#and hcl oral??! :(((
Text
hi guys have some RANDOM SOUKOKU HEADCANNONS because i’m procrastinating my holiday homework lol (like i genuinely can’t bring myself to do it so i’ll just uh, cram it all before school actually starts)
contrary to popular belief, dazai is actually the good cook between the two of them :) chuuya burned down the entire kitchen once when he tried to make rice, so dazai removed his kitchen-entering privileges. dazai can actually cook well, he just enjoys seeing the shocked/scared faces of the people he serves his food to when he makes it nasty
dazai replaced their couch with a foldable couch bed because whenever he makes chuuya mad, he gets sent to sleep on the couch, and their old one was uncomfortable and not big enough for his lanky ass legs
chuuya once thought dazai was a burglar when he was drunk and smacked him in the face with a frying pan, which broke dazai’s nose. he (chuuya) cried while apologising when he sobered up
they have movie marathon nights, except they speedrun movies separately and fight to see how many more movies they can watch than the other before the clock strikes 7:00am and dazai has to go to work
when dazai did the “that’s what i love about you!” thing to chuuya when they were younger, chuuya actually wanted to punch dazai because he was so flustered. he actually went back to his room to punch his pillow and scream into it about how much he liked dazai back and how he messed up his response
chuuya likes it when dazai drives, because it’s so adrenaline inducing and it’s funny to see the looks on civilian’s faces when they speed pass them and almost crash into the lamp post
dazai’s home wallpaper is a picture of chuuya drooling in his sleep, and chuuya’s one is of dazai screaming and running away from a dog
i feel like they would both be really good at styling hair and doing makeup from kouyou’s lessons and all the infiltration missions they have to go on... although, i can picture chuuya trying to pry a bite of lipstick out of dazai’s mouth because he read the contents and tried to commit suicide by eating it lol
they have a built in wine cellar in their house (inspo from my aunt’s house lol. she has a fucking wine cellar in there stock full of expensive alcohol and there’s even a catalogue) and it’s super super cold. they have two silly fuzzy pairs of slippers, one is crab designed and the other is slug designed lol
yes ig that’s all for now :D
#lei writes! ଘ(|lI.‸.)#i genuinely can't bring myself to do my work idk why#and exams are on the second week of the term aksjdhajdhka#and hcl oral??! :(((#ahhh this school is killing me but i don't wanna transfer#i worked so hard to get in here and i'm like#suffering more than my friends in other schools for some reason#like i get that we don't need to take o levels like the other schools but like??#why is our curriculum so fucked up??#why is our teaching system so messy??#bro the teachers aren't even actually teaching anymore tbh they just give us the work to figure out on our own#ahhhh anyways i need to get back to studying or smth#bungou stray dogs#bsd#soukoku#dazai x chuuya#dazai#chuuya
52 notes
·
View notes
Text
@downbadforpixels and i are literally talking about out chibi lives it's the cutest things we've talked about in a long time like we would be neighbours and tille would bake pies and tarts and i would grow a garden and we would have a pond full of algae and tiny flowers in thimbles and KAJSHDAKJDH
#lawnmower akutagawa =^. .^= ∫#tille is this our hcl oral coping mechanism#i think it is#well it's working
1 note
·
View note
Text
extremely bad crohns+pain day
1. using ketamine nasal spray, prn
ive done 4 sprays as of writing this
the bottle contains 15mL ketamine hcl (racemic), at a concentration of 100mg/mL. however it doesn’t say how many mL one spray administers so it’s kinda useless for figuring out how much I’m dosing per spray
2. vaping cbd, thc delta-8, specific terpenes, and thc delta-9, prn
3. hopefully i won’t need to i.v. buprenorphine or take oral morphine (I haven’t yet) but it’s there in case I need it
11 notes
·
View notes
Text
Psychomotor Stimulants: Cocaine
Cocaine and amphetamines belong to a class of drugs called psychomotor stimulants, which increase motor behavior, elevate a person’s mood, increase alertness and arousal, and cause behavioral excitement.
Cocaine: Background & History
- Cocaine is an alkaloid found in the leaves of the shrub Erythroxylon coca.
- It is native to South America and is cultivated in the northern and central Andes Mountains.
- The practice of chewing coca leaves began as early as 5000 years ago.

Map of principal coca-growing regions of South America

Bolivian miners chewing coca
- Cocaine was first isolated (extracted from coca leaves) in 1859 by German chemist Albert Niemann.
- Cocaine use became popular as many doctors and scientists lauded its properties.
- Sigmund Freud, who used the drug himself, was the first to broadly promote cocaine as a tonic to cure depression and sexual impotence. He declared that it was non-addictive.
- Cocaine also become popular in the USA and was used in many medications.
- In 1886, Coca-Cola was introduced, containing caffeine and cocaine. It was marketed as an alternative to alcohol as the temperance movement gained strength.
- Public pressure forced the Coca-Cola company to remove cocaine from the soft drink in 1903.
- Cocaine abuse became widespread. President Taft declared it to be “public enemy number one” in 1910.
- The 1914 Harrison Narcotic Act prohibited inclusion of cocaine (and opium) in over-the-counter medicines and specified other restrictions on import and sale.
- Today cocaine is a Schedule II drug.
- In the 1970s, cocaine use by snorting or IV injection increased. It emerged as the fashionable new drug for entertainers and business people.
- In the 1980s, smoking crack cocaine has driven a new epidemic of cocaine use.
- After cannabis, cocaine is the most frequently used (illegal) drug on a global scale.
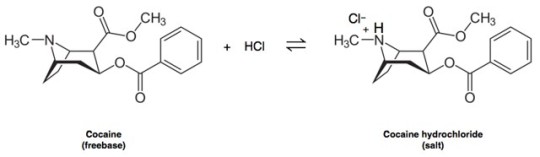
Preparation of Cocaine
- The cocaine alkaloid is extracted from coca leaves and then converted to a hydrochloride (HCl) salt and crystallized.
- Cocaine HCl is water-soluble and thus can be taken orally, intranasally (snorting), or by IV injection.
- It is not heat-stable, and cannot be smoked.

(left) prepared cocaine; (right) coca plant
- Cocaine HCl can be transformed into cocaine freebase.
- Freebase cocaine is “freed” from its natural salt.
- Crack cocaine is a lower quality freebase AKA less pure. The dried, hardened chunks make popping sounds when heated (which is why they call it “rock”).

- Freebase and crack can be vaporized through heating; those vapors are then inhaled.
- The term freebasing refers to smoking cocaine.
- Because the effects occur much faster, it’s more addictive.
- Crack can damage the lungs.
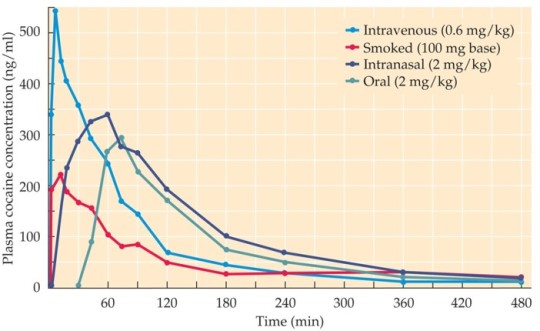
Pharmokinetics of Cocaine: Absorption
- Extremely rapid absorption occurs with IV injection and smoking (peak in seconds to minutes)
- Absorption is slower with snorting and oral use (peak in 30-60 minutes)
Pharmokinetics of Cocaine: Distribution
- Cocaine is sufficiently lipophilic (fat-soluble) that it passes readily through the blood-brain barrier.
- Rapid entry into the brain is believed to be an important factor in the strong addictive properties of crack cocaine.
Pharmokinetics of Cocaine: Metabolism
- Cocaine is broken down by enzymes in the blood and liver and is rapidly eliminated, with a half-life ranging from 0.5 to 1.5 hours.
- The “high” lasts only about 30 minutes.
- Breakdown products persist and can be detected in the urine for several days.
Pharmacodynamics: Behavioral Effects of Cocaine
- Typical aspects of the cocaine “high” are feelings of exhilaration and euphoria, a sense of well-being, enhanced alertness, heightened energy, and great self-confidence.
- Increased sociability and talkativeness
- Heightened sexual interest and performance
{note: if you have a penis, cocaine is very likely to make it flaccid, regardless of how psychologically ready you are for sex. so...keep that in mind.}
- Anger (increased aggression may contribute to the street violence associated with cocaine use)
- Appetite suppression (anorexia)
- Insomnia
- Severe effects are most likely with high dosages, particularly in chronic users:
Hostility
Extreme violence
Incoherent speech
Paranoia
Restlessness
Tactile hallucinations (”coke bugs”)

Mechanisms of Cocaine Action: Monoamine transporters
- Most of cocaine’s actions can be explained by its ability to block reuptake of three transmitters: dopamine, norepinephrine, and serotonin.
- These transmitters are cleared from the synaptic cleft by membrane transporters. Cocaine binds to the transporters and inhibits their function.

- Inhibition of the transporters leads to increased neurotransmitter levels in the synaptic cleft and a corresponding increase in transmission at the affected synapses.
- Cocaine binds most strongly (with highest affinity) to the serotonin transporter --> the dopamine transporter --> the norepinephrine transporter
- Blocking dopamine reuptake appears to be most important for cocaine’s stimulating, reinforcing, and addictive properties.
Mechanisms of Cocaine Action: The Reward System
- Nucleus accumbens dopamine has been implicated in cocaine reward using paradigms that test for drug-seeking behavior as a model of relapse. (VTA --> NAcc)
- Reinstatement of cocaine-seeking behavior in previously extinguished rats can be stimulated by microinjection of dopamine receptor agonists directly into the nucleus accumbens.
Pharmacodynamics: Physiological Effects of Cocaine
Local anesthesia
At high concentrations, cocaine inhibits voltage-gated Na+ channels in axons, blocking nerve conduction.
When applied locally, it acts as a local anesthetic by preventing transmission of signals along sensory nerves.
Cocaine is used by health care professionals to temporarily numb the lining of the mouth, nose, and throat (mucous membranes) before minor surgeries, biopsies, etc.
Other, non-addictive, local anesthetics - procaine (Novocain) and lidocaine (Xylocaine) - were developed from cocaine.
Sympathomimetic effects
- Cocaine is sympathomimetic; it produces symptoms of sympathetic nervous system activation: increased heart rate, vasoconstriction, hypertension, hyperthermia
- At low doses, these changes are usually not harmful to the individual. High doses, however, can be toxic or even fatal.
Overdose
- Can result from sniffing, inhaling, IV injection, etc.
- Disturbance of the heart and blood vessel system, resulting in...
high blood pressure
stroke
heart attack
- Increased core temperature
- Renal failure
- Psychosis, agitation
- Repeated convulsions, which can happen in such quick succession that consciousness cannot be restored.

Treatments
There is no specific pharmacological antidote for cocaine overdose, but strategies include:
Benzodiazepines, to reduce agitation and produce relaxation
Nitroglycerin or beta-blockers, to reduce blood pressure and relieve chest pain
Anti-psychotics
Cooling with a fan or water misting
Long-term health effects of cocaine
- Snorting cocaine:
Lost sense of smell
Nosebleeds
Chronically inflamed, runny nose
Damage to the walls of the nasal cavity
- Smoking crack
Lung damage
Worsening of asthma
- Cocaine reduces blood flow in the gastrointestinal tract, which can lead to tears and ulcerations.
- Many chronic cocaine users lose their appetite and experience significant weight loss and malnourishment.
- Toxic effects on the heart and cardiovascular system
- Increased risk of stroke
Drug Interactions
Alcohol or other depressants are sometimes taken along with cocaine to “take the edge off” the extreme arousal produced by cocaine.
- Cocaine when mixed with alcohol produces a unique metabolite called cocaethylene, which has activity similar to cocaine, but has a longer half-life.
- “Speedball” = mixture of cocaine and heroin
Aim is to increase “rush” and reduce negative effects
Danger of delayed opioid overdose
Danger of stroke and heart attack
Chronic Cocaine Exposure
- Most individuals who try cocaine do not progress to a pattern of abuse or dependence.
- About 10-15% of initial users develop a habit.
- People usually start cocaine by snorting. Some people have a strong anxiety response and do not try it again.
- Other factors that discourage habitual use include cost and availability, social and legal consequences, fear of addiction
{note: I have tried coke that was $40 a gram and coke that was $120 a gram and coke that was somewhere in between. Cheap, stepped-on coke made me feel tired and nauseous. Expensive, fish-scale coke was pleasant, but not quite euphoric. The anxiety usually happened at price points in the middle. Typically I would do one, maybe two lines over the course of the evening. I have not had coke in many years and would not care to try it again; the risks heavily outweigh the rewards, in my mind.}
- The stimulating, euphoric, and confidence-enhancing effects are powerful reinforcers in the early stages.
- Crack smoking or IV injection have greater abuse potential.
- Some individuals develop a pattern of cocaine binges, episodic bouts of repeated use lasting hours to days with little or no sleep. Afterwards, an abstinence syndrome occurs.
- Chronic exposure to psychostimulants can lead to tolerance (pharmacodynamics and behavioral).
- In humans, cocaine’s euphoric effects tend to show tolerance, which would contribute to increased drug-taking in an attempt to recapture the level of pleasure experienced during earlier episodes of use.
- The reverse effect, sensitization, is also seen. Just a few exposures to cocaine or amphetamine can produce an increased responsiveness that lasts for weeks, months, or even up to a year.
- Continuous cocaine infusion into rats causes tolerance to the locomotor-stimulating effect; once-daily injections lead to behavioral sensitization, shown by enhanced stereotyped behaviors.
- Although cocaine withdrawal is rarely serious, it produces a number of very unpleasant side effects. Symptoms generally only last for about a week or two and may include the following:
depression
fatigue
exhaustion
increased appetite
unpleasant dreams
difficulty concentrating
intense craving for cocaine
Treatment of Cocaine Use Disorder
- Presently there are no FDA-approved medications to treat cocaine addiction.
- Consequently, National Institute for Drug Abuse (NIDA) is working aggressively to identify and test new medications to treat cocaine addiction safely and effectively.
- While many have shown effectiveness in animal models, none are currently licensed for medical use due to unacceptable side effects and/or lack of therapeutic efficacy.
Search for New Therapeutics
- Various dopaminergic drugs, including receptor agonists, antagonists, and uptake inhibitors are being studied.
- Several compounds that compete with cocaine for access to the dopamine transporter show promise.
- Other drugs being studied target other neurotransmitters, including serotonin.
Repurposing Existing Drugs
- Modafinil: narcolepsy drug that acts as a selective (and weak) dopamine reuptake inhibitor
- Disulfiram (Antabuse) has produced the most consistent reductions in cocaine abuse:
popular drug for treating alcoholism
produces unpleasant symptoms after taking cocaine, such as anxiety
Scientists do not yet know exactly how disulfiram reduces cocaine use, though its effects may be related to its ability to inhibit an enzyme that converts dopamine to norephinephrine.
Behavioral and Psychosocial Therapies
- Typically conducted as outpatient programs
- Psychosocial treatment programs involve individual, group, or family counseling designed to educate the user, promote behavioral change, and alleviate problems caused by cocaine abuse.
- Twelve-step programs such as Narcotics Anonymous or Cocaine Anonymous are also available.
2 notes
·
View notes
Text
Smiling with Confidence Again: My Positive Experience with

For years, I neglected my dental health, leading to occasional gum sensitivity and a nagging fear of dentist visits. Concerned about these issues and wanting a natural solution to improve my oral health, I discovered DentiCore, a dental health supplement generating a lot of positive buzz online.
A Natural Path to a Healthier Smile
DentiCore appealed to me because it offered a comprehensive, natural approach to supporting oral health. The formula boasts a blend of vitamins, minerals, probiotics, and herbal extracts known for their potential benefits in promoting healthy gums, strengthening tooth enamel, and freshening breath. Ingredients like Alpha-Lipoic Acid, Berberine HCL, and Lactobacillus Reuteri stood out for their ability to reduce inflammation, combat bad breath-causing bacteria, and potentially support the growth of good bacteria in the mouth.
The focus on natural ingredients resonated with me, as I wanted to address my oral health concerns holistically without resorting to harsh chemical rinses. DentiCore offered a natural, multi-faceted approach to potentially improve my oral health and promote a brighter, healthier smile.
The DentiCore website provided clear information on each ingredient and its role in promoting a healthy mouth. They also offered studies and research highlighting the potential effectiveness of these natural components. This transparency and the focus on a natural approach instilled confidence in the product's safety and effectiveness.
Easy to Use and Integrate into My Routine
The convenience of DentiCore is one of the things I appreciate most. The capsules are easy to swallow and don't require any messy mixing or special storage. The recommended dosage is one capsule daily, which I easily integrated into my morning routine alongside my usual vitamins.
Gradual Improvement and a Healthier Mouth
Within a few weeks of taking DentiCore consistently, I noticed a significant improvement in my gum health. The occasional gum sensitivity I used to experience became less frequent, and my gums felt firmer and healthier overall. This improvement in gum health not only felt good but also motivated me to maintain a consistent oral hygiene routine.
Perhaps the most unexpected benefit was a noticeable improvement in breath freshness. The occasional bad breath I used to experience became a thing of the past, leaving me feeling more confident in social interactions. This newfound confidence in my breath was a welcome change.
Sustainable Support and a Brighter Smile
DentiCore offers a natural and sustainable approach to potentially promote healthy gums, strengthen teeth, and improve overall oral health. Unlike harsh chemical rinses with temporary effects, DentiCore's effects are gradual and improve with consistent use. This natural supplement has become an essential part of my daily routine, promoting improved gum health, fresher breath, and a renewed sense of confidence in my smile.
Important Note: It's crucial to remember that everyone's body reacts differently to supplements. While my experience with DentiCore has been positive, it's always advisable to consult with your dentist before starting any new supplement regimen, especially if you have a pre-existing dental condition.
Maintaining a healthy oral hygiene routine with regular brushing, flossing, and professional dental cleanings remains crucial for optimal oral health. However, DentiCore can be a valuable companion on your journey to a healthier mouth, a brighter smile, and a more confident you.
A Reliable Partner for a Healthy Smile
Overall, I've been very impressed with DentiCore. The convenient format, the natural formula, and the noticeable improvement in my gum health, breath freshness, and overall confidence in my smile have made it a valuable addition to my health regimen. If you're looking for a natural way to support your oral health, I highly recommend giving DentiCore a try. Remember, maintaining a good oral hygiene routine is key, and DentiCore can be a helpful tool on your path to a healthier, brighter smile.pen_sparktunesharemore_vert
0 notes
Text
Cold
Symptoms – sore throat, sneezing, runny/blocked nose, cough, mild fever, pressure in ears, headache, myalgia (pain in muscles)
Duration – 1-2 weeks, symptoms peak 2-3 days, incubation period 10-12 hrs
Referral criteria – suspected flu, earache not responding to analgesia, sinus pain not responding to decongestants, no improvement after 10-14 days self-medication
Complications - immunocompromised, who smoke, and with comorbidities such as diabetes mellitus, congestive heart failure, asthma, chronic obstructive pulmonary disease, cystic fibrosis, and sickle-cell disease
Sinusitis – prolonged nasal congestion and facial pain
LRTI - acute bronchitis, acute exacerbation of asthma or chronic obstructive pulmonary disease (COPD), and community-acquired pneumonia
Acute otitis media – common in younger patients
Differential diagnosis
Meningitis – high fever, drowsiness, blank expression, vomiting, loss of appetite, high pitched screaming, non-blanching rash, photophobia, severe headache, malaise
Upper airway obstruction – noisy breathing, drooling, inability to swallow.
Nasal foreign body – persistent discharge from 1 nose with no other symptoms
Management – paracetamol or ibuprofen for headache, muscle pain or fever – only continue use if distressed, change to other agent if not alleviated, don’t give both together
Paracetamol contraindicated in – liver/kidney problems, epileptic
Ibuprofen contraindicated in – pregnancy, perforated stomach, increased bleeding, severe HF, kidney or liver problems, high BP, asthma, hay fever
Intranasal decongestants – improve breathing and promote sleep and has fewer S/E than oral decongestants. Ephedrine HCL 0.5% nasal drops for 12 and older p 1-2 drops 4x daily for 1 week – contraindicated – diabetes, hypertension, hyper thyroidism, CVD, high BP, MAOI in last 2 weeks
Oral decongestants – relieve nasal congestion (phenylephrine) – max 1 week
Antitussive (cough) – dextromethorphan
Expectorants (guaifenesin)
Chlorphenamine or Beecham’s (contains phenylephrine and paracetamol) (Sedating antihistamine – dries up secretions)
Counselling points
Go to GP if
fever for more than 3 days
symptoms worsening after 5 days
symptoms not better after 10 days
follow up meeting
risk and complicated patients within the week
young children – 1 week
Headaches
Types of headaches
Primary – not associated with other conditions – migraines, tension types, cluster
Secondary – associated with other conditions – trauma/injury, vascular disorders, hyper-tension, withdrawal such as opioids, analgesics, or alcohol. Bacterial or viral infection.
Features of serious headache – referral
New severe or unexpected headache – sudden onset reaching max intensity 5 mins and new onset in over 50s
Progressive or persistent headaches that changed dramatically
Associated features – fever, impaired consciousness, seizure, stiffness, photophobia, neurological deficit, cognitive dysfunction, atypical aura (greater than 1 hour) or aura 1st time in patients using combined oral contraceptives.
Dizziness, visual disturbance, vomiting. Head trauma up to 3 months prior, triggered by coughing, sneeze, or physical exertion. Worsened by standing or lying down.
Compromised immunity
Diagnosis
Migraine without aura – at least 5 attacks lasting 4-72 hrs with unilateral location (half the face), pulsating, moderate to severe pain and aggravated by or causing avoidance of routine physical activity. Attack comes with nausea and/or vomiting, photophobia and phonophobia
Migraine with aura – 2 attacks with visual aura (zigzag lines or blind spots), pins and needles, speech/language symptoms, motor weakness, vertigo.
One aura spreading gradually for 5 mins and 2 or more occurring after
Each aura lasts for 5-60mins which is unilateral
Management – stop combined oral anticontraception – contraindicated
Ibuprofen 400mg, paracetamol 1g, advise med to be taken at start of attack – follow up 2 weeks
Tension type – recurrent episodes lasting 30 mins – 7 days with NO nausea or vomiting. May have phot/phono phobia
Bilateral (across head landscape), pressing or tight (not pulsating), mild to moderate pain, not aggravated by physical activity
Management – simple analgesia – paracetamol or NSAID
Identify comorbidities such as stress, mood disorders, chronic pain, sleep disorders to manage
Cluster headache – 5 attacks of severe/very severe unilateral orbital (around ONE eye), forehead or temporal pain lasting 15 mins to 3 hrs with nasal congestion, runny nose, eyelid oedema, sweating, facial slushing, fullness in ear or restlessness
Attacks occur between one every other day and 8 per day for more than half the time the disorder is active
Management – REFER
Advise to avoid triggers and risk of medication overuse, identify and manage comorbidities – insomnia, depression, and anxiety
Medication – occurs 15 days per month and have a pre-existing headache disorder. Regular overuse of drugs for 3 months
Management – withdrawal from medication and advice around this
Sinusitis
Sinusitis usually follows a cold and lasts less than 12 weeks
If over 12 weeks becomes chronic – risk groups are allergic rhinitis, asthma, immunosuppression
Symptoms
Adults
Nasal blockage (obstruction/congestion), nasal discharge, facial pain/pressure, frontal headache, loss, or reduction of smell, altered speech indicating nose blocked. Tenderness, swelling. Redness over cheekbone, cough, headache worse when bending or lying down. Toothache.
Children
Nose block, discoloured nasal discharge, facial pain, pressure and or cough at day or night-time
Bacterial sinusitis
More than 10 days, discoloured, pussy discharge (from 1 nose), severe local pain (1 side), fever over 38 degrees, deterioration after milder sickness
Refer to hospital immediately
If they have symptoms of acute sinusitis and;
Severe systemic infection
Intraorbital or periorbital complications, including periorbital oedema or cellulitis, displaced eyeball, double vision, or new reduced vision
Intracranial complications, including swelling over frontal bone, symptoms or signs of meningitis, severe frontal headache, or focal neurological signs
Refer to GP
Severe symptoms, painkillers don’t work, symptoms worsen, symptoms don’t improve after 1-week, recurrent infection, sudden worsening, antibiotic failure, unusual or resistant bacteria, recurrent episodes, immunocompromised, allergic cause
Treatment
Acute with symptoms less than 10 days
DON’T OFFER ANTIBIOTIC, assure that it usually self resolves without bacterial complications. Symptoms managed
Paracetamol or ibuprofen for pain, headache, and fever
Use nasal saline spray or decongestants spray
Clean nose with saltwater solution (boil 1 pint of water and add 1 teaspoon of salt and bicarbonate soda. Wash hands, stand over sink, cup the palm of 1 hand and pour small amount of solution into it. Sniff water into 1 nostril at a time, breath through mouth and allow water to pour into sink, don’t let it go into your throat. Do 3x daily)
Acute for 10 days or more with no improvement
High dose nasal corticosteroid for 2 weeks for over 12s (mometasone 200mcg 2x daily)
Counsel that It may improve symptoms but won’t make the infection any shorter, could have systemic effects, may be difficult to use correctly.
Symptoms should get better 3-5 days of treatment – REFER if not
1st line antibiotic for adult
If not life threatening - phenoxymethylpenicillin 500 mg four times a day for 5 days.
Is systemically unwell, symptoms of more serious illness or high risk of complications - co-amoxiclav 500/125 mg three times a day for 5 days.
Allergic or intolerant to penicillin - clarithromycin 500 mg twice a day for 5 days.
Pregnant or intolerant to penicillin - erythromycin 250 mg to 500 mg four times a day or
Children 1st line
Phenoxymethylpenicillin
1 to 11 months, 62.5 mg four times a day for 5 days.
1 to 5 years, 125 mg four times a day for 5 days.
6 to 11 years, 250 mg four times a day for 5 days.
12 to 17 years, 500 mg four times a day for 5 days.
If very unwell - co-amoxiclav
1 to 11 months, 0.25 mL/kg of 125/31 suspension three times a day for 5 days.
1 to 5 years, 5 mL of 125/31 suspension three times a day or 0.25 mL/ kg of 125/31 suspension three times a day for 5 days
6 to 11 years, 5 mL of 250/62 suspension three times a day or 0.15 mL/kg of 250/62 suspension three times a day for 5 days.
12 to 17 years, 250/125 mg three times a day or 500/125 mg three times a day for 5 days.
If allergic or intolerant to penicillin – clarithromycin
Under 8 kg, 7.5 mg/kg twice a day for 5 days.
8 to 11 kg, 62.5 mg twice a day for 5 days.
12 to 19 kg, 125 mg twice a day for 5 days.
20 to 29 kg, 187.5 mg twice a day for 5 days.
30 to 40 kg, 250 mg twice a day for 5 days.
12 to 17 years, 250 mg twice a day or 500 mg twice a day for 5 days.
2nd line – if symptoms are still worsening after 1st line treatment for 2-3 days
Adults – co-amoxiclav 500/125mg TD x 5 days
Children – specialist advice
ANTIHISTAMINES can be prescribed for allergic triggered sinusitis
Diabetes type 1
Body stops making insulin and the blood sugar (glucose) level goes extremely high - persistent hyperglycaemia (random plasma glucose of 11mmol/l or more). We must control glucose level with insulin injections, healthy diet and reduce the risk of other health complications. Typically occurs in children and young adults.
Symptoms of T1D- Frequently thirsty, pass a lot of urine, tiredness, weight loss and feeling generally unwell. Develops quite quickly, over days or weeks, as the pancreas stops making insulin.
Pathophysiology of T1D- Autoimmune disease (environmental & genetic factors). Antibodies attach to the beta cells in the pancreas destroying the cells that make insulin (pancreatic islet cells).
Diagnosing T1D- Simple dipstick test to detect glucose in a sample of urine BUT only way to confirm the diagnosis is to have a blood test to look at the level of glucose in your blood (level of 11.1 mmol/L or more in the blood sample indicates that you have diabetes) PLUS a fasting blood glucose level is taken (level of 7.0 mmol/L or more indicates that you have diabetes).
Management- Should be offered multiple daily injection basal-bolus insulin regimens as the first-line choice. Twice-daily insulin detemir should be offered as the long-acting basal insulin therapy. Once-daily insulin glargine may be prescribed if insulin detemir is not tolerated, or if a twice-daily regimen is not acceptable to the patient. Insulin detemir may also be offered as an alternative once-daily regimen. There are multiple types of insulin…
Rapid Acting- Insulin Aspart (Novorapid®), Lispro (Humalog®) and Glulisine (Apidra®)
Short Acting- Soluble insulin (Actrapid®)
Intermediate Acting- Isophane (Insulatard® or Humulin I®) & NPH - neutral protamine Hagedorn
Long Acting- Insulin glargine (Lantus®), detemir (Levemir®)
Combination insulins (biphasic)- e.g., Novomix 30®, Humalog Mix 25®, Humalog Mix 50®, Humulin M3® and Insuman Comb 50®
Diet & Lifestyle- Diet low in fat, salt, and sugar and high in fibre and with plenty of fruit and vegetables. If you are overweight try to lose weight, increase your physical activity even if it’s only going for a walk (community groups)
Other Health Complications- Get regular checks with your GP, podiatrist, and optometrist. Also get the flu jab every year.
Complications – microvascular, macrovascular (MI, stroke), metabolic (diabetic ketoacidosis) and hypoglycaemia (blood glucose less than 3.5mmol/l)
Psychological complications – anxiety, depression, and eating disorders and those at increased risk of developing autoimmune diseases
Suspect DKA in diabetics – greater than 11mmol/L
Increased thirst and urine frequency, inability to tolerate fluids, persistent vomiting, diarrhoea, visual disturbance, lethargy, fruity smell on breath, deep sighing when breathing and dehydrated
Management
HbA1c levels target of 48mmol/mol or lower - Measure 3-6 months but more often if not controlled
Self-monitoring – need glucose monitor, lancet, finger pricking device and testing strips
Taught at diagnosis and review technique 1 yearly.
Before breakfast, 2 hours after meals, during illness, before driving, if they feel hypo – at least 4 times a day including before and after meals and before bed.
More frequency required (up to 10x daily) if
Target HbA1c not achieved, frequency of hypo increases, during illness, before, during and after sports, planning, during and while breastfeeding.
Target glucose readings
Fasting plasma glucose level of 5–7 mmol/L on waking.
Plasma glucose level of 4–7 mmol/L before meals at other times of the day.
For adults who choose to test after meals, plasma glucose level of 5–9 mmol/L at least 90 minutes after eating.
Agree bedtime target plasma glucose levels with the person. This should:
Consider the timing of the last meal and its related insulin dose.
Be consistent with the recommended fasting level on waking.
Provide information of effects of food and drinks – carbohydrate training (match carb quantities to insulin doses)
Educate to be careful of body weight and diets, feasting and fasting, fibre and protein intake, diabetic foods and sweeteners, alcohol intake, matching carbs with insulin and physical activity
Advice on alcohol – avoid drinking on empty stomach, eat carb snack before and after drinking (extra insulin not required). Measure glucose more regularly and maintain it with carb intake. Alcohol can exacerbate or prolong hypoglycaemic effect.
Exercise – lower glucose levels and reduces CVD risk and can help weight
Sick day rules – never stop or skip insulin – dose may need altering seek advice. Check blood more frequently – 1-2 hours including in the night. Check blood or urine ketone levels – 3-4 hours including night and if 2+ or 3mmol/l or higher then contact GP immediately.
Maintain normal meal pattern where possible if not then replace meals with carb rich drinks, milk, fruit juices and sugary drinks. Aim to drink at least 3L of fluid to prevent dehydration.
Offer multiple daily injection basal-bolus insulin regimens as the first-line choice to all adults with type 1 diabetes.
Offer twice-daily insulin detemir as the long-acting basal insulin therapy
Offer a rapid-acting insulin analogue injected before meals for mealtime insulin replacement
If a multiple daily injection basal–bolus insulin regimen is not possible and a twice-daily mixed insulin regimen is preferred
Insulin pump therapy is recommended as a treatment option for adults with type 1 diabetes mellitus if condition isn’t controlled by treatment
Diabetes type 2
The body still makes insulin however, you do not make enough insulin for your body's needs OR the cells in your body do not use insulin properly (insulin resistance means you need more insulin than normal make to keep glucose levels down. Occurs mainly in people aged > 40 but inc diagnosed in younger people, commonly associated with obesity, physical inactivity, raised blood pressure, dyslipidaemia, and a tendency to develop thrombosis (CV risk).
Symptoms of T2D- Gradual (weeks-months) and can be quite vague at first. Frequent thirst, passing large amounts of urine, tiredness, which may be worse after meals. Some people also develop blurred vision and frequent infections, such as recurring thrush.
Management- Metformin HCl 1st choice for treatment of all patients (à weight loss, red risk of hypoglycaemic events and long-term CV benefits). Has an anti-hyperglycaemic effect, lowering both basal and postprandial blood-glucose conc. It does not stimulate insulin secretion and therefore, when given alone, does not cause hypoglycaemia. If metformin contra-indicated/not tolerated trial MR formulation or initial treatment should be a sulfonylurea e.g. gliclazide OR a dipeptidyl peptidase-4 inhibitor e.g. linagliptin OR Pioglitazone.
Insulin- can be added if intensification of treatment needed. If needed, bedtime basal insulin should be initiated, and the dose titrated against morning (fasting) glucose.
Diet & Lifestyle- Avoid foods heavy in saturated/trans fats, beef and processed meats, sugary drinks, high-fat dairy products and salty/fried foods & have fibrous fruits and vegetables, high omega-3 fatty acid food and poly/monosaturated fats. Lose weight and inc physical activity (min 5 x 30 min brisk walk / week) and smoking cessation. Also see optician regularly in case of damage to retina, GP and podiatrist.
EXTRA INFO FOR BOTH
Holiday- Pack about x3 the amount of insulin needed, test strips, lancets, needles or glucose tablets you would use, in case you need it (take cool bag to avoid insulin getting too hot). Carry your medicine in your hand luggage just in case checked-in bags go missing or get damaged (insulin can freeze and render it unusable). If injecting (i.e. will have needles/sharps) get a letter from your GP that says you need it to treat diabetes. If you use a pump or CGM, check with your airline before you travel about taking it on board as may require paperwork for medical equipment. If you use a pump, pack insulin pens in case it stops working. Take plenty of snacks in case there are any delays. Do not put your pump through the hand luggage scanner – let airport security know so they can check it another way.
<18 & Diabetic- Paediatric diabetes care team until 18 will help w injecting insulin, testing blood glucose levels, and diet. They can give advice on school or nursery and talk to your child's teachers and carers. Initially, every 1 - 2 weeks but will eventually be every 3 months.
Check Ups Needed- Annually get feet checked by podiatrist to check for loss of feeling in your feet, and for ulcers and infections. Get your eyes checked to check for any damage to blood vessels in the eyes, and checks for high blood pressure, heart, and kidney disease by your GP, also ensure to book in annually for a flu jab. Every 3 months have a blood sugar test (HbA1C test) checks your average blood sugar levels and how close they are to normal when newly diagnosed, then every 6 months once you're stable (~48-53 mmol/mol recommended).
Education- free education courses to help you learn more about and manage your diabetes, your GP will need to refer you. Diabetes UK run local charities for extra support, their website plus the NHS website offers a lot of diabetes information and advice. Maybe invest in a medical ID to carry w you.
Extra Lifestyle Advice- Eat a meal w carbs (e.g. pasta) before you drink alcohol and make sure people around you can recognise a hypo, choose diet soft drink mixers where possible, check your blood glucose regularly/before bed/the next day, drink plenty of water the next day. Avoid hypos by eating the right amount of carbs before, during and after exercise, adjust your insulin and check your blood glucose regularly, drink plenty of water. Recommended to have HbA1c <48mmol/mol when pregnant as high blood glucose levels can harm your baby, especially in the first 8 weeks of pregnancy, also a risk of having a large baby, which can cause complications during labour. Speak to your diabetes team If you're planning to get pregnant or if you get pregnant unexpectedly.
Item for disposal
Method of disposal
Needles
Sharps bin
Lancets
Sharps bin
Used blood test strips
Sharps bin
Leftover/expired insulin
Sharps bin/return to pharmacy
DVLA- tell the DVLA you’re diabetic or you could get fined due to hypoglycaemia/low sugar levels crisis. Check your blood glucose no longer than 2 hours before driving, check your blood glucose every 2 hours if you're on a long journey, travel with sugary snacks and snacks with long-lasting carbs, like a cereal bar or banana. If you feel your levels are low: stop the car when it's safe, remove the keys from the ignition, get out of the driver's seat, check your blood glucose, and treat your hypo, don't drive for 45 minutes from when you feel normal again.
Sharps Removal- Patients issued a sharps bin from the diabetes clinic/hospital on first diagnosis. Some pharmacies offer this sharps disposal service, or the diabetes clinic do too. Can arrange w GP/LHB for sharps collection (Cardiff Council does NOT offer kerbside sharps disposal)
Other Technologies- Insulin Pump (attached to skin via tiny tube which is replaced every 2-3 days & pump moved to diff part of body) will deliver a set background amount of insulin into blood day and night, can add your extra mealtime insulin using the pump. Continuous glucose monitoring (CGMs) means you can check your sugar levels at any time (see patterns in your levels, sends an alert if glucose too high/low) but as interstitial fluid sugar readings are a few mins behind your blood sugar levels you'll still need to do finger-prick checks every now and then. It’s a sensor you attach to your abdomen which needs replacing every 7 days, but some models can be worn for months. Free Style Libre is a flash glucose monitoring system measures your glucose levels continuously throughout the day via interstitial fluid (few mins behind). Attach sensor to your arm and a reader will scan to see your sugar levels (can also use a smartphone app to scan the sensor), sensors usually last for 14 days.
Testing blood glucose
Glucose monitor, specific in-date test strips, primed lancing device and cotton wool pad.
PRIMING LANCET
Twist cap off lancing device
Place fresh lancet into device so grooves line up and twist off the cover, so the needle is visible – change lancet every time so you don't get skin infections
Replace device cap - it should click and then adjust the depth metre – how far the needle will puncture – this is personal preference
Pull sliding barrel at bottom of device back to prime the lancet
CALIBRATING MONITOR
Turn on monitor – put new in-date test strip inside it and test it with in-date control solution – to make sure readings are correct
Do this every time you open a new pack of test strips, if you damage your monitor and if you think the readings are wrong.
TESTING process
Wash hands with warm water and soap and dry. Then rub hands for 10 seconds – warms hands to improve blood flow to fingers
Turn on monitor and place strip inside and wait for it say it’s ready for blood
Place device firmly on side of the finger (less nerves so less painful) and press release button then remove device from site. - change fingers regularly to stop hardening of skin.
Wipe first drop of blood away with cotton pad, use second one to test make sure by touching the blood onto the test strip
If successful wipe blood with cotton pad and apply plaster
Note readings
Remove cap of device exposing lancet. Place lancet cover on table and press lancet hard into this blue plastic cover – this will cover the needle and make it easy to remove
Place lancet and cotton pad in bin
Injecting insulin
Inject in stomach, thighs, or buttocks. Inject an inch away from previous site. Prevents lumps – this reduces absorption of insulin.
check that its correct insulin and is in date. Always check manufacturer’s instructions.
Wash hands with soap and warm water
Attach needle to pen – peel back cover, screw cap onto pen, remove white outer cover and the green cover to expose needle – change needle every time
Dial to 2 units and push plunger so you can see insulin coming out – to make sure no air stuck in there – can take multiple goes in new pens
Set correct dose
Press directly into skin and inject slowly – count to 10
Remove needle straight without bending it
Use the white outer cap to remove the needle and dispose in yellow sharps bin
Asthma
Symptoms – episodic, worse at night/early morning, triggered by exercise, infection and exposure to cold air or allergens. Triggered by emotion and laughter in children. In adults by NSAIDS and BB use.
Common with atopic eczema, dermatitis and allergic rhinitis and family history
ACUTE EXACERBATION OF ASTHMA IN ADULTS
First-line treatment for acute asthma is a high-dose inhaled short-acting beta2 agonist (such as salbutamol) given as soon as possible. For patients with mild to moderate acute asthma, a pressurised metered-dose inhaler and spacer can be used. For patients with acute severe or life-threatening symptoms, administration via an oxygen-driven nebuliser is recommended, if available. If the response to an initial dose of nebulised short-acting beta2 agonist is poor, consider continuous nebulisation with an appropriate nebuliser. Intravenous beta2 agonists are reserved for those patients in whom inhaled therapy cannot be used reliably.
In all cases of acute asthma, patients should be prescribed an adequate dose of oral prednisolone. Continue usual inhaled corticosteroid use during oral corticosteroid treatment. Parenteral hydrocortisone or intramuscular methylprednisolone are alternatives in patients who are unable to take oral prednisolone.
IN CHILDREN OVER 2
First-line treatment for acute asthma is an inhaled short-acting beta2 agonist (such as salbutamol) given as soon as possible. For children with mild to moderate acute asthma, a pressurised metered-dose inhaler and spacer device is the preferred option. The dose given should be individualised according to severity and adjusted based on response. For children with acute severe or life-threatening symptoms, administration via an oxygen-driven nebuliser is recommended, if available. Parents/carers of children with acute asthma at home, should seek urgent medical attention if initial symptoms are not controlled with up to 10 puffs of salbutamol via a spacer; if symptoms are severe, additional bronchodilator doses should be given as needed whilst awaiting medical attention. Urgent medical attention should also be sought if a child's symptoms return within 3-4 hours; if symptoms return within this time, a further or larger dose (maximum of 10 puffs of salbutamol via a spacer) should be given whilst awaiting medical attention.
COPD
Symptoms - persistent respiratory symptoms and airflow obstruction, which is usually progressive and not fully reversible, exertional breathlessness, chronic/recurrent cough, or regular sputum production, wheeze
Treatment – education on condition and risk factors, smoking cessation, pneumococcal and flu vaccination yearly, treatment of associated comorbidities
1st line – SABA or SAMA to relieve breathlessness and improve exercise tolerance – reviewing medication, adherence, and inhaler technique regularly
THEN IF they have NO asthmatic features or no features of steroid responsiveness – offer LABA AND LAMA
If they continue to have day-to-day symptoms, consider 3-month trial of LABA+LAMA+ICS
If NO improvement go back to LAMA+LABA only but if it works continue and review annually
If they have asthmatic or steroid responsiveness features offer LABA+ICS if they have day to day symptoms of 1 severe or 2 moderate exacerbations a year, then offer LABA+LAMA+ICS
WITH ICS DISCUSS RISK OF USING ICS including pneumonia
Acute exacerbation of COPD – triggered by infections, smoking and environmental pollutants
Severe breathlessness, increased cough, increased sputum production and change in colour, increased wheeze, and chest tightness, cold or sore throat, reduced exercise tolerance, ankle swelling, increased fatigue, and acute confusion
FOR SEVERE exacerbation – ADMISSION
FOR non-severe – increase dose or freq of SABA and maybe change to nebuliser for ease of admission
If no contraindications with significant increase in breathlessness – offer 30mg oral prednisolone OD x 5 days or if caused by infection then amoxicillin 500mg TD x 5 days, doxycycline 200mg day 1, 100mg OD x 5 days, or clarithromycin 500mg BD X 5 days
Epilepsy
Cause – abnormal excessive or synchronous brain activity
Symptoms
Short-lived (less than 1 minute), abrupt, generalised muscle stiffening with rapid recovery — suggestive of tonic seizure.
Generalised stiffening and subsequent rhythmic jerking of the limbs, urinary incontinence, tongue biting —suggestive of a generalised tonic-clonic seizure.
Behavioural arrest — indicative of absence seizure.
Sudden onset of loss of muscle tone — suggestive of atonic seizure.
Brief, 'shock-like' involuntary single or multiple jerks —suggestive of myoclonic seizure.
Management
During seizure – protect from injury by placing in recovery position. If tonic-clonic seizure is prolonged (more than 5 mins) or recurrent – emergency buccal midazolam or emergency admission
Annually reviewed – assess seizure control, how it’s affecting QOL, adverse effects and compliance with drug
Women of childbearing age – 13 to 60
Epileptic women not treated with drugs or on non-enzyme inducing antiepileptic (except lamotrigine) – contraceptive options are same as general population
Woman on exyzme-inducing drugs – drug can reduce effectiveness of combined hormonal contraception, progestogen-only pills, transdermal patches, the vaginal ring, and progestogen-only implants. OFFER medroxyprogesterone acetate injections or an intrauterine method (copper intrauterine device or the levonorgestrel-releasing intrauterine system)
Woman on lamotrigine – oestrogen containing contraceptive reduces efficacy of lamotrigine
USE progesterone only instead but educate them to report signs of lamotrigine toxicity
Category 1 (ensure the person is maintained on a specific manufacturer's product) — phenytoin, carbamazepine, phenobarbital, primidone.
S/E – common and usually mild, advise to report and can usually be fixed with dose adjustment or change of drug
Sedation and dizziness, suicidal thoughts and behaviour, acute psychotic reactions, weight gain and loss, skin rashes.
Safe in pregnancies – lamotrigine (Lamictal) and levetiracetam (Keppra) are safest options
Anxiety
Uncontrollable widespread worry and range of cognitive and behavioural symptoms
Slow onset and symptoms don’t usually improve but are better controlled with intervention
Diagnosis – worry associated with restlessness, insomnia and muscle tension, fatigue, poor concentration, irritable. ALWAYS ask about alcohol and drug use including OTC
Treatment
Establish diagnosis and severity of anxiety and any other comorbidities (usually insomnia and depression and whichever is the most pressing is treated first) – explaining the disorder and treatment opportunities and starting them with active monitoring of symptoms either self or through regular meetings
Offer CBT – non-facilitated self-help for 6 weeks, individual guided self-help, educational groups
High intensity CBT, applied relaxation or drug therapy
Drug therapy – 1st line is SSRI (sertraline, paroxetine, or escitalopram) 2nd line SNRI (duloxetine or venlafaxine). If both contraindicated or intolerable then Pregabalin.
Review effectiveness and ADR every 2-4 weeks during first 3 months then every 3 months.
Counsel on common effects during treatment initiation (suicidal thoughts and worsening of anxiety) but importance of reporting this instead of withdrawing from drug
SSRI – don’t take NSAIDS or if prescribed take with PPI
For pregnant women step 3
DO NOT give benzo or antipsychotics in primary care
Benzodiazepines (SCH 3 and 4)
Most commonly used anxiolytics and hypnotics
Short rem relief (2-4 weeks only) of anxiety that is severe, disabling, or causing the patient unacceptable distress
use to treat short-term ‘mild’ anxiety is inappropriate
Sch 4 CDs, apart from temazepam
Sch 3 (CD no register) and midazolam
Pharmacological effects of benzodiazepines
Sedation, sleep induction
sleep, but can still cause arousal
decreased anxiety, amnesia at higher doses
muscle relaxation (both midbrain and spinal effects)
anticonvulsant activity
Reduced aggression
Depression
Persistent low mood and/or loss of pleasure in most activities and range of emotional, cognitive, physical, and behavioural symptoms
Diagnosis
Low mood
Loss of interest/pleasure from normally pleasurable activities (anhedonia)
Reduced energy (fatigue)
Low self-esteem; feelings of guilt
Inability to think/concentrate
Altered psychomotor activity
Sleep disturbance; early morning wakening
Altered appetite
Suicidal thoughts
Diagnosis requires 2 core symptoms plus 2 or more others present for most of the day on most days for the last 2 weeks
Differential diagnosis
Ensure symptoms are not caused by physical illness, alcohol, medication, or illicit drug use
The symptoms aren’t caused by normal grief (death of family) – maybe consider very long grief
Never been a manic (severe levels of high mood) or hypomanic (to a reduced level) episode
Treatment
Dependant on accurate assessment and diagnosis of depression
Psychological
CBT, behavioural activation, interpersonal psychotherapy, problem solving therapy
Social
Identify stressors and work on strategies/signposting to other supporting organisations
Biological – moderate to severe
Antidepressant therapy or antidepressant and antipsychotic combination therapy in psychotic depression
Drug classes
Tricyclic antidepressants (TCAs) e.g., amitriptyline
Selective serotonin reuptake inhibitors (SSRIs) e.g., fluoxetine
Serotonin and NA uptake inhibitors (SNRIs) e.g., venlafaxine
Monoamine oxidase inhibitors (MAOIs)
Irreversible e.g., phenelzine (MAO-A and B)
Reversible e.g., Moclobemide
Atypical antidepressants e.g., Mirtazapine
Noradrenaline reuptake inhibitors (NRIs) e.g., Atomoxetine
TCA - S/E – Short lasting (days) sedation, confusion, and Incoordination in both normal and depressed patients, antimuscarinic effects, dry mouth, blurred vision, decreased mucus production. Dangerous CV effects in OD
Severe depressive at risk of suicide shouldn’t be given TCA
Interactions – potentiation of the effects of alcohol – alcohol is a depressant and will only compound the depressive effects
SSRI’s - S/E – nausea, anorexia, insomnia, and loss of sexual function
Less anticholinergic side-effects and less dangerous in OD than TCAs. Prolonged QTc – cardiovascular complications risk with citalopram
interactions – NSAIDs, Anticoagulants, triptans
SNRI’s - S/E – significant withdrawal effects – have short half-lives so need to be taken regularly to avoid these effects. Complex nature of TCAs makes them difficult to prescribe to complex patients unlike SNRIs
Interactions – NSAIDs and anticoagulants
MAOIs - S/E – antimuscarinic effects, restlessness as a result of CNS excitation
Interactions – serious food and drug reactions e.g., cheese (tyramine from food such as cheese is broken down by MAO. The lack of breakdown from MAOIs can lead to tyramine actively displacing neurotransmitters such as 5HT, DA, NA – causing hypertensive crisis
VERY IMPORTANT COUNSELLING POINTS
No other drugs or illicit drugs with this
Side effects
Drug and food interactions are unacceptable.
“Cheese reaction”: this occurs when amines that are generated during fermentation, like tyramine, are ingested and absorbed from the gut. (The main danger is ripe cheese, yeast products - Marmite).
Large rise in systemic tyramine indirectly results in a large release
of catecholamines
Hypertensive crisis characterised by throbbing
headache, tachycardia & cardiac arrhythmias.
Same can occur with drugs (Pseudoephedrine)
Atypical antidepressants - S/E- sedation, weight gain, increased appetite – good in patients with anorexia or depression causing loss of appetite or weight
Blood disorders – counselling
Withdrawal issues
Can be used with other antidepressants that cause sleep issues
Interactions – alcohol
FDA black box warning – suicide
Treatment
Mild symptoms – psychological therapy
Persistent mild symptoms or moderate to severe symptoms – combination of psychological and drug therapy
1st line treatment usually SSRIs
2nd line switch to alternate SSRI
3rd line switch to different class (normally an SNRI)
Practical issues
Initiating an antidepressant can cause feelings of anxiety consider co-prescribing short course of benzodiazepines to counteract the anxiety
During the first few weeks of antidepressant treatment can have worsening suicidal thoughts with improved motivation so ensure counselling and regular reviews
Consider prescribing limited supply of meds to reduce chance of OD
Side effects often transient and improve with time
Caution when switching antidepressants – table of different half-lives and how to taper them
Treatment approach
If no response to 3 antidepressants, then check concordance, review diagnosis, and consider if social problems are maintaining depression
Consider augmentation – addition of drug to the current therapy
Mirtazapine – sleep
Quetiapine – mood
Aripiprazole
Lithium – mood stabiliser
Lamotrigine – mood stabiliser
Electroconvulsive therapy
Response
2-4 weeks usually for response to be seen (longer in elderly)
Improvement greatest during weeks 1-2
If no response during 2–4-week period, consider first increase in dosage then if again limited efficacy, then switch to alternative
Extended duration if treatment trial will lead to additional benefit in some
Differences between drugs
Mirtazapine, escitalopram, venlafaxine, and sertraline
more efficacious than
duloxetine, fluoxetine, fluvoxamine, paroxetine and reboxetine
Reboxetine less effective overall
Escitalopram and sertraline
better tolerated than
duloxetine, venlafaxine, fluvoxamine, paroxetine and reboxetine
Preventing relapse
Relapse rate 3-6 months post remission is 50% with no drug treatment
A/D treatment reduces absolute risk of relapse by about 50%
After 1st episode continue for 6-9 months
After 2nd episode continue for 12 months
After 3rd episode continue for 2 years
Insomnia – difficulty in getting to sleep or staying asleep long enough to feel refreshed the next morning
Causes
Recreational drugs
caffeine, nicotine, alcohol, cannabis)
Medicinal drugs
anticonvulsants, antipsychotics, b-blockers, SSRIs, MAOIs, steroids, decongestants, Alpha agonists and antagonists, narcotic analgesics
Drug withdrawal
from CNS depressants (eg alcohol, anxiolytics/hypnotics)
Physiological
Diet, late night exercise, shift work (night and evening work)
Environmental
Noise, bright lights, extremes of temperature
Medical conditions
Psychological - anxiety, depression, grief, stress
Non-psychological eg chronic pain, gastric reflux, asthma, sleep apnoea
Types of insomnia
Primary insomnia - insomnia not attributable to a medical psychiatric or environmental cause
Secondary insomnia- insomnia secondary to another condition
Transient (2-3 days) – caused by changes in routine (for eg. change in time zone, alteration of shift work)
Short term (<3 weeks) – may result from temporary environmental stress
Chronic insomnia (>3 weeks) –usually secondary to other conditions
Treatment
FIRST LINE IS ALWAYS NON-DRUG treatments e.g., lifestyle changes and CBT
Drug therapy – Hypnotics
Benzodiazepines
Benzodiazepine-like drugs (Z-class)
melatonin
BEFORE hypnotic is prescribed the cause of insomnia must be established and where possible, underlying factors should be treated
NICE recommends
if hypnotic medicine is the appropriate way to treat one for only short periods of time and strictly according to the licence for the drug. (Usually, 1-2 weeks and max 4 weeks) and should be prescribed on a weekly basis
Benzodiazepines
Most benzodiazepines
decrease time taken to get to sleep
in individuals who habitually sleep <6hr, the drug increases duration of sleep
Few short-acting BDZs recommended for insomnia (short-term treatment – max 2-4 weeks)
Should only be used when SEVERE, DISABLING or causing EXTREME DISTRESS
Benzodiazepine – like drugs
Z -Hypnotics – Zaleplon, zopiclone, zolpidem (Short acting – t1/2 < 8 hr)
Short term use only (2-4 weeks)
Lack of anxiolytic effects –drowsiness or dizziness - just induce sleep
Melatonin treatment
Prolonged release melatonin available for primary insomnia in over 55yr olds (can be used up to 3 weeks)
Antihistamine gen 1 – can cause drowsiness
Anxiolytics
Kalms, Kalms day, Karma, Karmamood, Potters Newrelax, Relaxherb, Stressless
Hops, valerian, passionflower, passiflora, vervain, St John’s Wort
Sedatives
Kalms night, Kalms sleep, Dormesean, Niteherb, Nytol herbal, Potters Nodoff, sominex herbal
Hops, valerian, vervain, skullcap, wild lettuce, passiflora
Some herbal remedies do contain active ingredients so be careful of interactions
Lifestyle changes – promote sleep hygiene
establishing fixed times for going to bed and waking up
trying to relax before going to bed
maintaining a comfortable sleeping environment avoiding napping during the day
avoiding caffeine, nicotine, and alcohol late at night
avoiding exercise within four hours of bedtime
avoiding eating a heavy meal late at night
avoiding watching or checking the clock throughout the night
using the bedroom mainly for sleep if possible
avoid going on phone, looking at screens immediately before bed or whilst in bed
ADHD
Persistent developmentally with inappropriate levels of over reactivity, inattention and/or impulsivity
Diagnosis – based on observation there are no biomed tests
Symptoms – 9 symptoms across 2 domains
Hyperactivity/impulsivity
Inattention
Can be combined type or dominant in one
ADHD – Predominantly inattentive type
Fails to give close attention to details or makes careless mistakes.
Has difficulty sustaining attention.
Does not appear to listen.
ADHD – predominantly Hyperactive/impulsive type
Fidgets with hands or feet or squirms in chair.
Acts as if driven by a motor.
Blurts out answers before questions have been completed.
Difficulty waiting or taking turns.
Interrupts or intrudes upon others.
ADHD – Combined type
Patient meets both sets of inattention and hyperactive/impulsive criteria
ADHD – Differential diagnosis
Sensory impairment – leading to under or over-sensitivity to triggers
Epilepsy and related states – could present as inattention
Effects of head injury
Acute or chronic medical illness
Poor nutrition – linked to poor behavior – not directly linked to ADHD
Sleep disorders – linked to poor behavior – not directly linked to ADHD
Side effects of medication
School or classroom difficulties – bullying or other factors
Large links to exposure to smoking and drinking during pregnancy, childhood illness such as meningitis or other viral infection, low birthweight/prematurity. HIGH heritability
Treatment
Mild-moderate –1st line - parent-training/education programmes with parent and child, group based or individual sessions. Teachers receive ADHD training and offer intervention in schools.
2nd line – CBT or social skills training
3rd line – DRUG THERAPY ONLY FOR SEVERE and should be offered along with psychological, behavioural, and educational interventions
Drug therapy
Methylphenidate – generally first choice
Atomoxetine - if other tics, Tourette's syndrome, anxiety disorder, stimulant misuse or risk of stimulant diversion are present
D-amphetamine – ONLY if other drugs ineffective at raised doses – CD2 high risk in addiction and dependence and misuse so used as last resort
Decide which drug treatment to use based on:
their different adverse effects
potential problems with compliance (for example, if a mid-day dose is needed at school)
potential for drug diversion (taken by others) and misuse
preferences of the child or young person and their parent or carer
When a decision has been made to treat children or young people with ADHD with drugs, healthcare professionals should consider: –
methylphenidate for ADHD without significant comorbidity
methylphenidate for ADHD with comorbid conduct disorder
methylphenidate or atomoxetine when tics, Tourette’s syndrome, anxiety disorder, stimulant misuse or risk of stimulant diversion are present
atomoxetine if methylphenidate has been tried and has been ineffective at the max dose, or the child intolerant to low or moderate doses of methylphenidate.
Atomoxetine
Closely observe children or young people taking atomoxetine for agitation, irritability, suicidal thinking, and self-harming behavior, particularly during the initial months of treatment, or after a dose change.
Liver damage in rare cases (usually presenting as abdominal pain, unexplained nausea, malaise, darkening of the urine or jaundice).
Treatment of adults
In adults, methylphenidate normally first line treatment
Consider atomoxetine or dexamphetamine if symptoms do not respond to methylphenidate or the person is intolerant to it ~6 weeks.
Selection of appropriate medication
Immediate-release preparations if more flexible dosing is required or during initial titration to using methylphenidate, consider determine correct dosing levels
If there is a choice of more than one drug, use the drug of lowest overall cost
modified-release preparations for convenience…
their pharmacokinetic profile,
improving adherence,
reducing stigma (because the drug does not need to be taken at school)
reducing problems of storing and administering controlled drugs in schools
abuse liability
AUTISM
Symptoms
Socialization
Impaired use of non-verbal behaviors to regulate interactions
Delayed peer interactions, few or no friendships, and little interaction
Absence of seeking to share enjoyment and interests
Delayed initiation of interactions
Little or no social reciprocity and absence of social judgment
Communication
Delay in verbal language without non-verbal compensation (gestures)
Impairment in expressive language and conversation, and disturbance in pragmatic language use
Treatments
NEED early diagnosis and defined biomarkers
Currently intervention is through family and educational support
Only some specific programs have an evidence base
Aim is to ‘improve the functional status…through skill acquisition in core areas’
Eg developing relationships
Achieving social and environmental milestones through play
Positive reinforcement of social communication
Pharmacological treatments for co-morbidities
Developmental
Hyperactivity/impulsivity (see ADHD)
Psychiatric
SSRIs, other antidepressants for depression
atypical antipsychotics for OCD
SSRI or a2 agonists for anxiety
Behavioural
Atypical antipsychotics (irritability, aggression)
Sensory
Neurological
anticonvulsants and fits, a2 agonists for tics
Gastrointestinal
Sleep disruption
melatonin and clonidine
Dementia
Symptoms –
Higher cognitive function affected
Memory, thinking, comprehension, learning capacity, language (speaking and understanding it)
Daily living activities/emotional behaviour (non-cognitive symptoms)
Behavioural and psychological symptoms of dementia (BPSD) – include agitation, apathy, depression, anxiety, delusions, hallucinations, irritability, and wandering
Treatment -
Acetylcholinesterase (AChE) inhibitors (donepezil, galantamine, and rivastigmine) — as monotherapies for managing mild to moderate Alzheimer's disease.
Memantine (a N-methyl-D-aspartic acid receptor antagonist):
As monotherapy for managing Alzheimer's disease for people with moderate Alzheimer's disease who are intolerant of, or have a contraindication to, AChE inhibitors, or for people with severe Alzheimer's disease.
In addition to an AChE for people with established moderate or severe Alzheimer's disease who are already taking an AChE
For people with non-Alzheimer's dementia the use of AChE inhibitors or memantine is unlicensed, but they may be prescribed by a specialist for people with:
Mild to moderate dementia with Lewy bodies:
Donepezil or rivastigmine are recommended first line.
Galantamine is an option if donepezil and rivastigmine are not tolerated.
Severe dementia with Lewy bodies:
Donepezil or rivastigmine are recommended.
Vascular dementia:
AChE inhibitors or memantine are options if the person has suspected comorbid Alzheimer's disease, Parkinson's disease dementia, or dementia with Lewy bodies.
Risperidone and haloperidol are the only antipsychotics licensed for treating non-cognitive symptoms of dementia, although other antipsychotics are often prescribed off-label for this purpose.
Acetylcholinesterase inhibitors
NMDA receptor antagonist
Cholinesterase inhibitors for mild to moderate AD (eventually stop working)
NMDA receptor antagonist for severe AD and moderate AD in some cases
Treatment must be started only by a specialist clinician
Rheumatoid arthritis
Inflammatory disease causing persistent symmetric joint synovitis
Presents as pain and joint stiffness with heat and swelling progressing at rest and after periods of inactivity with malaise, fatigue, fever, and weight loss
Risk factors – smoking, eating large amounts of red meat, drinks excessive coffee
Symptoms
Joints
Pain
Swelling
Stiffness
Systemic
Fatigue, depression, irritability
Anaemia
Flu-like symptoms, such as feeling generally ill, hot, and sweating
Pain worse in morning
Treatment
Drugs, mild exercise (enhance flexibility of joint and muscle strength), lifestyle changes (rich antioxidant diet, no smoking)
Main types of RA meds
NSAIDs (short term symptomatic relief) – reduce inflammation. OTC (ibuprofen, naproxen). POM (celecoxib, etoricoxib)
S/E – GI irritation, ulcers (use at lowest dose and take with food, use PPI to lessen effects)
Caution – asthmatics and renal impairment and patients with increased CV risk
Disease-modifying anti-rheumatic drugs (DMARDs) – 1ST LINE for active RA (methotrexate, sulfasalazine)
S/E – Nausea, diarrhoea, oral ulceration, alopecia, cough, SOB, bone marrow suppression – CAN BE REDUCED by co-prescribing FOLIC acid 1mg daily
Biological therapies (type of DMARD) – used when DMARDS don’t control RA
Glucocorticoids – short term treatment when starting new DMARD for rapid symprom control - also used in flares
Analgesics (painkillers)
Drug Treatment Schedule
Start two DMARD regime once diagnosed, using titration regimens
Use anti-inflammatories (NSAIDs), paracetamol with or without corticosteroids until effective
Review after 6 months: increase dose or switch as clinical condition determines.
Patient counselling in RA
Place of drugs in therapy
Onset of action
Side effects
Immunosuppression
Regular painkillers
Regular monitoring including blood tests
Dexterity aids, prescription services
Osteoarthritis
Predominantly non-inflammatory and caused by cartilage loss from synovial joints and bone remodelling due to excessive and repeated overloading on weight bearing joints or stress of a joint over tome and specific injuries
Risk factors – genetic, age, gender, obesity, damage, occupational, and stress
Symptoms
Pain – tends to be worse when using the joint and at end of the day (Worsens on use, resolves at rest)
Stiffness – feel stiff after rest, usually wears off as you get moving
Grating or grinding sensation (crepitus) – joints creak or crunch as you move
Swelling – may be caused by osteophytes (bone outgrowth) or caused by synovial thickening and extra fluid
Muscles around joint look thin/wasted
Unable to use joint normally – doesn’t move as freely or far as normal
Joints give way – muscles have weakened, and joint is less stable
Management
Provide information on sources of advice and support
Advice on self-care strategies such as;
Weight loss, local muscle strengthening exercises and aerobic fitness training
Appropriate footwear, local heat, or cold packs
Odder psychosocial support – career and occupational health assessments if needed
Advice on simple analgesia
Arranging regular reviews to assess response to treatment
MANAGEMENT GOAL – pain reduction and symptomatic relief
First line:
Paracetamol regularly – 4g daily
Topical NSAIDs
Additional treatment:
Oral NSAIDs– not first line
-Start with ibuprofen
-Monitor for side effects
-Possible place for topical therapy
Topical capsaicin – adjunct and helpful in knee and hand – works by stimulating then decreasing the pain sensation
Corticosteroid injection: â pain and inflammation of flare-up
Role of pharmacist
Counselling:
dosage regimen
side effects
warnings
Monitoring for side effects
Weight loss advice
Physiotherapy advice
Compliance aids & living aids
Gout
Type of inflammatory arthritis – causes severe pain and damage to joints
Caused by abnormal high levels of uric acid in blood which deposits urate crystals in joints and tissue
3 phases
Asymptomatic hyperuricaemia – can remain in this stage for life
Acute attack of gouty arthritis – can vary from months to years before another attack
Final period of chronic tophaceous gout – nodules effecting joints
Treatment
Acute
Ice
Rest affected joint
NSAIDs – short term, 7-14 days, high dose, for pain relief and anti-inflammatory
Colchicine (Dose: 500mcg 2-4 x daily until symptomatic relief or SE (stomach cramps, diarrhoea, vomiting)), steroids (used when NSAID and colchine is contraindicated or not useful)
Choice of drug dependant on comorbidities and renal function (NSAID cause fluid retention whereas colchicine doesn’t)
Colchicine use limited as it can have sudden toxicity at higher conc
Combination treatment can be used as well if monotherapy isn’t controlling the attack
Long term treatment to reduce urate
Lifestyle modifications (reduce dietary intake)
Drug therapy: Allopurinol (1st line – offer to all, 100mg od, increased in 100mg increments every 2-3 weeks) S/E – rashes
Febuxostat (2nd line only use when allopurinol intolerant or contraindicated – 60mg OD dose)
Monitor urate level – aim for < 360 μmol/L or 6 mg/dl (critical level)
Muscoskeletal
Sprain
Commonly ankle, wrist, thumb, knees – pain, swelling, tenderness, bruising, disabled use and no weight
Strain
Common in legs and lower back – pain, swelling, bruising, red, and reduced function
BOTH
Self-limiting gets better in 4-6 weeks and full recovery in 12 weeks
Non-pharma advice
PRICE (Protect, Rest (48-72hrs), Ice immediately after, Compression bandages and Elevate to reduce swelling
Reduce HARM (Heat, alcohol, running and massaging for 72hrs.
Avoid NSAIDs for 72hrs
Exercises for sprains
Gently move joint in all directions to increase and maintain flexibility (lack of movement can delay recovery BUT severe sprains with complete lack of movement rest for 10 days first)
Treatment – topical and oral analgesics
Refer – severe pain, possible break or fracture, no alleviation with OTC meds
Lower back pain
Symptoms – pain, tension, soreness, stiffness without underlying cause
6 weeks usual recovery can be up to 12 weeks
Advice
Back exercises, improve posture, yoga, avoid lying or sitting for too long, remain active.
Sleep in different positions, pillows between legs, under knees, hot baths, hot water bottles, ice packs.
Treatment
OTC – topical analgesics or co-codamol if still painful
Refer
No improvement in 3 days, continues for more than 6 weeks, pain travels higher, pain after injury, younger than 20, older than 50, pain affects sleep, unsteady on feet, unexplained weight loss
EMERGENCY
Pins and needles in back, genital, bum, both legs, lose urine or bowel control
Conjunctivitis
Symptoms
Bacterial
Viral
Allergic
Eyes affected
1 or 2
Both
Both
Discharge
Pussy
Watery
watery
Sensation
Gritty
Gritty
Itchy
Co-presenting symptoms
None
Cough/cold
Rhinitis
If pussy, red or gritty it is contagious – allergic ISNT contagious
Advice
Don’t wear contacts, hold cold flannel on eyes for few mins to cool them, use FBC water to gently wipe lashes and clean off crust and clean with cotton wool pad. Use a different one for each eye
Control spread by – reg wash hands with hot soapy water, cover mouth and nose when sneezing, don’t share towels or pillows and don’t rub eyes
Refer
Baby less than 28 days old with red eyes, allergic reaction, or spots on eyelids. For all – symptoms not resolved after 2 weeks
111 - Severe pain, sensitive to light, sudden changes to vision
Treatment
Viral – self-limiting, use hygiene and non-pharma advice
Allergic – Opticrom eye drops (Adults and child – 1-2 drops in each eye up to 4x daily)
Bacterial – over 2, chloramphenicol drops/ointment (Optrex Bacterial Conjunctivitis 1%w/w Eye Ointment) - apply a small amount of ointment in the affected eye 3-4 times daily for 5 days
Blepharitis
Symptoms
NOT contagious, rims of eyelids are inflamed, burning, soreness or stinging in the eyes, crusty lashes that stick together, itchy eyelids
Advice
Clean eyelids at least 1x daily, clean eyes even if symptoms clear, don’t wear contacts, or eye makeup
Cleaning eyes – soak a clean flannel/cotton wool in warm water and place on eye for 10 mins, gently massage eyelids for 30 secs, clean lids using cotton wool. Baby shampoo at 10:1 ratio good.
Refer
No improvement after 2 weeks of cleaning eyes
Treatment OTC
Brolene eye drops – 1-2 drops in each eye up to 4 x daily. If not better in 2 days refer
Dry eyes
Symptoms
Dry feeling, sensation of something in eye, burning, grittiness, itching, light sensitivity, over-blinking, redness, excess tears (randomly tearing)
Causes – over 50, contacts, digital screens, AC, windy/cold/dry/ dusty environment, smoking, alcohol, meds (antidepressants/BP) medical conditions (blepharitis)
Refer
Treatment failure after 2 weeks, change in eyelid shape
111 – severe pain and red, contact wearer with red eyes (could be an infection)
999 A&E – sudden change in sight, bursts of light sensitivity, severe headache/nausea, dark red eyes, injured/pierced eye, something stuck in eye
Advice
Clean eyes daily, take breaks when using screens, use screens below eye level, use humidifier, wear glasses instead of contacts
Treatment
Light lubricant – Optrex Double Action Drops for Dry and Tired Eyes - Apply 1-2 drops in each eye.
Hyaluronic Acid - Artelac Rebalance Drops, long lasting relief - Place 1 drop into the conjunctival sac 3-5 times daily or more frequently if required.
Hypromellose drops – 1-2 drops 3 x daily
Excessive ear wax
Symptoms – hearing loss, earache, noise/ringing, vertigo, dizziness, and nausea
Causes – narrow/damaged canals, hairy canal, skin condition affecting scalp around ear, inflammation of ear canal
Refer – not cleared in 5 days, badly blocked, severe, complete loss of hearing, likely infection
Advice – don’t use fingers or cotton buds to remove wax
Treatment
Olive oil drops – 2-3 drops in affected ear and massage around outside of ear BD x 7 days
Use dropper when lying down with head to one side to allow oil into ear, over 2 weeks then lumps should fall out, but symptoms should be better within 5 days
Otitis externa
Symptoms - pain, discharge, itch, irritation, external ear/canal appears red, swollen, eczema, deafness, skin swells, tender to touch
Refer – ear pain in children, inflamed pinna, unsuccessful treatment (after 4 days), hearing aids, excessive discharge (wax or pus), high fever, vomiting, fatigue, confusion, dizzy, stiff neck, rash, slurred speech, fits, light sensitivity
Advice – avoid under/over dressing feverish child, lower heating, offer regular fluids, avoid dummies when lying flat, give paracetamol/ibuprofen if child is unwell/distressed (not together)
Treatment
Acute localised (furunculosis) – infected hair follicles in outer-ear causing swelling and irritation
Treatment – hot flannel, oral analgesics, antibiotics if severe
Acute diffuse (over 3 months – more widespread inflammation of skin, bacterial/fungal infection or contact dermatitis due to irritant/allergens
Treatment – earwax plus or EarCalm
Otitis media
Symptoms – earache, discharge, hot, irritable, sleeplessness, ear pulling/rubbing, crying, temporary deafness
Refer – recurrent infections, no improvement in 3 days
Treatment
Self-limiting should be better in 3 days, single analgesics for pain
Hyperthyroidism
Too much thyroid hormones produced naturally
Symptoms
Tremor, warm sweaty palms, weigh loss despite increasing appetite, heat intolerance, diffused alopecia, hair thinning, tachycardia, diarrhoea
Advice
Healthy diet with foods rich in antioxidants, green leafy vegetables (broccoli, cabbage etc)
Vitamin D, omega 3 fatty acids and calcium rich foods. Smoking cessation
Treatment
Carbimazole (adjunct B blocker propylthiouracil for adrenergic symptoms) – block and replace regime
Combo of fixed high dose carbimazole and levothyroxine
Radioactive iodine destroys thyroid cells, surgery to remove some thyroid
Hypothyroidism
Thyroid gland doesn’t produce enough hormones caused by immune system attacking thyroid gland and damaging ait or by damage to thyroid that occurs during treatments for a hyperthyroidism or thyroid cancer
Symptoms
Fatigue, muscle pain, weakness, weight gain, sensitive to cold, dry skin, brittle hair, nails, depression, reduced libido
Advice
Eat antioxidant rich food, seeds and nuts, tyrosine (meat, dairy, legumes)
Avoid – soy, iodine rick food, leafy green vegs, caffeine, alcohol – quit smoking, alcohol.
Inform GP if pregnant (needs treatment and monitoring during)
Treatment
Levothyroxine 1st line – dose depends on blood test and progression – take tablet at same time every day (MORNING) If taking too much causes sweating, chest pain, headaches, diarrhoea, vomiting. Supressing thyroid supressing hormone with high doses causes atrial fibrillation, stroke, osteoporosis
Cold sores
Symptoms
Simplex - Pain, burning, itching, tingling before lesions and lasts 6-48 hrs
Crops of vesicles burst and crust over and heal, commonly on lower lip and ends of mouth
Gingivostomatitis – fever, malaise, sore throat, painful nodules in cervix or under jaw, excessive salivation. Painful vesicles on a red swollen base that rupture to form ulcers inside mouth, covered with yellow/grey membranes
Refer – immunocompromised, unable to swallow, risk of dehydration, severe infection, complication, pregnant, recurrent
Treatment
Paracetamol/ ibuprofen for symptoms
Topical acyclovir/penciclovir OTC – use from onset of symptoms before lesions until lesions heal
OTC topical anaesthetic or analgesics, mouthwashes, or lip barriers – topical analgesics aren’t licensed in children
DON’T prescribe oral antiviral for healthy people
Consider prescribing oral antiviral for healthy people with episode of primary oral herpes simplex, recurrent labialis if lesions are severe, frequent, or persistent and recurrent
And for those who are immunocompromised
Should take at onset and until lesions have healed – minimum of 5 days
Choice of aciclovir or valaciclovir based on preference, dose, regimen, and adherence
Advice
Reassure its usually self-limiting and heals without scarring
Adequate fluid intake
Offer leaflets or websites for more info
Avoid kissing, oral until lesions fully healed, don’t share pillows, makeup, or lip balms. Don’t touch lesions other than when applying treatment – dab instead of rubbing. Wash hands after touching.
Athletes foot
Interdigital — most common; affects the lateral toe web spaces first; usually caused by Trichophyton rubrum.
Moccasin or dry — diffuse chronic scaling and hyperkeratosis affecting the sole and lateral foot; usually caused by Trichophyton rubrum.
Vesicobullous — least common; multiple small vesicles and blisters mainly on the arches and soles of the feet; usually caused by Trichophyton interdigital.
Risk – hot, humid, occlusive footwear excessive sweating, contaminated surfaces, immunocompromised
Advice
Wear well fitting, open footwear that keep feet cool and dry, replace old shoes that may be contaminated. Maintain good foot hygiene – wear different pair of shoes every 2-3 days. Wear cotton, absorbent socks, don’t scratch skin, after washing feet dry then well and between toes, don’t share towels and wash towel freq.
Treatment
Topical antifungal cream in mild, non-extensive disease
Terbinafine 1% cream (12 and over – apply thinly to affected area 1 or 2 daily for 7 days) or clotrimazole 1% cream (2-3 times daily and continue for 4 weeks minimum) okay for kids – OTC for some ages
Additional mild topical corticosteroid if there’s inflammation
Hydrocortisone 1% cream (OD for max 7 days)
Adult severe or extensive – oral antifungal with confirmed fungal infection
1st choice – terbinafine (250 mg once daily for 2–6 weeks, depending on the severity of infection)
2nd – itraconazole, Griseofulvin if not tolerated or contraindicated
Refer
Treatment failure, severe pain, got, painful and red (indicative of serious infection), infection spreads, diabetic patient, immunocompromised
Warts and verrucae
Warts – small, rough growths caused by infection of skin with HPV, form anywhere on skin most commonly on hand and feet
Verruca – (plantar wart) wart on sold of feet
Spread by direct contact, occur and clear spontaneously at any time or may take years
Common warts are firm and raised with a rough surface that resembles a cauliflower (common on knuckles, knees, and fingers).
Periungual warts are common warts around the nails that can be painful and disturb nail growth — nail biting is a risk factor.
Plane warts are usually round, flat-topped, and skin coloured or greyish yellow (common on the backs of hands).
Filiform warts have a finger-like appearance and may have a stalk (more common on the face and neck).
Palmar and plantar warts grow on the palms and the soles of the feet (verrucae). They often have central dark dots (thrombosed capillaries) and may be painful.
Mosaic warts occur when palmar or plantar warts coalesce into larger plaques on the hands and feet.
Not harmful and don’t come with symptoms and resolve with treatment
Advice
Reducing transmission and limit spread, keep feet dry, wear slippers or waterproof plaster in shower and communal areas. don’t share towels, socks, shoes. Don’t scratch lesions, bite nails or suck fingers with warts
Refer
Painful, facial, uncertain diagnosis, immunocompromised, extensively infected
Treatment
Only treated if painful, cosmetically unsightly, or patient request and persistent as the treatment is long and can have side effects.
Topical salicylic acid – up to 12 weeks
Duofilm® (salicylic acid 16.7% plus lactic acid 16.7%) — licensed for plantar and mosaic warts.
Bazuka® extra strength gel (salicylic acid 26%) — licensed for warts and verrucae.
Occlusal® (salicylic acid 26%) — licensed for common and plantar warts.
Salactol® (salicylic acid 16.7% plus lactic acid 16.7%) — licensed for warts, plantar warts, and verrucae.
Apply OD at night, file and soften area by soaking in warm water for 5-10 mins, peel of remaining film before administering next dose, don’t apply on healthy skin
Cryotherapy – every 2 weeks for max 6 treatments
Liquid nitrogen – only for older children and adults
Corns and calluses
Hard or thick areas of skin that can be painful
Corns – lumps of hard skin on knuckles and joints of toes
Callouses – larger patches of rough, thick skin
Both can be tender and painful
Refer
Diabetic, heart disease, circulation issues. Bleeding or puss, treatment failure after 3 weeks, severe pain
Advice
Wear thick, cushioned socks, wear wide, comfortable shoes with low heel and soft sole, use insoles or heel pads, soak corns and calluses in warm water to soften them, use pumice stone regularly or foot file to remove hard skin. Moisturise.
Don’t try to cut them, walk, or stand for long period, wear high heels or tight pointy shoes, go barefoot
Treatment
Heel pads and insoles, OTC products, pain relief
Carnation brand caps for both – adhesive dressing
Fungal nail infection
Caused by dermatophyte and non-dermatophyte moulds and yeasts
Symptoms
Discoloured, abnormal, small flaky white patches and pits on top of nail and becomes rough and eroded. Nail lifted, wite or yellow opaque streaks on one side of nail, scaling, thickening
Refer
Diabetic, severe, treatment failure, spread to other nails
Advice
Keep nails trimmed short and filed, don’t share clippers and files. Well-fitting shoes, cotton socks, maintain good foot hygiene, weak shoes in communal places, avoid nail trauma
Treatment
Not needed if patient not troubled by appearance and infection is asymptomatic
Advise antifungal treatment if – walking uncomfortable, distress, cosmetic, co-morbid complication, or complication
If dermatophyte or candida infection conformed – topical antifungal treatment 0f 50% of nail involved, 2 nails infected, contraindication to oral antifungal
Topical – amorolfine 5% mail lacquer – OTC apply 1 or 2 weekly to affected nail after gentle nail filing – 6 months minimum for fingernails, 12 months for toenails
If dermatophyte nail infection is confirmed:
Prescribe oral terbinafine first-line.
250 mg once a day for between 6 weeks and 3 months for fingernails, and for 3–6 months for toenails
Oral itraconazole if an alternative drug is indicated.
Prescribe as pulsed therapy 200 mg twice a day for 1 week, with subsequent courses repeated after a further 21 days.
If Candida or non-dermatophyte nail infection is confirmed:
Prescribe oral itraconazole first-line.
Prescribe as pulsed therapy 200 mg twice a day for 1 week, with subsequent courses repeated after a further 21 days.
Prescribe oral terbinafine if an alternative drug is indicated.
Prescribe 250 mg once a day for between 6 weeks and 3 months for fingernails, and for 3–6 months for toenails.
0 notes
Text
Comparing Sildenafil and Tadalafil: Understanding the Differences
Tadalafil and Sildenafil are used for the treatment of a medical condition called erectile dysfunction which is commonly called ED. However, these medicines are related to separate class of drugs on the basis of their specification and composition. We will see a detailed comparison of these medicines in this blog.
Classification
Tadalafil and Sildenafil are both linked to the class of PDE5 inhibitors, but there is a basic difference between their chemical compositions and also Tadalafil acts for a longer time as compared to Sildenafil.
Branding
Tadalafil – Sildenafil Citrate Dapoxetine HCL in USA medicine is known by the name of Cialis.

Sildenafil – The brand name of Sildenafil is popularly called Viagra.
Action
Whereas a Sildenafil Citrate Dapoxetine HCL in USA tablet reacts with the human body within thirty to sixty minutes of consuming, Tadalafil takes effect one to two hours after consumption and hence it lasts longer too.
Dosage
Sildenafil – Sildenafil Citrate Oral Jelly in California medicine is taken about 30 to 60 minutes prior to getting involved in sexual activity.
Tadalafil – Tadalafil Dapoxetine HCL in California tablet gives the choice to the user of taking it on a daily basis in the form of a lower dose or only consuming it an hour or two before getting involved in sexual activity.

Food Habits
Sildenafil – Users of this medicine must not take any meal containing high-fat as it may increase the time required for the medication to take effect.
Tadalafil – Unlike the Sildenafil tablet, food habits rarely affect the results and course of action of this medication.
Side Effects
The most common side effects for both of these medicines are digestive problems, nasal congestion, dizziness, headache and flushing. It should be noted that the severity of these side effects may vary from patient to patient on the basis of dosage and their body composition.
Dosage Available
Sildenafil is generally available in 25mg, 50mg and 100mg dosage tablets.
Tadalafil is easily available in 2.5mg, 5mg, 10mg and 20mg tablet form respectively.
Points to Remember
A patient must ensure that none of these medications is taken with other medicines like nitroglycerine because it may result in lowering the blood pressure severely and may prove to be fatal in rare cases depending on body composition of the user taking this pill.
It is always a good idea to consult with a physician about any previous medical condition or allergies before taking this tablet in order to ensure that there are no harmful effects of taking either of these medicines on the health of the user.
CONCLUSION
This blog is only designed to present an overview of these medicines in the present scenario. However, it is strongly advised that the patient takes these medications under direct supervision of a doctor or a certified medical practitioner to avoid any side effects from surfacing.
0 notes
Text
Unleash Your Fat-Burning Potential with ECA EXTREME from Swiss Pharmaceuticals
Are you ready to ignite your metabolism, crush cravings, and achieve your weight loss goals? Look no further than ECA EXTREME from Swiss Pharmaceuticals – the ultimate solution to help you torch stubborn fat and reveal your leanest physique yet. Let's dive into the key ingredients and why ECA EXTREME should be your go-to choice for maximizing fat loss:
Ephedrine HCl:
Ephedrine HCl is a powerful stimulant derived from the Ephedra sinica plant, known for its ability to increase metabolic rate, suppress appetite, and enhance energy levels. Ephedrine works by stimulating the central nervous system and increasing the release of adrenaline, leading to heightened alertness, focus, and physical energy. ECA EXTREME harnesses the fat-burning properties of ephedrine to help you achieve your weight loss goals more efficiently.
Dosage:
The recommended dosage of ephedrine HCl in ECA EXTREME typically ranges from 20-30mg per serving, taken orally. It's crucial to start with a lower dose and gradually increase it as needed, while always following the recommended guidelines to ensure safety and effectiveness. ECA EXTREME is typically taken once daily in the morning or early afternoon to avoid sleep disturbances.
Caffeine Anhydrous:
Caffeine anhydrous is a highly concentrated form of caffeine that provides rapid and sustained energy levels, making it a popular ingredient in fat-burning supplements. Caffeine works by blocking the action of adenosine, a neurotransmitter that promotes relaxation and sleepiness, leading to increased alertness, focus, and physical performance. ECA EXTREME combines ephedrine HCl with caffeine anhydrous to provide a synergistic effect that enhances energy and metabolic rate.
Dosage:
The recommended dosage of caffeine anhydrous in ECA EXTREME typically ranges from 200-300mg per serving, taken orally. It's best to start with a lower dose and gradually increase it as needed, while always following the recommended guidelines to ensure safety and effectiveness. ECA EXTREME is typically taken once daily in the morning or early afternoon to avoid sleep disturbances.
Aspirin (Acetylsalicylic Acid):
Aspirin is a nonsteroidal anti-inflammatory drug (NSAID) that helps reduce inflammation and improve blood flow. In the ECA stack, aspirin is included to enhance the effects of ephedrine and caffeine by prolonging their activity and preventing tolerance buildup. Aspirin also has mild blood-thinning properties, which may further enhance fat loss by improving circulation and nutrient delivery to muscles.
Dosage:
The recommended dosage of aspirin in the ECA EXTREME formula is typically low, ranging from 81-325mg per serving. It's best to start with the lowest effective dose and gradually increase it as needed, while always following the recommended guidelines to ensure safety and effectiveness. Aspirin is typically taken once daily with the ECA EXTREME capsule to maximize its synergistic effects.
Why Choose ECA EXTREME from Swiss Pharmaceuticals?
Maximized Fat Loss: ECA EXTREME combines the potent fat-burning properties of ephedrine HCl, caffeine anhydrous, and aspirin to maximize thermogenesis, increase metabolic rate, and promote fat oxidation. You'll experience accelerated fat loss and improved body composition, helping you achieve your weight loss goals faster than ever before.
Sustained Energy Levels: With its powerful blend of stimulants, ECA EXTREME provides sustained energy levels that keep you alert, focused, and productive throughout the day. Whether you're hitting the gym or tackling your daily tasks, ECA EXTREME will help you perform at your best and crush your goals with ease.
Appetite Suppression: ECA EXTREME contains ingredients that help suppress appetite and reduce cravings, making it easier to stick to your diet plan and control your calorie intake. You'll feel more satisfied and less tempted to indulge in unhealthy snacks, leading to better weight management and improved results.
Safe and Effective: Swiss Pharmaceuticals ECA EXTREME is manufactured in a state-of-the-art facility and undergoes rigorous testing to ensure purity, potency, and safety. It is formulated with high-quality ingredients and backed by scientific research, ensuring maximum effectiveness and minimal side effects.
Don't let stubborn fat stand in the way of your weight loss goals. Experience the power of ECA EXTREME from Swiss Pharmaceuticals and take your fat-burning efforts to the next level. Whether you're looking to shed a few pounds or completely transform your body, ECA EXTREME will help you achieve your goals and reach your full potential. Try it today and unleash the extreme fat-burning power within you.
"Stay ahead of the curve with our website's expert insights and industry updates."
0 notes
Text
Buy Phentermine Online
Phentermine Hcl is a generic prescription appetite suppressant to help patients lose weight. Phentermine Hcl is intended to help the patient eat less food while changing their food choices, modifying their behavior, and exercising more. The cash price of Phentermine Hcl is $39.66 for 30, 37.5MG Tablet, but with a Remedy Phentermine Hcl coupon, the price is $2.88. Remedy Pharmacy Phentermine Hcl coupons are accepted at many local pharmacies like Longs Drugs, Kroger, Harris Teeter, among others.
Here at Remedy Pharmacy 247 website we are going to educate you on just how effective Phentermine is and also introduce you to licensed online retail outlets where you will be able to buy your supplies of Phentermine 24 hours a day, and be guaranteed of a fast delivery of your order and bulk buy discounts are available.
Dosing information
Usual Adult Dose for Obesity:
8 mg orally 3 times a day 30 minutes before meals, OR
15 to 37.5 mg orally once a day before breakfast or 1 to 2 hours after breakfast.
Use: Short-term (a few weeks) adjunct in a regimen of weight reduction based on exercise, behavioral modification, and caloric restriction in the management of exogenous obesity in patients with an initial body mass index (BMI) of 30 kg/m2 or greater, or BMI of 27 kg/m2 or greater in the presence of other risk factors (e.g., controlled hypertension, diabetes, hyperlipidemia).
Usual Pediatric Dose for Obesity:
Age 17 Years and Older:
8 mg orally 3 times a day 30 minutes before meals, OR
15 to 37.5 mg orally once a day before breakfast or 1 to 2 hours after breakfast.
Tracking Number Available
Delivery takes 24 hours
Maximum 48 ours within USA & Canada
International delivery takes 3 to 4 working days world wide
0 notes
Text

This is a #prospective, #pilot, #open-label, #interventional, #comparative, randomized study, enrolled 60 patients with type 2 #diabetes mellitus (T2DM) to assess the effect of different doses of oral #vitamin B containing #Benfotiamine 300 mg versus intramuscular B vitamins containing watersoluble Thiamine HCl.
View more here: https://symbiosisonlinepublishing.com/endocrinology-diabetes/endocrinology-diabetes156.php
#scientificresearch #SymbiosisOnlinePublishing #InternationalJournal #Journals #Journal #ScientificJournal #openaccess #endocrinology #diabeteslife #diabetic #diabetologist #diabetescare #diabetessupport #Endocrine #diabeticlifestyle #sciencenews #scientificpublication #ScientificDiscovery #plasma #DiabeticPatients #Benfotiamine #immunesupport #ImmuneSystem #immuneboost #immunehealth #immunebooster
0 notes
Text
How Much Benadryl can I give my dog?

Have you ever heard about Benadryl? Have you asked yourself how much Benadryl can give your dog? are you tired of watching your furry friend suffer from allergies or discomfort? If so, you may be surprised to learn that Benadryl could be the solution you’ve been searching for.
While most people are familiar with Benadryl as a human medication, it can also be used safely and effectively for dogs. In this article, we will explore the various uses of Benadryl for dogs, including its dosage guidelines and potential side effects. By the end, you’ll have all the information you need to confidently use Benadryl to improve your dog’s quality of life.
What is Benadryl?
Benadryl is the brand name for the active ingredient diphenhydramine HCl. It is a medication that is used to treat allergies and other conditions. Diphenhydramine belongs to a class of drugs called antihistamines.
It is available over the counter (OTC) and in some pharmacies as a prescription drug. Benadryl is available in pet-approved forms, such as chewable tablets for dogs and oral syrups for cats.
Before knowing how much Benadryl to give your dog, you must know about the Safe Uses of Benadryl for dogs.
Use cases of Benadryl on dogs
Benadryl is a medication used to relieve symptoms of allergies and other conditions. There are many different uses for Benadryl in dogs, including:
Relief from itching and discomfort associated with fleas and tick infestation.
Swelling and inflammation.
Runny nose and coughing.
redness.
Asthma symptoms.
Some people also use it to treat anxiety or sleeping problems in their pets. Benadryl should not be used to treat severe health conditions or injuries and should only be given as directed by a veterinarian.
How Much Benadryl Can I give my Dog? – Finding the Right Dose
Finding the correct dose of Benadryl for your dog is essential, as too much can lead to serious side effects. Here are some tips for finding the right dose:
Start by checking your dog’s weight. Doses of Benadryl may be different depending on a dog’s weight.
Also consider your dog’s age and health condition. Younger dogs may need smaller doses than older dogs, and those with more severe health conditions might require higher doses of Benadryl.
Generally speaking, the dosages are as follows:
For dogs weighing less than 10 pounds, give them 1 mg of Benadryl per kilogram of body weight. One time a day.
For dogs weighing between 10 and 30 pounds, give them 2 mg of Benadryl per kilogram of body weight. Up to three times a day.
For dogs weighing more than 30 pounds, give them 4 mg of Benadryl per kilogram of body weight. Up to three times a day.
How Much liquid Benadryl can I give my dog.
In veterinary medicine, Benadryl is also given as a syrup or injection. The dosage instructions below are for dogs weighing 5 to 25 pounds.
For dogs over 25 pounds, give an adjusted dosage. Be aware that the absorption of liquid Benadryl is different than the tablet form.
For puppies and young dogs: Start with 1/4 teaspoon (2 milliliters) per 10 pounds (4 kilograms) of body weight once daily. This dose can be increased gradually as needed to achieve relief from symptoms. If your pet becomes very drowsy or falls asleep during the day, reduce the dosage until symptoms improve and resume the original dosage.
For older dogs: Start with 1/2 teaspoon (3 milliliters) per 10 pounds (4 kilograms) of body weight once daily.
Precautions when using Benadryl for your dog
Sometimes, a human-approved medication can be used instead of the vet-approved one. It is important not to rely on human dosage. It can be an overdose for your dog.
If you choose to use human Benadryl tablets or ointment, be sure to read the label first. Some of the products have different ingredients than those used in veterinary medicine and could cause serious side effects if given to a pet.
Ingredients like Decongestants and alcohol can be highly toxic for dogs.
Also, be sure to ask your pharmacist if the product you’re considering is approved for use in pets and humans.
It is essential to keep Benadryl away from the eyes and mouth of the dog. If it does come into contact with these areas, rinse immediately with water.
Benadryl should not be given to pregnant or nursing dogs.
Side effects of Benadryl on dogs.
Side effects of Benadryl on dogs
Benadryl can have side effects, some of which are listed below. Some dogs experience less serious side effects, while others experience more severe side effects. Benadryl can also interact with other medications, so you must talk with your doctor about any medications your dog is taking and whether they might interact with Benadryl.
Common side effects of Benadryl include drowsiness, dizziness, dry mouth, constipation, difficulty breathing, rapid heart rate, and hallucinations.
More serious side effects can include anaphylaxis (a severe allergic reaction that can cause respiratory failure), seizures, and coma.
If your dog has ever shown any signs of being out of balance – signs that may include vocalizing excessively, becoming overly active or restless, or displaying aggressive behavior – then it is essential to seek veterinary care as soon as possible. Benadryl can cause severe changes in a dog’s mood and mental state.
In conclusion, it is crucial to approach the use of Benadryl for dogs with caution and under the guidance of a veterinarian. The appropriate dosage depends on several factors, such as the dog’s weight, health condition, and specific symptoms. Giving an incorrect dose can lead to potential side effects such as drowsiness, dry mouth, or even more severe reactions.
It is always best to consult with a professional who can provide personalized advice and ensure your dog’s safety. Remember, when it comes to your beloved pet’s health, taking the necessary precautions is paramount.
ORIGINALLY FOUND ON-
Source: Poochamp(https://poochamp.com/how-much-benadryl-can-i-give-my-dog/)

1 note
·
View note
Text
Good Number Of Reviews Before Using Berberine

Berberine has become one of the most popular natural supplements for losing fat, because it is regarded an greatly reduce stomach fat more efficiently compared to slimming down alone. Additionally it is which is used to services middle overall health, reduced blood sugar level, in addition to revitalize your your metabolism. Berberine runs usually by trimming the hormone insulin weight as well as leading to AMP-activated meat kinase, the male body's metabolism professional move. This can possilby cholesterol together with blood pressure level.
Nevertheless, a few berberine nutritional supplements have been completely associated with stomach side effects like gas, bloating, and diarrhea. In case you are concerned with these complaints, find a liposomal berberine supplement applies natural phospholipid substances to secure any berberine as a result of nutrients and make it on the body meant for centered shipping. This unique supplement through Renue from Development makes use of this technology that is supported by technology to provide a concentrated however gentle blueprint.
Double Wood focuses on building easy effective vitamin supplements, and also their berberine is not an various. The product provides 500mg of pure berberine hcl in every ink container not to mention offers 2-4 capsules daily consumed four time separate by using meals. The organization offers totally free on the subject of all of the orders placed with a nice 30-day refund window, even though you may open up typically the bottles. The berberine right from Thorne is reached while in the United States at NSF and cGMP-certified facilities. It might be gluten-free not to mention vegan-friendly, with simply a fabulous hypromellose pill as well as calcium laurate while incorporated substances. You ought to notice that berberine shouldn't be fitted to pregnant ladies, now make sure you consult your medical professional ahead of this system. To know the particular area of one's best berberine supplement , individuals may well relate to the next backlink .
Barton Nutrition Berberine is surely an complex blood sugar levels help and support formula that could better the hormone insulin empathy and additionally will reduce associated with cholesterol. It really is 100 % natural ingredients are clinically analyzed to help you regulate type 2 diabetes not to mention increase your all around health. It provides a mixture of highly effective vitamins like milk thistle plus berberine to offer you long-term many benefits. It's non-gmo and gluten-free.
vimeo
Berberine can be described as chemical supplement found in vegetables just like Oregon grapes, forest turmeric extract, and also yellow closure. Many experts have utilized in traditional medicinal practises to relieve a range of sicknesses. Immediately, it’s obtainable in natural supplements and it is typically applied orally. Its a lot of well-known advantage is usually lowering blood glucose levels, but it can also help by using losing weight, in keeping with several scientific tests. It may possibly be mainly because it has an affect on the way the hormone insulin and also tummy micro organism communicate, as well as some research has revealed which often berberine decreases being hungry by way of boosting glucose levels control. Inside a investigation, berberine a lower hemoglobin A1c with clean defined people with diabates and even greater some other numbers in blood glucose manage, for example starting a fast carbohydrates and then triglycerides. What's more, it improved AMPK, a powerful enzyme which stimulates metabolism tracks and then markets healthy body mass. Greater may be to take a look here or even visit each of our standard web site to understand best berberine supplements.
0 notes
Text
HCL ORAL IS OVER I AM SO. SO. HAPPYYY cuz yay no more weighted assessments this term 🤩🤩
the teacher was so nice?? she kept smiling at me and laughed at my answers when it was meant to be funny is this a good sign please say yes
anyways time to start planning my new fic + study before my finals >:D
#ଘ(੭ˊᵕˋ)੭* ੈ✩‧₊ lei’s rambles#also i think i made a new friend after my oral#cuz there was a girl standing outside the exam hall and i was smiling and she asked me how it was#and we talked for a bit before i had to go#and on the way out of the school i saw her again and she told me she was skipping cca#AND I REALISED I DIDNT EVEN KNOW HER NAME OR HER CLASS JKSDHFSJKFH#i hope i meet her again :( she was so nice
0 notes
Text
How to draw human digestive system
The human digestive system starts with mouth and ends with anus. Intake of food into to mouth is called Ingestion.Mouth encloses a cavity within called Buccal cavity or Oral cavity. Three pairs of salivary glands pour their secretions called saliva in to this cavity. The muscular tongue pushes the food under grinding teeth as it mixes with saliva, this process is called "Mastication". Mastication makes the food into ball of paste. Salivary amylase" an enzyme in saliva starts the digestion of starch right away from mouth. As soft ball of food enters Oesophagus, the wavy movements (Peristaltic movements) drive the bolus into stomach. Oxyntic cells present in inner lining of stomach secrete Hcl acid which has killing action on Microbes and partially denatures the proteins in food.Slimy mucous secreted my mucous glands of stomach protect inner lining from self destruction due to acid. Gastric juices of stomach starts digestion of Proteins, lipids but not carbohydrates.
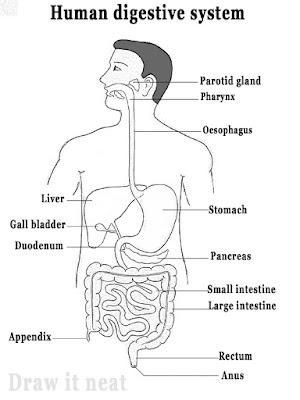
Human digestive system mainly have three parts to be drawn in proportion they are the Stomach, Liver and Intestines.Students feel difficult while drawing the duodenum, bile duct, Gall bladder and Pancreas in a narrow space. Even the coiled small intestines look complicated.Now, lets start drawing in easy steps.
Step 1:
Draw two parallel lines horizontally and two vertically as shown.
The middle box is for Stomach.
Step 2:
Draw Stomach as shown, ensure left side of stomach touches the left line. Accommodate Liver too as shown.

Step 3:
Draw bile duct opening into duodenum, represent overlapped part of liver on stomach with dotted lines
Draw pancreas below stomach as shown.
Step 4:
Draw large intestine along the guide lines as shown.
Step 5:
Draw folded patterns in large intestine as shown.

Step 6:
Draw a curve in the middle of large intestine.
Complete the man's face and now label the parts neatly.
0 notes
Text
Famotidine Pepcid For Dogs? What is that?
The generic name for the drug used to treat esophagitis, gastroesophageal reflux disease, and excessive stomach acid production is famotidine, also referred to as famotidine hydrochloride or famotidine HCl (GERD). It is one of the most often prescribed medications in the United States right now and is obtainable both on prescription and over-the-counter. Its brand names are “Pepcid®” and “Pepcid AC®,” respectively.
What Is Famotidine (Pepcid) Quick Facts?
Famotidine is a histamine receptor-2 (H-2) antagonist and an anti-ulcer medication. Gastric acid is secreted when H-2 receptors (targets) on the cell membranes of stomach cells are stimulated. The medication reduces the formation of stomach acid, giving the ulcer time to heal. Ranitidine (Zantac®), nizatidine (Axid®), and cimetidine (Tagamet®) are additional medications with comparable effects.
Famotidine works on the chemoreceptor trigger zone to reduce nausea in dogs.
Pets with stomach ulcers, esophagitis, gastric reflux, esophageal reflux, Helicobacter infections, and/or vomiting can be treated with Pepcid.
Famotidine may have a decreased effect when used regularly and continuously for an extended period of time, according to studies (more than 14 days). Due to this, it could be advised to take the medication twice daily.
Brand Names for Famotidine
Only using this medication for human use is registered and FDA approved.
Pepcid (Merck), Pepcid AC, and other brand names such as Act, Dyspep HB, Pepzan, Arfam, Pamacid, Peptris, Famotren, Famistine, and Fluxid are examples of human formulations.
Formulations for animals: none
Is Pepcid Routinely Prescribed to Pets?
Although the FDA has not approved this medication for use in animals, veterinarians may legally administer it as an off-label medication. Although famotidine is sold over the counter, it should only be used under a veterinarian’s supervision and direction. One of the 15 human over-the-counter medications that are deemed safe for dogs is Pepcid.
Famotidine Uses in Dogs
There are several uses for famotidine in humans, canines, felines, and other pets.
Gastric and intestinal ulcers or erosions are treated and prevented with the help of famotidine (shallow depressions in the stomach lining).

Treatment for stomach irritation brought on by kidney disease or kidney failure may involve the use of famotidine.
Mast cell tumors in dogs can create a lot of histamine, so famotidine or a comparable medication may be used to treat them.
Famotidine is sometimes administered to dogs that have diminished appetites and is used to treat a variety of causes of nausea in dogs. For more information on feeding a dog that won’t eat, click here.
Famotidine inhibits histamine, therefore it is occasionally used in conjunction with other drugs to treat allergic reactions, such as steroids or diphenhydramine (Benadryl®).
Numerous conditions that result in stomach issues, ulcers, or illnesses that induce nausea and vomiting are treated with famotidine. Examples include acute pancreatitis, inflammatory bowel illness, and infections like helicobacter or PetsCareTip canine parvoviral enteritis.
How Is Famotidine Supplied?
Both prescription and over-the-counter versions of famotidine are offered.
10 mg, 20 mg, and 40 mg tablets.
Oral powder for suspension is supplied at 50 mg/5 ml.
An injectable with a 20 mg/50 mL or 20 mg/2 mL concentration.
Dogs’ Pepcid Dosage
Never provide medication without first talking to your veterinarian. Before taking Pepcid for dogs, be careful to go through the right dosage and other safety measures with your veterinarian. Every 12 to 24 hours, a dose of 0.25 to 0.5 mg per pound (0.5 to 1.0 mg/kg) of famotidine is often administered. When used for longer than 14 straight days, the impact is lessened. Due to this, it could be advised to take the medication twice daily.
The ailment being treated, how the patient reacts to the medication, and if any negative side effects manifest themselves all influence how long the administration will last. Except as recommended by your veterinarian, make sure to finish the prescription. To prevent a sudden relapse, follow the entire treatment schedule even if your pet feels better.
Tablets should be kept at room temperature and away from light. Formulations that are liquids need to be chilled.
Famotidine Pepcid For Dogs and Potential Side Effects
If you see any of the following adverse effects and are worried that your pet may have consumed a hazardous dosage of medication, call your veterinarian right away:
Difficulty breathing.
Difficulty walking.
Lack of appetite.
Lethargy.
Pale gums.
Vomiting.
To be sure your pet is not exhibiting any of these signs, keep a close eye on them and pay attention to their behavior, urinating, and bowel movements. If you think your pet has swallowed a potentially hazardous amount of famotidine, call your veterinarian right away.
How to Avoid Unintended Exposure to Pepcid
It’s easy for curious animals to get into stuff, and it’s always preferable to avoid poisoning than to deal with it later. To prevent your pets from accidentally consuming a lethal dose of famotidine, take the following precautions:
All drugs should be kept out of pets’ reach.
Be especially careful when handling pill bottles and weekly pill organizers. The containers’ design and the noises they create when shaken can resemble toys, luring animals to play with or chew on them.
Avoid storing medications in plastic bags. Keep your prescription pills safe if you are traveling. Bags are simple to chew through and swallow.
If you have drugs in your purse, make sure to close it, hang it up, or place it somewhere your pet cannot get it.
Encourage visitors to keep their possessions locked up and their prescriptions out of the reach of your pets.
More Resources for Pet Emergency
Call the nearest emergency clinic if your pet ingests Pepcid and you are unable to reach your veterinarian. Calling a pet poison control hotline is an additional choice.
The two most common are:
FAQs About Famotidine for Dogs
What should I do if I forget to provide a famotidine dose?
Famotidine can be administered to your dog as soon as you remember to if a dose is missed. However, if it’s almost time for the next dose, only provide the standard dose rather than doubling it.
What is the most important thing I should know about famotidine?
Pepcid belongs to the “H2 blockers” class of pharmaceuticals, which also includes ranitidine and cimetidine (Tagamet) (Zantac). The amount of stomach acid produced is reduced with famotidine. The medicine is generally safe, and overdoses are rare. Pets include dogs, cats, and other animals are frequently prescribed Pepcid.
Before giving famotidine to my pet, what should I go over with my vet?
Before giving your pet any medication, you should talk to your veterinarian about the underlying problem. For instance, if your dog isn’t eating, you should talk about possible causes and come up with a solution. Additional symptoms include vomiting, diarrhea, lethargy, blood in the vomit or stool, and any other anomalies should be kept an eye out for.
Are there alternatives to famotidine?
Famotidine is a member of the “H2 blockers” class of drugs. Cimetidine and ranitidine are two further medications in this class that can also be used in dogs. Alternative medications with better stomach acid suppression include omeprazole, also marketed as Prilosec®. Treatment options for vomiting in dogs, such as cerenia, may be suggested based on their clinical symptoms.
Can you buy famotidine over-the-counter?
Famotidine is available over the counter in several sizes (10 mg is the most common).
What are contraindications to giving famotidine?
Use of famotidine in canines with renal and liver disorders should be cautious. Toxicity is a possibility because these organs process it. Having said that, famotidine is frequently advised, though some dogs may only need to take it occasionally or at a reduced dose.
Is it necessary to give Famotidine Pepcid For Dogs?
Famotidine is best administered without food and on an empty stomach.
What drugs interact with famotidine?
There are few medication interactions with famotidine. The pH change can, however, affect the absorption of other orally taken drugs because famotidine’s main action is to reduce gastric acid. Iron supplements and antifungal medications like itraconazole, ketoconazole, and fluconazole are among these medications.
To maximize famotidine absorption, cephalosporin antibiotics like cephalexin or cefpodoxime should ideally be administered two hours prior to or after. It’s normally advised to wait one hour between oral doses of different medications. The absorption of famotidine can be reduced by several antacids.
What is the difference between famotidine (Pepcid) and ranitidine (Zantac)?
Ranitidine (Zantac) and famotidine (Pepcid) are both members of the group of medications known as H2 receptor antagonists that inhibit histamine.
Source: PetsCareTip.Com
1 note
·
View note
Text
0 notes
Last Seen Blogs

emilyccfinds
Emily CC Finds

anderesich
nevermind.

arkhamsurviour
Straight Outta Arkham

khodipk
تعمیر خودی

sharesorrows
sharesorrows