#XXXIV. q
Text





Matter of Course
Black Sails Musical Parallels | XXXIV. XXXVII.
music variation note: the scenes in XXXVII are in a lower key than XXXIV.
I spent a year rewatching Black Sails and tracking all the bits of music that repeated at any point during the show, and my findings are reinforcing that Bear McCreary is a genius and this show should have been called 'parallels that will kill you over and over again'* (tag | chronological)
#black sails musical parallels#XXXIV. q#black sails#sabsmade#XXXIV#XXXVII#eleanor guthrie#bs madi#bs utley#james flint#captain flint#dooley#4.6#4.9#mine#bear mccreary#blacksailsedit
55 notes
·
View notes
Photo

A SONG OF JOY AND SORROW: yilling laozu and hanguang-jun, first disciple of yunmeng jiang and the second jade of lan, wei wuxian and lan wangji, wei ying and lan zhan. a mdzs fanmix 🧭
[spotify] 2h 34m
I. bastille - BLAME | II. alanis morissette - ALL I REALLY WANT | III. mikky ekko - KIDS | IV. aj rafael - GRAVITY | V. vitamin string quartet - HELL SONG | VI. wang yibo - WU JI | VII. brandon flowers - ONLY THE YOUNG | VIII. halsey - COLORS PT. II | IX. billy eilish with khalid - LOVELY | X. austra - DARKEN HER HORSE | XI. imagine dragons - MONSTER | XII. black veil brides - IN THE END | XIII. bold as lions - BETTER NOW | XIV. bastille - ICARUS | XV. badbitties ft. emily yacina - TREEHOUSE | XVI. a fine frenzy - RANGERS | XVII. sam tinnesz ft. zayde wølf - MAN OR A MONSTER | XVIII. bishop briggs - WHITE FLAG | XIX. broken iris - WHERE BUTTERFLIES NEVER DIE | XX. within temptation - A DEMON’S FATE | XXI. gang of youths - ACHILLES COME DOWN | XXII. blackbriar - DEADLY DIMINUENDO | XXIII. ruelle - TAKE IT ALL | XXIV. penelope trappes - I CAN HEAR YOUR... | XXV. arcade fire - WAKE UP | XXVI. ruelle - DEAD OF NIGHT | XXVII. the pretty reckless - HOUSE ON A HILL | XXVIII. gotye - SMOKE AND MIRRORS | XXIX. beautiful small machines - BRING OUT YOUR DEAD | XXX. tina guo ft. einar selvik - THE WITCHER 3: WILD HUNT | XXXI. adele - CHASING PAVEMENTS | XXXII. bastille ft. gabrielle aplin - DREAMS | XXXIII. beyoncé - PRAY YOU CATCH ME | XXXIV. beth crowley - WARRIOR | XXXV. abney park - HIS IMAGINARY WORLD | XXXVI. disturbed - LEGION OF MONSTERS | XXXVII. adam lambert - AFTERMATH | XXXVIII. alanis morissette - EMPATHY
resources: modao zushi audio drama covers from episodes s02e08, s02e14, and forgetting envies ending song
#wei wuxian#lan wangji#mdzs#mo dao zu shi#cql#the untamed#books#my mix#playlist#music#mine#to the surprise of nobody who's had to speak to me since november#the first fanmix i make in over two years is for mdzs#myedit
48 notes
·
View notes
Text
Descendants Wattpad Oneshots, Imagines and Books Masterlist
Thomas Doherty Imagines
Descendants Preferences, Oneshots and Imagines
Tumblr Imagines
I’ll Get You HOOKed - H.H.
I
II
III
IV
V (smut)
VI
VII
VIII
IX
X
XI
XII
XIII
XIV
XV
XVI
XVII
XVIII
XIX
XX
XXI
XXII
XXIII
XXIV
XXV
XXVI
Character Description
XXVII
XXVIII
XXIX
XXX
XXXI
XXXII
XXXIII
XXXIV
XXXV
XXXVI
XXXVII (smut)
XXXVIII
Quote #1
XXXIX
XXXX
XXXXI
XXXXII
XXXXIII
XXXXIV
XXXXV
XXXXVI
XXXXVII
XXXXVIII
XXXXX
A/N PLEASE READ
XXXXXI
XXXXXII
XXXXXIII
XXXXXIV
XXXXXV
XXXXXVI
XXXXXVII
XXXXXVIII
XXXXXIX
XXXXXX
XXXXXXI
XXXXXXII
Update
A/N (sorry not a chapter)
XXXXXXIII
XXXXXXIV
XXXXXXV
XXXXXXVI
XXXXXXVII
XXXXXXVIII
XXXXXXIX
XXXXXXX
XXXXXXXI
Drivers License
Sorry - i was tagged
XXXXXXXII
XXXXXXXIII
Q and A Questions
Q and A
22 notes
·
View notes
Text
Juniper publishers-Foot Problems in the Older Patient Diagnostic and Therapeutic Considerations Podogeriatrics for Geriatricians

Introduction
Foot problems in the elderly are common and are major factors in podalgia, limitation of mobility, developmental functional disability, impairment, ambulatory dysfunction, gait imbalance, increasing pain and discomfort. Foot impairments, changes, and deformities also present as risk factors for the development many significant complications of multiple systemic diseases and the potential for lower extremity amputation. Through the course of one's lifetime, the foot undergoes a great deal of trauma, use, misuse, and neglect. The stress of normal activity, changes associated with the aging process, systemic diseases, focal impairment, and environmental factors associated with ambulation create discomfort which can change the patient's ability to function as an independent member of society and generate additional psychological correlates.
Podiatric Assessment
The assessment, evaluation and examination of the elderly patient in relation to their podiatric or foot health concerns involves more than the clinical knowledge of the foot and its demonstrated symptoms and signs. It is important to recognize the patient's concerns and needs in relation to pain, limitation of walking. And a special concern for comfort. Attention to primary goals, i.e., to relieve pain, restore the patient to a maximum level of individual function, and maintain that function once achieved, provides the primary focus for care. The practitioner must anticipate projected changes that relate to ambulation and foot care needs and provide an assurance of individual dignity.
Foot complaints and/or conditions need to be related to both activities of daily living ambulation, dressing, grooming, bathing, etc) and to those independent activities of daily living (shopping, housekeeping, transportation, etc.). The initial element of the assessment should include the demographic data of the patient. The patient’s living conditions should also be included as a part of this initial review.
The chief complaint of the patient should be explored in the patient's own terms. There should be a review of the perception of the patient’s own condition and how his or her foot problems effect their daily lives and activities. Footwear should be assessed in relation to fit, function, use, and compatibility with foot type and ambulatory use. The present condition should be noted as to duration, location, severity, prior treatment, and results and in relation to other general medical conditions.
A systems review should be completed along with notation of other practitioners of record. Current medications and responses should be identified in relation to existing and past therapeutic programs. The past medical history should include infections, operations, fractures, injuries, and drug sensitivities, and allergies. In addition, a review should be noted of those problems and diseases that have pedal complications and/or effect care and ambulation. Examples such risk conditions as delineated in Medicare Regulations include as examples:
i. Diabetes Mellitus
ii. Arteriosclerosis
iii. Ischemia
iv. Burger's Disease
v. Chronic Thrombophlebitis
vi. Venous Stasis
vii. Peripheral Neuropathies
viii. Malnutrition
ix. Alcohol Abuse
x. Chemical/Substance Abuse
xi. Malabsorption
ix. Alcohol Abuse
x. Chemical/Substance Abuse
xi. Malabsorption
Pernicious Anemia
xiii. Anemia
xiv. Hemophilia
xv. Cancer
xvi. Drug Interactions
xvii. Toxic States
xviii. Multiple Sclerosis
xix. Uremia
xx. Renal Dialysis
xxi. Chronic and End Stage Renal Disease
xxii. Chronic Obstructive Pulmonary Disease
xxiii. Coronary Artery Disease
xxiv. Congestive Heart Failure
xxv. Hypertension
xxvi. Edema
xxvii. Post-Trauma
xxviii. Leprosy
xxix. Neurosyphilis
xxx. Hereditary Disorders/Diseases
xxxi. Mental Illness
xxxii. Mental Retardation
xxxiii. Cerebral Vascular Accidents/Stroke
xxxiv. Transient Ischemic Attacks
xxxv. Thyroid Disease
xxxvi. Milroy�s Disease
xxxvii. Patients on Anticoagulants
xxxviii. Hemiparesis or Quadriparesis
xxxix. Ventilator Dependence
xl. Rayland�s Disease/Syndrome
xli. Vitamin Deficiencies
xlii. Osteoarthritis
xliii. Rheumatoid Arthritis
xliv. Gout
xlv. Obesity
xlvi. Psoriasis
xlvii. Urticaria
xlviii. Atopic Dermatitis
xlix. Pruritus
l. Hyperhidrosis
li. Localized Neurodermatitis
lii. Hysterical Paralysis
liii. Psychogenic Tremors
liv. Parkinson�s Disease or Any Medical Condition
Associated with Tremors
lv. Functional Disability
lvi. Ambulatory Dysfunction
lvii. Organ Transplantation
lviii. Immunosuppression
lix. Hemorrhagic/Bleeding Conditions
lx. History of Artificial Joints, Heart Valves, or Blood Vessels
lxi. Chemotherapy
lxii. Antibiotic Prophylaxis
lxiii. HIV/AIDS
lxiv. Impaired Vision � Legally Blind
lxv. Inability to See, Bend, and/or Reach the Patient�s Own
Deet
lxvi. Living Alone
lxvii. Mentally Challenged or Retardation
lxviii. History of Stroke, Spinal Cord Injury, or Brain Injury
A review of the patient’s past podiatric history and foot care history should be noted as well as elements of self-care and the use of commercial foot care products. The past occupational history should be explored and include foot/work related activities, exposure, military service, geographic location, percentage of weight bearing, flooring and footwear should be noted. The social history should include the use of tea, alcohol, coffee, tobacco, sleeping habits, sedative and/or hypnotic use, narcotics and other drugs and the reaction of the patient to his or her own illness or condition. The subjective symptoms should be clearly noted as described by the patient and should attempt to focus on, the following, as examples:
Dermatologic
a) Exquisitely painful or painless lesions
b) Slow healing or non-healing wounds or necrosis
c) Skin color changes such as cyanosis or redness
d) Chronic itching, scaling or dry feet
e) Recurrent infections such as paronychia, athlete�s feet, fungal toenails, etc.
Peripheral Vascular
a) Cold feet
b) Intermittent claudication involving the calf or foot
c) Pain at rest, especially nocturnal, relieved by dependency
Musculoskeletal
a) Gradual change in foot shape
b) Change in shoe size
c) Painless change in foot shape
d) Ambulatory dysfunction
e) Joint changes and deformity
Neurologic
a) Sensory change
b) Burning
c) Tingling
d) Clawing sensation
e) Motor changes
f) Weakness
g) Foot drop
h) Autonomic, such as diminished sweating
Clinical findings of hyperkeratosis, onychial, and dermatologic lesions should be recorded as signs of disease, deformity, and/or a disorder. Examples include the following:
a) Dryness of the skin
b) Xerosis
c) Chronic tinea pedis
d) Keratotic lesions
e) Subkeratotic hemorrhage (plantar and digital)
Trophic ulcerations
a) Pressure ulcerations
b) Diminished or absent hair growth
c) Trophic nail changes (onychopathy)
d) Onychogryphosis (Ram�s Horn nail)
e) Onychauxis (hypertrophic and thickened nails)
f) Onychomycosis (fungal nails)
g) Onychophosis (calloused nail grooves)
h) Hypertrophic deformity
i) Subungual hemorrhage
j) Ulceration (disease complication)
k) Abscess
l) Ingrown toe nail (onychocryptosis)
m) Onychia (inflammation)
n) Paronychia (infection and inflammation)
o) Incurvated or involuted toenails
p) Foot type
q) Gait
r) Postural deformities
s) Palpation of pain
t) Range of motion
u) Angulation
v) Frank deformities (cavus feet, drop foot, hallux valgus,
digiti flexus (hammertoes)
w) Arthropathy
The pedal vasculature and related structures should be evaluated. Those findings and/or conditions, which allow Medicare to provide payment for primary foot care, should be identified. These basic elements include:
A. Class A - Nontraumatic amputation of the foot or an integral skeletal portion thereof.
B. Class B - Absent posterior tibial pulse
a) Absent dorsalis pedis pulse
b) Advanced trophic changes
c) Hair growth - decrease or absent
d) Nail changes - thickening
e) Pigmentary changes - discoloration
f) Skin texture - thin and shiny
g) Skin color - rubor or cyanosis
C. Class C - Claudication
a) Temperature changes, e.g., cold feet
b) Paresthesias, e.g., abnormal spontaneous sensations in
the feet
c) Burning
d) Edema
Absent p°pliteal or femoral pulses, bruits, dependentrubor with plantar pallor on elevation, and prolonged capillary filling time (above 3-4 seconds). Arterial skin temperature and blood pressure should be noted. Doppler studies, pulse volume recordings, and oscillometric readings, may also be useful. Radiographic studies should be obtained as indicated and may include weight and non-weight bearing comparisons. The neurologic elements should include gait review, reflexes (patellar, Achilles, and superficial plantar), ankle clonus, vibratory sense, weakness, sensory deficits (proprioception, pain and temperature perception), hyperesthesia and autonomic dysfunction).
The drug history should focus on but not be limited to antihypertensives, antidiabetics, cortisone, sedatives, topicals, antibiotics, antiarthritics, and other related medications utilized for and by the elderly. The use of over-the-counter foot care remedies including caustic foot keratotic applications should be explored. Some of the conditions, which precipitate pain and discomfort in the elderly and are related to functional imbalance and dysfunction include as examples:
a) Pes Planus
b) Pes Valgo Planus
c) Plantar Imbalance
d) Prolapsed Metatarsal Heads
e) Fasciitis
f) Myofasciitis
g) Tendonitis
h) Myositis
i) Hallux Valgus
j) Hallux Abducto Valgus
k) Digiti Flexus
l) Digital and Phalangeal Rotational Deformities
Hyperostosis
a) Exostosis
b) Spur Formation
c) Calcaneal Spurs
d) Bursitis
e) Fibrositis
f) Neuritis
g) Neuroma
h) Morton�s Syndrome
i) Soft Tissue Atrophy
j) Enthesopathy
k) Hallux Limitus
l) Hallux Rigidus
m) Varus and Valgus Deformities of both the anterior and posterior segments of the foot
The pedal manifestations of diabetes mellitus in the older person, as an example, involve multiple systems and are associated with a variety of symptoms and signs. Examples of such problems include:
Paresthesia
a) Sensory Impairment
b) Motor Weakness
c) Reflex Loss
d) Neurotrophic Arthropathy
e) Muscle Atrophy
f) Dermopathy
g) Onychopathy
h) Absent Pedal Pulses
i) Ischemia
j) Trophic Changes
k) Neurotrophic Ulceration
l) Angiopathy
m) Neuropathy
n) Infection
o) Necrosis and Gangrene
Peripheral arterial insufficiency is present to some degree in many older persons. Overt indications of decreased arterial supply include, as examples:
Muscle Fatigue
a) Cramps
b) Claudication
c) Pain
d) Coldness
e) Pallor
f) Paresthesia
g) Burning
h) Atrophy of Soft Tissue
i) Muscle Wasting
j) Trophic Skin Changes
k) Dryness
l) Hair Loss
m) Absent Pedal Pulses
n) Calcification Noted Radiographically
o) Edema
An example of an outline for the examination and recording of foot health date includes the following, as an example:
Vascular
a) Posterior tibial pulse
b) Dorsalis pedis pulse
c) Popliteal pulse
d) Femoral pulse
e) Doppler studies
f) Edema
g) Calf tenderness
Integument
a) Skin
b) Color
c) Moisture
d) Temperature
e) Texture
f) Interspaces
g) Fissures
h) Ulcers
i) Tinea
j) Tyloma
Heloma
a) Xerosis
b) Dermopathy
c) Atrophy
A. Toe Nails
b) Onychauxis
c) Hypertrophy
d) Onychogryphosis
e) Incurvation
f) Deformity
g) Onychocryptosis
h) Onychophosis
i) Onychomycosis
j) Onycholysis
k) Onychomadesis
l) Onychopathy
Onychia
a) Paronychia
b) Subungual heloma
c) Onychorrhexis
Neurologic
a) Achilles reflex
b) Patellar reflex
c) Superficial plantar reflex
d) Vibratory
e) Proprioception
f) Pain
g) Temperature
Musculoskeletal
A) Strength
a) Dorsiflexors
b) Plantarflexors
c) Invertors
d) Evertors
B) Atrophy
a) Foot
b) Leg
C) Deformities
a) Hallux valgus
D) Hammertoes
a) Spurs
b) Rotations
c) Varus and valgus deformities
d) Neurotrophic arthropathy
E) Gait evaluation
a) Foot type
b) Heel to toe
F) Eversion
a) Inversion
b) Foot structural change
c) Ambulation aids
Long Term Care
The Standards for Long Term Care as developed by the Joint Commission on Accreditation of Healthcare Organizations includes foot health and care as a quality assurance issue. A similar component is currently being instituted for the current revision to the Medicare and Medicaid, Conditions of Participation for Long Term Care. These documents suggest as a basic consideration, administrative projections to assure foot health and care for patient per the following Guidelines:
Long Term Care Guidelines
a) Foot care and/or podiatric services are organized and staffed in a manner designed to meet the foot health needs of patient/residents.
b) The facility's foot health services should be provided by a podiatrist or appropriately licensed practitioner with a consultant podiatric practitioner as a consultant.
c) A foot health program should be an integral part of the facility's total health care program.
d) Written policies and procedures should be developed to serve as a guide to the provision so podiatric/foot care services.
e) The consulting or supervising podiatrist participates in patient/resident care management as appropriate.
f) The quality and appropriateness of podiatric services are monitored as an integral part of the overall quality assurance program, consistent with other practitioner/ professional services.
Continuing Professional Education
A program of professional, in-service, and patient education should form a part of a total geriatric program. A projected outline for such an educational includes as an example, the following:
A. Relationship of foot problems to the total Geriatric Patient.
a) Needs
b) Ambulation and Independence
c) Risk Diseases
d) Factors which modify foot care in society and health care
B. Medicare and Medicaid
e) Mental health considerations
f) Long term care
g) Rehabilitation
C. Primary Foot Care
a) Assessment and examination
b) Nail disorders
c) Skin disorders
d) Hyperkeratotic disorders
e) Foot orthopedic and biomechanical
f) (pathomechanical) changes
g) Foot deformities associated with aging
D. Risk diseases
a) Diabetes Mellitus
b) Arthritis
c) Gout
d) Vascular insufficiency
e) Other
f) Management
g) Interdisciplinary considerations
h) Foot Health Education
i) 1. Professional and interdisciplinary
j) 2. Patient
E. Care Delivery
a) Ambulatory care
b) Acute hospital considerations
c) Rehabilitation
d) Long term care
e) Home care
f) Mental health and retardation
g) Interdisciplinary Education
h) Footwear and Related Considerations
6. Summary
The 1981 White House Conference on Aging, in its final Report, stated the following: "Recommendation Number 148: "Comprehensive foot care be provided for the elderly in a manner equal to care provided for other parts of the human body, to permit patients to remain ambulatory: Implementation: Remove current Medicare exclusions which preclude comprehensive foot care." The ability to ambulate requires appropriate foot health, as a catalyst. Keeping patients walking is a goal that needs to be met if older persons are to maintain a high degree of quality for their lives.
Other important factors that also need to also be considered include:
a) Mobility
b) Multi-Morbidity
c) Impairment
d) Functional Parameters
e) Walking � Ambulatory Speed
f) Stability
g) Physical Function
h) Deficits
Given the high prevalence and incidence of foot problems in the elderly, especially in those patients with chronic diseases and mental health problems, foot care needs are essential. Foot health, care, and foot health promotion should be part of comprehensive health care for older Americans. The ability to remain active and ambulatory is one means of assuring dignity and self-esteem for the elderly.
To read more articles in Journal of Gerontology & Geriatric Medicine
Please Click on: https://juniperpublishers.com/oajggm/index.php
For more Open Access Journals in Juniper Publishers
Click on: https://juniperpublishers.com/journals.php
0 notes
Photo
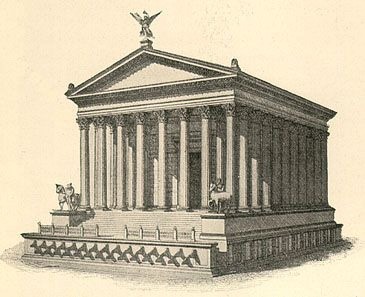
Sorry for the delay, life has had me busy. I present to you the temple of the week.
TEMPLE OF CASTOR AND PULLOX
Castor, aedes: a temple of Castor (or the Dioscuri?) in circo Flaminio, that is, in Region IX, to which there are but two references. Its day of dedication was 13th August (Hemerol. Allif. Amit. ad id. Aug.; CIL I2 p325: Castori Polluci in Circo Flaminio; Fast. Ant. ap. NS 1921, 107), and it is cited by Vitruvius (IV.8.4) as an example of an unusual type (columnis adiectis dextra ac sinistra ad umeros pronai), like a temple of Athene on the Acropolis at Athens, and another at Sunium (Gilb. III.76, 84).
Castor, aedes, templum: * the temple of Castor and Pollux at the south-east corner of the forum area, close to the fons Iuturnae (Cic. de nat. deor. III.13; Plut. Coriol. 3; Dionys, VI.13; Mart. I.70.3; FUR fr. 20, cf. NS 1882, 233). According to tradition, it was vowed in 499 B.C. by the dictator Postumius, when the Dioscuri appeared on this spot after the battle of Lake Regillus, and dedicated in 484 by the son of the dictator who was appointed duumvir for this purpose (Liv. II.20.12, 42.5; Dionys. loc. cit.). The day of dedication is given in the calendar as 27th January (Fast. Praen. CIL I2 p308; Fast. Verol. ap. NS 1923, 196; Ov. Fast. I.705‑706), but by Livy (II.42.5) as 15th July. The laterº may be merely an error, or the date of the first temple only (see WR 216‑217, and literature there cited).
Its official name was aedes Castoris (Suet. Caes. 10: ut enim geminis fratribus aedes in foro constituta tantum Castoris vocaretur; Cass. Dio XXXVII.8; and regularly in literature and inscriptions — Cic. pro Sest. 85; in Verr. I.131, 132, 133, 134; III.41; Liv. cit. and VIII.11.16; Fest. 246, 286;1 Gell. XI.3.2; Mon. Anc. IV.13; Plaut. Curc. 481; CIL VI.363, 9177, 9393, 9872, 10024 — aedes Castorus (CIL I2582.17) or Kastorus (ib. 586.1; cf. EE III.70) appear merely as variants of this), but we also find aedes Castorum (Plin. NH X.121; XXXIV.23; Hist. Aug. Max. 16.1; Valer. 5.4; Not. Reg. VIII; Chron. 146), and Castoris et Pollucis2 (Fast. p103Praen. CIL p.I2.308; Asc. in Scaur. 46; Suet. Tib. 20; Cal. 22; Flor. Ep. III.3.20, cf. Lact. Inst. II.7.9; CIL VI.2202, 2203, although perhaps not in Rome, cf. Jord. I.2.369), forms due either to vulgar usage or misplaced learning. Besides aedes, templum is found in Cicero (pro Sest. 79; in Vat. 31, 32; in Pis. 11, 23; pro Mil. 18; de domo 110; de harusp. resp. 49; ad Q. fr. II.3.6), Livy once (IX.43.22), Asconius (in Pis. 23; in Scaur. 46), the Scholia to Juvenal (XIV.261), the Notitia and Chronograph (loc. cit.). In Greek writers it appears as τὸ τῶν Διοσκούρων ἱερόν (Dionys. VI.13), τὸ Διοσκόρειον (Cass. Dio XXXVIII.6; LV.27.4; LIX.28.5; Plut. Sulla 33), νεὼς τῶν Διοσκούρων (Cass. Dio LX.6.8; App. B. C. I.25; Plut. Sulla 8; Pomp. 2; Cato Min. 27).
This temple was restored in 117 B.C. by L. Caecilius Metellus (Cic. pro Scauro 46, and Ascon. ad loc.; in Verr. I.154; Plut. Pomp. 2). Some repairs were made by Verres (Cic. in Verr. I.129‑154), and the temple was completely rebuilt by Tiberius in 6 A.D., and dedicated in his own name and that of his brother Drusus (Suet. Tib. 20; Cass. Dio LV.27.4; Ov. Fast. I.707‑708). Caligula incorporated the temple in his palace, making it the vestibule (Suet. Cal. 22; Cass. Dio LIX.28.5; cf. Divus Augustus, Templum, Domus Tiberiana), but this condition was changed by Claudius. Another restoration is attributed to Domitian (Chron. 146), and in this source the temple is called templum Castoris et Minervae, a name also found in the Notitia (Reg. VIII), and variously explained (see Minerva, Templum). It had also been supposed that there was restoration by Trajan or Hadrian (HC 161), and that the existing remains of columns and entablature date from that period, but there is no evidence for this assumption, and the view has now been abandoned (Toeb. 51). The existing remains are mostly of the Augustan period (AJA 1912, 393), and any later restorations must have been so superficial as to leave no traces.
This temple served frequently as a meeting-place for the senate (Cic. in Verr. I.129; Hist. Aug. Maxim. 16; Valer. 5; CIL I2586.1), and played a conspicuous rôle in the political struggles that centred in the forum (Cic. de har. resp. 27; de domo 54, 110; pro Sest. 34; in Pis. 11, 23; pro Mil. 18; ad Q. fr. II.3.6; App. B. C. I.25), its steps forming a sort of second Rostra (Plut. Sulla 33; Cic. Phil. III.27). In it were kept the standards of weights and measures (CIL V.8119.4; XI.6726.2; XIII.10030.13 ff.; Ann. d. Inst. 1881, 182; Mitt. 1889, 244‑245), and the chambers in the podium (see below) seem to have served as safe deposit vaults for the imperial fiscus (CIL VI.8688, 8689),3 and for the treasures of private individuals ( Cic. pro Quinct. 17; Iuv. XIV.260‑262 and Schol.). No mention is made of the contents of this temple, artistic p104or historical, except of one bronze tablet which was a memorial of the granting of citizenship to the Equites Campani in 340 B.C. (Liv. VIII.11.16).
The traces of the earlier structures (including some opus quadratum belonging to the original temple; see Ill. 12) indicate successive enlargements with some changes in the plan of cella and pronaos (for the discussion of these changes and the history of the temple, see Van Buren, CR 1906, 77‑82, 184, who also thinks that traces can be found of a restoration in the third century B.C.; cf. however, AJA 1912, 244‑246). The Augustan temple was Corinthian, octastyle and peripteral, with eleven columns on each side, and a double row on each side of the pronaos. This pronaos was 9.90 metres by 15.80, the cella 16 by 19.70, and the whole building about 50 metres long by 30 wide. The floor was about 7 metres above the Sacra via. The very lofty podium consisted of a concrete core enclosed in tufa walls, from which projected short spur walls. On these stood the columns, but directly beneath them at the points of heaviest pressure travertine was substituted for tufa. Between these spur walls were chambers in the podium, opening outward and closed by metal doors. From the pronaos a flight of eleven steps, extending nearly across the whole width of the temple, led down to a wide platform, 3.66 metres above the area in front. This was provided with a railing and formed a high and safe place from which to address the people. From the frequent references in literature (see above) it is evident that there was a similar arrangement in the earlier temple of Metellus. Leading from this platform to the ground were two narrow staircases, at the ends and not in front. The podium was covered with marble and decorated with two cornices, one at the top and another just above the metal doors of the strong chambers. Of the superstructure three columns on the east side are standing, which are regarded as perhaps the finest architectural remains in Rome. They are of white marble, fluted, 12.50 metres in height and 1.45 in diameter. The entablature, 3.75 metres high, has a plain frieze and an admirable worked cornice (for the complete description of the remains of the imperial temple previous to 1899, see Richter, Jahrb. d. Inst. 1898, 87‑114; also Reber, 136‑142; D'Esp. Fr. I.87‑91; II.87; for the results of the excavations since 1899, CR 1899, 466; 1902, 95, 284; BC 1899, 253; 1900, 66, 285; 1902, 28; 1903, 165; Mitt. 1902, 66‑67; 1905, 80; for general discussion of the temple, Jord. I.2.369‑376; LR 271‑274; HC 161‑164; Théd. 116‑120, 210‑212;a DE I.175‑176; WR 268‑271; DR 160‑170; RE Suppl. IV.469‑471; Mem. Am. Acad. V.79‑1024; ASA 70; HFP 37, 38).
This temple was standing in the fourth century, but nothing is known of its subsequent history, except that in the fifteenth century only three columns were visible, for the street running by them was called via Trium Columnarum (Jord. II.412, 501; LS I.72, and for other reff. II.69, p105199, 202; DuP 97). In the early nineteenth century it was often wrongly called the Graecostasis or the temple of Jupiter Stator.
#RomaAeternaOfficial#romanpagan#romanpolytheisim#hellenic pagan#hellenic polytheism#hellenic#classics#classical history#cultus deorum
4 notes
·
View notes
Photo

Las mejores aventuras se viven de esta forma... Si hace 3 años alguien me hubiese dicho que pesaría 83 kg, amaría ir al gym, enloquecería por el running y amaría cada entrenamiento y km dado... Le hubiese tachado de demente. 3 años después me he aventurado a hacer mi 1er medio maratón con algunos miedos (ahora ya vencidos, con orgullo digo). Ha sido una experiencia hermosa, y lo digo un año previo... XXXIV Medio Maratón de Guadalajara allá voy. Mi tiempo fue en oficial 2:15:05 y en mi chip fue 2:10. Estoy feliz, orgullosa, enamorada, deseando mi próxima carrera. Esta carrera es significativa porque cuando iba por el km 14 en Chapalita(creo) había un cartel que hablaba de la familia, recordé a mis tíos, a mis abuelos y a mi madre que me guían desde donde ellos estén, y empecé a llorar e hiperventilar... Tuve q tranquilizarme y seguir. Los sentimientos a flor de piel, porque cada competencia es para mis favorite 5, para mis 5 amores... Mi familia. Día mágico, día de aprendizaje y día de agradecimiento. Gracias a mis dos entrenadores, unos cracks y unos masters. Mi entrenadora Hinelda que aun y con su operación, siguió orientandome en mis entrenamientos y echándole ganas a cada sesión sencilla, dobles sesiones y en ocasiones triples sesiones. Y por supuesto a mi joven entrenador Haman... Por cada consejo, técnicas e ida a trotar/correr me sirvieron muchísimo y los aplique en su totalidad en esta prueba. El sprint fue ejecutado a la perfección gracias a como tú me lo enseñaste. Muchísimas gracias. Por hoy comparto esta parte de vivencia porque aún no están las fotos oficiales y no hay tiempos oficiales (los q yo di son los q vi en el reloj de la competencia y en mi tracker) #runner #run #lifestyle #trainee #training #jogging #runners #happiness #smile #selfie #friends #friendship #friendshipgoals #halfmarathon #mediomaratonguadalajara #runnerStuff #motivation #active #strong #runninggirl #runningday #runningmotivation #runningfriends #l4l #l4like #l4f #likeforlike #likesforlikes #likes4likes #taptap (en Medio Maraton Guadalajara 2019) https://www.instagram.com/p/BuSL569AJ7K/?utm_source=ig_tumblr_share&igshid=zwk2h6jbh6hx
#runner#run#lifestyle#trainee#training#jogging#runners#happiness#smile#selfie#friends#friendship#friendshipgoals#halfmarathon#mediomaratonguadalajara#runnerstuff#motivation#active#strong#runninggirl#runningday#runningmotivation#runningfriends#l4l#l4like#l4f#likeforlike#likesforlikes#likes4likes#taptap
0 notes
Text
Part XXXIV
Q: Sarahah is starting to say there s too many people asking and they all can't be sent but if this get a through. Who are you the closest too? Like who sees you the most. Not in person but like sees a different side of you ❤❤❤
A: definitely Sam
Q: You have 904k followers. How do you even manage to sleep??!?!?!??!?!??!
A: because Sam doesn’t let me see anything on Wattpad 😒😒
Q: Favorite thing to do during the summer
A: sleep, hangout, spend time with family. And I usually go to LA in the summer
Q: Most positive person in the group?
A: Scott probably
Q: Who's the most stubborn????
A: Sam or Danny or Ben
Q: I love youu
A: love you too!
Q: Are you even real
A: I think so, yes
Q: Who is a Liar???
A: I’d like to say no one
Q: Are you hungry
A: yes, always
Q: Worst pain you’ve ever felt?
A: physically? Probably when I sprained my MCL. Couldn’t walk on my leg.
Q: Where have you
Been wanting to cost?
A: sorry, I’m not sure what you’re asking here
Q: I love youuuuuu
A: I love you too!
Q: Is anyone manipulative? If so, who and how so
A: Sam can be. She knows how to kind of talk her way into people giving her things. Usually Ben or Josh
Q: I love you andyyyyyyy
A: love you too!!
- Andy
0 notes
Link
https://founders.archives.gov/?q=Date%3A1789-07-08%20Author%3A%22Jefferson%2C%20Thomas%22&s=1111311111&r=3 From Thomas Jefferson to Montmorin, 8 July 1789 Footnote: "During the turbulent days of July, TJ reported in letters and dispatches that he and Short had moved daily among the crowds without experiencing danger and that their slumber was undisturbed at night. Yet some of this may have been merely to reassure friends in England, who were worried: Hôtel de Langeac was broken into, and TJ was concerned enough about this and perhaps other dangers to have bars and bells put at the windows of the house (Short to TJ, 23 Dec. 1790), which may not have been due altogether to fear of ordinary breaking and entering: the present letter came only two days after Mirabeau had introduced TJ’s name in the National Assembly in connection with the shortage of bread. Montmorin referred the letter to St. Priest asking him to take measures “pour mettre son hotel a l’abri du pillage auquel il a deja été livré” (Montmorin to St. Priest, 30 July 1789; Arch. Aff. Etr., Corr. Pol., E.-U., xxxiv; Tr in DLC). the house … of the douane was vacant in 1789 (see Vol. 10: xxviii, 211). 1. A vertical line drawn in the margin, perhaps by Montmorin or Rayneval, indicates that TJ’s suggestion was given official attention."
0 notes
Text
Java Q/A Part XXXIV
Java Q/A Part XXXIV
How can a GUI component handle its own events?
A component can handle its own events by implementing the required event-listener interface and adding itself as its own event listener.
What is the difference between a while statement and a do statement?
A while statement checks at the beginning of a loop to see whether the next loop iteration should occur. A do statement checks at the end of a…
View On WordPress
0 notes
Text
Java Q/A Part XXXIV
Java Q/A Part XXXIV
Name the eight primitive Java types.
The eight primitive types
Name the eight primitive Java types.
The eight primitive types are byte, char, short, int, long, float, double, and boolean.
Which class should you use to obtain design information about an object?
The Class class is used to obtain information about an object’s design.
What is the relationship between clipping and repainting?
Whe…
View On WordPress
0 notes
Last Seen Blogs

raifitness-blog
Rai Fitness Smart Body Friends & Family

dokmixer
Thoughts and roughs

lovebugrattery
RATS & LOVE.

pamukajans
İsimsiz

brickrenouveautions
24 - 30 September