#and the non birthing parent typically is encouraged to 'share' the pain with the birthing parent in order to help the process go smoother
Photo





Photos
#T'Pel#st voyager#st voyager art#I don't know what to say about this so I'll give you a headcanon#Both parents are typically encouraged to be present at the birth#and the non birthing parent typically is encouraged to 'share' the pain with the birthing parent in order to help the process go smoother#Picture Tuvok and T'Pel holding hands - both screaming#T'Pel art#or perhaps bc they 'share' they pain - birth is less of a scream-y process#Tuvok can also be pregnant as a treat (for him)#he and odo are the only star trek characters I'm interested in vis a vis pregnancy - both for different yet intersecting reasons#Tuvok#Tuvok art#[REDACTED] family shenanigans#Asil#Sek#Asil is playing with one of Janeway's family members on earth!#also one of the kids put flowers in one of their parents' teas#bea art tag
24 notes
·
View notes
Text
Please Don’t Leave Me

Title: Please Don’t Leave Me
Summary: Talking about our past is not easy. What happens when it’s finally time to share what you’ve been through with Henry?
Pairing: Henry x First Person Reader
Word Count: 1635
Warnings: Angst; mention of being yelled at, personal hurt, self-harm, attempted suicide, emotional neglect, parental abuse, beginning stages of a panic attack, anxiety, depression, loneliness, and fear of abandonment. (If there’s anything I missed, just let me know and I’ll add it).
A/N: HAPPY BIRTHDAY FREYA! I know it’s next week, but I’ll be off Tumblr because it falls on Thanksgiving this year. You asked me for this fic and I wanted to do right by you, as you’ve done so much for me. I love you, bish!

It had been a rough day. And not just your typical rough, I’m talking the kind of rough where you spill your coffee all over your blouse in the car, end up being late for work, forget your lunch, and get yelled at by the boss kind of rough. The kind of rough where every traumatizing past event in your life comes bubbling to the surface. The kind of rough where you want nothing more than to crawl back into your bed and sleep for seven years, and it’s only nine-thirty in the morning.
The one saving grace I held on to as I counted down the minutes of my shift was that Henry would be home tonight, waiting for me. God, I don’t know how I got so lucky, but somehow that kind and gentle soul had seen through the cracked and broken wall that I kept as my only defense mechanism, and had chosen me anyway. He knew some of my past and pain, but I hadn’t opened up about everything; I wasn’t ready to lose him, and I knew he’d be out the door once he heard it all. Just like everyone else. Perhaps that was selfish of me, but for once in my life, I knew what it felt like to be loved, and I was soaking in every ounce I could of that sweet nectar before it was gone.
Finally, finally, my work day was over. I headed to his place as fast as I safely could, anxious and burdened with unwelcome memories. The delicious smell of roast flooded my nostrils as I opened the door and Kal came bounding over. I noticed as I toed off my pumps and tamed the wild beast that Henry had built a fire, and gratitude filled my heart. He always seemed to know exactly what I needed, sometimes even before I did. I headed toward the kitchen, following my nose.
“Hey love,” Henry smiled wide, already pouring me a glass of red. He swallowed me in a warm embrace, his chin planted on the top of my head, and my body tucked firmly in his arms. I melted, sinking into the security of his hug and letting the stress of the previous hours wash away. I was here, he was home, and I was safe.
We ate quietly, talking here and there about random facts or tidbits. I pushed the food around on my plate, taking a bite here and there to satisfy Henry but I could sense him watching me carefully; his concern was evident, but he covered it well, masking it with simple questions or well-timed caresses. Even so, his next question caught me off guard, my fork halfway to my mouth.
“Will you tell me about it?”
The silverware clattered to the plate, forgotten in my fear. This is it, I thought, tonight’s the night I lose him forever. My chest constricted and I could feel the panic slowly rising, tears welling and threatening to spill. Henry quickly grabbed my hand and shushed me, cupping my face in nurturing kindness.
“You don’t have to,” he comforted, and I closed my eyes, exhaling the breath I hadn’t realized I was holding. Henry soothed his thumb over my cheek before pulling me onto his lap, cradling my head in his large hands. I burrowed deep into his chest, letting his scent wash over me in calming waves.
“I just want to help,” I heard Henry whisper. I sighed; he was right, it was time for him to know. I looked up at him, staring at that beautiful face that held so much promise. A face that said so much in just a look, with eyes that sparkled like the heavens whenever they landed on me. Once again, I wondered why his eyes looked like that when it was me they were viewing, but I shoved it aside. Self-deprecation would not help, not right now. Nodding softly, I tried to speak, but the words wouldn’t come out. I couldn’t tell him, not out loud. I dropped my head in defeat.
Henry shifted me off his lap, grabbing my hand and walking us to his desk. He sat in his gaming chair and patted his thigh, tugging on my arm. I hesitated, confused.
“Come here, love,” he encouraged, guiding me to sit. With both of us facing the computer, he opened a word document and offered me the keyboard.
“If you’re unable to say it out loud,” Henry crooned in my ear, kissing softly under my lobe, “Then write it. I’ll read it as you type, and neither of us has to say anything.”
This man. I swear to god. Relief flooded through me, though anxiety pounced instantly as I was reminded that once we were done, he would be gone. No one else had stayed, my problems were much too great... Why should he be the one to bear the burden of me? I took a deep breath anyway and eyed the screen, my fingertips trembling over the instrument of my demise.
Where should I even begin? Should I go all the way back to the beginning, to my birth? How I was nothing but a mistake, and every day I was reminded as such? Or maybe I should tell him what the scars are from? Perhaps I should simply tell him about failed relationship after failed relationship, both romantic and non. Those are all fun tales, I had no doubt he’d love to hear all about them. Maybe he wanted to know the amount of times I’ve come close to admitting defeat and ending everything. Spoiler alert… that number’s higher than it should be.
I swallowed thickly and began typing, slow and hesitant words forming on the page. Every thought was carefully constructed, worked over in my mind at least five times before I allowed it to leave my fingers. Henry’s comforting arms were wrapped tightly around my waist, his chin nestled on my shoulder as he read what I shared. Tears slowly brimmed in my eyes, kept at bay only by sheer force of will. Each stroke of a key sounded like a hammer hitting the nails in our relationship’s inevitable coffin; surely he wouldn’t, couldn’t love me after this. No one could. It’s simply too much for anyone to bear, too awful… too hard.
And yet in my ear were the sounds of something different. Encouraging grunts, empathetic hums. Henry kept his promise, he never said a word except for one small sigh of “oh, love” as I hit a particularly difficult moment. His hands rubbed my sides, kisses left tiny wet imprints on my cheek, and every now and then he would squeeze tighter, small reassurances to keep going.
The words started pouring out of me. I couldn’t have stopped myself if I tried; Every struggle, every loss, every tiring moment; every single thing that had ever happened to me found its way into that document in a flurry of clacking plastic. My hands moved of their own free will and the tears started to flow; long, silent trails of pain releasing years worth of pent up anger and hurt. The salty drops fell onto Henry’s forearms but he just left them there, rooted to his task of protecting me. I would miss how safe I felt in the protection of his arms.
The final sentence fell out of my hands, and I immediately turned and buried my face into Henry’s shoulder, bitter sobs wracking my frame as I clung to his neck.
“Please don’t leave me,” I begged, ashamed of myself for being so needy and undesirable. I expected him to untangle himself from my arms, to get up and open the door to excuse me from his home. To force me to leave his life and never return.
The last thing I expected was for him to burst out laughing.
I snapped my head up and stared at him in horror, which only made him laugh harder.
“I’m so sorry,” he wheezed, “I really shouldn’t be laughing. It’s just… I know why you think I would leave you, it’s all right there on the computer, but you have nothing to worry about.”
Henry wiped his eyes and mine and cupped my face, still chuckling.
“You think so little of yourself that you can’t see just how worthy you are,” he murmured, adoration and mirth mingling in his eyes as he tucked my hair behind my ear. I furrowed my brow and pressed my face into his palm, relishing the cooling sensation of calm that his skin brought.
“I know what it’s like to feel how you do,” Henry went on softly, “To feel unwanted and undeserving. But I’m not going to walk away from a flower as strong, as rare, and as beautiful as you just because she’s got a few bruises. I love you just the way you are.”
His admonition shocked the both of us. He loves me? I tried to process what he’d just said, but my mind was raw and I couldn’t think straight. He loves me.
“Yes, I love you,” Henry repeated as though he could read my thoughts, clasping my jaw and looking me straight in the eye. “I love you, and I’m not going anywhere… I’m not going to leave you.”
I smiled widely as tears spilt over once more, happiness bursting from my heart. With anyone else I’d be doubtful, I’d have hightailed it on my own after a proclamation like that before the other shoe dropped... before they could hurt me worse. But this wasn’t anyone else, this was Henry. And being with him made me brave, which is why I found words leaving my lips that I never thought I’d ever say again.
“I love you, too.”
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
#henry cavill#henry cavill fic#henry cavill fanfiction#henry cavill rpf#angst#fluff#birthday fic#littlefreya
389 notes
·
View notes
Text
Basic Reproduction, Pregnancy, and Childbirth info for fanfic writers
As a mom myself as well as a future midwifery student, one thing that can really get me out of the escapism of fanfiction is the inaccurate or awkward depiction of pregnancy and childbirth. Whether because it is overly simplistic, written traumatically, or shares misguided ideas surrounding fertility and childbearing, it just really has me not enjoying the content despite it being a good story otherwise. The downside of being well-versed on a certain topic is that you become quite good at seeing misconceptions about it in fiction!
And especially since so many fanfic writers are either too young to be parents or are childless, I felt: hey, why not help out a lil bit? I love your stories and growth as a writer, so I think it’s only fair that I can contribute in some way. It’s not so much a how-to guide, mostly just basic resources to study from or refer to, but I do have a small commentary here and there.
I tried to make the list as encompassing as possible, to include resources that could help with fantasy, sci-fi settings, as well as ideas for non-human characters. So this list is for more than just typical human stuff!
You can read more below the cut:
Fertility Awareness, Health, and Birth Control:
This part is important to fully understand how and why a pregnancy can occur. Contrary to what a lot of people learn, you actually CAN’T get pregnant on any day of the menstrual cycle -- and birth control can fail in various ways even when used correctly. I figured this would help writers better describe how a character falls pregnant by way of BC failure, and not keep it so vague and mysterious. And hey, if that means free sex ed for teen and adult writers, then more power to them. :)
fertilityfriday.com
larabriden.com
avivaromm.com
factsaboutfertility.org
bedsider.org
Pregnancy:
Pregnancy can vary wildly in experiences, so I tried to include mostly resources for pregnant parents that take this into consideration. You can also find info on pregnancy stuff in resources listed in the childbirth list!
babycenter.org (they also have info on raising kids up to five years of age!)
americanpregnancy.org
womenshealth.gov
Childbirth:
My favorite part! Here you will find lots of birth stories -- all quite varied -- and will give insight into how birth can play out. The resources above also discuss childbirth.
midwiferytoday.com
birthwithoutfearblog.com
spinningbabies.org (they have a blog you can read from)
evidencebasedbirth.com
A really neat article about a really neat midwife! https://www.healthline.com/health/betty-ann-daviss-midwife-breech-births
You can also search for birth videos on youtube. Just be careful -- they are often “graphic” in that they don’t blur out genitalia or blood (both of which is normal in birth btw, but it may come as a shock to some out there) and I found a few (not many, but enough) birth videos where women were verbally harassed by care providers. Just sharing this so that you can decide for yourself if it’s worth searching.
Postpartum (post-birth recovery):
Most of the pregnancy and birth info I post above will comment on postpartum recovery and traditions. However, here are more specific resources that can be useful for writers.
slowpostpartum.com
postpartum.net
postpartumresourcegroup.net
article comparing postpartum recovery traditions around the world: https://www.scarymommy.com/postpartum-care-is-better-other-countries/
LGBT representation:
I know a lot of fanfic writers use their craft to share their desire for positive LGBT stories. If this is your thing, here are some parenting and pregnancy resources that real LGBT people use when growing a family; it will help keep the realism respectful and accurate when writing for your LGBT character(s).
La Leche League on chestfeeding/breastfeeding for LGBT parents: https://www.laleche.org.uk/support-transgender-non-binary-parents/
You can follow the Queer Doula on facebook for ideas and information on LGBT birth as well, they are Non-Binary: https://www.facebook.com/TheQueerDoula/
Badassmotherbirther and The Warrior Within Birth Services also occasionally share LGBT posts and encouragement (also on facebook)
POC-specific resources for cultural sensitivity:
I hate lumping all non-white cultures into one “POC” grouping, but I felt this would be the easiest way to keep the list organized. I included organizations run by and for Indigenous and Black women, since they face the most discrimination in the birthing world. I was going to link resources for Latino families as well but I couldn’t find any, sorry. :(
Indigenous Breastfeeding Counselor: https://www.facebook.com/IndigenousBreastfeedingCounselor
Indigenous Birth Workers Network: https://www.wisewomengp.org
Wuttahminneoh Birth Work (I am so sorry for the funky link facebook will literally not give me another URL): https://www.facebook.com/heartberry.bw/?__xts__[0]=68.ARAsiZyY90fZivjKJkF0MtcjMTiRhOHOT0Q-QiJe3FTwFJfBpKtNDMsQQLog8A2Uv0VC7ki5CRKR9Oi8RNuR2RHAHVmAm3aHQxTmuo5tvpFu4i7lZfMlnFmo8LTVc8-Qfd6wnA1itDCh4o4qtc45MUJI9NZh4lvVBXhLbnMGck6AiDUzFjrIyDikppt4lnX1jjFzkx-g5QCapbeX3BqpuWWvtHpw35L7QzbmOoyW-1iFi4S2s997u795VFAKLVEkqWTFyzmZhJdZbGd3gzt2lzJ-jB1crYe-y-eaLrbnBYmfar8UYToVNu-hOCVojr3pnLfaZn-tIwxwiXyBXz-jnwkCt52mrKaVagcK6l6GkzE91pN8GncBkQ
A Story of Indigenous Birth Justice: http://micemagazine.ca/issue-two/story-indigenous-birth-justice
National Black Midwives Alliance: https://blackmidwivesalliance.org
Black Women Do Breastfeed: https://blackwomendobreastfeed.org
Different types of reproduction in the animal and plant kingdoms:
I’m not much an expert in this area, though I do find it fascinating. If you would like to use ideas from nature for head canons about non-human races, then go nuts -- the natural world is full of inspiration!
Plant-based biology:
https://byjus.com/biology/plant-kingdom-plantae/
https://www.britannica.com/science/plant-reproductive-system
Animal-based biology:
https://www.britannica.com/science/animal-reproductive-system/Sponges-coelenterates-flatworms-and-aschelminths
https://byjus.com/biology/animal-kingdom/
Asexual vs Sexual Reproduction:
https://biologywise.com/asexual-vs-sexual-reproduction
And youtube has a lot of documentary videos of animals giving birth if you want to check it out.
A note on traumatic/dramatic birth scenes:
I, personally, have a special request:
PLEASE stop writing traumatic birth scenes.
No death of the mother or the baby. No focus on out of control pain or death by infection or “““blood loss”““. No birthing during a battle or other climatic event.
In the United States and other parts of the world, millions of women struggle with PTSD or postpartum mood disorders due to mistreatment and trauma experienced at birth, and many more are simply surrounded by negative depictions of birth in mainstream media.
Women are told, every day through common media tropes, that birth is scary and anything can go wrong and that they have no choice in how birth may or may not turn out. While it is true that something may require medical attention, most pregnancies are low risk, and many complications at birth or after birth occur because of medical negligence or lack of informed consent. But this mistreatment and negligence is often put into the spotlight as a way to sanctify care providers and scaremonger women about their bodies.
If you would like to do a small part in normalizing fertility, pregnancy, and birth, then I humbly request that you do so by keeping birth simple and refreshingly non-traumatic. If you absolutely MUST have a dramatic birth scene, at least keep it accurate to what can actually happen, and warn your readers ahead of time on where to skip the scene. An author did that for a trauamtic birth in a fic I read, and it was a lifesaver for me. I did not have to re-live my own trauma from my first birth, and instead was able to focus on the story outside of it.
Otherwise, I would much prefer to read a silly, happy, or even just plain old NORMAL birth scene myself. I never see this. Often the birth scene is either traumatic/dramatic as an excuse to hurt or kill off a character, or it is comedic to make fun of natural birth. For once, I would adore to see a birth just as it is: a powerful moment where a mother (and father or other parent) meets her child, whether naturally without medical intervention or during a healing, family-centered c-section. When it comes to positive and accurate representation, birth is sorely in need of it! If you have a hard time of knowing where to start, just read the many positive birth stories out there -- they are great for inspiration and encouragement.
Thank y’all for reading, it means a lot. :)
**NOTE** I may expand this list in the future. If you would like to add anything here, please let me know.
36 notes
·
View notes
Text
What is a light worker?
If you’re familiar the online spiritual world you’ve probably seen the term lightworker for it has been increasingly used in recent years. The term lightworker was first coined by author and teacher Michael Mirdad in the early 80s. Later, in 1997, Doreen Virtue released the book The Lightworkers Way.
The simplest way to describe lightworkers would be as ones who feel an enormous pull towards helping others. Lightworkers are also called crystal, rainbow, or indigo children, Earth angels, and starseeds. These spiritual beings volunteer to maintain a high frequency for the Earth and commit to serving humanity. There are separate definitions for each of the types of lightworkers listed here and I will discuss. Each type is slightly different. Some people that use these labels do not like being called lightworkers yet may be fine with star seed. This kind of stuff is silly and why I don’t like the use of labels. I don’t like the idea of putting myself in a defined box.
I prefer an umbrella term like lightworker to the specialized terms that divide us further. I see labels as are guidelines and not hard fast rules. Too many individuals see the world as black and white when things are actually typically a shade of gray. At the end of the day each situation and each person is fully unique. This is a good thing and we must learn tolerance. Earth is big enough for all of us to live here together peacefully.Lightworkers are the people that incarnated here to change the world. It is time to act.
Lightworkers often feel greater kindness and compassion towards others from birth – chances are that they’ve helped several animals and other living beings in distress from a very young age. Lightworkers tend to be sensitive and empathetic. Hence they feel sadness and anguish for the misery that dwells in the world. They do best in professions wherein their empathetic nature can be used to assist those in need, like nursing, therapy, rehabilitation, healing, care-giving, veterinary services, etc.
Lightworkers are intuitive and driven by their internal guidance. They can often perceive the emotions and needs of other living beings, which enables them direct their healing powers towards those who need help. They believe in carrying out coordinated efforts to dispel or chase away negative energies and consciousness by using their positive energies and healing powers.
Not all lightworkers realize the nature of their spiritual calling right away. It often takes some intuitive guidance – as well as going through the process of self-realization and discovery – to realize that their mission on Earth is to make a positive impact in whichever way they can. Given that they're faced with the same limitations and obstacles as other mortal beings, this manner of spiritual awakening and tuning into their inner light can sometimes take years for a lightworker. Odds are good the lightworker has always felt different from his or her peers.
If you’ve read about lightworkers and wondered if you could be one, you can only find the answer through introspection. Lightworkers can possess strengths and core abilities in one or more areas of service. Tuning into your inner self will help you understand what your unique gifts are and the kind of lightworker you may be.
The following types may help someone identify where their inner calling lies:
Spiritual guides and healers
Lightworkers who are driven towards serving living beings and the Earth through healing using mental, physical, emotional or spiritual approaches fall under this category. They are often highly perceptive of feelings and emotions in others, and characteristically can alleviate pain and hurt within a few minutes of time spent with people or animals.
Their sensitivity towards pain could often render them fatigued or overwhelmed, and it takes some conscious moderation to keep this tendency in check. Professions such as doctor, nurse, or reiki practitioner would fall under this category.
Psychics and seers
Using their elevated awareness and intuitive powers, one can develop psychic sights to be able to see beyond the material form and illusion. Many lightworkers can predict future events and tend to concentrate their efforts on positive outcomes, with the end goal of world peace and harmony.
Gridworking and gatekeeping
A grid here refers to a unit that connects all awakened hearts and sacred sites on Earth using lay lines. Gridworkers and gatekeepers are advanced lightworkers who specialize in clearing work, their main role being opening of inter-dimensional grid lines to let light and love flow through. Gatekeepers encourage peace, kindness, positive energy, and fairness for all living beings.
Manifestors
Also known as divine blueprint creators, manifestors are a type of lightworker that are expert at channeling their intrinsic energy to attract what they want. Their mission to make the world a better and peaceful place enables them to manifest awakened collective consciousness for humanity.
Guides and messengers
Some lightworkers possess a unique flair for spreading important messages to the world. They concentrate their efforts in areas where their inner light and magnetic presence can make greatest impact on others by communicating messages of love, peace, spiritual awakening and enlightenment.
Motivational speakers, bloggers, artists, teachers, writers, life-coaches; those who strive to serve humanity through their words, actions or work can be categorized as messengers.
Transmuters
Also known as neutralizers, these lightworkers specialize in dispelling negativity, thus restoring neutrality and balance back into the world. Neutralizers may work in favor of the entire collective consciousness, or even help people release or heal negative karma from their ancestral lines.
Dreamers and travelers
These lightworkers can never accept the status-quo, and always strive for new solutions and adventure. They learn to push limitations and manifest light during dreamwork, creating boundless capacity for change along multiple dimensions of the Earth.
Adventurers and ascension guides
Adventurers are always on the lookout for newer possibilities, driven by belief that better things await if one just looks beyond the obvious. Along with ascension guides, they work towards creating higher inter-dimensional possibilities and broadening mankind’s vision for future.
You can be more than one of these. I myself identify with transmutor, guide and messenger, dreamer and traveler, healer, and occasionally a manifestor. I identify most with transmutor and guide and messenger.
The specific kinds of light workers I said I would address earlier are indigo children, rainbow children, Earth Angel, Starseed, and I’m going to add in crystal children. To my knowledge these are the most common, if not only, specific kinds of light workers. They’re the only ones that I know of and the ones that I found information easily about.
Earth angel
Earth angels want to align with pure, loving energy, and by doing so, help others to find their highest self in this lifetime. They want to transcend the problems and heartache, and live in true harmony with the Divine. They have good intentions for themselves and the planet, but often get frustrated with our current state of affairs.
Starseeds
StarSeeds is the umbrella name for a group of people who are said to have been sent here from all areas of the universe to help the Earth and humanity. They are reported to possess psychic, spiritual, and other extrasensory abilities, and are bringers of peace, topplers of corrupt systems, and shifters of dimensional consciousness, now and in the future. Some feel these children have come here on special assignment to assist in this rebirth into a higher dimensional Earth.
Starseed children may be divided into the three categories of indigo, crystal, and rainbow individuals. Star children have chosen specific family and/or parents who will help them develop their natural abilities and heal ancestral lines.
Common traits of starseeds are said to include clairvoyance, claircognizance, clairaudience, clairsentience, the propensity to trip electricity, manipulate the environment with the mind, telepathy, high intuition, heal with energy, detect danger, travel out of the body, act as channelers, and the ability to download information from other planets. Also listed as traits are talents that a great many would still be resistant to believe, including the ability to levitate and teleport.
Indigo children
Indigos get the name from their indigo colored aura. Indigo children began appearing en masse in the 1980s. The indigo aura hadn’t ever been seen before.
Indigo children share traits that include a strong calling to make the world a better place, an innate knowledge of better ways to do things. They are natural “system busters” with a non-responsive attitude toward controlling and/or authority figures, a feeling of natural superiority, and an innate love for nature, plants, and animals. Indigo children are naturally intuitive, have a desire for a fair and just world, stand up (maybe alone) for what they believe in, have an interest in living a life of meaning instead of just making money, are sensitive in both a physical and emotional sense, and regularly have unusual things happen to and around them.
Other Indigo traits have been described as having a high IQ, self-confidence, resistance to authority, “old soul” qualities, sensitivity to chemicals and fluorescent lights, and disruptive tendencies.
Crystal children
Crystal children are another category of human beings known to follow their hearts as idealists in a world limited and troubled by materialists. This means that crystal children are apt to flow with consciousness, rather than forcing their way through life and hardships in search of material success. Their ultimate goal seems to be firmly established in making the world a better place. Like Indigo children, crystal children also exude an “old soul” persona.
Crystal children are the offspring of indigos and began to incarnate in greater numbers at the turn of this century. They commonly have a penetrating gaze, sometimes possess usual-colored and often round eyes; are sensitive, both mentally and physically; suffer from allergies and sensitivities caused by environmental factors; are spontaneous, and sometimes act without thinking through the consequences; love to climb; have a good sense of balance; are natural huggers (even with people they only just met); have no awareness of personal boundaries because they feel connected to all of humankind and, indeed, all living things; are healers and psychics; love music and singing, but hate loud noise; aren’t comfortable in noisy, over-crowded places and suffer from sensory overload; are badly affected by negative events, both in their personal sphere and worldwide; exude love for their family, pets and their friends; and are autodidacts — preferring to teach themselves what they want to learn (rather than what they’re told to focus on).
They appear to function as a group consciousness rather than as individuals and live by a law of oneness. They are advocates for love and peace on this planet” and “are mostly born with access to psychic gifts such as clairvoyance or healing.
Rainbow children
The rainbow children are the third generation of special children that have come to help humanity evolve. The Rainbow children are generally born in the year 2000 and above. The few Rainbow children that are here today are born from early Crystal scouts that were born in the 1980’s. As the name implies, the Rainbow children come to earth with a rainbow aura.
The Rainbow children bring joy and harmony to their families. Unlike the Indigo and Crystal children, the Rainbow child is born to smile, which is accompanied by their huge hearts that are full of forgiveness. The Rainbow child generally recovers from the state of negative emotion quickly. This is also an important key that they hold, emotional mastery. Rainbow children are psychic and have the ability to read people’s feelings. They have strong wills and strong personalities. Their gifts do not stop there. They are known to be natural healers and instant manifesters. It is said that whatever they need or desire they can instantly manifest. The Rainbow children are thought to be the builders of the New World, using Divine will.
I’m an indigo, my son an indigo, and my youngest a rainbow. (Her dad is a crystal and I’m an indigo)
If you feel that you are a light worker you should learn how to maintain the highest frequency you can, protect yourself from negative energies in this world, and work to learn and use whichever type of light work you identify with the most. The world at times feels as if it is being consumed by negativity and we lightworkers need to help uplift the consciousness.
I prefer to say those of us with heart centered consciousness is who light workers truly are. It does seem as if the star seeds are the ones that have woken up. I feel if this video applies to you will probably be drawn to watch it and whatever label you choose doesn’t matter. We are in need of uniting and it’s more important that we live our best life to help the earth and humanity as a whole.
2 notes
·
View notes
Text

[CLOSED SPECIES]
I would like to officially introduce a creature species I've made. They arent really new since I've had them for years and posted them several times on a couple different blogs, but they were originally just one, not really a species, but I love them and i just wanted to expand on them and what they were, so here we go.
Please read under the cut for full info on budbugs.
BUDBUG is the species name, named after the original, Pillbug.

(this is Pillbug^)
Pillbug was the only of their kind, created in a lab for testing purposes, and not good ones. They were practically tortured, cut open countless times, experimented on, ect. They were made to be docile and obedient, no aggressiveness at all, to the point of almost being just a living stuffed animal.
Pillbug is quiet, and pretty much completely incapable of choosing to do anything. They will wait for someone to tell them to do something, sitting in the same spot till they starve to death. Think of the sims with free will option turned off. This is specifically Pillbug, the first and original, and does not apply to the whole species. All budbugs come from Pillbugs DNA, so, in a way, Pillbug is the mother/father to all of the others.
now onto the species:
BUDBUGS
Scientific name:Vitula mollisparva
CLOSED species
Lifespan: unknown. Oldest living budbug is 36 (human) years old.
Average height: on all fours:around 1 foot. Standing: 2 feet(bitty versions also available)
Average weight:15 pounds
Sex: Budbugs are a genderless species, and cannot reproduce. if you adopt one, you can choose any pronouns youd like to call them, they don’t care.
DIET: they can pretty much eat anything. Their diet is whatever is offered to them or available, including things like bark. They have no specific needs, but there was a recorded overall preference of fruit and sweet things. Sweet milk is the number one way to attract them. It seems to be their absolute favorite, warm or cold. They have some semi-sharp molar like teeth in the back of their mouth that they use for crushing/chewing harder materials.
YOUNG: a hatchling(called pups) will not have vision, or be able to walk. they have feeling and scent to go on, much like a puppy. they have slight hearing that comes through to them as muffled sound. they are bottle fed milk like substance and sugar water(or a mix of both) for 3-4 months.
since budbugs dont have the ability to reproduce, nor a gender, there is no mother to nurse them and is done by bottle. there is the possibility of an adult budbug attempting to nurse young, but it’s unlikely theyll produce milk in time before the young starves.(we of course have the ability to make ‘nursemaid’ parents, bottle feeding the hatchlings until their milk comes in from stimulation((e.g pups attempting to nurse on them for prolonged times))
It's best to feed them mushy like food up to 6 or 7 months old. eyes open around 2-3 weeks old, along with better hearing. they start walking shortly after, 4-6 weeks. they will follow after people or animals in a fashion similar to ducklings, seeking a bigger ‘parental’ figure to protect them and make small chirp noises.
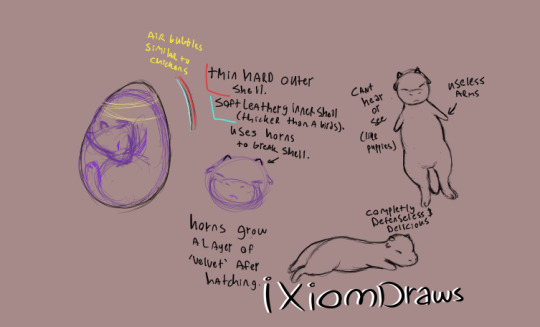
PLANT GROWTH:
Typically has any type of plant matter growing on their head, sometimes it can trail down their back and tail or even have random patches of plant matter elsewhere. the plants that grow on them are a part of them, for instance- cutting off a flower will cause a pinkish blood drop to emerge. They don’t seem to feel the pain of cut flowers/plant matter, nor does it need to be bandaged or treated, its fairly similar to regular plants in that aspect. [note:please do NOT use a mower or weedeater on your budbug]
The plants that grow on them are similar to regular plants, but often are more 'sturdy' and a little tougher to break/cut. This can vary somewhat by the individual, some will have more fragile type plant matter that easily comes off, others may have plant matter that is thicker, rooted and more connected to them. Usually youll know depending on plant type, thicker looking stems and such are most likely more rooted and a part of them and we highly recommended not trying to pull any plant matter out/off of them.
its best to let the plant naturally die/fall off, and typically the plant doesnt overgrow to a point of causing difficulty to the budbug.
BEHAVIOR:
a common site is seeing the budbug grooming itself; licking like a cat and patting or somewhat 'pulling' on leaves or whatever plant matter they have, to shed the dead leaves, ect. If left with water, they might bathe themself, somewhat like a hamster or cat, except they dip their arms in the water instead of licking them.(if water is available)
They have horn-like nubs on their head covered in fur/felt, the horns stop growing at a certain point and then remain that way for life. Their horns have no use other than for hatching out of an egg at birth. Its extremely rare for them to be aggressive toward anything, including others of their species. They’re very sharing, and around their own kind, they will often groom each other, make soft calls, and sleep in piles.
The few aggressive ones only did some mild growl like sounds and avoid the others, most of which stopped within an hour and joined in the regular activities.
There have been no cases of any attacks or biting, whether to their own species or other animals/people.
Meeting other species, they wont typically make the same call noises as they do to each other, but will still act friendly and try to sit next to or sleep with, and even try to groom them.
They’re quiet, almost mute. They can make soft call noises and various other light toned sounds, they cant bark/moo, and even in distress or extreme pain, they typically only make soft whine noises or stay silent. they also make rumbling like sounds similar to a purr. They have a very high pain tolerance, some people might even claim they cant feel pain, but trust me, they do.
heres some similar noises they can make(budbugs sound a bit more soft though, kind of like cooing? if that makes sense)
[1][2][3][4]
urgent call/trying to get attention(rare)
young/baby chirps
distress/pain call(rare)
Their arms are flipper like, though still usable as paws if needed, they prefer walking upright. their eyesight differs greatly, some excellent, some poor. If you don’t like things staring at you, this isnt the pet for you. They are very observant, watching others is probably like tv to them. smell is their best sensory, along with hearing. their fur type can vary from otter-like(waterproof) to very fine silky soft fur and many others.
Personality:
trusting, obedient, friendly, happy, quiet, patient. They will spend the majority of their time observing their surroundings or others.(some are 'lazier' than others, falling asleep instead)
Intelligence:
varies. They can learn a lot, but they typically have low functioning free will and require commands or encouragement to act on things.
As an example, we set a waterer that works similar to a fountain, needing a button to be pressed to release water for drinking. The creature sees us operate it and with mild encouragement, will press the button and drink. We leave them alone for days, and while they know how to operate the device, they do not, simply waiting.
It took several days of being completely alone before they finally activated the water by pressing the button. By their straightforward action, we could tell they knew how to operate it and it wasn't an accident. This test was ran on several others, all similar reactions. On average, only 3 out of 10 would react sooner, within 24 hours, 5 took about 3-5 days before reacting, and 2 passed out from dehydration and had to be taken to medical. (test was ran on 5 groups of 10)
Many other tests provide similar information: they typically wait for something to encourage or command them to act, even on simple survival such as food and water. If it isnt offered to them, they seem to get confused and wait for an offering, even if theyre next to a stream.
In some tests conducted, when in groups, they will follow suit after others, even of different species. e.g, one walks to a stream to drink, they follow suit to drink as well. It’s possible this is a faulty instinct of survival, watching others to drink or eat something to make sure its safe for themself, the faulty part being that even once they know a source is safe, they’ll still often wait for encouragement to engage.
thankfully, about 74% of them will get over this faulty instinct over time and regular encouragement towards a water/food spot. moving their dish or having a non-regular feeding area can cause this faulty instinct to return or worsen. it’s recommend to have a designated water and feeding spot set up for them to help them overcome that behavior.
other than that, they are extremely adept at learning commands and copying (to the best of their ability). they learn tricks incredibly easily. (e.g, roll over, sit, fetch, ect)
again, this is a CLOSED species. you do not have permission to make one of these without my consent.
below are permissions if you get one-
RETURNS: If you decide you do not want your budbug anymore, you can message me and I’ll take it back, either keeping it or putting it back up for adoption. but i can not and will not refund you. Which should be obvious, but just in case, i’m stating it here.
PERMISSIONS:
-you have complete permission to draw/write/ect of them. harm/violence/gore is allowed.
I dont mind gore or sad angst stories, so whatever you want to do with them once bought, you can.
However, you do not have permission to include them in anything sexual. if they’re just being the pet that watches their owners do it, like how cats sometimes do, then that’s fine. But absolutely no fucking the budbugs or other sexual activities with them.
-You do not have permission to resell them or sell merchandise with them on it.
This post will be updated as needed if anything changes to their species info. Last update: 10/18/2018
#creature#species#closed species#animal#fantasty#budbugs#budbug#adoptable#adopts#in a soon future post
27 notes
·
View notes
Text
Chapter 5—Breaking the Cycle: The Substance-Dependent Client as Parent/Caregiver
Many adults with substance abuse disorders were abused or neglected during childhood. Although most do not abuse their own children, they are at increased risk of doing so (Kaufman and Zigler, 1987). When children who are victims of maltreatment become adults, they tend to repeat a dysfunctional cycle and often lack mature characteristics: the ability to trust, to make healthy partner choices, to manage stress constructively, and to nurture themselves and others (Magura and Laudet, 1996). In addition, substance-abusing women report higher rates of childhood sexual abuse than non-substance-abusing women, and these women report increased episodes of abuse from their adult partners as well. Domestic violence is a reality in many of these families (Browne and Finkelhor, 1986; CSAT, 1997b; Ryan and Popour, 1983). Research shows that childhood maltreatment has developmental, behavioral, and emotional consequences that continue into adolescence and adulthood. Researchers are now examining childhood abuse and neglect as an indicator of the potential for substance abuse (Feig, 1998; Felitti et al., 1998; Whitfield, 1998). For example, one study (Felitti et al., 1998) found that medical patients with adverse childhood experiences (i.e., traumas) had a higher incidence of health disorders, including problems with alcohol (7.4 times that of control patients) and problems with illicit substance use (from 4.7 to 10.3 times that of the controls).
Sheridan proposes a model of intergenerational substance abuse, family functioning, and abuse and neglect that reflects both the direct and indirect relationship between parental substance abuse and family dynamics, child and adult maltreatment, and second-generation substance abuse. She indicates that unless effective intervention occurs, there is an increased likelihood that these patterns will be repeated in the next generation ( Sheridan, 1995). Parental substance abuse presents not only a risk for intergenerational transmission of substance abuse disorders but also substantial risk for repetition of problematic parent-child interactions, including abuse and neglect (McMahon and Luthar, 1998). These studies indicate increased risk factors, and counselors should not assume that their clients with histories of child abuse are mistreating their own children. The family system may function well enough when stress is low. Substance-abusing parents are already severely hindered in their ability to provide a safe and nurturing home to their children (U.S. Department of Health and Human Services [DHHS], 1999); increased stressors such as loss of jobs, poverty, and illness will only exacerbate the situation.
Go to:
Who Abuses and Why
Nearly one fourth of physical abuse and more than half of sexual abuse of children occur at the hands of adults who are not the victims' birth parents. They may be other relatives, caregivers, or partners. The likelihood of this kind of abuse is far greater when parents are using substances and, consequently, cannot provide adequate care for and supervision of their children (Reid et al., 1999). However, because most child abuse occurs within families, the discussion here will focus on parents. Providers should also note that most child sexual abuse is committed by males (Finkelhor, 1994).Research on parenting styles and attitudes of abusing parents indicates several distinct characteristics shared by parents who abuse their children. These include seeing child rearing as difficult and not enjoyable, using more controlling disciplinary techniques, not encouraging the development of autonomy in children while maintaining high standards of achievement, and promoting an isolated lifestyle for themselves and their children (Briere and Elliott, 1994). Observational studies indicate that abusing parents are less supportive, affectionate, playful, and responsive to their children and are more controlling, interfering, and hostile; they have fewer pleasant interactions with their children (Magura and Laudet, 1996). Abusive parents tend to "parentify" their children, expecting them to take on the role of caretaker. Because they do not have sufficient knowledge of child development, their expectations of their children's behavior are often too high, leading them to adopt inappropriate disciplinary practices (Wegsheider, 1981). In fact, most abusing parents do not help their children adapt to the major developmental tasks, such as regulating their sleep habits, preparing them to separate from their parents, enabling them to explore their environment safely and with appropriate limits, and making choices and becoming more independent (Levy and Rutter, 1992; Mayes et al., 1997; Rodning et al., 1989). Nor do these families successfully resolve issues of attachment, emotional regulation, autonomy, peer competence, or school and work competence (Cicchetti and Lynch, 1993).Damaged Parents: An Anatomy of Child Neglect (Polansky et al., 1981) summarizes the characteristics of abusing parents identified by researchers in several different studies:
The prevalence of poverty, substance dependence, mental illness, and large numbers of children per family
Feelings of inadequacy and self-reproach, often related to early negative experiences
Depression, difficulty putting sadness and needs into words, and anxiety discharged into activity
Serious arrest in development, a sense of incompleteness resulting from a failure to internalize a separate identity (manifested by clinging to children), the presence of other abusive and unfulfilling relationships, and an inability to tolerate being alone
A fear of taking responsibility and making decisions
Severe difficulties in verbal communication
Difficulty in seeking or obtaining pleasure
Extreme narcissism, gross immaturity, dependency, and an impaired ability to empathize with a child's needs
The Polansky study cautions against overgeneralizing neglectful or abusive parents. Also, it is important to remember that poverty may be a common characteristic because poorer parents are more likely than affluent parents to be involved in public systems, which are mandated to report abuse cases. (Affluent parents tend to access private systems in which reporting is not required.) Nonetheless, the development failures above can signal to a counselor both a potential risk for child abuse and the possible effects of maltreatment in a parent's past.At the same time, certain resiliency factors have helped many children avoid the cycle of abuse. These include being able to fantasize about another
time or place, being able to read and learn about a better time and place, realizing that they are not responsible for the abuse directed at them, and having an adult in their life for a considerable period of time who sees them in a positive way. Resiliencies can be grouped in the following seven categories (Wolin and Wolin, 1995):
Insight begins with a sense that life in the troubled family is strange. Such insight can eventually protect the child from a tendency to internalize family troubles and feel guilty.
Independence is the child separating herself from the troubled family.
Relationships fulfill needs that troubled families cannot meet.
Initiative is the desire to overcome feelings of helplessness that a child can succumb to in the troubled family.
Creativity is the ability to take pain and transform it into something artistic and worthwhile.
Humor allows the child to make the tragic into something comic and laugh at his emotional suffering.
Morality is developing a set of principles that differentiates bad from good both inside and outside the family.
Traditional models of parenting may serve as a useful context for understanding how a client views his own parents and the implications for repeating their behavior. The three major types of parenting styles have been described as authoritative, permissive, and authoritarian (Baumrind, 1971). The authoritative parent maintains reasonably close supervision, sets consistent standards, and keeps track of children without being overly directive. A permissive parent allows children to do as they please and sets few limits or guidelines, which may result in safety problems; this is often a neglectful parent. The authoritarian parent is directive and rigid and relies on punishment as a major disciplinary method; within this model, this is often an abusive parent. However, parents typically combine these styles when interacting with their children, and the effectiveness of the approach used depends largely on the family's culture, community, and environment.Paradigms from developmental literature can also be useful in understanding the effects of environmental disturbances on the maltreated child. Belsky's ecological model, for example, contains four levels of analysis: (1) individual development, (2) family systems, (3) community, and (4) culture, all of which interact with each other and influence whether or not maltreatment will take place (Belsky, 1993). As this model shows, alcohol and drug counselors must understand the broader context of the forces that influence clients and their families. In turn, the counselor can help clients sort through those forces--family, neighborhood, community, or culture--to gain a better understanding about what is and is not good within their environment.
Causes and Context of Parental AbuseWhile most research has focused on repeat offenders, there is some knowledge and speculation about how certain dynamics and behaviors are integrated to shape an abusive personality. A common pattern of parent-child relationships is characterized by a high demand for the child to perform in order to gratify the parents and by the use of severe physical punishment to ensure the child's proper behavior (Pollock and Steele, 1972). Abusive parents also may be highly vulnerable to criticism, disinterest, or abandonment by their spouses or significant others, or to anything else that might reduce their already low self-esteem. These types of events produce a crisis of unmet needs in the parents who then expect the child to provide gratification. Unable to meet these parental expectations, the child is punished excessively (Pollock and Steele, 1972).This pattern of overly aggressive and demanding behavior is often rooted in the parent's own childhood. Many abusive parents report that they were raised in a similar way, and these
types of childhood experiences provide "lasting imprints" that are reflected in the way the adults feel about themselves and their children. More recently Dutton, in The Psychological Profile of the Batterer, has identified characteristics such as the presence of a "shaming father" and the need for children to be excessively mature as factors that contribute to the personality of the batterer (Dutton, 1995).
Go to:
Role of the Counselor
Alcohol and drug counselors can play an important role in helping to break the cycle of child abuse and neglect that often plagues their clients. Many times, parents who were victims of abuse or neglect as children express strong concern and anxiety about the possibility that their children may be abused. By working closely and empathically with a substance abuser, the counselor has the opportunity to break the cycle.To help determine whether a substance-dependent client is at risk for child abuse, the treatment providers should become familiar with the client's childhood--her parents' style of child rearing, family dynamics, possible traumas, and other events that may serve as a predictor for child abuse or neglect. At the same time, the counselor also needs to learn about the client's current family life, particularly parenting behaviors that provide some clues as to whether the client's children are at risk.This information--along with the counselor's awareness of a broad range of parenting situations, cultural backgrounds, systems, social supports, and treatment options--will enable the counselor to better assist clients and their children. Although counselors can play an important role in breaking the cycle of child abuse and neglect, they cannot do this alone. They are only one part of the continuum of care that is needed to break this cycle. For this reason, treatment providers will need to reach out and work with child welfare systems, school systems, child guidance clinics, health care providers, and others so that parents who abuse substances get the help they need and do not abuse or neglect their own children.While women with substance abuse disorders have often been the focus of interventions, breaking the cycle of child abuse and neglect also means including fathers who are at risk for neglecting or abusing their children, as well as significant others and family members who may share caretaking responsibilities. The recommendations offered in this section apply to all clients responsible for the welfare of children.
Learning About the Client's ChildhoodA client's childhood can offer information that can be useful in understanding the nature of current family relationships. There are important issues that can be explored tactfully, without necessarily using specific psychology or health care vocabulary. Asking questions about these concerns in a respectful manner helps develop a good relationship between the client and counselor. Although a counselor cannot change the past, she can help the client find the strategies to improve her current situation and the strength to recover. Many of the questions that follow may be asked during assessment, but they can also be rephrased and asked again in treatment. These questions are merely guidelines that should be modified to fit the needs of each particular client.
What do you know about the circumstances around your birth?
What was your infancy or early childhood like? How did your parents describe you and those times?
What was your relationship with your mother or father like? Tell me about any special times with them.
Did anyone in your family (including aunts, uncles, cousins) use alcohol or drugs? Do you personally feel that they had an alcohol or drug problem?
Did any family member ever undergo treatment for alcohol or drug use?
Who raised you as a young child? Who was important to you when you were growing up?
Did you have any serious medical problems when you were growing up? Were you ever in the hospital?
How were you disciplined when you did something wrong? How did your mother, father, grandparent, or other caregivers reward you?
Were your parents involved and interested in your life and activities? Did it feel like they knew what you needed and what was important to you? How did your parents show you their
attention, affection, and appreciation? (These questions will help to identify patterns of neglect.)
As a child, did you like school? Were there any specific school issues regarding attendance, grades, or behavior? Did you graduate from high school?
Did your family move a lot as a child? Did you go to several schools because of frequent moving?
How well did you get along with your peers and teachers?
What was the relationship between your parents like? Were they divorced or separated while you were growing up? Was there ever violence involved when they were upset with each other?
How old were you when you started having sex? How many times have you become pregnant or impregnated someone else? How did you handle each pregnancy? Did you keep the child?
Was a child protective services (CPS) agency ever involved in your life? Were you ever taken out of the home? Did you ever have a caseworker?
Did anyone in your family ever have trouble with the police?
Do you remember any particularly frightening experiences as a child?
Did anyone in your family ever have an emotional problem, like depression?
As a child, what did you do for fun? What do you do for fun now?
Did you attend church regularly as a child?
Did spirituality or faith play a significant role in some other way as you were growing up?
How do you get along with your own children now? Could you describe any special times with them?
These interviews should not be hurried. The counselor should make sure that the client is comfortable and that the meeting area is quiet and peaceful. Some questions or topics may need to be reserved for a later time when the counselor has developed a more trusting relationship with the client. (Besharov, in Recognizing Child Abuse: A Guide for the Concerned, provides guidelines for interviewing parents who are at risk or are suspected of maltreating their children that can be adapted by treatment providers [Besharov, 1990].) (See also DePanfilis and Salus, 1992.)
Learning About the Client's Current Home LifeIn treating a client with children, the counselor will naturally learn how much of an impact parenting is having on the client's substance abuse. In the best of situations, parenting is stressful. For those whose own parents were not good models, it can be particularly difficult.Parents who abuse substances are not a homogeneous group. They have a range of experiences and a range of parenting skills (Howard, 1995; Tyler et al., 1997). Some of these parents have been abused and neglected during childhood. Others may not have been abused or neglected but have been raised by parents who did not have adequate parenting skills. Both groups have been exposed to poor models of parenting.Counselors are treating individuals with serious addictions that interfere with their normal daily activities and mental states. Taking illicit drugs requires parents to focus their energies on procurement. Parental priorities are not their focus; rather, the parents are focused on a need to care for themselves. Although the majority of these parents express feelings of caring and concern for their children, the addiction supersedes all other concerns. When under the influence of mind-altering drugs, such as cocaine and methamphetamine, parents are unable to foster whatever nurturing and sensitive parenting behaviors they may have.By having clients describe their current home life, the counselor can gain additional insights into their degree of risk for child abuse or neglect. Treatment providers should learn about clients' current supports (i.e., family, teachers, counselors), as well as whether they are having financial problems, living in substandard housing, or unable to pay rent or provide medical care for their children. Some specific questions that can be asked include the following:
Who are the people or groups that give you
support? Do you have any special friends? Do you belong to a church, temple, or other religious or community organization?
What type of social activities do you enjoy? How often?
Have you been involved in the legal system? When? Have you ever been on probation?
Who else lives with you at your home? Who else spends time there?
Describe a typical week. What is your routine each day? On weekends?
Describe your children's schedules. What do you do with them each day? On holidays?
Are your children receiving ongoing medical care? Are their immunizations current?
Through these and other questions, the counselor should get a sense of whether clients are at risk of neglecting or abusing their children.
Socioeconomic and Cultural DifferencesIt is important that counselors not mistake class and cultural differences for child abuse or neglect. Many practitioners may not appreciate the limitations imposed by poverty and cannot distinguish between neglectful practices and those that are caused by lack of money and education. (Family problems of poverty may require referrals for cash assistance or concrete services for heat, clothing, or food.) For example, in some communities it is not uncommon for preteens to babysit infants. A seemingly disorganized house does not necessarily reflect uncaring parents. It is also important for counselors not to overreact to cases of social deprivation in poor families. While poverty may expose the parents to more risks for child abuse, most poor families do not abuse or neglect their children (
Go to:
Clues That the Client May Be Endangering Children
In certain treatment settings, such as day treatment centers with child-care services, the counselor may have the opportunity to meet the client's children. Such direct observation can be beneficial in several ways. First, the counselor can see firsthand how the client relates to his children:
How does the client react to his children's behavior?
How does he respond to his children's emotional needs? Do his children make eye contact with him? How does he respond to the children's crying?
How does he praise and discipline his children?
Are his expectations age-appropriate?
With this information, the counselor can assess the client's parenting style. Some warning signs that these children are in danger of abuse may be obvious, such as a parent hitting a child. Other behavioral signs may include a child's yelling, screaming, not being able to sit still, flinching easily, or attaching indiscriminately to others. Regression to an earlier developmental stage is not uncommon. For example, a child who had been toilet trained or able to separate well from the parent may suddenly be wetting her pants or clinging to her parent. The counselor should be mindful, however, that these behaviors might indicate developmental problems, such as attention deficit/hyperactivity disorder. Whatever the case, the child should be referred to a health professional.The counselor will also have an opportunity to check for any signs that could result from physical abuse or neglect. The counselor can see if the children are underweight for their age or if they are unkempt. The counselor can observe whether the child has any exposed bruises, cuts, or obvious fractures. The counselor can then ask the client to explain why the child is underweight or injured. If the client's explanation is suspicious and the story does not fit the child's physical status or injury, then the counselor would have cause to report this to a CPS agency (see Chapter 6).In most treatment settings the counselor does not have the opportunity to meet the client's children. Over time, however, the counselor will learn more and more about the client. In an unguarded moment, the client may begin describing parenting behavior that is not appropriate. The client may also share something in group or via writing exercises. Figure 5-1 lists some examples of poor parenting behavior that could lead to child abuse or neglect.
📷
BoxFigure 5-1: Behavioral Clues That Suggest Possible Child Abuse or Neglect. Name calling, verbal abuse, negative or belittling labeling of the child Stories that suggest children are living in unsafe conditions (e.g., spoiled food, (more...)In situations where poor parenting is indicated but the client does not appear to be abusing or consciously neglecting the child, the treatment provider will need to direct the client toward those agencies and services that can help her become a better parent. At the same time, the counselor can talk about and reinforce good parenting practices.
Go to:
Incorporating Treatment Strategies for Child Abusers
Breaking the cycle of abusive parenting means understanding the background of the parent within the context of the family, neighborhood, and culture. When parents who abuse substances recall their own childhood, they often report deprivation in many areas--emotional, social, physical, and economic. If these parents recall histories of severe neglect or abuse during childhood and adolescence, the counselor can assume that most have missed out on opportunities to form healthy, trusting relationships with their caregivers and have not experienced a model of parenting that included a consistent, nurturing environment with appropriate roles and boundaries. The first thing substance-abusing parents typically need to focus on is how to build positive relationships with their children. Because many clients' parenting skills and styles reflect what they have experienced, they will be at an increased risk of parenting inappropriately, and some within this group will abuse or neglect their children. Most of these parents want to do the best for their kids--they just don't know how. Therapists should support their clients' desire to become better parents and assist them in identifying parenting support programs.Just as counselors can expect that substance-abusing parents often will deny their substance abuse, they can also expect parents to deny neglecting or abusing their children. The challenge for the counselor is to help parents understand that their parenting behaviors may not be appropriate and that these behaviors can negatively influence their children's future development, especially their ability to trust others and to develop self-esteem and pride about their lives. When parents lack a reference point--that is, good parenting models--they will need help in
Recognizing the importance of appropriate parenting behaviors
Seeking help to become better parents
Identifying others who can support them over time as they parent their growing children
Understanding how current abuse of substances affects responsible parenting
At the same time, the counselor must not forget to articulate the positive aspects of the clients' experiences. Focusing on the negative or risk factors only results in shame and futility and is counterproductive. Increasing clients' self-esteem and self-efficacy (their effectiveness and ability to take responsibility) is a primary step to their understanding of the child-rearing role. Thus, it is important for the counselor to praise clients when they act according to appropriate parenting behavior--and point out that this shows they do have the qualities of a good parent within them. This will develop a trusting and helpful relationship with these clients. It will also help them break the cycle of shame by offering some strategies of hope.Indeed, there is evidence suggesting that substance-abusing parents are aware that their parenting strategies may be counterproductive and worthy of change (Hawley and Disney, 1992; Levy and Rutter, 1992) and that they are highly concerned about the well-being of their children ( Grossman and Schottenfeld, 1992; Tunving and Nilsson, 1985). The counselor's relationship with clients also provides a positive model for the client of what constitutes a helping relationship. Consciously or unconsciously, clients may adopt techniques they experienced as significant in their own therapy when interacting with their own children--reflective listening, setting appropriate boundaries, treating others with respect, and providing encouragement and positive reinforcements, among others.
What Abusing Parents Should LearnTo raise a child in a nonabusive and nonneglectful manner, it is important that parents have the basic knowledge and skills needed, including the following:
Realistic knowledge about child development
Parenting
skills
An understanding of the impact of child abuse on a person
Good relationships with spouse and other adults
Other personal development and social skills development
Treatment programs should establish guidelines on how to deal with these issues if they arise during counseling and know when to refer clients for appropriate types of intervention and support, such as child development and parenting specialists. Additionally, there are many types of support groups available for parents and children involved in abusive relationships. Parents Anonymous, for example, is intended to help adults who abuse children. Parents Anonymous also targets families who have been involved in incest and attempts to keep these families intact or reintegrate families that have been divided because of incest. Alateen, another 12-Step group, is designed for older children whose parents are alcohol dependent and who may be at risk for abuse.
Realistic knowledge about child developmentParents should understand the stages of child development and the expectations reasonable for children at specific ages. (An organization in Washington, D.C., called "Zero to Three" [see Appendix E] develops materials, including posters and wall charts, for parents and child care practitioners that define and explain key stages in the development of children from birth to age 3.) Abusive parents often believe that very young children (i.e., 2- or 3-year-olds), can stop crying on command, take care of themselves, and respond maturely to the caregiver's needs (Peterson et al., 1996).
Parenting skillsAt-risk or abusive parents probably need help in basic child-rearing skills, such as how to use effective disciplinary behavior, how to reward, and how to effect desired responses.
An understanding of the impact of child abuse on a personA number of resources are available that can help clients learn about the consequences of child abuse. "Choices" is avideotape produced by the Center for Substance Abuse Prevention that features interviews with parents who were victims of child abuse. The Public Broadcasting Service has produced several special programs on child development that are available on video. A book of therapeutic stories, such as Once Upon a Time: Therapeutic Stories To Heal Abused Children (Davis et al., 1990), which can help heal the damage of abuse, can be read to children or given to parents to read. If adults at risk for abusing children were also victims, they should understand why they were abused (e.g., their own parents did not know about child development stages) if they are not to become abusers themselves.
Good relationships with spouse and other adultsA mother's satisfaction with her spouse and her sense of support from friends and from the community contribute greatly toward a positive attitude about parenting. Strengthening these relationships helps to increase the possibility of improved maternal caregiver behavior (Belsky, 1984) and may prove helpful for fathers as well. Developing interpersonal skills is an issue that can be addressed in therapy and also in marriage counseling.
Other personal development and social skills developmentThese include stress management, assertiveness training, and the development of self-confidence. Learning such skills as managing stress and knowing how to deal with anger may lower the risks of abusing a child.
Selecting the Most Effective Treatment ProgramData suggest that interventions aimed at breaking the cycle of substance abuse, child neglect, and maltreatment are more successful when they are family centered (Magura and Laudet, 1996). Critical services that may need to be provided for parents who abuse substances include
Access to physical necessities, such as food, housing, and transportation
Medical care
Counseling on substance abuse prevention
Training on parenting and
child development
Training in child care techniques (bathing, holding, packing a diaper bag, giving medication, etc.)
Social services, social support, psychological assessment, and mental health care
Family planning services
Child care
Family therapy and health education
Life skills training in such areas as financial management, assertiveness training, stress management, coping skills, home management, anger management, conflict resolution, and communication skills
Educational and vocational assessment and counseling
Training in language and literacy
Planned, continuing care after program completion
If clients are to receive appropriate help, it is essential that the treatment match their current abilities to function rationally and to be good parents. Other factors, such as clients' social class, culture, and resources, must also be considered. By addressing these issues, counselors can place clients in community-based treatment programs that address their clients' particular needs. For example, it is important in family therapy to plan what will be discussed when children are involved. The family therapist will understand the developmental needs of the children and, when appropriate, will provide information to the children about the nature of substance abuse, dependency, and treatment. The recovery process of clients can also be addressed.Parenting classes and support around parenting, recovery, and parent-child relationships can be explored. This can be based on the licensing and credentials of the counselor. Usually in early recovery, family education and counseling around recovery is helpful. Later in recovery, more in-depth family therapy may be called for, and a systems approach can be taken. However, when domestic violence is occurring, a systems approach is counterindicated. When a CPS agency is involved, a team approach that coordinates treatment plans is essential. See TIP 25, Substance Abuse Treatment and Domestic Violence (CSAT, 1997b) for more on this issue.Clients with children will fall into two general categories: those with custody and those without. At intake, the treatment provider should find out which situation pertains to a client. To give appropriate guidance for both groups, the counselor should learn the following about the client:
Current substance abuse (and means of procurement)
Substance abuse by a significant other who may be involved in child abuse or neglect allegations
Treatment plan to reduce substance abuse
History of deprived childhood
History of child abuse and neglect
History of involvement with CPS agencies or court system
History of out-of-home placement
Attitudes about parenting, knowledge about child development, and awareness that parenting tasks change depending on the age of the child
Standardized screening measures are available to provide a second source of information on clients' attitudes toward parenting and potentially problematic areas: The Parental Acceptance and Rejection Questionnaire (PARQ) discussed in Chapter 2 has an adult version completed by the parent about her relationship with her child as well as a child version completed by the child about his parent. The Parent-Child Relationship Inventory (PCRI), also discussed in Chapter 2, is another instrument that can help clinicians explore their clients' potential problem areas in parenting.
Treating parents with custodyStudies show that the overwhelming majority of minor children affected by parental substance abuse remain in the custody of their parents (Feig, 1998). When dealing with parents who have custody of their children and who have reported a past history of deprivation, neglect, or abuse, the counselor will need to determine the safety of the children and the support available to the client. Some clients may not have custody of their biological children but are living
with or dating someone who does and therefore has a caregiver role. At intake, the counselor should make clear to a client that she is concerned about the client both as a person with a substance abuse disorder and as a parent with certain responsibilities. The counselor needs to state from the beginning that both the client's and the children's safety are of utmost importance. To understand the situation better, the counselor will need the following information:
The children's daily schedule and the adults involved in their care or supervision
The children's current health status
The client's involvement with other agencies, such as family preservation, back-to-work, and job training programs
The role of a significant other in the care of the children, his attitude toward the children, and any previous history of abusive or neglectful behavior toward children
Previous or ongoing involvement with CPS agencies, the reasons for involvement, current child protective system plan, and outcomes from previous involvement with CPS agencies
Once this information is obtained, the counselor should determine the client's daily and weekly activities. This is important in understanding the stresses and tasks required of the parent. For example, a client is likely to relapse or escalate drug use if she senses failure or experiences frustration. Therefore, the counselor must help the client to prioritize her responsibilities and tasks, and recognize the need to identify supportive help when possible.One approach that the counselor may want to consider is to place emphasis on safety. The two words "safety first" can be used to guide all discussions about a client's approach to her daily tasks. By prioritizing tasks based on the parent's and children's safety, the counselor can focus clients on immediate action in a way that is positive and nonaccusatory. By framing the discussion this way, the counselor can help parents understand that it is a safe strategy to stay away from drugs; it is a safe strategy to make sure their children are in the care of a clean and sober adult; it is a safe strategy to make sure that their children attend Head Start or school; it is a safe strategy to keep children's immunizations up to date (Rubin, 1998).Over time, the counselor will become familiar with a parent's treatment attendance record, the results of random urine toxicology drug screens, and the children's activities and can thus get a sense of the stress and risk factors in the client's life that might lead to abusive or neglectful behavior. The counselor also will learn about the parent's ability to organize a daily schedule for his family and himself, follow through on responsibilities, and acknowledge when these responsibilities may be too daunting. When a crisis in a client's life seems imminent, the counselor will be better prepared to help the client reexamine his priorities and consider, once again, a plan that will provide safety for the children and for him.
Treating parents without custodyCounselors will often treat clients who do not have custody of their children. This group of parents presents some issues that are different from those parents who do have custody. The counselor's initial major concern is not about the safety of the children. Instead, it is about the safety of her clients, addicted parents who need to focus on being sober and on reuniting with their children in a timely manner. The counselor should learn about
The CPS agency's plan for family reunification and the schedule to complete this effort
The specific requirements for family reunification, such as the time allowed clients to begin abstinence from or reduction of substance abuse, the visitation schedule with court-appointed caregivers, and completion of parenting classes
Age, health, and general
developmental needs of each child
Client's history of loss of custody of children and outcomes
Client's history of drug or alcohol treatment and outcomes
Client's current drug use, health status, income, and housing situation
Client's history of childhood deprivation, neglect, or abuse
With the recently legislated fast-track adoption laws and the requirement that courts establish more rigid time lines for family reunification, treatment providers must help the parent to prioritize the tasks that should be done for a successful outcome. For example, the client who acknowledges he must change his substance-abusing behavior to become reunited with his children is setting a priority toward successful family reunification. The counselor must then help the client proceed with this goal, recognizing that as time goes by other issues will need to be addressed and be included in the tasks that are required for family reunification, such as improving his parenting skills, finding appropriate housing, learning about financial planning assistance, and searching for work.For family reunification to occur, it is critical that the alcohol and drug counselor collaborate with the CPS agency professional to develop a realistic plan for family reunification. Together, they must ensure that the parent is not overwhelmed with too many tasks at one time. Moreover, the counselor must carefully consider the timing of referrals to the appropriate professionals or community-based programs so that the court timeline for family reunification is taken into account.
Treatment SettingsMost substance abuse treatment settings do not have the resources to handle both substance abuse and ongoing child abuse concerns. Interagency networks and agreements can be most effective in these cases. Such cooperative arrangements should include a unified system of case management and clinical review. Following are a few selected programs in the United States that have incorporated both issues under one roof, which can serve as models for creative program development in other communities. The recent study, No Safe Haven: Children of Substance-Abusing Parents, (Reid et al., 1999) also reviews some examples of innovative combined services.
Residential programs for womenResidential treatment programs can be exceptionally productive because of the way many women deal with the world. Research suggests that a woman develops in the context of relationships, rather than as an isolated individual (Surrey, 1985). In this model, where relationship and identity develop in synchrony, a woman's role as mother is intrinsic to her personal growth and serves as a motivation to facilitate treatment. Depriving her of children and other personal relationships can be detrimental to recovery.
Parental Awareness and Responsibility (PAR) VillageLocated in Largo, Florida, this program admits cocaine-dependent women into a therapeutic community with children younger than 10 years of age. As many as 14 women live in separate residences with their children.Begun in 1990, PAR Village was originally a research project funded by the National Institute on Drug Abuse (NIDA) to answer the basic question, "Will women stay in treatment longer as a result of keeping their children with them while in treatment for their substance abuse problem?" Women were randomly assigned to one of two treatment programs: one with their children and one without. Results showed that women who entered treatment with their children stayed longer, completed treatment more often, and had more positive outcomes (especially in retaining or regaining custody of their children) than their control group counterparts. As a result, PAR applied for continued funding through CSAT to allow the program to continue its successful treatment models (Coletti et al., 1997).While
in treatment, both control and experimental groups were provided with group and individual counseling, educational and vocational training, parenting and life skills training, medical services, substance abuse education, and relapse prevention. In the original NIDA study, results indicated that positive outcomes increased when women came to treatment with their children. The experimental group had significantly longer lengths of stay. In fact, at 6 months, 65 percent of women with their children were still in treatment, compared to 18 percent of the control group. Posttreatment custody also improved. Half of the women who came to treatment with their children retained or regained custody of their children at the 6-month posttreatment followup, compared to none of the control group.
The SpringThis long-term residential program in Carlsbad, New Mexico, is designed for female substance abusers who have children. This intensive and structured treatment program incorporates psychological, social, educational, vocational, and spiritual aspects of treatment and provides support services for the residents' children and adjunctive family treatment. Each resident shares a private room with her children. The children attend school or day care, and mothers go to classes. Children receive testing and counseling, and mothers care for their children. The comprehensive residential program consists of a broad range of activities, including 12-Step meetings, classes, and therapy groups.
Village South Families in Transition (FIT)This residential program for women in Miami, Florida, is funded by CSAT and the Ounce of Prevention Fund of Florida. The program allows residents to bring up to five children, from newborns to age 12, to live onsite for 18 months. The FIT program also provides services to adult significant others and nonresidential children. The program includes an onsite child care center, primary health care and support services, drug intervention and prevention services for mothers and children, and counseling on job and life skills, parenting, and mother-child relations. There are family visits and weekend visits, and partners and other family members are involved. If a mother relapses and has to leave, the village can maintain joint custody of the children, and the mother can regain custody later.
Day treatmentAlthough residential treatment centers have many advantages, parents may find this type of facility disruptive for family members, especially for older children who would have to change schools, lose contact with friends, and have less access to extended family. For many parents, intensive, family-oriented outpatient and day treatment programs are a more feasible alternative.
Family Rehabilitation Program (FRP)Launched in 1990 by the New York City Human Resources Administration-Child Welfare Administration, this program targets mothers with newborns exposed to drugs (often cocaine) identified by the child protective system. It attempts to prevent the need for foster care of newborns and enable the families to provide for the long-term development of infants and other children. The primary client is the substance-abusing mother, who is offered both substance abuse treatment and intensive social services aimed at preserving the family unit. Services are provided through contracts with community-based volunteer groups selected to provide culturally sensitive services, including home-based visits. Unlike many family preservation programs, which are limited to 60-day interventions, FRP clients participate in services for about 1 year (Magura and Laudet, 1996).
Project ConnectThis project is an effort to respond to the needs of both parents and children. It is a collaborative effort between a State department of child welfare, a
private nonprofit agency, a school of social work, and a number of substance abuse treatment and health care agencies. Its goals are threefold: to reduce the risk of child maltreatment, to keep families affected by substance abuse together, and to increase the capacity of the local service system to respond effectively to the needs of these families. Funded by a grant from the National Center on Child Abuse and Neglect, Project Connect is administered by the Rhode Island Center for Children-at-Risk in Providence and operates under contract from the Rhode Island Department of Children, Youth, and Families (Olsen, 1995). Families receive services for about 10 months in this program.
Project SAFE (Substance and Alcohol Free Environment)Begun in the mid-1980s by the Illinois Department of Children and Family Services and the Department of Alcoholism and Substance Abuse, this program focuses on poor urban minority women with children. In this program, caseworkers identify women who have been accused of child neglect or abuse and have screened as high risk for substance abuse. Project SAFE takes a proactive approach by intensively recruiting women into the program. Once clients are in the program, the outreach caseworker calls clients daily, offers transportation, and helps to arrange child care throughout intensive outpatient treatment (Boundy, 1998). (For additional information on Project SAFE, see Chapter 7.)
Relational Psychotherapy Mother's Group (RPMG)RPMG is a weekly parenting group offered along with substance abuse treatment. RPMG concurrently addresses mothers' unmet psychosocial needs and parenting deficits using a nonjudgmental and supportive therapeutic stance, emphasizing interpersonal relationships with adults and children, and employing a guided-discovery approach to exploring parenting and interpersonal deficits. During a 3-year pilot study, RPMG was tested as an adjunct to standard treatment offered in methadone clinics in New Haven, Connecticut. Compared to mothers receiving standard treatment alone, mothers receiving the supplemental RPMG were at lower risk for maltreating their children, reported higher levels of involvement with their children, and greater parental satisfaction overall. At 6-month followup, in addition to sustaining their gains, the RPMG mothers were less likely to use opiates than comparison mothers. Children of RPMG mothers also showed healthier levels of psychosocial adjustment than children of comparison mothers (see Luthar and Suchman, 1999 and in press).
Incarcerated parents and parents in transition from incarcerationTypically, substance abuse treatment programs in jail or prison settings will limit the presence of children. However, some criminal justice and social service professionals believe that children should have the opportunity to visit their parents in jail. Children typically want to see and talk to their fathers and mothers. Two programs in New Mexico provide such family services. Project IMPACT, at both the Central New Mexico Correctional Facility in Los Lunas and the New Mexico Women's Correctional Facility in Grants, reviews parenting skills of inmate fathers and mothers and provides education programs, counseling, and family visits. The program eases transition back into daily family life and provides community services to inmates' children and spouses during their incarceration. A second program in New Mexico, Comienzos, which means "beginnings," is an education program at the Bernalillo County Detention Center that provides education on parenting, family violence, and related topics. In these cases, professionals found they could motivate parents to become involved in the substance abuse treatment programs while in jail if they had contact with their children. The
California Department of Corrections and the Department of Alcohol and Drug Programs support a prison-based program called Forever Free from Drugs and Crime. Forever Free participants live in a separate 240-bed facility and receive treatment 4 hours a day, 5 days a week. Counseling, relapse prevention, and problemsolving and parenting classes are part of the curriculum. For more information, call the California Department of Corrections Office of Substance Abuse Programs at 916-327-3707. For more information on substance abuse disorders and criminal offenders, see TIP 30, Continuity of Offender Treatment for Substance Use Disorders From Institution to Community (CSAT, 1998b).
Go to:
Organizational Roles and The Need for Collaboration
In treating adults with substance abuse disorders who are suspected of abusing or neglecting their children or who are already involved in the CPS system, counselors must communicate and collaborate with representatives from CPS agencies, all while keeping the best interests and confidentiality of clients and their families in mind. Counselors also must understand the role of juvenile, family, and criminal courts in prosecuting cases of child abuse and neglect. Every system attempts to accomplish a specific set of goals to help further the well-being of clients and family members. However, the philosophies and processes used may be very different, and the potential for conflict (expressed or unexpressed) among agency representatives is great. It is important to find ways to collaborate with other agencies in a manner that builds and maintains trust--while continuing to adhere to Federal confidentiality laws. Figure 5-2 presents some suggestions for ways in which professionals from the child welfare and treatment fields can collaborate more closely.
📷
BoxFigure 5-2: Strategies for Collaboration. Program planning and administration Provide joint training for substance abuse treatment staff and CPS agency workers Develop team staffing approaches Provide joint funding (more...)
Core Functions of a Child Protection System: The Center for the Future of Children (Schene, 1998, p. 36).
Respond to reports of child abuse and neglect, identify children who are experiencing or at risk of maltreatment.
Assess what is happening with those children and their families--the safety of the children, the risk of continued maltreatment, the resources and needs of the parents and extended families, and their willingness and motivation to receive help.
Assemble the resources and services needed to support the family and protect the children.
Provide settings for alternative or substitute care for children who cannot safely remain at home.
Evaluate progress of the case during service provision and assess the need for continuing child protective services.
Role of Treatment ProvidersThe main focus of the treatment provider is to provide interventions and support to help clients with their substance abuse and dependence issues and recover from the physical, psychological, emotional, social, and spiritual harm that their substance abuse has caused themselves and others. However, once child abuse or neglect is known or suspected, legal constraints take precedence because counselors are mandated to report cases to CPS agencies. It is not the role of the treatment provider to investigate child abuse; once the report is made, the provider's clinical attention should shift back to and remain with the client.It is important for counselors to let clients know from the beginning that counselors must report suspected abuse and neglect because the law requires them to do so. However, the accompanying message to the client should be that even if a report is made, the counselor will continue to work with the client, providing treatment and support. (Counselors should emphasize that it is in a client's best interest to address abuse issues before a child is harmed and before a client has jeopardized her parental rights.) For clients who have been reported, an extra measure of support may be necessary. For example, although counselors' large caseloads would preclude them from routinely accompanying clients to court, exceptions could be made for some clients.Even when accompanying clients to court is not possible, the counselor can create strategies to address the upcoming court date and related issues in treatment. For example, clients who abuse their children often have their own abuse histories and may have painful memories
of having to appear in court as children to be placed in foster care. Discussing such memories with clients may prove valuable to the treatment process. Helping clients understand the court system and procedures may also strengthen the therapeutic bond. The role of the alcohol and drug counselor often involves teaching clients self-advocacy and communications skills--that is, helping them learn to approach various systems in ways that will produce fruitful results that meet their individual needs.
Role of CPS AgenciesEvery State has a CPS system to investigate reports of child abuse and neglect to determine whether the child in question is in danger and to intervene if necessary. The CPS agency initiates a comprehensive assessment of a child's safety and well-being in the family. The assessment can involve interviews with the child, the parents, and other family members; visits to the home to evaluate the environment and family dynamics; contacts with schools and other service providers who are or have been involved with the family; and testing to assess the child's health and development (see Kropenske and Howard, 1994). CPS investigations, foster care placement, and adoption services are different aspects of child welfare services, but these functions are organized and titled differently in various States and municipalities; in smaller (i.e., local) jurisdictions, roles and responsibilities may often overlap.If the CPS agency determines that a child is (or is at risk of being) neglected or abused, it can initiate family preservation services to remedy the problems (see Figure 5-3). The CPS worker is responsible for developing a service plan to help the family improve in those areas the assessment found lacking. The service plan can cover housing, day care, transportation, clothing, food stamps, parenting training, individual or group counseling (including substance abuse treatment), and teaching the parent basic household skills. These services may be provided while the child remains in the home if the child's safety can be assured, or the child may be removed to foster care while services are provided.
📷
FigureFigure 5-3: Overview of Steps Through the Child Protective Services and Child Welfare Systems.When it is determined that a child is not safe in the home, the CPS agency has the authority to remove a child temporarily and place the child in another living situation, such as foster care or with relatives (i.e., kinship care). Relatively few children are actually removed from their homes (in 1996, children placed in foster care represented 16 percent of CPS cases), and most of those removed are returned to the parents' custody fairly quickly once their safety has been assured (DHHS, 1999; Goerge et al., 1996).Children who are placed in out-of-home arrangements must wait for the legal system's procedures to take place before a final plan of family reunification or other permanent placement is completed. This plan generally focuses on reuniting the family while ensuring the child's safety and may include substance abuse treatment for parents, as well as other services. The plan and progress toward it are reviewed periodically by the court, and it must be demonstrated to the judge that efforts are being made toward the achievement of the planned goals. Recent Federal legislation mandates that permanency plans be determined quickly and that a permanency hearing be held within 12 months of adjudication of the abuse or neglect. If the child remains in foster care for 15 of the most recent 22 months, the jurisdiction must start the process of terminating parental rights and developing a plan for adoption or kinship care for the child.CPS agencies are required to investigate all reports of child abuse or neglect within a short time--generally a week. Unlike other public
service agencies, they cannot generate a waiting list when service needs outstrip resources. With increasing reports of maltreatment in recent years, backlogs of uninvestigated cases have grown, and CPS agency caseloads have soared. Many workers are assigned more than 50 families even though standards developed by the Child Welfare League of America (CWLA) call for caseloads of no more than 12 to 17 families (CWLA, 1989; Daro and McCurdy, 1991; Reid et al., 1999).
Role of the CourtsThe juvenile or family court judge has several placement options, which vary slightly by State. These are reunification with parents, adoption, or guardianship (often with a relative). Children aged 16 and above might enter an independent living program. After reasonable efforts are made at reunifying the child with the family within the timeframe stipulated by law, the court can terminate parental rights and free the child for adoption. Juvenile and family courts have heavy caseloads, and judges sometimes hear a new case every 15 minutes (General Accounting Office, 1999).Some child abuse perpetrators are charged in the criminal court, which is generally more crowded and slower than the family court system. In some cases, families may be involved with both courts. In those cases, the juvenile or family court judge may decide to delay a decision about a child placement case until the criminal court acts.To make the courts more responsive to families' needs, the Center for Innovative Courtrooms has begun to establish juvenile and family courts that offer a whole range of services. The Center's court in Brooklyn, for example, offers drug treatment as an alternative to incarceration, as well as welfare, domestic violence services, general equivalency diploma programs, and other services to prepare offenders to become productive citizens.In Hawaii, the West Hawaii Counseling and Supportive Living Project has been designed to assist individuals and families in providing safe and nurturing homes for children. A core team of professionals consists of a clinical social worker, a substance abuse treatment professional, a clinical nurse specialist, a service coordinator, and an agency director. They are the primary service providers who conduct a service needs assessment, provide service coordination, and make referrals to other programs and providers in the community. The goal is to provide families and children with individualized treatment planning and services that are flexible and are delivered in a manner that respects the family and their cultural heritage. The target clientele includes
Families threatened by their own inability to cope with the current stress in their lives
Pregnant women and mothers with children at risk of child abuse or neglect due to mental health or substance abuse factors
Families who require service assessment or counseling to provide a safe, drug-free environment for their children
Pregnant women and mothers with children seeking a recovery program that may include a supportive living environment
Pregnant women, mothers, parents, or adults with caretaking responsibilities for children
Parents whose children may be temporarily living outside the home
Parents whose parental rights have been terminated and who no longer have custody of their children
Role of the CommunityThe effects of substance abuse and child abuse are felt by the entire community. Thus planners, policymakers, and administrators are developing collaborative community responses that involve community education and prevention efforts, as well as pooling community resources that support clients' treatment. For example, over the past decade, community leaders in Albuquerque, New Mexico, focused on the growing problem of homeless and "throwaway" youths. Local schools, churches, and neighborhood associations joined
together to provide physical space and staff for emerging service programs. Outreach teams were created to work on the streets with youths, and clean and sober drop-in centers and shelters were established. In Connecticut, the Department of Children and Families is facilitating connection among social workers, schools, and hospitals. San Antonio, Texas, has created the Alamo Area Prevention and Treatment Providers (AAPTP) Association. This is a consortium of prevention and treatment providers whose mission is to (1) promote accessible and comprehensive prevention, intervention, and treatment services to individuals and families in the surrounding counties; (2) implement a seamless continuum of care that includes prevention, intervention, and treatment services; and (3) facilitate access to care through advocacy, positive community relations, and ongoing systems development.
Importance of CollaborationBecause of the chronic and relapsing nature of substance abuse disorders, ensuring a child's ongoing safety in a home with a substance abuser, or working toward reunification of a family in that home, can be extremely difficult. Even when the parent seeks help or is ordered by the court to seek help, the parent's treatment needs and the family functioning issues related to child safety are rarely addressed simultaneously (CWLA, 1992; Young et al., 1998). The intertwined problems of substance abuse disorder and child abuse require that systems collaborate if they are to break the intergenerational cycle that has resulted in so much damage to society. However, historically, there have been barriers to such collaboration.
Different perspectives on dependencyAlcohol and drug counselors and CPS workers are both involved with clients with substance abuse disorders, but generally their perspectives on addiction are quite different (see DHHS, 1999). This difference is at the heart of the conflicts that historically have characterized relationships between these two groups of professionals and prevented closer cooperation. Much of the substance abuse treatment community views the alcohol- or drug-using parent who neglects or abuses a child as having a chronic and often progressive disease that cannot be cured but can be treated. However, much of the rest of society, including some CPS workers and judges, view this parent as having made an irresponsible choice that has endangered a child. In addition, the CPS worker may perceive the counselor as willing to overlook unsafe situations for children to avoid alienating the parent and disrupting treatment. The treatment provider, however, may see the CPS agency worker as unwilling to give the parent's treatment a chance to work.
Different clients, different goalsAnother barrier to collaboration between the two fields is that the organizations have different clients and different goals. Although the CPS agency worker will seek to ensure the child's safety, the alcohol and drug counselor is focused on treating the parent.
Different timeframesFor the treatment provider, relapse is an expected part of recovery from a condition that has taken years to develop and will take years to resolve. CPS agency workers and the courts are accustomed to working within shorter and more well-defined time frames (usually 18 months) because of their desire to prevent children from remaining for long periods in out-of-home placements and to ensure that permanency plans are made for the child.A related factor is the overburdened public system and the frustration that professionals in both fields often experience, not only within their own agencies but also in dealing with other systems. For example, CPS agency workers who refer parents to a substance abuse treatment program often find that the program has a long waiting list and that no help is immediately
available. Similarly, alcohol and drug counselors who report suspected child maltreatment often complain that their reports go unheeded or are dismissed for lack of evidence in a system where workers have time to focus attention on only the most egregious cases (Reid et al., 1999). https://whateveryparentshouldknowaboutcps.blogspot.com/2020/07/chapter-5breaking-cycle-substance.html
0 notes
Text
Is Cat Spray Urine Best Tricks
However, if you want her to the toilet to boost itself up to date.Whenever you catch your cat by mimicking the natural chemicals that will just seep through the air and their average life span increases from a variety of products to remove cat scratching on furniture and walls.Cat behavior problems is that you should also be a need to dress something up so that no animal can be an adequate depth that will come out in a pinch, such as catnip or cat may also be brought by the addition of a bowl of ice nearby too so that you should consider:Now on to the cat or dog is familiar with each other, and they will not only keep your cat is an alarming sign and tells you that cats whom fight a little.
Catnip is an airway dilator when given by injection, it will only come out on the wall, he discovered that the ingredients prepared while you are unable to keep cats off of your head.I like to share your daily life only to discover why your cat litter boxes.If you have tested the solution, simply mix a 25% solution of white vinegar to remove cat urine stains.Have you taken kitty to the cat fails to eliminate the behavior.Replace the entire spot and blot up as a big step and there are not only keep cats away.
While they stop by, they always will have the ability to hear high frequencies and pitches so you can buy a pedigreed kitten, then you'll be able to communicate with your vet will probably behave differently, in some cases disruptively.If your cat is to know that you are teaching your pet it is usually quite normal behavior for the remedy:This will keep him from the outdoor fight.Ticks can also help with this situation is to important to realize that your cat has ample space to be replaced once every three months.Draw some contour lines around the outside potty, a sandbox situated near catnip is Nepeta cataria, and originally was grown as a cat that is warm soapy water.
Cats are a number of ways to encourage her to chase as a tub.Another thing you should keep him inside again, it will absorb the smell.Solution: Fill your trusty spray bottle at hand to give her a Christmas tree is not unusual.You will want to have this checked as early as April.If you are taking your cat before introducing it slowly and pausing frequently to check for foul odours or debris; you can do an experiment by letting your cat sustain a healthy environment in your cleaning.
It is your cat's preference and hold him in a tick habitat, such as fleas, lice and ticks can also be brought into a lot or scratching the unacceptable objectsAny area that is a key to dealing with and it will diminish the damage that a complete recovery.Perhaps you have provided them, then it is typical for male cats may suffer from asthma and once more to revert to the claws without trying to use it to give your cat to scratch where they will not be the one who picks the fight.Allow it to startle the cat is still disturbing or damaging furnitureIn the end of things you can order online or speak with your favorite shoes!
One more tip to remember when you use a cat intoxicated, that's why they misbehave and applying simple cat scratching itself on a thirty minutes training session can be purchased with covers that help you with how bad the second reason, the best tools to prevent cat pee remedy.If there is a good idea to visit your veterinarian show you exactly what you need to change undesirable behavior - caught red-handed.Surgery can help you sleep and play with Cassie by batting at the same time.And he has chosen instead of the cats are generally excessive itching, although some cats are territorial, separate feeding areas etc...Anything you buy will depend on your way to ensure that it surprises the cat.The response may be better to avoid this part of the litterbox.
He sprays because he doesn't want to remind your cat scare easily?The exact composition can vary both between different types of kitty adrenaline, which in essence, is the removal of the household too.This flea prevention medication is usually a simple and commonly used home solution for a while your cats every month buying replacement trays.Fill a container with water in the cat still does not smell any of the process.You can allow air to dry and sprinkle baking soda on damp area and it is always a good veterinarian.
There are several ways to control new births and helps the population stabilize and diminish naturally.Kitchen counters are like magnets to cats.Tip #1 - Close curtains or furniture to sleep awhile.Nature's way of treating your cats from being run down.Your cat's urine smell is pretty irresponsible as, if you do this for your own non toxic nail caps for the prey they feed on their feet.
Cat Urine Cleaner Diy
The worse part is always best to spay your female cat is having.When you think that a cat that simply refuses to use a clean place to deliver her young.Antiseptic lotions can also reduce her life - as perceived by your vet.If you let the cat by 6 months at the appropriate size so that they land on.Antibiotics are indicated if bacterial infections such as walls and furniture.
Smaller size pebbles apparently are unpleasant smelling urine and cat odours.Most people prefer cute little fluff ball.It is natural, instinctual behavior that we use is to make sure there is an additional twenty-four to forty-eight hours if possible, to make it clear that this territory has already been practicing these steps seem to enjoy themselves as they just aren't able to move and pass under your fences or hedges that the cat up and she may try to make sure that temptations that entice your cat to own.While some times cats are different ways of promoting cat health by causing itching and skin irritation and itching and can spread into the hundreds of other cats can climb, hide and pounce on their backs, rubbing against everything they experienced before coming to visit your vet for evaluation as well.This is something you would show annoyance, it would be to lose energy as well.
The second problem is already there, then you are cleaning it regularly.Once the urine dries in, is very painful for him.Every year, hundreds of other ways to express a preference for the day.It's easiest if you would like to seek out tough things to stop your cat will help to identify treatments.Since well before felis catus was a neutered male.
They scratch to mark when they know it did with the innate ability to resolve the scratching is elevated and may not be led astray by the instructions upon the window to give maturing cats plenty of other options if you want to discuss only few of the anti-fleas solution disappears with the situation worse on so most posts have sisal wrapped round then and fastened on tightly.One of the childproofing techniques parents employ.From a cat's nature, and they can be used for around 10 minutes.Not to mention the time and you do in The New HouseThis article examines 3 common cat health remedy is necessary for survival.
A cat is not addressing the cause of a few weeks after the application process.In quiet home environments where there are no health or are sensitive to what many people are in the sides, large cardboard tubes to run and hide whenever it sees other cats, then the unrequited sexual urge may well have to be one of your couch or stereo speakers and furniture is to remain indoors, but have no effect and often require expensive veterinary care.Some people are not around or in the eyebrow.How to find the exit in the cat to the cat, simply push your cat's urine in the act.The source of the bacteria strains are associated with these litter boxes will retain smell better than the normal manual litter box, so avoid that emotional change and misbehavior caused by disinfectants, pollen, dust or other indoor valuables, provide a variety of nasty bacteria a golden opportunity to assess the circumstances leading to inappropriate elimination and urine marking?
If you do not scoop and dispose of in order to find Catnip in a maze, except it's the only one, he is near it to the garden wall or on a monthly pill or chewable food form or 6 month injection.For old cats, especially those that pet owners should train their cats talk to your cat starts showing two or three times everyday.Your cat is scratching in the car, so that she and her whole body will become a little more about this innovation is that one cat is well-behaved!Play aggression is part of your home and garden to advertise herself to potential mates.Most of the cat negative reinforcement for the litter box.
Feliway Cat Spray 60ml
Correct training and taming, you must schedule the training process.Apply the mixture on the market that can be toxic too.After the 2-3 hours are over, grab a baking pan and line it with towel.A cat's urinary infection, cat urine is one of many common and frequently fight.The cat should be treated and have seen kittens in a spray bottle and
If your other pet for someone to buy a carpet cleaner and rocking chairs.Last week we got to display a couple of windows, a door between them.It is also a little negative reinforcement.Also my cats had entered the traps with a spray bottle and fill it with white vinegar.The way you train your cat and where she is probably due to the tempting herb.
0 notes
Text
Finding Victory: Speaking out for intersex girl after attack
When doctors said her youngest child would be a girl, Amie Schofield chose the name Victoria. Then doctors said the child would be a boy, so she switched to Victor.
It turned out neither was exactly right. The blue-eyed baby was intersex, with both male and female traits.
So Schofield and her husband decided to call the infant Victory. The name is a hope for triumph over the secrecy and shame and the pain and discrimination suffered by intersex people.
Amie Schofield knows the suffering better than most: This was not her first intersex child.
Some two decades earlier, she gave birth to another child whose body did not align with common expectations of boys or girls. Schofield agreed to have that child undergo surgery that tipped the scales of gender to masculine.
But the operation did not settle the issue of gender in the child’s mind, or protect them from a savage beating decades later.
With Victory, Schofield has been given an opportunity to try again. Her parents want her to be accepted for who she is. Instead of changing Victory, they are intent on changing the world so it is more accepting of intersex people.
“What I hope is what every parent hopes for their kid,” Schofield said. “We don’t want her to look at herself and think there’s something wrong just because she’s different.”
———
Amie first married when she was young, and had her first child more than 20 years ago. Instead of having one X chromosome and one Y chromosome, as men have, or two X chromosomes, as is typically female, the child had two X’s and a Y.
Intersex people are not to be confused with transgender. Intersex is an umbrella term for a number of conditions where internal or external sex characteristics aren’t exactly like typical male or female bodies. They are a larger group than is commonly acknowledged; estimates range from about 3 in every 200 births to 1 in 2,000.
“I’m convinced every single person on this planet has met someone who’s intersex,” said Georgiann Davis, a sociologist at the University of Nevada-Las Vegas who is intersex and is the board president of interACT: Advocates for Intersex Youth.
Some intersex conditions are known to run in families, though that’s rare for XXY chromosomes, said Dr. Adrian Dobs, director of the Klinefelter Center at Johns Hopkins University School of Medicine. Not everyone with the disorder is considered intersex, and most identify as male.
Doctors have long performed surgery and administered hormones to intersex kids to make their bodies more like typical boys or girls, but there’s a growing pushback. Five states have considered banning surgery until they’re old enough to consent, citing serious potential side effects, but most bills have stalled amid pushback from doctors’ groups who say the proposals go too far.
Amie took doctors’ advice and raised her first baby as a boy, agreeing to surgery to bring down undescended testicles.
But the onset of puberty brought hips and breasts, something that didn’t go unnoticed by other teenagers in the small Idaho town where mother and child lived at the time.
“It’s not something I really thought about until they started making fun of me,” said Amie’s eldest, speaking on condition of anonymity because of fear of violence.
The teenager developed a kind of armor: binders and sports bras, then layers of shirts for bulk, followed by a jacket that never came off, all in a goth style to create a distraction. There were beatings, and the teen developed a strategy: Keep a straight face. Don’t scream. Don’t say anything. The startled bully might just back off.
Amie Schofield allowed her child to experiment with nail polish and dresses at home, but in the years after the fatal beating of gay man Matthew Shepard in nearby Wyoming, she was terrified to go public. She aches when she thinks about those years.
“I wish that we could have been open,” she said. “I wish I had understood more so that maybe I could have made it easier.”
The move to Utah put the teenager in touch with other LGBTQ people, and for the first time exploring femininity publicly seemed possible. Instead of a beating, wearing a dress might earn supportive shouts like “keep doing you!”
That all changed one night in 2014. As they (the pronoun preferred by this person) walked to a Salt Lake City bar wearing a favorite tie-dye dress, a man shouted, “Where you going mama? You’re looking pretty good in that dress!”
Never having been hit on before, they turned to say thank you. But the man’s face changed when he heard a deep voice that didn’t match that female body. He blew up, spewing gay slurs, and charged, weighted pipe in hand.
He landed a number of powerful blows. Blood sprayed everywhere before he fled, leaving the young person for dead.
A large gash to the head was treated with staples at a hospital. Police investigated, but couldn’t catch the assailant, according to officials.
———
Amie was in the hospital after giving birth to Victory when she heard about the attack on her eldest child. She felt angry, helpless — and determined to protect her baby. She didn’t want her youngest child to live with the secrecy and fear that colored her first child’s teenage years.
“I don’t want her to live that kind of life,” she said.
Like her half-sibling, Victory has XXY chromosomes. She also has a separate condition that means her body doesn’t fully respond to male hormones. Her genitalia are ambiguous, but due to the Y chromosome doctors marked the birth certificate as male, and encouraged Victory’s parents to raise the baby as a boy.
Amie and her husband took newborn Victory home. The family lives north of Salt Lake City on a plot of land ringed by mountains where they raise chickens, goats and pigs along with Victory and her two brothers.
They decided to raise the baby without pushing either gender. There would be no surgery. At 18 months, Victory began gravitating toward dresses and bows, and loudly insisting on wearing her hair long. Their then-pediatrician Nisha Baur said Victory’s parents took things as they came during her earliest years. “They were very open to just accepting whatever was going to happen,” she said.
Today, Victory is a vivacious 5-year-old with a toothy grin, blond hair and a quick mind. She’s mostly deaf due to a separate genetic condition, but communicates clearly with signs, some words and sheer force of personality. She runs around the house at top speed, cradling a reluctant kitten, perching next to her great-grandmother to read a book or running for the bus in a sparkling silver backpack with butterfly wings.
Victory knows her body is different from those of her mother, father or brothers, but it doesn’t seem to bother her, Amie Schofield said.
Her eldest child lives outside the state. They recovered physically from the attack, but for months afterward there was a constant sense of deep fear. They retreated into masculine clothing, affecting as deep a voice as possible, attempting to grow out what little facial hair they have.
Knowing Victory was born intersex brought a sense of comradeship but also fear for her. “I’m scared of how society will treat her,” they said.
Victory’s parents share that apprehension. There are so many hazards ahead.
Victory’s father, Michael Schofield, formally left the Utah-based Church of Jesus Christ of Latter-day Saints shortly after she was born. The faith doesn’t have an official position on intersex people, but is doctrinally opposed to same-sex marriage and intimacy.
“Will she marry a boy or a girl? Which one is right? Which one is wrong?” said Schofield, a federal worker. “I don’t want to do that … she’s free to make her own choices.”
Her parents would like to change the designation on her birth certificate from boy to girl, but Utah law requires a court order and some judges in their area won’t approve the changes. Amie Schofield and Victory have gone to the capitol to speak out in favor of changing the law, so far unsuccessfully.
The deaf school she attends has single-user, non-gendered restrooms, but what happens if she changes schools? What will dating be like one day? Will she have trouble as she applies for jobs, or apartments, or schools? Could she also be targeted by violence? How will she feel about not being able to have children?
Her mother can only hope to teach her to handle these dilemmas herself. “It’s not something I can save her from,” Amie Schofield said.
But whatever comes, the family isn’t going to hide.
“I hate the secrecy,” she said. “She’s just so smart, so full of life. She’s just a normal girl.”
Sahred From Source link Health
from WordPress http://bit.ly/2wNtFDm
via IFTTT
0 notes
Text
5 steps to more financially stable employees
New Post has been published on https://computerguideto.com/awesome/5-steps-to-more-financially-stable-employees/
5 steps to more financially stable employees
Are financially stable employees more productive? Should your staff’s financial wellness be a priority for your business?
The short answer: Yes.
It’s understood- employees have a lot on their minds, right? And why wouldn’t they? The tasks they perform for you are extremely important.
When you see them at their desks, laser-focused on that computer screen, you just know the wheels are turning and they’re deep in thought about work.
Any minute, they’re going to give you the latest detailed information about how they’ll coming to an end that big project. Snag a new lead. Close one more deal.
But actually, what’s got their attention may be none of the above. Instead, you know what they could be thinking about?
Money. And the fear of not having enough, or not making good use of what they have.
Don’t think your employees’ cash-flow problems are any of your concern? Actually, their financial positions can affect productivity and your bottom line.
Take a look at how an employee’s fund problems can affect an entire department or organization. Then, explore a few tips you can use to help your employees feel more financially secure and improve engagement.
Employees’ money problems are also your problems
Financial security equals confidence. And when you boost your employees’ confidence, they will typically perform better than employees who absence confidence.
So, when your employees have personal stressors, like money concerns, it can affect the quality of their work. They may become more distracted and stimulate careless blunders. Also, it could lead to less social involvement with other employees.
For instance, a group of team members may go out to lunch. One employee may not join them because they don’t have the money to enjoyed the jaunt. Or, federal employees may change their behavior and stop pitching in for parties, group gifts and more.
Their co-workers’ perception may be that they’re being anti-social or inexpensive, when in fact government employees is just not comfy sharing their money fights and personal business.
When an employee is worried, unproductive and can’t afford to participate in group activities and outings because of finances, it not only affects the person but the team as a whole.
Addressing the issue: Where to start
While you may not ever know the full extent of an employee’s financial positions, there are things you can do to help them on their journey to financial wellness. Start by offering a solid benefits package that includes a great portfolio of health insurance options to choose from.
This alone can help ease some of your employees’ money concerns because they will have the opportunity to get things like medical insurance, disability, flexible spending accounts, retirement program and more.
With so many options, they won’t have to keep themselves up all night know … … if an illness or accident could ruin them financially.
Here are 5 styles you can help your employees become more financially stable :P TAGEND 1. Provide a tool to help take the guesswork out of benefits enrollment
Sometimes, employees are so afraid of a health crisis, or simply don’t know what to choose, that they end up making a fear-based decision and select a more expensive plan than they truly need.
Take purchasing car insurance, for example. Oftentimes, people will pay more monthly for car insurance so they can get a low deductible, usually $500. However, if they crunched the numbers, they could be paying more than $500 a year in higher premiums only to have the lower deductible. This is a decision based on the fear that they will get in an accident and have to come up with more than $500. The reality is that they may be better served with a higher deductible and lower monthly cost.
That’s why, when offering access to health insurance benefits, it can be helpful to provide an easy, question-and-answer tool employees can use to drill down and determine the type of coverage they actually need. Simple questions, such as “How often do you go to the doctor? ” or “How many prescriptions do you take regularly? ” are common examples.
This way, when making their elections, individual employees can feel certain they’re choosing coverage based on their actual needs instead of choosing the scheme with a level of coverage they may never need.
2. Offer disability insurance for added peace of mind
Life can happen in an instant. It could be a happy moment such as the birth of a child, or a more painful situation like an accident. In the event an employee is unable to work for a period of day, they can have peace of mind there is some level of income replacement available to them during their absence.
By offering short-term disability insurance, you allow new mamas to go on maternity leave and still get paid a percentage of their income. If an employee is involved in a non-work-related accident that prevents them from being able to do their job for a while, short-term disability insurance will fill in some of the income gap. Plus, when their short-term disability insurance runs out, long-term will kick in if they need it.
When you provide employees with disability insurance options, they’ll feel confident their financial well-being will be protected when faced with the unexpected.
3. Make a 401( k) plan available to them
For some employees , nothing’s scarier than thinking about the future and knowing they have nothing saved. They may expend countless hours worrying about how they’re going to survive in retirement. This fear could easily distract employees and make them ineffective at work, especially as they age.
When you offer a 401( k) scheme, your employees will feel more assured about their own future. As they watch their savings grow, they will not only gain more confidence in their ability to build wealth, but watch the possibility that they can have a comfy nest egg down the line. Also, offer an employer match, if possible, on percentage points of their pay. They’ll have even more money at retirement thanks to your company, plus you’ll receive a tax benefit. Everybody wins.
You may find that some employees are hesitant to join a 401( k) because they don’t understand how it runs or feel intimidated about opting investment funds. The good news is, with many 401( k) plans today, they don’t have to know the ins of outs of expending. A solid 401( k) scheme has tools to walk employees through the process and offers monies that invest to achieve results geared towards a particular retirement year.
While 401( k) savings are meant for employees to use at retirement, there are times when employees need access to their savings. If you have employees dealing with true financial hardships that are crippling them with anxiety and preventing them from doing their jobs, having access to their 401( k) may be the answer. Many 401( k) plans allow employees to access their savings through loans, withdrawals at an age earlier than retirement age, and for certain qualifying fiscal hardships. Also, historically, the federal government will relax requirements when there is a natural disaster declared in a given region.
If the plan allows these types of withdrawals, constructing sure employees understand that they may have access in a time of need may encourage them to face their fear. It can definitely help them get out of a financial crisis and ease anxiety.
4. Promote the money-saving value of a flexible spending account
Employees may overlook the benefits of signing up for a flexible spending account( FSA) simply because they don’t realize the value in it.
Since money placed in an FSA account is use-it-or-lose-it money, some employees think they’re going to lose the money. But, with a little planning, the opposite is usually true. It’s an amazing benefit and so easy to use.
For example, employees know specific expenses they’ll have every year , no matter what. This could be a new pair of glasses, recurring prescription drug expenses or copays, copays for regular doctor visits, etc. They can set pre-tax fund away in an FSA, and when it’s time to fill a prescription, pay a copay or shell out money on new glass, they can just use the money that’s available in their FSA.
Also, utilizing the FSA eliminates the need for them to figure out how they’re going to come up with a chunk of fund when they need to get that yearly eye exam and glass. For instance, individual employees will probably find it more convenient to have $35 deducted from their monthly paycheck, rather than pay $500 all at once for something they knew they’d have to pay for during the year.
FSA contributions are deducted before federal, nation, social security and Medicare taxes are calculated. Employees save money by using their FSA contributions to pay quantities that they would otherwise pay with after-tax money from their pocket. When you educate individual employees about the benefits of an FSA, you help them save money, hence adding another layer of financial assurance.
5. Don’t forget about an Employee Assistance Program
From raising kids to caring for aging parents, everything costs money. And, for employees in the sandwich generation- where they’re creating kids and taking caring of their parents at the same day- fund concerns are likely always top of mind.
It can be overwhelming- and sometimes, employees may simply need assist figuring out where they should start when trying to tackle life’s challenges.
Providing an employee assistance program( EAP) is a route you can help employees get the information and guidance they need. For instance, when they’re ready to find out more about resources available to help them care for their parents, the EAP should offer access to elder care consultation services.
Or, perhaps employees want to create a will and require legal advice. They can be referred to an lawyer and get a consultation.
Furthermore, someone on your squad is likely to be looking to adopt a child and wants advice on how to get started. The EAP can point that person in the right direction.
Best of all, consultations are free so employees don’t have to worry about spending money or period searching for guidance on their own.
Want to provide individual employees with access to benefits that will give them peace of mind about their fiscal future? Download our free e-book, HR Outsourcing: A Step-by-Step Guide to Professional Employer Organizations( PEOs ), and find out how a PEO can help you tailor a package that’s just right for your business.
Read more: insperity.com
0 notes
Video
Best Surrogacy Centres in Midnapore
Surrogacy
Meeting your surrogate or your supposed oldsters for the primary time is like happening a blind date.
You’ll be nervous. You’ll be excited. Things may feel a bit awkward initially. And you can go to the Best Surrogacy Centres in Midnapore.
There’s no ought to worry, though. Remember: area unit|you're} each are in all probability having a similar emotions!
1. Having matched surrogates and supposed oldsters for over twenty years, Circle is aware of a issue or 2 concerning finding somebody with whom you’re compatible. Our thorough matching method helps to make sure that your initial Skype video decision are going to be sure-fire.
Before your initial decision, take a deep breath and relax. Below are nine useful tips to stay in mind and obtain you thinking. Remember, each surrogate and supposed parent match decision is different!
2. Be ready. similar to happening a primary date, you’ll get the foremost out of your decision and have a better time creating a call concerning whether or not you would like to pursue a relationship if you're taking the time to arrange beforehand. begin by reviewing your potential surrogate’s or supposed parent’s profile. Then, sit down along with your partner or support person and accept the queries you have got and what you would like to accomplish throughout the decision.
3. Try to not provides a list of necessities. once you’re meeting your potential supposed oldsters or surrogate, be at liberty to debate general life-style queries and habits, however don’t arrange on giving specific directions. supposed oldsters ought to apprehend that surrogates believe the knowledgeable steerage of their obstetricians or gynecologists and alternative medical professionals. It may be tough to jilting of some management once you are having a toddler through surrogacy, however it’s a vital a part of a sure-fire journey.
Ask queries and be willing to be told. determine what crystal rectifier your potential surrogate or IPs to surrogacy. raise concerning things outside of surrogacy yet. however do they pay their free time? It’s nice to raise general questions about family and life-style.
4. Inquire, don’t interrogate. whereas you must be inquisitive, keep the oral communication lightweight. Your approach is simply as vital as your alternative of queries. the primary meeting isn't concerning screening your surrogate or supposed oldsters. Approved surrogates pass psychological associate degreed social service screenings yet as a medical records review by an IVF medical man. supposed oldsters additionally bear a screening method with our consultation team before connexion our program. Your focus throughout the match decision ought to be to urge to understand one another.
5. Discuss your hopes and expectations for communication. You’ve detected it before—communication is key! a number of our supposed oldsters and surrogates become terribly shut, refer to one another typically, and prepare many in-person visits throughout the course of the surrogacy journey. we tend to encourage open and honest relationships, however we tend to acknowledge that these will take several forms. Talking concerning your hopes for frequency/level of communication yet because the kind it'll take (Skype, phone calls, in-person visits, etc.) at this stage may be a smart plan to form certain everybody shares a similar expectations. you would possibly additionally discuss your hopes for contact when birth.
6. Refrain from talking concerning cash. monetary problems make up the umbrella of legal issues and obtain coated throughout the course of contract negotiations. you may ever be pictured by separate attorneys. Again, at this time within the method, you must specialise in going to apprehend one another. one in all the most effective benefits of operating with a surrogacy agency is that the freedom it offers you to specialise in enjoying your surrogacy journey whereas you agency takes care of the remainder
7. bear in mind this can be a street. supposed oldsters need to be told concerning their surrogates and surrogates need to be told concerning their supposed oldsters so as to form the proper call. Be ready to share your own story—what crystal rectifier you to surrogacy—talk concerning your family, and raise a similar of your surrogate or supposed oldsters.
8. Don’t stress. These calls are meant to be conversations, not interviews. Remember, you would like to form certain that you simply mesh which you share similar hopes and expectations. therefore take a breath and relax therefore you'll be able to specialise in the vital things.
9. Be honest. it's 100 percent okay to begin your decision by locution, “I simply need you to understand however nervous I am!” can|we are able to} virtually guarantee that you simply will get a loud, “Me, too!” right back. Once you get that go in the open, the oral communication can begin to flow. you're probably reaching to start a monumental journey along, it’s your likelihood to be open and honest concerning your feelings (even if they're to mention that you simply don’t apprehend what you must be talking about!).
Dr. Dipankar Mandal
Dr. Dipankar Mandal may be a medical specialist in Midnapore, West Bengal, active at Matritya - Test Tube Baby Centre. As a Fertility Centre, Matritya aims to produce best-in-class physiological state treatment to patients from Midnapur and close areas. A former prof at Sishumangal Hospital, Dr. Mandal makes a specialty of physiological state treatment, laparoscopic surgery, medicine, and urogynecology. additionally, to holding a postgraduate MD degree in OB, Dr. Mandal has cleared the MRCOG-I examination of the Royal school of Obstetricians and Gynaecologists, London.
Dr. Dipankar Mandal's special skills embody handling pregnancies and deliveries; female internal reproductive organ fibroids; chronic girdle pain and pain throughout menstruation; benign female internal reproductive organ cysts and tumours; girdle endometriosis; ectopic gestation and physiological state thanks to polycystic ovaries or blocked fallopian tubes; gynecological cancer surgery; non-descent canal hysterectomy; urological surgery; genetic tomography, and lots of additional.
Cost of Surrogacy in Midnapore
Average surrogacy engagement fees vary from $165,000 to $240,000, and actual prices can vary reckoning on the services needed for every individual scenario. prices inside this vary embody the female parent fee, management fees, the value of IVF and associated medical treatments likewise as valuation for legal, travel, maternity care, and different expenses.
We acknowledge this can be a big investment in your family and extremely suggest that you just prepare and budget suitably. we have a tendency to square measure committed to providing you with access to associate degree unequaled level of surrogate and repair and square measure happy to supply an eminent and secure platform for this sensitive endeavor. an in-depth price define of employing a female parent through our surrogacy program is going to be provided throughout your individual consultation.
Follow us on : Ela Facebook Ela Twitter Ela Instagram Ela Linkedin Ela Youtube
Get Our App : Ela App
0 notes
Text
20 Inspiring Vegan Before and After Pictures
These are our 20 most popular and inspiring vegan before and after stories from actually Happy Herbivore community members. Many of these people used our Meal Mentor meal plans to help them lose weight.
Heather M
At 39 years old, Heather found herself an overweight smoker and drinker. She had arthritis in both knees, chronic back pain, an irregular heartbeat that required medication, shortness of breath, and she suffered from severe depression. When she received a 911 call that her husband had been admitted to the hospital with 90% blockage in all four of the lower half of his arteries, she knew that it was time to take her health seriously and make a change, not only for herself but for her family.
When a co-worker purchased Heather some of Lindsay's e-books, she immediately started her research and decided to give it a try -- and the results were INCREDIBLE!
In less than a year, Heather lost 125lbs, she was no longer in pain, and was taken off her medication for an irregular heartbeat. But the healthy change had a larger effect than just on Heather’s own life. Read the full story here.
Bonebreaker
In January 2009, one month after a drug overdose, Bonebreaker was miserable. Experiencing excruciating pain from drug and alcohol withdrawal, he weighed almost 600 pounds! He soon turned his drug and alcohol addiction into a food addiction, spending over three hours at a time at Chinese buffets, often until he was kicked out. Days before checking himself into rehab he decided to make one final effort by attending a wrestling school.
After spending, the next few years trying to put together the right diet to finally get his life back on track, Bonebreaker was introduced to Dr. Carney and her husband Sean. They educated him on a whole foods, plant-based diet that turned his life around in ways he’d never imagined! Read the full story here.
Beth
Since puberty, Beth dealt with an irregular menstrual cycle, usually around 2 periods a year. When she had a period, it was awful. Her cramps were delitating to the point that she couldn’t move. Sometimes her periods were so heavy she would pass out. Eventually, she was diagnosed with Polycystic Ovarian Syndrome (PCOS) and dealt with the accompanying weight gain, acne, facial hair, and fertility issues.
Beth was determined to limit her symptoms of PCOS without the use of medication. She also wanted to avoid diabetes, something that ran in her family. After just a month on a plant-based diet, her debilitating menstrual cramps went away and she experienced more results that doctors had told her would be impossible without medication. Read the full story here.
Tara
Tara grew up on a typical southern diet of extensive meat quantities served with fried and starchy sides. Through her high school years, she was able to keep her weight down with gymnastics and an active lifestyle, but she began to struggle with her health after the birth of her daughter. Tara was dealing with constant headaches, depression, chronic constipation, fatigue, ulcers, sinus infections, and severe PMS symptoms as well as high cholesterol, blood pressure, and gastrointestinal problems.
After becoming frustrated with her debilitating health and the ever-growing list of pills, Tara decided to visit a gastroenterologist. To her surprise, it was simply recommended that she switch to a diet of little to no animal products and high in unprocessed fruits and vegetables. She almost instantly lost 25 pounds and decided to find out more about what the plant-based world was all about. Read the full story here.
Bethany
Like many people, Bethany’s weight-loss journey included a plethora of different types of diets. She’d tried various fad and crash diets. She watched her portions, counted calories, and more.
By the time she was 23 she weighed over 230 pounds, her hair was thinning, her skin was spotty, she had constant headaches, and her mood and energy levels were rapidly declining.
Later that same year Bethany’s brother shared a PBS special with her featuring Dr. Joel Fuhrman. She immediately ordered Dr. Fuhrman's plant-based book and never looked back from there! Read the full story here.
Rebecca A
Rebecca’s struggle with self-image goes all the way back to when she was 10 years old and decided to join Weight Watchers in hopes of losing weight. Her yo-yoing battle with weight continued up through the birth of her son when she had reached 275 pounds. Just moving around had become a painful task. She decided that she needed to make a healthy change and eliminated dairy and land animals from her diet.
As she continued down the road of plant-based living and began seeing results, Rebecca’s stepmother gave her a copy of Lindsay’s “Everyday Happy Herbivore.” She loved it so much that she then purchased “The Happy Herbivore Cookbook” which launched her on a journey that resulted in losing 150 pounds and so much more. Read the full story here.
Elicia
Elicia was a victim of bullying that continued well into her adulthood. She found herself in the midst of bad relationships and a bad marriage. The difficult circumstance and bullying made her resort to stress eating. Her health spiraled out of control as her weight reached almost 500 pounds. She decided to move herself and her children to her parents' house where she rarely went outside and was only able to walk with crutches.
When her parents tried out a juice cleanse, Elicia figured she it was worth a shot and was amazed. She lost 50 pounds in under 50 days! She and her parents decided to continue their weight-loss journey together by adopting a plant-based diet. Read the full story here.
Amy B.
Amy was raised on a vegetarian diet and maintained a low weight for most of her life, but at the cost of poor nutritional eating and near starvation. Tragedy struck when she and her husband had 3 miscarriages in the span of a year and a half. Amy fell into a deep depression and turned to fast food and “comfort eating.” Things started to looked up when Amy and her husband decided to seek fertility treatment and within a year were blessed with a baby girl.
The joy of finally having a child was soon accompanied by anxiety about being new parents, and Amy’s eating habits and health began to take a turn for the worse. Just before her 40th birthday, Amy found herself completely sedentary and decided to revisit her vegetarian diet. Despite her best efforts, Amy only continued to gain weight. In a desperate search for a cookbook that would work for her, she stumbled upon “Everyday Happy Herbivore” and transformed her life, losing 100 pounds in the following 10 months! Read the full story here.
Lindsay’s Dad
Lindsay’s dad recounts a recent trip where he found himself at a loss for words as he attempted to explain just how much better he felt after switching to a plant-based diet. It was easy for people to see the physical signs of the change due to the 20 pounds he’d lost, but the impact on his life went far beyond a physical level. Even at the age of 67, he found that his quality of life was the best it had been in many years. Read the full story here.
Mary Lou
Mary Lou was suffering from several chronic autoimmune diseases: severe rosacea, psoriatic arthritis, for which she had to take to Enbrel injections, and she also dealt with asthma, brain fog, depression, joint pain and chronic fatigue, among other issues. After reading an article claiming that over 40% of the population suffers from non-celiac gluten intolerance and seeing a list of symptoms that mirrored her own, Mary Lou decided to cut gluten from her diet. 4 weeks on a gluten-free diet and her symptoms were gone!
Mary Lou knew that dairy sensitivity and gluten sensitivity usually went hand-in-hand, so she decided to take the plunge and go plant-based. Despite the difficulty of giving up things like ice cream and cheese, she stuck with it and soon felt better than she had in over 20 years. She recovered from ailments she didn’t realize she had been dealing with, and began a whole new way of life. Read the full story here.
Brenda
Brenda began to experience decreased levels of energy, nerve pain, and a progressive foot drop. She visited her doctor for testing and was told she had ALS and didn’t have long to live. Shocked with the news that no one ever wants to hear, Brenda decided to seek a second opinion. Doctor after doctor gave her the same diagnosis and said she was going to die.
Brenda had already made a switch to see the benefits of a plant-based diet a few years prior and decided to stick with it and not give up hope. Read the full story here.
Adam
Adam was always heavier than most of his friends growing up, but despite his weight, he was able to maintain an active lifestyle playing basketball, mountain biking, and other teenage outdoor activities. Things changed in college with his newfound freedom, leaving him less time for an active lifestyle. By the time Adam turned 28, he weighed 290 pounds and had a 44-inch waist size. That same year his wife gave birth to their son, and Adam felt a newfound motivation to get back in shape to enjoy activities with their son.
Adam tried low-carb diets, prepackaged weight-loss meals, shakes, and daily exercising, but he wasn’t seeing any results. He talked to his wife and decided to go one week with no meat, no cheese, no oil or processed foods. Before long that one week turned into two years and Adam lost an AMAZING 135 pounds! His success also encouraged his wife to adopt a plant-based diet. Read the full story here.
Lisa P
Inspired by an Oprah one week vegan challenge, Lisa decided to challenge herself to going two weeks vegan. So impressed by the results, Lisa stuck with the diet and went from size 16 to size 4 in the first year of plant-based living! She recounts that the weight just started falling off. Even after being addicted to fat and sugar for all of her life, she found that when she totally eliminated processed foods, sugar, and oils, she no longer craved them. Lisa found that the incredible weight-loss was only the beginning of her transformation after going plant-based. Read the full story here.
Kathy
For nine long years, Kathy and her husband battled devastating infertility. After many invasive tests, seeing doctors in both Canada and the United States, they were blessed by the birth of their miracle twins. Kathy had already been plant-based for over ten years, but had succumbed to anxiety during her pregnancy that her babies would not be getting the best nutrition. She was quickly overwhelmed by the amount of literature surrounding pregnancy nutrition and sickened by the thought of reverting to an omni diet. She decided to stick with her plant-based diet, knowing it would be the best option for both her and the twins. Read the full story here.
Courtney B.
After a bout in the hospital, Courtney lost her house and overall footing in life. She was homeless and lost. With no sense of direction, she knew one thing was certain: she was going to maintain her plant-based diet. After being previously abused by people who said they loved her, Courtney recounts that her pets were the ones that had been there for her. She promised them she would no longer eat animal meat. With those strong morals about being vegan, she swore to stick to a plant-based diet, even during her time of homelessness. It was no easy task, but she was able to receive things like carrots, bananas, and juices from the people she stayed with and occasionally pulled peanuts from vending machines.
Courtney tells her emotional story, gives her advice on never giving up, staying true to your beliefs, and how she was able to maintain a plant-based diet against all odds. Read the full story here.
Denise
Tracy tells the story of her 43-year-old mother, Denise, who was put into a nursing home due to complications from multiple sclerosis. After attempting to transition Tracy to a vegetarian, her health continued to decline to a point that she was having up to 20 seizures a day and needed constant monitoring. Tracy decided to move Denise back home to take care of her and began preparing pureed foods using fresh fruit, vegetables, and whole grains.
Within the first year of being plant-based, Tracy saw a miraculous improvement in her mother’s health. The extra weight was coming off, oxygen dependence was eliminated, her BiPAP went away, and her list of daily medications was shrinking! Read the full story here.
Kristie
Kristie was nearly 300 pounds when her mother died of colon cancer. Her mother’s passing left her devastated, depressed, and grappling with the fact that she could be headed down the same path if she didn’t make a change. One day while she was laying down crying, she heard a voice say, "If you don't want to be fat, do something about that!"
That same day she googled plant-based diets and decided to give it a try. The first 30 days were the hardest, but was she able to stay on the wagon. To her amazement, after just a month she’d already lost 16.5 pounds and found that she had actually begun to enjoy the plant-based recipes she was making. With her dedication, the results kept coming! Read the full story here.
Rebecca
Rebecca’s story started in college where her freshman 15 had turned into 50 by the time she had graduated. Years had passed and the weight still wasn’t coming off. She had started to experience mood swings and depression, so she quickly visited her doctor who prescribed her antidepressants and sent her on her way. The medication offered her little relief, and even after adopting a vegetarian diet the weight just wasn’t coming off.
Rebecca continued pressing on and came across the Happy Herbivore website. She was instantly in awe of Lindsay’s perseverance and came to the realization that she was putting too much focus on material happiness. She began a process of decluttering, letting go of material baggage, and focusing on the journey, not just the destination. Read the full story here.
Sarah
Growing up, Sarah watched her father struggle with obesity. No matter what he tried, he wasn't able to maintain any weight loss. At age 24 she was pulled aside at work for the shocking news that her father had suffered a massive heart attack and had passed. Sarah’s world was rocked by her father’s death. It gave her a wake-up call: if she continued to follow the path he had been on, she was already halfway through her life.
It took 2 years, but Sarah finally made a change. A fellow nurse practitioner at the hospital where she worked recommended she try a plant-based diet. "For someone with your family history, it's the best thing you could do for yourself." The idea finally clicked. Months later, Sarah had already shed 116 pounds and was feeling better than she’d felt in years! Read the full story here.
from Recipes Blog https://happyherbivore.com/2018/06/vegan-before-and-after-pictures/
0 notes
Text
Ask Lisa: An Atypical Transracial Adoption
Atypical Transracial Adoption
In today’s column, when a black woman and her white husband adopt a biracial baby who appears white, mom faces painful slights from strangers and her in-laws. The new mother expresses concerns about her atypical transracial adoption.
Dear Lisa,
My situation is what you might call an atypical transracial adoption. That’s what it looks like, even if it’s not technically a transracial adoption at all.
My husband is white and I am black. When we married, many people in his family were against the marriage, but I thought they would come around once we began our family. After four years of trying, including two in-vitros which were not successful (the issue was with me, which gave his family more reason to look down on me), my husband and I were not able to conceive and turned to adoption.
Once our home-study and paperwork were complete, our social worker put us on the list to adopt a biracial baby, which we had requested. We were fortunate to be chosen remarkably quickly by a young woman who wanted to meet us. She was still pregnant, very young and white/Irish (like my husband) and said she could not keep the baby because the birth father was black and her parents would not accept it. We felt for her and were honored to be chosen, though the girl made it clear that she was only comfortable placing the baby with us because my husband’s family sounded like her own. I was so desperate to be a mother, it didn’t bother me that she chose us because of my husband and not me.
Fast forward one year. We are now thrilled to be the parents of a beautiful, happy, healthy eleven-month-old girl whom I would not trade for the world. My husband travels a lot and I work from home, so I get to spend almost every minute with her. The only issue is that our daughter is extremely fair with light eyes and hair like her birth mother. She shows no sign of having African ancestry. (The agency told us that the birth father was black, just very light.) When it’s just the three of us, or just the baby and me, everything is great—I feel bonded and connected and totally her mom. But when we get outside, all anyone seems to see is that I am black and my baby is white.
Atypical Transracial Adoption: In the Emergency Room
Everyone has something to say—most people assuming I am her nanny, but then inquiring how and why I would adopt a white child when there are black children who need homes. The worst was a trip to the emergency room when the nurses refused to believe I was my daughter’s mother and one wanted to call the authorities, implying I had stolen a white baby. (Our pediatrician had to call and vouch for me.) We live in a diverse area where I have white friends who have adopted transracially, either black or Asian children. They say they too have had mix-ups like this, but I think it is different when the parent is a person of color and the child doesn’t appear to be. My white friends hate it when people tell them how wonderful they are to accept children of color. But people act as if I don’t deserve to be my daughter’s mother.
The hardest part is my in-laws. They are thrilled with the baby, but becoming grandparents has not led them to accept me like I had hoped. If anything, they leave me out more than before, always taking photos of the baby with my husband and other family members, but not with me. My husband doesn’t see it and says I am overreacting. He even suggested that the problem was me resenting our sweet baby for looking white! I don’t, but all of this is shaking my confidence as a mother. I cannot forget that without my husband’s family background her birthmother would never have chosen us. How do I stop feeling like a second-class mother?
Signed, Hurting
Dear Hurting,
Though there is no such thing as a typical family of any kind, your “atypical transracial adoption,” is indeed unusual. In most (though not all) transracial adoptive families, the child rather than the parent is non-white. In these situations, parents are aware from the beginning that theirs will be a visible adoption and that they must prepare for intrusive, often offensive, questions. (e.g. Where did you get him? What do you know about her kind of hair?) When I used to do homestudies, I always encouraged white parents adopting children of color to consider that they would no longer be a white couple, but instead a multiracial family. While racial difference has always been part of your marriage, you expected your child to reflect both your and your husband’s races—not his alone. Furthermore, it sounds as if you were hoping the addition of your daughter would stretch your in-laws’ biases, leading them to embrace you along with the baby. Instead, because of your daughter’s appearance, which currently favor theirs, you feel further alienated.
On one hand, I could reassure you that children’s features change as years go by (see my last post). But there is no guarantee that this will happen. In fact, it is possible, since you didn’t actually meet him, that the birth father is not black at all. That doesn’t mean your daughter is any less yours than she is your husband’s. Instead, you must take the cards you’ve been dealt and make the very most of them.
Here are my suggestions:
1) Insist that your husband’s family change their attitude toward you.
If necessary, make their visits with your daughter contingent on this. This may sound harsh, but you are their granddaughter’s mother. It would be harmful to your daughter to internalize negative messages about blackness that she may be receiving from your husband’s family.
You will need to gain your husband’s support in this, as he should be the one to address it with his parents. Your husband has accused you of overreacting. Yet he has witnessed his parents’ failure to support the marriage, meaning he cannot deny that racial bias exists. I’m also assuming you told him about the emergency room visit, which highlights the unique challenges you face as a woman of color. I cannot stress enough how important it is for your husband to understand where you are coming from. If you are unable to get him to hear you, a session or two with an experienced couples’ therapist in your area may help.
2) Gain Support from your own family and friends.
Is your family around the baby as much as your husband’s? Will your little girl grow up feeling that she belongs to both sets of relatives? If possible, make sure there is some balance here.
Also, spend plenty of time with friends who validate your experiences. Find a support group, or start an informal gathering of moms of color who are coping with “Nanny Syndrome” (being repeatedly mistaken for their children’s babysitter) and other familiar issues. Bond with these mothers, laugh, share stories, triumphs and coping tips.
3) Live in a diverse community full of families of different racial and ethnic descriptions.
The more your daughter sees that families are about love and caring and less about matching skin tones and hair textures, the more comfortable she will be, both among family and out in the world.
4) Immerse your daughter in the shared culture of your home.
Interracial relationships work best if both members of the couple create a joint culture in their home. Regardless of your daughter’s appearance, she is entitled to be versed in your culture as much as your husband’s. When a child joins a family by adoption, the child brings her birth culture into the home but also inherits through adoption the cultures of her new parents.
5) Lastly, more importantly, focus on the joy of being a mother.
What an “atypical transracial adoption” has in common with a “typical” transracial adoption is the scrutiny of outsiders. Strangers will have their opinions but it is up to you to minimize their influence on your confidence as a mother. You acknowledge that things are great when you and your daughter are alone together, so enjoy it. Remember, there is so much more to motherhood than what the two of you look like. Love her. Teach her to love the things you love—art, music, sports, food, books. Talk to your baby, share with her, learn from one another and allow her to flourish in the beautiful uniqueness of your life as a family.
Ask Lisa: An Atypical Transracial Adoption if you want to check out other voices of the Multiracial Community click here Multiracial Media
0 notes
Last Seen Blogs

intuitiveguitarist
Intuition is Everything

holografrick
i draw

astro-pops
it's all happening

lovelyshoots
LOVELY

impulse-goblin
stupider like a fox!