#blood csf barrier
Text
The blood-brain barrier (BBB) penetrating drugs market is estimated to be worth USD 900 million in 2030
Advances in biotechnology have enabled the development of versatile in vitro (static and dynamic), in vivo (micro-dialysis), and in situ (brain perfusion) blood–brain barrier models, allowing more effective and safe delivery of drugs across brain capillaries
Over time, extensive R&D efforts have resulted in the development of a number of versatile BBB penetration technologies. These technologies have been designed either to externally alter the permeability of the blood csf barrier or augment the BBB penetrating capabilities of compatible pharmacological interventions.
Roots Analysis is pleased to announce the publication of its recent study, titled, “Blood-Brain Barrier (BBB) Market (2nd Edition), 2020-2030: Focus on Non-Invasive Drug Delivery Technology Platforms and Therapeutics.”
To request a sample copy / brochure of this report, please visit
https://www.rootsanalysis.com/reports/310/request-sample.html
The report features an extensive study of the current market landscape, offering an informed opinion on the likely adoption of BBB penetration technologies and affiliated drugs, over the next decade. The report features an in-depth analysis, highlighting the diverse capabilities of stakeholders engaged in this domain. In addition to other elements, the study includes:
§ More than 110 drugs, capable of penetrating this elusive barrier are currently being evaluated for the treatment of CNS drugs disorders; there are 35+ technology platforms for the development of BBB penetrant drugs
§ An overview of the overall landscape of BBB penetration technologies, featuring an in-depth analysis of the technologies based on a number of parameters
§ A detailed assessment of the current market landscape of BBB penetrant drugs.
§ Identification of contemporary market trends depicted using three schematic representations, which include [A] a tree map representation, [B] a bubble analysis and [C] an informative heptagon representation.
§ An insightful competitiveness analysis of BBB penetration technologies, taking into consideration the supplier power and key technology specific information.
§ Elaborate profiles of prominent technology developers that are engaged in the development of at least four drugs.
§ An analysis of the partnerships that have been established in the domain, in the period between 2014 and 2020.
§ An elaborate discussion on the deal structures of various types of technology licensing agreements inked in this domain.
§ An analysis of the investments made in the domain, in the period between 2014 and 2020 (till March).
§ An in-depth analysis of the various patents that have been filed / granted related to BBB penetration technologies, till November 2019.
§ An insightful chessboard analysis highlighting the most preferred / popular drug development strategies / paths adopted by majority of the drug developers (with clinical candidates) in order to progress their lead drug candidates.
§ An assessment of the most commonly targeted disorders affecting the central nervous system , shortlisted on the basis of number of BBB penetrant drugs in development.
§ A list of 240+ drug developers targeting Alzheimer’s disease and Parkinson’s disease that are likely to partner with BBB penetration technology providers.
§ A case study highlighting the working principle of the most common approaches that are being employed for the development of BBB penetration technologies.
§ An informative analysis of contemporary Google Trends in the time period between 2015 and 2019 (till December) and insights generated from recent news articles related to the BBB, indicating the increasing popularity of this domain.
A detailed market forecast, featuring analysis of the current and projected future opportunity across key market segments (listed below) :
§ Type of Payment Model Adopted
§ Upfront payments
§ Milestone payments
§ Type of Molecule
§ Small Molecules
§ Biologics
§ Target Disease Indication
§ Brain Metastases in Breast Cancer
§ Glioblastoma Multiforme
§ Hunter Syndrome
§ Hurler Syndrome
§ Leading Technology Platforms
§ G®-Technology
§ J-Brain Cargo® Technology
§ LRP-1 Technology
§ Trojan Horse Technology
§ Leading Drug Developers
§ 2-BBB
§ Angiochem
§ ArmaGen
§ JCR Pharmaceuticals
§ Key Geographical Regions
§ North America
§ Europe
§ Asia-Pacific
Transcripts of interviews held with the following senior level representatives of stakeholder companies
§ Ram Bhatt (Chief Executive Officer, Chairman and Founder, Innovative California Biosciences International (ICBI))
§ Frank S Walsh (Chief Executive Officer and Founder, Ossianix)
§ Pieter Gaillard (Chief Executive Officer and Co-Founder, 2-BBB)
§ Rob Hutchison (Chief Executive Officer and Chairman, biOasis Technologies)
§ Mathias Schmidt (Chief Executive Officer, ArmaGen)
§ Mark L Peterson (Chief Operating Officer, Cyclenium Pharma)
§ Xavier Rivero (Chief Operating Officer, Sagetis Biotech)
§ Carole Desseaux (Head of Clinical Affairs, CarThera)
§ Jamal Temsamani (Head of Drug Development, Vect-Horus)
§ Kevin Kit Parker (Professor, Wyss Institute, Harvard University)
Key companies covered in the report
§ Angiochem
§ ArmaGen
§ BioArctic
§ Cyclenium Pharma
§ Denali Therapeutics
§ ICB International
§ Iproteos
§ JCR Pharmaceuticals
§ Lauren Sciences
§ Medesis Pharma
§ Ossianix
§ Vect-Horus
For additional details, please visit
https://www.rootsanalysis.com/reports/view_document/blood-brain-barrier-drug-delivery/310.html or email [email protected]
You may also be interested in the following titles:
1. Novel Coronavirus (Covid-19): Preventive Vaccines, Therapeutics and Diagnostics in Development
2. DNA-Encoded Libraries: Platforms and Services Market
3. Global Stem Cells Market: Focus on Clinical Therapies, 2020–2030
About Roots Analysis
Roots Analysis is one of the fastest growing market research companies, sharing fresh and independent perspectives in the bio-pharmaceutical industry. The in-depth research, analysis and insights are driven by an experienced leadership team which has gained many years of significant experience in this sector. If you’d like help with your growing business needs, get in touch at [email protected]
Contact:
Ben Johnson
+1 (415) 800 3415
+44 (122) 391 1091
0 notes
Text
BED Disorder(sleep disorder)
If you’re referring to a disorder related to beds or sleep, it’s important to note that I am an AI language model and not a medical professional. However, I can provide you with some general information.
If you’re having difficulties with sleep or experiencing disruptions in your sleep patterns, it’s possible that you may be dealing with a sleep disorder. Sleep disorders can affect the quality,…

View On WordPress
#anatomy#animation#basal ganglia#blood-brain barrier#brain#cerebellar#cerebellum#cerebral#cns#crest#csf#dopamine#embryology#exam#explain#HEALTH#htownrush#hypothalamus#infection#kaplan#khan#limbic#local#medicine#medulla#motor#nervous system#neural#neurology#neuron
0 notes
Text
Psychopharmacology, pt. 2: Pharmacokinetics
Bio-availability: amount of drug in the blood that is free to bind at target sites.
Pharmacokinetic factors determining drug action:
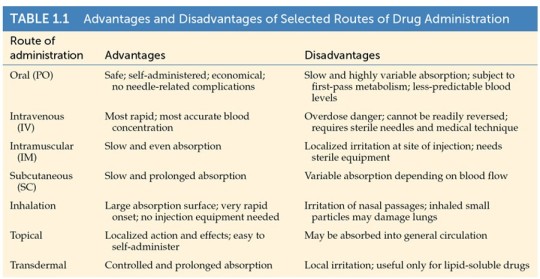
1. Routes of administration
2. Absorption
3. Distribution
4. Binding/effects
5. Inactivation (metabolism)
6. Excretion
Routes of Administration
Drugs must get into the nervous system to have an effect.
The way that a drug enters and passes through the body to reach its target is called route of administration.
oral
injection
inhalation
topical application
transdermal
To bypass the blood-brain barrier: injection in the cerebro-spinal fluid or directly in the brain.

The route of administration affects the dosage of a drug, i.e. the amount of drug needed to have a psychoactive effect.
Ex. amphetamine:
1000 mg - orally
100 mg - injected or inhaled
10 mg - injected into the CSF
1 mg - injected directly into the brain

Oral Administration
PO = per os (Latin, “by mouth”)
Pros:
Safest, easiest, and most common way to take drugs
Longest route
Cons:
Affected by how much food is in the stomach
Delivery often erratic and incomplete
Most difficult pathway to the brain, because the drug has to...
survive stomach acid and enzymes
be absorbed by intestine
enter into the blood stream
pass through the blood-brain barrier
Example: Insulin is not resistant to stomach acid and enzymes, so it cannot be given orally.

Injections
Before a drug (including cocaine, amphetamines, barbiturates, morphine, and heroin) can be injected, it must be liquid.
Vehicle:
normal saline (0.9% NaCl)
viscous oil (often sesame oil) for depot injections
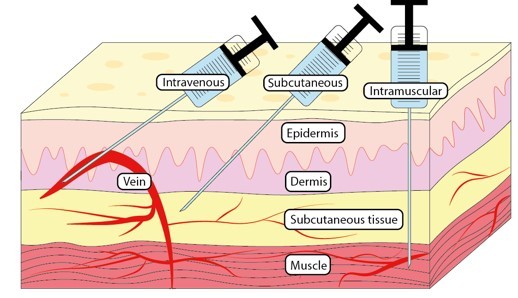
Intravenous (IV) - into the blood stream
Intramuscular (IM) - into a muscle
Subcutaneous (SC) - under the skin
In the CSF
Intracranial (IC)
Intravenous Injections
Pros:
fastest and most accurate method; drug reaches brain instantly
fewer barriers to pass
Cons:
painful, invasive
quick onset of drug effect can be a hazard, because you have little time to correct an overdose or allergic reaction. the drug cannot be removed from the body as it can by stomach pumping.
lack of sterility can result in infectious diseases, including HIV (this risk is reduced with free needle exchanges)
Intramuscular Injections
Pros:
slower than IV, more even absorption over period of time
absorption can be slowed by combining the drug with another drug that constricts blood vessels, or with vegetable oil
Cons:
injection solution can be highly irritating, causing significant muscle discomfort
Subcutaneous Injection
- drug injected just below the skin
- absorption is slow but can be variable; can be slowed by vegetable oils or implantation of a pellet or delivery device
Ex. SUBLOCADE (buprenorphine XR) is used for subcutaneous injection only. It is designed to deliver buprenorphine at a controlled rate over a one month period.
Inhalation
- smoke of burning dried plant material (tobacco, cannabis), aerosol/vapor, gases can be inhaled and absorbed through the lungs
- takes effect quickly
- rapid absorption because the lungs have large surface area and many capillaries
Topical Application
- drug is applied to mucous membranes in the eyes, nose, colon, or vagina
- mostly local effects, but drug can be absorbed into the bloodstream and have systemic effects
- oral topical application: drugs that may be chewed, but not swallowed (ex. chewing tobacco)
Intranasal Administration/Insufflation
- can cause local effects such as relieving nasal congestion, but can also have systemic effects
- drug effect peaks in 15 to 30 minutes
- powdered drugs (ex. cocaine), medicinal nasal sprays (ex. ketamine for depression)
Transdermal Administration
- administration via skin patches: controlled and sustained delivery of drug
- nicotine patches: to treat nicotine use disorder
- fentanyl patches: to alleviate pain
Absorption: movement of the drug from site of administration to the blood circulation.

Factors that Influence Absorption:
drug solubility
stomach contents
concentration of the drug (generally high concentrations are absorbed more rapidly than low concentrations)
size and sex of individual (a larger person has more body fluid to dilate a drug; AFAB people tend to have less body fluid than AMAB people)
circulation to side of absorption (increased blood flow due to massage or local application of heat enhances absorption)
area of absorbing surface (drugs are absorbed very rapidly in regions with large surface areas such as the lungs and the intestines)

Fat-soluble drugs: can easily pass through the cellular membranes by passive diffusion.
Cell membranes are primarily phospholipids, which have a negatively charged region (hydrophilic) and two uncharged tails (hydrophobic), arranged in a bilayer.

Heroin vs. Morphine
Heroin is derived from morphine; they stimulate the same receptors.
However, heroin is 2-3x more potent than morphine, because it is more fat-soluble.

Distribution
- highest concentration of a drug will occur where blood flow is greatest
- blood brain barrier limits movement of ionized molecules
- Because the brain receives about 20% of the blood that leaves the heart, lipid-soluble drugs are readily distributed to brain tissue.
Blood-Brain Barrier
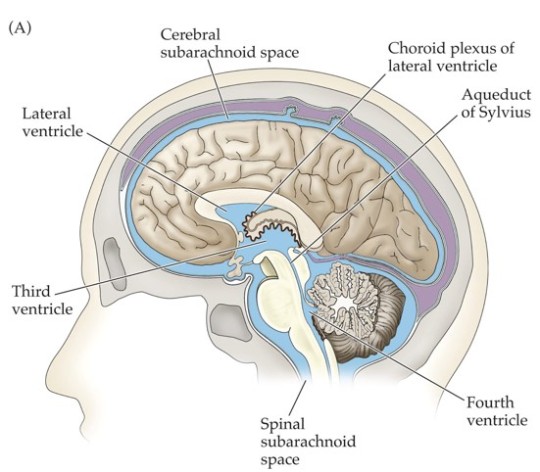
Cerebrospinal fluid (CSF) fills the subarachnoid space around the brain and spinal cord, ventricles, and canals.
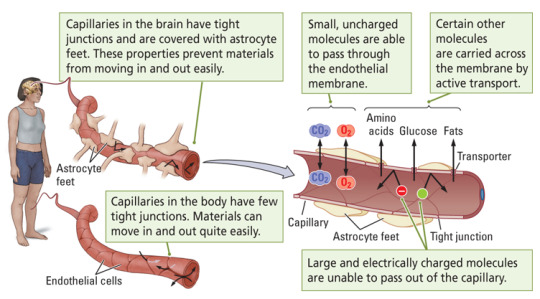
Blood-brain barrier: the separation between brain capillaries and the brain/CSF.
Many substances that diffuse out of the blood do not enter the CSF.
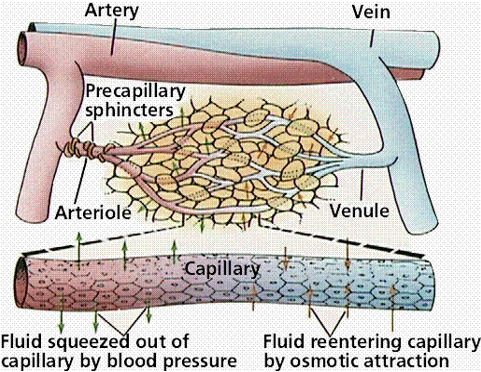
Typical capillaries are designed to allow movement of materials between the blood and surrounding cells.
Brain capillaries have no clefts, movement of water-soluble molecules is minimized.
Astrocytes help maintain tight junctions between capillary endothelial cells.

It is important to know whether a drug can cross the blood-brain barrier.
Physostigmine crosses the blood-brain barrier.
- blocks AChE and increases availability of the neurotransmitter acetylcholine
- the antidote for anticholinergic poisoning with scopolamine, atropine
Neostigmine does not cross the blood-brain barrier.
- also blocks AChE and increases acetylcholine, but only peripherally
- treatment for diseases such as myasthenia gravis (muscle weakness) without CNS side effects
Oxycodone crosses the blood-brain barrier:
binds to opioid receptors
painkiller
can produce euphoria
side effects include constipation
Loperamine (Imodium) does not cross the blood-brain barrier:
binds to peripheral opioid receptors in the intestines
treatment for diarrhea
Drug depots: binding at inactive sites where no biological effect is initiated (plasma proteins, muscle, fat)
Drug molecules tied up in these depots cannot reach active sites or be metabolized by the liver, but binding is reversible.
Depot binding affects magnitude and duration of drug action: it reduces concentration of drug at its sites of action and delays effects.
Depot binding can result in drugs remaining in the body for extended periods.
- Ex. Tetrahydrocannabinol (THC) can be detected in urine for several days after a single dose.
Thiopental is a rapid-onset, short-acting barbiturate (administered as general IV anesthetic)
- used for medically induced coma, euthanasia, status elipepticus
- previously the first of three drugs administered during most lethal injections in the USA
- due to depot binding, thiopental brain levels drop within 5 minutes
Inactivation and Elimination
- molecules of drugs are transformed (metabolized) with the help of enzymes
Metabolism: the processes involved in transforming/destructing drug molecules.
Drugs are broken down in the kidneys, livers, and intestines. Most biotransformation occurs in the liver. Metabolites are excreted.
Drug clearance from the blood is usually exponential (first-order kinetics).
Only a small fraction of clearance sites are occupied, so the rate is concentration-dependent.
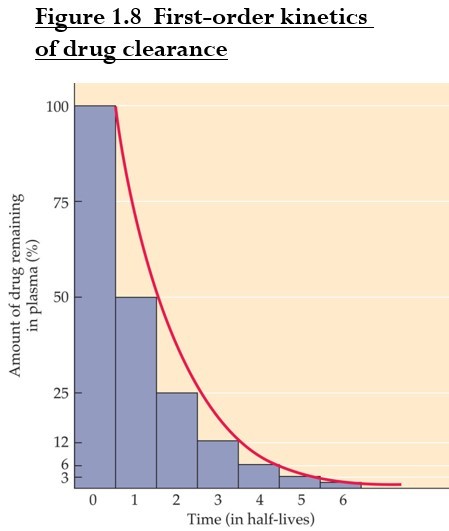
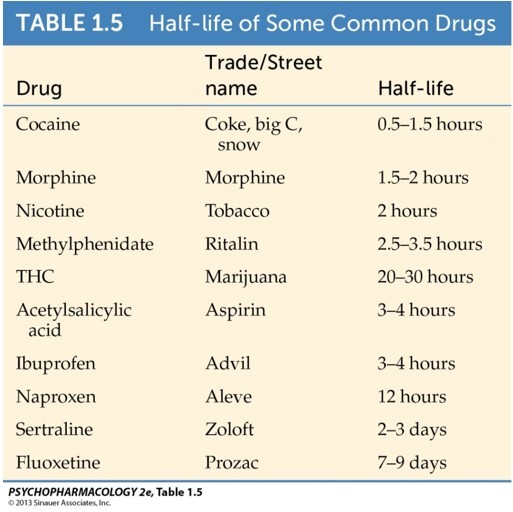
Half-life: amount of time required for removal of 50% of the drug (t 1/2).
Half-life affects interval between doses. A drug with a shorter half-life should be taken more often.
Drug almost eliminated after 4-5x half-life.
Goal: maintain concentration of a drug in blood plasma at a constant level.
Steady state plasma level: absorption/distribution phase is equal to the metabolism/excretion phase.
Target therapeutic concentration is achieved only after multiple doses, usually 4-5.

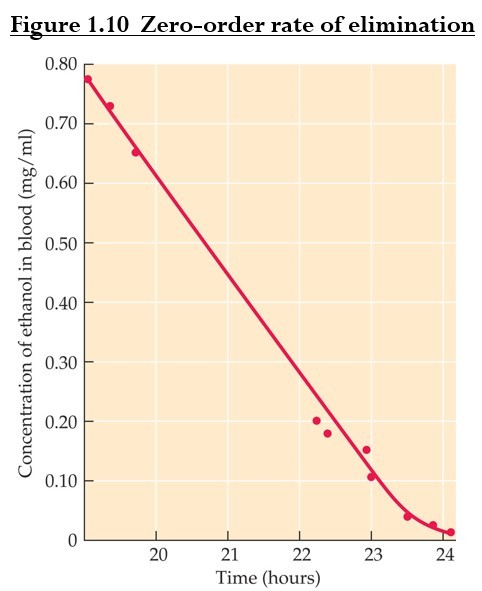
Some drugs are eliminated according to zero-order kinetics: molecules are cleared at a constant rate regardless of concentration.
It occurs when drug levels are high and routes of metabolism or elimination are saturated (ex. alcohol).
First Pass Metabolism
First pass metabolism of drugs that are taken orally, swallowed and absorbed from the digestive system occurs mostly in the liver.
Alternative routes of administration avoid the first-pass effect (e.g. intravenous, inhalation, transdermal and sublingual)
Some therapeutic drugs must be administered by injection, or in high doses.

Drugs can be modified through oxidation, reduction, hydrolysis, or synthetic reactions.
Microsomal enzymes: liver enzymes that metabolize psychoactive drugs.
They lack strict specificity and can metabolize a wide variety of chemicals.
The cytochrome P450 (CYP450) enzyme family are responsible for oxidizing most psychoactive drugs.
Factors that modify biotransformation capacity include:
Enzyme induction
Enzyme inhibition
Drug competition
Individual differences in age, gender, and genetics
Enzyme induction: repeated use of a drug increases number of enzyme molecules and speeds biotransformation.
Repeated drug use ----> Increase in enzymes ---> Higher metabolism ---> Lower bioavailability
Drug can induce its own enzymes. In this case, drug tolerance happens = drug becomes less effective with repeated use.
Sometimes enzymes for the other drugs are induced. For example, cigarette smoking increases CYP450 enzymes. People who are heavy smokers may need higher doses of drugs such as antidepressants and caffeine that are metabolized by the same enzyme.
Enzyme inhibition: a drug may inhibit an enzyme, also reducing metabolism of other drugs. Effects are more intense or prolonged; toxicity is possible.
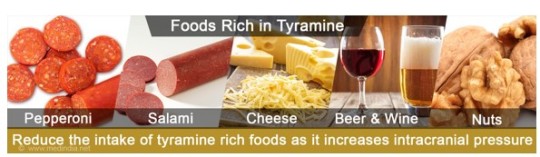
Example: Antidepressant drugs monoamine oxidase inhibitors (MAOIs) inhibit enzyme MAO. MAO metabolizes monoamines, including tyramine, which is found in red wine, beer, some cheeses, etc. When individuals who are taking these antidepressants eat foods rich in tyramine, dangerous high blood pressure and cardiac arrhythmias can occur, making normal foods potentially life threatening.
Drug competition for an enzyme: elevated levels of one drug reduces metabolism of the second, causing potentially toxic levels.
- Example: alcohol + sedatives (such as Valium) compete for cytochrome P450.
Excretion: the processes of eliminating waste products.
Drugs are excreted in urine, feces, sweat, breast milk, and exhaled air.
Urine is the most important route for drug elimination.
- The kidneys filter materials from the blood, unless they are large or bound to plasma proteins.
Drugs can be excreted changed and/or unchanged.

3 notes
·
View notes
Quote
The microbiota-gut-brain axis is a highly popular concept in neurobiology, medicine, and immunology. This is anatomically founded on the obvious connections between the intestinal mucosa and the central nervous system (CNS). There are ascending neural pathways conveying sensory information via the spinal cord and brain stem, and the descending autonomic nervous system (ANS) modulates a spectrum of gastrointestinal functions. The immunological evidence for this axis stems from the observations that (1) the presence of the microbiota (compared with germ-free status) alters the composition and function of glial cells (both macroglia and microglia) and neurons in the CNS, (2) the integrity of the blood-brain barrier (BBB) is also shaped by microbial colonization of the intestine, and (3) during autoimmune inflammation, both B and T cells can enter the leptomeninges, cerebrospinal fluid (CSF), or CNS parenchyma as active leukocytes after induction in the mucosal immune system.1 Given the long-established paradigm of the BBB and an immune-privileged CNS that will potentially tolerate transplantation of xenobiotic tumors into the brain parenchyma, it is still surprising that the microbiota—which has a relatively compartmentalized biomass in the lower intestine and on other body surfaces—has such clear immunological and neurological consequences.
One representation of the microbiota-gut-brain axis is a balanced triangular interaction between each of the three components. Designating the gut and brain nodes as information-processing centers and referring to them as the “gut connectome” and “brain connectome,” respectively,2 helps us consider the mechanisms underlying the potentially pervasive nature of the interactions on each edge of the conceptual triangle. Nevertheless, the reality is that there is compartmentalization of the microbiota, the neuro-immune system of the gut, and the CNS. In this review, we explore the interconnections between these nodes that retain the anatomical and functional perspectives of the largely autonomous intrinsic neural circuits of the gut (enteric nervous system [ENS]), the CNS immune privilege, and the distinct nature of mucosal immunity to focus on how and why interactions between these systems can escape compartmentalization. We consider how the gut connectome is composed of an independent integrative ENS, an epithelial paracellular permeability barrier, and endothelial barriers.
Boundaries and integration between microbiota, the nervous system, and immunity - ScienceDirect
0 notes
Text
Nanoparticles Treat Tumors of Deadly Brain Cancer - Technology Org
New Post has been published on https://thedigitalinsider.com/nanoparticles-treat-tumors-of-deadly-brain-cancer-technology-org/
Nanoparticles Treat Tumors of Deadly Brain Cancer - Technology Org
Using nanoparticles administered directly into the cerebrospinal fluid (CSF), a research team has developed a treatment that may overcome significant challenges in treating a particularly deadly brain cancer.
Illustrative image related to a brain cancer. Image credit: Yale University
The researchers, led by professors Mark Saltzman and Ranjit Bindra, administered to mice with medulloblastoma a treatment with specially designed drug-carrying nanoparticles. The study, published in Science Translational Medicine, showed that mice who received this treatment lived significantly longer than mice in the control group.
Medulloblastoma, a brain cancer that predominantly affects children, often begins with a tumor deep inside the brain. The cancer is prone to spread along two protective membranes known as the leptomeninges throughout the central nervous system, particularly the surface of the brain and the CSF. Leptomeningeal spread is seen in a number of primary brain tumors, as well as in brain metastases from solid tumors in the breast, lung, and other places. Because there are no anatomic barriers in the CSF to prevent further growth, these cancers can spread rapidly.
Targeting tumors in the CSF has proven difficult, in part because the fluid rapidly cycles through the central nervous system about four times a day in humans, typically flushing away anti-tumor drugs before they’ve had a chance to accumulate and have any effect.
“It’s like a waterfall system, with a fast, rapid fluid flow,” said Minsoo Khang, lead author of the study and a former graduate student in Saltzman’s lab.
To overcome this obstacle, the research team fabricated nanoparticles that adhere to tumors. Designed in Saltzman’s lab, these nanoparticles are made with degradable polymers that slowly release a DNA repair inhibitor, talazoparib, which is FDA-approved and currently used in the clinic for a number of cancers. The drug is one of a relatively new class of cancer drugs known as PARP inhibitors, which block an enzyme that helps repair DNA. Without the ability to repair their DNA, tumor cells are more likely to die.
The nanoparticle treatment is injected intrathecally – that is, it’s delivered directly between the leptomeninges protecting the CSF. Over a period of weeks, the researchers detected the presence of the nanoparticles in the CSF for as long as 21 days after a single dosing.
“We were very excited to have found a medium that has long-term retention in this fluid space, which is otherwise challenging,” Khang said.
Treating brain cancers in general is challenging since few treatments can penetrate the blood-brain barrier, a natural defense system that can block potentially helpful drugs. The research team’s method could offer a solution.
“There’s been very little work on intrathecal delivery of nanoparticles, so we’re very excited because it can allow us to go after the leptomeningeal spread of disease from brain metastases,” said Bindra, the Harvey and Kate Cushing Professor of Therapeutic Radiology and Professor of Pathology. “This has really opened up an entirely new way to treat these patients, although much more work needs to be done.”
Using the nanoparticles to target the tumors allowed the researchers to use the drug talazoparib, which has proven to be effective in a number of solid tumors outside of the brain. Because the drug has limited to no penetration of the central nervous system, however, an orally delivered dose would have limited efficacy against tumors with leptomeningeal spread.
“By encapsulating it in a nanoparticle and directly injecting it into the CSF, we now get very high exposure in just that area,” said Saltzman, the Goizueta Foundation Professor of Biomedical Engineering, Chemical & Environmental Engineering & Physiology, and a member of Yale Cancer Center.
Delivering the drug intrathecally also avoids injecting it directly into the brain, a technique referred to as convection-enhanced delivery. This very challenging procedure can be performed only a few times a year. Intrathecal injections, in contrast, are much less invasive and can be given without a hospital stay.
“This is huge for us, because now we can do multiple nanoparticle treatments over time,” Bindra said.
In addition to the nanoparticle injection, mice were also given an oral dose of a chemotherapy drug known as temozolomide.
“It’s a new platform where we can give these oral chemotherapies that get across the blood-brain barrier and a targeted agent just in the central nervous system,” Bindra said. “In essence, this compartmentalization of combination therapy will enhance synergistic tumor cell killing while minimizing systemic toxicity.”
The mice that received the nanoparticle-based treatment lived significantly longer than the mice who received drug therapy that didn’t use nanoparticles and even longer than the mice that received no treatment. Further, there was much less cancer spreading in the mice that received the drug-carrying nanoparticles.
The researchers said the next steps will be to validate the approach in larger animal models, eventually followed by human testing. The team also plans to test the treatment method on other cancers, particularly those that tend to spread to the brain.
Source: Yale University
You can offer your link to a page which is relevant to the topic of this post.
#amp#approach#barrier#Biotechnology news#blood#blood-brain barrier#Brain#brain cancer#brain tumors#Cancer#cancer drugs#cell#Cells#chemical#Chemistry & materials science news#chemotherapy#Children#defense#Disease#DNA#DNA repair#drug#drugs#engineering#Environmental#enzyme#FDA#Featured life sciences news#Foundation#growth
0 notes
Text
The Different Kinds of Nervous Tissue
Nervous tissue is responsible for transmitting and processing information in the body. It consists of two main types of cells: neurons and neuroglia (or glial cells). Here are the different kinds of nervous tissue:
Neurons:
Neurons are the functional units of the nervous system, responsible for transmitting electrical impulses.
Sensory Neurons: Carry signals from sensory receptors (e.g., in the skin, eyes, ears) to the central nervous system (CNS).
Motor Neurons: Transmit signals from the CNS to effectors such as muscles and glands, enabling movement and response.
Interneurons: Connect sensory and motor neurons within the CNS, facilitating integration and coordination of signals.
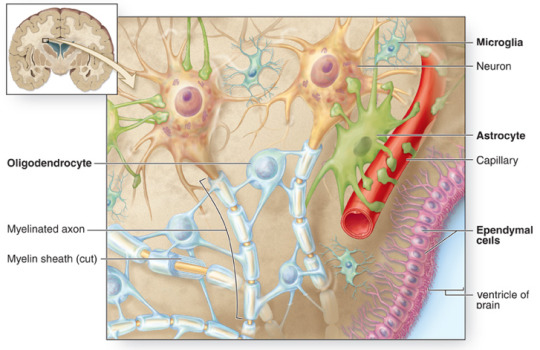
Neuroglia (Glial Cells):
Glial cells provide support, protection, and nourishment to neurons.
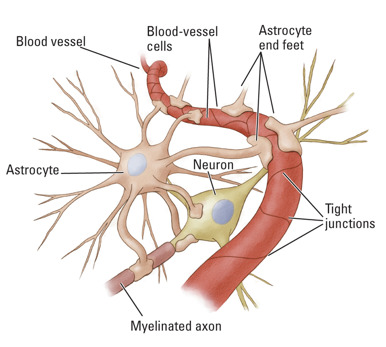
Astrocytes: Maintain the blood-brain barrier, regulate nutrient and ion concentrations, and provide structural support.
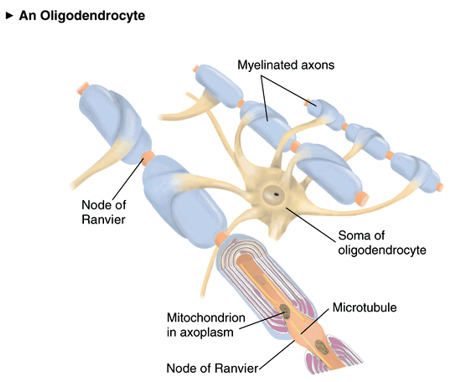
Oligodendrocytes: Produce myelin, a fatty substance that wraps around axons in the CNS, speeding up signal transmission.
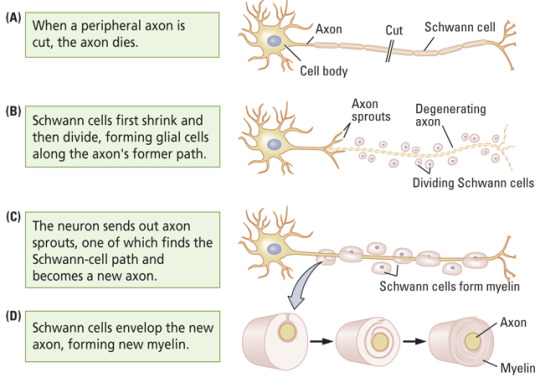
Schwann Cells: Similar to oligodendrocytes but found in the peripheral nervous system (PNS), where they produce myelin.
Microglia: Act as immune cells, removing debris, pathogens, and damaged cells in the CNS.
Ependymal Cells: Line the ventricles of the brain and central canal of the spinal cord, producing cerebrospinal fluid (CSF).
The combination of neurons and glial cells allows for the proper functioning of the nervous system. Neurons transmit signals, while glial cells support and protect them, ensuring optimal communication and functioning throughout the body.
0 notes
Text
Procure high-quality CSF Samples for research.

What exactly are CSF samples?
Cerebrospinal fluid (CSF), also known as brain fluid, is a clear, colorless, watery bodily fluid circulating the brain and spinal cord's structures that control and coordinate the functions of the central nervous system (CNS) in our body. It acts as a cushion for preventing damage to the brain and spinal cord in case of mechanical injury or trauma. Also, it helps transport neuromodulators and neurotransmitters in the body and excretes the metabolic waste products from the brain tissues. Moreover, CSF plays a crucial role in providing immunological protection to brain tissues.
CSF Biomarkers for Neurological Diseases
Biomarkers are the proteins that alter their expression in various illness conditions. For decades, medical professionals and clinical researchers have used biomarkers to track the development of diseases and how well they respond to treatment. To replace or supplement subjective techniques of diagnosing individuals with neurological illnesses, biomarkers could offer an objective evaluation of the disease. On the other hand, plasma proteins might not correctly represent illness processes in the brain because the blood-brain barrier keeps circulating blood from entering the brain. In contrast, the CSF surrounding the brain and spinal cord may include more reliable biomarkers of neurological illnesses. Against this background, finding robust CSF biomarkers to monitor the onset and progression of neurological disorders is currently of particular interest to scientists, clinical researchers, and medical professionals to understand more about the disease's nature and pathophysiology. CSF analysis aids in the diagnosis of a variety of illnesses, including meningitis, encephalitis, brain disorders, autoimmune diseases, Alzheimer's disease, etc.
High-quality Human CSF Samples are Now Available Online:
Central BioHub is one of the world's leading human biospecimens providers with successful records of serving hundreds of well-reputed research organizations, pharmaceuticals, and in-vitro diagnostic R&D units, located in different parts of the world.
It's time to say goodbye to the old, tedious process of biospecimen acquisition. Ramping up research on banked cerebrospinal fluid samples for a high-impact medical breakthrough, Central BioHub offers a wide range of clinically graded CSF samples collected from patients diagnosed with neurological disorders to progress further CSF research around the globe. We offer CSF biospecimens for research that have completed CSF analysis for specific disease biomarkers and are stored in sterile, cryogenic conditions at our supplier's biobank. Each CSF biomarker sample is richly annotated with an extensive clinical evaluation profile and medical history.
To simplify the biospecimen acquisition process, Central BioHub connects top-tier accredited human biospecimen biobanks and biorepositories with scientists worldwide to hasten the drug discovery and development process. Customers can now purchase the biospecimens they need online in a few quick steps. Get ready for a life-changing experience. Start with Central BioHub today - the world's leading online human biospecimen marketplace.
0 notes
Text
Neurologic sequalae of COVID-19 are determined by immunologic imprinting from previous Coronaviruses.
Preliminary report; Coronavirus disease 2019 (COVID-19), which is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), remains a global public health emergency. Although SARS-CoV-2 is primarily a respiratory pathogen, extra-respiratory organs, including the central nervous system (CNS), can also be affected. Neurologic symptoms have been observed not only during acute SARS-CoV-2 infection, but also at distance from respiratory disease, also known as long-COVID or neurological post-acute sequelae of COVID-19 (neuroPASC). The pathogenesis of neuroPASC is not well understood, but hypotheses include SARS-CoV-2-induced immune dysfunctions, hormonal dysregulations, and persistence of SARS-CoV-2 reservoirs. In this study, we used a high throughput systems serology approach to dissect the humoral response to SARS-CoV-2 (and other common Coronaviruses - 229E, HKU1, NL63, OC43) in the serum and cerebrospinal fluid (CSF) from 112 infected individuals who developed or did not develop neuroPASC. Unique SARS-CoV-2 humoral profiles were observed in the CSF of neuroPASC. All antibody isotypes (IgA, IgM, IgA) and subclasses (IgA1-2; IgG1-4) were detected in serum, whereas CSF was characterized by focused IgG1 (and absence of IgM). These data argue in favor of compartmentalized brain-specific responses against SARS-CoV-2 through selective transfer of antibodies from the serum to the CSF across the blood-brain-barrier, rather than intrathecal synthesis, where more diversity in antibody classes/subclasses would be expected. Moreover, compared to individuals who did not develop post-acute neurological complications following infection (n=94), those with neuroPASC (n=18) exhibited attenuated systemic antibody responses against SARS-CoV-2, characterized by decreased capacity to activate antibody-dependent complement deposition (ADCD), NK cell activation (ADNKA) and to bind Fc{gamma} receptors. However, surprisingly, neuroPASC showed significantly expanded antibody responses to other common Coronaviruses, including 229E, HKU1, NL63, and OC43. This biased humoral activation across coronaviruses was particularly enriched in neuroPASC individuals with poor outcome, suggesting an original antigenic sin (or immunologic imprinting), where pre-existing immune responses against related viruses shape the response to current infection, as a key prognostic biomarker of neuroPASC disease. Overall, these findings point to a pathogenic role for compromised anti-SARS-CoV-2 responses in the CSF, likely resulting in incomplete virus clearance from the brain and persistent neuroinflammation, in the development of post-acute neurologic complications of SARS-CoV-2 infection. https://www.medrxiv.org/content/10.1101/2022.11.07.22282030v1?rss=1%22&utm_source=dlvr.it&utm_medium=tumblr Read more ↓
0 notes
Text
Venous Drainage of The Brain
Venous Drainage of The Brain
The veins of the brain drain into the intracranial dural venous sinuses, which eventually open into the internal jugular veins of the neck.
The veins emerge from the brain, traverse the subarachnoid space, pierce the arachnoid mater and meningeal layer of dura mater to drain into the venous sinuses.
The characteristic features of venous drainage of the brain are:
• The venous return in the…

View On WordPress
1 note
·
View note
Photo

T Cells and Neurons Talk to Each Other
By Ashley Yeager (The-Scientist). Image & Infographic: STOCKSY.COM, ADDICTIVE CREATIVES and CATHERINE DELPHIA.
Conversations between the immune and central nervous systems are proving to be essential for the healthy social behavior, learning, and memory.
Tiroyaone Brombacher sat in her lab at the University of Cape Town watching a video of an albino mouse swimming around a meter-wide tub filled with water. The animal, which lacked an immune protein called interleukin 13 (IL-13), was searching for a place to rest but couldn’t find the clear plexiglass stand that sat at one end of the pool, just beneath the water’s surface. Instead, it swam and swam, crisscrossing the tub several times before finally finding the platform on which to stand. Over and over, in repeated trials, the mouse failed to learn where the platform was located. Meanwhile, wildtype mice learned fairly quickly and repeatedly swam right to the platform. “When you took out IL-13, [the mice] just could not learn,” says Brombacher, who studies the intersection of psychology, neuroscience, and immunology.
Curious as to what was going on, Brombacher decided to dissect the mice’s brains and the spongy membranes, called the meninges, that separate neural tissue from the skull. She wanted to know if the nervous system and the immune system were communicating using proteins such as IL-13. While the knockout mice had no IL-13, she reported in 2017 that the meninges of wildtype mice were chock full of the cytokine. Sitting just outside the brain, the immune protein did, in fact, seem to be playing a critical role in learning and memory, Brombacher and her colleagues concluded.
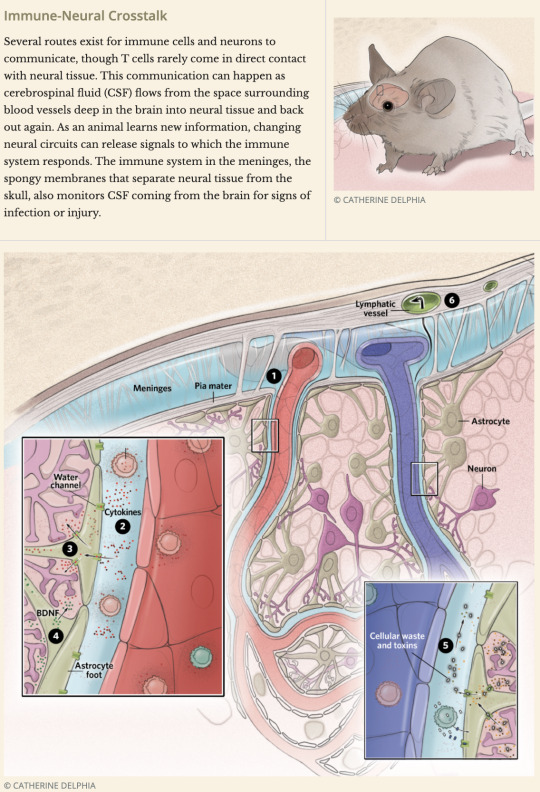
As far back as 2004, studies in rodents suggested that neurons and their support cells release signals that allow the immune system to passively monitor the brain for pathogens, toxins, and debris that might form during learning and memory-making, and that, in response, molecules of the immune system could communicate with neurons to influence learning, memory, and social behavior. Together with research on the brain’s resident immune cells, called microglia, the work overturned a dogma, held since the 1940s, that the brain was “immune privileged,” cut off from the immune system entirely.
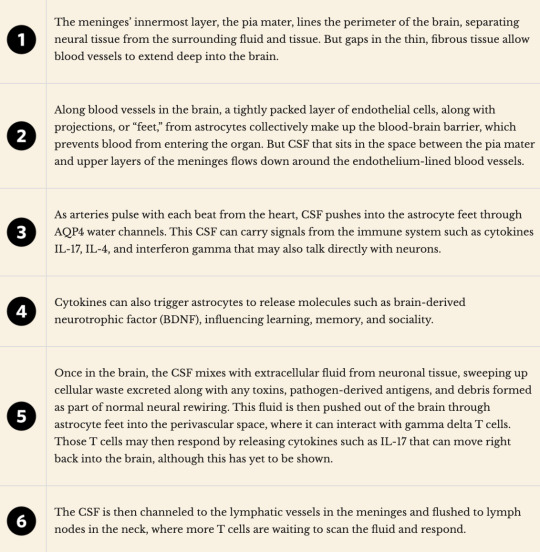
Into the brain: Astrocytes (green) have long, thin extensions called feet that line the blood vessels in the brain. Those feet contain water channels (purple) that allow cerebrospinal fluid, including the molecules within it, to move into the astrocytes and out into the brain, where it can interact directly with neurons. J. ILIFF AND M. NEDERGAARD
Brombacher and others are now starting to identify how communication between the nervous system and the immune system happens. In 2012, molecular imaging revealed that fluorescently labeled proteins could flow through a layer of projections, or “feet,” of neuronal support cells called astrocytes. Astrocytes are star-shaped cells that sit at the border of neural and meningeal tissues and along the blood vessels of the brain; their foot layer is the barrier that separates cerebrospinal fluid (CSF), the watery liquid that envelops the brain and spinal cord, from the neurons of the central nervous system. If those fluorescently labeled molecules could cross the astrocyte layer and move into and out of the brain, so could CSF-based immune-system proteins, which are smaller, scientists figured.
Experiments have also shown that cytokines in the blood can cross the blood-brain barrier (BBB—which, in addition to the wall of astrocyte feet, includes a tight layer of endothelial cells surrounding the brain’s vasculature—and may influence neurons. A third mode of communication, Brombacher notes, is through immune cytokines’ interactions with astrocytes themselves: it seems that the signaling molecules don’t have to penetrate neural tissue at all to influence the brain. Her work shows, for example, how cytokines such as IL-13 spur astrocytes to release brain-derived neurotrophic factor (BDNF) and other proteins that bolster neural development and influence learning and memory.
This line of work has led to rapid developments in neuroimmunology, a growing field of research that focuses on understanding the ways in which the nervous system draws on immune cells during normal function, and how that interaction plays a role in learning, memory, and social behavior, as well as neurological disease. Some researchers even propose that the immune system might be key to treating some forms of impaired cognition.
Cytokines that influence cognition
One of the first teams to make the connection between the immune system and brain function included Jonathan Kipnis, now at the Washington University School of Medicine in St. Louis. In 2004, Kipnis and colleagues showed that mice without adaptive immune cells such as T cells had trouble remembering the location of a submerged platform while they were swimming. A few years later, the group focused in on a T cell cytokine called interleukin-4 (IL-4), which helped mice with functional immune systems form long-term memories about the platform’s location. IL-4 is secreted by T cells in the body that can migrate to the meninges, and was somehow affecting the brain.
Following up on that work, Kipnis’s then-postdoc Anthony Filiano, now an assistant professor of neurosurgery at Duke University, found that mice lacking T cells didn’t socialize with others the way normal mice did. If the immune-deficient mice got an infusion of immune cells at around four weeks of age, they became much more social, mimicking the behaviors of normal mice just a few weeks after their immune supplementation. An analysis of gene expression data collected from both sets of mice revealed that interferon gamma, a cytokine essential for the body’s defense against viral and bacterial pathogens, was associated with sociality.
To see if interferon gamma had a direct effect on the brain, Filiano and his collaborators knocked out the gene for the cytokine receptor in neurons in the mouse prefrontal cortex, a region important for social behavior. This caused mice to spend less time interacting with other mice, a sign that they were feeling less social; the result offered evidence to suggest that interferon gamma from T cells in the meninges was acting directly on the cortical neurons.
Inspired by Kipnis and Filiano’s work, Brombacher and colleagues decided to set up a similar experiment. The team first tested IL-4 knockout mice against wildtype mice in a water maze and successfully replicated Kipnis’s original results—the immunodeficient mice were learning impaired. Then, Brombacher tried the experiment with mice lacking IL-13, which is closely related to IL-4, and got the more dramatic results: “learning was abrogated,” she says. Both cytokines clearly affected learning, but IL-13 appeared to play a more significant role than IL-4, perhaps because of some underlying biochemistry: IL-13 and IL-4 share a receptor on the surface of cells called IL-4 receptor alpha, but IL-13 can also transmit its signal using another receptor. Brombacher is now setting up experiments to remove the cell receptors and see what happens to the mice’s performance in the water maze.
Evidence is also mounting for interleukin 17’s involvement in learning and sociality. In 2016, Gloria Choi of MIT’s McGovern Institute for Brain Research and colleagues linked the cytokine to signs in mouse pups similar to symptoms of autism spectrum disorder (ASD) in humans. Specifically, animals that developed infections while pregnant gave birth to babies that exhibited ASD-like behavioral traits. Interleukin 17 (IL-17) was among the immune signals secreted to help combat the pathogen, the researchers found, and baby mice born to mouse moms with infections had a higher abundance of IL-17 receptors on their brain cells than mice born to uninfected moms. Blocking those IL-17 receptors with drugs during gestation protected pups against the effects of higher maternal IL-17; the pups were born without the signature behavioral issues associated with ASD. Stimulating the release of IL-17 or administering the cytokine directly also appeared to attenuate ASD-like symptoms in young and old adult mice that had been exposed to the high IL-17 levels in utero, suggesting that exposure to elevated maternal IL-17 during development also paradoxically “primes” the immune system for rescue by the cytokine in maturity.
Last year, neuroimmunologist Julie Ribot of the University of Lisbon and her colleagues added to the IL-17 story when they discovered that mice lacking a certain type of T cell or the cytokine had trouble making short-term memories when exploring a Y-shaped maze. This is in contrast to the effects on long-term memory formation that researchers have uncovered for IL-4 and IL-13 in the water maze. The different effects of the interleukins, Ribot says, could have something to do with the fact that the gamma delta T cells that produce IL-17 reside in the meninges, where they could act within seconds during short-term memory formation. T cells that produce IL-4 and IL-13, on the other hand, have to be recruited to the meninges from elsewhere in the body, which takes time, suggesting they support the creation of memories that take longer to form, she notes.
The role of gamma delta T cells and IL-17 in cognition doesn’t end with links to memory and autism, though. The cells and their cytokine may play a role in anxiety, according to Kipnis’s latest experiments. His team recently showed that the release of IL-17 from gamma delta T cells correlates with anxiety-like behavior in mice, and that deleting the IL-17 receptor from glutamatergic neurons in cortical regions involved in threat perception and response reduced anxiety-like behaviors.The major takeaway from each of these IL-17 papers is the same, Kipnis says. “We’re showing that you have a population of immune cells sitting outside the brain that impact neurons inside it.”
In parallel with these studies demonstrating the capacity of cytokines to affect learning and memory, anxiety, and social behavior, researchers are beginning to pull back the curtain on the communication channels that T cells use to talk with neurons. Although it is still unclear exactly how the two systems physically interact, several possibilities have been identified, including direct messages from T cells sent via cytokines interacting with neurons and indirect signals generated through the interaction of cytokines with astrocytes.
Communication lines between immune cells and neurons
Some neuroscientists remain adamant that, with the exception of some drugs, most molecules do not get through the barriers that separate the brain from the rest of the body unless there’s a rupture to the boundary layers intended to cordon off the central nervous system. But research from several groups now challenges this idea. A key study in disproving the long-held assumption that the brain is immune privileged came from the lab of neuroscientist Maiken Nedergaard of the University of Rochester Medical Center. In 2012, she and her colleagues watched fluorescent and radiolabeled tracers flow from the CSF into the brains of anesthetized mice.
Specifically, Nedergaard’s team recorded the movement of the tracers into and out of the animals’ cerebral cortex, the brain’s outer layer of folded gray matter, which is essential for consciousness, attention, and making memories. The researchers learned that CSF carrying cytokines and other signaling molecules flows from the meninges into the space surrounding the brain’s vasculature. As the arteries pulse with each beat of an animal’s heart, the blood vessels expand, and the CSF is pushed through water channels in the astrocyte feet and then into the brain.The reverse flow also takes place: CSF that has entered the brain and mixed with the extracellular, or interstitial, fluid—and that now carries waste proteins ready for clearance—is pressed back through astrocytes into the space surrounding the blood vessels. “Maiken showed this very, very elegantly,” Kipnis says. It completely overthrew the dogma that the brain is immune privileged, he says.
Earlier this year, Andrew Yang of Stanford University and colleagues extended this finding to specifically show that cytokines released from T cells in the blood can also reach the brains of mice. The researchers extracted blood from the animals, separated out plasma proteins, labeled them with a fluorescent tag, then injected them back into the bloodstreams of the mice they came from. In healthy young adult mice, lots of the fluorescently tagged proteins crossed the BBB to enter the interstitial fluid in the brain. “This finding suggests that a wide variety of neural functions . . . could be modulated by systemic protein signals,” Roeben Munji and Richard Daneman of the University of California, San Diego, wrote in a commentary accompanying Yang’s study.
Cytokines in the meninges or possibly even in the blood might not have to enter the brain at all to affect the central nervous system, according to Brombacher’s studies. IL-13 and other cell signaling molecules in the CSF or blood could interact with astrocytes at the BBB or at the perimeter of the brain. In cultured astrocytes, treatment with IL-13 spurred the production of BDNF and triggered the production of glial fibrillary acidic protein (GFAP), an indication that neural connections are undergoing rewiring. Ribot’s study on IL-17 also showed that the cytokine could spur mice’s astrocytes to release BDNF into the brain. Both BDNF and GFAP, which boost synaptic rewiring, are associated with learning and memory.
Communication between the immune and nervous systems can also happen in the reverse direction, with signals from the brain reaching T cells of the spongy, membranous meninges and of the rest of the body. Until a few years ago, researchers agreed that the brain lacked a drainage, or lymphatic, system to clear away its waste and to transport immune cells. But to Kipnis, it just didn’t make sense that one of the most important organs in the body would not have that kind of plumbing. So he and his colleagues went looking for it, and in 2015, they found it—mice’s brains did, in fact, have lymphatic vessels that shipped waste and T cells from the meninges to deep cervical lymph nodes in the animals’ necks.“These structures are bona fide vessels—they express all the same markers as lymphatic vessels in every other tissue,” he told The Scientist at the time.
In mice, T cells residing in the meninges scan the CSF for the cellular waste generated as neuronal circuits undergo changes, whether in response to learning and memory formation or in the case of dysfunction. Then, T cells in the lymph nodes get a chance to check the CSF for potential threats such as pathogens, he says. Tracking that lymphatic system in people’s brains is much harder, but Kipnis says there’s some evidence that what scientists are finding in rodents does translate to human biology. In 2017, he and collaborators at the National Institute of Neurological Disorders and Stroke used MRI to noninvasively confirm the existence of meningeal lymphatic vessels in humans and nonhuman primates.
Understanding immune cell–neuron crosstalk—both the way T cells respond to what’s in CSF coming from the central nervous system and how they send signals into the brain—could be important for understanding neurological disorders, such as Alzheimer’s disease, autism, schizophrenia, and even the cognitive decline associated with aging. “With many of these neurological disorders, there’s been reports that there’s some kind of dysregulation of the immune system,” Filiano says. Identifying faulty signals from neurons in the fluid leaving the brain could lead to diagnostic tools for neurological disorders, he notes. And given that CSF can carry cytokines and other proteins to neurons, Kipnis says he suspects that “putting [immune-based] therapies into that fluid will probably be a very, very efficient route for treating patients.”
Treating brain disorders with cytokines
Developing molecules to infuse into the blood or CSF to communicate with the brain requires a better understanding of how cytokines affect neurons, astrocytes, and micro-glia over the course of a lifetime. Interferon gamma, for example, appears to have two faces when it comes to influencing neuronal circuits. In Kipnis’s studies of young mice, the cytokine was essential for the animals to be social. But an analysis of the brains of old mice shows that the same cytokine might be detrimental to making new neurons in aged mice. Giving the old mice an antibody that neutralizes the immune cytokine restored neurogenesis in the animals’ brains, a team of researchers reported in 2019.
A similar tactic might provide a novel way to treat various neuropsychiatric disorders such as schizophrenia. Analyses of immune cells in the blood of schizophrenia patients show that these individuals have higher levels of a variety of cytokines, including IL-13 and interferon gamma, than healthy individuals do. People with schizophrenia treated with anti-inflammatory and antipsychotic drugs also tend to have fewer cognitive problems than individuals treated with only antipsychotics, hinting that reducing cytokine levels could improve patients’ symptoms. While the neuronal changes that cause schizophrenia are far from clear, studies suggest that when certain neurons produce lower-than-expected levels of dopamine, they alert T cells to a problem, and the T cells respond by releasing cytokines that prompt disease-related deficits in memory, learning, social behavior, and resilience to stress.
Filiano and Kipnis have found evidence that a similar approach might work for helping individuals with autism. In experiments with mice lacking T cells, the researchers found that the animals not only had social deficits but also showed hyperactivity in neural circuits that often have abnormal activity in the brains of people with autism. Not only did social behavior improve when the team infused the mice with immune cells, but the animals’ abnormal neural activity subsided too. Meticulously tweaking the immune system might reverse the cognitive and social deficits of the disorder, the experiments suggest.
For now, the results leave Filiano wanting to know more. He explains, “We’re really interested in how these immune cells talk to the brain, how these signals get from the immune cells to these neural circuits, how that communication happens in health and disease.”


104 notes
·
View notes
Text
HSV encephalitis is a devastating infection of the central nervous system. Even with early administration of therapy after onset of disease, nearly two-thirds of survivors will have significant neurologic deficits [4]. For this reason, empiric therapy with IV acyclovir (10 mg/kg IV every 8 hours) should be initiated as soon as the diagnosis is considered. We do not recommend oral antiviral therapy (eg, valacyclovir) for the treatment of HSV encephalitis.
IV acyclovir was shown to be the treatment of choice for the reduction of mortality and morbidity from HSV encephalitis in the mid-1980s. A series of trials compared its efficacy with vidarabine, which had earlier been shown to be better than placebo [68,69]:
●Patients who underwent brain biopsy for presumptive HSV encephalitis were randomly assigned to treatment with either vidarabine or acyclovir for ten days. One-third of the patients had biopsy-proven disease. Mortality was significantly reduced in the acyclovir-treated patients (28 percent versus 54 percent) [68].
●In another study, 127 patients with suspected HSV encephalitis were randomized to a 10-day course of acyclovir versus vidarabine [70]. The diagnosis of HSV encephalitis was verified by brain biopsy and/or antibody responses in serum and CSF in 53 patients. Mortality was significantly decreased in the acyclovir group compared to the vidarabine group (19 percent versus 50 percent).
●In both of the above studies, six-month assessments confirmed that functional status was significantly better in the acyclovir-treated patients compared to those assigned to the vidarabine arm [68,70].
Because acyclovir is only effective in halting viral replication, it should be given early, to prevent extensive replication and subsequent CNS damage. Early treatment is defined as any one of the following [71]:
●Before loss of consciousness
●Within 24 hours of the onset of symptoms
●Glasgow Coma Scale score of 9 to 15
Early, aggressive antiviral therapy can prevent mortality and limit the severity of chronic postencephalitic behavioral and cognitive impairments [33]. Suspected cases of HSV encephalitis should receive acyclovir (10 mg/kg IV every 8 hours) with dose adjustment for renal insufficiency. The mechanism of action and toxicity profile of acyclovir are discussed in detail separately. (See "Acyclovir: An overview" and "Treatment and prevention of herpes simplex virus type 1 in immunocompetent adolescents and adults".)
Acyclovir must be infused slowly and with a fluid bolus to prevent crystalluria and renal failure [2]. Neurologic toxicity has only been observed at extremely high doses (>10 mg/kg every 8 hours) or in cases of renal failure without dose adjustment [2]. (See "Acyclovir: An overview".)
Although the original trials cited above used only 10 days of acyclovir, the duration of treatment of HSV encephalitis in immunocompetent patients should be 14 to 21 days since shorter time periods have been associated with occasional relapse with acyclovir-sensitive HSV [52,72,73]. This phenomenon has been mainly observed in children [72,73]. The low toxicity profile of the drug makes longer duration of therapy possible.
One study evaluated the pharmacokinetics of orally administered valacyclovir (1 g orally three times daily for 21 days) in four patients with HSV encephalitis [74]. The patients achieved and maintained therapeutic concentrations of valacyclovir in the CSF for the duration of therapy, although the CSF concentrations dropped over time, likely reflecting a reduction in blood-brain barrier permeability with healing of the infection. Further study is necessary before valacyclovir can be recommended for HSV encephalitis.
Shortages of intravenous (IV) acyclovir have occurred. If IV acyclovir is not available, alternative agents must be used. Specific recommendations are presented separately. (See "Acyclovir: An overview", section on 'If there is an acyclovir shortage'.)
DISCONTINUATION OF THERAPY BASED ON PCR RESULTSIn patients with a low prior probability of HSV encephalitis (normal neuroimaging, <5 cells/mm2 in CSF, normal mental status), a negative CSF HSV PCR result reduces the likelihood of disease to <1 percent [8]. Antiviral therapy may thus be discontinued if a negative CSF HSV PCR result is obtained after 72 hours following onset of neurological signs and symptoms.
In contrast, in patients with a high prior probability of HSV encephalitis (suggestive neuroimaging findings, CSF pleocytosis, positive EEG findings, or seizures), a negative PCR result reduces the disease likelihood to approximately 5 percent. In addition, clinicians must consider alternative reasons for a false-negative CSF PCR result, including early testing after the onset of symptoms, antiviral therapy, or presence of PCR inhibitors (eg, hemoglobin degradation products in bloody CSF).
SUMMARY AND RECOMMENDATIONS
Herpes encephalitis is the most common cause of fatal sporadic encephalitis in the United States and involves all age groups. In nearly all cases of herpes encephalitis beyond the neonatal period, the etiologic agent is herpes simplex virus type 1 (HSV-1). In neonates, herpes encephalitis may be caused by either HSV-1 or HSV-2. The clinical syndrome is often characterized by the rapid onset of fever, headache, seizures, focal neurologic signs, and impaired consciousness.
Diagnosis
●We recommend lumbar puncture for cerebrospinal fluid analysis and polymerase chain reaction (PCR) testing for HSV in any patient with encephalitis. (See 'Diagnosis' above.)
●We also recommend brain magnetic resonance imaging (MRI) to assess signs of temporal lobe involvement, which would support the diagnosis. Absence of this finding does not alter decisions regarding empiric therapy. Brain MRI would also eliminate other alternative causes of mental status changes, such as brain abscess. (See 'Imaging studies' above.)
●We recommend brain biopsy if the patient clinically deteriorates on appropriate therapy and PCR testing is negative for HSV. (See 'Brain biopsy' above.)
Treatment
●We recommend that patients with suspected HSV encephalitis receive empiric therapy, since delays of treatment have led to significant neurologic sequelae (Grade 1B). (See 'Treatment' above.)
●We recommend the use of acyclovir (10 mg/kg IV every 8 hours) for empiric therapy (Grade 1A). Treatment duration is 14 to 21 days. (See 'Treatment' above.)
Initial Assessment and Management of Acute Stroke:
SUMMARY AND RECOMMENDATIONS
●The main goals in the initial phase of acute stroke management are to ensure medical stability, to quickly reverse conditions that are contributing to the patient's problem, to determine if patients with acute ischemic stroke are candidates for reperfusion therapy, and to begin to uncover the pathophysiologic basis of the neurologic symptoms. (See 'Initial assessment' above.)
●Important aspects of acute stroke evaluation and management include the following:
•Assessing vital signs and ensuring stabilization of airway, breathing, and circulation. (See 'Airway, breathing and circulation' above.)
•Obtaining a rapid but accurate history and examination to help distinguish stroke mimics and other disorders in the differential diagnosis (table 1) of acute stroke. (See 'History and physical' above and 'Neurologic evaluation' above.)
•Obtaining urgent brain imaging (with computed tomography [CT] or magnetic resonance imaging [MRI]), neurovascular imaging (with CT angiography or magnetic resonance angiography [MRA]) and other important laboratory studies, including cardiac monitoring during the first 24 hours after the onset of ischemic stroke. (See 'Immediate laboratory studies' above and 'Neuroimaging' above and 'Cardiac studies' above.)
•Managing volume depletion and electrolyte disturbances. (See 'Fluids' above.)
•Checking serum glucose. Low serum glucose (<60 mg/dL [3.3 mmol/L]) should be corrected rapidly. It is reasonable to treat hyperglycemia if the glucose level is >180 mg/dL (>10 mmol/L) with a goal of keeping serum glucose levels within a range of 140 to 180 mg/dL (7.8 to 10 mmol/L).
•Assessing swallowing and preventing aspiration. (See 'Swallowing assessment' above and "Complications of stroke: An overview", section on 'Dysphagia'.)
•Optimizing head of bed position. For patients with intracerebral hemorrhage, subarachnoid hemorrhage, or ischemic stroke who are at risk for elevated intracranial pressure, aspiration, cardiopulmonary decompensation, or oxygen desaturation, we recommend keeping the head in neutral alignment with the body and elevating the head of the bed to 30 degrees (Grade 1C). For patients with stroke who are not at high risk for these complications, we suggest keeping the head of the bed in the position that is most comfortable. (See 'Head and body position' above.)
•Evaluating and treating the source of fever, if present; for patients with acute stroke, we suggest maintaining normothermia for at least the first several days after an acute stroke (Grade 2C). (See 'Fever' above.)
●The management of blood pressure in acute stroke depends on the type of stroke. (See 'Blood pressure management' above.)
•For patients with acute ischemic stroke who will receive thrombolytic therapy, antihypertensive treatment is recommended so that systolic blood pressure is ≤185 mmHg and diastolic blood pressure is ≤110 mmHg prior to treatment and <180/105 mmHg for the first 24 hours after treatment (table 6). This issue is discussed in detail separately. (See "Intravenous thrombolytic therapy for acute ischemic stroke: Therapeutic use", section on 'Management of blood pressure'.)
•For patients with acute ischemic stroke who are not treated with thrombolytic therapy, we suggest treating high blood pressure only if the hypertension is extreme (systolic blood pressure >220 mmHg or diastolic blood pressure >120 mmHg), or if the patient has another clear indication (active ischemic coronary disease, heart failure, aortic dissection, hypertensive encephalopathy, or pre-eclampsia/eclampsia) (Grade 2C). When treatment is indicated, we suggest cautious lowering of blood pressure by approximately 15 percent during the first 24 hours after stroke onset (Grade 2C). (See 'Blood pressure goals in ischemic stroke' above.)
•In both intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH), the approach to blood pressure lowering must account for the potential benefits (eg, reducing further bleeding) and risks (eg, reducing cerebral perfusion). Recommendations for blood pressure management in acute ICH and SAH are discussed in detail separately. (See 'Blood pressure in acute hemorrhagic stroke' above and "Spontaneous intracerebral hemorrhage: Treatment and prognosis", section on 'Blood pressure management' and "Aneurysmal subarachnoid hemorrhage: Treatment and prognosis", section on 'Blood pressure control'.)
●For eligible patients (table 2) with acute ischemic stroke, intravenous alteplase therapy is first-line therapy, provided that treatment is initiated within 4.5 hours of clearly defined symptom onset. Patients with acute ischemic stroke due to a proximal large artery occlusion who can be treated within 24 hours of time last known to be at neurologic baseline should be evaluated for treatment with mechanical thrombectomy (algorithm 1). The eligibility criteria and utility of thrombolytic therapy, mechanical thrombectomy, and the treatment of patients not eligible for thrombolysis are discussed separately. (See "Approach to reperfusion therapy for acute ischemic stroke" and "Antithrombotic treatment of acute ischemic stroke and transient ischemic attack".)
●In addition to reperfusion therapy, a number of interventions for ischemic stroke are associated with either reduced disability, complications, or stroke recurrence, including (see 'Acute therapy' above):
•Antithrombotic therapy with aspirin initiated within 48 hours of stroke onset. (See "Antithrombotic treatment of acute ischemic stroke and transient ischemic attack", section on 'Aspirin'.)
•Prophylaxis for deep venous thrombosis and pulmonary embolism. (See "Prevention and treatment of venous thromboembolism in patients with acute stroke", section on 'Approach to VTE prevention'.)
•For patients with acute ischemic stroke, we suggest starting or continuing statin treatment as soon as oral medications can be used safely (Grade 2C). (See 'Ischemic stroke management' above.)
7 notes
·
View notes
Text
BED Disorder(sleep disorder)
If you’re referring to a disorder related to beds or sleep, it’s important to note that I am an AI language model and not a medical professional. However, I can provide you with some general information.
If you’re having difficulties with sleep or experiencing disruptions in your sleep patterns, it’s possible that you may be dealing with a sleep disorder. Sleep disorders can affect the quality,…

View On WordPress
#anatomy#animation#basal ganglia#blood-brain barrier#brain#cerebellar#cerebellum#cerebral#cns#crest#csf#dopamine#embryology#exam#explain#HEALTH#htownrush#hypothalamus#infection#kaplan#khan#limbic#local#medicine#medulla#motor#nervous system#neural#neurology#neuron
0 notes
Text
Microanatomy of the Nervous System, pt. 2
Glial Cells
- Greek: “glue”
- Support, nurture, and protect neurons
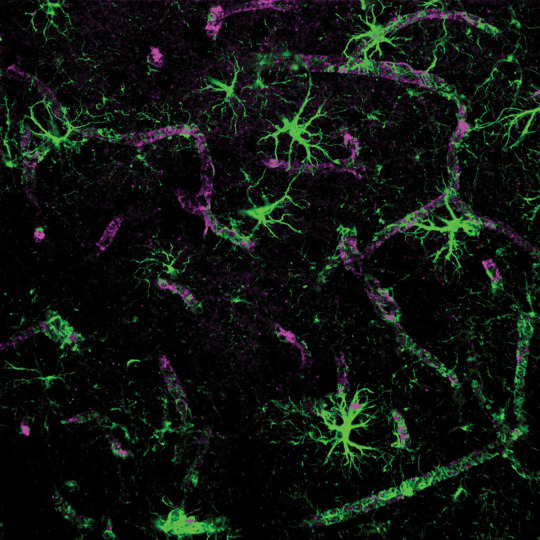
Ependymal Cells
- Small, ovoid; found in the walls of the ventricles
- Make and secrete cerebrospinal fluid (CSF)

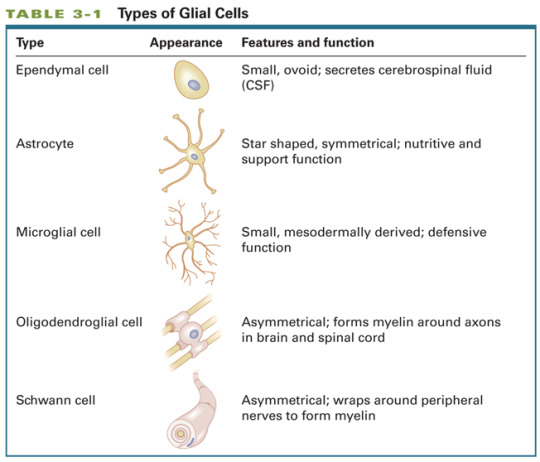
Microglial Cells
- Originate in the blood as offshoot of immune system
- Can change their shape
- Provide immune defense
- Phagocytosis: scavenging debris (e.g. dead cells)
- Aid in cell repair
Astrocytes
- Greek: astron “star” + cyte “cell”
- Star shaped, symmetrical
- Structural support for neurons, scar tissue formation
- Regulate transport of substances between neurons and capillaries (blood-brain barrier)
Oligodendroglial Cells
- AKA oligodendrocytes
- Glial cells in the central nervous system that myelinate axons
- Myelin: glial coating that surrounds axons in the central and peripheral nervous systems
Loss of Myelin in Multiple Sclerosis
- Symptoms include:
muscle weakness
trouble with coordination
trouble with sensation (e.g. double vision)


Schwann Cells
- Glial cells in the peripheral nervous system that myelinate axons

Cellular Organization of the Nervous Tissue
Blood-Brain Barrier
- Blood vessels are a tissue comprising individual vascular cells arranged in series to form long hollow tubes.
- The blood-brain barrier is the tight junctions between the cells of blood vessels in the brain that prevent the passage of large molecules into the brain.
- A few brain regions have a reduced or absent BBB:
pineal gland (in the thalamus)
pituitary gland (in the hypothalamus)
area postrema (in the medulla)

1 note
·
View note
Link
1) Maderna & Phiser innoculations are not "Vaccines" and are also manufactured "gain of function" genetic material. Phiser admits that COVID mRNA Vaccine is -Not A Vaccine- at all!! Its "Chemotherapy" and Gene Therapy. It is unlawful under the FTC Act, 15 U.S.C. 41 et seq., to advertise that a product or service can prevent, treat, or cure human disease unless you possess competent and reliable scientific evidence, including, when appropriate, well-controlled human clinical studies. https://banned.video/watch?id=60076fda8c03b74ce0e2f6f5
Ebola Virus and Species Patent owned by the U.S. Department of Health. November 12th 2015 Chapel Hill NC gain of function research on bats stirs debate over risky research. Merck and Astrazenica abandoned development and testing of coronavirus vaccines. March 14th 2016 SARS-like WIV1-CoV poised for human emergence | PNAS
2) Two types of "Vaccines" described at the National Institute of Health 1) makes your own cells manufacturer the viral genetic material 2) mRNA, recombinant DNA, by definition, physically changes your DNA. Safety and efficacy studies at the NIH or by the manufacturer are only looking for "Immunoresponses, NOT for Viruses; despite the vaccine companies writing their own studies and fast-tracked. "They use a safe virus to deliver the genetic code (DNA) of the SARS-CoV-2 spike protein to human cells so that the cells can make the protein. JNJ-7843672 uses a human adenovirus to deliver the code for the SARS-CoV-2 spike protein." https://niaid.nih.gov/diseases-conditions/covid-19-vaccine-faq.
In the same fashion, Koch Postulates to "Isolate" a "Virus" or duplicated "genetic material" for Covid has only been done with Monkeys, with anal swabs, and only found "virus particles". https://ncbi.nlm.nih.gov/pmc/articles/PMC7095368/
3) Covid-19 AI Scenario was predicted by Tesla Leaks as the most likely response to the domination of Tesla & Nikola Tesla; at The Rise of the Jedi Podcast on December 22nd-December 26th 2019 at 1AM Rise of the Jedi Podcast
4) The Great Reset and Plandemic was pre-planned; as their New World Order was at risk of collapse - Joe Biden, January 2016
5) Plandemic was pre-planned at the 2019 World Economic Forum; under the title Event 201 Scenario by Johns Hopkins Center for Health Security in collaboration with the World Economic Forum and the Bill & Melinda Gates
6) Just as their old order of oil, gas, propane, coal and tree buring failed; as their prices collapsed and renewable energy reached "negative prices"; they shut down Tesla Factories in the U.S and Shanghai
7) Hosptitals don't provide or use the words "Cures" to anything, more or less anything for a cold virus, they use the word "Treat"
8) The 2002-2004 SARS outbreak sourced "hospital staff" as the originators of SARS, 500,000 yearly cases of sepsis and other infectious diseases. March 2003 report where 200 hospital staff get SARS and spread it to patients.
9) All real medical cures from Ozone, to UV, to Plasma, to filtering your blood with Electric Fields; are banned by hospitals; while also not covered by Insurance
10) WHO lies about UV-C light and Sunlight; claiming UV-C does-not kill Coronavirus. FDA: UV-C destroys SARS-Coronavirus. The destruction of the protein shell ultimately leads to inactivation of the virus. UV-C is safe for human skin
11) EPA banned peer review of the first study by Trump team on UV-C lights with resperators on humans, citing alleged danger.
12) Governments and Hospitals banned Primatene Mist in 2011 to breath, and instead they use incubators to kill 90% of you. Just 1 mask reduces O2 intake by 20% and causes carbon dioxide poisoning.
13) Mainstream Media ignores real cures of virus and disease. AMA bans electric healing in the early 1900's calling it "quackery" clack clack clack, and Pseudo-Scientific. Electricity Greatest of All Doctors - Nikola Tesla to the IEEE in 1899
14) No authentic pictures exist of Coronavirus; without a Scanning Electron Microscope (SEM) or TEM Microscope and Photoshop. SARS-2 Photoshop Cartoon
15) Covid from Bat guano in China is only #blamed and never has been proven in any way. Chinese Officials Blame US Army for Coronavirus; citing "this is the Black Swan event the Globalists have been waiting for"
16) No #causation ever proven between any particular virus and a particular disease; not even HIV & AIDS; citing "The correlation between antibody to HIV and AIDS does not prove causation" - NIH
17) Hospitals are empty; emergency tents are empty; have been already torn down. U.S. Field Hospitals Stand Down, Most Without Treating Any Covid Patients - PBS
18) Flu disappeared in 2020 all counted as Covid cases and deaths
19) Swab tests, Anal probes and other test look for antibodies or reactions, not for a particular virus - NIH. Tanzania President shows how Goats show false-positives to Covid tests and "has technical errors". Austrian politician presents a False-positive test using Coca-Cola. Coca Cola and Pepsi join the hoax and promote using thier plastic bottles for covid testing.
20) mRNA therapeutics, by definition, changes your DNA. This mRNA "Vaccine" is from the lung tissue of an aborted child from 1966.
21) PCR test copies genetic material; 40X with errors each replication, looks for only "markers", to become anything they want; and not for diagnosing any illness or disease. However, it must be noted that detection of microbes in the CSF does not always indicate a CNS infection, since impairment of the blood-brain barrier may permit transit of microbes. - NIH
22) Temperature readings of 98.8, is not an accurate gague of a disease. Testing machines are also faulty. The human body is not uniform in its temperature; thus, measurements at different locations can yield varying results. The most accurate way to measure temperature is to take a rectal reading. See China Anal Probe test for Covid.
23) Immunologic Adjuvant "Vaccines" never have been and never will be a cure for anything; other than a poison to solicit a reaction, to reduce or increase T-Cells.
24) All Vaccines contain unregulated nano-particles of protein snippets of #whatchamacallit; nano-organic mercury; nano aluminum, and other so-called adjuvents. The #1 side effect of all mercury derivatives in all innoculations is "brain damage" - NIH
25) Vaccines, by definition, are designed create a cytokine storm of rogue antibodies in which the innate immune system causes an uncontrolled and excessive release of pro-inflammatory signaling molecules called cytokines. Cytokine Storms May Be Fueling Some COVID Deaths - WebMD
26) Trump, Jones, Fauci & NIH claim Hydro-cloro-quine (Hydrogenated Chlorine (Bleech) + AmphetamIne (Ine)) + stinky Sulfer is a "cure" for cold virus's. The FDA & NIH and the larger scientific community have warned against the use of the Hydroxychloroquine to treat COVID-19, citing ineffectiveness, lack of benefits and risk of heart rhythm problems. The New England Journal of Medicine and The Lancet could not verify the data on which the results depended. It's not a Malaria (Hoax) cure either. It simply reduces your T-cells by 40%, reducing the "cases" by 40%, Malaria still ends up killing the patient. Therapies to decrease CD8 immune activation
27) The holes in a paper mask are 1000X bigger than genetic material at .02-.20 Microns. HEPA 2.5 is 10-100X bigger than a Virus. Masks only prevent large particles, not nano-particles. - NIH. To cover for their original lie that "just wear the mask" - Joe Biden; Experts are now claiming you need to wear 2 or 3 masks.
28) Masks in many ways, by touching your ass and face and then mask, foster disease and infection, it doesn't provent them. Bacterial Pneumonia (spread by the hospital staff) Caused Most Deaths in 1918 Influenza. - NIH & Fouci, 2008
29) Masks suffocate and train to suffocate children, elderly, asthmatics and others. Wearing a mask can be dangerous or pose a suffocation hazard
30) Join the Dark Side, We have Masks! Masks are worn by Darth Vader, Storm Troopers, Empire's minions and Walmart employees
31) Psychological effects of mask wearing is astouonding and innumerable. Evidence suggests that there may be consequential psychological impacts of mask wearing on the basic psychological needs of competence, autonomy, and relatedness - NIH
32) Dead Virus's are not Transmittable, despit what you've been told. No one you know died of Coronavirus, that didn't have 5+ pre-existing conditions. Death Counts are considered "Provisional" - CDC. 94% of U.S. COVID-19 deaths had numerous contributing health problems - CDC. But, the fake news does claim Lions at zoo's can get Coronavirus; while the CDC admits that Some coronaviruses, such as canine and feline coronaviruses, infect only animals and do not infect people.
33) There is no newspaper death notices, funerals etc. for any of the alleged deaths. Since there is no funerals, instead Biden to hold national memorial service for US Covid victims.
34) Children have less than a .2% death rate, even with phoney death numbers. Few US children are dying from covid-19 - The Washington Post.
35) There was no dead people in body bags in NY as Trump suggested. He is lying to prop-up the Hoax. Trump Describes Seeing Bodies in Body Bags At NYC
36) There is less overall deaths in 2020 in the U.S. than there was in 2019; when removing the increase in suicide, drug overdoses, poverty; the reduction in traffic deaths and un-registered illegals being counted as deaths.
37) All the politicians and are actors that said they had Covid, had no side effects whatsoever; Larry King did not die of Covid. - Shawn King. Boris Johnson didn't even clear his throat once in his Live Interview.
38) Lockdowns have officially made 40 Million people homeless; without the Presidential Directive banning evictions. USAToday. Lockdowns made 120 Million Jobless.
39) Lockdowns cause people to congregate at home, the opposite of the reason for a lockdown
.666) The 6' X 6' X 6' social distancing is, you've got it, 666, or 12' X 12' X 12' is, you've got it 3 6's, or 666.
40) The species name of Covid-19 is (HEL1) spoken "hell one" helical virus; categorized as a family of cold virus by the U.S. National Library of Medicine and in the 1989 AMA Encyclopedia. Coronavirus nsp13 SF1 Helicase (HEL1) - NIH
41) Psychological effects of social distancing, no hugs, hand shakes, kissing or sex; is astounding and innumerable. No sources needed.
42) Rockefeller (Oil) Foundation & US DOS wrote a report on Operation Lockstep; for public policing policy called #lockstep; a prison term. The US Department of State is policing the population policy 1999, NIH. - Rockefeller Foundation is the founder and funder of the World Health Organization.
43) U.N. is threatening a global food pandemic of Apocolyptic proportions
44) 10 Million people have already starved to death because of lockdowns. 132 Million into Hunger - UN
45) 50%-80% of businesses in the U.S. could go out of business, leaving just Taco Bell. Coronavirus Bankruptcy Tracker
46) HIPAA medical privacy laws and dozens of others are cancelled by directives & orders. Trump suspends HIPAA penalties with national emergency declaration
47) $6.66T bailouts and free money to the people behind all these scams. U.S printed $6.66T in phoney currency in 2020.
48) Bill Gates said he will make 200X his investment into his operating system Vaccines
49) First you needed a Vaccine, now multiple Vaccines, next you'll need 100; and still have to wear 3 masks, social distance and a Tattoo of phosphorescent nano-dots. There are currently more than 50 COVID-19 vaccine candidates.
50) CNN admits that you will need a Certificate of Vaccination 2019 (Covid-19) passport to leave your house
51) CNN admits the Contact Tracing APP will ensnare anyone you've been near; to be forceaby quarrantined. Contact tracing will be conducted for close contacts (any individual within 6 feet of an infected person for a total of 15 minutes or more) - CDC. Could your child or pregnant wife be a victim of medical kidnapping?
52) Masks, Contact tracing and Temperature readings are all a violation of HIPAA medical and other privacy laws.
53) Vaccine Mandates or you will not be able to have a job, get government funds or go outside your house without taking Bill Gate's OS vaccines.
54) Citizens around the world have been threatened by merchants, other citizens and police with death from day 1, if they don't do as their told. Police make 6500 arrests in the U.K. for breaking mask and distancing guidelines.
55) Once mandatory by December 9, 2020, national guard, police and military will use the Martial Law to National Guard will administer the vaccines force vaccinate you and your family. - Military Times
56) Local police are now setting up Mask Squads to round up people not obeying their rules (or whatever else they say)
57) Banks are now closing customer bank accounts and destroying your business if you don't wear a mask, or anything else they say
58) False-Flag operations are now in effect, to blame truth, freedom and the American Way and/or God. Oregon Senator correctly describes the Capitol "attack" as a False-Flag Operation to treat American's as Terrorists.
59) Mainstream news is now lying about every event that happens on the ground, making claims of fact we all know are false; such as proven voter fraud and the phoney attack on the Capitol. The company Scytl Secure Electronic Voting, S.A, (also stylized SCYTL) is a Spanish provider of electronic voting systems and election technology; that counts the votes for the U.S., then returns the results, It has board members from the Rockefellers, Rothchilds, JP Morgan Chase, Goldman Sachs, Russia & Others.
60) Covid was a cover for the facist communists to steal the election using dozens of fraudulent vote counting methods. Dominion Voting Systems are a complete fraud. The data is always accessable by the manufacturer.
61) All Presidential Directives, Orders & Mandates are Unconstitutional; the Constitution and Bill of Rights has been CANCELLED! Despite this lack of constitutional authority,...
62) "Rules" are not "Laws"; in the dictionary. To make you think they are the same, they use the term Rule of Law to make it so. A Rule, of a Law, means that government beurocrats can make-up 1000 rules, to supposedly abide by a particular law.
63) Governments are now making Sex Rules where you must not have sex, but masterbate in front of your partner, social distanced and be wearing 3 masks
64) Homeland Security is rolling out Social Distancing Shock Collars for the Slaves as a "cure" for Coronavirus. Social Distancing is a mis-nomer and worthless. Nano-particles float in the air like smoke for at least 45 minutes. Nano-particles from just speech float for 8 minutes.
((Predictive Programming in Movies: In the 1991 movie "Wedlock"; if you venture too far from your controllers, the shock bracelet around your neck; blows your head off)) https://en.wikipedia.org/wiki/Wedlock_(film)
65) Medicare pays $13K to $300K to list any case or death as a Covid-19 death
66) Weapons confiscation before the government agents and NWO stooges come to kill you. Pelosi wants security money for Stormtrooper Mask and Body Armor to face the "enemy within" House of Representatives
#covid#hoax#mask#mandates#lockdowns#business#vaccine#sideeffects#medical#health#who#nih#cdc#billgates#fauci#biden#warpspeed
5 notes
·
View notes
Text
Nanoparticles Deliver Treatment Directly to Tumors of Deadly Brain Cancer - Technology Org
New Post has been published on https://thedigitalinsider.com/nanoparticles-deliver-treatment-directly-to-tumors-of-deadly-brain-cancer-technology-org/
Nanoparticles Deliver Treatment Directly to Tumors of Deadly Brain Cancer - Technology Org
Using nanoparticles administered directly into the cerebrospinal fluid (CSF), a research team has developed a treatment that may overcome significant challenges in treating a particularly deadly brain cancer.
The researchers, led by professors Mark Saltzman and Ranjit Bindra, administered to mice with medulloblastoma a treatment with specially designed drug-carrying nanoparticles. The study, published in Science Translational Medicine, showed that mice who received this treatment lived significantly longer than mice in the control group.
Medulloblastoma, a brain cancer that predominantly affects children, often begins with a tumor deep inside the brain. The cancer is prone to spread along two protective membranes known as the leptomeninges throughout the central nervous system, particularly the surface of the brain and the CSF. Leptomeningeal spread is seen in a number of primary brain tumors, as well as in brain metastases from solid tumors in the breast, lung, and other places. Because there are no anatomic barriers in the CSF to prevent further growth, these cancers can spread rapidly.
Targeting tumors in the CSF has proven difficult, in part because the fluid rapidly cycles through the central nervous system about four times a day in humans, typically flushing away anti-tumor drugs before they’ve had a chance to accumulate and have any effect.
“It’s like a waterfall system, with a fast, rapid fluid flow,” said Minsoo Khang, lead author of the study and a former graduate student in Saltzman’s lab.
To overcome this obstacle, the research team fabricated nanoparticles that adhere to tumors. Designed in Saltzman’s lab, these nanoparticles are made with degradable polymers that slowly release a DNA repair inhibitor, talazoparib, which is FDA-approved and currently used in the clinic for a number of cancers. The drug is one of a relatively new class of cancer drugs known as PARP inhibitors, which block an enzyme that helps repair DNA. Without the ability to repair their DNA, tumor cells are more likely to die.
The nanoparticle treatment is injected intrathecally – that is, it’s delivered directly between the leptomeninges protecting the CSF. Over a period of weeks, the researchers detected the presence of the nanoparticles in the CSF for as long as 21 days after a single dosing.
“We were very excited to have found a medium that has long-term retention in this fluid space, which is otherwise challenging,” Khang said.
Treating brain cancers in general is challenging since few treatments can penetrate the blood-brain barrier, a natural defense system that can block potentially helpful drugs. The research team’s method could offer a solution.
“There’s been very little work on intrathecal delivery of nanoparticles, so we’re very excited because it can allow us to go after the leptomeningeal spread of disease from brain metastases,” said Bindra, the Harvey and Kate Cushing Professor of Therapeutic Radiology and Professor of Pathology. “This has really opened up an entirely new way to treat these patients, although much more work needs to be done.”
Using the nanoparticles to target the tumors allowed the researchers to use the drug talazoparib, which has proven to be effective in a number of solid tumors outside of the brain. Because the drug has limited to no penetration of the central nervous system, however, an orally delivered dose would have limited efficacy against tumors with leptomeningeal spread.
“By encapsulating it in a nanoparticle and directly injecting it into the CSF, we now get very high exposure in just that area,” said Saltzman, the Goizueta Foundation Professor of Biomedical Engineering, Chemical & Environmental Engineering & Physiology, and a member of Yale Cancer Center.
Delivering the drug intrathecally also avoids injecting it directly into the brain, a technique referred to as convection-enhanced delivery. This very challenging procedure can be performed only a few times a year. Intrathecal injections, in contrast, are much less invasive and can be given without a hospital stay.
“This is huge for us, because now we can do multiple nanoparticle treatments over time,” Bindra said.
In addition to the nanoparticle injection, mice were also given an oral dose of a chemotherapy drug known as temozolomide.
“It’s a new platform where we can give these oral chemotherapies that get across the blood-brain barrier and a targeted agent just in the central nervous system,” Bindra said. “In essence, this compartmentalization of combination therapy will enhance synergistic tumor cell killing while minimizing systemic toxicity.”
The mice that received the nanoparticle-based treatment lived significantly longer than the mice who received drug therapy that didn’t use nanoparticles and even longer than the mice that received no treatment. Further, there was much less cancer spreading in the mice that received the drug-carrying nanoparticles.
The researchers said the next steps will be to validate the approach in larger animal models, eventually followed by human testing. The team also plans to test the treatment method on other cancers, particularly those that tend to spread to the brain.
Source: Yale University
You can offer your link to a page which is relevant to the topic of this post.
#amp#approach#barrier#Biotechnology news#blood#blood-brain barrier#Brain#brain cancer#brain tumors#Cancer#cancer drugs#cell#Cells#chemical#chemotherapy#Children#defense#Disease#DNA#DNA repair#drug#drugs#engineering#Environmental#enzyme#FDA#Foundation#growth#human#humans
0 notes
Text
Pharmacology - Chapter 2 - Basics of Pharmacology (Part 2)
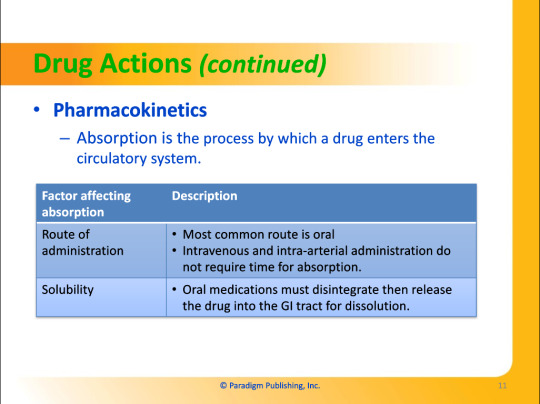
Part One
Part Three
Transcription under the cut!
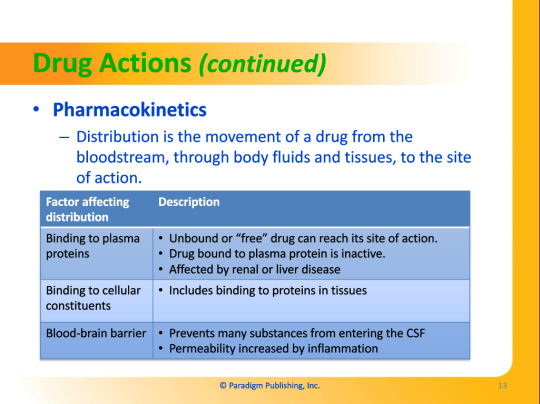


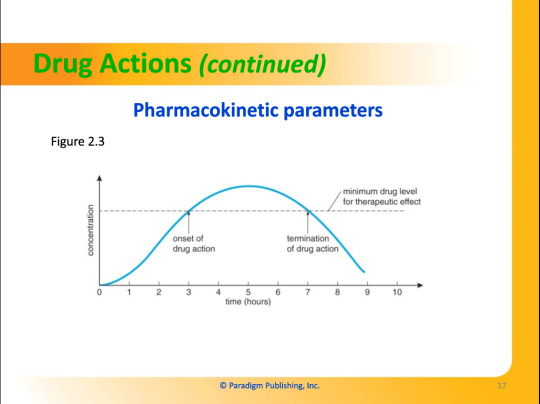


Drug Actions
Pharmacokinetics
Absorption is the process by which a drug enters the circulatory system.
Route of administration
Most common route is oral.
Intravenous and intra-arterial administration do not require time for absorption.
Solubility
Oral medications must disintegrate then release the drug into the GI tract for dissolution.
Absorption
Occurs in the small intestine
The faster the rate of gastric emptying, the more rapid the absorption rate of a drug.
Practice Tip
Absorption of certain drugs depends on food. Some drugs are absorbed better by the body on an empty stomach. Others are better absorbed with food. As a pharmacy technician, you can help patients by placing auxiliary labels on drugs that require special attention to food.
Distribution is the movement of a drug from the bloodstream, through body fluids and tissues, to the site of action.
Binding to plasma proteins
Unbound or "free" drug can reach its site of action.
Drug bound to plasma protein is inactive.
Affected by renal or liver disease.
Binding to cellular constituents
Includes binding to proteins in tissues.
Blood-brain barrier
Prevents many substances from entering the CSF.
Permeability increased by inflammation.
Metabolism converts drugs to other biochemical compounds and then excretes them through metabolic pathways.
Induction
An increase in enzyme activity which can increase metabolism.
Inhibition
A reduction in enzyme activity which can decrease metabolism.
Elimination is the removal of a drug or its metabolites from the body.
Occurs mainly in the kidneys and liver but can also occur via the lungs, perspiration, saliva, and breast milk.
Pharmacokinetic Parameters
Dose
Quantity of drug administered at one time.
Dosage
The administration of a specific amount, dose number, and dose frequency of a drug.
Ceiling Effect
As greater dosages of drug are given, the point at which either no improved clinical response occurs or the adverse effects outweigh the beneficial effects.
Bioavailability
The fraction of a dose available to the target tissue.
First-Pass Effect
Metabolism of a drug in the liver before it reaches the systemic circulation.
Pertains to oral medications.
May result in reduced bioavailability.
Requires some drugs to be given by injection only.
Therapeutic range is the range of serum concentrations for a drug that provides the optimal probability of achieving the desired response with the least probability of toxicity.
Underdosing
Little effect
Therapeutic effects
Weak to strong effects
Excess dosing
Side effects (toxicity, death)
Therapeutic Level
The amount of drug in a patient's blood which gives the desired response.
Duration of action
The length of time a drug is at the therapeutic level.
0 notes
Last Seen Blogs

bishiemakeovers
The name says it all.

doorkickersinc
DOORKICKERSINC.
nmdgrr
Nom de Guerre

i-fairoz-blog
Untitled

scuderiahockeyfc
football and f1