#internalmedicine
Text

Tuesday, 28 November 2023
I went put and studied with my friends today. I also found an amazing way to actually retain info in residency; it’s doing what i did in med school but with a twist (wow shocker). I’m going to be making anki decks. No surprise there.
#medstudyblr#medicine#productivity#being productive#internal medicine#internalmedicine#residency#medstudlife#medstudent#med student#100 days of productivity#productive#coffeeshop#study time#study notes
49 notes
·
View notes
Text
Embark on a journey with Jennifer Carlquist, PA-C, and course director of The Urgent Care EKG Course as she shares 12 essential insights for navigating through EKGs in the urgent care setting.
1. When a patient has an irregular rhythm, it is important to look closely for P waves. If they are the same shape and distance from the QRS complex, you could be dealing with sinus arrythmia. This is usually caused by breathing.
2. If you have a patient with palpitations, you may find a clue to the cause by asking the patient when the palpitations happen. Often, palpitations only occur when the patient is about to go to sleep which could be caused by anxiety, although this is a diagnosis of exclusion.
3. When you have a patient with tachycardia, make sure you can explain why. Pulmonary embolus can cause tachycardia and will not always be associated with an s1q3t3.
4. If you have a very short PR interval, the first thing you should look for is a delta wave. This is what you will see with Wolff-Parkinson-White syndrome, which can be fixed with an ablation.
5. If a patient has experienced a recent stressful event such as the death of a spouse and has new onset heart failure, consider Takotsubo cardiomyopathy. This can present a myriad of EKG findings, including STEMI.
6. PVCs are not always benign. They can lead to heart failure if there are enough of them.
7. There is always a reason for sinus tachycardia, while supraventricular tachycardia (SVT) comes on suddenly for no good reason. It’s hard sometimes to tell the difference between the two, but when you start to sort through the history, that’s where it really starts to make sense. Sinus tachycardia will have volume loss, fever, anemia, or anxiety, while SVT patients will usually have none of those. The exception would be if a patient has anxiety after they started feeling the SVT, which is a whole different story.
8. When interviewing a patient about their palpitations, it is always helpful to ask if they have anxiety as well. If they do, ask them which came first: the palpitations or the anxiety. If the anxiety came first, then it is most likely anxiety causing the palpitations, although this would be a diagnosis of exclusion. If the patient feels palpitations and then anxiety comes on, that’s more likely arrhythmia based.
9. It is impossible to diagnose Takotsubo cardiomyopathy from an EKG alone. There are many different presentations of the condition, including STEMI, nonspecific STT-wave changes, T wave, and inversions that are symmetric. If you have a patient with a classic story that involves recent major stress in their life, then absolutely consider this diagnosis. It can be seen during their angiogram, where it will look like apical ballooning, and they will have a reduced ejection fraction.
10. ST-segment elevation can be very minimal and still deadly. It is important when you are screening for ST elevation to look closely at the TP segment. This is the most isoelectric line, and this is where you should draw your line to see if there’s any elevation or depression. As little as 1 mm can be significant for STEMI in the inferior leaves, so it really does matter here. Get serial ECGs.
11. When looking at the intervals at the top of the EKG, one of the most important numbers to look at is the QTC. The QTC should be <460 ms to be normal in women and <450 ms in men. If it is longer than that, consider adjusting the patient’s QT-prolonging medication. We do not usually see Torsades de Pointes until they get >500 ms, but it’s still a good idea to minimize risk by getting the patient off any QT prolongers you can.
12. Torsades de Pointes is lethal and most likely stems from a prolonged QT. Unlike in VT, the treatment is magnesium, but prevention is always the key. Amiodarone can also prolong the QT and can be proarrhythmic, so you may have to choose a different drug in some cases.
This course is ideal for PAs and NPs practicing in urgent care. Whether you’re new to practice or have many years of experience, you’re sure to learn practical, evidence-based tips you can use on your next shift. You can sharpen your EKG interpretation skills, improve your accuracy, become more proficient, and boost your clinical confidence with The Urgent Care EKG Course.
Visit https://www.ebmedicine.net/ekg to learn more.
Even more content:
Check out one of our latest reels (less than one minute!) by Jennifer Carlquist, the course director.
18 notes
·
View notes
Text

Rheumatoid arthritis is a well-known cause of inflammatory polyarthropathy that affects hands, feet, and other joints.RA also has many potential extra-articular manifestations, as shown in the image.
Reference: FA Figus, et al. Autoimmunity Reviews 2021 (20),
#TeachingRounds#FOAMEd#FOAMRad#internalmedicine#familymedicine#rheumatology#arthritis#rheumatoidarthritis
6 notes
·
View notes
Text

Rheumatoid arthritis is a well-known cause of inflammatory polyarthropathy that affects hands, feet, and other joints.
RA also has many potential extra-articular manifestations, as shown in the image.
Reference: FA Figus, et al. Autoimmunity Reviews 2021 (20),
#TeachingRounds#FOAMEd#FOAMRad#internalmedicine#familymedicine#rheumatology#arthritis#rheumatoidarthritis
3 notes
·
View notes
Video
youtube
Chronic pancreatitis 1
2 notes
·
View notes
Photo

#ScrubLife #RVT #VetTechLife #VeterinaryNurse #MsEnvy #BullyGirl #VetTechProblems #RegisteredVeterinaryNurse #WearFigs #InternalMedicine https://www.instagram.com/p/CjA0t67L_1l/?igshid=NGJjMDIxMWI=
#scrublife#rvt#vettechlife#veterinarynurse#msenvy#bullygirl#vettechproblems#registeredveterinarynurse#wearfigs#internalmedicine
2 notes
·
View notes
Text
A Little Less Alone
“Ma, pagaling kayo. Kaya nyo ‘yang sakit nyo. Mahal na mahal ka namin.”
These are the words from the daughter of an intubated patient who requested to talk to her mother admitted at the red zone. With tears falling down my patient’s face, she nodded—as if re-assuring her daughter that she is fine and that soon, they will see again see each other and feel each other’s warm embrace.
The red zone is such a lonely place. Patients are alone and cannot be taken care of my their relatives. The hospital is also short-staffed and cannot attend to all the concerns of the patients. For patients, I know it is difficult for them to recuperate from their illness without their loved ones.
It is unfortunate that COVID prevented our patients from being with their relatives while they are admitted. COVID robbed our patients from having a loved on to listen about their discomfort and a hand to hold them on difficult times of their hospitalization. COVID prevented our patient from feeling the warmth of the hugs of their loved ones when they need it the most.
Honestly, I cannot imagine being sick and alone. So I told myself, that if a patient asks for my help to someone talk to their relatives, I make a way to make it happen. Whenever I do my daily rounds at the red zone, patients would clamor at me and would ask me to reach for their relatives. “Dok, pakisabi sa anak ko ok lang ako at saka padala ng jacket”, a patient would tell me. So I’d call the Social Service and relay their messages. Sometimes, patients would ask for a pen and paper to write their message for their relatives outside the red zone. This is the least I could do for my patients who cannot see their relatives and at the mercy of the hospital staff if they message would be relayed.
Social support is indeed an important part of the recovery of our patients. I realized that helping patients connected with their loved ones helped them emotionally. Seeing them smile after a seeing their relatives via a video call, after a long time of seeing hopelessness in their faces is priceless. Others, who already refused treatment and hospitalization, would agree to medical management after talking to their relatives.
Communication both with the patient and to their relatives is also important. Patient’s relatives mostly relay on our updates on their patients. I have learned that through communicating well to my patients’ relatives about their condition and current treatment plan will enable me to establish rapport with them.
The red zone has been my battle ground but it has thought me some of the most important lessons as a physician. One of them is that the presence of family—whether in flesh or virtually—is intricately entwined with a patient’s recovery. Hence, I commit myself to ensure that my patients would be able to connect to their family and loved ones and make them feel a little less alone.
3 notes
·
View notes
Text
I am a big fan of ABGs, there’re countless videos explaining the different ways to interpret an ABG paper but this is my cheatsheet (Unfortunately, I don’t remember the source of this picture but i am keeping whoever made it in my prayers)

1 note
·
View note
Text

"Discover, Learn, Succeed: Be Part of Our Workshop!"
Visit the community with Probulin Probiotics! We appreciate the opportunity to extend a chance to you to join us for our expected workshop and learn the amazing advantages of our probiotic products!
Workshop Title: The Evolution in Probiotic Therapy
For workshop details, visit here: https://gastroenterology.universeconferences.com/the-evolution-in-probiotic-therapy/
#ProbulinProbiotics#GutHealth#Workshop#DigestiveHealth#InternalMedicine#GIdoctors#IBD#ProbioticsWorkshop#gastroWorkshop#hepathologyWorkshop#IBDWorkshop#GIWorkshop#GutWorkshop
0 notes
Text

Come experience an amazing workshop with us.
Attend the workshop led by Dr. Jason Mitchell of Probulin Probiotics. We are happy to extend an invitation to you to attend the free workshop at Grand Hyatt Dubai Riyadh Street, United Arab Emirates, on May 21, 2024.
Workshop Title: The Evolution in Probiotic Therapy
For workshop details, visit here: https://gastroenterology.universeconferences.com/the-evolution-in-probiotic-therapy/
#nurselife#InternalMedicine#ProbioticTherapy#ProbulinProbiotics#ProbioticsHealthProfessionals#Workshop#GutHealthSpecialists#GP#Medicine#Gastroenterologists#DigestiveDiseases#MedicalProfessionals
0 notes
Text

Monday, 4th of December 2023
I went to a coffee shop to study. It was hella productive. Did 30 MKSAP nephrology questions AND made anki cards. Love that.
#medstudyblr#medicine#medstudlife#medstudent#med student#productivity#being productive#productive#study notes#study time#internalmedicine#internal medicine#nephrology#coffeeshop
15 notes
·
View notes
Text

9 notes
·
View notes
Text
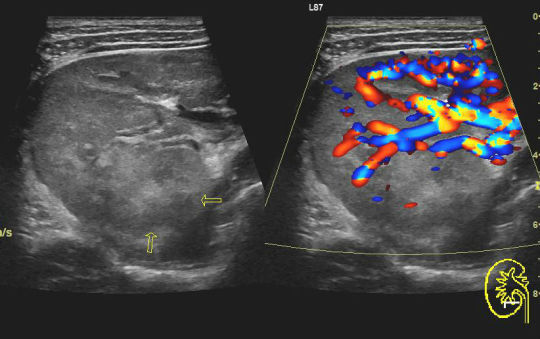

Today's case is a renal ultrasound from a 35-year-old man with a known UTI. The right kidney is hypervascular with heterogeneous echotexture. There is urothelial thickening. Findings are compatible with pyelonephritis.
Imaging is not required to diagnose acute pyelonephritis, but when imaging is needed, ultrasound can be utilized to minimize the patient's radiation exposure.
Case courtesy of Maulik S Patel, Radiopaedia.org, rID: 49259
3 notes
·
View notes
Text
We are delighted to extend an invitation to you to participate in a complimentary, thought-provoking session at the Grand Hyatt Dubai Riyadh Street, UAE on May 21, 2024.
Workshop Title: The Evolution in Probiotic Therapy
For workshop details, visit here: https://gastroenterology.universeconferences.com/the-evolution-in-probiotic-therapy/
#ProbulinProbiotics#Evolution#ProbioticTherapy#Workshop#GutHealthSpecialists#GP#InternalMedicine#Gastroenterologists#DigestiveDiseasesMedicalProfessionals#GIdoctors#IBD#hepathology#Gastroenterology
0 notes
Photo
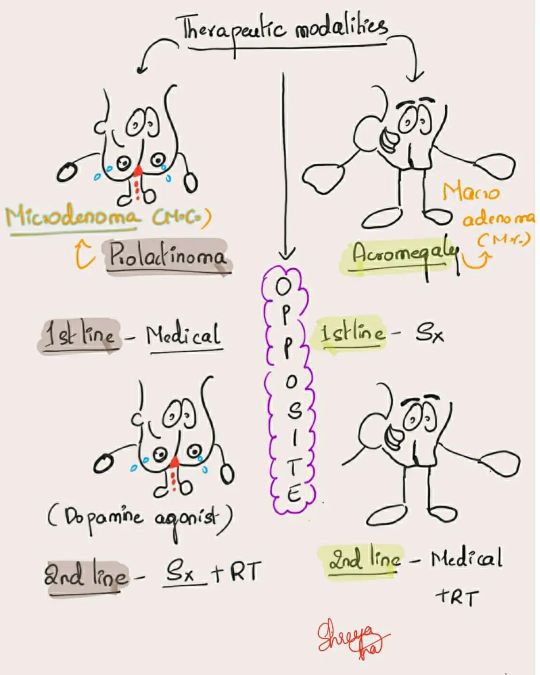
Therapuetic modalities of prolactinoma and acromegaly difference #medicine #medicalmnemonics #usmle #mbbs #medical #medicalstudent #medicalstudent #medicowesome #neet #pgcet #mrcp #internalmedicine #ABIM #internalmedicineresidency #internalmedicineresident #endocrinology #medicalinspiration #studygram #studymotivation #studywithme #studynotes #medblr https://www.instagram.com/p/CeRtQVluUUI/?igshid=NGJjMDIxMWI=
#medicine#medicalmnemonics#usmle#mbbs#medical#medicalstudent#medicowesome#neet#pgcet#mrcp#internalmedicine#abim#internalmedicineresidency#internalmedicineresident#endocrinology#medicalinspiration#studygram#studymotivation#studywithme#studynotes#medblr
7 notes
·
View notes
Video
youtube
Esophagitis part 4 (Eosinophilic esophagitis)
3 notes
·
View notes
Last Seen Blogs
evrendebirmerkur
*siz

gustavosaulle
gustavo saulle

waninerd-blog-blog
Yup ._.

killraf-blog
Senza titolo

ramawira-blog
Untitled