#but you work in healthcare scheduling and particularly in primary care you have to expect some reqs that are just unreasonable
Text
Materials Right Now: Proceedings Materials Tech 2022 Second Worldwide Conference On Materials And Technologies
Representative Dean Phillips introduced his run in opposition to Biden on October 26. Trump has made repealing the Affordable Care Act, better known as Obamacare, a key issue of the 2024 election. The problem of healthcare and drug coverage, including whether or not the United States should shift to a common healthcare system, and the COVID-19 pandemic is expected to play a key position within the 2024 presidential election. During the Israel–Hamas warfare, Biden announced "unequivocal" military help for Israel, and condemned the actions of Hamas and other Palestinian militants as terrorism. Kennedy condemned Hamas' attacks on Israeli civilians and declared help for help to Israel.
Delegates to the nominating conventions shall be chosen by voters in state-level caucuses and primary elections.
By April 2023, a big majority of Republican-controlled states had passed near-total bans on abortion, rendering it "largely illegal" all through much of the United States.
Liberals are probably to imagine that conservatives are threatening the nation with autocratic tendencies and their attempts to overturn the 2020 election.
Biden's support for Israel has significantly damaged Muslim assist for Democrats in polling.
Some Republican candidates and prospective candidates see training as a profitable campaign problem.
Ji et al. discovered that the k0 worth decreased by increasing the oxygen-containing teams on the basal plane of pyrolytic graphite electrodes oxidized for 12 h in air, and of multi-walled carbon nanotubes oxidized in air for greater than 1 week. Pumera et al. found that oxygen-containing teams play a serious position on edges-like sites on the walls of multiwalled carbon nanotubes, and have a good influence on the k0 worth for [Fe6]3-/4- redox couple. However, the kind and content material of the oxygenated functional teams aren't thought of of their dialogue. Anti-vaccine activist and environmental lawyer Robert F. Kennedy Jr. has drawn help amongst impartial and anti-establishment voters disillusioned with mainstream American politics, winning a plurality among independents in some polls. He has faced criticism for supporting numerous conspiracy theories, particularly on the John F. Kennedy assassination and COVID-19 vaccines. Left-wing activist and intellectual Cornel West announced a campaign as an impartial after initially saying a run as a People's Party and later a Green Party candidate.
The 2024 United States presidential election would be the 60th quadrennial presidential election, scheduled for Tuesday, November 5, 2024. Incumbent President Joe Biden, a member of the Democratic Party, is working for re-election. His predecessor Donald Trump, a member of the Republican Party, is working for re-election to a second, nonconsecutive term.
Successful candidates will be employed as PI and receive maximal assist from the university. The coming year shall be pivotal for these combating in opposition to the proliferation of such content material. Techniques to track and mitigate it content are still in early days of growth. Watermarks, similar to Google DeepMind’s SynthID, are nonetheless mostly voluntary and not completely foolproof.
Robert Kennedy, Jr. has acknowledged that he supports securing the border and the actions taken by states to safe it themselves within the absence of Federal motion to do so. This will be the first U.S. presidential election to happen after the reapportionment of votes in the United States Electoral College following the 2020 United States census. This apportionment of electoral faculty votes will stay solely by way of the 2028 election. Reapportionment might be performed once more after the 2030 United States census.
Structure Of Graphite Oxide Revisited
Here, you can uncover if there have been adjustments to account restoration options, applications and services that have been granted access to your account, whether you may have 2FA activated and what methods you might be utilizing to offer it and delicate Gmail settings. The latter can embrace reply-to addresses completely different from your account default, sent-from addresses which are additionally completely different and any addresses that have been blocked and so go straight to your spam folder. Blocking security alert addresses, for instance, would be a easy method to prolong unauthorized exercise going unnoticed.
If first article checks reveal deviations from contract necessities, the Contractor shall, on the location designated by the Government, make the required modifications or replace all objects produced underneath this contract at no change in the contract value. Davey Winder/GoogleScroll to the underside of your Gmail inbox and find a function called final account activity. This will immediately inform you of the time of the previous entry to Gmail and whether it's being accessed from a different location. However, you’ll need to click by way of this to open the complete exercise monitor to get the full access picture. This will then reveal all access dates and instances as well as the user’s IP tackle and the device or application being utilized by them.
youtube
The acceleration of this development has been credited with tipping the 2020 presidential election in favor of Democrat Joe Biden, because the incumbent Trump was historically unpopular within the suburbs for a Republican candidate, underperforming there considerably. Article Two of the United States Constitution states that for an individual to function president, the individual must be a natural-born citizen of the United States, be at least 35 years old, and have been a United States resident for a minimum of 14 years. The Twenty-second Amendment forbids any individual from being elected president greater than twice. Major party candidates search the nomination through a collection of major elections that select the delegates who select the candidate on the get together's national conference. Each celebration's national conference chooses a vice presidential operating mate to kind that celebration's ticket.
House; several states may even be holding gubernatorial and state legislative elections. Polling has shown that border safety and immigration are among the many high issues concerning potential voters within the 2024 presidential election. In 2023 and 2024, a surge of migrants getting into the country via the United States' border with Mexico occurred. In response to the influx of migrants, Republican controlled states corresponding to Texas and Florida have been busing migrants to main Democrat controlled sanctuary cities corresponding to New York and Chicago. The Biden administration has undertaken a policy of offering short-term protections to migrants from sure nations such as Venezuela, Ukraine, Nicaragua, Cuba and Haiti.
While it’s onerous to say how much these examples have influenced the outcomes of elections, their proliferation is a worrying trend. In an already inflamed and polarized political climate, this might have extreme penalties. In 2024, generative AI would possibly truly become helpful for the common, non-tech particular person, and we are going to see more folks tinkering with 1,000,000 little AI models. State-of-the-art AI fashions, such as GPT-4 and Gemini, are multimodal, which means they can process not only text but pictures and even videos. For instance, a real estate agent can upload text from previous listings, fine-tune a powerful mannequin to generate comparable text with just a click of a button, addContent movies and photographs of recent listings, and easily ask the personalized AI to generate a description of the property.
Prior to the final election, political events will select their nominees at nominating conventions. Delegates to the nominating conventions might be chosen by voters in state-level caucuses and first elections. In October 2023, anti-vaccine activist and environmental lawyer Robert F. Kennedy Jr. announced his run as an independent presidential candidate. By the following month, Kennedy's polling was at the highest levels for a candidate exterior the two major parties since Ross Perot in 1992.
Republicans in states across the country are defiantly pushing for the criminalization of abortion — of the process, of abortifacient medicine and of those who journey out of state to terminate pregnancy... Calculated by taking the difference of 100 percent and all other candidates combined. Former UN ambassador Nikki Haley has since gained ground and was in second place in New Hampshire, in polling averages compiled by RealClearPolitics, as of early November 2023.
Ultra-thin Freestanding Graphene Movies For Environment Friendly Thermal Insulation And Electromagnetic Interference Shielding
GO consists of graphene layers modified with oxygen functional teams such as hydroxyl and epoxy teams principally situated on the basal airplane, with smaller amounts of carboxyl ketone at the edges. These oxygen functional groups confer to GO flakes a great dispensability in polar solvents , biocompatibility and affinity for specific biomolecules , . They additionally provide chemical flexibility to GO which might, for instance, be used as cross-linker between a substrate and molecules of interest via π-π stacking, electrostatic interactions or chemical bonds , , . In sum, Trump posted on Truth Social that, what he believed to be, election fraud in the 2020 presidential election allows "for the termination of all rules, regulations, and articles, even these discovered within the Constitution." For that purpose, we rated this declare "Correct Attribution." Author Marianne Williamson announced her candidacy in February 2023, before Biden introduced his personal candidacy for re-election. Williamson had previously sought the Democratic presidential nomination in 2020.
The Government may waive the requirement for first article approval take a look at where provides identical or just like those called for in the schedule have been beforehand furnished by the offeror/contractor and have been accepted by the Government. Details associated to materials, instrumentation, and physicochemical characterization methods of the EGO are presented within the supporting data . "Americans agree that the 2024 election will be pivotal for democracy, but for various causes".
In this study, we use a platform based on the self-assembly of EGO sheets onto the surface of a GCE using a p-aminophenyl linker , for the systematic electrochemical characterization of the EGOs. Compared to different methods, the self-assembly methodology can reduce the re-stacking of EGO, and provides a greater management of the thickness and homogeneity of the EGO movies on the electrode substrate. This is as a result of the negatively charged EGO sheets are self-assembled on the positively charged electrode surface through the electrostatic interplay and π-π stacking between them , . The EGO/AP/GCE electrodes are electrochemically characterized by cyclic voltammetry in 1 mM [Fe6]3-/4- inner-sphere redox couple which could be very delicate to floor structure of carbon supplies .
A wide range of EGO materials with totally different quantities and kinds of oxygenated teams, structural defects, sheet sizes can in principle be obtained by this methodology , , , . However, only a few works report on the influence of the experimental parameters on the EGO structural defects, surface composition, number of layers, and on their electrochemical properties together with electron switch commonplace rate constant and electrochemical floor space . One example is the work of Ambrosi et al. the place the electrochemical properties of EGO obtained by electrochemically exfoliated graphite with 10 V and a pair of cm in three different electrolytes were investigated. The EGO flakes were dispersed in DMF and deposited on glassy carbon electrode by drop-casting methodology.
Temporary childcare measures, together with an expanded child tax credit as part of the American Rescue Plan, have been introduced as strategies designed to help the economic situation of oldsters, however these would expire before the 2024 election. Selection and peer-review beneath responsibility of the scientific committee of the “Material TECH 2022 ”. An important round-up of science information, opinion and evaluation, delivered to your inbox every weekday. To get hold of the most effective expertise, we recommend you employ a more updated browser .
In Situ Era Of Diazonium Cations In Natural Electrolyte For Electrochemical Modification Of Electrode Surface
"American decline isn't inevitable—it is a selection...I am working for president of the United States to steer our nice American comeback", DeSantis added. His campaign acknowledged to have raised $1 million within the first hour following the announcement of his candidacy. Speaking on Fox & Friends, he said that he would "destroy leftism" in the United States. At the top of July 2023, FiveThirtyEight's national polling average of the Republican primaries had Trump at 52 percent, and DeSantis at 15. While independent/third-party candidates typically do higher in polls than actual election performance, early polling suggests there could presumably be a powerful exhibiting for third-party candidates in 2024. Third-party candidates presently have the strongest exhibiting in polls since Ross Perot's high poll numbers in the Nineteen Nineties.
Donald Trump's 2024 marketing campaign has been criticized by the media for making increasingly violent and authoritarian statements, which some consider the Trump campaign is deliberately leaning into. If recent elections are anything to go by, AI-generated election disinformation and deepfakes are going to be a huge problem as a record number of people march to the polls in 2024. In Argentina, two presidential candidates created AI-generated pictures and videos of their opponents to attack them. In Slovakia, deepfakes of a liberal pro-European get together chief threatening to raise the value of beer and making jokes about child pornography spread like wildfire in the course of the country’s elections.
Ensure you do this no less than once every 24 months and your account, as well as your content, will abe secure from deletion. Use the Google account recovery process which requires a recovery e mail or telephone quantity. https://asc247.com.au/ 'll get a verification code sent by email or SMS, and then when you attempt to log in with an incorrect password you may get the chance to reset the password via the forgotten password route. 5, the voltage of discharge peak present for N-GC is higher than that for Xingcheng graphite (easy to insert Li-ion for N-GC), while the voltage of charge peak current for N-GC is lower than that for Xingcheng graphite (easy to deinsert Li-ion for N-GC). The developed pore of carbon materials is very conducive to the advance of capacitive lithium storage capability [47–51].
#Cleaning Services#Office Periodic Cleaning Services#Office Consumables#Commercial Cleaning Services#School Carpet Cleaning Solutions#cleaning contract#sanitary bin service brisbane
1 note
·
View note
Text
Video Chat by Phone with Tele Doc Psychiatrist: Your Top-Rated Telehealth Provider
In today's fast-paced world, accessing quality healthcare services has become more convenient than ever. One area that has seen tremendous growth and innovation is telehealth, allowing individuals to connect with healthcare professionals from the comfort of their own homes. Among the many specialties in telehealth, psychiatry is one that has greatly benefited from this technology. With the rise of Tele Doc Psychiatrists, individuals can now receive Top Rated Telehealth Provider mental health care via video chat on their phones, eliminating the barriers of time, distance, and stigma.

The Telehealth Revolution
Telehealth, also known as telemedicine, has revolutionized the way healthcare services are delivered. This innovative approach allows patients to connect with healthcare professionals, including psychiatrists, through video chat on their smartphones. Telehealth has become particularly crucial in the field of psychiatry, where mental health support is essential, and timely access to care is paramount.
Why Choose Tele Doc Psychiatrists?
Convenience: The primary advantage of choosing a Tele Doc Psychiatrist is convenience. You can schedule and attend appointments without the hassle of commuting or waiting in a crowded waiting room. Simply use your phone to connect with your psychiatrist from the comfort of your own home.
Accessibility: Tele Doc Psychiatrists are accessible to individuals living in remote areas or those with mobility issues. This accessibility ensures that mental health support is available to anyone, regardless of their location.
Reduced Stigma: Telehealth services can help reduce the stigma associated with mental health care. Some individuals may feel uncomfortable visiting a physical clinic due to concerns about privacy or judgment. Video chat allows you to receive the care you need discreetly.
Top-Rated Providers: Telehealth platforms often feature a wide network of top-rated psychiatrists. You can choose from a variety of professionals to find the right fit for your needs, all while benefiting from their expertise and experience.
Flexible Scheduling: Telehealth appointments offer flexibility in scheduling. You can find appointment times that work for you, including evenings and weekends, making it easier to fit mental health care into your busy life.
Consistent Care: Tele Doc Psychiatrists can provide ongoing care and support for chronic mental health conditions. Regular check-ins through video chat ensure that you receive continuous and consistent care.
The Telehealth Experience
When you choose a Tele Doc Psychiatrist, you can expect a high-quality healthcare experience. During your video chat appointments, you'll have the opportunity to discuss your concerns, symptoms, and treatment options just as you would during an in-person visit. Your psychiatrist can provide diagnoses, prescribe medications if necessary, and offer therapy or counseling services through the secure and confidential telehealth platform.
Is Telehealth Right for You?
Telehealth, including video chat appointments with Tele Doc Psychiatrists, is suitable for a wide range of mental health concerns, including anxiety, depression, bipolar disorder, ADHD, and more. It's important to consult with a healthcare provider to determine if telehealth is the right option for your specific needs.
In conclusion, Video Chat By Phone With Tele Doc Psychiatrist through a top-rated telehealth provider offers a convenient, accessible, and effective way to receive mental health care. This innovative approach to psychiatry allows individuals to prioritize their mental well-being without the constraints of traditional healthcare delivery. Embrace the future of mental health care by exploring the benefits of Tele Doc Psychiatrists and telehealth services today. Your mental health is worth it.
0 notes
Text
Finding the Best Pancreatic Cancer Surgeon: A Guide to Exceptional Care
Pancreatic cancer is a complex and aggressive disease that requires specialized care from highly skilled medical professionals. When facing a diagnosis of pancreatic cancer, finding the best surgeon is crucial for achieving the best possible outcome. In this article, we will discuss the qualities that define a top pancreatic cancer surgeon and provide guidance on how to identify and choose the best surgeon for your needs.
Qualities of a Top Pancreatic Cancer Surgeon:
Expertise and Experience:
The best pancreatic cancer surgeons possess extensive expertise and experience in the field of pancreatic surgery. They have undergone rigorous training, completed fellowships or specialized programs, and have performed a significant number of pancreatic cancer surgeries. Look for surgeons who are board-certified and affiliated with reputable medical institutions known for their excellence in pancreatic cancer treatment.
Specialization in Pancreatic Surgery:
Pancreatic surgery is a highly specialized field within surgical oncology. Look for surgeons who have dedicated their practice to pancreatic cancer and have a specific focus on pancreatic surgical procedures. These surgeons will have a deep understanding of the complexities associated with pancreatic cancer and will be up-to-date with the latest advancements in surgical techniques.
Team Approach:
Pancreatic cancer treatment requires a multidisciplinary approach involving various healthcare professionals. A top pancreatic cancer surgeon works closely with a multidisciplinary team comprising medical oncologists, radiation oncologists, gastroenterologists, radiologists, and other specialists. They collaborate to create an individualized treatment plan tailored to each patient's unique needs.
Track Record of Successful Outcomes:
One of the most important factors in evaluating a pancreatic cancer surgeon is their track record of successful outcomes. Look for surgeons who have consistently achieved positive results in terms of complete tumor removal, low complication rates, and improved patient survival rates. Reliable sources for this information include reputable medical databases, patient testimonials, and peer-reviewed publications.
Patient-Centered Care:
A top pancreatic cancer surgeon prioritizes patient-centered care. They have excellent communication skills, taking the time to listen to their patients' concerns and addressing them with compassion and empathy. They provide clear explanations of the treatment options, potential risks, and expected outcomes, empowering patients to make informed decisions about their care.
Finding the Best Pancreatic Cancer Surgeon:
Seek Recommendations:
Start by seeking recommendations from your primary care physician, oncologist, or other healthcare professionals. They can provide valuable insights and referrals to surgeons with exceptional reputations in pancreatic cancer surgery.
Research Credentials and Experience:
Conduct thorough research on the recommended surgeons. Review their credentials, including education, training, certifications, and affiliations. Look for information on their experience, particularly the number of pancreatic cancer surgeries they have performed and their success rates.
Evaluate Hospital Affiliations:
Consider surgeons who are affiliated with renowned medical institutions known for their expertise in pancreatic cancer treatment. Leading cancer centers often have dedicated pancreatic cancer programs that bring together experts from various disciplines to provide comprehensive care.
Consultation and Second Opinions:
Schedule consultations with potential surgeons to discuss your case and treatment options. Seek second opinions to gain different perspectives on your diagnosis and treatment plan. This process will help you assess the surgeon's expertise, communication style, and compatibility with your needs.
Consider Clinical Trials and Innovations:
Top pancreatic cancer surgeons are often involved in cutting-edge research, clinical trials, and innovative treatments. Inquire about their participation in such programs, as it reflects their commitment to staying at the forefront of advancements in pancreatic cancer care.
0 notes
Photo

I recently received two very important and interrelated questions:
Anon 1:
My psychologist don’t believe my mental illness, I feel like I couldn’t take it anymore, I want to choke myself until I passed out.
Anon 2:
Hello, I’ve been seeing a psychologist for a few months now. I’ve had problems with emotion dysregulation and abandonment issues for almost my entire life, but recently I’ve started reading about BPD and looking at the symptoms, I can say that I’ve never related to anything else more in my life. I’m not 18 yet, but is it still worth bringing it up to my psychologist? Ugh, sometimes I feel like I’m just faking it for attention.
I get questions like this frequently and have addressed them many times on this blog. However, considering the fact that this is clearly a persistent and pressing issue for many people, I’ve decided to do the following:
I’ll give a deep-dive answer to both these questions that is hopefully informative and helpful.
I’m working on a new resource that offers guidance and solutions to the frequent, common problems of BPD.
Before you read on any further, I want to emphasize that dying is absolutely out of the question. Not an option. No dying allowed on my blog. Life is short. You don’t have forever. So please don’t cut your precious time off prematurely.
But this only points to the fact that this incredibly overwhelming impulse is an (over)reaction to the desperate, stressful, and toxic situation that is reinforced by psychologists, psychiatrists, and therapists. There’s a problem where there should be a solution, blame and shame where there should be help and support.
The misbeliefs that Borderlines have about themselves are prevalent and persistent, both out of the sheer ignorance as well as the viciously cruel design of the psychiatric community. It’s time to start changing the way we think about mental health and mental help.
In the plainest possible terms, it’s really hard to find a good mental health worker. The only way to actually do it is through trial and error. Misdiagnosis. Informing yourself and building your own networks when you get referrals from doctors. Going out of town because no one in your area is accepting new patients, then having to pay all the gas and parking bills yourself.
This is all assuming that you can afford a decent mental health worker, of course.
People caught up in the healthcare system, especially in North America, quickly find out how uncaring and ineffective it really is. Why? Because the way it is set up is to run exclusively for profit.
Healthy people are not profitable.
For example, this is reflected in the mentality that pills are given to patients as the very first option for “care.” Psychiatrists in particular receive kickbacks from leading pharmaceutical companies depending on the kinds of pills they prescribe. But pills are not a viable long term solution, in my opinion, because they do not teach life skills and healthy recovery.
So, it is no surprise that a mental health worker who is concerned about profit over long term care will push pills as the first (and often primary) option.
Another example is that there are tiers of help, according to how much you can pay a certain type of mental health worker.
Psychiatrists are trained medical doctors, which means that they can prescribe medications, and often exclusively develop a medication management plan as the only course of treatment. Typically, you can expect to pay up to $500 for an initial consultation, and at least $100 per hour for ongoing services.
Psychologists focus extensively on psychotherapy (i.e. talking through experiences) and treating emotional and mental suffering in patients with behavioral intervention. Psychologists can also be exclusively academic researchers. They are qualified and trained to critically assess a person’s mental state in order to determine the most effective treatment plan, which often includes total lifestyle changes.
Both of these are psychotherapists, in that they use a form of therapy (medication, behavioural intervention) to treat your mental health (the psyche). Hence the term psychotherapy. Given these definitions, personality disordered people should lean toward seeing psychologists.
In North America, some psychologists can charge as much as $200 or more per session, but most will charge around $75-$150 a session. Many also work with a sliding scale fee schedule, which means their fee will depend on your income level (a crucial point for young people and young professionals).
University/college mental health workers (including counselors) are always understaffed and over worked. They are paid from a portion of tuition, so technically their services are free. But their “walk in services” are often the first line of defense, but their sessions are limited to 15-30 mins. There is very little accountability both for the worker and the patient; you’re seen as just another number in a very long, long line. When it’s determined that you’re “well enough”, you will be kicked out to make room for the rest of the people who are waiting. This is the lowest tier of care and it also happens to be the one that is accessed the most often.
Whoever the mental health worker is, then, they are working within a profit driven system. On the one hand, they need problems in order to generate profit. On the other hand, this promotes the idea that mentally ill people (particularly the most “difficult” personality disordered people) should be reduced to nothing more than a problem.
As if it isn’t incredibly dehumanizing and disgusting to reduce us to nothing more than a problem to be solved, at a significant cost.
Then on top of that, we have limited means to complain if we are abused by the system and all the people in it; we cannot hold mental health workers accountable for misdiagnosis, unproven treatments and pills, sudden appointment cancellations, and lack of follow up because we are dismissed as just being “too difficult” and “too crazy” to be listened to.
I was doing some consulting work for the largest mental health organization in my region. They were under pressure to have their services evaluated. They were by no means underfunded or understaffed; they had hundreds of psychologists and psychiatrists. The facility was modern, clean, environmentally friendly. They treated even the most “severe” patients, including Borderlines and Narcissists.
Yet they had no complaint process or means for mentally ill people to provide feedback. Why? I was told it was because the feedback that these people could potentially provide could never be trusted, due to the fact that it’s coming from an unstable mind.
I suggested that resources need to be created with mentally ill people in mind, and that they should be written in language that each person, given their mental illness, can easily understand and implement. I was told the pros had never even considered this idea before.
I was told that people with BPD and NPD in particular were just “too difficult.” They were drug addicts. They were irresponsible. They were violent. They were prone to suicide. One client had killed themselves recently, and when the outraged family demanded accountability, they had no course of action because there was no framework put in place by the organization. The mental health worker responsible for care was not held accountable because they had washed their hands of that client. They were already “too difficult” and suicidal, so their death came as no surprise.
Mentally ill people are not taking responsibility, I was told, because they are lazy and unwilling to work for recovery. Why? They supposedly like their mental illness. And these mental health workers apparently work oh so hard, but it is useless because their clients cannot be cured. The topic of E-health was touched on as a means to counter the fact that a lot of mentally ill people are too intimidated or too ill to actually come in for a session. But this organization did not want to implement even monitored Skype calls because “bringing the care to the people who need it most” was too complicated and they didn’t have any accountability measures in place. E-health is an emerging field, and as such, I was told that it is too risky to try this suggested approach.
Sitting there and listening to all this made me sick to my stomach.
I recall a tumblr post along these lines:
“if you want us to see a doctor so bad does that mean you’ll pay for our doctors appointment, pay for all our sessions, get rid of our fear of doctors, shorten the absurd amount of time we have to wait to get appointments, take away the intense stigma professionals have against people with certain mental disorders, transport us to our sessions, remove us from abusive environments that prevent us from booking appointments, make sure that professional diagnosis is always 100% right every time, and remove all the abusive psychiatrists in the system??? (x)
Essentially, the underlying message that is given to mentally ill people on behalf of the health care system and its workers is that no one gives a fuck about us.
Yet somehow, we are still expected to invest tremendous amounts of money, time, and energy to get better- because despite reaching out for help from professionals who we expect will competently do their job with our well being in mind, the entire burden of being mentally well still falls entirely on us.
And we’re supposed to be the crazy ones?
The Validity of Self-Diagnosis:
Taking all this into consideration, I think that self-diagnosis is valid.
As personality disordered people, when we are faced with incompetent mental health workers whose professionalism is questionable at best and life threatening at worst; when there is such prevalent stigma against personality disordered people out there; when we cannot afford care; when the quality of that care is poor; and when we’re so scared and confused that we turn to finding information on our own and then find it accurately applies to our life-
Why wouldn’t we frame our own thoughts, feelings, and lived experiences (for free!) within a diagnostic framework that matches our internal processes?
It’s true that not everyone has a psychology degree. It’s true that the DSM is a flawed diagnostic manual (something I extensively critique in my own work Between The Lines: Comparing BPD + NPD and suggest five keys ways it can be improved). It’s true that there’s a chance for misdiagnosis.
But that chance is still 50/50, because despite the “professionalism” of mental health workers, they are also just as likely to misdiagnose personality disordered people (most notably, with anxiety/depression/bipolar) than they are to accurately “prove” that we are accurately mentally ill.
It’s really no wonder that people like Anon 2 feel that they are “just faking” their mental illness for “for attention.”
Dear Anon 2, you’re not “just faking it for attention.” Your thoughts and feelings about your own mental health are real and valid. If you relate so strongly with the symptoms of BPD, then that demonstrates your admirable level of self-awareness and willingness to recover! I talk about situations just like yours here and here.
Please don’t let people invalidate you out of their own sheer ignorance, arrogance, cruelty, and lack of compassion.
The “expertise” of Professional Diagnosis:
People like Anon 1 have been so deeply invalidated and dismissed by their mental health worker that they feel suicidal.
Please take a moment to let that sink in.
All mental health care workers follow the “medical model.” That is to say, you are either “sane” or “insane.” As a result, diagnostic criteria are developed with the assumption that there is only one “normal,” “right” and “healthy” way to live. Everything else is just pathologized and labelled as a disorder (especially in North American society, which has a disturbing propensity for black and white thinking as well as pathologizing emotions)
In contrast, Neurodiversity itself “ is the infinite variation of neurocognitive functioning within our specifies and it is a biological fact.”
Building off of this, the neurodiversity paradigm suggests that the diversity in our ways of thinking and feeling makes us stronger as a species, as communities, and as people. The neurodiversity paradigm is a specific perspective on neurodiversity – a perspective or approach that boils down to these fundamental principles:
1) Neurodiversity is a natural and valuable form of human diversity.
2) The idea that there is one “normal” or “healthy” type of brain or mind, or one “right” style of neurocognitive functioning, is a culturally constructed fiction, no more valid (and no more conducive to a healthy society or to the overall well-being of humanity) than the idea that there is one “normal” or “right” ethnicity, gender, or culture.
3) The social dynamics that manifest in regard to neurodiversity are similar to the social dynamics that manifest in regard to other forms of human diversity (e.g., diversity of ethnicity, gender, or culture). These dynamics include the dynamics of social power inequalities, and also the dynamics by which diversity, when embraced, acts as a source of creative potential.
This is where the terms neurodivergent and neurotypical come from:
Neurodivergent, sometimes abbreviated as ND, means having a brain that functions in ways that diverge significantly from the dominant societal standards of “normal.”
Neurodivergent is quite a broad term. Neurodivergence (the state of being neurodivergent) can be largely or entirely genetic and innate, or it can be largely or entirely produced by brain-altering experience, or some combination of the two (autism and dyslexia are examples of innate forms of neurodivergence, while alterations in brain functioning caused by such things as trauma, long-term meditation practice, or heavy usage of psychedelic drugs are examples of forms of neurodivergence produced through experience).
A person whose neurocognitive functioning diverges from dominant societal norms in multiple ways – for instance, a person who is Autistic, dyslexic, and epileptic – can be described as multiply neurodivergent.
Some forms of innate or largely innate neurodivergence, like autism, are intrinsic and pervasive factors in an individual’s psyche, personality, and fundamental way of relating to the world. The neurodiversity paradigm rejects the pathologizing of such forms of neurodivergence, and the Neurodiversity Movement opposes attempts to get rid of them.
Other forms of neurodivergence, like epilepsy or the effects of traumatic brain injuries, could be removed from an individual without erasing fundamental aspects of the individual’s selfhood, and in many cases the individual would be happy to be rid of such forms of neurodivergence. The neurodiversity paradigm does not reject the pathologizing of these forms of neurodivergence, and the Neurodiversity Movement does not object to consensual attempts to cure them (but still most definitely objects to discrimination against people who have them).
Thus, neurodivergence is not intrinsically positive or negative, desirable or undesirable – it all depends on what sort of neurodivergence one is talking about.
Neurotypical, often abbreviated as NT, means having a style of neurocognitive functioning that falls within the dominant societal standards of “normal.”Neurotypical can be used as either an adjective (“He’s neurotypical”) or a noun (“He’s a neurotypical”).
Neurotypical is the opposite of neurodivergent. Neurotypicality is the condition from which neurodivergent people diverge. Neurotypical bears the same sort of relationship to neurodivergent that straight bears to queer.
Hence, neurodivergence is a very real and very valid approach to mental health, especially when it comes to personality disordered people. It is supported and used by some credited therapists as well, such as the website Eggshell Therapy.
Despite this reality, mental health workers generally remain unwilling to acknowledge it. This is highly unprofessional. A competent, knowledgeable mental health care worker should be willing to consider all possible perspectives when it comes to the way a human mind works. But as we’ve established, most mental health care workers are far from professional.
They rigidly cling to the medical model because it justifies the existence of their particular field of study and somehow automatically qualifies them to (mis)diagnose people, all while being paid very well for it. Dismissing self-diagnosis and neurodiversity invalidates mentally ill people; increases the risk of misdiagnosis; blocks the development of a meaningful and practical treatment plan; and obviously makes for a very strained working relationship.
Talking To Mental Health Workers About Your BPD:
Before you start you first assessment or initial session with a mental health worker (and even if you make it past the very first one), it’s a good idea to ask them what they think their job really is. Literally. Ask them for a job description, in their own words, about their work and how they view their client relationship.
Chances are, they’ll spew something along the lines of:
“My job is to help you. But you have to put in the work yourself.”
We’re already off to a bad start here: being condescendingly reminded that you have to actually make the right choices for yourself and learn how to live in a healthy way is a moot point. If you are coming in to see a psychotherapist, it is very probable that you have already put in most of the work (including self-diagnosis or at the very least, prepared points and questions) but that you are expecting a professional to competently and compassionately help you have the capacity to implement positive changes for your mental health.
My naïve understanding of the work that mental health workers do is that, precisely because of their “expertise”, they would be able to make up for the skills and knowledge that I could not do on my own. Instead, the concept of “self-help” keeps getting shoved down the throats of people who are tremendously vulnerable due to their mental illness. If you wanted to rely solely on self-help, it is fair to presume that you would not be seeking professional help.
Of course, “help” in their eyes is usually supplying pills (especially if the mental health worker is a psychiatrist). Even if your body reacts badly to it. The rest is, of course, up to you. Just help yourself!
On top of all this, mental health workers are operating under the assumption that they will “cure” you of your mental illness, even though they should know that this is impossible. In other words, they aren’t there to help you learn to live with your mental illness in a healthy way (because that’s not profitable). They’re here to tell you what you should do about how “wrong” you are according to the medical model, while you pay them to help yourself.
And if you really want to reaffirm that point, ask them next what they think of the concept of neurodivergence and how it applies to you (you can even use Eggshell Therapy as a reference point). Their answer will likely be dismissive and re-emphasize that if you do not follow their specific treatment plan, then your condition will just worsen-maybe to the point that they cannot even “help” you anymore.
Having said all this, I don’t want to paint all mental health workers with the same bush. There are brilliant young professionals and aspiring mental health workers out there now who are working their asses off to make mental health better and more accessible for all. But I’m still talking about how the health care system is right here and right now. Good mental health can’t wait.
It’s also important to keep in mind that personality disordered people can cross the line as well: resenting authority and stubbornly refusing to implement a mutually agreed upon treatment plan; acting out and raging; manipulating mental health workers; failing to show up for appointments all together; lying and smearing; threatening; being “offended” by deep, probing discussions about their own mental health; and dropping out of care without a valid reason after only one or two sessions.
There are evidently massive issues coming from both sides. The key takeaway is that bringing up mental health to your psychotherapist cannot possibly thrive in a climate of intimidation, confusion, and invalidation.
When you discuss your mental illness, it is important to draw from facts, your own lived experiences, seek clarification about the DSM criteria, and have plenty of examples how your daily behaviour fits into this framework. What prompted you to relate to this criteria so strongly, and why is it worth considering?
It’s always important to be as polite and respectful as possible. That goes both ways. And although it feels like you’re going through the wringer, if one mental health worker doesn’t work out, you are not chained to that situation. You are free to leave and seek out the services of someone else who is, in your opinion, more qualified to help you. This does take a lot of time and effort, with plenty of mistakes thrown in during the meantime.
But you are not alone.
Start building support networks: family, friends, teachers, social workers, colleagues…anyone who is willing and able to help you. Good mental health is not something that you should feel like you have to achieve on your own. You should be supported and cared for.
Hopefully, mental health care will improve drastically within our lifetime. I want us to keep in mind that we are striving for our own recovery in a kind way. That we can set good examples of how important it is to make sure no one gets left behind.
Above all, despite these systemic obstacles, we do need to talk about our mental health because that’s the only way anyone will ever listen to us.
#q + a#anon#cluster b#bpd#borderline personality disorder#actuallybpd#actuallyborderline#mental health#mental illness#psychology#recovery#resource#textsfromtheborderline
40 notes
·
View notes
Link
Overwhelmed by your pick of dentists? Want to make sure you know how to find a good dentist? I’m confident you will have the tools you need to choose the perfect dentist’s office by the end of this article.
We’ll talk about what you need to know before selecting a new dentist, ways to find a great dentist, the right kind of questions to ask, and even how to spot a bad dentist.
Whether you’re looking because you’re in a new city, your employer switched dental insurance plans, your dentist is retiring, or you’ve just waited a really long time for a dental visit…No need to worry. There are many simple, straightforward ways to choose a dentist who’s right for you and your family.
Disclosure:
Ask the Dentist is supported by readers. If you use one of the links below and buy something, Ask the Dentist makes a little bit of money at no additional cost to you. I rigorously research, test, and use thousands of products every year, but recommend only a small fraction of these. I only promote products that I truly feel will be valuable to you in improving your oral health.
5 Factors to Consider Before Choosing a Dentist
How can you find a good local dentist? The best approach is to take it in stages.
Start by creating a short list of offices to check, then prepare to gather information. Before you know it, you’ll begin a new relationship with a great dentist that can last for years.
So, how do you begin making that list? Let’s look at five important factors in narrowing down your list of potential new dentists.
Factor #1: Is this provider in your dental insurance network?
US readers: dental insurance, particularly for preventative dental care (such as cleanings), may be a factor in choosing a dentist. Since it doesn’t work the same way as medical health insurance, I’ve outlined a few ways to understand working with a new dental practice below based on your insurance status.
If you’re unsure of the answer to this question, your healthcare provider should have a list of participating local dentists. This can typically be found on your health insurer’s website or through your employer (HR is a good place to start). The list can serve as a starting point in the search for the perfect dentist for you and your loved ones.
No dental insurance? No problem! Check out this article on how to keep up with dental visits sans dental insurance. (It’s not as hard as you might think.)
Here are a couple of great questions I’ve been asked on the topic of finding a dentist in your insurance network:
What if I’m satisfied with my current dentist, but they’re not in my network?
Keep going to the dentist you love!
To understand why this is probably the best choice, it’s important to know that dental prices are not standardized like medical charges.
In-network providers sign a contract in which they agree to be paid less than they’d hope to in exchange for being included in the network. The fee isn’t massive, and it’s worth it for many providers. However, if you’re out-of-network, you can technically charge anything you want.
Here are the two options I would recommend, in this order:
Show them your new dental insurance plan to find out if they’re willing to accept whatever the insurance company is willing to pay, then write off the rest. The downside to this is that you could eat up the cap on your dental insurance benefits for the year, which isn’t great if you have major work needed.
Ask for an “in-network fee schedule.” That schedule is set up to normalize every dental billing code and how much they agree to make from every insurance company for those codes. Most offices are willing to accept this, and it means you’ll pay similar prices with your existing dentist as you would by switching to an in-network provider.
Either way, the dental office will still file the claim for you. I suggest setting up an agreement for one of the above options before your appointment, so you understand what you will (and won’t) be required to pay.
What if I want to find a functional dentist, but don’t see one in my list of participating providers?
If your insurance doesn’t cover your ideal functional dentist, you may still be able to find a dentist with similar ideals.
Even if a dentist isn’t classified as a “functional” dentist or registered with that kind of academy of dentistry, dentists should all be familiar with the way diet influences dental health as well as the mouth-body connection. By asking questions about these issues up front, you may be surprised to find a dentist who takes a more functional approach than you first expect. (I discuss this in more detail below.)
Most offices are happy to listen to concerns, answer questions and have you come in for a first-time consult and tour of their office. And if they’re not, think of it as an easy cross off your list!
Plus, refer to the bullets above—even an out-of-network dentist is able to bill your insurance and may be willing to work with you on fee schedules.
Factor #2: Should you choose a dentist who’s a member of the ADA?
Many insurance plans and other resources (websites, etc.) will recommend you only see a dentist approved or registered with the American Dental Association (ADA). But there are other options out there to find a high-quality dentist.
For instance, I am a member of the American Academy of Dental Sleep Medicine (AADSM), among others. (See my bio with the full list here.) I am not an ADA-registered dentist, though—I believe their recommendations on things such as fluoride and amalgam fillings aren’t evidence-based.
The dental professionals in the AADSM, and other similar organizations, are fully qualified Doctors of Dentistry. This association focuses much attention, research and training in the area of dental sleep medicine, including sleeping disorders and dental appliances that can be utilized to treat and reverse sleep disorders.
If you’re more comfortable with an ADA-registered dentist, that’s completely okay, too. Other organizations that a good dentist might belong to include:
American Academy of Dental Sleep Medicine (AADSM)
Academy of General Dentistry (Chicago, IL)
American Academy for Oral Systemic Health (AAOSH)
Keep in mind: All of these academies are “pay-to-play.” A dentist selects the ones that line up best with his or her approach to dentistry, but any board-certified dentist can pay for membership. As a member of any academy of dentistry, each dentist commits to that academy’s code of conduct and treatment standards, but they aren’t actively regulated by the association or academy. They do, however, have to keep up with that organization’s continuing education.
More important than the academies they belong to, your dentist should be board-certified and have a current registration with their state’s dental board.
So, should you choose a dentist who’s a member of the ADA? Not necessarily. If you know you struggle with bruxism or sleep apnea, it might make a good idea to partner with a dentist from one of the dental sleep medicine academies. If you’re more concerned with the impact your dental problems might be having on your overall health, an AAOSH dentist may be a better fit.
Don’t live in the US? Organizations like the British Dental Association, Canadian Dental Association, and Australian Dental Association may work for your needs.
Factor #3: Are you looking for a functional dentist?
I practice and promote functional dentistry. In short, this approach to dental care aims to solve problems at their root (no pun intended!) and treat the whole person, understanding that dental health is intrinsically linked to overall health.
More than just regular checkups, cleanings, fillings, crowns, and extractions, the functional dentist will educate you on how best to care for your teeth between regular visits. They will discuss the importance of diet beyond cutting out sugary drinks and candies. You may be prescribed dietary changes or less “mainstream” interventions for your dental health issues.
If that’s not what you’re looking for, that’s okay. Not everyone is interested in functional dentistry.
But if you do want to restrict your search that way, here are links to a few databases that might help to form a list of potential new dentists:
Holistic Dentistry
Campaign for Mercury-Free Dentistry
International Academy for Biologic Dentistry and Medicine (IABDM)
Huggins Applied Dentistry (this requires an application for the organization to connect you with an appropriate dentist)
Mercury-Safe Dentist Directory
Factor #4: What type of dental work are you looking for?
This is paramount to your final decision of which dentist to choose. The answer for how to find a good dentist is tied to what you feel are your greatest dental needs.
Do you want mainly regular checkups and cleanings? The field is wide open. Look for an office where you are comfortable with the dentist and staff, in a friendly but professional environment.
Have questions about sleep habits, apnea, or teeth grinding (bruxism), etc.? The sleep medicine dentist is likely the best choice for you, so you’ll want to search specifically within sleep dentistry organizations.
Are you looking for cosmetic work or other aesthetic dental treatments? In these cases, search for cosmetic dentists with plenty of reviews and before/after evidence for their cosmetic work.
Is your primary focus on your children’s dental care? Pediatric dentists go through the same rigorous education as any other dentist, but their offices are tailored to the young ones in our lives. Be sure to take your child/children with you when looking for the right office. Their first impression will be your most valuable form of discernment! (Here’s more on how to pick a great dentist specifically for your kiddo.)
Have you had a history of frequent cavities or more extensive dental procedures, such as dental surgeries? There are many dentists who share a practice with a specialist who performs root canals and other more extensive oral procedures. They may also have a great referral program with a local endodontist.
There are many other specialist for oral and dental needs, and unlike medical insurance, dental insurance typically doesn’t require a referral to cover these visits. Here are a few specialists you might consider seeing instead of a general dentist for your particular concerns:
Orthodontists deal specifically with treatment of misaligned teeth.
Periodontists specialize in dental treatment and prevention of gum-related diseases. If you have advanced gum disease, it’s a good idea to find a periodontist to partner with for treatment.
Prosthodontists restore and/or replace broken or missing teeth.
Endodontists perform root canals and monitor the healing process for about two years. However, your general/family dentist will be responsible for the accompanying dental crown, so it’s a good idea to work with both dentist and endodontist for a root canal treatment.
Oral/Maxillofacial Surgeons specialize in deep sedation surgeries (beyond laughing gas, etc.) for complex procedures like irregular tooth extractions, cleft palate surgery, or surgery to correct the jaw.
Factor #5: Does the dentist offer a translator?
Many folks speak great conversational second languages but may not be as comfortable or familiar with medical terminology, or know how to have an informed discussion about in-depth treatment plans, etc..
If you live in an area where your first learned language is uncommon, ask the offices you research if they have a translator that speaks your primary language.
What if one is not available, but you like the dentist office for other reasons? I would recommend taking a friend or family member with you who can easily translate, especially if you feel the least bit anxious about your visit or discussions of more extensive medical information.
7 Ways to Find a Good Dentist
I’m often asked: How do I find the best dentist in my area? How do I choose a new dentist?
Once you’ve considered the factors above, you’re ready to narrow down the exact dentist who’s right for you. Here are the best ways to find a good dentist you and your family will love.
1. Ask People You Trust
Ask people you know and trust, like family, close friends, and co-workers. Do they have a happy, bright smile? Find out who keeps it that way! As soon as one of them begins to rave about their dentist, get that name and number.
The best advice I can give about how to find a good dentist is this:
Who do you know who’s had extensive work done beyond standard cleanings or whitening? Find the person you know that raves about a dentist after considerable work, and you’ll be on the right track.
2. Get a Referral from a Physician or Pharmacist
Ask your family doctor or your local pharmacist. It’s a safe bet that these medical professionals have vetted out the dentists they use. These other medical providers probably get feedback on these dentists, so many times, you’ll get a great idea of the best dentists in your area using this method.
3. Search the Database of Your Chosen Dental Society
Compare practices from different associations such as the AADSM, ADA, AGD, etc. Here are links to dentist searches at the major associations listed above:
Find an AADSM Dentist
Find an AGD Dentist
Find an AAOSH Health Professional
American Dental Association: Find a Dentist
British Dental Association: Find a Member Practice
Canadian Dental Association: Contact Your Provincial Dental Association
Australian Dental Association Find a Dentist
4. Review Your Dental Insurance Network
Although dental insurance doesn’t necessarily need to play a part in this decision like medical insurance might, this is still one good way to find a good dentist.
Review the list of general dentists your insurance company provides who participate in your plan. Then, consider the factors I listed in the first section to figure out if one of them is right for you.
5. Google It (Or Use a Dental Provider Review Site)
It sounds almost too simple, but reading patient recommendations will answer many questions you have, and help add to, or eliminate some offices from your list. You can even start by searching “dentist near me” and sorting by the top-rated reviews.
Sites such as CareDash or ZocDoc rely on patient reviews to sell or discourage from one practice or another. These can help you get more specific reviews than a basic Google search may provide.
6. Narrow It Down with Questions + A Website Visit
Once you find your top picks using the above methods, go to their office website and look around.
A good dentist does not have to have a good website. However, a well-designed website, with lots of info about the practice, the staff, their specialties and strengths (and more patient reviews), can be a great indicator of a solid choice for you.
7. Double-Check Board Certification and State Licensure
Are dentists board certified? I’ve been asked this in the past. And the answer is yes.
You can read more about certification, and find out the certifications of your “short list” by visiting the American Board of Dental Specialties (ABDS). Almost every single time, you’ll find that your dentist is board certified and has a current state license.
However, there might be that one incredibly rare time that a dentist has failed to complete the necessary steps to get or renew one of these items. In these cases, I’d suggest looking elsewhere.
10 Questions to Ask Before or At Your First Appointment
There are several questions I’d recommend asking your dentist before the end of your first appointment. Depending on your specific needs, there isn’t necessarily a “wrong” answer to most of these questions.
Q:
Do you offer patients nutritional counseling?
A: There are probably traditional dentists who will talk to you about diet. However, they are likely to focus on the no-nos, such as foods and drinks high in sugar or acid content.
A functional dentist, however, will probably share many other nutritional tips and simple lifestyle changes. These will give you the added benefit of stronger teeth, healthier gums, and few cavities, PLUS a healthier you from head to toe. (More on what to eat for better dental health can be found here.)
If you’re not interested in the functional route, this answer may also be important. Some people don’t want nutritional counseling from the dentist and would be put off by it.
Q:
What are your primary goals in patient care?
A: I believe the most desirable answer is something like this: To do as little invasive work as possible, while giving the patients the best opportunity to avoid future problems, and extensive dental work.
Functional dentistry or not, you should look for a dentist who’s hoping to do the least work possible in correcting problems. Good dental health is all about prevention. An answer that sounds like they hope to do more work sounds to me like someone who may be trying to rip you off.
Q:
What will care in your office cost?
A: Ask for a price list of all standard procedures, including in-network and out-of-network prices. How much will x-rays cost? What if I need a filling? Many offices have a ready-made list they might be willing to email or fax you.
Others may suggest you come in for a face-to-face conversation, to go over any insurance you might have, or special prices for cash-only patients. If you have no dental insurance, this additional legwork is important to make sure you’re not being charged significantly more..
Don’t be afraid to ask about payment plans the dental office may offer, such as CareCredit. Especially for work beyond cleanings, it’s a good idea to have a plan to pay off this kind of work before having it done.
Q:
What work is done ‘in-house’, versus procedures that have to be referred out?
A: There are many functional dentists who do almost no procedures in the office. My personal recommendation would be to strike these practices off your list.
The best answer to this question would be something like: “I handle less invasive procedures in the office. However, if my exam indicates you need more extensive dental treatments or dental surgeries, I can refer you to other specialists I’ve come to know and trust.“
Q:
Where did you receive your degree?
A: All dental schools within the US are accredited, but the if the dentist was educated in a country with different standards and requirements, you might want to do more digging. Even if the school is within the US, look them up online to see what kind of reputation they have.
Q:
How long have you been in practice?
A: Ask this question to discover more about the experience of the dentist. A good dentist will be glad to share info about his/her dental school, years in practice, etc.
But I would also add that finding a new dentist who is only recently out of school doesn’t mean s/he isn’t capable, or that your care would be less than great. You might be talking to a young superstar who will provide amazing dental care and oral health for your and your family members for years to come.
Benefits of an established dentist might be that s/he has plenty of experience with patients, procedures, etc. A newer dentist might be more familiar with cutting-edge dental science.
Q:
How do you approach patients with dental anxiety/fear/phobia?
A: Many practices proudly advertise being great with “wimps.” Ask if they use any kind of gas to calm the nerves during procedures. (Don’t forget to check out the cost of gas; many insurance plans won’t cover it.)
You may also want to find out if they suggest using CBD for dental anxiety or other anxiety relief methods.
Q:
What is your procedure for dental emergencies?
A: Find out about any emergency hours or how a call service is used, what is the normal response time, etc. Some offices make this much easier than others, and it might be important when establishing a patient-dentist relationship.
Q:
Do you participate in a regular course of continuing education? If so, what is it?
A: It may seem like an invasive question, but a confident dentist who keeps his knowledge base up to date and growing will gladly provide an answer.
Q:
What are your office hours? And do those office hours include emergencies, or evening/weekend times?
A: This question may help you know how much the dentist considers the needs of working families. It may not be the major factor in how to find a good dentist, but it’s definitely an important one, especially if all the adults in your family have full-time day jobs.
How to Spot a Bad Dentist
I try to think the best of people, and this includes dentists and other medical professionals. Knowing how gratifying it is to work with a patient and see them implement positive dental health habits, it’s hard to imagine any other way to practice dentistry.
I’ve had a number of opportunities to serve as an expert witness for both the prosecution and the defense in cases where dentists are accused of malpractice. That experience, coupled with my years of service in dentistry, have given me a unique opportunity to see and compare dental offices of all kinds.
Here are several red flags you could encounter as you’re searching for the right dentist for you and your family members:
An unkempt office. Before you ever meet the staff or dentist, you first walk into the office. Pause to take a look around. Surfaces should be shiny and free of dust or smudges. Even older office space, with outdated carpet or furniture styles can be kept nice and tidy for a comfortable atmosphere. And look for a sparkling clean bathroom.
Rude or impatient staff. A good dentist will hire a staff who reflects well on him or her. Considering the trepidation many patients feel about coming to the dentist, a friendly staff go a long way in setting patients at ease before they ever meet the dentist.
A negative response from your child. When looking for a good pediatric dentist to care for children and teens, be sure the kids are present when you go to the office for a consult (once they are old enough to give you clues). Does your child respond well to the staff? Bottom line: The more at peace children are with their dentist, the more likely they are to continue good oral health into adulthood.
Defensiveness about treatment-related questions. In many cases, there are multiple treatment options you can choose from to correct or resolve dental problems. So, ask questions. A bad dentist might tell you there is only one way to approach treatment, and would then seem frustrated or put out for you to suggest some other way. That’s when you know it’s time to find another dentist.
A defensive attitude. No confident, quality dentist will have an issue with a patient asking for copies of dental records for a second opinion. If you feel any negativity or questioning about why you would want to get another dentist’s opinion, consider that another red flag, an indicator that it’s time to move on. (Side note: For a simple second opinion, try JustAnswer.com.)
Multiple, extensive procedures out of the blue. Some dentists will unnecessarily recommend multiple procedures from fillings to root canals to extra whitening services. Be leary of these kinds of pitches. It is unlikely many people would have 12 cavities in the space of a year, or be sent to the chair for 3 root canals in the same time period. Although not impossible, I would say those numbers are high and it’s a good idea to schedule a second opinion before agreeing to anything.
An uncomfortable feeling. Trust your gut! From the moment you enter the office, until the time you head toward the door to leave, you should feel comfortable and welcomed. If at any time this changes, it’s okay to walk away and find another provider.
Key Takeaways: How to Find a Good Dentist
Start by deciding what you want from a dentist. Whether you dread dental visits or have no particular issue with dental procedures, knowing what you’re looking for in a dentist is the springboard to finding the perfect fit for you and your family.
Do some research. Whether you use online resources to find a dentist or word of mouth referrals, form a short list of practices you think might be right for you and your family.
Ask some questions, then ask some more. The better the dentist, the more willing s/he will be to accommodate your inquiries. Whether your needs are simple and routine—checkups and cleanings—or you require more extensive work, the more you can discover up front will pay off in the end.
Lastly, don’t discount the red flags that might pop up, telling you a particular office isn’t good for you. Most of us know when we are being patronized, as well as we know when we’re being welcomed.
A good dental office will do all they can—with a clean, welcoming environment, and a friendly, well-informed staff—to win new patients over. And let’s face it: your teeth deserve the best care you can give them.
read next: No dental insurance? Here’s what to do.
The post How to Find a Good Dentist: 7 Tips + 10 FAQs appeared first on Ask the Dentist.
from Ask the Dentist https://askthedentist.com/find-good-dentist/
1 note
·
View note
Text
Back to School with Diabetes Amidst the COVID-19 Variants – Diabetes Daily
New Post has been published on https://depression-md.com/back-to-school-with-diabetes-amidst-the-covid-19-variants-diabetes-daily/
Back to School with Diabetes Amidst the COVID-19 Variants – Diabetes Daily

This content originally appeared on Beyond Type 1. Republished with permission.
By Lala Jackson
This article was published on August 13, 2021. As of Monday, August 23, the FDA has granted the Pfizer and BioNTech COVID-19 vaccine full approval for ages 16 and up, with the Emergency Use Authorization (EUA) still in effect for ages 12-15 and for booster doses for immunocompromised individuals. Full approval for other COVID-19 vaccines currently under EUA is expected soon.
While hopes were high that we could head back to school for the 2021 school year as though we were closer to “normal,” the development of COVID-19 variants amidst low vaccination rates has thrown a wrench in plans. But when kids need to get back to in-person schooling for quality of life, quality of learning, and socialization, how can we best keep them safe?
To help answer this and other questions about going back to school safely, JDRF—in collaboration with American Diabetes Association and Sansum Diabetes Research Institute—hosted a conversation with doctors and experts from the CDC, ADA, and the Fairfax County Health Department (Virginia).
Moderator Dr. Kristin Castorino, senior research physician at Sansum Diabetes Research Institute, kicked off the event with the most pressing question—is it even safe for students and their teachers who have diabetes to return to in person schooling, particularly for those under 12 who cannot be vaccinated yet?
“I’d change the question from ‘is it safe?’ to ‘is it appropriate?’ and I think it is,” answered Dr. Fran Kaufman, pediatric endocrinologist and chief medical officer at Senseonics. “There aren’t known answers as things change… but we need to get our kids back to school, not only for learning but for socialization.”
Dr. Kaufman stressed that the best way to make school safe is for everyone who can get vaccinated to do so. Dr. Christa-Marie Singleton, MD, MPH, senior medical advisor at the CDC later elaborated, “Vaccines protect folks against serious symptoms, hospitalization, and death. The best way to protect ourselves, our families, and our youngest people is for the adults and kids over the age of 12 around them to get vaccinated.”
“We also know about the importance of masking,” continued Dr. Kaufman. “It’s important to follow the CDC’s recommendation that all children and adults should be masked in the indoor school environment.”
What About the Legal Rights of Kids With Diabetes?
Particularly as some states ban school districts from being able to require masks in indoor learning environments, what legal protections do kids with diabetes have to stay safe in school? Crystal Woodward, MPS, director of the ADA’s Safe at School campaign, stressed “the rights of students with diabetes do not go away during a pandemic. They have legal protections under federal and state laws. Those accommodations may look a little different, but they do not go away.”
Similarly to how the Americans with Disabilities Act protects people with diabetes in the workplace, section 504 of The Rehabilitation Act protects the education of children with disabilities like diabetes. This law allows children with diabetes and their families to create what are known as 504 plans, which clearly outline agreed upon accommodations for students with disabilities at school.
While parents cannot dictate the actions of other students, they can include directives for their own children to stay safer from COVID-19 in 504 Plans, like instructions that their student must always wear a mask or will need extra physical distance in a classroom setting.
“It’s imperative that [children with diabetes] have a section 504 plan,” Crystal explained. “Everyone needs to be clear on what accommodations will be provided and by whom, like the student having the ability to take an exam at an alternate time if blood glucose levels are out of range during the scheduled test time.” Ensuring the student also knows what is in their own 504 plan can help them feel more empowered and comfortable asking for what they need.
For distance learning, 504 plans can dictate that children with diabetes can take snack or meal breaks at times best for the student, or have an agreed upon communication method with the teacher if the student needs to take a break to attend to a low or high blood sugar.
“Bottom line: the rights of students do not go away,” Crystal reiterated. “Students with diabetes and their families should work with schools and everyone needs to understand their role and responsibilities, and the plan should be updated as needed. It’s always better to get it in writing. Put the 504 plan in place while everything is going well—you never know if a principal or a nurse or a teacher is going to be there throughout the year.” Panel members stressed that families who don’t speak English, particularly in public schools, have a legal right to translators who can help establish 504 plans.
Jacqueline McManemin, RN, BSN, certified diabetes education and care specialist (CDECS) and assistant nurse manager for the health services division of Fairfax County Health Department in Virginia, spoke about what they’re continuing to do in their school district (one of the 15 largest in the nation) to keep students safe. “Parents should expect to see much of the same precautions this year that were in place last year. Particularly when students are inside, they should be masked.”
School administrators across the country can work to make schools more safe for all children, particularly those with chronic illnesses like asthma and diabetes, by putting in protective measures like establishing two different health clinics—one for people exhibiting symptoms of COVID-19 or other communicable illnesses and a separate clinic for routine care and injury treatment. Meals can be eaten outside as weather permits and student interaction in hallways can be minimized by teachers rotating between classrooms rather than groups of students switching classrooms every period. Protocol also needs to be clearly communicated with all staff and parents about what to do if a student starts showing symptoms of COVID-19 while at school.
Getting Kids Mentally Ready for in-Person School
Back to school doesn’t just mean a change of location, it’s a change in schedules, types of interaction and stimulation, and levels of distraction that can also impact diabetes care. Psychologist Cynthia E. Muñoz, PhD, MPH, assistant professor of clinical pediatrics at the University of Southern California’s Keck School of Medicine and president of healthcare and education for the American Diabetes Association, reminded the community that the impact of the pandemic on each individual has been unique and therefore approaches to regain a sense of normalcy must be unique too.
“For parents and guardians, be aware of how you’ve been impacted. Seek support, through family, through primary care, through a therapist. Find ways to talk about your fears or concerns,” encouraged Dr. Muñoz. She went on to suggest ways to get kids mentally and physically ready for school again.
“Now that schools are starting to open, it’s time to start looking at sleep schedules, screen time, and start shifting routines and schedules to get children ready for the new routine,” she noted. “Many people watch a lot of content on social media or television—not just kids, everyone—but it’s a passive interaction with others. Shifting to a more active form of communication with others can be another way to help people ease into the change of a lot more interaction than people have had in the last year or so.”
Helping Kids Who Feel Singled Out
Kids with diabetes often deal with feelings of being the odd kid out, having to visit the school nurse, having to deal with special routines. When COVID-19 is added, kids with diabetes may feel like they’re the only ones taking special precautions, which can be additionally isolating. How can parents help children dealing with these feelings?
“I like to approach this question around the concept of support, building layers of support around the student,” Dr. Muñoz explained. “One level should be ensuring that someone at the school should know that the child has diabetes and knows what kind of support they need. Another category is who could know [the student has diabetes], but doesn’t necessarily have to, like friends. For the student with diabetes, getting support from a friend or classmate they trust could go a long way. If the student feels like they’re going to be the only one wearing a mask, they can ask a friend to wear it with them.”
“I think it’s important for adults to be sensitive to this,” Dr. Muñoz continued. “Saying “everyone has something different” might minimize how a student feels. Acknowledging their feelings and taking the time to ask them what will help goes a long way.”
To get advice from other parents and guardians or to help your student with diabetes find other kids who understand, be sure to join the Beyond Type 1 community.
Learn more about the JDRF – Beyond Type 1 Alliance here.
You Can Watch the Entire Conversation Here:
youtube
Post Views:
4
Read more about American Diabetes Association (ADA), COVID-19, diabetes at school, Diabetes Research Institute (DRI), eversense, Intensive management, JDRF, kids with diabetes, pfizer, school.
window.fbAsyncInit = function () //Initialize the Facebook JavaScript SDK FB.init( appId: '8485090309', //App ID from the app dashboard channelUrl: 'http://www.diabetesdaily.com/channel.php', //Channel file for x-domain communication status: true, //Check Facebook Login status xfbml: true //Look for social plugins on the page );
//Logged In Users FB.getLoginStatus(function (response) if (response.status !== "unknown") ga('set', 'dimension1', 'Logged In'); );
//Facebook Likes FB.Event.subscribe('edge.create', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Like', 'socialTarget': href, 'page': currentPage ); );
//Facebook Unlikes FB.Event.subscribe('edge.remove', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Unlike', 'socialTarget': href, 'page': currentPage,
); );
//Facebook Send/Share FB.Event.subscribe('message.send', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Send', 'socialTarget': href, 'page': currentPage ); );
//Facebook Comments FB.Event.subscribe('comment.create', function (href, widget) var currentPage = jQuery(document).attr('title'); ga('send', 'hitType': 'social', 'socialNetwork': 'Facebook', 'socialAction': 'Comment', 'socialTarget': href, 'page': currentPage ); ); ;
//Load the SDK asynchronously (function (d, s, id) var js, fjs = d.getElementsByTagName(s)[0]; if (d.getElementById(id)) return; js = d.createElement(s); js.id = id; js.src = "https://connect.facebook.net/en_GB/all.js"; fjs.parentNode.insertBefore(js, fjs); (document, 'script', 'facebook-jssdk'));
Source link
0 notes
Text
90 Helix Piercing Concepts In the Trendiest Self

In general, rings tend to maneuver more, which might prolong therapeutic and encourage swelling and scar tissue formation. Most piercings may be switched to rings once they are healed when you favor that aesthetic. DON’T TOUCH YOUR PIERCING. During your bathe, permit the water to rinse over the piercing for about seconds. Check out our piercing aftercare information for extra in-depth cleaning ideas. As at all times, call us with any questions, issues,and to schedule your follow-up visit.
Do helix piercings get infected easily?
Just like all piercings, a cartilage piercing (AKA helix piercing) will be a bit tender while it heals. Bumping it on something (like a hairbrush), getting hair caught on it, and — yes — sleeping on it can cause your piercing to swell or become painful. And it can stay that way, for days even.
Your piercer will be capable of present steerage, however the primary figuring out issue of helix piercing location is your personal preference, so ultimately, it’s as much as you. Today we are going to be supplying you with 5 reasons on why we hate helix piercings. Sometimes, two helix piercings maintain the identical piece of jewellery, often a barbell, which is known as an industrial piercing.
What Type Of Earring Do You Utilize For A Helix Piercing?
Most of those ear piercing salons would most likely have already got established themselves out there. If they've, and if they're performing that well, they want to already have received good critiques on-line. Also, you may want to verify if they've posted photos of their works. The diameter ought to be at minimum the same as the size of the barbell—5/16”.
Can I change my own helix piercing?
The piercing takes more time to do than most other piercings, about 6 to 9 seconds, which could prolong the pain. After a daith piercing is finished, most people report a dull, achy pain for a few days.
How painful is it?Part of the earDescription of areaPain levelForward helixinner thin upper part of your ear512 more rows•May 6, 2020
Always make certain to use a light-weight hand when doing this and try to not move the jewelry a lot. There is all the time a risk related to piercings, that simply comes with the physique modification territory. However, as a outcome of cartilage is a fragile tissue, you probably can expect that it'll have a better danger of an infection and damage from being pierced. This may be scary, but with continued correct remedy, this infection can go away. If you consider you have an infection that could probably be dangerous, it is better to contact a health care provider sooner rather than later. If an infected piercing is left untreated for too lengthy, it might possibly depart everlasting injury to the ear, generally requiring surgery to fix.
Helix Piercings Can Take Up A To A Year To Heal
Peroxide is simply too strong for most piercings and can prolong the therapeutic course of, trigger a lot of ache, swelling, and even blistering of the pores and skin. An skilled skilled healthcare marketing consultant provides people advises and tips on how to complete the helix piercing successfully. Depending on your age, well being, and skin sort, you have to go for difficult outpatient surgery at the clinic or salon. Book the proficient surgeons who've fame and goodwill to pierce the helix a half of the ears. This is essentially the most excessive type of helix piercing and the preferred as well.
Also simply because the gun is a sooner and cheaper option than the professional piercing doesn’t imply it's better.
Do your finest to refrain from sleeping on the jewellery, and keep away from hats or different head gear which may contact or transfer the jewellery during therapeutic.
Needless to say that this is additionally essentially the most painful sort of piercing.
The reason for this is because the fixed stress really irritates the piercing itself.
The helix occurs to be the preferred of the cartilage piercings because it provides plenty of versatility by method of jewelry selections. Some swelling in the first days after your helix piercing is to be anticipated. If things proceed to escalate although, you may wish to have a doctor take a look at your ear, particularly if the swelling is accompanied by sizzling feeling pores and skin.
Their piercing will heal nicely without any problems. However, every so often, one thing goes wrong and an an infection units in. That can help reduce down on any bumps that may be tempted to form there.
It could improve relying on the jewellery that is being used. Neglecting to frequently clean can end result in a longer healing time general. Also, if you would like to include solely black beads, then try to pierce no much less than three on the higher cartilage of your ear, so the texture looks nice and terrific to every crossing sight. The massive query that comes to thoughts when thinking about body piercing is, does cartilage piercing hurt?
youtube
0 notes
Link
Alzheimer’s disease is not limited to the elderly. Although rare, some individuals are diagnosed with younger-onset Alzheimer’s disease in early adulthood—some as early as their twenties and thirties. Quarter-lifers who are diagnosed with Alzheimer’s struggle with unique challenges. While coping with the symptoms of Alzheimer’s, they are also transitioning to adulthood, launching their careers, getting married, and having children. It is possible for quarter-lifers, particularly quarter-life couples, to enjoy life and manage this disease. For these reasons, it is particularly critical for Quarter-life couples to prepare for the changes associated with early-onset Alzheimer’s disease by communicating about important, and sometimes difficult, topics.
8 Important Topics to Discuss:
1. Adjusting to the Diagnosis
What is your understanding of Alzheimer’s disease? Where can you get information you need? How do you each feel about your diagnosis? What are your hopes, concerns, fears, and expectations about this diagnosis?
2. Medical Care
Do you like and trust your medical providers? Most likely, your neurologist and primary care doctor will be the physicians managing this disease. What will your medical care look like over time? What medications will be prescribed and what tests will be run? Do you want to consider genetic testing for you and your children?
3. Psychological Support
Where can you get the emotional support you need? There is a range of support services for Alzheimer’s disease: support groups for patients and caregivers, seminars, conferences, professional counseling, and online forums. The Alzheimer’s Association and the Alzheimer’s Foundation of America are good resources.
4. Social Support
Which family members and friends would you like to inform about the diagnosis of Alzheimer’s? How would you like to talk to your children about this diagnosis? Whom can you depend on for support over the course of the disease? Who will serve as the primary caregiver for the person with Alzheimer’s?
5. Career
How will your diagnosis affect your ability to work? How will this diagnosis affect your spouse’s ability to work, if there are significant caregiving responsibilities?
6. Finances
How will this diagnosis change your family’s financial situation? Be sure to research benefits and disability insurance that may be available to you and your partner. Look into Medicare benefits and retirement benefits, as well.
7. Healthcare Planning
What legal paperwork should be completed to plan for your healthcare in the future? Consider meeting with an attorney to create a Last Will and Testament, Power of Attorney, Healthcare Proxy, and Living Will.
8. Finding Joy
Most importantly, talk about what brings you joy and how you can maximize experiences that are fulfilling for you and your family. Be patient with yourself as you adjust to this diagnosis. Are there certain experiences you’d like to share and/or important conversations you’d like to have with loved ones before the disease progresses? How can you plan for these things? How can you make the most of your life while also attending to this disease?
If you’re interested in scheduling an appointment or you’d like more information, please contact us.
0 notes
Text
Alzheimer's Association Chicago
Multidisciplinary Clinical Diagnosis Of Alzheimer Disease

All participants receive regular care related to the trial and opportunities to talk to clinical trial staff. Dementia care is a daunting task, but may not be as challenging as you expect. Having a schedule can reduce the time you spend figuring out what needs to be done and when, and makes you more successful in accomplishing your goals and limiting mistakes. When your memory is in good working order, you can recall most things without always having to write them down or be reminded. In order to participate, physical clearance from a primary care physician within the last year is required. You have the right to expect the services you hire and the products you purchase to help you, not harm you.
google_ad_client = "pub-4090994097430346";google_ad_width = 468;google_ad_height = 60;google_ad_format = "468x60_as";google_ad_type = "text_image";google_color_border = "FFFFFF";google_color_bg = "0000FF";google_color_link = "FFFFFF";google_color_text = "000000";google_color_url = "008000";google_ui_features = "rc:6";
Alzheimer Disease Or Other Related Memory Loss Diseases
Neurodegenerative disease is the group of condition or disease which mainly affect the neurons of the brain. Many teams are named in honor of a loved one who suffers from the disease. Participants complete each one, every day, in four short sessions, and do that for a week. Much of the increase will be in developing countries like Western Europe and North America. When you are thinking hard, your brain may use up to 50 percent of the fuel and oxygen. The diameter of the reactor has been increased by about 12 percent, but little else has changed, Greenwald says.
Diagnosis Of Alzheimer Disease Or Mild Cognitive Impairment
Many people have amyloid plaques in the brain but have no symptoms of cognitive decline or Alzheimer's. Schneider thought the speed of the cognitive and structural brain changes indicate the two may be linked. People who had had symptoms for more than five years, or signs of another neurodegenerative disorder, were excluded. The success of the Alzheimer Association, which now sponsors the largest and most impactful international scientific meetings on the disorder, cannot be overestimated. A clinical report is any variety of clinical analysis together with people, paying very little heed as to if it is Associate in Nursing an intercession. Over the last 40 years, disparities among people with developmental disabilities have been one of the main issues.
Primary Goal Of Attending An International Conference
Clinical trials are part of clinical research and at the heart of all medical advancement. Neurological manifestations may happen because of the contamination itself or because of a safe reaction. To better comprehend the premise behind medication advancement, one should first see how neurons speak with each other. In the current version of Chicago, the 17th version, ibid is accepted but not preferred. Based on the results, the vaccine will continue to be studied in the next level of clinical trials. A greatly little extent under five level of neurodegenerative infections are caused by hereditary changes.
A Research Scientist At The University
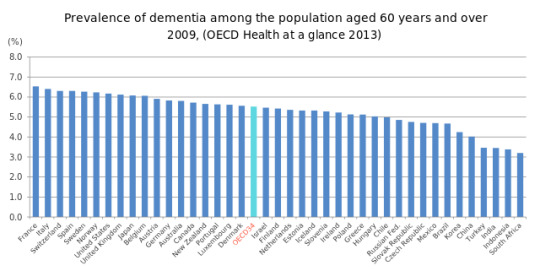
Penn Medicine is committed to improving lives and health through a variety of community-based programs and activities. Penn Medicine is powered by a talented and dedicated workforce of more than 43,900 people. Whether your loved one is still living or has passed on, you can show your appreciation. You will feel energized and rejuvenated to return to the university and continue with the job after attending the conference. You will need time to adjust your lifestyle and to find help when you need it. The course of dependence Dependence may get worse, remain stable, or get better over time.
Full-text Biomedical Journal Articles
Clinical trials are research studies conducted with human volunteers to determine whether treatments are safe and effective. No unexpected impediments or surprises have shown up, and the remaining challenges appear to be manageable. Clinical trials are one of the final stages of a long and careful research and development process. The process often begins in a laboratory, where scientists first develop and test new ideas. There has not been enough scientific research to establish an appropriate dose of superoxide dismutase. The license may not give you all of the permissions necessary for your intended use.
Scientific Research And Development

All services are designed to help families meet the challenges and opportunities of later years. The most important think really is to be gentle both on yourself and on the person affected directly, trying to see things from their, now increasingly limited perspective. You may already be aware of changes in your ability to complete daily tasks that once came naturally to you.
Self Care In Health Policies And National Healthcare

Comparison of prevalence of dependence among older people between high income and lower income countries 3 a lower prevalence of chronic diseases that contribute to disability and dependence. Drug development pipelines are full but mostly focus on potentially profitable diseases that mainly affect high-income countries. The instructors are very well trained and responsive to the needs of an older population. With an increasing older adult population and people with disabilities living longer, the need for caregiving is growing. Older adults with dementia are vulnerable when hospitals are unable to meet their special needs.
Increasing Blood And Oxygen Flow In The Brain
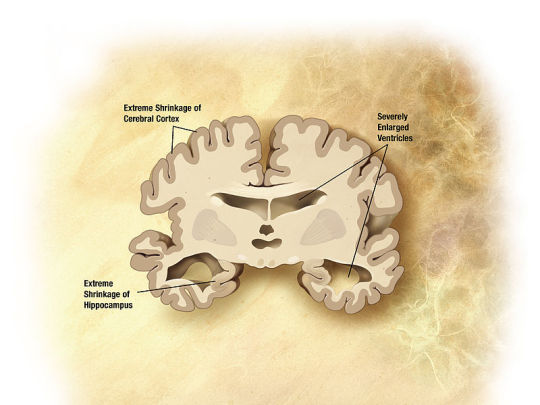
Previous research has suggested a link between type 2 diabetes and an increased risk of dementia. The test must now be studied on many more people to make sure it is as accurate as it appears. The risk of developing AD rises after age 65, and rises sharply after age 75. Animal models are important for research, particularly in testing some of the potential therapeutic approaches. The researchers have dubbed the recombinant seed competent and inert monomers Ms and Mi, respectively.
from Blogger https://ift.tt/3nF76tN
via Alzheimer's Help and Resources
0 notes
Text
Rotator Cuff Pain? Why To Avoid It ?
Overview
The rotator sleeve is a gathering of muscles and ligaments that encompass the shoulder joint, keeping the top of your upper arm bone solidly inside the shallow attachment of the shoulder. A rotator sleeve injury can cause a dull hurt in the shoulder, which frequently intensifies with utilization of the arm away from the body.
Rotator sleeve wounds are normal and increment with age. These may happen prior in individuals who have employments that require consistently performing overhead movements. Models incorporate painters and craftsmen.
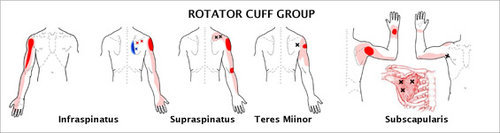
Numerous individuals with rotator sleeve malady can deal with their manifestations and come back to exercises with active recuperation practices that improve adaptability and quality of the muscles encompassing the shoulder joint.
Now and then, rotator sleeve tears may happen because of a solitary physical issue. In those conditions, clinical assessment ought to be given as quickly as time permits to examine the job of medical procedure. Broad rotator sleeve tears may not be fixable, and move of elective ligaments or joint substitution might be conceivable.
Symptoms

The torment related with a rotator sleeve injury may:
Be depicted as a dull throb somewhere down in the shoulder
Disturb rest
Make it hard to brush your hair or reach despite your good faith
Be joined by arm shortcoming
3MEDS-online pharmacy store in India,is concerned with health and fitness of their customers and therefore believes in providing knowledge about healthcare to their customers.
Causes
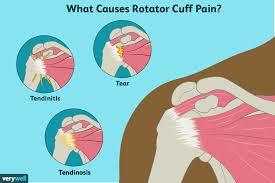
Rotator sleeve ailment might be the consequence of either a significant injury to the shoulder or to dynamic degeneration or mileage of the ligament tissue. Redundant overhead movement or hard work over a delayed timeframe may disturb or harm the ligament.
Hazard factors
The accompanying components may expand your danger of having a rotator sleeve injury:
Age. As you get more established, your danger of a rotator sleeve injury increments. Rotator sleeve tears are generally normal in individuals more seasoned than 60.
Construction occupations. Occupations, for example, carpentry or house painting require tedious arm movements, regularly overhead, that can harm the rotator sleeve after some time.
Family history. There might be a hereditary segment associated with rotator sleeve wounds as they seem to happen all the more ordinarily in specific families.
Entanglements
Without treatment, rotator sleeve issues may prompt changeless loss of movement or shortcoming, and may bring about dynamic degeneration of the shoulder joint. In spite of the fact that resting your shoulder is important for your recuperation, keeping your shoulder immobilized for a delayed time can cause the connective tissue encasing the joint to get thickened and tight (solidified shoulder).
Counteraction
On the off chance that you are in danger of rotator sleeve wounds or in the event that you've had a rotator sleeve injury before, day by day shoulder fortifying activities can help forestall future injury.
A great many people practice the front muscles of the chest, shoulder and upper arm, yet it is similarly imperative to fortify the muscles in the rear of the shoulder and around the shoulder bone to improve shoulder muscle balance. Your primary care physician or a physical specialist can assist you with arranging an activity schedule.
Determination
During the physical test, your primary care physician will push on various pieces of your shoulder and move your arm into various positions. The person will likewise test the quality of the muscles around your shoulder and in your arms.
Now and again, the individual may suggest imaging tests, for example,
X-beams. Albeit a rotator sleeve tear won't appear on a X-beam, this test can picture bone prods or other possible foundations for your torment —, for example, joint inflammation.
Ultrasound. This kind of test utilizes sound waves to deliver pictures of structures inside your body, especially delicate tissues, for example, muscles and ligaments. It permits dynamic testing, surveying the structures of your shoulder as they move. It likewise permits a fast examination between the influenced shoulder and the solid shoulder.
Magnetic reverberation imaging (MRI). This innovation utilizes radio waves and a solid magnet. The pictures got show all structures of the shoulder in extraordinary detail. The nature of the pictures relies enormously upon the nature of the hardware utilized
Purchase all your medicines online at the click of your finger on 3MEDS-Indias online medical store.
Treatment For It
Traditionalist medicines —, For example, rest, ice and non-intrusive treatment — once in a while are everything that is expected to recuperate from a rotator sleeve injury. On the off chance that your physical issue is serious, you may require medical procedure.
Infusions-In the event that moderate medicines haven't decreased your agony, your primary care physician may suggest a steroid infusion into your shoulder joint, particularly if the torment is meddling with your rest, day by day exercises or non-intrusive treatment. While such shots are regularly incidentally supportive, they ought to be utilized sensibly, as they can add to debilitating of the ligament and may bring down the achievement of medical procedure if this is inevitably required.

Exfusions-Exercise based recuperation is generally one of the primary medicines your PCP may propose. Activities custom fitted to the particular area of your rotator sleeve injury can help reestablish adaptability and solidarity to your shoulder. Non-intrusive treatment is likewise a significant piece of the recuperation cycle after rotator sleeve medical procedure.
Medical procedure
A wide range of kinds of medical procedures are accessible for rotator sleeve wounds, including:
Arthroscopic ligament fix. In this methodology, specialists embed a little camera (arthroscope) and apparatuses through little cuts to reattach the torn ligament deep down.
Open ligament fix. In certain circumstances, an open ligament fix might be a superior choice. In these kinds of medical procedures, your specialist works through a bigger cut to reattach the harmed ligament deep down.
Tendon move. On the off chance that the torn ligament is too harmed to even consider being reattached to the arm bone, specialists may choose to utilize a close by ligament as a substitution.
Shoulder substitution. Enormous rotator sleeve wounds may require shoulder substitution medical procedure. To improve the fake joint's solidness, a creative method (switch shoulder arthroplasty) introduces the ball part of the fake joint onto the shoulder bone and the attachment part onto the arm bone
Way of life and Home Cures
The torment from a minor rotator sleeve injury regularly lessens all alone, with appropriate consideration. Quit doing what made the torment and attempt maintain a strategic distance from excruciating developments. Cutoff hard work or overhead action until your shoulder torment dies down. Icing your shoulder may assist it with feeling much improved. Over-the-counter torment relievers, for example, ibuprofen (Advil, Motrin IB) or acetaminophen (Tylenol, others) likewise might be useful.
Various medicines may be provided by various specialist in your clinical group.Buy your medicines online now at Indias best online store-3MEDS
Synopsis
Agony, solidness, and growing of the shoulder are side effects of rotator sleeve wounds. While numerous patients report that their manifestations had an intense beginning, research has demonstrated that the side effects are likely the consequence of degeneration and debilitating of the rotator ligaments after some time. People who participate in overhead games, for example, tennis, racquetball, and baseball are at an expanded danger of enduring a rotator sleeve injury.
There are different treatment choices accessible for people experiencing rotator sleeve wounds, going from traditionalist techniques including rest and exercise to more forceful choices including steroid infusions and medical procedure. A treatment plan comprising of different treatment strategies may give the most advantage to patients experiencing a rotator sleeve injury. Patients are urged to talk with their doctors to concoct a reasonable treatment plan for their condition.
-Vikrant Bhagat
#3MEDS#besthealthcarecomapnyinindia#24hoursmedicinedelivery#rotatorcuff#ibuprofen#advill#motrin#medicines#ligament
0 notes
Text
INDEPENDENCE, THE PRECIOUS NIGERIAN CHILDREN AND THE SOUL OF THE NIGERIAN STATE: A SOBERING OBSERVATION

INDEPENDENCE, THE PRECIOUS NIGERIAN CHILDREN AND THE SOUL OF THE NIGERIAN STATE: A SOBERING OBSERVATION
‘There can be no keener revelation of a society's soul than the way in
which it treats its children. ‘Nelson Mandela
On October 1, 1960, a series of nebulous negotiations between the colonial masters and our Nigerian independence negotiators, delivered
on our laps as peoples of many nations, earlier amalgamated for economic and convenient administrative reasons what we today refer to and hypocritically celebrate as independence.
The arrangement as we can see has not delivered much in terms of the dividends of a modern state under a social contract. A social contract has one major provision: the welfare and the security of the people shall be the primary aim of government at all levels.
What we have today as the evidence of that 1960 arrangement are awfully unreliable social services, which I refer to as factory rejects, which emanate from the foundational errors of the production lines of state and governance as established by negotiators of the so-called independence and their protégés they handed over
The production plant of state and governance obliviously was not
properly set up on and before 1960. I think those who worked out the
arrangement were either myopic in their understanding of the requirements for setting up a working state for peoples with diverse social, political and economic identities or they were distracted by their personal interest to bequeath to us a liability as a state.
‘If the foundation is faulty, what shall the righteous do,’ so says the book that I read. The righteous today seems not to have come to the realization that our fundamental problem is our foundation as a nation and until we revisit that foundation for the purpose of rebuilding it, we will continue to go in directionless circles, pretending that all is well, expect the best from a dysfunctional
system of state, erected on a faulty foundation by those who negotiated the 1960 nebulous arrangement and gather every October 1 to pretend to celebrate an arrangement that has not in any way delivered social, political and economic freedom, which should be the vigorous
goal of a truly independent state.
Having pioneered a Social Empowerment Advocacy aimed at Securing A Friendly and Protective Environment for the precious African child through the STANDARDS of Systems Approach and Family Strengthening since 1997, I have come to the irresistible conclusion that the state of our nation is the state of our precious children and to change the
state of our precious children we must change the state of our nation; anything short of the foregoing remains in the social masturbating exercise in tokenism.
I have continued to postulate that until we address the issue of poverty, we cannot be serious about addressing the issues of Securing a Friendly and Protective Environment™ for the precious Nigerian children. I have said it to power many times that we cannot expect a set of caregivers, particularly parents, whose existence is abused and
do not enjoy any support from the state to be effective in protecting their precious children from abuse. There is no meaningful nation on earth where the responsibility of raising and protecting children rest solely on the shoulders of the parents and private institution.
I have continued to argue that there are four rings of protection, namely, family, community, state and international community. While it is the primary role of the family to raise and protect their precious children, it is however the primary responsibility of the community
(neighbors, media, institution of learning, religious places of worship, NGOs, FBOs, CBOs, for-profit organizations and all private and para-state institutions within the community) and state to support
the family and create an enabling environment for the family, sometimes with the support of the international. Once the community and the state fail in their sacred responsibilities as highlighted above, they put the family under unnecessary pressure.
Today’s Nigerian parents are nations to their precious children. Their children are their citizens as they are saddled with the responsibilities of providing for their precious children all the social services the state should provide for them. Maternal care, education, primary health care, shelter, nutrition, clothing is
provided by the parents, who have the means and those who do not have
the means are left to their fate. Their precious children either suffer outright neglect or they are exposed to a kind of social services that leave them half-backed and dehumanized at the end of the day.
It seems to me that the way it is now, the parents of the Nigerian children are the citizens and the precious children are ‘grandcitizens’ and Nigeria is their ‘grandcountry’. It is just that in this arrangement the country does not support the ‘parentcitizens’ to meet the basic needs of their citizens (children) to who the state is now is their ‘grandcountry.’ The sad thing is that the state of the Nigeria and obvious neglect of her people, particularly her precious
children seem to have been accepted as the norm.
Since there is no such concept as grandcitizenship or grandcountry in
the global social dictionary, the fate of the precious Nigerian child is in a horrible state of emergency.
Consider the pictures that we see where children are compelled to drink dirty water, live on refuse dump sites, pack themselves as 140 students in classroom built for 40; sit on the bare floor or used car tyres, sit under the tree to be taught, laid on plastic chairs as newborn and you will agree with me that the fate of the precious Nigerian child is in a horrible state of emergency.
Consider the fact that 13.5 million Nigerian children are out of school and Nigeria has the highest number of children out of school in the world; that one in five Nigerian children never reach the age of 5 and that nearly 20% of all global maternal deaths happen in Nigeria, the precious Nigerian child is in a horrible state of emergency.
Consider that the Nigerian children are two generations behind schedule in learning the basics and being ready for the 21st century world of work, the precious Nigerian child is in a horrible state of emergency.
Consider that we erroneously and frequently refer to our precious children, who are denied of basic needs of life like healthcare, education, shelter, food and water and clothing as underprivileged when in actual fact they are the denied, the abused and the ‘wretched of the earth,’ in the words of Franz Fanon, whose parents are the
hewers of woods and drawers of water, the Hoi polloi, who what they are actually denied of are their basic rights to livelihood and not privileges, the fate of the precious Nigerian child is in a horrible
state of emergency. Privileges only kick in after universally
recognized rights have been met.
The disposition of the Nigerian state today is a keen revelation of our soul as a society and if the fate of the precious Nigerian child is in a horrible state of emergency, then the Nigerian state is in a horrible state of emergency. I round up this call to action and genuine advocacy for a better nation and attention to our precious children, which I find no better day to address than today with the instructive words of V.R. Tenaja, ‘so long as there is one child who has failed to obtain the precise educational treatment his individuality requires; so long as a single child goes hungry, has nowhere to play, fails to receive medical attention he needs; so long as the nation fails to train and provide scope for every atom of
outstanding ability it can find; so long as there are administrators or teachers who feel no sense of mission, who cannot administer or who cannot teach, the system will remain incomplete.’
I remain sober on my knees today, praying that God help us to accept
the wisdom not to continue to sacrifice our collective future for the selfish expediency of today, playing victims of faulty past and foundation as a state.
Do have an INSPIRED day.
Yours IN THE BEST INTEREST OF THE PRECIOUS AFRICAN CHILD,
Taiwo AKINLAMI
The Preacher
www.taiwoakinlamiblog.com
234- 8033620843
Read the full article
0 notes
Text
Quarter-lifers Coping With Alzheimer’s

Alzheimer’s disease is not limited to the elderly. Although rare, some individuals are diagnosed with younger-onset Alzheimer’s disease in early adulthood—some as early as their twenties and thirties. Quarter-lifers who are diagnosed with Alzheimer’s struggle with unique challenges. While coping with the symptoms of Alzheimer’s, they are also transitioning to adulthood, launching their careers, getting married, and having children. It is possible for quarter-lifers, particularly quarter-life couples, to enjoy life and manage this disease. For these reasons, it is particularly critical for Quarter-life couples to prepare for the changes associated with early-onset Alzheimer’s disease by communicating about important, and sometimes difficult, topics.
8 Important Topics to Discuss:
1. Adjusting to the Diagnosis
What is your understanding of Alzheimer’s disease? Where can you get information you need? How do you each feel about your diagnosis? What are your hopes, concerns, fears, and expectations about this diagnosis?
2. Medical Care
Do you like and trust your medical providers? Most likely, your neurologist and primary care doctor will be the physicians managing this disease. What will your medical care look like over time? What medications will be prescribed and what tests will be run? Do you want to consider genetic testing for you and your children?
3. Psychological Support
Where can you get the emotional support you need? There is a range of support services for Alzheimer’s disease: support groups for patients and caregivers, seminars, conferences, professional counseling, and online forums. The Alzheimer’s Association and the Alzheimer’s Foundation of America are good resources.
4. Social Support
Which family members and friends would you like to inform about the diagnosis of Alzheimer’s? How would you like to talk to your children about this diagnosis? Whom can you depend on for support over the course of the disease? Who will serve as the primary caregiver for the person with Alzheimer’s?
5. Career
How will your diagnosis affect your ability to work? How will this diagnosis affect your spouse’s ability to work, if there are significant caregiving responsibilities?
6. Finances
How will this diagnosis change your family’s financial situation? Be sure to research benefits and disability insurance that may be available to you and your partner. Look into Medicare benefits and retirement benefits, as well.
7. Healthcare Planning
What legal paperwork should be completed to plan for your healthcare in the future? Consider meeting with an attorney to create a Last Will and Testament, Power of Attorney, Healthcare Proxy, and Living Will.
8. Finding Joy
Most importantly, talk about what brings you joy and how you can maximize experiences that are fulfilling for you and your family. Be patient with yourself as you adjust to this diagnosis. Are there certain experiences you’d like to share and/or important conversations you’d like to have with loved ones before the disease progresses? How can you plan for these things? How can you make the most of your life while also attending to this disease?
About the Quarterlife Center (QLC):
Our QLC Counselors specialize in working with individuals and couples in their 20s and 30s in a supportive, caring, confidential setting. We will work with you to help you identify your passions, achieve your goals and thrive in your life.
Quarterlife Center offers the following services:
Individual Counseling
Couples Counseling
Premarital Counseling
Career Coaching
Perinatal/Postpartum Counseling
If you’d like more information or you’re interested in scheduling an appointment, please contact.
#Individual Counseling#Couples Counseling#Premarital Counseling#Postpartum Counseling#Perinatal Counseling#Career Coaching#Quarterlife Crisis#Quarterlife Counseling#Mental Health#Mental Health Counseling
0 notes
Text
Hospitals Squeal Like Stuck Pigs Over Trump Proposal to Force Disclosure of Insurance Company Discounts
Digital Elixir
Hospitals Squeal Like Stuck Pigs Over Trump Proposal to Force Disclosure of Insurance Company Discounts
In one of his intermittent gestures of concern for ordinary people, Trump made what ought to be a modest proposal: to require hospitals to disclose the discounted prices they have negotiated various insurers. Hospital industry spokescritters reacted as if Trump was planning to throw their children in a vat of boiling oil.
The vehemence of the hospitals’ response, along with the ludicrous claims made, seems surprising given how toothless the Trump proposal is. Hospitals that don’t play ball would be fined up to $300 a day. Yes, you read that correctly. $300 a day, maximum.
However, as we’ll discuss, even a weak proposal like this could have significant impact if even a few hospitals were to accede to the Administration’s wishes.
First, a brief overview of the Trump plan, courtesy the Wall Street Journal:
Hospitals would have to disclose the discounted prices they negotiate with insurance companies under a Trump administration rule that could upend the $1 trillion hospital industry by revealing rates long guarded as trade secrets.
Hospitals that fail to share the discounted prices in an online form could be fined up to $300 a day, according to a rule proposed in the Federal Register. The price-disclosure requirements would cover all the more than 6,000 hospitals that accept Medicare.
Comments on the proposal would be due in September and, if completed, the rule would take effect in January.
Hospitals would have to disclose the rates for services and treatment that they have negotiated with individual insurance companies such as Aetna Inc., Cigna Corp. and Anthem Inc. under the proposal released Monday. The Trump administration is also working on initiatives that could compel insurers to disclose their rates, part of a push to publicize costs that is likely to spur lawsuits and sharp resistance from the industry.
The initiative represents the Trump administration’s growing effort to shift away from rolling back the Affordable Care Act rollback and put its own stamp on health care instead. Central to that strategy is the notion that more price transparency will inject greater competition into the market and lower costs.
An additional element, per CNBC:
As part of the proposal, the administration would require hospitals to publish insurer-specific prices for at least 300 “shoppable services” consumers might consider beforehand, such as X-rays or lab tests.
We have to stop and note that the Journal dignifies the laughable industry assertion that negotiated prices constitute a trade secret. A trade secret is intellectual property developed by the producer that is so important to its competitive standing that disclosure would amount to irreparable harm. Classic examples of a trade secret are the formula for Coca Cola and the designs for chips. The claim that a mere figure that was the result of a negotiation between two parties could ever be deemed to be a trade secret is ludicrous.
The fact that an industry shill managed to get the Journal to run such palaver is a sign that hospitals don’t have good legal arguments for preserving the secrecy of this information if government bodies require them to disclose it.
So what are the hospitals so keen to hide? That the discounts can be massive. One account from a reader who has lots of doctors in the family. A woman in California had her mother come from India to pay a visit. During her stay, the mother was diagnosed with breast cancer. The daughter wanted her to have surgery in the US. The mother did not have insurance. The hospital gave a rate of $120,000 for the procedure.
The daughter was able to ascertain that only about $7,500 was the hospital’s charge for the operating room; the rest was for the doctors. She contacted the surgeon whose fee was roughly $100,000. She was able to get him to agree to take only half. She continued working on him. By the time she was done, he agreed to charge the rate that would have been billed to an insurer: $3,800.1
Moreover, so far, hospitals appear to have had to do very little to beat back other reforms, such as a California bill to bar the abuse of “surprise billing,” also known as balance billing. As we noted in a post earlier this month:
This article demonstrates the power of health care industry incumbents. “Surprise billing” is pure and simple price gouging, particularly since hospitals routinely game the system, such as by scheduling doctors who are not in a patient’s network on his operation, even when the patient has gone to considerable lengths to try to prevent that.
All these hospitals did was the equivalent of yelling “Boo” at the legislature, and the legislation to combat surprise billing was yanked, even though there has been a great deal of deservedly critical press coverage of this abuse.
On this issue, the hospitals’ mouthpieces have roused themselves to muster arguments but they don’t stand up to scrutiny. From the Journal:
Industry groups have argued that mandatory price disclosure could push up costs if hospitals see competitors are getting higher payments and demand the same. They say the federal government is overstepping its statutory authority and interfering in private contracts between insurers and hospitals. The contracts are generally bound by confidentiality agreements.
Tom Nickels, executive vice president of the American Hospital Association, has said consumers care more about their expected out-of-pocket costs.
“Disclosing negotiated rates between insurers and hospitals could undermine the choices available in the private market,” he told the Journal in March, when the White House was considering initiatives on price disclosure. “While we support transparency, this approach misses the mark.”
Help me. How does disclosing prices reduce choice? This is bafflegab.
It is also not a secret that some hospitals, particularly teaching hospitals, demand and get higher reimbursements from insurers. And some even stare them down. For instance, the University of Alabama at Birmingham has the best med school in the South. The contracts between United Healthcare and UAB Health System members, such as the UAB hospital, Kirklin Clinic (a huge outpatient center), all other UAB Medicine primary care, specialty care, and urgent care clinics, as well as other operations expires today. That means anyone with United Healthcare who goes to a UAB System participant, save for the emergency room, will pay the full rack rate.
And what hospitals are keen to hide is the gap between their out of network versus in network rates, which per the comment above, they are desperate to hide because putting out of network doctors in an operating team is their big way of larding up prices to patients. Exposing the size of the gap between the rack rate and the insurers’ prices will put pressure on hospitals to end or at least curtail this abuse.
It is entirely possible that even if the Administration prevails, some or even many might defy the new rule and pay the fine. But they run the risk that Trump will use his media megaphone to hector them. That has driven down stock prices upon occasion, hitting execs in their weak spot. And local media and local politicians might name and shame the refusniks.
This Trump plan is clearly just an opportunistic gesture to allow the GOP to pretend they are serious about combatting ever-rising health care prices. But it’s also a sign that more and more Republicans see defending the status quo as a political loser.
____
1 The part that is not obvious from this interaction is how much of the doctor’s fee actually went to the hospital. Calling it a surgeon’s fee, implies that it all or largely went to the surgeon personally, which is not the case.

Hospitals Squeal Like Stuck Pigs Over Trump Proposal to Force Disclosure of Insurance Company Discounts
from WordPress https://ift.tt/2GOIpHN
via IFTTT
0 notes
Text
The Scoop: June 17, 2020 Edition
In this edition
COVID-19 special enrollment periods extended in New York, Vermont
Enrollment in Medicaid and exchange plans increases sharply due to COVID-19
Colorado legislature passes bill to make individual health coverage more affordable
Missouri Chamber of Commerce endorses Medicaid expansion ballot initiative
CMS gives insurers the option to pay MLR rebates early this summer
Trump administration rolls back Obama administration’s healthcare nondiscrimination protections
COVID-19 special enrollment periods extended in New York, Vermont
Most of the fully state-run health insurance exchanges opened up special enrollment periods this spring to address the COVID-19 pandemic. Several of them are still ongoing, including New York’s and Vermont’s. Those were scheduled to end earlier this week, but both were extended at the last minute. Uninsured residents in New York now have until July 15 to enroll in a health plan; uninsured Vermont residents have until August 14.
The COVID-19 enrollment window in Massachusetts is scheduled to end next Tuesday, June 23. California’s is scheduled to end the following week, and DC’s continues until mid-September.
In every state, Medicaid and CHIP are available year-round to people who meet the eligibility criteria (which vary by state). And people in any state are allowed to enroll in an individual market health plan if they recently lost – or are about to lose – other health coverage, since that’s a qualifying event. But people who aren’t eligible for Medicaid and who don’t have a qualifying event would normally have to wait until the fall open enrollment period (November 1 – December 15) to sign up for a self-purchased health insurance plan. The COVID-19 special enrollment periods – including the ones that were just extended in New York and Vermont – give people in this situation an opportunity to enroll in coverage mid-year, even if they don’t have a qualifying event.
Mid-year health plan enrollments increase dramatically in 2020 due to COVID-19
The COVID-19 pandemic has ravaged the American job market. Although the rate of job losses has slowed in recent weeks as businesses begin to reopen, there are still millions of Americans who are out of work. The majority of non-elderly Americans get their health insurance from an employer, so job losses tend go to hand in hand with loss of health insurance coverage – particularly alarming when the source of the job losses is a pandemic.
But the loss of an employer-sponsored health plan is a qualifying event that triggers a special enrollment period during which a person can buy coverage in the individual market – through the exchange or off-exchange. And in most states, Medicaid becomes available if a person’s monthly income drops below 138 percent of the federal poverty level (that amounts to about $1,467/month for a single person this year), even if they were earning too much to qualify for Medicaid earlier in the year.
It’s important to note, as Andrew Sprung explains here, that the availability of Medicaid for people experiencing a sudden drop in income is not as well-publicized as it should be. Nevertheless, Medicaid enrollment is increasing sharply as a result of the pandemic, even in states that haven’t expanded Medicaid. And in some states that have expanded Medicaid, enrollment is growing faster due to pandemic-related job losses than it did in 2014, when Medicaid expansion first took effect.
According to an analysis by the Georgetown University Health Policy Institute, Medicaid enrollment across a subset of 21 states grew by 2.8 percent from February to April. And the states with the sharpest Medicaid enrollment growth included Missouri and Florida, neither of which have expanded Medicaid under the Affordable Care Act.
HealthCare.gov declined to open a COVID-19 special enrollment period for people who didn’t have a qualifying event and weren’t eligible for Medicaid, but enrollment via HealthCare.gov has certainly climbed sharply this spring, due to enrollments among people who did have qualifying events (in most cases, loss of other coverage). With the exception of Idaho, all of the fully state-run exchanges opened COVID-19 special enrollment periods, and saw significant enrollment as a result. Several of them have published enrollment data stemming from their COVID-19 enrollment windows (generally including enrollments among people who had a qualifying event as well as those who did not):
California: More than 155,000 people enrolled (COVID-19 enrollment window continues through June 30)
Colorado: More than 14,000 people enrolled
Connecticut: More than 37,000 people enrolled
Maryland: 14,000 enrolled in private plans, plus about 26,000 enrolled in Medicaid
Minnesota: More than 9,400 people enrolled in private plans (and enrollment in MinnesotaCare, the state’s BHP, grew by more than 16,000)
Nevada: More than 6,000 people enrolled
Washington: 22,000 people enrolled
As expected, these numbers are all significantly higher than they would normally be outside of open enrollment.
Colorado legislature passes bill to make individual health coverage more affordable
Last week, we told you about Colorado Senate Bill 215, which had passed the Senate and been sent to the House. The legislation, which is designed to make individual health coverage more affordable in Colorado, has now passed the House and been sent to Gov. Jared Polis. If signed into law, the legislation will add another five years of funding for Colorado’s existing reinsurance program, and will also provide state-based subsidies to make coverage more affordable, particularly for people with modest incomes (up to 300 percent of the poverty level) who aren’t eligible for the ACA’s premium subsidies. This includes people subject to the family glitch as well as undocumented immigrants.
Missouri Chamber of Commerce announces support for Medicaid expansion
Missouri voters will have an opportunity to vote on Medicaid expansion this summer, with a Medicaid expansion initiative (Amendment 2) that will be on the state’s August 4 primary ballot. Late last week, the Missouri Chamber of Commerce endorsed Amendment 2, noting that expanding Medicaid would create 16,000 jobs per year for the next five years in Missouri, and would increase the state’s economic output by $2.5 billion (data based on this report from the Missouri Foundation for Health). The Missouri Chamber of Commerce tends to side with Republican lawmakers, but has endorsed Medicaid expansion despite the fact that Republican Gov. Mike Parson and many of the state’s GOP lawmakers are opposed to Amendment 2.
CMS gives insurers the option to pay MLR rebates early this summer
In guidance issued last Friday, CMS announced that health insurers will have the option to estimate and prepay medical loss ratio (MLR) rebates this summer. The rebates are normally paid in a lump sum by the end of September, or credited to premiums that are due on or after September 30. This year, CMS is allowing insurers to estimate the MLR amounts (which are expected to be much larger than they’ve been in prior years), and issue rebates to consumers earlier than normal. Especially for insurers that provide premium credits, this could help to offset premiums that people will owe over the next several months, making it easier for people to maintain their coverage.
Trump administration rolls back Obama administration’s nondiscrimination healthcare protections
Late last week, HHS and the Office for Civil Rights published a new final rule for how Section 1557 of the ACA should be interpreted. Section 1557 provides broad framework for non-discrimination in healthcare, but as with many aspects of the ACA, specific guidance was left to HHS. The Obama administration had published a final rule in 2016 that extended nondiscrimination protections to include termination of pregnancy, gender identity, and sex stereotyping. The new rule replaces the 2016 rule, and significantly rolls back the nondiscrimination protections that the Obama administration had put in place.
HHS had published the proposed rule change last summer, and received nearly 199,000 comments on its proposal (as opposed to about 25,000 comments that were submitted in 2015, when the initial Section 1557 implementation rules had been proposed under the Obama administration). But the final rule that was issued last week was mostly unchanged from what the administration had proposed last summer.
The final rule is wide ranging, and includes a rollback of the Obama-era requirement that healthcare entities provide tag lines in multiple languages on various communications they send to consumers. But one of the most significant changes was the elimination of nondiscrimination protections for transgender Americans in terms of their health insurance coverage and access to healthcare.
Just three days after the rule was finalized, however, the Supreme Court issued a landmark 6-3 ruling that protects the LGBTQ community from discrimination in the workplace. It’s unclear whether the Trump administration’s new healthcare discrimination rules can stand in the face of the Supreme Court’s ruling that discrimination “on the basis of sex” includes discrimination based on sexual orientation and gender identity.
Louise Norris is an individual health insurance broker who has been writing about health insurance and health reform since 2006. She has written dozens of opinions and educational pieces about the Affordable Care Act for healthinsurance.org. Her state health exchange updates are regularly cited by media who cover health reform and by other health insurance experts.
The post The Scoop: June 17, 2020 Edition appeared first on healthinsurance.org.
from RSSMix.com Mix ID 8246807 https://www.healthinsurance.org/blog/2020/06/17/the-scoop-june-17-2020-edition/
0 notes
Last Seen Blogs

kifs1990
Keeping It Firme Since 1990

marvelwomen-simp
🧍🏻♀️

fuxepovumega
Untitled

suikatto
mari

cutieaimirul
cutieaimin