#pfizer vaccine all coronaviruses
Text
Pfizer plans a vaccine against all coronaviruses
Pfizer plans a vaccine against all coronaviruses
June 30, 2022 – Ask a celebrity sibling and they’ll tell you they don’t come close to getting the same attention. The same goes for coronaviruses – the one that causes COVID-19 has been in the spotlight for over 2 years now, while the others are currently circulating in relative obscurity.
Knowing that one of the other coronaviruses could pose a serious future threat, Pizer and his partner…

View On WordPress
#biontech#covid vaccine#COVID-19#is there a vaccine for variants?#pfizer#pfizer vaccine#pfizer vaccine all coronaviruses#pfizer vaccine for all coronaviruses#SARS-CoV-2#vaccine for variants#virus that causes covid
0 notes
Text
Vaccines currently in development
(I did not create this list and I'm sorry I don't know the original OP who compiled it.)
These are all currently in development to come to market in the next 2 years. If just one really works it will be a game changer
MT-001 a novel protein component vaccine candidate, MT-001, based on a fragment of the SARS-CoV-2 spike protein that encompasses the receptor binding domain (RBD) | A SARS-CoV-2 Vaccine Designed for Manufacturability Results in Unexpected Potency and Non-Waning Humoral Response - https://www.mdpi.com/2076-393X/11/4/832 Mice and hamsters immunized with a prime-boost regimen of MT-001 demonstrated extremely high anti-spike IgG titers, and remarkably this humoral response did not appreciably wane for up to 12 months following vaccination. Further, virus neutralization titers, including titers against variants such as Delta and Omicron BA.1, remained high without the requirement for subsequent boosting.
DCFHP a ferritin-based, protein-nanoparticle vaccine candidate that, when formulated with aluminum hydroxide as the sole adjuvant (DCFHP-alum), elicits potent and durable neutralizing antisera in non-human primates against known VOCs, including Omicron BQ.1, as well as against SARS-CoV-1. | A ferritin-based COVID-19 nanoparticle vaccine that elicits robust, durable, broad-spectrum neutralizing antisera in non-human primates https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10110616/#MOESM3
ISM3312 a COVID-19 drug entirely designed by generative AI works by inhibiting a protein called 3CL protease — a critical factor in viral replication and a popular target for anti-COVID drugs. Unlike similar therapeutics, it works on a very broad spectrum — showing efficacy not only against all current COVID variants, but also coronaviruses other than SARS-CoV-2. As such, it may possess the ability to resist future mutations, providing a solution to drug-resistant strains. | ‘It’s perfect’: World’s first generative AI-designed COVID drug to start clinical trials https://www.thestar.com/news/canada/2023/02/23/its-perfect-worlds-first-generative-ai-designed-covid-drug-to-start-clinical-trials.html
BNT162b4, composed of a T cell antigen mRNA encoding for SARS-CoV-2 non-spike proteins that are highly conserved across a broad range of SARS-CoV-2 variants and will be evaluated in combination with the Omicron BA.4/BA.5-adapted bivalent COVID-19 vaccine | Pfizer and BioNTech Advance Next-Generation COVID-19 Vaccine Strategy with Study Start of Candidate Aimed at Enhancing Breadth of T cell Responses and Duration of Protection https://investors.biontech.de/news-releases/news-release-details/pfizer-and-biontech-advance-next-generation-covid-19-vaccine
25F9 and 20A7 identified as two highly potent broadly neutralizing antibodies, making them promising prophylactic candidates against sarbecovirus infection |Broadly neutralizing antibodies against sarbecoviruses generated by immunization of macaques with an AS03-adjuvanted COVID-19 vaccine – Science Translational Medicine – https://www.science.org/doi/10.1126/scitranslmed.adg7404
ChAd-SARS-CoV-2-BA.5-S, which encodes for a pre- fusion and surface-stabilized S protein of the BA.5 strain. | A bivalent ChAd nasal vaccine protects against SARS-CoV-2 BQ.1.1 and XBB.1.5 infection and disease in mice and hamsters https://www.biorxiv.org/content/10.1101/2023.05.04.539332v1
#covid#covid vaccine#vaccines#treatment#will it be like this forever#'will you mask forever?'#research#science#neutralizing vaccine#coronavirus
4 notes
·
View notes
Text
Health Department v.s. COVID-19: Acts Against the Virus
Health Department v.s. COVID-19: Acts Against the Virus
The coronavirus pandemic (COVID-19) is arguably the biggest and most impactful health crisis the world has ever witnessed. From the closing of schools to the implementation of mask mandates and full-blown economic shutdown, COVID-19 changed how the world operated for the better part of a two-year duration, and even still, the effects of the national health emergency still linger. In light of the impact of the pandemic, the question of if the United States health departments did all that they could to cease the shock to the general public during the pandemic stands. Said health departments mainly include the Centers for Disease Control and Prevention (CDC), the United States Food and Drug Administration (FDA), and the World Health Organization (WHO), as these departments had a major hand in the research and development of COVID-19 procedures and vaccinations. In strenuous times of uncertainty, The United States health departments worked endlessly to provide the public with new information and data about the virus and overall crisis whenever possible. It is because of these hard-working officials that the pandemic was handled as swiftly as possible and new developments were made so frequently.
According to the CDC Museum COVID-19 Timeline, on January 3rd, 2020, China first informed WHO about the identification of over 40 cases of an unidentified pneumonia-like disease that did not respond well to standard treatments. By January 5th, 2020, the CDC’s National Center for Immunization and Respiratory Diseases (NCIRD) had enacted a response team to investigate the virus. By January 10th, 2020, the WHO had announced the outbreak of the coronavirus in Wuhan, China, and the CDC had published information about the fast-spreading virus on its website. Once aware of the situation, the U.S. health departments wasted no time informing the public and looking into the severity of the situation. In one week, WHO and the CDC investigated the virus’s destructive potential and issued information to the public to warn them of the possibility of a threat. Responding in such a timely manner is key when dealing with a virus of COVID-type destructibility, and U.S. health departments did exactly this to inform U>S> citizens about the virus at once.
Once it was established that the COVID-19 virus would be wreaking havoc around the world for quite some time, it was clear that a kind of cure or vaccine would need to be developed sooner rather than later. With fatalities high and still so much that was unclear about the circumstances surrounding the virus, the public turned to the government for answers. In under a span of one year, by December 11th, 2020, the Pfizer vaccine was the first to be given emergency authorization by the FDA.
Creating a vaccine for such a widespread issue in under a year was, of course, not easy. However, given the pressure and conditions, the vaccine was created with endless work and collaboration. Even so, many of the public refused to receive the vaccine, unsure about the side effects of something that was developed so quickly. Medical News Today (MNT) states that “...making a vaccine can take up to 10–15 years. This is because of the complexity of vaccine development.” What many don’t realize is that researchers and developers working on the creation of COVID-19 vaccines did not start completely from scratch. SARS-CoV-2, the very element of COVID-19, belongs to a family of coronaviruses. On the contrary, coronaviruses are not as new as one may think, and according to Dr. Eric J. Yager, a professor at Albany College of Pharmacy and Health Sciences who responded in an interview with MNT, scientists have been researching coronaviruses for over five decades. Due to the data already existing on this kind of virus, the creation of the vaccine was able to move swiftly.
Some would argue that although the COVID-19 vaccines were developed and issued to the public, they are not foolproof. In an article titled “COVID-19 Vaccines are Effective” by the CDC, it is noted that some people who are vaccinated will indeed still get sick and/or have a breakthrough infection. This is not a knock on the vaccine’s overall effectiveness, however. It is simply a reality for all vaccines as none are 100% effective or capable of stopping the disease from penetrating a human’s immune system. While the public would like this to be possible, especially for a virus as severe as COVID-19, the reality is that it is not. However, the CDC and the FDA have worked endlessly to provide U.S. citizens with three options of vaccines that are all equipped to fight the effects of the coronavirus. For a fatal virus that has been a threat for almost three years, three options for vaccination is a very good development.
While the U.S. health departments have done endless work to combat the aggressive force of COVID-19 since its development, there are surely things that they could have done differently. However, this does not mean the progress they have made and the developments implemented are not impressive and ground breaking. U.S. citizens should be more than grateful to the workers within these departments that have made this progress possible. Without the work of the WHO, CDC, and FDA, the COVID-19 pandemic could have looked a lot different in a very negative way for the United States.
Sources:
https://www.cdc.gov/museum/timeline/covid19.html
https://www.medicalnewstoday.com/articles/how-did-we-develop-a-covid-19-vaccine-so-quickly#Other-coronaviruses
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/index.html
0 notes
Text
Pfizer Plans a Vaccine to Target All Coronaviruses
Pfizer Plans a Vaccine to Target All Coronaviruses
June 30, 2022 – Ask the sibling of any celebrity and they’ll tell you they don’t get anywhere near the same attention. The same is true for coronaviruses – the one that causes COVID-19 has been in the spotlight for more than 2 years now, while the others at the moment circulate in relative obscurity.
With the knowledge that any of the other coronaviruses could pose a serious future threat, Pizer…
View On WordPress
0 notes
Note
I won't darken your ask box again, but I've just lost whatever scrap of hope the vaccines gave me when it became clear that there was a new variant and that vaccine rollout will be so slow it's guaranteed to produce more, vaccine-resistant variants. And every public health official and pundit just talks about "hunkering down" and I can't do that anymore than I already do, and I'm sure it won't end. I just want someone in power to be honest with me that my life is over and no help is coming.
Oh hon, darken my ask box as much as you like! I have an ear and a shoulder and they’re both available to you, albeit only virtually.
In fact, I woke up in the middle of the night absolutely convinced of exactly what you’re saying. (I think I had an anxiety dream I didn’t remember). I’m fighting the same battle.
So, experts are looking into the concern with the new variants. Every expert believes the vaccines will work against them, with a worst case scenario of an efficacy drop of about 10%. Note that the vaccines we have approved have a very high efficacy, so while this sucks, it’s not the end of the world.
BioTech and Moderna are constantly testing their vaccines against every mutations that show up. To put this in perspective:
B1.1.7, which is the UK strain, has a mutation that causes 8 amino acid changes on the spike protein. That’s what’s making people panic. However, there are 1,273 amino acids in the spike protein! Coronaviruses are big viruses.
(Source: https://www.wusa9.com/article/news/verify/do-not-publish-verify-are-current-covid-19-vaccines-effective-against-variant-strains/65-8734e2a6-a18f-49ab-b2b5-6d198da45782)
So, we have no vaccine-evading variants yet, and if you look at that, it would take a lot, a lot of mutations to the spike protein to evade the vaccine.
Experts believe the vaccines will be fully efficacious against B1.1.7.
501.V2, the South African variant (and note, these are not strains) is a little more worrying, but we will know very soon if it evades the J&J vaccine, which is being tested there. The Oxford vaccine is also in trials in South Africa.
Some experts believe that there might be a 10% or so efficacy drop against this variant, which still means the vaccines will work very well. If the J&J vaccine works well against it, then we should be able to deal with it by using that vaccine in South Africa and anywhere else that variant spreads to, for example.
(And the J&J vaccine will be better for remote areas as it’s a single dose).
(Source: https://www.cbsnews.com/news/covid-vaccine-new-strain-south-africa/)
So, on to your next worry, that an actual vaccine-evading variant will show up before we get everyone vaccinated.
The first piece of good news is that coronaviruses do not mutate as quickly as orthomyxoviruses (the viruses that cause influenza). Flu strains evade the vaccine all the time, which is why we don’t yet have a universal flu vaccine (one was well into development but the researchers dropped it to focus on COVID-19) and why flu vaccine efficacy varies so much from year to year.
COVID-19 mutates much more slowly. Like all coronaviruses it has an enzyme called ExoN, which proofreads its code and keeps the copies close to each other. Furthermore, the viruses target the spike protein, which is highly conserved due to already being very good at its job.
Now, vaccines do mutate, and yes, it is absolutely possible that an escape variant will evolve in the future. However, because of the proofreading, this is less likely than with most viruses. An escape variant would reduce the effectiveness of vaccines and necessitate boosters. When is this likely to happen? In, worst case, a couple of years. At which point we will probably be needing boosters anyway due to waning immunity (Pfizer’s educated guess is that their vaccine will be effective for 2 to 5 years).
Finally, on the slow roll out, honestly, it’s mostly teething problems. The pace is already starting to speed up. There are things we need to consider doing. Many dentists, for example, have volunteered to administer shots; administering a vaccine is much easier than administering local anesthesia to the mouth. There’s also been some talk of recruiting veterinarians and vet techs, as giving a shot to one species isn’t hugely different from giving it to another. But we’re working the problem.
And I know you can only hunker down so far. But again, darken my ask box *any time you want*. You are valid and I absolutely understand your fears.
172 notes
·
View notes
Text
Why Are So Many Vaccinated People Getting COVID-19 Lately?A couple of factors are at play, starting with the emergence of the highly contagious omicron variant. Omicron is more likely to infect people, even if it doesn't make them very sick, and its surge coincided with the holiday travel season in many places. People might mistakenly think the COVID-19 vaccines will completely block infection, but the shots are mainly designed to prevent severe illness, says Louis Mansky, a virus researcher at the University of Minnesota. And the vaccines are still doing their job on that front, particularly for people who've gotten boosters.


The Next Variant Is Just Around the Corner': Experts Warn the World's at Risk Until All Are Vaccinated. Two doses of the Pfizer-BioNTech or Moderna vaccines or one dose of the Johnson & Johnson vaccine still offer strong protection against serious illness from omicron. While those initial doses aren’t very good at blocking omicron infection, boosters particularly with the Pfizer and Moderna vaccines rev up levels of the antibodies to help fend off infection. Omicron appears to replicate much more efficiently than previous variants. And if infected people have high virus loads, there's a greater likelihood they'll pass it on to others, especially the unvaccinated. Vaccinated people who get the virus are more likely to have mild symptoms, if any, since the shots trigger multiple defenses in your immune system, making it much more difficult for omicron to slip past them all. Advice for staying safe hasn't changed. Doctors say to wear masks indoors, avoid crowds and get vaccinated and boosted. Even though the shots won’t always keep you from catching the virus, they'll make it much more likely you stay alive and out of the hospital. The omicron variant accounted for 95% of new coronavirus infections last week, according to U.S. health officials’ latest estimates. The Centers for Disease Control and Prevention posted its newest estimates Tuesday. The CDC uses genomic surveillance data to make projections about which versions of the COVID-19 viruses are causing the most new infections. The latest estimates suggest a dramatic swing in just one month in which version of the coronavirus is most abundant. Beginning in late June, the delta variant was the main version causing U.S. infections. The CDC said more than 99.5% of coronaviruses were delta as recently as the end of November. The CDC’s estimates are based on coronavirus specimens collected each week through university and commercial laboratories and state and local health departments. Scientists analyze their genetic sequences to determine which versions of the COVID-19 viruses are most abundant. However, those specimens represent just a small fraction of what’s out there. More than 2.2 million cases were reported in the last week in the U.S. The CDC has been revising estimates for past weeks as it gets more data.
Pourquoi tant de personnes vaccinées reçoivent-elles le COVID-19 ces derniers temps ? Quelques facteurs sont en jeu, à commencer par l'émergence de la variante hautement contagieuse de l'omicron. Omicron est plus susceptible d'infecter les gens, même s'il ne les rend pas très malades, et sa poussée a coïncidé avec la saison des vacances dans de nombreux endroits. Les gens pourraient penser à tort que les vaccins COVID-19 bloqueront complètement l'infection, mais les injections sont principalement conçues pour prévenir les maladies graves, explique Louis Mansky, chercheur en virus à l'Université du Minnesota. Et les vaccins font toujours leur travail sur ce front, en particulier pour les personnes qui ont reçu des rappels. La prochaine variante est juste au coin de la rue les experts avertissent le monde en danger jusqu'à ce que tous soient vaccinés. Deux doses des vaccins Pfizer-BioNTech ou Moderna ou une dose du vaccin Johnson & Johnson offrent toujours une forte protection contre les maladies graves causées par l'omicron. Bien que ces doses initiales ne soient pas très efficaces pour bloquer l'infection à omicron, les rappels, en particulier avec les vaccins Pfizer et Moderna, augmentent les niveaux d'anticorps pour aider à repousser l'infection. Omicron semble se répliquer beaucoup plus efficacement que les variantes précédentes. Et si les personnes infectées ont une charge virale élevée, il est plus probable qu'elles la transmettent à d'autres, en particulier aux non vaccinés. Les personnes vaccinées qui contractent le virus sont plus susceptibles de présenter des symptômes bénins, le cas échéant, car les injections déclenchent de multiples défenses dans votre système immunitaire, ce qui rend beaucoup plus difficile pour omicron de les franchir toutes. Les conseils pour rester en sécurité n'ont pas changé. Les médecins disent de porter des masques à l'intérieur, d'éviter les foules et de se faire vacciner et booster. Même si les injections ne vous empêcheront pas toujours d'attraper le virus, elles augmenteront vos chances de rester en vie et hors de l'hôpital. La variante omicron représentait 95% des nouvelles infections à coronavirus la semaine dernière, selon les dernières estimations des autorités sanitaires américaines. Les Centers for Disease Control and Prevention ont publié mardi leurs dernières estimations. Le CDC utilise des données de surveillance génomique pour faire des projections sur les versions des virus COVID-19 qui causent le plus de nouvelles infections. Les dernières estimations suggèrent une variation spectaculaire en seulement un mois au cours de laquelle la version du coronavirus est la plus abondante. À partir de la fin juin, la variante delta était la version principale à l'origine des infections aux États-Unis. Le CDC a déclaré que plus de 99,5 % des coronavirus étaient des deltas à la fin novembre. Les estimations du CDC sont basées sur des spécimens de coronavirus collectés chaque semaine par des laboratoires universitaires et commerciaux et des services de santé étatiques et locaux. Les scientifiques analysent leurs séquences génétiques pour déterminer quelles versions des virus COVID-19 sont les plus abondantes. Cependant, ces spécimens ne représentent qu'une petite fraction de ce qui existe. Plus de 2,2 millions de cas ont été signalés la semaine dernière aux États-Unis. Le CDC a révisé ses estimations au cours des dernières semaines à mesure qu'il obtenait plus de données.
Données du 6 janvier 2022
4 notes
·
View notes
Text
Michael Yeadon, former Vice President and Chief Scientific Officer of pharma giant Pfizer for 16 years, discusses his thoughts as to why the lockdown was a mistake, and why the government strategies to manage the pandemic are only making things worse.
[EDITED (for brevity) TRANSCRIPT OF THE VIDEO]
"I’ve worked my entire life on the research side of the pharmaceutical industry, both big pharma and also biotech. My specific focus has been inflammation, immunology, allergy in the context of respiratory diseases."
"I became very perturbed about increasing restrictions on the behavior and movement of people in my country, and I could see no reason for it then and I still don’t."
"Government’s response to emergencies is guided by the [UK] scientific group who sit together under the Strategic Advisory Group for Emergencies [SAGE]. SAGE has got several fundamental things wrong and that has led to advice that’s inappropriate, has horrible economic effects, but has had continuing medical effects in that people are no longer being treated properly."
"SARS-CoV-2 was 80% similar to another virus called SARS that moved around the world a bit in 2003. When I heard that there was this coronavirus moving across the world, I wasn’t worried. Since there are four common cold causing coronaviruses, quite a lot of population would have a substantial protective immunity. Milkmaids never suffered from things like smallpox. The reason they had the protection was that they were exposed to a more benign-related virus called cowpox. Edward Jenner acquired some of the liquid from a person infected with cowpox. He got some of this and he scraped it into the skin of a small boy. He obtained some liquid from some poor person that was dying of smallpox and infected the boy. Lo and behold, the boy did not get ill. And that gave birth to the whole field of what’s called vaccination."
"At this time of year, about 1 in 30 people have a cold caused by one of these coronaviruses. People exposed to having had a cold caused by one of these coronaviruses are immune to SARS-CoV-2. 30% of the population was protected before we started. SAGE said it was zero which is impossible to justify. The percentage of the population that SAGE asserts have been infected to date by the virus is 7%. A document they published in September 'Non-Pharmaceutical Interventions' says more than 90 percent of the population is still vulnerable [unbelievably wrong!]. On the percentage of care home residents who have antibodies: they picked out residents that never were PCR-positive. These were people who never got infected. 65% of them had antibodies to the virus. There was a high prevalence of immunity in that population prior to the virus arriving."
"Big story in the media: the percentage of people with antibodies against the virus in their blood was falling. This was cast as a concern, "immunity to SARS-CoV-2 doesn’t last very long". Anyone with knowledge of immunity would reject that. It’s not the way immunity to virus works. That would be T cells. If the antibodies are falling gradually over time, the prevalence of the virus in the population is falling. That’s why the antibody production gradually subsides."
"Less than 40 percent of the population are susceptible. That’s too small a number to support a growing outbreak [community immunity, herd immunity]. SAGE says we’re not even close. The best science by the best scientists in the world, published in the top peer-reviewed journals, says they’re wrong. That is more than 60% of the population are now immune. It’s simply not possible to have a large and growing pandemic."
"Why are we not talking about the 50% that have got T cell immunity? I believe, fundamentally, it is over. The number of people dying of SARS-CoV-2 in the capital is less than 10, so it’s down by 98%. The reason it’s down is because there are too few people in London susceptible to allow the virus to magnify, to amplify, to get an epidemic."
"Why isn’t the media telling us that the pandemic is over? It’s not over because SAGE says it’s not. I found, to my horror, that all the way through the spring and summer SAGE did not have on their committee someone who was an immunologist."
"There is a test that’s performed where people have their noses and tonsils swabbed [PCR test]. What they’re looking for is a small piece of genetic sequence [RNA]. It’s going to be found if they were infected weeks or even sometimes a small number of months ago. If you’ve been infected and you’ve fought off the virus, you’ll have broken dead bits of virus. Over a period of weeks or months, you bring up cells that contain broken dead pieces of the virus that you have conquered and killed. The PCR test is not able to detect whether the viral RNA has come from a living virus or a dead one. A large proportion of the so-called positives are what I call cold positives. They’re identifying viral RNA in the sample but it’s from a dead virus that can’t hurt them.
They’re not going to get ill.
They can’t transmit it to anybody else.
They’re not infectious.
Why are we using this test that cannot distinguish between active infection and people who’ve conquered the virus? This test has never been used in this way. It’s the kind of technique you would use for forensic purposes. You would not be doing these tests by a windy supermarket car parking. It’s not suitable at all and shouldn’t be done in the way it’s been done. It’s subject to many handling errors. If this was a test being used for legal purposes, the judge would throw out this evidence and say it’s not admissible. It produces positives even when there’s no virus there at all."
"The pandemic having passed through the population won’t return. Why won’t it return? They’ve got t-cell immunity. Just because the antibody falls away, doesn't mean you've lost immunity again. That’s not the way the human immune system works."
[cont. in video]
19 notes
·
View notes
Photo

The Vaccine News Continues to be Better than Many People Realize.
From New York Times – Morning Report, Feb 1, 2021 by David Leonhardt
Infections aren’t what matters
The news about the vaccines continues to be excellent — and the public discussion of it continues to be more negative than the facts warrant. Here’s the key fact: All five vaccines with public results have eliminated Covid-19 deaths. They have also drastically reduced hospitalizations. “They’re all good trial results,” Caitlin Rivers, an epidemiologist at Johns Hopkins University, told me. “It’s great news.”
Many people are instead focusing on relatively minor differences among the vaccine results and wrongly assuming that those differences mean that some vaccines won’t prevent serious illnesses. It’s still too early to be sure, because a few of the vaccine makers have released only a small amount of data. But the available data is very encouraging — including about the vaccines’ effect on the virus’s variants. -“The vaccines are poised to deliver what people so desperately want: an end, however protracted, to this pandemic,” as Julia Marcus of Harvard Medical School recently wrote in The Atlantic.
Why is the public understanding more negative than it should be? Much of the confusion revolves around the meaning of the word “effective.”
What do we care about?
In the official language of research science, a vaccine is typically considered effective only if it prevents people from coming down with any degree of illness. With a disease that’s always or usually horrible, like ebola or rabies, that definition is also the most meaningful one.
But it’s not the most meaningful definition for most coronavirus infections.
Whether you realize it or not, you have almost certainly had a coronavirus. Coronaviruses have been circulating for decades if not centuries, and they’re often mild. The common cold can be a coronavirus. The world isn’t going to eliminate coronaviruses — or this particular one, known as SARS-CoV-2 — anytime soon. Yet we don’t need to eliminate it for life to return to normal. We instead need to downgrade it from a deadly pandemic to a normal virus. Once that happens, adults can go back to work, and children back to school. Grandparents can nuzzle their grandchildren, and you can meet your friends at a restaurant. As Dr. Ashish Jha, the dean of the Brown University School of Public Health, told me this weekend: “I don’t actually care about infections. I care about hospitalizations and deaths and long-term complications.”
The data
By those measures, all five of the vaccines — from Pfizer, Moderna, AstraZeneca, Novavax and Johnson & Johnson — look extremely good. Of the roughly 75,000 people who have received one of the five in a research trial, not a single person has died from Covid, and only a few people appear to have been hospitalized. None have remained hospitalized 28 days after receiving a shot. To put that in perspective, it helps to think about what Covid has done so far to a representative group of 75,000 American adults: It has killed roughly 150 of them and sent several hundred more to the hospital. The vaccines reduce those numbers to zero and nearly zero, based on the research trials.
Zero isn’t even the most relevant benchmark. A typical U.S. flu season kills between five and 15 out of every 75,000 adults and hospitalizes more than 100 of them. I assume you would agree that any vaccine that transforms Covid into something much milder than a typical flu deserves to be called effective. But that is not the scientific definition. When you read that the Johnson & Johnson vaccine was 66 percent effective or that the Novavax vaccine was 89 percent effective, those numbers are referring to the prevention of all illness. They count mild symptoms as a failure. “In terms of the severe outcomes, which is what we really care about, the news is fantastic,” Dr. Aaron Richterman, an infectious-disease specialist at the University of Pennsylvania, said.
The variants
What about the highly contagious new virus variants that have emerged in Britain, Brazil and South Africa? The South African variant does appear to make the vaccines less effective at eliminating infections. Fortunately, there is no evidence yet that it increases deaths among vaccinated people. Two of the five vaccines — from Johnson & Johnson and Novavax — have reported some results from South Africa, and none of the people there who received a vaccine died of Covid. “People are still not getting serious illness. They’re still not dying,” Dr. Rebecca Wurtz of the University of Minnesota School of Public Health told me.
The most likely reason, epidemiologists say, is that the vaccines still provide considerable protection against the variant, albeit not quite as much as against the original version. Some protection appears to be enough to turn this coronavirus into a fairly normal disease in the vast majority of cases.
“This variant is clearly making it a little tougher to get the most vigorous response that you would want to have,” Dr. Francis Collins, director of the National Institutes of Health, said. “But still, for severe disease, it’s looking really good.”
What would an expert do?
The biggest caveat is the possibility that future data will be less heartening. Johnson & Johnson and Novavax, for example, have issued press releases about their data, but no independent group has yet released an analysis. It will also be important to see much more data about how the vaccines interact with the variants. But don’t confuse uncertainty with bad news. The available vaccine evidence is nearly as positive as it could conceivably be. And our overly negative interpretation of it is causing real problems.
Some people worry that schools cannot reopen even after teachers are vaccinated. Others are left with the mistaken impression that only the two vaccines with the highest official effectiveness rates — from Moderna and Pfizer — are worth getting.
In truth, so long as the data holds up, any of the five vaccines can save your life.
Last week, Dr. William Schaffner of Vanderbilt University told my colleague Denise Grady about a conversation he had with other experts. During it, they imagined that a close relative had to choose between getting the Johnson & Johnson vaccine now or waiting three weeks to get the Moderna or Pfizer vaccine. “All of us said, ‘Get the one tomorrow,’” Schaffner said. “The virus is bad. You’re risking three more weeks of exposure as opposed to getting protection tomorrow.”
#couldn't find another post about this so i decided to make it myself#great vaccine news#coronavirus#vaccines#new york times
17 notes
·
View notes
Text
COVID VACCINE HESITANCY?
The FDA is likely going to approve the Pfizer Covid vaccine when they meet on December 10th. The Moderna vaccine will probably be approved shortly thereafter. This is an incredible feat of modern medicine, and our best chance to hopefully get our lives back to near normal relatively soon. However, it is new and it was done quickly, so understandably, people may be hesitant to get it; even people who vaccinate against all other diseases.
Will I be getting the vaccine? ABSOLUTELY. As a physician, I will probably have the opportunity to be immunized prior to New Year's and yes, I will be taking it as soon as possible.
But, it is a new vaccine technology and done in record time, so aren't I worried about its safety? Nope, not any more so than any other vaccine or other medical intervention.
Why? Let's start with how this vaccine works. This is an mRNA vaccine. Past vaccines typically use a live but weakened "attenuated" virus, or dead viral material "inactivated" virus, or a piece of the virus's protein or even a toxin produced by the virus. The Covid vaccine is very different. It contains mRNA (messenger genetic material) that encodes for the Covid spike protein. This causes your cells to then produce the Covid spike protein. In contrast, when you are sick with Covid, the virus hijacks your cell to produce many copies of the entire virus. Then it destroys the cell, busting it open to release its newly formed viral particles. When your cells release just the spike protein, it will stimulate your immune system to form antibodies to the Covid spike protein without you getting sick. There is no possibility of getting Covid from the vaccine. When your body is subsequently exposed to Covid, it will quickly recognize the spike protein and destroy it before it can make you sick. This was 95% effective in preventing Covid, which is an even better percentage than most other vaccines. However, you must take both doses (about 3-4 weeks apart).
Am I concerned about it being new? And previously untested? No, I'm not. This type of technology is not entirely new. It has been studied and used in cancer research. They have been making mRNA vaccines and studying them to specifically target proteins on tumor cells and train your immune system to then destroy the tumor. In this case, it is not a vaccine in the preventive sense, as it is targeted to a tumor that you already have. It is not currently widespread because it has to be custom made for each tumor. But, it has been "around the block" for a while now. The technology was also being studied for other Coronaviruses. It never came to fruition, because the diseases never reached pandemic proportions, and then the funding dried up. The mRNA does not enter the nucleus of the cell, and it does not affect your DNA, and therefore has no lasting impact on your cell.
Am I concerned about the speed with which it was developed? Weren't significant corners cut in order to get this out so quickly? No and no. What was cut out of the equation was mostly red tape, and what was added was technology and funding. We were given the genetic code by scientists in China to start vaccine production in January; before Covid was even documented to have reached our shores. From there, the vaccine was developed from the technology we had from the prior Coronavirus and cancer research, and was completed in March. Normally, there would be months of waiting for the FDA to even look at the work done prior to approving Phase 1 trials. Because of the urgent nature of this, it was essentially put on the top of the wait pile, which cut out months of waiting, but did not cut any corners. Between the Moderna and Pfizer vaccines (both mRNA, with a slightly different delivery system), they were tested in 37,000 people in Phase 3 (and an additional 37,000 received a placebo). That is on par with, if not better than the vaccines currently available.
Aren't I concerned that the FDA is about to approve it, and there may be side effects that haven't been seen yet? Nope on this one too. We know from decades of vaccine research, since you typically just get 1, 2 or 3 doses and then you are done with it, that nearly all side effects from vaccines occur in the first 6 weeks. Like other vaccines, minor side effects may occur(soreness at injection site, muscle aches, fever). Severe adverse reactions are extremely rare, and again, occur quickly if they are going to occur at all. As a healthy 40-something year old woman, my risk of dying from Covid is about 1 in 250 to 1 in a 1,000. That is not a rare event! And even if I don't die from it, I could have long term lung damage and other issues that affect my quality of life. Because vaccines are given to healthy people (unlike medications for treating a disease that is already present) they are held to a much higher standard for approval. My risk of having a significant adverse reaction from the Covid vaccine is minuscule in comparison to my risk with Covid. In fact, there have been no severe reactions to the Pfizer or Moderna vaccine to date.
For the rest of the population (outside of healthcare workers or those in nursing homes), who will likely be able to get the vaccine in February or March, there will be even more time passed and more people who have received the vaccine to be the "guinea pigs" here.
Anyone who is pregnant - it has not yet been tested in your group (although I do know that many pregnant front line health care workers are planning to take it). For those under 18 years old - it is also not yet tested. Moderna will be starting a trial shortly. Hopefully it will be approved by summer. But for everyone else, I highly recommend getting it as soon as you can; for you, for your loved ones, for those who cannot (perhaps because they are immunocompromised), for the many businesses that are on the verge of permanent shut down, and for kids to safely return to schools. I will be rolling up my sleeve for it as soon as it is offered.
If you'd like, please do feel free to cut and paste on your own social media sites. Sharing of information is so important to combating this pandemic. We have now surpassed 15 million documented Covid cases in our country (5 million of which were in the last 30 days) and over 2,000 people are dying per day. I do not plan on making the post shareable, as I don't need militant anti-vaxers tracking me down.
Samara Friedman, M.D.
Orthopaedic Surgery
(While, I am not an expert in vaccines, as a physician, I do have the necessary skills to interpret medical studies and evaluate data. Additionally, I have been listening to the experts in virology, infectious disease, and epidemiology.)
24 notes
·
View notes
Text
Vaccine hesitancy, molecular mimicry, and blood clots (oh my!)
There were many mixed messages in the world of coronavirus last week. Just as it appears that Michigan is the lead state in the fourth wave of the virus, the US is about to hit a “vaccine wall” as demand drops for vaccinations even though the supply is greatly improved. In the first three months of the rollout for the Pfizer, Moderna, and the Johnson & Johnson/Jantzen (J&J) vaccines, getting shots into arms of the most vulnerable has required a full court press from public health departments and the healthcare establishment, as well as persistence on the part of those trying to wrangle an appointment. The results from state to state have been uneven.
Figure 1

So far 14 states have administered fewer than 75% of the doses distributed to them with Alabama having the lowest vaccination rate per capita. Twenty states have administered more than 80% of the doses distributed to them with the most vaccinations per capita in New Hampshire.[1]
Vaccine Hesitancy:
The good news for those who want to get vaccinated is that it is a whole lot easier to get an appointment now. That said, the goal of herd immunity is a long way off and with demand dropping for jabs, we may not get there. Vaccine hesitancy is an important reason for declining demand and that is a shifting picture.
In a study that was put out by the Kaiser Family Foundation (KFF) in December, 52% of Black Americans said they would “wait and see” before signing up for the vaccine while only 20% said they wanted the shot as soon as possible. The share of Black people who were skeptical of the vaccines was higher than for White respondents (36%) and Latinx (43%).[2]
By March of this year, 55% of Black respondents to another KFF survey said they had been vaccinated or wanted the vaccine as soon as possible. Twenty-four percent were still holding back. Blacks have been one of the hardest hit demographics of COVID-19 and that has, no doubt, played a part in changing minds. Another possible reason for the turnaround in willingness to get vaccinated is because there has been a concerted outreach effort tapping trusted sources such as Barack Obama, sports stars, and other influencers such as Black ministers to address vaccine hesitancy among Black people.
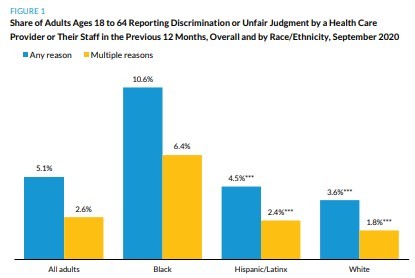
The Urban Institute’s September 2020 Coronavirus Tracking Survey, a nationally representative survey of adults ages 18-64, asked people whether in the last 12 months they had ever felt a doctor, other health care provider, or their staff judged them unfairly or discriminated against them based on their race/ethnicity, gender, gender identity, sexual orientation, a disability, or a health condition and about the consequences of these experiences. This survey indicated that perceptions of discrimination and unfair judgement while seeking health care were higher among Black adults than among Hispanic and White adults in the previous 12 months (September 2019-September 2020).[3]
Figure 2
A “food desert” is described as an urban area that does not have a grocery store within one mile or a rural area that does not have one within ten miles. There is also a “pharmacy desert” that generally occurs in primarily Black neighborhoods in urban areas as well as in rural areas. People of color are less likely to have a family primary care provider and so access to information about the individual’s risks and benefits of getting vaccinated from a trusted source, much less getting an appointment for the vaccine itself, is often more challenging than it is for White people. My guess is that these experiences and the barriers to appropriate care contributed to the initial skepticism among people of color generally and Black people specifically in the initial rollout phase.
FIGURE 3
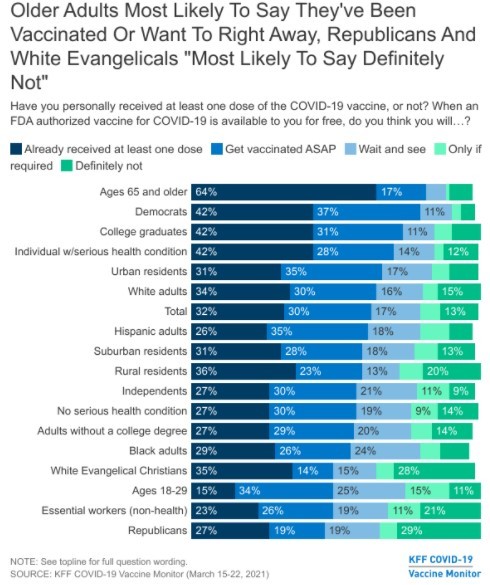
Meanwhile, Republicans and Evangelical Christians were the most likely groups to say they will not get vaccinated, according to the KFF survey.[4] I do not have an explanation for that. I also don’t know how wearing masks got politicized last year. If anyone has an explanation that doesn’t involve a gang of Democratic, cannibal pedophiles, I am really interested in hearing it.
Molecular mimicry and autoimmune disease:
There are science-based reasons that some are reluctant to get vaccinated. An issue that has been little discussed publicly is molecular mimicry. The theory is that some part of the spike protein of SARS-CoV-2, the virus that causes COVID-19 and is replicated in our cells, is similar enough to our own tissues that the immune system starts attacking our own cells thinking that those cells are the virus. Thus, the vaccine could trigger an autoimmune disease like rheumatoid arthritis, lupus, multiple sclerosis, or other autoimmune condition.
In one study looking for similar protein sequences between the SARS-CoV-2 virus with protein sequences in humans and other mammals, as well as other human coronaviruses, the number of shared protein sequences at two particular sites was quite high for humans, rats, and mice but miniscule or not at all with other human coronaviruses, cats, dogs, rabbits, chimpanzees, gorillas, or macaques.[5] Sadly, the investigators did not include bats, which I think of as flying rats, but that’s just me. It has been hypothesized that the original source of COVID-19 was from bats. Could the virus have molecular mimicry with bats? If so, what does that mean for the species?
These authors believe that much of the damage seen in the “cytokine storm” that causes the worst damage in COVID-19 may, in fact, be due to this molecular mimicry between the virus and, for example, lung tissue. It should also be noted that molecular mimicry from the whole SARS-CoV-2 virus is much more likely than it is from a small part of the virus (the spike protein). If the vaccine can trigger an autoimmune disease, so can the whole virus.
The presence and level of autoantibodies (AAbs) that attack our own cells, frequently detected in patients with COVID-19, are significantly associated with hospitalization and more severe prognosis. Clinically, these patients are more likely to have respiratory distress, acute cardiac injury, acute kidney injury, multi-organ dysfunction with such common complications as coagulopathy and thrombocytopathy (put a pin in this one as it is also at play with blood clots). [6]
Blood Clots and the J&J and AstraZeneca (AZ) vaccines:
Last week the J&J vaccine rollout was put on pause by the Food and Drug Administration (FDA) because six women developed unusual blood clots after receiving this vaccination. This was six out of seven million shots given. Some saw this as an over-reaction by the FDA that would likely lead to more vaccine hesitancy. However, these blood clots are different from clots that occur from “the usual suspects” like oral contraceptives and smoking.
Figure 4
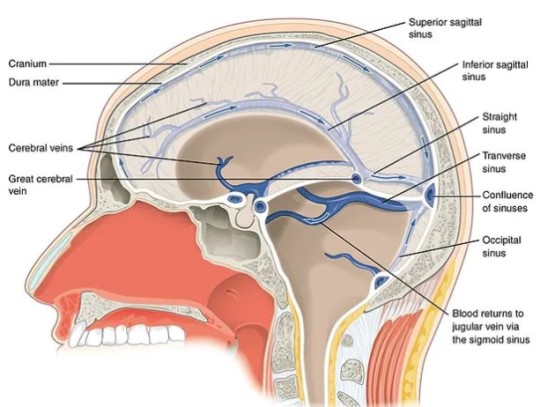
A normal number of platelets is between 150,000-450,000 per microliter of blood (there are 1,000 microliters in one milliliter). If you have less than 150,000 platelets per microliter, you have a deficiency called thrombocytopenia. In the clots associated with the viral vector vaccines (J&J in the US and AZ in Europe), the platelets tend to stick together in the veins of the brain, which causes a blockage known as a cerebral venous system thromboembolism (CVST). This creates back pressure of blood in the brain itself, causing damage in the same way a hemorrhagic stroke would. [7]
“Normal” clots are usually treated with a blood thinner called heparin. With vaccine-induced prothrombotic immune thrombocytopenia (VIPIT), there is a deficiency of platelets and so that treatment would only make things worse. While the Centers for Disease Control and Prevention (CDC) and the FDA are getting the word out to doctors not to use heparin, they are also looking for ways of figuring out which people are more at risk for this extremely rare complication. Putting the vaccine on pause was clearly the ethical thing to do and this kind of transparency gives me greater confidence in the vaccine rollout.
As is the case with molecular mimicry, the danger of VIPIT happening if a person gets COVID-19 is much higher than it is from either the J&J or the AZ vaccine.
“…If the mechanism is the same, one can speculate that the high occurrence in COVID-19 vs. vaccination is because the whole virus is more thrombogenic [likely to cause clots] than the spike protein alone.” Paolo Madeddu, professor of experimental medicine at the University of Bristol[8]
Symptoms associated with VIPIT include headache, tiny red spots under the skin, blurred vision, fainting or loss of consciousness, impaired movement in parts of the body, or coma. With either of these vaccines these blood clots, so far, only occurs 4-20 days after vaccination. Scientists believe that symptoms before or after that window are likely due to another cause.
It is important to note that COVID-19 itself has been reported to lead to thrombocytopenia (low blood platelets) in up to 41% of positive patients, with the figure going up to 95% of those with severe disease.[9]
Cause for cautious optimism:
Two separate studies published in the New England Journal of Medicine on April 9 indicated that in the case of the AZ vaccine, used in Europe, VIPIT was due to rogue antibodies against platelet factor 4 (PF4). This complication is similar to heparin-induced thrombocytopenia (HIT) and is diagnosed and treated the same way. It can be diagnosed with a lab test called ELISA that is pre-treated with PF4. If there is a big immune response, that means the patient has VIPIT. To be clear, there are lots of things that can cause blood clots and health professionals want to know what the cause is because the appropriate treatment is dependent on what is causing the problem. VIPIT from the AZ vaccine is treated with the administration of intravenous immunoglobins (IVG) and anti-coagulants. The J&J vaccine was not used in either of these studies and so we do not yet know if the same is true for that vaccine, but both are the same type of (viral vector) vaccine and both use an adenovirus as the viral vector.[10]
If we can get the one-and-done J&J vaccine back in use safely, that would be especially helpful for vaccinating unsheltered people. It would also be much easier to use in rural areas because J&J can be stored in a regular refrigerator unlike the Pfizer and Moderna vaccines that must be kept frozen.
My take:
For those who choose not to get vaccinated, for whatever reason, hoping to ride the coronavirus out, you should know that even without a vaccine, the SARS epidemic that hit Asia in 2002 did eventually go away, or, more likely, mutated to a less lethal virus. It took four years, but it can happen. However, that is not what always happens. Case in point, smallpox, which was around since at least the fourth century until it was declared eradicated by the World Health Organization in 1980. I don’t think I know anyone who has had smallpox and I may not know anyone who knows anyone who has had smallpox. In that case, the vaccine worked as intended.
Maybe you may feel like you are strong and healthy and even if you got COVID-19, you are unlikely to get significantly sick. Consider the possibility that you could be asymptomatic but still spread the disease. There are just no options that are completely risk free. Choose wisely.
[1]Romeo, A. (4/15/2021). America is about to hit a “vaccine wall” as demand drops—with or without Johnson & Johnson, Yahoo News.
[2]Bunn, C. (4/12/2021). Vaccine hesitancy among Black Americans has turned a corner. Here’s why.”, NBC News.
[3]Gonzalez, D., Skopor, L., McDaniel, M., Kenney, G.M. (4/2021). Perceptions of discrimination and unfair judgement while seeking health care, findings from the September 11-28 Coronavirus Tracking Survey, Urban Institute Health Policy Center. Retrieved from: https://www.urban.org/sites/default/files/publication/103953/perceptions-of-discrimination-and-unfair-judgment-while-seeking-health-care_0.pdf
[4] Hamel, L., Lopez, L., Kearney, A., Brodie, M.(3/30/2021) KFF COVID-19 monitor: March 2021. Retrieved from: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-march-2021/
[5]Kanduc, D., Shoenfeld, Y. (9/18/2020). Molecular mimicry between SARS-CoV-2 spike glycoprotein and mammalian proteomes: implications for the vaccine, Immunol. Res. doi: 10.1007/s12026-020-09152-6
[6]Macela, A, Kubelkovak, K. (3/22/2021). Why does SARS-Co-V-2 infection induce autoantibody production? Pathogens, 10(3). doi: 10.3390/pathogens10030380
[7]Taylor, A. (4/16/2021). Blood clot risks: comparing AstraZenica vaccine and the contraceptive pill, The Conversation. Retrieved from: https://theconversation.com/blood-clot-risks-comparing-the-astrazeneca-vaccine-and-the-contraceptive-pill-158652
[8]Russell, P. (4/15/2021). Vaccines carry far lower risk for rare blood clots than COVID, study shows, Medscape News UK
[9] Op cit Taylor, A. (4/9/2021).
[10] Grenacher, A., et. al. (4/9/2021). Thrombocytic thrombocytopenia after ChAdOx1 nCoV-19 vaccination, NEJM. doi:10.1056/NEJMoa2104840Schulz,NH, et. al. (4/9/2021). Thrombocytic thrombocytopenia after ChAdOx1 nCoV-19 vaccination, NEJM. doi: 10/1056/NEJMoa2104882
#vaccination#covidー19#astrazeneca vaccine#johnson and johnson#blood clots#molecular mimicry#autoimmune disease
4 notes
·
View notes
Text
COVID VACCINE HESITANCY?
The FDA is likely going to approve the Pfizer Covid vaccine when they meet on December 10th. The Moderna vaccine will probably be approved shortly thereafter. This is an incredible feat of modern medicine, and our best chance to hopefully get our lives back to near normal relatively soon. However, it is new and it was done quickly, so understandably, people may be hesitant to get it; even people who vaccinate against all other diseases.
Will I be getting the vaccine? ABSOLUTELY. As a physician, I will probably have the opportunity to be immunized prior to New Year's and yes, I will be taking it as soon as possible.
But, it is a new vaccine technology and done in record time, so aren't I worried about its safety? Nope, not any more so than any other vaccine or other medical intervention.
Why? Let's start with how this vaccine works. This is an mRNA vaccine. Past vaccines typically use a live but weakened "attenuated" virus, or dead viral material "inactivated" virus, or a piece of the virus's protein or even a toxin produced by the virus. The Covid vaccine is very different. It contains mRNA (messenger genetic material) that encodes for the Covid spike protein. This causes your cells to then produce the Covid spike protein. In contrast, when you are sick with Covid, the virus hijacks your cell to produce many copies of the entire virus. Then it destroys the cell, busting it open to release its newly formed viral particles. When your cells release just the spike protein, it will stimulate your immune system to form antibodies to the Covid spike protein without you getting sick. There is no possibility of getting Covid from the vaccine. When your body is subsequently exposed to Covid, it will quickly recognize the spike protein and destroy it before it can make you sick. This was 95% effective in preventing Covid, which is an even better percentage than most other vaccines. However, you must take both doses (about 3-4 weeks apart).
Am I concerned about it being new? And previously untested? No, I'm not. This type of technology is not entirely new. It has been studied and used in cancer research. They have been making mRNA vaccines and studying them to specifically target proteins on tumor cells and train your immune system to then destroy the tumor. In this case, it is not a vaccine in the preventive sense, as it is targeted to a tumor that you already have. It is not currently widespread because it has to be custom made for each tumor. But, it has been "around the block" for a while now. The technology was also being studied for other Coronaviruses. It never came to fruition, because the diseases never reached pandemic proportions, and then the funding dried up. The mRNA does not enter the nucleus of the cell, and it does not affect your DNA, and therefore has no lasting impact on your cell.
Am I concerned about the speed with which it was developed? Weren't significant corners cut in order to get this out so quickly? No and no. What was cut out of the equation was mostly red tape, and what was added was technology and funding. We were given the genetic code by scientists in China to start vaccine production in January; before Covid was even documented to have reached our shores. From there, the vaccine was developed from the technology we had from the prior Coronavirus and cancer research, and was completed in March. Normally, there would be months of waiting for the FDA to even look at the work done prior to approving Phase 1 trials. Because of the urgent nature of this, it was essentially put on the top of the wait pile, which cut out months of waiting, but did not cut any corners. Between the Moderna and Pfizer vaccines (both mRNA, with a slightly different delivery system), they were tested in 37,000 people in Phase 3 (and an additional 37,000 received a placebo). That is on par with, if not better than the vaccines currently available.
Aren't I concerned that the FDA is about to approve it, and there may be side effects that haven't been seen yet? Nope on this one too. We know from decades of vaccine research, since you typically just get 1, 2 or 3 doses and then you are done with it, that nearly all side effects from vaccines occur in the first 6 weeks. Like other vaccines, minor side effects may occur(soreness at injection site, muscle aches, fever). Severe adverse reactions are extremely rare, and again, occur quickly if they are going to occur at all. As a healthy 40-something year old woman, my risk of dying from Covid is about 1 in 250 to 1 in a 1,000. That is not a rare event! And even if I don't die from it, I could have long term lung damage and other issues that affect my quality of life. Because vaccines are given to healthy people (unlike medications for treating a disease that is already present) they are held to a much higher standard for approval. My risk of having a significant adverse reaction from the Covid vaccine is minuscule in comparison to my risk with Covid. In fact, there have been no severe reactions to the Pfizer or Moderna vaccine to date.
For the rest of the population (outside of healthcare workers or those in nursing homes), who will likely be able to get the vaccine in February or March, there will be even more time passed and more people who have received the vaccine to be the "guinea pigs" here.
Anyone who is pregnant - it has not yet been tested in your group (although I do know that many pregnant front line health care workers are planning to take it). For those under 18 years old - it is also not yet tested. Moderna will be starting a trial shortly. Hopefully it will be approved by summer. But for everyone else, I highly recommend getting it as soon as you can; for you, for your loved ones, for those who cannot (perhaps because they are immunocompromised), for the many businesses that are on the verge of permanent shut down, and for kids to safely return to schools. I will be rolling up my sleeve for it as soon as it is offered.
If you'd like, please do feel free to cut and paste on your own social media sites. Sharing of information is so important to combating this pandemic. We have now surpassed 15 million documented Covid cases in our country (5 million of which were in the last 30 days) and over 2,000 people are dying per day. I do not plan on making the post shareable, as I don't need militant anti-vaxers tracking me down.
Samara Friedman, M.D.
Orthopaedic Surgery
(While, I am not an expert in vaccines, as a physician, I do have the necessary skills to interpret medical studies and evaluate data. Additionally, I have been listening to the experts in virology, infectious disease, and epidemiology.)
3 notes
·
View notes
Text
Classifying the COVID-19 diagnostic tests and vaccinations underdevelopment and/or already available nowadays based on their DNA or RNA structure
“SARS-CoV2”, a previously unknown strain of coronaviruses caused a severe respiratory disease called Coronavirus disease (COVID-19) which emerged from Wuhan city of China on 30 December 2019, and declared as Global health problem by World Health Organization within a month. In less than two and half months (11 March, 2020)

Diagnosis of COVID-19
A rapid and sensitive diagnosis of COVID-19 is still unavailable, although some diagnosis methods are available presently (Fig. 1) for virus detection, each having different degree of specificity and based on single or multiple target molecule from the SARS-CoV2. (Kumar, R., Nagpal, S., Kaushik, S. et al.)
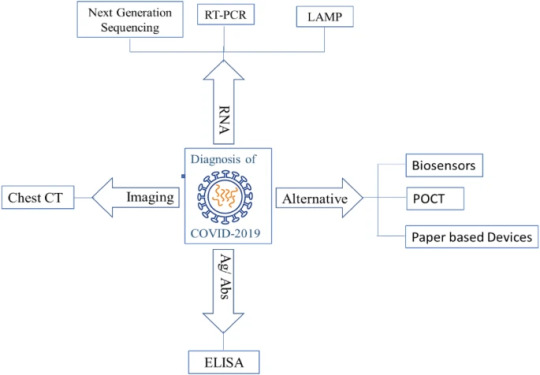
Nucleic acid based method
Nucleic Acid based technologies are utilizes the genetic material such as DNA/RNA and are based on the principle of their highly specific base paring with homologous strands. Genetic materials-based detection and diagnostics are comparatively faster than traditional culture-based methods ( Kumar, R., Nagpal, S., Kaushik, S. et al.)
Next generation sequencing (NGS)
The, next-generation sequencing (NGS) is also called as high-throughput sequencing (HTS). By this method we can determine the genomic sequence, even more than 1 million base pairs in a single experiment. By this technique, we can diagnose the inheritable diseases, cancer, and infectious diseases even Covid-19 ( Kumar, R., Nagpal, S., Kaushik, S. et al.)
Treatment for Covid-19
There has been progress in getting treatment for COvid-19 in a form of a vaccine this was found by the mRNA-1273 Study Group from The New England journal of medicine they found:
After the first vaccination, antibody responses were higher with higher dose (day 29 enzyme-linked immunosorbent assay anti–S-2P antibody geometric mean titer [GMT], 40,227 in the 25-μg group, 109,209 in the 100-μg group, and 213,526 in the 250-μg group). After the second vaccination, the titers increased (day 57 GMT, 299,751, 782,719, and 1,192,154, respectively). After the second vaccination, serum-neutralizing activity was detected by two methods in all participants evaluated, with values generally similar to those in the upper half of the distribution of a panel of control convalescent serum specimens. Solicited adverse events that occurred in more than half the participants included fatigue, chills, headache, myalgia, and pain at the injection site. Systemic adverse events were more common after the second vaccination, particularly with the highest dose, and three participants (21%) in the 250-μg dose group reported one or more severe adverse events this lead them to conclude that the mRNA-1273 vaccine induced anti–SARS-CoV-2 immune responses in all participants
(The mRNA-1273 Study Group,2020)

What does RNA research got to do with Covid-19
A graphic created by the New York Times illustrates how the coronavirus that causes COVID-19 enters the body through the nose, mouth, or eyes and attaches to our cells. Once the virus is inside our cells, it releases its RNA. Our hijacked cells serve as virus factories, reading the virus’s RNA and making long viral proteins to compromise the immune system. The virus assembles new copies of itself and spreads to more parts of the body and—by way of saliva, sweat, and other bodily fluids—to other humans. (University of Rochester,2020)
This means that Covid-19 Spreads it selves through our body's through the release of its RNA this is why the research of RNA is important to the treatment of Covid-19 it is also why we are developing RNA based vaccines but how do they work?
RNA-based vaccines—such as those developed by Pfizer/BioNTech and American biotechnology company Modern—do not introduce an antigen, but instead inject a short sequence of synthetic messenger RNA (mRNA) that is enclosed in a specially engineered lipid nanoparticle. This mRNA provides cells with instructions to produce the virus antigen themselves. Once the mRNA from a vaccine is in our body, for example, it “instructs” the protein synthesis machinery in our cells, which normally generates proteins from the mRNAs that derive from our genes, to produce a piece of the SARS-CoV-2 virus spike protein. Since the SARS-CoV-2 virus spike protein is foreign to our bodies, our bodies will then make antibodies that inactivate the protein (University of Rochester,2020)
An RNA-based vaccine therefore acts as a code to instruct the body to make many copies of the virus protein—and the resulting antibodies—itself, resulting in an immune response. (University of Rochester,2020)
I had trouble understanding the basics but I just watched a video that I think explains it, could someone tell me if the following explanation is accurate?
1.There is a protein that is part of the virus that we would like our antibodies to target.
2.The vaccine introduces mRNA into our bodies that codes for that protein.
3.Our body's ribosomes read off the mRNA and create that protein as they would for any other mRNA.
4.The body's immune response then targets this foreign protein.
5.When live virus is introduced, the body's antibody response knows how to target this foreign protein.
6.It is less dangerous than attenuated virus because the full virus is never created -- just the single protein.
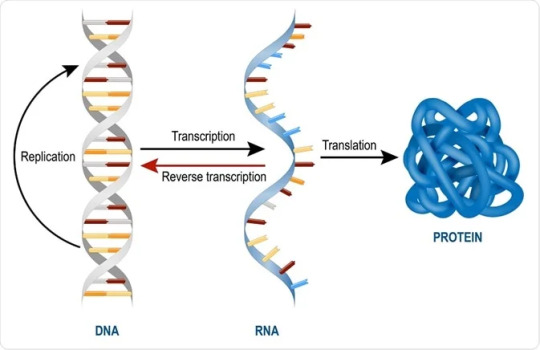
7.It also doesn't require any sort of genetic manipulation because there is no transcription or reverse transcription, mRNA is introduced as already transcribed.
Conclusions.
The importance of understanding of understanding of doing research specially on such relevant issues such as covid-19 is extremely important before this I knew next to nothing that's obviously why I failed but after doing this i know more about Covid knowing more makes me understand why people are being victims to fear mongering about the vaccine as humans we fear the unknown. It is our responsibility to get educated about topics like this not only to enrich ourselves with knowledge but to literally saves lives by taking decisions such as being vaccinated against the disease. I definitely understand more about How Covid uses RNA to spread itself through out our body and why we need to combat it with its own RNA based vaccine. Its easy to see the connection to what we saw in class considering how everything to do with covid and its treatment is based on RNA
REFERENCES
Deutsche Welle (www.dw.com). (n.d.). What’s the science on DNA and RNA vaccines? DW.COM. Retrieved January 22, 2021, from https://www.dw.com/en/whats-the-science-on-dna-and-rna-vaccines/a-54097063
Kumar, R., Nagpal, S., Kaushik, S., & Mendiratta, S. (2020, June 13). COVID-19 diagnostic approaches: different roads to the same destination. VirusDisease. https://link.springer.com/article/10.1007/s13337-020-00599-7?error=cookies_not_supported&code=86e493fb-130e-4c77-845c-e3cc75756fa7#citeas
RNA Science and its Applications—a look toward the future: Albany, NY USA, November 3–4, 2011. (2012, August 1). PubMed Central (PMC). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3551859/
Schmidt, C., & Schmidt, C. (2020, June 1). Genetic Engineering Could Make a COVID-19 Vaccine in Months Rather Than Years. Scientific American. https://www.scientificamerican.com/article/genetic-engineering-could-make-a-covid-19-vaccine-in-months-rather-than-years1/?error=cookies_not_supported&code=102d1714-09e6-452d-b816-45c765f7aa1c
T.R.N.A.-S.G. (2020, November 12). An mRNA Vaccine against SARS-CoV-2 — Preliminary Report. The New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/nejmoa2022483
Valich, L. (2020, December 22). COVID-19 vaccine: What’s RNA research got to do with it? NewsCenter. https://www.rochester.edu/newscenter/covid-19-rna-coronavirus-research-428952/
1 note
·
View note
Text
https://www.aier.org/article/an-education-in-viruses-and-public-health-from-michael-yeadon-former-vp-of-pfizer/
➖➖➖Dr. Michael Yeadon is an Allergy & Respiratory Therapeutic Area expert with 23 years in the pharmaceutical industry. He trained as a biochemist and pharmacologist, obtaining his PhD from the University of Surrey (UK) in 1988.
Dr. Yeadon then worked at the Wellcome Research Labs with Salvador Moncada with a research focus on airway hyper-responsiveness and effects of pollutants including ozone and working in drug discovery of 5-LO, COX, PAF, NO and lung inflammation. With colleagues, he was the first to detect exhaled NO in animals and later to induce NOS in lung via allergic triggers.
Joining Pfizer in 1995, he was responsible for the growth and portfolio delivery of the Allergy & Respiratory pipeline within the company. He was responsible for target selection and the progress into humans of new molecules, leading teams of up to 200 staff across all disciplines and won an Achievement Award for productivity in 2008.
Under his leadership the research unit invented oral and inhaled NCEs which delivered multiple positive clinical proofs of concept in asthma, allergic rhinitis and COPD. He led productive collaborations such as with Rigel Pharmaceuticals (SYK inhibitors) and was involved in the licensing of Spiriva and acquisition of the Meridica (inhaler device) company.
Dr. Yeadon has published over 40 original research articles and now consults and partners with a number of biotechnology companies. Before working with Apellis, Dr. Yeadon was VP and Chief Scientific Officer (Allergy & Respiratory Research) with Pfizer.
Below is a transcript of the video above:
My name is Dr Michael Yeadon.
My original training was a first-class honours degree in biochemistry and toxicology. Followed by a research-based PhD into respiratory pharmacology; and after that I’ve worked my entire life, uh, on the research side of the pharmaceutical industry – both big pharma and also biotech. My specific focus has been inflammation, immunology, allergy in the context of respiratory diseases (so the lung, but also the skin). So I would say I’m a kind of a deeply experienced inflammation, immunology, pulmonology kind of research person.
I initially became concerned about, the, our response to the coronavirus pandemic towards the middle or back end of April as early as that. It had become clear that if you look at the number of daily deaths versus the date the pandemic had turned. Really, pleasingly, already the wave was fundamentally over, and we would just watch it fall for a number of months – which is what it did. And so I became very perturbed about increasing restrictions on the behavior and movement of people in my country and I could see no reason for it then and I still don’t.
Government’s response to emergencies is guided by the scientific group who sit together under the Scientific Advisory Group for Emergencies or SAGE. So they should provide scientific advice to the government about what’s appropriate to do. SAGE has got several things wrong, and that has led to advice that’s inappropriate and – uh, not only has had horrible economic effects, but has had continuing medical effects in that people are no longer being treated properly.
SAGE took the view that since SARS-CoV-2 was a new virus that they believed there wouldn’t be any immunity at all in the population. So, I think that’s the first thing. I remember hearing that and I puzzled, because I already knew – because I read the scientific literature that SARS-CoV-2 was 80% similar to another virus you may have heard of called SARS that moved around the world a bit in 2003, and more than that: it’s quite similar, in pieces of it, to common cold-causing coronaviruses.
So, when I heard that there was this coronavirus moving across the world I wasn’t as worried as perhaps other people were, because I figured that since there are four common cold-causing coronaviruses, I figured that quite a lot of the population we’ve been exposed to one of those viruses, and would probably have a perhaps substantial protective immunity. And just to explain why I was so confident everybody knows the story of Edward Jenner and vaccination, and the story of cowpox and smallpox. And that the old story was that milkmaids had very, uh, clear complexions: they never suffered from things like smallpox, that if it didn’t kill you would leave your skin permanently scarred. And the reason that they had the protection was that they were exposed to a more benign, related virus called cowpox.
Edward Jenner came up with the idea that if it’s cowpox that saves the fair maid – he reasoned that if he could give another person an exposure to the cowpox, he would be able to protect them from smallpox. Now, he did an experiment that you can’t do now – and he never should have done it – but apocryphally, or really, or maybe you’re ill, we’re not sure. Edward Jenner acquired some of the liquid from a person infected with cowpox. Relatively mild pustules that then go away. And he got some of this and he – he scraped it into the skin of a small boy and a few weeks later, he obtained some liquid from some poor person that was dying of smallpox and infected the boy. And, lo and behold, the boy did not get ill and that gave birth to the whole field of what’s called vaccination. And vax, the vaccine’s “vac.” It comes from “vaccus,” the Latin name for cow. So, we are really familiar with the principle of cross immunization.
I’ve thought quite a lot about, you know, the vulnerable people in in care homes and there’s an awareness that, even though people really careful using PPE and so on, but that’s only going to go so far in a kind of, hot house environment where people are pretty close together in a care home. So the question I’ve had all year is: once one or two people, you know, got the virus in a care home, why wouldn’t almost everyone get infected? And of course the truth is, they didn’t. And one interpretation of that distinction is that a large proportion of people in the care homes had prior immunity.
At this time of year, about 1 in 30 people have a cold, caused by one of these coronaviruses. And just like the protection against smallpox provided by previous exposure to cowpox, so people exposed to having had a cold caused by one of these coronaviruses they’re now immune to SARS-CoV-2. So, 30% of the population was protected before the start. SAGE said it was zero – and I don’t understand how they could possibly have justified that. There’s a second, and equally fatal, unaccountable error that they have made in their model. The percentage of the population that SAGE asserts have been infected to date by the virus is about seven percent. I know that that’s what they believe and you can see it in a document they published in September called “Non-pharmaceutical interventions” and it says sadly more than 90% of the population is still vulnerable.
It’s unbelievably wrong. And I’m just going to explain why: they’ve based their number on the percentage of people in the country who have antibodies in their blood. And only the people who became most ill needed to actually develop and release antibodies around their body. So, it is certainly true that the people who have lots of antibodies were infected. But a very large number of people had milder symptoms, and even more people had none at all. And the best estimates that we can arrive at is that those people either made no antibodies, or so low amounts that they will have faded from now.
A recent publication on the percentage of care home residents who have antibodies to the virus very, very interesting. This time they were using high sensitivity tests for antibodies and they carefully picked out residents that never were PCR-positive: these are people who never got infected. And they found that 65% of them had antibodies to the virus; they never got infected. So I believe there was high prevalence of immunity in that population prior to the virus arriving. Big story in the media, recently, was that the percentage of people with antibodies against the virus in their blood was falling. Now, this was cast as a concern that immunity to SARS-CoV-2 doesn’t last very long. Well, you know, anyone with knowledge of immunity would – would just simply reject that. It’s not the way immunity to virus works – that would be T-cells. So, if the antibodies are falling gradually over time – which they have – from spring to present, the only plausible explanation is that the prevalence of the virus in the population is falling, and that’s why the antibody production gradually subsides.
Less than 40% of the population are susceptible. Even theoretical epidemiologists would tell you that that’s too small a number to support a consolidated and growing outbreak, community immunity, herd immunity. So, SAGE says that we’re not even close, and I’m telling you that the best science, by the best scientists in the world, published in the top peer-reviewed journals, says they’re wrong: that more than 60 of the population are now immune, and it’s simply not possible to have a large and growing pandemic.
Really good news, genuine good news, to hear that there’s data emerging from the vaccine clinical trials, and we are seeing vaccines that raise not just antibodies – but they’re also producing T-cell responses. This is great; back to proper science, proper immunology. That’s how immunity to viruses works. So, my surprise though, and it’s just annoying that when we’re talking about, uh, the percentage of the population that’s still susceptible we only talk about antibodies, like seven percent from SAGE. Why are we not talking about the 50% that have got T-cell immunity?
And so you might be thinking if Mike – and Dr Mike Yeadon is telling you these things… – or how come the pandemic isn’t over? Well, this may come as a surprise to you, but I believe fundamentally it is over. The country has experienced almost a complete cycle now of the virus sweeping through the land, and we are at the end of it. London was –was horribly affected in the spring, and somewhere in early April they were experiencing several hundred deaths per day from people dying with similar symptoms in respiratory failure and, uh, inflammation. And at the moment the number of people dying of SARS-CoV-2 in the capital is less than 10. So it’s down by 98, or something like that. And, the reason it’s down, is because there are now too few people in London susceptible to allow the virus to magnify, to amplify, to get an epidemic. And, and they would have been hit by now, because they were the first place hit in the spring. And I think what we’re seeing now in the Northeast and the Northwest would be the dying embers of the spreading out of this virus. And I’m very sorry that it is still true, that a small number of people are catching it, getting ill, and dying.
So why aren’t the media telling us that the pandemic is over? It’s not over because SAGE says it’s not. So SAGE consists of very many scientists, from a range of disciplines – mathematicians and clinicians – and there are multiple committees. But I found to my surprise – and I’m actually going to use the word – horror, that in the spring, all the way through the spring and summer, SAGE did not have on their committee someone who I would call a card-carrying immunologist; a clinical immunologist. I have to say I think that in the spring and summer SAGE was deficient in the expertise it had. They should have armed themselves, you know, with – around the table all the people required to to understand what was happening, and they didn’t do that. People asked me then, “Well Mike, if it’s, you know, if it’s fundamentally over, why are we still getting hundreds of deaths a day from SARS-CoV-2?” And I’ve thought a lot about this. There is a test that’s performed where people have their noses and tonsils swabbed, and then a test (called a PCR test) is performed on that. And what they’re looking for isn’t the virus – you might think it’s looking for the virus, but it’s not. What they’re looking for is a small piece of genetic sequence; it’s called RNA. Unfortunately, that bit of RNA will be found in people’s tonsils and nose not if they’ve just caught the virus, and they’re about to get ill, or they’re already ill. It’s also going to be found if they were infected previously weeks – or even, sometimes, a small number of months ago. Let me just explain why that is.
If you’ve been infected, and you’ve fought off the virus (which most people do), you’ll have broken, dead bits of virus. These are tiny things smaller than your cells, perhaps spread all the way through your airway, embedded in bits of mucus, maybe inside an airway lining cell. And so over a period of weeks or months you bring up cells that contain broken, dead pieces of the virus that you have conquered and killed. However, the PCR test is not able to detect whether the viral RNA has come from a living virus or a dead one (as I’ve just described). So I think a large proportion of the so-called positives are, in fact, what I call “cold” positives: they’re correctly identifying that there is some viral RNA in the sample – but it’s from a dead virus. It can’t hurt them, they’re not going to get ill, they can’t transmit it to anybody else. So they’re not infectious. So that accounts for a large number of the so-called positive cases. These are people who’ve beaten the virus. Why are we using this test that cannot distinguish between active infection and people who’ve conquered the virus?
This test has never been used in this way – and I’ve worked in this field. It’s not a suitable technique it’s a – it’s the kind of technique you would use for forensic purposes, if you were trying to do a DNA test to establish whether or not a person was at the scene of a crime. You would not be doing these tests by a windy, supermarket car parking; what looks like plastic marquee tents; on picnic tables. It’s not suitable at all – and it definitely shouldn’t be done in the way it’s been done. It’s subject to many mechanical errors, should we say, handling errors. If this was a test being used for legal purposes, for forensic purposes like a DNA identity test, the judge would throw out this evidence; would say it’s not admissible. It produces positives even when there’s no virus there at all. We call that a false positive.
As we’ve increased the number of tests done per day, so we’ve had to recruit less and less experienced laboratory staff – and now we’re using people who’ve never worked professionally in this area. What that does is it increases the frequency of mistakes, and the effect of this is that the false positive rate rises and rises. So, if you had a false positive rate of one percent – which Mr. Matt Hancock [British Secretary of State for Health and Social Care] told us was roughly the number they had in the summer – then if you tested a thousand people that had no virus ten of them would be positive, astonishingly. If the prevalence of the virus was only one in a thousand, that’s 0.1% – as the Office for National Statistics told us it was through the summer – then if you use the PCR test only one of them will be positive and genuinely so. But if the false positive rate is as low as one percent, you’ll also get 10 positives that are false.
Some people did say to me, “Well, there’ll be a higher percentage of people coming forward for testing in the community,” so-called “Pillar 2” testing, because they’ve been instructed only to come if they’ve got symptoms. But I call B.S. on that one. I don’t think that’s true. I know lots of friends and relatives who’ve been told by an employer, “Well, you’ve sat near someone who’s tested positive, and I don’t want you to come back to work until you’ve got a negative test.” I’ve seen information from many towns in the North – certainly Birmingham was one; Manchester was another; Bolton – where councils (and I really think they were trying to be helpful) were out leafleting the people of their cities saying, “We’re going to come round and swab you all because we want to track down this virus.” Now once you start testing people, more or less randomly, instead of [those] having symptoms you get the same amount of virus in the population as the Office of National Statistics found which is, at the time was, one in a thousand. And I’ve just told you Matt Hancock confirmed during the summer they had a false positive rate of about one percent. So that means out of a thousand people 10 would test positive, and it would be a false result, and only one would test positive and it was correct.
This test is monstrously unsuitable for detecting who has live virus in their airway. It’s subject to multiple distortions that are worsening as we get into the winter. As the number of tests done per day increase[s], the number of errors made by these overworked, not very experienced lab staff increase[s]. I think it’s not unreasonable to say a best guess of the false positive rate at the moment – what’s called the operational false positive rate is about five percent. Five percent of 300,000 is 15,000 positives. I think some of those positives are real; I don’t think it’s very many. Now, the problem with this false positive issue [is] it doesn’t just stop it at “cases”: it extends to people who are unwell and go to hospital. So people who go to hospital having tested positive – and it could be a false positive, and I think most of them are at the moment – if you go to hospital and you’ve tested positive previously, or you test positive in hospital, you’ll be counted now as a Covid admission.
Although there are more people in hospital now than a month ago, this is normal for autumn. Regrettably, people catch respiratory viruses and become ill, and some will die. I just don’t believe it’s got anything to do with Covid-19 anymore. There are more people in intensive care beds now than there were a month or so ago. That’s entirely normal as we move through late autumn into the early winter: those beds become used. But there aren’t more people than is normal for the time of year, and we’re not about to run out of capacity, certainly at a national level. But I think you know it is going now: if you should now die, you’ll be counted as a Covid death. But that’s not correct; these are people who might have – have gone to hospital having had a broken leg, for example, but they’ll – three percent of them will still test positive, and they’re not, they haven’t got the virus. It’s a – it’s a false positive, and if they die they’ll be called a Covid death – and they are not. They’ve died of something else.
One of the most troubling things I’ve heard this year was Mr. Johnson telling us about the “Moonshot” testing everybody often, maybe every day, is the way out of this problem. I’m telling you it’s the way to keep us in this problem: that number of tests is orders of magnitude higher than we’re already testing now, and the false positive rate (however low it is) will be far too large to accept. It will produce an enormous number of false positives.
What we should do is stop mass testing. Not only is it an affront to your liberty, it will not help at all: it will be immensely expensive and it will be a pathology all of its own. We’ll be fighting off stupid people – mostly government ministers – I’m sorry to say, who are not numerate, and do not understand statistics. If you test a million people a day with a test that produces one percent false positives, 10 000 people a day will wrongly be told they’ve got the virus. If the prevalence of the virus was say 0.1%, like the Office of National Statistics said it was in summer, then only a tenth of that number, uh, 1,000 would correctly be identified. But you can’t distinguish amongst the 11,000 who have genuinely got the virus and who are false positives. Moonshot, I think, will have a worse false positive rate. It’s not fixable, and it’s not necessary either. The pandemic – having passed through the population not only of, of the UK, but of all of Europe – and probably all of the world quite soon – it won’t return. Why won’t it return? Well, they’ve got T-cell immunity. We know this. It’s been studied by the best cellular immunologists in the world.
Sometimes people will say, “Well, it looks like the immunity is starting to fade.” You’ll sometimes see [statements] like that, and when I saw the first headline like this I remember being really quite confused, because that’s not the way immunology works. Just think about it for a moment. If that was how it worked it could kill you. When you had to fight it off, and if you had successfully done that, it somehow didn’t leave a mark in your body. Well, it does leave a mark on your body. The way you fought it off involved certain pattern recognition receptors, and has left you with – as it were – memory cells that remember what it was they fought off. And if they see that thing again it’s very easy for them to get those cells to work again in minutes or hours, and they will protect you. So the most likely explanation is it’ll last a long time.
So I read a bit more about this so-called tailing off of immunity – and I realized they were talking about antibodies. Just incorrect to – to think that antibodies, and how long they stay up, is a measure of immune protection against viruses. I mean you can tell I’m – I don’t agree with this. It says there have been some classic experiments done on people who have inborn errors in parts of their immune system, and some of them have inborn arrows that means they can’t make antibodies, and guess what: they – they are able to handle respiratory viruses the same as you and me. So, I don’t think it’s harmful to have antibodies, although some people are worried about the potential for amplifying inflammation from antibodies, but – but my view is that they’re – they’re probably neutral, and you definitely should not believe the story that because the antibody falls away you’ve lost immunity. Again, that’s just not the way the human immune system works.
The most likely duration of immunity to a respiratory virus like SARS-CoV-2 is multiple years. Why do I say that? We actually have the data for a virus that swept through parts of the world 17 years ago called SARS, and remember SARS-CoV-2 is 80% similar to SARS, so I think that’s the best comparison that anyone can provide. The evidence is clear. These very clever cellular immunologists studied all the people they could get hold of who had survived SARS 17 years ago. They took a blood sample, and they tested whether they responded or not to the original SARS, and they all did. They all have perfectly normal, robust T-cell memory. They are actually also protected against SARS-CoV-2 because it’s so similar, it’s cross-immunity. So, I would say the best data that exists is that immunity should be robust for at least 17 years. I think it’s entirely possible that it is lifelong. The style of the responses of these people’s T-cells were the same as if you’ve been vaccinated and then you come back years later to see, has that immunity been retained? And so I think the evidence is really strong that the duration of immunity will be multiple years, and possibly lifelong.
There have been but a tiny handful of people who appear to have been infected twice – now they’re very interesting, we need to know who they are and understand them very well, they’ve probably got certain rare immune deficiency syndromes. So I’m not pretending no one ever gets reinfected, but I am pointing out that it’s literally five people (or maybe 50 people), but the World Health Organization estimated some weeks ago that 750 million people have been infected so far by SARS-CoV-2. That means most people are not being reinfected, and I can tell you why that is: it’s normal. It’s what happens with viruses, respiratory viruses. Some people have – have called for “zero Covid” as if it’s some political slogan. And there are some people I’ve heard calling for it almost every day; they’re completely unqualified to tell you anything.
Something that’s really important to know is that SARS-CoV-2 – it’s an unpleasant virus. There’s no question about it, but it’s not what you were told in spring. We were originally told that it would kill perhaps three percent of people it infected – which is horrifying. That’s 30 times worse than flu. We always overestimate the lethality of new infectious diseases when we’re in the eye of the storm. I believe the true infection fatality ratio of Covid-19, the true threat to life is, the same as seasonal flu.
So there’s no reason why you would want to try and drive Covid to zero. It’s a nonsense – that’s just not how biology is. And all the means I have heard, uh, proposed, as ways to get us there are much more damaging and pathological, I would say, than than the virus itself. It’s simply not possible to get rid of every single copy of the Covid-19 virus, and the means to get you there would destroy society. Forget the cost – although it would be huge – it would destroy your liberty, you would need to not go out until you’ve been tested and have your result back. And I have described how the false positive rate would just destroy it from a statistical perspective. I don’t believe it can be done: it’s not scientifically realistic, it’s not medically realistic, and it’s not what we have ever done.
As the virus swept towards the UK in the – in the late winter and early spring I too was concerned, because at the time we were told perhaps three percent might die. So when the Prime Minister called for a lockdown I wasn’t pleased about it, but I understood that we should try this. But it’s important that you understand, that when we look at the profile of the pandemic as it passed through the population, that it was clear that the number of infections every day was falling. We’d passed the peak quite a long time before lockdown started. So we took all that pain, that locked down pain which was multiple weeks – I don’t remember exactly how many multiple weeks – we took it for nothing. If there was a really important effect of lockdown on the number of people who died, or the rate of it, you should at least be able to order them. Like, these people had locked down, and these didn’t – and you cannot. All heavily infected countries’ shapes are the same, whether they had locked down or not. They don’t work. I don’t know why anyone is allowing you, know you, to be pushed into this corner.
I don’t think we entirely know why it is that some countries were hit harder than others, but I have to say I think scientifically the smart money is on a mixture of forces. One would be this cross immunity. Although China had an awful time in Wuhan, in Hubei province, it didn’t spread elsewhere in the country, and I suspect that meant because a lot of them had this cross immunity. And I think nearby countries, in the main, had lots of cross immunity. So that’s one possibility. The other one, though, is in terms of the severity of what did the virus do to a particular population. We’ve seen devastating effects in countries like UK and in Belgium, uh, France, and maybe even in Sweden, and much smaller numbers of deaths in other countries like – like Greece and in Germany. And you might think, “Well, was that was it something that they did?” And I wish it was true, because if it was something we did we could learn from it and do it and it would work in the future. But there’s no evidence whatsoever that it was anything humans did. The passage of this virus through the human population is an entirely natural process that completely ignored our puny efforts to control it.
So there is this theory – I don’t like the name very much – but it’s called “dry tinder.” If people in a country who are vulnerable for to dying in the winter (usually of respiratory viruses), if you have a very mild winter season, like UK did – we had a very mild seasonal flu last year and the year before and so did Sweden – then what happens is there are larger number of very vulnerable people who are even older than usual, and – and I think that’s why we suffered a rather large number of deaths. It was still only 0.06% of the population, equivalent to about four weeks of normal mortality. But countries that had very severe winters recently, and Greece and Germany certainly had very lethal winter flus in the last two years. I think then, they had a smaller population of very vulnerable people, and that is the main reason why they lost fewer people. It’s not to do with locking down, it’s not to do with testing, or tracking, or tracing. I personally don’t think any of those measures have made any difference at all. So Belgium and UK and Sweden were particularly vulnerable, whereas adjacent Nordic countries – I – I get fed up with hearing about this, uh, idea that they locked down and that’s why it saved them and afraid the other Nordic countries had normal flu epidemics the last two or three years. Sweden, like UK, had very mild epidemics: you can just go and look at the number of deaths, it’s sub-normal for UK and Sweden. And now we’ve got a supra-normal, a larger-than-normal, number of deaths from Covid.
Now there may be other reasons, I’m not saying there are not but I think those two main forces – the amount of prior immunity and the so-called “dry tinder,” what vulnerable fraction of the population did you have as a result of seasonal flu being intense or not – I think that accounts for most of it. And it’s – it’s just puberistic and, uh, and – and kind of silly that our government and advisors tell you that doing things that have never worked in the past, like lockdown are going to make any difference to the transfer of respiratory viruses. I don’t believe it for a moment. There’s no scientific evidence behind it and there are much stronger scientific hypotheses that do explain it. You might think that in terms of numbers of deaths – excess deaths – that Covid has produced such a large number that this will be an awful year for excess deaths, but surprisingly not. 2020 is lining up to be about eighth in a list since 1993.
Roughly 620,000 people die every year in this country. They say in life we are also in death – and it’s true, it’s been awful for those who have been personally affected by illness and death, but it’s not particularly unusual in terms of the number of people who’ve died. So one of the things I’ve noticed has happened in – in recent years is that we almost seem to be moving, uh, you know post-science, post-fact as if – as if facts don’t matter. For someone who’s qualified and practiced as a professional scientist for 35 years I think it’s deeply distressing that, I don’t think you should listen to me if I talked about – I don’t know, the design of motorways or something – like, I don’t know anything about motorways or – or how to grow trees better, I don’t know anything about that. But I do know quite a lot about immunology, infection, inflammation, and the way infectious organisms move through a population.
I’ve no other reason for giving this interview other than I really care what happens to my country – and we have to pull ourselves out of this. And I personally believe the way forward is twofold, it’s not difficult. One, we should cease mass testing of the mostly-well in the community immediately – it only provides misleading and grey information, and yet we’re driving policy almost completely based on it. It’s definitely wrong, we should not do it. Use the tests in hospital – I’m not saying don’t test – don’t continue mass testing, and for God’s sake, don’t increase the number of tests. It is a pathology all of its own which must be stamped out by right thinking people. And I’m afraid the people on SAGE, who have provided the modeling, the predictions, the – the measures that should be taken, that their work is so badly, and obviously flawed – lethally incompetent, that you should have no more to do with these people. They should be fired immediately. And the effect of that advice has been to – have cost lots of innocent people their lives from non-Covid causes, they should be dismissed and reconstituted using an appropriate group of skilled individuals – especially avoiding any who might even have the suggestion of a conflict of interest. I think we’re right at the edge of the precipice. I really hope that we can pull back.
1 note
·
View note
Text
Fauci Accuses Fox News of Vaccine Lies
LOS ANGELES (OnlineColumnist.com), Jan. 26, 2022.--Sinking in the ratings since 75-year-old former President Donald Trump left office Jan. 20, 2021, the left wing media has taken their ire out on Fox News, receiving a surge in viewership, now eclipsing rivals CNN and MSNBC by a long shot. CNN and MSNBC have watched their ratings crater while Fox New has gone up like a rocket. When it comes to the deadly novel coronavirus pandemic, the liberal networks now pounce on popular Fox New host Tucker Carlson who likes to give the contrarian view on vaccines and masking. “You can’t walk away from the facts. And the facts are stunningly obvious,” Dr. Anthony Fauci said at the White House pandemic response team briefing. Fauci responded to the Washington Post saying that Carlson’s segment was the “most dishonest and dangerous pandemic segment yet,” referring to an appearance by former New York Times reporter Alex Berenson.
Berenson told Tucker that the mRNA vaccines, from Pfizer-BioNTech and Moderna, were a “dangerous and ineffective product that “don’t really work at all against Omicron, the new variant now accounting for 99.7% of Covid-19 cases in the U.S. Fauci and the left-wing press have been attacking Carlson and Fox News for offering an alternative view about the vaccine and its ability to fight the Omicron variant. Called “The Pandemic’s Wrongest Man,” by Atlantic Magazine, they accuse Bersonson and Fox News of disseminating dangerous propaganda about vaccines to the public. White House officials boast about 75% of the U.S. population that’s had at least one does of either the mRNA or adenovirus vaccines. Only 63.4% have received at least two vaccines doses, with only 40.3% receiving booster or third does of the original vaccines, leaving a lot of susceptible citizens.
Liberal cable news networks like CNN and MSNBC try to get back their ratings by attacking Fox New as a “propaganda network.” But liberal cable networks spent four years using the airwaves to accuse Trump as serving the Russian government. Even today the same irrational voices on CNN accuse Fox News, of all things, of taking Russian President Vladimir Putin’s side. CNN host Don Lemon spent his Jan. 25 show calling Fox News a propaganda network for, among other things, showing respect to Russian President Putin. Trump was accused by CNN and MSNBC for colluding with dictators like Putin, making it impossible to improve U.S.-Russian relations. With 79-year-old President Joe Biden U.S.-Russian relations have hit rock bottom, almost to the point of blows. Liberal publications like the New York Times have nearly pushed Biden into WW III.
Fauci likes to talk about the “facts,” as long as he can make up whatever facts suits his defense of his work. When he was called out by Sen. Rand Paul (R-Ky.) under oath in the U.S. Senate July 20, 2021, Fauci stomps his feet, calling Paul a liar. Fauci has been caught red handed funneling money to the tune of $15 million to his friend New York-based EcoHealth Alliance CEO Peter Daszak who spent million on bat coronvirus experiments at the Wuhan Institute of Virology. When Paul dared to call the experiments “gain-of-function” research, increasing the infectiousness of bat coronaviruses, Fauci went ballistic. Fauci told Paul, he resents the insinuation that he had anything to do with creating the deadly novel coronavirus. But clearly giving money to Wuhan Institute of Virology chief virologist Shi Zhengli’s lab held create the virus. Fauci has covered up from the beginning a lab leak origin of the virus.
Fauci says he has the facts on his side yet he’s presented zero evidence that the deadly novel coronavirus emerged naturally in Wuhan. Published email under the Freedom of Information Act show Daszak thanking Fauci for supporting the natural occurrence theory. Daszak was the first U.S.-based scientist to pull a group of 27 scientists together to reject the lab leak theory way back in February 2020. Daszak also led the World Health Organization investigation to Wuhan China in 2021, concluding that the lab leak theory was the least likely explanation for the deadly novel coronavirus. Neither Fauci nor Daszak said anything when Chinese Communist Party spokesman Zhao Lijian said March 13, 2020 that the deadly virus was made in America and planted in Wuhan by the U.S. military. Lijian made his statement only two days after WHO declared a global pandemic March 11, 2020.
When it comes to basic facts about the deadly novel coronavirus, Fauci has been covering up the origin of the virus because he “resents” any suggestion that he has blood on his hand for supporting Shi Zhengli’s “gain of function” research. Zhengli took, with the help of U.S. and foreign scientists, harmless bat coronviruses and engineered them into the most contagious pathogens known to humankind. Fauci said he never funded “gain of function” research, but he gave Daszak’s EcoHealth alliance who gave Zhengli at least $600,000 for her bat coronavirus experiments. “Sen. Paul, you don’t know what you’re talking about,” Fauci told Paul July 20, 2021 under oath in the U.S. Senate. No one in the liberal press asks Fauci anything about the National Institute’s of Health [NIH] funding Zhengli’s experiments through EcoHealth Alliance. Fauci continues to cover up the origin of the deadly novel coronavirus.
About the Author
John M. Curtis writes politically neutral commentary analyzing spin in national and global news. He’s editor of OnlineColumnist.com and author of Dodging The Bullet and Operation Charisma.
1 note
·
View note
Text
Pan-coronavirus vaccines is our best bet to win this fight: How to grab them
New Post has been published on https://behealthy99.com/pan-coronavirus-vaccines-is-our-best-bet-to-win-this-fight-how-to-grab-them/
Pan-coronavirus vaccines is our best bet to win this fight: How to grab them
The world is breeding new variants so fast, it may not make sense to chase them one at a time. Global regulators don’t necessarily think it’s the right approach. The World Health Organization and the U.S. Food and Drug Administration say omicron-specific vaccines might not be needed, and that public-health agencies around the world — not drug companies — should work together to decide the composition of the next vaccines.
A wiser strategy is one that many vaccine scientists are already working on: the development of pan-coronavirus vaccines, capable of quashing any variant that exists or might emerge.
It’s certainly possible that the omicron-specific vaccines that Pfizer and Moderna are working on will turn out to be useful, Anthony Fauci told me — at least for a while. But, he said, “we’ve got to be careful because you may be playing some sort of whack-a-mole approach as newer variants go.” In addition to advising President Joe Biden on Covid response, Fauci is head of the National Institute of Allergy and Infectious Diseases, which is funding various efforts to create pan-coronavirus vaccines.
Chances are good that a new Covid-19 variant is already lurking that might look nothing like omicron. Virus experts have been “humbled” by the range of mutations this coronavirus can produce, says Penny Moore, a virologist at University of the Witwatersrand in South Africa. The changes in the spike protein — the target of our current vaccines — have jumped around from beta to delta to omicron, enough to suggest that an omicron-specific vaccine might be powerless against the next variant.
In a perfect world, the quickest way to end this variant chase would be to immediately vaccinate the entire world with the existing shots. Omicron has shown it can break through Pfizer and Moderna’s protection, but these vaccines still defend against severe disease, hospitalization and death. For now, countries with inadequate vaccine supplies are a breeding ground for new variants.
One smart way to fight back is to create and test pan-coronavirus vaccines — and lay out a plan to produce enough of these for all countries. But they can’t be created as fast as variant-specific vaccines can. Fauci estimates it could take many months or even, if we’re unlucky, years to perfect them. But given the probability that the world will be living with SARS-CoV-2 for a long time, it’s essential to try to build universal protection against any and all variants that might develop.
So what exactly is a pan-coronavirus vaccine? The term has become a catchall for both vaccines that could protect against any current and future SARS-CoV-2 variants and those that could also provide immunity against SARS, MERS and any other coronaviruses that might come along. Scientists have reason to be optimistic that either kind is possible. Design templates already exist for universal vaccines against flu and HIV. The trouble is, none of these designs has yet made it to the marketplace, and many have failed altogether.
Coronaviruses may be easier targets, however. Their built-in error-correcting mechanism causes them to mutate much more slowly than flu viruses or HIV do.
So scientists in academic and government labs are working with a specific design that has shown promise against the flu: a nanoparticle studded with pieces of the virus that are known to be important for eliciting a strong immune response.
Researchers at many labs — including the Walter Reed Army Institute of Research, the National Institutes of Health, the California Institute of Technology, the University of Washington’s Institute for Protein Design and Northwestern University — are experimenting with various kinds of nanoparticles decorated with spike proteins taken from various SARS-CoV-2 variants.
The idea is that exposing the immune system to a few different spike proteins will enable it to mount a defense against any it might encounter. Last month, Walter Reed scientists published data showing that their pan-coronavirus vaccine caused nonhuman primates to produce neutralizing antibodies against not only SARS-CoV-2 but also SARS-CoV-1, the strain responsible for the 2003 SARS outbreak. These researchers have already begun an early Phase 1 trial in humans to ensure it is safe and gauge the immune response it elicits.
Another experimental pan-coronavirus vaccine created by Pamela Bjorkman’s lab at CalTech has room for even more spike proteins than the Walter Reed one has. She’s preparing to begin a trial in the U.K.
Another way to create a pan-coronavirus vaccine is to target the parts of the virus that remain the same even as it mutates, perhaps a small region on the spike protein. But because so many of the virus’s mutations are on the spike, this may not be easy. Vir Biotechnology Inc., which makes the only antibody therapy still effective against omicron, is well on its way to identifying these so-called highly conserved areas on the virus, says Herbert “Skip” Virgin, Vir’s chief scientific officer. The hope is that a vaccine targeting these spots could offer several years of broad protection against coronaviruses.
“But discovering these vaccines will take time,” Fauci says. “It’s not going to be tomorrow.” In making the initial Covid vaccines, scientists were able to quickly build upon years of work to make the spike protein in the proper shape to show the human immune system. Doing that again for whatever area remains unchanged in the spike? “That could take a long time,” Fauci says.
Directing greater effort into the projects could move them along faster. In September, NIAID gave out $36.3 million in pan-coronavirus grants, and that’s a start. Getting big drug firms — and their vast research budgets — involved would also help. It’s not too soon for companies such as Pfizer and Moderna to turn their attention to pan-coronavirus vaccines.
This story has been published from a wire agency feed without modifications to the text. Only the headline has been changed.
Subscribe to Mint Newsletters
* Enter a valid email
* Thank you for subscribing to our newsletter.
Never miss a story! Stay connected and informed with Mint.
Download
our App Now!!
0 notes
Text
My last 2021 blog
‘Voices like The CP Diary brings us together collectively to fight this virus, with the spirit of common sense and facts. Thank you for that, Ilana’ – Tim.
As I bring 2021 to a close on my blog, my attentions are turned to Covid-19 again. Over the last couple of years since the UK got to hear about Covid, I have tirelessly intuitively continued to source my own insightful facts, the facts, as you say Tim, are ‘in the spirit of common sense and facts’ the facts we’re not being told, so that we all get to understand the issues more clearly.
Hearing anecdotal stories of the Covid vaccine, it’s become easier to understand why many people think the Covid vaccines aren’t right for them. But in any event, it is important to continue with the precautionary measures so that we can all stay safe.
The scientists continue to tell us that we still need to practice social distancing, wear masks and wash our hands routinely. It is the physical precautionary measures that are continuing to keep us safe.
Both the AZ vaccine and Pfizer have been associated with myocarditis (inflammation of the heart) and pericarditis, (inflammation of the outer lining of the heart) and blood clots and as a result they’re not free of risk. It is partly the reason why people are still hesitant in taking the current Covid vaccines.
Being double jabbed you can still catch and spread Covid, but taking the booster means you are less likely to catch Covid, and you can still spread it, therefore it is important to continue with all precautionary measures so that we can all stay safe.
We know the current Covid vaccines can prevent us from dying but taking the vaccines right now don’t stop us from catching or spreading the virus, because as we’re getting back into our lives, cases are continuing to rise. The question is, if we are vaccinated, how are we still able to catch and spread the virus?
With the current vaccines, as soon as the vaccines are administered, their effectiveness declines. Depending on how strong your immunity is, scientists aren’t sure how long you will be protected for and that also depends on whether your immunity is suppressed, particularly if you have an underlying condition. It also depends on how strong your immunity is.
Scientists are aware of the difficulties with the current vaccines and as a result are now working on a new needle-free Covid-19 vaccine being trialled by Southampton University that could give us ‘wide-ranging protection.’ It is being produced to source out any new variants and coronaviruses.
Clinical Chief Investigator and director of the NIHE Southampton Clinical * To all my readers, thank you so much for taking the time to read my blogs throughout the year and to those people who have kindly responded on my blogs. I hope that the incoming year brings you lots of joy and happiness. Thank you for being so supportive. Happy New Year.* Facility, Saul Faust said, “This isn’t simply yet another coronavirus vaccine as it has both Covid-19 variants and future coronaviruses in its sights.”
Conclusion
In 2022, it is important to listen to the science, for us to stay vigilant and also continue with the necessary precautionary measures, so that we may all stay safe. In doing so, you’re not only keeping yourself safe, but you’re protecting the more vulnerable people of society.
I hope my Covid-19 blogs over 2021, have gone some way to help you understand the facts. Writing about ‘worldly’ issues on my blog and finding explanation and understanding, helps my anxiety reduce.
Dealing with autism, I am never far away from feeling overwhelmed. My writing reins me back in and helps me to understand; therefore lessening my anxiety.
Source: https://www.cdc.gov https://www.piedmont.org
* Happy New Year to all my readers. thank you so much for taking the time to read my blogs throughout the year and to those people who have kindly responded on my blog. I hope that the incoming year brings you lots of joy and happiness. Thank you for helping make The CP Diary, such a wonderful and supportive community. *
For more inspirational, life-changing blogs, please check out my site https://www.thecpdiary.com
#thecpdiary#mylast#2021#blog#blogging#newblogpost#writing#writingblog#mentalhealth#healthylifestyle#mentalhealthblog#positivementalhealth#emotionalhealth#emotionalhealthblog
0 notes
Last Seen Blogs

manishanilgupta
Untitled

witches--brew
BY THE LIGHT OF THE MOON

thecarnivalofcarnage
Wicked Fucking Clowns

askbenimsendekahrolusumdur
sudenaz

mackallen
Sparks Fly