#akinesia
Note
Hey there, do you have some cool sources on other types on involuntary movement that are not tics?
Yes, I do! Here is a list of involuntary movements, a simple description, and links to resources on them:
Akathisia -> an inability to remain still
StatPearls article
cleveland clinic article (very good)
Akinesia -> the loss of spontaneous, voluntary muscle movement
StatPearls article (free article)
healthline article
Athetosis -> slow, continuous, involuntary writhing movements commonly affecting arms and hands
healthline article
Chorea -> rapid, chaotic movements that seem to flow from one body part to another
NINDS article
StatPearls article
Dystonia -> sustained or repetitious muscular contractions; often produces abnormal posture
mayo clinic article
NINDS article
StatPearls article
Hemiballismus -> sudden, intermittent, flinging, or ballistic high amplitude movements commonly affecting proximal limb muscles
StatPearls article
Myoclonus → sudden, brief, involuntary muscle twitches
mayo clinic article
NINDS article
StatPearls article
Parkinsonism -> a clinical syndrome characterized by slowness, rigidity, tremor, and postural instability
StatPearls article
parkinson's disease vs parkinsonism
types of parkinsonism (parkinson's UK)
types of parkinsonism (parkinson's foundation)
Stereotypies -> repetitive, rhythmic movements with typical onset in early childhood
stereotypies in adults
medlink article
Tardive Dyskinesia -> uncontrollable and repetitive movements of the tongue, lips, face, trunk, and extremities
webmd article
Tics -> sudden, rapid, recurrent, and nonrhythmic movements or vocalizations
mayo clinic article on tourette syndrome
NINDS article on tourette syndrome
child mind institute article on tics and tourette
Tremor -> rhythmic back-and-forth or oscillating involuntary movements
NINDS article
classification of tremor
(at request I can find Tumblr or blog posts talking about personal experiences with some of these movements)
Basic definitions come from this article: https://www.psychiatrist.com/pcc/effects/drug-induced-abnormal-involuntary-movements-prevalence-and-treatment/
#asks answered#anon asks#involuntary movements#akathisia#akinesia#athetosis#chorea#dystonia#hemiballism#hemiballismus#myoclonus#parkinsonism#stereotypies#tardive dyskinesia#tics#tremor#links
17 notes
·
View notes
Text
5 notes
·
View notes
Text
Neurodegenerative Diseases
Neurodegenerative diseases are incurable and debilitating conditions that result in progressive degeneration and/or death of nerve cells.
- Parkinson’s Disease (PD)
- Alzheimer’s Disease (AD)
- Huntington’s Disease (HD)
- Amyotrophic Lateral Sclerosis (ALS)
Stephen Hawking lost control of his skeletal muscles due to ALS.
Parkinson’s Disease
Parkinson’s disease (PD) is a chronic, progressive, neurodegenerative disorder.
- First described by James Parkinson, an English doctor in 1817.
- Risk of PD increases with age, but an early-onset variant occurs before age 40.
Diagnosis
- neurological symptoms
- imaging tests
- reaction to anti-Parkinson’s drug L-DOPA
if symptoms improve with L-DOPA, then patient has PD.
- post-mortem examination of the brain
Symptoms
(A) Motor
- Tremor: The most visible outward sign of PD is a tremor that occurs when limbs are relaxed, but disappears with intentional movement.
- Rigidity: shuffling gait caused by rigid joints.
- Postural instability: Disorders of posture and impaired balance may cause patients to lean forward or backward when upright, and have stooped posture.
- Slowness of movement
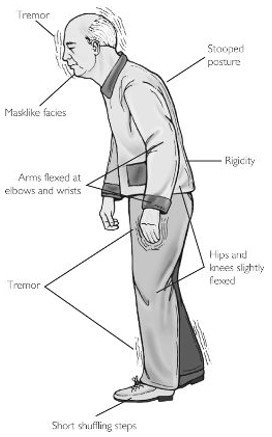
- Akinesia: difficulty initiating movement
- Involuntary movements
- Less movement of facial muscles: reduces the range of facial expressions possible. Many patients with PD are described as “stone-faced.”
- Speech disturbances: decreased speaking volume, and monotonous speech or uncontrollable acceleration of speech.
(B) Cognitive/Emotional
- Impoverishment of feeling, motive, and attention
- Cognitive slowing
- Possible/occasional anxiety
- Parkinson’s patients may also develop dementia (Parkinson’s disease dementia, or PDD). This is difficult to distinguish from comorbid Alzheimer’s disease (AD).
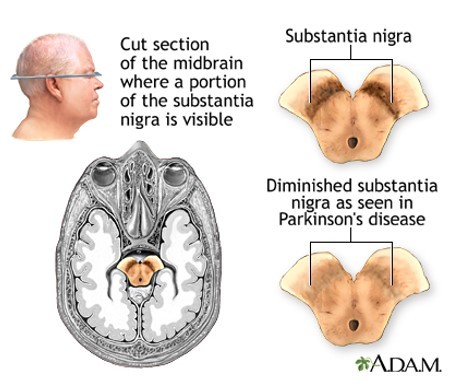
Post-mortem Examination
- A definitive diagnosis of PD is currently not possible until after death.
- Depletion of melanin due to the death of neurons in the substantia nigra in Parkinson’s disease is typically indicated by loss of brown color in this area.
- Microscopic examination reveals presence of Lewy bodies.
Brain Imaging
- A marker or test that reliably indicates PD in live patients would be useful for determining treatment options.
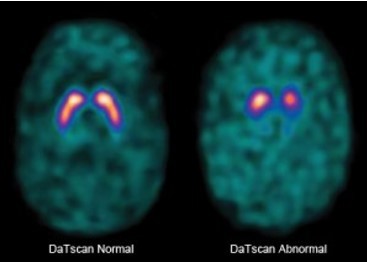
- DaTscan was approved by the FDA in 2011 for striatal dopamine transport visualization to assist in the evaluation of adult patients with suspected PD.
Unfortunately, this is prohibitively expensive, and dopamine transporter can be reduced in other neurological diseases, so the results are not conclusive.
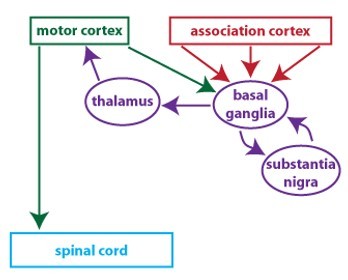
Pathophysiology
- Aside from the resting tremor, all motor symptoms are explained by loss of dopaminergic cells in the substantia nigra.
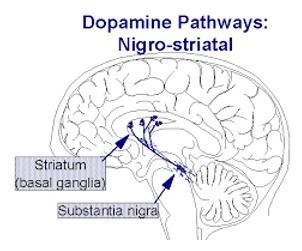
- As a result, there is insufficient amount of dopamine in the basal ganglia.
- Malfunction of the basal ganglia results in motor disturbances.
Several processes contribute to degeneration of neurons, including mitochondrial dysfunction, oxidative stress, inflammation, excitotoxicity, protein misfolding.
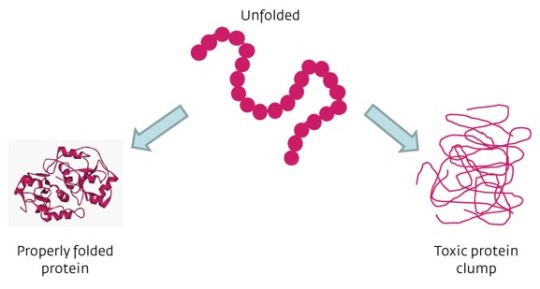
Protein Misfolding
- Protein folding is a physical process of the formation of a highly organized molecular structure, with a characteristic and thermodynamically stable conformation, by a polypeptide chain.
- In many neurodenerative diseases, proteins that do not fold properly (misfolded proteins) produce pathological changes in the brain.
- In PD, pathology is linked to misfolded a-synuclein.
- In healthy cells, a-synuclein mediates vesicle movement at axon terminals.
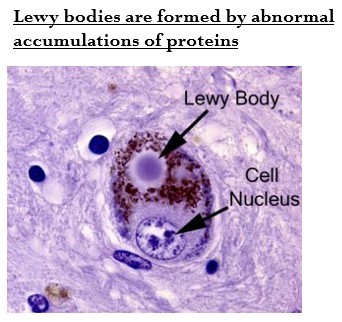
Lewy Bodies
Lewy bodies = dense, circular clusters (or aggregates) of protein within cells.
- They consist of a-snyuclein and other proteins.
- Misfolded a-synuclein molecules tend to aggregate and form Lewy bodies.
- They interrupt cell function and trigger apoptotic cell death.
- They can be detected during post-mortem examination of PD brain.
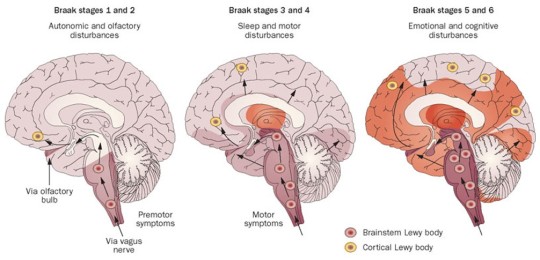
Spread of Parkinson’s Disease in the Brain
(1) Olfactory structures = sense of smell is lost.
(2) Brainstem nuclei: the raphe (serotonergic neurons) and locus coeruleus (norepinephrine neurons).
(3) Substantia nigra, amygdala = motor symptoms begin at this stage.
(4) Temporal cortex, premotor cortex
(5) Other sensory cortices, motor cortex
Etiology of Parkinson’s Disease
Although there are genetic and environmental risk factors, a definitive cause has not yet been discovered.
(A) Genetics
15% of PD patients reported an affected family member.
5-10% of PD cases are linked to known mutations.
(B) Aging
Due to an aging population, researchers project the number of people with Parkinson’s will double by 2040.
(C) Traumatic brain injury
Researchers looked at the medical records of >300,000 veterans and found that mild TBI increases risk of PD by 56%, while moderate to severe TBI increases risk of PD by 84%.
(D) Environmental factors
MPP+
1976: Bad batch of synthetic heroin (containing MPTP contaminant) produced “instant” Parkinson’s.
- MPTP is oxidized to MPP+ that damages dopaminergic cells.
- Paraquat is structurally similar to MPP+ and is currently used as an herbicide.
A known fast-acting inducer of Parkinson’s disease in primate brains
In 2011, a US National Institutes of Health study showed a link between paraquat use and Parkinson’s disease in farm workers.
Paraquat has been banned in the European Union since 2007. It can be used in the US with a license.
TCE
- Trichloroethylene, a solvent used to clean metals and remove stains, has exactly the same effect on human brains.
- It is still widely used and is detectable in high concentrations in groundwater.
- There have been many lawsuits about TCE groundwater and drinking water that’s been contaminated by industrial discharge.
Behavioral Treatments
physical therapy
exercise programs
speech therapy
Pharmacological Treatments
- drugs that increase dopamine response:
L-DOPA
Dopamine receptor agonists
MAO inhibitors
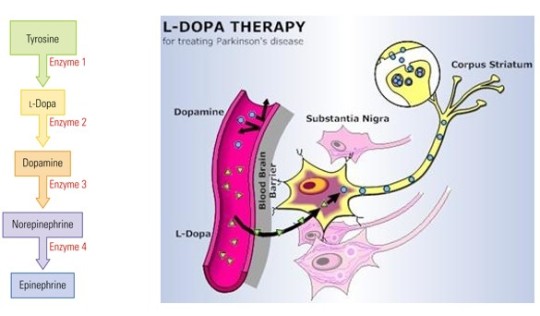
Levodopa (L-DOPA)
metabolite of the amino acid tyrosine
immediate precursor of DA in its metabolic pathway
L-DOPA can cross the blood-brain barrier, but DA cannot.
L-DOPA is extremely effective, compared to other DA agonists.
Side effects include motor fluctuations, dyskinesias, and unwanted movements (such as severe tics)
Other treatments are also aimed at increasing dopamine signaling in the brain.
- Dopamine receptor agonists bind to dopaminergic post-synaptic receptors in the brain, have similar effects to levodopa.
Bromocriptine, apomorphine
Side effects: impulse control disorders, such as compulsive sexual activity, compulsive eating, pathological shopping, and gambling
- Monoamine oxidase B (MAO-B) inhibitors prevent breakdown of dopamine (ex. Selegeline)
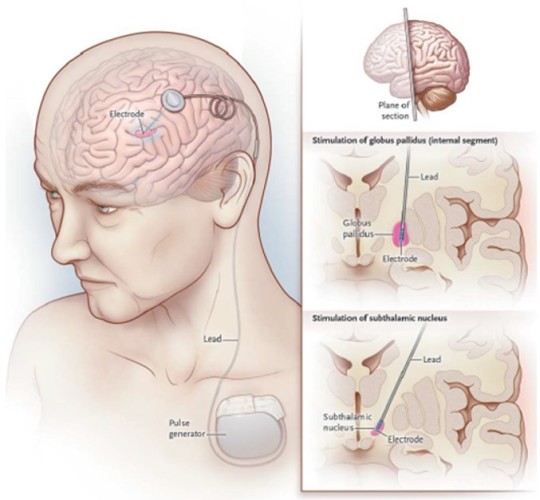
Surgical Treatments
These treatments reduce rigidity and tremor.
Lesioning of the basal ganglia
Deep brain stimulation of the basal ganglia
Stem Cell Treatment
Stem cells can be used in a lab to generate many other types of cells, including dopamine cells. Introducing new dopamine cells into the brain may help replace lost cells in PD.
October 2019: In Kyoto, Dr. Takahashi and his staff completed the first transplant into a human brain. They plan to complete six additional operations by 2022.
They used induced pluripotent stem cells (iPS cells) are derived from adult cells (usually from skin or blood) and can be manipulated to act like stem cells.
- In the US, Dr. Studer is about to move to clinical trials with dopamine cells derived from human embryonic stem cells.
Alzheimer’s Disease
Alzheimer’s disease (AD) is a chronic, progressive dementia disorder that is much more widespread than PD.
- Dementia is an acquired and persistent syndrome of intellectual impairment.
- Described in 1907 by Alois Alzheimer
- Due to aging population, cases of AD in United States are expected to increase.
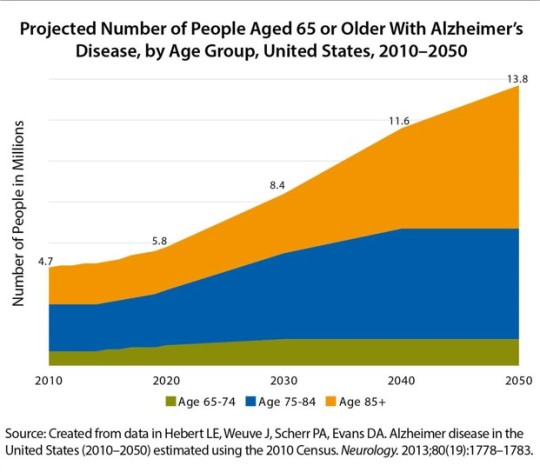
- Alzheimer’s is preceded by mild cognitive impairment (MCI).
- While all cases of AD are precede by MCI, not all cases of MCI develop into AD.
- As MCI progresses to AD, the first symptom is general forgetfulness, leading to progressive loss of memory.
Diagnosis
Neurological symptoms
Imaging tests
Post-mortem examination of the brain
Early Symptoms
Memory loss that disrupts daily life
Misplacing things and losing the ability to retrace steps
Challenges in planning or solving problems
Confusion with time or place
New problems with words in speaking or writing
Decreased or poor judgment
Withdrawal from work or social activities
Changes in mood and personality
Later Symptoms
Physiological problems: disrupted sleep, incontinence, and difficulty swallowing are seen
Psychiatric symptoms: delusions, hallucinations, depressed mood, and agitation (including violent outbursts)
Communication skills are diminished.
Advanced Stages
- Much of our sense of “self” comes from our memory and cognitive function, which is lost in those with advancing AD.
- AD will eventually take away completely the ability to use language, interact with or even recognize family and friends, or live independently.

- AD cannot be definitively diagnosed until after death. A histopathologic confirmation including a microscopic examination of brain tissue is required.
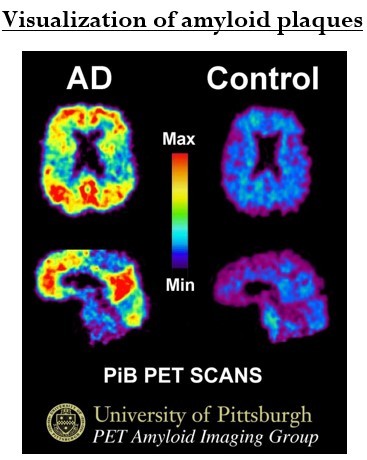
PET Scan with PiB compound
- Imaging of pathological A-beta protein with the help of Pittsburgh compound B can potentially help with diagnosis.
Etiology
Risk factors for AD include:
Advanced age
Family history of dementia or AD (1-5% genetic predisposition)
Obesity, untreated hypertension, high cholesterol, chronic stress, and sedentary lifestyle
Head trauma or hypoxic brain injury, depression, bipolar disorder, or PTSD
Environmental toxins (ex. aluminum)
Slow-acting viral infection
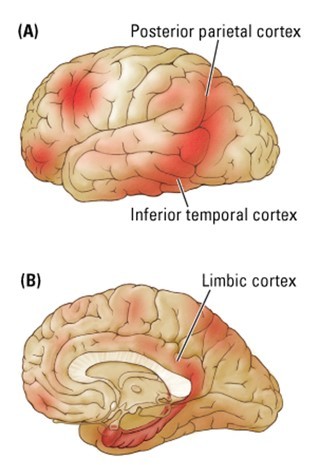
Cortical Degeneration
- Most heavily affected areas are the entorhinal cortex, some parts of the frontal cortex, hippocampus, inferior temporal cortex, and posterior parietal cortex.
- The primary sensory and motor areas are spared, as well as most of the brainstem, cerebellum, and spinal cord.
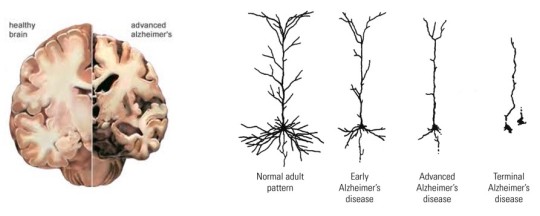
- Cerebral atrophy may be due in large part to the loss of dendritic arborization.
- A significant loss of synapses (up to 45%) may be the basis for the cognitive deficits.
- Cellular pathologies and neuronal cell loss in AD are associated with pathological formations in the brain:
Amyloid plaques (located in the extracellular space, also found in aging brains)
Neurofibrillary tangles (located inside neurons)
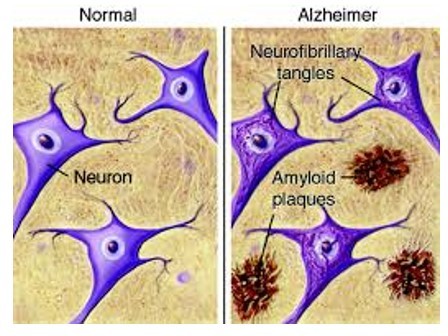
Amyloid plaques = fibrous deposits around neuronal cells
- A plaque has a core of beta-amyloid protein surrounded by abnormal processes (dendrites or axons), with microglial cells or reactive astrocytes on the periphery.
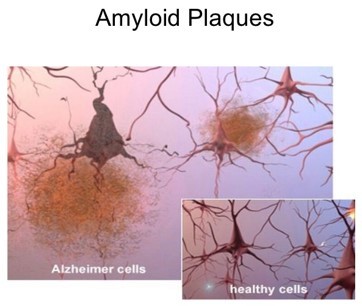
- Molecules of beta-amyloid protein (or A-beta) are pathologically misfolded and tend to aggregate.
- Protein misfolding is a pathology common for many diseases (e.g. Parkinson’s).
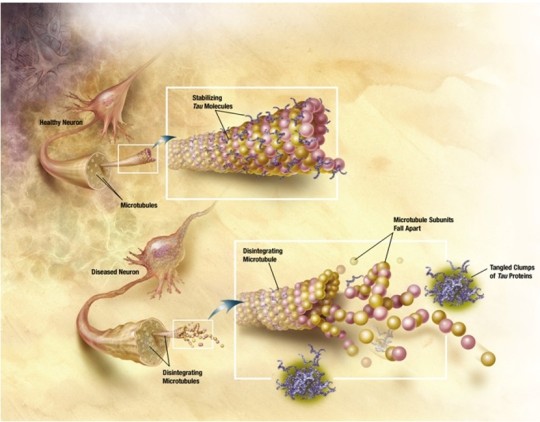
Neurofibrillary tangles (NFTs) = fibrous inclusions in neuron cytoplasm.
- Pyramidal neurons are particularly susceptible.
- The misfolded tau protein is the main component. Tau protein maintains the stability of axonal microtubules.
Treatments
- Currently, there are no available treatments that stop or reverse the progression of the disease, only treatments that help the symptoms.
(A) Behavioral/Lifestyle:
Mental stimulation
Physical exercise
Balanced diet
(B) Pharmacological:
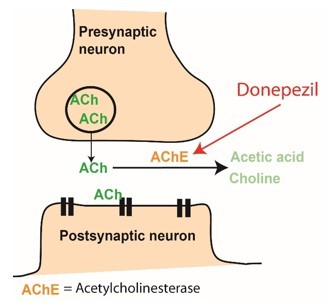
- Acetylcholinesterase inhibitors increase amount of acetylcholine in the synaptic cleft (Donepezil, tacrine, galantamine).
- NMDA receptor inhibitor (Memantine)
(C) Very New/Future Treatments
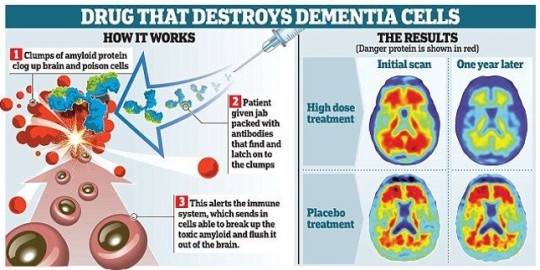
- Aducanumab (brand name Aduhelm)
cleared by the FDA on June 7, 2021
developed by biotech company Biogen in Cambridge, Mass
antibody therapy that targets amyloid plaques
first approved drug that treats a cause of the neurodegenerative disease, rather than just the symptoms
- Antibodies to A-beta
currently in clinical trials
Solanezumab is a monoclonal antibody being investigated by Eli Lilly as a neuroprotector for patients with AD. It failed in patients with moderate AD, but the trial for patients with mild AD (should have been) finalized in 2020. {note: if you know whether these trials were finalized, delayed, or terminated, let me know in the comments!}
- Drugs that block enzyme responsible for production of A-beta
September 2019: companies Biogen and Eisai announced termination of Phase 3 trial of Elenbecestat, another failure :(
- Antibodies to tau
currently in animal studies (preclinical phase)
Antibodies could decrease levels of phosphorylated tau proteins in mouse brains.
2 notes
·
View notes
Photo
2011-04-30
我當時是CR, 那一天很忙很忙,值班CV1, 從早到晚都在接全院的照會電話,這個奶奶是病房在治療UTI and DKA. 結果中午突然血壓掉。我去床邊聽診聽到pan-systolic murmur, 床邊一看,有很明顯的 low EF 以及apical and anterior wall akinesia. 因為還有個急診的急導管。我就把病人從樓上弄到樓下的3B心臟加護病房。隔了四個小時,急診的另一個急導管完成後,我去CCU再掃心超,花了時間,找到了post-MI VSD. 也有辦法解釋為什麼血壓掉了。
���下來就是再說服把老奶奶弄進導管室,作診斷導管,放IABP. 隆君老師 (她門診的VS) 也親自到院來看她。晚上就被陳益祥教授開刀開好了。
超音波是救命的診斷工具
1 note
·
View note
Text
A Rare cause of Troponin elevation: Focal Takotsubo Cardiomyopathy by Arzu Canan in Journal of Clinical Case Reports Medical Images and Health Sciences

CASE PRESENTATION
A 61-year-old woman with acute encephalopathy and acute cholecystitis, was found to have elevated troponin (high-sensitive troponin: 978 ng/L; >52 ng/L: abnormal), regional wall motion abnormality of mid anterior and septal segments and 50% LVEF on transthoracic echocardiography (Movie 1), without EKG changes. Patient denied chest pain, shortness of breath or palpitation. Subsequent CTA demonstrated no coronary artery disease.
Cardiac MRI revealed LVEF 45%, focal akinesis of mid anterior and septal segments (Movie 2), and mild native T1 and T2 elevation without late gadolinium enhancement (Figure 1). Considering the concomitant medical stress and spontaneous troponin down titration (978 à 764 à711 ng/L), the patient was diagnosed with focal Takotsubo cardiomyopathy. Follow-up echocardiogram two weeks later demonstrated full recovery of wall motion abnormalities and 59% LVEF (Movie 3).
Takotsubo cardiomyopathy is usually associated with physical-emotional trigger and characterized by a variety of wall-motion abnormalities and transient LV dysfunction. Neurological disorders is a well-known trigger of Takotsubo cardiomyopathy and is more compared to patients with acute coronary syndromes. Although common presentation is acute chest pain, incidental troponin elevation or EKG changes can be the only finding. The most common type is the apical involvement resulting in apical ballooning. Isolated mid ventricular or basal involvement can also be seen. Focal anterior wall involvement is the rarest form and may mimic acute myocardial stunning or focal myocarditis. Small group of patient can have abnormal LGE while the majority of cases do not demonstrate any abnormal enhancement which can be helpful in distinguishing from other entities in addition to clinical and other ancillary findings.
Figure 1:
(a) 2-chamber steady state free precession still image in diastolic phase demonstrates minimal wall thinning of the mid anterior segment.
(b) 2-chamber steady state free precession still image in systolic phase shows focal akinesia of mid anterior segment resulting in focal bulging (arrow). Note the normal contraction at the basal and apical segments.
(c) 2-chamber phase sensitive inversion recovery (PSIR) image shows no late gadolinium enhancement.
Movie Legends:
Movie 1: Parasternal long axis view from the initial transthoracic echocardiography demonstrates the focal wall motion abnormality in the mid septal segment.
Movie 2: 2-chamber (a) and 3-chamber (b) steady state free precession cine clips from cardiac MRI demonstrates the mid anterior and septal wall motion abnormality.
Movie 3: Parasternal long axis view from the follow-up transthoracic echocardiography demonstrates the resolution of previously identified wall motion abnormality in the mid septal segment. Also note that, overall LV function has improved.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#echocardiography#encephalopathy#CTA#abnormality#transthoracic#Neurological#cardiomyopathy#EKG#LGE#phase sensitive inversion recovery#Arzu Canan#jcrmhs
0 notes
Link
Eye surgery. Requirements for eye surgery: Akinesia of the eye Intense analgesia Minimal bleeding (avoid HT or movement of eye) Management of oculo -cardiac reflex Control of intra-ocular pressure (IOP) Beware of drug interactions Smooth recovery with no PONV. Oculo -cardiac reflex. Slideshow...
1 note
·
View note
Text
Epidemics, Protocols, and the Trouble regarding Athens: Experience through Thucydides
Total satisfaction as well as power ended up significantly larger inside the fresh party. For health solutions utilization. a reduced amount of appointments with crisis bedrooms and also hospitalizations as compared to expected ended up being affecting your fresh cohort. Conclusion. Your PRISMA product increases the usefulness in the medical program pertaining to weak seniors.There was restored curiosity about the actual surgical procedures of Parkinson's ailment (PD) in the last 20 years. From the 40's for you to Sixties several PD individuals have neurosurgical processes for you to ablate specific human brain targets to help remedy tremor as well as, into a smaller extent, akinesia along with rigidity. With the intro associated with levodopa from the Nineteen sixties, along with the realization of the company's stunning benefits, surgical procedure of movement problems essentially disappeared. Eventually, limits and side effects related to drug treatment started to be very obvious. With complications linked to long-term medications, especially levodopa-induced electric motor variances and also dyskinesias, restricting therapeutic success in lots of individuals, surgical procedure continues to be reexamined to cope with this particular unmet will need. It is result in the development along with, right now, widespread usage associated with high-frequency heavy human brain excitement (DBS). DBS can be described as a secure and efficient treament regarding dopaminergic electric motor signs and symptoms of PD, specifically tremor, solidity, as well as bradykinesia, and has triggered essential reductions in engine complications associated with medical therapy. Although DBS provides essential characteristic gain, it does not appear to customize the organic good PD. Some other surgery strategies, including cellular transplantation as well as gene remedy aiming in neural restoration along with recovery, are still getting looked at, however, these have yet to be verified useful.Aberrant neuronal re-entry into the mobile or portable routine is emerging as any pathological mechanism in Alzheimer disease (Advert). However, even though cyclins, cyclin centered kinases (CDKs), and also other mitotic components are generally ectopically indicated within nerves, many of these proteins can also be involved in various other pathological and physical techniques, generating carried on discussion about no matter whether this kind of marker pens are really suggestive of the authentic cell routine method. To handle this challenge, have a look at assessed among the minichromosome maintenance (Mcm) meats that plays a role in Genetics reproduction along with becomes phosphorylated by the S-phase selling CDKs and also Cdc7 throughout Genetic synthesis. We all found phosphorylated Mcm2 (pMcm2) significantly linked to neurofibrillary knots, neuropil post, along with dystrophic neurites throughout Advert and not within aged-matched settings. These types of files not simply provide additional evidence with regard to cell period aberrations within Advertisement, though the cytoplasmic, instead of atomic, localization of pMcm2 recommends the unusual mobile distribution of the crucial reproduction element in Advertisement that could explain resultant cell click here cycle stasis along with resultant neuronal degeneration.
#AdipoRon#SB-297006#Valproic acid#PTC-209#Takinib#NT157#Lys05#GCN2iB#Tegatrabetan#AZD-5153 6-hydroxy-2-naphthoic#CHIR-98014#Ki16198#LY2874455#JSH-23#CP-673451#Epoxomicin#PD-1/PD-L1 Inhibitor 3#C646#Apitolisib#Mivebresib#Ritonavir#ARRY-382#Sodium L-lactate#Tolebrutinib#VU661013#Monastrol#MLT-748#VE-822#NSC-185#Dactinomycin
0 notes
Text
Acute Coronary Syndrome with ST Segment Elevation: New Electrocardiographic Pattern
A 58-year-old man with a history of hypertension and diabetes, presented to the emergency department (ED) after 2 hours of oppressive, severe chest pain radiating to the left arm and associated with dyspnea. Upon arrival he was stable, an ECG was performed that demonstrated an isolated elevation of the J point in DIII, with depression of the J point in DI, DII, AVL, V4 to V6, with isoelectric ST segment in AVF. Troponine was not expected because an ST equivalent pattern was suspected. Should the patient be treated for an acute coronary syndrome with elevation of the ST or non-ST elevation based on the ECG findings
The ECG in Figure 1 shows an isolated elevation of the J point in DIII without concomitant elevation of the contiguous derivatives in the inferior face (subtle under-elevation of the J point in DII and isoelectric ST segment in AVF) and ST-segment depression in DI, AVL, V4 to V6 as reciprocal changes on the lateral side in the setting of an inferior ST myocardial infarction.
The patient received aspirin, clopidogrel and IV nitroglycerin, he was then transferred for urgent cardiac catheterization that showed an anterior descending coronary artery with 99% occlusion in its proximal and middle portion, the right coronary artery was codominant with 100% occlusion in the proximal third, the circumflex artery with multiple tandem lesions and 99% occlusion of chronic appearance. The patient was transferred to the intermediate care unit and received treatment with IV Tirofiban. The echocardiogram revealed a preserved ventricular function with 45% ejection fraction and akinesia of the inferobasal segment. He was referred for surgical revascularization due to multivessel disease and impossibility of percutaneous intervention Figure 2.
https://www.stephypublishers.com/sojccts/pdf/SOJCCTS.MS.ID.000508.pdf
0 notes
Text
Sindrome de duplo y pdf file
SINDROME DE DUPLO Y PDF FILE >>Download (Telecharger)
vk.cc/c7jKeU
SINDROME DE DUPLO Y PDF FILE >> Lire en ligne
bit.do/fSmfG
This manual describes the implantation and usage of the Vercise™ Deep Brain Neuroleptic malignant syndrome or acute akinesia can occur very rarely. Volume 9-Issue 3: Stepping into the Role of Direct Support Professional Volume 7-Issue 2: 22q11.2 deletion syndrome (22q)[PDF] DM 2 18 XXX. que la fillette possède une particularité chromosomique, le syndrome « triplo X » Document : caryotype de Louise Dàprès Docteur Hélène the AMS 800 Urinary Control System Operating Room Manual. Brief Device Description by opening and closing the urethra at the control of the patient. ATENÇÃO: Leia atentamente o manual de instruções syndrome des vibrations du système main-bras, également Classe II - Duplo isolamento. Informação. wARNING: The vibration emission value during actual use of the power tool can differ This tool may cause hand-arm vibration syndrome if its use is not
, , , , .
1 note
·
View note
Text
An instance of Retroperitoneal Synovial Sarcoma while pregnant Addressed with Antepartum Doxorubicin plus Caramboxin Radiation treatment
Honey has been used as a classic foodstuff and also health care resource since ancient times. Nevertheless, lately a lot of scientists have been focusing on your antioxidant home of honey. Simply by use of human being renal cancer malignancy mobile collections (ACHN), we all looked at the antiproliferative exercise, apoptosis, and the antitumor action regarding honey. Materials and techniques: Cellular matrix had been classy inside Dulbecco's modified Eagle's moderate along with 10% fetal bovine serum helped by different concentrations of mit regarding darling for 3 successive days. Mobile possibility had been quantitated from the 3-(Some,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay. Apoptotic tissues had been decided making use of Annexin-V-fluorescein isothiocyanate (FITC) through circulation cytometry. Final results: Honies reduced your mobile or portable stability from the dangerous tissues in a concentration-and time-dependent manner. The IC50 valuations against the ACHN cell lines ended up determined as A single.Seven +/- Zero.04% and a couple of.1 +/- Zero.03% mu g/mL right after Twenty four and 72 they would, respectively. Honies induced apoptosis of the ACHN tissues in the concentration-dependent way, since driven by flow cytometry histogram involving taken care of cells. Conclusion: It may be concluded that darling might cause mobile or portable loss of life within the ACHN cellular material, through which apoptosis has #Link# an important role. The majority of the drug treatments employed in cancer remedy are usually apoptotic inducers, hence apoptotic nature involving honey is considered crucial. Therefore, it motivated all of us to research honies as a possible choice regarding renal cancer treatment method.North American associates in the genus Radiolucina tend to be examined. A lectotype for that type types, Radiolucina amianta, is specified and also explanations and designs are offered. An explanation of the new species, Radiolucina jessicae, in the west shoreline involving Central america is actually presented. Important diagnostic kinds characteristics are usually defined and also in contrast amid members of the genus.Track record: Metabotropic glutamate receptors (mGluRs) have been shown be potential goals for various nerve ailments, which include Parkinson's illness (PD). We previously documented which ACPT-1, any non-selective class 3 #Link# mGluRs agonist, injected locally in to the globus pallidus, striatum as well as substantia nigra pars reticulata (SNr), significantly attenuated the actual haloperidol-induced catalepsy in test subjects. N,N'-dibenzhydryl-ethane-1,2-diarnine dihydrochloride (AMN082) is a strong, brain going through mGluR7 agonist, discerning more than additional mGluRs. Approaches: The purpose of the present examine ended up being determine whether (One #Link# ) initial of mGluR7 by simply endemic management involving AMN082 may well generate antiparkinsonian-like outcomes inside the haloperidol-induced catalepsy and resetpine-induced akinesia versions in rats; (A couple of) striatal as well as nigral mGluR7 probably will help with this type of effect. Results: We all discovered that AMN082 (1 and 3 mg/kg) lowered the haloperidol (2.30 mg/kg)-induced catalepsy, however has not been successful within attenuating the actual reserpine (2.Your five mg/kg)-induced akinesia. While provided in your neighborhood, AMN082 in addition drastically declined catalepsy throughout rats; nevertheless, the successful striatal dosages have been 10-fold under those used in the actual SNr (Two.
0 notes
Text
Cortical Navicular bone Come Cell-Derived Exosomes' Healing Effect On Myocardial Ischemia Reperfusion along with Cardiovascular Afatinibg
These kind of files declare that the akinetic appearance from the apex could be in connection with the prime systolic circumferential wall membrane anxiety of this type, which usually disagrees with circumferential fiber reducing thereby apical akinesia and ballooning might be primarily the consequences regarding LV geometry-induced localised variations in walls tension, instead of a results of significantly impaired myocardial contractility within apical locations. (Chemical) '08 Elsevier Ireland in europe Ltd. Almost all protection under the law set-aside.Myoendothelial gap 4 way stop (MEGJ), a single kind of gap 4 way stop involving vascular endothelial mobile along with vascular clean muscles cellular, can send electrical as well as compound alerts to maintain the electrical along with machinery action synchronism involving vasculature, After extreme stress or surprise, general reactivity for you to vasoconstrictors or vasodilators is cut down tremendously. Nevertheless, regardless of whether MEGJ takes part inside the regulating general reactivity after hemorrhagic surprise, which MEGJ is included, and what's the possible procedure tend to be unfamiliar. With the hemorrhagic shock Sprague-Dawley rodents along with their outstanding mesenteric arteries (SMAs), the effects involving Eighteen alpha-glycyrrhetic acid, any lipophilic aglycone which disturbs gap junction plaques, about vascular #Link# contractile reply to norepinephrine (endothelium-independent general constrictor), myricetin (endothelium-dependent vasoconstrictor) and rest reactivity for you to sodium nitroprusside (endothelium-independent vasodilator), as well as acetylcholine (Ach and every; endothelium-dependent vasodilator) had been seen. Meanwhile, the relationship with the mRNA/protein phrase involving connexins Thirty-seven, 40, along with 43(Cx40 as well as Cx43) for the modifications of vascular reactivity right after hemorrhagic jolt and the effect of antisense oligodeoxynucleotide of Cx40 or Cx43 in vascular calcium level of responsiveness along with vascular reactivity were investigated. The final results established that 20 alpha-glycyrrhetic chemical p antagonized myricetin and also Ach-induced SMA reactivity, yet did not have any relation to norepinephrine- as well as sea salt nitroprusside-induced general reply. The particular mRNA as well as health proteins appearance involving Cx37 along with Cx40 of SMA ended up adversely linked to the general reactivity, although Cx43 appeared to be an optimistic romantic relationship to be able to general reactivity. Antisense oligodeoxynucleotide of Cx40 drastically increased the actual calcium awareness, myricetin-induced vasoconstriction, and Ach-induced vasodilation, while antisense oligodeoxynucleotide associated with Cx43 despondent these people. It turned out recommended that MEGJ plays a huge role inside the regulation of endothelium-dependent general reactivity right after hemorrhagic jolt. Your involved kinds had been mainly Cx40 along with Cx43. The potential system which Cx40/Cx43 handles the endothelium-dependent vasoconstrictor reactivity may be in connection with their own regulating effects for the calcium level of responsiveness associated with general clean muscle mass mobile or portable.Child particles regarding non-enveloped lytic parvoviruses ended up earlier confirmed to be make an effort to transported on the #Link# cell periphery by means of vesicles within a #Link# gelsolin-dependent way. This procedure involves rearrangement as well as deterioration involving actin filaments, even though microtubules turn into protected through the an infection. The following the target is actually about the intra-cellular egress pathway, with its influence on the components and launch of child virions. By colocalization along with cell phone gun proteins and certain modulation of the walkways through over-expression regarding alternative effector genetics transduced by recombinant adeno-associated trojan vectors, many of us show that progeny Sun contaminants turn out to be engulfed in to COPII-vesicles within the endoplasmic reticulum (ER) and so are transferred through the Golgi to the plasma tv's membrane.
1 note
·
View note
Text
whats it like having a body that... works
when you want to accomplish a task you just coordinate your brain and appendages?? sounds fake
10 notes
·
View notes
Photo
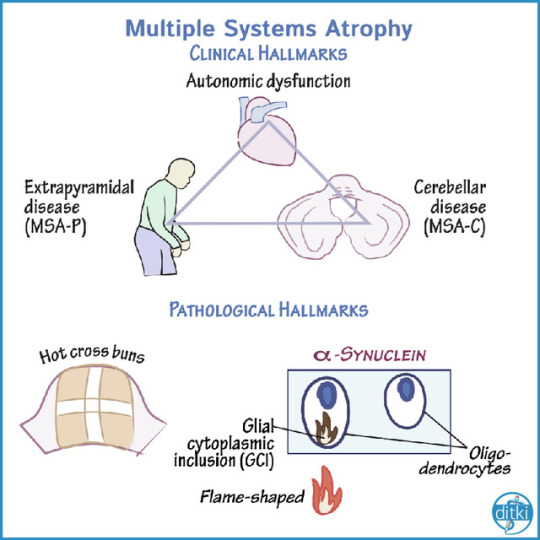
Clinical Hallmarks
Multiple Systems Atrophy (MSA) involves the clinical triad of:
Autonomic dysfunction
Extrapyramidal disease
Cerebellar dysfunction
Inspiratory stridor is a common, important clinical manifestation in MSA.
Key features are orthostatic hypotension, urinary retention/incontinence, erectile dysfunction, anhidrosis, and other features.
Note that there is no MSA-A, since prominent autonomic dysfunction is always required.
Akinesia, rigidity, and postural instability most often without tremor; it resembles PD more-so than PSP.
We use MSA-P (formerly striatonigral degeneration, SDN), if parkinsonian symptoms predominate.
Ataxia and possible cerebellar speech.
We use MSA-C (formerly, olivopontocerbellar atrophy, OPCA), if cerebellar symptoms predominate.
Pathological Hallmarks
"Hot cross buns sign" is a vommon radiographic finding in MSA.
Oligodendrocytes comprise glial cytoplasmic inclusions (GCI)
We show the pons in cross-section with a hot cross bun on top.
The white strips represent degenerated pontine white matter pathways within the pons (for more on these tracts, see our tutorial on the cortico-ponto-cerebello-thalamo-cortical pathway).
These are flame-shaped inclusions of alpha-synuclein.
Lewy bodies in PD also comprise alpha-synuclein but in PD the accumulation occurs in neurons; here, the accumulation is most notably in glial cells (namely, oligodendroctyes).
#ditki#neuroscience#neuropathology#hotcrossbuns#atypical parkinsons#multiple systems atrophy#pathology#medicalscience#usmle#comlex#apbn#ataxia#akinesia
21 notes
·
View notes
Text
When akinesia is kicking your butt
and by kicking your butt I mean “making your body unliveable’ but you can’t switch antipsychotic again because the others don’t suit you and you’ve JUST been taken off supervised medication taking so you can’t come OFF it.
SO WHAT DO I DO?
An aside, in America and place do they do that thing where theres something put in place where professionals come to house to watch you take your medications else they can haul your ass back to hospital cause…I’m in the UK and it’s r e a l
1 note
·
View note
Text

Intoducing Akinesia!
A genetically altered human created by Dr. Blut- made up from snake and human dna. Her bones have been edited in a way that cause her to have more than double the average human, allowing amazing flexibility without breakage. When she isn’t working, she is the most human out of all the crew, and acts similarly to how she did before she was modified- though she doesn’t actually remember very much about who she used to be.
#villainous#villainous au#Fiendish#Akinesia#Demencia#tide pod snake girl#akinesia fiendish#my art style is so messy and i love it#villanos#villanos au
10 notes
·
View notes
Text
Deathsomnia share "Akinesia" music video
Band: DeathsomniaSong: “Akinesia”Album: You Will Never Find PeaceRelease Date: September 3rd, 2021Label: Isolation Records
Vocalist Kadri Sammel shares of the song origins:
“The origin points of ‘Akinesia’ are night terrors and sleep paralysis, where reality becomes a distortion, and the body is contained and powerless. In a state of fear and disorder, a primordial dichotomous perception guides…

View On WordPress
0 notes
Last Seen Blogs

jalopeura
lamentable is the autumn picker content with plums

pleiadia7
༊*·˚Love & Light࿐

cecildoesthings
cecil B)

spidermanspants
spidertwink

ministryofchamps
Ministry of Champs