#vocal cord dysfunction
Text
Shout out to people with breathing related disabilities because this shit sucks
People who need inhalers and nebulizers. People who use ox tanks. People who can’t stand or walk too much because it makes breathing harder. People who have given up important parts of their life because of their breathing issues. People who need assistance and caregivers. Especially huge shoutout to people whose breathing problems don’t have any treatments and/or are getting worse with time
In my experience, we are often left out of the disabled community, either implicitly or explicitly. Needing assistance with chores and errands is so common for disabled people yet when it’s a lung or airway issue that causes us to need that assistance, we’re left out of the convo. Conditions like cystic fibrosis, COPD, lung cancer, VCD, asthma, anaphylaxis, and more can all be seriously disabling. We deserve a voice
Anyways, big hugs for people with breathing issues that want one. We deserve more love <3
#Lincoln logs#disability#actually disabled#VCD#vocal cord dysfunction#asthma#mopping three tiles worth of flooring made my airway close up and it’s got me feeling things
3K notes
·
View notes
Text
So I'm on Zoom, with the nurse to get checked in, and they said, "I can't hear you," so I sent a message in chat, "I can't talk"
"Why?"
"VCD"
And then we go on with the usual questions in the Zoom chat box. During this, the nurse turns their screen to the side a bit and asks, while bearly moving their mouth, "What is this?"
"VCD? Vocal cord disorder" the other nurse who isn't in screen answer
The two nurses then have a vocal conversation. The one in screen bearly moving their mouth, while I'm there answers texts in chat as if I couldn't hear them.
Once again, if I can't talk, I obviously can't hear :D
Anyways- Did you know that changing your clothes is good for sensory input? If you stay in the same clothes for too long then your nervous system will think it's just not focusing on the sensory input and will focus more so it can feel the change in input- which can cause an increase in pain
#chronic illness#disabled#postural orthostatic tachycardia syndrome#ehlers danlos syndrome#chronic pain#hypermobile ehlers danlos#chronically ill#disability#pots syndrome#spoonie#vocal cord dysfunction#nonverbal
154 notes
·
View notes
Text
i have to go to speech therapy because apparently my vocal cords close up whenever i breathe wrong

60 notes
·
View notes
Note
Hey Joy! Feel free to ignore if you've got low spoons 😊
I was diagnosed with Vocal Cord Dysfunction a few years ago, and it's been annoying but not majorly concerning until recently. My major symptom is gagging, and I've been have gagging episodes nearly every day (sometimes until I vomit) which is extremely discouraging. It tends to flare up when I speak a lot, which I can manage at home but is impossible to avoid at work.
Are there any exercises or tips that you use to help manage your VCD? My PCP tends to brush off most of my issues as anxiety related, which means he gives advice and not any useful information. I'm planning on getting a new PCP, but dealing with insurance is a nightmare lol.
Thank you so much Joy, hope your migraines ease up and please give the mop a smooch for me!
Hey, I'm sorry to hear you're dealing with this, and I'm sorry your PCP is being so dismissive.
If you can, push to find a speech therapist. They can better guide you through breathing and speech exercises that can help you identify your specific triggers and the best way to prevent future attacks. They may also recommend more targeted physical therapy that works to keep the throat and neck muscles in good condition.
Something else you can try is also called a "rescue breath." I'll see if I can describe it, but basically, you purse your lips together (like you're going to blow out a candle) and exhale for as long as you can through your lips, then take two quick breaths through your nose. You do it a couple of times (or however many it takes) to return your breathing to normal. I'm probably not explaining it well, but if you do it right, you can sometimes stop an attack if you can feel one coming on or stop it from getting worse.
But yeah, absolutely find yourself a speech therapist. Also, do your best to keep your neck muscles relaxed. I use heat wraps multiple times a day and also try to roll the tension out when I notice the muscles seizing up--though the way I do that is specific to my cranial instability, so I'd be reluctant to give you the same technique in case it's the opposite of what you need 😅 I also find cervical traction devices helpful, but again mileage may vary.
Best of luck. I hope things improve for you.
175 notes
·
View notes
Text
Me every single day:

#guess who can't fucking breathe rn due to their vocal cord dysfunction#vocal cord dysfunction#deviated septum#asthma#breathing problems#I made this meme like 5 years ago but it's still relevant unfortunately
5 notes
·
View notes
Text
I finally got a diagnosis!!! Vocal cord dysfunction. It's why my voice goes hoarse at work. Why my voice changes and I can never keep one pitch. It's why I lose my voice. Why I physically can't speak with strong emotion. Or sometimes just at other times for reasons I don't know. Why I feel short of breath despite enough oxygen and inhalers do not help. It's why I wheeze amd cough so much. Fucking hell. I just wish they looked into it before it caused difficulties at work or more like I wish that wasn't the reason it was looked at. But oh well. With a lot of work it can be managed. This will be so helpful to point at so people understand why I'm not vocally speaking to then or why I can't
12 notes
·
View notes
Text
What is Vocal Cord Dysfunction and what does it look like?
#spoonie#disability#chronic disability#disabilities#vocal cord dysfunction#vcd#vocal cord#voice#speech#speech pathology
0 notes
Text
man i love my throat burning from having the audacity to take my dog out to use the bathroom for a whopping 2 minutes
#fireworks#my vocal cord dysfunction and reflux laryngitis have combined to make me suffer at the mildest inconvenience#and the only way to calm my dog down is if i sing to her#so i probably won’t be able to eat anything without paying for it#at least the wheezing and coughing stopped#can’t wear a mask either without wheezing my life is a terrible sitcom#and i’ve been assigned the role of dying grandparent
0 notes
Text
…something been in draft for while:
idk how say this exactly but often like. use what look like binary clear cut dichotomy that have set definition this is this that is that. because oftentimes call “cake” “cake” instead of “flour milk egg baking powder salt etc etc” that kind language faster simplier and nuance can easily put word count 10k+. and. with language communication disabilities not always able translate all nuance into tangible word on paper/screen/type sometimes have to call something with imperfect blanket word. and then you find out other people not really hold as much nuance as you & still simplify your nuance into something binary this this that that
but reality rarely that binary— say on here that nonverbal mean not mouth speak at all all time & semiverbal is struggle all time but can mouth speak some & verbal but actually more nuanced than that like some severely apraxic people who mouth do say thing but not in their control not what they want say & they still call self nonspeaking because it not intentional meaningful speech; or someone labeled nonverbal who actually do commmunicate with mouth words just not full sentence & not full clear pronounce but still labeled nonverbal anyway as almost like microaggression of not recognize their single or two word mouth word phrase as valid enough communication worth listen to; or someone with echolalia that not mean anything with it (vs someone with echolalia that is use echolalia as communication (think gestalts, etc)); or some research showing even able say 1-2 words more ability than those with 0 word; or research debate about where minimally verbal end is it 20 words 30 words 50 words
when combat “go nonverbal” crowd often say there is clear cut about what nonverbal and what isn’t and yeah there is clear cut but also is there
many not ready for this level muddiness & nuance because some take bring nuance as invite to say like “i nonverbal but can still (intentionally) mouth speak” or gateway to claim nonverbality as if fun new identity collect instead of some complicated complex experience with mixed emotion but often some level of grief at some point that get lot targeted awful ableism & discrimination like denied education refuse accommodation like IEP or put in segregated classroom without even consider accommodation in general ed to isolate away from peers n not actual to help nonverbal person where they best thrive, or secluded or restrained, or denied healthcare, denied communication, which all still happen now btw it still common now it not rare obsolete it majority still
which make me feel like this image

[id: meme. left side is philosophers (school of athens painting) with caption “talking about nonverbal nonspeaking with other nonverbal people”. middle say “vs”. right side image is parent guiding infant to look play at toy and captioned “talking about nonverbal nonspeaking with not nonverbal people. end id]
because sometimes really is that but also even this is binary. thinking about how some motor nonspeaking people without intellectual disability who language okay say their mind intact that they not stupid thus deserve education and not deserve abuse and throw people with ID & language impairment. or how nonverbal nonspeaking from autism so different from (but so similar to) from motor apraxia from cerebral palsy from intellectual disability from genetic or chromosomal disorders from stroke from TBI from aphasia from vocal cord dysfunction from dementia from from from… how talking to someone nonspeaking from primarily motor reasons without cognitive intellectual language disabilities as someone nonverbal because high level autism cognitive language disabilities, we not guarantee understand eachother experience, same with talk someone from acquired things vs mine neurodevelopmental, how what i say about nonverbal here may not apply to someone who not speak not because autism etc
but “if words so meaningless if experiences so boundless let abolish all” not helpful because for all kind way be nonverbal there experiences that 100% not nonverbal there experiences so different from nonverbal “not able meaningfully intentionally speak all the time” for every meaningless there meaningful reason nonverbal people use nonverbal and deserve word “nonverbal” for ourselves and how this difference in experience is intracommunity issue issue within nonverbal nonspeaking community something we have to grapple with and not invitation for people outside to talk about how “if nonverbal so wide, drawing line at going nonverbal & say that isn’t nonverbal is ridiculous and gatekeep” because as much vast different experience there is reason why there community why there this word we all call ourselves and. not one. of the reason is we can slide in and out of not speak and speak daily or weekly or monthly or regularly. there still common theme to what we call nonverbal despite different
wide word isn’t “functionally useless” it just you not know how n when use it
& this conversation not just apply to nonverbal but many other words n other things as well
130 notes
·
View notes
Text
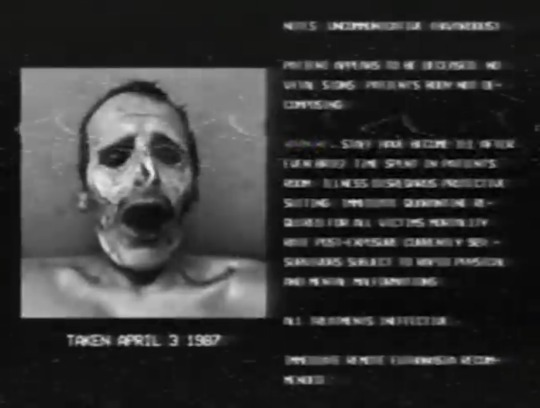
Decided to do some stuff on the Greylock Tapes. Like other mutations the survivors had that we didn’t see in the pictures shown.
Warning! Body horror galore below the cut!
Thomas Rockford

Other mutations: Just ever so slightly taller than he was before the incident. Adrenal glands are also discolored and dysfunctional, which causes the random outbursts.
Samuel Washington

Other mutations: Mutated thalamus produces psilocybin nonstop, which causes the constant delusions and paranoia. One side of the jaw is also grossly elongated, and flesh around the shoulders is sloughing off.
Ramón Herrera
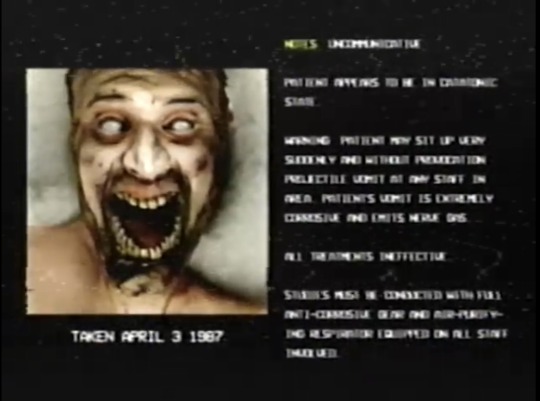
Other mutations: Aside from the broken-looking neck, several organs have fused into one large sack-like structure that produces a highly acidic compound (it’s not puke anymore) that must be expelled every now and then. This compound, as it evaporates, emits a highly potent nerve agent that is structurally similar to Novichok. Arms and legs are slightly atrophied due to lack of use.
Charles Flemming

Other mutations: Aside from the obvious, his brain is relatively untouched and he would be more talkative (though he’d mostly beg for God to save him and the other patients) if his vocal cords didn’t crap out. Even though he’s still mostly sane, his ‘attack and eat on sight’ thing is less a sight thing and more a physical proximity thing, and he seemingly blacks out shortly before going on the attack. His feet are also digitigrade, like the feet of a dog or wolf (long feet, heel always off the ground). This means he’s REALLY fast once he starts running.
Scott Oakhurst

Other mutations: Sociopathic narcissistic asshole before he mutated, and he’s even worse now that he’s a metahuman freak. That large wounded eye of his was not there before. He lost the old one five years prior to mutating. His new teeth are also self-sharpening, meaning that whenever he shuts his mouth, the teeth get sharper as they rub against each other. The bones in his fingers also burst through his skin and basically became claws. And not only is his increased bite force strong enough to crush bones like crackers, but the motherfucker chewed through a wooden door made from Australian Buloke like a beaver on steroids during the April 6th, 1987 incident.
Eduard Kowalski

Other mutations: In comparison to the others in terms of psychology, the original Eduard Kowalski is just not there anymore. Physically, those eyes of his should be functionally blind, consisting mostly of scar tissue and… something else. However, he can see in the infrared spectrum of light just fine, so he isn’t blind. Plus his arms are a lot longer than they were prior to mutation, and in comparison to the anatomy of normal people, his proportions are more similar to those of gibbons than people. And as for his newfound ability to get people to do just about anything using only his words… Those eyes of his might have something to do with it.
John Rafferty
Other mutations:
Poor little Johnny…
Poor weak, pathetic little Johnny…
Too afraid to be himself…
Too weak to be anything else…
31 notes
·
View notes
Text
chp. 4 - "sins of our fathers" (rival gang eremika au)

READ ON AO3
rating: explicit (fic ongoing)
pairing: eremika (with minor background relationships)
tags: modern rival gang au, enemies to lovers, forbidden love, age difference, sociopolitical issues, racism, economic disparity, political corruption, family dysfunction, smut, angst, bit of a low burn...
chapter preview:
“You are meant for more than the small-town politics that we are all steeped in now.” Kiyomi looks toward their car, now pulled up to the curb. “Your uncle knows it. Your cousin knows it. Both clans in their entirety know it. We’ve readied you as best we can, and we are ready for you now. This is your time.”
Mikasa tastes warm iron. Sometime amidst her aunt’s speech, she had gnawed the inside of her cheek raw. She runs her tongue over the damaged tissue.
“What if—“
The words whither on Mikasa’s tongue when Rin appears at her side. He wordlessly beckons for the garment bag. Mikasa gladly relinquishes it. But the heaviness remains.
Mikasa’s throat feels like sandpaper, coarse and painful. She forcefully swallows to lubricate her vocal cords, to enable speech as Rin returns to open the door, to assist Kiyomi into the car.
“What if I’m not ready, Aunt Kiyomi?” Her voice is sharp and gasping, as if she had been drowning. “What if I don’t want this to be my time?”
18 notes
·
View notes
Text
situational/selective mutism list thing
Temperamental Inhibition
Social Anxiety Symptoms
Social Being: most have 'age-appropriate social skills'; some don't
Physical Symptoms: stomach, joints, head, chest etc. (will add the SM Throat Pain™)
Appearance: blank face, stiff body, freeze; some appear relaxed perhaps because sympathetic nervous response.
Emotional: depends on age/social acceptability of mutism
Developmental Delays: motor, communication, social (asd, pdd)
Sensory Integration Dysfunction (DSI)
Common symptoms: sensory problem, defiant behaviour, hesitant to respond, social withdrawal, focus on academics
Behavioural: maladaptive coping mechanisms, inflexible, moody, stubborn
Co-Morbid Anxieties
Social Engagement Difficulties
source: selective mutism pdf by Dr Elisa Shipon-Blum. elmtreeclinic
long long post with more detail. seriously very very long🌹🌹
1. Temperamental Inhibition: Timid, cautious in new and unfamiliar situations, restrained, usually evident from infancy on. Separation anxiety as a young child.
2. Social Anxiety Symptoms: Over 90% of children with Selective Mutism have social anxiety. Uncomfortable being introduced to people, teased or criticized, being the center of attention, bringing attention to himself/herself, perfectionist (afraid to make a mistake), shy bladder syndrome (Paruresis), eating issues (embarrassed to eat in front of others).
3. Social Being: The majority of children/teens with SM have age appropriate social skills and are on target developmentally, although some do not. Most children on the autism spectrum struggle with speech/language skills, social skills and have developmental challenges.
4. Physical Symptoms: MUTISM, tummy ache, nausea, vomiting, joint pains, headaches, chest pain, shortness of breath, diarrhea, nervous feelings, scared feelings.
5. Appearance: Many children with Selective Mutism have a frozen-looking, blank, expressionless face and stiff, awkward body language with lack of eye contact when feeling anxious. This is especially true for younger children in the beginning of the school year or then suddenly approached by an unfamiliar person. They often appear like an animal in the wild when they stand motionless with fear! The older the child, the less likely he/she is to exhibit stiff, frozen body language. Also, the more comfortable a child is in a setting, the less likely a child will look anxious. For example, the young child who is comfortable and adjusted in school, yet is mute, may seem relaxed, but mutism is still present. One hypothesis is that heightened sympathetic response causes muscle tension and vocal cord paralysis.
6. Emotional: When the child is young, he/she may not seem upset about mutism since peers are more accepting. As children age, inner turmoil often develops and they may develop the negative ramifications of untreated anxiety (see below).
7. Developmental Delays: A proportion of children with Selective Mutism have developmental delays. Some have multiple delays and have the diagnosis of an autistic spectrum disorder, such as Pervasive Developmental Disorder, or Autism. Delays include motor, communication and/or social development.
8. Sensory Integration Dysfunction (DSI) symptoms, Processing Difficulties/Delays: For many children with SM, sensory processing difficulties are the underlying reason for being 'shut down' and their mutism. In larger, more crowded environments where multiple stimuli are present (such as the classroom setting), where the child feels an expectation, sensory modulation specifically, sensory defensiveness exists. Anxiety is created causing a 'freeze' mode to take place. The ultimate 'freeze mode' is MUTISM.
9. Common symptoms: Picky eater, bowel and bladder issues, sensitive to crowds, lights (hands over eyes, avoids bright lights), sounds (dislikes loud sounds, hands over ears, comments that it seems loud), touch (being bumped by others, hair brushing, tags, socks, etc), and heightened senses, i.e., perceptive, sensitive, Self-regulation difficulties (act outing, defiant, disobedient, easily frustrated, stubborn, inflexible, etc).
10. Common symptoms within a classroom environment: Withdrawal, playing alone or not playing at all, hesitation in responding (even nonverbally), distractibility, difficulty following a series of directions or staying on task, difficulty completing tasks. Experience at the Smart Center dictates that sensory processing difficulties may or may not cause learning or academic difficulties. Many children, especially, highly intelligent children can compensate academically and actually do quite well. MANY focus on their academic skills, often leaving behind 'the social interaction' within school. This tends to be more obvious as the child ages. What is crucial to understand is that many of these symptoms may NOT exist in a comfortable and predictable setting, such as at home. In some children, there are processing problems, such as auditory processing disorder, that cause learning issues as well as heightened stress.
11. Behavioral: Children with Selective Mutism are often inflexible and stubborn, moody, bossy, assertive and domineering at home. They may also exhibit dramatic mood swings, crying spells, withdrawal, avoidance, denial, and procrastination. These children have a need for inner control, order and structure, and may resist change or have difficulty with transitions. Some children may act silly or act out negatively in school, parties, in front of family and friends. WHY? These children have developed maladaptive coping mechanisms to combat their anxiety.
12. Co-Morbid Anxieties: Separation anxiety, Obsessive Compulsive Disorder (OCD), hoarding, Trichotillomania (hair pulling, skin picking), Generalized Anxiety Disorder, Specific phobias, Panic Disorder.
13. Communication Difficulties: Some children may have difficulty responding nonverbally to others, i.e., cannot point/nod in response to a teachers question, or indicate thank you by mouthing words. For many, waving hello/goodbye is extremely difficult. However, this is situational. This same child can not only respond nonverbally when comfortable, but can chatter nonstop! Some children may have difficulty initiating nonverbally when anxious, i.e., have difficulty or are unable to initiate play with peers or go up to a teacher to indicate need or want.
14. Social Engagement Difficulties: When one truly examines the characteristics of a child with Selective Mutism, it is obvious that many are unable to socially engage properly. When confronted by a stranger or less familiar individual, a child may withdraw, avoid eye contact, and 'shut down,' not only leaving a child speechless but preventing him/her from engaging with another individual. Greeting others, initiating needs and wants, etc., are often impossible for many children. Many shadow their parents in social environments often avoiding any social interaction at all. The common example given is; 'A child in grocery story can sing, laugh and talk loudly, but as soon as someone confronts him/her, the child freezes, avoids and withdraws from social interaction. As the child ages, freezing and shutting down rarely exist, but the child remains either noncommunicative or will respond nonverbally after an indeterminate amount of warm up time.
source: selective mutism pdf by Dr Elisa Shipon-Blum. elmtreeclinic
#situational mutism#selective mutism#mentalheathawareness#sensory processing#communication#sm tag#chaos-exhausted
21 notes
·
View notes
Text
Every time I go to acupuncture, the same nurse checks me in and does all my blood pressure, heart rate, oxygen checks, so they know I can't talk but can hear and talk to me the whole time about whatever they have to say for medical purposes or just asking about my day or telling me about theirs.
Today however, I was checked in by a new nurse. She talked at first, but then I signed that I couldn't speak, just so she knows I wasn't ignoring her when I don't answer. The signs were quite obvious as to what I'm saying, by the way. So after I tell her i can't talk, she gets quite as she goes through the checks, and I realize my mistake. So I stop the nurse and grab her attention with a wave of my hand and point to my ear then both signed yes and nodded my head, then pointed to my mouth and shook my head.
She was a bit flustered at that fumble in communications but recovered well and we both had a laugh about it. The nurse cares on with her tasks, talking this time, and we have a conversation about her tattoo, because they were beautiful.
#chronic illness#postural orthostatic tachycardia syndrome#disabled#ehlers danlos syndrome#chronic pain#hypermobile ehlers danlos#pots syndrome#chronically ill#disability#spoonie#nonverbal#psychogenic vocal cord dysfunction#vocal cord disorder#vocal cord dysfunction
99 notes
·
View notes
Text

Not all "difficulty breathing during exertion" is "exercise-induced asthma."
If someone has SOB, wheezing, and difficulty EXhaling with any kind of exercise, treat as asthma with a beta-2 agonist.
Exercise-induced bronchoconstriction (EIB) develops after 5-15 minutes of exertion (especially in dry air, like a track rather than the wet air of a pool) and lasts ~15 mins. Warm up for 10-15 mins +/- beta-2 agonist. May be asthma precursor.
Exercise-induced laryngeal dysfunction and/or vocal-cord dysfunction (VCD) is difficulty INhaling +/- stridor due to exertion. Refer to Speech for vocal relaxation rather than a beta-2 agonist.
17 notes
·
View notes
Note
Hiya
I'm wondering if anything in particular has helped you with talking/generally keeping your throat area together.
EDS tends to make everything migrate when you need it.
(disclaimer I am getting medical attention and will not take any answer to constitute medical advice, in so much as medical advice and daily life can be make seperate categories when chronically ill)
Hey! Thanks for the ask (and the disclaimer!)
A fun side effect of my EDS is that it affects my vocal cords in the form of vocal cord dysfunction, as well as a lot of just general muscle dysfunction.
Something I've found to be very helpful is speech therapy, working with a certified speech therapist to work on muscle control. Additional physical therapy that targets the neck and jaw joints might also be beneficial.
I get a lot of relief and help from myofascial release therapy. There are a lot of wild claims about MRT, but honestly, I ignore most of them and focus on the actual benefits which are healthier soft tissue and pain reduction, which makes it a lot easier to do strengthening PT in the long run.
I also find 'face yoga' that targets the jaw/throat area also really helpful for easing a lot of the pain I experience in the throat/neck due to my EDS. Ignore the "helps with jaw definition" or any of the "get rid of your double chin" claims you might see on YT. The exercises are just really good for doing some gentle neck/throat work which often gets neglected. It's just a shame they couch it in diet culture to get views. Just make sure when you put any pressure near the front of your throat, you are being as GENTLE as possible.
The temptation to dig into muscles is real, especially because it sometimes feels like the pain is bone-deep, but there are a lot of delicate veins and arteries in that area and you really only need the lightest of touches and stretching. (This is why I like MRT, it can feel like the benefits of deep tissue massage without having to dig into the muscles, which is often problematic for folks with EDS anyway because of how fragile our skin/soft tissue is.)
Anyway, I hope those give you some new starting points to look into.
And good luck, the neck, and throat is such a bastard area to try and care for.
183 notes
·
View notes
Text
I've had breathing problems for as long as I can remember. I usually breathe through my mouth, not my nose, and I would have frequent episodes where it felt like I couldn't get any air at all, which would often cause panic attacks, which would in turn make things worse. And when I didn't have episodes like those, I would still frequently have these high-pitched "gasps" where I would very suddenly take in a huge breath.
I had been tested for asthma when I was a kid. The tests were negative. It wasn't asthma, so what was it?
Finally, after years of suffering, my parents were able to get a doctor to inspect my nose and down my throat with a camera. I was somewhere between the ages of 15 and 17, I can't quite remember.
It turns out that there were two problems. First, I had a deviated septum, meaning that the wall between my nasal passages was off-center. This explained my difficulties breathing through my nose.
The second problem was that I had vocal cord dysfunction. Vocal cord dysfunction is when your vocal cords don't open up all the way when breathing. This can result in feeling like you can't breathe. It also explained the little gasps I would often have.
My doctor gave me a sinus rinse, recommended a nasal gel, and sent me to speech therapy, where I would learn breathing exercises that would supposedly ease my symptoms.
Unfortunately, I have ADHD, which makes my memory the absolute worst. So, guess who hasn't done any of that shit in years and is having difficulty breathing right now?
#vocal cord dysfunction#deviated septum#also another fun fact about having a deviated septum: you can't fucking blow your nose#I always have to take tissues and use them to basically pick my nose because that's literally the only way to clear my nose#I always wondered how the hell blowing your nose worked for everyone else but not for me#also another fun fact: most of the time vocal cord dysfunction is misdiagnosed as asthma#the key difference between the two is that inhalers don't work with vocal cord dysfunction#that was how we ruled out asthma#anyway i'll shut up now#breathing problems
1 note
·
View note
Last Seen Blogs

askashishaggarwal
Ashish Aggarwal

bombusherru
Congrats you found me by accident or something

auriantheman
AurianTheMan
youliveonavenueq
Untitled
askashishaggarwal
Ashish Aggarwal