often those with brain challenges like Autism and Aspergers, drink almost no water each day, only accentuating the problems in brain functioning. In Autistics and others where brain inflammation is high, toxins can more easily cross the blood brain flooding the brain with free radicals. Kangen Water® has been providing my clients with a strong source of antioxidants and improved hydration. In our brain programs we observed that our therapeutic expectations have been significantly exceeded by adding Kangen Water® to the treatment plan.”
~ Dr. Corinne Allen, Nutritionist (see footnote, #3)
Dr. Dave Carpenter

“This [alkalizing] program contains a whole new way of looking at diet and nutrition. When followed, it leads to a healthy, lean, trim body and an enhanced level of wellness, energy, and mental clarity most people have not experienced previously.
“Based on years of research and observation, we have concluded that over acidification of the body is the underlying cause of all disease. Because many people consume a diet primarily comprised of acid forming foods, (i.e. sugars, meat, dairy, yeast breads, coffee, alcohol, starches, etc.) rather than whole plant foods, they are frequently sick and tired.
“In my experience, Kangen Water® supercharges your nutritional program better than anything. Water is the key and this [Enagic® Kangen® Water] is the best water I know of. Anyone who gives it an honest try will experience it in their own health, without question!”
~ Dr. Dave Carpenter, Naturopathic Physician (see footnote, #4)
Dr. Fereydoon Batmanghelidj

“I am a researcher. I have researched dehydration for the past 20 years. When I discovered that the solution to most of the disease conditions of our society is not a moneymaker, I decided to take my information to the public. My research revealed that unintentional dehydration produces stress, chronic pains and many degenerative diseases. Dry mouth is not the only sign of dehydration and waiting to get thirsty is wrong. Medicine has based its understanding that it is solid matter in the body that regulates all functions of the body. I have explained scientifically at the molecular level that it is water that regulates all functions of the body including functions of solid matter. 75% of our bodies are composed of water. The brain is 85% water. It is water that energizes and activates the solid matter. If you don’t take enough water, some functions of the body will suffer. Dehydration produces system disturbances. When I use the word water cure, I am referring to curing dehydration with water.”
~ Dr Fereydoon Batmanghelidj, Medical Doctor, Researcher (see footnote, #5)
Dr. Otto Warburg

Dr. Otto Warburg in his lab at the Max Planck Institute for Cell Physiology in Berlin-Dahlem. 1960s
“All normal cells have an absolute requirement for oxygen, but cancer cells can live without oxygen – a rule without exception.
“Cancerous tissues are acidic, whereas healthy tissues are alkaline.”
~ Dr. Otto Warburg, Chemist, Nobel Prize Winner (see footnote, #6)
Dr. William Howard Hay

“All disease is caused by auto-toxification (self-poisoning) due to acid accumulation in the body.
“Now we depart from health in just the proportion to which we have allowed our alkalies to be dissipated by introduction of acid forming food in too great amount… It may seem strange to say that all disease is the same thing, no matter what its myriad modes of expression, but it is verily so.
“It was said earlier that all we can do for disease is to stop creating this background of acid end-products of digestion and metabolism, and this is true, for if disease comes always and only from this acid collection, then it must be evident to anyone that the cure lies in the discontinuance of this accumulation.
“Pneumonia, erysipelas, typhoid fever, influenza, acute arthritis, colitis, hay fever, all subside when the body is fairly detoxicated and the diet so corrected as to stop this excessive formation of the acid end-products, simply because each was expressing the end-point of tolerance of toxins, and each was the means by which the body sought to unload this unwanted mass.
“If the blood develops a more acidic condition, then these excess acidic wastes have to be deposited somewhere in the body. If this unhealthy process continues year after year, these areas steadily increase in acidity and their cells begin to die. Other cells in the affected area may survive by becoming abnormal, these are called malignant. Malignant cells cannot respond to brain commands. They undergo a cellular division that is out of control. This is the beginning of cancer.”
~ Dr. William Howard Hay, Surgeon, Developer of Hay Diet (see footnote, #7)
Dr. Keiichi Morishita

“Modern medicine… treats these malignant cells as if they were bacteria and viruses, it uses chemotherapy, radiation and surgery to treat cancer. Yet none of these treatments will help very much if the environment of the body continues to remain acidic.
“Drinking water that has a high alkaline pH, because of its de-acidifying effect, will help in preventing cancer. In Asia, alkaline water is regularly served to patients, and is considered a regular part of treatment.”
~ Dr Keiichi Morishita, Director of the Ochanomizu Clinic in Japan and the Head of the International Natural Medicine Association (see footnote, #9)
Dr. Robert C. Atkins

“Just about every condition I can think of, from arthritis to diabetes to cancer, is associated with acidity. It is no coincidence that many of our modern habits such as alcohol consumption, smoking, eating sugar, and stress, all tend to increase acidity. The only parts of our body that are supposed to be acidic are the contents of the stomach, the skin, and perspiration. Virtually everything else is supposed to be at least slightly alkaline.”
~ Dr. Robert C. Atkins, Physician, Cardiologist (see footnote, #9)
Footnotes:
1. Dr. Hiromi Shinya was born in 1935 in Fukuoka. After graduating from Juntendo Univesity, School of Medicine, he was internationally active and made a phenomenal impact as a pioneer in the field of Gastrointestinal Endoscopy. Dr. Hiromi Shinya is a clinical professor of surgery at Albert Einstein College of Medicine at Yeshiva University; head of the endoscopic center at Beth Israel Medical Center in New York, New York; and Vice-chairman of the Japanese Medical Association in the United States. He is also affiliated with both the Maeda Hospital and Hanzoo-mon Gastrointestinal Clinic in Japan. Dr. Shinya pioneered modern colonoscopic techniques, and invented the electrosurgical polypectomy snare now common on colonoscopes, allowing for removal of colon polyps without invasive surgery. He also authored of The Enzyme Factor, the English translation of his book on the relationship between enzymes and health that has sold two million copies in Japan. In his book and even on the cover Dr. Shinya extols the virtues of drinking alkaline ionized water, specifically, Kangen Water® produced only by the Enagic® devices. Dr. Shinya puts all his patients on Kangen Water® as part of his recommended diet.
2. Dr. Horst Filtzer, M.D. a Harvard Medical School graduate cum laude is a Vascular Surgeon. Horst has 35 years of active surgical practice in General and Vascular Surgery at Cambridge City Hospital in capacities as Assistant Director, Department Chairman, and Program Director He is also Director of the Wound Care Center in Western Arizona Regional Medical Center, Bullhead City, AZ.
3. Dr. Corinne Allen is an international researcher and practitioner in natural health and nutrition and has been in practice for more than 30 years. After receiving her doctorate in nutrition, Dr. Allen went on to more training in neurokinesiology and brain-stimulation techniques. She is recognized for her natural and practical approach to health regarding natural and alternative methods of stimulating permanent changes in the brain in dyslexia, ADD, autism, Asperger’s syndrome, learning disabilities, academic and behavioral issues and brain injuries. She runs the Advanced Learning & Development Institute.
4. Dr. Dave Carpenter is a member of the Idaho Association of Naturopathic Physicians. He is currently the President of the International Iridology Practitioners Association (IIPA), has served on the Board of Directors of IIPA since 1996 as Public Relations Director and Vice-President. Dr. Dave Carpenter is a Licensed Acupuncturist, Fellow of the International Academy of Medical Acupuncturists, and an IIPA Certified Comprehensive Iridologist (CCI). He is also a member of the American Naturopathic Medical Association, the Idaho Acupuncture Association, faculty member of the Intermountain Institute of Natural Health, and a graduate of Central States College of Health Sciences as a Naturopathic Medical Doctor, and the Royal Academy of Naturopathy in Australia as a Naturopathic Doctor, a graduate of the International Academy of Medical Acupuncturists. Dr. Carpenter also holds a BS degree in Nutrition.
5. Dr. Fereydoon Batmanghelidj, M.D., an internationally renowned researcher, author and advocate of the natural healing power of water, was born in Iran in 1931. He attended Fettes College in Scotland and was a graduate of St. Mary’s Hospital Medical School of London University, where he studied under Sir Alexander Fleming, who shared the Nobel Prize for the discovery of penicillin. Dr. Batmanghelidj practiced medicine in the United Kingdom before returning to Iran where he played a key role in the development of hospitals and medical centers. His groundbreaking book, Your Body’s Many Cries for Water (1992), has been translated into 15 languages and has sold over a million copies.
6. Otto Heinrich Warburg was born on October 8, 1883, in Freiburg, Baden. His father, the physicist Emil Warburg, was President of the Physikalische Reichsanstalt, Wirklicher Geheimer Oberregierungsrat. Otto studied chemistry under the great Emil Fischer, and gained the degree, Doctor of Chemistry (Berlin), in 1906. He then studied under von Krehl and obtained the degree, Doctor of Medicine (Heidelberg), in 1911. He served in the Prussian Horse Guards during World War I. In 1918 he was appointed Professor at the Kaiser Wilhelm Institute for Biology, Berlin-Dahlem. Since 1931 he is Director of the Kaiser Wilhelm Institute for Cell Physiology, there, a donation of the Rockefeller Foundation to the Kaiser Wilhelm Gesellschaft, founded the previous year.
For his discovery of the nature and mode of action of the respiratory enzyme, the Nobel Prize has been awarded to him in 1931. This discovery has opened up new ways in the fields of cellular metabolism and cellular respiration. He has shown, among other things, that cancerous cells can live and develop, even in the absence of oxygen. Otto Warburg is a Foreign Member of the Royal Society, London (1934) and a member of the Academies of Berlin, Halle, Copenhagen, Rome, and India. He has gained l’Ordre pour le Mérite, the Great Cross, and the Star and Shoulder Ribbon of the Bundesrepublik. In 1965 he was made doctor honoris causa at Oxford University. Copyright © The Nobel Foundation.
7. Dr. William Howard Hay graduated from the New York University Medical College in 1891 and spent 16 years in regular medicine, specializing in surgery. He later developed Bright’s Disease, and was unable to cure it using accepted medical methods of the time. This led him to find alternative methods to rid himself of disease. He came up with the concept of food combining (also known as the Dr. Hay diet), the idea that certain foods require an acid pH environment in digestion, and other foods require an alkaline pH environment, and that both cannot take place at the same time, in the same environment. After curing himself through proper diet, he wrote several books, started a sanatorium, and lectured throughout United States and Canada.
8. Dr. Keiichi Morishita is Director of the Ochanomizu Clinic in Japan and the Head of the International Natural Medicine Association. He is also an Honorary Professor, Georgia Tbilisi State Medical University, Professor, Choson University & Graduate School, Korea, Visiting Professor, Shenyang Pharmaceutical University, China and Honorary Director, China Health Care Food Association & Senile-Resistant Association, Honorary Director, Non-Pharmacotherapy Treatment & Research Center, Heilongjiang Province China, and Honorary President, Guangxi Pama Institute of Longevity, China, among many others. He is the author of The Hidden Truth of Cancer 1950 Graduated from the Tokyo Medical University where he majored blood physiology. 1955 Received Ph.D. from Chiba University, the school of Medicine. 1960 Presented a basic theory of Natural Medicine for cancer treatment and longevity (Morishita Theory) 1966 Testified as a member of the academic panel at the hearing on cancer by the special Committee for Advancement of Scientific Technologies of the Japanese House of Representatives. 1970 Established the Natural Medicine Society, the Life Science Association and Ochanomizu Clinic 1977. The effectiveness of Natural Medicine was endorsed by the McGovern Report written by Senator George McGovern of the U.S.A. 1982. The validity of the theory, diet of meat produces cancer; diet of grain/vegetables prevents cancer, presented at the hearing was proven by the National Academy of Science (USA) Recommendation.
9. Dr. Robert C. Atkins, a physician and cardiologist was one of the pioneers of complementary medicine in the United States and one of the most famous, successful and enduring nutrition experts of the last 40 years. He was the founder of The Atkins Center for Complementary Medicine and Atkins Nutritionals, Inc. He also authored more than a dozen health and nutrition books, including Dr. Atkins’ New Diet Revolution, one of the 50 best-selling books of all time, and Atkins for Life, which quickly joined Dr. Atkins’ New Diet Revolution on The New York Times bestseller list.
0 notes
Text
Michael Mell is on the spectrum
In BMC- the clips we've seen of the show- in all the scenes where Michael is wearing his hoodie, if he is stressed, or has something to lose (when Jeremy is receiving the squip and Michael is apprehensive, when Jeremy goes to get the girl, when Jeremy stomps off after saying he hates the school, when Jeremy hasn't acknowledged him all day because of optic nerve blocking, when Jeremy chooses to side with the squip and the upgrade instead of following Michael, etc) whenever something stressful, unnerving, or hurtful happens- MICHAEL WEARS THE HOOD UP TO COVER HIS HEAD- This may not seem like a big deal to some people but as someone on the autism spectrum- this is a clear coping mechanism that a lot of people on the spectrum use- It helps to kind of hide you a bit and give you some kind of little relief and sanctuary- the same thing with headphones- wearing headphones can help block out unwanted noise that you are overly sensitive to and drown it out with noise that brings you comfort (in michael's case- sometimes Bob Marley) Another common trait in people on the spectrum, is anxiety over change. People on the spectrum typically grow attached and accustomed to their routines and get startled and disoriented by change. This is another trait that can be seen in michael- in the opening number- he is introduced for the very first time singing: "Jeremy, my buddy, how's it hanging? Lunch is banging. Got my sushi, got my slushy and more!" First of all, it is arguable that when Michael says "Got my sushi, got my slushy, and more" it is a glimpse of these said patterns that tend to fall into place and make people on the spectrum more at ease. Notice how he doesn't say "I got sushi and a slushy" he says "got my sushi, got my slushy"- he states it simply like this because Jeremy is his best friend and knows his patterns and habits- which is why he so plainly states it like everybody knows about them. I think this is an example of Michael's system- he gets his sushi, he gets his slushy, he listens to his music, he wears his same hoodie, and he goes to school. Second of all (and this is more debatable than the rest) before Michael goes on to share his routinely patterns, something that stuck out to me was that Michael wasn't as socially adept as other characters- he addresses his friend and does the socially acceptable thing by asking how he is doing, but then immediately moves on without receiving an answer. This isn't because he is selfish or a dick- in my mind it's another trait of people on the spectrum. For people with high functioning autism, social interactions can be extremely difficult because it is hard to comprehend what is socially acceptable and what isn't. This can make some relationships hard because they may come off as rude or uncaring when in reality they just aren't able to easily slide into conversation and act completely normally. Third of all, when he says "and more" I thought it was cute because it showed his excitement for having accomplished something. For people off of the spectrum, little things like accepting a little change isn't anything out of the norm because life is unpredictable and things change all the time. But for people on the spectrum, even little things like being able to roll with one simple change can be a huge victory. Change is a lot harder for us so being able to deal with slight change is a big deal. After this line- Michael says "the roll was Mekhi maki and I'm feeling kind of cocky, cause the girl at sev-elev gave me a generous pour". Just the little change of the extra pour, extra slushy, Michael was able to accept and that was a win for him, enough to make him feel confident and cocky. Throughout the musical and album there is more evidence of this but I think that it is at least debatable that Michael may be on the spectrum. Honestly it wouldn't surprise me for George Salazar to portray a character like that as he has been good with mental health representation in the past. I honestly love the idea of an autistic character in a musical because there isn't a whole lot of positive representation elsewhere. You don't have to agree but I'm probably going to always see Michael now as a representation for me
#michael mell#michael in the bathroom#bmc#bmc musical#be more chill#be more chill musical#george salazar#musicals#autism#autistic headcanon#autistic characters#autistic love#autism positivity#autism spectrum#aspergers#sensory processing disorder#sensory sensitivity
2K notes
·
View notes
Video
youtube
I’m back with another review of the School Daze series. This time, the third book, AUTISM BELONGS.
You can support my autism-related ramblings and reviews on Patreon for as little as $1 a month, and right now you'll get access to some behind the scenes stuff on my upcoming video essays (the first of which will be on Reginald Barclay, Sherlock Holmes, and Accidentally Autistic Characters, with the second being on Why Social Skills Training is Bullsh*t).
Script below the cut.
Back into the School Daze series, is the third book a return to form for the series?
-Intro-
Spoilers: Yes, but let’s see why.
Overall Opinion
**** - As always, the book was a generally enjoyable read.
Clarity of Autism
***** - As always, the characters’ autism is stated in the text.
Stereotype or Person
***** - So, this book, as with the other two, introduces a new autistic character to the neighbourhood. Manny is from a Latinx family - though there’s no specificity here, all you know is that they’re Spanish-speaking immigrants and his mother makes churros sometimes. Idk, they could be, like, Spanish, but the book is set in the US, so I guess Latinx is more likely.
In case my accent doesn’t make it clear, I’m British. Spanish + churros would normally mean Spain to me. But again, the book’s set in the US, so I’m gonna assume Latinx.
Side note: There’s stuff with his family and, like, the enforcement of traditional gender roles in immigrant families and stuff that someone who is way more qualified than me should be commenting on. I’m just here for the autism. But I feel like I should at least mention that it is something touched upon in the book.
So, why does this book get five stars for not relying too heavily on stereotypes? Well, Manny meets up with Jeff and Kyle, meaning that we now have a pretty solid look across the spectrum. Not complete, but enough to reinforce the idea that autism looks different in kids of a similar age, in a way that was lacking in the first book with just Kyle and Jeff. And the fact that Manny is from a working class, Latinx family also works against the middle-class white boy stereotype.
But wait, I hear you say. Didn’t Ethan reinforce that same idea in the second book? You gave that book two stars for the Jeff Problem. Did this book solve that?
Eh, not entirely, but Jeff was much more of a background character, so his teachable moments weren’t as constant. Plus, when he was doing stuff, there was quite a bit of standing up for the kids, which was super relatable and made him more human.
You might also notice that I didn’t mention Ethan being in this book. That’s because he wasn’t. And he also wasn’t mentioned, which after the end of the last book…
#IsEthanOkay2k17
Accurate Autism
***** - Back to five stars for this one.
Again, what truly dragged down the second book was Jeff and a lack of nuance when it comes to how the expression of autistic traits change as autistic people grow into adults. But in this book, he goes back to the background and Manny is allowed to the foreground.
As with Kyle, Manny’s story revolves around his parents misunderstanding his attempts at communication or them simply not having the tools and knowledge to communicate with him in a way that works for him. As the book goes on, they meet the characters from the previous books and they get that help and support. As with the first book, it’s clearly evident that the author knows what she’s talking about when it comes to autistic children.
Storylines
**** - The autistic characters have story and plot, but it primary revolves around their autism.
As I said with the first book, that’s fine. That is what these books are about, after all. It would be nice to see them branch out, but the parents are the main characters, so it’s understandable that they don’t.
It’s worth noting that this book really hammered home the problems of the second book. As I said in my review of AUTISM RUNS AWAY, all of the attempts to get Ethan’s mother to relax and start supporting her son kind of fall flat, and before she makes any real progress, Ethan runs away and gets hit by a car, almost validating her viewpoint that her son was too much of a danger to himself for his teacher’s methods to work.
It was a total downer ending and lacked the hopefulness of the first book.
#IsEthanOkay2k17
I started to read the third book before I went on hiatus, and then I put it down quite quickly. When I went to read it again once I was back, I started from the beginning and quickly remembered why I had put it down so quickly.
Manny starts in a bad place, and after the downer of Ethan’s ending, I wasn’t ready to subject myself to that kind of downer message again.
But this time I pushed through the beginning, when Manny has destructive meltdowns that often hurt those around him. And then I got to the parts where the characters from the previous books helped Manny’s parents to figure out how to reduce the number of meltdowns he had through better communication and allowing their son to have a normal life.
Where the second book ended on a downer note, this one ended on a hopeful one. I don’t need to ask if Manny is going to be okay. He’s in pretty good hands.
Now, side note, I’m going to contradict myself and say that if anything, there was a touch too much positivity, but that’s not to do with Manny’s circumstances, but the fact that this book is sending a message to parents.
A common line throughout the book is other characters asking Manny’s parents why Manny’s not in school, and they come back with perfectly reasonable fears.
Except in this circumstance, their fears are unfounded because the local school is so great with disabled kids.
I do think that it is important to appreciate that these kinds of schools are rare. There’s an optimism to the way kids behave and treat each other, and that can be very true in the right environment. I would argue that it’s not in the majority of environments, and I think for a lot of disabled kids, while it’s not easy for parents to do, homeschooling can still often be the best route to take. Hell, for able-bodied, neurotypical kids, homeschooling may have a bad reputation for making kids socially isolated and unprepared for the adult world, but studies have shown that the opposite is actually true and that homeschooled kids tend to lack the trauma that most schools still inflict.
Idk, maybe I just went to really shitty schools up until sixth form, but my middle and high schools were regarded as the best high school in the city, so…
Maybe that’s just living in Newcastle… *insert Geordie Shore clip*
Respect
***** - While this book still has the problem of the second, where autistic characters were shown conscious and deliberate respect, but not really given it by the narrative through having stories of their own, the fact that the characters are in more secondary roles, like in the first book, makes that easy enough to forgive. After all, allistic characters in similarly secondary roles got the same amount of character development, so it’s not a huge issue.
This book also dropped both Asperger’s and functioning labels. I tend not be too lenient on stuff for being written in the past, because the point of these reviews are to educate allistic people and to warn/recommend stuff to other autistic people, but it does occur to me that this change probably coincides with the release of the DSM V, which makes previous uses slightly more forgivable. Not that the autistic community didn’t object to these things before the DSM V came out - where do you think the changes came from? - but it’s a more understandable oversight that’s righted in this book.
Overall, that brings AUTISM BELONGS to a near-miss 4.5 stars. It would have been nice to see an autistic character have a storyline outside of their autism, but other than that, it’s a solid book. The only question now is if the second book was a one-time misstep, or if, like the Star Trek films, you’ll be able to identify the good ones based on their divisibility by two. I guess we’ll find out two weeks from now when I review AUTISM TALKS AND TALKS. In the meantime, however, I have some things to say about the overuse of mentally ill villains. See you next week!
#actually autistic#actuallyautistic#writing diversity#disability#diversity in writing#diversifyyourwriting#write diversity#asd#asperger's#aspergers#aspie#aspie thoughts#aspie life#aspie problems#autism#video#video review#book review
13 notes
·
View notes
Text
Tips for using your Infrared Sauna
For optimal benefits, set your controls to maintain a sauna temperature of 110F-130F (43C-54C). Please remember that infrared heat is simply radiant energy in the form of a band of light that radiates heat penetrating the skin to a depth of 1-½ inches or more. This radiant heat is efficient because it warms the body internally, not the air. Setting higher temperatures may add to personal discomfort with very little therapeutic value. The Sauna should never be set over 150F (65C). To regulate the temperature in your system during use open the door for cooling.
For optimal results refrain from using the sauna on a full stomach.
It is important to remain hydrated. For best results drink water prior, during and after your sauna session.
Do not apply excess body lotion to your body prior to a sauna session.
Use at least 2-3 towels:
Sit on one folded towel for perspiration absorption and cushioning.
Use another towel on the floor to absorb extra sweat.
Use a third towel to wipe off your body surface sweat.
At the first sign of a cold or flu, increasing sauna sessions may be beneficial in boosting the immune system and decreasing the reproductive rate of viruses and bacteria.
As your body becomes more heat conditioned, you may want to increase your sauna session to 45 minutes or longer. Please remember to hydrate your system with plenty of water during the full session.
Note: many people with heavy metal, chemical or pesticide toxicity levels may find it difficult to sweat initially; for some individuals it may require 5-10 sessions before measurable sweat volume is evident, but continuous water intake will enhance detoxification. Even without measurable sweat, the IR sauna is helping to eliminate toxins through urine, bowels and hair.
To treat your ankles and feet more effectively, elevate them while in the sauna. Any area you wish to achieve a specific deep heating effect should be placed as close to the IR emitters as feels comfortable.
MERCURY DETOXIFICATION PROTOCOL
DETOX IN THE SAUNA
DIETARY MURCURY DETOX
Diet
Avoid all sugar and milk, limit all processed foods and most grains, especially wheat.
It will be important to have a high protein diet as the sulfur bearing amino acids in the protein will greatly facilitate detoxification. Do NOT attempt to fast during DMPS mercury detoxification. If you are a vegetarian you will be at HIGH risk for complications from DMPS unless you have a large amount of protein.
Whey protein can be used as a supplement as it is high in glutathione and branched chain amino acids. Two large tablespoons are used per drink and that can be taken once a day and twice a day for the week prior to DMPS chelation.
Autistic children can’t use this product as it contains casein. They can use pure branched chain amino acids. You can start with one capsule twice daily and mix with food. Work up to two capsules twice a day for the week prior to DMPS chelation.
Beneficial Bacteria
Take one quarter to one half teaspoon once a day of a high potency high quality strain. It is vital to have an optimized bowel flora for detoxification.
Maintain two to three bowel movements per day
If you are not having this many bowel movements make certain that your thyroid status has been checked. It is very common for mercury to affect the thyroid. If your thyroid function is fine then you should add some magnesium.
If you are on long-term magnesium it is important to take some calcium with it or after awhile you will develop an imbalance in your calcium magnesium ratio which could result in severe cramping.
Freshly ground flax seed several teaspoons per day will facilitate intestinal movement and also contribute some healthy essential fatty acids.
Unload the connective tissue with Chlorella or ProChitosan
Chlorella and ProChitosan are an important part of the detoxification program, as approximately 90% of the mercury in our bodies is eliminated through the stool. Chlorella is an algae and, unlike Protchitosan, has protein high levels of chlorophyll and other nutrients which can be used for nourishment.
The chlorella powder is the most cost effective approach but some people will prefer the tablets or capsules for convenience. A simple way to dissolve the powder is to place it in a container with a lid partially filled with water. Then tighten the lid and shake to dissolve and drink the solution.
Caution: About 30% of people can’t tolerate chlorella. This may be due to optimized function of the enzyme cellulase. If you are unable to tolerate this it would be wise to consider adding an enzyme with cellulase in it to help digest the chlorella.
Dose: One can start out with a one quarter of a teaspoon of the powder (one 500 mg tablet) once a day initially to confirm that there is no hypersensitivity present. Work up slowly over one to two weeks to a dose of one teaspoon (ten tablets or capsules) per day. Once you tolerate this dose you are able to use it to bind the mercury. Use this dose starting two days prior to your chelation and for one day afterwards. The chlorella will thoroughly coat your intestine and bind like a sponge to any mercury that the DMPS liberates into the gut.
The above dose is based on a 150 pound adult. If you are using the program for children reduce the dose proportionately. (So a 30 pound child would have have 30/150 or 1/5 (20%) of the dose).
Caution: If at any time one develops nausea or starts “burping up” the chlorella taste then the chlorella should be stopped immediately as a food sensitivity is developing which will only worsen if you continue taking it. If this happens you should switch to ProChitosan This binds similarly to mercury. Its dose is dependent on your bowel movements.
If you have one bowel movement a day or less you should start two days prior to the DMPS . If you have two or more bowel movement you can start 24 hours prior to the DMPS. Stay on it for 24 hours after the DMPS. So you will be on it either two or three days. The dose is two capsules three times a day. Be sure to drink it with plenty of water and increase magnesium if constipation develops.
Porphrazyme from Biotics Research is another alternative to chlorella that many clinicians have had success with in mercury detoxification.
Start Garlic or MSM
It would be wise to start on garlic regularly to enhance sulfur stores. Use the food, rather than the supplement garlic. Try to get in three cloves per day, but decrease the dose if your odor becomes socially offensive.
Again, as indicated in the chlorella section above, children will have proportionately lower doses.
MSM is a form of sulfur which will help your body to remove the mercury. The initial dose is one capsule twice a day. Increase by one capsule a day until you are at three capsules twice a day. If you have root canals and are chronically sick you may want to increase to five capsules three times a day.
Start Cilantro
Cilantro will help mobilize mercury out of the tissue so the DMPS can attach to it and allow it to be excreted from the body. The best form of cilantro is a tincture available from Dragon River (505-583-2348).
The dose is one dropper applied on the wrists and rubbed in twice a day for the two weeks preceding the DMPS IV. It is used the morning prior to the DMPS chlelation but can be stopped for the following two weeks. The tincture is also particularly useful for any joint pain and could be rubbed on the joint that is hurting as an alternative.
You can also augment the tincture with using the herb. It is not as potent, but certainly will add to the program. However, like chlorella, many people are sensitive to oral cilantro. So, if you develop any nausea or discomfort after eating cilantro do not use it orally.
Mineral Replacement
It is important to have a generally healthy mineral base. The body works better with toxic metals than no metals at all. Enzymes have certain binding sites that require a metal for them to perform their function as a catalyst. When you are deficient in magnesium, sodium, zinc and other minerals, the body does not let go of the toxic metals very easily.
Selenium and zinc are particularly important trace minerals in mercury detoxification and should be used for most people.
Generally the citrate form of minerals works quite nicely unless one has a low blood phosphorous level. It is important to not take copper or iron though unless a clinician has examined a hair analysis and or blood work and recommended these minerals. Thorne Research has Citramins II, which is citrated minerals without copper or iron.
Hydrochloric Acid: If you do not have a sufficient amount of hydrochloric acid secreted by your stomach then it will be very difficult to ionize mineral supplements to absorb them properly. There is a hydrochloric acid reflex present on the lowest rib approximately one inch lateral to the midline. If this area on the rib is tender to palpation there is a strong likelihood the person is deficient in hydrochloric acid and would benefit from supplementation.
This is especially common in individuals over 50 years old, and also in individuals with food allergies. One to six capsules or more of Betaine hydrochloride is generally taken with the first bite of every meal for proper digestive support. The Betaine can be discontinued once the reflex point in non-tender to deep palpation.
Monitoring Your Mineral Dosing
It will be very important to monitor your mineral levels during the detoxification program. This should be done initially and at least every 6-12 weeks. I only recommend two labs to do this work. Trace Elements and Analytical Research as they are the only two labs that do not wash the hair samples prior to analysis.
Digestion and Gall Bladder Support for Autism
Liver and gallbladder congestion are major issues in states of toxicity. To insure that your gallbladder bile flow is functional add magnesium taurate or taurine, butyric acid (Butryex 559-433-3110)
The dose of the Butyrex initially is 1/8-1/4 of capsule. Gradually increase the dose to 5 capsules 3 times daily. The Butyrex has a offensive odor which is lessened by keeping it in the freezer. Additionally inserting the powder in applesauce, raw honey or elderberry cough syrup may improve compliance.
Digestive enzymes (containing lipase) and CCK (stimulates contraction of the gall bladder. These can be used one hour after meals containing fat. CCK is taken after dinner (high fat meal)
· young children 1/4 tablet
· older children 1/2 tablet
· teenagers 1 tablet
· adults 2 to 4 tablets
Your ability to clear toxins will be impaired if you do not have proper fats to support digestive function. Your diet should contain adequate fat from unprocessed pure oils. Omega Nutrition, Flora or Arrowhead Mills
· sunflower
· safflower
· sesame
OR fats naturally found in foods:
· seeds
· nuts
· avocado
· free range organic poultry, eggs, or meats
Antioxidants
Vitamin C and E. It would be wise to take Unique vitamin E one capsule per day and about 250-500 mg of vitamin C with each meal. If you are exercising aggressively you can take 1000 mg of C 15-30 minutes prior to exercising. It is also wise to consider adding 2-4,000 mg of Vitamin C powder to a half gallon of water and drinking that throughout the day.
It will be VERY important to take 2000 units (typically five of the 400 unit capsules) of vitamin E the day of and the day after the DMPS injection as this will decrease the side effects of the detoxification reaction considerably. You can also take 1-2 grams of vitamin C immediately prior to the DMPS injection.
Start Monthly DMPS Injections, Suppositories or Transdermal
You should not have DMPS if you still have amalgam fillings. If they have been removed the injections can be started on a monthly basis. Collection of the urine is then down to analyze how much mercury is being excreted. One must urinate completely prior to the injection.
I perform the analysis at 90 minutes as that is most convenient, but others do four or 24 hour collections. The DMPS injections are generally given about six times or until the level drops into single digits or you are feeling better.
For pediatric patients
You can click here to find out why I don’t recommend DMSA mercury chelation. Since an IV is such a traumatic event for most children it is probably wise to use a rectal suppository version of DMPS which is available from most compounding pharmacists. Another alternative is to apply the dose transdermally with DMSO. This is very similar to the way that the hormone secretin is being used for many autistic patients.
The dose is 5 mg of DMPS per kg of body weight and is generally given once a month. The urine collection for pediatric patients incorporates a bag to collect the urine for mercury analysis.
DMPS Alternative
Some people do not tolerate DMPS well. This is especially true for those who have damage in the central nervous system, such as those with MS or ALS or children with fragile brain architecture. If this is the case there are several options. PCA (peptid clathrating agent) spray can be used. The dose is 4 sprays under the tongue every day or every other day. One may use a dipeptide amino acid or mixed mineral succinates such as Champion Nutrition Muscle Nitro.
from WordPress http://ift.tt/2ppijCb
via IFTTT
0 notes
Text
Berend Verhoeff, Autism in flux: a history of the concept from Leo Kanner to DSM-5, 24 History of Psychiatry 442 (2013)
Abstract
In this paper, I argue that a new relation between past and present – a supposed historical continuity in the meaning of autism – is created by the histories written by the discipline itself. In histories of autism written by ‘practitioner-historians’, a sense of scientific progress and an essentialist understanding of autism legitimize and reinforce current understandings and research directions in the field of autism. Conceptual discontinuities and earlier complexities and disputes concerning classifying and delineating autism are usually left out of the positivist narrative of autism. In an alternative history of the concept of autism, I demonstrate that there have been major shifts in the type of symptoms, signs and impairments that were – and are – thought to be essential and specific for autism.
Introduction
With the latest fifth edition of the American Psychiatric Association’s Diagnostic and Statistical Manual for Mental Disorders (APA, 2013), the history of autism enters a new era. The Neurodevelopmental Disorders (ND) Work Group, responsible for the formation of criteria and diagnostic categories of autism and related disorders, included Asperger’s disorder, along with PDD-NOS1 and autistic disorder, in the new category of autism spectrum disorder (ASD). The main argument for the creation of one ASD category was that ‘there is little evidence to support the current diagnostic distinction between Asperger disorder and high-functioning autism’ (Happé, 2011: 541). Studies that compared clinical and demographic characteristics, neuropsychological profiles, comorbidity and prognosis between autism and Asperger’s disorder did not, in the main, support a diagnostic distinction between the two diagnostic categories (Witwer and Lecavalier, 2008). As stated by one of its prominent members, the DSM-5 ND Work Group’s aim in proposing the new ASD category was to ‘recognize the essential shared features of the autism spectrum’ (Happé, 2011: 541, emphasis added).
In the Work Group’s reflection on the current state of autism research, autism is depicted as a discoverable entity with particular trans-historical essential features, and autism research is presented as a growing body of scientific knowledge in relation to that particular entity. With this conception of autism and autism research, current developments and decisions concerning autism in DSM-5 have become a logical and inevitable outcome of the present state of autism research. Furthermore, the dominant positivist understanding of autism underlies recent debates on the existence or non-existence of an autism epidemic and it underlies the current tenacious search for autism’s neurobiological essence (see Verhoeff, 2012). This particular understanding of autism is being reinforced by the histories written by the discipline itself, depicting a more or less chronological, linear and progressive development towards current understandings of autism. However, this paper will illustrate that this is a limited representation of autism and its history.
For a better understanding of what is happening in the field of autism today, it is essential to explore its historical development in more detail. As stated by the Polish medical doctor and philosopher of science Ludwik Fleck, ‘at least three-quarters if not the entire content of science is conditioned by the history of ideas, psychology, and the sociology of ideas and is thus explicable in these terms’ (Fleck, 1935/1979). The primary aim of the present paper is to explore the historical development of scientific ideas about autism in more detail, with a particular focus on how autism has been conceptualized since Leo Kanner (1894–1981) first described autism as a distinct nosological entity. Thereby, a new perspective on the idea of an autism spectrum and on the rise and fall of Asperger’s disorder will emerge.
In the first part of this paper, some historiographical points will be made, and I will demonstrate a specific way in which the discipline’s history is being reorganized according to current understandings of autism. I will argue that a new relation between past and present – a supposed historical continuity in the meaning of autism – is created through historical perceptions and references to classic autism studies. The second part of this paper presents an alternative history of the concept of autism that challenges the general sense of continuity and progress. Instead of emphasizing the widely presumed historical stability of the core meaning of autism, I focus on the historical irregularities that are often overlooked, denied or misunderstood.
Even so, it is often noted that autism has gone through major changes since Leo Kanner first described the syndrome in 1943. Explanatory theories, interventions, public awareness and specialist services have clearly changed considerably over the past 70 years. In addition, a progressive broadening of the concept of autism is generally accounted for in, for instance, explanations for the extraordinary rise in the number of people diagnosed with autism (see e.g. Fombonne, 2005; Wing and Potter, 2002). As is visible through an evident widening of diagnostic criteria for autistic disorder in successive editions of the DSM, the broadening of the concept of autism is unambiguous. However, the exact nature and scope of this broadening remain largely opaque and unexplored. I suggest that there has not just been a dimensional broadening, but that there have been major shifts in the specific type of symptoms, signs and impairments that were – and are – thought to be essential and specific for autism.
Recurrent histories of autism
Books on the history of autism are not as numerous as autism novels, parent guides, autobiographies and textbooks. Of the small number of histories that are available, there is a wide variety of depth and specific focus of historical attention. Some recent histories of autism have as their object the pioneers in research, treatment and care (Feinstein, 2010), the role of parents and parent organizations (Silverman, 2011), or the social and cultural conditions that made autism possible (Eyal et al., 2010; Nadesan, 2005). However, most histories of autism have been written by autism researchers and experts – or ‘practitioner-historians’ – often as an introductory first chapter to the topic in text- and handbooks, or as a short introduction in review articles or empirical studies. A common denominator of these latter histories is that they approach their main object – autism – as a static, decontextualized ‘thing’, discoverable by science. Moreover, these histories present a more or less chronological, linear and progressive development towards an ‘inevitable’ current understanding of autism, while mentioning the myths, mistakes, struggles and scientifically unsound convictions of earlier darker periods. For example:
We have come a long way from the era of myths and legends, through the unhappy deviation into psychoanalysis, to the practical realism of the present day that is accepted by most, though sadly not all, professionals in the field. We now know that there is a wide spectrum of autistic conditions, with Kanner’s and Asperger syndromes each forming only a part of these. (Wing, 1997: 20)
Such histories might seem to be little more than the memory of a science and a subordinate distraction from what the topic is really about, but if we follow the French historians and philosophers of science, particularly Gaston Bachelard (Gutting, 1987) and Georges Canguilhem (1994), a discip-line’s history has become a central part of the discipline itself. In a discipline’s history there is ‘the tendency to see the history of the subject in the light of today’s truth, which is easily confused with eternal truth’ (Canguilhem, 1994: 42). A discipline’s history serves as an important legitimization of a science, with the current knowledge about a subject matter as a necessary endpoint of scientific development; it confirms the idea, favourable to the discipline, of a science as a rational inquiry with a coherent accumulation of knowledge through history. The historical awareness of scientists is ‘recurrent’ in a sense that:
The history they construct for themselves is always constructed from the present and its criteria for truth. The perspective of the present reorganizes the past according to its own relevances. A mutation in current conceptions of scientific truth brings elements from past and present into new relations … Hence, as science corrects its errors, it rewrites its history. (Rose, 1998: 166)
In the field of autism, two types of frequently combined ‘recurrent histories’ can be distinguished. The first I call ‘positivist histories’. These emphasize the progressive and cumulative nature of knowledge about autism and the maturation of the research field, while judging earlier theories, interventions and perspectives in the light of current expert convictions.
‘The history of ideas on autism: legends, myths and reality’ (1997) by Lorna Wing, British psychiatrist and autism expert, makes a clear example of a positivist history of autism. She depicts the idea of a spectrum of autistic conditions as something in nature that was out there waiting to be discovered through a laborious process in which plain myths and Freudian mistakes had to be defeated by proper science. This resulted in ‘the increasing knowledge of the nature of autistic disorders’ (p. 20). Earlier aetiological hypotheses of autism attributing an important role to psychogenic causes, of which the infamous ‘refrigerator mother’2 received most attention, are discarded as ‘unhappy deviations’ since current research has shown that ‘complex genetic factors are important in the causation but there are other physical causes that can lead to autistic conditions’ (p. 20). Earlier ideas on autism are neatly divided into plain myths or reality, and earlier legends in the field are deemed either right or wrong. Current knowledge about autism acts as an endpoint and norm to judge history, while knowledge about autism cumulated in a linear and chronological way towards the contemporary view that ‘autistic spectrum conditions are developmental disorders caused by physical abnormalities in parts of the brain’ (p. 20).
The recursive process in positivist histories of autism can be noticed by focusing on how autism researchers refer to earlier criteria and understandings of autism. In choosing the diagnostic criteria for autism in DSM-IV (APA, 1994), Waterhouse, Wing, Soitzer and Spiegel (1992) provide a history of the development of the criteria for autism in DSM-III-R (APA, 1987). They state that the DSM-III-R criteria:
represent a reorganization and elaboration of DSM-III criteria that reflect a return to the criteria of Kanner’s (1943) original case study descriptive accounts of impaired sociability, impaired social communication, and the presence of stereotypies or repetitive behaviors. (Waterhouse et al., 1992: 531)
Besides the suggested fundamental continuity in diagnostic criteria for autism, the ‘triad of autistic impairments’ popularized by Wing and Gould (1979), is rather unproblematically projected onto Kanner’s original description of early infantile autism. The ‘extreme autistic aloneness’ mentioned by Kanner (1943: 242, original italics) is nevertheless quite different from impaired sociability, just as impaired social communication is different from the severe deficits in language development that were illustrated by Kanner, such as complete muteness and (delayed) echolalia. In addition, for Kanner, ‘the child’s behavior is governed by an anxiously obsessive desire for the maintenance of sameness that nobody but the child himself may disrupt’ (Kanner, 1943: 245, original italics). An extreme resistance to changes in restricted routines and rituals or changes in furniture arrangements is again in many ways distinct from the ‘presence of stereotypies or repetitive behaviors’.
The point here is that in a brief historical reference, Kanner’s work is confidently connected to recent criteria of autism, with a suggestion of both continuity and refinement. Volkmar (1998: 46) similarly claims that the DSM-IV (APA, 1994) and ICD-10 (WHO, 1993) diagnostic systems have a ‘fundamental continuity with the original description of autism made by Leo Kanner (1943)’. Volkmar (1998: 46) suggests that Kanner emphasized as central to the definition of autism: ‘the characteristic impairment of social interaction’. Earlier ‘truth’ about autism is thus coloured in the light of current ‘truth’ and the connections between them are being reinterpreted to legitimize and reinforce the current status of autism research.
The increasingly popular practice of retrospectively diagnosing historical figures with autism is part of what I call ‘essentializing histories’ of autism. These particular histories are not primarily concerned with the development of the scientific field, but above all with affirming the validity and trans-historical continuity of the specific object under study: autism. Apart from being a recognizable disorder (Frith, 1989; Volkmar, 1998), autism is currently first and foremost ‘a highly herit-able neurodevelopmental disorder’ (Mosconi et al., 2010) and ‘among the most heritable of all mental disorders’ (Lichtenstein et al., 2010). If autism is such a recognizable phenomenon and if it is a current fact that autism is a heritable brain disorder, traces of autism must be found in distant pre-Kannerian times.
Indeed, traces have been found. Historical accounts of feral children, eccentric geniuses, religious figures and even fictional literary protagonists have been productive for retrospectively diagnosing autism. To name only some of those diagnosed, there are ‘The blessed fools of Old Russia’ (Challis and Dewey, 1974), the extraordinary case of Hugh Blair of Borgue in eighteenth-century Scotland (Houston and Frith, 2000) and, according to Fitzgerald’s (2005) endless list, Isaac Newton, Michelangelo, Ludwig Wittgenstein and Albert Einstein.3 According to Frith (1989: 17), retrospective diagnosing helps to ‘distil those features that are the essence of the disorder beyond our immediate time and cultural context’. She points out that ‘autism is not a modern phenomenon, even though it has only been recognized in modern times’ (Frith 1989: 16), and she and Houston try to find what they call ‘the unchanging core of autism’ (Houston and Frith, 2000: 4). However, it is this assumed trans-historical, essential core of today’s autism that is being recognized in the many recent examples of peculiar historical figures, and these historical cases, in turn, support the legitimization of the current ‘tenacious search for autism’s essence’ (Verhoeff, 2012) at neurobiological levels. It is only in present times that these peculiar historical figures have become part of the history of autism.
Three phases in the history of the concept of autism
The following history of autism will not explicitly search for explanations, causes, events, decisive scientific moments or the final truth about autism. Nor will it trace, like the histories of Nadesan (2005) and Eyal et al. (2010), the socio-political, economic, ideological and technical factors that might have made the emergence and reshaping of autism possible. These histories give important and detailed accounts of the role of parental activism; the availability of new treatments and services; the demand for educable conditions; and the reorganization of expertise, in understanding shifts in thinking about autism. However, the aims for the second part of the present paper are different, and the primary aim of the following history of autism is to give a basic description of the development of scientific notions of autism.
With landmark scientific articles, definitions, diagnostic criteria, case studies and descriptions of characteristic phenomena, ideas about what makes a typical case of autism will be reviewed. However, a straightforward and unambiguous identification of earlier notions of autism is a chimera. Ideas about autism are not fixed but constantly in flux. There is not a single test, definition, article or researcher that marks a definite idea of autism in a specific period. Hence, a history of the concept of autism will always remain an imperfect approximation of a general (scientific) sense of the meaning of autism at a particular moment in time. Yet in the history of ideas about the characteristic features of autism, three periods can be distinguished. However, these periods are not marked by clear events and probably reflect more gradual and partial – rather than radical or revolutionary – changes, and they are above all a heuristic for structuring the historical analysis and for helping to bring to light important modifications in thinking about autism.
Phase 1: Extreme autistic aloneness and insistence on sameness (1943–65: Leo Kanner)
Most histories of autism start with Kanner, a pioneer in the field of child psychiatry and the founder of the first clinic for children with psychiatric problems at John Hopkins University in Baltimore. He introduced the diagnostic category of childhood autism in his famous and canonical case series of 11 children with ‘autistic disturbances of affective contact’ (Kanner, 1943). This was indeed the moment that autism, as a separate and unique psychiatric entity, became visible for the first time. However, if we want to retrieve the specific meaning of this new disorder, it might be better to start with the well-known Swiss psychiatrist Eugen Bleuler. He had already coined the term ‘schizophrenia’ in 1908, and was the first to use the word ‘autism’ somewhere around 1910 (Kuhn, 2004). He began using the term ‘autism’ to refer to what he considered to be one of the most important symptoms of schizophrenia.4 Together with association loosening, ambivalence and affect inappropriateness (Berrios, 1996), autism was one of the primary symptoms of schizophrenia, and it was characterized by ‘a definite withdrawal from the external world’ (Bleuler, quoted in Kanner, 1973: 94).5 In the decade after its introduction, Bleuler’s use of the term started to develop and expand to include a more moderate and non-pathological form of ‘autistic thinking’ that included daydreaming and fantasy (see Bleuler, 1919).
For Frith (1991), and for many other contemporary autism researchers, Bleuler’s schizophrenic autism and autistic thinking are unrelated to the disorder that came to be referred to by the same name. As Frith (1991: 38) notes, ‘autistic thinking in Bleuler’s sense has nothing to do with autism as we know it’. Maybe, if we think of the recursive processes that are active in rewriting the history of autism, it is because of the current disconnection between autism and schizophrenia that Bleuler seems to have disappeared from the discipline’s history.6 However, it was not without reason that Kanner borrowed Bleuler’s (by then) popular term.7 As Nadesan (2005: 40) says, it is not surprising that ‘Leo Kanner and Hans Asperger elected to describe their patients in terms of the concept of autism. Autism was a phrase with wide currency and applicability, particularly in German psychiatry’.8 Bleuler’s autism, which describes a certain break with reality combined with other dissociations of affect, provided the framework for Kanner to introduce a new diagnostic category. In a discussion on the problems of nosology and psychodynamics of early infantile autism, Kanner (1949: 418) considers that ‘the extreme isolation from other people, which is the foremost characteristic of early infantile autism, bears so close a resemblance to schizophrenic withdrawal that the relationship between the two conditions deserves serious consideration’ and early infantile autism ‘may be looked upon as the earliest possible manifestation of childhood schizophrenia’ (p. 419). In one of his later articles, Kanner (1973: 94, original italics) explains that ‘in my search for an appropriate designation, I decided on the term early infantile autism, thus accentuating the time of the first manifestations and the children’s limited accessibility’. Kanner recognized in his autistic patients a remoteness from affective contact with other people, similar to the remoteness of Bleuler’s schizophrenic patients.
However, unlike Bleuler’s schizophrenic patients, who withdrew from previous participation, Kanner’s children never participated in the first place. They began ‘their existence without the universal signs of infantile response’ (Kanner, 1973: 94). Furthermore, as Kanner pointed out, ‘they develop a remarkable and not unskillful relationship to the inanimate environment’ (p. 95). Instead of a turning away from the external world, Kanner’s autistic patients ‘can cling to things tenaciously, … They are so concerned with the external world that they watch with tense alertness to make sure that their surroundings remain static’. Despite a fundamental aloofness that relates the two autisms, and despite Kanner’s explicit recognition of an intrinsic relationship between his autism and Bleuler’s (group of) schizophrenia(s), he concluded that his early infantile autism ‘does not seem to fit in with Bleuler’s criteria for autism’ (Kanner, 1973: 95).
Let us get back to Kanner’s landmark case series that for the first time illustrated the new psychiatric condition he designated early infantile autism. Donald T. – his first and most detailed case – was a remarkable little boy who was happiest when left alone. He did not seem to notice when someone entered or left the room he was in, and he was indifferent to visiting relatives, potential playmates, and he even failed to pay the slightest attention to Santa Claus in his full costume. When petted he showed no apparent affection and he gave the impression of being self-sufficient. At the age of two he developed an obsession for spinning blocks and pans and virtually all round objects that could be spun. A spinning pan for instance, could keep him fascinated for hours and, when interfered with, he had destructive temper tantrums. The majority of his actions were endless repetitions performed in exactly the same way as they had been carried out originally. Furthermore, he never spontaneously spoke just to chat or to share his thoughts. When he spoke, he seemed either to ejaculate irrelevant utterances randomly, such as ‘chrysanthemum’ or to parrot what he had heard said to him at some other time (Kanner, 1943).
After the description of 10 more cases, Kanner’s paper ends with a discussion of a number of common characteristics of early infantile autism that appear essential. Among them are:
an extreme autistic aloneness … [a] limitation in the variety of spontaneous activity … performances [and verbal utterances that] are monotonously repetitious … the child’s behavior is governed by an anxiously obsessive desire for the maintenance of sameness … [the child has] excellent rote memory. (Kanner, 1943: 242–3, original italics)
Certain language problems are also mentioned. In later papers, Eisenberg and Kanner (1956: 557) present a somewhat stricter definition of early infantile autism:
In the light of experience with a tenfold increase in clinical material, we would now isolate these two pathognomonic features, both of which must be present: extreme self-isolation and the obsessive insistence on the preservation of sameness, features that may be regarded as primary, employing the term as Bleuler did in grouping the symptoms of schizophrenia.
Kanner investigated the phenomenon – fundamental for autism – of ‘obsessive desire for the preservation of sameness’ in more detail in a separate study (Kanner, 1951). He argued that the autistic child desires ‘to live in a static world, a world in which no change is tolerated … The slightest change of arrangements, sometimes so minute that it is hardly perceived by others, may evoke a violent outburst of rage’ (p. 23). Furniture arrangements, the arrangement of toy building blocks, beads or sticks, the precise route to school, and the position of the dishes on the table are typical examples of things that must not be changed. Autistic children, Kanner concluded, find ‘security in sameness, a security that is very tenuous because changes do occur constantly and the children are therefore threatened perpetually and try tensely to ward off this threat to their security’ (p. 26).
The frequently described problems with language and speech were not considered to be core features of autism. Although they are ‘often the most striking and challenging of the presenting phenomena, [they] may be seen as derivatives of the basic disturbance in human relatedness’ (Eisenberg and Kanner, 1956: 557). Furthermore, simple repetitive activities may be seen in severely retarded children and may offer a diagnostic problem, but ‘the presence of elaborately conceived rituals together with the characteristic aloneness serves to differentiate the autistic patients’ (p. 558).
Robinson and Vitale (1954) discussed another diagnostic problem for autism at the annual meeting of the American Orthopsychiatric Association in 1953. They presented three cases of children with circumscribed interest patterns and ‘a limited establishment of interpersonal relationships’ (Robinson and Vitale, 1954: 755). These children were all introvert, had average or above average intelligence, good language skills and circumscribed interests in rather unusual topics. Tom, for instance, was unable to participate in activities with other children, but developed an intense interest in and a hunger for knowledge about chemistry and finance by the age of eight years. Nine-year-old Billy had an ‘amazing knowledge of trolley routes and an unusual interest in and knowledge of calendars and maps’, and John, also nine years old, ‘preferred to play by himself’ and was ‘particularly interested in astronomy’ (pp. 758–9). The behaviour of these children shows a striking similarity with that of the children described by Hans Asperger (1944/1991) and they would probably now be diagnosed with Asperger’s disorder or high-functioning autism (Gillberg, 1998).
However, clearly unaware of Asperger’s earlier cases, Robinson and Vitale (1954: 760) explicitly distinguished these children from autistic children in ‘that they have not presented the early infantile incapacity for emotional responsiveness’. Furthermore, they ‘present a lesser degree of “withdrawal from contact with people” and a lesser measure of the “obsessive desire for the preservation of sameness”’ (p. 760). In a response to their article, Kanner himself agreed that autism was a different condition, and he added that the rituals and fixated patterns in autism were qualitatively and aetiologically distinct from the circumscribed interest patterns described by Robinson and Vitale. For as far as autistic children exhibit a circumscribed interest, it ‘has often been foisted on the children by their parents’ (Kanner in Robinson and Vitale, 1954: 766) and is not seen as a core feature of the syndrome.
Debates on the possible causes of autism erupted soon after Kanner’s original paper was published. Initially, Kanner (1943: 250) emphasized that autistic children ‘have come into the world with innate inability to form the usual, biologically provided affective contact’. Somewhat later, with the growing psychoanalytic influence in American psychiatry, he came to place a greater emphasis on psychogenic factors like the obsessive traits, emotional coldness and lack of affection that he saw in the parents (Eisenberg and Kanner, 1956). Arguing that ‘early infantile autism is a total psychobiological disorder’, Kanner often defended a middle course between a psychogenic and an innate biogenic origin of autism, which required ‘a comprehensive study of the dysfunction at each level of integration: biological, psychological, and social’ (Eisenberg and Kanner, 1956: 564). Various psychiatrists and psychologists argued that autism was mainly a psychogenic disorder (e.g. Bettelheim, 1967; Despert, 1951), whereas others regarded autism primarily as an organic brain disorder (Rimland, 1964; Rutter, 1968).
However, discussions on aetiology aside, Kanner’s first description of autism as a diagnostic entity, characterized by extreme emotional withdrawal and tenacious insistence on sameness, remained largely unchallenged for approximately the first two decades after its introduction. Despite discussions on the possible nosological relations between early infantile autism and (childhood) schizophrenia (Kanner, 1965), and despite some unsuccessful proposals to lump autism together with childhood schizophrenia, mental retardation and organic brain disease under the broad term ‘atypical child’ (Rank, 1949; Szurek, 1956), it was not until the 1960s that the concept of autism started to change.
Phase 2: Language and other perceptual and cognitive abnormalities (1960–80)
From the 1960s on, as early infantile autism slowly entered the public arena and organized research communities started to replace the earlier observation-based case descriptions with the first epi-demiological and experimental studies with autistic children, the concept of autism was altered significantly. Influenced by new types of investigation and new scientific methods, an important shift in emphasis occurred: from severe affective withdrawal as the essential defect in autism, towards language and other cognitive and perceptual abnormalities as essential and primary in autism. Whereas Eisenberg and Kanner (1956: 557) regarded ‘the vicissitudes of language development’ as derivatives of the fundamental disturbance in affective contact, many autism researchers in the 1960s and 1970s not only observed accurately but also actively tried to engage with the autistic child. They argued that the basic defect in autism was the inability to develop a normal use and understanding of language, in combination with a global defect in the integration of other sensory stimuli. In spite of the popular but barely empirically studied, often vague and contradictory hypotheses that autism had a psychogenic basis, deficits in language, speech and cognition became cardinal features and key characteristics in diagnosing and recognizing autism.
This new way of thinking about autism was backed up by empirical evidence from several new studies and methods in autism research. For instance, the first longitudinal studies on autism (Lockyer and Rutter, 1969) showed that Kanner’s primary disturbance in affective contact and the profound withdrawal tend to lessen considerably as the autistic child grows older, while other symptoms like language deficits and intellectual shortcomings tend to persist. The first systematic psychological experiments with autistic children (e.g. Frith, 1970; Hermelin and O’Connor, 1970) that tested intellectual (language and performance), receptive, integrative, and expressive abilities suggested that language and speech problems were not due to profound affective withdrawal or motivational failure, but instead due to a poor understanding of the meaning of spoken words. Furthermore, these experimental studies showed that the autistic child: had difficulties with the use and understanding of gesture; was particularly unresponsive to verbal stimuli; lacked the ability to associate words semantically; had difficulties with grammatical aspects of language; and made little use of concepts in memorizing. Additional difficulties with the transformation of information from one sensory modality to another and in perceiving temporal patterns in visually presented stimuli ‘suggested a central defect in the processing of any sort of coded, meaningful, or tempor-ally patterned stimuli’ (Rutter and Bartak, 1971: 27). A new discourse, profoundly influenced by the cognitive and computer sciences which were emerging at that time (see Gardner, 1987) and using terms like codes, processing, stimuli and sensory modalities, became dominant in investigating, recognizing and thinking about autism. Furthermore, in addition to the familiar observations and parents’ descriptions of the child’s behaviour, (neuro)psychological tests and experiments became an integral part of the diagnostic process.
More than a disorder of language, ‘the central problem, present in even the most mildly handicapped autistic people appears to be a specific difficulty in handling symbols, which affects language, nonverbal communication, and many other aspects of cognitive and social activity’ (Ricks and Wing, 1975: 214). In a review of concepts of autism, Rutter (1968: 21, original italics) explicitly states that ‘contrary to earlier views, infantile autism is not anything to do with schizophrenia, and is not primarily a disorder of social relationships’. Language and cognitive defects were thought to constitute the primary handicap in autism, with ‘the social and behavioral abnormalities arising as secondary consequences’ (Rutter and Bartak, 1971: 29). Kanner’s cardinal resistance to change and insistence on routines were also thought to be secondary and were explained by deficits in processing and integrating visual perceptual information (Wing and Wing, 1971).
This major shift in thinking about autism was reflected in the first formal diagnostic criteria for autism in DSM-III (APA, 1980). Besides a ‘pervasive lack of responsiveness to other people’, the second cardinal criterion became ‘gross deficits in language development’, and ‘if speech is present, peculiar speech patterns such as immediate and delayed echolalia, metaphorical language, [and] pronominal reversal’ were central in diagnosing autism (p. 89). The third and final criterion became ‘bizarre responses to various aspects of the environment, e.g., resistance to change, peculiar interest in or attachments to animate or inanimate objects’ (p. 90). The dominant theory of a basic defect in the use and understanding of language, in combination with a global defect in the integration of other sensory stimuli caused by deficits in processing and integrating perceptual information, reshaped and redefined how autism could be detected and recognized, and how the stereotypical autistic child was imagined. In spite of the ambition (of those involved in putting together the DSM-III) to produce ‘theory neutral’ descriptions of observable behaviour distinctive for each disorder (Spitzer and Cantwell, 1980), autism’s diagnostic criteria undeniably reflected theoretical commitments.
Phase 3: Deficits in social cognition and instinct (1980–present)
A second major shift in thinking about autism started some time in the early 1980s. I will highlight two events in the autism research field – with Lorna Wing playing a significant role in both of them – that anticipated, influenced and illustrate this second shift. The first event is one of the first epidemiological studies on autism, which was carried out in London. This study investigated the prevalence of social, language and cognitive impairments found in intellectually disabled children, and it investigated to what extent these distinct impairments tended to occur together (Wing, 1981b; Wing and Gould, 1979). From a larger sample, 132 children were selected on the basis of exhibiting at least one impairment in social interaction, language development, intellectual functioning or repetitive stereotyped behaviours. The value of this epidemiological approach, Wing (1981b: 32) argued, ‘was that it allowed the examination not only of “pure” syndromes but also of borderline and partial forms, within the context of a larger, geographically defined population’. The children were split into two groups. The first group consisted of sociable children ‘in whom social interaction was lively, positive, and a source of great pleasure’ and the second group consisted of socially impaired children ‘who were inappropriate in their social interaction’ (p. 34). This second group consisted not only of socially aloof and unresponsive children, but also included children who interacted passively and ‘amiably accepted approaches from others without initiating … [and children who] made peculiar one-sided approaches to others, approaches that were not adapted to the responses of the person approached’ (p. 34). The study subsequently demonstrated that the children with social impairments, the second group, all had ‘repetitive stereotyped behavior and almost all had absence or abnormalities of language and symbolic activities. Thus, the study showed a marked tendency for these problems to occur together’ (Wing and Gould, 1979: 25). In contrast, most of the children in the first sociable group had symbolic pretend play, and repetitive activities and language impairment were found in a minority of the sociable and severely retarded children.
Wing (1981b: 37) argued that ‘the abnormalities of social interaction, verbal and nonverbal communication, and imaginative activities so consistently occurred together … that they could be referred to as “the triad of social and language impairment”’; she thought that there was no clear division between Kanner’s autism and other less severe forms of social impairment. The nature of autism, Wing (1981b: 38) suggested, can only be understood ‘in the wider context of the triad of language and social impairment’, and Wing and Gould (1979: 25) argued that ‘the clustering of the social, language, and behavioral abnormalities … provided support for the main division into the socially impaired and the sociable though severely retarded groups’. This somewhat circularly justified division between ‘socially impaired’ and ‘sociable’ now provided a new basis for categorization, and social impairment became a central distinguishing aspect in the study of autism. Furthermore, social impairment was not understood as ‘extreme autistic aloneness’ but as a subtle deficit in the use and understanding of the ‘unwritten rules of social behavior’ (Wing, 1981b: 42).
The second important event was the introduction of the work of the Austrian paediatrician Hans Asperger (1906–80) into the Anglo-Saxon autism literature. Although Van Krevelen (1971) and a few others had already discussed Asperger’s cases of ‘Autistische Psychopathie’ (Asperger, 1944) in English, an article by Wing (1981a) followed by Frith’s 1991 translation of Asperger’s original cases aroused substantial international interest in what became known as Asperger’s syndrome. Based on four cases, Asperger (1944/1991) described a ‘particularly interesting and highly recognizable type of child’ (p. 37). This type of child exhibited ‘the essential feature of … a disturbance of adaptation to the social environment’ (p. 87). Apart from this essential feature, Asperger described a variety of behavioural and physical peculiarities in his cases, such as: odd, idiosyncratic or pedantic speech; absence of a sense of humour; little facial expression and limited gestures; an almost ‘aristocratic’ appearance; an over-sensitivity to criticism; manipulative, vindictive and antisocial acts; difficulties in learning simple practical skills; an absence of feelings of shame or guilt; hyper- or hyposensitivity to noise; extreme egocentrism; a lack of affection; clumsy movements; single-mindedness, as manifested in peculiar and limited interests; a gift for logical, abstract and original thinking; and more. Despite acknowledging certain similarities, Asperger (1979: 48) considered his autistic personality disorder to be basically different from Kanner’s autism:
Kanner’s early infantile autism is a near psychotic or even a psychotic state, though not identical with schizophrenia. Asperger’s typical cases are very intelligent children with extraordinary originality of thought and spontaneity of activity though their actions are not always the right response to the prevailing situation.
Furthermore, Asperger argued that his children developed highly grammatical speech, while Kanner’s children ‘generally avoid communication … [and] do not develop speech or develop it very late’ (p. 48). In contrast, Wing (1981a) argued that Asperger’s cases and Kanner’s cases were essentially similar. Despite the variations in terms of severity of impairments, Wing argued that both disorders shared a common and essential characteristic: the impairment of two-way social interaction.9 This impairment:
is not due primarily to a desire to withdraw from social contact. The problem arises from a lack of ability to understand and use the rules governing social behaviour. These rules are unwritten and unstated, complex, constantly changing, and affect speech, gesture, posture, movement, eye contact, choice of clothing, proximity to others, and many other aspects of behaviour. (Wing, 1981a: 116)
A new way of distinguishing and thinking about autism arose, influenced by: an international introduction of Asperger’s work; a growing awareness of the existence of Asperger’s new ‘type of child’; the recognized and emphasized similarities between Kanner’s and Asperger’s cases; and by Wing’s epidemiological study arguing that certain problems affecting early child development tend to cluster together. From a rare disorder characterized by a pervasive lack of responsiveness and gross deficits in language development, autism became first and foremost a disorder of sociality. The lack of intuitive skills that make complex social interaction possible is now central in yet again a new way of conceptualizing autism. Next to psychiatric and psychological assessments and tests, information on a child’s (dys)functioning at school, among peers and in other social activities gets a central position in diagnosing autism.
This way of thinking about autism became more explicit and formalized in the revised version of DSM-III. In only seven years, the criteria for autistic disorder in DSM-III-R (APA, 1987) changed remarkably compared with the earlier criteria for autism in DSM-III (APA, 1980). A ‘pervasive lack of responsiveness to other people’ (DSM-III) changed into ‘qualitative impairment in reciprocal social interaction’ as, for instance, manifested by ‘no or abnormal seeking of comfort at times of distress’ or ‘gross impairment in ability to make peer friendships’ (DSM-III-R). Likewise, ‘gross deficits in language development’ were no longer central to or necessary for an autism diagnosis and were replaced by a new domain of ‘qualitative impairments in verbal and nonverbal communication’. This domain included ‘marked abnormal nonverbal communication’ and ‘marked impairment in the ability to initiate or sustain a conversation with others, despite adequate speech’ (DSM-III-R). Furthermore, whereas DSM-III required an onset before 30 months of age, autism lost its adjective ‘infantile’ and became ‘autistic disorder’ in DSM-III-R. Autistic disorder could now be diagnosed not only during infancy but also during childhood when (latent) more subtle problems with social interaction and communication become visible.
DSM-5 and the short life of Asperger’s disorder
Debates about whether Asperger’s disorder is a distinct nosological entity, identical with ‘high-functioning’ autism or part of a broader autism spectrum started right after the publication of Wing’s (1981a) influential article (see Macintosh and Dissanayake, 2004). On the eve of the publication of DSM-IV (APA, 1994), Rutter and Schopler (1992: 476) argued: ‘As there is an obvious research need to compare autism with Asperger syndrome, we suggest that there is a need for a … category for Asperger syndrome in order to encourage and facilitate that research’. Mainly for research purposes, Asperger’s disorder became a distinct DSM diagnostic category in 1994 (Szatmari, 1992). However, the concept of autism had already been influenced by Asperger’s ‘type of child’, and the essential ‘disturbance of adaptation to the social environment’ (Asperger, 1944/1991: 87) of Asperger’s children had become the central characteristic of autism in the 1980s.
In order to assess the validity of viewing Asperger’s disorder as a distinct category, and to compare Asperger’s disorder with autistic disorder on multiple characteristics such as course, prognosis, neuropsychological profiles and underlying neurobiological markers, Rutter and Schopler (1992: 476) acknowledged that it would be necessary ‘to define the syndrome in such a way that there is no overlap with autism’. However, despite the fact that Michael Rutter was a member of the Work Group responsible for creating criteria for autism and related disorders in DSM-IV, criteria for Asperger’s disorder and autistic disorder hardly differ in DSM-IV. Both disorders require ‘qualitative impairment in social interaction’ and ‘restricted repetitive and stereotyped patterns of behavior, interest, and activities’. The major differences are that for a diagnosis of Asperger’s disorder ‘there are no clinically significant delays in language’ (APA, 1994: 75) and that for autistic disorder ‘qualitative impairments in communication’ are required. But, as we have seen, delays in language were no longer at the core of, or necessary for, a diagnosis of autistic disorder, and most people who meet criteria for Asperger’s disorder also show ‘marked impairment in the ability to initiate or sustain a conversation’ sufficient to meet the impairments in communication criteria for autistic disorder. Because of this significant overlap of the two disorders, in combination with ‘the precedence rule: diagnose Asperger disorder only if criteria for autistic disorder are not met’ (Happé, 2011: 541), several autism researchers even concluded that a diagnosis of Asperger’s disorder is impossible using DSM-IV criteria (Mayes, Calhoun and Crites, 2001; Szatmari et al., 1995).
The problems with applying the DSM-IV Asperger’s disorder criteria resulted in wide variation in how the term Asperger’s disorder was, and still is, used in clinical practice and research (Happé, 2011). Lord and colleagues (2012) recently showed that the best predictor of an Asperger’s disorder diagnosis is not the characteristics of the individual, but the specific clinic the individual goes to. In defence of the decision to insert Asperger’s disorder into the new category of autism spectrum disorder (ASD), Work Group member Happé explains that ‘There is no evidence of differential treatment response or etiology to date, and claims for a distinct neurocognitive profile in Asperger disorder have received mixed results’ (Happé, 2011: 540). He concludes that ‘there is little evidence to support the current diagnostic distinction between Asperger’s disorder and high-functioning autism’ (p. 541).
However, as the history of the concept of autism reveals, even before Asperger’s disorder became an official diagnostic category in the 1990s, Asperger’s ‘autistic psychopathy’, and Wing’s interpretation of it, influenced a shift in thinking about autism in the early 1980s. Wing (2005: 198) later acknowledged that she ‘always considered Asperger’s syndrome to be part of the autistic spectrum. It shares the impairments of social interaction, social communication and social imagination and the repetitive pattern of activities and interests that characterize the spectrum’. It is not just the lack of empirical ‘evidence to support the diagnostic distinction’ between autistic disorder and Asperger’s disorder, but also this earlier broad interpretation of autism as ‘the absence or impairment of the social instinct’ (p. 201) that made the separate category of Asperger’s disorder scientifically fragile. The impossible task of contrasting a new category with an already very broad conceptualization of autism made defining Asperger’s disorder as a distinct diagnostic category rather prospectless even before it officially existed. Additionally, the seemingly recent introduction of an ‘autism spectrum’ is not as new as it might seem, but just a new term for an already accepted and established understanding of autism as a wide and heterogeneous disorder of social contact.
The DSM-5 Work Group for neurodevelopmental disorders might make history repeat itself by the introduction of, next to ASD, a new category of Social Communication Disorder (SCD). Even though history is often unsuited for predicting future developments, the introduction of this category resembles the introduction of Asperger’s disorder in DSM-IV and PDD-NOS in DSM-III-R. As a residual category for those who did not fully fit the autistic disorder category, PDD-NOS was thought ‘to describe the (very rare) children who appear to merit special diagnostic notation’ (Cohen, Paul and Volkmar, 1986: 217, emphasis added), but PDD-NOS became far more commonly diagnosed than autistic disorder (Chakrabarti and Fombonne, 2001). Today, the DSM-5 will include SCD ‘to describe the rare individuals who display significant social/communication impairments of ASDs without restrictive/repetitive behaviors’ (Mahjouri and Lord, 2012, emphasis added). However, Lord argues elsewhere that ‘How many individuals fall into this group is not clear … No data are yet available about its reliability, validity or prevalence’ (Lord and Jones, 2012: 499). It is unclear if and how SCD is different from ASD, for instance, in terms of aetiology, symptom profile and management. Furthermore, as Ozonoff (2012) pointed out, it seems ‘logically and internally inconsistent for the DSM-5, so pioneering in its dimensional approach, to introduce a separate category that is so qualitatively similar to another condition’ (original italics). The way in which SCD enters the DSM is highly reminiscent of the way in which Asperger’s disorder entered it, and I would not be surprised if it becomes far more commonly diagnosed than ASD and if it then – just like Asperger’s disorder – disappears again to be incorporated into the qualitatively similar autism spectrum.
Conclusions
This historical analysis of the concept of autism might not be directly helpful for a deeper understanding of why ideas about autism have changed, but it is a necessary first step towards such an understanding as it illustrates how autism as an object of scientific inquiry and clinical practice evolved and mutated. More than just a broadening of the concept or an inclusion of milder forms of an essentially similar deficit, what is considered essential in autism has gone through major changes, from profound affective withdrawal and aloofness, to language and other perceptual and cognitive abnormalities, to deficits in social cognition and intuition. In addition, the rise and fall of Asperger’s disorder is not an inevitable result of scientific scrutiny, but deeply bound to earlier conceptualizations of autism and Asperger’s disorder.
Contrary to the assertions of ‘practitioner-historians’ who argue that ‘Ever since Kanner’s first descriptions in 1943 … there has been agreement on the core symptoms’ (Sponheim, 1996: 513), this history makes room for unacknowledged discontinuities and irregularities, which are often found in the same canonical texts that are used for the positivist and essentialist narrative of autism. In this narrative, a sense of progress indirectly legitimizes current understandings, research directions, and decisions concerning classifying autism in DSM-5, while conceptual discontinuities and earlier complexities and disputes concerning classifying and delineating autism are left out. One tends to see and describe those aspects of earlier accounts of autism that corroborate current views of autism and thereby confirm the validity of autism as a recognizable disease characterized by a particular essential or core deficit.
However, in describing the reshaping of the concept of autism, the historicity, provisionality and plurality of knowledge and truth about autism become apparent. As a consequence, such a historical reflection destabilizes the present ‘truth’ about autism as a neurodevelopmental spectrum disorder of social cognition localized in an individual’s brain, and as it destabilizes the present ‘truth’ it creates space for other possible perspectives and conceptualizations of autism in the present and future. The point is, however, not to dismantle the very idea of autism, but merely to correct a positivist and essentialist understanding of autism as a discrete and stable entity in nature that we get to know and understand better and better as science progresses and knowledge accumulates.
Notes
Pervasive Developmental Disorder Not Otherwise Specified, also considered part of the autism spectrum.
The creation and popularization of this term ‘refrigerator mother’ is often attributed to Bruno Bettelheim – for many years most popular public autism expert – and his widely read book The Empty Fortress (1967).
Michael Fitzgerald, Professor of Child and Adolescent Psychiatry, diagnosed most of these historical geniuses with Asperger’s disorder. From the perspective of ‘recurrent histories’ of autism, it will be interesting to follow up on what will happen with his huge amount of retrospective diagnoses of Asperger’s disorder now that Asperger’s disorder ceases to be an official diagnosis in DSM-5.
Bleuler looked upon schizophrenia not as a distinct disease entity but as a common name for a group of particular symptoms. He referred to this group by speaking of the ‘group of the schizophrenias’ and not of schizophrenia in the singular (Berrios, 1996).
For more on Bleuler’s conception of schizophrenia and autism, see e.g. Berrios (1996); Bleuler (1911); Gundel and Rudolf (1993).
6. For instance, Bleuler is not mentioned in the history of autism by Wing (1997).
The nature of autism as a symptom of schizophrenia and the nature of autistic thinking were actively debated in psychiatric circles in the 1920s and 1930s, for example by Ernst Kretschmer and Hans Gruhle (Gundel and Rudolf, 1993).
Asperger (1944) introduced the term ‘autistic psychopathy’ only one year after Kanner (1943) introduced his ‘early infantile autism’, and there is much speculation and debate (e.g., in Feinstein, 2010; Eyal et al., 2010) about how it is possible that these two clinicians came up with very similar and new childhood disorders almost at the same time, while they were ‘separated by an ocean and a war’. Hacking (2006: 4) argues that this is certainly not a coincidence, as ‘Asperger, a generation younger than Kanner, had trained under August Homburger, the author of one of Kanner’s main German textbooks, who wrote about childhood schizophrenia and other developmental disorders. They came from the same medical culture (each had served in the Austrian army, although in different wars)’.
Timimi, McCabe and Gardner (2011) highlight the differences between Asperger’s cases and Wing’s (1981a) case descriptions of children she diagnosed with Asperger’s disorder. For example, most of Wing’s cases started talking late, whereas Asperger’s cases talked early. Furthermore, ‘most of Wing’s cases were described as having little capacity for analytical thought whereas Asperger’s cases were thought by him to be highly analytical. None of Wing’s cases could be described as manipulative, mendacious, cheeky, confrontational or vindictive (terms of description used by Asperger about his cases)’ (Timimi et al., 2011: 61). Timimi et al. (2011) argue that Wing’s understanding of Asperger’s disorder was fundamentally different from Asperger’s own understanding of the condition he delineated. This created a misleading link between Asperger’s and Kanner’s cases.
References
APA (1980) Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition (DSM-III). Washington, DC: American Psychiatric Association.
APA (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition-Revised.(DSM-III-R). Washington, DC: American Psychiatric Association.
APA (1994) Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV). Washington, DC: American Psychiatric Association.
APA (2013) Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). Washington, DC: American Psychiatric Association.
Asperger H (1944) Die “Autistischen Psychopathen” im Kindesalter.
Archiv für Psychiatrie und Nervenkrankheiten
117: 76–136; translated and annotated as: Autistic psychopathy in childhood. In: Frith U (ed.) Autism and Asperger Syndrome (1991). Cambridge: Cambridge University Press, 37–92.
Asperger H (1979) Problems of infantile autism. Communication 13: 45–52.
Berrios GE (1996) The History of Mental Symptoms: Descriptive Psychopathology since the Nineteenth Century. Cambridge: Cambridge University Press.
Bettelheim B (1967) The Empty Fortress: Infantile Autism and the Birth of the Self. New York, NY: Free Press.
Bleuler E (1911) Dementia Praecox oder Gruppe der Schizophrenien. Leipzig and Vienna: Deuticke.
Bleuler E (1919) Consciousness and association. In: Jung CG, Eder MD (eds) Studies in Word Association: Experiments in the Diagnosis of Psychopathological Conditions Carried Out at the Psychiatric Clinic of the University of Zurich. New York: Moffat, Yard & Company, 266–296.
Canguilhem G (1994) A Vital Rationalist: Selected Writings from Georges Canguilhem. New York: Zone Books.
Chakrabarti S, Fombonne E (2001) Pervasive developmental disorders in preschool children. JAMA: The Journal of the American Medical Association 285(24): 3093–3099.
Challis N, Dewey HW (1974) The blessed fools of Old Russia. Jahrbücher für Geschichte Osteuropas 20: 1–11.
Cohen DJ, Paul R, Volkmar FR (1986) Issues in the classification of pervasive and other developmental disorders: toward DSM-IV. Journal of the American Academy of Child Psychiatry 25(2): 213–220.
Despert JL (1951) Some considerations relating to the genesis of autistic behavior in children. American Journal of Orthopsychiatry 21(2): 335–350.
Eisenberg L, Kanner L (1956) Early infantile autism, 1943–55. American Journal of Orthopsychiatry 26: 556–566.
Eyal G, Hart B, Onculer E, Oren N, Rossi N (2010) The Autism Matrix. Cambridge: Polity Press.
Feinstein A (2010) A History of Autism: Conversations with the Pioneers. Oxford: Wiley-Blackwell.
Fitzgerald M (2005) The Genesis of Artistic Creativity: Asperger’s Syndrome and the Arts. Philadelphia, PA: Jessica Kingsley Publishers.
Fleck L (1979) Genesis and Development of a Scientific Fact. Chicago: University of Chicago Press; originally published in German in 1935.
Fombonne E (2005) The changing epidemiology of autism. Journal of Applied Research in Intellectual Disabilities 18: 281–294.
Frith U (1970) Studies in pattern detection in normal and autistic children. II. Reproduction and production of color sequences. Journal of Experimental Child Psychology 10(1): 120–135.
Frith U (1989) Autism: Explaining the Enigma. Oxford: Blackwell.
Frith U (1991) Autism and Asperger Syndrome. Cambridge: Cambridge University Press.
HE (1987) The Mind’s New Science: A History of the Cognitive Revolution. New York: Basic Books.
Gardner HE (1987) The Mind’s New Science: A History of the Cognitive Revolution. New York: Basic Books.
Gillberg C (1998) Asperger syndrome and high-functioning autism. British Journal of Psychiatry 172: 200–209
Gundel H, Rudolf GA (1993) Schizophrenic autism. 1. Historical evolution and perspectives. Psychopathology 26(5–6): 294–303.
Gutting G (1987) Gaston Bachelard’s philosophy of science. International Studies in the Philosophy of Science 2(1): 55–71.
Hacking I (2006) What is Tom saying to Maureen? London Review of Books 28(9): 3–7.
Happé F (2011) Criteria, categories, and continua: autism and related disorders in DSM-5. Journal of the American Academy of Child and Adolescent Psychiatry 50(6): 540–542.
Hermelin B, O’Connor N (1970) Psychological Experiments with Autistic Children. Oxford: Pergamon.
Houston R, Frith U (2000) Autism in History: The Case of Hugh Blair of Borgue. Oxford: Blackwell.
Kanner L (1943) Autistic disturbances of affective contact. Nervous Child 2: 217–250.
Kanner L (1949) Problems of nosology and psychodynamics of early infantile autism. American Journal of Orthopsychiatry 19(3): 416–426.
Kanner L (1951) The conception of wholes and parts in early infantile autism. American Journal of Psychiatry 108(1): 23–26.
Kanner L (1965) Infantile autism and the schizophrenias. Behavioral Science 10(4): 412–420.
Kanner L (1973) The birth of early infantile autism. Journal of Autism and Childhood Schizophrenia 3(2): 93–95.
Kuhn R (2004) Eugen Bleuler’s concepts of psychopathology. History of Psychiatry 15(3): 361–366.
Lichtenstein P, Carlström E, Råstam M, Gillberg C, Anckarsäter H (2010) The genetics of autism spectrum disorders and related neuropsychiatric disorders in childhood. American Journal of Psychiatry 167(11): 1357–1363.
Lockyer L, Rutter M (1969) A five- to fifteen-year follow-up study of infantile psychosis. British Journal of Psychiatry 115(525): 865–882.
Lord C, Jones RM (2012) Annual research review: re-thinking the classification of autism spectrum disorders. Journal of Child Psychology and Psychiatry and Allied Disciplines 53(5): 490–509.
Lord C, Petkova E, Hus V, Gan W, . (2012) A multisite study of the clinical diagnosis of different autism spectrum disorders. Archives of General Psychiatry 69(3): 306–313.
Macintosh KE, Dissanayake C (2004) Annotation: the similarities and differences between autistic disorder and Asperger’s disorder: a review of the empirical evidence. Journal of Child Psychology and Psychiatry and Allied Disciplines 45(3): 421–434.
Mahjouri S, Lord CE (2012) What the DSM-5 portends for research, diagnosis, and treatment of autism spectrum disorders. Current Psychiatry Reports 14: 739–747.
Mayes SD, Calhoun SL, Crites DL (2001) Does DSM-IV Asperger’s disorder exist? Journal of Abnormal Child Psychology 29(3): 263–271.
Mosconi MW, Kay M, D’Cruz AM, Guter S, . (2010) Neurobehavioral abnormalities in first-degree relatives of individuals with autism. Archives of General Psychiatry 67(8): 830–840.
Nadesan MH (2005) Constructing Autism: Unravelling the ‘Truth’ and Understanding the Social. New York: Routledge.
Ozonoff S (2012) DSM-5 and autism spectrum disorders: two decades of perspectives from the JCPP. Journal of Child Psychology and Psychiatry and Allied Disciplines 53(9): 4–6.
Rank B (1949) Adaptation of the psychoanalytic technique for the treatment of young children with atypical development. American Journal of Orthopsychiatry 19(1): 130–139.
Ricks DM, Wing L (1975) Language, communication, and the use of symbols in normal and autistic children. Journal of Autism and Childhood Schizophrenia 5(3): 191–221.
Rimland B (1964) Infantile Autism: The Syndrome and its Implications for a Neural Theory of Behavior. New York: Appleton-Century-Crofts.
Robinson JF, Vitale LJ (1954) Children with circumscribed interest patterns. American Journal of Orthopsychiatry 24(4): 755–766.
Rose N (1998) Life, reason and history: reading Georges Canguilhem today. Economy and Society 27(2–3): 154–170.
Rutter M (1968) Concepts of autism: a review of research. Journal of Child Psychology and Psychiatry and Allied Disciplines 9(1): 1–25.
Rutter M, Bartak L (1971) Causes of infantile autism: some considerations from recent research. Journal of Autism and Childhood Schizophrenia 1(1): 20–32.
Rutter M, Schopler E (1992) Classification of pervasive developmental disorders: some concepts and practical considerations. Journal of Autism and Developmental Disorders 22(4): 459–482.
Silverman C (2011) Understanding Autism: Parents, Doctors, and the History of a Disorder. Princeton, NJ: Princeton University Press.]
Spitzer RL, Cantwell DP (1980) The DSM-III classification of the psychiatric disorders of infancy, childhood, and adolescence. Journal of the American Academy of Child Psychiatry 19(3): 356–370.
Sponheim E (1996) Changing criteria of autistic disorders: a comparison of the ICD-10 research criteria and DSM-IV with DSM-III-R, CARS, and ABC. Journal of Autism and Developmental Disorders 26(5): 513–525.
Szatmari P (1992) The validity of autistic spectrum disorders: a literature review. Journal of Autism and Developmental Disorders 22(4): 583–600.
Szatmari P, Archer L, Fisman S, Streiner DL, Wilson F (1995) Asperger’s syndrome and autism: differences in behavior, cognition, and adaptive functioning. Journal of the American Academy of Child and Adolescent Psychiatry 34(12): 1662–1671.
Szurek SA (1956) Psychotic episodes and psychotic maldevelopment. American Journal of Orthopsychiatry 26(3): 519–543.
Timimi S, McCabe B, Gardner N (2011) The Myth of Autism. Basingstoke: Palgrave Macmillan.
van Krevelen DA (1971) Early infantile autism and autistic psychopathy. Journal of Autism and Childhood Schizophrenia 1(1): 82–86.
Verhoeff B (2012) What is this thing called autism? A critical analysis of the tenacious search for autism’s essence. BioSocieties 7(4): 410–432.
Volkmar FR (1998) Categorical approaches to the diagnosis of autism: an overview of DSM-IV and ICD-10. Autism 2: 45–60.
Waterhouse L, Wing L, Spitzer R, Siegel B (1992) Pervasive developmental disorders: from DSM-III to DSM-III-R. Journal of Autism and Developmental Disorders 22(4): 525–549.
WHO (1993) The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. Geneva: World Health Organization.
Wing L (1981a) Asperger’s syndrome: a clinical account. Psychological Medicine 11(1): 115–129.
Wing L (1981b) Language, social, and cognitive impairments in autism and severe mental retardation. Journal of Autism and Developmental Disorders 11(1): 31–44.
Wing L (1997) The history of ideas on autism: legends, myths and reality. Autism 1(1): 13–23.
Wing L (2005) Reflections on opening Pandora’s box. Journal of Autism and Developmental Disorders 35(2): 197–203.
Wing L, Gould J (1979) Severe impairments of social interaction and associated abnormalities in children: epidemiology and classification. Journal of Autism and Developmental Disorders 9(1): 11–29.
Wing L, Potter D (2002) The epidemiology of autistic spectrum disorders: is the prevalence rising? Mental Retardation and Developmental Disabilities Research Reviews 8(3): 151–161.
Wing L, Wing JK (1971) Multiple impairments in early childhood autism. Journal of Autism and Childhood Schizophrenia 1(3): 256–266.
Witwer AN, Lecavalier L (2008) Examining the validity of autism spectrum disorder subtypes. Journal of Autism and Developmental Disorders 38(9): 1611–1624.
1 note
·
View note
Text
There’s such a thing as “autism camouflaging” and it might explain why some people are diagnosed so late
While autism is usually diagnosed in childhood, some people remain “off the radar” for a long time and only receive a diagnosis much later. One possible reason is that they have learned socially appropriate behaviours, effectively camouflaging their social difficulties, including maintaining eye contact during conversations, memorising jokes or imitating facial expressions. This pattern of behaviour could have serious consequences for the lives of some people with autism. It is easy to imagine that camouflaging demands significant cognitive effort, leading to mental exhaustion over time, and in extreme cases perhaps also contributing to anxiety and depression. If there are gender differences in camouflaging, this could also help explain the well-known male preponderance in autism spectrum disorders. At least part of the gender imbalance may, in fact, stem from an under-diagnosis of autism in girls because they are better at “masking” symptoms. Before now, autism camouflaging has not been studied in a systematic and standardised manner: a recent open-access study in the journal Autism, by Meng-Chuan Lai and his colleagues, is the first to offer an operationalisation of camouflaging, which they define as the discrepancy between internal and external states in social-interpersonal contexts. For instance, if an autistic person maintains eye contact during a conversation because they have learnt that this is socially appropriate, even though this clashes with how they really want to behave, this would be an example of camouflaging. Lai and his colleagues used clinical instruments that are well established in autism research to measure the contrast between internal and external signs of autism among 30 women and 30 men with an established diagnosis of autism. Both gender groups were matched on age (average age: males 27.2 years and females 27.8 years) and intelligence and were free from intellectual disability. The researchers used the Autism Diagnostic Observation Schedule (ADOS), which includes several tasks requiring social interaction with an experimenter, to measure overt behaviour (external state). And they used the Autism Spectrum Quotient (ASQ; a questionnaire assessing autistic traits) and the “Reading the Mind in the Eyes” test (a computerised task that measures social cognitive ability, e.g. inferring how people feel based on their facial expression) to provide information about internal states. Relatively low scores on the ADOS (i.e. few signs of autism), combined with poor performance on the ASQ and the Reading the Mind in The Eyes, was taken as a sign of camouflaging. Because camouflaging likely comes at considerable cognitive and emotional costs, the researchers also studied their participants’ levels of anxiety and depression, as well as their executive function. Finally, they also used magnetic resonance imaging to scan the structure of their participants’ brains. As the researchers expected, women with autism had significantly higher camouflaging scores than their male counterparts, although there was considerable variability in both groups. Across the whole sample, higher camouflaging scores were associated with higher levels of depression, but not anxiety. When looking at gender differences, the association between camouflaging and depression remained significant only in the men (so it could be speculated that men are more susceptible to the negative consequences of camouflaging). Conversely, verbal intelligence was not associated with camouflaging in either the whole sample or genders separately. Interestingly, camouflaging correlated with executive function in females, but not males. This indicated that women who camouflaged more tended to have better executive function. The extent to which individuals with autism engaged in camouflaging was not related to their age. This indicates that camouflaging may not necessarily increase with greater learning experience, as might be expected with older age. Neuroanatomical findings differed between sexes, with links between brain structure and camouflaging generally more pronounced in the women. For instance, higher camouflaging was associated with smaller volume in temporal, cerebellar and occipital brain regions in women, but not in men. While there is no easy explanation for this sex difference, it could be speculated that the involved brain areas have a different function in camouflaging for women compared with men. These brain regions are associated with emotional processing, so perhaps they are involved in an emotional component of camouflaging that is more relevant to women. However, this needs to be rigorously examined in future studies. This study is the first to offer systematic, methodologically sound evidence in support of higher camouflaging in women than men with autism. As such, these results support reports from parents or clinicians that hint at better social skills in girls with autism as compared with boys. However, as the study found evidence of men who engaged in camouflaging and women who did not, camouflaging is unlikely to constitute a uniquely female presentation of autism. There are several points that limit the scope of this study. First, the sample size was modest and only included individuals with an established diagnosis of autism who were free from intellectual disability. To study the “real world” implications of camouflaging, it would have been interesting to study people with sub-threshold autistic scores because camouflaging might be one of the reasons why they have remained below diagnostic threshold in the first place. This information might also be relevant for healthcare professionals in terms of both diagnosis and treatment. Finally, the operationalization of camouflaging may be vulnerable to subjective bias: For example, ADOS raters may be guided by implicit gender stereotypes, leading them to give inappropriately high autism scores to girls who behave in more “boyish” ways. To conclude, this study provides the first systematic definition of camouflaging in individuals with autism and shows that this behaviour is more common in women than men. These clear-cut gender differences highlight the need to consider camouflaging in clinical contexts in the future. By Helge Hasselmann
0 notes
Text
Robert B. Dudas, et al., The overlap between autistic spectrum conditions and borderline personality disorder, 12 PLoS ONE e0184447 (2017)
Abstract
Background
Both people with autism spectrum conditions (ASC) and borderline personality disorder (BPD) are significantly challenged in terms of understanding and responding to emotions and in interpersonal functioning.
Aims
To compare ASC, BPD, and comorbid patients in terms of autistic traits, empathy, and systemizing.
Methods
624 ASC, 23 BPD, and 16 comorbid (ASC+BPD) patients, and 2,081 neurotypical controls (NC) filled in the Autism Spectrum Quotient (AQ), the Empathy Quotient (EQ) and the Systemizing Quotient-Revised (SQ-R).
Results
On the AQ, the ASC group scored higher than the BPD group, who in turn scored higher than the comorbid group, who scored higher than controls. On the EQ, we found the comorbid and ASC groups scored lower than the BPD group, who were not different from controls. Finally, on the SQ-R, we found the ASC and BPD group both scored higher than controls.
Conclusions
Similar to ASC, BPD patients have elevated autistic traits and a strong drive to systemize, suggesting an overlap between BPD and ASC.
Introduction
Autism Spectrum Conditions (ASC) are diagnosed by the presence of social and communication difficulties, alongside unusually strong, narrow interests and/or unusually repetitive and stereotyped behaviour (DSM-5, [1]. We prefer the term ASC rather than ASD (Autism Spectrum Disorder) because it is less stigmatising. Also, ASC is more consistent with the fact that these individuals have not only disabilities requiring a medical diagnosis, but also areas of cognitive strength. Autistic traits are continuously distributed in the general population, and the threshold for diagnosis is determined by clinical judgement. The prevalence of ASC is estimated at 1% and is more often diagnosed in males [2].
Borderline Personality Disorder (BPD) has a lifetime prevalence of 5.9% and is more often diagnosed in females [3] and, according to DSM-5 [1], is characterised by impairment in interpersonal functioning (including poor empathy, and problems with trust and intimacy) [4] and difficult personality traits, such as disinhibition and antagonism, and impulsivity [5–8].
The exact aetiology, including the contribution of genetic and environmental factors, of ASC or BPD is not known, and even less is known about the psychopathological relationship between ASC and BPD. The symptomatic overlap of ASC and BPD has been noted for some time [9,10] and at the cognitive level, ASC includes difficulties in reading others’ emotions [11,12] and core cognitive features of BPD also include altered social cognition [13,14].
To our knowledge, only one study has compared BPD and ASD on personality traits [15], which used the NEO-Personality Inventory-Revised (NEO-PI-R) and found more neuroticism, extraversion, and openness for experience but less conscientiousness and the same level of agreeableness in BPD vs. ASC. They also found, using the Dimensional Assessment of Personality Pathology Questionnaire (DAPPBQ), more emotional dysregulation and dissocial behaviour and less inhibition and compulsivity in BPD vs. ASC. Looking at the items of these subscales, there was no difference between the two groups in terms of intimacy, social avoidance, restricted expressiveness and callousness. The symptomatic overlap of ASC and personality disorders can lead to differential diagnostic uncertainty, particularly in women [16–19]. Looking at patients with Asperger Syndrome, Hofvander et al. found that 42 out of 62 (68%) met DSM-IV criteria for at least one personality disorder and, similarly, Lugnegard et al. found 26 out of 54 (48%) did. Conversely, Ryden [20] looked for ASC in BPD patients and found that 6 out of 41 BPD patients fulfilled criteria for ASC.
Correct clinical diagnosis is important, as the existing relatively small amount of evidence, especially as regards adult autism, suggests that different intervention approaches might be effective in the two conditions. For example, self-harm in ASC has been found to be strongly associated with sensory overload [21], while in BPD it tends to occur in the context of interpersonal conflict and emotional dysregulation. Thus, in ASC it may seem reasonable to manage it by reducing activities causing sensory overload, while in BPD there is evidence for the efficacy of psychological interventions that reduce emotional dysregulation or prompt ‘mentalizing’ [22,23]. In addition, patients can be diagnosed with both ASC and BPD, and there is some indication that this comorbid population may be at increased risk of suicide [20], which further highlights the importance of appropriate diagnosis.
In the present study we aimed to investigate 3 areas of psychological functioning in order to identify symptomatic signatures in these patient groups: autistic traits, empathizing, and systemizing. The first two of these are well established. The construct of systemizing is defined as the drive to analyse or build a system, which itself is defined as any rule-based pattern of information [24]. For each of these traits, a reliable, validated self-report questionnaire exists. The identification of profiles might prove useful in a clinical setting, as they can be measured in an inexpensive, quick and relatively easy way. In BPD, very little is known about autistic traits and although several studies have investigated different aspects of emotional intelligence [4,14] and have looked at cognition, none have specifically investigated systemizing.
To measure the extent of autistic traits in any individual, we used the Autism Spectrum Quotient (AQ; [25]), an easy to administer instrument with good discriminative validity and screening properties [26]. The AQ has been used by many studies and norms are available for clinical and non-clinical groups from a systematic review of 78 studies, detailing 6,934 nonclinical participants as well as 1,963 matched clinical cases of ASC [27]. As a short and simple self-report questionnaire, it enabled us to achieve a high number of online responses.
In 2009, Baron-Cohen proposed the Empathising-Systemizing (E-S) theory of autism [28], based on the observation that people with ASC had below average empathy with average or above average systemizing. These can be measured using the Empathy Quotient (EQ; [11]) and the Systemizing Quotient (SQ; [24]. In the latter study of 47 adults with Asperger syndrome (AS) or high functioning autism (HFA) compared with 47 matched adults from the general population, adults with AS/HFA scored significantly higher on the SQ than matched controls, and significantly lower on the EQ than matched controls. This pattern of results was replicated in a much larger study [29].
In a comprehensive review [13] of the ‘borderline empathy paradox’, initially described by Krohn [30], both enhanced and impaired levels of empathy in BPD patients have been described. This paradox may reflect variations in the method used to measure empathy or state-based/situational factors (if the individual is stressed, their empathy is reduced). In addition, in BPD, reduced interpersonal trust may lead the individual to be hyper-vigilant about other’s facial expressions or tone of voice, leading to enhanced emotion recognition skills even if talking about other’s mental states (“why are you angry with me?”, or “are you fed up with me?”), which may be socially inappropriate. There is more consistent evidence supporting the borderline empathy paradox from more socially interactive experimental methods of assessment [31–33], as opposed to tests using more passive stimuli, such as the ‘Reading the Mind in the Eyes’ Test (RMET) [34–37]. This may reflect a greater sensitivity of interactive stimuli to test empathic enhancement in BPD patients, however further research in this area is required to better understand this.
Two studies have used self-report questionnaires to investigate empathy in BPD—both used the Interpersonal Reactivity Index (IRI) [38,39] and found a decrease in cognitive empathy. However, while Guttman & Laporte found increased affective empathy, Harari et al found there was no statistically significant difference compared to nonclinical controls. To our knowledge, the present study is the first to investigate systemizing in BPD. Also, as far as we are aware, no studies have investigated autistic traits, emotional intelligence or systemizing ability in patients who are comorbid with both ASC and BPD.
Recent research is focusing on the possible under-diagnosis or mis-diagnosis of ASC in females [40,41], on the assumption that females may experience greater societal pressure to conform and be part of a peer group and so are more motivated to learn how to hide their autism (so-called “camouflaging”) and thereby go “under the radar” of clinicians or school psychologists, by “pretending to be normal” [42]. This may lead to them either receiving their ASC diagnosis far later than males, and/or being diagnosed with other conditions (anorexia, depression, anxiety, or BPD) because clinicians are not looking for how ASC may present itself differently in females [43].
The current study can thus test if BPD and ASC share a common underlying cognitive phenotype (higher AQ, and SQ>EQ) irrespective of the clinical label they are given.
Methods
Participants
Participants were recruited from the Cambridge Autism Research Database (CARD), based at the Autism Research Centre, University of Cambridge. Participants with formal clinical diagnosis of ASC, according to DSM-IV or 5 or ICD-10 criteria, register online at www.autismresearchcentre.com and provide details of when and where they received their ASC diagnosis. Participants from the general population, without a formal diagnosis of ASC, register at a separate website (www.cambridgepsychology.com). All participants are asked to provide demographic details (age, education background, any clinical diagnoses), and complete a variety of self-report measures including the AQ, EQ and SQ-R.
The Full Sample. Data from a total of 2,744 online responders were analysed. 624 responders indicated that they had been diagnosed with an ASC, 23 with BPD, and 16 with both (ASC+BPD). 2,081 responders reported no diagnosis (NC). There were thus 4 groups in the study: BPD, ASC, BPD+ASC, and Controls.
The Random Sample. In order to circumvent the problem of unbalanced group sizes (and the assumption of homogeneity of variance being violated), we also tested our hypotheses in a smaller sample (N = 89). 25 ASC and 25 NC responders were randomly selected from our full sample.
Ethical approval for the research database was obtained from the Psychology Research Ethics Committee (PREC), University of Cambridge, UK. Consent was obtained online when participants registered to join the research database, where they have the opportunity to read the Terms and Conditions. This describes how the research data they provide (questionnaire and performance data) will be used in a variety of future research studies in an anonymised form, and that their personal information is only seen by named database managers who take legal responsibility for data protection.
Instruments
The AQ.
The Adult Autism-Spectrum Quotient (AQ) is a 50-item, self-report questionnaire for use with adults with normal intelligence to assess for the presence of traits associated with the autistic spectrum [25]. The questions assess 5 different areas, each consisting of 10 items on each: social skills, attention switching, attention to detail, communication, and imagination. Each AQ item is a brief statement followed by 4 possible ratings: “definitely agree,” “slightly agree,” “slightly disagree,” or “definitely disagree.” Each item is scored 1 point if the responder endorses the behaviour either mildly or strongly, resulting in a maximum possible score of 50. Higher AQ scores indicate a higher degree of autistic features, and a threshold of >26 is a good predictor of diagnosis [26].
The EQ.
The Empathy Quotient (EQ) is a 60-item, self-report questionnaire for use with adults with normal intelligence for the quantitative measurement of empathy [11]. It consists of 40 empathy items and 20 filler/control items. On each of the empathy items a person may score 2, 1 or 0, which correlates with the responder reporting the behaviour strongly, mildly or not at all. Therefore the maximum score is 80 and the minimum is zero. 80% of people with ASC score <30.
The SQ-R.
The Systemizing Quotient-Revised (SQ-R) is a 75-item, self-report questionnaire for use with adults with normal intelligence for the quantitative measurement of systemizing ability [44]. On 39 items, ‘strongly agree’ responses score two points and ‘slightly agree’ responses score one point, and on 36 items, ‘strongly disagree’ responses score two points and ‘slightly disagree’ responses score one point. The maximum score is 150 and the minimum is zero.
Brain types.
The D score or ‘Brain Type’ is a measure of the standardized difference between an individual’s empathizing and systemizing scores. The raw SQ-R and EQ scores are standardized by subtracting the typical population mean (denoted by <…>) from the participant’s score and then dividing this by the maximum possible score (S = (SQ-R–<SQ-R>)/150 and E = (EQ–<EQ>)/80). The control group means are used as estimations of the typical population means in this standardization procedure: EQ (mean = 45.38, SD = 14.98) and SQ-R (mean = 58.55, SD = 22.34). The difference (D) between the standardized EQ and SQ-R scores is then calculated by: D = (S–E)/2. Using the D score, individuals can be classed into one of five cognitive profiles, or ‘brain types’. ‘Brain types’ based on D score are defined quantitatively, based on a previous study [45] that classed the lowest and highest 2.5th percentiles of scores in a large, population-based, typically developing group as ‘Extreme Type E’ (E>>S) and ‘Extreme Type S’ (S>>E), respectively. Those scoring between the 2.5th and 35th percentiles are classed as ‘Type E’ (E>S), those between the 35th and 65th percentiles as ‘Type B’ (balanced, E≈S), and those between the 65th and 97.5th percentile as ‘Type S’ (S>E).
Statistical analysis
We used a one-way analysis of variance (ANOVA) to compare means scores on dependent variables (AQ, EQ and SQ), between the four groups (Control, ASC, BPD, ASC+BPD), and post-hoc Games-Howell tests used to follow up significant main effects. We checked our findings with appropriate non-parametric tests (Kruskal-Wallis and Mann Whitney U tests) where our variables did not follow a normal distribution and their distribution could not be normalized by square root or logarithmic transformation. Cohen’s d was calculated as a measure of effect size for post-hoc comparisons, with > = 0.2 indicating a small, > = 0.5 a medium and > = 0.8 a large effect.
Results
Analysis of the full sample
The mean age of the sample was 39.43 years (SD = 12.3), and the 4 groups did not differ from each other on age (ANOVA F3, 2740 = -.395; p = 0.757, n.s.). The BPD group, and to a lesser extent the NC group, showed a female preponderance, whilst the ASC groups were well-balanced. Responders predominantly attended mainstream schools (S1 Table).
The AQ scores.
The AQ scores followed a normal distribution in the groups (S2 Table). Each group was significantly different from one another in terms of this measure (ANOVA F3, 2727 = 445.65; p < 0.001), resulting in the following pattern: NC < BPD < ASC < ASC+BPD (Fig 1A). Post hoc comparison with the Games-Howell test between the NC and BPD groups yielded a significant p value of 0.014 (Cohen’s d = 1.08), however, the difference between the BPD and the ASC group was only marginally significant (p = 0.047; Cohen’s d = 0.51). Patients with both conditions, the ASC+BPD group, scored highly significantly higher than those with ASC (p = 0.001; Cohen’s d = 0.71). The AQ scores of the two ASC patient groups very clearly separated them from the responders with no diagnosis (p < 0.001; Cohen’s d = 1.62 and 2.75, respectively for ASC and ASC+BPD).
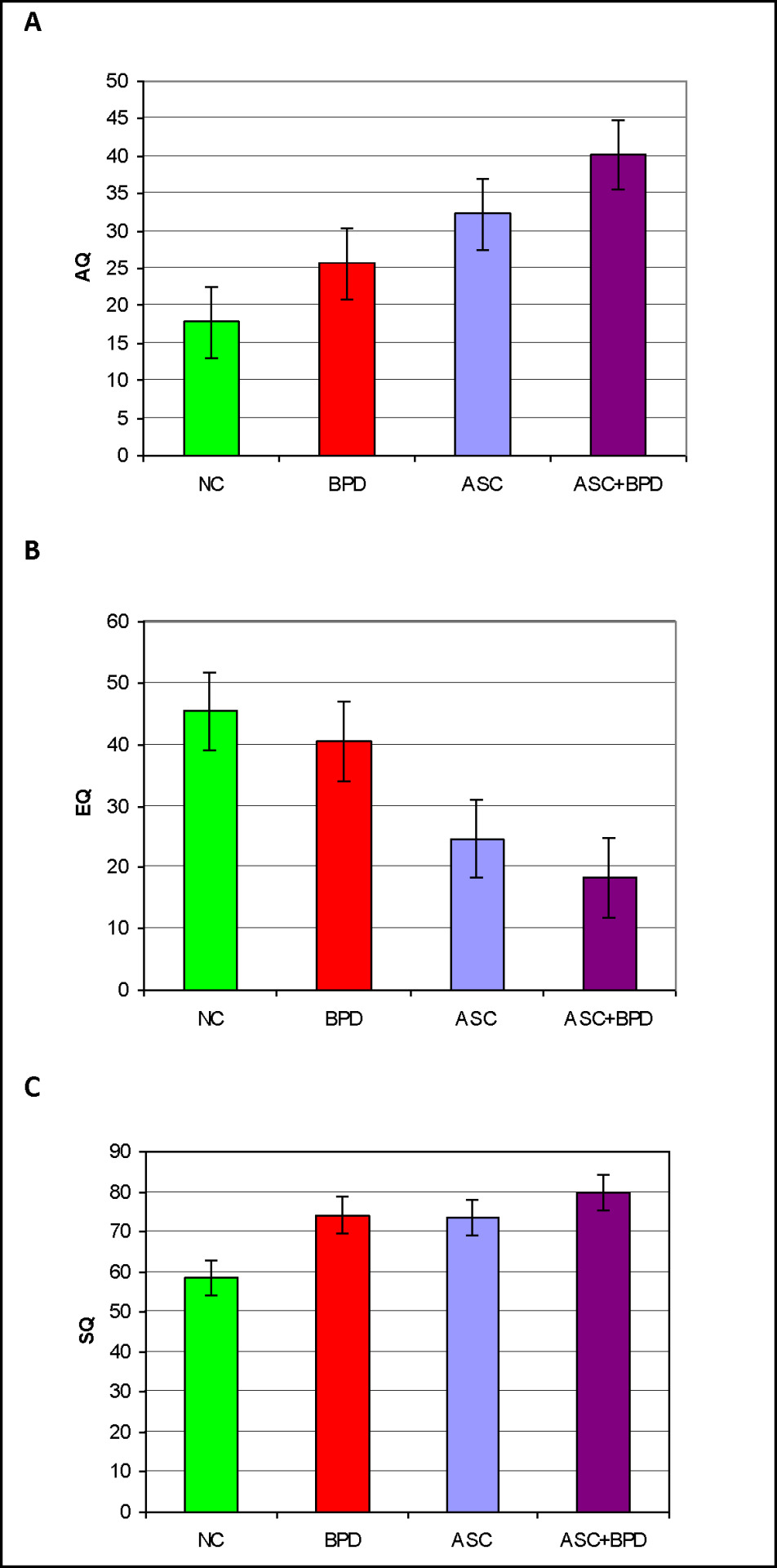
Fig 1. A Mean scores (and error bars) of the 4 diagnostic groups on the AQ in the full sample. B Mean scores (and error bars) of the 4 diagnostic groups on the EQ in the Full Sample. C Mean scores (and error bars) of the 4 diagnostic groups on the SQ-R in the Full Sample.
The EQ scores.
The EQ scores of the ASC+BPD group were positively skewed (skewness = 1.87, SE = 0.56; kurtosis = 3.07, SE = 1.09), and square root or logarithmic transformation only made the distributions less normal. A one-way ANOVA revealed highly significant between group differences (ANOVA F3, 2424 = 265.66; p < 0.001), with the BPD and NC not being different from each other but both scoring higher than the ASC and ASC+BPD groups (each p value < 0.001; Cohen’s d values: ASC vs NC = -1.37, ASC+BPD vs NC = -1.81, ASC vs BPD = -1.01, ASC+BPD vs BPD = -1.42), which were again not different from each other (Cohen’s d = -0.40; Fig 1B), resulting in the following pattern: NC = BPD > ASC = ASC+BPD. We checked our findings with the Kruskal-Wallis test, which was highly significant (p < 0.001). Mann Whitney U tests confirmed that the BPD and NC groups (p = .282) and the ASC and ASC+BPD groups (p = 0.05) respectively were not different from each other, but the NC and BPD groups scored significantly higher than the ASC group (p < 0.001 in both cases).
The SQ-R scores.
The SQ-R scores were again relatively normally distributed and produced another pattern (ANOVA F3, 2326 = 62.51; p < 0.001), with both the BPD (Games-Howell: p = 0.016, Cohen’s d = 0.7) and the ASC (G-H: p < 0.001, Cohen’s d = 0.65) groups scoring significantly higher than the NC group: NC < BPD = ASC. The ASC+BPD group was not statistically different from any other group in our post hoc comparisons despite its mean being higher than that of any other group. However, Cohen’s d values indicated a large effect when looking at ASC+BPD compared to NC (d = 0.95), and a small effect when comparing the ASC+BPD group with the BPD (d = 0.22) or ASC (d = 0.24) groups, as suggested by a bar chart of the data (Fig 1C).
“Brain types”.
An analysis of brain types revealed the expected pattern of distribution in the NC group (Fig 2). Approximately 80% of the ASC group had an “S” or “extreme S” type brain. Interestingly, over 50% of the BPD group also had “S” or “extreme S” type brains, largely due to a larger proportion of Extreme S brains relative to controls. By far the largest proportion (around 50%) of “extreme S” type brains was found in the ASC+BPD group.

Fig 2. Proportion of brain types within the diagnostic groups.
Analysis of the random sample
The groups were well-matched on age (ANOVA F3, 85 = 0.64; p = 0.592, n.s.). Generally, there was a female preponderance in the sample, with this being, again, particularly salient in the BPD and NC groups. Most responders attended mainstream school, but responders in the patient groups also reported having received education in special schools, their own homes, or via other arrangements (S3 Table).
The AQ scores.
The AQ scores were normally distributed in the sample (Fig 3A, S4 Table). A one-way ANOVA demonstrated significant between-group differences (ANOVA F3, 85 = 18.52; p < 0.001) with the patient groups scoring significantly higher than NC group (BPD vs. NC: p = 0.011, Cohen’s d = 1.1) the ASC and ASC+BPD groups vs. NC: both p < 0.001, Cohen’s d = 1.51 and 2.68, respectively). In this random sample, the mean score of the BPD group was not statistically different from that of the ASC group (Cohen’s d = 0.41). The ASC+BPD group scored higher than the NC and BPD groups, but its slightly higher mean score was not statistically different from that of the ASC group (p = 0.084, Cohen’s d = 0.63). These results were a partial replication of the pattern seen in the Full Sample: NC < BPD, BPD < ASC+BPD, (BPD = ASC).
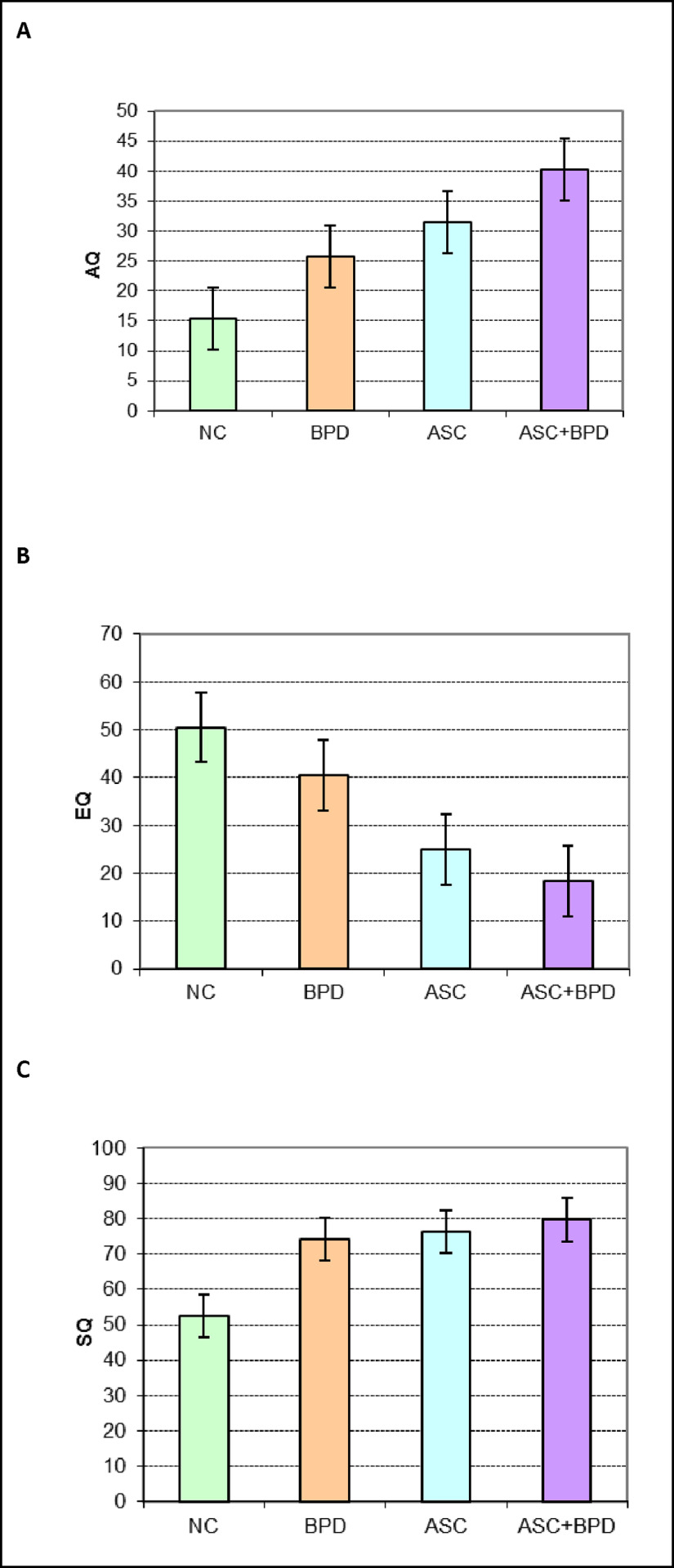
Fig 3. A Mean scores (and error bars) of the 4 diagnostic groups on the AQ in the random sample. B Mean scores (and error bars) of the 4 diagnostic groups on the EQ in the Random Sample. C Mean scores (and error bars) of the 4 diagnostic groups on the SQ-R in the Random Sample.
The EQ scores.
The EQ scores were non-normally distributed and were analysed following square root transformation. A one-way ANOVA revealed significant between-group differences (F3, 74 = 15.75; p < 0.001), with the BPD and NC not being different from each other (NB. Cohen’s d = -0.61) but both scoring higher than the ASC and ASC+BPD groups (each p value < 0.001, Cohen’s d: BPD vs ASC = -0.84, BPD vs ASC+BPD = -1.42, ASC vs NC = -1.5, ASC+BPD vs NC = -1.95), which were again not different from each other (Cohen’s d = -0.37, Fig 3B). This was the same pattern as observed in the Full Sample: NC = BPD >> ASC = ASC+BPD.
The SQ-R scores.
The SQ-R scores were non-normally distributed and therefore analysed after square root transformation. A one-way ANOVA indicated significant between-group differences (F3, 74 = 4.48; p = 0.006) with the patient groups all scoring significantly higher than the NC group (BPD vs. NC: p = 0.032, Cohen’s d = 0.76; ASC vs. NC: p = 0.025, Cohen’s d = 0.83; ASC+BPD vs NC: p = 0.022, Cohen’s d = 0.95). This pattern (NC < BPD = ASC = ASC+BPD) was similar to that found in the Full Sample (Fig 3C).
We summarized our findings in Table 1.

Table 1. Autistic traits, empathizing ability and systemizing ability in ASC, BPD, and comorbid patients relative to controls.
Discussion
To our knowledge, this is the first study to investigate autistic traits, empathizing and systemizing abilities in ASC, BPD, comorbid ASC+BPD, and controls. The mean AQ scores found in our ASC and control groups were comparable to those reported by a recent systematic review for nonclinical populations (16.94, 95% CI 11.6, 20.0) and for ASC (35.19, 95% CI 27.6, 41.1) [27]. Our finding of the comorbid ASC+BPD group scoring higher than the ASC group was consistent with a previous study reporting higher AQ scores in people with Asperger Syndrome who also met criteria for a personality disorder [17]. We are only aware of one previous study that reported results with the AQ in people with BPD [46]. Out of 38 women with BPD, almost half of them scored above the cut-off of the AQ. The difference on the AQ between the BPD and the ASC group was not statistically significant in our random sample, suggesting that people with BPD may have as high levels of autistic traits as people with ASC. This finding would need to be replicated in a larger sample but is in line with the idea that some females with BPD have undiagnosed ASC, due to ASC not being easily detected in females.
As expected, people with an ASC scored lower than controls on empathizing. The finding of no difference between people with BPD and controls on empathizing ability is consistent with one [39] but not another previous study [38] that used a self-report questionnaire to examine empathy.
As expected, participants reporting an ASC diagnosis on average reported higher levels of systemizing than those without such a diagnosis. A trade-off between empathizing and systemizing has been proposed, with ASC patients showing below average empathizing but intact or superior systemizing [44]. Our “brain type” analysis suggested a shift in those with BPD (either alone or comorbid with ASC) toward having a more systemizing type brain. As far as we are aware, no previous study has investigated systemizing in BPD. Our findings suggest that people with BPD also report elevated systemizing relative to controls, without a statistically significant difference between them and the ASC groups. It is possible that increased systemizing might be a compensatory mechanism for their emotional instability but, alternatively, elevated systemizing may be part of the phenomenology of BPD, just as it is in ASC. Our findings highlight the need for careful examination for autistic traits in patients referred for an assessment for BPD, especially in those without a history of significant childhood abuse or neglect. Some of these patients may have been misdiagnosed (their ASC was overlooked), and a proportion of them may have both conditions.
This study has two key limitations: the small size of the BPD and ASC+BPD groups, and that diagnosis was based on self-report. Self-report is common in large, online samples and is unlikely to be responsible for the differences found, as the group means in the ASC and NC groups were very similar to those derived from samples with a clinically verified diagnosis. The current findings need to be replicated, ideally using experimental paradigms that are more able to control for current mood state and less susceptible to bias in memory [47] and lack of insight. Finally, future research may investigate patterns with these instruments in other personality disorders, such as schizoid, schizotypal, and antisocial personality disorder.
References
1.APA (2013) Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C.: American Psychiatric Association.
2.Baron-Cohen S, Scott FJ, Allison C, Williams J, Bolton P, et al. (2009) Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry 194: 500–509. pmid:19478287
3.Grant BF, Chou SP, Goldstein RB, Huang B, Stinson FS, et al. (2008) Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry 69: 533–545. pmid:18426259
4.Lazarus SA, Cheavens JS, Festa F, Zachary Rosenthal M (2014) Interpersonal functioning in borderline personality disorder: a systematic review of behavioral and laboratory-based assessments. Clin Psychol Rev 34: 193–205. pmid:24534643
5.Dougherty DM, Bjork JM, Huckabee HC, Moeller FG, Swann AC (1999) Laboratory measures of aggression and impulsivity in women with borderline personality disorder. Psychiatry Res 85: 315–326. pmid:10333383
6.Dowson J, Bazanis E, Rogers R, Prevost A, Taylor P, et al. (2004) Impulsivity in patients with borderline personality disorder. Compr Psychiatry 45: 29–36. pmid:14671734
7.Rentrop M, Backenstrass M, Jaentsch B, Kaiser S, Roth A, et al. (2008) Response inhibition in borderline personality disorder: performance in a Go/Nogo task. Psychopathology 41: 50–57. pmid:17975328
8.Lawrence KA, Allen JS, Chanen AM (2010) Impulsivity in borderline personality disorder: reward-based decision-making and its relationship to emotional distress. J Pers Disord 24: 786–799. pmid:21158600
9.Pelletier G (1998) Borderline personality disorder vs. Asperger's disorder. J Am Acad Child Adolesc Psychiatry. United states. pp. 1128.
10.Fitzgerald M (2005) Borderline personality disorder and Asperger syndrome. Autism 9: 452. pmid:16320474
11.Baron-Cohen S, Wheelwright S (2004) The empathy quotient: an investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. J Autism Dev Disord 34: 163–175. pmid:15162935
12.Cassidy S, Ropar D, Mitchell P, Chapman P (2014) Can adults with autism spectrum disorders infer what happened to someone from their emotional response? Autism Res 7: 112–123. pmid:24307231
13.Dinsdale N, Crespi BJ (2013) The borderline empathy paradox: evidence and conceptual models for empathic enhancements in borderline personality disorder. J Pers Disord 27: 172–195. pmid:23514182
14.Jeung H, Herpertz SC (2014) Impairments of interpersonal functioning: empathy and intimacy in borderline personality disorder. Psychopathology 47: 220–234. pmid:24577235
15.Strunz S, Westphal L, Ritter K, Heuser I, Dziobek I, et al. (2015) Personality Pathology of Adults With Autism Spectrum Disorder Without Accompanying Intellectual Impairment in Comparison to Adults With Personality Disorders. J Autism Dev Disord 45: 4026–4038. pmid:25022250
16.Hofvander B, Delorme R, Chaste P, Nydén A, Wentz E, et al. (2009) Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry. pp. 35. pmid:19515234
17.Lugnegard T, Hallerback MU, Gillberg C (2012) Personality disorders and autism spectrum disorders: what are the connections? Compr Psychiatry 53: 333–340. pmid:21821235
18.Anckarsater H, Stahlberg O, Larson T, Hakansson C, Jutblad SB, et al. (2006) The impact of ADHD and autism spectrum disorders on temperament, character, and personality development. Am J Psychiatry 163: 1239–1244. pmid:16816230
19.Lai MC, Baron-Cohen S (2015) Identifying the lost generation of adults with autism spectrum conditions. Lancet Psychiatry 2: 1013–1027. pmid:26544750
20.Rydén G, Rydén E., & Hetta J. (2008) Borderline personality disorder and autism spectrum disorder in females: A cross-sectional study. Clinical Neuropsychiatry 5: 22–30.
21.Duerden EG, Oatley HK, Mak-Fan KM, McGrath PA, Taylor MJ, et al. (2012) Risk factors associated with self-injurious behaviors in children and adolescents with autism spectrum disorders. J Autism Dev Disord 42: 2460–2470. pmid:22422338
22.Rathus JH, Miller AL (2002) Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav 32: 146–157. pmid:12079031
23.Stoffers JM, Völlm BA, Rücker G, Timmer A, Huband N, et al. (2012) Psychological therapies for people with borderline personality disorder. Cochrane Database of Systematic Reviews
24.Baron-Cohen S, Richler J, Bisarya D, Gurunathan N, Wheelwright S (2003) The systemizing quotient: an investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. Philos Trans R Soc Lond B Biol Sci 358: 361–374. pmid:12639333
25.Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E (2001) The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord 31: 5–17. pmid:11439754
26.Woodbury-Smith MR, Robinson J, Wheelwright S, Baron-Cohen S (2005) Screening adults for Asperger Syndrome using the AQ: a preliminary study of its diagnostic validity in clinical practice. J Autism Dev Disord 35: 331–335. pmid:16119474
27.Ruzich E, Allison C, Smith P, Watson P, Auyeung B, et al. (2015) Measuring autistic traits in the general population: a systematic review of the Autism-Spectrum Quotient (AQ) in a nonclinical population sample of 6,900 typical adult males and females. Mol Autism 6: 2. pmid:25874074
28.Baron-Cohen S (2009) Autism: the empathizing-systemizing (E-S) theory. Ann N Y Acad Sci 1156: 68–80. pmid:19338503
29.Baron-Cohen S, Cassidy S, Auyeung B, Allison C, Achoukhi M, et al. (2014) Attenuation of typical sex differences in 800 adults with autism vs. 3,900 controls. PLoS One 9: e102251. pmid:25029203
30.Krohn A (1974) Borderline "empathy" and differentiation of object representations: a contribution to the psychology of object relations. Int J Psychoanal Psychother 3: 142–165. pmid:4435991
31.Ladisich W, Feil WB (1988) Empathy in psychiatric patients. Br J Med Psychol 61 (Pt 2): 155–162.
32.Flury JM, Ickes W, Schweinle W (2008) The borderline empathy effect: Do high BPD individuals have greater empathic ability? Or are they just more difficult to ‘read’?. Journal of Research in Personality 42: 312–332.
33.Franzen N, Hagenhoff M, Baer N, Schmidt A, Mier D, et al. (2011) Superior 'theory of mind' in borderline personality disorder: an analysis of interaction behavior in a virtual trust game. Psychiatry Res 187: 224–233. pmid:21129781
34.Fertuck EA, Jekal A, Song I, Wyman B, Morris MC, et al. (2009) Enhanced 'Reading the Mind in the Eyes' in borderline personality disorder compared to healthy controls. Psychol Med 39: 1979–1988. pmid:19460187
35.Frick C, Lang S, Kotchoubey B, Sieswerda S, Dinu-Biringer R, et al. (2012) Hypersensitivity in borderline personality disorder during mindreading. PLoS One 7: e41650. pmid:22870240
36.Preissler S, Dziobek I, Ritter K, Heekeren HR, Roepke S (2010) Social Cognition in Borderline Personality Disorder: Evidence for Disturbed Recognition of the Emotions, Thoughts, and Intentions of others. Front Behav Neurosci 4: 182. pmid:21151817
37.Scott LN, Levy KN, Adams RB Jr., Stevenson MT (2011) Mental state decoding abilities in young adults with borderline personality disorder traits. Personal Disord 2: 98–112. pmid:22247796
38.Guttman HA, Laporte L (2000) Empathy in families of women with borderline personality disorder, anorexia nervosa, and a control group. Fam Process 39: 345–358. pmid:11008652
39.Harari H, Shamay-Tsoory SG, Ravid M, Levkovitz Y (2010) Double dissociation between cognitive and affective empathy in borderline personality disorder. Psychiatry Res 175: 277–279. pmid:20045198
40.Bargiela S, Steward R, Mandy W (2016) The Experiences of Late-diagnosed Women with Autism Spectrum Conditions: An Investigation of the Female Autism Phenotype. J Autism Dev Disord 46: 3281–3294. pmid:27457364
41.Hull L, Petrides KV, Allison C, Smith P, Baron-Cohen S, et al. (2016) “Putting on my best normal”: A qualitative study of social camouflaging in adults with Autism Spectrum Conditions. UCL.
42.Holliday Willey L (1999) Pretending to be Normal: Living with Asperger's Syndrome. London and Philadelphia: Jessica Kingsley Publishers Ltd.
43.Lai MC, Lombardo MV, Baron-Cohen S (2014) Autism. Lancet 383: 896–910. pmid:24074734
44.Wheelwright S, Baron-Cohen S, Goldenfeld N, Delaney J, Fine D, et al. (2006) Predicting Autism Spectrum Quotient (AQ) from the Systemizing Quotient-Revised (SQ-R) and Empathy Quotient (EQ). Brain Res 1079: 47–56. pmid:16473340
45.Goldenfeld N, Baron-Cohen S, Wheelwright S (2005) Empathizing and systemizing in males, females and autism. Clinical Neuropsychiatry 2: 8.
46.Nanchen K, Brodführer A, Heinrichs M, Philipsen A, Elst LTv, et al. (2016) Autistische Züge bei Patientinnen mit Borderline-Persönlichkeitsstörung unter besonderer Berücksichtigung der Empathie. Zeitschrift für Psychiatrie, Psychologie und Psychotherapie 64: 247–255.
47.Baer RA, Peters JR, Eisenlohr-Moul TA, Geiger PJ, Sauer SE (2012) Emotion-related cognitive processes in borderline personality disorder: a review of the empirical literature. Clin Psychol Rev 32: 359–369. pmid:22561966
#research#psychology#personality#development#comorbidity#autism#autism spectrum disorders#empathy#studies#dysfunction#systematizing#borderline personality disorder
0 notes
Last Seen Blogs

lelbaia
lelbaia للبيع

flydeiple2
Лечу К Суециду В Обьятия

hellonheelz93
Ars longa, vita brevis
demonic-piece-of-cake
Hi! Welcome to Chilis

godbold13
Godbold@InkCompany