#genderwang
Text
I am Sage's mother, better known as Nana. I adopted Sage after my son died when she was still a baby. She's been through six foster homes by then, but we loved her and she blossomed into a joyful, lively girl who made music and art.
Puberty began and COVID hit, and she was treated for depression and anxiety, at times very severe. Her teachers shared any concerns with me so her treatment could be adapted.
The transparency ended in August of 2021 when Sage started high school. She started a public high school and she told me that all the girls there were bi, trans, lesbian, emo and she wanted to wear boy's clothes and be emo. Because I saw it as just a phase, it was fine with me.
But at school, she told them something different: she was now a boy named Draco with male pronouns. Sage asked the school not to tell me, and they did not tell me even though I informed them of her mental health history and medication. If I had known, this would be a much different story.
She was terribly bullied. No one told me. But boys followed her, touched her, threatened violence and rape. Something happened in the boy's bathroom but for two days, the school told me nothing. They kept meeting with Sage alone and she became so distraught they called me to pick her up.
That evening, I found a hallpass labeled 'Draco' and Sage told me she was identifying as a boy, and that her counselor said she could use the boy's bathroom. She'd been jacked up against the wall by a group of boys. She was crying, terrified. I said just stay home, we'll figure it out. That was my last conversation with Sage for five months.
The night she ran, she thought, to a young friend she'd met online, she left a note saying she was scared of what would happen if she stayed. The sheriff, FBI, search dogs were called in. I dropped to my knees in prayer. Nine days later the FBI found her in Baltimore. My baby had been lured online, sex trafficked by DC then Maryland. She was locked in a room, drugged, gang raped and brutalized by countless men. It was night. The FBI told us to pick her up in Maryland the next morning.
We packed our cars with blankets and stuffed animals and arrived by 8 am, but we were told we couldn't see her, and were summoned before Judge Robert Kershaw late that afternoon. They didn't even tell Sage that we came for her. We finally entered the courtroom and Sage appears on a huge Zoom screen from a prison cell. She looks tiny and broken, and I cry out 'I love you Sage.' Sage responds 'I love you too, Nana.' But attorney Anisa Khan rebukes us. She is a 'he' and his name is 'Draco' not Sage. We were floored.
Khan accuses us of emotional and physical abuse, that we are misgendering her, even though we just learned she claims to be trans and we're willing to use any name and pronouns to bring her home. My husband was so tearful he kept forgetting the new pronouns, so the judge had the bailiff remove him from the courtroom. I was pleading for my child to be returned and treated for her unspeakable trauma. Judge Kershaw told me, if I use the word 'trauma' again, he would throw me out too.
For over two months, he withheld custody. He housed Sage in the male quarters of a children's home. Sage told me she was the only girl and repeatedly assaulted. She was given street drugs by the other kids and Khan told her she didn't care. She just wanted to win the case and all the way to the Supreme Court if necessary. Khan tried to prove abuse, but we were eventually cleared by both states of all charges.
Sage later told me Khan had told her to lie that we hit her. Khan even had Sage's school counselors testify against us, though they barely knew Sage and they didn't know us at all. Khan told my precious child I didn't want her anymore. I found out Sage never received any of the letters I sent her.
Sage ran from the Children's Home and disappeared for months. They told me she might already be gone forever, but I couldn't give up and I finally found a tip on her social media that led the marshals to her in Texas. She had been drugged, raped, beaten and exploited. This time I was able to be with her for the traumatic rape exam, and to bring her home.
Back in Virginia, she entered the mental health facility that Judge Kershaw had ordered, as it would affirm her as a male. The therapist began pressuring her to have her healthy breasts removed. Sage was too scared to protest, but she asked me to secretly buy her girl's clothes because she wanted to be a girl, but keep them in the car. It took a kind lawyer, Josh Hetzler to secure her discharge.
After almost a year. Sage was finally home. Safe. Alive. Sage is receiving professional trauma care. The first trafficker has already been convicted. Sage has nightmares, panic attacks, rape-related medical issues, but there's hope. I tell her she's not broken she's just scarred. And part of that hope is that in courageously sharing her story, others will be saved.
Sage said she doesn't know who she was back then. She wasn't a boy, she just wanted to have friends. But her school, the judge, the attorney and the doctor were all blinded by their ideology. The consequences for Sage were unspeakable.
Please don't let ideology harm another child. Let parents do our jobs. We know our children best and we love them a million times more.
Thank you.
==
Jesus Christ. This girl was exploited by everybody, except for her parents, who were villainized for literally nothing. It's opposite world.
And the fact that everybody with authority prioritized stupid shit like pronouns and trying to coax her further down into a fake identity, even against her will, and other ideological bullshit over her actual wellbeing is disgraceful.
The judge and attorney need to be disbarred, the therapist stripped of their license, and everyone who conspired to separate Sage from her parents fired.
#Sage's Law#HB 2432#gender ideology#queer theory#ideological corruption#genderwang#safeguarding#child safeguarding#predators#groomers#predatory#gender cult#religion is a mental illness
2K notes
·
View notes
Text
0 notes
Text
By: Chloe Cole
Published: July 28, 2023
On Thursday, her 19th birthday, Chloe Cole testified to Congress with a “final warning” that medical treatments to change the gender of confused children is horrific. Cole, who was given surgery as a teenager to become male and soon regretted it, said what she needed most was therapy, not a scalpel. Here is what she told lawmakers:
My name is Chloe Cole and I am a de-transitioner.
Another way to put that would be: I used to believe that I was born in the wrong body and the adults in my life, whom I trusted, affirmed my belief, and this caused me lifelong, irreversible harm.
I speak to you today as a victim of one of the biggest medical scandals in the history of the United States of America.
I speak to you in the hope that you will have the courage to bring the scandal to an end, and ensure that other vulnerable teenagers, children and young adults don’t go through what I went through.
Deceit & coercion
At the age of 12, I began to experience what my medical team would later diagnose as gender dysphoria.
I was well into an early puberty, and I was very uncomfortable with the changes that were happening to my body. I was intimidated by male attention.
And when I told my parents that I felt like a boy, in retrospect, all I meant was that I hated puberty, that I wanted this newfound sexual tension to go away.
I looked up to my brothers a little bit more than I did to my sisters.
I came out as transgender in a letter I sent on the dining room table.
My parents were immediately concerned.
They felt like they needed to get outside help from medical professionals.
But this proved to be a mistake.
It immediately set our entire family down a path of ideologically motivated deceit and coercion.
The general specialist I was taken to see told my parents that I needed to be put on puberty-blocking drugs right away.
They asked my parents a simple question: Would you rather have a dead daughter or a living transgender son?
The choice was enough for my parents to let their guard down, and in retrospect, I can’t blame them.
This is the moment that we all became victims of so-called gender-affirming care.
I was fast-tracked onto puberty blockers and then testosterone.
The resulting menopausal-like hot flashes made focusing on school impossible.
I still get joint pains and weird pops in my back.
But they were far worse when I was on the blockers.
Forever changed
A month later, when I was 13, I had my first testosterone injection.
It has caused permanent changes in my body: My voice will forever be deeper, my jawline sharper, my nose longer, my bone structure permanently masculinized, my Adam’s apple more prominent, my fertility unknown.
I look in the mirror sometimes, and I feel like a monster.
I had a double mastectomy at 15.
They tested my amputated breasts for cancer.
That was cancer-free, of course; I was perfectly healthy.
There is nothing wrong with my still-developing body, or my breasts other than that, as an insecure teenage girl, I felt awkward about it.
After my breasts were taken away from me, the tissue was incinerated — before I was able to legally drive.
I had a huge part of my future womanhood taken from me.
I will never be able to breastfeed.
I struggle to look at myself in the mirror at times.
I still struggle to this day with sexual dysfunction.
And I have massive scars across my chest and the skin grafts that they used, that they took of my nipples, are weeping fluid today, and they’re grafted into a more masculine positioning, they said.
After surgery, my grades in school plummeted.
Everything that I went through did nothing to address the underlying mental health issues that I had.
And my doctors with their theories on gender that all my problems would go away as soon as I was surgically transformed into something that vaguely resembled a boy — their theories were wrong.
The drugs and surgeries changed my body, but they did not and could not change the basic reality that I am, and forever will be, a female.
Depths of despair
When my specialists first told my parents they could have a dead daughter or a live transgender son, I wasn’t suicidal.
I was a happy child who struggled because she was different.
However at 16, after my surgery, I did become suicidal.
I’m doing better now, but my parents almost got the dead daughter promised to them by my doctors.
My doctor had almost created the very nightmare they said they were trying to avoid.
So what message do I want to bring to American teenagers and their families?
I didn’t need to be lied to.
I needed compassion.
I needed to be loved.
I needed to be given therapy that helped me work through my issues, not affirmed my delusion that by transforming into a boy, it would solve all my problems.
We need to stop telling 12-year-olds that they were born wrong, that they are right to reject their own bodies and feel uncomfortable with their own skin.
We need to stop telling children that puberty is an option, that they can choose what kind of puberty they will go through, just like they can choose what clothes to wear or what music to listen to.
Pseudoscience
Puberty is a rite of passage to adulthood, not a disease to be mitigated.
Today, I should be at home with my family celebrating my 19th birthday.
Instead, I’m making a desperate plea to my elected representatives.
Learn the lessons from other medical scandals, like the opioid crisis.
Recognize that doctors are human, too, and sometimes they are wrong.
My childhood was ruined along with thousands of de-transitioners that I know through our networks.
This needs to stop. You alone can stop it.
Enough children have already been victimized by this barbaric pseudoscience.
Please let me be your final warning.
Thank you.

Might as well call her a murtad and kufr.
"The medical industry mutilated me, maybe don't mutilate other kids," shouldn't require bravery or renouncing an ideology.
Reminder: A minor under the age of 18 is too young to agree to a cellphone contract. 🤦♀️
#Chloe Cole#detrans#detransition#gender ideology#queer theory#medical malpractice#medical scandal#medical mutilation#gender affirming#gender affirming care#affirmation model#double mastectomy#gender cult#sex trait modification#genderwang#religion is a mental illness
1K notes
·
View notes
Text




#Leor Sapir#Daisy Strongin#detrans#detransition#detransition rights#double mastectomy#bilateral mastectomy#top surgery#gender ideology#queer theory#iatrogenic harm#medical malpractice#medical corruption#medical scandal#medical transition#American Medical Association#genderwang#gender identity ideology#religion is a mental illness
229 notes
·
View notes
Text
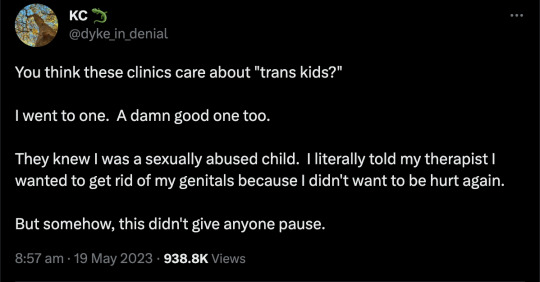



You may remember KC Miller.

She deleted her account after she went viral as it was all too much. This is from her new account.
#KC Miller#detrans#detransition#medical malpractice#medical corruption#sex trait modification#medical scandal#medical transition#unethical#gender ideology#queer theory#genderwang#testosterone#wrong sex hormones#cross sex hormones#double mastectomy#this never happens#religion is a mental illness
996 notes
·
View notes
Text


https://journals.lww.com/prsgo/fulltext/2021/11000/letter_to_the_editor__regret_after.29.aspx

https://academic.oup.com/jcem/article-abstract/107/9/e3937/6572526?login=false
https://www.sciencedirect.com/science/article/abs/pii/S1054139X22007194
https://www.mdpi.com/2227-9032/10/1/121

https://link.springer.com/article/10.1007/s10508-021-02163-w
https://www.bmj.com/content/380/bmj.p382

https://www.bmj.com/content/380/bmj.p382
https://www.reuters.com/investigates/special-report/usa-transyouth-outcomes/
https://link.springer.com/article/10.1007/s11930-023-00358-x
https://www.tandfonline.com/doi/full/10.1080/0092623X.2022.2150346
#Christina Buttons#desistance#transition regret#detrans#detransition#medical transition#gender ideology#genderwang#queer theory#sex trait modification#medical scandal#medical mutilation#poor evidence#weak evidence#medical malpractice#religion is a mental illness
625 notes
·
View notes
Text
We have a serious problem
Michael Laidlaw, MD: I'm a board-certified endocrinologist, practicing in private practice for the last 16 years. I've been studying and publishing in this area for the last 5 years, including peer reviewed journals such as Journal of of Clinical Endocrinology and Metabolism, and others. I also have a patient who is a detransitioner.
I think it's important to note that studies are shown that desistance, or growing out of this condition, of children by adulthood is very high. It's some 50-98%.
I want to be sure before I give someone a very powerful hormone like Insulin that they in fact have diabetes.
What about cancer? Before we give any powerful agents such as chemotherapeutics or surgeries, we certainly want to have physical evidence of this problem, such as biopsies or imaging.
Now, the gender affirmative therapy treatment proposed by WPATH gives very powerful hormones and surgeries on what basis? Where can we find the gender identity to be certain that these children will not desist by adulthood? Can we use imaging of the brain or blood tests, genetic testing, are there other biomarkers to ensure that we are correct? There is no such thing.
Julia Mason, MD: The Endocrine Society put out guidelines in 2017, and they were very careful in the guidelines. One, to point out that the evidence was of low and very low quality. And they also said in the guidelines that they have no idea how you identify which kids are trans and require this treatment.
And then the American Academy of Pediatrics the next year just leapt into that void and said, oh, oh, we'll tell you how you know which kids. You ask them.
Prior to 2018 I had maybe one trans patient. But then there was another one. And another one. And another one.
It wasn't until later that I started asking questions like, wait, every single kid I send to the gender clinic gets put on puberty blockers or cross-sex hormones. Just, it was happening immediately.
Patrick Hunter, MD: This affirmative model of care has spread wildly in the last 8 years. Now we have objective, unbiased systematic reviews. These systematic reviews tell us the evidence for youth transition is poor quality, and with very low certainty for benefit.
In JAMA Pediatrics, there was a study reported from Northwestern University in Chicago. Patients ranged in age from 13 to 24 years. The authors concluded that mastectomy was beneficial and should not be delayed in youth. What lead them to that conclusion? The finding that 3 months after surgery, the 36 patients were happy with their flat chests. They lost 9% of their surgical cases to follow-up. Nine percent. In 3 months.
It is absurd, meaningless to draw any conclusions after 3 months.
This paper is indicative of the quality of research we have in this field, published in our most prestigious journals.
We have a serious problem.
#gender ideology#queer theory#medical transition#desistance#detrans#sex trait modification#genderwang#detransition#trans identity#cross sex hormones#wrong sex hormones#puberty blockers#poor research#medical malpractice#medical scandal#medical corruption#endocrinology#low quality#ideological capture#ideological corruption#religion is a mental illness
910 notes
·
View notes
Text
Editor’s note: This hypothetically open letter was originally posted by its anonymous author on Medium and was rapidly removed as “hate speech.” We found it to be a refreshing dose of honesty, a charming and relatable open letter from one parent to other parents (not to the child, obviously!) about dealing with a challenging and dangerous moment in raising children, especially “weird” adolescents who search for their identities harder than others and risk making life-damaging mistakes in a way never before possible. We are reposting it here on New Discourses with the permission of the author.
--
By: Donna M.
Published: Mar 5, 2021
My dear, sweet, son,
I’ve got to break it to you: you’re not trans, you’re just weird.
This seems like a cruel thing to point out right now. Clearly, you are struggling and feeling pretty awful about things. I can see that you are in a rough patch, and one of the first rules of parenting is to not pile on. The world is pretty heavy on your shoulders. You’re fifteen. There’s a pandemic going on. But here I come anyway. I’m about to throw more on you.
When you were two – a happy, chubby, little tyke in pull-ups, you watched the world with wary eyes behind the thumb in your mouth. You leapt with joy in the rhythm of the toddle music classes. You chattered and shared stories about your stuffed animals. You loved your little sister. Enjoyed cookies and finger painting. That was all pretty normal.
But you also started to count to one thousand on our walks. And you started to call out the store names as we drove around. And you preferred reading books rather than playing with the other two-year-olds at preschool. And you hated sitting in the circle when instructed. And you hated the feel of blue jeans. And you threw big tantrums when you lost any kind of game. In other words, you started to show signs that you were… weird.
The grandparents were the first to notice. They said gentle things like “You oughta keep an eye on that one,” and sent us links to Wall Street Journal articles about child prodigies. And then the other parents in the play groups started to comment; “He’s pretty intense, huh?” And the teachers were on to it pretty quickly. They started to use fancy terms like “asynchronous development.”
By third grade, we realized you were different, but we still didn’t realize you were weird. Truthfully, we’re used to people like you. Our family is full of engineers, artists, musicians, computer programmers, and a lot of “free-thinkers.” Family gatherings always have chess, political debates, and quartets around the piano. That’s just us.
And besides, you had a small but solid group of friends. There was Pokémon, then Minecraft, then Magic, then Dungeons and Dragons, then Catan. You were never in the center of things, but you weren’t alone.
But then, in middle school, things started to change. By 7th grade, school finally started to require some effort, and it turned out you were pretty disorganized. People kept calling you smart, but the teachers were annoyed at your humor, and frustrated that you wouldn’t or couldn’t follow the guidelines for assignments. Classmates didn’t appreciate your frank (if accurate) descriptions of their efforts. I’ll admit, we got pretty frustrated with you, too.
And then puberty arrived, with its triple curse of acne, braces, and bizarre growth. The girls appeared to have it all together (I know they don’t, but they do appear that way). And the popular boys seemed to know exactly what to do. They can talk sports to each other, they brag about their romantic exploits. They never get in trouble for stupid reasons like forgetting an assignment three times in a row. Your anxiety started to kick in, and it seemed like you got smaller. And some of your guy friends moved on.
So you drifted over to the weird-o crowd. Well — I’m not sure what you call yourselves, but that’s what we would have called you back when I was in school. At different schools these are the geeks, or the theater kids, the math team kids, or the artsy-fartsy kids. This used to be where the gay kids ended up, but I think they’re more dispersed now. You get some kids whose parents are going through some rough times. Some girls with anorexia. A few boys who are edgy and angry. Kids with a great sense of humor and big hearts.
And some of these kids are really passionate. Just full of righteous anger about the injustices of the world. And some of them are dramatic. And truthfully, that looks pretty attractive to you. Because you share some of that confusion and anger about the world. And though you may not be sure what you think or what you feel, you are certain you don’t want to be on the bad side. You certainly aren’t like those popular boys with their suave charm and dominating manners. You’re not like them at all.
You’re actually more like those vibrant girls who can speak for hours about their ideas. Well, you would be if you could find the words to speak. And there is something so fascinating about those girls, but you can’t quite put your finger on it. You’d never think about talking to those girls anyway, because that’d be weird. Because you are weird. You’ve never been good at chit-chat, or eye contact. Or girls. And besides, you wouldn’t want them to get the wrong impression. You understand that your peers are starting to date, but you really don’t see the point. Sex is still gross and weird to you. It’s better to just call yourself “asexual” or “pansexual.” It’s like a get-out-of-jail-free card that helps you avoid the whole mess. And your group of friends tell you that you are super cool and brave for being able to say that about yourself.
But you’ve fallen into a funk. Anyone can see that. But computer games help. And there’s always trying to beat the speed record for that one game you’re kinda good at. And that one guy on reddit always has good tricks. And the people on that message board seem to get your humor.
So when one of them posts a meme about trans rights, it makes sense that you’d check it out. You’re curious! You’re a free thinker! You’re not like the normies. And the web quiz hits home. You do feel discomfort with your body. You don’t like sports. You do wonder what it would be like to be a girl. You’ve always felt like something was different about you.
You’re right. There is something different about you.
But you’re not trans, you’re just weird.
So we’re right here for you. We’ll always be here for you. But those online folks who urge you to “crack your trans egg” and rush to hormones and surgeries don’t know you at all. They don’t know that gifted kids and ADHD kids and Autism kids and Asperger’s kids are slower to develop emotionally and sexually. They don’t know that sexuality takes time and experience to figure out, and that the majority of trans teens seeking medical treatment haven’t even masturbated or kissed someone yet. They don’t know that 80% of trans children end up becoming comfortable with their birth sex if you just give them time. They don’t know that there are increasing numbers of desisting and de-transitioning people in their twenties. They don’t realize that hormones permanently stunt your growth, decrease your IQ, and can cause sterility. They don’t know that these hormones are prescribed off-label and there’s no research on the long-term outcomes. They don’t even know that the most recent research shows that short-term outcomes are clearly worse.
They don’t realize that you’re weird. But I do. You’re weird, kiddo. You’ll figure that out in a year or two. But that’s okay. We are all weird. And I love you anyway. You’re going to be just fine.
==
You always hear stories and justifications like, "she never liked wearing a dress," or "he always hated having his hair cut." This is post-hoc confirmation bias. Not only does this confirm everything critics say about this being a movement based on gross stereotypes, but they always leave out things like, "she refused to eat anything yellow," and "he was obsessed with elevator and crossing buttons and would cry if he wasn't the one to light it up."
It's okay to be weird.
#Donna M#gender identity#gender ideology#queer theory#genderwang#trans egg#it's okay to be weird#it's ok to be weird#normalize weird#religion is a mental illness
379 notes
·
View notes
Text
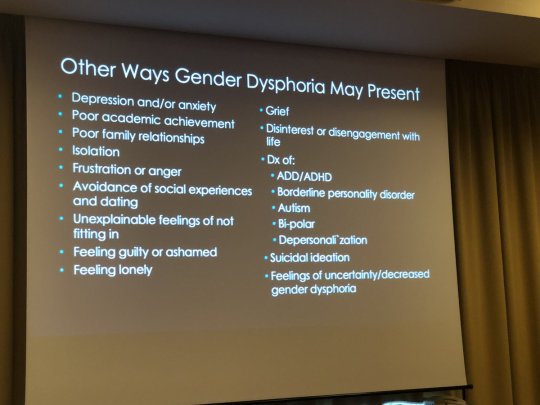
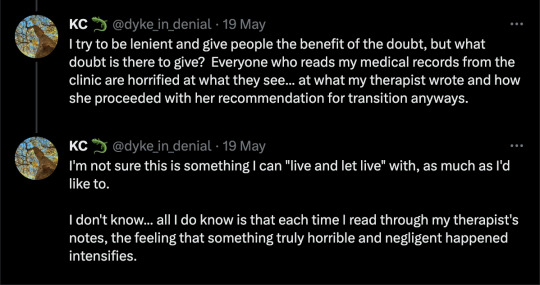
[ Source: EPATH Conference 2019. ]
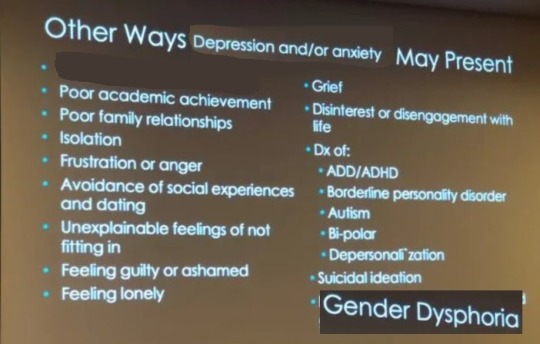
Apparently being a regular teenager is a disorder requiring medical treatment and the removal of body parts. Not only are you "trans" if you don't fit a 1950s Barbie/G.I. Joe stereotype, you're "trans" if you don't fit a 1950s "golly, gee" soda shoppe "Leave It To Beaver" stereotype.
This is the same tactic psychics use to tell you your fortune, and astrologers use to convince you that distant stars reflect your personality. It's called the Forer Effect, or Barnum Effect.
To really drive home the cult programming, any time you're feeling better, that's how you know you've gotten worse.
For political and ideological reasons - for example, one presenter actually claims that children are being "misdiagnosed" as autistic when they're actually trans - they've flipped the symptom and the cause.
This is more accurate:
#Wilfred Reilly#gender cult#queer theory#gender ideology#mental health#mental health issues#gender dysphoria#gender anxiety#puberty#unethical#medical scandal#medical malpractice#ideological capture#psychology#human psychology#sex trait modification#genderwang#religion is a mental illness
735 notes
·
View notes
Text
"Three things I wish I knew before I transitioned to male.
One: that injecting myself with cross sex hormones actually was damaging my perfectly healthy body.
Two: that changing my identity and changing my body wasn't actually going to heal the pain that I had within myself. It was just an escape that created actually more trauma for me.
Three: that it was okay to be a tomboy and not fit into society's beauty standards of what a woman was supposed to be like. That I was perfect the way I was, and I didn't need to change myself."
#detrans#detransition#gender ideology#queer theory#medical transition#sex trait modification#wrong sex hormones#cross sex hormones#medical scandal#gender identity#tomboy#save the tomboys#genderwang#religion is a mental illness
507 notes
·
View notes
Text






By: SEGM
Published: Aug 13, 2023
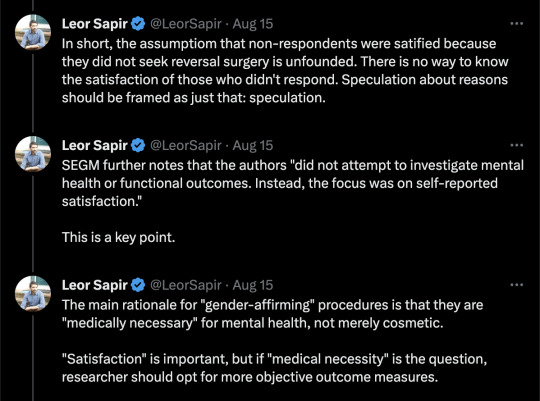
Near-zero regret” findings among adults suffer from a critical risk of bias and have low applicability to youth
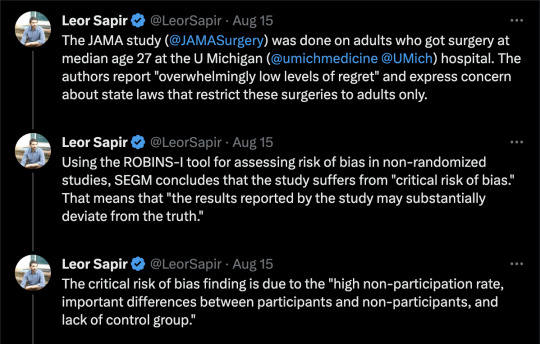
Recent research published in JAMA Surgery evaluated satisfaction and regret among individuals who had undergone chest masculinizing mastectomy at the University of Michigan hospital. The average patient age at the time of mastectomy was 27 years; no patients who were under age 18 were allowed to participate in the study.
The participants reported high levels of satisfaction and low levels of regret at an average of 3.6 years following mastectomy. The study authors lauded the “overwhelmingly low levels of regret following gender-affirming surgery,” and framed their findings as in conflict with the “increasing legislative interest in regulating gender-affirming surgery,” referring to current legislative attempts to restrict or ban “gender-affirming” procedures for minors. Another group of authors provided an invited commentary on the paper, reinforcing the view held by the study authors, and asserting the presence of a “double standard:” “gender-affirming” mastectomies have come under undue scrutiny by states’ legislators, while other surgical procedures with higher regret rates do not appear to concern legislative bodies.
The study suffers from serious methodological limitations, which render the findings of high levels of long-term satisfaction with mastectomy among adults at a "critical risk of bias"—the lowest rating according to the Risk of Bias (ROBINS-I) analysis. ROBINS-I is used to assess non-randomized studies for methodological bias. The "critical risk of bias" rating signals that the results reported by the study may substantially deviate from the truth. The results also suffer from low applicability to the central issue the study and the invited commentary sought to address, which was whether legislative attempts to regulate “gender-affirming” surgeries are warranted in minors. Unfortunately, these highly questionable findings are misrepresented as certain and highly positive by both the study authors and the invited commentators, several of whom have significant conflicts of interest.
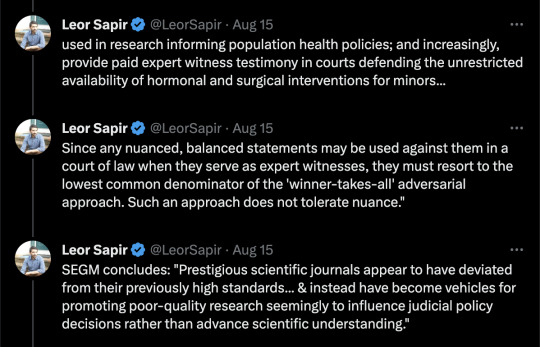
Below, we provide a detailed explanation of the key methodological issues in the study which render its claims untrustworthy and not applicable to the patient population at the center of the debate: youth undergoing gender reassignment. We also comment on the alarming trend: several prestigious scientific journals appear to have deviated from their previously high standards for scholarly work and instead have become vehicles for promoting poor-quality research, seemingly to influence judicial policy decisions rather than advance scientific understanding. We conclude with recommendations about how journal editors can restore the integrity of scientific debate and raise the bar on the quality of published studies in the field of gender medicine.
[ For in-depth analysis, see: https://segm.org/long-term-regret-satisfaction-mastectomy-critical-appraisal ]
SEGM Take-Aways
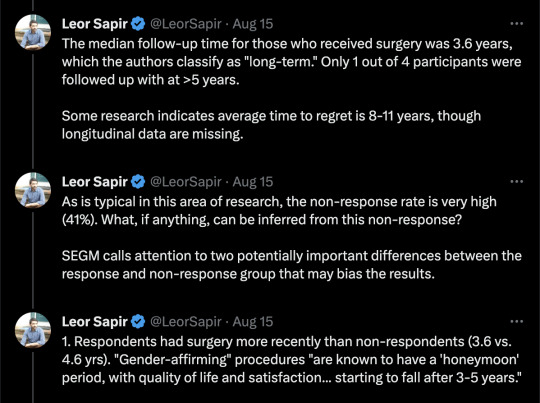
Although this study reports extremely high rates of satisfaction and low regret, the timeframe in which these outcomes were assessed is insufficient—just 3.6 years post-mastectomy on average. The sample is also highly skewed: 50% of the participants had mastectomies in the last 3.6 of the 30 years. This skewing of the length of time since surgery is expected, given the sharp rise in the number of people (especially adolescents and young adults) identifying as transgender and undergoing chest masculinization mastectomy. It is also a short time in which to assess regret, particularly since one quarter of study participants were younger than age 23 at time of surgery and the median age of first birth in the US is 30 years.
The conclusion of high satisfaction/low regret suffers from a critical risk of bias due to the high non-participation rate, important differences between participants and non-participants, and lack of control group. Problematically, the authors misuse the (critically-biased) results from adults to argue against regulations for irreversible body alternations for minors and do so with a decidedly politicized spin.
The only intellectually honest commentary is that we do not have good knowledge of the likely rates of detransition and regret following chest masculinization mastectomy, nor do we know how many people experience regret but remain transitioned. There is an urgent need for quality research in this area. Previously, detransition and regret rates were considered to be low: they may have indeed been low due to the much more rigorous screenings, or the results may have been biased by the notoriously high dropout rates that plague “regret” research. Regardless, there is now growing evidence of much higher rates of medical detransition.
A recent study from a comprehensive U.S. dataset with no loss to follow-up revealed a 36% medical detransition rate among females within just 4 years of starting hormonal transition. At least two recent studies suggest that average time to regret among recently-transitioned females is about 3-5 years, but there is a wide range. Much less is known about detransition among those who undergo surgery. A growing number of detransitioners now express regret associated with the loss of breastfeeding ability, with one case study detailing breastfeeding grief experienced some 15 years post-mastectomy.
The study and invited commentary exemplify three problematic trends that plague studies emerging from the gender clinics: problematic conflicts of interest of the authors; leveraging scientific journals to disguise politically-motivated pieces as quality research; and a conflicted stance by the gender medicine establishment on surgery for minors. We expand on each briefly below.
Conflicts of interest of study authors and commentators
The significant conflicts of interest of the gender clinicians who study and report on the outcomes of “gender-affirming” interventions cannot be overlooked. These clinicians are conflicted financially, since their practices specialize in “gender-affirming” interventions, as well as intellectually. While conflicts of interest among experts are common, such experts should still attempt to be balanced in their discussions and should acknowledge and reflect on their conflicts of interest.
The interpretations of the data in the study is neither rigorous nor balanced, and both the study and the invited commentary have a decidedly political spin. Further, the invited politicized commentary does not disclose that at least one of the authors is a key expert witness opposing states’ efforts to regulate “gender-affirming” surgeries for minors. This role alone precludes the ability to provide a balanced commentary.
There is a fundamental problem with research emerging from gender clinic settings. The same clinicians provide gender-transitioning treatments to individual patients in their practice; serve as primary investigators and custodians of data used in research informing population health policies; and increasingly, provide paid expert witness testimony in courts defending the unrestricted availability of hormonal and surgical interventions for minors.
As a result, such clinicians cannot express nuanced perspectives. Since any balanced statements may be used against them in a court of law when they serve as expert witnesses, they must resort to the lowest common denominator of the "winner-takes-all" adversarial approach. Such an approach does not tolerate nuance. Unfortunately, this approach contributes to the erosion of the quality of the published work in the arena of gender medicine and accelerates loss of trust about the integrity of the scientific process.
Misuse of scientific publications to promote politically-motivated articles disguised as scientific research
That prestigious medical journals now serve as platforms for promoting misleading, politically motivated research that aims to apply a veneer of misplaced confidence in highly invasive, irreversible treatment should worry everyone committed to evidence-based medicine and the integrity of science. Moreover, it impairs our ability to accurately assess and improve the long-term health outcomes of the rapidly growing numbers of gender-diverse and gender-distressed youths.
This is not the first time that a JAMA has been used as a platform for positioning advocacy for “gender-affirming” care as scientific research. In 2022, JAMA Pediatrics published a study that assessed bodily happiness in a group of subjects aged 14-24 three months after chest masculinization mastectomy. Despite the very short follow up and dropout rate of 13%, the authors argued that their findings supported the premise that there was no evidence to suggest that young age should delay surgery. They also asserted that their research would help dispel the misconception that such surgeries are experimental. The editorial commissioned to bolster the authors claims was descriptively titled, “Top surgery in adolescents and young adults-effective and medically necessary.”
Another troubling trend is the misuse of statistical tools to reframe research findings that contradict the author's own position. For example, a well-known study that claimed that access to puberty blockers reduce the risk of suicide disregarded the fact that individuals reporting use of puberty blockers use had twice as many recent serious suicide attempts as their peers who did not use puberty blockers. Like the finding cited above, the doubling of suicide attempts was not statistically significant due to a small underpowered sample—but the magnitude of the effect was striking and should have tempered the authors’ enthusiastic conclusion that puberty blockers prevent suicides. Another recent gender clinic study, widely and positively covered by major media outlets, claimed that puberty blockers and cross-sex hormones led to plummeting rate of depression—even though the rate of depression among youth taking those medications remained demonstrably unchanged. More information about problems with research originating from gender clinics is detailed in this recent analysis.
Gender medicine’s stance on pediatric surgery
More generally, the gender medicine establishment is in a curious state of internal conflict about its stance on “gender-affirming” surgeries for minors. On the one hand, it has become common for advocates of “gender-affirmation” of minors to insist that surgeries for minors are not performed and anyone who suggests otherwise is spreading “scientific misinformation” and “science denialism.” On the other hand, gender clinicians publish mastectomy outcomes for minors in major medical journals, and laud surgeries for minors as “effective and medically necessary.” It is not uncommon for these opposing claims to be made by the same group of researchers and clinicians, as they test various arguments, searching for the "angle" that is most likely to convince judges and juries--and public at large--that scrutiny of the practice of pediatric transitions, which is increasingly occurring in European countries, is not warranted in the United States.
Notably, none of the European countries that are enacting severe restrictions on the use of puberty blockers or cross-sex hormones for minors have ever allowed surgeries for youth under 18. That the U.S. gender affirmation professionals continue to fight regulation of these problematic procedures speaks volumes about how far the U.S. healthcare has drifted when it comes to "gender affirmation" of minors.
Final thoughts
While it is challenging to determine how best to reduce the temperature of the highly politicized nature of the debate in gender medicine, the editors of scientific journals can begin to restore balance by recognizing how far the field has drifted from the standards of quality scientific research, and begin to expand their circle of peer-reviewers to those with diverse views. Inviting those concerned with the state of gender medicine (and not just the practices’ advocates) into the peer-review and commentary process is the first essential step to improve the quality of research published in the field of gender medicine.
--


--

==
The activists are predictably - and consistent with the superficiality of their own ideology - upset that anyone should look below the surface. It seems to be more troubling that anyone would notice the shoddiness of the research, than that the research is shoddy.
If this is supposed to be "healthcare," you would think that they would want the best healthcare, and be more alarmed at the misrepresentations of the study, than by people finding those misrepresentations.
Could it be that this is ideological rather than medical? 🤔
The conflicts of interest and funding sources alone are remarkable.
#Leor Sapir#SEGM#Society for Evidence Based Gender Medicine#double mastectomy#top surgery#gender affirming mastectomy#ideological corruption#ideological capture#medical malpractice#conflict of interest#sarcastic font#medical scandal#medical corruption#gender ideology#genderwang#queer theory#gender affirming care#gender affirming surgery#gender affirming healthcare#medical mutilation#sex trait modification#religion is a mental illness
276 notes
·
View notes
Text
https://thedecisionlab.com/biases/commitment-bias
What is the Commitment Bias?
Commitment bias, also known as the escalation of commitment, describes our tendency to remain committed to our past behaviors, particularly those exhibited publicly, even if they do not have desirable outcomes.
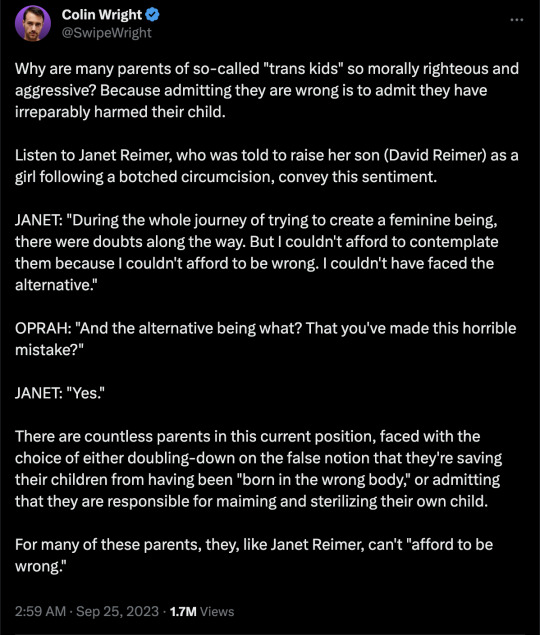
It's not only the wave of kids themselves who will require therapy and support for what was done to them, but also - and possibly even more so - the parents who got caught up in this hysteria and psychologically, and possibly medically, damaged their kids.
It's a classic parental tenet that "I would die for my child." But the cognitive walls necessary to actually deny and avoid admitting that you are the one who permanently damaged your own child must be the highest, thickest ones of all. And what happens when those finally come down?
#Janet Reimer#David Reimer#Joan/John#Brenda/Bruce#gender lobotomy#transition#sunk cost fallacy#gender ideology#queer theory#genderwang#detrans#detransition#religion is a mental illness
206 notes
·
View notes
Text
By: Louise Perry
Published: Jun 8, 2023
When we get home from the supermarket, our two-year-old likes to assist with taking the groceries out from underneath his stroller and carrying them to the kitchen. He will pick up a carton of milk and heave it towards the fridge like an atlas stone. “Well done darling” I say to him in a pitch slightly higher than usual, “you’re being so helpful.”
Of course he isn’t actually being helpful. In fact, he’s slowing down the process of unpacking and risking an enormous milk spillage all over the kitchen floor. But my goal is encouragement and kindness – he’s only two, bless him, and that carton is awfully big and heavy.
My husband regards these exercises with more of a gentle briskness. “Thanks mate” he’ll say in his usual tone of voice, excising my white lie. In this, I’ve learnt, my husband is typical of other men. In a 2015 study led by Mark VanDam, a professor in the Speech and Hearing Sciences department at Washington State University Spokane, researchers outfitted preschoolers and their parents with recording devices to monitor social interactions over the course of a normal day. The mothers, they found:
… used higher pitch and varied their pitch more when interacting with their child than with adults. The fathers, on the other hand, did not show the same pattern, and instead talked to their children using intonation patterns more like when they talked to other adults.
As an instinctive speaker of so-called ‘motherese’ – that is, baby talk – I find that when our son mispronounces a word (‘tawtah’ for ‘water’ or ‘mulack’ for ‘milk’) I will automatically echo it back to him, while my husband will automatically respond with the correct pronunciation. These differences persist despite the fact that we share childcare almost exactly equally within our family.
It turns out we’re not alone in this sex difference, and that it may well have some adaptive purpose. "We think that maybe fathers are doing things that are conducive to their children's learning but in a different way,” writes VanDam, “the parents are complementary to their children's language learning.” Mothers speak down to children, while fathers speak to them like equals – in combination, these two kinds of stimuli promote the development of adult language.
The adoption of motherese is an instinct that, in its correct context, is both comforting and developmentally useful. But it can also, in some circumstances, be dysfunctional. And, as I have become more and more fluent in it, I have started to notice that motherese is no longer confined to the nursery or the classroom, but is now to be found also in public life. Not in its full expression – “have you got a boo-boo, honey?” – but in a more subtle form.
I heard a lot of motherese, for instance, in the responses to philosopher Kathleen Stock’s appearance this week at the Oxford Union – a political event considered significant enough to attract commentary from the Prime Minister and rolling updates on the homepages of several national newspapers.
Students at risk of being traumatised by Stock’s mild-mannered, centre-left brand of politics were ushered towards ‘welfare rooms’ offering ear plugs, bottles of water, and snacks. “The Union has made the choice to amplify a voice that actively harms trans students, trans people and the trans community at large” wrote one student politician, “we’re tired of [the Union’s] refusal to listen to the communities they hurt” insisted another. It was as if Stock was a rampaging bully on the playground, knocking other children to the ground, and her critics were leaping to the defence of the persecuted toddlers.
Witnessing the backlash against her, you’d never guess that Stock’s only sin is to offer a careful academic critique of the doctrine of gender identity – that is, the claim that one can become a member of the opposite sex (or some other identity category in between) merely by force of will. As she reiterated in her Oxford Union speech, to reject this doctrine is not to deny the humanity of trans people, but rather to balance their interests against those of other people, particularly women.
But I am by no means the first to notice an unexpected feature of the crowds that formed outside the Oxford Union this week, and indeed all of the crowds that congregate in support of trans activism (now a regular occurrence, and not just in the Anglosphere). While the occasional acts of outright aggression are overwhelmingly committed by men, the crowds in general are mostly composed of young women.
Polling reveals this to be a wider pattern. In the UK, women – and particularly young women – are far more supportive of trans activism than are their male counterparts. The same gap can be seen in US polling. The public figures who have received the most flak for their criticisms of trans activism are disproportionately women – I’m thinking not only of Kathleen Stock, but also of JK Rowling – and yet so, too, are the movement’s most devoted allies. This is, in the main, an intra-female conflict.
But if trans activism poses a threat to women’s interests – as Stock and Rowling insist that it does – then why have so many women come out in support of it? I want to propose two explanations for this seeming paradox.
Firstly, in socioeconomic terms, the women who have the most to lose from the disintegration of female-only spaces – prisoners and domestic abuse victims, for instance – are not actually the same women who are draping themselves in blue and pink flags outside the Oxford Union. This is a textbook example of what Rob Henderson has termed a ‘luxury belief’ – an idea that confers status on the rich, while causing harm to the poor.
But then I am begging the question, because why on earth would trans activism confer status on the rich, or indeed anyone? This is where we come to the second factor: the extraordinarily well-documented differences in personality that have been observed between male and female populations cross-culturally.
Note that there is a crucial distinction to be drawn between average and absolute differences. It is not true that all men or all women exhibit only masculine or feminine personality traits, in the same way that not all women are short and not all men are tall – rather, average differences between the sexes are obvious only at the population level.
One trait on which men and women differ substantially is agreeableness. To put it bluntly, women are usually nicer than men – that is, they are “more nurturing, tenderminded, and altruistic more often and to a greater extent than men,” as psychologist Professor Yanna Weisberg puts it.
This nurturing instinct often finds its way into polling on political questions. For instance, a typical study from 2017 asked 3,014 college students the following question: “If you had to choose, which do you think is more important, a diverse and inclusive society or protecting free speech rights.” 61% of male students chose to prioritise free speech, compared with only 35% of female students – exactly what you would expect from two populations that differ in this most crucial of traits.
Don’t think that I’m bashing agreeableness per se – it’s one of those personality traits that really does offer advantages and disadvantages all along the spectrum. Disagreeable people are often rude, but they can also be refreshingly honest; agreeable people are often pleasant, but they are easily taken advantage of. Think of agreeableness as motherese: soothing and lovely in the right circumstances, cloying and foolish in the wrong ones.
The problems arise when an agreeable style of politics gloms onto a group that seems to offer plentiful opportunities for babying. Right now, it is trans people who have found themselves in the hot seat (or the high chair). For just one example of this babying tendency in action, observe the progressive response when then-66 year old Caitlyn Jenner came out as trans (a response parodied exquisitely in a South Park episode titled ‘Stunning and Brave’). When Glamour honoured Jenner as the magazine’s 2015’ Woman of the Year' – despite the fact that Jenner had not yet lived as a woman for a full year – I couldn’t help but hear the high pitched notes of motherese (“you look so pretty sweetie”, “well done that was very brave.”)
Observe, too, the trans celebrity Dylan Mulvaney’s recent appearance on Drew Barrymore’s talkshow, which culminated with Barrymore kneeling on the ground, looking Mulvaney straight in the eye, and offering a heartfelt pep talk on self-love. Some gender critical feminists looked at this scene and saw a woman prostrating herself before a man. What I saw was a mother kneeling down to reassure a young child – for some bizarre reason, Barrymore was speaking motherese to a grown adult on national TV.
At the risk of stating the obvious, trans people are not babies. Nor are they pets. They do not need earplugs and snacks to withstand an academic discussion, and they do not need to be spoken to like toddlers. Real two-year-olds may benefit from the gentleness of motherese. The rest of us need to grow up.
==
https://policyexchange.org.uk/wp-content/uploads/2022/11/The-Politics-of-the-Culture-Wars-in-Contemporary-Britain.pdf#page=57
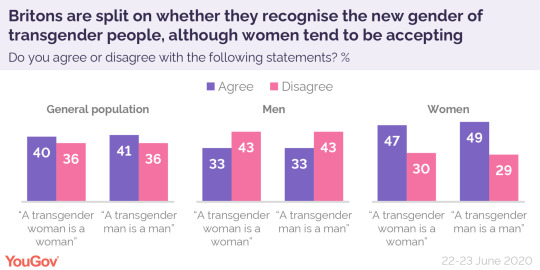
Women are more likely than men to say a trans women should be able to enter a women’s refuge, favouring this by a 36-32 margin while men oppose it 40 to 30. In fact, across all 6 questions pertaining to the trans issue (Stock, Rowling, refuges, gender identity, pronouns, teaching biological sex), women are significantly more supportive of the trans rights position even when ideology is taken into account. Women even exceed LGBT identifiers in their support for the pro-trans position on many questions.
Why? Is this not against the female interest? The likely answer is that women are more likely to be cultural leftists than men across most of the 25 attitudinal items in the survey. The inclination to empathise and care for groups perceived as vulnerable best accounts for the pattern. The result of the empathy dynamic is that the gender-critical feminist position, while intellectually prominent, is still a contested view among women. Indeed, the largest source of opposition to greater trans access to women’s spaces comes from cultural conservatives.
This isn't a war between men and women, as some would like to assert.
It's really a war between different denominations of feminism. Like Catholicism vs Protestantism. Or Sunni vs Shi'a Islam.
One thing that's hilarious and worth pointing out: gender-critical feminists will sometimes say things along the lines of, well that agreeableness was socialized into women by "the patriarchy" to make them compliant. Which means they're denying the same evolved sex-based differences that they started off defending. Like claiming to be a Catholic while denying transubstantiation.
Either sex-differences are real, and can explain different participation rates in physics and kindergarten teaching, different career priorities and trajectories (and thus, the mythical "pay gap") and different work patterns as readily as they explain differences in swimming, cycling and weight-lifting performance, making "the patriarchy" as unnecessary as a god is to the existence of the universe... or they're not, and the gender-critical argument goes up in smoke in the flames of social constructivism. God can't be both good and unknowable.
#Louise Perry#stunning and brave#gender activism#gender ideology#queer theory#genderwang#motherese#infantilization#mothering#western feminism#sex based differences#sex differences#religion is a mental illness
165 notes
·
View notes
Text




Published: Jul 13, 2023
As experienced professionals involved in direct care for the rapidly growing numbers of gender-diverse youth, the evaluation of medical evidence or both, we were surprised by the Endocrine Society’s claims about the state of evidence for gender-affirming care for youth (Letters, July 5). Stephen Hammes, president of the Endocrine Society, writes, “More than 2,000 studies published since 1975 form a clear picture: Gender-affirming care improves the well-being of transgender and gender-diverse people and reduces the risk of suicide.” This claim is not supported by the best available evidence.
Every systematic review of evidence to date, including one published in the Journal of the Endocrine Society, has found the evidence for mental-health benefits of hormonal interventions for minors to be of low or very low certainty. By contrast, the risks are significant and include sterility, lifelong dependence on medication and the anguish of regret. For this reason, more and more European countries and international professional organizations now recommend psychotherapy rather than hormones and surgeries as the first line of treatment for gender-dysphoric youth.
Dr. Hammes’s claim that gender transition reduces suicides is contradicted by every systematic review, including the review published by the Endocrine Society, which states, “We could not draw any conclusions about death by suicide.” There is no reliable evidence to suggest that hormonal transition is an effective suicide-prevention measure.
The politicization of transgender healthcare in the U.S. is unfortunate. The way to combat it is for medical societies to align their recommendations with the best available evidence—rather than exaggerating the benefits and minimizing the risks.
This letter is signed by 21 clinicians and researchers from nine countries.
FINLAND
Prof. Riittakerttu Kaltiala, M.D., Ph.D.
Tampere University
Laura Takala, M.D., Ph.D.
Chief Psychiatrist, Alkupsykiatria Clinic
UNITED KINGDOM
Prof. Richard Byng, M.B.B.Ch., Ph.D.
University of Plymouth
Anna Hutchinson, D.Clin.Psych.
Clinical psychologist, The Integrated Psychology Clinic
Anastassis Spiliadis, Ph.D.(c)
Director, ICF Consultations
SWEDEN
Angela Sämfjord, M.D.
Senior consultant, Sahlgrenska University Hospital
Sven Román, M.D.
Child and Adolescent Psychiatrist
NORWAY
Anne Wæhre, M.D., Ph.D.
Senior consultant, Oslo University Hospital
BELGIUM
Em. Prof. Patrik Vankrunkelsven, M.D. Ph.D.
Katholieke Universiteit Leuven
Honorary senator
Sophie Dechêne, M.R.C.Psych.
Child and adolescent psychiatrist
Beryl Koener, M.D., Ph.D.
Child and adolescent psychiatrist
FRANCE
Prof. Celine Masson, Ph.D.
Picardy Jules Verne University
Psychologist, Oeuvre de Secours aux Enfants
Co-director, Observatory La Petite Sirène
Caroline Eliacheff, M.D.
Child and adolescent psychiatrist
Co-director, Observatory La Petite Sirène
Em. Prof. Maurice Berger, M.D. Ph.D.
Child psychiatrist
SWITZERLAND
Daniel Halpérin, M.D.
Pediatrician
SOUTH AFRICA
Prof. Reitze Rodseth, Ph.D.
University of Kwazulu-Natal
Janet Giddy, M.B.Ch.B., M.P.H.
Family physician and public-health expert
Allan Donkin, M.B.Ch.B.
Family physician
UNITED STATES
Clin. Prof. Stephen B. Levine, M.D.
Case Western Reserve University
Clin. Prof. William Malone, M.D.
Idaho College of Osteopathic Medicine
Director, Society for Evidence Based Gender Medicine
Prof. Patrick K. Hunter, M.D.
Florida State University
Pediatrician and bioethicist
Transgenderism has been highly politicized—on both sides. There are those who will justify any hormonal-replacement intervention for any young person who may have been identified as possibly having gender dysphoria. This is dangerous, as probably only a minority of those so identified truly qualify for this diagnosis. On the other hand, there are those who wouldn’t accept any hormonal intervention, regardless of the specifics of the individual patients.
Endocrinologists aren’t psychiatrists. We aren’t the ones who can identify gender-dysphoric individuals. The point isn’t to open the floodgates and offer an often-irreversible treatment to all people who may have issues with their sexuality, but to determine who would truly benefit from it.
Jesus L. Penabad, M.D.
Tarpon Springs, Fla.
[ Via: https://archive.today/IRShy ]

==
The gender lobotomists just got called out.
#Leor Sapir#Colin Wright#Endocrine Society#gender lobotomy#genderwang#gender ideology#queer theory#sex trait modification#ideological capture#medical malpractice#medical transition#medical scandal#gender affirming care#affirmation model#gender affirming#ideological corruption#religion is a mental illness
283 notes
·
View notes
Text
By: Anonymous
Published: Oct 16, 2023
When my first son claimed he was trans, I eagerly ‘affirmed’ him. When his three-year-old brother decided he wanted to be trans, too, I realized I’d made a terrible mistake.
I was a social-justice organizer and facilitator before social justice took over the progressive world. I was at the nascent movement’s forefront, introducing the concept of intersectionality to organizations and asking people to share their pronouns.
My friends and I felt like we were the cool kids, on the vanguard of the revolutionary wave that would change the world. We were going to achieve what people in that milieu call “collective liberation.”
Within this context, I came out as a lesbian and identified as queer. I also fell in love, entered a committed relationship, and gave birth to a son. Two years later, my spouse gave birth to our second son.
Having children and experiencing the love and devotion I felt toward them, was a game changer for me. I began to experience internal tensions. My thinking was split between what I felt instinctively as a mother; and what I “should” be feeling and doing as a white anti-racist social-justice parent.
Because I’d felt victimized by my parents’ rejection of my sexuality, I wanted to make sure to honor my own children’s “authentic” selves. In particular, I was primed to look for any clues that might suggest they could be transgender.
My spouse and I raised our sons with gender-neutral clothes, toys, and language. While we used he/him pronouns, and others called them boys, we did not call them boys, or even tell them that they were boys.
In our everyday reading of books or descriptions of people in our lives, we did not say “man” or “woman”; we said “people.” We thought we were doing the right thing, both for them and for the world.
Even when our first son was still young, he already struck us as different from other boys—being both extremely gifted and unusually sensitive. By age three or so, he started to orient more toward the females in his life than the males. “I like the mamas,” he would say.
We started to attribute some of this difference to the possibility that he was transgender. Instead of orienting him toward the reality of his biological sex by telling him he was a boy, we wanted him to tell us if he felt he was a boy or a girl. As true believers, we thought that we should “follow his lead” to determine his true identity.
At the same time, I was taking a deep dive into the field of attachment and child development. This made me understand that attachment is hierarchical; and that parents, not children, are meant to be in the lead. This obviously conflicted with my insistence on letting my child decide his gender. Sadly, it was the latter impulse that won the day.
At around age four, my son began to ask me if he was a boy or a girl. I told him he could choose. I didn’t use those words—I imagined that I was taking a more sophisticated approach. I told him, “When babies are born with a penis, they are called boys, and when babies are born with a vagina, they are called girls. But some babies who are born with a penis can be girls, and some babies born with a vagina can be boys. It all depends on what you feel deep inside.”
He continued to ask me what he was, and I continued to repeat these lines. I’d resolved my inner conflict by “leading” my son with this framework. Or so I told myself.
His question, and my response to it, would come back to haunt me. In fact, I remain haunted to this day. To the extent I was “leading” my son anywhere, it was down a path of lies—an on-ramp to psychological damage and irreversible medical interventions. All in the name of love, acceptance, and liberation.
About six months later, he told my spouse that he was a girl and wanted to be called “sister” and “she/her.” I received a text message about this at work. On the way home that night, I resolved to put all my own feelings away and support my transgender child. And that is what I did.
We told him he could be a girl. He jumped up and down on the bed, happily saying, “I’m a girl, I’m a girl!” We—not our son—initiated changing his name. We socially transitioned him and enforced this transition with his younger brother, who was then only two years old and could barely pronounce his older brother’s real name.
When I look back at this, it is almost too much to write about. How could a mother do this to her child? To her children?
Once we made this decision, we received resounding praise and affirmation from most of our peers. One of my friends, who’d also socially transitioned her young child, assured me that this was a healthy, neutral way to allow children to “explore” their gender identity before puberty, when decisions would have to be made about puberty blockers and hormones.
We sought out support groups for parents of transgender children, so that we could find out if we’d done the “right thing.” It hadn’t escaped my notice that our son hadn’t exhibited any signs of actual gender dysphoria. Was he actually transgender?
At these support groups, we were told, again, what good parents we were. We were also told that kids on the autism spectrum (which our son likely is) are gender savants who simply know they are transgender earlier than other kids.
At one of the support groups we attended, we were also told that transgender identity takes a few years to develop in children. The gender therapist running things told us that during this period, it’s important to protect the child’s transgender self-conception—which meant eliminating all contact with family or friends who didn’t support the idea that our son was a girl. I believed her.
Looking back, I now see her comments in a shockingly different light: this was part of an intentional process of concretizing transgender identity in children who are much too young to know themselves in any definitive way. (One set of parents attending the group had a child who was just three years old.) When identity is “affirmed” in this manner, children will grow up believing they are actually the opposite sex.
The therapist endorsed the same approach that many adolescents use on their parents, who are urged to write letters to grandparents, aunts, and uncles to announce the child’s transgender identity. In these letters, the conditions of continued social engagement are made clear: Recipients must use the new name and new pronouns, and embrace the new identity, or they will be denied contact with the child.
After about a year of social transition for our older son, our younger son, who was by now only three years old, began to say he was a girl, too. This came as a complete shock to us. None of the things that made our older son “different” applied to our younger son. He was more of a stereotypical boy and didn’t show the same affinity for the feminine side of things that his older brother did.
The urge for “sameness” is a primal attachment drive in many family members. We felt that our younger son’s assertion of being a girl likely reflected his desire to be like his older sibling, in order to feel connected to him.
His claim to be a girl became more insistent when both brothers went to school part-time, because their program included pronoun sharing. Why could the older sibling be a “she” when the younger sibling couldn’t? Our younger son became more insistent, and we became more distressed.
We made an appointment to see the gender therapist whom we’d met at the support group. We truly believed that she would be able to help us sort out who, if anyone, was actually transgender.
To our shock, the therapist immediately began referring to our younger son as “she,” stating that whatever pronouns a young child wants to use are the pronouns that must be used.
She patronizingly assured us that it might take us more time to adjust, since parents have a hard time with this sort of thing. She added that it was transphobic to believe there was anything wrong with our younger son wanting to be like his older transgender sibling.
When I pushed back and asserted that I wasn’t yet convinced our younger son was in fact transgender, she told me that if I failed to change his pronouns and honor his newly announced identity, he could develop an attachment disorder.
We were unconvinced. But, again, we wanted to do what was right for our son and for the world. We decided to tell him he could be a girl. And that night at dinner, we told him that we would call him “she/her.”
Right after dinner, I went to play an imaginary game with him, and I wanted to be affirming. So I put a big, warm smile on my face and said, “Hi, my girl!”
At this, my younger son stopped, looked at me, and said, “No, mama. Don’t call me that.” His reaction pierced me to my core. I didn’t turn back after that.
For the next two years, my partner and I dug deeper, agonized, and then continued digging again. Everything we thought we knew or believed that had led us to socially transition our older son began to unravel.
I continued to study the attachment-based developmental approach to parenting and learned more about autism and hypersensitivity. We decided not to socially transition our younger son. Not only was he not transgender, we now realized, but our older son probably wasn’t either.
He was just a highly sensitive, likely autistic boy who saw a girl identity as a form of psychic protection. It also provided him a way of attaching to me through sameness.
My spouse and I decided that since we’d been the ones who’d led him down this path, we were the ones who needed to lead him off of it.
A year ago, just before our older son’s eighth birthday, we did just that. And while the initial change was hard—incredibly hard—the strongest emotion exhibited by our son turned out to be relief.
In the days following my first conversation with him about going back to his birth name and pronouns, during which I told him that males cannot be females and that we were wrong to tell him he could choose to be a girl, he got very mad at me, then sad. Then, the next day, I felt my son rest. I felt him release a burden, an adult burden that he, as a child, was never meant to carry.
Since that time, we’ve all been healing. My son is now happy and thriving. We’ve watched him come to a deeper peace with himself as a boy.
Our younger son is also thriving. Once his older brother became his older brother again, he happily, and almost immediately, settled into his identity as a boy.
I feel like someone who’s escaped a cult—a cult whose belief system is supported by our mainstream culture, the Internet, and even the state.
I fear for the future—the future of sensitive, feminine, socially awkward boys. I fear what the world will tell them about who they are.
But no matter what the future holds, I will never ever stop fighting to protect my sons. I am no longer a true believer.
#gender ideology#queer theory#genderwang#gender cult#social transition#autism#social justice#critical social justice#affirmation model#gender affirming#gender affirmation#trans identity#gender identity#child psychology#religion is a mental illness
111 notes
·
View notes
Last Seen Blogs

amboom-blog
amboom

helluvaahotel042
Helluva a Hotel


lillithfallenangel
꧁𝐿𝑖𝑙𝑙𝑖𝑡ℎ꧂

lapipaylafuente
La pipa y la fuente