#i have an immune disease so covid is lasting longer than expected
Text

DO U. SEE WHAT I MEAN HERE
#bbc ghosts#ghosts#the captain#six idiots#i have an immune disease so covid is lasting longer than expected#so if this seems#wild#that’s why#also#i love the stupid official photos they’re like stock images
56 notes
·
View notes
Text
📆 29 Sep 2023 📰 Public Health silent on what New Brunswickers can expect from COVID-19 this fall 🗞 CBS News
This despite the fact some New Brunswickers say their latest COVID infection was their most severe yet.
CBC News requested an interview with Dr. Jennifer Russell, chief medical officer of health, about what people can expect from COVID-19 this fall and the province's plans.
CBC also requested any modelling projections regarding COVID case counts, hospitalizations and deaths.
The Department of Health replied with an emailed statement.
"Public Health officials continue to monitor the spread of COVID-19 within New Brunswick through its routine reporting practices, wastewater surveillance and through genetic sequencing," Sean Hatchard said in part.
Rod Russell, a professor of immunology and virology at Memorial University in Newfoundland and vice-dean of research and graduate studies for the faculty of medicine, said he doesn't expect any major changes.
"We're going to have our respiratory viruses coming back very soon, if not already, because we have kids going back to school, people coming off vacations.
Hospitalizations, however, could be lower than previous years of the pandemic as people continue to build immunity through vaccinations and infections, he said.
"So I think the severity of disease is just going to keep getting less and less for most people."

Cindy Colwell, 60, of Saint John, doesn't know which strain she had at the end of August, but it hit her fast and hard, she said.
She got a call one morning from a co-worker she sat beside at a meeting, advising her that she had tested positive.
By the afternoon, Colwell was feeling ill. She had a fever, was dizzy and weak, she said.
She also had a cough and "burning" in her bronchial tubes that got progressively worse, nausea and "intestinal issues."
"Where I'd had two vaccines [and a previous infection], I was thinking if I did get it, it wouldn't be as bad as the first time."
When Colwell got COVID last September, she had a fever, body aches, a sore throat and bronchial issues, but they weren't as severe as this time around, she said.
"I just, I felt so bad for at least … like four days. Really bad."
"The couple times that I did try to get up and do something, I would end up back in bed."
"It was a full-body experience," said Colwell.
She was "kind of surprised," she said. She expected it to be more like a cold.
"Where I'd had two vaccines [and a previous infection], I was thinking if I did get it, it wouldn't be as bad as the first time."
When Colwell got COVID last September, she had a fever, body aches, a sore throat and bronchial issues, but they weren't as severe as this time around, she said.
"I just, I felt so bad for at least … like four days. Really bad."
"The couple times that I did try to get up and do something, I would end up back in bed."
Russell has heard about similar experiences and admits it's puzzling because in general, the more someone is exposed to something, the less it's going to impact them, so second and third COVID infections are typically not as bad as the first for most people.
He has a theory though.
"We know that the antibody levels in the blood wane, right? This is why the vaccines don't protect us from infection as long as we'd like," only for two or three months before we're susceptible again, he said, although they do provide longer protection against severe illness and hospitalization.
So when a new infection sets in, there's "not a lot of antibody around to contain that virus," he said.
"So although the infection in the first few days might feel worse, I think it's just because there's that delay while the memory response is getting going. And then you get, I think you're getting a … quicker resolution of the sickness."
Many New Brunswickers like Colwell had their last COVID-19 vaccine at least a year ago.
Anybody who hasn't had a COVID booster or infection for five or six months is "definitely susceptible to getting infected again," said Russell.
Colwell, who got "quite sick" from her first two shots, hasn't had any boosters and doesn't plan to get any.
"I just I feel like the two vaccinations were supposed to work for us. They were the be all to end all. And I still got ill … So I'm just not going to put anymore vaccines in my system."
Russell encourages everyone to get the latest booster once it's available. The closer the vaccine is matched to the current circulating strain, the more benefit, he said.
0 notes
Photo

The Pandemic After the Pandemic
Long COVID isn’t going away, and we still do not have a way to fully prevent it, cure it, or really to quantify it.
The world was slow to recognize long COVID as one of the most serious consequences of the coronavirus. Six months into the pathogen’s tear across the globe, SARS-CoV-2 was still considered an acute airway infection that would spark a weeks-long illness at most; anyone who experienced symptoms for longer could be expected to be dismissed by droves of doctors. Now long COVID is written into CDC and WHO documents; it makes a cameo in the newest version of President Joe Biden’s National COVID-19 Preparedness Plan.
But for all we know now about long COVID, it is still not enough. Researchers still don’t know who’s most at risk, or how long the condition might last; whether certain variants might cause it more frequently, or the extent to which vaccines might sweep it away. We do not have a way to fully prevent it. We do not have a way to cure it. We don’t even have a way to really quantify it: There still isn’t consensus on how common long COVID actually is. Its danger feels both amorphous and unavoidable. People already struggle to deal with well-known risks, let alone fuzzy, slippery ones. “You can be too afraid of what you don’t understand or just say, ‘It’s not well defined; I’m not going to think about it,’” says Erin Sanders, a nurse practitioner and clinical scientist at MIT. Concern, when we let it, can act like a gas. It expands to fill the space we give it.
But even if long COVID’s prevalence turns out to be a single-digit percentage of SARS-CoV-2 infections—proportionally much smaller than most experts estimate—in absolute terms “that is not small,” says Ziyad Al-Aly, the director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System. Millions of people have already developed long COVID; many of them, an untold fraction, have not recovered. This is the challenge of chronic illness: When people join its ranks, they do not always exit. With each new case of long COVID, the virus’s burden balloons.
“I worry, now that everyone is moving to the post-pandemic world, we’re going to sweep all these patients under the rug,” Al-Aly said. Long COVID struggled to gain a toehold in the national consciousness; now it threatens to be one of the first major COVID impacts to slip back into the margins.
Researchers have known for many months that long COVID is more a category than a monolith. Al-Aly very roughly likens it to the way we talk about cancer—an umbrella term for diseases that are related but that require distinct diagnoses and treatments. Long COVID has hundreds of possible symptoms. It can batter the brain, the heart, the lungs, the gut, all of the above, or none of the above. The condition can start from a silent infection, an ICU-caliber case, or anything in between. It can begin days, weeks, or months after the virus first infects someone, and its severity can fluctuate over time. “We lump all of that into one broad thing,” Al-Aly said. “It is not.”
The condition’s root causes, accordingly, are also diverse. In some cases, long COVID may be collateral damage from the war waged between virus and immune system; in others, it might sprout out of a chronic SARS-CoV-2 infection or, conversely, a quick viral encounter that sets bodily systems on the fritz. These hypotheses aren’t comprehensive or mutually exclusive: There are only so many ways for bodies to run smoothly, and infinite ways to throw those processes out of whack.
All of this means that even diagnosing long COVID—an essential step toward understanding it—is still a battle. We don’t have a clear-cut, consensus clinical definition, a single name for the condition, or a standardized set of tests to catch it. Even the CDC and the WHO can’t agree on how long a person must be sick before they meet the condition’s criteria. Some researchers and health-care providers favor one agency’s definition; others, dissatisfied with both, come up with their own. And “there are still doctors out there that do not think long COVID exists,” says Alexandra Yonts, a pediatric-infectious-disease specialist at Children’s National Hospital, in Washington, D.C.
In an ideal experimental world, to understand long COVID’s risks, researchers would systematically survey large swaths of the population over long periods of time, watching to see who gets infected, who goes on to develop the condition, what form it takes, and how it impacts people’s health, says Shruti Mehta, an infectious-disease epidemiologist at the Johns Hopkins Bloomberg School of Public Health who is studying long COVID. But few institutions have the resources for such an undertaking, which could span many months or years. So many researchers have to make do with the limited data sets that are already available to them. As a result, some studies end up biased toward patients who were hospitalized, while others wind up favoring people who have the time, means, and trust in the health-care system to sign up for long-term studies. Neither group fully captures long COVID’s wide-ranging toll. The situation’s especially tough for pediatric patients, who might be too young to articulate the severity of their symptoms and are often excluded from long-COVID studies. Long COVID certainly exists in kids, but it may not perfectly mirror what goes on in adults: Children’s susceptibility to the virus is different, and their bodies are so rapidly changing, says Yonts, who runs a pediatric-long-COVID clinic in D.C.
All told, the study of long COVID has become, as Sanders of MIT puts it, “a data disaster.” Some researchers estimate that a single-digit percentage of SARS-CoV-2 infections bloom into long COVID; Al-Aly is one of them. Others, meanwhile, favor larger numbers, with a few even insisting that the rates are actually more than half. Most of the experts said they feel comfortable working in the 10 to 30 percent range, which is where many studies seem to be starting to converge. Finding one answer is tricky, without knowing how many forms long COVID can take—some could be more common than others. Formally splitting the disease into subdivisions could help address some of these ambiguities. But we don’t know nearly enough to start slicing and dicing, says Bryan Lau, an infectious-disease epidemiologist working with Mehta and Priya Duggal.
If researchers aren’t comprehensively capturing who currently has long COVID, they can’t say for certain who’s most likely to get it either. Many researchers have found that women contract long COVID more frequently than men. Others have uncovered evidence that people who end up infected with gobs of the coronavirus, or who produce antibodies that attack the body’s own tissues, also seem to tilt toward long COVID. Chronic health issues, including diabetes, could up a person’s chances of getting sick and staying sick as well. So might a lingering Epstein-Barr virus infection. But some of these trends are still being confirmed, experts said, and the extent to which they toggle risk up or down isn’t known. And it’s definitely too early to pinpoint any of these factors as long-COVID causes. “For acute COVID, we know what the risk factors are,” Akiko Iwasaki, an immunologist studying long COVID at Yale, said. “For long COVID, it’s much less clear.”
Still, a couple of other variables feel a bit more nailed down. “The risk is high in people who need hospitalization or ICU care,” Al-Aly said. Deepti Gurdasani, an epidemiologist at Queen Mary University of London, says she’s fairly confident that the nature of a person’s exposure to SARS-CoV-2 plays a role as well: Heavier and more frequent viral encounters seem to tip the scales toward symptoms that last and last. That’s a concern for people in essential occupations, who “aren’t able to shield themselves,” she said.
If these last few factors directly affect how and whether long COVID unspools, vaccination—which reliably staves off hospitalization and, to a lesser degree, infection—could be a partial preventive. Several studies have shown that shots do seem to muzzle long-COVID rates. They don’t, however, eliminate long COVID’s odds. To date, experts have yet to find any demographic that has been spared from the condition, despite persistent myths that certain groups, particularly kids, are somehow immune. “We’ve seen it in children of all ages,” says Laura Malone, a pediatric neurologist at the Kennedy Krieger Institute, in Baltimore. Some of her patients are toddlers. The virus isn’t pulling any punches either. Every iteration we’ve encountered so far, Omicron included, seems capable of causing long COVID. “No one is not at risk,” Al-Aly said.
To this day, most countries do not keep a running tally of long-COVID cases. But ballparks of the burden are staggering. Some 2 percent of all U.K. residents—not just those with documented infections—might currently have long COVID, according to the Office for National Statistics. Another analysis estimates that up to 23 million Americans have developed the condition since the pandemic’s start. More will join them. But Davis worries that those numbers will continue to be left off of national dashboards, and thus out of the public eye. Now that the federal government has tightened the boundaries of its concern to hospitalizations and deaths, the public does not even really have to look away from the national perspective on long COVID: There is next to nothing to see.
As people rack up different combinations of shots and infections with different variants, what worsens or soothes long COVID is also getting harder to understand. Many of the experts think long COVID is essential to study, it’s too complex for them to want to tackle themselves. Meanwhile, long COVID remains the pandemic’s looming specter. We are told there is risk, but not exactly how much; we are told that avoiding long COVID would be ideal, but lack the practical guidance to do so—the virus is so widespread that eventual infection, for many people, feels almost inevitable.
At the same time, as researchers look deeper and deeper into the bodies of infected people, they’re only seeing more damage. With each passing month, more studies emerge documenting how the coronavirus alters the function of vital organs such as the heart and the brain. The public has been cultured to think that most SARS-CoV-2 infections are trivial, and the repercussions brief, especially for the young, healthy, and privileged. But long COVID breaks the binary of severe and mild. “It’s going to continue to affect people, even people who are protected from severe illness during the acute phase of infection,” Michael Peluso, an infectious-disease physician and long-COVID researcher at UC San Francisco, said.
No matter where the true numbers on long-COVID risk sit, they are too large to ignore. “Whether it’s 10 percent or 50 percent, at both levels you have to do something about it,” Gurdasani said. Statistics will help sharpen and clarify the condition’s boundaries, and are still worth seeking out. They will not, however, change long COVID’s threat, at its core.
Davis, who is nearing her second anniversary of developing long COVID, feels this deeply. She is still experiencing cognitive dysfunction and memory loss. Her heart still races when she stands. “You cannot live your life like you used to,” she said. “Your life just becomes this shell.” For individuals, for societies, “this is not going away.” Even after much of the world puts the pandemic in its rearview, long COVID will keep filling hospitals and clinics. It will dot the pages of scientific texts, and linginfer in the bodies of millions of people worldwide. Hospitalizations and ICU admissions are not the only COVID outcomes that can buckle a health-care system.
That strain is already being felt by the health-care workers on long COVID’s front lines. Yonts, the Children’s National pediatrician, said that she’s currently booking patients “out to Memorial Day.” COVID’s global crisis can, in some ways, end when we decide to treat it as done. But that is not an option for a growing fraction of the planet, who cannot put COVID fully behind them. “This is going to be the pandemic after the pandemic,” Gurdasani said.
Source: Katherine J. Wu (The Atlantic). Image credit: Leo Correa/Redux.
119 notes
·
View notes
Text
Why are there no new comics today?
so obviously there’s a lot going on in the world right now, and the comic industry is not immune to that, because of the virus Diamond (the company that handles pretty much all distribution of comics to local comic shops) has stopped their distribution for the foreseeable future, obviously this isn’t forever but there’s no timeline given as far as I could find. Marvel and DC are also delaying their digital released this Wednesday (I’ve seen people say they’re delaying weeks past this but I could only find statements about the 4/1/2020, if someone has sources about later weeks please let me know)
I know times are tight for a lot of people out there but this is going to hit local comic shops very hard, especially if Marvel or DC do decide to go ahead with digital distribution in the future, LCS have always been pretty fragile and not huge money makes even when times are good, if you want to support your LCS now is a great time, many are closed but I know quite a few opening back up for curb-side service, if there’s a back issue or trade you’ve been holding off on now would be a great time to pick it up (especially now that you don’t have the excuse of not having the free time to read it haha) I’m sure it would really help them out
I’m going to put Diamond’s statement under the cut because it is rather long but it has some good information to anyone interested in the situation, also I know the timing is a little unfortunate but please know none of this is an april fools joke
Steve Geppi Addresses Coronavirus’ Effect on Distribution
A Message from Steve Geppi,
Chairman & CEO,
Geppi Family Enterprises
Founder, Diamond Comic Distributors
CORONAVIRUS EFFECTS ON DISTRIBUTION
As everyone knows, the world faces ever-increasing challenges related to the COVID-19 pandemic. Its effects on the comics & collectibles and tabletop gaming industries have been felt far and wide. We are hearing from thousands of retailers that they can no longer service their customers as they have in the past, many of them forced to close by government action or resort to in-person or curbside delivery. Even those still open are seeing reduced foot traffic in most cases, a situation that seems likely to worsen with time.
Our publishing partners are also faced with numerous issues in their supply chain, working with creators, printers, and increasing uncertainty when it comes to the production and delivery of products for us to distribute. Our freight networks are feeling the strain and are already experiencing delays, while our distribution centers in New York, California, and Pennsylvania were all closed late last week. Our own home office in Maryland instituted a work from home policy, and experts say that we can expect further closures. Therefore, my only logical conclusion is to cease the distribution of new weekly product until there is greater clarity on the progress made toward stemming the spread of this disease.
EFFECTS ON DIAMOND COMIC DISTRIBUTORS
Product distributed by Diamond and slated for an on-sale date of April 1st or later will not be shipped to retailers until further notice. For the time being, however, we have been able to develop procedures with our teams at the distribution center in Olive Branch, MS to safely continue fulfillment of direct ship reorders for the retailers who are able to receive new product and need it to service their customers. It’s unlikely that orders will be filled on the same day they are placed, and these plans are subject to change if any point we no longer feel that we can safeguard our teams while fulfilling orders.
Product distributed by Diamond UK and slated for an on-sale date of March 25th or later will not be shipped to retailers until further notice. Further updates with regard to reorders and other Diamond UK-specific information will be communicated directly to their customers as information becomes available.
EFFECTS ON ALLIANCE GAME DISTRIBUTORS
Product distributed by Alliance has been shipping from our Fort Wayne, IN and Austin, TX warehouses. Both are closing at the end of the day on Tuesday, March 24th, in the interest of employee safety and to comply with direction from local governments. Any orders not shipped by that time will not be processed until further notice. Your dedicated sales team will still be working remotely and help you with any orders you’d like to place today or questions you may have.
OUR SHARED PATH FORWARD
With these changes in our distribution strategy, we will work with our publishing partners to develop programs that will address product already in the pipeline and what will happen when we resume distribution. We know that during this time you will face many challenges, and we will direct our energies toward addressing them, rather than fighting on increasingly numerous fronts to get product out.
For those retailers who remain open in various forms, I encourage you let loose your own creativity. For the time being, you will be able to replenish your perennials from Diamond and/or Alliance, but you should also remember the stock you already have in your stores. If your doors remain open, it’s likely you will have customers who will continue to seek diversion from events of the world. Special sales, promotions, and even eBay can help you bring in cash during this trying time. Product for which you’ve already paid may well hold some of your answers. There have been many solid suggestions offered about how to help our retailers, and we will bring many of them together in future communications.
Besides the industry’s most immediate needs, we have been and will continue looking toward the future, when we see stores reopening, bringing staff back onboard, and getting customers in the door. We are looking at issues like debt accrued due to this crisis, what reduced ordering means for your discount tiers, and the availability of credit to help stores through and after this difficult time. We don’t have all those answers today, but we understand the many issues you are facing and look forward to addressing them as partners who all have an interest in the long-term health of the industry we love so much.
As I mentioned in my last update, this industry has been one of the greatest joys of my life, from my days as a collector to a retailer to today. I and my Leadership Team have made these decisions knowing full-well the effect this will have on all of you, as well as our publishing partners and our own team members around the world. At the end of the day, the safety and security of our teams and yours, along with the many customers we all serve, is paramount. I again thank you for your ongoing patience and support.
Thank You,
Steve Geppi
Chairman & CEO, Geppi Family Enterprises
382 notes
·
View notes
Text
Story at-a-glance
In October 2019, mere months before the pandemic was announced, the Bill & Melinda Gates Foundation co-hosted Event 201, in collaboration with the World Economic Forum and Johns Hopkins School of Public Health, funded by billionaire technocrat Michael Bloomberg. This tabletop exercise simulated the global response to a fictional coronavirus pandemic
Amid predictions that 65 million people were dying, mass lockdowns and quarantines were implemented around the world, and alternative viewpoints were suppressed through censorship under the guise of fighting “disinformation”
Event 201 confirms that even if the virus itself wasn’t preplanned, the unprecedented and draconian response to it was
The goal of this pandemic is to usher in the Great Reset, a strategy developed and promoted by the World Economic Forum. Previously referred to as the New World Order, this “reset” of the global economy and society as a whole has been carefully planned for decades
A key component of this agenda is the transfer of global wealth and assets into the hands of the wealthy
source please go to source for video
In this video, Ronnie Cummins, founder and director of the Organic Consumers Association, and I discuss “The Truth About COVID-19 — Exposing the Great Reset, Lockdowns, Vaccine Passports and the New Normal,” which we co-wrote.
The book was released yesterday. If you preordered, thank you! If you didn’t, you can now pick it up without delay.
Thanks for all your support with the book. This is going to be an overwhelming best seller, and likely No. 1 in the U.S. We preordered 50,000 copies, but Amazon told us a few weeks ago that they needed 100,000 copies, which only happens a few times a year for any new book. The orders were placed weeks ago, but this pandemic has massively disrupted the printing industry so it is taking far longer to print books than it used to.
For that reason, your books will be delivered just a bit later than anticipated. However, if you are like me and only read Kindle books, you can get the book now! The good news is that at least 50,000 of you will get the book next week and start to understand the deep web of deception you have been led into. I deeply appreciate all your support on this book and the project to educate the masses about the truth about COVID-19.
As mentioned by Cummins, the COVID-19 pandemic surprised a lot of people, but in researching this book, we learned that vaccine companies and their investors had been anticipating a scenario like this for a very long time.
Event 201 — A Prescient Foreshadowing
Interestingly enough, in October 2019, mere months before the pandemic was announced, the Bill & Melinda Gates Foundation co-hosted Event 201, in collaboration with the World Economic Forum and Johns Hopkins School of Public Health, funded by billionaire technocrat Michael Bloomberg. This tabletop exercise simulated the global response to a fictional coronavirus pandemic.
Amid predictions that 65 million people were dying, mass lock downs and quarantines were implemented around the world, and alternative viewpoints were suppressed through censorship under the guise of fighting “disinformation.” They even discussed the possibility of incarcerating people who question the pandemic narrative.
The need for radical censorship was perhaps one of the most striking foreshadowing in that exercise. In my view, Event 201, as a whole, confirms that even if the virus itself wasn’t preplanned, the unprecedented and draconian response to it certainly was, and Gates is a key figure in this scheme.
He may not be the mastermind, and he’s certainly not the only person involved, but he appears to be one of the front men for the technocratic elite who are using this pandemic to further their own agenda, which is nothing short of world domination through subjugation of the people.
Science and Facts Tossed by the Wayside
Many of the containment measures employed during this pandemic have never been used before, ever. Among them are the shutting down of businesses and forcing people to self-isolate at home for weeks and months on end — around the whole world! It’s quite unbelievable, and few would have thought it possible.
Clearly, it would not have been possible were it not for having spent long periods of time grooming the right people, infiltrating the right organizations and government agencies, influencing politicians and granting nongovernmental bodies global influence.
The goal of this pandemic is to usher in the Great Reset, a strategy developed and promoted by the World Economic Forum. Previously referred to as the New World Order, this “reset” of the global economy and society as a whole has been carefully planned for decades.
We’ve also never quarantined healthy people before. Usually, you isolate the sick and contagious. This is standard practice. But you don’t isolate non-sick people. This is a brand-new idea that has never been tried before and has no scientific basis whatsoever.
They were able to do all of this because the World Health Organization is the de facto ruler when it comes to global pandemics. What they say is what member nations will follow. And who’s the primary funder of the WHO? Not any nation, but Gates. He has, by the way, been involved with the WHO for over a decade, so this is not something he or anyone else dreamed up over some weekend event.
The End Goal Is to Usher in the Great Reset
As we describe in the book, the goal of this pandemic is to usher in the Great Reset, a strategy developed and promoted by the World Economic Forum. Previously referred to as the New World Order, this “reset” of the global economy and society as a whole has been carefully planned for decades.
A key component of this agenda is the transfer of global wealth and assets into the hands of the wealthy. According to a September 2020 economic impact report1 by Yelp, 163,735 U.S. businesses had closed their doors as of August 31, 2020, and of those, 60% — a total of 97,966 businesses — were permanent closures.2
Meanwhile, between March 18, 2020, and April 12, 2021, the collective wealth of American billionaires increased by $1.62 trillion — 55% — from $2.95 trillion to $4.56 trillion. One-third of the total wealth gains by billionaires since 1990 occurred in the last 13 months!3
As noted by Frank Clemente, executive director of Americans for Tax Fairness, “Never before has America seen such an accumulation of wealth in so few hands.”4 The primary benefactors of the pandemic measures include the finance and tech industries and the pharmaceutical and military-intelligence sectors.5
Vaccine Passport Is Your Ticket to Tyranny
As you’d expect, vaccine companies have been able to exploit this pandemic, in large part due to the heavy censoring of any and all preventive and early treatments. Without that censoring, I don’t believe as many people would be lining up to get these shots, seeing how they are experimental gene therapies miscategorized as vaccines.
None of the COVID-19 vaccines currently on the market has been licensed. They are all being used under emergency use authorization, and a condition for an EUA is that there are no other effective treatments available. This, I believe, is the real reason why effective prevention and alternative treatments were so heavily suppressed. They, quite simply, would have rendered the vaccine moot.
In the book, we also detail how inaccurate tests, used inappropriately, created the illusion of a highly infectious pandemic and served as the basis for the fearmongering spewed by the media. In reality, the vast majority of “cases” actually weren’t. They were false positives and/or people being counted multiple times because they kept being retested, and instead of counting people, they were counting tests.
Fatality statistics were also grossly inflated by suddenly changing how death certificates are filled out and marking any person who died having had a positive PCR test within the last month, or who was simply suspected of being positive, as a COVID-19 death. Even the U.S. Centers for Disease Control and Prevention admitted that 94% of COVID-19 deaths were people who died with the virus, not from it. The real cause of death was another underlying, often long-term chronic condition.
All of these statistics were artificially manipulated to make it appear we are in a sufficiently deadly and horrible situation to warrant vaccine passports, without which you won’t be allowed to participate in certain social activities or travel.
The irony is that the COVID-19 vaccines are not designed to prevent infection or spread of the virus, so being vaccinated won’t do a thing for public health. At best, it may protect the vaccinated individual from having a more serious case of COVID-19 if or when they do get infected. They encourage everyone to get vaccinated in order to ensure we reach herd immunity, yet these “vaccines” aren’t designed to provide immunity!
Since vaccination won’t prevent viral spread, the vaccine passport will fulfill but one purpose, and that is to usher in a digital surveillance mechanism that can then be expanded to encompass many other areas of life, including financial data. So, the vaccine certificate is not a passport to freedom. It’s your ticket to tyranny.
How to Take Control of Your Health
I believe your best bet, moving forward, is to address your foundational health, starting with your metabolic flexibility. You want to be metabolically flexible. What does that mean? It means that your body can seamlessly transition between burning fat and burning carbohydrates as its primary fuel. This is important, because when your body can do this, it means you are not insulin resistant.
When you’re insulin resistant, you’re more likely to have complications such as immune insensitivity, obesity, high blood pressure and distorted cholesterol patterns. Your risk for severe COVID-19 will also be dramatically increased. Thankfully, many of these issues can be simply reversed for no cost with time-restricted eating.
Secondly, you need to have enough vitamin D. For optimal health, you’ll want your vitamin D level, which you must measure using a simple blood test, to be between 60 ng/mL and 80 ng/mL (100 nmol/L and 150 nmol/L).
My peer reviewed published study6 on the “Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity” is available for free on the journal’s website. In the book, we go into more specific details about these strategies, and many others.
Freedom of Speech Is Officially Dead
“The Truth About COVID-19” will become all the more important to own and share in days to come, as I was recently forced to permanently remove all articles on vitamins D, C and zinc, as well as most articles on COVID-19, from my website. This book will now be a primary source of such information.
Over the past year, I’ve been researching and writing as much as I can to help you take control of your health, as fearmongering media and corrupt politicians have destroyed lives and livelihoods to establish global control of the world’s population, using the COVID-19 pandemic as their justification.
Through these progressively increasing stringent measures, I have refused to succumb to these relentless attacks. I have been willing to defend myself in the court of law, as I’ve had everything reviewed by some of the best attorneys in the country.
Unfortunately, threats recently became very personal and intensified to the point I could no longer preserve much of the information and research I’ve provided to you thus far. These threats are not legal in nature, and I have limited ability to defend myself against them.
Politicians in January 2021 managed to pass the COVID-19 Consumer Protection Act of the 2021 Consolidated Appropriations Act.7 This piece of legislation was hidden in a 2,100-page bill8 that now provides the government with enormous legal authority to prosecute anyone for “crime” of disagreeing with the official narrative that the vaccine is the ONLY approved approach to treat or prevent COVID-19. Here is the relevant portion of this Act:
This Act makes it unlawful under Section 5 of the Federal Trade Commission Act for any person, partnership, or corporation to engage in a deceptive act or practice in or affecting commerce associated with the treatment, cure, prevention, mitigation, or diagnosis of COVID-19 or a government benefit related to COVID-19.
Remember, Hitler and Mussolini came to power LEGALLY, because they subverted the legal structures of their country. Folks, you are now seeing the same kind of subversion happening in real time in the U.S. It is obvious that this is the first assault, designed to remove your personal freedom and liberty. This law essentially abolishes the First Amendment of the U.S. Constitution with respect to ANY dialog on COVID-19.
3 notes
·
View notes
Text
What Can Go Wrong?
What Can Go Wrong?
One key take-home from the Nature Reviews Drug Discovery article5 cited above is that replacing rare codons “must be used judiciously,” as rarer codons can have slower translation rates and a slowed-down rate is actually necessary to prevent protein misfolding.
The spike protein is the toxic part of the virus responsible for the most unique effects of the virus, such as the blood clotting disorders, neurological problems and heart damage. To expect the COVID shot to not produce these kinds of effects would be rather naïve.
A (adenine) and U (uracil) in the third position are rare, and the COVID shots replace these A’s and U’s with G’s (guanine) or C’s (cytosine). According to Seneff, this switch results in a 1,000-fold greater amount of spike protein compared to being infected with the actual virus.
What could go wrong? Well, just about anything. Again, the shot induces spike protein at levels unheard of in nature (even if SARS-CoV-2 is a “souped up” manmade concoction), and the spike protein is the toxic part of the virus responsible for the most unique effects of the virus, such as the blood clotting disorders, neurological problems and heart damage.
So, to expect the COVID shot to not produce these kinds of effects would be rather naïve. The codon switches might also result in protein misfolding, which is equally bad news. As explained by Seneff in our previous interview:
“The spike proteins that these mRNA vaccines are producing … aren’t able to go into the membrane, which I think is going to encourage it to become a problematic prion protein. Then, when you have inflammation, it upregulates alpha-synuclein [a neuronal protein that regulates synaptic traffic and neurotransmitter release].
So, you're going to get alpha-synuclein drawn into misfolded spike proteins, turning into a mess inside the dendritic cells in the germinal centers in the spleen. And they're going to package up all this crud into exosomes and release them. They’re then going to travel along the vagus nerve to the brainstem and cause things like Parkinson's disease.
So, I think this is a complete setup for Parkinson's disease ... It's going to push forward the date at which someone who has a propensity towards Parkinson's is going to get it.
And it's probably going to cause people to get Parkinson's who never would have gotten it in the first place — especially if they keep getting the vaccine every year. Every year you do a booster, you bring the date that you're going to get Parkinson's ever closer.”
Immune Dysfunction and Viral Flare-Ups
Other significant threats include immune dysfunction and the flare-up of latent viral infections, which is something Mikovits has been warning about. In our previous interview, she noted:
“We use poly(I:C) [a toll-like receptor 3 agonist] to signal the cell to turn on the type I interferon pathway, and because [the spike protein your body produces in response to the COVID shot] is an unnatural synthetic envelope, you're not seeing poly(I:C), and you're not [activating] the Type I interferon pathway.
You've bypassed the plasmacytoid dendritic cell, which combined with IL-10, by talking to the regulatory B cells, decides what subclasses of antibodies to put out. So, you've bypassed the communication between the innate and adaptive immune response. You now miss the signaling of the endocannabinoid receptors …
A large part of Dr. [Francis] Ruscetti’s and my work over the last 30 years has been to show you don't need an infectious transmissible virus — just pieces and parts of these viruses are worse, because they also turn on danger signals. They act like danger signals and pathogen-associated molecular patterns.
So, it synergistically leaves that inflammatory cytokine signature on that spins your innate immune response out of control. It just cannot keep up with the myelopoiesis [the production of cells in your bone marrow]. Hence you see a skew-away from the mesenchymal stem cell towards TGF-beta regulated hematopoietic stem cells.
This means you could see bleeding disorders on both ends. You can't make enough firetrucks to send to the fire. Your innate immune response can't get there, and then you've just got a total train wreck of your immune system.”
We’re now seeing reports of herpes and shingles infection following COVID-19 injection, and this is precisely what you can expect if your Type I interferon pathway is disabled. That’s not the end of your potential troubles, however, as these coinfections could accelerate other diseases as well.
For example, herpes viruses have been implicated as a trigger of both AIDS6 and myalgic encephalomyelitis7 (chronic fatigue syndrome or ME-CFS). According to Mikovits, these diseases don’t appear until viruses from different families partner up and retroviruses take out the Type 1 interferon pathway. Long term, the COVID mass injection campaign may be laying the foundation for a rapidly approaching avalanche of a wide range of debilitating chronic illnesses.
Are COVID Shots Appropriately Optimized?
As noted in the Vaccines article cited earlier, the codon optimization in the Pfizer and Moderna shots could be problematic:8
“As mammalian host cells attack unmodified exogeneous RNA, all U nucleotides were replaced by N1-methylpseudouridine (Ψ). However, Ψ wobbles more in base-pairing than U and can pair not only with A and G, but also, to a lesser extent, with C and U.
This is likely to increase misreading of a codon by a near-cognate tRNA. When nucleotide U in stop codons was replaced by Ψ, the rate of misreading of a stop codon by a near-cognate tRNAs increased.
Such readthrough events would not only decrease the number of immunogenic proteins, but also produce a longer protein of unknown fate with potentially deleterious effects …
The designers of both vaccines considered CGG as the optimal codon in the CGN codon family and recoded almost all CGN codons to CGG … [M]ultiple lines of evidence suggest that CGC is a better codon than CGG. The designers of the mRNA vaccines (especially mRNA-1273) chose a wrong codon as the optimal codon.”
The paper also points out the importance of vaccine mRNA to be translated accurately and not merely effectively, because if the wrong amino acids are incorporated, it can confuse your immune system and prevent it from identifying the correct targets.
Accuracy is also important in translation termination, and here it comes down to selecting the correct stop codons. Stop codons (UAA, UAG or UGA), when present at the end of an mRNA coding sequence signals the termination of protein synthesis.
According to the author, both Pfizer and Moderna selected less than optimal stop codons. “UGA is a poor choice of a stop codon, and UGAU in Pfizer/BioNTech and Moderna mRNA vaccines could be even worse,” she says.
What Health Problems Can We Expect to See More Of?
While the variety of diseases we may see a rise in as a result of this vaccination campaign are myriad, some general predictions can be made. We’ve already seen a massive uptick in blood clotting disorders, heart attacks and stroke, as well as heart inflammation.
More long term, Seneff believes we’ll see a significant rise in cancer, accelerated Parkinson's-like diseases, Huntington's disease, and all types of autoimmune diseases and neurodegenerative disorders.
Mikovits also suspects many will develop chronic and debilitating diseases and will die prematurely. At highest risk, she places those who are asymptomatically infected with XMRVs and gammaretroviruses from contaminated conventional vaccines. The COVID shot will effectively accelerate their death by crippling their immune function. “The kids that are highly vaccinated, they're ticking time bombs,” Mikovits said in my May 2021 interview.
What Are the Options?
While all of this is highly problematic, there is hope. From my perspective, I believe the best thing you can do is to build your innate immune system. To do that, you need to become metabolically flexible and optimize your diet. You’ll also want to make sure your vitamin D level is optimized to between 60 ng/mL and 80 ng/mL (100 nmol/L to 150 nmol/L).
I also recommend time-restricted eating, where you eat all your meals for the day within a six- to eight-hour window. Time-restricted eating will also upregulate autophagy, which may help digest and remove spike protein. Avoid all vegetable oils and processed foods. Focus on certified-organic foods to minimize your glyphosate exposure.
Sauna therapy may also be helpful. It upregulates heat shock proteins, which can help refold misfolded proteins. They also tag damaged proteins and target them for removal.
1 note
·
View note
Text
The CoViD Vaccine
I first posted this to facebook because of the high number of anti-vaxxers on the media. But I figured I’d post it here, too. This is a quick study of why the CoViD-19 vaccine was developed so quickly and why it’s likely safe. Sources at the bottom of the post.
===
Part 1: Why was the CoViD vaccine developed so quickly while other vaccines take years?
Some people cite the inability to produce an HIV/AIDS vaccine after so long as a justification for stating that the CoViD vaccine could not possibly be developed in such a short time. However, there's a very good reason with the HIV/AIDS vaccine is taking so long, and it's found in the genetic makeup of the virus.
HIV is a strange virus, in that it completes its cycle insanely fast (within 24 hours in some cases) and because of this, it's prone to mutations. Because little to nothing was done about the AIDS epidemic in the 1980s, the virus was allowed to spread, unchecked, rapidly mutating and developing into HUNDREDS of strains.
You know how we have to get a new flu shot every year because the virus has mutated into something new? That's HIV, but instead of a new strain appearing once a year, a new strain can appear in the course of one single viral generation. When HIV is transmitted to someone else, it may already be a slightly different virus than it was in the transmitter. This means that a vaccine developed to work in the person who transmitted the virus would not work for the newly-infected person.
That's why, at this point in time, antiretrovirals (drugs that disrupt the replication of the virus by preventing it from attaching to RNA) actually work better than a vaccine.
As well, HIV/AIDS specifically attacks the immune system, hampering any efforts at strong immune response. That is, by the time a vaccinated immune system recognizes the virus as a threat, it has already destroyed part of the immune system AND mutated itself, meaning the even a vaccine that would otherwise work can no longer be effective. This is a known phenomenon called "immune exhaustion."
Lastly, HIV is really good at hiding from detection as a dormant phase of the viral particles (called provirus) can remain within cells for years before lysing from/destroying the cells they're inside. And HIV creates these provirus particles every single cycle, which means even if a vaccine is developed and destroys all free-floating viral particles, the dormant particles will always be around to start a new phase of infection, once again leading to immune exhaustion.
In the case of HIV, the hope of a vaccination lay within the blood of people with a natural immunity to HIV, which is a brand new frontier of vaccine development that is poorly understood.
Conversely, CoViD-19 does have a semi-quick mutation rate, but not as fast as HIV. It was also immediately taken seriously by medical professionals, and the development of the vaccine started soon after the virus's discovery. Unlike HIV, CoViD does NOT attack the immune system (instead, it triggers a massive immune response called a cytokine storm) and it also does not hide undetected within cells. (...Probably. We are still learning about the virus.)
Part 2: Genome Mapping
First, it's important to note that data sharing and sequencing equipment is much more sophisticated than it used to be. This means that several labs can work on the genetic mapping of CoViD at the same time, and share that data in real time. Powerful software allowed the geneticists to connect the various strands of viral RNA gathered from patients presenting with the virus, and it was quickly determined that CoViD-19 (AKA SARS-CoV-2) was remarkably similar to SARS-CoV years before. The viruses share between 88%-90% of the same genetic code; some scholars refer to both viruses as the same "species."
The full method used to determine the genome can be found here: https://www.thelancet.com/.../PIIS0140-6736(20.../fulltext (very long, but pretty cool!)
During the sequencing, it was also determined that while CoViD-19 showed mutations between each case, the faithfulness of the virus to the control was about 99%--suggesting that it was mutating slower than expected. This meant that a quick response could prevent the evolution of the virus to a point where vaccines would be ineffective. While there are multiple strains of CoViD-19, it's likely that they are all currently very similar.
The genome also showed that, like SARS from years past, the CoVid-19 virus contained the same protein receptor--known as ACE2--which had already been studied. The receptor (or spike, as it's called) is what allows the virus to bind to a host cell and release its RNA.
Other factors to consider that are related to the genome mapping itself is that the COST of mapping is far less than it has been in the past, and it also faster and more accurate. Development of vaccines for other diseases (such as chicken pox and HPV) were often hampered by cost, time, and inaccuracy. Conversely, every time the CoViD-19 virus was mapped, the resulting data was nearly the same.
In short, one of the hindrances to vaccine production is often the genome mapping. It's impossible to create a vaccine without knowing the full details of the virus, as a vaccine's purpose is to produce an immune response. That's essentially tricking the immune system into believing it's fighting a virus. The hardest part of vaccine development for CoViD-19 is already done, and it was done in record time.
Part 3: Messenger RNA and synthetic RNA
Before discussing the vaccine, I need to talk about what messenger ribonucleic acid (AKA mRNA) is.
When a cell splits, it needs to make an EXACT copy of its DNA for both cells. Because DNA is fairly complicated, it can't just split in half like the rest of the cell. It needs a set of instructions, which is where transcription comes in.
An enzyme called RNA polymerase makes a near-exact copy of the DNA strand, except for the nucleotide thymine, which is found in DNA, is transcribed as Uracil on the mRNA strand. A lot of stuff happens after that, but the important part is that this mRNA strand is read by ribosomes and TRANSLATED into proteins.
There's... a lot more to it than that, but that's the basic gist.
Which takes us to the question: What is an mRNA vaccine?
It's taken a long time to develop synthetic mRNA. Katalin Karikó, a Hungarian scientist, believed messenger RNA could be harnessed to create all sorts of disease resistances, but the synthetic material was quickly identified and destroyed by the body's immune system.
Because Karikó was experimenting with an idea that other scientists had dismissed as impossible, it took her FIFTEEN YEARS to create something with such promise that she finally received grants to further her work. It wasn't until 2005 that Karikó discovered a way to trick the immune system into NOT immediately attacking the synthetic RNA.
Only 15 years ago. And even then, because many of Karikó's peers had already dismissed messenger RNA as a valid medical tool, it took them a long time to get them on board, and research crawled forward and a snail's pace.
Her accomplishments DID interest a post-doc named Derrick Rossi, who successfully used the synthetic RNA to create proteins in a petri dish out of various polypeptides. Most interestingly, an introduced immune contingent would ignore the mRNA, as if it was supposed to be there.
It was this work, in 2010, that made Rossi realize that mRNA could be used to create vaccines.
This inkling of an idea required "proof of concept" in order to receive funding for further research--which was slow in coming. Any new technology, even discoveries that are microscopic, carries risks, and it turned out that repeated doses of mRNA could produce unwanted side-effects. It wasn't until 2018 that Moderna (which should be a familiar name to everyone by now!) Developed a two-dose therapy that would not produce significant negative effects in humans.
Just in time, too. CoViD-19 appeared in 2019. And while Moderna, Pfizer, and several other companies had been experimenting with mRNA as a vessel for vaccines, nothing had yet been approved for use.
Remember when I talked about the genetic map of CoViD-19 in my last post? With that, scientists creating an mRNA vaccine did not actually need the virus in order to work on the vaccine. All they needed was the genome--and they could then synthesize RNA, which could then be used to build the protein shell of the virus, producing an immune response.
Unfortunately, companies developing the vaccines came under fire for essentially using the promise of a save, synthetic material to fill their coffers. But of course, that's capitalism, and that's a different story.
But essentially, rather than a traditionally-created vaccine which uses dead or modified live viruses, an mRNA vaccine has never touched a virus, has never been injected into an animal in order to synthesize more vaccine, and is able to be ready-made in a lab using messenger RNA.
Of course there is concern about possible long-term effects of this new type of vaccine. The cool thing about mRNA, though, is built into its very code. After it does what it's supposed to do (in the case of the CoViD vaccine, that job is "building a viral envelope that contains no actual viral RNA," it self-destructs. That's why it has to be stored at such low temperatures. anything higher than that and you'd have what's essentially a slurry of random synthesized polypeptides that wouldn't do a damn thing.
So the worry isn't really whether there will be long-term effects from this vaccine, but whether the synthetic mRNA will be able to survive long enough to produce enough fake virus shells to create an immune response. So far, trials have proved successful.
Part 4: Polio, and Why Most Vaccines Are So Extensively Tested
There's a good reason that the FDA requires such extensive, lengthy testing on vaccines, and it has to do with the polio vaccine.
I'm sure most opponents of vaccination cite the early polio vaccine as a reason not to vaccinate--that vaccines are inherently dangerous and should be approached with caution.
Trials of the polio vaccine went well, and were well-tolerated, which meant scientists were initially baffled when a vaccine caused 40,000 cases of polio in children, 200 of which were left paralyzed, and 10 of which died.
At first, people were convinced that this meant vaccines were dangerous--many blamed Jonas Salk for pushing the vaccine through R&D and dooming everyone who'd gotten the vaccine to polio.
So what happened? Did dangerous chemicals in the vaccine cause a weak immune system leading to polio? Was the process itself flawed? Was it time to give up on vaccines as a valid form of disease protection???
Fortunately, no.
Just like today, there were many nay-sayers about vaccines, and those who were against putting them into their body. See, Salk used formaldehyde to de-activate the virus, which people recognized as being very poisonous. despite the fact that the vaccine itself contained none of the chemical, the public demanded an alternative if they were to take it.
So a company called Cutter Labs decided not to use formaldehyde to deactivate the vaccine. In fact, they didn't de-activate the vaccine at all. Because of a lack of rigorous safety protocol at the time, the error was then missed by health inspectors, who ok'd giving a completely live virus to 40,000 children.
This incident, called the Cutter Incident, led to more rigorous oversight and testing when it came to vaccination. It also let to what's called "attunated" viruses, which are weakened, but still living viruses. These attunated viruses have been responsible for outbreaks of poliomyelitis around the world, all because people feared the process used to kill the virus.
The point is, the reason it takes so long to approve vaccines under normal circumstances is that you are dealing with a medication that contains actual viruses (albeit usually dead viruses) plus agents designed to provoke an immune response, such as aluminum. Deactivated vaccines also used to contain thimerosal as a binding agent preservative. While not elemental mercury, thimerosal was derived from mercury, and thus just as suspect as Salk's formaldehyde.
In any case, there's a lot of people concerned about what they are putting into their bodies. And while the use of aluminum adjuvants has been proven safe over decades of vaccinations, every single one still must be tested in order to determine efficacy and safety. Pushing a vaccine that doesn't work is just as bad as pushing a vaccine that causes harm to the patient.
To be fair, it is likely the alum compound that causes vaccine reactions, which means it's up to medical science to do better! Thankfully there are many new adjuvants on the market, including MF59, an oil emulsion which is derived from shark liver; most people consider this a much better option than heavy metal, and it is the most likely candidate for use as an adjuvant in the CoViD-19 vaccine.
If, that is, an adjuvant is needed at all. Currently, there's some speculation that the mRNA in the CoViD vaccine could alone provoke a strong immune response.
Part 5: Putting it all together!
1. Coronavirus was caught quickly and an immediate medical response was established. Using new genetic mapping technology that has only been developed within the last decade, CoViD-19's genome was mapped and made available.
2. CoViD-19 does not hide in, nor does it attack the immune system. For this reason, it's much easier to create an immune response to a vaccine as compared to, say, the HIV virus. Unlike the HIV virus and the common cold, CoViD-19 also currently has limited strains and mutations, making it the perfect time to create a vaccine.
3. The vaccine does not use viral particles. It doesn't need to be "incubated" and then tested after each incubation period. There is no chance for the vaccine to cause the virus in any dose. Instead, it uses synthetic messenger RNA in prompt the body into synthesizing the protein shell of the virus, which activates our immune system.
4. It contains a natural adjuvant found in shark liver oil, rather than heavy metal aluminum. This cuts down on the testing time. Adjuvants provoke an immune response more quickly than the virus alone, although Pfizer stated that the vaccine would likely work without one.
5. Lastly, this can't be overstated enough, the idea behind testing is to have a successful trial in as many people as possible. Other vaccines fail because of unfavorable trials. (For example, chicken pox took so long to develop a vaccine for because of the lack of technologies we had today leading to low efficacy rates in test subjects.) Compared with the MMR vaccine, which has an average efficacy of 90%, the CoViD-19 vaccine achieved a 95% efficacy rate in 10 months. There was very little "back to the drawing board" except in one case where the company developing a vaccine trial dropped completely.
I do want to state here that it is normal for medical science to work faster and better as time progresses. Vaccine science IS medical science, and has only been utilized for the last hundred years. All medical sciences progress and become more reliable as time goes on, including heart transplants, treatment of HIV, diabetes, hell--even Alzimers may have a cure in the next decade thanks to various breakthroughs in the last three years.
It is okay to be cautious. It is not okay to dismiss science because you're afraid or because you don't understand it. It's okay to ask for help learning about these things.
We science people aren't here to lie to you. We look forward to a future where serious disease is a simple hindrance, and not a life-changing event.
Sources:
https://horizon-magazine.eu/article/covid-19-how-unprecedented-data-sharing-has-led-faster-ever-outbreak-research.html?fbclid=IwAR2V_HfDaloTaNfBJ489f1fmdsBbWaYp5j72d3AYo9roKJNaiUATkYc3rA8
https://www.centerforhealthsecurity.org/resources/COVID-19/COVID-19-fact-sheets/200128-nCoV-whitepaper.pdf?fbclid=IwAR3p00yVtK16aduVIF5LV6dgetFEuho4CoxX7ifmVlDcSSPei6p79IyNzpQ
https://www.verywellhealth.com/hiv-vaccine-development-4057071
https://www.statnews.com/2020/11/10/the-story-of-mrna-how-a-once-dismissed-idea-became-a-leading-technology-in-the-covid-vaccine-race/?fbclid=IwAR0brQXhvrs4pMp9AwXOU5KT0z1B-VsbMn8R3RS65Hv_gLqo5gButRTftyg
https://www.jpost.com/health-science/could-an-mrna-vaccine-be-dangerous-in-the-long-term-649253?fbclid=IwAR1MM2vpKrUucLGwEb2T5OZAADMFp3oABJFTcG5F8xDfPfykx5gGwZIWHaE
(And apparently I forgot to save my sources about adjuvants. :|)
#covid-19#coronavirus#vaccine safety#health and safety#not bestiary#i hesitate to tag it this way but#american politics#because you know people here#think this is political
9 notes
·
View notes
Text
As much for myself as anyone else, I would like to provide an overview with how India into the absolute mess with the pandemic that it is in, today. Most of this is from memory and opinion and frankly it isn't really coherent.
Covid-19 came to India early. The first reported cases were from individuals returning from China in December 2019 and January 2020. This was in the southern state of Kerala, which quickly got a handle on the situation. In February and March, as the cases in Europe were rising the borders were wide open and, more importantly, no testing was done.
Around 14 March 2020 was the first sign things were getting out of hand (I remember as I had received a new job offer on that day). All educational institutions were closed - but the regulations were unclear. Note that, at this point, the pandemic was a disease of the well-to-do - those who travelled abroad were the primary vectors of the virus.
And then came 24 March. On that evening, the government declared a country-wide absolute lockdown, starting from midnight, 25 March. Less than 4 hours of notice. I come from a well-off family and we weren't ready; 80% of Indians are daily wage labourers, migrant labourers or a combination of the two - if they don't work, they don't eat, and they had no place to stay that could remotely be considered sufficient for physical isolation. The suffering caused by this decision was unimaginable on par with that caused by the demonetisation decision in November 2016 (with a similar modus operandi).
And in the days that followed, the government just kept dropping the ball. Not because they were incompetent, but because they just didn't care. The migrant labourers walked hundreds, sometimes thousands of kilometers to get home, possibly taking the pandemic with them; police sprayed them with concentrated, industrial grade disinfectant; and an unknown number of people died on the march.
Through it all, the government of India has, still, refused to declare that there is community transmission of the virus in India. All that I could find was that one minister accepted that there was community transmission is isolated areas - this was in October 2020, the peak of the Indian first wave. Even now, I can find no statement about it.
And despite having the second/third highest numbers, despite the immense undercount, until the end of 2020, India was lucky. We had an abnormally low mortality rate, for reasons that - as far as I know - are still not understood.
For the government, this pandemic was and continues to be a weapon to deal with their perceived enemies. The CAA Bill was passed in December 2019, and internment camps were opens on the Bangladesh border. These remain open, thousands of people still confined and all but forgotten. The government has singled out Muslims as the scapegoats for the spread of the virus, I keeping with their ideological leanings. But no real controls have been implemented - if anything, we seem to have taken the worst of the responses in Europe and USA as examples of the best possible way to deal with the pandemic, while ignoring the more stringent controls countries in Asia and Africa followed to control the virus the first time around.
And so we come to today. India still does not admit that there is community transmission. We do not have the resources to stress for the pandemic at sufficient scale, we do not possess the resources to treat all those who are affected by the disease. India has not only all the major recorded mutants for SARS-CoV-2, but also it's own native mutant, B.1.617, that combines the ability to slip past the immune system with increased transmission of the virus.
I'm still lucky. I work from home, my parents are retired and my sister is studying from home. But there are countless others who are not. Getting the vaccine, even via the national vaccination drive, costs money; as of last week, the only way to get vaccinated in my city was to have connections and to travel to outlying areas.
It's not pretty, and it's only going to get a whole lot worse. Current predictions are that this wave will peak in May, but I expect that it will go on longer. My state has declared a lockdown from today evening and the knock-on effects have already begun.
2 notes
·
View notes
Text
A New Adventure - Pt. 5
Okay, y’all, I know I have been extremely absent on this fic and it’s because I’m taking inspiration for this from my real life, but Covid literally destroyed all my plans and therefore put a halt on my inspiration for this. Also, feedback and people asking about if this would be continued literally saved this fic’s life! Don’t ever think that I don’t read your comments or put any weight to your feedback, because that is literally what got things rolling again for this one. Anyways, rant done! Happy reading!
Masterlist
Read on AO3

Quarantini, anyone?
(Authors note: A lot of things, especially towards the end, are extremely fictional and have very little fact and I gloss over the aspect of time. Please don't hate me for that. I'm writing this purely for fun!)
Weeks before you'd met Arthur, you'd heard of the Corona virus. But it was in China then, certainly not a problem in your state.
After meeting Arthur though, the first case in Utah was reported. Still, it wasn't a bother. You thought nothing of it.
That was until, a few weeks later, news reports were that reported cases were skyrocketing. You looked up the symptoms and who was most at risk. Your heart dropped. Arthur was the perfect target as his immune system was highly affected by the TB.
By this point, everyone in your office knew you had a roommate, but not much more than that.
When you discovered Arthur was highly at risk, you decided not to take chances with him and asked to work remotely, to self quarantine.
A week later has gone by and the entire state is in quarantine anyway.
Arthur's confused. He's never heard of Covid, obviously. Why would he have? He finds it incredibly strange that a disease that was first reported in Asia has so quickly become a problem in the states. You have to explain internationality to him and how the entire world is basically connected.
Unlike the rest of the state, you decide not to go crazy and wipe out the shelves of toilet paper and other items. You're lucky in that you bought a large packet not long before this started.
Still, the demand for certain items surprises you and Arthur.
"What you supposed to do during a… quarantine like this?" he asks.
"I don't know, Arthur. The last big pandemic was during 1920 I think. Obviously long before my time."
This is a whole new experience for both of you.
Luckily you're easily able to set up an office at home so you can still work and not have to worry too much about money. However, your amount of work is affected.
You get worried rather quickly about how much work you're going to get. If you don't get work, you don't get paid.
Arthur sees you worrying, even though you don't say anything. He tries to help lighten the load, but there's not much he can.
Money is getting tight. You're starting to have to withdraw from savings. It doesn't help that Arthur will need a refill on his meds and they weren't cheap the first time. How the hell are you going to afford to take care of him and your dog?
Arthur is starting to worry about you. He knows how little sleep you've been getting, despite barely leaving the house.
One night, Arthur sits you down on the couch before dinner and asks you to share your worries with him.
You've been so strong in front of him up to this point, not wanting him to see you as weak or pathetic. But that night, you break down. It helps to voice your worries, even though you know there's nothing he can do.
At least that's what you think.
The weekends are when you go to the store. Arthur's been coming with you more and more to the store. He likes to see what the world is like now.
When you tell him to get ready to go to the store, he says he's not feeling very well. He has days where his TB is just worse than others. Although he's responding wonderfully to the medicine, it still seems to kick his ass. So he says he's going to stay home, get some rest.
You bid him goodbye, saying you'll be longer than usual as you need to go to the pharmacy and get him more medicine.
Your stomach drops when the pharmacist tells you the price. Thank God for your flex spending account, but it doesn't pay for the inhaler refills. Those you have to buy yourself, and it's nearly $100. You sigh. As much as you love having the Arthur Morgan as your roommate, right now is the worst time with this pandemic.
When you get home and get the groceries carried in, Arthur puts a hand on your shoulder.
"Y/N, before we put things away, I need to show you something."
"Arthur, I got cold stuff. Will you help me? It'll be twice as quick."
He gives you a sweet grin that makes you blush and agrees. Funny. You know what he's like on the days when he really doesn't feel good. He's usually lethargic and coughs a lot. Sometimes he even vomits. Once he fell unconscious and you had to drag him to bed (which was nearly impossible. He's a big, broad guy).
Today though he's acting relatively normal. As you look a little harder at him as you move around the kitchen, putting things away, you notice he's got dirt on his skin, under his nails. His right elbow has a large scrape on it.
As soon as everything's been put away, Arthur offers you his hand. This makes your stomach flip. He's never tried to hold your hand before this.
He leads you into his bedroom and flips on the light. On his bed lies a large pile of money. Stacks and stacks of bills, piles of coins. What the hell?
After inspecting them, you notice the bills are not common day dollars. They're much bigger, the designs different. They're bills from the 1890's. The coins are exactly the same.
"I knew you was worried about money and I know I been a burden." You try to argue but he stops you. "So, when you was at the store, I snuck back to my world."
He coughs as he says this. He's visited there a couple of times and every time he does, his TB comes back in full swing, making him relapse until he returns.
"I found a few treasure maps long before I got here," he continues. "So I managed to track 'em down. Also pulled a quick robbery on a bank stage. Anyways, thought this could be my way of contributing."
You can't believe he's done this for you. You know Arthur has a soft, gentle side, but even you didn't expect this.
After counting the money, it all comes to over $1500. That will cover your expenses for over a month and adding what money you are making, you'll be fine. For a few months anyways and hopefully by that point, quarantine will be lifted.
This all adds up and you realize you don't have to worry about money anymore. Arthur has done more for you than you could imagine and it brings tears to your eyes.
He's worried when he sees you beginning to cry, thinking he did something wrong. When you tell him it's because you're so grateful, he gives you another dazzling smile.
"I just couldn't stand letting you do all the work and me just taking advantage. Maybe I'm just so used to helping folk I care about…"
He's cut off by you hugging him. You're not a hugger, typically, but this has definitely earned him one. You hear him huff a little and he pats your back.
"Thank you so much, Arthur."
After doing some research on how to trade old bills for current ones, you end up with even more money because the money Arthur provided ends up being considered antique and "museum quality" (according to the appraiser). This means you leave with well over $50,000.
"Well well, Arthur," you say with a sly smile. "Turns out your robbing ways are still highly useful, even in my day."
33 notes
·
View notes
Link
* * * *
LETTERS FROM AN AMERICAN
January 15, 2021
Heather Cox Richardson
Two stories jump out at me tonight.
The first is the question of why Trump seems so desperate to stay in a job he clearly has no interest in doing. Today, reporters caught sight of Michael J. Lindell, the CEO of MyPillow, going into the White House. Lindell has been strong advocate of the idea that the 2020 election, which Democrat Joe Biden won by more than 7 million votes and by a vote of 306 to 232 in the Electoral College, was fraudulent. Washington Post photographer Jabin Botsford snapped an image of the papers Lindell was carrying with him, and the words on it seem to offer a plan for Trump to invoke martial law through the Insurrection Act.
Lindell later told reporters his meeting with Trump had been brief and unproductive, but the very fact he got a hearing testifies to Trump’s desperation.
That desperation suggests that Trump knows he is facing something bad the minute he is out of the presidency. It is reasonable to assume that trouble will come from the fact his immunity from prosecution under the 1973 Department of Justice memo saying that a sitting president cannot be prosecuted will end at noon on January 20, 2021. It also seems likely that the American people are going to learn that some of the actions of the Trump administration cannot bear scrutiny.
Signs that there might be damaging information about the January 6 attack on the Capitol showed today. Stories of the fighting inside the building continued to emerge today, and the stories reveal armed insurgents who attacked with the belief that they were doing Trump’s bidding. Officers were badly outnumbered, and beaten with their own batons, American flags, and the “thin blue line” flag that those who fly it have insisted represents support for the police. Officer Christina Laury told NBC’s Jackie Bensen, ““I remember people swinging metal poles at us,” she said. “They were pushing and shoving. They were spraying us with bear mace and pepper spray.”
The assistant director of the FBI Washington Field Office, Steven M. D’Antuono, today told reporters that the department, working together with the Washington, D.C., U.S. Attorney’s Office, has identified more than 270 suspects involved in criminal activity around the Capitol on January 6, and law enforcement officers have more than 100 of them in custody. He noted that the FBI had received more than 140,000 photos and videos from the public, and warned perpetrators: “To those of you who took part in the violence, here’s something you should know: Every FBI field office in the country is looking for you.” He told reporters that the investigation was still in its earliest stages.
House Speaker Nancy Pelosi announced today that she has asked retired Lieutenant Russel Honore to lead a review of the security arrangements for last week, and warned that if lawmakers are found to have aided the insurgents, they will face consequences in Congress and also in court. While several agencies are investigating what led to last week’s crisis and why the Capitol Police were left unsupported for hours, Pelosi’s public statement was the first to acknowledge the swirling rumors that the insurgents might have had inside help.
News broke today that prosecutors in Georgia appear to be considering a criminal investigation against Trump for his efforts to bully election officials in the state into changing the results of the election. Michael J. Moore, the former United States attorney for the Middle District of Georgia, told New York Times reporters Richard Fausset and Danny Hakim: “If you took the fact out that he is the president of the United States and look at the conduct of the call, it tracks the communication you might see in any drug case or organized crime case. It’s full of threatening undertone and strong-arm tactics.”
We also learned today that New York prosecutors met yesterday with Trump’s former fixer Michael Cohen to ask about Trump’s finances, especially his relationship with Deutsche Bank, which continued to lend to him even after other sources of financing dried up.
And yet another story emerged today that reflects badly on the administration. Its vaccination rollout is far behind where officials had promised it would be by now, and three days ago, on January 12, Secretary of Health and Human Services Alex Azar announced the government would no longer hold back second doses of the vaccine, expecting that pharmaceutical companies could keep pace and produce enough vaccines for the second dose as it was needed. The popular understanding was that they had held back half the available doses for that second necessary shot.
But today we learned that when Azar made that announcement, there was no reserve; the available vaccines had already been distributed. State health officials are outraged that vaccines they had counted on are not available, another sign of just how chaotic the vaccine rollout has been. Chicago Public Health Commissioner Allison Arwady told Washington Post reporters Isaac Stanley-Becker and Lena H. Sun, “I have stopped paying a whole lot of attention to what is being said verbally at the federal level right now.”
Tonight, Azar handed his resignation to Trump, effective at noon on January 20, the minute Trump leaves office. His resignation letter touts the administration’s “remarkable response to the pandemic” and insists that “our early, aggressive, and comprehensive efforts saved hundreds of thousands or even millions of American lives.” It goes on to list what he considers the many triumphs of the administration in health care. Azar appears to suggest that he is resigning because of “the actions and rhetoric following the election,” although he never identifies Trump as being behind those actions and rhetoric.
In light of all that has happened in the past two weeks, it seems noteworthy that Trump’s appointees in the Pentagon stopped sharing information with Biden’s team in mid-December. Trump appointees also refused to share information with Biden’s people about their plan for the coronavirus vaccine. When they finally did, Biden expressed concern at what seemed to him a lack of a detailed plan. Azar dismissed Biden’s concerns as “nonsense.”
If Trump’s eagerness to cling to the presidency and cover up his actions is one of today’s stories, the other is that President-Elect Joe Biden is stepping into the space the current president has abandoned. He is taking on the coronavirus crisis with the seriousness it deserves. The pandemic has reached appalling levels, with well over 3000 deaths and more than 200,000 infections every day. Almost 390,000 of us have died of Covid-19 to date, and a far more contagious version of the disease is spreading.
In a speech today, Biden announced he will use the Federal Emergency Management Agency (FEMA) and the National Guard to build clinics to distribute the coronavirus vaccine, and that he will make sure doses are available at local pharmacies. He promised to invoke the Defense Production Act—a law that lets the government tell a company what to make and then guarantees a market for all of that item it produces-- to guarantee there are enough supplies of vials, syringes, needles, and so on, to move the vaccine and get it into people’s arms.
“This will be one of the most challenging operation efforts ever undertaken by our country, but you have my word,” Biden said. “We will manage the hell out of this operation.”
—-
LETTERS FROM AN AMERICAN
HEATHER COX RICHARDSON
#Letters From An American#Heather Cox Richardson#political#January 6 2020#insurrection#sedition#corrupt GOP#criminal GOP
3 notes
·
View notes
Text
What does 'recovered from coronavirus' mean? 4 questions answered about how some survive and what happens next
by Tom Duszynski

Recovery is the result for most coronavirus patients. AP Photo/Tony Dejak
The coronavirus is certainly scary, but despite the constant reporting on total cases and a climbing death toll, the reality is that the vast majority of people who come down with COVID-19 survive it. Just as the number of cases grows, so does another number: those who have recovered.
In mid-March, the number of patients in the U.S. who had officially recovered from the virus was close to zero. That number is now in the tens of thousands and is climbing every day. But recovering from COVID-19 is more complicated than simply feeling better. Recovery involves biology, epidemiology and a little bit of bureaucracy too.
How does your body fight off COVID-19?
Once a person is exposed the coronavirus, the body starts producing proteins called antibodies to fight the infection. As these antibodies start to successfully contain the virus and keep it from replicating in the body, symptoms usually begin to lessen and you start to feel better. Eventually, if all goes well, your immune system will completely destroy all of the virus in your system. A person who was infected with and survived a virus with no long-term health effects or disabilities has “recovered.”
Your immune system finds and destroys viruses in the body, and will remember invaders it has seen before. Keith Chambers/Science Photo Library via Getty Images
On average, a person who is infected with SARS-CoV-2 will feel ill for about seven days from the onset of symptoms. Even after symptoms disappear, there still may be small amounts of the virus in a patient’s system, and they should stay isolated for an additional three days to ensure they have truly recovered and are no longer infectious.
What about immunity?
In general, once you have recovered from a viral infection, your body will keep cells called lymphocytes in your system. These cells “remember” viruses they’ve previously seen and can react quickly to fight them off again. If you are exposed to a virus you have already had, your antibodies will likely stop the virus before it starts causing symptoms. You become immune. This is the principle behind many vaccines.
Unfortunately, immunity isn’t perfect. For many viruses, like mumps, immunity can wane over time, leaving you susceptible to the virus in the future. This is why you need to get revaccinated – those “booster shots” – occasionally: to prompt your immune system to make more antibodies and memory cells.
Since this coronavirus is so new, scientists still don’t know whether people who recover from COVID-19 are immune to future infections of the virus. Doctors are finding antibodies in ill and recovered patients, and that indicates the development of immunity. But the question remains how long that immunity will last. Other coronaviruses like SARS and MERS produce an immune response that will protect a person at least for a short time. I would suspect the same is true of SARS-CoV-2, but the research simply hasn’t been done yet to say so definitively.

A coronavirus test kit. Necessary before a person can be declared officially recovered. AP Photo/David J. Phillip
Why have so few people officially recovered in the US?
This is a dangerous virus, so the Centers for Disease Control and Prevention is being extremely careful when deciding what it means to recover from COVID-19. Both medical and testing criteria must be met before a person is officially declared recovered.
Medically, a person must be fever-free without fever-reducing medications for three consecutive days. They must show an improvement in their other symptoms, including reduced coughing and shortness of breath. And it must be at least seven full days since the symptoms began.
In addition to those requirements, the CDC guidelines say that a person must test negative for the coronavirus twice, with the tests taken at least 24 hours apart.
Only then, if both the symptom and testing conditions are met, is a person officially considered recovered by the CDC.
This second testing requirement is likely why there were so few official recovered cases in the U.S. until late March. Initially, there was a massive shortage of testing in the U.S. So while many people were certainly recovering over the last few weeks, this could not be officially confirmed. As the country enters the height of the pandemic in the coming weeks, focus is still on testing those who are infected, not those who have likely recovered.
Many more people are being tested now that states and private companies have begun producing and distributing tests. As the number of available tests increases and the pandemic eventually slows in the country, more testing will be available for those who have appeared to recover. As people who have already recovered are tested, the appearance of any new infections will help researchers learn how long immunity can be expected to last.

Drive-by testing stations are opening across the U.S. as tests become more available. AP Photo/David J. Phillip
Once a person has recovered, what can they do?
Knowing whether or not people are immune to COVID-19 after they recover is going to determine what individuals, communities and society at large can do going forward. If scientists can show that recovered patients are immune to the coronavirus, then a person who has recovered could in theory help support the health care system by caring for those who are infected.
Once communities pass the peak of the epidemic, the number of new infections will decline, while the number of recovered people will increase. As these trends continue, the risk of transmission will fall. Once the risk of transmission has fallen enough, community-level isolation and social distancing orders will begin to relax and businesses will start to reopen. Based on what other countries have gone through, it will be months until the risk of transmission is low in the U.S.
But before any of this can happen, the U.S. and the world need to make it through the peak of this pandemic. Social distancing works to slow the spread of infectious diseases and is working for COVID-19. Many people will need medical help to recover, and social distancing will slow this virus down and give people the best chance to do so.

About The Author:
Tom Duszynski is the Director of Epidemiology Education at IUPUI
This article is republished from our content partners over at The Conversation under a Creative Commons license.
30 notes
·
View notes
Text
Three years ago I was in a serious wreck that wasn’t my fault. It resulted in three horrible back surgeries that culminated with a 12 level fusion with rods and screws. I’ve been on narcotic pain meds the whole time. I’m finally experiencing exponential improvement. The struggle ahead now is getting off the narcotics.
I’ve been through this a number of times before with over 20 abdominal surgeries over a 37 year span of time. The older I get the harder it is to kick the pills. I’m 100% dependent on them now. I intend to chronicle the journey here.
The first thing it takes is an acceptance that some uncomfortable times lay ahead. Bouts of radical anxiety and insomnia. Mental toughness is called for along with the knowledge it won’t be fatal but there might be times I’ll wish I no longer existed. My goal however is to be free of narcotics within three months. At my age (67) it’s dangerous in Covid times as narcotics impair the immune system.
I’ll be updating this blog religiously and rereading my entries to affirm my commitment. I’m open to any advice or comments along the way.
Installment Two...
I picked up a script for valium yesterday and had my first night in forever without a pain pill. Only had two pain pills this morning instead of usual three. Went five hours before taking last dose of the day of two more at noon. Four a day, down from ten or twelve just a month ago. Picking up steam.
Time for some honesty here. Countless times I’ve feigned agony in order to get my wife (THE KEEPER OF THE PILLS) to hand me up to three early. Had nothing to do with pain but more just to feel centered and normal. This is your ultimate proof you’re snared and completely dependent. This is when you’re lying constantly.
I have an observation I don’t entirely understand. When my consumption of pills was ravenous I was always adamant about getting off them. When out of necessity the amount had to be cut in half I was longing for the previous higher amount. Confused opioid receptors talking to the rest of my brain.
One thing I’m completely mortified by is the way I subtly manipulated a few others into generously sharing their pain pills. I did it by lying that doctors refused to prescribe them to me. I even intimated a few times I was suicidal because of my pain level. Lies lies and more lies. I was solely after the buzz. I’ve heard other people on pain meds awhile say they had no affinity or attraction to them. They complained such things as they kept them sleepy or caused disturbing dreams. They were the people who never finished a script. I’m one of those who gets a switch thrown in my brain immediately that tells me all I need is a steady intake of more more more.
I guess that’s the defining characteristic of an addictive personality. It must be something you’re hard wired for. I find the disease concept of addiction laughable. I’ve only known a few others like me and when we’d get pills from each other we fastidiously kept track of what we were owed back. Loan shark collection tactics weren’t out of the question.
Next installment will have the story of a younger brother who was hopelessly addicted to narcotics and his tragic end.
The Story of Brother Kenny
I had a younger brother once who enlisted in the Army. He developed back issues while stationed in Germany and was diagnosed with ankylosing spondylitis. He eventually was awarded a full service related disability which payed him $3,300 monthly in the 90’s. Of course he opted not to work.
Back then you could still do a walkin off the street to most doctors offices and leave with a generous narcotic script. Kenny claimed his back condition was unbearably painful even though I read the condition usually only caused mild discomfort. He became a prolific doctor shopper. Eventually you could never see him when he wasn’t fully under the influence of huge narcotic doses.
I visited him one day and found him a blithering idiot. I told him I expected him to be dead within two months. He was visibly shaken. Nearly two months later I found him dead on his kitchen floor in his underwear. After the funeral people came for his body I found three different prescription pain meds from no less than five doctors. I’m convinced addiction runs in families. I, however, in many accumulated years of pain management never once od’d on pain meds. Kenny wasn’t so lucky and left us at age 47.
I took a large quantity of his meds home with me and hid them in my garage. I was very distraught over his death and someone gave me xanax pills which I took too much of. I decided to try and reverse the sedation with cocaine. My son later found me unresponsive and called an ambulance. I’m told I was comatose for three days during which my brother’s funeral had to be delayed. That was my greatest humiliating moral failure I’ve never forgiven myself for. I still believe I deserve a catastrophic event as punishment. I scarred my family and took years to rebuild trust.
Continuation...
It’s six days till next pain management appointment. I’ve managed to sneak and coerce enough extra doses that I’m nursing along at 2 pills a day instead of 7. I know that if I manage to sneak more I’ll be in misery a few days before next refill. I’ll have to visit with the doctor in extreme discomfort it’ll take all I have to hide from him. Somehow that matters little to me. Soon as my wife’s attention is diverted I’ll grab extra pills. It’s what that switch in my brain compels me to do.
I’ve gotten to the point that every aspect of my life seems dependent on having narcotics onboard. Visiting family, playing guitar, picking up groceries, even having grandkids over all require narcotic doses. My life doesn’t feel at all normal without it. I’d rather spend the entire day in bed than to not be able to take pills.
I remember six years ago when we moved onto this rural street with fabulous neighbors. The first street bbq we were invited to I was in withdrawals from morphine. I drank a helluva lot of moonshine to feel comfortable in my skin. My wife had to lead me home. I later had to apologize to the host who laughed it off thankfully.
I eventually attained a few years of complete normalcy I remember well. I played music in public and was comfortable around people I didn’t know well. It was a great time. Then came a cervical fusion surgery and months later lumbar fusion after a car wreck. Back on pills I desperately needed for horrible pain. Back to the switch in my brain being thrown. I’m recovered enough now it’s an abject lie to claim I still need them. I long for the normalcy again.
A goal I have is to not take a handful of pills when I pick up next refill again. I seriously doubt I’ll attain the goal but have ascribed it as a benchmark I’ll have to meet if I’m to be successful getting off this nightmare roller coaster. I’m like a dual personality at war with myself. Neither has the power to overcome the other.
I’m waiting for a delivery of thc gummies a cousin is sending me from Michigan. I’ve used them before and had better pain control with them. I can cut pain meds dosage in half when combined with thc gummies. I intend to try a rapid taper by using thc which I could always stop with no issues. I know I’m gonna have lingering discomfort for awhile. I’ll likely end up getting xanax from my long time primary doctor for the anxiety, insomnia and restless leg that hangs around a week or two. We’ll see how this goes. Pain meds have been in my life too long. The pain from the fusion is at a level I think I can tolerate with mental toughness now. Here’s hoping.
April 22, 2021
Yeah I know... I’ve not written anything in awhile. Short whirlwind of activity. I got my accident settlement money and we bought a bus type motorhome and had a big pool installed. Also had to go out of state for a week for a family member’s funeral. That’s my excuse.
As for the pills... the last quantity prescribed was exactly half the amount of a few months back. I was still down to none by the day before the appointment just like the previous three times. Sneaking pills when my wife’s attention is diverted has become an art form. It’s compulsive behavior that embarrasses me but I seem powerless to overcome. At least the rapid tapering regimen is in full swing and being successfully adhered to. I’ll end this session by reiterating I’m tired of being snared by these fucking pills and look forward to the glorious day they are out of my psyche.
Long overdue update. In rereading this treatise I’ve realized my initial projection of being off pain pills in a few months is in serious jeopardy. The last dosage reduction caused me to hit a wall. The pain levels have increased and I’m walking like a bent over geriatric cripple again. I’m having to realize pills will apparently be in my future for an indeterminate time. That means the lies and stealthy thievery will continue. I so wish I could conquer this compulsion but the fact remains. I can’t feel normal without them, even though after so much time on them the relief is only very minimal.
I can’t stress enough how this is not where I want to be. I long for the time again when these fuckin pills are a distant memory. If not that then I long to take them responsibly. My brain won’t allow that. It isn’t even a choice available to me. The longing to simply cease to exist pops up now and again but thankfully I can’t do that to my family. I’m considering starting a podcast to address these issues. I know millions of people like me exist in this hell. I’m not sure if I could do it other than as an anonymous person. Who the fuck wants the world to know they’re stuck in this void?
1 note
·
View note
Link
Delta Air Lines was hoping to restart flights next month from New York to Athens and Lisbon, two popular summer destinations, but it will probably have to wait a little longer.
The European Union is planning to bar most Americans even as it welcomes travelers from more than a dozen other countries next week, dealing a blow to Delta and other airlines hoping to revive their business as travel across the Atlantic Ocean typically peaks.
International flights make up a minority of flights for U.S. airlines but are typically much more profitable than domestic ones. And flights to and from Europe are generally the most important. U.S. and European airlines had reduced the number of available seats on flights connecting the two markets by about 75 percent next month compared with last July, according to the aviation data provider OAG. A travel ban on Americans, which European Union officials confirmed on Friday, will probably lead to even deeper cuts.
“It’s a huge deal,” said John Grant, a senior analyst at OAG. “It is by far the jewel in the crown for many major airline networks, in terms of both revenue and profitability.”
Last year, flights across the Atlantic, to Europe and other destinations, accounted for about 17 percent of passenger revenue for United Airlines, or about $7.4 billion. Such flights generated about 15 percent of all passenger revenue for Delta, or $6.4 billion, and about 11 percent of passenger revenue, or $4.6 billion, for American Airlines. They were particularly important to United and Delta, generating a quarter of passenger profits last year, according to the Transportation Department.
Tens of millions of people flew between the United States and European Union countries in 2019. Many traveled for business to and from cities like New York, Los Angeles and San Francisco and Amsterdam, London, Paris and Frankfurt. Many others fanned out farther to vacation, particularly in the summer, when international flights are often nearly full as American families jet off to Italy and Greece, and Europeans check out New York and California.
Of course, travel between the United States and the European Union has been restricted since March, when governments on both sides of the Atlantic barred most visitors to prevent the spread of the coronavirus, with exceptions for repatriations and “essential” travel by medical professionals.
At the time, the United States had just over 1,100 coronavirus cases as the virus spread extensively in Italy and Spain. Today, the United States leads the world with more than 2.4 million cases, and infections are surging in Arizona, California, Florida, Texas and other states. As a result, European Union officials have decided to keep Americans out — along with travelers from dozens of other countries — for fear that they could further spread the virus.
Because of the size of the United States, a vast majority of tickets sold by American carriers are for domestic travel. Those flights have led the industry’s recovery, as Americans slowly start to visit friends and family and make limited vacation plans, a pattern unfolding in countries around the world. Higher-profit business and international travel is expected to follow far behind.“I think international travel is probably going to lag domestic by up to 12 months,” Ed Bastian, Delta’s chief executive, told shareholders on a call last week, citing travel bans around the world as one reason.
The large difference in demand for domestic and international travel is also reflected in flight schedules. American, for example, plans to operate about 55 percent as many domestic flights next month as it did last July, but only about 20 percent as many international flights. The airline has delayed restarting service between the United States and a number of European destinations until August, a month later than planned.
The Coronavirus Outbreak
Frequently Asked Questions and Advice
Updated June 24, 2020
What’s the best material for a mask?
Scientists around the country have tried to identify everyday materials that do a good job of filtering microscopic particles. In recent tests, HEPA furnace filters scored high, as did vacuum cleaner bags, fabric similar to flannel pajamas and those of 600-count pillowcases. Other materials tested included layered coffee filters and scarves and bandannas. These scored lower, but still captured a small percentage of particles.
Is it harder to exercise while wearing a mask?
A commentary published this month on the website of the British Journal of Sports Medicine points out that covering your face during exercise “comes with issues of potential breathing restriction and discomfort” and requires “balancing benefits versus possible adverse events.” Masks do alter exercise, says Cedric X. Bryant, the president and chief science officer of the American Council on Exercise, a nonprofit organization that funds exercise research and certifies fitness professionals. “In my personal experience,” he says, “heart rates are higher at the same relative intensity when you wear a mask.” Some people also could experience lightheadedness during familiar workouts while masked, says Len Kravitz, a professor of exercise science at the University of New Mexico.
I’ve heard about a treatment called dexamethasone. Does it work?
The steroid, dexamethasone, is the first treatment shown to reduce mortality in severely ill patients, according to scientists in Britain. The drug appears to reduce inflammation caused by the immune system, protecting the tissues. In the study, dexamethasone reduced deaths of patients on ventilators by one-third, and deaths of patients on oxygen by one-fifth.
What is pandemic paid leave?
The coronavirus emergency relief package gives many American workers paid leave if they need to take time off because of the virus. It gives qualified workers two weeks of paid sick leave if they are ill, quarantined or seeking diagnosis or preventive care for coronavirus, or if they are caring for sick family members. It gives 12 weeks of paid leave to people caring for children whose schools are closed or whose child care provider is unavailable because of the coronavirus. It is the first time the United States has had widespread federally mandated paid leave, and includes people who don’t typically get such benefits, like part-time and gig economy workers. But the measure excludes at least half of private-sector workers, including those at the country’s largest employers, and gives small employers significant leeway to deny leave.
Does asymptomatic transmission of Covid-19 happen?
So far, the evidence seems to show it does. A widely cited paper published in April suggests that people are most infectious about two days before the onset of coronavirus symptoms and estimated that 44 percent of new infections were a result of transmission from people who were not yet showing symptoms. Recently, a top expert at the World Health Organization stated that transmission of the coronavirus by people who did not have symptoms was “very rare,” but she later walked back that statement.
What’s the risk of catching coronavirus from a surface?
Touching contaminated objects and then infecting ourselves with the germs is not typically how the virus spreads. But it can happen. A number of studies of flu, rhinovirus, coronavirus and other microbes have shown that respiratory illnesses, including the new coronavirus, can spread by touching contaminated surfaces, particularly in places like day care centers, offices and hospitals. But a long chain of events has to happen for the disease to spread that way. The best way to protect yourself from coronavirus — whether it’s surface transmission or close human contact — is still social distancing, washing your hands, not touching your face and wearing masks.
How does blood type influence coronavirus?
A study by European scientists is the first to document a strong statistical link between genetic variations and Covid-19, the illness caused by the coronavirus. Having Type A blood was linked to a 50 percent increase in the likelihood that a patient would need to get oxygen or to go on a ventilator, according to the new study.
How many people have lost their jobs due to coronavirus in the U.S.?
The unemployment rate fell to 13.3 percent in May, the Labor Department said on June 5, an unexpected improvement in the nation’s job market as hiring rebounded faster than economists expected. Economists had forecast the unemployment rate to increase to as much as 20 percent, after it hit 14.7 percent in April, which was the highest since the government began keeping official statistics after World War II. But the unemployment rate dipped instead, with employers adding 2.5 million jobs, after more than 20 million jobs were lost in April.
What are the symptoms of coronavirus?
Common symptoms include fever, a dry cough, fatigue and difficulty breathing or shortness of breath. Some of these symptoms overlap with those of the flu, making detection difficult, but runny noses and stuffy sinuses are less common. The C.D.C. has also added chills, muscle pain, sore throat, headache and a new loss of the sense of taste or smell as symptoms to look out for. Most people fall ill five to seven days after exposure, but symptoms may appear in as few as two days or as many as 14 days.
How can I protect myself while flying?
If air travel is unavoidable, there are some steps you can take to protect yourself. Most important: Wash your hands often, and stop touching your face. If possible, choose a window seat. A study from Emory University found that during flu season, the safest place to sit on a plane is by a window, as people sitting in window seats had less contact with potentially sick people. Disinfect hard surfaces. When you get to your seat and your hands are clean, use disinfecting wipes to clean the hard surfaces at your seat like the head and arm rest, the seatbelt buckle, the remote, screen, seat back pocket and the tray table. If the seat is hard and nonporous or leather or pleather, you can wipe that down, too. (Using wipes on upholstered seats could lead to a wet seat and spreading of germs rather than killing them.)
What should I do if I feel sick?
If you’ve been exposed to the coronavirus or think you have, and have a fever or symptoms like a cough or difficulty breathing, call a doctor. They should give you advice on whether you should be tested, how to get tested, and how to seek medical treatment without potentially infecting or exposing others.
“Demand is increasing, but those numbers, while they’re increasing, are still a fraction of what they were last year, particularly internationally,” Doug Parker, American’s chief executive, told shareholders this month.
The International Air Transport Association called on governments this week to avoid quarantine measures that can discourage travel in favor of less severe measures, like asking sick passengers to stay home and increasing testing.
After dropping to record lows in April, the number of people going through U.S. airport checkpoints is up to about 20 percent of last year’s levels, according to the Transportation Security Administration. That’s not nearly enough to sustain the nation’s largest airlines, which are losing tens of millions of dollars every day, but it has restored a sense of vitality to an industry ravaged by the pandemic.
And while international travel could remain subdued for months, airlines have found other ways to drive revenue, including operating cargo-only flights, which are in high demand.
“That’s going to stay in place until passenger demand starts to recover,” Scott Kirby, United’s chief executive, said at an investor conference last month. “So there’s an international hedge that cargo is going to stay strong until passenger demand recovers, and then passenger demand will take over for it.”
9 notes
·
View notes
Text
Traveling After a Pandemic

If you knew the angst that went into simply agreeing on a title for this piece, you would laugh. This is our current world. We have a scarcity mindset, mixed with some fear over what we’ve been through this past year. I’ve had seasons of scarcity, fearfulness, and oh the worry. Worry laced everything in 2020 and tied it in a bow, so when I shared my potential title, I was met with, “but we’re still IN a pandemic.” Are we?
According to historians, pandemics typically have two types of endings: the medical, which occurs when the sicknesses or death rates plummet, and the social, when the epidemic of fear about the disease wanes.
“When people ask, ‘When will this end?’ they are asking about the social ending,” said Dr. Jeremy Greene, a historian of medicine at Johns Hopkins.
In other words, an end can occur not because a virus has been vanquished but because people grow tired of panic mode and learn to live with a virus.
I chose the title I did, because, for me, it is the truth. The cool thing is that you get to decide for yourself, your family, and your life experience what is true for you. After this way-too-long discussion with some fellow authors, there was a moment when I said, “no more.” No longer will I live in fear, and no longer will I worry myself about what may happen. Death rates have plummeted (one of the medical ends to a pandemic) and the virus strand is weakening. This is great news! Precautions I’ve taken since last March can now soften a bit. I definitely won’t worry about things out of my control. An example of something out of my control… what others think of my life decisions.

When some of the world lifted their restrictions on air travel, my husband and I booked a few flights to some of our favorite places. “You’re going to travel out of the country, right now?” It echoed for several days, but it’s just one more reminder to make your own rules for your life. Yes, the pros outweighed the cons, for us, and that is enough. I wondered what it would be like “out there,” and what the experience would really be, and curiosity squashed fear. We considered our safety, security, and health, in this decision to fly internationally, and we booked accordingly. You see, for us, the world is vast and there’s opportunity to expand one’s life perspective with traveling and seeing the world. Staying at home doesn’t make sense to us, as a long-term decision, especially if health and vitality are the goal. We take good care of our health, and we take proper precautions, so for people in our situation, travel is an option. If you have the travel bug, I invite you to get out there again, too. I’ll explain why later in this article.
When the COVID-19 flu strand pushed us into a global pandemic, my husband and I were crushed. We had four trips we now had to cancel or that were canceled on us. Birthdays, anniversaries, France, Spain, British Virgin Islands, and Cabo San Lucas all vanished off the calendar. We were sad but worked to quickly shift mindsets. We would have different types of adventures for a while. We would make an adventurous life at home, under these new daily, safety standards. We would enjoy the Texas beach house more. We would spend time enjoying new hobbies, activities and a slower pace. The re-wiring of adventure expectations took some ebb and flow (especially by me—I already purchased new outfits for Spain and for France), and while I look back on the memories, we made last year, I am grateful for them. More on that later… let’s get to the good stuff. Traveling internationally, after a pandemic, was different but worth it. It’s easier if you plan ahead, set some new expectations, and give just about everything and everyone some added grace.
Here are my tips and awareness (based on separate trips to Cabo San Lucas, and Riviera Maya, Mexico, flying commercial airlines, and staying at a resort & spa property (not private residence):
1. Clean up your diet, increase your fitness routine, and be impeccable with nutritional supplements months before traveling. Do a 7-14 day detox if possible. This is key! Don’t travel with a weak immune system.
2. Don’t fight the masks. It’s happening, and it’s nobody’s preference. (At least, I don’t think anyone loves wearing them?) As of today, wearing a mask is required in all airports, on all commercial aircraft, and it was required in the lobby areas and restaurant entries. You can wear a mask whenever you want, but these are the places a mask was required. I wore a separate mouth and nose covering for the flight that met the required standards. It was more comfortable than my mask and worked well.
3. Bring your own anti-bacterial soap. At the end of each day, it felt nice to scrub away the day with an extra anti-bacterial protection. Even if you don’t usually use an anti-bacterial soap, use one now for ease of mind. One bar of Dial soap lasted 10 days.
4. Pack a pen! In addition to the usual customs and immigration forms, there’s a new COVID disclaimer form to fill out and turn in upon arrival at the airport and again at your lodging.
5. Bring your usual daily multi-vitamin, but add in the following every day: Zinc, an immune modulator, extra vitamin C & D. These helped me feel armed against new elements, foods, and the new environments.
6. Expect delays at check-ins. We arrived at the airport, our hotel, and even at restaurants that each had their own added health screenings or checks. The oddest one was a device you step into (think air brush tanning days) that sprays you with an antimicrobial solution. It’s light and dries quickly, and at its worst, just slightly annoying. They spray your baggage on arrival at the hotel with this solution, too. Some take your temperature, and some offer you (and expect you to take) hand sanitizer.
7. Make reservations! Most restaurants are requiring them to comply with the distancing needs of the tables (Mexico restaurants and bars filled up but we were spaced out really well.) Don’t expect to just show up, without a reservation, and get seated anywhere. If it happens, yay!
8. Hire private ground transportation. This minimizes your exposure to new taxi cabs and drivers each time you need to go somewhere. Walk whenever and wherever you can. Exercising keeps everything moving, even the bad bacteria and virus strands, and these getting stuck in our body cause the problems.
9. Tip generously, when appropriate. Hearing the stories of how this year has been for different people, really opened my eyes to the outlier issues we’re now facing, outside of the actual sickness. By traveling soon, you are helping to reverse some long-standing financial damage people and businesses are facing, due to closures and restrictions. Select local businesses, restaurants, foods, and entertainment when possible. You can immerse yourself into the culture of where you’re visiting, and meet some wonderful people at the same time.
10. Call ahead and ask what’s new due to the pandemic. Being aware of expectations, protocols, and changes will allow you to prepare yourself accordingly and to enjoy the experience better. None of us are at our best when expectations are not met. Proactively do some research and set yourself up for success.

Go explore! My soul came alive immediately as I started roaming one of my favorite areas of Mexico. Being in the elements, the sun, especially, taking in the sights, sounds, and feelings filled me up with vitality. Don’t wait any longer! Find your next adventure spot and start booking. I am grateful for our continued health, and we remain protective of it. You are in control of how you protect yourself, and it is possible to feel safe and protected while traveling the beautiful world again. Be respectful of others’ “house rules,” as everyone is trying to help everyone feel as comfortable as possible right now, and by respecting these efforts, we all get to feel a little more freedom.
For us, the pandemic was a temporary situation, not a permanent change to our way of life. This travel experience has been educational for us, as many things felt differently than what we’re used to, but necessary for where we currently are with pandemic concerns. While we hope even more of the restrictions lift and more countries open up to American travelers, we hope some of the new practices never leave. Airplanes, airports, hotel rooms, and bathrooms have never been cleaner! I see people giving everyone space and washing their hands longer. Que Maravilla! On that note alone, take a deep breath and go explore somewhere new. Let me know what you find!
#mexico#travel#healthytraveler#pandemictravel#eldoradoresorts#pueblobonitoresorts#detox#bewell#beyou#laceypruett
1 note
·
View note
Text
So, here goes...
I have been asked to comment on Sweden’s handling of the Corona Virus/Covid-19 pandemic and why Sweden has opted to go a different way from the rest of Europe and our immediate neighbors and, frankly, most of the countries in the world that have experienced an outbreak of the virus.
Let me first begin by saying that this is written by someone who is not an epidemiologist, nor in no way even remotely associated with any medical profession. This is my interpretation and shall in no way what so ever be taken at a weight even slightly near the official information of the Swedish government or Folkhälsoinstitutet (the “peoples health institute” is the direct translation) the government organization that is responsible for handling the current crisis. Official information is available HERE (in English).
As I write this (April 11, 7p.m) the current statistics are as follows:
Confirmed number of infected in Sweden: 10 151
Confirmed deaths: 887
People currently in intensive care: 774
Source: Folkhälsomyndigheten (updated April 11, 14.02)
In case anyone is interested in the total spread of contamination and of deaths over the country I will add a picture at the end of this post. Now, let’s get on to the topic proper.
Early on in the decision was made to fokus on protecting the risk groups in the Swedish society – meaning that protecting the elderly and the sick was the number one focus on the plan to battle the virus. People above the age of 70 were told to self isolate and only go out to get the essentials. Everyone were encouraged to not visit the elderly in order to keep the risk of infecting them as low as possible. At the same time everyone that showed even the slightest symptoms: sniffles, a headache, a sore throat – where told to go into self isolation until they had been free of symptoms for at least two days. We were encouraged to help each other in those situations, friends and family doing some shopping and delivering groceries and essentials, or just doing online shopping. At the same time the government issued a decree that all higher education – meaning High school and university – education that is not mandatory, should be conducted as distance education. However, schools in year 1 to 9 were still to be open as usual (and still are). The reason for keeping the schools open for the younger children is that 1, children are not a primary carrier of the virus and 2, as a mean to make sure that essential functions in society will have staff – primarily the health care sector. If the schools close down then the parents will have to stay at home in order to care for them.
Where Sweden has differed from the rest of the world in the most obvious way is that we have not gone into a full lockdown mode. We are still, if we feel healthy and don’t have any symtoms, encouraged to go out and to meet friends, go to restaurants and the like – one of the reasons is that we need to have a slow, semi controlled spread in society in order to create a herd immunity – the people that are currently moving around are primarily those that are not in the risk groups – they will, if they catch the virus, get a mild infection – or, as in my case, a semi mild infection, but they will not need to visit the hospital or get medical treatment other than which you can get from online consultations. This is important to slow down, but not to stop, the spread of the virus in society at large. If we completely stop the spread the risk is that it will come back again, and at force, as soon as the quarantine is lifted – it is better, according to the Swedish authorities, to allow the infection to spread at a slow pace and create a wider immunity whilst keeping the groups that are at risk of needing intensive care or facing death if infected as safe as possible.
Many companies have started different work from home programs letting their employees do just that, it seems to work well. The company that run the public transport has a campaign out now that states that “if you are not an essential worker, please don’t travel with us right now”. People are complying. We are still out and about, we take walks, we visit friends – sometimes even go out for a beer. But in general it is, as expected, much more sombre. We stay at home – because we do not want to risk to get infected or accidentally spreading it to someone we love or care about – or someone we don’t know.
Other actions that have been taken is that there is a limit on the size of groups of people that can gather. It started out at a 500 person limit, which has now been lowered to 50 people. We are no longer allowed to order alcohol at bars, it is only table service allowed, and the tables must be “well spaced”. Right now the authorities are out and checking that restaurants follow the guidelines. If they don’t they will be forced to close. In general I would say that people do follow the guidelines. We are generally fairly well behaved like that. The Germans of the north, we are. We have trust in the machine – which is the reason why the person that is in the lime light during this trying time is not the King nor the prime minister, but rather a middle level management bureaucrat: Anders Tegnell – the chief Epidemiologist at Folkhälsoinstitutet.
The reason for this trust in the machine depends on many things I’d say. We have historically had a large state with a fairly large control system – the unofficial motto of the Social Democrat party has been “trust in the state, we will make it right”. Another aspect is that we have not really been in a war since 1809 (we don’t count the Norwegian campaign of 1814 because: Norway). We have not needed the consolidating power of a church or a sovereign to help us through trying times, and times of national crisis – as so many countries experienced during the 20th century. Sweden came through the wars unscathed, for good and for bad. And it has made us into a people of secular individualist with a strong belief in a all knowing state. Silly paradoxes we are.
So, now to the important stuff: has this tactic worked. Yes and no, I am sad to say. The goal of keeping the number of cases that need intensive care and hospitalization down as to not over crowd the hospitals have worked. There is still ample room at the intensive care units around the country. The staff are working like madmen and they deserve all the recognition that they get for their hard work. Unfortunately the authorities did not quite count on the virus getting such a grip on the treatment homes for the elderly as it has. There has been a fairly wide spread of the disease in nursing homes across the country, leading to a large number of deaths. Also, the information about the disease in languages other than Swedish were slow to get spread leading to an unusually large representation of hospitalizations and deaths of people with other ethnical backgrounds; especially the Syrian/Assyrian-Swedish population and the Somali-Swedish population have been hard struck – many of the cases being linked to large weddings and funerals that occurred just before the pandemic started. The availability of information has been bettered since then, but naturally that is of very little comfort when loved ones are getting sick and dying.
Another tragedy is that is not limited to Sweden alone is that the people that are most sensitive to this disease are the elderly – and don’t think that I am putting anyone infront of another, but I have to say a particular part of this tragedy is that with our elder our history die – we have seen a large number of holocaust survivors pass the last days and weeks here in Sweden, and I am sure that we are not the only country where this has happened, and with them the voice of a horrible past die forever. We must be aware that this tragedy does not just strike us personally, when a loved one dies – but also as a human collective when the voices of the past slip away from us.
We are in a time now where it is more important than ever to remember.
As promised: a map. The left column is number of infected, the right column is reported deaths. Oh, and I should mention that we do not have mandatory testing for corona virus in Sweden. The decision was taken early on to only test the ones that were in need of hospitalization. So the number of infected are much likely higher.
If you have any questions, please send them to me and I will try to answer them, but please remember: I know nothing, really.
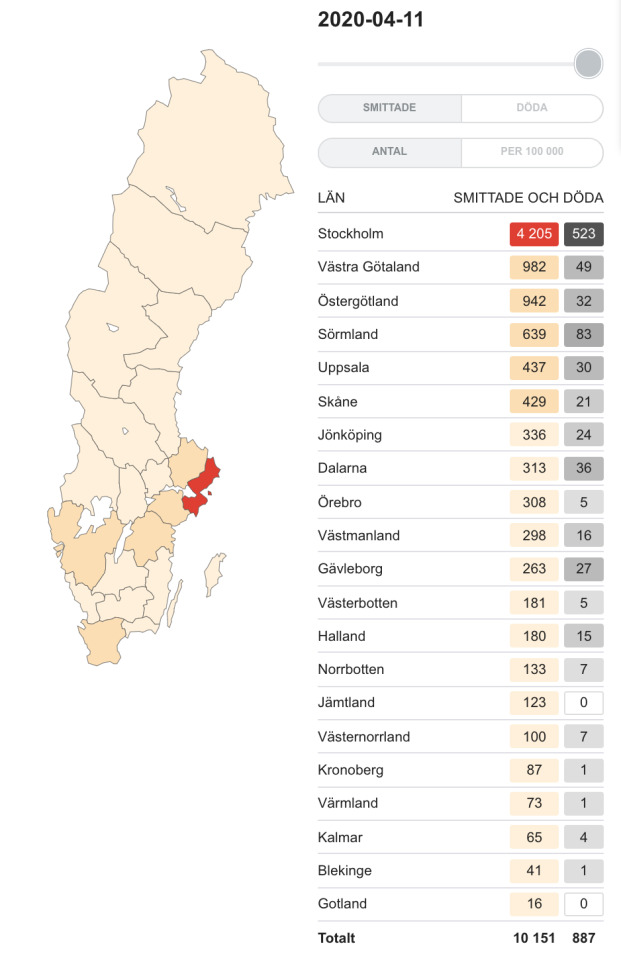
Update: I got a question about the age of the people that have died in Covid-19 in Sweden to date, and I did a quick search and found the following numbers on the official website (in Swedish):
1-9 yo: 0
10-19 yo: 0
20-29 yo: 3
30-39 yo: 2
40-49 yo: 4
50-59 yo: 34
60-69 yo: 64
70-79 yo: 228
80-89 yo: 362
90+: 190
Here is a picture of the live update page linked above with a quick English translation of the key items in case you want to check the page out for yourself.
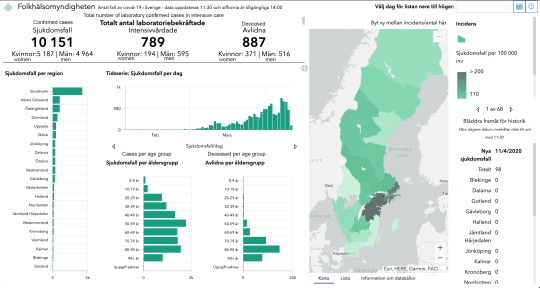
13 notes
·
View notes
Text
COVID-19 and the Epidemiology of Zoonotic Disease in Relationship to Modern Human Industry: Educated Guesses from an Amateur’s Brief Research
Wikipedia's basic description of the SARS-COV-2 says that while bats are the most likely natural reservoir, the genome of the virus as it exists in bats is just different enough from the human strain that there was probably an intermediate host between bats and humans. In other words, the virus probably did not come from people EATING bats, nor purchasing bats from the market, but perhaps it did come from going to the market to purchase bats for eating.
I find Wikipedia's explanation plausible because of an article I read on Chuangchn.org, which asserts that we get epidemics when an expansion of human activity into wild microbial reservoirs allows certain viruses to hit crowded populations with low immunity, be they livestock feedlots or slums full of severely stressed humans. Normally those reservoirs have buffers against infecting humans because of a great genetic variety among the wildlife, such that any one strain can only spread so far; as modern capitalism steadily reduces the size and genetic variety of wild populations, their attendant microbial parasites have fewer barriers against reaching humans.
So you get one virus running into, say, a vast pen of cattle, and as the cattle have no immunity, the virus faces very little selection pressure that would force a greater genetic variety. Instead the selection pressure is to spread as fast as possible, which means to grow as fast as possible, and the faster a virus grows, the more strain it places on the host, so within a short time the virus goes from benign to deadly.
And so you tend to get epidemics coming close on the heels of major capitalistic shifts in the concentration of living creatures. English outbreaks came in the era when they began to enclose their cattle in pens; the Spanish Flu started in the pigs of a Kansas stockyard shortly following the rise of American industrialized agriculture.
Admittedly these viral outbreaks can occur with direct human incursions into the wild, either by incorporating wild animals into modern markets or simply pushing industrialism into wild areas. Ebola seems to have appeared first in the 1970s with an English-owned cotton mill operation that planted itself in the central African jungle and occurred again every time that sort of industrialism increased its presence in the area. Likewise HIV is said to have come from humans eating "bushmeat", which is any manner of monkey meat, as if humans had not been doing such a thing before, so that they had no immunity to what they found within those animals -- maybe, then, they were going after bushmeat because their usual food sources were out of reach? Oh, wouldn't it be interesting if HIV and Ebola came from the same damn cotton mill!
This is not the case. According to the Chuangchn article, Ebola was first recorded in 1976 where the most common strain of HIV appears to come from early-20th-century Kinshasa, or should I say Leopoldville, the capital of the Belgian Congo and centerpoint for a great deal of environmental degradation and societal upheaval through modern capitalism. Bushmeat had been a common food source for a long time, with Simian Immunodefficiency Virus being endemic in wild primates. People used to catch SIV all the time. They resisted it well and fast enough that it could never spread from human to human. Then Leopoldville created a world where increased prostitution could spread syphilis more quickly, such that the ulcers which present the greatest danger of transferring SIV were all over the place, and SIV was now able to jump from one person to another fast enough to mutate into HIV.
Now as for Ebola and HIV, both of those diseases are more deadly than the diseases that seem to come from livestock concentration. One of them is a hundred percent fatal, the other fifty percent without treatment. Likewise the source of the Black Plague was Central or East Asian rodents moving into human agricultural areas due to climate change, and the disease itself appears to have an untreated mortality rate of thirty to sixty percent if bubonic, one hundred percent if pneumonic or Septicimic -- as if a wild microbe that hits human populations without an intermediary host is invariably more deadly than one that arises out of the intermediary host.
That's assuming the Plague hit humans directly through people eating gerbils in the manner of people eating Bushmeat to catch SIV, and that neither rats nor fleas were the intermediate host where the bacteria could go from benign to virulent. To compare the Black Plague to Ebola is also to conflate the behavior of viruses with bacteria. I do not know if they would react to certain selection pressure the same way.
All I know is that these microbes which become dangerous among crowded livestock seem to have a lower, or perhaps slower, mortality rate than the ones which develop from direct wild-to-human transfer. The zoonotic diseases that humans are supposed to have picked up from livestock at the beginning of human-animal domestication -- Tuberculosis, Smallpox, Cowpox, Glanders, Escheria Coli, and so forth -- generally have a much lower mortality rate than Ebola, with only Smallpox reaching the untreated mortality rate of the Black Plague --
In populations already exposed to the disease, at any rate. For virgin populations such as the entire Western Hemisphere circa 1492, the untreated mortality rate was something even Ebola could not match. It may simply be that the zoonotic diseases livestock herders are familiar with are less deadly because their most dangerous strains burned themselves out tens of thousands of years ago. In that sense, the only real difference between zoonotic diseases incubating in livestock and those hitting humans directly would be the novelty, where these wild diseases, being invariably new to us, have not yet burned through enough people to create a selection pressure towards less fatal strains.
One might argue that Rabies has been known for many thousands of years and remains as deadly as it ever was, and is a very good example of how dangerous a virus can be when it infects humans directly from the wild. But the fact that Rabies spreads though biting means that it's not viral in the same way as most other diseases. Despite the fact that the virus itself has an evolution rate similar to any other RNA virus, it doesn't have the transmission rate of most other RNA viruses, so I would expect that its effective rate of evolution is much too slow to force it into something less deadly.
In point of fact, of the seven major species in the Lyssavirus family, nearly all of them follow the same pattern as Rabies: bats as a wild reservoir, human transmission through biting, fatal if untreated, human transmission extremely rare. Only Mokola Virus is endemic in mammal populations like the Rabies we know, and then only in South Africa; as it has the possibility of being transferred by Mosquitoes, it may have a much shorter time scale for selection pressure than any other Lyssavirus and, as it happens, one of the two humans who contracted the disease recovered. Nor do the cats infected with Mokola Virus exhibit unprovoked aggression in the manner of Rabies. While all these strains appear to have evolved within the last 1500 years, only Mokola Virus appears to face enough selection pressure to evolve into a milder form. For the rest, they still run wild, and it will be a long, long time before they settle down.
Rabies remains deadly for being new in comparison to its evolutionary time scale, and HIV remains deadly for being new in relation to its own time scale, and Ebola remains deadly for being new in general, where livestock-zoonotic diseases have been facing more intense selection pressure for quite a while longer than these diseases direct from the wild. We're all virgin populations for Ebola, Rabies, and HIV like the Western Hemisphere was a virgin population for Smallpox. That's a more prosaic explanation for this discrepancy than some aspect of livestock that makes their epidemics less deadly...
Especially since James Gallagher at the BBC News says HIV is already adapting into a slightly less deadly form as it gets used to human immune systems.
And yet the initial outbreak of SARS in 2003 was entirely novel, it came from a wild vector and its case fatality rate was an average of nine percent. That looks like a case of a novel wild virus with direct transfer being much less than fatal. Palm Civets, there you go, there's the vector, right? Except that these palm civets were in the wild-animal MARKET, and the virus itself has a wild reservoir in bats, so if the civets were shoved in close together like any livestock then the disease would have developed within their population just the same as if they were all pigs. I can't say that SARS was a direct transfer from the wild.
As for this Novel Coronavirus...while Hubei does a lot of livestock operations but the pandemic has been traced to Wuhan's Huanan Seafood Wholesale Market, which also sells lots and lots of wild animals, quite similar to the meat market in Guandong where the 2003 SARS came from. As I imagine it, the virus started from one bat, incubated among wild animals crowded together, and developed in just the same way as 2003 SARS.
The fact that the virus appears to have a low variability among known genomic sequences stands in marked contrast to HIV, which has a great deal of genetic variability in its many subtypes, and Ebola, which is an entire genus of viruses, as well as the aforementioned seven species of Lyssavirus, of which Rabies is but one part. It is as if this novel Coronavirus hit a crowded population just once and took off from there, facing, as I said, no selection pressure to force genetic variety, where viruses picked up directly from the wild have competed against their wild hosts a long time before ever reaching humans.
I imagine the scenario as follows:
1. A living landscape in its proper state has a great deal of genetic variety among its multicelled organisms.
2. This variety creates an evolutionary selection pressure in their attendant microbial populations, which means these microbial populations will have a degree of genetic diversity matching the macrobial popluation.
3. Humans pushing their industry into these areas for the first time reduce the genetic diversity of the area, thereby reducing the diversity of immune responses, and letting certain microbes spread farther.
4. At the same time, humans pushing industry into these areas are coming across populations of wild microbes that still have a high degree of genetic diversity.
5. Humans doing the grunt work in this industrial push have many opportunities for contact with this population of wild microbes through direct contact with wild animals.
6. Wild microbes enter the human population with multiple strains, be they subtypes or whole species, where a wild microbe hitting a stockyard first would be only one or a very few strains.
7. Having a high degree of genetic variety from the start, they have much more chance to compete against human immune systems than the intermediary-incubated epidemics, so they are invariably more damaging to their human host.
8. By the same token, they cannot be endemic among human populations like the diseases that grew out of microbes hitting livestock operations, because as they have survived within wild macrobial populations that resist them well, they are optimized for surviving within a host and against virulence. Their methods of human-to-human transfer, be it saliva, sexual intercourse, or skin contact, have a low rate of success compared to the livestock-incubated diseases.
See for example Leprosy, which appears to have a wild reservoir in Red Squirrels, does terrible things to its victims, and...is not very contagious between humans.
The existence of Cholera complicates this picture because it is an incredibly deadly disease like Ebola, and it seems to be endemic to human populations, in contrast to Ebola which disappears until industry expands into the jungle again. And it is extremely virulent, without having a stealthy effect on humans. How does Cholera win the epidemic jackpot? By having its wild microbial reservoir in water. Water contaminated with fecal matter causes zooplankton to pick up the bacteria; oysters then eat the zooplankton; humans eat the oysters, and get sick; suddenly they’re contaminating the water with their own fecal matter and the disease is living free in the local water for a while, and everyone else gets it. Cholera is unusual for having a wild reservoir that is invariably close to human habitation, such that it remains endemic without becoming any less wild. Let us say, then, that Cholera is not endemic to humans, but is endemic to a source so close to them that it might as well be. It comes in waves, because it comes on the waves.
Perhaps not so unusual. There is a land-based wild reservoir that resembles that of Cholera. Once upon a time, there was once another extremely virulent and deadly disease in the manner of Cholera, called the English Sweating Sickness. It killed its victims in the space of hours, and had outbreaks from 1485 to 1551. The most likely source was a strain of Hantavirus with a wild reservoir in rodents. Like the schools of wild fish, its reservoir was constantly interacting with human populations, as rodents broke into human food stores. English Sweating Sickness has never been seen again, but Hantaviruses remain quite dangerous, enough so that a discovery of mouse droppings in a human space demands immediate and thorough cleanup.
I find it telling that the aforementioned article mentions this English Sweating Sickness coming in a time of agricultural and social upheaval. I also find it telling that Wikipedia attributes the first major recorded Cholera epidemic to increased commerce, pilgrimage and migration. Just like folks in China hitting the SARS viruses, eh? Wuhan’s meat market has a bunch of wild animals to sell because people are running into them more, as they push capitalist industry further into wild spaces. So those wild microbes hit populations that are tailor-made for turning a virus into an epidemic. These wild reservoirs are somewhat dangerous on their own, as Rabies and Lyme Disease will tell. You can walk in the forest without fear of breathing them in, as long as you avoid getting bit by anything. But to destroy their habitats, to reduce the genetic diversity of those places, so that there's less buffer between the viruses and us, just for the sake of making more money faster, well...that’s when these critters get into our lungs.
It’s the interface of an increase in Intensive Industrialism with Wilderness that does the trick.
As I live in the Northeast United States, in the foothills of the northern Appalachian Mountains, I and all my friends deal with this every damn summer when we have to worry about Deer Ticks. Those didn’t become a problem until people shoved their big suburban houses up against the woods just as they were coming back, and in the new forest with new deer populations there were no wolves, so there’s deer everywhere and there are deer ticks everywhere. Lyme Disease gets into a person and it never goes away on its own, but gums up your joints and wears you down over the years if left untreated. Call it the AIDS of New England. Human immune systems can’t handle AIDS nor Lyme Disease, and I don’t think that’s a coincidence. Lyme Disease is yet another virus direct from the woods.
Supposedly Poison Ivy comes from the same issue, for as people shove their houses up against the woods they create more of the edge-forest area where Poison Ivy thrives.
It’s that edge that does it. The edge between Industry and Wilderness, that’s where the world boils and roils and spits out hot stuff like someone put too much oil in the fry pan. Edge environments always have the most activity in the first place even if they’re All Natural. Continental shelves, forest edges, river banks, lake shores, swamps, salt marshes, whatever the biologists will call an Ecotone. That’s where the living world boils and roils, as the creatures of one biome meet another. If Intense Human Industry barges into the place and smashes it up without an ounce of caution -- well, the results are like someone smashing a fist into a frypan of simmering oil.
“That’s what you get for messing with the Wilderness!” cry the Eco-facists and all the folks who think humans are a disease upon the earth. “Mother Gaia takes her revenge! So there!”
And there I come to the one part of Chuangchn’s article that I really disagree with. The author thinks that we’re Losing The Wilderness. But I don’t think we’ve ever really had any. Not Wilderness with a capital W, at any rate. Humans have been significant shapers of the living landscape for tens of thousands of years. Our species has been fairly well integrated with the world and highly influential, a lot like beavers making ponds all across northeast North America. In the same time period as beavers, humans were setting enough small fires in the Jemez Mountains of New Mexico to be a bigger factor for forest fires than the climate was. Likewise the Amazon Rainforest that we think of being a Pristine Landscape Untouched By The Hand Of Man was actually shaped by centuries of human activity. Humans made all the terra preta that you can find throughout the rainforest. Hard to believe that they could make fertile soil without livestock! I will leave you to guess of where that manure came from.
Indeed, to speak of "wilderness" implies that we are separate from the world, and it is this mindset that leads us to set aside certain areas as Natural Pristine Beauty and then pave over everything around them. Both lands are thus diminished by the desire for Purity. If we were willing to incorporate the rest of living world, letting it live and grow with our influence but not our destruction, as once we used to, such that the genetic variety of the world was not reduced -- perhaps then we would not have these epidemics after all. It is not that we need to Preserve The Wilderness so much as we need to become part of the world again.
As it is, capitalism prefers that this does not happen, because it means a slower increase in personal wealth for the select people holding all the money. Capitalism does not live and let live. It cannot. The system wants more, more, more, faster and faster. To clarify: certain people holding all the money want more, more, more, faster and faster. There is no place they would let alone if they could make lots of money off it soon, nor any place they would let make money slowly when it could make money quickly. So you see people choosing to strip-mine a place instead of sell tickets for river rafting.
This was never necessary, except to serve the greed for personal wealth and power. And yet, was it even necessary for that? The Empire of the Incans functioned without money or markets, as did every civilization for thousands of years, until someone invented coinage around the 600s BCE. Plenty of wealth and power to be had without coins, surely! The real value of money is liquidity and speed, and some people want their fortune Now. Maybe it’s the Greed For Speed that makes the difference between the power-grabbing of an aristocrat and the power-grabbing of a merchant.
And so as we alter the landscape too fast it cannot adapt in time, and suffers greatly.
We see the results in one epidemic after another. It’s not Gaia’s Revenge; it’s just the fallout of us setting things up to make a virus’s happy accident our unhappy accident, time and again.
#Coronavirus#covid-19#epidemic#epidemiology#capitalism#if I was a real researcher this thing would have taken me a week and it would be closer to the mark#as it is it took a day#but I have done my best from the sources I could find#I have tried to make sure that my educated guesses are reasonable and well-supported#such that this essay will contribute to your understanding of the issue#instead of leading you astray#make of it what you will
14 notes
·
View notes
Last Seen Blogs

mythenmetzsche-abschweifung
Für Leseratten und Bücherwürmer

juicygf
you should fuck me

dambong
제목 없음
l0st-in-th0ught
Imlit

thin-mintx
thin. / side blog.