#SSRI's
Text
Long overdue and sorely needed, research into chronic fatigue syndrome has picked up speed since the pandemic illuminated the lasting and debilitating effects of long COVID.
The possible causes of chronic fatigue syndrome, otherwise known as myalgic encephalomyelitis (ME) or ME/CFS, remain elusive despite this new research effort, although they are slowly coming into focus. Past viral infections triggering an overactive immune system and malfunctioning mitochondria depleting cells of energy are possible explanations for how chronic fatigue syndrome develops.
Now a new study based on mice suggests that some drugs used to treat depression, which commonly accompanies ME/CFS, could also ignite the condition.
Continue Reading.
#Science#Immunology#Neurology#Health#Medicine#Antidepressants#Selective Serotonin Ruptake Inhibitors#SSRI's#Long Covid#Myalgic Encephalomyelitis#ME#ME/CFS#Chronic Fatigue Syndrome#CFS
87 notes
·
View notes
Text
if u take zoloft and/or spironolactone be careful in the hot months u will dehydrate and be prone to overheating. drink. Water
36K notes
·
View notes
Text
Doctor prescribing antidepressants: so this medication can cause side effects such as memory loss, seizures, eating disorders, stomach issues, rashes, fatigue, and could actually make you want to kill yourself even more. This is perfect for you
Doctor prescribing pain meds: Are you sure you don't want to try diet and exercise first? These pills are so bad for you. Yeah technically the list of side effects for this pain medication is a lot shorter than it is for your other medications, but the thing is, they might make you TOO happy. And we hate addicts. I just think destroying your stomach lining and liver with 2000mg acetaminophen and 1600mg ibuprofen per day would be a lot safer, because you definitely don't want "happiness" as a side effect of medication. Not being in pain and being happy is just too addictive and addiction is bad.
#.bdo#my pain medication does help with my focus and my mood a lot too#i mean yeah I'm happier when I'm not in pain lol#my pain medication keeps me from wanting to die unlike the SSRIs they gave me that made me damn near kill myself
7K notes
·
View notes
Text
TIL that you can assign an AO3 next of kin to control your account in case of your death???
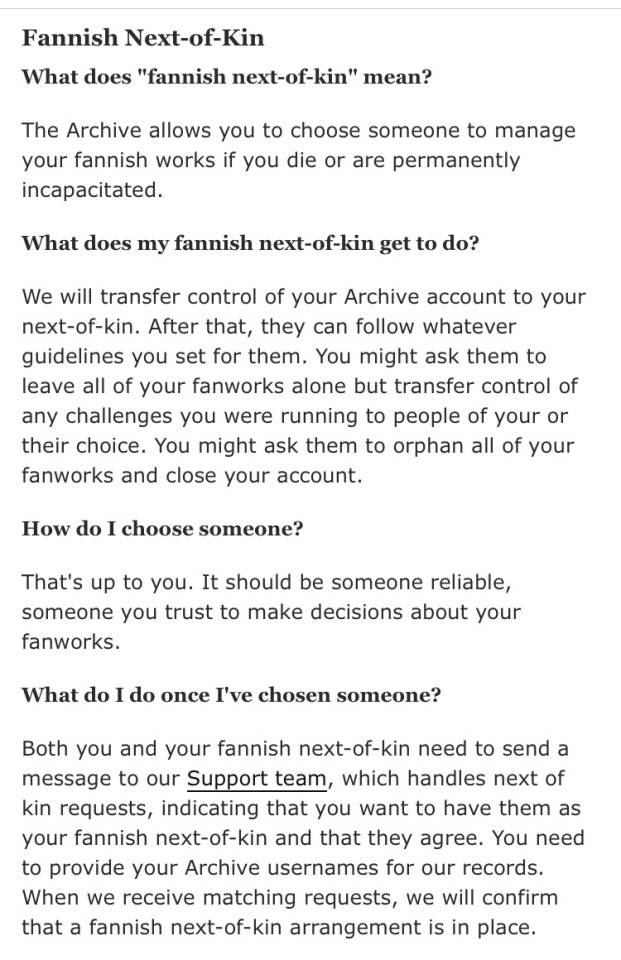
#ao3#this is actually really neat#I had a will at one point that included passwords and usernames specifically for my sister so she could manage certain social media#including my fanfic accounts#if anything happened to me#I need to update it it's been like...idk a decade#who makes a will when they're sixteen you might ask#ppl who want to be dead I will answer very seriously while shaking my bottle of SSRI like a baby rattle
3K notes
·
View notes
Text
stevie my beloved, you’re so cringefail i’m obsessed with you (affectionate) | steve harrington incorrect quotes/textposts pt. ??




#put him in therapy#and on an ssri#asap#he is bisexuality incarnate#steve harrington incorrect quotes#steve harrington textposts#stranger things incorrect quotes#steddie#steve harrington#fruity four#stranger things#steve harrington headcanon#gay steve harrington#bisexual steve harrington#steve x eddie#eddie x steve#stranger things steve#steddie brainrot#steve harrington my beloved#joe keery
4K notes
·
View notes
Text
i hate this one specific type of anxiety i experience where i just feel like i did something wrong. Like almost as if i did something really bad and im waiting for the consequences. and it takes me out of my headspace and im just sitting here thinking...what did i do? what am i not remembering?
#i know this is common#but my anxiety manifests in a lot of ways and is usually very physical#versus the intrusive thoughts#as im tying this i remember i stopped taking my SSRI#and that probably explains why im feeling this way and havent otherwise the past year or so :')
2K notes
·
View notes
Text


teenage superheroes and father/son relationships that are sooo so normal i promise
#invincible#mark grayson#nolan grayson#omni man#art tingz#started watching it last weekend w my brother and just finished s1!! the brains sure are worming#‘you dad i’d still have you’ is kind of fucking with my brain chemistry. i don’t think we can ssri ourselves out of this one gang#blood tw#violence tw
401 notes
·
View notes
Text
It is interesting how much math comes into even the most basic of like. Making things. Making almost anything. And often not numbers necessarily but proportions and geometry. I think all the time about how castles were built with geometry at the heart of it. And I use the same kind of proportional math to make socks fit. And none of my pieces are ever knit with a prime number of stitches--because you use factors to make neat colorwork and ribbing and different stitches. Idk ! I remember constantly thinking 'how the hell is THIS gonna come in useful ?' But it always does. Math is at the heart of everything, and knowing how to apply it is a tool of critical importance to Thinking Up A Shape And Making It.
#it turns out it is not covid vaccine making me highly fucked up but rather this new med which is fun#um#one of thise 'high but wow. in such a bad way' kinda experience atm#almost fell down the stairs#tripped while just standing#and its like. ok so the thing is i go to pain management to manage my pain right ? makes sense#and then all they have to offer is shit that fucks me up more. the muscle relaxant that seems to have permanently#loosened all my joints so they are WAY WORSE NOW#stupid ssris that make me fall constantly and fuck with my brain#i literally just need a painkiller that works. that is all. we know what was effective from surgery#but they of course will never prescribe opiods. oh the horror. imagine.#i could scream#anyway. uh thinking about the interconnectedness of math in all things is much more fun than screaming#knitting
281 notes
·
View notes
Text
the medical field will always be an institution of violence as long as your doctor is able to cancel your prescription unilaterally and as long as pharmacists can refuse to fill it unilaterally.
#this is about estrogen#but it applies birth control. SSRIs. antipsychotics. pain medication. insulin. your doctor can simply tacitly sign your death warrant#by simply not signing your prescription papers.
187 notes
·
View notes
Text


#covid#covid19#health#healthcare#gastrointestinal#GI tract#serotonin#ssri#coronavirus#fatigue#memory loss#gastrointestinal tract#long covid#thank u person who rb'd this that gave me the idea to add that tag#honestly really obvious choice in retrospect but oh well
249 notes
·
View notes
Text

to be loved is to be changed. sorry.
#serial experiments lain#lain iwakura#lain ps1#if you understand this post lets all take ssris together
638 notes
·
View notes
Text
Wandsworth Roundabout underpass (NW exit), SW18

SSRIs can't cure poverty
239 notes
·
View notes
Text
so are we going to talk about how SSRIs, even taken for short periods of time, cause long term sexual dysfunction that can, and for many people does, persist for decades after they stop taking the medication? were we ever going to talk about that? were any of my doctors ever going to warn me that taking this medication could damage my sex life permanently? are we going to talk about this in the context of the frankly alarming number of young people who are put on these medications as teenagers? or the sudden sharp rise in people id'ing as asexual? no?
#the hawk speaks#literally thought i was fucking broken turns out i can trace my loss of sex drive PRECISELY to when i started taking SSRIs#and i haven't taken any in almost 7 years#but guess what! problem remains!#LOVE THAT FOR ME#ssris
108 notes
·
View notes
Note
hi i just saw some of ur posts on anti-psychiatry and then kept reading more on ur blog about what it is. for the most part i agree with what you've said about how capitalism uses psychiatry to designate people who are bad/abnormal and how it aligns itself w/ misogyny, racism, and so on. with that said i think i have some similar concerns/questions as another asker about what this means for those who do/would suffer even in a non-capitalist society, even if we didn't ascribe a specific label to X symptoms. if we are opposed to psychiatry, what are the options for people today who are suffering and want help? are you opposed to psychopharmaceuticals and therapy? i dont mean to ask this in a confrontational/accusatory way, i'm just new to this and genuinely curious
There are a few different parts to your question & so there are a few different angles to approach it from—
are you opposed to psychopharmaceuticals and therapy?
If this means "are anti-psych writers and activists opposed to individuals seeking treatment that they personally find helpful," then, no—a couple posts in my psychiatry tag do clarify this.
If it means "are there anti-psych critiques of psychopharmaceuticals and therapy," then, yes. Keep in mind that I'm not a neurobiologist or otherwise an expert on medications marketed as treatments for mental illnesses, but:
The evidence for the effectiveness of SSRIs in particular is sort of non-existent—even many psychiatrists who promote the biomedical model of mental illness doubt their efficacy, and refer to the "chemical imbalance" theory that enforces their usage as "an outmoded way of thinking" or "a kind of urban legend—never a theory seriously propounded by well-informed psychiatrists." But promoting SSRIs (and corresponding "serotonin deficiency" theory of depression, despite the fact that no solid evidence links depression to low serotonin) is very profitable for pharmaceutical companies. Despite the fact that direct-to-consumer advertisements are nominally regulated in the U.S., the FDA doesn't challenge these claims.
Other psychotropic drugs, such as "antipsychotics" or "antianxiety" medication, shouldn't really be called e.g. "antipsychotics" as if they specifically targeted the biological source of psychosis. No biological cause of any specific psychiatric diagnosis has been found (p. 851, section 5.1). In fact, rather than "act[ing] against neurochemical substrates of disorders or symptoms," these medications "produc[e] altered, drug induced states"—but despite the fact that they "produce global alterations in brain functioning," they are marketed as if they had "specific efficacy in reducing psychotic symptoms." Reactions to these medications that don't have to do with psychosis or anxiety (blunted affect, akathisia) are dismissed as "side effects," as though they don't arise from the same global alteration in brain function that produces the "desirable" antianxiety/antipsychotic effect. This doesn't mean "psychiatric medication turns you into a zombie so you shouldn't take it"—it means that these medications should be marketed honestly, as things that alter brain function as a whole, rather than marketed as if they target specific symptoms in a way that they cannot do, in accordance with a biomedical model of mental illness the accuracy of which has never been substantiated.
Psychiatrised people also point out that meds are used as a tool for furthering and maintaining psychiatrists' control: meds that patients are hesitant about or do not want are pushed on them, while patients who desire medication are "drug-seeking" or trying to take on the role of clinician or something and will routinely be denied care. Psychiatrised people who refuse medications are "noncompliant" and prone to psychiatric incarceration, re-incarceration, or continued/lengthened incarceration.
As for therapy: there are critiques of certain therapies (e.g. CBT, DBT) as unhelpful, status-quo-enforcing, forcing compliance, retraumatising &c. There are also critiques of therapy as representing a capitalist outsourcing of emotional closeness and emotional work away from community systems that people largely don't have in place; therapy as existing within a psychiatric system that constrains how therapists, however well-intentioned, are able to behave (e.g. mandatory reporting laws); psychotherapy forced on psychiatrised people as a matter of state control; therapists as being in a dangerous amount of power over psychiatrised people and being hailed as neutral despite the fact that their emotions and politics can and do get in the way of them being helpful. The wealth divide in terms of access to therapy is also commonly talked about; insurance (in the U.S.) or the NHS (in England) may only pay for pre-formulated group workbook types of therapy such as DBT, while more long-form, free-form, relationship-focused talk therapy may only be accessible to those who can pay 100-something an hour for it.
None of these critiques make it unethical or something for someone to get treatment that they find helpful. It's also worth noting that some of these critiques may be coming from "anti-psych" people who criticise the sources of psychiatric power, and some of them may come from people who think of themselves as advocating for reform of some of the most egregious effects of psychiatric power.
if we are opposed to psychiatry, what are the options for people today who are suffering and want help?
This looks like a few different things at a few different levels. At its most narrow and individual, it involves opting out of and resisting calls for psychiatrisation and involuntary institutionalisation of individuals—not calling the cops on people who are acting strange in public, breaking mandatory reporting laws and guidelines where we think them likely to cause harm. It involves sharing information—information about antipsychiatry critiques of psychiatric institutions, advice about how to manage therapists' and psychiatrists' egos, advice about which psychiatrists to avoid—so that people do not blame themselves if they find their encounters with psychiatry unhelpful or traumatising.
At the most broad, it's the same question as the question of how to build dual power and resist the power of capitalism writ large—building communal structures that present meaningful alternatives to psychiatry as an institution. I think there's much to be learned here from prison abolitionists and from popular movements that seek to protect people from deportation. You might also look into R. D. Laing's Kingsley Hall experiment.
what does this mean for those who would suffer even in a non-capitalist society, even if we didn't ascribe a specific label to X symptoms?
It means that people need access to honest, reliable information about what psychotropic medications do, and the right to chuse whether or not to take these medications without the threat of a psychiatrist pulling a lever that immediately restricts or removes their autonomy. It means that people need to be connected to each other in communities with planned, free resources that ensure that everyone, including severely disabled people whom no one particularly likes as individuals, has access to basic resources. It means that people need to be free to make their own choices regarding their minds and their health, even if other people may view those decisions as disastrous. There is simply no defensible way to revoke people's basic autonomy on the basis of "mental illness" (here I'm not talking about e.g. prison abolitionist rehabilitative justice types of things, which must restrict autonomy to be effective).
Also, I've mostly left the idea of who this would actually be untouched, since my central argument ("psychiatry as it currently exists is part of the biomedical arm of capitalism and the state, and the epistemologies it produces and employs and the power it exerts are thus in the service of capitalism and the state") doesn't really rest on delineating who would and wouldn't suffer from whatever mental differences they have regardless of what society they're in. But it's worth mentioning that the category of "people who are going to suffer (to whatever degree) no matter what" may be narrower than some would think—psychosis, for instance, is sometimes experienced very differently by people in societies that don't stigmatise it. I see people objecting to (their interpretations of) antipsych arguments with things along the lines of "well maybe depression and anxiety are caused by capitalism, but I'm schizophrenic so this doesn't apply to me"—as though hallucinations are perforce more physically "real," more "biological," more "extra-cultural" in nature than something like depression. But the point is that positing a specific neurobiological etiology for any psychiatric diagnosis is unsubstantiated, and that capitalist society affects how every "mental illness" is read and experienced (though no one is arguing that e.g. hallucinations wouldn't always exist in some form).
#psychiatry#long post /#mental illness#antipsych#antipsychiatry#Anonymous#questions#psychotropic drugs#ssris
717 notes
·
View notes
Text
nie poczujesz straty, jeśli nie poczujesz przywiązania.
#cytat#cytaty#cytat po polsku#ludzie#życie#miłość#emocje#po polsku#cytaty po polsku#poezja#strata#problemy w związku#związek#red flags#przyjaźń#rodzina#leki#ssri
408 notes
·
View notes
Text

dante have no object permanence
#dante needs ssris#the divine comedy would be three tercets if dante had prozac#dante alighieri#dante's divine comedy#dante's inferno#dante#paradiso#purgatorio#ancient rome#greek mythology#roman mythology#beatrice x dante
139 notes
·
View notes
Last Seen Blogs

horzagobuchul
Just Horza

butterflywellnessprogram-blog
Butterfly Wellness Program 2017

immahashley
Untitled

footballnew
Untitled

moopeymywife
I love Moopey