#healthinequalities
Text
UKHSA Urges Vaccination: Winter Health Shield
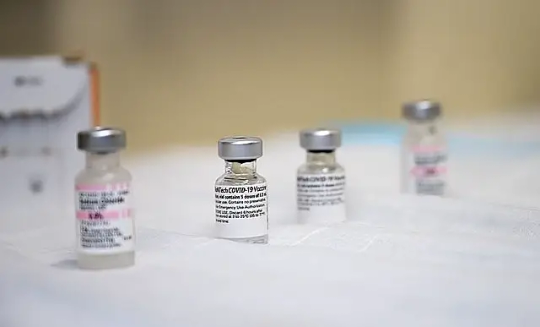
The UK Health Security Agency (UKHSA) is amplifying its call for eligible individuals from ethnic minority groups to prioritize their health by booking both flu and COVID-19 vaccines. This urgent appeal, specifically directed at people from Pakistani and black Caribbean ethnic backgrounds and those residing in more deprived areas, aims to shield them and their families from the heightened risks of these infections during the winter months.
Inequality Insight: Emergency Hospital Admissions
Recent data from UKHSA's report on emergency hospital admission rates for influenza and COVID-19 in England reveals alarming disparities. Emergency hospital admission rates for both illnesses were significantly higher among individuals living in the most deprived areas compared to those in the least deprived areas. Persistent differences in admission rates among ethnic groups were also observed.
Key Findings from the Report:
- Influenza admission rates for the Pakistani ethnic group were 2.7 times higher than the white ethnic group.
- Black, African, Caribbean, or black British ethnic groups had influenza admission rates 1.6 times higher than the white ethnic group.
- Emergency hospital admission rates for both influenza and COVID-19 were 2.6 and 2.1 times higher, respectively, for individuals in more deprived areas.
Analysis and Future Investigations:
While the report highlights these inequalities, it doesn't delve into the underlying factors driving these differences. The complex landscape of health inequalities involves multiple overlapping factors, including existing social and economic disparities, healthcare intervention coverage, and pre-existing health conditions.
This analysis lays the foundation for future investigations, emphasizing the need for a closer examination of underlying reasons and the delivery of interventions.
Call to Action: Improving Vaccine Coverage
The findings underscore the urgent need to enhance vaccine coverage across ethnic groups and different levels of deprivation. Dr. Mary Ramsay, Director of Immunisation at UKHSA, emphasizes the importance of taking both flu and COVID-19 vaccines for optimal protection against these viruses during winter.
Voices Supporting Vaccination:
- Dr. Mary Ramsay: Encourages eligible individuals, especially those from ethnic minority backgrounds, to get vaccinated against these preventable diseases.
- Dr. Shona Arora: Acknowledges observed disparities and urges eligible individuals to book flu and COVID-19 vaccinations promptly.
- Dr. Salman Waqar: Emphasizes the significance of vaccination from a religious perspective and encourages eligible individuals not to delay getting vaccinated for free.
Closing the Gap: Vaccine Uptake Data
Previously published UKHSA vaccine uptake data reveals disparities in influenza and COVID-19 vaccine coverage. Among individuals aged 65 years and over, there were significant differences between ethnic groups, with lower vaccine coverage in certain communities.
Easy Booking Process: Protect Yourself Today!
Both the flu and COVID-19 vaccines can be booked conveniently through the NHS website, NHS app, or by calling 119. The vaccines can be given simultaneously for enhanced protection. With robust safety profiles and proven advantages, there's no reason to delay. Book your vaccination appointment now and ensure a healthier winter for you and your community.
Sources: THX News & UK Health Security Agency.
Read the full article
#covid-19vaccine#Emergencyhospitaladmissions#ethnicgroups#ethnicminoritygroups#Fluvaccine#Healthinequalities#UKHSA#vaccinationdisparities#Vaccinecoverage#winterinfections
0 notes
Photo

Bloomberg Global Equality Summit. What a day. #menopauseawareness #genderequity #menopauseatwork #genderhealthgap #womenshealthcare #healthinequalities #workplacewellbeing #bloomberg #womensnetwork #maleallies #maleally #inclusiveculture https://www.instagram.com/p/ClBApRGjoy4/?igshid=NGJjMDIxMWI=
#menopauseawareness#genderequity#menopauseatwork#genderhealthgap#womenshealthcare#healthinequalities#workplacewellbeing#bloomberg#womensnetwork#maleallies#maleally#inclusiveculture
0 notes
Text
0 notes
Photo
Too good not to share! #Repost @ijustwannalive2020 ・・・ #TrumpsArmy #HomeGrownTerrorist #VoteAwayThePlague #RockThaVote2020 #45bucketsOfLies #TimeToRecognize #BreonnaTaylor #VOTEearly #JacobBlake #BlackLivesMatter #HealthInequalities #StopKillingUs #StopVoterSupression #1619Project #GoodTrouble #TrumpetIdiots And all his #MaskMurderers #IJustWannaLive #ThAttaway https://www.instagram.com/p/CGJYgKgh35v/?igshid=1p92q4mf2e0lj
#repost#trumpsarmy#homegrownterrorist#voteawaytheplague#rockthavote2020#45bucketsoflies#timetorecognize#breonnataylor#voteearly#jacobblake#blacklivesmatter#healthinequalities#stopkillingus#stopvotersupression#1619project#goodtrouble#trumpetidiots#maskmurderers#ijustwannalive#thattaway
0 notes
Photo

American Kidney Fund @KidneyFund Tomorrow, AKF President LaVarne Burton will be a special guest in the fifth installment of @CBCFInc Virtual Brain Trust Series. She and other health professionals will discuss the root causes of #healthinequity and strategies for recovery. Register here: http://ow.ly/7nV750A44kg (at Hammond, Indiana) https://www.instagram.com/p/CBROKIgD1kC/?igshid=vhvpnjfinpyv
0 notes
Photo
#stillnotfree #transformed #jimcrow #polltaxes #redlining #massincarceration #lynching #discrimination #segregation #stopandfrisk #policebrutality #cashbail #wealthgap #policingblackbodies #publiceducation #underserved #undervalued #healthinequity #privateprisons #transportationaccess #fooddeserts #prisonindustrialcomplex #felonydisenfranchisement #votinglaws #stillnotfree https://www.instagram.com/p/By6DPzvj76q/?igshid=6za9pae4e21f
#stillnotfree#transformed#jimcrow#polltaxes#redlining#massincarceration#lynching#discrimination#segregation#stopandfrisk#policebrutality#cashbail#wealthgap#policingblackbodies#publiceducation#underserved#undervalued#healthinequity#privateprisons#transportationaccess#fooddeserts#prisonindustrialcomplex#felonydisenfranchisement#votinglaws
1 note
·
View note
Text
Covid19, the Cumberlege Review, and the future of Hysterical Women
An update on #HystericalWomen and why, post-Covid19 and the Cumberlege Review, it's more important than ever to keep shouting about #healthinequalities. Here's how you can help:
It’s probably an understatement to say it’s been a weird few months since I last posted way back in February. When Covid19 hit, I took the decision to put Hysterical Women on the back burner, partly to concentrate on my (paid) freelance work, and partly for the sake of my own mental health – both of which have taken a significant hit. At the start of lockdown, it felt like there was really only…
View On WordPress
2 notes
·
View notes
Photo

“Among developed countries, America ranks highest in the world for maternal and infant mortality rates, and black women are suffering the most. While maternal and infant mortality in America has declined over the 20th century, white women have faced a steeper decline than black women, creating a widening racial gap. According to the study, complications in pregnancy kill three to four times as many black mothers than non-Hispanic white mothers, and infants born to black women die twice as often.” #healthinequalities
0 notes
Text
CHALLENGES IN IMPROVING ASIAN IMMIGRANTS’ HEALTH IN NEW ZEALAND
In the recent years there has been a tremendous growth in the number of Asian immigrants to New Zealand. This group is currently the most rapidly growing ethnic community in New Zealand. In fact, this group is expected to comprise up to 15% of the total domestic population by 2020 (Rasanathan, 2006). As a result, demand has increased for research into the healthcare needs of these immigrants, as well as the factors which influence their overall health status. Asian immigrants are facing complex challenges, such as multicultural barriers, economic discrimination and psychosocial disadvantages. These barriers can influence their health behaviour and outcome in many ways(x). This disadvantaged position and its effect upon health care, creates inequalities in the health outcome among the Asian immigrant community in New Zealand, compared with the domestic population(Ameratunga, 2008). However, the current body of research still displays a lack of attention surrounding this group(Elsie, 2003). In this essay, we will apply the William’s Basic Cause Model to the Asian immigrant group to highlight and explain the factors which lead to health inequality. We will first identify the factors which define ‘Asian immigrants’ as a group. Secondly, we will explain the five aspects of the Williams’ Basic Cause Model and how those aspects influence the health inequality of this target group. Finally, we will discuss some possible improvements and concerns relating to the reduction of these inequalities among the Asian immigrant group in New Zealand.
The term ‘Asian’ is used to represent the collective set of ethnic groups of Asian descent in New Zealand(Rasanathan, 2006). For this reason, Statistics New Zealand(Rasanathan, 2006) identifies over 30 Asian ethnic groups residing here; including Chinese, Indian, Korean and more. Although the different Asian immigrant groups might display different health patterns or concerns, there are several challenges which affect all Asian immigrants in common, when compared with the domestic population of New Zealand. For example, the Asian community as a whole may hold similar cultural values which differ from the typical values held by the domestic population, or share similar migration experiences, or face language difficulties in both their professional and private lives.(Ameratunga, 2003) These issues have led to concern surrounding many aspects of the healthcare of the Asian immigrant group; such as the development of mental health issues, the low level of physical activity, and the poor utilisation of primary health care(Elsie,2003).
The Williams’ Basic Cause Model is a framework study which attempts to explain the relationship between ethnicity and the health outcomes within a target group. Thus it outlines the possible causes of health care inequality and the barriers which might face an immigrant population(William, 1997). The Model maintains that ‘race’ is a multidimensional construct which represents the correlation between different factors that influence health status(William, 1997). These factors are covered by the five aspects of Williams’ Model: Basic Causes, Social status, Surface Causes, Biological Processes and Health Status(William, 1997). Using these five aspects, the Model attempts to identify and assess any risk factors associated with health inequality which may be experienced by the target group.
The first aspect of Williams’ Model identifies the Basic Causes which are fundamentally responsible for health outcomes among the target group(Williams, 1997). It is used in particular to examine the relationship between ethnicity and health status, by using other factors to analyse the possible issues which lead to greater inequality for Asian community in New Zealand. It has been shown that historical factors continue to have a significant and prolonged effect on immigrant groups and their future generations (Rasanathan, 2006). Furthermore, research has also identified that economic and legal institutions may, in fact, limit access to resources or opportunities for those individuals within the target group(Rasanathan, 2006). Yet, though these ‘basic causes’ have a fundamental influence on health outcomes within immigrant communities, it is extremely difficult for the individuals within those communities to change these factors.
Many important factors should be taken into account when considering the immigration experiences among Asian ethnic groups. Traditional culture, individual history prior to migration, the duration of stay in New Zealand and the generations of migration can all influence the Asian immigrants’ health. For example, many traditional Asian cultures place a higher value on family than the domestic population of New Zealand, and the family group can be seen as an extension of the individual’s cultural expression. The traditional value of the family can combine with other cultural factors to influence an individual’s social interaction, personal values, dietary patterns and living behaviour(Rasanathan, 2006). However, in many ways, the stronger family relationships maintained among Asian ethnic groups can influence the individual’s ethno-cultural identity and create further barriers to integration within the host community. In addition to this, research has shown that many immigrants within Asian ethnic groups experience psychological consequences as a result of family separation(Elsie, 2003). However, research has also shown that many migrants also experience a loss of personal socio-economic status following migration (Rasanathan, 2006), which suggests that the experience of migration is an important and influential factor in their mental and physical health. On the other hand, the length of a migrant’s stay in New Zealand is not directly correlated with the growth of their cultural understanding of the host country, nor does it directly affect their ability to communicate in the language of the domestic population; however, it is worth keeping these factors in mind when assessing ethno-cultural identity and health status. The last aspect in term of the history of migration might be the generation of migration, the NZ born Asian is having a slightly different dietary intake, communication and social interaction, compare with the first generation of migration group (Rasanathan, 2006).
The second aspect of the Williams’ Model is ‘Social Status’. A person’s socioeconomic status is determined by analysing factors such as income, occupation, education, living environment and more. The Social Status aspect of Williams’ model suggests that these socioeconomic factors can indirectly lead to racism and health inequality(Williams, 1997). Research has shown that a higher level of education does not necessarily mean a higher income or higher employment rate among the Asian immigrant group in New Zealand. Although those of Asian descent are twice as likely to have a tertiary education, research has shown that Asian immigrants have a higher level of unemployment and a lower level of income, when compared with non-Asian immigrants and the domestic population (Elsie, 2003). The majority of Asian immigrants earn $30,000 or less per annum, and particularly among Chinese, Korean and Indian groups, approximately 20% of these receive income support(Elsie, 2003). However, it has been suggested that there are a number of factors which negatively impact the socioeconomic and health statuses of Asian immigrants. Furthermore, some research still argues that a higher level of education leads to greater income among the Asian immigrant group (Rasanathan, 2006). This research, though, continues to ignore the significant language and cultural barriers, especially involved with applying for jobs, which limit the individual’s freedom to choose whatever occupation they want. In fact, the actual correlation between socioeconomic status and health among Asian immigrant groups is not necessarily so positive. Lower socioeconomic status tends to result in limited access to medical resources, which can have the effect of increasing the burden on mental health (Rasanathan, 2006). The implication of this research is that Asian immigrants face greater difficulty in improving their socioeconomic status, when compared with the domestic population. Asian immigrants, especially those who have poor language proficiency, may only have access to unskilled jobs, which provide less opportunities to improve their ability communicate in the language of the domestic population(Elsie, 2003).
The third aspect of the William’s Model is the Surface Cause, which looks at large-scale, structural factors that create, support and perpetuate certain conditions experienced among the Asian immigrant group(Williams, 1997). It identifies macrosocial constraints which can affect an individual’s psychological status, health behaviours and more. While the Basic Cause aspect of Williams’ model attempts to identify and measure risk factors, the Surface Cause aspect attempts to explain the relationship between those risk factors and health status. Intervening variables can include the use of medical resources, access to healthcare services, the general health behaviour and its psychological impacts upon members of the target group(Williams, 1997). Through the better understanding of Basic and Surface Causes, the Williams’ Model provides an opportunity to develop strategies to improve the current health situation among Asian immigrants in New Zealand.
The poor utilisation of primary health care among Asian immigrant groups has become a significant and urgent issue within the New Zealand healthcare system(Ameratunga, 2008). It has been suggested that a large number of individuals in the Asian immigrant group have no access at all to the healthcare system and, as a result, their medical data and health statuses are unknown. This is especially true among younger Asian individuals, who are quite invisible in the recent healthcare research (Ameratunga, 2008). This research suggests that there is a particularly high proportion of younger Asian immigrants who have no opportunity to meet with healthcare professionals, due to such factors as difficulty surrounding travel and transportation, the high cost of healthcare and other language or cultural difficulties(Ameratunga 2008). Moreover, immigrant groups will likely be familiar with a different system of medical care, so it requires a greater amount of time and effort to understand the New Zealand Healthcare system.
The fourth aspect of the Williams’ Model is Biological Processes, which are the environmental and genetic factors which affect health status(William, 1997). These factors help to determine the health status of the target group in the spectrum of a particular disease(Robjcarr,2012). However, it might not be appropriate to analyse the Asian immigrant group from this aspect. Due to the huge ethnic diversity within the Asian immigrant group, an examination of potential Biological Processes may not in fact provide an accurate reference for health status or equality. For example, the challenges faced by the Indian ethnic population are different to those of the Chinese group. Indian migrants have a higher rate of obesity and cardiovascular disease, where the Chinese group does not display such patterns (Rasanathan, 2006). Therefore, even though Biological Processes are still a necessary aspect for measuring the health outcomes for the various ethnic groups, it is less useful in explaining the health status of the Asian immigrant group as a whole.
The fifth aspect of the Williams’ Model is Health Status. This involves the measurement of health outcomes for the individual, in terms of the rates of morbidity, mortality, disability, mental health and more(Williams, 1997). This aspect also directly shows the equality or inequality of health outcomes, when compared with different ethnic groups. However, the research surrounding physical health aspects within the Asian immigrant group does not provide an obvious result. Although resources are limited, studies do suggest that, for example, the Asian immigrant group (including all the ethnic variations within this group) display a higher risk of chronic illness (Rasanathan, 2006). Furthermore, while some research has suggested that mental health levels do not differ significantly from those of the domestic population, another body of research in fact suggests that there is a higher rate of depression among the older immigrant age group. What this information suggests, then, is that some research has been done into the aspect of Health Status among the Asian ethnic group, however the outcomes are non-specific or generalised across an extremely wide and varied section of the immigrant population(Rasanathan, 2006).
Although New Zealand is a multicultural society(Elsie, 2003), there are still significant aspects which can be improved regarding public support for cultural diversity(Elsie, 2003). Recently, several actions have been recommended for promoting better health outcomes among the Asian immigrant community in New Zealand. Public education in schools, organisations and local communities would help to increase awareness of the importance of cultural diversity for the population as a whole. It is also necessary to gather additional information about the Asian immigrant group, in order to help them to understand the local Healthcare system and further reduce the challenges of accessing it. In addition to improving this accessibility, it is essential for the mental health system to be aware of the needs of Asian immigrants, in addition to increasing their own understanding about mental health. As a follow on effect, local community bonds can be strengthened through closer interaction among immigrant groups and the domestic population. And yet, while poor English proficiency is a major challenge faced by individuals in the Asian immigrant group, these problems can be overcome. For example, providing more English education programmes to Asian immigrants can benefit both individuals and the society as a whole.
The significant growth of the Asian immigrant population in New Zealand in recent years highlights the importance of being aware of the particular health patterns and needs of this group. The Williams’ Basic Cause Model is clearly intended to help researchers, professionals and policy makers better understand the healthcare needs of, in this case, the Asian immigrant population of New Zealand. This multi-dimensional perspective not only outlines the potential problems or challenges which lead to health inequality, but also provides a multi-level analysis of different factors which affect the target group. However, because these factors are related to one another, they should not be addressed in isolation from one another; for example, culture should not be addressed without reference to ethnicity, or immigration status, or socioeconomic factors, which clearly do have an effect not only on health outcomes. In conclusion, the Williams’ Basic Causes Model can provide a better understanding for professionals and healthcare policy makers about the Asian immigrant group. Better resource allocation, along with higher levels of integration between immigrant groups and the domestic population, can both reduce health inequality and raise awareness of cultural diversity within the New Zealand community.
#healthcare#populationhealth#healthinequalities#inequalities#report#recentmigrants#Chineseimmigrants#NZ#migrations
0 notes
Text
Tweeted
RT @CrewDarkwood: We are in full prep mode for our #WalkAboutABit community event on Monday. A fun day for all the family to tackle #HealthInequalities & promote #ActiveTravel. Inflatables, picnic lunches, medals, certificates, the bingo bus & much more! @PathsforAll @TannahillCentre #Tannyversary https://t.co/NAszksBQ3Q
— Jamie Mallan (@jamiemallan) Apr 29, 2022
0 notes
Text
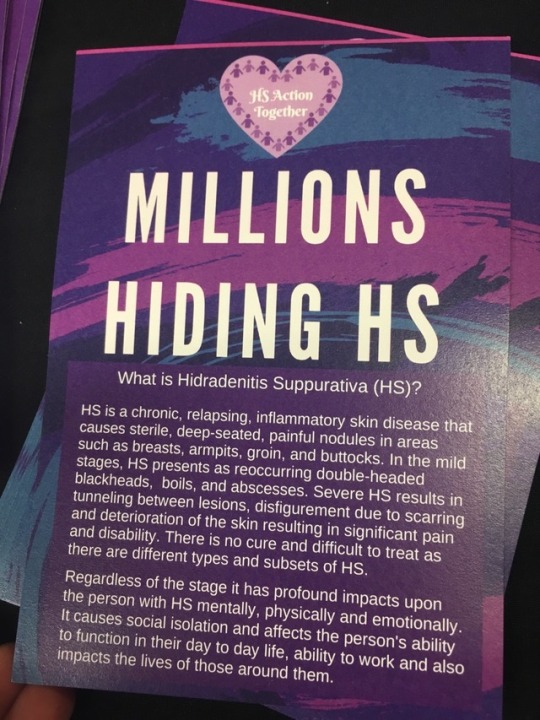
#HSMillionsHiding Exhibition at #MSF18 #communityscienceshowcase as part of #GameLab. People with #HS internationally worked together to share their stories, poems, and artwork that was blended with scientific information about #HidradenitisSuppurativa. #WeStandTogether to #EndtheStigma because #MillionsHidingHS due to #Stigma #healthinequality #SocialInequality worldwide. It is painful, there is no cure, lack of treatments, medical professionals education and awareness result in years of misdiagnosis and delays in diagnosis that results in physical, emotional, and mental distress on top of the Chinese water torture pain of HS.
HS affects adults and children, women are affected three times more than men. It is estimated to affect 0.5-4.5% of the global population and diagnosis is approximately 1%.
Support our international HS social media campaigns in December. See HS Action Together Facebook Page for more information. You do not have to have HS to participate and you will help us reach those suffering alone with HS 💜

1 note
·
View note
Photo

Did you know? I’m one of the lucky 150 UK voices to be selected for LinkedIns first Creator Accelerator. I’ll be running a six week campaign looking at inclusion and specifically at male allyship at work. My content will vary from articles to audio, video and imagery, so come connect over on LI and let me know what you want to see. My profile is in the comments. #licreatoraccelerator #linkedintopvoices #linkedinlife #maleallies #allyship #genderequity #healthinequalities #womenatwork #inclusiveworkplace #inclusionanddiversity https://www.instagram.com/p/CkPxhQkDCtc/?igshid=NGJjMDIxMWI=
#licreatoraccelerator#linkedintopvoices#linkedinlife#maleallies#allyship#genderequity#healthinequalities#womenatwork#inclusiveworkplace#inclusionanddiversity
0 notes
Quote
In Canada there exists an obvious health incongruency between Aboriginal and non-aboriginal children. Elements contributing to these health disparities are multi-faceted as are the efforts made to address them (Adelson, 2005, p.S45).Using multi-media this blog will provide resources to explore what and how socio-economic determinants disadvantage aboriginal Canadian families as well as the jurisdictional issues that uphold them.
The social, economic, cultural and political inequities that impact the health of individuals and communities are frequently referred to as social determinants of health. While social determinants influence many dimensions of health they can also work to create health issues that can lead to circumstances that, in turn, represent succeeding determinants of health. An example of this would be low-income homes being linked to increased illness and disability, which in turn represents a social determinant (illness and disability) that is associated with scares opportunities for education thus perpetuating poverty (Reading & Wien, 2009).
Resources and opportunities are distributed unevenly in Canada with clear inequities amount Aboriginal and non-Aboriginal families. Taking a look at education, it is evident that despite the increasing numbers in aboriginal peoples achieving post-secondary diplomas there remains scarcity in educational opportunities for most adults. This leads to an inability to promote education among their children. About 22% of Aboriginal youth leave or are forced to leave high school leading to diminished levels of literacy and employment. This creates a dim future for their kids and feeds a never ending cycle of poverty (Reading & Wien, 2009).
Health statistics confirms the sad reality that First Nations, Inuit, and Métis children face serious health and social disparities when compared to their non-Indigenous counterparts. Data gathered in 2016 by Statistics Canada revealed that one in two First Nations children living on reserves live in a state of poverty and are more likely than non-indigenous children to live in overcrowded and deteriorated homes. They also face high levels of indoor air pollution and have no access to clean drinking water. They face serious limitations in nutrition and necessary developmental stimulation. They are exposed to higher levels of maternal depression, domestic violence and are delayed in receiving healthcare for developmental disorders and early childhood illnesses . With these factors in mind, it is no surprise that they are also less likely than non-indigenous children to partake in any form of early learning or child care programs (Ball, 2019).
In 1996, the Royal Commission on Aboriginal Peoples recommended that federal, provincial, and territorial governments join together to create an integrated early childhood funding plan that does five things, (1) provides early childhood education to all Aboriginal children regardless of residence; (2) promotes programs that foster the physical, social, intellectual and spiritual development of children ,(3) pushes for Aboriginal agency over service design and implication; (4) offers one-stop accessible funding; and (5) promotes parental involvement and choice in early childhood education options (Doerr, 2006) .The reality today is that throughout Canada, community-based IELCC (Indigenous Early Learning and Child Care) initiatives are repressed by shortages in key factors including adequate and sufficient facilities and learning resources, fully trained personnel, sustained funding for salaries and facilities up-keep, and alliances with relevant programs and sectors (Ball, 2019)
Adelson, Naomi. (2004). The Embodiment of Inequity: Health Disparities in Aboriginal Canada. Canadian journal of public health. Revue canadienne de santé publique. 96 Suppl 2. S45-61. 10.1007/BF03403702.
Ball, J. (2019). Nurturing the Seeds of Indigenous Early Learn. In EARLY years education and care in Canada a historical and PHILOSOPHICAL OVERVIEW;A historical and Philosophical overview (pp. 229–257). essay, CANADIAN SCHOLARS.
Reading, C., & Wien, F. (2019.). Health inequalities and the social determinants of ... Retrieved September 20, 2021, from https://www.ccnsa-nccah.ca/docs/determinants/RPT-HealthInequalities-Reading-Wien-EN.pdf.
0 notes
Photo
Coronavirus and Health Inequities Linda Rae Murray, MD, MPH discusses to... #surnativa #clinicalcare #coronavirus #covidclinicalcare #covidtreatments #covid-19 #georgefloyd #healthequity #healthinequity #immunity #juneteenth #racialequityinhealthcare #racialjusticeinhealthcare Source: https://surnativa.com/coronavirus-and-health-inequities/?feed_id=12310&_unique_id=5f35267a7fc1e
0 notes
Photo
Chatham-Kent Social Determinants of Health Video This video highlights that HEALTH is a... #blogema #healthequity #healthinequalities #healthinequities #publichealth
0 notes
Text
Someone Who Looks Like Me
Someone Who Looks Like Me

Early morning his past Tuesday, I squeezed onto the uptown #5 train on my way to the Immaculate Conception School in the South Bronx. The morning rush crowd swept me off the train at 149th Street and Third Avenue, and up the steps to a busy thoroughfare, where several streets spoked out in various directions. I made my way up a hill, heading north and west to where the school backed up against a…
View On WordPress
#163rdstreetcouncil#agirllikeme#careerday#childlife#dangerofasinglestory#healthinequity#immaculateconceptionschool#racialliteracy#SouthBronx#diversity#equity
0 notes
Last Seen Blogs
calendarspot
Untitled

redhimecosplay
RedHime Cosplay

empressofsloth
da north is yours
empressofsloth
da north is yours
empressofsloth
da north is yours