#accreta
Text
CASTIEL'S PENDING RESOLUTION;
we're turning over all the cards.
youtube
Death and the goddess, something took hold of the darkness; the dark side of the moon. The ego's searching light through the darkness that might reveal the garden within.
youtube
2. You've arrived, then. The answer to life's greatest question. Nothing gold can stay. Something too precious to let go. What is your Whole World. The good and the bad. It was done for one thing. Cas, there's something I have to say. It's in just saying it.
youtube
3. Burn my dread, face myself. What do you fear. I know what you hate. I know who you love. What you fear. There is nothing for you here. Let the sun shine on your face. Very violently. Death is the infinite vessel. The Universe/The Whole World; what is your whole world. The Shadow, the thing that rules the empty. Humanity. I love you. It's a Supernatural love story. Tick tock, we're running out of time. It's in just saying it, in just Being.
Death is an infinite vessel.
OMITTED - the glass cliff
PERSONA 3 FES
WINCHESTERS FES
Follow the given timestamps:
0:00-7:07: Aeon; skip to:
19:50-21:10: The World; The Universe
We already saved the Whole World once, this is just our Encore.
youtube
I don't have many regrets but the few I do still haunt me; empty is just... regrets. I don't think he has any regrets. The Great Seal. The Tzimtzum. Graveyard dirt, Angel Blood, A Human Heart, My own still coursing blood, and my The Final Breath. Death is an infinite vessel. The One True Thing. In Order to be In The Garden-- He's watching us. The whole world.
youtube
VITRIOL is an acronym for Visita Interiora Terrae Rectificando Invenies Occultum Lapidem which translates into “Visit the interior of the earth, and by rectifying what you find there, you will discover the hidden stone (philosopher’s stone)”.
Or, loosely translated, in order to be in the occultum, the occultum/garden must be in you. Let in the light, let the sun shine on the moon and raise mind to soul. And soul to mind. In the garden. Where we belong, and always did. What is real. People, families. Chuck only wins if you let life's machinations beat you down. That's the babysteps. Now keep moving.
Let man know that he himself is deathless, for the cause of Death is Love, but Love is The All.
#the shadow#akrida#arcadia#accreta#castiel's uterus#tzimtzum#the great seal#death#the answer to life's greatest question#i know what you hate#i know what you fear#who you love#occultum#garden#akrida radio#the akrida hide in your deepest trauma thought box#who we are#who i am#it's in just being#it's in just saying it#there's something i have to say#persona 3#castiel's path#heart#winchesters codex#Youtube
20 notes
·
View notes
Text
Tocolytics should be administered if labor begins prior to 34 weeks' gestation. Indomethacin is preferred prior to 32 weeks, and nifedipine is preferred after 32 weeks.
Placenta accreta spectrum can usually be detected reliability by 18-24 weeks with ultrasound specifically looking for large, irregular intraplacental sonolucent spaces (placental lacunae).
Prior to treating an ectopic pregnancy with methotrexate, there must be certainty there is no intrauterine pregnancy in order to avoid significant damage to a developing fetus. Serial bHCG levels and possibly repeat ultrasound confirming there is no intrauterine pregnancy must be performed prior to initiation of methotrexate. Candidates for methotrexate include patients who are stable with no hepatic or renal impairment and who will be able to follow up. Hemodynamically unstable patients with ectopic pregnancy require emergent surgical intervention and are not candidates for medical or expectant management.
Diagnosis of HELLP (hemolysis, elevated liver-enzyme levels, low platelet count) syndrome is vital, because it carries a mortality rate of up to 20% and is often initially misdiagnosed. Diagnosis is made by evidence of hemolysis, low platelet count (100,000/μL or less), and elevated levels of liver enzymes (defined as aspartate- or alanine-transaminase concentrations that are twice the upper limit of the normal range).
In some percentage of diabetic women, pregnancy will result in accelerated diabetic retinopathy and should be closely monitored. All women with diabetes who are pregnant or contemplating pregnancy should be extensively counseled about the increased visual screening requirements and risks associated with pregnancy.
Patients with preeclampsia with severe features before 34 weeks gestation require inpatient admission with corticosteroid administration and delivery at 34 weeks gestation. Fetal or maternal instability may require even earlier delivery under certain circumstances.
While preparing for delivery, administration of betamethasone may be considered in pregnant women less than 34w0d of gestation who are at risk of preterm birth within 7 days. A Cochrane review showed that the use of steroids had an overall reduction in neonatal death, respiratory distress syndrome, cerebroventricular hemorrhage, necrotizing enterocolitis, respiratory support, intensive care, and systemic infections in the first 48 hours of life.
#tocolytics#placental lacunae#placenta accreta#ectopic pregnancy#MTX#HELLP#HELLP syndrome#gestational diabetes#preeclampsia
2 notes
·
View notes
Text
#high risk obstetrics in mumbai#top gynecologist in mumbai#best obstetrician in mumbai#best gynecologist and obstetrician in mumbai#placenta accreta#dr neelima mantri#gynecologist mumbai
0 notes
Note
whats up with abortion in illinois?
It's legal and access is enshrined in the state constitution for one!
In Illinois you can access medication abortion both in person and via telehealth up to 12 weeks (through Carafem) or 11 weeks (through Planned Parenthood). Several Planned Parenthood locations offer procedural abortions, including one in Chicago, one in Aurora, one in Flossmoor and one in Springfield, and near the border in the St. Louis area there are PPs that offer procedural abortion up to 26 and 28 weeks as well as an independent site called Hope Clinic which goes to 24 weeks. In Chicago, there is another private stand alone clinic called Family Planning Associates that offers abortion to 24 weeks, and several Chicago area hospitals including Northwestern and UIC provide the procedure "to viability" which is at physician discretion and allows for later term, "medically indicated" abortions.
Several organizations exist to facilitate access to abortion. Abortion (and its associated medications, including sedation) is covered by Illinois medicaid (public assistance insurance) and many patients who don't qualify for medicaid qualify for a type of temporary medicaid available to pregnant women which can also cover the procedure. Midwest Access Coalition is a practical support fund which can offer travel, housing and gas assistance both to Illinois residents and people traveling to Illinois for abortion. Chicago Abortion Fund can provide vouchers for part of the cost of a procedure. Hoosier Abortion Fund helps Indiana residents traveling for abortion, often into Illinois. Both Planned Parenthood and Family Planning Associates have internal funding sources which can reduce procedure cost. The IL state government has a helpline named CARLA (The Complex Abortion Regional Line for Access) which assists patients and their providers in coordinating care for more complex abortion procedures which cannot be done outpatient (ie, if a patient has a bleeding disorder, uncontrolled seizures, placenta previa or accreta, etc).
If you need an abortion and are overwhelmed with planning the logistics, especially if you are traveling from out of state or from Southern Illinois, you can call the Regional Logistics Center for help scheduling an abortion.
15 notes
·
View notes
Text


source link
it is an understatement to call this horrific. the slides do speak for themselves however i would like to point out a few things as well —
c sections without anesthetic: keep in mind, it’s not like they’re not just having their stomachs cut into. during a c section there are seven different layers that have to be cut into, pulled out of the way, and then stitched back up after the baby is removed. it is major surgery.
there are also women with complications such as placenta accreta which poses a risk for significant blood loss and makes vaginal delivery impossible. please try to imagine knowing the only way to keep you and your baby safe is to have a cesarean… and that you need to do it with full sensation in your body.
they are sent home only 3 hours after delivery but WHO suggests a minimum 24 hour stay for anyone who has given birth vaginally to minimize the risk of hemorrhaging. there’s also a risk of postpartum preeclampsia up to 6 weeks after delivery, which can be deadly.
this is not to mention that once you get past the horror of delivery, what if the baby is premature? the lungs finish developing last at around 36 weeks. because of this these babies born at 34 weeks and before usually need help breathing. micro preemies almost always require respiratory support. imagine giving birth to a baby that could usually survive with interventions, like temperature regulation and ventilations (28 weekers have up to a 90% survival rate for reference) and they die despite that because there’s no fucking electricity.
the horror in gaza is multifaceted and neverending.
27 notes
·
View notes
Text
Ricochet
Part IV: "... This Isn't What I Wanted (or Is It Everything?)"
Need to Catch up?
A New Boss (a prequel of sorts)
Part I: “Like Moths to the Flame”
Part II: “So Far Away, but Still So Near”
Part IIIa: “And I Know It Gets Dark…”
Part IIIb: "...But I Know the Way."
Pairings: Ethan Ramsey x F!OC (Tatum Erikson); Tobias Carrick x F!OC (Tatum)
Series Music Inspo: Ricochet by Starset (more of an acoustic fan? Check it here.)
Chapter Music Inspo: "Shapeshifting" by Taylor Acorn
Series Summary: Almost two decades ago, he gave love a chance–and she betrayed him. Now after all of this time, Dr. Ethan Ramsey and Dr. Tatum Erikson realize that their past feelings might not exactly be ancient history–especially now that they are forced to work together.
Chapter Summary: Tatum has called for assistance from the main OR, but will they be any help when several emergencies emerge at the same time? Tatum takes courage and finds her voice when she remembers an awful experience; she meets a new, young surgical resident
Warning: 🔞mature audiences only 🔞 TW: dub-con/non-con 🍋; strong depiction of a medical procedure; strong depiction of a medical emergency involving newborn infant and mother; language (including a slur against woman); angst; discussion of infidelity
Word Count: 4300 (+/-)
A/N: Characters and some plot belong to Pixelberry! Not beta'd, so please excuse my errors. Fair warning: this is not my strongest chapter (I mean, it took my FOREVER to actually finish it and post), but I hope you enjoy the journey regardless.
A/N 2: It really has been forever and day, so here's a recap: *clear throat* Previously in Ricochet... Unable to sleep after his encounter with Casey at Raf and Sienna's wedding, Ethan's heads in to the hospital despite it being his day off; after a challenging talk with Tobias about unspoken intentions with Tatum, the chief heads over to the L&D ORs, where he finds a terrified Tatum in the midst of a rare, very lethal surgery, and her hesitation doesn't go unnoticed by the staff in the observation deck as they ridicule the new chief of OB, Tobias being the ringleader of the hate; Ethan sternly bans them from witnessing the once-in-a-lifetime surgery before turning to encourage Tatum in the most Ethan-way possible: with just a look...
~🖤~
Remaining in her sterile surgical gear, Tatum carefully takes a seat on a metal stool, saving her back for the arduous surgery staring at her on the operating table. She anxiously chews on her lip, her eyes darting across her patient's open abdomen before fixating on her fresh set of steel tools.
The procedure she knows like the back of her hand: clamp, cut, control bleeding. But, with the placenta growing outside of the uterus and into other organs, into the delicate vasculature of the pelvis, it's like going into this surgery blindfolded.
The uterus has to come out–and the patient is well aware of this and prepared. But, this isn't like any other hysterectomy. Will it cost the patient her ovaries? Her bowels and bladder? Her life?
Tatum urgently stands back up, staring at the clock on the wall. It had been over twenty minutes, and her STAT page was yet to be answered by surgery. Too slow for L&D standards; way too slow for her own standards. And at this rate, the patient’s spinal anesthesia is going to dissipate before they even start.
Damnit… think, Tatum, think…
She could always page Ramsey.
No.
Tatum refuses to resort to that. Well, not that calling on him for assistance would be the worst thing in the world.
She had a brief moment of weakness–more like a moment of uncertainty, actually–when she discovered her patient’s unknown lethal condition, and Ethan clearly recognized the fear etched on her face from the gallery; truth be told, the accreta scared him, too.
However, Tatum is a highly skilled physician; her reputation for excellence precedes her. If she needs help, she will ask for it–and she has.
She's embarrassed that she even needed Ethan's reassurance earlier, even if it was just for that moment, that simple nod of 'I believe in you.' Sure, it was supportive, and it gave her that extra push she needed to power forward.
But that look, that damn crystal gaze…
Damnit, why did she have to freeze? It was only for an instant, a very brief second. Tatum Erikson doesn't need a vote of confidence. Not from anyone, not even from the famous Dr. Ethan Ramsey. She is independently strong, independently capable.
But now, Tatum feels as if she's accidentally exposed a secret side to herself, like her own Achilles' heel; it's quite possible now he knows he still has an effect on her.
Worse, now she knows he still has an effect on her.
She turns to Wanda the charge nurse, who shrugs her shoulders to the physician's unspoken question.
Tatum takes a deep cleansing breath, trying her best to stay calm. "Can someone please tell me where the hell is my backup ?"
"Right here, Doctor…"
Hearing the monotoned boredom of an unfamiliar male voice, Tatum spins around to find two gentlemen moseying into her operating room, drying off their hands with blue sterile towels. The tension raking her nerves is instantly relieved, seeing her help arrive.
The older of the men continues. "I'm Dr. Aaron Tanaka, chief of surgery," he nods his head towards the taller gentleman. "And this is one of my fourth-years–"
"Sup?" The young surgical resident smoothly winks at Tatum, popping gum under his mask.
Oh great, a kindergartner… Tatum rolls her eyes as the healthcare team assists the men into their protective gowns. As the physicians roll their gloves over the cuffs of their sleeves, Tatum escorts them over to her patient, catching them up to speed on what has happened so far. Together, Dr. Tanaka and Dr. Erikson develop several plans of how to overcome the patient's lethal risk of hemorrhaging.
"Whoa…" the younger surgeon exclaims, "I have never seen anything like that–"
Tatum clears her throat, glaring at the amateur physician.
"Should I start charging admission?" The patient jokes on the other side of the blue drape, causing the room to snicker loudly.
Tatum leans toward the young doctor, her tone low and syrupy. And quite sarcastic. “Try not to say everything that pops into that feeble little brain of yours–” He pops his chewing gum, winking with a finger gun. Fucking residents…
As the room quiets down, the patient softly whistles to get her surgeon's attention. "Dr. Erikson?" Tatum tucks in her hands, carefully wiggling her body closer to the head of the table to hear the patient clearer.
"Yes ma'am? You ready?"
The patient lowers her voice. "He's not, eh, doing the surgery, is he?" referring to the surgical resident who was shocked by the scene.
The blonde guffaws. "No, ma'am," she glances back to the young doctor who is now talking cooly with her staff, the nurses dow-eyed and eagerly laughing at everything he says. But suddenly, he fixes his flirty, soft copper eyes on Tatum. His intense gaze fools her into inadvertently staring too long as she begins to take note of his tall, trim physique. He begins to smolder, causing her to turn her attention back to her patient. "H–He's here for… my entertainment."
“Is he hot? He sounds hot.” Tatum gives a dramatic wink while her patient shoots a knowing look in return, clicking her tongue and giggling.
“Erikson?” The anesthesthetist breaks her from her reverie, confirming the case status. “We’re ready.”
"Perfect.” Tatum takes her place on a metal step stool, matching her height with her assists. She’s above average height for a woman at five-foot-nine-inches, but still, the men tower over her. She looks around the room with a commanding stance. “Are we set then?"
"Ready when you are, Doc," Dr. Tanaka affirms, others nodding in agreement.
Tatum cracks her neck, taking a big deep breath. "Okay, then," she exhales, surveying her staff, "now who's ready to have a birthday party?"
After a few shared chuckles, the patient was safely intubated and given the proper amount of anesthesia. Seeing that she was safely asleep under the appropriate gasses, Dr. Erikson quickly proceeds with her cesarean surgery, and in record time, she delivers a beautiful six-pound, thirteen-ounce baby girl.
The OB takes the tiny infant in her arms, making cooing noises to welcome the tiny one into the world as she suctions out the mouth and nose with a green bulb syringe.
But as the birthday cheers begin to quiet down around the room, the situation abruptly becomes dire: the baby is limp, her skin becoming dusky gray at the cut of her cord. Tatum continues to stimulate the baby to breathe with no avail.
"C'mon, baby girl," Tatum's words become gruffly matter-of-fact. She wrestles with her legs, flicking her feet vigorously with her fingers, but her tiny frame lays flaccid in the physician's hands like a limp fish.
Lifeless.
No cry.
"Nurse?" Tatum urgently calls out, quickly handing off the stunned baby to the waiting NICU staff. "Keep me updated–" she orders as the team hooks the baby up to specialized monitors, performing the necessary interventions to resuscitate.
Tatum briefly closes her eyes, taking a deep breath before she focuses on the surgery. Opening her eyes, she nods assuredly to Tanaka before continuing. “Pickups.” The surgical tech hands the obstetrician a pair of tissue forceps and a cauterizing tool to continue with her surgery. "I need an update, ladies," Tatum shouts. Her tone is assertive and controlled, commanding and clear. Inwardly she is panicked, but she remains calm, a testament to her leadership skills and her quick thinking.
"We're just past a minute of life. Pulse is 52. Starting compressions… draw up epi… let's get an umbilical line…"
Fuck. Tatum's nerves tangle as she listens to the baby's team of professionals administer medications and physical maneuvers to make her spontaneously breathe on her own. Still, the OB continues steadily and carefully with her surgery, glancing over at the baby every few seconds.
C'mon, baby girl. Cmon. Mama needs you–
Suddenly, a trill of alarms begin to blare rapidly, stealing everyone's attention. Before realizing what had happened, warm, crimson fluid spatters across the surgical field, saturating Tatum's arms, gloves and gown; her mask and shield are covered with blood.
"Erikson!" Shouts the anesthetist, "BP 67/23… heart rate now in the 150s…"
"That vessel on the lateral portion of the accreta blew. She's bleeding out, Erikson–" Tanaka quickly suctions the field of the pooling blood. "She's getting shocky… and fast. How should we proceed?"
Fuck. Tatum grabs a stack of lap pads and tosses them to the young resident. "We need to find the source of this bleeding." He nods and instantly begins soaking up the copious amounts of fluid with the large, thick pieces of gauze as Tatum explores the body cavity with Tanaka.
"BPs dropping," anesthesia hollers.
"Give me a second–"
"Erikson! She doesn't have a second–"
"Bolus her and mass transfuse four units–" Feeling their stares, Tatum looks up at her concerned anesthesia team. "Now!" She growls, her eyebrows furrowing as she returns to the carnage. "Then cross and match four more units… and buy me a goddamn second!"
Taking a deep breath, Tatum flickers her attention to her assistants, both of them giving her an approving nod.
"Damnit! Dr. Erikson! I can't get this intubation on the baby. We need you–"
"Dr. Erikson! Vitals not improving–"
“Dr. Erikson–!”
“Dr. Erikson–!”
Tatum glances around the room, her paralyzing fear slowing down time. All she can hear is the thunder of her own heart racing, the rasp of her breathing echoing in her head. She sees the concerned faces; she hears the whispers of doubt and concern from her colleagues
She’s losing them. The possibility of losing either of them never crossed her mind, but both? A mother and child? This wasn’t the plan; this was never part of the fucking plan.
The sting of tears pricks at Tatum’s reddening eyes.
What do I do?... what have I done?
------
The torrential downpour hushes to a dull tapping of raindrops as hollow roars of thunder rumble in the distance; but, the storm was just beginning for Tatum as she lays frozen in her bed, her sanctuary that she shared only with the love of her life.
And now, his best friend.
The room suddenly feels so different, so strange and unknown. It seems so ordinary, no longer special. The warmth of home has melted away, leaving a peculiar chill of unfamiliarity.
There's a handsome smell, a spicy musk that hangs in the air. But, it’s not Ethan.
There’s a pair of distressed jeans tossed carelessly on the carpet, but the body heat that lingers isn’t from him either.
There’s a set of arms possessively wrapped around her naked body. The skin feels … different. The hair? Different. The actual grip and weight on top of her: it’s different.
It’s not Ethan.
What have I done? Tatum’s eyes pain with the threat of tears, her chest beginning to rise and fall in search of fresh air, in search of clarity. But with each gasp of a new breath, she quietly whimpers in agony for the ache in her heart.
She had broken the most precious thing she owned. That she will ever own.
"You awake?" Tobias croons in her ear as his large hand massages the soft, flat planes of her belly. He tenderly works his way down, his fingers intimately petting her sore, swollen lips between her thighs.
She winces, her toes curling as her body grows rigid from his unwanted touch. She consciously holds her breath, hoping he won't notice her terrified nerves.
"What’s wrong, baby girl?" he whispers, pressing his full lips against her neck, biting at the sensitive area. “Are you needing more already?”
Tatum can feel his heavy erection against her hip, his intentions painfully aware. He slowly rocks himself against her body as if to charm her like a serpent, hypnotizing her to give him exactly what he wants. Another rendezvous; another fuck; another sin.
Desperate for a gentle hand, she foolishly lost herself in Tobias’s caress earlier that evening. She was vulnerable, inebriated, and lonely. In her altered mind, even for just a small moment, being in his arms made sense–well, being in someone's arms made sense. She needed Ethan. She was broken and hurt, and she despairingly needed her boyfriend’s love and comfort.
But, Tobias was there. His words, the look on his face, the heat in his touch: it was exactly what she needed to sooth her wounds. For the moment.
And now, he wants to claim her once more.
Shit, can a woman deny a man if she’s already given in once? Does he have a claim over her, a right, an expectation? The conversation played out in her head: 'You said, ‘yes’ earlier, you tease. You whore…'
Oh God, would he turn on her? Shame her publicly? Worse, would he tell Ethan before she could… that is if she decided to actually tell her boyfriend–no, she had to, right? But if Tobias told Ethan before her, would he be honest about what happened? Or would she become another victim of slut-shaming? 'She couldn't be faithful; what else is she lying about?'
It was one time; it was one mistake. Does that unravel three years of trust? Three years of commitment? Three years of love?
Tatum already knew the answer, and the taste of bile grazes the back of her throat.
She needed to stop this from happening again. But how can she while still protecting herself?
This was a grave mistake…
Tobias gently rolls her over, kissing hungrily against her pout. His tongue swipes across her plump lips, his large hand roaming down the outside of her thigh. But then he stops, sensing her awkwardness. “You okay?” His voice is haunting, dark, his gray eyes piercing her vacant stare.
No. “Uh-huh,” she lies with a nod. The corners of her mouth begin to curl as his hand grips behind her knee, hitching her leg around his waist. Goosebumps ignite across her skin in betrayal as he pushes himself against her throbbing clit.
Stop, her brain screams.
“Relax, Tate,” he growls before reclaiming her lips, nipping and bruising them. "Let me make you feel good."
Tell him to stop.
“Is this okay?”
No. She reluctantly shakes her head 'yes' in agreement.
He aligns his girth with her entrance, fisting the sheets next to her head as he hovers above her docile form.
Say something! Do anything! she screams to herself, but she is paralyzed by fear. It's more than just the fear of the consequences of what's happening. Tatum is terrified of herself.
Then again, maybe she believes she deserves this. It wasn't going to be pleasurable for her, rather an act of attrition. Maybe that's why her body allowed his advances. Maybe she needed to feel the discomfort as a form of punishment for what she had done against Ethan. Maybe this was a last ditch effort to settle the score, to make things even.
Feeling Tobias's weight begin to push into her, she turns her head to her phone laying on the bedside table, praying for Ethan to call her, text her, anything to interrupt this.
But nothing comes through.
And suddenly, she sobs out a painful moan.
------
“Dr. Erikson—!”
Say something… Do anything…
Tatum subtly shakes her head, the horrid memory fleeing her thoughts. The frantic voices of the NICU team pull her attention to the struggling infant.
“Please, doc, we need this intubation. We don’t have time to wait for our back-up–”
Tatum watches the mother’s abdomen pool with blood before turning a pleading stare to her colleague. “Tanaka–?”
“I’m on it.” He elbows his wide-eyed resident, “Suction.”
Say something… Do anything…
Seeing the men take over, Tatum instantly rips off her dirty gown and gloves and positions herself at the head of the baby’s bed.
“Would you like for us to call our back-up?” The neonatal practitioner urgently interrupts.
Tatum remains silent, seemingly ignoring her. She slides a metal apparatus into the infant’s mouth before guiding a clear plastic tube inside the throat and past the vocal cords. Attaching an ambu bag to the special tube to assist with the baby’s breathing, she watches the tiny chest rise and fall in coordination with the squeezing of the ventilation. Tatum steals a stethoscope from a nearby nurse’s neck and listens closely to the lungs.
“Breath sounds…” she moves the flat, round bell to the other side of the tiny torso, “equal and bilateral.” Tatum smirks as on-lookers silently praise her with sighs of relief. “Now,” she continues, “get this kid some epi. Oh! And ma’am?” She turns to the practitioner while handing the stethoscope back to the nurse. “I don’t need back-up.”
Slipping back into her sterile apparel, Tatum rejoins Tanaka and his resident, but quickly notices that he still hasn’t been able to find the source of the bleeding. She looks to anesthesia, “Where are we on our blood?”
“The first unit is pouring into her, but–”
“--she’s bleeding it back out–shit!” Tatum stares at the flood of viscous crimson.
“How would you like to proceed?” Dr. Tanaka questions. “Maybe order some more blood?”
Tatum thinks in silence, racking her brain for a solution.
“Should we call someone? Maybe someone who knows?” Anesthesia sardonically suggests, earning him a hateful side-eye.
“Maybe you should just plug the hole up with your finger,” the resident chuckles, his attending suddenly glaring in disapproval. Tatum glances at him, her eyes squinting into a glower as her eyebrows furrow.
These idiots–
But then she stops. She slowly cocks her head with curiosity as she suddenly considers his words.
Actually…
"My apologies, Dr. Erikson,” Tanaka interjects. “Perhaps we should–"
“--plug the hole up,” Tatum interrupts the seasoned surgeon, echoing the resident's poor joke, only this time, there is a certainty in her voice. "I’m going in." She instantly sticks her gloved hand into the open abdominal cavity, gently feeling her way around the thick, warm fluid.
“Dr. Erikson,” Dr. Tanaka chides, “this… is… highly unusual–”
“Just keep suctioning,” she orders, her hands tenderly brushing against the fragile uterus and the delicate vessels.
Tanaka scoffs, giving a knowing look to a worried anesthesia provider. The tall, young resident looks to his mentor, unsure of what to do… or if there was anything to do. He nervously looks back to Dr. Erikson, but suddenly his jaw falls open.
Her eyes are closed.
"Erikson–?" the anesthesiologist attempts to get her attention.
"Give me a sec," she carefully feels her way through the body.
His voice grows frantic. "Her vitals are–"
"Got it!" She instantly peers up at her staff with relief before turning to her tech. Her hand remains deep inside the patient, her arm twisted at an odd angle. "Get me a 3-O vicryl suture on an SH. Now please."
Tatum works quickly in silence as she temporarily fixes the weak, broken vessel. It wasn't a long-term answer, but this would buy them time to thoroughly clear the area of the accreta while cauterizing the necessary vessels before they performed the hysterectomy.
"Okay, so–" She flashes an innocent gaze to anesthesia, batting her eyelashes. "What were you saying about those vitals, doctor?" She's grateful she's wearing a mask to hide her smirk, but she knows her eyes are giving her away.
"Stabilizing, ma'am, uh. Doctor."
Shaking his head in disbelief, Dr. Tanaka suctions to clear the field–and it stays that way.
"How did you know that would work?" The resident questions, his warm gaze fixating on the blonde OB.
Tatum stops, thoughts racing through her mind as she considers her words. She then subtly shakes her head, returning to the operation. "I didn't… but sometimes even when you don't know what the answer is, you just have to do something. It’s way better than nothing."
------
Impressive. That's the word men use when a lady doctor kicks ass. The anesthesia team along with Dr. Tanaka couldn't stop talking about Tatum's heroic move of plugging up the ruptured vessel with her finger–and doing so only by her sense of touch, completely blind. If she were a man, they would've given her a cigar; but to be described as impressive? She knows her battles; she'll take it.
As they transfer the patient to recovery, Tatum takes a moment to herself to bask in the relief of saving a life. Of saving two. She slips back into the sink area to be alone in silence.
Taking in a deep cleansing breath, she allows her nerves to relax for the first time in several hours. She tightly clenches her watering eyes shut, taking pleasure in the subtle sting of warmth after being in the frigid sterile air.
She grips firmly to the edge of the sink as she wiggles and contorts her body, feeling the sudden release of tension as her joints crack and pop.
She's grateful; she knows the success of the surgery was not by her doing alone. She would never be foolish enough to be that cocky, to truly think that something like this was completely in her control. There's only so much in her power, so much that science and her skills can fix. But when lives are left to chance, she’s grateful that the gamble fell into her favor.
"Am I interrupting anything?"
Instantly recognizing the familiar lax vocal timbre, Tatum looks up from the large steel sinks to find the tall, surgical resident, leaning against the doorway outside the operating room. She smiles appreciatively at him as he takes off his blue mask.
He's young– maybe in his late twenties–and handsome with a natural caramel glow to his skin. The lines of his face are cut sharp, chiseled into perfect angles. He’s slender, but well-toned; his green scrub top pulls snug around the musculature of his biceps. Although his hibiscus-laden scrub cap covers his head, his sun-kissed brunette tresses are pulled back into a tiny ponytail. Most of the hairs, however, have already worked their way out of the elastic, resting on the nape of his neck.
"No," Tatum shakes her head, "not at all."
He steps into the room, casually sliding his hands into his pockets. “Can I just say… that was incredible.”
Tatum stifles a bright smile, feigning nonchalance as she picks at her nails. "I mean–" She glances back up at him, but seeing the glint of excitement reciprocated, she instantly forgets whatever smart-ass comment she was about to make and squeals. “God, that was fucking cool, wasn’t it?”
"The fucking coolest! One of the most interesting cases I've seen in a while," he sucks in his bottom lip, his dimpled grin plastered wide across his face. "You just…” he snickers under his breath, “wow, I don't see myself forgetting this anytime soon."
Their playfulness quickly vanishes as Tatum catches a hint of something in his tone. Is he flirting? Becoming hyper-aware of his proximity, an err of awkwardness falls between them. Feeling heat bloom on her cheeks, Tatum quickly attempts to rectify the situation by clearing her throat, rolling back her shoulders to straighten out her back. “By the way, thank you," she starts, "for your help in there with the, uh… with the, um–" Unable to find the right words, she begins holding up her pointer finger, spinning it around in the air. "Um… You know? The whole fingering thing–I mean–"
He chuckles, coyly looking down at the ground before meeting her gaze again, flashing his pearly whites. "Dr. Erikson, are you accusing me of 'fingering' in your OR?"
Tatum's eyes widen. She purses her lips together to stifle her laughter. Oh, so you're a bad kindergartner… "That… that's not what I meant, uh… doctor… um–"
"Bryce," he holds out his hand to take hers. "Bryce Lahela."
Speechless, Tatum mindlessly places her hand in his palm. She clears her throat again as she shakes his hand sternly in a poor attempt of being professional. "Nice to officially meet you--" she states matter-of-factly, "--Bryce. I'm–"
"--going to Donahue's," he interrupts.
"What?"
He snickers. "You're going to Donahue's for a drink."
"Oh, am I now?"
"You are," he takes a step closer, the front of his Crocs kissing the toes of her tennis shoes. "With me. Those are the rules."
"Rules?"
"Mhmm," he hums as he lifts up her hand. Tatum didn't realize that he was still holding on even after their professional handshake. He points to the small tattoo on her wrist that she normally covers with her watch. "See this right here?"
"My tattoo?" She giggles sardonically to herself, curious as to what line he's about to feed her.
"You're a Virgo," he flashes a smirk, "which means we need to satisfy that impulsive side of yours by grabbing drinks together. In celebration of your badassery today, of course."
"Oh, of course," Tatum jests, pulling her hand away from him. "Too bad I'm not a Virgo," she turns to walk away, but stops herself, glancing back to him. "Also… you suck at astrology," she giggles before walking away from the sink area.
Bryce chuckles under his breath before jogging to catch up with her. "What’s with the Virgo ink then?"
Tatum rolls her eyes, glancing briefly at the collection of connected stars. "Long story–"
"--which… you can tell me… over drinks at Donahue's!" They both fall into laughter as Tatum comes to a stop in the hallway.
"You're not going to let this go, are you?"
"Hey, I wasn't lying about the rules. We have to celebrate."
Tatum looks up and down the empty corridor before crossing her arms, considering his proposition. God, is this what she is resorting to these days? Last night, Tobias and tonight, a resident? Who really is this guy anyway?
Tatum wasn't sure if he was messy or complicated; but he was gorgeous, and he was available. Maybe. And he wasn't Ethan Ramsey.
"One drink. As colleagues. That's it."
~🖤~
Tags (please let me know if you'd like to be added/removed):
PERMA
@alj4890 @ao719 @charlotteg234 @issabees @kat-tia801 @kingliam2019 @mainstreetreader @mom2000aggie @neotericthemis @nikirennie87 @peonierose @socalwriterbee @tessa-liam
ALL OPH
@alyshak92 @annfg8 @bisexualdisasteracd @cariantha @coffeeheartaddict2 @lsvdw-blog @mvalentine @ofmischiefandmedicine @rookiemartin @starrystarrytrouble @youlookappropriate
------
Thank you so much for your support! Every like, comment and reblog means the world to me! 🖤
#open heart#choices open heart#choices oph#ethan ramsey#dr. ethan ramsey#ethan ramsey x f!oc#ethan ramsey x tatum erikson#ethan x tatum#tathan#tobias carrick#dr. tobias carrick#bryce lahela#dr. bryce lahela#aaron tanaka#dr. aaron tanaka#choices fanfic#ricochet#open heart ricochet#tw dubcon#tw dubious consent#tw noncon#tw
32 notes
·
View notes
Text
So sorry to post another article about the Kardashians but I really wanted to highlight the term “Vanity Surrogacy”
Everyone thinks Kim Kardashian didn’t want to get fat but actually, she didn’t want to die.
A hole in her uterus caused by the ripping fingernails of a medical professional was the last straw in a macabre conga-line of fertility issues for the woman who has everything.
An emergency after the birth of her first child, North, meant: "My doctor had to stick his entire arm in me and detach the placenta with his hand, scraping it away from my uterus with his fingernails," she wrote. After that, everything about her second pregnancy was complicated.
Threatened miscarriage. Endo. Pre-eclampsia. Placenta accreta. Failed surgeries.
It’s a list that would leave a lot of women – ordinary, feet-of-clay women – thinking that two kids were enough kids.
But Kim Kardashian is not an ordinary woman, and she wanted more babies. And so, she called someone. And she started researching and, two children later, she’s the self-confessed surrogacy whisperer for Hollywood’s elite.
Her sister, Khloé, sought her advice when her obstetrician told her that having a second baby would be complicated and risky for her health, too.
"I'm not gonna get into specifics on camera," Khloé said on an episode of The Kardashians. "But they said it's an 80 per cent chance I'll miscarry... [My doctor] said she would feel terrible putting [an embryo] in without warning me that most likely I wouldn't be able to carry."
And Paris Hilton, who was once Kim’s boss, but now inhabits an entirely different world, called her when she got married, and wanted a baby, but didn’t want to get pregnant or give birth.
“Kim told me about (surrogacy) as well,” Hilton told Glamour magazine. “I’m using the same doctor, Dr Huang, who’s the best, and he has a concierge team that deals with everything.”
She’s helpful like that, Kim. She’s a get-s**t-done kind of woman, and she has strong opinions on the right way to treat the person who’s going to be implanted with your embryo and carry them to full term.
You should give them extra money for organic fruit and veggies, so you know what’s going in (sister Kourtney thinks you should get to dictate what kind of TV your carrier watches while she’s pregnant, but Kim thinks that’s woo-woo), she said in the same episode of The Kardashians. Kim knows you need to negotiate out all the details upfront, and that you should be mindful of your gestational carrier's feelings.
"I think the right thing to do is get them to come and see the baby at some point before they leave [the hospital]. You have to make decisions like do you want them to pump and send the milk to you every few days."
Luckily, what Kim also knows is that in Los Angeles, you don’t have to think of all this stuff yourself, because it's a town full of surrogacy attorneys, and surrogacy concierges. In the "surrogacy capital", it's a multi-million dollar business, and although we may never know how much the Kardashian sisters pay for their babies to bake, with all the discretion and extras required, we do know that a more basic model would set you back around $150,000 US.
Here in Australia, it’s entirely different.
Surrogacy as a business model is illegal. People who want or need to use a surrogate are only allowed to compensate for expenses incurred. And, although rules vary from state to state, most places in Australia require proof that a surrogate is needed, not only wanted.
So Kim and Khloé yes, but Paris, probably not.
Back in LA, there are no such boundaries, unless fertility clinics choose to put them in place. And there are two schools of thought about how appropriate that is.
On the one hand, reproductive science has made parents out of armies of people who might otherwise never have become parents, never experienced parental love, and never have built families they now couldn’t imagine being without. A selfless act of service, to carry a baby for someone who desperately wants one. The most beautiful gift.
On the other sits a discomfort with the idea of the rich renting the bodies of the less-rich to do the undoubtedly difficult and often risky business of carrying their children. Avoiding the physical toll of pregnancy for a variety of reasons, and the one that people can't shake a suspicion about is... vanity.
Vanity surrogacy, or Lifestyle Surrogacy, is a contentious issue to some.
And it doesn't matter how many times Kim or Khloé talk about why they made the choices they made to build their families, there's a bubbling argument that they – and other celebrities, like Hilton – are normalising surrogacy at scale, and it's not to be celebrated by all.
For example, Proud Fertility, a surrogacy clinic in Canada, declares its opposition to the process on its "about" page.
"Vanity Surrogacy does away with honour and the sole purpose of being a surrogate. It is when a woman who is medically capable of carrying her own baby refuses to do so for cosmetic reasons such as maintaining their body shape. Vanity Surrogacy can only be described as renting the womb of another woman... It is similar with putting up babies for sale or even breeding animals for the market. A woman who chooses to be a Surrogate Mother should do so from her own willingness to give the gift of family to those who are not able to have it."
While others insist it's not anyone's business why a woman chooses not to carry a child, or why another chooses to carry one for her.
“I don’t have issues with it,” Dr Vicken Sahakian from Pacific Fertility Centre in Los Angeles, told The Guardian. “What’s the end result here? Somebody wants to be a parent. I’m facilitating that."
He says that it's not usually superstars like Kardashian who would use "vanity" surrogacy anyway, but mid-tier actresses and models whose livelihood depends on their bodies, and whose schedules will not allow for breaks to get pregnant and give birth.
"I understand that it’s controversial, it’s borderline unethical for some people, but put yourself in the shoes of a 26-year-old model who is making her living by modelling swimsuits. Tell me something – is it that unethical, to say let’s not destroy this woman’s career?
“If you’re a 28-year-old model or an actor and you get pregnant, you’re going to lose your job – you will. If you want to use a surrogate, I’ll help you.”
Thanks to Hollywoods sexism and ageism the average of a model is 21 to 23. Using fear of losing jobs to postpone the aging out of a highly competitive industry is a disingenuous reason to exploit another woman.
That's a reality felt by Jamie Chung, an American actress who had twin boys via surrogate in 2021 because she felt she couldn't risk pausing her career.
"I was terrified of becoming pregnant," she said at the time. "In my industry, it feels like you're easily forgotten if you don't work within the next month of your last job."
For Paris Hilton, her fear wasn't work or money, but birth itself. She has spoken about being assaulted in faux-medical exams as a teenager at boarding school, and said her fear of blood tests and examinations is overwhelming.
"When I was in The Simple Life," she said. "I had to be in a room when a woman was giving birth and that traumatised me as well. But I want a family so bad, it’s just the physical part of doing it. I’m just so scared… childbirth and death are the two things that scare me more than anything in the world.”
After listening to Kim's advice, Khloé Kardashian did go ahead with surrogacy, and brought her son, Tatum, home in July last year. Just last week, she spoke about how hard it was to go through that process, even with all the concierges in the world.
“A surrogate process – Kim knows – is very hard for me. It’s a mindf**k. It really is the weirdest thing,” she said, on The Kardashians. “People do say it takes a minute to feel connected, but Kim said hers was easy. This is not easy.”
As no choices women make about fertility ever are. However and why ever they make them.
#USA#australia#vanity surrogacy#anti surrogacy sunday#surrogacy exploits women#babies are not commodities#Women who already have kids using surrogacy to bond with a new man#What protections do surrogates have against those who want to control what TV she watches while pregnant?#The existence of surrogacy attorneys and concierges just mean it’s a big business#Lifestyle surrogacy#Most Actresses and models don’t have long standing careers due to sexism and ageism#How much longer will using a surrogate actually extend the average modeling career?
9 notes
·
View notes
Text
The Winchesters: Pilot Highlights and Thoughts
Better late than never, sorry guys. The cards weren’t in my favor yesterday, or today. It was long and detailed originally when l lost it and would have had to retype it all. So instead, here are a few highlights and my post thoughts.
WARNING: SPOILERS AHEAD!!!
Loved the opening. The foggy cemetery, dark of night with only Samuel added a spookiness to it. The caverns were just as creepy but filled me with curiosity and suspense.
The moment the sigil was revealed, l smiled with recognition but didn’t want to jump the gun just yet…
“See ya around Soldier Boy.” (2)
💚🫡💚
John and Mary looking for their missing fathers. Similar parallels, SPN Pilot. Also, Mary's wanting out is another similarity. Sam wanted out, wanted normalcy and went to Stanford…
So many SPN Easter eggs I couldn't write them all down, lol.
BUNKER!!! I squealed when the lights sprang on and I saw the map table, John and Mary standing on the upper walkway looking around with wonder. Took me back to SPN season 8…
Men Of Letters! Because the chamber Samuel was in was so dark at first, even with his light, the sigil was still a little difficult to see.
The Accreta??? There’s a force out there, that’s stronger than Chuck!? aka God himself!? Oh, I can’t wait to learn more!
I was hooked 10 min into it. It was a surreal experience for me, not just as a fan but for me personally. Meg and Drake are the perfect John and Mary. The sheer raw emotion they put into their characters is truly amazing. One thing that stood out was how they seem to mirror Sam and Dean...
Don't let appearances deceive you, Just because Mary mirrors Dean and John mirrors Sam that it means they're all the same...
Dean's narration intro was a surreal moment for me as a fan that came in a year after SPN ended... I grind like a loon and my heart fluttered, lol. When his physical intro scene came in, I shouted in my seat. 🤭
Too many Easter eggs to go over, however, it's the ones that have yet to be seen that have my attention... 😁 I can't wait to see where John and Mary's journey takes us and how all the puzzle pieces fall into place.
#the winchester spoilers#spn prequel#the winchesters#spn#dean winchester#supernatural#jackles#my thoughts#my episode rewrite thoughts#good night tumblr
7 notes
·
View notes
Note
Not here to argue further, just here to give a link regarding the opinion pieces you offered. https://healthfeedback.org/claimreview/lila-rose-claim-that-abortion-is-never-medically-necessary-is-inaccurate-it-is-necessary-in-certain-cases-to-preserve-mothers-life-young-america-foundation/
I'd like to firstly state that this link doesn't address the actual ARTICLE that I provided, and only a VIDEO made by Lila Rose. These are not the same.
A thing that stroke me in the narrative of these obstetricians is that they seemingly associate "terminating the pregnancy" with KILLING THE FETUS, WHEN BOTH AREN'T THE SAME AND THEY PURPOSELY PLAY ON THAT AMBIGUITY TO ARGUE THEY ARE
"if the pregnant woman develops a serious condition at 20 weeks, (...) it is critical to terminate the pregnancy quickly to save her life. There is no chance that the fetus can survive, and an abortion would be the fastest and safest way to terminate the pregnancy"
None of that justifies killing the fetus or letting them die even out of the womb. "quickly" is a purposely(?) unclear term that doesn't mean there's no room of time to wait for a time when the fetus has enough chances to survive.
"abortion later in pregnancy may also be necessary when complications severely compromise a woman’s health or life, conditions which may also reduce the possibility of fetal survival. These might include premature rupture of membranes and infection, preeclampsia, placental abruption, and placenta accreta"
The article I pulled out characterized the difference between removing the fetus out the mom's belly WHILE trying to keep them both alive (and they did) AND removing a fetus to let it die. Nine
Later, the article pull out a link to an article written by a "Dr Jen Gunter" arguing that abortion after 24 weeks is necessary, here's her justification of abortion
"There is a false belief that induction of labor early for a lethal anomaly is not an abortion. It is.
The end."
WOW. What a groundbreaking demonstration. NOWHERE does that "induction of labor" justifies letting that fetus die once out of the womb. She then pulls out her credentials which are about performing abortion at 24 weeks....really? How does any of that justifies letting a fetus die out of the womb/revoke the possibility to wait for a term more favorable for them to have the best chances to survive outside the womb.
Anyway, pro choicers stay taking L with their misguiding "fact checkers" that can be debunked by a rando like me.
Fascinating how despite these doctors promoting the importance of abortion to save women's life, plentiful of developed countries have death in pregnancy rates edging on 0% (in mine, France, it's 0.1%). And guess what, abortion is proportionally LOWER than in the USA. Maybe---just maybe abortion is NOT necessary to "save" women after all ?¯_(ツ)_/¯
Maybe these people are just mediocre OB-GYN that compulsively kill fetus to cope up with their low skills? ¯\_(ツ)_/¯
This is the last time I address your questions. Next time you have inquiries about pro choicer mediocrity from my pro life stance, YOU WILL HAVE TO PAY ME (I am not joking).
Now leave me alone, and have a nice day.
10 notes
·
View notes
Text
I’m against surrogacy for any reason, but HOW people are trashing the Kardashians for using surrogates isn’t sitting well with me.
Kim and Khloe both said they used surrogacy because of previous pregnancy complications. Kim had preeclampsia and placenta accreta during both pregnancies (resulting in her needing 5 surgeries to fix internal damage). Khloe‘s pregnancy with True was “high-risk” and the doctors told her any further pregnancies would also be high risk with over 80% miscarry rate.
The fact that they used surrogates after facing pregnancy complications is awful—knowing the potential horrors they are subjecting another woman too. But saying they used surrogacy for vanity reasons instead of medical completely glosses over the dangers or pregnancy.
Nick Jonas and Priyanka literally said they used a surrogate bc they couldn’t find time to fuck while she was ovulating and no one batted an eye.
4 notes
·
View notes
Text
Postpartum hemorrhage is 1000 mL of blood loss within the first 24 hours of giving birth.
The 4 Ts are the causes of postpartum hemorrhage:
1) Tone - uterine atony; most common cause of postpartum hemorrhage. In those cases, the uterus can be palpated above the level of the umbilicus and it's boggy. A normally contracting uterus should be below the level of the umbilicus, but if your uterus is tired of contracting, you'll feel it above the umbilicus. First do uterine massage. If that fails, oxytocin. If that fails, methylergonovine (caution in pts with HTN). Next is carboprost (aka "hemabate;" analogue of PGF2α; caution in pts with asthma).
Uterine inversion can also cause postpartum hemorrhage.😱 Try putting the uterus back in. If it's contracting so hard it doesn't want to go back in, use tocolytics (terbutaline). Then replace the uterus and resume oxytocin.
2) Tissue - retained tissue (placenta) or fetal parts. Blood vessels should not go to the edge of the placenta. Sometimes the placenta has an extra lobe and if a lobe gets torn and stays attached to the uterus, you'll know because you'll see blood vessels going to the edge of the piece of placenta that did come out. This is why you always inspect the placenta after it comes out. You use your hands to get the other piece out. If that doesn't work, you can try forceps. If that doesn't work, D&C or D&E (she's already dilated so it's either curettage or evactuation). You do not do this in placenta accreta! If you did that, you'd just end up making her bleed to death. That's why you can use TVUS to make sure you're doing the right thing.
3) Trauma - vaginal or uterine lacerations
4) Thrombin - delivery can be a catalyst for disseminated intravascular coagulation. A normal fibrinogen level is actually abnormal in pregnancy.
2 notes
·
View notes
Text
That’s Republican Distraction
Endorsement by losing Prunt
Before Isreal distraction
And shaking Hands
Con cedar tall
By hello Halley
Make us all stupid
Republican
Hog wash
Dear Iowa how’s the weather
Not paying enough attention
This is not the U.N.
Iowa holds the votes for a country
Toppled down what with Tornados
The whirlwinds provided by IOWA
In our Prseidencies
Mother Nature gives a finger!
Will you fuck up again
Or vote correctly
Don’t cry over rain from sky
Hot cold pressures
Are what you like before an election
Enjoy the political weather!
Iowa-ians
Most sad
Most sad
Most sad
You run into others
You have early detection alarms
The most sad from Iowa
Lost personal property
You Insured?!
You placenta accreta
And your poles control all of U.S.
No band aid on ur votes
Mother Nature calling out to you!
My shed was auctioned
Florida gave first kid locked in a car
In the heat
Republican distractions
A Prunt !shocks humans!
#sideshow distraction#Prunts#At play |>#wordsbymm#concede#even bitches do#shake that hand#loser#Republicans and distractions#thank you N H gnarly#the pictured captured pock#you ur not really#but pretty ugly Halley#contender consider con the seeders#words#rough bitch#vent#mmybsdrow#need my capsule#it’s in between#see blue from background white#in reds#most sad#mossad#mostly sad#in aliens#NE towards Middle East above equator
0 notes
Text
The common risk factors associated with high-risk pregnancies
Dr. Shubhra singh
Dr. Shubhra Singh, a prominent gynecologist in Jaipur, often deals with high-risk pregnancies and understands the common risk factors associated with them. High-risk pregnancies are those that pose a potential threat to the health of the mother, the baby, or both. Several factors contribute to the classification of a pregnancy as high-risk:
Maternal Age: Advanced maternal age, typically defined as being 35 years or older at the time of delivery, is a significant risk factor. Older mothers are more prone to complications such as gestational diabetes, hypertension, and chromosomal abnormalities in the fetus.
Medical Conditions: Pre-existing medical conditions such as diabetes, hypertension, thyroid disorders, autoimmune diseases, and heart conditions can increase the risk of complications during pregnancy. These conditions require careful management and monitoring by a skilled healthcare provider like Dr. Shubhra Singh.
Previous Pregnancy Complications: Women who have experienced complications in previous pregnancies, such as preterm birth, preeclampsia, gestational diabetes, or miscarriage, are at a higher risk of recurrence in subsequent pregnancies.
Multiple Gestation: Carrying twins, triplets, or higher-order multiples increases the complexity of the pregnancy. Multiple gestations are associated with a higher risk of preterm birth, low birth weight, and complications such as twin-to-twin transfusion syndrome.
Lifestyle Factors: Smoking, alcohol consumption, substance abuse, and inadequate nutrition can significantly impact pregnancy outcomes and increase the risk of complications for both the mother and the baby.
Obesity: Women with obesity are more likely to experience complications such as gestational diabetes, hypertension, preeclampsia, and cesarean delivery. Managing weight and adopting a healthy lifestyle before and during pregnancy is crucial for reducing risks.
Genetic Factors: Certain genetic factors, such as a family history of genetic disorders or chromosomal abnormalities, can increase the risk of genetic conditions in the baby and may require specialized genetic counseling and testing.
Placental Disorders: Conditions affecting the placenta, such as placenta previa, placental abruption, or placenta accreta, can lead to complications such as bleeding, preterm birth, and fetal growth restrictions.
Dr. Shubhra Singh emphasizes the importance of early prenatal care, personalized risk assessment, and close monitoring for women with high-risk pregnancies. By identifying and addressing these risk factors proactively, she aims to optimize outcomes for both mother and baby during this critical period.
0 notes
Text
Expert High-Risk Pregnancy Specialist in Thane - Ensuring Safe and Healthy Pregnancy: Dr. Arohi Tasgaonkar

A high-risk pregnancy specialist, like Dr. Arohi Tasgaonkar, High-Risk Pregnancy Specialist in Thane is a crucial resource for expectant mothers who face greater challenges during pregnancy. These specialists ensure the best possible care for both the mother and the baby, helping them navigate the increased risks associated with high-risk pregnancies.
Pre-Existing Factors for High-Risk Pregnancy:
Several pre-existing factors can contribute to a high-risk pregnancy, such as cardiovascular disease, hypertension, obesity, diabetes, sexually transmitted illnesses, autoimmune diseases, blood disorders, and maternal age. Dr. Arohi Tasgaonkar, a high-risk pregnancy specialist in Thane, is experienced in managing these conditions to ensure a safe and healthy pregnancy.
Pregnancy-Related Conditions:
Some pregnancy-related conditions, like preeclampsia, HELLP syndrome, multiples, gestational diabetes, placenta previa, placental abruption, and placenta accreta, can also lead to high-risk pregnancies. Dr. Arohi Tasgaonkar, a high-risk pregnancy specialist, is skilled in identifying and managing these conditions to minimize risks for both the mother and the baby.
When to Consult a High-Risk Pregnancy Specialist:
If you experience symptoms like dizziness, chills and fever, swelling in multiple regions, changes in fetal movement, vaginal bleeding, watery discharge, blurry eyesight, severe headache, constant cramping, discomfort in the lower abdomen, urinary discomfort, vomiting, or nausea, it's essential to consult a high-risk pregnancy specialist like Dr. Arohi Tasgaonkar.
High-Risk Pregnancy Tests:
Dr. Arohi Tasgaonkar may perform special ultrasounds, cervical length ultrasounds, prenatal cell-free DNA analyses, and genetic testing to monitor and manage high-risk pregnancies. These tests help identify potential issues and ensure the best possible care for both the mother and the baby.
Prevention Factors:
Preventing high-risk pregnancies involves scheduling preconception appointments, avoiding harmful substances, making frequent OB/GYN appointments, and following healthy lifestyles. Dr. Arohi Tasgaonkar, a high-risk pregnancy specialist, can provide guidance and support to help expectant mothers reduce the risk of complications.
Treatment for High-Risk Pregnancy:
Dr. Arohi Tasgaonkar may recommend taking folic acid, receiving proper immunizations, following a regular physical activity chart, maintaining a healthy diet and weight, and avoiding harmful habits like drugs, drinking, and smoking. Regular appointments with a high-risk pregnancy specialist like Dr. Arohi Tasgaonkar are crucial for managing high-risk pregnancies and ensuring the best possible outcomes for both the mother and the baby.
Dr. Arohi Tasgaonkar, a High-Risk Pregnancy Specialist in Thane, is dedicated to providing expert care and support for expectant mothers facing high-risk pregnancies. With her guidance and expertise, mothers can navigate the challenges of high-risk pregnancies and ensure the best possible outcomes for both themselves and their babies.
Consult Dr. Arohi Tasgaonkar, High-Risk Pregnancy Specialist in Thane at Complete Women’s Care Clinic near Panch Pakhdi in Thane West or Contact us on +91 98330 74977.
#gynecologist in ghodbunder road thane#dr. arohi tasgaonkar#complete women’s care#gynecologist in manpada#gynecologist in thane#gynaecologist in hiranandani estate thane#gynecologist in ghodbunder road thane.#gynaecologist in bethany hospital thane.#gynecologist in waghbil#gynecologist in kasarvadavali
0 notes
Text
Spatial proteomics and transcriptomics of placenta accreta spectrum
In severe Placenta Accreta Spectrum (PAS), trophoblasts gain deep access in the myometrium (placenta increta). This study investigated alterations at the fetal-maternal interface in PAS cases using a systems biology approach consisting of immunohistochemistry, spatial transcriptomics and proteomics. We identified spatial variation in the distribution of CD4+, CD3+ and CD8+ T cells at the maternal interface in placenta increta cases. Spatial transcriptomics identified transcription factors involved in promotion of trophoblast invasion such as AP1 subunits ATF3 and JUN, and NFKB were upregulated in regions with deep myometrial invasion. Pathway analysis of differentially expressed genes demonstrated that degradation of extracellular matrix (ECM) and class 1 MHC protein were increased in increta regions, suggesting local tissue injury and immune suppression. Spatial proteomics demonstrated that increta regions were characterised by excessive trophoblastic proliferation in an immunosuppressive environment. Expression of inhibitors of apoptosis such as BCL2 and fibronectin were increased, while CTLA4 was decreased and increased expression of PDL1, PDL2 and CD14 macrophages. Additionally, CD44, which is a ligand of fibronectin that promotes trophoblast invasion and cell adhesion was also increased in increta regions. We subsequently examined ligand receptor interactions enriched in increta regions, with interactions with ITGB1, including with fibronectin and ADAMS, emerging as central in increta. These ITGB1 ligand interactions are involved in activation of epithelial mesenchymal transition and remodelling of ECM suggesting a more invasive trophoblast phenotype. In PAS, we suggest this is driven by fibronectin via AP1 signalling, likely as a secondary response to myometrial scarring. http://dlvr.it/T4dJDr
0 notes
Text
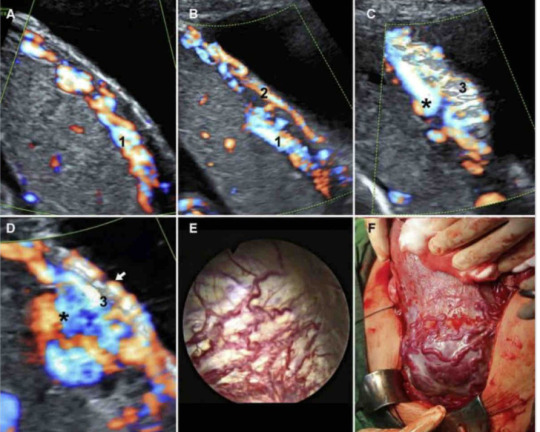
El "signo del riel": un hallazgo ecográfico en el espectro de la placenta accreta que indica una invasión vellositaria profunda y resultados adversos
Angiogénesis incremental del espectro de placenta accreta y el signo del riel
A-B, Ecografía Doppler color para una paciente con placenta previa creta. R. En esta paciente, solo existía hipervascularización subplacentaria (indicada con "1") a las 30 semanas de gestación. B. La hipervascularización uterovesical (indicada con "2") apareció solo después de las 33 semanas de gestación; C-D: Interrogatorio Doppler color en una paciente con placenta previa percreta e invasión vesical a las 34 semanas de gestación. C, Numerosos vasos recién formados en forma de coral (indicados con "3") se extienden perpendicularmente desde la placenta hasta la mucosa de la vejiga (los llamados vasos puente). D, La hipervascularización subplacentaria y uterovesical se fusionaron (indicado con un asterisco) e incluso progresaron a un aneurisma (Video 2). La hipervascularización subplacentaria o uterovesical paralela y la neovascularización de la mucosa vesical (indicada por una flecha corta), junto con los vasos puente interconectados (indicados por "3"), constituyen el "signo de riel" en (D). (E) y (F) fueron las imágenes correspondientes de la cistoscopia y los hallazgos quirúrgicos de los pacientes en (C) y (D).
http://ow.ly/kwQQ50MXmOi
0 notes
Last Seen Blogs

bluefairy-speaks
i will STOP mortimer

longarm7676
Untitled

--antjee--
~Antje~

kajakinfo
Kajakinfo

marifer-1-blog
SEMPITERNA bohemia