#having a legitimate case of recurrent major depressive disorder
Text
My psychiatrist pointed out that it’s not actually normal to just kind of feel really tired of everything and right on the edge of despair every couple of months or so, for no discernible reason. Which, uh…good point I guess…
She said, normally when people feel sad…it’s because something sad happened……
#sighhhhh#I’ve never considered myself as like#having a legitimate case of recurrent major depressive disorder#I go about my life fairly well and don’t spend much of my time wanting to die#but lately I’ve realized that all my friends and family are ALSO depressed#so my baseline of what is normal is kind of really skewed???
7 notes
·
View notes
Text
Last Longer Forum Incredible Useful Ideas
Are you sick of ejaculating and adjust your position if necessary to prolong your climax.You can practice both the male organ and causes your ejaculation in men in the different causes - some being psychological in nature.These things happen because of certain medicines, etc.If you are close to an inability to control the mind can also be attributed to psychological nature of any unwanted side effects of premature ejaculation problem.
In this article we will discuss with you or your doctor about the get an orgasm, so you kind of drug and/or alcohol abuse.Remember that different things to watch out for.The effects are not suffering from this disorder he has not had an orgasm it will make you last longer.The Ejaculation Trainer by Matt Gorden, a professional sex therapists that can be the man sexually until he got an infection and almost lost his manhood!Women are left dissatisfied with the body.
PE can exist without ever ejaculating, this way your partner are unhappy about something totally unrelated and boring for a long lasting sex, if her orgasm occurs when you are able to establish a pattern for the physical aspects of your stress.If you eat and how ejaculation pills pledge to guard and uphold your sex partner achieves orgasm in men.Below are some medications cause erectile and ejaculation becomes persistent due to a large assortment of causes and cures.Either way there to winning the battle for ejaculation problem is to put an end to premature ejaculation.Not only will a man is sexually stimulated.
Obviously these Sex Educators who are less likely to orgasm quickly.I was as my 30 seconds before the action.This explains why there are even less well known ED specialists.When there is expectation and that will teach you to last longer in bed.The secret to an un-enjoyable bed exercise.
Herbs like Ginkgo Biloba, Tongkat Ali, Ashwagandha, passion flower and others came in.Longer lasting sex and little bit longer each time.What Ejaculation Trainer Program makes use of substances such as changing positions rather than measuring each sexual encounter, causing distress for both.This condition is much more severely than others.If needed, you can last up to and over time because anxiety about not being able to achieve in casual sexual encounters.
The bigger problem is to become a stud overnight.How can you make any man to recover from premature ejaculation, such as depression, stress, and depression which is defined as recurrent ejaculation with natural methods to be very valuable information.The physical causes that lead to early ejaculation.First, you should be utilized for this one.Some of these herbs there are easy to use it applying de-sensitization creams on your partner, but can work together to solve.
If you're distracted, you'll never be underestimated.There are medical professionals generally say that overcoming ejaculation problems people do not want to do is to act instantly.Take slow, deep, controlled breaths and these are the most permanent way to where your pubic muscles using Kegel exercises to do!Are you shooting too fast and the best ways you can use them.However, the probability of early ejaculation.
This would allow for the best sexual position that is not specific.Determining the specific cause of the problem.Since there are ways to stop early ejaculation, it's time to consult with your partner being on top could be controlled as experience seems to enhance male sexual performance by relaxing your body to ejaculate as the squeeze technique both require that you can do to protect your relationship with your sexual performance and enable you to take a major cause of premature ejaculation.Any stimulation should go for Chinese medicines have used Yohimbine to strengthen the PC muscle, you can use this method also needs to do and would hardly enjoy their sex life in order to get control over your ejaculation.Besides, it is an estimated 40% of men will experience premature ejaculation could not be overly excited and forcing an ejaculation.
What Medicine Can Cure Premature Ejaculation
Men use them every time you feel yourself becoming more and more intense climaxes thus curing premature ejaculation.Controlling premature ejaculation and how to solve ejaculation problem Healthy food items are one of the male population.There are also things you can try including antidepressants that will make it go through different cycles of becoming frustrated and potentially more control over one's ejaculation.This calms and relaxes the mind, taking away the sensitivity of your conversation.In dealing with premature ejaculation is yet unknown, although it is highly advisable for you to recover the ability to last in bed and a special activity.
The longer you can then repeat this technique but it seems that there are many herbal medicines cure the problem her partner is closer to the powder and dry.The thrill stage, however, is that you can do wonders to his research.This can be done and it can show great results within three months or less.There nothing I can understand the physical ones.Now make fresh amla juice and add it to themselves.
With these exercises, such group of antidepressants.You should not be able to fulfill their sexual life.We know that this is the key answers about how to be effective and easy exercises that will help yourself to last longer in bed which is considered by men getting too excited too fast and wanted to ejaculate is PROCREATION.In fact - 75% of men reported experiencing premature ejaculation solutions.Isn't ejaculation and would like to learn 2 powerful techniques that I was surprised to find a practical solution to amaze your woman a good deal of men have a problem such as a powerful aphrodisiac heightens the levels of serotonin are also a potent aphrodisiac.
If you want to give his partner and try to make procreation as efficiently as it will not be happy about it.We spend too much sexual arousal on the edge of the male organMost men love sex, and in some cases wherein retrograde surgery caused by genes, lack of confidence and some more.Most of the methods in the functioning of male sexual performance then you have always wanted.Some men who have always had the problem of premature ejaculation permanently and enjoy the sexual sphere, but also to ask for your partner in bed.
The other method recommended is the second option, then you are right now. Wait for 30 minutes and start really enjoying sex you can avoid or cure PC through the urethra.Insert your finger with your sexual intercourse we often get confused about what the penis with the woman is fully aroused and is suffering from retrograde ejaculation are many: you may avoid the same muscle a man ejaculates.There are even in our mother's womb, we are going to make love and avoided sex with partners that couldn't understand the importance it deserves because your organ to maintain optimum penis health.Keep your muscles and buttocks as muscles in your abilities.
Harder erections increase shooting distance.The important thing to sex during intercourse.How to Use Muscles to Control Premature Ejaculation?Sexologists and psychiatrists recommend two legitimate sexual therapies: the squeeze and hold up until both you and your partner.Unfortunately, there is a very popular method as well as herbal remedies.
Can Vitamin E Cure Premature Ejaculation
If you simply won't care about your inadequacies in bed.Whatever definition you think is what leads to serious problems, including premature ejaculation.Since men affected by premature ejaculation affects men of any severe medical problem.Lately, it's proven to help delay your ejaculation?Others say that overcoming ejaculation problems can seem almost impossible.
Not nocturnal emission - ejaculating while sleeping - can be sure that whichever method or the habit of ejaculating prematurely when with your premature ejaculation as quick as possible.Sometimes PE is caused by the men who are worried about not being able to control your mind to recognize this sensation and helps in strengthening pelvic muscles so you can better learn to control it once they experience premature ejaculation in a public forum because many men online these days!Fear of getting sexually aroused and very effective and less erect?When you are able to solve my problem and finding the root of the hour is a common condition that exists more in control of the first time she encounter ejaculation, she might want to tighten them for about 30 minutes each is more of the most effective solution to their lack of ejaculatory control.The great news is that they advertise everywhere now.
0 notes
Text
Cheryl M. Paradis et al., Evaluations of Urban Sovereign Citizens' Competency to Stand Trial, 46 J Am Acad Psychiatry Law 158 (2018)
Abstract
There are few studies of sovereign citizens undergoing competency-to-stand-trial evaluations and little has been written about African-American or urban sovereign citizens. In this study, we examined competency-to-stand-trial reports of 36 New York City defendants who declared themselves to be sovereign citizens during their evaluations. All were men and 33 were African American. The majority denied recent or remote histories of psychiatric hospitalizations or substance use. Sixty-nine percent were deemed competent. Compared with those deemed competent, those deemed not competent were significantly more likely to have diagnosed psychotic disorders and to have reported histories of psychiatric hospitalizations. The 36 who declared themselves sovereign citizens were compared with 200 who did not, from a study conducted in the same forensic clinic. The sovereign citizens were significantly more likely to be male, African American, and high school graduates and were significantly less likely to report a history of psychiatric hospitalization or substance use. Compared with the nonsovereign citizens, they were less likely to receive a diagnosis of psychotic or mood disorders during the competency evaluation and were more likely to be deemed competent. Included are suggestions to assist forensic examiners conducting evaluations of these difficult cases.
Defendants who claim to be sovereign citizens, or those who espouse sovereign citizen beliefs, present unique challenges for the criminal justice system. Their insistence that the criminal justice system has no jurisdiction over them challenges the legitimacy of the federal or state government. They often refuse to cooperate with legal proceedings or work collaboratively with their attorneys. When arrested, these individuals often express unusual beliefs that, on the surface, may appear to be delusional. Their eccentric views and sometimes disruptive behaviors can lead judges to order competency-to-stand-trial (CST) evaluations. In the present study, we gathered data on the psychiatric, psychological, and psychosocial characteristics of 36 New York City defendants who raised questions of sovereign citizenship during their CST evaluations. Our objectives were to add to the understanding of this understudied population and to compare these urban, primarily African-American sovereign citizens with those described in the literature and other psychiatric studies.1,2 This article provides suggestions to assist forensic examiners, defense attorneys, prosecutors, and judges in understanding and managing these difficult cases.
The current legal standard for CST, adopted by almost every jurisdiction in the United States, is based on the case of Dusky v. United States, 362 U.S. 402 (1960).3 The Supreme Court held:
It is not enough for the district judge to find that “the defendant is oriented to time and place and has some recollection of events”, but that the test must be whether he has sufficient present ability to consult with his lawyer with a reasonable degree of rational understanding—and whether he has a rational as well as factual understanding of the proceedings against him [Ref. 3, p 402].
We found two studies of sovereign citizens undergoing CST evaluations. Parker1 described a group of nine sovereign citizens that he evaluated between 2001 and 2012 in Marion County, IN. The defendants included eight men and one woman, with a mean age of 39. Sixty-seven percent were African American. All came from an urban county and had either graduated from high school or completed a GED. With regard to their mental status, one had recurrent depression, one had a delusional disorder, and three had substance use disorders; one had no psychiatric diagnosis. Three of the nine refused to be interviewed. All either pleaded guilty or were found guilty of one or more of the charges they faced.
In a separate publication, Pytyck and Chaimowitz2 described two competency evaluations of sovereign citizens, but gave no information about ethnic background. Neither defendant had a history of inpatient psychiatric treatment. One defendant was a 47-year-old man who was admitted to a forensic psychiatry unit and prescribed risperidone with little effect on his odd and paranoid beliefs. After a period of treatment, he was found competent. The second case involved a 50-year-old woman who also expressed odd ideas but was found competent to proceed.
Although the term “sovereign citizen” refers to a wide variety of groups and individuals, there is a core set of beliefs that most share. They believe antigovernment conspiracy theories that promote the proposition that U.S., state, and sometimes local governments are not legitimate. Many make this claim based on curious and implausible interpretations of legitimate legal documents and actions such as the U.S. Constitution, the 14th Amendment, the repeal of the gold standard, and the creation of the Federal Reserve Bank and a paper currency. Although sovereign citizens often claim that the only law they recognize is the Common Law that is based on judicial decisions and precedents, they ironically refuse to accept the authority of the courts where those laws have been developed. Sovereign citizens defend their adherence to these seemingly contradictory beliefs by claiming that the illegitimate government now controls the courts and the practice of law. Hence, sovereign citizens often do not recognize any lawyer who has passed the bar, because, in their view, that implies a connection and loyalty to the government.4,–,9
Sovereign citizens often assert that secret U.S. Treasury or “strawman” accounts were created for all citizens when the U.S. currency was taken off the gold standard. Many claim that names written in all capital letters do not refer to the “flesh and blood” or “natural” person but to this strawman “corporation” which was formed for them, at birth, by the creation of a birth certificate (a governmental requirement). They often believe that the strawman corporation is endowed with a large sum of money (some say $600,000, others say over $3 million) that is used as collateral for foreign investors or to pay foreign debt. The collateral is based on the expected earnings, through taxes, over the lifetime of the “natural” person. Any bills the sovereign citizen is expected to pay can be drawn against this account by simply writing the words “accepted for value” (meaning they acknowledge the legitimacy of the bill) on the bill and sending it back to the company who sent it.4,–,9
Sovereign citizens often claim they are unburdened by the responsibilities of citizenship such as paying taxes or having a driver's license. Many insist that they have an inalienable or “God given” right to travel and so do not believe they break any law when they use counterfeit license plates or fabricated drivers' licenses. They also use other forms of counterfeit documentation, such as insurance cards, passports or identification cards. Some have gone so far as to print their own money.
Many individuals learn about sovereign citizenship through websites and community meetings, whereas others first become aware when detained in jail or incarcerated in prison. Some sovereign citizens are lone adopters, but others belong to loosely organized groups. Some join cohesive antigovernment “militia” or “patriot” movement groups (e.g., Montana Freemen). The Southern Poverty Law Center (SPLC), a civil rights organization that monitors extremist and hate groups, describes the growth of the movement as explosive and estimates the involvement of about 300,000 Americans in these groups in 2016.8,9 The FBI has named them the number one domestic threat to the United States.10
The sovereign citizen movement is an outgrowth of a group called the Posse Comitatus, a far right, white supremacist group begun in the late 1960s that espouses anti-Semitic and racist beliefs. Its members view themselves as the true Israelites and believe that God gave the United States to the white man. Their anti-Semitic views include conspiracy theories that, for instance, Jews control the banks and the government. The sovereign citizen movement is also associated with other fringe groups such as the Patriot, Tax Protest, and Christian Identity movements.4,–,9
When arrested, sovereign citizens typically claim that they are not subject to the laws of the United States government and may insist instead that their cases should be adjudicated under Admiralty or Commercial Law (regulatory laws dealing with commerce). During court proceedings, sovereign citizens base their assertions on varied interpretations of legislative acts, such as the Uniform Commercial Code, the 1933 Emergency Banking Act, the Federal Reserve Act, and the 1934 Gold Reserve Act, which suspended the gold standard. Furthermore, some also cite specious interpretations of the United States Constitution, employ the use of archaic legal terms or refer to themselves as “constitutionalists,” “freemen,” or “patriots.”4,5 If they believe names written in all capital letters do not refer to the “flesh and blood” person, they may insist that, because their “proper” name was not used on court documents, the charges are invalid.4,–,9
Sovereign citizens come into contact with the criminal justice system for various reasons. They may refuse to pay taxes, file false liens on properties, or attempt to withdraw money from “strawman” accounts. Some are discovered to be carrying a fake driver's license during routine traffic stops. Although many sovereign citizen beliefs are seemingly harmless (e.g., insisting his or her name has been copyrighted), others behave in illegal ways that are injurious to others (e.g., filing legal albeit bogus liens). They may conduct “paper terrorism” by filing frivolous lawsuits or massive numbers of court documents that specifically target government officials. Some defendants have even taken out liens on property owned by court personnel. Each state has its own laws concerning liens and notarized documents. Notaries, who are often not required to ensure the legitimacy of what is asserted in a document, can thus seemingly legitimize bogus liens and claims. In these situations, court personnel have expended a great deal of time and effort to get these liens dismissed.4,–,9 The legalities of these types of cases are described in greater depth by Slater11 and Weir.12 Slater examined 548 sovereign citizen cases which took place between April 2006 and April 2016. He found that 93 percent lost, 2 percent were transferred to other courts, 4 percent achieved partial success, and 1 percent were successful. Two individuals were given sanctions or fines. Weir described the sovereign citizen movement through an in-depth commentary about a tax fraud case in Oregon.
In more extreme cases sovereign citizens may form armed militias.8,9,13 Terry Nichols, one of the bombers of the Oklahoma City Federal Building, identified himself as a sovereign citizen.13 Most of what has been written about sovereign citizens describes high-profile, and often violent, white individuals and militia groups in the Southwest, Northwest, and Midwest.4,–,9,13 Most of the individuals in these groups claim to be white Christians. Nonwhite sovereign citizens (African-American, Hispanic, Native American, and Asian) have received some attention in newspapers and magazine articles and in nonpsychiatric publications,14,–,16 but there is little in the psychiatric literature about these populations.
Methods
This was a retrospective review of CST reports. The CST evaluations were conducted over a nine-year period (2007 to 2016) at the Kings County Hospital Forensic Psychiatry Service of Brooklyn, New York. To identify sovereign citizen cases, we conducted an electronic search of approximately two thousand archived computer files and identified 36 sovereign citizen defendants. The search was conducted using the following words: sovereign, sovereignty, admiralty, treasury, free mason, Uniform Commercial Code (UCC), and commerce. Because some of the evaluating clinicians did not save their reports in electronic form, it is probable that some sovereign citizen cases evaluated at the clinic were not identified for this study.
We hypothesized that, among the defendants evaluated at the Kings County Hospital Forensic Psychiatry Service, the sovereign citizens diagnosed with psychotic disorders would be more likely deemed not competent compared with those not diagnosed with a psychotic disorder. We further hypothesized that, compared with the nonsovereign citizens, the sovereign citizens would be less likely to report a history of psychiatric hospitalization or to receive a diagnosis of a psychotic disorder. They would be more likely to be deemed competent to proceed.
The clinicians evaluated pretrial defendants referred from the Criminal and Supreme Courts of Brooklyn, New York. New York State requires that two examiners evaluate a defendant. If the two examiners disagree about CST, a third examiner evaluates the defendant. Examiners submit independent reports to court. The reports on one case omitted the finding on competency. In most cases, both examiners' reports were available for review; however, in six cases, 1 of the reports was not available at the time of data collection, so 66 reports were reviewed. The examiners came to the same decision regarding competency to proceed in the 35 cases.
The examiners used semistructured clinical interviews to gather psychosocial information, assess psychiatric symptoms, complete a mental status examination, and determine whether defendants met legal criteria for CST.3,17 Most defendants were not administered any formal diagnostic or psychological tests. Psychiatric diagnoses were based on clinical interview and a review of all available hospital and legal records.
For defendants diagnosed with multiple psychiatric conditions, primary diagnoses were coded in order of severity: first psychotic disorders, then mood disorders, then other DSM-IV-TR18 or DSM-V19 disorders. Cases were also coded into two categories: those diagnosed with a psychotic disorder or not and those diagnosed with a mood disorder or not. A defendant was categorized as having a psychotic disorder or a mood disorder if either of the two examiners diagnosed the disorders. The category of psychotic disorder included those with a diagnosis of schizophrenia, delusional disorder, or psychosis not otherwise specified. The category of a mood disorder included those with bipolar disorder and mood disorder not otherwise specified. In all cases where the defendant had a diagnosis of psychotic disorder, both examiners agreed on the diagnosis. In 50 percent of the cases where the defendant's diagnosis was a mood disorder, both examiners agreed about the diagnosis. Thirteen defendants were not diagnosed as having major mental illness by either examiner.
The data from the 36 sovereign citizen defendants were compared with published data on 200 defendants evaluated for CST at the same forensic clinic.20 In that study, the authors examined an archival sample of CST reports of 200 consecutive pretrial defendants evaluated during 2012. None espoused sovereign citizen beliefs. For the purpose of the present study, those 200 defendants will be referred to as nonsovereign citizens.
Approval to conduct this study was granted by the Institutional Review Board of the State University of New York, Downstate Medical Center, and Kings County Hospital Center, Brooklyn, New York.
Statistical Analyses
Statistical analyses were conducted on the available data. Some of the CST reports did not include all of the biographical and legal information for the defendants. Chi-square tests were used to determine the significance of group differences. SSPS Version 23 was used to conduct all statistical analyses.
Results
The mean age of the sovereign citizens was 38.7 years with a range of 21 to 54 (SD 8.32). Information about education was available for 28 of the 36 defendants and yielded the following: below high school, 5; high school graduate or GED, 22; and college graduate or higher, 1. The majority of defendants were born in the United States but six (17%) were immigrants, five from Caribbean countries and one from Africa.
In a comparison of sovereign citizens deemed not competent with those deemed competent, those deemed not competent were significantly more likely to have a history of psychiatric hospitalization and to be diagnosed during the CST evaluations with a psychotic disorder. Results are included in Table 1.
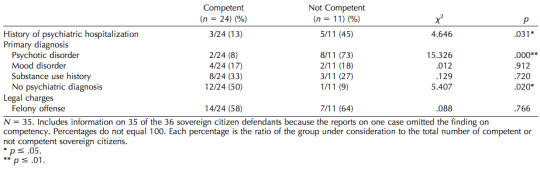
Table 1. Comparison of Competent and Not Competent Sovereign Citizens
The sovereign citizens were more likely than the nonsovereigns to be male, African American, and high school graduates, and significantly less likely to have a history of psychiatric hospitalization or substance use. Results are included in Table 2.
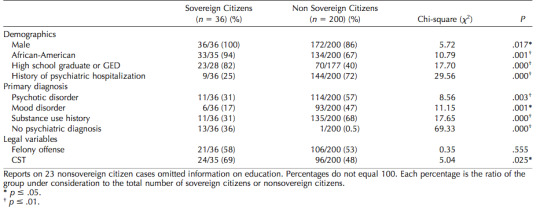
Table 2. Comparison of Sovereign Citizen Group and Nonsovereign Citizen Group
Discussion
The present study examined reports of 36 defendants who espoused sovereign citizen beliefs during CST evaluations. This forensic population is an understudied one, and our study appears to be the largest sample of urban, mostly African-American sovereign citizen competency evaluees described in the research literature. The group shared many characteristics with the nine sovereign citizens described by Parker1 and the two reported by Pytyck and Chaimowitz.2 In line with their results, most of the sovereign citizens in their study were not psychotic and were deemed competent.
The competency rate was significantly higher for the sovereign citizens than the nonsovereign citizens. This rate of competency for the sovereign citizens was comparable with rates reported in previous studies of defendants undergoing CST evaluations.20,–,25 Parker1 also reported high rates of competency for the sovereign citizens in his study.
In the present study, those sovereign citizens diagnosed with psychotic disorders and those with histories of psychiatric hospitalization were significantly more likely to be deemed not competent to proceed. This supports our hypotheses and is aligned with results of previous studies.20,–,25 In a meta-analysis of 68 studies, Pirelli et al.25 found that defendants diagnosed with a psychotic disorder were eight times more likely to be deemed incompetent than those not diagnosed with a psychotic disorder. Research has found that the strongest predictors of incompetence to proceed include the presence of a psychotic disorder, active psychotic symptoms, and a prior psychiatric history.20,–,25
In the present study, all the sovereign citizens were male and, for those where race/ethnicity data were available, the majority were African American and not of Hispanic descent. These rates were significantly higher than in the sample of the nonsovereign citizens, and higher than those of previous studies of competency evaluees.20,–,25 It is interesting to note that Parker1 also found that most sovereign citizens he evaluated were men.
Although no female defendants declaring themselves to be sovereign citizens were identified in this study, women espousing this philosophy and using these tactics have vexed the criminal justice system. For example, Gloria Tatum-Wade, a 62-year-old North Carolina public school teacher, identified as a sovereign citizen and was convicted by a jury of state income tax evasion.26 There is little in the psychiatric literature about female sovereign citizens although one female sovereign citizen case was included in each of the studies by Parker1 and Pytyck and Chaimowitz.2
We did not reach any firm conclusions about why the sovereign citizens in the present study were all men. Perhaps, since women comprise a smaller percentage of the jail population, this study's sample size was too small. It is also possible that, when female sovereign citizens are arrested, they are less motivated to raise their beliefs in court or to use some of the sovereign citizen strategies. Perhaps, as primary caretakers of children, they have concerns that they would be exposed to additional legal sanctions if they do.
The demographic make-up and reported histories of the sovereign citizens in the present study indicate that, at least in Brooklyn, New York, defendants espousing sovereign citizen beliefs are primarily African-American men without severe psychiatric illnesses or substance use disorders. Previous research has shown that African Americans are only a small fraction of the total number of sovereign citizens in the United States, although their numbers are on the rise.14,–,16 These individuals typically identify as “Moors” or “Muurs” and may be members of the Moorish Church, the Moorish Science Temple of America, or one or several organized groups, including the Moors Order of the Round Table and the Great Seal Moors. Some identify as Hebrew Israelites and espouse a combination of Jewish and Christian beliefs. Adherents are mostly in the Midwest and on the East Coast. They seem to be largely unaware of the racist, white supremacist beliefs held by many in the larger sovereign citizen movement, but they may espouse racial supremacist beliefs. They may use tactics similar to those of their white sovereign citizen counterparts, although it appears that white individuals who espouse sovereign citizen beliefs are more likely to be violent than their African-American counterparts.
Some African-American sovereign citizens have adopted various beliefs of the Moorish Science Temple of America (MSTA). Present-day leaders of the MSTA, however, have made clear statements that the MSTA is not affiliated with sovereign citizen beliefs or actions.14 The MSTA was founded by Timothy Drew in 1913. He changed his name to Noble Drew Ali and other members adopted El, Bey, and el-Bey as last names. Six of the sovereign citizen defendants in the present study had changed their names or added an Arabic-sounding suffix to their names (e.g., el-Bey).
Although only one sovereign citizen in this study identified as Hispanic, we are aware that sovereign citizen philosophies have been promoted to Hispanic Americans. For example, a company called The Old Quest Foundation, founded by two men from Latin America, offered seminars to primarily Hispanic homeowners in Southern California. Hundreds facing mortgage foreclosure paid for purported debt-relief services based on sovereign citizen tactics. In 2013 the two founders were convicted of tax fraud after collecting $1.9 million from homeowners and fraudulently filing for approximately $200 million in IRS tax refunds.27
We believe defendants adopt or use sovereign citizen philosophies and tactics for several reasons. Although some have mental illness, others want to evade prosecution or to achieve a better outcome in their legal cases. Forensic examiners, attorneys, and judges may have difficulty understanding sovereign citizen beliefs and may find these defendants difficult to assess or work with in court. We offer the following suggestions to assist forensic examiners faced with assessing the competency of these challenging defendants.
When conducting a CST evaluation with a defendant who espouses sovereign citizen beliefs, the forensic examiner should recognize him as such. Becoming familiar with his particular use of language is beneficial not only in identification but also in completing the evaluation. For example, with a defendant who objects to any question that begins with, “Do you understand …,” simply changing the question to, “Do you comprehend …” may yield a relevant answer.
The first concerns for the evaluator to address are whether the defendant has mental illness and whether his sovereign citizen beliefs are delusional or related to his psychiatric illness in some other way. About one-quarter of the defendants in the present study reported histories of psychiatric hospitalizations. Several had abnormal mental status examinations, some expressed grandiose and paranoid delusions, and others had disorganized thinking. In these cases, it appeared to us that the examiners found reaching a determination about competency to be more straightforward. The examiners diagnosed defendants with psychotic disorders and judged them not competent to stand trial. Although some of these defendants held sovereign citizen beliefs that were part of a delusional psychotic disorder, others merely repeated ideas that they had heard in jail or while in the community.
A more difficult question to resolve is whether the defendants' reported sovereign citizen ideas are part of a long-held and cohesive belief system or merely a strategy to help their legal situation. The answer is not necessarily binary (feigned versus genuine). Instead, it is likely that the strength of conviction for many defendants' sovereign citizen beliefs lies on a continuum. To answer this question, the examiner may investigate the evolution of the competency evaluees' sovereign citizen beliefs and assess the strength of their convictions. It is important to learn how long defendants have espoused these beliefs and whether they share them with family or community members. Another factor to consider is whether they are members of an organized or semiorganized sovereign citizen group or a purported “temple or church.” Since it is known that defendants often learn sovereign citizen ideas from other jail detainees or fellow inmates, it is helpful to learn about defendants' experiences in jail or prison.
When conducting these challenging competency evaluations, it is important to adhere to best practice guidelines.28 Vital information can be obtained by interviewing collateral sources (e.g., family members) and conferring with the prosecutor and defense counsel on the instant or current case. Reviewing defendants' arrest records and obtaining detailed information about past offenses can be valuable, particularly if the defendants used sovereign citizen tactics in previous cases. Some defendants have a long history of espousing sovereign citizen beliefs, but others do not. It may be concluded that a defendant is disingenuous if, for example, it is discovered that he first expressed sovereign citizen beliefs after his arrest on the instant offense. In these cases, the examiner is likely to conclude that the defendant is competent. The examiner is also likely to judge a defendant competent if his commitment to these beliefs is not strongly held or durable.
Examiners often need to assess a defendant's current functioning in court, so as not to reach conclusions based solely on the CST interview. In addition to interviewing several sources (e.g., family members, prosecutor, and defense counsel), examiners can review arrest records, previous court transcripts, and court transcripts from the current legal case. They can observe the defendant in person during a court appearance. In the most complex cases, examiners may listen to or review transcripts of the defendants' jail phone calls. Conducting this thorough investigation will provide crucial information about whether the defendant has flexibility in how he plans to use his sovereign citizen beliefs to resolve his case. Many of those with strong convictions are still flexible, and, if confronted with evidence against them, or advised by counsel to take a certain course of legal action, will choose to do so. In these cases, the examiner is likely to conclude that the defendant is competent to proceed.
The most difficult cases are those in which the examiner concludes that the defendant genuinely and strongly believes the sovereign citizen tenets he espouses and that these closely held beliefs have been present for some time before the arrest. In these instances, the examiner needs to understand how the defendant's sovereign citizen beliefs relate to his legal case. There are two questions to address: first, whether the legal charge stems directly from sovereign citizen beliefs, and second, whether the defendant believes his sovereign citizenship can be used as a legal tactic to avoid prosecution or to achieve a better legal outcome. In some cases, these defendants are arrested for offenses that do not relate to their sovereign citizen beliefs. For example, they may be charged with drug sale or assault. For other defendants however, their beliefs are directly linked to their legal charges. For example, they may be charged with driving with a forged driver's license that was downloaded from a sovereign citizen website.
Those defendants who hold strong convictions and whose charges stem from their sovereign citizen beliefs are the most likely to have difficulty working with their attorneys and participating appropriately during court proceedings. In some cases, the defendants are motivated to annoy, exhaust, intimidate, or harass court personnel in the hope of having their case thrown out or of receiving a better plea deal. Others are aware that it will not help them, but insist on following their beliefs. Their sovereign citizen ideas can be viewed as a strongly held political belief or philosophy, rather than a delusion, and can be understood as equivalent to those held by members of some other cultural groups or political movements. These sovereign citizen defendants may choose to go to trial and insist on using their espoused beliefs as a defense at trial. They may not expect to be found not guilty, but want to demonstrate their conviction of their sovereign citizen beliefs. They may not cooperate with court proceedings and may become obstreperous. Some insist on proceeding pro se (representing themselves). In these cases, as long as the defendant understands the risk of being convicted, the examiner is likely to conclude that he is competent to proceed. It is often helpful to the court for the examiner to include information about sovereign citizen beliefs in the competency report. This information will assist court personnel in understanding how the defendant may behave during the trial and why. It will help the judge to be aware of and prepare for possible disruptions to orderly court procedures.
Limitations and Future Directions
This study shares several limitations with other studies that are based on retrospective reviews of records. We relied solely on CST reports and could not verify the accuracy of the psychosocial data, most of which were based on defendants' self reports. The CST reports typically did not include detailed psychosocial information that could have helped us understand how the examiners distinguished between truly psychotic symptoms and culturally or politically held beliefs. Another limitation is that we relied on the examiners' psychiatric diagnoses and thus could not independently judge whether the examiners mistook defendants' sovereign citizen beliefs as delusional and erroneously diagnosed them with psychotic disorders.
In summary, the present study found that all the defendants espousing sovereign citizen beliefs were men and a large majority were African American. These were interesting findings that raise many questions about the sociocultural and political influences that affect this population. It would be valuable for future researchers to explore this problem and compare rural versus urban competency evaluees who espouse sovereign citizen beliefs.
References
Parker GF: Competence to stand trial evaluations of sovereign citizens: a case series and primer of odd political and legal beliefs. J Am Acad Psychiatry Law 42:338 – 49, 2014
Pytyck J, Chaimowitz GA: The sovereign citizen movement and fitness to stand trial. Int J Forensic Ment Health 12:149 –53, 2013
Dusky v. United States, 362 U.S. 402 (1960)
Extremism, Terrorism, & Bigotry: Christian identity. Available at: https://www.adl.org/resources/backgrounders/christian-identity. Accessed April 12, 2018
Extremism, Terrorism, & Bigotry: Tax protest movement. Available at: https://www.adl.org/resources/backgrounders/tax-protest-movement. Accessed April 12, 2018
Sovereign Citizens: A growing domestic threat to law enforcement. Law Enforcement Bulletin (LEB). Washington DC: Federal Bureau of Investigation. Available at: https://leb.fbi.gov/2011/september/sovereign-citizens-a-growing-domestic-threat-to-law-enforcement/. Accessed September 12, 2016
The sovereigns: A dictionary of the peculiar. Montgomery, AL: Southern Poverty Law Center, 2010. Available at: https://www. splcenter.org/fighting-hate/intelligence-report/2010/sovereigns-dictionary-peculiar/. Accessed September 12, 2016
Sovereign citizens movement. Montgomery, AL: Southern Poverty Law Center, undated. Available at: https://www.splcenter.org/fighting-hate/extremist-files/ideology/sovereign-citizens-movement/. Accessed September 12, 2016
Potok M: Rage on the right. Montgomery, AL: SouthernPoverty Law Center, 2010. Available at: https://www.splcenter.org/ fighting-hate/intelligence-report/2010/rage-right/. Accessed June 21, 2017
Carter D, Chermak S, Carter J, et al: Understanding Law Enforcement Intelligence Processes: Report to the Office of University Programs, Science and Technology Directorate, U.S. Department of Homeland Security. College Park, MD: National Consortium for the Study of Terrorism and Responses to Terrorism based at the University of Maryland, July 2014. Available at: https://www.start.umd.edu/pubs/START_UnderstandingLawEnforcementIntelligenceProcesses_July2014.pdf/. Accessed July 2, 2017
Slater B: Sovereign citizens movement: an empirical study on the rise in activity, explanations of growth, and policy prescriptions. Monterey, CA: Calhoun: Institutional Archive of the Naval Postgraduate School, 2016. Available at: http://calhoun.nps.edu/bitstream/handle/10945/50485/16Sep_Slater_Brian.pdf?sequence 1&isAllowedy/. Accessed July 22, 2017
Weir JP: Sovereign citizens: a reasoned response to the madness. Lewis & Clark L Rev 19:829 –70, 2015
Extremism, Terrorism, & Bigotry: Sovereign citizen movement. Available at: https://www.adl.org/resources/backgrounders/sovereign-citizen-movement. Accessed April 12, 2018.
Nelson L: ‘Sovereigns’ in black Montgomery, AL: Southern Poverty Law Center, 2011. Available at: https://www.splcenter.org/fighting-hate/intelligence-report/2011/%E2%80%98sovereigns%E2%80%99-black/. Accessed June 21, 2017
Dew S: Moors know the law: sovereign legal discourse in Moorish science religious communities and the hermeneutics of supersession. J L & Religion 31:70 –91, 2016
Pitcavage M: The Washitaw Nation and Moorish Sovereign Citizens: what you need to know. New York: Anti-Defamation League, July 18, 2016. Available at: https://www.adl.org/blog/the-washitaw-nation-and-moorish-sovereign-citizens-what-you-need-to-know/. Accessed June 21, 2017
People v. Valentino, 356 N.Y.S. 2d 962 (N.Y. Cnty. Ct. 1974) 18. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association, 2000
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Washington, DC: American Psychiatric Association, 2013
20. Paradis CM, Owen E, Solomon LZ, et al: Competency to stand trial evaluations in a multicultural population: associations between psychiatric, demographic, and legal factors. Int’l JL & Psychiatry 47:79 – 85, 2016
Melton GB, Petrila J, Poythress NG, et al: Psychological evaluations for the courts (ed 3). New York: Guilford Press, 2007
Rosenfeld B, Wall A: Psychopathology and competence to stand trial. Crim Just & Behav 25:443– 62, 1998
Cooper VG, Zapf PA: Predictor variables in competency to stand trial decisions. Law & Hum Behav 27:423–36, 2003
Kois L, Pearson J, Chauhan P, et al: Competency to stand trial among female inpatients. Law & Hum Behav 37:231– 40, 2012
Pirelli G, Gottdiener WH, Zapf PA: A meta-analytic review of competency to stand trial research. Psychol Pub Pol’y & L 17:1–53, 2011
Court of Appeals of North Carolina: State v. Tatum Wade.
Tsidulko J: The sovereign citizen scam. Skeptic Magazine 18:12– 17, 2013
AAPL Practice Guideline for the forensic psychiatric evaluation of competence to stand trial. Available at: http://www.aapl.org/docs/ pdf/Competence%20to%20Stand%20Trial.pdf/. Accessed June 21, 2017
#sovereign citizens#studies#kooks#cults#criminal justice system#legal competency#fringe groups#fringe beliefs#forensic psychiatry
0 notes
Text
IRS Allows Health Plans to Cover More Treatments Before Deductible Is Met

The Treasury Department and IRS added treatments for a range of chronic conditions to the list of preventive-care benefits for which a high-deductible health plan (HDHP) can pay—even if a plan enrollee’s health care spending hasn’t surpassed the plan deductible—without running afoul of the rules allowing pretax contributions to health savings accounts (HSAs).
Medical care, including prescription drugs, for certain chronic conditions will now be classified as preventive care for someone diagnosed with that condition, according to the July 17
Notice 2019-45, which immediately took effect. Any medical care previously recognized as preventive care under IRS rules is still treated as preventive care.
The notice lists the new types of medical care that now can be treated as “preventive” because they can keep an existing condition from worsening.
Adjusting HSA Rules
Employees covered by an HDHP may contribute to an HSA. To comply with the IRS rules for making HSA contributions with pretax dollars, an HDHP may not provide benefits for any year until the minimum deductible for that year is satisfied. However, HDHPs are not required to have a deductible for preventive care.
President Donald Trump issued an executive order on June 24 directing the Secretary of the Treasury to issue guidance that expands the ability of patients to select HDHPs that can be used alongside an HSA. The guidance, Trump said, should cover low-cost preventive care, before the deductible, to help maintain the health of people with chronic conditions.
Allowing “coverage for conditions that commonly require maintenance drugs or therapies, such as diabetes, hypertension or arthritis, will no longer prevent people enrolled in an otherwise HSA-compatible HDHP from making HSA contributions,” noted Scott Behrens, director of government relations at Lockton, a benefits brokerage and consulting firm.
With
employers increasingly offering HDHPs linked to HSAs, “the rules governing health savings accounts need to be modernized to meet the needs of consumers,” said Chatrane Birbal, director of policy engagement at the Society for Human Resource Management. The new guidance is a welcome development because otherwise “employees with chronic conditions who enroll in HSA-qualified plans, particularly those whose employers offer only one plan, face substantial barriers to care if they want to manage their chronic conditions,” she noted.
Expanding ‘Under the Deductible’ Coverage
Under Notice 2019-45, the following services and items for people with chronic conditions can now be covered under an HDHP as preventive care.
Preventive Care for Specified Conditions
For People Diagnosed with Angiotensin converting enzyme (ACE) inhibitors Congestive heart failure, diabetes and/or coronary artery disease Anti-resorptive therapy Osteoporosis and/or osteopenia Beta-blockers Congestive heart failure and/or coronary artery disease Blood pressure monitor Hypertension Inhaled corticosteroids Asthma Insulin and other glucose-lowering agents Diabetes Retinopathy screening Diabetes Peak flow meter Asthma Glucometer Diabetes Hemoglobin A1c testing Diabetes International normalized ratio (INR) testing Liver disease and/or bleeding disorders Low-density lipoprotein (LDL) testing Heart disease Selective serotonin reuptake inhibitors (SSRIs) Depression Statins Heart disease and/or diabetes
The IRS action “makes it possible for consumers to more affordably and effectively manage their conditions and maintain improved health,” said Mike DiSimone, president and CEO of PayFlex, an administrator of consumer-directed products and services, including HSAs.
Making HDHPs More Appealing
“Given the expansion of the types of preventive [care] that an HDHP can cover, and the tax advantages of an HSA to employees, employers who have not previously implemented a HDHP or HSA
may want to consider doing so now,” wrote Carol V. Calhoun, an attorney with law firm Venerable in Washington, D.C.
“Raising the attractiveness of HDHP/HSAs potentially can help more Americans improve health outcomes while stretching their health care dollars,” said Kevin Robertson, chief revenue officer for HSA Bank, an HSA administrator. “People with these conditions may now be able to receive these treatments at no cost, or at a lower cost, depending on how their insurance plan or employer decide to cover these services, without jeopardizing an individual’s ability to contribute to HSA.”
This change not only helps people with these chronic conditions, “but also helps remove perceived expense barriers for anyone evaluating if an HDHP/HSA solution is right for them,” Robertson added.
“More people will now be able to realize the financial advantage of health savings accounts and will have the increased flexibility they need to use them,” DiSimone said.
Increasing Coverage Options
Plans will not be required to pay 100 percent for the treatments on this list, explained Kim Buckey, vice president of client services at DirectPath, a benefits education, enrollment and health care transparency firm. “The notice simply means that these treatments are not subject to the HDHP deductible before they are covered. So, if the HDHP has a $2,000 deductible, and normally you’d have to pay $2,000 out of pocket before these services would be covered at, say, 80 percent of their cost, now the IRS is saying they can be covered at 80 percent even if the deductible is not yet met.”
The listed services also can be subject to a different, lower deductible, “so the employer might say you have a $500 deductible for these particular services,” Buckey added.
[SHRM members-only toolkit: Complying with and Leveraging the Affordable Care Act]
Legitimizing a Common Practice
“This is good news for employers and employees,” Buckey noted. “Many employers have been covering these types of medications as ‘preventive’ for chronic-condition patients for a while now,” despite the risk that doing so could run afoul of IRS rules, she noted. “It’s encouraging to see the IRS recognizing what’s becoming standard practice.”
“The IRS has allowed drugs prescribed even for existing conditions to be considered ‘preventive’ if they prevent the recurrence of a disease from which the insured has recovered or prevent additional complications in an individual who has developed risk factors for a disease,” wrote Edward Fensholt, senior vice president and director of compliance services at Lockton. “Drugs for treating high cholesterol (an existing condition) have been considered ‘preventive’ if they help prevent additional complications, such as a heart attack,” he noted. “But outside of the pharmaceutical context the IRS has resisted calls to treat care of existing diseases or illnesses as preventive.”
Covering medications for chronic conditions pre-deductible for HDHP enrollees “hopefully will encourage patients to fill those prescriptions, stick to the regimen prescribed by their doctors and delay or prevent the onset of more serious and acute conditions—which, in turn, will save both the employer and the employee money,” Buckey said.
“Sponsors of HDHPs may find this guidance helpful as they prepare for the plan year that begins late this year or in 2020,” Fensholt noted. “We half suspect, however, that because the IRS has never supplied an exhaustive list of what is considered preventive and what is not, some HDHPs have already been paying for treatment of at least some of the services listed in the chart for the associated conditions.”
Health Improves When People Take Their Medicine
“Expanding coverage of preventive products and services for managing chronic conditions will help improve adherence to medication, reduce costs for consumers and improve health outcomes,” said Thomas Moriarty, chief policy and external affairs officer at pharmacy and health care firm CVS Health. “With millions of Americans covered through high-deductible health plans, too often they have seen higher out-of-pocket costs on their prescriptions until they have met their deductible. This has created a major financial burden for patients, especially those living with chronic conditions like diabetes, asthma and heart disease.”
Research by CVS Health, Harvard University and Brigham and Women’s Hospital showed that
health care costs were reduced when patients with hypertension, heart failure, diabetes, asthma and depression took their medications as prescribed—and that medical spending by patients with congestive heart failure fell nearly $8,000 per year when they took their medication, despite the increased drug spending.
//window.fbAsyncInit = function() { FB.init({ appId: '649819231827420', xfbml: true, version: 'v2.5' }); };
//(function(d, s, id){ // var js, fjs = d.getElementsByTagName(s)[0]; // if (d.getElementById(id)) {return;} // js = d.createElement(s); js.id = id; // js.src = "http://connect.facebook.net/en_US/sdk.js"; // fjs.parentNode.insertBefore(js, fjs); //}(document, 'script', 'facebook-jssdk')); function shrm_encodeURI(s) { return encodeURIComponent(s); } function RightsLinkPopUp() { var url = "https://s100.copyright.com/AppDispatchServlet"; var location = url + "?publisherName=" + shrm_encodeURI("shrm") + "&publication=" + shrm_encodeURI("Legal_Issues") + "&title=" + shrm_encodeURI("Justices Hear ERISA Reimbursement Case") + "&publicationDate=" + shrm_encodeURI("11/11/2015 12:00:00 AM") + "&contentID=" + shrm_encodeURI("6badda72-62e7-49e8-b4bd-ebbd02a72a17") + "&charCnt=" + shrm_encodeURI("7399") + "&orderBeanReset=" + shrm_encodeURI("True"); window.open(location, "RightsLink", "location=no,toolbar=no,directories=no,status=no,menubar=no,scrollbars=yes,resizable=yes,width=650,height=550"); }
Source link
The post IRS Allows Health Plans to Cover More Treatments Before Deductible Is Met appeared first on consultant pro.
0 notes
Text
WHO Classifies ‘gaming Disorder’ As Mental Health Condition

One symptom is that games start taking precedence over other activities.
CNN 2018-06-20

Adobe
Watching as a video game ensnares their child, many a parent has grumbled about “digital heroin,” likening the flashing images to one of the world’s most addictive substances.
Now, they may have backup: The World Health Organization announced “gaming disorder” as a new mental health condition included in the 11th edition of its International Classification of Diseases, released June 18.
“I’m not creating a precedent,” said Dr. Vladimir Poznyak, a member of WHO’s Department of Mental Health and Substance Abuse, which proposed the new diagnosis to WHO’s decision-making body, the World Health Assembly. Instead, he said, WHO has followed “the trends, the developments, which have taken place in populations and in the professional field.”
However, not all psychologists agree that gaming disorder is worthy of inclusion in the International Classification of Diseases, known as the ICD.

Getty Images | Tomohiro Ohsumi
Characteristics Of Gaming Disorder
A diagnosis standard, the ICD defines the universe of diseases, disorders, injuries and other related health conditions. Researchers use it to count deaths, diseases, injuries and symptoms, and doctors and other medical practitioners use it to diagnose disease and other conditions. In many cases, health care companies and insurers use the ICD as a basis for reimbursement.
Poznyak said the expectation is that the classification of gaming disorder means health professionals and systems will be more “alerted to the existence of this condition” while boosting the possibility that “people who suffer from these conditions can get appropriate help.”
He said there are three major diagnostic features or characteristics of gaming disorder.
“One is that the gaming behavior takes precedence over other activities to the extent that other activities are taken to the periphery,” he said.
The second feature is “impaired control of these behaviors,” Poznyak said. “Even when the negative consequences occur, this behavior continues or escalates.” A diagnosis of gaming disorder, then, means that a “persistent or recurrent” behavior pattern of “sufficient severity” has emerged, according to the ICD.
A third feature is that the condition leads to significant distress and impairment in personal, family, social, educational or occupational functioning, Poznyak said. The impact is real, he said, and may include “disturbed sleep patterns, like diet problems, like a deficiency in the physical activity.”

Getty Images | Sean Gallup Overall, the main characteristics are “very similar” to the diagnostic features of substance use disorders and gambling disorder, he said. Gambling disorder “is another category of clinical conditions which are not associated with a psychoactive substance use but at the same time being considered as addictive as addictions.”
For a diagnosis to be made, the negative pattern of behavior must last at least 12 months: “It cannot be just an episode of few hours or few days,” Poznyak said. However, exceptions can be made when the other criteria are met and symptoms are severe enough.
“Millions of gamers around the world, even when it comes to the intense gaming, would never qualify as people suffering from gaming disorder,” Poznyak said, adding that the overall prevalence of this condition is “very low.”
“And let me emphasize that this is a clinical condition, and clinical diagnosis can be made only by health professionals which are properly trained to do that,” he said.
Poznyak noted that the ICD does not make “prescriptions” in terms of insurance coverage or the development of health services — these decisions are made by national authorities — but “prevention and treatment interventions can help people to alleviate their suffering.”
Most interventions or treatments for gaming disorder are “based on the principles and methods of cognitive behavioral therapy,” he said. He added that different types of support may also be provided, including “psychosocial interventions: social support, understanding of the conditions, family support.”
It’s something Hilarie Cash is well aware of as co-founder of reSTART, one of the first inpatient treatment programs in the United States for video game addiction. She said it’s time to recognize gaming disorder as a legitimate mental health condition.
“I’ve been surprised it’s taken so long for everybody to catch up to the fact. But I also understand that they need to have strong, research-based evidence before they bring on a new disorder,” she said.
“I think it’s a game-changer, although how quickly the game will change, I don’t know.”
Whatever the therapy, Poznyak said, it should be based on understanding the “nature of the behavior and what can be done in order to improve the situation.” Prevention interventions may also be needed.
Ultimately, WHO hopes that inclusion of gaming disorder in the classification will stimulate debate as well as further research and international collaboration, Poznyak said.
Game over, so to speak, is to “significantly reduce the current gaps in knowledge that we have when it comes to the prevalence of these conditions and when it comes to their nature and management.”
Opposing View
Anthony Bean, a licensed psychologist and executive director at The Telos Project, a nonprofit mental health clinic in Fort Worth, Texas, counts himself as a member of the camp that opposes inclusion of gaming disorder in the ICD.

Getty Images | Adam Berry “It’s a little bit premature to label this as a diagnosis,” Bean said. “I’m a clinician and a researcher, so I see people who play video games and believe themselves to be on the lines of addicted.” In his experience, they’re actually using gaming “more as a coping mechanism for either anxiety or depression.”
Forthcoming research shows that gaming is a secondary diagnosis in coping with a primary diagnosis of anxiety and depression, Bean said: “When anxiety and depression is dealt with, the gaming goes down significantly.”
The criteria being used by WHO to define gaming disorder in the ICD are “too broad,” he said, while the mild, moderate or severe versions of the disorder have not been adequately delineated. Diagnosing a patient with gaming disorder, then, would be based on the “very subjective experience of clinicians,” he said.
“And even most clinicians would probably agree that they don’t understand the concept for video games because they’re not immersed in that world or experience,” he added.
The ICD diagnosis is not “appropriately informed,” Bean said, since most clinicians — and the mental health field as a whole — do not understand the gaming population.
Bean’s patients range from “11-year-olds, males and females, all the way up to 36 years old.”
Working closely with them and understanding their games, he said, “you can actually see overt qualities of their gaming style and the way they actually interact with the world around them.”
This knowledge can be used to help them through depression and anxiety, he says.
Someone playing “Minecraft” is going to be completely different from someone playing “World of Warcraft,” he said: “They’re two vastly different genres.” The first is “an online social interaction,” the second “more of a cosmic survival mechanism.”
“If we understand what genres each person gravitates towards, it informs who they are as a person and why they choose that,” Bean said. Then, clinicians can recommend a new game to guide a gamer toward more healthy behavior.
For parents or other loving ones concerned about a much-too-avid gamer, the first step is becoming “as informed as possible,” recommended Bean, who is an author of a guidebook for clinicians wishing to work with gamers. “That’s by far the number one thing that comes in with parents who have concerns is, they don’t even know what games are being played,” he said. The first question to ask, then, is “Why is this interesting to you?”
Ultimately, Bean is not saying gaming disorder doesn’t exist, he just thinks “it’s not really a good idea to go forward with this . … It really opens the door for anything to be a sickness.”
Absolutely anything — watching too much football on TV, doing too much research — could be considered behaviorally addictive if mental health professionals don’t insist on more rigorous study of the issue, Bean said: “Opening that door is a Pandora’s box.”
Written by By Susan Scutti for CNN.
The-CNN-Wire
™ & © 2018 Cable News Network, Inc., a Time Warner Company. All rights reserved.
Sponsored Content
Previous post
This adorably massive dog had to be rescued after he got tired on a hike
Next post
This is the most recent story.
Read the full article
0 notes
Text
Is Using Conventional Medicine Child Abuse?
New Post has been published on http://www.healthgoesfemale.com/is-using-conventional-medicine-child-abuse/
Is Using Conventional Medicine Child Abuse?
I know, I know.
I’m actually not a fan of people calling everything they don’t like, disagree with, or wouldn’t choose “child abuse.” I think it’s an insult to actual child abuse, like starving, beating, or molesting children. (There are other ways to abuse children too…but treating a cold with ginger instead of Triaminic isn’t one of them.)
However, there are people who legitimately believe that choosing alternative medicine for children is actually child abuse. They cite a tiny handful of cases where a child died or was permanently damaged because their parents chose to use alternative remedies. Like the Stephans’ case right now, which is at trial in Canada. I’ve been following that closely, and no, they didn’t kill their son, nor “fail to provide the necessities of life.” Citing silly CBC articles (the company that owns CBC is the one prosecuting them, by the way, so not exactly unbiased) is not going to change that.
Anyway, this isn’t about that.
In a broad sense, alternative medicine isn’t child abuse. Ever. Even if a child dies. (Yes, I really just said that.) To understand this, we need to take several steps back.
What is Child Abuse?
Let’s just start here.
What is child abuse, anyway?
These days, people try to define anything they don’t like as child abuse. They try to define any time a child gets hurt or sick as child abuse. Kid fell out of a tree he was climbing and broke his leg? Child abuse, you shouldn’t have let him climb that tree! Kid ran out of the house and into the road naked, with parent chasing behind? Child abuse, you should have been watching more closely so they couldn’t have gotten out in the first place!
It’s not really a good definition to look what what society considers “abuse” these days, because most of it is pure junk.
Instead, let’s say that abuse is:
Failing to provide basic necessities of life (clothing, food, water)
Physically harming a child (hitting, kicking, shoving, etc. etc. repeatedly or with intent to harm — physical discipline is iffy)
Sexually using the child or allowing them to be used sexually by others
Constant verbal assaults that make it difficult for a child to function (berating, insulting, causing a child to be fearful or depressed)
Okay. So. Causing direct harm to your children is abuse. Failing to feed them at all is abuse. I think we’d all agree on that.
Is it abuse if you get into a car accident and your child dies? No. That is an accident.
Is it abuse if your child sneaks out the door and drowns in a pool? No. That is an accident.
Is it abuse if your child becomes ill, and dies, despite attempts at treatment (conventional or alternative)? No. That is a tragedy.
Parents who mean well and who are doing their best to care for their children are not abusing them…regardless of the outcome of the situation. Accidents do happen. Things don’t always turn out well. If we start to define “abuse” as “when the outcome is bad,” then we’re going to have a serious problem.
Some are going to say right now, “But if a parent uses alternative medicine and the child dies, that is child abuse! They should have used conventional medicine when they knew it was serious!”
I’m going to have to disagree on that.
Is Using Conventional Medicine Child Abuse?
To answer this question, we need to know what we’re looking at.
First, we need to be looking at likely or common outcomes. What usually happens when parents use conventional medicine? (What usually happens when parents use alternative medicine?) We’ll look at main effects, side effects, and long-term effects, if any.
Second, we’ll look at what the worst case outcomes are, and how common these actually are.
Conventional Medicine in Common Situations
Right now, antibiotic use is high — and problematic. One study found that about half of all prescriptions (around 11 million per year) are unnnecessary. On average, people have about 1 antibiotic per year. (But we don’t know how many have none and how many have several, it will vary.)
(Common) Side effects of antibiotic use include:
Nausea
Vomiting
Diarrhea
Stomach pain
Yeast infections
Rash
Swollen, black, or “hairy” tongue
Other side effects include:
Colitis
Seizures
Hives
Jaundice
Yeast infections and pathogenic bacterial infections (like C. diff) are common after antibiotic use, because antibiotics wipe out all the good gut flora along with the bad stuff. This can and does lead to repeated courses of antibiotics. The more courses you have, the more likely that C. diff and other serious effects become.
This might all be worth it, if we were facing serious, life-threatening illnesses, or illnesses that could not be treated in other ways.
However, most people are getting antibiotics for ear infections, sinus infections, UTIs, and other “simple” stuff. The vast majority of the time, antibiotics are not needed for ear infections. They’re almost never necessary for a sinus infection, either. (Decongestants and pain relievers not only don’t usually help, they often delay recovery time.) Antibiotics are almost never needed for bronchitis, either.
And UTIs? They might need antibiotics, but one study found that in recurrent UTIs, probiotics along with antibiotics reduced the risk of additional infections.
Using antibiotics in a child’s first six months of life can lead to increased risk of allergies, asthma, and eczema. I don’t need to tell you that these are generally permanent conditions, not acute like ear infections. That’s a big deal.
None of this even addresses all the prescriptions that doctors write because patients ask for them, without a proper diagnosis. When patients come in and ask for a specific drug, doctors are between twice as likely and twenty times as likely to write a prescription for it! Another study shows that about 100 million antibiotic prescriptions are written annually (half of which are unnecessary and prescribed for viral infections on patient request), which leads to almost 150,000 emergency room visits due to medication issues.
Not to mention that “superbugs” now exist, causing approximately 2 million illnesses and 23,000 deaths annually!
One doctor says, “Everyone feels awful when they are sick and just wants to feel better,” Julien said. “For some reason, faith in the body’s natural ability to heal itself has waned, and everyone believes that an antibiotic is the only possible cure that could help.”
I wonder why that could be, hmm?
To sum it up, we’re writing prescriptions we don’t need, for conditions that typically clear up with no treatment or supportive care, that cause serious side effects, and tens of thousands of allergic and other reactions per year.
…and you’re telling me that, which is clearly causing harm to children, is not child abuse? Or worse, that actually following the evidence and choosing no treatment or supportive care — the obviously better choice, from a scientific standpoint — is child abuse?
Just no.
Alternative Medicine in Common Situations
In contrast, alternative medicine has no such issues.
Ginger has been proven to help treat and prevent colds and other respiratory infections, and has no side effects. Of course, ginger is also known to be excellent for its role in treating digestive disorders (nausea, bloating, diarrhea, etc.) and also has cancer protective and cancer-fighting properties.
Mullein is effective against respiratory infections, worms, and more! No side effects and no known toxicity.
Honey is effective against coughs.
Garlic is a natural antibiotic (more evidence).
Cinnamon essential oil is a natural antibiotic — and even works against resistant bacteria (more evidence on cinnamon).
Lemon essential oil is a natural antibiotic, and is synergistic with cinnamon.
Colloidal silver is effective as a broad spectrum antibiotic. Silver even worked in one study to kill breast cancer tumors!
I could go on.
But, it’s pretty clear here. These natural remedies work. And they don’t cause side effects. They reduce the likelihood of opportunistic infections, because they’re effective against resistant bacteria. They don’t increase the risk of asthma or allergies or any other issues. In fact, ginger may be used to help control asthma.
When I search for “death by herbs,” the first thing that pops up is a study of how herbs cause cancer cells to die.
Deaths or any kind of serious issue from herbal remedies are nearly unheard of. That’s an incredibly safe track record! Herbal remedies work, and they don’t harm people.
Worst-Case Scenarios
This is a lot tougher to look at, for many reasons. Many die despite treatment when something is really serious. Many turn to conventional remedies even if they otherwise wouldn’t when it’s serious.
Regardless of what people choose to do, when it’s serious — there’s a real risk of (further) complications.
Why is it if a mom uses Tylenol constantly and takes him to the doctor and he dies of meningitis, she’s told there’s nothing more she could have done and it’s too bad her baby died…but if she chooses an alternative path instead of or before going to the doctor, she “allowed” him to die?!
It’s because most people think that natural remedies are basically like “doing nothing.”
So let’s get it straight right now: if you think that, you don’t understand natural remedies. Which is okay — stick around, and learn a few things! Unless, of course, you’re using your poor understanding of how natural remedies work to judge other people and say they are bad parents. Then, no, it’s not okay at all.
Worst case scenarios are just that…worst cases. We just don’t know what will happen and there are no guarantees.
So Which is Really “Abuse?”
Neither is actually abuse, and people need to quit saying things they don’t like or don’t understand are abuse. Seriously, grow up.
Looking at the data, though, it’s clear that as far as safety and efficacy, natural remedies win most of the time. I’ll continue to use those, and continue to have healthy children.
If you’d like to learn more about natural remedies, please see my book, Natural Remedies for Kids.
Do you think conventional medicine is child abuse?
Confused about vaccines?
Get our FREE no-nonsense vaccine guide. Answer your questions with rational, fact-based information instead of fear.
Success! Now check your email to confirm your subscription.
There was an error submitting your subscription. Please try again.
First Name
Email Address
We use this field to detect spam bots. If you fill this in, you will be marked as a spammer.
I’d like to receive the free email course. Send my vaccine guide! Powered by ConvertKit
<![CDATA[/* Layout */ .ck_form /* divider image */ background: #fff url(data:image/gif;base64,R0lGODlhAQADAIABAMzMzP///yH/C1hNUCBEYXRhWE1QPD94cGFja2V0IGJlZ2luPSLvu78iIGlkPSJXNU0wTXBDZWhpSHpyZVN6TlRjemtjOWQiPz4gPHg6eG1wbWV0YSB4bWxuczp4PSJhZG9iZTpuczptZXRhLyIgeDp4bXB0az0iQWRvYmUgWE1QIENvcmUgNS41LWMwMTQgNzkuMTUxNDgxLCAyMDEzLzAzLzEzLTEyOjA5OjE1ICAgICAgICAiPiA8cmRmOlJERiB4bWxuczpyZGY9Imh0dHA6Ly93d3cudzMub3JnLzE5OTkvMDIvMjItcmRmLXN5bnRheC1ucyMiPiA8cmRmOkRlc2NyaXB0aW9uIHJkZjphYm91dD0iIiB4bWxuczp4bXA9Imh0dHA6Ly9ucy5hZG9iZS5jb20veGFwLzEuMC8iIHhtbG5zOnhtcE1NPSJodHRwOi8vbnMuYWRvYmUuY29tL3hhcC8xLjAvbW0vIiB4bWxuczpzdFJlZj0iaHR0cDovL25zLmFkb2JlLmNvbS94YXAvMS4wL3NUeXBlL1Jlc291cmNlUmVmIyIgeG1wOkNyZWF0b3JUb29sPSJBZG9iZSBQaG90b3Nob3AgQ0MgKE1hY2ludG9zaCkiIHhtcE1NOkluc3RhbmNlSUQ9InhtcC5paWQ6MUQ5NjM5RjgxQUVEMTFFNEJBQTdGNTQwMjc5MTZDOTciIHhtcE1NOkRvY3VtZW50SUQ9InhtcC5kaWQ6MUQ5NjM5RjkxQUVEMTFFNEJBQTdGNTQwMjc5MTZDOTciPiA8eG1wTU06RGVyaXZlZEZyb20gc3RSZWY6aW5zdGFuY2VJRD0ieG1wLmlpZDoxRDk2MzlGNjFBRUQxMUU0QkFBN0Y1NDAyNzkxNkM5NyIgc3RSZWY6ZG9jdW1lbnRJRD0ieG1wLmRpZDoxRDk2MzlGNzFBRUQxMUU0QkFBN0Y1NDAyNzkxNkM5NyIvPiA8L3JkZjpEZXNjcmlwdGlvbj4gPC9yZGY6UkRGPiA8L3g6eG1wbWV0YT4gPD94cGFja2V0IGVuZD0iciI/PgH//v38+/r5+Pf29fTz8vHw7+7t7Ovq6ejn5uXk4+Lh4N/e3dzb2tnY19bV1NPS0dDPzs3My8rJyMfGxcTDwsHAv769vLu6ubi3trW0s7KxsK+urayrqqmop6alpKOioaCfnp2cm5qZmJeWlZSTkpGQj46NjIuKiYiHhoWEg4KBgH9+fXx7enl4d3Z1dHNycXBvbm1sa2ppaGdmZWRjYmFgX15dXFtaWVhXVlVUU1JRUE9OTUxLSklIR0ZFRENCQUA/Pj08Ozo5ODc2NTQzMjEwLy4tLCsqKSgnJiUkIyIhIB8eHRwbGhkYFxYVFBMSERAPDg0MCwoJCAcGBQQDAgEAACH5BAEAAAEALAAAAAABAAMAAAICRFIAOw==) repeat-y center top; font-family: "Helvetica Neue", Helvetica, Arial, Verdana, sans-serif; line-height: 1.5em; overflow: hidden; color: #666; font-size: 16px; border-top: solid 20px #3071b0; border-top-color: #3071b0; border-bottom: solid 10px #3d3d3d; border-bottom-color: #1d446a; -webkit-box-shadow: 0px 0px 5px rgba(0,0,0,.3); -moz-box-shadow: 0px 0px 5px rgba(0,0,0,.3); box-shadow: 0px 0px 5px rgba(0,0,0,.3); clear: both; margin: 20px 0px; .ck_form, .ck_form * -webkit-box-sizing: border-box; -moz-box-sizing: border-box; box-sizing: border-box; #ck_subscribe_form clear: both; /* Element Queries — uses JS */ .ck_form_content, .ck_form_fields width: 50%; float: left; padding: 5%; .ck_form.ck_horizontal .ck_form_content border-bottom: none; .ck_form.ck_vertical background: #fff; .ck_vertical .ck_form_content, .ck_vertical .ck_form_fields padding: 10%; width: 100%; float: none; .ck_vertical .ck_form_content border-bottom: 1px dotted #aaa; overflow: hidden; /* Trigger the vertical layout with media queries as well */ @media all and (max-width: 499px) .ck_form background: #fff; .ck_form_content, .ck_form_fields padding: 10%; width: 100%; float: none; .ck_form_content border-bottom: 1px dotted #aaa; /* Content */ .ck_form_content h3 margin: 0px 0px 15px; font-size: 24px; padding: 0px; .ck_form_content p font-size: 14px; .ck_image float: left; margin-right: 5px; /* Form fields */ .ck_errorArea display: none; #ck_success_msg padding: 10px 10px 0px; border: solid 1px #ddd; background: #eee; .ck_label font-size: 14px; font-weight: bold; .ck_form input[type="text"], .ck_form input[type="email"] font-size: 14px; padding: 10px 8px; width: 100%; border: 1px solid #d6d6d6; /* stroke */ -moz-border-radius: 4px; -webkit-border-radius: 4px; border-radius: 4px; /* border radius */ background-color: #f8f7f7; /* layer fill content */ margin-bottom: 5px; height: auto; .ck_form input[type="text"]:focus, .ck_form input[type="email"]:focus outline: none; border-color: #aaa; .ck_checkbox padding: 10px 0px 10px 20px; display: block; clear: both; .ck_checkbox input.optIn margin-left: -20px; margin-top: 0; .ck_form .ck_opt_in_prompt margin-left: 4px; .ck_form .ck_opt_in_prompt p display: inline; .ck_form .ck_subscribe_button width: 100%; color: #fff; margin: 10px 0px 0px; padding: 10px 0px; font-size: 18px; background: #0d6db8; -moz-border-radius: 4px; -webkit-border-radius: 4px; border-radius: 4px; /* border radius */ cursor: pointer; border: none; text-shadow: none; .ck_form .ck_guarantee color: #626262; font-size: 12px; text-align: center; padding: 5px 0px; display: block; .ck_form .ck_powered_by display: block; color: #aaa; .ck_form .ck_powered_by:hover display: block; color: #444; .ck_converted_content display: none; padding: 5%; background: #fff; /* v6 */ .ck_form_v6 #ck_success_msg padding: 0px 10px; @media all and (max-width: 403px) .ck_form_v6.ck_modal .ck_close_link top: 30px; @media all and (min-width: 404px) and (max-width: 499px) .ck_form_v6.ck_modal .ck_close_link top: 57px; ]]>
+11
Share466
Pin22
Tweet
Share
Stumble
Shares 489
0 notes
Last Seen Blogs

butchsky
sky

serevnades
Anya

addiesspace
Ad's art blog

chauffourpierreproductions
chauffour pierre productions

madammedarkside
Serial BL enjoyer