#phallo education blog
Note
do you have any advice abt how to explain scars from phallo while staying stealth? I was going to say I had underdeveloped genitalia and needed surgery to fix it (not technically a lie since all fetuses start female and become male or don't) but I dont wanna coopt the experiences of intersex people or anything
Hello,
I tell people I have a scar from a bad burn when I was younger. I have found the remaining scar looks only like a normal skin graft like a burn would. Most people will assume you had some accident on your arm (passers by), people who stop to ask you, honestly, they don't need an answer. You don't have to say anything to anyone. You can say "I don't like to talk about what happened its hard" or a "long story to talk about".
I flat out told everyone I had a bad burn and it needed to be grafted. Usually if anyone says anything they already have a story they want to tell you and don't really care about yours (in my experience). I usually spend way longer listening to other people.
I know people who find good tattoo artists to cover the scar too (but work with the artist to make sure the design will hide it).
I know it's hard, but outside the community (at least in my experience) no one has a clue what phalloplasty even is, let alone that my arm is a scar from that. Therefore, no one will really know what it is, I learned not to worry.
You can cover it up? I used to wear huge leather cuffs when I first was "showing" my scar. This can get kind of uncomfortable just as an FYI, especially when it's hot.
If you want, you can look up something like common injuries to the forearm that require skin grafts, I'm sure google can give you some ideas.
If you pick a story, stick to it, though. So keep it simple to remember. Like I said, people treat you to opening this conversation as show and tell for themselves. Comparing scars and telling you their stories in detail. Your story kind of becomes irrelevant at that point in my humble opinion.
If you want you can even say they took that as the graft for somewhere else? (This was just a random thought I just came up with)
If you want to say something along the lines of being towards the truth, you could say you had an injury to your phallis you were (re)born with. Or [I haven't looked into this in eons mind you] you can say you were born with a microphallis/penis and you wanted to get it enlarged. That's the best I could come with along your lines (being truthful-ish), and trying to not get lumped into the intersex box.
I hope I helped anon, I'm sorry about it taking so long. I spent all day thinking about the best ways and as many ways as I could to help.
Stay golden ✌️ 💙 💜
#anon ask#anon questions#transgender#trans ftm#transman#phalloplasty#ftm transition#ask me things#ftm phalloplasty#phalloplasty blog#phalloplasty education blog#phallo education blog#phallo education
10 notes
·
View notes
Text
real meaningful problems to postop transmascs/transmascs seeking bottom surgery
bottom surgery too much money call that shit expensive
lack of education about bottom surgery to people who don't actively look for it so allies and enemies alike dont know shit about bottom surgery and people who would benefit from it dont even know what their options are
medical gatekeeping forcing people to jump through absurd hoops only to have coverage denied for anesthesia
good fucking luck finding a urologist who has any experience with post-op patients, idiot
difficult to find clinics outside of the USA and Thailand bc while they do exist most resources assume you either live in the US or have the resources to travel to Thailand
postop/seeking op people having the topic treated like its a very serious tragic discussion so we're not included in any conversations unless people are sharing articles about gender clinics being bombed or reminding trans people that bottom surgery sucks
postop people being seen as incapable of sex or having lost their transgender sex appeal so people feel pressured not to get bottom surgery lest they lose their boypussy which theyre acutely aware is seen by many people as the only reason you would fuck a transmasc person
again bottom surgery being seen as this worldending tragedy only the most selfhating transgendereds resort to is like The biggest problem for postop people and contributes to the isolation/alienation a lot of postop people feel. making jokes about bottom surgery and bringing it up in casual conversation is Good Actually and i wish more nonop people did it so i didnt feel like i only exist when its time for people to talk about how glad they are that they arent like me
transmisogyny in the transmasc community leading people to lash out at transfems for having "too much visibility" which prevents us from working together to strike back against the real enemy, healthcare providers forcing me to get updated mental health letters to prove im sound of mind for seeking phallo stage 2 as if im going to regret Just the tip
not real meaningful problems
random trans women making posts on their personal blogs about being trans women including posts about vaginoplasty
people making jokes about bottom surgery
postop people identifying with a variety of labels or having their identity change throughout the course of getting bottom surgery, yeah even people who end up not iding as trans anymore. not my business and not yours either
non-transmasc people seeking phallo/metoidio. aside from the extremely legitimate reasons intersex people who had surgeries performed on them without their consent/ppl with natal penises who have been in a Penis Accident would get it, or nonbinary people seeking it for the same reasons i am, who am i to judge if a cis woman wants to piss standing up. again why would i waste any energy on this when insurance companies exist
#c.paradisi#was origuinally gonna be about last rb but ended up being mostly about other things#can you tell ive been trying to get everything set up for phalloplasty stage 2. can you feel my agony#why the fuck do i need a letter from someone with a phd to confirm i do in fact want my urethral stricture repaired
4 notes
·
View notes
Note
Re: “It'll be bigger in the end than what it is to begin with, though, just not a huge amount like with phallo.”
Actually, only some people report gaining size with metoidioplasty; other people experience retraction and find that they actually lost length after healing. (And that’s pretty common!)
If you haven’t researched this and aren’t familiar with what I’m talking about, you can see an example of a minor case of post-op retraction in the photos on this blog.
Please stop “educating” people about surgeries that you haven’t had!
It’s misleading to state “It'll be bigger in the end than what it is to begin with,” as a blanket universal statement because that simply isn’t true for everyone.
"Only some" is misleading: clitoral release is a major aspect of most/all forms of metoidioplasty, and it's what most people undergo the surgery for. The majority of the time, folks who start with a decent sized clitoris and undergo meta with clitoral release will end with a larger penis than they started with (and the satisfaction rate for meta is fairly high).
I was not aware that retraction was a risk, though, and I do appreciate the information!
Please don't scaremonger, or talk down to me about this. I include a lot of "if I remember correctly"s and "from what I know"s as-is because I am generally speaking from a place of research, but sometimes it's personal research that isn't recent- and I prefer people do their own research and reach out to folks who know more on the subject directly, even when I do research things thoroughly for a specific post. A disclaimer I literally included in the post you're referring to.
I do my best to give folks the information I do have, and encourage people to do their own research & understand that I'm not a perfect source. I'm gonna be wrong sometimes; I try to own up and update when that happens. That's all anyone can do.
29 notes
·
View notes
Text
So you just had surgery...
It is best not to apply anything (creams, gels, etc.) to your scars until at least 3-4 weeks or when your surgeon says it's okay. It's always a good question to ask the doctor. [Source 1]
Massaging the scar using gentle pressure allows the wound to heal in a way that the restored skin is soft and has the normal range of movement and elasticity. [Source 1]
As the scar is healing it is important to protect it from sunlight to prevent it becoming dark and prominent. It is a good idea to keep it covered for a year or more. Alternatively use a suntan lotion or cream or sun block of SPF 35 or greater if your back is going to be exposed to the sun. [Source 1]
An itchy, hot painful scar can be a sign of infection which will need medical attention, from a doctor or a prescribing nurse. If the scar is just itchy, taking antihistamine tablets can help to stop the itching. This in turn stops the itch scratch cycle, so helping to prevent infection. [Source 1]
The best treatment for an itchy or dry scar is to wash the skin with a moisturising shower gel or a bath additive. This will prevent the skin from becoming dry. Then, apply and massage a fragrance free moisturiser cream or ointment into clean dry skin. You will need to do this on a daily basis for several months and maybe even longer. Silicone based gels and sheets can be particularly effective for stubborn deep scars. [Source 1]
Your surgeon(s) may advise you to use one or more of the following over-the-counter (a.k.a OTC) treatments after 2 to 3 weeks: silicone strips (also known as kinesiology tape), tapesilicone gel, recommended (and approved by your surgeon) certain brands or types of products your surgeon may advise against using even though it may be on a list online. [Source 2]
It takes about 12 months on average for a wound/scar to completely heal [Source 2]
This is for all surgeries, but more specifically, top surgery. Not many people like having big scars after any surgery. With that being said, I feel like this is appropriate for any procedure that may create scarring from top to bottom.
Source 1 link: https://www.axahealth.co.uk/health-information/skin/cream-for-scar-post-surgery/#:~:text=scar%20becoming%20darker.-,Silicone%20gel,to%20clear%20the%20scar%20tissue.
Source 2 link:
https://www.healthline.com/health/top-surgery-scar#short-answer
#dealing with scarring after surgery#ftm top surgery#ftm bottom surgeries#trans ftm#transgender#transman#ftm phalloplasty#phalloplasty blog#phallo education blog#phalloplasty education blog#ftm gender affirming surgery blog#ftm transition#phalloplasty#lgbtq
13 notes
·
View notes
Text
Many patients mistakenly believe that the longer the operation, the better the healing results, and that short surgery is a sign that the surgeon is in a hurry or is not meticulous.
These myths can be a major source of anxiety for patients. However, the opposite is true: the longer the surgery time, the more the healing time and the risks associated with the intervention increase.
While it is true that operating time is an important indicator of risk factors and possible complications, the type of surgery and procedural complexity are also determining factors. Although often independent, these risk factors can sometimes be interrelated.
Infections and complications
The link between wound infection and operative time has been known for a long time. Every additional minute of surgery has a direct impact on the rate of wound infection.
As proof, a study on breast reconstruction with implants published in 2019 clearly demonstrated that the possibility of medical complications or wound infections increases when the surgery time goes beyond three hours. There would be a direct causal link between complications, preoperative health conditions, and longer operative time.
While the complication rates vary little for surgeries of less than 3 hours, the risks multiply by 1.6 times after 3 hours. Each successive operating time interval is accompanied by an associated growth in complications, with rates increasing 3-fold after 4.5 hours and almost 5-fold for a 6.8 hours procedure.
When surgery lasts longer than 6 hours, every additional hour increases the risk of cardiovascular, kidney and pulmonary complications. The same goes for the increased rate of infection. Surgeries lasting longer than 3 hours increase the risk of erythema and bruising, and often involve slower healing of the wounds.
Morbidity
The main issue regarding the risk of morbidity is the complexity of the procedure, not the duration of the operation. Indeed, according to a study published in 2014, complications can vary between two surgeries of more or less equal duration. For example, surgeries to the head or neck cause more complications than breast or limb surgeries, although the duration is similar, due to the complexity of these procedures. Delicate procedures on smaller surfaces requiring less manipulation cause less morbidity than reconstruction or dissections or excisions of body contouring procedures. On the other hand, studies indicate that operating times of more than three hours also increase the risk of morbidity. All these factors must be taken into account by the surgeon during the preoperative preparation.
The duration of the operation is therefore a key factor in the recovery of patients and in the severity of postoperative complications. It would be an indicator of complications, with a marked increase in risks if the surgery lasts more than three hours.
Surgeons are highly trained professionals. Although an experienced surgeon works quickly, other factors can contribute to the length of the operation, some of which may be beyond his control, such as excessive bleeding which can slow down the procedure. However, speed of execution does not necessarily guarantee better results, as operating time is not the only factor to consider in the event of complications.
So patients don’t have to worry if the surgery is shorter than expected. This does not indicate shoddy work. Longer surgery will not necessarily give better results. Surgery time is an important factor in recovery, but so too are the type of surgery and procedural complexity. Above all, be sure to ask questions before surgery so that you are fully aware of the risks.
Source
#healing after gender affirmation surgeries#healing after surgery#myths about gender affirming surgery#transgender#trans ftm#transman#phalloplasty#phalloplasty education blog#phallo education blog#gender affirming surgery blog#grs montreal#trans man#trangender#ftm transition#ask me things#phalloplasty blog#lgbtq#ftm phalloplasty#infection#morbidity (death of tissue)
5 notes
·
View notes
Text
I'm fighting to get the images to show guys... I don't know if it's going to happen, and I do not have enough money to buy a website...
If anyone has ideas, I'm open...
#tumblr staff shut down my images#transgender#transman#phalloplasty#trans ftm#ftm transition#ask me things#ftm phalloplasty#phalloplasty blog#educational purpose only#phalloplasty education#phallo education blog
3 notes
·
View notes
Note
I'm the anon that asked about the ejaculation thing. Feel free to post them here. Thanks so much for all that you do bro
Okay so my questions are:
How long ago was the first surgery(just phallo alone) ?
How long ago were you finished?
Did you have your urethra lengthened ?
If you feel comfortable the surgeon and/or clinics name (I will dive into research with this info)
I just wanted to say, my partner and I were talking about me ejaculating, and apparently I didn't start until I was finished for about two years or so. I am just not sure if your friend is just still healing, basically I'm asking how new everything is, because everything takes awhile to happen.
I do still really suggest if the problems persist after my (non-professional) advice, you talk to all doctors involved, your family doctor, your surgeron(s), the clinic, and maybe perhaps if they wouldn't mind sending me the clinic they went to, I can maybe do some investigating as well. But I like to give people their privacy and always ask before I just assume it's okay.
So if it's okay with you anon/anon's friend, if you could provide me with question four? I will have no idea who you are, that is not my intent to find out. I like to do research on doctors. I am actually in the middle of researching the best doctors in certain areas. This could help me too, if you could be so kind.
Also tell your friend if they want to talk or you anon, I made an email for this blog [email protected]
Feel free to send an email if either of you need/want to talk, ask questions, etc.
Stay golden you two ✌️💙💜
Edit: and thank you and your friend who have started to look at this blog. I made it for people like you. No need to thank me
I am not going to lie, though the thanks does put a giant smile on my face! So thank you, Anon(s)!
#ask answersfromtheshadows#anon ask#transgender#trans ftm#transman#phalloplasty#ftm transition#ask me things#ftm phalloplasty#phalloplasty blog#lgbtq#phalloplasty education blog#phallo education#phallo education blog#educational blog#gender affirmation surgery#mtf transgender#trans man
2 notes
·
View notes
Text
Improved Blog Directory - Find what you need
BLOG RULES: PLEASE READ
Educational Article on the Phalloplasty Surgical Procedure -self written
How to choose clothing/shoe sizes during transition - clothing on smaller feet and frames
Formal Wear - how to dress formally during transition.
Need to speak to someone? Do you need help with your legal name change? Please click here. Translifeline.org
USA Safe States for Trans-People (Constantly Updated by the website Owner)
What to Update After Legal Name Change
Hormone Replacement Therapy (HRT) Testosterone - storage, travel, and injection advice
Facial Hair Information- Tips and Tricks on How to Shave (HRT)
Frequently Asked Questions about Phalloplasty - My [personal] Experiences
How can one ejaculate after phalloplasty procedure? -ask answered.
Common Phalloplasty Misconceptions- Article
Male Mannerisms- help to know male gestures, wording, and attitude- (ask)
Beginning testosterone, testosterone hormone therapy
Testosterone Experiences That Caught Me Off Guard - (Ask)
Safe Binding and Packing - Articles Purchase Sites Also
Staying Stealth During Surgeries, Explaing Scarring - advice (ask)
Top Surgery (both ftm & mtf), procedures, and approximate costs.
Can I have top surgery and be overweight?
Keyhole Top Surgery Procdure- Outline and what qualifies you as a potential candidate
Finding a Top Surgeron in North America
So You Just Had Surgery (Top)- Advice on the best way to heal after surgery/ minimize scarring.
Is more time on the operating table really better? Operating time and infection information.
Metoidioplasty FAQ
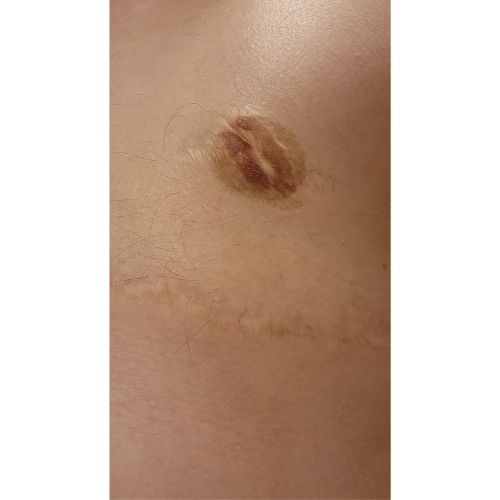
My arm and upper thigh after about a decade after phalloplasty.
My Personal Surgeon and Their Clinic
Interview with Dr. Chen about Bottom Surgery
Penile/ Phalloplasty Erectile Devices
Expectations- Personal Advice on Setting Expectations
Urethra lengthening Procedure Information- Self written article.
Importance of Uriologist
Phalloplasty Website - Includes Parents Guide
Urethra Lengthening Procedure
General Surgical Risks
Plus Sized Surgery Risks
List of Phalloplasty Surgerons in the USA
Vaginal-Perservering Phalloplasty Procedure
Graft SiteCare for Forearm -Free Flap Phalloplasty
What Happens if Erectile Device Breaks?
Image of My Phalloplasty (wearing underwear) Educational Purposes Only
Phalloplasty Procedure Outline by GRS Montreal - (Link to Webpage)
First Every Phalloplasty Procedure - Surgeon
Michael Dillon- Trans Pioneer (First phalloplasty patient)
How to Find Proper Sources of Information in a World of False Information/ Online Safety
Why certain terms can be hurtful. Please respect my/others views.
Tattooing over your forearm skin graft -ask
Testosterone and Hair Loss Information
If there are any other posts/ other topics I should add to this directory, please send me an ask. I will never post your username without your expressed consent in the ask.
#phallollasty education blog#transgender#trans ftm#transman#ftm transition#phalloplasty#ftm phalloplasty#phalloplasty blog#phallo education#blog directory#find what you need quickly#lgbtq#this took me a long time#ftm top surgery educational blog#ask me things#ftm trans education
264 notes
·
View notes
Text
***Educational Purposes Only***
Normal questions for phallo (my personal experience, and facts)
"Do you feel anything?" - yes, I feel everything from touch, stroking, temperature, pain, pressure, pleasure, gusts of cold air. They do disconnect and reconnect nerves, so it does take time (years) depending on how you heal to have complete sensation. But you always have sensation there even beforr you are fully healed. I found the Urethral Lengthening Procedure and the Implants (erectile device and prothetic testicle). It took probably 3 years after all of the procedures for me to have what is called "complete tactile function".
"How do you get erect?" - it's a pump, after they create the scrotum (they use the labia for this), you get your pump installed into your main hand side (ex. My pump is on the right testie), and the other testie is just an implant. I squeeze my pump (or my partner), and then saline water is pumped from the testicle into two tubes (one on each side on my penis). Creating a natural looking erection besides having to pump. It only takes about six pumps for me. Doesn't take much effort. I have a three part inflatable device.
"How do you "deflate"/ go down after an erection" -on the testie that is the pump, there is a small button above it, it is actually kind of a small box with a button on it. I hold the button for about 15 seconds and just let my erection naturally go down.
"How many surgeries does it take?" - well, I guess four in total. You have your hysterectomy (which included for me a complete oophorectomy as well, recent advancements in this procedure have made it so an oophorectomy is now optional), then your phalloplasty the building and attaching of the phallis and vaginectomy only at this part. The next surgery was to connect my urethral, called urethra lengthening. The last surgery was to install the penile pump and testicular implant.
"What are the chances it will fall off?" - less than 1% in the hands of a skilled surgeon. (My surgeon told me this information as the source) - note post operative care is the most important part of healing properly.
"Where did they take the skin?" - they took the skin for my phallis from my forearm and used a thin layer of the skin on my upper thigh to cover the tissue left exposed on my arm.
"Do you have any issues today?" - No issues, I've been finished for quite a bit now. I enjoy sex, it feels good. It looks good. I've never been clocked even naked in a locker room. I do dribble sometimes if I hurry while urinating, and I have to use a special technique to ensure 100% emptiness, but I can pee just fine. I found the installation of the pump helps me urinate easier than without.
"Can you ejaculate?" - Yup! I can, at least. I also have pre-ejaculate. I ejaculate almost everytime I orgasm. (With this said, the ability to ejaculate, amount of, and frequency of are all variable factors that can depend on person to person)
"Is the orgasm different?" -yes! It feels better to me. It could be comfort, but ejaculating does feel good when you orgasm. Ejaculating can vary from person to person. This ejacuate is not like cis men's, it is a clear fluid from the Skenes Glands.
"Did you have any major issues?" - not really, I did have to see a wound clinic for my implant surgery. I had wounds that needed care. I got a bladder infection with the catheter during the healing stage of urethral lengthening and had it removed after just over two weeks (it was supposed to be in for six weeks), as a reference though one of my urine bags broke and I had a plastic baggie to try to repair it until I could get a replacement (i had to wait hours), I also have a compromised immune system. For my arm, I wore my compression sleeve 100% of the time, and my arm healed extremely well and flat. You just need to listen to the rules and be sure not to break them.
"Do you have to do anything (e.g weekly)?" - sorta, I have to make sure I pump fully once a week.
"Any issues urinating?" - nope, takes some getting used to, though (standing). I find that I dribble, but it's only when I'm rushing when I shake. I still sit most of the time, it's even very common in cis men as an FYI. (I asked a large group of cismen)
"Does it look real?" -Yes, my wife said she never would have known I was trans until I told her. All penises look different. Even getting an erection looks natural.
"Did you have any corrective surgeries?" -No, I got pretty great results the first time. I do plan on going to closer, regular plastic surgeon to put in a larger implant as my left testicle (non-pumping side).
Have any of your own questions? Send me an ask, I'll be happy to answer!
Stay Golden Everyone ✌️💙💜
#pride month blog#trans ftm#transgender#transman#transman phalloplasty#phalloplasty#i love my phalloplasty penis#phallo#my experience with phallo#person#if i can help put info out there i would love that#phalloplasty education blog#phalloplasty experience blog#phallo education#phallo blog#/r phallo#ftm transition#ftm bottom surgery#ftm phalloplasty#phalloplasty blog#ask me things#lgbtq
154 notes
·
View notes
Text
Penile/ Phalloplasty Erectile Devices
There are two main types of penile implants:
Inflatable Devices
Semi-Rigid Rods Device
We will go over inflatable devices first. There are two mainly used types of inflatable penile implants used in phalloplasty, as well as cis men with health issues.
What are they?
Inflatable devices are the most common type of penile implant used, especially on phalloplasty procedures.
The two types are:
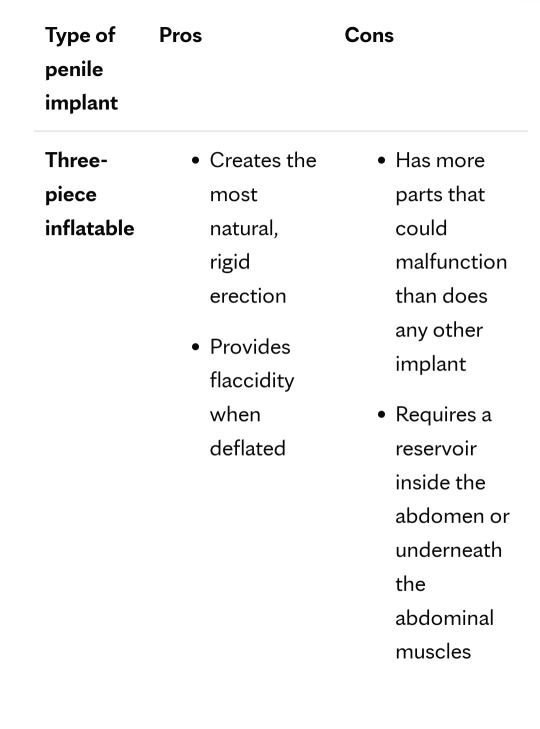
Three- Piece Penile Implant
Source
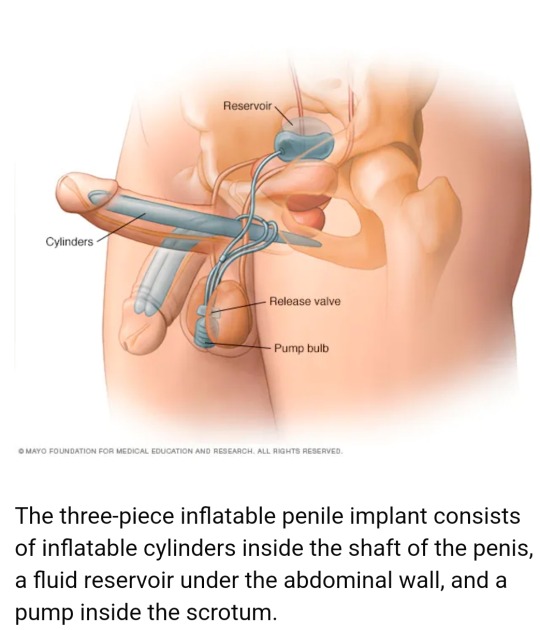
Three-piece inflatable implants use a fluid-filled reservoir implanted under the abdominal wall, a pump [in your main hand side] and a release valve placed inside the scrotum [and slightly located above the pumping mechanism], and two inflatable cylinders located on each side of the penis.
To achieve an erection, you pump the fluid, which is salt water (saline fluid), from the reservoir into the cylinders. Afterward, you release the valve inside the scrotum to drain the fluid back into the reservoir. Usually, this is done by holding a small button on the release valve.
In both devices, the reservoir is filled with salt water (saline water) the day of surgery and remains in the device.
This particular system [three-piece] is how I get an erection/ deflate my erection.
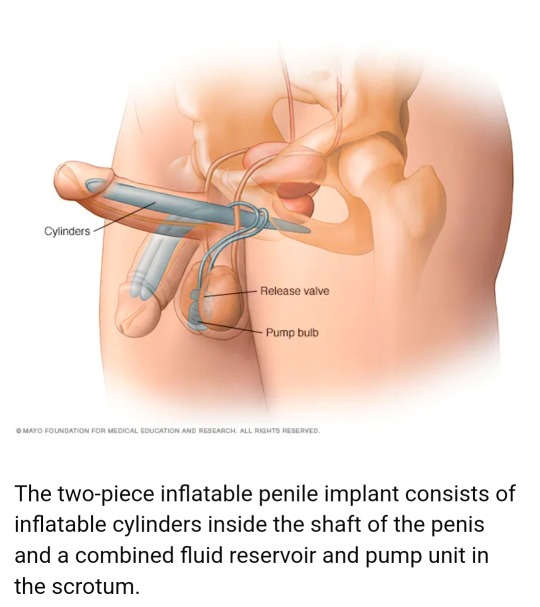
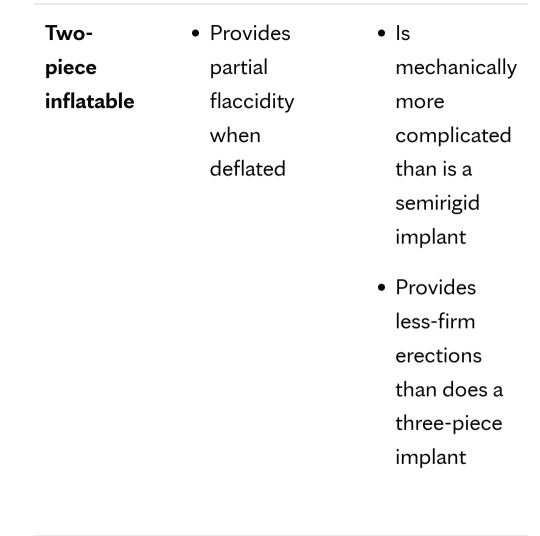
Two - Piece Penile Implant
Source
The two-piece model works similar to the three- piece, but the fluid reservoir is part of the pump implanted in the scrotum. This device is not the most effective at maintaining total flaccidity (it may sometimes look slightly erect). This device has more limitations on types and styles of penetration/sex. Be sure to ask if there are limitations with the device and its particular model that was implanted.
In both devices, the reservoir is filled with salt water (saline water) the day of surgery and remains in the device.
The last commonly used erectile device is called:
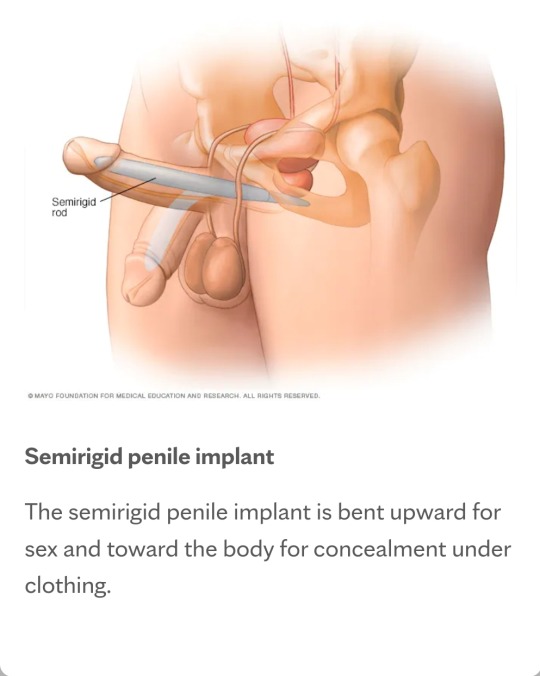
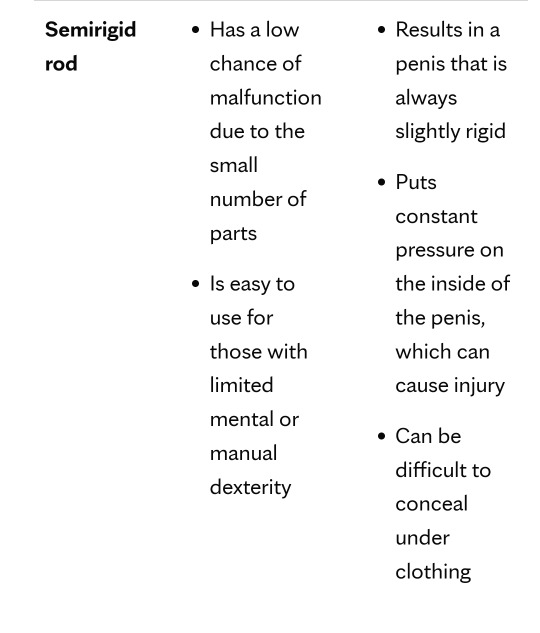
Semi-Rigid Rod Penile Implant
Source
Semirigid rod devices styles are always firm. The penis can be bent away from the body for sexual activity and toward the body for concealment. There is no inflating or deflating.
A "positionable penile implant" is a semirigid device with a central series of segments that are held together with a spring on each end. It can maintain upward and downward positions better than other semirigid rods can.
What is best for you? Comparison Images:
Source
Most clinics have their own style of procedure that involves a certain type of erectile device. You may or may not have a choice with certain clinics, so make sure you research clinics and make sure they fit with your chosen device and procedure.
This article was written about just implantation of these devices in general, the different devices, and their functions. If you are interested in sexual intercourse, especially penetration, consider where you want to penetrate.
For example, some men are not able to perform anal sex with the two-piece option, while some men are able. Always ask your doctor before leaving the clinic about the sexual acts you can/ cannot perform. You can seriously injure yourself if you try something your device is not capable of.
I hope you enjoyed the article and know a little bit more about the selection of erectile devices for phalloplasty. I hope this helps you make an informed decision.
Stay Golden Everyone ✌️ 💙 💜
Source used 1
Source used 2
Source used 3
#transgender#trans ftm#ftm transition#transman#phalloplasty#ftm phalloplasty#phalloplasty blog#lgbtq#phallo education#transman phalloplasty#ftm phalloplasty education blog#female to male affirmation surgery blog#female to male transition information#ftm bottom surgery education blog#ftm top surgery education blog#ask me things#erectile devices#educational post#types of erectile devices used in phalloplasty#ftm trans resources#phalloplasty education blog#ftm transgender resource blog#trangender#educational blog#erectile device education#ftm erectile device resource#ftm transgender resources#ftm bottom surgery resources
25 notes
·
View notes
Text
For those of you on hormones replacement treatment (HRT) Testosterone;
a shaving kit makes a great and natural way to store and travel (where legal) with your testosterone. Going to a friend's house? Bam, it's natural to have a shaving kit. Or I found emptying out the hard case of a set of old hair clippers. If you carry needles and you are stowing your needles, I recommend using a hard case of some sort. I've had the airline break my syringes/ needles before, and when you have to ask a pharmacy that doesn't know, they may be hesitant to give you any needles without knowing the medication you are on.
Do research on where you are going if leaving the country, make sure you have what you need (if you can) to be able to have legal possession in that country and any other country where you may stop or another potential area to explore.
Keep yourself safe, it's always good to keep a note from the doctor and your prescription history.
If you, for some reason do no longer have your testosterone, missing a dose or two will not cause any issues (I was told this by my family doctor).
Also, it's a good idea to perhaps take your vial and put it safely in a carry-on. They will not let you take your syringes (if they have needles attached, they will not let these on your carry-on).
It's good to have a hard case for long distance travels, otherwise a shaving bag works well. Find a more padded one if you can, and that closes securely.
I like to keep all my things together (Needles, testosterone, alcohol/alcohol wipes, and cotton balls/pads.) So that if you ever need to leave in a hurry you have to only go to one place and grab one thing.
I try to buy syringes with needles by the box. They cost me about $0.25 each and I get 100 in a box, all for $25.
It is also important to get a proper sharps disposal. You can usually ask the pharmacy and they will give you one. (In Canada I believe they are free).
About injection,
Unless instructed how to properly by a health care professional, I would not use your thigh for intermuscular injection. A great place, and the least painful I have found is in your gluteal muscles. It is important to rotate injection sites/sides. Give the muscles a break, especially if you need a dose weekly like I do.
Try to get air out before injection
Make sure you pull back the plunger to make sure you do not inject into a vein. If you pull the plunger and you see blood, do not inject. Find another location.
Do not use a needle more than once if possible (during a single injection, you can use attempt a few times), try to get it right the first poke, and it will hurt less.
The more a needle is used, the more it actually starts to spur at the tip, which means it's going to be harder to poke yourself, and it can be more painful
Do not share needles
Dispose of your needles properly by using a sharps container. Return it to the pharmacy when finished and they should give you a free exchange for a new one.
Do not throw needles out in the trash even with the cap on it can still be dangerous. I've personally seen (had) a needle peirce through the cap, have gotten stabbed.
Try to minimize air bubbles in the needle. But if you are scared of air bubbles. My cousin is a nurse practitioner, and she told me that it takes a lot more air than that empty syringe can hold to cause an embolism. But it is still important to minimize bubbles just to be easier on your body and help better absorption. So, a couple of tiny little bubbles are okay.
Make sure you are using a sterile area to place your things.
Make sure your hands are clean and sanitized.
Afterwards, press and slightly massage the injection site for at least 1 minute to help the testosterone absorb and to stop the bleeding.
The rule of thumb if you ever forget where to inject into your butox, upper and outer area of your gluteal muscle (so upper and outer buttcheeck).
Before you poke yourself, I find it helpful to press with your finger/alcohol pad and find a nice area, I usually do it as I apply the alcohol to sterilize the area. I find it helps me get it right the first time.
Any other questions? Let me know!
Do not inject yourself unless you have been properly taught how.
Do not fool around with your dose, more is NOT better
It may take a few years to fall into the safe/average hormone levels areas or what arrangement you have discussed with your prescribing physician.
Be careful! I am not a physican, always listen to the professional and be safe!
Stay Golden
✌️ 💙 💜
#transgender#trans ftm#ftm transition#transman#ask me things#phalloplasty#ftm phalloplasty#phalloplasty blog#lgbtq#phallo education#tw medication#tw needles#tw injections#injection advice for testosterone#adivce on injecting t
27 notes
·
View notes
Text
We hear about the surgeon of the first phalloplasty procedure, but we don't hear about the man under the knife Laurence Michael Dillon, or Michael Dillon (article)
Pink News Article about Michael
Commonly known as Michael Dillion, he was born in 1915 London, but grew up in Iceland.
After graduating university in 1938, he began to transition, and was prescribed hormone tablets (testosterone).
After a horrible experience working (being misgendered and mocked), he found a plastic surgeon who performed his top surgery and allowed legally change his name, with the note of the surgeon.
Some time after his transition, he became a follower of Buddhism and settled in a Buddhist colony without anyone knowing he was transgender.
And that's just a tiny snippet of his amazing, yet tragically short, life.
Be sure to check out the amazing articles I have found on him!
Sources: https://www.thepinknews.com/2023/03/31/laurence-michael-dillon-trans-man/
https://www.st-annes.ox.ac.uk/life-here/library/blog/michael-dillon/
#Michael Dillon#trans pioneer#transgender#trans ftm#first man to get phalloplasty#transman#ftm transition#ask me things#phalloplasty#ftm phalloplasty#phalloplasty blog#lgbtq#phallo education#ftm top surgery educational blog#ftm educational blog#ftm advice blog
33 notes
·
View notes
Text
Phalloplasty Procedure Full Outline Offical (Radical Free Flap Procedure)
What is phalloplasty/ phallo?
Phalloplasty - "includes several surgical procedures that aim to construct male genitalia that looks as natural as possible. The surgery is divided into several steps that may vary from patient to patient. Generally, they are the three following steps" (Source1) . We aren't going to count if the prerequisite of hysterectomy. Since my surgical procedure, they have removed the requisite of an oophorectomy, that procedure is now optional thanks to the always advancing technology.
The first step:
a surgery that consists of creating a penis from a skin flap from a specific area of your body (most common areas are forearm and lower back) of the body that you would chat about with the surgeon(s) and that specific skin will be grafted to the genital area.
The second step:
Here, surgeons construct the urethra that will llow urination. This is known as Urethra Lengthening (often referred to UL) (Urethra Lengthening Procedure Post)
The third step:
At this stage, you will receive testicular and erectile implants that will allow for penetrative sex. Note: this is not the only type of phalloplasty sugerical options.
The first surgical step consists of:
the creation of a penis or phallus from a skin flap and fatty tissue of the donorn site involving the removal of blood vessels (to create a blood supply) and nerves (this is where nerves are disconnected and reconnected, which can take some time to gain full tactile function or feeling. This skin will be grafted to the genital area where a penis would naturally sit on your body. The next part of the procedure is:
"the burial of the clitoris at the base of the phallus;
the creation of the penile urethra within the phallus;
the lengthening of the biological urethra;
the creation of the glans;
the creation of the scrotum;
the closing of the vaginal cavity; and
the removal of a layer of skin from the thigh to compensate for tissue loss
on the donor arm." - (Source1) Some of these things are not the same for every surgeon, be sure to ask about if your clitoris could be not buried for example, or different pumping systems, varying styles in surgerical procedures from clinic to clinic, even surgeon to surgeon.
The second step consists of the construction of the urethra:
This procedure connects the penile urethra so the part of the urethra inside the phallus itself to your biological urethra that was elongated in the first step of the phalloplasty surgical procedure. The connection of the urethra is made by creating a tube from the skin of the scrotum between the openings of both parts of the urethra.
Note that the anatomical makeup of the phallus is composed of only skin, fatty tissue, blood vessels, and nerves.
It does not contain any muscles or a sphincter (a muscle that opens and closes like your butt does aka "the breakwall"), which means that after the second step, you may have to empty your urine either temporarily or permanently manually from the portion of the phallus by applying pressure to the phallus. (UL Article)
A minimum of a six month waiting period is necessary between this and the next stage planning.
Permanent hair removal from the area that will be used to construct the urethra is also required to avoid complications (unless during the consult the doctor states otherwise). Note that it is impossible to determine in advance which area will be depilated since it must be evaluated after Step one. It is at this time that you will receive information about hair removal,
The third step:
Involves insertion of implants (erectile device and testicular implants).
This procedure will allow you to be able to get an erection in your penis (phallus) and now you have the ability of penetrative sex. Erectile Devcies Post
You will have to wait a minimum of three to six months after the second step (healing and surgeon(s) pending) and have no urinary problems before planning the third step. If complications do come up, they will have to be completely treated and healed before the implant surgery can be performed.
"Depending on the surgeon's assessment, the second and third steps may be reversed." (Source1)
Everyone has to decide whether to undergo one, two, or all three steps. Meaning you can stop after any phase/step of the three)
This choice is super personal and must be made according to what you need, your expectations of the outcome, and the impact it has on your daily life.
There are a few factors that may influence your decisions, such as wanting to urinate while standing, the desire to have penetrative sex, having more masculine genitalia, etc.
The estimated time to complete all three stages of phalloplasty can vary from two to three years, including the waiting I'm between surgeries.
These results may vary according to the age, weight, quality, and elasticity of the skin at the donor site, the scarring process, lifestyle habits and the overall health of the patients, healing, how well you take care of yourself, etc. The radial forearm free-flap technique is shown to produce the best results from bottom masculinizing surgery options.
Mandatory Prerequisites for Phalloplasty:
Hysterectomy with removal of the cervix done minimum six months before the phalloplasty procedure. *There are two options for this: removing the uterus only (called "total hysterectomy"), or option two removing the uterus, fallopian tubes, and the ovaries, also called "total hysterectomy with salpingo-oophorectomy"*
Permanent hair removal (second step when recommended to start). The recommended options are laser hair removal or electrolysis, which may be more beneficial for results. from the area of the phallus donor site to prevent complications with hair growth (fistuals), which can cause issues such as infection and even surgerical intervention to fix the issue area(s). Surgeons typically like to see the graft site not have any hair growth for a minimum of three months.
Talk to your primary physician and/or gynecologist to help you make an informed decision about your choice on the type of hysterectomy you get.
And talk to your surgeon and your primary doctor about which option of hair removal is better suited if one is not insisted on you using it.
A vaginectomy can be removed since only 2 cm will be used for the phallus.
Body Mass Index (BMI)
Before phalloplasty can be performed, it is important to know that you must have a healthy weight or have a BMI under 30, and you can not have excessive fat accumulation in your abdominal area.
"Being overweight and abdominal fat can compromise the connection of blood vessels during the procedure and lead to significant surgical complications.
If your BMI is 31 or higher you be most likely required to lose weight before the surgeon will perform the procedure.
Patients with a high BMI also have a decreased potential for healing and decreased satisfaction with surgical results." - (Source1)
Source List:
Source1 -GRS Montreal,Quebec, Canada - downloadable PDF -used as the direct quotes and most of the information
John Hopkins Hospital - used for an information source. -https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/phalloplasty-for-gender-affirmation
Cleveland Clinic -an information source (I barely used this)- https://my.clevelandclinic.org/health/treatments/21585-phalloplasty
Article- Self written on Urethra Lengthening Procedure
Article- Self Written - Erectile Devices Available
#transgender resources#ftm trans resources#female to male affirmation surgery blog#educational blog#phalloplasty resources#phalloplasty procedure layout#phalloplasty procedure#transgender#trans ftm#ftm transition#transman#ask me things#phalloplasty#ftm phalloplasty#lgbtq#phalloplasty blog#phallo education#bottom surgery resource#ftm bottom surgery resources#ftm trans ed
12 notes
·
View notes
Text
15ish Years Post Op - Shadows' chest.
I decided to show you all my chest. It has been about 15ish years since my top surgery.





I lost 1 1/2 of my nipples during the healing process. After three or four years, I had them tattooed back on. My left looks near perfect to me, and that one was just a tiny little spot of nipple left. I know exactly it was 100% my fault. I was told to take the bandages off wet (you want to get into the shower with the bandages on and soak them through. The goal here is to gently part the bandage from your nipple skin without pulling or tearing your nipple skin), but my young self 'knew better' apparently. I also did not realize the 'scab looking' things were my actual nipples.
Before chest surgery I worked out a lot to build my chest up. The spots also have sensation in other ways as well.
Yes, I do feel more sensitive over the spots where my real nipples used to compared to the rest of my chest. I love chest rubs.
Listen to what the professionals have to say.
Some advice I have to help prevent losing your nipples after the flap procedure never take your bandages off dry (soak them as mentioned above), do not touch/pick at them (skin or bandages), not scratching when it itches even over the bandage, just let the soapy water cover your nipples when showering, and do not scrub, and follow surgeon's and nurses' orders of your chest/nipple care when you get home.
Good luck with your journey, everyone!
Stay Golden Everyone ✌️ 💙 💜
#chest surgery#flap chest surgery#transman#transgender#ftm top surgery educational blog#ftm top surgery image#ftm top surgery#ftm education#ftm advice blog#answersfromtheshadows#trans ftm#ftm transition#ask me things#phalloplasty#ftm phalloplasty#phalloplasty blog#lgbtq#phallo education#tw male chest nudity
20 notes
·
View notes
Text
Phalloplasty and Urethra Lengthening Procedure - Personal Article
***Make sure you come home with antibiotics***
Definition of a catheter: A catheter is a tube that is inserted into your bladder, allowing urine (wee) to drain freely. The catheter tube is attached to a drainage bag (a catheter bag), where the urine can be collected.
How a catheter works: Catheters are usually inserted through the urethra (the narrow tube that connects your bladder to the outside). The catheter is kept in place by a ball filled with saline that sits against your bladder wall. This can cause bladder spams.
What is the Procedure?
After phase one, Phalloplasty, a skin-tube urethra (created and placed during the first phase of phalloplasty). After phase one (a minimum of six months between procedures is a common healing period) they make an incision in your scrotum and connect the urethra in the phallis is connected to your original (but lengthened) urethra. It is a short procedure. After the procedure you will have a catheter inserted and you will have it outside of the hospital from two to six weeks (time varies from clinic to clinic). Where it will most likely be removed by your primary health care provider. The catheter is used to protect the new urinary tract as it heals post- operation.
Wearing boxers and loose underwear can help you feel more comfortable while the catheter is in. While more tight underwear such as boxer briefs and briefs are better for after your healing period to help keep your phallis from creating a potentially unwanted bulge in your thigh of your pants.
Findings and Advice:
Bladder spams can be an irritating and annoying type of pain, more annoying than painful. They come and go randomly, but they are something to be aware of.
I was in surgery for about an hour and a half for this particular part. Then, about the same amount of time in the OR (Operating Room) care unit. When I was in there, they offered to let me go as soon as I was wide awake and completely responsive. I received a [intramuscular] shot of morphine. I have a habit of getting sick (vomiting) if I get the entire dose at one time. So I informed the nurse that I get extremely neausous with the full amount of morphine and I was told to do it in two doses. The nurses were nice, they did what I asked. They gave me half then about 20 minutes later gave me the other half. Since I had to take the pain medication, I had to stay an extra 45 minutes. Where as if you don't need anything for pain you can go back to your room after a few minor "tests" of your body and mind.
I know you want to get out of that room, but take your time and rest. Take the pain medication if you need it.
Do not let your pain get over a 7/10 on the pain scale. Once you get to 7,8, or above, you can have a hard time getting comfortable.
Do not try to tough out the pain at any stage. If you are in pain, let a medical professional know.
Ask your surgeon any and all questions you have. They talk to you for a reason. They want you to be informed and heal properly.
Try to have someone who can be around a lot to look after you for a few days after the procedure.
You may have a wound between your phallis shaft and your scrotum. That is where they went in to connect the new and preexisting urethra. (At least for me)
Watch for signs of infection, and if you are concerned, go to the Emergency Room, call your clinic, or whoever provides you Healthcare. (red, irritation, heat, puss, a bad smell, ect.)
If you are leaking from your catheter, speak to a health care professional. Leakage can be a problem if the catheter isn't placed right. Catheter Info
The type of catheter they most likely will use is called: Long-term indwelling catheter: The catheter is passed through the urethra and left in place. This time can range from two to six weeks before it may removed. Surgerons times may vary, average I see is about three weeks. Mine, they wanted six weeks.
WASH YOUR HANDS ALWAYS AS IF YOU HELPED YOUR FRIEND DISPOSE OF A DEAD BODY!!!
The catheter can be in from two to six weeks. This is a long time with a catheter, so be prepared mentally.
You will need some extra catheter bags, hand sanitizer (multiple bottles), medical tape (something easy on your skin), non-scented body wash, some antibacterial wipes, a plastic leg covering from a medical supply store (if required), ice packs, boxers (plain, loose fitting boxers while you have the catheter in) maybe something to put to protect your mattress if you want to, big comfortable sweatpants (get or have at least five pairs to rotate through), a number to your clinic, all of your medications given and taken as instructed, make sure you get antibiotics!
Dripping after you are healed is normal for even cis men (usually its only a few drops)
I drip if I don't shake enough or take my time
How to reduce leakage, dribbling, and general mess:
After passing urine, wait for a few seconds to allow the bladder to empty
Place the fingertips of your hand on your mid taint, behind the scrotum and apply gentle pressure also slight pushing of your pelvic mucles may help
Keeping the pressure in the mid line, gently but positively draw the fingers forwards towards the base of the penis under the scrotum
This pushes the urine forward into the penile urethra from where it can be emptied by shaking or squeezing in the usual way
Before leaving the toilet, repeat the technique twice to ensure that the urethra is completely empty. Source
I do the last step at least three times. I also take time between the three attempts. I will let my penis rest with gravity, I do a slight push, then I can almost feel if anything is left or not. Always do a couple security shakes.
Pro-tip when urinating standing, use the pocket in your underwear, try not to pull your phallis over your waistband (usually you pull your boxer wistband down and flop your phallis over. This is okay to do by all means, but it does work against gravity and makes it more difficult to completely empty. So my recommendation is to use the pocket in your boxers. Just undo your zipper and button (or if you have sweats or something you have to pull them down, but make sure the waistband doesn't touch your shaft or even try to hold it lower than your scrotum. I kind of use my remaining fingers to block my waistband from touching me in sweats or something without buttons or zippers
It gets easier to pee if/ when your pump is implanted. Since you are always slightly pumped (most models of pumps require a pump at all times (min) ask your doctor about your oumping situation, the booklet clinics tend to give out dont always give you all you need to know), there is enough rigidity (hardness/stiffness) to keep your urethra more straight). I found my penile implant really helped with my urination and being able to completely empty my bladder. It also allows urine to flow more freely when I do urinate. This isn't to say before your pump you will have issues, more you have to support your phallis as you urinate a lot more to keep that tract straight. If you get penile implants, for example, you can pee with no hands. If you do with no implant, you may pee on yourself because there is no rigidity, but I'm sure there is someone out there who can and more who will be able to. Like I said, all of our bodies are different
Gravity is your friend
No sex (even anal) of any kind for usually at least 6-8 weeks
Try to relax
I can feel awkward peeing in a urinal with someone next to me because I shake more than I feel is socially typical. Comfort is a big factor in peeing in general. I have anxiety about going to the bathroom in public, I usually use a stall if I can. It's not a big deal.
You can still get pleasure and have orgasms in this state. I do not recommend trying to do penetrative sex, but this is a good question to ask your doctor
I had a lot more sensation after I was healed.
I find that it's easier to wear underwear that is more supportive, eg., Boxer briefs, briefs, pocket underwear. You don't shrink a lot when you're not erect, so you have more to tuck away than the average cis man. I find boxers and loose fitting underwear can cause an unwanted bulge in one inner thigh or the other when wearing especially sweatpants and jeans.
Wearing the above kind of underwear can reduce mess after your catheter is removed and drippage as you learn as well. You're probably gunna pee down your leg as you learn.
Carry a extra pair of underwear with you when you go somewhere, before your catheteris removed as well. If you are learning and you make a mess, you can have a clean pair of underwear to put on. It's not fun sitting in pee soaked underwear...
Wear dark pants at first (hides if you have an accident)
There is a huge learning curve, you don't expect it, but it's not as easy as it seems to hit the target when you stand to pee, and learning to be patient and effective at emptying your bladder.
It is ABSOLUTELY NORMAL TO URINATE SITTING DOWN!!! I did a small survey in a Facebook group for males (i was actually impressed it had over 200 votes, plus over 100 comments in total). Many comments and votes say it's perfectly fine to sit peeing and many people have different reasons. Mine is I want to play on my phone, plus sometimes my feet are tired... It's normal to sit.
Be careful with your urine bags and always ALWAYS have extra urine bags ON HAND/ AT YOUR CURRENT LOCATION!!! And no a plastic ziplock baggie will not do. Trust me.
Have tons of hand sanitizer around the house and bathroom, antibacterial soap, unscented soap (for your body), and make sure that you keep your hands and valve on your catheter always sanitized.
If you feel pain in your member or bladder or anywhere inbetween, go to the Emergency Room, if you feel hot go to the E.R right away. Better to be safe than sorry.
Keep hand sanitizer literally on the back of toilet so it is convenient.
Even with the catheter in, you feel the urge to urinate. I found that I could ease the feeling for a bit if I "urinated" in my usual position (I found sitting to be most comfortable)
You are going to be very tender and sore
Swelling will go down
Make sure you stay clean and dry. Especially where your wound is.
The doctor who does a lot of the work during this phase of surgery is called a urologist. So research them as well as your surgeon. You want every member of the team of your entire procedure to be great at what they do.
Do not try to remove the catheter yourself. You will not be successful. If you are having issues go to the Emergency Room, clinic, or whoever provides proper health care to you.
Do not take any chances with infection. Hands clean, valve sterilized and closed, urine bag attached properly and tightly.
Wait to shower until you are instructed to.
Try to shower as often as they tell/let you. You want to stay clean to avoid infection. Of course you also don't want to overdo it.
Showering with a catheter is a challenge. I found that the plastic covers made for covering wounds/bandages/ etc. Depending on what your surgeon says, you may not have to cover your catheter bag at all. Be sure you ask your clinic!
When you are showering, be super mindful you have a catheter. Any tugging or too much movement can hurt and possibly affect your healing. So be gentle. Also, be careful when washing the tip of your phallis at this stage.
Dry your wound/ pubic area by patting dry and not wiping. Be gentle.
During my showers, I would use medical tape to kind of keep everything (tubing) in one place.
Your catheter may not come with anything to hold it onto your leg. While catheters i noticed usually come with a soft elastic band with snaps that you'd tie to your leg. If you dont recieve that in the clinic, ask a nurse if they can give you some dressing mesh and ask if they can teach you how to make a pocket you can tie to your ankle (that's what I did, the elastic band would slide down my leg). There may be other options for holding your catheter. I do not recommend anything that would cut off blood flow to your leg and/or something that restricts or affects the functionality of your catheter.
Be mindful of your catheter at all times.
If you are going insane with the feeling of having to urinate, try looking at your unit and tell yourself "I don't need to pee, I'm fine. I will not mess myself". It especially helps when I would sit on the toilet as I did this.
Shave your inner legs if you have to, because you will want to tape the tube to your leg, at least in the shower. This helps so you don't pull/tug it. Trust me again. Pulling/ tugging on it even slightly by accident is not a good time.
Always double check to make sure your valve is closed, leaving it open is a welcoming hall for viruses and bacteria directly into your bladder
I know that catheter is going to drive you mad, DO NOT TUG ON IT!!! I tugged (because it was making me not comfortable), and it actually moved the catheter out of place. This caused me to be urinating directly through my new urethra before it could have been ready. It was actually really painful (burning). So please do not tug, go see your medical professional if you are feeling very irritated and/or uncomfortable. Sometimes, the [catheter] line needs to be "flushed" (flushed: when they "rinse out" the catheter system with saline water).
Take your meds as instructed, especially your antibiotics. If you have to take meds at certain times or time intervals, set alarms, tell someone. For many antibiotics, timing matters and is a huge factor in how well they function
Do you feel yourself pee when you are completely healed? - Yes, I can feel it, especially when it's been cold outside
Do you feel yourself pee with a catheter before the swelling goes down? - For me? No, your bag just fills up. But contrary to what I always think (everytime i have a catheter think "i dont have to get up to pee for awhile, niiiice", im always wrong), it does make you uncomfortable as in feeling like you have to urinate constantly. That's a lot thanks to the bladder spasms.
Here are the sources I used:
https://www.healthdirect.gov.au/catheter-problems
https://cranects.com/urethral-lengthening/
I will post my story another day. I want this information to be heard and sink in first.
If you have any questions, or concerns please feel free to send an ask or email.
If you'd like anything added, or you have questions about this. Also feel free to contact me.
Stay Golden Everyone ✌️ 💙 💜
#transgender#ftm transition#trans ftm#ask me things#transman#phalloplasty#ftm phalloplasty#phalloplasty blog#lgbtq#phallo education#phalloplasty surgery#transitioning#transgender ftm affirming procedures#ftm urethra lengthening procedure#urethra lengthening procedure#phalloplasty with urethra lengthening#tw drugs mention#tw opiate mention#tw pain medication#tw medication
21 notes
·
View notes
Text
Phalloplasty and Metoidioplasty Comparison (Surgical information)


***Your preference is also super important***
I found this gem of a file from Bostons Children's Hospital. It goes over everything rather well. (It also saves my hands, I apologize everyone)
If you need anything cleared up, or I missed anything, please let me know!
I am here to provide recent and accurate information on phalloplasty, and I've been doing research on metoidioplasty, which I may start sharing information on that surgery as well.
From a personal perspective, I am not opposed to posting about metoidioplasty, I just don't have any personal experience in that area, I also feel phalloplasty has a very bad rap and needs some light shed on how much things have changed since a lot of outdated information.
Stay golden ✌️💙💜
#transgender#trans ftm#transman#phalloplasty#ftm transition#ask me things#ftm phalloplasty#phalloplasty blog#lgbtq#phalloplasty education blog#phalloplasty education#phallo education#ftm bottom surgery#ftm transition blog#ftm bottom surgeries#which surgery is for me?
31 notes
·
View notes
Last Seen Blogs

pizza-games-and-more
Join the Vigi Fan Club!

joriskan
Jorio nuotykiai Švedijoj

artificial-friend
mercurial

sevenoaksroofuk
Untitled

spacework008
Untitled