#clinical trial management training
Text
Introduction to Clinical Trial Training
The field of clinical research has seen a significant rise in demand over recent years, with the evolving landscape of the pharmaceutical and biotechnology industries playing a significant role. A clinical research associate (CRA) is a crucial part of the clinical trial process, as they are responsible for overseeing the well-being of subjects and ensuring that the study complies with regulatory requirements. With the clinical research market set to experience growth, it's essential to have a thorough understanding of clinical research training, encompassing its components, course options, and benefits.
I. Clinical Research Training: Background and Importance
Before diving into the specifics of clinical research training, it's necessary to understand what clinical research is and its importance in the field of medicine. Clinical research refers to the systematic study of potential new drugs, medical devices, and techniques to establish their safety and efficacy before they can be approved for use by regulatory authorities. In simple terms, clinical research aims to ensure that new treatments and therapies are both safe and effective for human use, protecting the public from potentially harmful side effects or complications.
Clinical research, thus, plays a key role in the process of bringing novel medical treatments to market. It is a multifaceted process that requires a range of skill sets, from data analysis to ethics and compliance. Clinical research associates (CRAs) are responsible for managing clinical trials and ensuring that they adhere to relevant laws and ethical guidelines. As such, clinical research training equips potential CRAs with the necessary skills to excel in their roles and contribute to the safe development of new therapies and medical products.
II. Components of Clinical Research Training
Clinical research training typically comprises several essential components, each designed to provide a comprehensive understanding of the clinical research process. Some of the critical elements of clinical research training include the following:
1. Basic Principles of Clinical Research: An overview of the fundamentals of clinical research, including the phases of clinical trials and the importance of randomization, blinding, and placebo controls.
2. Good Clinical Practice (GCP): A thorough understanding of GCP guidelines set by regulatory authorities like the International Council for Harmonisation (ICH) and the Food and Drug Administration (FDA) to ensure the safety, integrity, and quality of clinical trials.
3. Protocol Development: Training in the design and development of clinical trial protocols, with an emphasis on creating study objectives, inclusion/exclusion criteria, and the types of assessments required.
4. Ethics in Clinical Research: In-depth exploration of ethical considerations in clinical research, including informed consent, institutional review board (IRB) approval, and data protection.
5. Regulatory Compliance: Gaining a comprehensive understanding of the role of various regulatory authorities in the clinical research process, and ensuring compliance with relevant regulations.
6. Data Management and Biostatistics: Knowledge of essential data management techniques, including data collection and validation, data quality control, and the application of biostatistics in clinical research.
7. Clinical Trial Management: Training on the roles and responsibilities of the clinical trial team and best practices in trial management, including site selection, patient recruitment, and study closeout.
8. Safety Reporting and Pharmacovigilance: An understanding of safety reporting requirements and the importance of pharmacovigilance in maintaining patient safety throughout the clinical trial.
III. Clinical Research Training: Course Options and Certifications
Numerous clinical research training programs are available for those wishing to enter or advance within the clinical research field. These programs typically cater to diverse educational backgrounds and levels of expertise, ensuring that all prospective CRAs have access to the necessary training. Courses generally range from short-duration workshops to comprehensive diploma or degree programs.
One popular and widely recognized accreditation is the Clinical Research Associate (CRA) Certification. Obtaining this certification demonstrates a commitment to excellence and professionalism in clinical research. Several organizations offer clinical research associate certification online, making it an easily accessible option for many individuals.
In conclusion, clinical research training is essential for anyone wishing to pursue a career in clinical research. It equips learners with the skills and knowledge necessary to conduct and manage clinical trials, ensuring public safety and helping to bring life-enhancing treatments to market. With various course options available, including the Clinical Research Associate Certification Online, gaining the required qualifications is more accessible than ever before.
#clinical trials training#clinical trial training#clinical trial manager training#citi clinical trial training#clinical trial administrator training#clinical trial agreement training#clinical trial assistant training#clinical trial associate training#clinical trial audit training#clinical trial budget training#clinical trial coordinator training#clinical trial investigator training#clinical trial management system training#clinical trial management training#clinical trial management training courses#clinical trial project management training#clinical trial protocol training#clinical trial site training#clinical trial training program#clinical trials monitoring training#clinical trials sas programming training#clinical trials training courses#edc training clinical trials#iata training clinical trials#medical device clinical trial training#medical device clinical trials training#nida clinical trials network free gcp training#nida clinical trials network gcp training#nih clinical trials training#oncology clinical trials training
0 notes
Text
Kaladin Didn’t Invent Therapy (And Why That’s Actually Great)
“...You need someone to talk to, Noril, when the darkness is strong. Someone to remind you the world hasn’t always been this way; that it won’t always be this way.”
“How do you … know this?” Noril asked.
“I’ve felt it,” Kaladin said. “Feel it most days.”
- Rhythm of War, Ch. 25 Devotary of Mercy
I’m writing as someone with a background in psychotherapy and peer support, and I'm bursting with excitement about one of my favourite topics. You can imagine why I love Kaladin’s arc in Rhythm of War so much! I actually yelled out loud when I read some of these parts the first time.
I’ve seen people online saying and making jokes that Kaladin invents therapy, and while that could eventually be true, what Kaladin actually invented in RoW is mental health peer support. Psychotherapy as most people would understand it simply doesn’t exist yet on Roshar. However, peer support is a legitimate modality for healing on its own merits. Even more importantly for the story, peer support is something Kaladin would personally really benefit from, and it fits his narrative arc way better than therapy would.
1. Therapy as we know it won’t exist for a while yet.
“We need to study their responses, use an empirical approach to treatment instead of just assuming someone who has suffered mental trauma is permanently broken.”
- Rhythm of War, Ch. 25 Devotary of Mercy
“Someone needs to talk to them, try different treatments, see what they think works. What actually helps.”
- Rhythm of War, Ch. 25 Devotary of Mercy
Obviously, Kaladin has not been educated in battle shock or melancholia or any other diagnosis. In Alethkar there's hardly any knowledge to be had on the subject. Even now in real life, research into effective interventions for various diagnoses is still ongoing, over 100 years after modern therapy was founded.
Building an empirical knowledge base* will take time, not to mention the years it will take to train new therapists across Roshar in how to provide interventions specific to various issues. Therapy as we know it today generally includes time in mentorship with another therapist, so in a way, the first therapist isn't a therapist. 😅 In the meantime, there are people who need help today, including Kaladin.
Peer support can fill that gap because its knowledge base is different. Peers bring their expertise, which is their years of trial and error, successes and failures - their lived experience. Peer facilitators need to know the basics of managing a group, and they have to be willing to share their own experiences and learn from the group. Thus, training peer leaders is relatively quick, and incredibly scalable and adaptable across cultures and many issues/diagnoses.
2. Peer Support is a distinct path to recovery that doesn’t require an expert in therapy.
Kaladin located six men in the sanitarium with similar symptoms. He released them and got them working to support each other. He developed a plan, and showed them how to share in ways that would help...Today they sat in seats on the balcony outside his clinic. Warmed by mugs of tea, they talked. About their lives. The people they’d lost. The darkness.
- Rhythm of War, Ch. 33 Understanding
“While you can’t force it, having someone to talk to usually helps. You should be letting him meet with others who feel like he does.”
- Rhythm of War, Ch. 25, Devotary of Mercy
Kaladin is already positioning himself to align with the values of peer support. Some of these values overlap with therapy, such as dignity, respect, inclusion, hope, and trust. What makes peer support different is a particular emphasis on equal relationships, self-determination, and personal growth (Peer Support Canada, 2022).
In peer support, the group facilitator is not considered an authority like a therapist would be. A peer leader may be further on the road to recovery, but they may not be. They are expected to listen and grow just like any other group member.
Because the leader of the group is also a learner, peer support groups tend to be more collaborative and open-ended. Everyone in the group has something they can take out of it and something to give. Everyone in the group is responsible for managing their own self care, and everyone in the group is responsible for the direction of their own growth. This is different from most therapy groups, which often have a specific focus or goal that the therapist is responsible for implementing. And speaking of responsibility...
3. Peer Support Fits Kaladin’s Narrative Arc Better than Therapy
At his father’s recommendation—then insistence—Kaladin took it slowly, confining his initial efforts to men who shared similar symptoms. Battle fatigue, nightmares, persistent melancholy, suicidal tendencies.
-Rhythm of War, Ch. 33 Understanding
…he’d learned—these last few months—that his battle shock could take many forms. He was getting to where he could confront it.
-Rhythm of War, Ch. 39 Invasion
I think everyone can agree that Kaladin needs to participate in therapy just as much as the other battle-shocked men he finds in the Devotary of Mercy.
However, in therapy, the focus is solely on the needs of the clients. A therapist should not be distracted by their own issues (when this happens, it’s called countertransference). Further, therapy is generally framed such that the therapist is the only expert in the room, which means therapists have a higher level of responsibility for how the clients are doing (which varies depending on the issue, the therapy modality, and the circumstances).
In his own recovery, Kaladin is working on trying to take less responsibility for others, so setting him up as a therapeutic authority could be harmful for him. In a position of authority, he might be tempted to replicate the hierarchical structure he was in before (which would impede his own growth), or try to save everyone (which could impede everyone's growth). He simply doesn’t have the mentorship or knowledge base he'd need to work through those issues before leading as an expert.
In contrast, the point of peer support is the mutual sharing of lived experience. The group facilitator is expected to share their own struggles (as a model of recovery), and allow others to support them. In the context of a more balanced power dynamic, Kaladin can give the other group members the space they need to grow, and he can pursue his own recovery without feeling like he’s letting others down. Also, he will be able to leave the group during KOWT without worrying that the group won't be able to run without him. Everyone in the group carries some responsibility for each other, so group members can come and go with less stress than a change in therapist would cause in group therapy.
This is the beauty of peer support. It can happen anywhere people with similar experiences get together. No formal education is required. What is required is a willingness to know yourself as well as you can; to share your experiences; to listen to others tell their stories; to question your own assumptions as you learn how others handle things differently; to look out for each other's safety; to care.
Peer support creates a place of belonging and a community repository of shared wisdom. Kaladin almost had it on Bridge Four, but his position of authority wouldn’t allow him to grow the way he needed. Peer support is what Kaladin needs - he needs a place where he can take off his armour among people who get it because they're struggling with similar issues, and without having a position of responsibility over them. When he (eventually**) attends the groups, they help him grow!
Anyway, that's why Kaladin didn’t invent therapy, and why I think that's great.
For the men chatting together softly, the change was in being shown sunlight again. In being reminded that the darkness did pass. But perhaps most important, the change was in not merely knowing that you weren’t alone—but in feeling it. Realizing that no matter how isolated you thought you were, no matter how often your brain told you terrible things, there were others who understood.
- Rhythm of War, Ch. 33 Understanding
---
*Funny enough, empirical research could lead Rosharan researchers right back to peer support. Empirical research on Earth has shown that modern therapy and peer support have similar levels of effectiveness (for example, for depression and PTSD).
**Look who’s resisting attending the groups he founded…KALADIN!! (shakes fist in the general direction of the sky) (This is the most relatable passage for me in this whole book, by the way, helper types unite lmao):
Kaladin looked down at the table. Had it? Had talking to Noril helped?
“He’s been avoiding joining in,” Teft said.
“I haven’t,” Kaladin snapped. “I’ve been busy.”
Teft gave him a flat stare. Storming sergeants. They always heard the things you weren’t saying.
- Rhythm of War, Ch. 38 Rhythm of the Terrors
Peer Support Canada. (2022). Peer Support Core Values. Accessed from https://peersupportcanada.ca/ Jun 27, 2022.
#I shared this on reddit a while ago but it got archived so here#enjoy#this is not an april fools thing this is just bad timing on my part#kaladin stormblessed#rhythm of war#row spoilers#kaladin didn't invent therapy#peer support#stormlight archive#the stormlight archive#stormlight essay#stormlight meta#god i love kaladin so much
147 notes
·
View notes
Text
German Political Prisoner: Ludwig Worl
The First Righteous

Ludwig Worl was a German human rights activist who spent 11 years in Nazi concentration camps and went to extraordinary lengths to help the Jews imprisoned there.
Born in Germany in 1906, Ludwig was trained as a carpenter. As the Nazi party rose to power in the 1930’s, Ludwig was strongly opposed to their fascist ideology and became an early anti-Nazi activist. In 1933, soon after Hitler came to power, the Nazi leader began building concentration camps to incarcerate his political opponents. Ludwig became aware of the horrific conditions in the camps, and decided to do something to raise public awareness of the human-rights abuses there. He self-published informational pamphlets about the persecution of German political prisoners and handed them out on street corners.
The Nazis arrested Ludwig in 1934 and he was imprisoned at Dachau and held in a squalid holding cell for nine months. He was then transferred to the camp’s carpentry shop, and after that to the medical clinic, where he trained to become a paramedic. He spent eight years in Dachau and then in 1942 he was transferred to Auschwitz because of a typhoid epidemic there. Tens of thousands of prisoners and staff were dying of typhus, and Ludwig was part of a team of seventeen male prisoner/medics who went to manage the outbreak.
Highly intelligent and effective at his job, Ludwig became the manager of the Auschwitz hospital barracks, mostly filled with Jews. Against direct orders, he covertly employed Jewish doctors in the clinic, saving them from the gas chambers. Ludwig cared for his Jewish patients with great dedication, and took significant personal risks to get medical supplies for them. He also falsified patient data lists to save Jews from being marked for death. His brave actions led to him being taken from the clinic and put in solitary confinement. After a few months, he was released because the Nazis required competent medical personnel at Guntergrube, a forced-labor camp nearby.
At Guntergrube, Ludwig was put in charge of his fellow prisoners. In this position, he continued to break camp rules and help Jewish prisoners. He found warm clothing to help them survive the brutal Polish winter, and food rations to keep them from starving. He also exempted sick prisoners from hard labor. As the Russian Red Army approached to liberate the camps, the Nazis forced Jews onto death marches, and Ludwig helped several Jews escape.
After the war, Ludwig started the Auschwitz Prisoners Organization to help survivors rebuild their lives. At a time when many Germans wanted to forget what had happened, Ludwig remained an outspoken opponent of Nazism. He obsessively searched for former concentration camp guards, determined that they be punished for their crimes against humanity. In 1963 he testified at the Auschwitz war crime trial in Frankfurt. He spent the final years of his life speaking publicly about Auschwitz, to make sure that the horrors he witnessed there were never forgotten.
On March 19, 1963, Israeli Holocaust Memorial Yad Vashem honored Ludwig Worl as Righteous Among the Nations. He was the first person to be so honored. Eleven years in Nazi concentration camps ruined Ludwig’s health, and he died in Germany in 1967 at 61 years old.
For protecting Jews and bringing Nazis to justice, we honor Ludwig Worl as this week’s Thursday Hero.
29 notes
·
View notes
Text
Where and how did the Inhumane Society keep Lizzie captive?
The organization had four willing members and three unwilling members. The willing ones were Hangfire, Stew Mitchum, Nurse Dander, and Dr. Flammarion (it was never explained why the latter two allied with him). The unwilling ones were Sharon Haines, Sally Murphy, and Ellington Feint (and technically Kellar too, for a while).
But after WDYSHL, there were only two willing members - Hangfire and Stew. Nurse Dander, and Dr. Flammarion got arrested and sent to the city to stand trial (or so we're told. I don't suppose it was confirmed if they actually got there?). That leaves only Hangfire and STew, the latter of whom is a boy who can't be much older than thirteen, to imprison Lizzie.
Sharon and Sally obviously weren't helping to keep Lizzie captive, because the only reason they were helping Hangfire in the first place was because he was blackmailing them with Lizzie's safety.
And Hangfire and Stew were busy with Hangfire's plans throughout the series. They both make multiple appearances in SYBIS; clearly, they were not actively guarding Lizzie or whatever.
In WITNDFAON, Sally somehow rescues Lizzie, disguises her, and sneaks her onto the train. She believes that she'll never be free of Hangfire, that he'll likely kill her like he tried to, but she's determined to at least get Lizzie out safely. (Lizzie's acting skills were a lot better than hers, but I think that can be explained away to extreme nervousness and stress.)
But if Sharon knew where Lizzie was, why didn't she try to rescue her before, instead of being blackmailed by Hangfire?
She may only have found out recently, being somewhat affiliated with the Inhumane Society. Okay then. So she managed to rescue her - Hangfire was unaware that his hostage was gone.
But who was supposed to be holding her hostage? Every member of the Inhumane Society was on the train. Lizzie was not supposed to be on it.
Lizzie wasn't in Wade Academy, obviously, since Sharon and Kellar were there. She couldn't have been in the Colophon Clinic, at least not after it was all but destroyed.
Stain'd-By-The-Sea has any number of abandoned buildings, Lizzie could have been in one of those. But who was watching her to make sure she didn't escape? After all, Nurse Dander was with Ellington disguised as Cleo to make sure she didn't escape.
Did Hangfire just keep her drugged with laudanum and locked in a room somewhere without bothering to guard her? Under the influence of laudanum, she wouldn't be able to escape by herself; and, indeed, she didn't, until Sally found her.
#atwq#all the wrong questions#lemony snicket#lizzie haines#sharon haines#hangfire#armstrong feint#sally murphy#dame sally murphy#inhumane society#the inhumane society#kellar haines#stew mitchum#dr. flammarion#nurse dander
9 notes
·
View notes
Text
Historic Gotham: Part Two

Novick Building: The Novick Building was built in the early 1800s and was part of Alan Wayne's plans to expand Gotham City into a more modern metropolis. It's one of the tallest landmarks in the Old Gotham district. The Novick Building has been used for various purposes during its existence. It was once the home of a newspaper agency, a library, a bank and temporarily housed the Labor Union before they relocated to the West End. It is now used as an office space for various small- time companies and start-ups. I once considered using the empty dome at the top of the building as the location for what later became the Belfry base but decided against it as there are no easy access points and renovations would have been too noticeable.
Notes: The Novick Building provides a good vantage point of the Courthouse and City Hall. Can use it to supervise transport for trials.

Gotham City Post Office: The Gotham City Post Office has been open for more than a century, handling everything from letters to ship cargo. It houses over thirty employees and sends out hundreds of mailmen and women across the city every day. The Riddler once used the post office for an intricate scheme using letters, since they can't be as easily traced as digital information. But the workers at the post office went on strike, which made his whole plan fall apart. I later found the Riddler at Robinson Plaza trying to catch birds to train them to be carrier pigeons. I've since made a contact at the post office who warns me of any suspicious activity taking place there. Along with my other contact at the Dixon Docks, we've managed to find and destroy many packages of contraband.
Notes: All of my non-essential packages are sent to the post office under the pseudonym Jack Shaw.
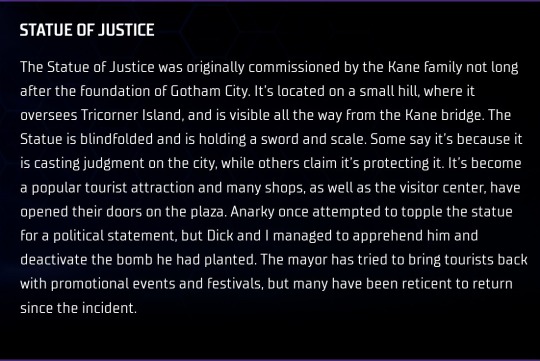
Statue of Justice: The Statue of Justice was originally commissioned by the Kane family not long after the foundation of Gotham City. It's located on a small hill, where it oversees Tricorner Island, and is visible all the way from the Kane bridge. The Statue is blindfolded and is holding a sword and scale. Some say it's because it is casting judgment on the city, while others claim it's protecting it. It's become a popular tourist attraction and many shops, as well as the visitor center, have opened their doors on the plaza. Anarky once attempted to topple the statue for a political statement, but Dick and I managed to apprehend him and deactivate the bomb he had planted. The mayor has tried to bring tourists back with promotional events and festivals, but many have been reticent to return since the incident.
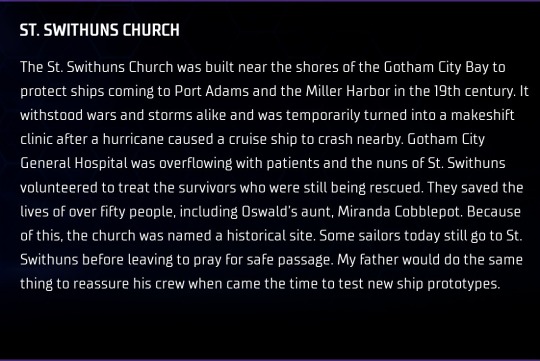
St. Swithuns Church: The St. Swithuns Church was built near the shores of the Gotham City Bay to protect ships coming to Port Adams and the Miller Harbor in the 19th century. It withstood wars and storms alike and was temporarily turned into a makeshift clinic after a hurricane caused a cruise ship to crash nearby. Gotham City General Hospital was overflowing with patients and the nuns of St. Swithuns volunteered to treat the survivors who were still being rescued. They saved the lives of over fifty people, including Oswald's aunt, Miranda Cobblepot. Because of this, the church was named a historical site. Some sailors today still go to St. Swithuns before leaving to pray for safe passage. My father would do the same thing to reassure his crew when came the time to test new ship prototypes.
3 notes
·
View notes
Text
Pleading With The Dead
A Count The Days AU - Ten Years Under A Different Hand. Continues from here. Contains starvation and hunger references, passive suicidal ideation, mouth stitched shut trope and associated nastiness, mentions of a character wetting themselves, death mentions.
---
Of all the classes he took, of all the training he has had, Haskell has spent more than enough time faced with the same facts. A human being survives, on average, three minutes without air, three days without water, and three weeks without food. He is acutely aware that he is on a schedule here.
He isn’t sure how long it has been, at all, and he tries to do the maths and fails miserably. It’s been maybe a week, total, since the trial. He shudders, remembering it.
He starts to pace the empty basement, back and forth, back and forth. Using one corner as a makeshift toilet, using the opposite corner to sit and weep over his situation. What else is there to do, he thinks. What else can he do but weep? He sleeps without dreaming for the first few days- long, blank stretches of fifteen hours at a time, then an unimaginably long stretch staring into the darkness. He tries not to think about that night when he killed Jacob. He fails. He tries not to think about how it felt to be crawling around on the floor licking up the blood of the man he used to call his friend, the blood that he shed. He fails. The stitches in his face seem to be so hot to the touch he thinks he is boiling alive, from the inside out.
When the hunger fades, he knows he’s hit ketosis- and he knows it’s a brief plateau in a steep decline. It is, as far as he can work out, about two weeks since his last meal. A clingfilm-wrapped sandwich, which he didn’t manage to keep down, utterly wracked with anxiety over his imminent trial. He remembers at the time being terrified they’d hang him.
Oh, how he wishes they had, now. The survival part of his brain takes over- scrapes a thick, fresh layer of sawdust over the urine-soaked far corner of the room, and sits him in the opposite, mainly motionless, conserving his energy.
His fever peaks up, and along come the fever dreams. Jacob, always Jacob, always calmly asking the same thing. “Why did you do this?”
Haskell falls apart a little. He doesn’t know why. He doesn’t know. He doesn’t know- he doesn’t want to know. It’s simpler to simply turn the tables than to look at himself. So he reasons Jacob provoked him.
The dead man’s figure rising from his dreams is still calm. ”Why did you do this?”
Haskell is not. “I’m asking you the same fucking thing!” he screams. In his dreams he shouts and he screams and he still remains a prisoner of consciousness. “I’m asking you the same fucking thing, Jacob, why did you do this to me?” he howls.
The dream dissolves without an answer. The hunger returns, ravenous.
Mere comes to give him water. He isn’t gentle. It hurts. Haskell’s hands come up, tense, to try to brush Mere off. They are, like his uncomfortable squirming as the metal straw cuts into inflamed flesh, ignored. “I’ll ask you again before it gets really unpleasant for you,” says Mere, cleaning off the metal straw from where he’s forced it between the infected weeping of the stitches. “Will you come upstairs?”
Haskell barely has to consider. He has the same response- the same defiant gesture, deliberately obscene.
Mere leaves without a word. He doesn't ask the question again when he visits next. Just the same silent, almost clinical look on his face, the same lukewarm water through a metal straw. Haskell nearly starts to cry- though he never really stops, save for when there are simply no more tears left- when Mere re-opens the freshly-scabbed wounds in the process.
---
Over the next couple of days- or at least, between Mere’s visits, which he has no real way of knowing how far apart they are- he realises he is wasting away in the most visceral sense. He goes from sitting down, to slumped over, to lain down in the sawdust, too weak to move.
There comes a time where he can barely even lift his head. He isn’t quite sure how long passes- though he suspects it isn’t nearly as long as it feels- but the featureless room spins and his head pounds and he can’t even sit up, shivering and sweating with a fever that feels like it’ll break him before it breaks.
And with the fever, come the fever dreams. This time, he can’t escape the basement even in his sleep. Once again, there is Jacob Kay, standing over him. Dead. “Why did you do this?” asks Kay. He’s still not angry. Even with a smashed in-skull, bloodied, the arc of his head caved-in.
“You did this,” screams Haskell, face to the dreamed sawdust. His voice breaks. “You did this to me! This is your fucking fault!”
No answer.
Haskell wakes with a painful twitch, and stares into the heavy darkness, before sinking right back into a dreamless sleep, slumped on the sawdust, soaked in his own sweat. As he drifts off, he becomes acutely aware that he has wet himself, too tired to even get up to go. He remembers gasping in horror through a clenched jaw right before sleep takes him.
When he wakes his filthy trousers have only barely dried off. He reaches a hand down to feel the fabric, and when he realises he is still damp, he just lies there still, staring into the darkness, watching the swimming of his own tears play across his vision. His cheeks burn with shame and if he had the strength, he knows he would bawl his eyes out over it. All he can smell is bitter ammonia.
He finds himself wishing for Mere to return. To rescue him. To let him change clothes, at least. Somehow, the damp trousers are a million times worse in his starved brain than the lack of food. He stopped actually feeling the gnawing hunger a little while ago and it hasn’t returned. He doesn’t think that’s a good sign, but at least it feels better.
Asleep, again. The same dream- the same dead man standing over him. “Why did you do this?”
“You did, you did!” screams Haskell, tasting blood. “This is your fault! Make it stop!” Jacob just stares at him, as best as he can with one eye-socket caved inwards and an eye that is crimson-red and barely holding on. “Please!” weeps Haskell. “Please, please, make it stop!” Jacob just stands there, motionless.
Haskell cries at the feet of the dead man until Mere shakes him from fitful sleep. Haskell rolls onto his back as best as he can, and just lies there, staring at the Special, staring into his heavyset face and eyes devoid of pity.
“So you are alive, then,” he muses. “This basement reeks and you’ve been lying on the floor for almost two weeks now, in sawdust soaked with your own urine. Do you have no shame or do you really wish to behave like an animal?” Haskell shakes his head, almost imperceptibly. Fuck, he thinks, feeling his cheeks burn again.
Mere notices. “Isn’t this embarrassing for you, now? Isn’t it?”
Haskell squirms uncomfortably again, but nods all the same. Again the movement is barely visible, but Mere sees it.
Mere stoops down to Haskell’s level. “Within half an hour, I can have a Special Division doctor here to sort you out. I can have you cleaned up, get you clean clothes, and a clean bed. All you have to do, Haskell, and this is all I’m asking of you now, and we can work from there, is you let my housekeeper shave your head, and you don’t fight her. That’s it. Are you really going to let yourself die over that?”
Haskell considers for a moment, eyes full of tears, and then ever-so-slightly, shakes his head.
“No? You want to come upstairs? You agree to no screaming, no shoving, no punching, no whatever?” Mere spits the last word like it tastes bad.
Haskell squirms in the sawdust, trying to sit up. The tears in his eyes spill down his cheeks. He knows that it’s not as simple as Mere is portraying it- that letting him have an inch will become a mile, and that mile will become a lifetime of austere silent servitude under the threat of humiliation and pain, stripped of all honour and status. But he has no choice now. He has no choice.
Because Mere is right.
He’s not going to let himself die when the solution is right fucking there. And surely most things are less humiliating than starving to death in a ruined, urine-stained and crumpled suit.
Mere is right. And that’s what hurts the most.
Haskell sniffs back the tears and nods.
Mere considers for a moment, and with a slight expression of disgust, picks Haskell up as if he weighs nothing at all, slinging him over his shoulder, and climbs the stairs out of the basement without a word.
#whumpblr#not gonna tag some things lest i end up on edblr sorry#writeblr#count the days#haskell haveter#mouth gore#fever whump#kind of i guess#villain whumpee#also kind of i guess#hi if you actually read these tags#whump#whump writing
11 notes
·
View notes
Text
Clinical SAS programming A complete guide
Introduction
Clinical SAS programming is a specialized field that utilizes the SAS programming language to handle the vast and complex data generated in clinical trials. SAS, a statistical software package, is extensively employed by pharmaceutical and biotechnology companies for its robust data management, analysis, and reporting capabilities.
In terms of data management, SAS is used to clean, transform, and manage large datasets, ensuring they are organized and ready for analysis. This is a critical step in clinical trials, where large volumes of data are collected and need to be processed efficiently.

For analysis, SAS can perform a wide range of statistical analyses, including descriptive statistics, inferential statistics, regression analysis, survival analysis, and analysis of variance (ANOVA). These analyses are crucial in interpreting the data collected in clinical trials and drawing meaningful conclusions.
Finally, Clinical SAS programming is also used for reporting. It can generate various reports, including integrated summaries of safety and efficacy (ISS/ISE), clinical study reports (CSRs), and other regulatory documents. These reports are essential for communicating the results of clinical trials to regulatory authorities, medical professionals, and the public.
SAS in Clinical Domain
Data Management: SAS is used to clean, transform, and manage clinical trial data. It can handle large datasets and perform data validation, data integration from different sources.
Statistical Analysis: SAS is used for statistical analyses, such as descriptive statistics, inferential statistics, regression analysis, survival analysis, and analysis of variance (ANOVA). These analyses help researchers and clinicians to draw conclusions from clinical trial data.
Data Validation: Checking the accuracy, consistency, and completeness of clinical trial data by performing data validation checks, identifying discrepancies, and resolving data-related issues.

Safety Reporting: Generating safety reports and listings to monitor adverse events and safety data during the trial.
SDTM (Standard Data Tabulation Model) Conversion: Converting clinical trial data into SDTM format, which is a standardized data model for regulatory submission.
ADaM (Analysis Data Model) Implementation: Creating ADaM datasets, which are analysis-ready datasets used for statistical analysis.
Report Generation: Preparing clinical trial reports, including integrated summaries of safety and efficacy (ISS/ISE), clinical study reports (CSRs), and other regulatory documents.
Data Quality Control: Implementing quality control procedures to ensure the accuracy and reliability of analysis results.
Data Visualization: Creating data visualizations, such as graphs and plots, useful for data exploration and presentation of result.
Automation: Creating SAS macros to streamline and automate repetitive tasks and improve programming efficiency.
Medical Coding: Performing medical coding of adverse events, concomitant medications, and medical history terms using standardized dictionaries like MedDRA (Medical Dictionary for Regulatory Activities) and WHO Drug.
Career in Clinical SAS
A career in Clinical SAS programming is rewarding and offers a wide range of opportunities. The SAS Academy for Clinical Programming offers a comprehensive training program that prepares you to work as a SAS Certified Clinical Trials Programming Professional. The combination of coursework and hands-on learning helps you build a foundation of clinical research theory and data analysis skills.
Conclusion
Clinical SAS programming is indeed a vital skill in the pharmaceutical and biotechnology industries. With a solid foundation in SAS programming and a comprehensive understanding of clinical trials, you can pave the way for a successful career in this field.
Whether you’re a biostatistician, a clinical SAS programmer, or someone interested in the field, learning Clinical SAS programming can open doors to a plethora of opportunities. It’s not just about job prospects; it’s about contributing to the advancement of medical research and the development of new treatments and therapies.
In conclusion, mastering Clinical SAS programming is not only professionally rewarding but also offers the chance to make a significant impact in the healthcare industry.
what are the best ways to learn Clinical SAS?
We run a training institute in Hyderabad named Brolly Academy. We do offer best Clinical SAS training in Hyderabad with job assistance. Now when you list the best ways to learn Clinical SAS include Brolly academy's Clinical SAS Training as one of the way.

2 notes
·
View notes
Text

Joseph N. Welch, Lee Remick, and George C. Scott in Anatomy of a Murder (Otto Preminger, 1959)
Cast: James Stewart, Lee Remick, Ben Gazzara, Arthur O'Connell, Eve Arden, Kathryn Grant. George C. Scott, Joseph N. Welch. Screenplay: Wendell Mayes, based on a novel by John D. Voelker (as Robert Traver). Cinematography: Sam Leavitt. Production design: Boris Leven. Film editing: Louis R. Loeffler. Music: Duke Ellington
An exceptional film, far more deserving of the year's best picture Oscar than the bombastic Ben-Hur (William Wyler), Anatomy has a lot of great things going for it: the wonderful courtroom conflict between old Hollywood pro James Stewart and Method-trained newcomer George C. Scott; the tension and volatility of Ben Gazzara as the defendant; the presence of such scene-stealers as Arthur O'Connell and Eve Arden in the supporting cast, along with other character actor stalwarts like Murray Hamilton, John Qualen, Orson Bean, Howard McNear, and Jimmy Conlin. And even the "stunt casting" of non-actor Joseph N. Welch, famous for the integrity he showed in his confrontation with Senator Joseph McCarthy during the Army-McCarthy hearings five years earlier, pays off handsomely, with Welch bringing both gravitas and humor to his role as the trial judge. The soundtrack by Duke Ellington also adds a touch of greatness to the movie, which David Thomson calls "magnificent." Where I think it falls short of magnificence is in the treatment of the rape victim played by Lee Remick. There is, of course, some ambiguity remaining in the film as to whether she was in fact raped, but the part as written by Wendell Mayes and the performance as directed by Preminger treats the presumed victim as an air-headed sex kitten. It's possible that Hollywood, so long precluded by the Production Code from even treating the subject of sexual assault, hadn't yet developed a grammar and vocabulary for dealing with the subject. Remick was a fine actress, and she does manage to show moments of vulnerability in her performance, but the general impression of the character given by the film verges on the despicable "she was asking for it." Preminger had been flouting the Code since The Moon Is Blue (1954) and The Man With the Golden Arm (1955), challenging the strictures on language (the words "virgin" and "seduce") in the former and drug use in the latter. Anatomy continued Preminger's assault on prudishness, though few who watch it today will be shocked by its rather clinical discussion of whether Laura Mannion was indeed raped, or be inclined to sniff daintily, as Time magazine did in its review, that the film "seems less concerned with murder than with anatomy."
6 notes
·
View notes
Text
[fic] but I am too weak to be your cure
pairing: jen x judy
Nights like these are the hardest.
It had been the chemo that you dreaded at first. They’re the most vivid memories you have of your mom, after all — sitting in a hospital room and watching the poison get pumped into her body. You’d blocked out the worst of it. The days following treatment were always brutal. A total fucking nightmare. The nausea, the vomiting, the pain.
Maybe you subconsciously thought that Judy was stronger, somehow. Healthier. That it wouldn’t affect her the way it did your mom. But it’s the first day after her third round of chemo and she’s so run down while you run around — clandestine meetings with Perez and phone calls to clinical trials and taking care of the boys and making sure Judy has everything she needs and fuck, are you exhausted. You put on a brave face for everyone, reassure them that everything is going to be okay but you’re fucking drowning.
Most nights you barely make it to the room before you’re shaking, throat tight from swallowing around the lump that formed within it fucking hours ago. Tonight is no different. Henry is tucked in and Charlie has retired to the guest house for the evening (and god, you don’t even have the energy to think about what he’s getting himself into over there). Judy has been asleep for the last couple of hours, but you find yourself at her bedside, fingers raking through her hair, and you’re almost grateful for how heavily she sleeps now because you’re positively vibrating.
Your breath is shaky, the image in front of you obstructed through the moisture in your eyes. She’s gripping that baby blanket as tight as she can and you wish for nothing more than the ability to shrink yourself down and go in and chisel out those fucking cancerous invaders yourself. It’s such a helpless feeling, being human, when you want nothing more than to morph into Judy’s blood cells and go to fucking war for her.
Brown eyes blink open and a vibrant smile spreads across chapped lips and your heart immediately seizes in your chest, stealing the breath from your lungs as it hits you all at once how fucking in love with this woman you are. Your hands shake as they pull away and you’re choking on sobs. You can’t help but note how difficult it is for her to sit up, her expression morphing to concern as she pulls you in. It’s a sudden turn of events, your head in her lap as she runs her fingers through your hair, soothing you with her voice. It’s just the chemo, she tells you, it’ll be okay.
“How the fuck are you the one comforting me right now?” The worlds are muffled against her thigh between sobs and you manage to choke out a laugh.
Your name leaves her lips on a shaky exhale. You shake your head, knowing exactly where her mind is going. There’s no way you can listen to her spout off bullshit about being a burden right now.
“No,” you tell her, and you can feel her sigh more than you can hear it.
“Jen,” she tries again, and this time you’re forced to gather yourself, leaving no room for argument.
Her eyes are watery and the corner of her lips are twitching downwards and you absolutely fucking refuse to entertain this train of thought. The tone of your refusal is very much what Judy refers to as your mom voice — the same one you use to end an argument with Charlie. Judy can’t help but smile.
You pull yourself together long enough to climb into the bed, a warmth spreading throughout your chest as the brunette immediately snuggles into you. The lump in your throat releases, if only marginally, allowing your voice to regain its usually steadiness.
“It’s just been a long fuckin day, Judes. And I just — I missed you today.”
She grins and you try to suppress this newfound desire to press a kiss into the creases that line her smile.
“Lucky for you, I’m feeling much better.”
And you know it’s a lie. She knows that you know it’s a lie. The circles beneath her eyes are pronounced and her uncharacteristically pale skin is coated in a sheen of sweat. But you don’t have it in you to call her out on it. Not today.
“How about I whip us up something to eat? We can grab a bottle of wine and take it to the back yard.”
It’s such a fucking Judy thing to offer, when she’s barely able to stay conscious, let alone upright.
“Or,” you argue, “take out and tv.”
“With wine?”
“With wine.”
“Deal.”
Her eyes light up, the only real sign of life that you’ve seen all day, and your laugh is more out of relief than anything else. But then her shoulder nudges yours and when you meet her eyes, the laughter you find behind them makes it all worth it.
#lol this is me spiraling#dead to me spoilers#dead to me#dead to me fic#judy x jen#jen x judy#enjoy my mental illness at work
12 notes
·
View notes
Text
the man I am now
(a very long look back at the year)
2022 marks my 10th year on tumblr, my 25th year of life, and the ending of a strange, dark, 33-month winter that I entered too young and emerge from feeling entirely too old.
At the beginning of this year, my dad noticed that he was having some cognitive problems, assuming they were side-effects of the medication he took to manage his oesophageal cancer, and he asked me to move back home to be his carer, since my brother worked and studied full-time and I had just quit my job.
Only now, in retrospect, do I know that there is no world, anywhere in all of possibility, where I said no. It wasn't a choice, no matter how I agonised over it. I got to work and to complaining right away. I handled it about as gracelessly as any human being can do anything.
The week before I dragged all my crap across the city back to my family home, dad had a fall, and went to the emergency room. There, he was diagnosed with a brain tumour.
I think I gave up on my father more times than I can count. So many nights, waiting in an empty house, imagining his hospital bed growing cold.
Because no matter how much good news he wrung from his test results, no matter the optimism his doctors showed, no matter the plans we so doggedly laid, we had been here before.
My mother died on March 25th, 2020, only three months after being diagnosed with lung cancer.
When dad passed, we knew what crematorium to use, where his ashes would join hers in the memorial garden. All of that had been sealed in stone from the moment of his diagnosis. Because no matter how many medical professionals tried to reassure us that my mother's death had been an anomaly, a tragedy, a hideous confluence of malignance - this was our story. We knew every line, every movement, every futile rise and fall, and we played our parts as precisely as ever.
Everyone feels guilty when someone they love dies. I was sure of my role in his death before he even stopped breathing. I can play the innocent, say I was fumbling blindly through a period of life no one ever wants to imagine, let alone live through, but I know better. I knew what I was doing, when I suggested he try a week in the hospice to see how he found it, and so did he. No matter how I phrased it as a temporary stay, an introduction to the facility, he knew what was happening. When we loaded him into the patient transport to the palliative care hospice, he told me he was beginning the first day of the last stage of his life. I told him not to think like that. As though I didn't know. As though there was ever any other path.
Never once this year did I want him to die. Never once this year did I doubt he would.
I remember thinking that if he died before mid-November, my brother could still go on his Europe holiday. And he did, and he did. I remember thinking if I applied for a course in the US, I'd have something to do next year. And I did and I do.
It's not that I feel like I manifested his death personally. Perhaps, if I had gone a different kind of mad, if I had thrown myself at the bounds of this story with all my strength, I might have lucked into something. Stumbled across some clinical trial that might have done something, anything, even if only alleviate the mystery pain in his left hand that remained until he died. But I didn't. I knew, with the same certainty that I was alive, that he was going to die. And so he did.
Do I feel guilty for capitulating to that certainty? For challenging it only superficially, in a useless and often insulting attempt to cheer my dad up? Do I feel guilty for my inability to imagine another story, not even another ending, just a different middle, a final year of life where I didn't set my house on fucking fire, where we didn't snap at each other as the walls closed in, where he made that stupid train, where I did something, anything, except sit in my room and grow less and less solid, until the only ghost left in the house was me?
I don't know what I feel.
Something was my fault. A lot of things were - arguments, oversleeping, buying the wrong brand of rice, the fire (my god my god. All my furniture was thrown out. I live in a room of strange new things, objects that had never been breathed on by my mother. One bedroom in a four room house. Full and empty and full and empty). But something else was my fault, too. Something More.
I think I'll spend my life looking for it, this thing that burdens me, that overweighs my mind and crushes memories beneath its inscrutable mass.
If I knew what it was, I would understand, then. I'd understand it all, who I am, where I came from, where I'm going, what happened to me, who my parents were - everything, all of it will become clear as soon as I realise what it is I did wrong.
What I could have done differently.
I remember, perhaps a day or two before he went into hospice, waking him up from a fitful and unpleasant nap so he could have dinner. He spoke of an argument with me, and I don't even know what he accused me of saying, just that it was so awful, so directly drawn from the very worst parts of my psyche, that I could focus on nothing but reassuring him that it had just been a dream. But the other conversation he recalled, he could not be convinced was a dream. I wasn't there for his last meeting with his oncologist, doing my best to "give him privacy" (slack off) ((hide from reality)), but it was a month or two before he passed. And my dad felt then, with his transfer from oncology to palliative care, that his doctor had given up on him.
I hated to hear him say that, the bitterness and fear in his voice. I hated to hear him say that, knowing I had given up on him first.
But these are the people we are. We are crushed by the weight of life to the shape it has taken so far, anticipating it to continue in much the same way.
Dad had a few genuine high moments of optimism last year, when it was just oesophageal cancer, when it was one foe, as yet asymptomatic, that could be grappled with, one-on-one. But after the brain cancer diagnosis, we couldn't keep the darkness at bay.
My father wasn't a religious man. His mind was his soul. This was the one death he couldn't bear to die.
And so it was the only death that could take him.
He stayed, right until the very end. It was him that I saw, behind eyes he struggled to move, trying to force breath past lips that could not move.
He was so afraid of being Mum. Mum, who, for the last two? - three? - days of her existence, could not respond. Who could be woken, but not to a world she could see or interact with. Whose eyes darted, vague and furious, as she failed to meet mine. She frightened me then, the wild, lost look on her face. And she frightened Dad, who begged me, in his last week of life, to reassure him that he did not look like that. That he was not leaving me in such an ugly procession.
That he could ask was proof enough. And then his voice deserted him, and it was only with his careful, pleading eyes that he could beg.
What a relief it was when I showed him the pictures I took of the lunar eclipse of the night before and he could respond, in genuine, true reaction, surprise and wonder in his raising eyebrows, the widening of his eyelids.
That night they called me in to say goodbye.
I ran 3 kilometres uphill in the dark, wearing a jacket that seemed to float around me, like I weighed nothing, like I was nothing, like I was flying, furling out into the night, moving at last without the burden of breath or need for fuel, simply going as fast as possibly could.
Not fast enough.
When my mother died I was eating a bowl of spaghetti.
When my father died I was waiting for the lights to change across from the train station.
Life ends in much the same manner in which it is lived.
Weeks in the hospital, watching, wondering, knowing, and still I couldn't be there to say goodbye.
Perhaps that's it, the source of the guilt. Perhaps it's just another thing, another instant of existence to regret. Something you can't change.
A choice that isn't a choice at all.
I died this year.
We all die every year: a hundred tiny deaths as strangers forget our faces, as someone stops ordering their tea the way you first recommended it, as you ignore a text from someone for the last time, and your lives forever diverge. No doubt I died this way as many times as usual. But I have, I feel, become something else, too.
Something I don't particularly like, with so many of the same old flaws and failings - oversleeping, failing to think of others, walking in that hunched way that hurts my shoulders, but something new all the same.
When I first started this blog, I was fourteen years old. I was so loud, and I took up all the wrong space, moving in an awkward, unintentionally exaggerated manner, and annoying everyone for it.
Now I go days without speaking. My tongue sticks to the roof of my mouth and takes effort to dislodge. Something about my body language makes me hard to see, and I'll stand at a shop counter for eons, always surprising the cashier when they turn around, no inkling that anyone was there. There are few other situations beyond shopping where I will interact with someone.
On Christmas Eve I delivered a box of chocolates to my neighbours, and with their combined six extroverted bodies, was shepherded inside to sit in their sunroom and share a platter of fruit with them. It was such a strange and alien bliss, cold grapes in summer, the gentle licks from their dog, the awkward bend of my legs upon the floorboards as I asked my neighbour what she was studying, only to be overcome with an inexplicable gratitude when she said nursing.
But some of this is old, too. You can go back, dig through my archives, my personal posts, my plaintive adolescent agonies that persist, no matter how I try to articulate them better, that feel just as wretched as when I was fourteen, fifteen, sixteen, eternal, undying.
I've always felt other, separate. It scares me to have proof of it. What then, what now? How do I tether myself to the belief that I am human, that I must be, if only because there is nothing else I could be? I'm no longer anyone's child.
I talked about this with my mother once, saying it was funny that we still call people's offspring their "children" even when they're grown, when they're old, and she said that I'd always be her baby, even when I was old and she was even older. Well I'm young and she's gone and I'll never be anyone's baby again.
I feel the need to disclaim that I'm never gonna kill myself. For a variety of reasons, but lately, most of all, because dying is so fucking difficult. I don't really trust anyone to get it right for me. And that's the scariest part about death. No one dies alone. No matter how long it takes to run up that steepest of hills. It's a process, a long drawn out one, even when the death is sudden and an anomaly to oncologists everywhere. The death begins at a point I can't find, and never really ends. Not even when you're forgotten - you're still dead then and you're still dying, as the universe dies around you. Beyond nights in hospitals and days in legal offices, you die over and over, constantly, in everyone's minds, in everyone's lives, as they become people you can't know, needing help you will never be able to provide, and still and still they carry you with them, your dusk-tossed dust long gone while the spectre of the person you once were to them hammers away in their heart.
I'm not gonna kill myself. I don't think I'm qualified to die.
But I'm not sure I can figure out how to be born again, either.
"Das Ei ist die Welt. Wer geboren werden will, muss eine Welt zerstören" [The egg is the world. Whoever wishes to be born must destroy a world]. I don't know what world I have left to destroy.
I have become strange to myself, to the lonely teenager that first settled into this digital space, even as I have failed to ease any of his pains. I never was cut out to be a carer. I'm forgetting how to care at all. I'm becoming thin (my doctor's worried about my diet but I can't remember to eat) and thinner (sometimes I feel like you can see the world through me, transparent and just as frangible as a window, too). I won't let myself die. But that's all I have. I can no longer think in future tense, not specifically, not beyond the pretentious, sweeping eternalisms I declare in an attempt to hitch myself to something bigger than myself.
Nothing is big enough. Multiplying by zero always gets you to the same place.
I set out to write a summary of the year, to try and get my head around this epicentre of my existence. I'm not sure what I ended up with, or where I am. Certainly not how to finish.
My bad.
When I write fiction, I've had the most success by starting with an ending, and building the most satisfying leadup I can to make it worthwhile. Probably should have done that here.
Then again, this year has shown me all too well what happens when you decide on the ending before your story is done.
#personal#death and dying talk#fred says a thing#this started out as a kind of#2022 year in review#Thing.#but there's really only one thing i can talk about#one framework for the life i have lived for the past 12 months#i really did try to find a hopeful note to end on#but sometimes ambiguity is all the comfort you can get#still its there#in the unknowns and unknowables#potential for something#ill be ok#i dont know how to be anything else
9 notes
·
View notes
Text
well im getting pretty good at giving myself 10+ subQ injections in one sitting in part thanks to being trained to know how + having yrs of practice doing it to other ppl (like as a medical assistant... not for fun lol). which is pretty good exposure therapy for my fear of injections (which is useful in case I get switched to a biologic that has no auto-injector pen option or if I get on a healthcare plan that won’t cover auto injector pens) . i used to have terrible nightmares where id be the patient at the clinic getting subQ injections instead of the one giving them. and while having had countless IV injections from being chronically ill i no longer have a fear of those anymore but i can’t do them to myself for shit, for one it’s extremely hard to do correctly and for another i always have to look away when I’m getting them so idk the technique at all. I have no earthly idea how IV drug users manage to do that on themselves because it’s FUCKING difficult to do right. makes me respect the hell out of them for being able to do that with no professional training cuz seems like they have to learn by just trial and error?? and my attempts on myself have always been failures. im seriously considering becoming a phlebotomist just so i can learn how to properly do IVs. cuz subQ is fine and all but it’s just not as good as IV for bioavailability and it’s not as immediate .... i probably sound crazy but when im having really bad crohns flares I need opiates but taking them orally takes too long to kick in for it to be useful (and since during a flare im liable to vomit anything i ingest so it’s a waste of pills anyway If im gonna throw them up immediately)
however intramuscular injections are my absolute worst phobia and when i had a psych he was like exposure therapy is the only way to get over that ... and i have absolutely no desire to do exposure therapy for that, it’s much easier to just get loaded on benzos any time I need a vaccine
#not having healthcare be like#injection phobia#need phobia#drugs#crohns#besides when i got hospitalized for crohns they never let me have more than 5mg of oxy a day which does absolutely nothing#until I got out of the hospital and got a script for oxy and was able to take as much as I wanted but by that time my flare was over so#that was pointless#like they gave me a script for me to get addicted since i didn’t need it — then they cut me off bc of the crackdown on ope scripting#like k thanks for getting me addicted and then cutting me off suddenly without weaning me or anything#idk the medical system is stupid which is why im just taking it into my own hands
11 notes
·
View notes
Text
What is CRO and its role in clinical trials?
CRO stands for Clinical Research Organization. It is an organization that provides services to the pharmaceutical, biotechnology, and medical device industries to assist in the clinical development of their products. CRO`s provide a range of services, including clinical trial design, protocol development, data management, statistical analysis, and regulatory affairs.

They also provide support for clinical trial sites, such as patient recruitment, training, and monitoring. CROs play an important role in the clinical trial process, as they help to ensure that the trial is conducted in a safe and ethical manner, and that the data collected is accurate and reliable.
What is the basic principle of Clinical Research Organization?
The basic principle of Clinical Research Organization (CRO) is to provide services to the pharmaceutical, biotechnology, and medical device industries to help them develop new drugs, treatments, and medical devices.
Clinical Research Organization provide a range of services, including clinical trial design, data management, regulatory affairs, and quality assurance. They also provide expertise in areas such as clinical trial management, data analysis, and statistical analysis.

What are the main components of Clinical Research Organization?
1. Regulatory Affairs: This includes the development and implementation of regulatory strategies, preparation of regulatory documents, and communication with regulatory authorities.
2. Clinical Operations: This includes the management of clinical trials, including protocol design, site selection, patient recruitment, data collection, and data management.
3. Quality Assurance: This includes the development and implementation of quality systems, monitoring of clinical trials, and auditing of clinical sites.
4. Data Management: This includes the collection, storage, and analysis of clinical trial data.
5. Medical Writing: This includes the preparation of clinical trial documents, such as protocols, investigator brochures, and clinical study reports.
6. Project Management: This includes the coordination of all aspects of a clinical trial, including budgeting, timelines, and resource allocation.
3 notes
·
View notes
Text
Who is clinical research coordinator?
A Clinical Research Coordinator (CRC) is a vital member of a clinical research team who plays a significant role in the conduct of clinical trials. In this blog, we will explore what a CRC does, their qualifications, and the skills required to be successful in this role. If you want to do clinical research course you must have a bachelor's degree and at least 3,000 hours of experience as a CRA. There are Top Clinical research training institute field gives you potential to make a difference in people's lives by curing diseases and preventing illnesses, thereby enhancing people's quality of life.
What does a Clinical Research Coordinator do?
A CRC is responsible for coordinating the daily operations of a clinical trial. Their primary role is to ensure that the study is conducted in compliance with the protocol, regulatory requirements, and good clinical practice guidelines. If you want to get proper knowledge of clinical research course you must enroll Clinical Research Course The following are some of the key responsibilities of a CRC:
Protocol Development: A CRC may assist in the development of a research protocol, which outlines the study's objectives, methodology, and data analysis plan. They may also help with the design of data collection tools such as case report forms (CRFs) and electronic data capture (EDC) systems.
Recruitment and Screening of Participants: A CRC may identify and screen potential study participants for eligibility criteria, obtain informed consent, and enroll them in the study. They may also be responsible for tracking and maintaining participant files and medical records.
Study Coordination: A CRC is responsible for coordinating study visits, scheduling procedures and tests, and ensuring that study procedures are performed according to the protocol. They may also monitor participant safety and adverse events, and report them to the sponsor and regulatory authorities as required. Clinical Research course helps you to get knowledge in deep about clinical research.
Data Collection and Management: A CRC is responsible for collecting and managing study data, including ensuring that data is accurate, complete, and entered into the study database in a timely manner. They may also perform data quality checks and resolve any discrepancies.
Study Closeout: A CRC may assist in the study closeout process, which includes archiving study documents, completing study reports, and preparing for audits and inspections.
What are the qualifications of a Clinical Research Coordinator?
To become a CRC, one typically needs a bachelor's degree in a relevant field such as nursing, life sciences, or health sciences. Some employers may require additional certifications, such as the Certified Clinical Research Professional (CCRP) certification from the Society of Clinical Research Associates (SoCRA) or the Association of Clinical Research Professionals (ACRP). Additionally, some employers may require previous experience in clinical research, such as working as a clinical research assistant or study coordinator.
What skills are required to be a successful Clinical Research Coordinator?
To be a successful CRC, one needs to have a combination of technical, interpersonal, and organizational skills. The following are some of the key skills required:
Knowledge of Regulations: A CRC should have a good understanding of regulatory requirements for clinical trials, such as Good Clinical Practice (GCP) guidelines, International Council for Harmonisation (ICH) guidelines, and local regulatory requirements.
Attention to Detail: A CRC should have excellent attention to detail to ensure that study procedures are followed correctly and that data is accurate and complete.
Communication Skills: A CRC should have excellent communication skills to effectively communicate with study participants, study staff, sponsors, and regulatory authorities.
Time Management: A CRC should be able to manage their time effectively to ensure that study procedures are performed according to the timeline outlined in the protocol.
Problem Solving: A CRC should be able to identify and solve problems that arise during the course of the study, such as adverse events or protocol deviations.
In conclusion, a Clinical Research Coordinator is an essential member of a clinical research team who plays a critical role in the successful conduct of clinical trials. They are responsible for coordinating the daily operations of the study, ensuring that it is conducted in compliance with the protocol, regulatory requirements, and good clinical practice guidelines. Hence, Clinical Research Training is the best way to learn easily clinical research. To be a successful CRC, one needs to have a combination of technical, interpersonal, and organizational skills.
2 notes
·
View notes
Text
Metacell Weight Loss - BRAND NEW
Dietary supplement - weight loss
Unveiling Metacell Weight Loss: Fact or Fad for Shedding Pounds?

Metacell Weight Loss bursts onto the scene with a "BRAND NEW" label and a "HOT OFFER," promising to revolutionize your weight loss journey. But before you reach for your credit card, let's dissect the claims and explore whether Metacell lives up to the hype.
The Allure of Weight Loss Supplements
The struggle with weight management is real. Many people turn to dietary supplements like Metacell, hoping for a magic bullet to accelerate fat burning and achieve lasting results. Metacell touts a unique blend of ingredients designed to:
Boost Metabolism: A faster metabolism burns more calories at rest, promoting weight loss.
Suppress Appetite: Feeling less hungry can lead to reduced calorie intake, aiding weight loss efforts.
Target Stubborn Fat: Metacell claims to specifically target areas prone to fat storage.
These promises sound enticing, but is the science behind Metacell solid?
Lifting the Veil: Transparency Matters
A significant concern with Metacell is the lack of transparency regarding its ingredients and their dosages. Without this information, it's impossible to assess the supplement's effectiveness and potential side effects.
Clear Ingredient List: Knowing the exact ingredients allows for research on their potential benefits and side effects.
Dosage Transparency: Understanding the amount of each ingredient helps assess if it's within a safe and effective range.
Clinical Backing: Ideally, the manufacturer should provide evidence from clinical trials supporting the supplement's claims.
Unfortunately, Metacell seems to fall short in these crucial areas.
Sustainable Weight Loss: Beyond the Supplement
Building healthy habits is the cornerstone of successful and sustainable weight loss. Here are some proven strategies to consider:
Balanced Diet: Prioritize whole, unprocessed foods like fruits, vegetables, whole grains, and lean protein.
Portion Control: Be mindful of how much you eat. Using smaller plates and measuring portions can help.
Regular Exercise: Engage in physical activity most days of the week. Aim for a combination of cardio and strength training.
Quality Sleep: Strive for 7-8 hours of sleep each night. Poor sleep can disrupt hormones that regulate appetite and metabolism.
Stress Management: Chronic stress can lead to weight gain. Practice relaxation techniques like yoga or meditation.
These strategies, combined with consulting a healthcare professional or registered dietitian, can create a personalized and effective approach to weight loss.
The Bottom Line on Metacell Weight Loss
While Metacell's "BRAND NEW" label and "HOT OFFER" might grab attention, the lack of transparency and scientific backing raise red flags. Focusing on sustainable lifestyle changes and consulting a healthcare professional are more reliable paths to achieving your weight loss goals. Remember, there's no magic bullet for weight loss. Aim for healthy habi
#Metacell Weight Loss#Dietary Supplement#Weight Loss#Fat Burning#Metabolism Boost#Appetite Suppressant#Ingredient Transparency#Clinical Trials#Sustainable Weight Loss#Balanced Diet#Portion Control#Exercise#Sleep#Stress Management#Consult a Healthcare Professional#Registered Dietician
0 notes
Text
The Evolution of Weight Loss Surgery: From Traditional Methods to Intragastric Balloon
In the realm of medical advancements, the evolution of weight loss surgery stands as a testament to the relentless pursuit of healthier lives for those grappling with obesity. As a seasoned medical professional deeply invested in bariatric surgery and metabolic diseases, it’s fascinating to witness the journey from conventional approaches to innovative techniques like the Intragastric Balloon (IGB).
Allow me to introduce myself: Dr. Shashank Shah, a distinguished figure in the field of weight loss surgery and laparoscopic surgery. With a repertoire of qualifications including an M.B.B.S., M.S., FAIS, and honorary affiliations with esteemed medical societies, my journey has been dedicated to transforming lives through comprehensive obesity treatment and surgical interventions.
At the helm of the Laparo-Obeso Centre, a beacon of excellence in bariatric and metabolic surgery, I’ve had the privilege of witnessing the evolution of weight loss surgery firsthand. Our center, affiliated with Boston University for bariatric training programs, serves as a training ground for aspiring surgeons, fostering innovation and expertise in the realm of obesity management.
Traditionally, weight loss surgery predominantly comprised procedures like gastric bypass and sleeve gastrectomy, which aimed to reduce stomach capacity and alter digestive processes. While these techniques have proven efficacy, the landscape of weight loss surgery has expanded with the introduction of minimally invasive approaches and innovative devices.
One such innovation that has garnered attention is the Intragastric Balloon (IGB). This non-surgical procedure involves placing a deflated balloon into the stomach, which is then inflated to occupy space and induce a feeling of fullness. Unlike traditional surgeries, the IGB offers a less invasive option for individuals seeking weight loss interventions.
The journey towards the adoption of IGB in weight loss surgery has been marked by rigorous research, clinical trials, and advancements in medical technology. As a proponent of evidence-based practice, I’ve closely followed the evolution of IGB and its integration into comprehensive obesity treatment protocols.
The appeal of IGB lies in its minimally invasive nature, shorter recovery times, and potential for reversible weight loss interventions. For individuals who may not be suitable candidates for traditional bariatric surgeries due to various reasons, such as medical comorbidities or surgical risks, IGB offers a viable alternative.
Moreover, the versatility of IGB extends beyond weight loss alone. Studies have demonstrated its efficacy in improving metabolic parameters, such as glycemic control in individuals with type 2 diabetes, further highlighting its potential as a tool for holistic metabolic health management.
As we navigate the ever-evolving landscape of weight loss surgery, it’s imperative to prioritize patient-centric care, tailored interventions, and multidisciplinary approaches. At the Laparo-Obeso Centre, we remain committed to advancing the field of bariatric and metabolic surgery, leveraging innovative techniques like the Intragastric Balloon to empower individuals on their journey towards healthier lives.
In conclusion, the evolution of weight loss surgery from traditional methods to innovative approaches like the Intragastric Balloon underscores the transformative power of medical advancements in combating obesity and metabolic diseases. With a focus on evidence-based practice and patient-centered care, the future of bariatric surgery holds promise for continued innovation and improved outcomes.
0 notes
Text
Prime Minneapolis, Mn Biotech Firms 2024
Through extra intelligent—and extra connected—solutions, we assist simplify routine workflows and communication, enabling care teams to focus on their passion—helping patients get better sooner. And we constantly increase the bar on quality and safety, building upon our legacy of trust with suppliers around the globe. As healthcare continues to evolve, we’re here to support the people on the coronary heart of it. For over 30 years, Miltenyi Biotec has been a significant provider of services that drive biomedical analysis and enhance cell and gene therapy. More than three,500 workers in 28 nations mix excellence in research with innovative merchandise to create cutting-edge solutions that make most cancers and other illness history. Our expertise spans analysis areas including immunology, stem cell biology, neuroscience, and cancer, and clinical analysis areas like hematology, graft engineering, and apheresis.
Decide which of these instruments you want in place and the way you want to set them up. Advance directives is an umbrella time period that may check with any document relating to future medical decision-making. A residing will states your preferences relating to health care planning, corresponding to whether you need life-extending treatment, how you want to manage long-term care, what procedures you do or do not want, and other end-of-life issues.
The value of estate planning software program varies greatly, from free instruments to people who cost a number of hundreds of dollars per person per yr. Many tools function on a subscription model, where you pay a month-to-month or annual fee for access. AlTi Global supplies comprehensive options like threat profiling, asset allocation, and tax planning. Moreover, it provides integration with financial databases for real-time asset valuations and financial knowledge updates, thus preserving your wealth management on level.
Aside from that investment, the two corporations just lately spent $81.1 million in March to buy a multi-level parking garage at 10 Necco Street. Alexandria additionally partnered with Anchor Line Partners to develop a nine-story laboratory facility in South Boston at 99 A Street. Educating and training the subsequent generation of scientists and professionals in cutting-edge applied sciences. Solutions for feeding a rising inhabitants through crop productiveness and meals expertise developments. Development of biosensors for real-time monitoring and quality management in manufacturing. Sustainable farming practices with the development of biopesticides and biofertilizers.
Sarepta continues to be developing therapies for DMD; lots of the firm's more than forty programs target the disease. In January, Sarepta Therapeutics started a phase three clinical trial for a possible therapy for Limb-Girdle muscular dystrophy, a gaggle of rare ailments that have an result on sufferers' muscles. Many leading biotechs develop revolutionary, life-saving therapies, a enterprise that will only be phased out as soon as we find an all-purpose remedy for all illnesses.
Working with biotech investment advisors boston may include potential downsides corresponding to payment of charges (which will cut back returns). There are not any guarantees that working with an adviser will yield optimistic returns. The existence of a fiduciary responsibility doesn't stop the rise of potential conflicts of curiosity. It is essential to be sure that your debts are paid and family members financially taken care of.
The Headquarters Complex includes two high-rise workplace towers, which offer normal and premium workplace areas overlooking the Dubai skyline. DuBiotech is a subsidiary of the federal government of Dubai’s holding company, Dubai Holding, and a member of Dubai Holding’s actual estate unit, Tecom Investments. Dubai Science Park (DuBiotech) is a science and business park positioned in Al Barsha, Dubai, United Arab Emirates (UAE), that helps the biotechnology and pharmaceutical industries. Cabg Medical is a developmental stage medical technology firm looking for to enhance the therapy of coronary coronary heart disease. Inspire Medical Systems, Inc. has developed the world’s first absolutely implanted neurostimulation device accredited by the FDA for the therapy of Obstructive Sleep Apnea (OSA).
#biotech wealth management#biotech financial services#biotech investment advisors#biotech tax planning#biotech estate planning#biotech investment planning#biotech retirement planning#biotech financial services boston#biotech investment advisors boston#biotech tax planning boston#biotech estate planning boston#biotech investment planning boston#biotech retirement planning boston
1 note
·
View note
Last Seen Blogs

hooliganx
Sweet & Tender Hooligan♥

ultrasafe054
ULTRASAFE

arimamary-danmei
Danmei Stuff

honeyraindrop
Life at it's finest

bestcustomerreviews2023
Sem título