#virtual clinical trials
Text
0 notes
Text
According to MarkNtel Advisors’ research report titled “North America Virtual Clinical Trials Market Analysis, 2020”, the North America Virtual Clinical Trials (VCTs) market is anticipated to grow at a considerable CAGR of during 2020-25F. The booming aging population, growing incorporation of patient-facing technology such as tablets, wearable sensors in the virtual clinical trials, and increasing inclination to conduct safe and effective research at a lower cost remotely is surging virtual clinical trials leverage to incline toward the use of telehealth technologies like remote patient monitoring and wearable mHealth devices. Thus, this is projected to drive the growth of the market in the coming years. Moreover, the COVID-19 pandemic has had an optimistic impact on the growth of the virtual clinical trial market due to the rise in the adoption of VCTs on account of extensive demand for vaccines and also due to lockdown restriction which has surged the rate of patient’s inclination toward video conference calls, online chat, and apps for communicating with healthcare providers.
0 notes
Text
The global virtual clinical trials market size was exhibited at USD 8.9 billion in 2022 and it is expected to hit around USD 15.64 billion by 2032, growing at a CAGR of 5.8% during the forecast period from 2023 to 2032.
0 notes
Photo

Human-Centric eClinical Trial Platform | Jeeva Trials
The Jeeva eClinical Cloud was developed by researchers with empathy who listen and learn to help clinical researchers, hospital sites, academic medical centers, CROs, and biopharmaceutical sponsors accelerate patient enrollment by 3x faster.
#Patient Recruitment#Patient Reported Outcomes#Clinical Outcomes Assessment#Epro#Ecoa#Virtual Trials#Clinical Research#Patient Engagement#Cloud Technology#Saas#Eligibility Screening
1 note
·
View note
Text
Virtual Clinical Trials Market is estimated close to $8 Bn in 2020 and is likely to grow at a healthy CAGR of above 10% by 2025
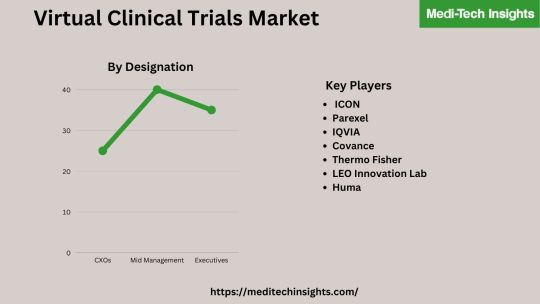
A virtual clinical trial (also known as remote/decentralized clinical trials) refers to digitally empowered clinical trial processes.
GlobalVirtual Clinical Trials Marketis estimated close to $8 Bn (2020) growing above 10% CAGR. The market growth is driven by rising adoption of virtual trials following outbreak of COVID-19 pandemic.
Virtual trials enable easy patient enrolment and remote monitoring
Virtual trials are based on telemedicine and utilize specialised applications for patient engagement and tracking. They significantly reduce the time and financial costs. Additionally, using AI technology helps speed up the process of synthesising and analyzing ever-growing data. Clinical trial sponsors/life science companies are becoming ever more interested in virtual clinical trials due to these advantages.
“AI likely to play important role in virtual clinical trials. Conversational AI for natural language processing (NLP) and image-based AI will increasingly become part of virtual trials. Conversational AI help maintain the patient-clinician engagement while imaging AI to play key role in trials that require radiology”– CTO, Leading Clinical Trial Solutions Company
VC fundings increased significantly post-covid
The number of venture capital funding deals have increased post covid. There were six deals in 2018 which increased to 18 in 2020. Most VC funding occurred in Q3 2020 (10 deals). Notably, Medable - one of the fastest growing decentralized trials platform providers - raised $524 million from various rounds since 2020. One of the biggest rounds occurred in October 2021, where the company received a huge $304 million Series D funding. Growing VC funding will allow companies to develop new technologies and expand their customer and geographic reach. This will then increase overall adoption and virtual clinical trials market growth.
Explore Premium Report on Virtual Clinical Trials Market @ https://meditechinsights.com/global-virtual-clinical-trials-market/
Regional Adoption: Virtual Clinical Trials Market
The US is now the largest market for virtual clinical trials, according to a comprehensive geographical analysis of the global virtual clinical trials market. On the other hand, European life science/medical device companies have not moved as rapidly to accept virtual trials as U.S. However, there have been developments taking place in EU those are expected to propel the adoption steadily.
For instance,
In September 2019, the Trials@Home project was launched by the public-private partnership viz. Innovative Medicines Initiative (IMI) - to augment the use of digital tools in conduct of clinical trials.
There are 31 members in this large-scale collaborative project from the European Federation of Pharmaceutical Industries and Associations (EFPIA), academics, small and mid-sized life science companies, and patient organizations.
Competitive Landscape Analysis of Virtual Clinical Trials Market
Some of the key players in global virtual clinical trials market are ICON, Parexel, IQVIA, Covance, Thermo Fisher, LEO Innovation Lab, Huma, Medidata, Oracle, CRF Health, Medable, Signant Health, and Clinical Ink.
For More Detailed Insights, Contact Us @ https://meditechinsights.com/contact-us/
About Medi-Tech Insights
Medi-Tech Insights is a healthcare-focused business research & insights firm. Our clients include Fortune 500 companies, blue-chip investors & hyper-growth start-ups. We have completed 100+ projects in Digital Health, Healthcare IT, Medical Technology, Medical Devices & Pharma Services.
Contact:
Ruta Halde
Associate, Medi-Tech Insights
+32 498 86 80 79
0 notes
Text
Virtual Clinical Trials Market Size Reaches USD 12.9 Billion By 2030
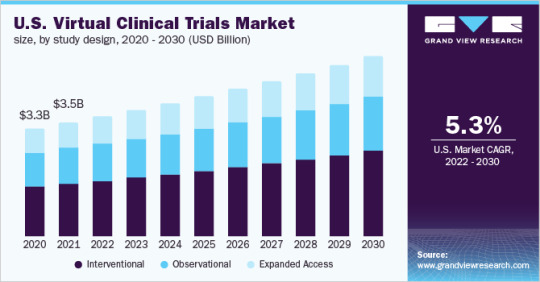
The global virtual clinical trials market size is expected to reach USD 12.9 billion by 2030, according to a new report by Grand View Research, Inc. The market is expected to expand at a CAGR of 5.7% from 2022 to 2030. The COVID-19 pandemic has significantly impacted the market. The growing need for patient diversity clubbed with enhanced data collection in clinical trials is boosting the market growth.
There has been a rise in the R&D of new drugs and vaccines that has increased the volume and complexity of clinical trials. Virtual clinical trials eliminate challenges posed by traditional clinical trials for example delays in patient recruitment and time-consuming procedures. Also, studies have revealed that around 75.0% of people favored a mobile trial over traditional ones and 80.0% of patients are more likely to participate in a clinical trial that uses mobile technology.
The market is recovering at a significant pace after the pandemic as it offers various benefits to patients as well as sponsors. During the pandemic, traveling was potentially dangerous. It can be expensive, even incurring lost wages or requiring that childcare/eldercare be hired. These drawbacks limit initial interest and provide a simple solution for virtual clinical trials. Virtual clinical trials offer various benefits such as effective data collection, analysis, and monitoring large amounts of data in real-time.
Virtual trials make use of monitoring devices, software apps, online social engagement platforms to conduct every step of the clinical trial process including patient recruitment, counseling, measuring clinical endpoints, informed consent, and adverse reactions. Telehealth, home care, and remote patient monitoring has been gaining momentum as a healthcare offering, and the COVID-19 is adding more horsepower to this initiative.
Browse Full Report: https://www.grandviewresearch.com/industry-analysis/virtual-clinical-trials-market
Virtual Clinical Trials Market Report Trends and Growth
The oncology segment held 25.2% of the revenue share in 2021. The increasing adoption of virtual trials especially in oncology clinical research for the diverse populations is responsible for the growth of the segment
The interventional design segment accounted for the largest revenue share of 46.7% in 2021
North America held 49.2% of the revenue share in 2021. Favorable government initiatives and the presence of large numbers of players in the U.S. offerings advanced services are responsible for market growth
In Asia Pacific, the market is expected to witness the fastest CAGR of 6.8% over the forecast period owing to the increasing patient pool and cost-efficient services
Key Companies and Market Share Insights
The market for global virtual clinical trials is highly competitive. Significant factors affecting competitive nature are the quick adoption of advanced technology for improved healthcare. Besides, players are also acquiring, collaborating, partnering with other firms to gain the market share. For instance, in May 2020, Covance announced expanding its technology ecosystem to accelerate decentralized clinical trials adoption. The company is doing so through an alliance with Medable, a prominent software provider for digital clinical trials. Some of the prominent players in the virtual clinical trials market include: ICON, Parexel International Corporation, IQVIA, Covance, PRA Health Sciences, LEO Innovation Lab, Medidata, Oracle, CRF Health, Clinical Ink, Medable, Signant Health, Clinical Ink, Halo Health Systems, Croprime
Request Free sample Report: https://www.grandviewresearch.com/industry-analysis/virtual-clinical-trials-market
#Virtual Clinical Trials Market Trends#Virtual Clinical Trials Market Size#Virtual Clinical Trials Market Forecast
0 notes
Text
The Best News of Last Week
🦾 - High-Five for Bionic Hand
1. Houston-area school district announces free breakfast and lunch for students

Pasadena ISD students will be getting free breakfast and lunch for the 2023-24 school year, per an announcement on the district's social media pages.
The 2023-24 free lunch program is thanks to a Community Eligibility Provision grant the district applied for last year. The CEP, which is distributed by the Department of Agriculture, is specially geared toward providing free meals for low-income students.
2. Dolphin and her baby rescued after being trapped in pond for 2 years
youtube
A pair of dolphins that spent nearly two years stuck in a Louisiana pond system are back at sea thanks to the help of several agencies and volunteers.
According to the Audubon Nature Institute, wildlife observers believe the mother dolphin and her baby were pushed into the pond system near Grand Isle, Louisiana, during Hurricane Ida in late August 2021.
3. Studies show that putting solar panels over waterways could boost clean energy and conserve water. The first U.S. pilot project is getting underway in California.

Some 8,000 miles of federally owned canals snake across the United States, channeling water to replenish crops, fuel hydropower plants and supply drinking water to rural communities. In the future, these narrow waterways could serve an additional role: as hubs of solar energy generation.
4. Gene therapy eyedrops restored a boy's sight. Similar treatments could help millions

Antonio was born with dystrophic epidermolysis bullosa, a rare genetic condition that causes blisters all over his body and in his eyes. But his skin improved when he joined a clinical trial to test the world’s first topical gene therapy.
The same therapy was applied to his eyes. Antonio, who’s been legally blind for much of his 14 years, can see again.
5. Scientists develop game-changing vaccine against Lyme disease ticks!

A major step in battling Lyme disease and other dangerous tick-borne viruses may have been taken as researchers announced they have developed a vaccine against the ticks themselves.
Rather than combatting the effects of the bacteria or microbe that causes Lyme disease, the vaccine targets the microbiota of the tick, according to a paper published in the journal Microbiota on Monday.
6. HIV Transmission Virtually Eliminated in Inner Sydney, Australia

Sydney may be the first city in the world to end AIDS as a public health threat by 2030. Inner Sydney has reduced new HIV acquisitions by 88%, meaning it may be the first locality in the world to reach the UN target to end AIDS as a public health threat by 2030
7. New bionic hand allows amputees to control each finger with unprecedented accuracy

In a world first, surgeons and engineers have developed a new bionic hand that allows users with arm amputations to effortlessly control each finger as though it was their own body.
Successful testing of the bionic hand has already been conducted on a patient who lost his arm above the elbow.
----
That's it for this week :)
This newsletter will always be free. If you liked this post you can support me with a small kofi donation:
Support this newsletter ❤️
Also don’t forget to reblog.
895 notes
·
View notes
Text
With the Alberta government announcing a ban on gender-affirming care until 16 years old, let’s take a minute to correct some misinformation using peer-reviewed publications. A thread.🧵
“High quality evidence doesn’t support gender-affirming care.”
‘High quality evidence’ is a technical term that essentially just means ’no randomized controlled trials.’ RCTs are not scientifically feasible for trans youth care and would be unethical (link).
The evidence-base for gender-affirming care is quite robust and is at least as good at the evidence base for comparable interventions like abortion and birth control. For an overview of available studies, albeit already few years outdated, see page 144 onwards (link).
“Over 80% of kids grow out of being trans.”
That’s just not true. The claim is based on old, poor-quality studies that included tons of kids who never claimed to be trans (link).
But even if we took the percentage at face value, it would be irrelevant since it’s based on pre-pubertal data and virtually all the so-called ‘desistance’ occurred before puberty, when gender-affirming care becomes available (link).
More recent, better studies suggest that only around 2.5% have ‘grown out of it’ after 5 years (link).
“Kids falsely believe that they are trans because of social contagion.”
There is no evidence for that claim. It’s based on the reports of transphobic parents who were surprised that their kid came out ‘out of the blue’ and happened to have trans friends, as trans kids tend to do. For a careful explanation of why the claim is completely unsupported by evidence, see this (link).
Studies of trans youth that used clinical data to look into the claim have also failed to find any evidence of epidemic or large-scale social contagion (link).
“We need a years-long diagnostic process to make sure kids are ‘truly’ trans before they transition.”
There is no evidence that gender assessments fare any better than self-report at predicting future outcomes, as we explain in our recent review (link).
“Gender-exploratory therapy can help identify the trauma that made these kids gender dysphoric.”
Gender-exploratory therapy is extremely difficult to distinguish from classic conversion therapy, which also starts from the premise that ‘trauma’ makes people LGBTQ2S+ (link).
Since conversion therapy is known to be harmful, we have reasons to believe that gender-exploratory therapy would be as well.
Self-directed exploration is good. Forced exploration rooted in suspicion towards trans identities isn’t. If you’re starting from the belief that trans identities are inherently suspicious, you’re not doing therapy, you’re doing transphobia.
Any more myths about gender-affirming care you’d like me to bust, Tumblr?
#transgender#trans#lgbtq#lgbtqia#queer#lgbt#gender affirming care#gender affirming healthcare#trans healthcare#science#misinformation
253 notes
·
View notes
Text
“If the practice stopped, top-level women’s sport as we know it might cease to exist.”
Full text below cut
My wife and I are lifelong runners. It’s the sport we fell in love with, and ended up excelling at—during our wedding, every speaker from the preacher to the best man mentioned some variation of “Can you imagine how fast their future kids are going to be?” My wife, Hillary, is by far the more accomplished athlete. I made the NCAA championship; she was an All-American. I had dreams of qualifying for the Olympic trials; she actually did it. By many measures, she’s simply better. But not by all of them.
We both got our start in middle school. When Hillary was in seventh grade, she ran a 5:42 mile. At the same age, my best was virtually identical at 5:40. If we had lined up for a race, there would have been a close dash to the finish line. Fast-forward to ninth grade, and we were both ranked among the top freshman runners in Texas. But a clear difference had emerged: Her time had steadily decreased to 5:13, while mine had shot all the way down to 4:22. At the end of our collegiate running careers, the massive gulf remained: She ran 4:43 and I ran 4:01. I didn’t train more, care more, or possess more grit. She surpasses me on all of those things. I just had an inherent advantage: my biology.
It’s no secret that sports-performance differences between sexes are a flashpoint in an American culture war that goes beyond athletics into ideology and identity. I’m not here to tackle the tough and important questions of sport and sex, such as how to include trans athletes and people who have differences of sexual development in a sporting world that is mostly divided along binary lines. What I am here to address is one of the simplest debates. Over the past few years, some cultural commentators and sociologists have minimized the impact of sex-based biological differences on sporting performance. Some claim that men’s biological advantages in speed, strength, or endurance are scientifically debatable. (This magazine recently published such arguments in an article about youth sports.)
Here is what the facts say. Sport for women is generally undervalued and under-resourced in America, and this can affect women’s performance levels. Coed sports at recreational and youth standards—played as part of living a good life, not to develop elite athletes—can be both fun and competitive. But at the highest, rarefied levels of many professional sports, men and women appear to have different performance ceilings.
The research is clear: The difference in my wife’s and my athletic progression is not unusual. With young kids, the best boys tend to be only a hair better than the best girls. We can see this in age-group records: The boys’ and girls’ records for the 9-to-10-year-old 100-meter-sprint are nearly identical (12.73 versus 12.85). But in the 15-to-16-year-old records, the gap has gone from a crack to a gulf (10.51 versus 11.34).
A study by Mike Joyner and his colleagues at the Mayo Clinic found the same trend when analyzing the top 100 freestyle-swimming times of boys and girls from ages 5 to 18. Before the age of 10, both sexes are remarkably similar in performance, with the best young girls actually tending to swim faster than the best boys. But after 10, the boys get ahead. By 17, the average difference is 8.4 percent. Researchers found the same trend when evaluating more than 400,000 ordinary kids in the P.E.-class shuttle run: similar speeds early on, but an ever-widening gap starting at about age 10.
The reason for this is simple: puberty. The overwhelming driver for the sudden jump in male performance seems to be the surge, at this specific time of an athlete’s life, in the steroid hormone testosterone. This hormone influences muscle size and strength as well as the amount of oxygen-carrying red blood cells in our body. A large analysis on running, jumping, and swimming found that the rise in testosterone during puberty in males coincided with a steep improvement in performance. When puberty occurs, girls, on average, continue steadily improving their sporting performance into their teens. But boys get a rapid shift upward in their trajectory.
When looking at elite runners—whether sprinting 100 meters or racing many miles—once athletes hit physical maturity, the best men have anywhere from a 9 to a 12 percent advantage over the best women. A significant gap can be seen in cycling, swimming, speed skating, high-jumping, and a variety of other athletic feats. The gap is even larger in sports that depend highly on strength. For example, when looking at elite weight lifters in the same weight class, the performance gap is about 24 to 30 percent.
It’s important to note a few caveats. First, most of the best research is on sports that are easily quantifiable. For example, there’s no way to directly compare the skill levels of elite tennis players to measure for tiny performance differences unless they play one another. What we know is that the less a sport relies on speed, power, or endurance, and the more it relies on skill, the smaller the gap is. In sports like shooting and archery, the difference between men and women is negligible at best. Second, the performance gap of course doesn’t mean that all men will triumph over all women all the time. My comparatively unathletic brother would get beaten by thousands of women in a mile-long race. And if my wife showed up to a local turkey trot, she’d likely decimate all the men. Third, because there is significant overlap between males and females in performance, female outliers can shine, particularly in niche sports with a small number of competitors (e.g., ultrarunning).
But at the top of the top of the athletic world, in widely played sports with elite coaching, the gap between the sexes seems almost insurmountable. Take the queen of track and field, Allyson Felix. The 11-time Olympic medalist’s best 400-meter time ever is 49.26. In just the 2022 season, that would have put her 689th on the boys’ high-school performance list.
None of this is meant to disparage the phenomenal women athletes at the top of their game. But if we stopped dividing sport by sex, elite women’s sport as we know it could cease to exist. We might miss out on Megan Rapinoe at the World Cup or the spectacle of Sydney McLaughlin effortlessly gliding over hurdle after hurdle. Acknowledging the performance differential should encourage us to do everything possible to make sure female athletes can keep competing at these levels.
But how do we know that the gap between the sexes isn’t sociological, like we’ve seen in fields such as math, where research suggests that social factors explain much of the gender gap in average performance? The history of sport is rife with sexism that has held back women. Take, for example, the 1928 Olympics, where Knute Rockne, the famed Notre Dame football coach (and newspaper columnist), reported in The Pittsburgh Press that after the 800-meter final, five women collapsed and that “it was not a very edifying spectacle to see a group of fine girls running themselves into a state of exhaustion.” Following public outcry, the 800-meter was removed from the Olympics for 32 years. But the reports were false—women weren’t collapsing left and right. The top-three women actually broke the former women’s world record that day.
Women today still face inequality in sport. Many professional sports have a significant pay gap, limiting the ability of women to focus solely on it as a career. Media attention for women’s sport is severely lacking, with 95 percent of sports TV coverage in 2019 going to men, according to a USC/Purdue University study. In some colleges, a significant difference in funding and severe lack of female coaches—who act as both a role model and an advocate for women’s sport—can impact participation rates. Yet even in sports where sexist sociological barriers have been lowered, a performance gap can persist.
Women were barred from major marathons for much of the 20th century. The Boston Marathon, for example, didn’t allow women to compete until 1971. At that point, the women’s unofficial world record was about 2 hours and 45 minutes. At the same time, the men’s record stood at 2:08:34. That’s a massive 30 percent performance gap. By the summer of 1984, when women were finally able to run the marathon in the Olympics, they’d massively cut into the men’s lead, leaving only a 11 percent gap. These kinds of gains bred a sense of optimism. “We’re nearer and nearer the men now,” said the second-place female finisher of the 1983 Boston Marathon. But the trend faltered. In the nearly four decades since then, women have kept improving, but the current gap still stands at 10.7 percent.
Every sport is different. Some are still like 1970s marathoning—the chasm between men and women is caused in large part by discrimination. Those gaps need shrinking. But the same trajectory we saw in the marathon occurs in most women’s sports that remove sexist barriers. For example, a 2010 study traced the progression of male and female performance across the prior decades in 38 athletic events in five different sports: swimming, cycling, speed skating, weight lifting, and track and field. It found that the gender gap had been fairly stable for more than two decades, and concluded, “After a significant narrowing of gender gaps, women and men now evolve in parallel, in the same direction.”
The upside of acknowledging that sex differences in performance exist is that we can discuss the vital, knotty debates that emerge from this biology. For example, would creating more coed sporting opportunities before, say, age 10, keep girls in sport longer? How should schools and clubs handle a young female athlete who wants to play football even though there’s no girls’ team? Should we get rid of sex-based divisions in sports like shooting, where the performance gap is minimal? We certainly need to figure out better answers for trans athletes and people like Caster Semenya, who, because she has differences of sexual development, is allowed to compete in the 5K but not the 800-meter race.
To solve these questions, we need to first accept the premise that puberty can create unequal sporting ability. Doing so doesn’t mean that we stop fighting inequality or dismiss tricky edge cases. It actually should free us from arguing over what should be a noncontroversial claim. We can then shift our focus to making sure women have the space, resources, and opportunities to show their talents. We can acknowledge that though I might have run faster at my peak, my wife’s performance and achievements are undoubtedly more impressive. We can stop judging female athletes against their male counterparts and enjoy their athleticism on its own accord.
Steve Magness is a performance coach and sports scientist. He is the author of Do Hard Things: Why We Get Resilience Wrong and the Surprising Science of Real Toughness.
442 notes
·
View notes
Text
Not to take away from what is happening in the US, but in light of Amanda Knox' horrible, horrible tweet I thought I would share some information about Legge 194 and its actuation (or lack thereof). Legge 194 is the law that finally decriminalized abortion in Italy in May 1978. As can be expected, Catholic groups and the Catholic Church itself opposed the law at the time and continue to do so. To this day, Italian gynecologist are not legally bound to perform abortions as they can choose to be conscientious objectors (with some specific exceptions, obviously) – this should not constitute a big issue as the same law also dictates a fair allocation of non-objectors to every hospital, clinic, or structure so that the service can be guaranteed to every citizen who shall need it. Except the reality of it is very different. As of May 2022, there were a total of 31 hospitals/clinics where 100% of practicing gynecologists, anesthesiologists, and nurses are conscientious objectors, 50 hospitals/clinics where the percentage is over 90% and 80 where it is over 80% (source). The average of conscientious objectors among Italian doctors is 70% (source), making about 40% of Italian hospitals inadequate to adhere to national law (source). This means that there are entire areas of this country where it is virtually impossible or extremely difficult to access abortions (see map), to the point that Mario Puiatti (president of AIED) once quite famously said "if you want to get an abortion in Sicily, the best way to get it is to jump on a plane" (source). What this means is that, more than 40 years after its promulgation, Legge 194 is de facto not actualized in vast areas of the country. Moreover, instead of decreasing as one would expect, the number of conscientious objectors has increased by 10% in the last ten years (source).
Amanda Knox' tweet is in very poor taste not just because of That One reason but also because it is wildly inaccurate and dismissive of the struggle of Italian women and women who reside in Italy. But yeah, I am sure one sick joke in the form of a snappy tweet is more important than the plight of women worldwide if it helps you further your career and online persona, both built on the back of a fraudulent murder trial.
634 notes
·
View notes
Text
An anime pfp transwoman with nudes all over their profile demanded I define sex based oppression today. This was the response I wrote up in just over 5 minutes. I'd love for yall to add all the things you can think of. I intend to add more myself later on, but was too exhausted to right now.
If you buy into the idea that misogyny is based on a "female identity" rather than the female sexed body, you must also believe that all of the following either don't exist, or could be avoided if the victim simply called herself a boy:
• Infant girls around the world are tortured and/or murdered as infants for not being born male.
• Girls around the world are denied access to education entirely or to higher education.
• Girls around the world, many of single-digit ages, are sold into marriage with middle-aged men - often arranged before she is even born in exchange for a small money loan.
• Women and girls around the world are forcibly impregnated (and remember, pregnancy is life-threatening), forced to give birth, and forced into motherhood.
• Women and girls in many places are "trained" to become mothers and housewives in place of education.
• Women and girls in many places are forced to stay in dangerous, unhygienic conditions away from society while menstruating, thus losing a week per month of school, work, and their lives, and possibly becoming sick or even dying.
• Males are significantly more likely to survive things such as car accidents because the dummies used to design and test are based on male bodies.
• Symptoms of many serious conditions are different in males and females, but typically the male symptoms are more taught and/or better known and understood than the female symptoms. Most of us know the example of heart attacks.
• Sex education teaches girls very little about their bodies and natural processes. Many girls are taught more about male sex organs than about their own. There is also a focus in many sex ed classes on shaming girls for their bodies and natural sexual desires.
• Women and girls around the world are sold into sexual slavery at approximately twice the number of men and boys.
• FGM. And no, circumcision is not even remotely the same thing.
• Breast ironing, foot binding, and other torturous practices reserved for female people.
• Female socialization. Be quiet, your beauty is your worth, you exist to please and serve men, apologize for everything, never take up space, don't play in the mud and dirty your dress, be ashamed of your body's female characteristics, etc.
• Viagra is a wildly successful treatment for menstrual cramps, but virtually nobody knows that and it won't be prescribed to female patients. It is much more important for a man to be able to get hard than to alleviate a woman's suffering.
• Female bodies were left out of medical trials for most of medical history, and this has a massive ongoing impact on the treatment women and girls receive. Many medications should be dosed entirely differently for women, but aren't, and female patients pay the price.
• Underdiagnosis in girls of conditions like autism and ADHD due to clinical models being based exclusively on boys
• Female pain is taken less seriously and investigated and treated less aggressively than male pain in all medical settings.
• Medical conditions that primarily affect women are overwhelmingly underfunded, under-researched, underdiagnosed, and improperly treated.
• In nearly every country on earth, including the USA, people have a sex preference for sons over daughters. It is common for parents, especially fathers, to be visibly or openly upset upon learning they will be having a daughter instead of a son.
• Reproductive rights and bodily autonomy are virtually nonexistent in most of the world if you're female.
• Sex roles (aka "gender") are legally enforced in many places and socially enforced essentially everywhere.
Honestly, this is a miniscule proportion of examples of sex-based oppression, but I wore myself out just writing this. There is SO much more, and this is only current shit, too, not even including historical matters, as well as not even getting into sexual terrorism, and this is only off the immediate top of my head. Female oppression starts before we are even born, and much of the worst of it occurs in girlhood, well before most trans-identified people announce their identity. And even then, trans identity will not protect female people from all aspects of sex-based oppression, though it may reduce interpersonal discrimination in some places for some (usually passing) FTM individuals.
I especially am aiming for examples that can't possibly apply to transwomen like FGM, the car crash risk stats, etc., since I know they'll try to pull the "well we suffer too!" MRA line and ignore the massive disparities in rate/frequency etc.
#mine#radblr#radfem#radical feminism#gender ideology#gender cult#genderism#sex based oppression#female oppression#misogyny#radfems interact#radfems do touch#radfem friendly#radfem safe#tra nonsense#trans ideology#gender critical#gc#gender criticism
193 notes
·
View notes
Text
I Love You
Read on AO3 here.
Maggie knows the second she sees her son walk out of the Kindergarten building that he’s coming down with something.
Jay is sluggish and his face flushed despite the warm weather.
He makes a beeline for her and, despite feeling her heart break as she does so, she has to step back.
Due to a recent cancer treatment her immune system is virtually non-existent. She can’t afford to get whatever he has and she can’t even hug him without guaranteeing that she will.
She can’t give her baby the cuddles he so desperately wants.
“I’m sorry sweetheart.” she says, putting her hand up. “I can’t hug you, not today. In fact, you’ll need to walk a little ahead of us. Please stay where I can see you.”
Jay frowns, glancing between her and Will in confusion.
“Okay.” he says finally, shifting his backpack higher and setting off for home.
She watches him walk for a moment, the hunch of his tiny shoulders screaming for her to forget about her immune system and wrap him in a tight hug until he feels better.
They reach the first crosswalk and he stops, turning to look back at her.
“Will, can you walk your brother across the street?” she asks.
“I don’t want whatever he has.” Will says, shaking his head.
“It’s not anything bad.” she tries to explain.
“Then why don’t you walk him?” Will asks, tilting his head to the side.
“Because … for me it is.” she says weakly.
She doesn’t want to try to explain her immune system to her two little boys out here on the sidewalk.
“You’ll be okay, Jay.” she calls. “Just make sure you look both ways, sweetheart.”
His face falls.
“But… it’s not safe.” he says, glancing back at the road.
“You’ll be okay.” she repeats and he slowly turns, searching the road in both directions before walking across.
The next ten minutes are the longest walk she’s ever been on and then finally she’s walking into her living room.
There’s no sign of Jay and she makes her way up the stairs, standing outside his bedroom door to listen to her little boy cry.
Her heart aches and she wants so badly to throw the door open and pull him into her arms.
But she can’t. She can’t get his cold or she’ll be ejected from the clinical trial that she’s in.
She has to put being alive to be there for both of her sons in the future over holding Jay right now. No matter how much it hurts.
Swallowing hard, she turns and walks back down the stairs.
Jay walks up to his dad calling his name and sits up, rubbing sleep from his eyes.
“Hey kiddo.” Pat says, pressing a hand to his son’s cheek. “You wanna come down for dinner.”
He shakes his head.
“Momma doesn’t want me there.” he says, sniffling. “She hates me.”
“Hey, no.” Pat says, sitting on the bed next to him. “Your mom doesn’t hate you.”
“Yes she does.” Jay insists, wrapping his arms around himself.
“You know how your mom’s been sick?” Pat asks.
Jay shrugs.
“Well because of that, she can get sick in other ways a lot more easily.” Pat explains. “And her body can’t handle it the way the rest of us can.”
He tilts his head.
“I don’t understand.” he says finally.
“You don’t necessarily need to understand the specifics.” Pat says with a sigh. “As long as you believe me when I tell you that your mom loves you and wishes more than anything that she could give you the world’s biggest hug.”
Jay shrugs.
“I guess I believe you.” he says.
“You ready to come down for dinner?” Pat asks.
“I can’t.” Jay says. “Mom can’t get sick.”
“Alright.” Pat says after a minute. “I’ll bring your dinner up.”
Jay pulls the blanket out from under himself and wraps it around his shoulders.
He’s really cold.
Pat comes back with two bowls, setting them on the side table while he shifts Jay to sit against the headboard and then climbs onto the bed, sitting next to him.
He grabs the bowls, handing one over and then starting to eat his own food.
“How are you feeling, bud?”
“‘m cold.” Jay mutters. “And my throat hurts.”
“Yeah.” Pat says. “You’re a little feverish. I’ll get you some medicine after dinner.”
“Tastes yucky.” Jay mutters, making a face.
Pat chuckles.
“Yeah but it will get that fever down and help your throat feel better.” he tells him. “Now eat up. Your mom made chicken soup cause she knew you weren’t feeling well.”
“She made this for me?” Jay asks, eyes wide as he sips at the broth.
“Yeah.” Pat confirms. “It’s the best way for her to help you right now.”
Jay nods and they finish their soup in silence. Pat moves the bowls back to the side table and then coaxes his son out of his blanket to change into his pajamas.
Jay picks out his warmest fleece ones and then climbs back into bed, settling in under the covers.
Pat grabs the cold medicine while he’s changing. Jay makes a face when he hands him the medicine cup but swallows it with a shudder.
Pat settles back on the bed next to him with the book that Maggie has been reading to him in his hands.
“Do you mind if I read to you?” he asks. “Or would you rather leave it until your mom can read it with you again.”
“You can read it.” Jay says, shifting closer.
“Alright.” Pat says, smiling down at him and then opening to Maggie’s bookmark.
By the time he finishes the chapter, Jay’s passed out against him and he gently shifts him down on the bed, tucking the covers around him.
“Sleep tight, baby boy.” he whispers, pressing a kiss to the top of his head. “Get better soon so you and your momma can have the cuddles you both need.”
And then he slowly backs out of the room, closing the door behind him.
Maggie is waiting on the stairs and he sinks down next to her.
“Is he okay?”
“He’ll be fine.” he says, kissing the top of her head. “He’s running a bit of a temp but he took the medicine and he’s sleeping now.”
She sniffles, leaning into his side.
“I hate this, Pat.” she whispers. “Of all the difficulties since my diagnosis I never expected this. Never expected to have to turn away my little boy when he was just looking for a hug.”
“We talked.” Pat tells her, wrapping an arm around her. “I think he understands why you couldn’t. At least he knows that you wanted to.”
She nods and he pulls her closer.
“He loves you.” he tells her. “And this seems like forever right now but in a few days he’ll be feeling better and you can give him as many hugs as you want.”
She doesn’t answer but that’s okay. He’ll sit here with her as long as she needs him to.
Jay misses two days of school before he wakes up feeling much better.
He’s just started getting dressed when his dad comes into the room.
“Hey bud.” he says. “Why don’t you take one more day? Go ahead and stay in your pajamas, okay?”
He frowns in confusion but nods, pulling his pajama shirt back over his head.
“Meet me in the kitchen, okay?” Pat says before disappearing back into his own room.
Jay walks down to the kitchen and freezes when he sees his mom at the stove. Before he can turn and run back upstairs, she turns and smiles at him.
“Good morning, sweetheart.” she says. “Come hug your momma.”
“I can’t.” he says, stepping back. “Dad said I should stay home. I’m still sick.”
“You wanna know a secret?” she asks.
He nods.
“I told your dad to tell you that.” she says with a grin. “But you’re not sick any more, sweetie. I just thought maybe we could spend the day together. To make up for not being able to take care of you this week.”
“Really?”
“Really.” she says. “Can I have a hug now?”
He runs across the room to tumble into her arms.
“I missed you momma.” he says quietly, burying his face in her shoulder.
“I’ve missed you too, baby.” she tells him, kissing the top of his head. “You wanna help me make breakfast? And then we can do whatever you want.”
“Even color?” he asks.
“Sure.” she agrees. “We can color.”
“I love you.” he tells her, burrowing deeper into the hug.
“I love you too.” she tells him. “More than anything.”
3 notes
·
View notes
Last Seen Blogs


omeehayo
zunda log

arlynquinnart
Dibujo y Foto D Arlyn Quinn

daddyklingon
DawnBatKMT, Wayward Apprentice.

sweeneytolstrup
The Life of Meyer 976