#healthcare data governance
Text
25 Ways Healthcare Data is Revolutionizing the Healthcare Industry
An exhaustive list for healthcare and healthcareIT colleagues and friends. Happy Reading!
Healthcare data refers to the information collected from various sources in the healthcare system, including medical records, laboratory results, and insurance claims. This data can be used in numerous ways to advance healthcare and improve patient outcomes. From improving patient safety to developing personalized treatment plans, healthcare data is a valuable tool that can help healthcare…

View On WordPress
#big data in healthcare#electronic health records#health data privacy#health data security#health information technology#healthcare AI#Healthcare Analytics#healthcare blockchain#healthcare data#healthcare data ethics#healthcare data governance#healthcare data integration#healthcare data mining#healthcare data storage#healthcare data visualization#healthcare data warehousing#Healthcare Interoperability#healthcare machine learning#medical informatics#patient outcomes#personalized medicine#Population Health Management#predictive analytics in healthcare#telemedicine#wearables in healthcare
1 note
·
View note
Text
Y'all ever look at this?
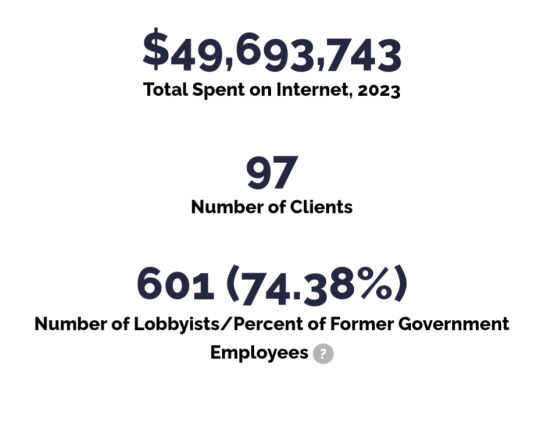
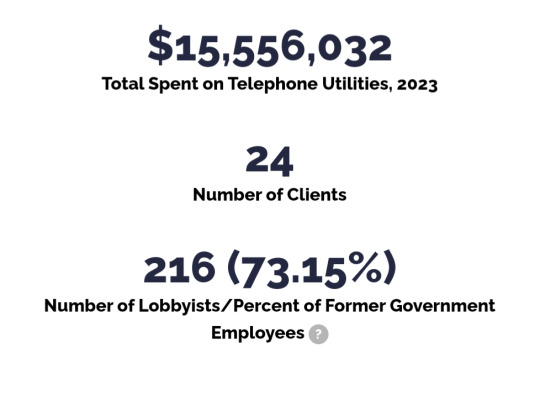
I was doing some research about healthcare and stumbled into this lobbying tracker and I am...pissed off???
Free rage machine over at opensecrets


#politics#Lobbying#us politics#us government#congress#senate#oil#gas#clean energy#climate change#data protection#capitalism#healthcare#health insurance#oil company#gas company
64 notes
·
View notes
Note
nate being the only doctor makes me wonder what he's had to do for the others before

Nate does a lot for the crew. (Also woo look at his human disguise!)
When he's not actively treating or checking on them, he's constantly working to compare studies and test data to understand how to treat his friends, seeing as they have widely different genetic makeups and could react in ways that are *catastrophically* unexpected.
He can't use human rules when working on them, which greatly complicates things when he's educated in treating humans. Sera and Vince naturally have nucleated blood cells for greater oxygen input since they're always in rigorous activity, but this is a sign of leukemia or other major deficiency in humans. How do drugs interact with their bodies? what reaction will their immune systems have? do they have an intolerance to certain chemical developments?
This is partly why Vincent underwent so much testing and experimentation- to catalogue and document an atlas for the reproduction and understanding of this hybrid Variant species, and how every facet of its anatomy works in that respect. Like a rough draft you don't care about messing up, and use only to learn from.
Sorry Vince.
It's a wonder how Nathaniel was able to successfully recompile enough information to save his friends at all. It's a lot of stress on one guy with no nurses! That goes without saying for Amon (who is a beastshifter) Sonia... (Who is a living chemical synthesis lab) The various other people who end up joining... (Who shall remain incognito)
...Yikes.
He has likely seen all of them naked at least once, due to emergencies. He's extremely professional, so it's like it never happened... But it's still never fun to have to use that kind of ER protocol on your injured friends and associates.
Everyone except for Vincent, since V never lets Nathaniel treat him for anything, even when he needs it.
Instead, everyone caught a harrowing and unwanted glimpse of Vincent when he landed back home after streaking in the rain. He now flies with his pants duct-taped on. And goggles. For the glare and the overwhelming surplus of bugs he slams into at twice the speed of a f1 car.
#devarambles#nathanieltag#one of the awkward facts about their situation as rogues is they have zero medical support besides Nathaniel.#and he has to constantly inform himself on their respective anatomy because theres so much undocumented info on variant medicine#Despite all of the extensive testing and processing reports done on variants#which is done in reference to improving human medicine. not necessarily variant healthcare. useful data regarding treating people is...#few and far between. Private research and study is usually done for variations that prove useful to government positions.#So variant healthcare is usually employed towards certain government divisions or certain levels of corporate practices. otherwise they#simply don't bother. “it costs less money to replace you than it does to keep you alive.”#Lol nate chose a shorter and thinner appearance when masking as a human. It makes him look a lot more approachable and his knees don't hurt#Sera... feels somewhat unnerved by his human form. It feels like she's cheating on him somehow. She has him change back when he's home.#He's perfectly happy with that since he doesn't like being disguised much either. He's pleasantly surprised to see that she prefers him#to be true blue. Most previous partners would request him to change into other forms. Sometimes he was even asked to turn into celebrities.#Not fun. Really not fun. He'd eventually associate his true self with something undesirable enough to be rejected over.
14 notes
·
View notes
Photo

U.S. Marshalls Spied on Abortion Protesters Using DATAMINR >
Twitter’s “official partner” monitored the precise time and location of post-Roe demonstrations, internal emails show.
DATAMINR, AN “OFFICIAL PARTNER” of Twitter, alerted a federal law enforcement agency to pro-abortion protests and rallies in the wake of the reversal of Roe v. Wade, according to documents obtained by The Intercept through a Freedom of Information Act request.
Internal emails show that the U.S. Marshals Service received regular alerts from Dataminr, a company that persistently monitors social media for corporate and government clients, about the precise time and location of both ongoing and planned abortion rights demonstrations. The emails show that Dataminr flagged the social media posts of protest organizers, participants, and bystanders, and leveraged Dataminr’s privileged access to the so-called firehose of unrestricted Twitter data to monitor constitutionally protected speech.
[Sam Biddle, The Intercept, May 15 2023]
#twitter#elon musk#musk#social media#abortion#roe v wade#roe vs wade#abortion rights#pro-abortion#abortion access#healthcare#body autonomy#supreme court#politics#us politics#us government#privacy policy#privacy#datamining#data for sale#government privatization#policing#surveillance#free speech#right of assembly#corporate spying#protest#demonstration#activism#activists
19 notes
·
View notes
Text
2 notes
·
View notes
Text
Removing Bias From Healthcare AI Tools - Technology Org
New Post has been published on https://thedigitalinsider.com/removing-bias-from-healthcare-ai-tools-technology-org/
Removing Bias From Healthcare AI Tools - Technology Org
A stethoscope. Image credit: Darko Stojanovic via Pixnio, CC0 Public Domain
Researchers from Oxford University’s Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences (NDORMS), University College London and the Centre for Ethnic Health Research, supported by Health Data Research UK, have for the first time studied the full detail of ethnicity data in the NHS. They outline the importance of using representative data in healthcare provision and have compiled this information into a research-ready database.
The new study, published in Nature Scientific Data, is the first part of a three-phase project to reduce bias in AI health prediction models trained on real-world patient data. The project addresses ethnicity disparities highlighted during the pandemic and is part of the UK Government’s COVID-19 Data and Connectivity National Core Study led by Health Data Research UK.
[embedded content]
The researchers used de-identified data on ethnicity and other characteristics from general practice and hospital health records, accessed safely within NHS England’s Secure Data Environment (SDE) service, via the British Heart Foundation Data Science Centre’s CVD-COVID-UK/COVID-IMPACT Consortium. This is the first time that patient ethnicity data has been studied at this depth and breadth for the whole population of England. The researchers were able to combine records to analyse patient self-identified ethnicity recorded through over 489 potential codes.
Researchers analysed how more than 61 million people in England identified their ethnicity in over 250 different groups. They also looked at the characteristics of those with no record of their ethnicity, and how conflicts in patient ethnicity data can arise. The data, now available for other researchers to use, shows that 1/10 patients lack ethnicity records, and around 12% of patients had conflicting ethnicity codes in their patient records.
Sara Khalid, Associate Professor of Health Informatics and Biomedical Data Science at NDORMS, explained: ‘Health inequity was highlighted during the COVID19 pandemic, where individuals from ethnically diverse backgrounds were disproportionately affected, but the issue is long-standing and multi-faceted.
‘Because AI-based healthcare technology depends on the data that is fed into it, a lack of representative data can lead to biased models that ultimately produce incorrect health assessments. Better data from real-world settings, such as the data we have collected, can lead to better technology and ultimately better health for all.’
Professor Cathie Sudlow, Chief Scientist at Health Data Research UK and Director of its BHF Data Science Centre said: ‘We are delighted to be supporting hundreds of researchers to harness the power of the UK’s rich health data. This study on ethnicity recording highlights how different sources of health data from the whole English population can be accessed and analysed in a safe and secure way, providing insights that are relevant to everyone. The findings will empower health professionals, patients, carers and policy makers to make better decisions that will benefit people of all ages, ethnic groups, and social backgrounds across the country.’
The study assessed the available detail of ethnicity data in NHS England, including across different types of ethnicity codes. For example, NHS hospitals record patient data via 19 ethnicity codes, while GPs use the globally recognised SNOMED-CT Codes, of which there are 489. However, health researchers lose the finer detail from these recording systems as they typically collapse these groups into just 5 or 6, potentially leading to less accurate research.
The researchers plan to demonstrate the value of these findings in the subsequent phases of the project, which will first focus on using these detailed results on ethnicity data to better describe how different the COVID-19 pandemic impacted ethnicities, and then feed into more equitable artificial intelligence and machine learning tools suitable for use by diverse patient groups.
Source: University of Oxford
You can offer your link to a page which is relevant to the topic of this post.
#250#A.I. & Neural Networks news#ai#ai tools#artificial#Artificial Intelligence#artificial intelligence (AI)#Bias#college#connectivity#covid#data#data science#Database#English#Environment#Explained#Foundation#Full#Government#GPS#Health#Health & medicine news#Health care#healthcare#healthcare technology#heart#hospitals#how#impact
0 notes
Text
The Impact of AI on Everyday Life: A New Normal
The impact of AI on everyday life has become a focal point for discussions among tech enthusiasts, policymakers, and the general public alike. This transformative force is reshaping the way we live, work, and interact with the world around us, making its influence felt across various domains of our daily existence.
Revolutionizing Workplaces
One of the most significant arenas where the impact…

View On WordPress
#adaptive learning#AI accessibility#AI adaptation#AI advancements#AI algorithms#AI applications#AI automation#AI benefits#AI capability#AI challenges#AI collaboration#AI convenience#AI data analysis#AI debate#AI decision-making#AI design#AI diagnostics#AI discussion#AI education#AI efficiency#AI engineering#AI enhancement#AI environment#AI ethics#AI experience#AI future#AI governance#AI healthcare#AI impact#AI implications
1 note
·
View note
Photo

myScheme One-stop #search & #Discovery #platform for #Governments #Schemes (myscheme.gov.in) #AatmanirbharBharat #DigitalIndia #DigitalTransformation #SocialMedia #influencer #socialservices #help #govt #Data #development #innovation #health #healthcare #AI #food #startup https://www.instagram.com/p/Cir6gkhp4r468LGurc1ICIwHlJmisRG9ZsV1d00/?igshid=NGJjMDIxMWI=
#search#discovery#platform#governments#schemes#aatmanirbharbharat#digitalindia#digitaltransformation#socialmedia#influencer#socialservices#help#govt#data#development#innovation#health#healthcare#ai#food#startup
0 notes
Text
In the last two decades, there has been a growing body of literature on trans health in India. However, most research is limited to HIV/AIDS and primarily focuses on trans women. Studies on trans men or transmasculine identities and their healthcare needs and experiences in India have received little scholarly attention.
Even globally, the literature on trans men’s health is relatively scant, with existing studies conducted mainly in Western countries. There exists a dearth of government data and statistics on trans men in India. The only attempt to enumerate the transgender population was made by the national census, which categorised them as ‘other.’
The census estimated 4,87,803 transgender people in India. However, several transgender activists have argued that this number is a considerable miscalculation and an inaccurate representation of the entire transgender community in India. Moreover, the lack of official data on trans men also risks under-allocating funds for much-needed welfare programmes.
Moreover, trans men experience direct and indirect discrimination in healthcare settings. Such experiences include being asked invasive or inappropriate questions about their bodies, invalidating their gender identity via misgendering, deadnaming, and being denied healthcare or receiving low-quality care. Sometimes, it also includes physical mishandling and verbal harassment by the hospital staff and co-patients or not being allowed to enter certain hospital wards or spaces.
[...] For many trans men, the family becomes the first space for mental and physical violence and outright rejection of their identity, with instances of forced heterosexual marriages or corrective rape.
Vinay (name changed), a 30-year-old trans man from Punjab, says, “Family says ‘you’re ruining our reputation, get married, have one-two kids and then everything will be fine.’ They even use rape as a measure saying ‘you don’t know who you are, and when it happens, then you’ll know [your true sexual orientation].’”
Many have to deal with uninformed healthcare providers unwilling to treat them because of their gender identity. Lack of knowledge amongst medical professionals and poor social understanding of trans men means that trans men often have to self-advocate and explain their health-related issues and gender identity to medical practitioners who constantly challenge or dismiss their identity.
This self-advocacy and mental effort to explain or justify one’s gender identity and expression often leads to emotional exhaustion. Soham (name changed), a 24-year- old trans man from New Delhi, recounts his experience of going to a hospital,
“The doctor came and shouted my dead name. There were a lot of people in the emergency room and I remember feeling numb for a second…He shouted, ‘Is this you? Yehi naam hai aapka?’ (‘Is this you? Is this your name?’)…Then he literally pointed at my chest and said your chest is so flat, do you have your periods? I was numb and I didn’t say anything. I didn’t get my medicine, I didn’t tell him my problem, I just went home and I locked myself in my room for a week.”
— I Didn’t Get My Medicine, And I Locked Myself In My Room For A Week (Trans Men Are Invisible in India's Healthcare) by Arushi Raj and Fatima Juned
#m.#rape tw#examples of transandrophobia#transandrophobia#transmisandry#anti transmasculinity#transunity
423 notes
·
View notes
Text
Consider the following:
The treatment of the unhoused/poor, including making being unhoused a crime.
The rising inability to afford housing, groceries, and utilities, even with full-time jobs that pay more than the minimum wage.
The genocide occuring in Palestine and the use of US funded weapons to commit it.
Rising rates of Neo-Nazis, antisemitism, and islamophobia.
The beating of a trans, Native American child at a public school, which resulted in death, being praised by an active senator who called trans people filth, when addressing the issue (Rest in Peace, Nex).
Trans people increasingly having their rights, especially to healthcare, taken.
Women increasingly having their rights to healthcare taken.
The migrants who are fleeing their home countries, leading them to the US-Mexico border, are being met with police violence, razor wire, and detention centers that have been reported to separate and "lose" children, as well as treat those within its walls with cruel amounts of negligence.
The subways of New York becoming flooded with cops and National Guard, making it a police state checkpoint for anyone that enters.
Police being able to justify the murder of a Black, autistic teenager, in front of his family.
However, the US government has deemed TikTok to be the largest threat to the nation and is the issue that they can all, collectively, agree on. Certainly can't be because it's been the main place for younger people to find current news that isn't gripped by corporate media. Can't be because it's a place for people to find information on the continued boycotts, divestments, and protests that are currently occurring and costing corporations millions of dollars, effecting how much those corporations can lobby their representatives. Can't be because it is the place people often go to when mainstream media refuses to cover the big stories that would otherwise be pushed under the rug. Can't be because our representatives, the people that we put in charge of making our voices heard, are sick of hearing what we have to say about their actions within and outside of their offices. Must just be because TikTok has a parent company in China (while the US servers and data are run through US based company, Oracle) and that it's a dangerous threat.
130 notes
·
View notes
Text
“There are thousands of FGM survivors like Araweelo across the country. In 2011, the Home Office data estimated there were 137,000 people living with FGM in England and Wales, but with more than 5,800 survivors newly identified by the NHS between April 2022 and March 2023, the numbers could be much higher.
In 2014, the government and NHS England launched a £1.4m FGM prevention programme to educate healthcare professionals, and NHS guidance states that such professionals should seek to support women by “offering referral to community groups for support, clinical intervention or other services as appropriate, for example through an NHS FGM clinic”. Yet this year, nearly a decade later, an independent report carried out by the Vavengers – a London-based charity fighting FGM - showed that two thirds of the 670 NHS staff surveyed reported receiving either no or minimal training on how to deal with survivors.
…
Charities, pressure groups and FGM experts say that the UK is lagging far behind in offering survivors surgical reconstruction. There are now 26 clinics across 11 different European countries offering reconstructive surgery to FGM victims.
Many groups believe that British doctors already possess the required skills to perform such surgeries on survivors but that their injuries are simply not being considered a priority.”
145 notes
·
View notes
Text
02/27/2024: THE BILL HAS NOT PASSED THE SENATE YET. BUT IT IS COMING TO VOTE WITHIN THE NEXT FEW DAYS.
CONTACT YOUR SENATORS TO DEMAND THEY VOTE NO ON THIS BILL.
CONTACT YOUR REPRESENTATIVE ALSO AS IT WILL GO TO THE HOUSE NEXT
CALL SCRIPT:
My name is __________. I am a constituent, and my zip code is _______. .
To your Senators :
I’m urging you to vote no on Senate Bill 1409. This is yet another attempt to shove censorship and surveillance down our throats “for the children” and I’m urging you not to fall for this LIE. Thank you.
To your Representative:
I’m asking you to please vote no on Senate Bill 1409 if it passes the Senate. This is yet another attempt to shove censorship and surveillance down our throats “for the children” and I’m asking you not to fall for this lie. Thank you.
Background
We all benefit when we can all access the public square and speak our minds freely, even—maybe especially—about sensitive topics and traumatic experiences. We need to be able to discuss these things, not just as cold abstractions but as personal experiences, to do the work of reducing the amount of harm in the world.
From time to time, lawmakers—well-intentioned or otherwise—try to take away our access to the public square, our right to speak freely in it, or both, often in the name of “protecting our children” from some of those harms. But we cannot repair or prevent those harms if we cannot discuss them.
The latest attempt is S.1409, deceptively named the “Kids Online Safety Act”. This one leverages anger at Big Tech over social media moderation decisions as an excuse to force harmful blanket policies on all Americans.
KOSA is one of the Electronic Frontier Foundation’s “Bad Internet Bills” for two main reasons:
KOSA would require you to show papers to use the internet
KOSA would require messaging services (think iMessage, Signal, or WhatsApp) and social media websites to try to shield the eyes of minors against certain topics. It’s likely that these services would comply with these requirements by forcing users to provide proof of age.
Realistically, this means forcing people to prove their identity to every service they sign up for.
The age requirements affect everyone. If this bill passes, you will have to submit to some sort of identity verification to prove your identity and thus your age every time you sign up on a new service. You will always have to do this, over and over again, for the rest of your life.
How that verification works is not specified. It might be one of the sketchy automatic-verification services like the one the IRS almost used, or they might simply ask you to upload some form of identity documentation. Tough luck if you’re undocumented, a victim of identity theft, transgender, or actually underage. Even if you’re none of those things, you will still have lost your anonymity—your identity is only one successful subpoena or data breach away from being in the wrong hands.
There are very real hazards that come from pairing identity verification with private or anonymous communications. At a time when healthcare decisions like abortion or gender-affirming care are being criminalized in some states, and workers are forming unions and facing unfair labor practices, and activists like us are holding government accountable, we must recognize the importance of protecting the right to speak privately or anonymously whenever we want or need to.
You have the right to speak anonymously, and the right to choose what you disclose and what you keep private. We must protect these rights.
KOSA would require messaging services and social media companies to censor you
Currently, you are legally responsible for what you say online—not the companies who own the services you say it on.
This is thanks to a law from the 1990s known as “Section 230” (specifically, Section 230 of the Communications Decency Act of 1996). Law professor and author Jeff Kosseff called Section 230 “The Twenty-Six Words That Created the Internet” in his book by that title, recounting the history of conflicts between the First Amendment (and its broad protections of speech) and the harms that can be done with speech, and the development of the Act in that context. Kosseff argues that the internet as we know it today, as a public square where anyone can participate, was created because Section 230’s protections enabled freedom to flourish.
KOSA threatens to undermine those protections by obligating companies to intervene when people talk about certain topics on their platforms. This would create, in effect, a censorship regime—if you’ve ever seen the lengths TikTok users go to in order to try to exercise their free-speech rights without saying things that will get them suspended, you’ve seen what this looks like in action. KOSA would make it legally mandatory on all messaging services and all social media.
No good would come out of forcing these companies to insert themselves into our conversations.
The minute a system exists that tries to decide what people can and can’t say—on the internet or otherwise—that system begins chilling speech. If this bill passes, you will have to think about what you are and are not willing to discuss with others, even in private via instant-messengers, much less in the public square via social media.
You will choose to refrain from talking about some things—your speech will have been chilled. When you do choose to talk about some things, you will have to contort your speech to evade censorship.
And there will always be false positives and false negatives. People who didn’t fall afoul of the law will get censored anyway because the system made a mistake. People who did say something on the proscribed list may get lucky—until they don’t.
This affects all communications, public and private
It’s bad enough to censor people’s public discussions on social media and limit who can contribute to such discussions. It’s even worse to censor people’s private communications via iMessage, WhatsApp, and other messaging services.
You have the right to have private conversations without anybody sticking their nose in, no matter who you are or what you’re talking about.
Beware of simple “solutions”
People are complicated and that makes the rights and responsibilities of speech complicated. There are no simple answers.
Speech can cause harm. The classical example of speech not protected by the First Amendment is shouting “fire!” in a crowded theater—that is, causing a panic, a stampede, injuries, possibly deaths. The fact that the cause of the panic was an act of speech does not shield the speaker from responsibility for the harms that act caused. For a more recent example, consider Trump’s lies about the 2020 election before, during, and after it, by which he fomented an insurrection on January 6, 2021, for which he has been criminally indicted. The First Amendment protects his right to lie, but does not give him a right to start an insurrection.
Speech can also do great good. People have the right to cry out for help, or to speak about injustice. We can work together to solve problems—if we can talk about those problems in the first place.
KOSA is promoted as a simple solution to complex harms. As such, we can recognize that it is a false solution that would do more harm than good. We must protect our right to participate fully and frankly, in both public discourse and private conversation, against this sort of attack.
The EFF is right: This is a bad internet bill
This bill would, in effect, force instant-messaging services and social-media services to begin dossiers on their users and impose a censorship regime. This will not solve any problems; it will only take away our right to use the internet to speak freely.
In spite of these dangers, the bill has the bipartisan support of 43 senators. It wouldn’t take many more for it to have a real chance at passing the Senate. The time to stop it is now.
References
S.1409, Kids Online Safety Act (118th Congress)
“The Kids Online Safety Act is Still A Huge Danger to Our Rights Online”, Electronic Frontier Foundation, 5/2/2023
98 notes
·
View notes
Text

🎇 NYE COVID-19 RED ALERT - AVOID CROWDS & MASK UP 🎆
You wouldn't know it from our governments, but Turtle Island, aka the US & Canada, are in the worst spike of illness and deaths since 2020's deadly Omicron surge.
That means it's more dangerous to go to a New Years party this weekend than it's been for approximately 96.4% OF THE ENTIRE PANDEMIC. It's bad out there tonight, and your odds of staying healthy after an unmasked gathering are NOT good.

The more people at your party, the higher the chance you'll catch COVID-19. You may think it's worth the risk, since many people appear to have "mild" infections, but that's not the whole story.
The first 2 weeks of COVID-19, aka the "acute phase", are just the beginning. Even if you don't need emergency hospitalization, or even if you never have any symptoms at all, the virus SARS-CoV-2 responsible for COVID-19 silently turns your immune system against you and shreds the lining of your circulatory and nervous systems. This can permanently elevate your risk of heart attacks, strokes, digestive problems, and even life-changing disabling disorders like ME/CFS.
And even if you escape relatively unscathed, you could pass the virus onto loved ones who WILL get hit hard, and survive with new life-long disabilities, or not survive at all.

COVID-19 never left, and our healthcare systems are NOT looking out for us. We have to take care of each other. Please, please rethink going out to that party tonight. If you can't avoid socializing, please protect yourself as much as you can:
Wear WELL-FITTING respiratory masks like N95s & KN94s
Use nasal sprays before & after, & CPC mouthwash after
Gather outdoors whenever possible
Get good air circulation indoors with air filters like CR Boxes, or open windows for outside air (bundle up if it's cold)
More resources on these tips, and how to reduce the damage if you do get sick, can be found on this COVID Safety Roundup list. All graphics courtesy of the Pandemic Mitigation Collection and Dr. Michael Hoebert, from their website. Hoebert further breaks down the data on his twitter too.
You can also ask me any particular questions and I'll do my best to help! We all deserve to survive this, and we'll do it together.
#covid 19#long covid#still masking#mask up#actually disabled#covid isn't over#covid19#new year#happy new year#new years eve
89 notes
·
View notes
Text
The government is facing calls for a public inquiry into the scandal of sexual abuse in mental health hospitals, following an investigation by The Independent.
Rape Crisis England and Wales has warned that the “alarming” scale of abuse within the UK’s psychiatric system requires “major intervention” from ministers.
It comes after an expose by this publication and Sky News revealed that almost 20,000 reports of sexual incidents – involving both patients and staff – had been made in more than half of NHS mental health trusts in the past five years.
As well as a public inquiry, which would give survivors the chance to give evidence, Rape Crisis England and Wales wants the government to appoint a named minister with responsibility for addressing the problem.
PraisingThe Independent and Sky News for shedding light on the scandal, chief executive Ciara Bergman said: “That anyone in the already vulnerable position of needing or being detained for in-patient care because of their mental health needs should experience sexual violence and abuse whilst in the care of the state, is deeply concerning.
“We are concerned that without major intervention and leadership at the highest levels, this could lead to more incidents of sexual violence and abuse happening, and this behaviour being accepted as inevitable, when it is not, and is indeed absolutely preventable.”
The charity added that it had been raising our concerns about widespread safeguarding issues uncovered by The Independent for many years. “It is disturbing that so little has seemingly changed,” it added.
As part of the investigation, The Independent published a series of harrowing stories revealing allegations of rape and sexual assault on patients and staff in mental health hospitals.
In an exclusive podcast, Patient 11, one woman, Alexis Quinn, revealed the harrowing story of having to escape a mental health ward after claiming she was sexually assaulted twice.
We also revealed shocking failures by the NHS and police to follow up on allegations, with figures showing just 26 charges came from nearly 1,400 reports to the police.
After the revelations, the health minister said allegations of sexual abuse in mental health settings would become part of a major review.
Rape Crisis England and Wales also called for hospitals to ensure they have women-only wards after figures showed more than 500 claims of assaults and rape on mixed sex wards have been made since 2018.
Despite the NHS launching a “sexual safety” programme in 2019, The Independent and Sky News revealed hospitals are not adhering to key requirements of the guidance.
The news comes after NHS England published new survey data last week showing 80,000 – 8 per cent – of NHS staff reported experiencing unwanted sexual behaviour from colleagues and patients last year.
An NHS spokesperson said: “Any form of abuse or sexual violence is completely unacceptable. Everyone deserves to feel safe when they come to the NHS for their healthcare needs, often at a time when they are vulnerable.”
In September NHS England published its NHS Sexual Safety Charter which provides guidance for healthcare systems in addressing sexual misconduct risks and signing up to a “zero tolerence” approach. So far 260 organisations have signed up.
“The NHS has made clear that every provider of our services has a legal and moral duty to safeguard patients, to report all incidents of sexual violence, and to take appropriate action with the criminal justice system and safeguarding bodies where harm has occurred,” it added.
A Department of Health and Social Care spokesperson said: “Sexual violence or misconduct of any kind is unacceptable and NHS organisations have a responsibility to protect both staff and patients. The Department has zero tolerance and is clear that the NHS should work to stop sexual assaults happening in NHS services and premises.
“We have been clear patients should not have to share sleeping accommodation with others of the opposite sex and should have access to segregated bathroom and toilet facilities, and we expect NHS trusts to comply with these measures.”
It did not respond to calls for a public inquiry but said it was working with mental health services to ensure every patient has safe care and that safety body the Health Services Safety Investigations Body has launched a national investigation into mental health inpatient settings.”
38 notes
·
View notes
Text
Ending the COVID emergency will further harm Black maternal mortality | The Hill
this year’s calls to celebrate Black Maternal Health Week ring hollow because the Biden administration recently ended the COVID-19 national emergency ahead of schedule and will allow the public health emergency to expire on May 11. This means that most Americans, and certainly those from historically excluded groups, will no longer have access to free at-home COVID tests or vaccines and testing services without cost sharing. Hospitals and clinics across the U.S. have ended or are ending mask mandates, which places patients and newborns at higher risk of COVID exposure. These actions have been met with shockingly little public pushback from advocates for Black reproductive health, despite the fact that COVID has disproportionately orphaned Black children.
It is now clear that COVID likely drove much of the sizable increases in deaths resulting from pregnancy, including an 18 percent increase from 2019 to 2020 and a nearly 40 percent increase from 2020 to 2021. For Blacks, the data are bleakest: the overall mortality rate is the highest seen in recent history — 69.9 per 100,000 live births. Contracting COVID during pregnancy increases the risk of health complications, including maternal morbidity and within-hospital mortality. COVID is why Atlanta resident Marrisha Kindred Jenkins died before getting to hold her infant son for the first time. This much we know.
But there is much that is unknown. We do not yet have a complete picture of the long-term effects of COVID on reproductive health. Yet, if the past remains prologue, Black people will likely shoulder a disproportionate share of long COVID’s effects on reproduction. While prenatal vaccination can reduce COVID-related risks during pregnancy and pass on protection to babies, vaccination rates for the pregnant remain low, particularly among Blacks.
267 notes
·
View notes
Note
I'm curious if you've come across any examples of what you would consider effective communication or collective organizing around Covid? I know of a few groups who I think are doing good work to get people access to masks and rapid tests, making connections to broader issues such as lack of sick leave, barriers to healthcare etc, but they're also relying on things like questionable wastewater data extrapolation to make their points. I don't really know what to do about the latter issue, since we've just had access to all data taken away from us by the government. (I know it's not an effective tool for collective action, but tbh I also struggle with the idea that all alarmism is bad, because I am high risk and I am scared!)
well 1st of all to be clear, i think wastewater data are valuable and i do look at them. what i don't do is make wildly overconfident guesses from those data about exactly how many people are infected, how many sick people are standing in any given room, how many people will eventually qualify for a long covid dx, etc. i think wastewater data are a rough proxy but still an important one, and generally more useful at the local level (where they can be cross-referenced with factors like vaccine uptake, circulating variants, and municipal public health policy) than at national or regional levels (where the necessary amount of aggregation makes it difficult to tease out much useful information about any one town or city).
2nd, i don't know what country you live in but i do look in on CDC's covid dashboard, which includes data on hospitalisations, emergency department visits, deaths, vaccine uptake, test positivity rates, &c. if this is applicable to you i strongly encourage always reading the footnotes as these statistics vary in accuracy (in particular, test positivity rate is very unreliable at this point). i consider a lot of these numbers useful primarily as indicators of comparative risk: eg, i assume hospitalisation numbers have been inaccurate lowballs for the entirety of the pandemic; however, it is still useful imo to see whether that number is trending in a particular direction, and how it compares over time. again, local results are sometimes more helpful as well. i also glance in on the census bureau's household pulse survey results, which come out numerous times throughout the year and include questions about duration of covid symptoms, ability to function, and vaccine uptake. these numbers skew in the opposite direction to many of CDC's, because the phrasing of the covid questions is intended to be broad, and does not attempt to distinguish between the sort of long covid that entails a 6 or 12 month recovery period, vs the sort of long covid that turns out to be me/cfs or other chronic long-term post-viral complications. again, i still think these numbers are useful for viewing trends over time; no data will ever be completely 100% without flaw, and i'm not holding out for that. what does frustrate me, though, is people (with any and all ideological axes to grind!) interpreting any of these numbers as though they are in fact perfect flawless representations of reality, with no further caveats or critical analysis needed. that's what i'm pushing back on, whether it comes from the "pulse survey says long covid prevalence is decreasing, so fuck it!" crowd or the "biobot says last week was a micro-surge so we're all going to die!" crowd.
as far as local orgs or groups doing actual action, like distributing masks or vaccine clinics, i don't put so much stock in what they say on instagram or whatever because frankly i think it matters very little. the masks and vaccines and air filters and so forth are useful in themselves; that work is valuable. if someone's positioning themselves primarily as a communicator then yes, i'm going to scrutinise their communication methods more. if it's an action org i'm honestly less concerned, unless there is egregiously unreliable information being propagated or they're communicating in the sort of stigmatising manner that many peak Posters have adopted (people who got sick are stupid / immoral / deserve it, etc).
i'd also just like to make it clear that like... i live with someone who is at high risk, i accordingly treat my own covid precautions as though i am also at high risk, and i wouldn't want covid regardless... like, please understand that when i talk about this i'm not coming at it from a perspective of someone who's unaware of the need for caution! my concern is, again, that caution and risk discussion are not synonymous with "making frightened guesses and asserting them with 100% confidence" or "selectively attributing truth to data because they agree with me, regardless of the actual methodology and any problems therein". i understand that when people are behaving recklessly and being encouraged to do so by state and medical authorities, it is tempting to look at that situation and think that communicating the seriousness of the virus is worth risking a little bit of inaccuracy if it protects people. however, i do not think that strategy actually pays off in the long or short term as far as changing people's behaviour (if it did, wouldn't it have by now?) and i think it is playing with fire to encourage this manner of interpreting and disseminating scientific information as though it is a kind of ideological buffet requiring no further verification or investigation beyond a cherry-picked deference to the stated objectivity and ideals of The Scientific Method.
26 notes
·
View notes
Last Seen Blogs

almostmypeanut
Life Hard, Tiddy Soft

spike343
Lion King obsessed

sindriastwinwarriorsmoved
Attila and Emese

jas-is-jessica
please keep all hands and feet inside the blog at all times

heydicalix-blog
It's me