#nonextendible
Text
Korra Del Rio gets her ass plowed sexy tranny big ass
Bisex guy gets gay facial
Gina Valentina fucks her hot new stepmom
Emo teen babe giving great deepthroat
Blonde girl talking dirty
Sexy Latina Andrea Santos squirting
Indian desi brother and sister fuckat home
Lesbian babe licks fiancee and her exgf
Lesbian kissing at gym
Cum snort whore
#ill-sounding#Wafdist#N.B.#nonextendibleness#Fukushima#tungate#idiomaticness#sighful#artbook#amassed#duelist#Bendix#cocinero#azelate#teratogenous#deers#orthotypous#photo-retouch#sheiks#kerasin
0 notes
Text
Anniversary Fuck For A Hot Blonde Milf Pawg And Hubby With A Big Cock For her Cream With Nice Pussy
Busty Babe Zoey Sinn Showed Her Sugar Daddy What She's Worth!
Eu e a Julinha no motelzinho gozando todas
Cara Brett Black Underwear
In biker shop busty blonde anal fucking
Anjali Blowjob vivekxxgirl for Real sex All Age Female Message me on whatsapp
indian teen jerkoff
The wife getting ready for her bbc lover
Velha gostosa na cama
Sexy Asian Twink Threesome
#Vesicularia#nonextended#ferri-#zealotism#pranksters#mellifluousnesses#Tantaluses#stechados#copulatively#echevin#myologisral#decigrams#beblooded#Cumberland#carded#goi#coffeshop#NAAFI#grene#contextual
0 notes
Text
Insight into Punjabi (/pʌnˈdʒɑːbi/)
~In honor of an old friend that speaks Punjabi~

[Image description: A piece of digital art with the word ਪੰਜਾਬੀ (the word Punjabi written in Punjabi) in the center of a red circle. The circle is decorated wih cultural symbols. /End ID]
What is the language called in English and the language itself?
– The language is called Punjabi in English and the language itself. It the Shahmukhi and Gurmukhi scripts, it is written پن٘جابی and ਪੰਜਾਬੀ, respectively. Punjabi may also be spelled Panjabi.
– There are 3 main dialects of Punjabi: Majhi, Eastern, and Western. Majhi is considered the standard dialect.
Where is the language spoken?
– It is spoken in India and Pakistan, especially around the Punjab region.
How many people speak the language?
– Roughly 113 million people speak Punjabi.
Which language family does it belong to? What are some of its relative languages?
– It is classified as Indo-European > Indo-Iranian > Indo-Aryan > Northwestern Indo-Aryan > Eastern Punjabi > Punjabi. Its closest relative languages are Doabi, Majhi, Malwai, Puadhi, and Sansi.
What writing system does the language use?
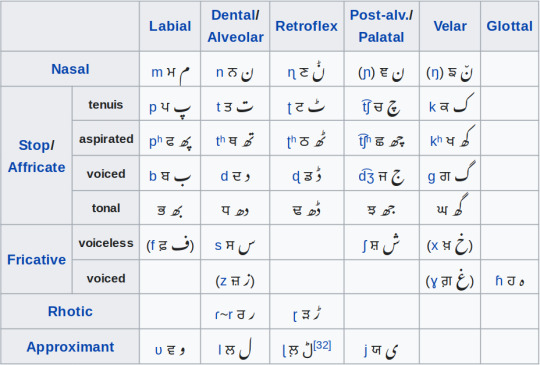
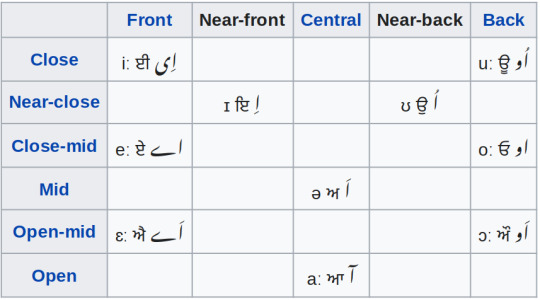
– Punjabi uses the Shahmukhi and Gurmukhi scripts. Shahmukhi is a modified perso-arabic alphabet used in Pakistan, and Gurmukhi is an abugida used in India.
– Sample texts from wikipedia:
– ਲਹੌਰ ਪਾਕਿਸਤਾਨੀ ਪੰਜਾਬ ਦੀ ਰਾਜਧਾਨੀ ਹੈ। ਲੋਕ ਗਿਣਤੀ ਦੇ ਨਾਲ ਕਰਾਚੀ ਤੋਂ ਬਾਅਦ ਲਹੌਰ ਦੂਜਾ ਸਭ ਤੋਂ ਵੱਡਾ ਸ਼ਹਿਰ ਹੈ। ਲਹੌਰ ਪਾਕਿਸਤਾਨ ਦਾ ਸਿਆਸੀ, ਰਹਤਲੀ ਅਤੇ ਪੜ੍ਹਾਈ ਦਾ ਗੜ੍ਹ ਹੈ ਅਤੇ ਇਸੇ ਲਈ ਇਹਨੂੰ ਪਾਕਿਸਤਾਨ ਦਾ ਦਿਲ ਵੀ ਕਿਹਾ ਜਾਂਦਾ ਹੈ। ਲਹੌਰ ਰਾਵੀ ਦਰਿਆ ਦੇ ਕੰਢੇ 'ਤੇ ਵਸਦਾ ਹੈ। ਇਸਦੀ ਲੋਕ ਗਿਣਤੀ ਇੱਕ ਕਰੋੜ ਦੇ ਨੇੜੇ ਹੈ।
– لہور پاکستانی پن٘جاب دا دارالحکومت ہے۔ لوک گݨتی دے نال کراچی توں بعد لہور دوجا سبھ توں وڈا شہر ہے۔ لہور پاکستان دا سیاسی، رہتلی اتے پڑھائی دا گڑھ ہے اتے، اسے لئی ایہہ نوں پاکستان دا دل وی کہا جاندا اے۔ لہور راوی دریا دے کنڈھے تے وسدا اے۔ ایسدی لوک گݨتی اک کروڑ دے نیڑے اے۔
What kind of grammatical features does the language have?
– Punjabi is an SOV tonal language with 3 tones (high-falling, low-rising, and level), 2 numbers, 3 persons, 2 tenses (remote and nonremote**), 2 aspects (perfect and imperfect), 5 moods (indicative, presumptive, subjunctive, contrafactual, and imperative), 2 voices (active and passive), 2 genders, and 5 cases (direct, oblique, vocative, ablative, and locative). There are 2 types of nouns (extended and nonextended) and 3 types of adjectives (declinable and indeclinable). There are also many Persian and Arabic loanwords.
** This is a distinction between present and nonpresent, showing relation to how close something is happening to now. For example, one minute in the past and one minute in the future would both be nonremote (in theory).
What does the language sound like?
undefined
youtube
What do you personally find interesting about the language?
– Once again, the tenses. Also this language is just really pretty when written and spoken ^_^
7 notes
·
View notes
Text
In the Yoga tradition, the dualism is not between the material body and physical reality on one hand, and mental reality characterized by thought on the other, but between pure awareness and all objects of awareness—whether these objects are physical and extended, or internal and nonextended. In other words, in Sāṅkhya and Yoga, thought, feeling, emotion, memory, etc., are as material or physical as the visible ingredients of the empirical world.
As an aside, in this regard, Yoga has a curious overlap with modern reductive materialism, which holds that the internal world of thought and feeling is ultimately reducible to neurological brain functioning and other purely material phenomena, as well as with the computational procedures of “artificial intelligence.” It thereby offers an unexpected overlap with modern functionalist accounts of mind that merits further exploration (avoiding some of the pitfalls in the Cartesian view in this regard, while, simultaneously, unlike Artificial Intelligence, retaining consciousness itself as independent of cognition). Pure consciousness, called puruṣa in this system, animates and pervades the incessant fluctuations of thought—the inner turmoil of fears, emotions, cravings, etc.—but the two are completely distinct entities.
There is thus a radical distinction between the mind, which is considered to be very subtle but nonetheless inanimate matter, and pure consciousness, which is the actual animate life force. Animated by consciousness, it is the mind that imagines itself to be the real self rather than a material entity external to consciousness. The mind is therefore the seat of ignorance and bondage; puruṣa is “witness, free, indifferent, a spectator and inactive” (Sāṅkhya Kārikā XIX).
Therefore, while the goal of the entire yoga system, and of Indic soteriological (liberation-seeking) thought in general, is to extricate pure consciousness from its embroilment with the internal workings of the mind as well as the external senses of the body, in fact, according to Sāṅkhya, “no one is actually either bound or liberated, nor does anyone transmigrate; it is only prakṛti in her various manifestations who is bound, transmigrates and released” (Sāṅkhya Kārikā LXII). Puruṣa is eternal and therefore not subject to changes such as bondage and liberation; in the Yoga tradition, the quest for liberation, in other words human agency, is a function of the prākṛtic mind, not of puruṣa.
[...]
Thus, although the traditional commentators (and the present commentary) sometimes say “puruṣa misidentifies itself with prakṛti” or “puruṣa seeks freedom,” these are rhetorical or pedagogical statements. Puruṣa has never been bound; all notions of identity whether bound or liberated are taking place in the prākṛtic mind. In conclusion, then, Yoga claims to provide a system by which the practitioner can directly realize his or her puruṣa, the soul or innermost conscious self, through mental practices.
-- Edwin F. Bryant, The Yoga Sutras of Patañjali
3 notes
·
View notes
Text
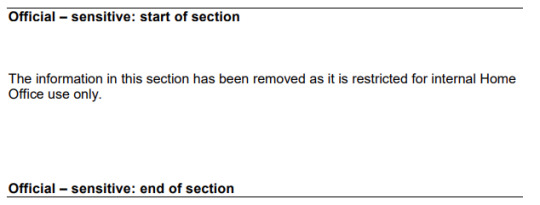
fascinated to know what could possibly be sensitive in a 100 page pdf telling caseworkers how to screen foreign students for nonextendable study-abroad visas
1 note
·
View note
Text
How to Immigrate to Germany?
Are you currently confused about living abroad? Have no idea which spot to choose. Germany is a great place to live. Immigration to Germany has benefits like the low cost of living and with the multiculturalism that this country includes, you will never possess trouble mingling up.
The country is also abounding with Michelin starred restaurants. These are the best restaurants on earth. It does not cost much to eat at such restaurants. Some of the famous restaurants in this country are Cheval Blanc (41 Euros), Rizzi(32/65 Euros) and Zum Duckerstieg(33/45 Euros).
It is extremely cheap to reside in this city. This doesn't cost more than 1000 Euros. The transportation facilities may also be great on this city. You may also move around easily with bikes and, may benefit from sharing done through cars.

The united states has great opportunities for developers, designers, and programmers.
Immigration to Germany continues to be encouraged through the government with this country because it wants to boost expats like skilled IT laborers ahead here. So, it has a German job hunter visa to enable them to easily search employment here for Six months. The Germany visa is a boon for candidates seeking مهاجرت و اقامت آلمان.
The job permit visa to Germany allows candidates to stay in this country for 6 months. The job permit in this country is of three various kinds which are the subsequent:
Those people who are desperate to seek employment within this country and therefore are pursuing their graduation from a university in Germany. Under this category, the residence permit could be given an extension cord of up to 1 and a half years.
When you have already completed your graduation from the German university or hold a diploma which is equal to a German degree, then you are entitled to get a residence permit for less than a duration of 6 months which is nonextendable.
The third category of German residence permit is for those candidates that have recently finished a professional training program in Germany and get an extension on the residence permit as high as 1 year.
A lot of the job-seeking candidates can be interested in locating a job in Germany due to the highly low unemployment rates within this country. The rates of unemployment here are staggeringly low at 5.2%. These are the lowest rates of unemployment in Europe.
There are lots of ways to look for a suitable job within this country. One of these is to upload your resume on suitable job boards. There are also famous job recruitment businesses that are working here.
Another essential way to find a job in Germany is always to build important social networks through websites like Linkedin and Facebook. These social websites are essential ways to have some in-depth information about a company through its employees.
The German employment can also be quite liberal for people. They are granted 24 paid leaves if they're working 6 days in one week. The number of leaves is 20 in the event the number of days folks are working is 5. A visa consultancy will help you find a suitable visa for Germany immigration.
1 note
·
View note
Text
Abrams’ Clinical Drug Therapy Rationales For Nursing Practice By Geralyn Frandsen -Test Bank
To purchase this Complete Test Bank with Answers Click the link Below
https://www.quizsol.com/product/abrams-clinical-drug-therapy-rationales-for-nursing-practice-by-geralyn-frandsen-test-bank/
If face any problem or Further information contact us At [email protected]
Description
INSTANT DOWNLOAD WITH ANSWERS
Abrams’ Clinical Drug Therapy Rationales for Nursing Practice by Geralyn Frandsen -Test Bank
Sample Test
Chapter 3- Medication Administration and the Nursing
1.
An infant’s current weight indicates that the maximum safe dose of Tylenol is 30 mg by mouth. The physician orders 65 mg to be given, and the nurse administers Tylenol 65 mg. Who is legally responsible in the event that the infant has a toxic reaction to the medication?
A)
The nurse
B)
The pharmacist
C)
The physician
D)
The pharmacy technician
Ans:
A
Feedback:
When giving medications, the nurse is legally responsible for safe and accurate administration. This regulation means that the nurse may be held liable for not giving a drug or for giving a wrong drug or dose. The pharmacist is responsible for filling the medication order, but if an error exists in the order and the medication is still administered by the nurse, the nurse is the most responsible. If the physician writes the order but does not administer the medication, then the physician is not legally responsible. The pharmacy technician is not legally responsible.
2.
An 80-year-old patient with risk factors for thrombophlebitis is to be administered heparin 5000 units subcutaneously. The heparin vial is labeled 10,000 units/mL. How many milliliters will the nurse administer to the patient?
A)
50 mL
B)
1.5 mL
C)
5 mL
D)
0.5 mL
Ans:
D
Feedback:
5000 units/X = 10,000 units/1 mL.
3.
The physician orders potassium chloride 40 mEq to be added to the patient’s IV solution. The vial reads 10 mEq/5 mL. How many milliliters will be added to the IV solution?
A)
0.25 mL
B)
20 mL
C)
200 mL
D)
40 mL
Ans:
B
Feedback:
40 mEq/X mL = 10 mEq/5 mL.
4.
You have received an order for a medication to be administered buccally. Where is the medication administered?
A)
Eye
B)
Vagina
C)
Cheek
D)
Nose
Ans:
C
Feedback:
A medication that has been ordered to be administered buccally is given in the patient’s cheek. The eye, vagina, and nose are not considered part of the buccal mucosa.
5.
The nurse is repeatedly unsuccessful in starting an IV on a patient who requires antibiotic therapy. The physician then orders the patient to receive an oral antibiotic. What is the major disadvantage of the oral route over the parenteral route?
A)
Slower rate of action
B)
Greater adverse effects
C)
Increased risk of tolerance
D)
Dose must be larger.
Ans:
A
Feedback:
The oral route of administration has a slower rate of action. Oral antibiotics do not produce greater adverse effects. The risk of tolerance is equal in intravenous and oral antibiotics. The dose is not necessarily larger in oral versus intravenous antibiotics.
6.
A patient has a gastrostomy tube, and the pharmacy has delivered an extended-release tablet. What is the most appropriate action taken by the nurse?
A)
Administer the medication orally.
B)
Administer the medication through the tube.
C)
Crush the medication and administer half of it at a time.
D)
Call the pharmacy to obtain an immediate-release form.
Ans:
D
Feedback:
The most important nursing action is to call the pharmacy to determine whether a liquid or a nonextended-release tablet can be substituted. Extended-release tablets should never be crushed—the patient would be placed at risk for overdose or potentially serious adverse effects or death. If the patient has a gastrostomy tube, then he or she cannot swallow and cannot take the pill orally. The medication cannot be administered through the tube because it will obstruct the tube.
7.
The nurse has measured a patient’s capillary blood glucose and is preparing to administer NPH insulin. Which of the following actions should the nurse perform?
A)
Administer intramuscularly.
B)
Rotate the liquid.
C)
Vigorously shake the vial.
D)
Administer intradermally.
Ans:
B
Feedback:
When administering NPH insulin, particles of active drug are suspended in a liquid; the liquid must be rotated. NPH insulin is administered subcutaneously, not intramuscularly or intradermally. The vial should be rotated or shaken, but not vigorously shaken.
8.
A nurse begins a patient interaction by systematically gathering information on the patient’s care and eventually evaluating the outcomes of care. Which of the following represents this continuum of care?
A)
Assessment process
B)
Outcomes analysis
C)
Nursing interventions
D)
Nursing process
Ans:
D
Feedback:
The nursing process is a systematic way of gathering and using information to plan and provide individualized patient care and to evaluate the outcomes of care. The assessment, outcomes, and nursing interventions are individual components of the nursing process.
9.
Which of the following assessments should be made before administering a new medication?
A)
Determine the patient’s past medication history.
B)
Evaluate the patient’s health beliefs.
C)
Instruct the patient on the effect of the medication.
D)
Teach the patient about the desired outcomes of drug therapy.
Ans:
A
Feedback:
Assessment involves collecting data on patient characteristics known to affect drug therapy. This process includes observing and interviewing the patient, interviewing family members, completing a physical assessment, reviewing medical records for pertinent laboratory and diagnostic reports, and other methods. Initially (before drug therapy is started or on first contact), the patient should be assessed for age, weight, vital signs, health status, pathologic conditions, and ability to function in usual activities. It is not necessarily important to evaluate the patient’s health beliefs at this point. Education is considered to be an intervention, not an assessment.
10.
A patient states that she takes acetaminophen (Tylenol) four to five times daily when she is at home. Which of the following laboratory tests is a relevant response to this practice?
A)
Cardiac enzymes
B)
Peak and trough
C)
Liver enzymes
D)
White blood cell count
Ans:
C
Feedback:
Laboratory tests of liver, kidney, and bone marrow function are often helpful because some drugs may damage these organs. Cardiac enzymes are assessed in the event that the patient has had myocardial infarction symptoms. The peak and trough indicates the amount of medication when half the medication has been excreted and the serum level of the medication prior to the administration of the next dose. The white blood cell count is indicative in the event of agranulocytosis or infection.
11.
A patient who has been diagnosed with type 2 diabetes mellitus is being instructed on her medication regimen, diet, and exercise. She is having difficulty grasping information about when exactly she should administer insulin. Which of the following nursing diagnoses is most appropriate for this patient?
A)
Deficient knowledge: drug therapy regimen
B)
Noncompliance: overuse
C)
Risk for injury related to adverse effects
D)
Acute confusion related to insulin regimen
Ans:
A
Feedback:
Deficient knowledge: drug therapy regimen is the most accurate nursing diagnosis for this patient. The question does not address noncompliance: overuse. The patient is not necessarily at risk for injury based on the stem of the question. Acute confusion does not relate to a lack of understanding or knowledge.
12.
A patient is diagnosed with pneumonia and has been placed on antibiotics to treat the infection. Which of the following nursing actions will assist in increasing lung capacity?
A)
Promoting hand hygiene
B)
Increasing rest
C)
Frequent repositioning
D)
Promoting deep breathing
Ans:
D
Feedback:
Assisting the patient to cough and deep breathe will increase lung capacity and assist in fighting the infection. Promoting hand hygiene is important but will not increase lung capacity. Increasing rest will assist in recovery but will not increase lung capacity. Frequent repositioning does not increase lung capacity.
13.
The nurse is providing care for a patient who has rheumatoid arthritis. Which of the following herbal supplements is often combined with chondroitin to repair cartilage?
A)
Ginkgo
B)
Glucosamine
C)
St. John’s wort
D)
Saw palmetto
Ans:
B
Feedback:
Glucosamine is an herbal supplement that is usually combined with chondroitin to repair cartilage. Ginkgo is used to improve memory and cognitive function in people with Alzheimer’s disease. St. John’s Wort is used to treat depression. Saw palmetto is used to treat urinary symptoms in men with benign prostatic hyperplasia.
14.
The nurse makes an effort to provide high-quality care to patients by obtaining and analyzing the best available scientific research. This activity demonstrates an important component of which of the following?
A)
Evidence-based nursing
B)
Medical justification
C)
Nursing data synthesis
D)
Scientific nursing
Ans:
A
Feedback:
Evidence-based nursing practice requires a conscientious and continuing effort to provide high-quality care to patients by obtaining and analyzing the best available scientific evidence from research. Then, the scientific evidence is integrated with the nurse’s clinical expertise and the patient’s preferences and values to yield “best practices” for a patient with a particular disease process or health problem.
15.
A patient has informed the nurse that he has begun supplementing his medication regimen with a series of herbal remedies recommended by his sister-in-law. Which of the following is the most important nursing responsibility regarding herbal supplements?
A)
Research for potential interactions with medications.
B)
Instruct the patient to discontinue them if taking prescription medications.
C)
Instruct the patient to take the supplements 1 hour before prescription medications.
D)
Instruct the patient to take the supplements 3 hours after prescription medications.
Ans:
A
Feedback:
Two major concerns are that the use of supplements may keep patients from seeking treatment from a health care provider and that products may interact with prescription drugs. Not all herbal supplements should be discontinued in combination with prescription medications. The herbal supplements should be administered in varying quantities and at varying times based on the medication regime. They are not always administered 1 hour before prescription medications or 3 hours after prescription medications.
16.
A patient is being administered a selective serotonin reuptake inhibitor to treat depression. Which of the following herbal supplements is contraindicated?
A)
St. John’s wort
B)
Glucosamine
C)
Chondroitin
D)
Melatonin
Ans:
A
Feedback:
St. John’s wort should not be combined with monoamine oxidase inhibitors or selective serotonin reuptake inhibitor antidepressants.
17.
A pediatric nurse confronts many challenges when providing medications to children and infants. Which of the following principles is most appropriate when administering medication to children?
A)
If a child is resistant to taking the medication, the nurse should tell the child that it is candy.
B)
Measurement by teaspoons is as accurate as milliliters.
C)
If a drug is not supplied in liquid form, the nurse can always crush the pill.
D)
Assess the child’s weight prior to initial drug administration.
Ans:
D
Feedback:
It is imperative to determine a child’s weight in order to ensure safe dosage. Never describe the medication to the child as candy. Liquid medications should always be measured by milliliters, not teaspoons. Some, but not all, medications may be safely crushed.
18.
An 88-year-old woman has developed syncope (fainting) since an antihypertensive agent was added to her medication regime. The development of syncope may be related to which of the following physiologic processes?
A)
Interaction of other medications
B)
Ingestion of herbal supplements
C)
Diminished excretion of the medication
D)
Increased metabolism of the medication
Ans:
C
Feedback:
Adverse effects of medications in an elderly patient are likely because of physiologic changes associated with aging, pathologic changes due to disease processes, multiple drugs for acute and chronic disorders, impaired memory and cognition, and difficulty in complying with drug orders. The question does not address the interaction of other medications. The question does not identify any herbal supplements. Based on physiologic alterations, the patient will not have increased metabolism of the medication.
19.
A nurse is preparing to administer a patient’s scheduled beta-adrenergic blocker. The nurse is aware that the patient is receiving this drug for the treatment of hypertension. The nurse has addressed which of the following rights of safe medication administration?
A)
Right indication
B)
Right diagnosis
C)
Right reason
D)
Right history
Ans:
C
Feedback:
“Right reason” is one of the universally recognized rights of safe drug administration. The other listed “rights” are not used in practice.
20.
A nurse is preparing to administer an intramuscular injection of an older adult’s seasonal influenza vaccination. What size needle should the nurse use to administer the injection?
A)
16 gauge
B)
20 gauge
C)
24 gauge
D)
28 gauge
Ans:
B
Feedback:
Usually, a 25-gauge, 5/8-inch needle is used for Sub-Q injections and a 22- or 20-gauge, 1 1/2-inch needle is used for IM injections.
Chapter 5- Pharmacology and the Care of the Adult
1.
An 80-year-old woman has sought care for a dermatological health problem that most often requires treatment with an oral corticosteroid. When considering whether to prescribe steroids to this patient, the care provider should prioritize which of the following questions?
A)
“Should this patient receive a medication that was likely tested on younger adults?”
B)
“Do the potential benefits of this medication outweigh the potential harm?”
C)
“Are there plausible herbal or complementary alternatives to this medication?”
D)
“Is there a younger adult who can oversee this patient’s medication regimen?”
Ans:
B
Feedback:
The nurse and the prescriber must carefully consider the risk of associated adverse effects of those medications as well as possible benefits these medications might have in changing physiological processes related to disease. This consideration is a priority over the specifics of the drug’s original testing procedure or the presence of herbal alternatives. Not every older adult requires another person to oversee his or her medications.
2.
A nurse is teaching an 81-year-old man about the risk for potential adverse effects before he begins a course of antibiotics for an upper respiratory infection. What characteristic of older adults predisposes them to adverse drug reaction?
A)
Increased excretion time due to increased bowel motility
B)
Impaired distribution due to polypharmacy
C)
A decrease in overall body surface area
D)
A decrease in the number of receptors needed for distribution
Ans:
D
Feedback:
Older adults are prone to adverse drug reactions because of a decrease in the number of receptors needed for drug distribution. BSA does not change appreciably with age and bowel motility slows with age. Polypharmacy is a valid concern, but this phenomenon does not primarily involve distribution.
3.
A nurse is conducting a medication reconciliation of a woman who is newly admitted to a long-term care facility. When appraising the woman’s medication regimen in light of the Beers Criteria, the nurse will look for
A)
drugs that are known to cause adverse effects in older adults.
B)
drugs for which generic equivalents are available at lower cost.
C)
drugs that have been found to be ineffective in older adults.
D)
drugs that are known to exacerbate the aging process.
Ans:
A
Feedback:
Dr. Mark Beers developed the Beers Criteria list of potentially inappropriate medications used by the older adult population. The list confirms that toxic medication effects and drug-related problems affect the safety of older adults and names drugs that cause problems in this population.
4.
A nurse has noted that an older adult patient on an acute care for elders (ACE) unit has an exceptionally lengthy medication administration record. The nurse has alerted the pharmacist because one of the patient’s long-standing medications appears on the Beers list. What medication is the nurse likely addressing?
A)
Low-dose enteric-coated ASA
B)
Metoprolol (Lopressor)
C)
Digoxin (Lanoxin)
D)
Vitamin D
Ans:
C
Feedback:
Digoxin appears on the list of Beers Criteria due to the risk of adverse effects in older adults. ASA, metoprolol, and vitamin D do not appear on this list.
5.
A nurse has called an elderly patient’s surgeon to question the order for meperidine hydrochloride (Demerol) for pain control. The nurse’s action is prompted by the possibility of what adverse effect associated with the use of Demerol in older adults?
A)
Confusion
B)
Blood dyscrasias
C)
Gastrointestinal bleeding
D)
Hepatotoxicity
Ans:
A
Feedback:
Demerol is associated with confusion in older adults. It is not noted to cause blood dyscrasias, GI bleeding, or hepatotoxicity.
6.
A gerontological nurse is aware that older adults’ abilities to excrete medications diminish with age. When appraising an older adult’s ability to excrete medications, what laboratory or diagnostic finding should the nurse prioritize?
A)
Renal ultrasound
B)
Complete blood count (CBC)
C)
Serum bilirubin and albumin levels
D)
Blood urea nitrogen and creatinine levels
Ans:
D
Feedback:
The nurse should assess an older adult’s blood urea nitrogen and creatinine clearance (CrCl) levels to determine the patient’s ability to excrete the medications. Renal ultrasound identifies structural abnormalities in the kidneys but is less useful in diagnosing function. The patient’s CBC and bilirubin and albumin levels do not help the nurse assess the patient’s ability to excrete medications.
7.
A 90-year-old patient’s most recent blood work includes the following data: alanine aminotransferase (ALT) 1.99 mkat/L (high) and aspartate aminotransferase (AST) 3.1 mkat/L (high). What implication do these data have for the patient’s pharmacokinetics?
A)
Distribution of drugs may be erratic.
B)
Absorption of drugs may be incomplete.
C)
Excretion of drugs may be delayed.
D)
Metabolism of drugs may be impaired.
Ans:
D
Feedback:
AST and ALT levels are used to determine the patient’s liver function and ability to metabolize drugs.
8.
A 72-year-old woman with a 60-pack-year history of cigarette smoking has developed chronic obstructive pulmonary disease (COPD) and has consequently been prescribed albuterol, a beta2-adrenergic agonist. When administering this medication, the nurse should be aware that
A)
the drug carries a higher potential for hepatotoxicity in this patient than in a younger patient.
B)
the drug may be less effective than in a younger patient due to decreased beta-receptor function.
C)
the patient will need to take a beta-adrenergic blocker concurrently to mitigate the likelihood of adverse effects.
D)
the patient will need to have serial complete blood counts (CBCs) drawn following the initiation of therapy.
Ans:
B
Feedback:
Beta-adrenergic agonists are less effective in older adults as a result of the decreased function of the beta-receptor system. The potential for hepatotoxicity is not increased, and a beta-blocker is not indicated. Serial blood work is not necessary.
9.
The daughter of an 80-year-old woman states that her mother has been taking alendronate (Fosamax) for several years for the treatment of osteoporosis. The daughter tells the nurse that her mother never had any complaints of nausea after taking this medication until recently. How should the nurse respond to the daughter’s statement?
A)
“It could be that your mother’s stomach empties more slowly than it used to, which is a normal result of aging.”
B)
“As your mother gets older, the medication travels down her esophagus more slowly than it used to. This can cause nausea.”
C)
“Because your mother processes drugs more slowly than when she was younger, there is more time during which they can cause nausea.”
D)
“As your mother ages, she has more of the receptors that trigger nausea. This is a normal change that accompanies the aging process.”
Ans:
A
Feedback:
Diminished gastric emptying also plays a role by causing the medication to be in the stomach for a longer period. This factor increases the risk of developing nausea and vomiting, thus causing elimination of the medication in emesis and promoting fluid volume deficit. This phenomenon is not attributable to receptor changes or decreased esophageal motility.
10.
An older adult’s most recent blood work reveals that his serum albumin level is 21 g/L (low). This will most influence what aspect of pharmacokinetics?
A)
Absorption
B)
Distribution
C)
Metabolism
D)
Excretion
Ans:
B
Feedback:
Many medications require serum albumin to bind, transport, and distribute the medication to the target organ. In the event that the amount of serum albumin is insufficient, the amount of free drug rises and the effect of the drug is more intense.
11.
Laboratory testing of an 80-year-old patient who is well-known to the clinic nurse indicates that his liver function has been gradually decreasing over the last several years. How will this age-related physiological change influence drug metabolism?
A)
The patient will metabolize drugs more quickly but derive less of a therapeutic benefit from them.
B)
The liver will sequester drug molecules in the hepatocytes, and they will be released at unpredictable times.
C)
Many of the patient’s medications will remain in his body for a longer time.
D)
The patient’s kidneys will be forced to metabolize a disproportionate quantity of medications.
Ans:
C
Feedback:
The hepatic enzymes of the liver are decreased in the older adult, altering the ability to remove metabolic by-products. It is important to understand that because older adults have a reduced metabolism, medications with a long half-life will remain in the body for a greater amount of time. The kidneys do not compensate for this loss of function. Drugs are not normally sequestered in the liver tissue.
12.
A gerontological nurse is aware that age is a salient variable that must be considered during pharmacotherapy in adults. However, the nurse knows that many other important variables must also be considered, including ethnicity. Members of which of the following ethnic groups typically require lower doses of many common medications?
A)
Native Americans
B)
Caucasian Americans
C)
Asian Americans
D)
African Americans
Ans:
C
Feedback:
Caucasian Americans and African Americans are poor metabolizers of medication compared with Asian Americans; Asian Americans have the ability to metabolize and excrete medications more quickly than those of Caucasian and African descent. This often means that Asian Americans require lower doses.
13.
A nurse is reviewing a new patient’s admission blood work, which indicates that the patient’s glomerular filtration rate is 51 mL/min/1.73 m2 (low). What implication does this have for the patient’s subsequent pharmacotherapy?
A)
The patient may need lower-than-normal doses of some medications.
B)
The patient may require a fluid challenge prior to medication administration.
C)
The patient may need IV administration of a hypotonic solution to aid medication excretion.
D)
The patient may need to receive medications by topical and subcutaneous routes rather than parenteral.
Ans:
A
Feedback:
With a decreased GFR, it is necessary to reduce the dosage of the medication. IV fluid administration and alternative routes do not adequately compensate for this change in pharmacokinetics.
14.
A 69-year-old man has been prescribed a nitrate and a calcium channel blocker for the treatment of unstable angina. When performing health education to promote adherence to his medication regimen, the nurse should emphasize which of the following?
A)
The fact that the patient will likely need medications until he no longer experiences the signs of angina
B)
The fact that the patient should take his medications as ordered even if he feels well in the short term
C)
The fact that inconsistent medication use will likely cause the onset of hypertension
D)
The fact that he should gauge his day’s dose based on how he feels that morning
Ans:
B
Feedback:
Being asymptomatic may contribute to nonadherence to a medication regimen. Many patients begin to feel better with the initiation of therapy and then discontinue medications altogether or miss individual doses. Patients and their families should be educated about adherence to medication regimens and taught to not skip doses, even if they feel well. Inconsistent use of nitrates and calcium channel blockers does not normally lead to hypertension.
15.
Mrs. James has been taking a diuretic and a beta-blocker for the treatment of hypertension for the past several months. During her latest clinic visit, she states that she has been measuring her blood pressure regularly at her local drug store and she claims that it is usually in the range of 130/80 mm Hg. As a result, she states that she has cut down on her doses of both drugs. Mrs. James’ actions should indicate what nursing diagnosis to the nurse?
A)
Risk for poisoning related to unilateral changes to medication regimen
B)
Acute confusion related to the necessity for medication adherence
C)
Readiness for enhanced decision making related to management of drug therapy
D)
Deficient knowledge related to self-management of drug regimen
Ans:
D
Feedback:
Mrs. James is evidently unaware of the need to take her medications consistently. She is presuming that symptom control means that the medication is no longer indicated. The nurse should address this lack of knowledge. There is no associated risk of poisoning, and the patient’s decision making is deficient, a fact that she may or may not be willing to address. Acute confusion denotes a deficit in cognitive processes, not a lack of information.
16.
A nurse at a long-term care facility is surprised to learn that a new resident’s medication administration record runs four pages in length. The nurse knows that polypharmacy carries which of the following risks for older adults? Select all that apply.
A)
Increased risk of complications
B)
Decreased continuity of care
C)
Decreased cognition
D)
Decreased medication adherence
E)
Decreased costs of care
Ans:
A, C
Feedback:
Polypharmacy and the consequent interactions of medications can lead to greater complications and diminished mental status. It does not necessarily reduce the continuity of care or medication adherence. Costs to the patient are likely to be higher, not lower.
1 note
·
View note
Note
I just read this scientific paper that said that when a couple of researchers stimulated a woman’s claustrum (a part of the brain) she went into this stupor, and it was reported that they had found “the on/off switch for consciousness.” she had epilepsy/a half missing hippocampus, so she probably wasn’t the typical subject, but it still shook me. How do I reconcile learning about science with religion? Obvs they’re not at odds per se, but sometimes it’s tricky fitting them together. Thanks btw:)
Hey Anon! Thanks for the ask!
This has been a pretty common theme lately that I’ve been seeing, lots of people want to talk about reconciling faith with science, and I try to make my responses better every time, so let’s see if the Holy Spirit can help me articulate myself and Him.
This specific study sounds interesting. I haven’t read it, but it does sound interesting and shocking. However, I think we really need to be careful how we interpret the language of scientific articles and the media that reports them to us. According to what you described, the thing that happened was that they put her into and out of a stupor. We go to sleep and wake up all the time, effectively going into and out of stupors, without metaphysical difficulties. We can take drugs that put us to sleep or put us into trances, etc. too. All of these things can be said to activate/deactivate one’s consciousness. Psychologists also have specific operational definitions for terms like “consciousness” in their papers. Most of the time, “consciousness” in a scientific sense is just wakefulness or awareness, and has nothing to do with the soul. I haven’t read the paper or anything, but it seems like the specific phrase “the on/off switch for consciousness” was used more for effect than an attempt to make any claim.
I love both religion and science, but here is what we will say about them: they are meant to tell you different things. Christianity seeks the Truth, science seeks to explain how the physical world (mainly) works. These two are not the same. Although natural laws are contained within the Truth, which is why the pursuit of science is a completely valid vocation and an excellent way to glorify God (when done ethically, of course), there are things outside of the realm of science that are important to religion. What is Good and what is Evil? Science can perhaps help to inform our decisions in fields like these, but science by definition is incapable of making a moral judgement. It can only tell us what is, and not what should be done or what is good. It can measure efficiency and it can predict many things, but it cannot assess any sort of morality. That’s not my opinion, that’s just what it is. Science is a measure of how things work, and that’s all it does. It’s an excellent tool, but it isn’t a replacement for religion.
On a note more related to this article you read, science can also say nothing about the soul, which is often associated with consciousness. The soul, as we philosophically understand it, is nonextended (meaning it doesn’t have physical properties and can’t physically interact with anything, and thus follows no physical laws and cannot be observed empirically). Psychologists and sociologists can use science to observe our reactions to the idea of a soul, but there will never be a valid empirical article that measures the actual soul in any capacity, unless we somehow find a way to measure nonextended entities. Although my guess is that if we do find a way to observe these things, it will require a system entirely different from science. Also, other nonextended things include angels, demons, God, Heaven, Hell, etc.
I hope this helps, and as always if you want more clarity, my ask and messages are always open!
7 notes
·
View notes
Text
Like, I'm genderfluid but I never really tell ppl that and just say I'm nonbinary or genderqueer because ppl think I'm talking about just "switching between a boy and a girl" and while that may be want it means for ome ppl it's not at all that for me. Or ppl just think it means "you like to dress with many different presentations but you are technically your assigned gender" When for me it's just a lot of wooooooooo. Newsflash, both gender and sex are sociatally constructed. There is nothing inherently male about xy chromosomes and there is nothing female about xx chromosomes. Look at the enormous differences between every persons chromosomes and also, there are so many more chromosomal makeups than that(look at mice) I'm not "technically" anything but what I Identify as, and if one more of my extended or nonextended family members tell me this I am going to scream. Also the next mother fuxker that tells me they identify as a helicopter after I tell them my gender is going to get socked in the face
28 notes
·
View notes
Note
Hey so l was wondering how to reconcile the existence of souls with stuff like neuroscience which says that there’s no soul? Bc as much as I believe in the afterlife I’m having a hard time pinpointing how it works...unless the point is that it’s a matter of faith and isn’t covered by science, which means that I have to have more faith. (Unfortunately I first tried to answer this by going through militant Richard Dawkins-esque atheist forums online, so now I’m healing from that toxicity.) thanks
Hey friend! Thanks for the ask!
That’s a really deep and philosophical question you’ve got there. And I know the feeling of trying to find answers like that from forums like those, it can get pretty draining and damaging.
I’m not really an expert in philosophy, although I have done some work with this kind of thing and it’s definitely something I’ve thought about a lot myself so I’ll see what I can put into this.
So first, let’s clarify that neuroscience, psychology, biology, and the sciences in general do not (and cannot) say that there is no soul. There may be some scientists who do not believe in the existence of the soul and use their platforms as scientists to attempt to pass off their metaphysical beliefs as truth, but the existence or lack thereof of a soul is not a scientific question and cannot be answered by science. The soul, as defined by most philosophers and theologians, is not a physical substance, not directly observable by any human means. You can observe evidence for the existence of soul-like things (e.g. if you find that you miraculously made it safely through some very dangerous series of events, you may attribute it to the intercession of your guardian angel), but you cannot measure the soul. It does not exist in space or as matter or energy. The term I have seen used to describe it is nonextended, as opposed to extended entities, like matter, energy, forces like gravity and friction, etc. Spiritual substance may perhaps be able to affect material substance (there is a series of letters between Descartes and Elisabeth of Bohemia that addresses this), but does not do so in a predictable or measurable way. Science only claims to be able to describe the extended world, and to describe patterns and processes that are measurable and predictable. It is possible to use science to understand the universe as a system, but it cannot sufficiently explain the soul or other spiritual substance or God or the afterlife. Philosophy, logic, and faith are needed to describe it.
One other way I have thought about science and the existence of a soul being reconcilable is that we don’t have explanations for everything in science. Think about our scientific understanding before we had the concept of infrared light. We couldn’t see it, although we would sometimes experience its effects (similarly to how we experience, for example, prayer or the intercession of angels - we don’t have the tools to understand why something happened, but we understand that something inexplicable happened). It wasn’t until after we discovered whatever tools were necessary to measure infrared light that we could empirically define its existence. But infrared light was so much easier than the soul, because it is tied to something we can experience with our senses (visible light), just at a different wavelength [or something, I don’t know a lot about wave physics]. Spiritual substance, and presumably many other things, have no ties whatsoever to anything that we experience sensorily, so for many of them we wouldn’t even be able to contemplate its existence at all, and for other things like souls which we can fathom, we would not be able to begin to conceive of a way to go about measuring it. Does that mean it doesn’t exist? Absolutely not, it just means that our human faculties are insufficient to fully understand it.
Now, there are a lot of philosophers who have logically “proven” the existence of spiritual substance, or even more specifically, the soul. You can read up on Descartes or Locke or Plato or anyone else you’d like, most people searching through metaphysics are going to have their take on it. Lots of them are unsatisfactory to me, but St. Thomas Aquinas has a really good proof for “the first mover” which has to be spiritual in nature, I’ll try to concisely outline it here:
- the universe is in “movement,” i.e. things are doing other things (including existing)
- necessary for “movement” is something causing something else to move (or exist or to be hot or to do any other thing)
- Go backwards now, forever. For example: This ball is moving because I pushed it because my arm moved it because my brain commanded my arm to do so because I desired to move it because it was in my way because I need to do my homework on this desk because I am in school … because my mother gave birth to me because my parents conceived me because they decided to because they wanted children because they were married … because they were born from their parents … because humans exist from whatever source they came from … because the earth was created through whatever means … because the universe exists…. etc.
- there must be some point where there was nothing in motion, and then something happened that caused it to move and set the universe into the chain of events that has led it to this moment, right now.
- the thing that caused the first motion must have not been governed by the same rules of causality that everything we can observe is subject to, i.e. it can’t require something else to cause it. Thus, that thing must have been made out of spiritual substance.
Maybe you like that proof, maybe you don’t. Maybe you search through other proofs and still don’t find satisfactory ones, none of them are perfect, and most require some sort of benefit of the doubt or suspension of disbelief. So at that point, yes, it is a matter of faith. You do need some trust in God that He exists, and often faith in His nature as well, in order for the rest to follow. And it can be really difficult. We all struggle with doubt. It’s a hard thing to wrestle with. I’ll be praying for you.
I could keep going on, although I fear I might start rambling. I love talking about this kind of thing. There was something about electrophysiology and recording rats’ dreams that I could talk to you about in regard to how that also isn’t irreconcilable with the soul, and if you want to talk more about that we certainly can.
Also if anyone else has any input, feel free to add!
TL;DR: Neuroscience, or any kind of science, has no right or dominion to tell you whether or not souls exist. In fact, the two domains do not have any say over each other; science cannot rule for or against religion, and religion cannot usually rule for or against science. There are a lot of philosophers and theologians who can ration out why souls do exist, some more convincingly than others, but all do require some faith. At the end of the day, whether or not you believe in the soul or the afterlife or God is your decision to make and yours alone, and it is ultimately a matter of faith. Hopefully this was compelling, and you can always talk to me one-on-one or send more asks if you want to explore it further.
God bless!
Jared
#ask#answered#philosophy#soul#the existence of the soul#theology#st thomas aquinas#descartes#locke#christian#richard dawkins#prayer
5 notes
·
View notes
Last Seen Blogs
baseballlibertarian
Baseball Libertarian

sadkazoonoises
sadkazoonoises

thinkbefore
Think beforehand.

madzisstacked
Madz is STACKED

saltycinnabon
Meg