
ghostyboy29
Peter Whittum
aroace|| diagnosis: PTSD, Bipolar, GAD, ADD, Psychosis || Male (ftm) || He/They || 15 || Mental Health/Disability acc ||
60 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

themorningjen
Love The Morning Show

bladedlion-blog
S e e D
bladedlion-blog
S e e D

mature-men-art
Mature Men Art

isadoraguerrero
ISADORA GUERRERO
Text
So uh we arent a system
So to explain all of the system posting, i thought i was a system but after a trip to the psych ward turns out it was psychosis lol and after getting on meds all the voices stopped.
15 notes
·
View notes
Text
Talked to my therapist about possibly having osdd-1b, she didnt deny it lol. Only our firest session tho so. alsooo getting an autism assesment soon
12 notes
·
View notes
Text
The Star System Intro :3
Introducing . . .
✎. ﹏ THE STAR SYSTEM!
╭ ˗ˏˋ age: 15
┊pronouns: He/They
┊gender: Genderfluid (?)
┊orientation: aroaceflux
╰ ˗ˏˋ status: confused
. . . . . . . . . . . . . . . . . . . . .
≫ System info . . .
⁀➴ system type: OSDD type 3
⁀➴ alter count: 10
⁀➴ frequent fronters:
╰ Felix‣ Gatekeeper‣ He/They‧₊˚
╰ Elliot‣ Emotionalist‣ They/He‧₊˚
╰ Kai‣ Internal protector‣ They/He‧₊˚
╰ Jeff‣ protector/persecutor(?)‣ He/Him‧₊˚
⁀➴ other alters:
╰ Toby - He/Him
╰ Liam - He/Him
╰Peter - He/Him
╰ Bubbles - They/Them
╰ Josh - He/Him
╰ Jade - She/They
. . . . . . . . . . . . . . . . . . . . .
︵ Boundaries . . . Just be nice pls :,3
⤻ DMs: ok
⤻ Pings: pls
. . . . . . . . . . . . . . . . .
⸝⸝ ❝ Yippee !!❞
0 notes

Text
God i cant remember anything i hate this why cant i remember my fucking life.
god what is wrong with me
6 notes
·
View notes
Note
Plural culture is being asexual but sometimes having sexual thoughts and not being sure if you might be asexual with some libido or if that’s an allosexual alter getting a little close to the front
.
73 notes
·
View notes
Text
Reminder
if it helps it helps
2 notes
·
View notes

Text
Our opinion on endos
All systems are traumagenic. Period. No way around it. But we don’t hate endos, in fact they deserve just as much support as the rest of us. Why?
The job of DID is to hide trauma. Endogenic systems probably just don’t remember it, are in denial, or think it wasn’t ‘bad enough’.
So to yall endo’s- sorry to break it to you, but your traumagenic. Your trauma is valid and it’s ok if you don’t remember it. You still deserve love.
148 notes
·
View notes
Text
someone in the system decided to randomly get into astronomy and now we have random knowledge 🫶
0 notes
Text
The Basics of DID/OSDD
DID, or Dissociative Identity Disorder, is a trauma-caused disorder that forms in early childhood, anywhere before the age of 9 (cutoff age is debated but the typical range is before age 6-9, but some people extend it to 10 because that's the typical age where your identity starts forming independant of your primary caregivers)
Most of the established and spread facts about DID come from the Theory of Structural Dissociation (TOSD)
Here's a good resource explaining The TOSD:
To sum things up, there are levels of dissociation that can occur, and disorders that fall into each level. The lowest end of this spectrum is PTSD, and the highest is DID. Here's a graphic of those levels, and I'll go into each disorder briefly:
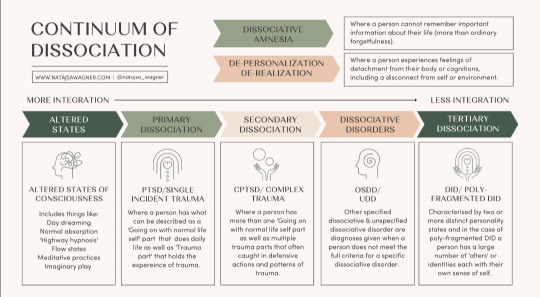
Altered States
Altered states are normal, and likely to occur in everyone at some point. No trauma is required to cause these states. Altered states include normal daydreaming (not including MaDD which is disordered)
Primary Dissociation
Primary Dissociation occurs in people with PTSD. This presents as having one ANP (Apparantly Normal Part, aka you) and one EP (Emotional Part, which occurs when having PTSD flashbacks)
This level is specifically for single-event PTSD, as C-PTSD falls under the next level:
Secondary Dissociation
Complex-PTSD falls under this level because of the occurance of multiple EPs, but still one ANP. These EPs are for a myriad of traumas a person with C-PTSD has experienced.
Dissociative Disorders
This is where we start touching on systems. This level includes OSDD and UDD.
OSDD (Otherwise Specified Dissociative Disorder) is a bit of an umbrella disorder, and it encapsulates multiple different types of OSDD. The one you've most likely heard of is OSDD1b, but I'll go into all of them.
OSDD1a is a disorder in which a person has multiple identity states but they lack distinction. They have intense enough amnesia to qualify for DID, but their identity states aren't differentiated enough to fully qualify for DID. This can sometimes (not always, of course) present as multiple identity states that are all one person, just at different ages when trauma happened.
OSDD1b is a disorder in which a person has multiple identity states that qualify for DID, but have no amnesia. A common misconception is that to be diagnosed with DID, you have to have blackout amnesia (will explain amnesia types later in the post), but any type of amnesia can qualify. OSDD1b is for systems who have absolutely no amnesia.
OSDD2 is a disorder in which there are identity disturbances and dissociation caused by brainwashing, torture, cults, and things of that sort. From what I understand, OSDD2 occurs after the cutoff age of DID or OSDD1, hence why this disorder does not cause a system.
OSDD3 seems to be a temporary diagnosis for symptoms of dissociation, derealization, depersonalization, amnesia, sudden loss of motor skills, ect for less than one month, occuring directly after a traumatic event. If the symptoms persist after this one month period, another diagnosis may be looked at.
OSDD-4 is a disorder in which people experience dissociative trances that do not have any known cause. People slip in and out of these trance states, often unaware of their environment while in them, and may "come to" confused and with amnesia from their time in the trance state.
And lastly, UDD. UDD, or Unspecified Dissociative Disorder, is exactly as it sounds. It's a catchall diagnosis for when a dissociative disorder is present, but it's unknown exactly which one. This can include systems, or it can include other dissociative disorders.
Tertiary Dissociation
Teritary Dissociation is what includes DID, C-DID, and HC-DID.
DID is the disorder we are all reading this post for. It is a disorder that causes multiple identity states that are distinctly different, called alters (or other terms depending on the system's comfort, such as headmates or sysmates), and amnesia between these identity states.
C-DID is a community term which stands for Complex DID. It is synonymous with Polyfragmented DID; they both mean the same thing. C-DID is characterized by a more complex system structure and the presence of many fragments, occuring because of more complex and longterm trauma that starts before the age of 5 (so earlier than the DID cutoff), and typically continues long after the system forms. There are many signs of polyfragmentation in a system, but the most siginifigant are the earlier onset of trauma, presence of many fragments, and more complex internal structure.
HC-DID is another community term which stands for Highly Complex DID. This term is synonymous with programmed systems/RAMCOA systems. These systems formed because of childhood trauma involving Mind Control (the MC of RAMCOA), aka programming. I won't go too in-depth on HC-DID systems, because I'm not confident in my knowledge at this time. However a great blog I can recommend for anyone wanting to learn more is @cultishhellvent
Misc.
You might have noticed at the top of the graphic I included earlier a little blurb about DPDR, or Depersonalization Derealization Disorder. This is a dissociative disorder characterized by, well, persistant depersonalization and derealization. This disorder cannot co-occur alongside DID, but DID can cause depersonalization and derealization. The DPDR diagnosis is for those who don't have another dissociative disorder like DID, but do experience those specific symptoms of depersonalization and derealization.
P-DID, or Partial DID, is a version of DID in which one alter is almost always fronting. Other alters are present, and may front in specific situations, but typically the one alter will stay at front and other alters will come and go from co-con or co-front.
Things To Know About Systems
So here is a bunch of catagories of info about systems that I feel are necessary to know if you're looking to know the basics.
Amnesia Types
Blackout Amnesia is amnesia that is full and total. Periods of blackout amnesia will be fully gone from the person's memory. However, contrary to popular belief, blackout amnesia does not entail literally 'blacking out' and 'waking up' at a later time. It simply means the memories from a time period are totally and utterly gone and inaccessable to you.
Greyout Amnesia has two typical definitions. The first is amnesia that slowly occurs as time goes on, like slowly forgetting the days as you pass them, at a faster rate than would be considered typical for those without a dissociative disorder. The second definition is similar to blackout amnesia, except some memories can be retained. So you may not fully remember an event you went to last week, but you might be able to recall a few blips of major things that took place. Most detail is usually lost.
Emotional Amnesia is when you remember the actual event or time frame, but none of the emotions attached to it. This usually presents as being able to remember a traumatic event, but feeling numb or disconnected to it, or like it happened to someone else.
And something important to keep in mind is that these amnesia types are not hard rules, and amnesia is often somewhere between these three labels.
Innerworlds
Innerworlds, or headspaces, are internal worlds in which alters can go when they aren't fronting (fronting meaning to be in control of the body)
Not all systems have innerworlds, and many systems with Aphantasia (when you can't visualize) simply don't have the ability to create them.
Innerworlds are often created unintentionally as the system grows up, but they can be intentionally created and that can be a beneficial process to the system.
Alter Roles
Alter roles are labels systems can assign to their alters to describe what role they play in the system's life. Some common ones include Host (primary fronter), Protector (self-explanitory), Persecutor (causes the system harm for whatever reason), Traumaholder (alters who hold trauma), and Littles (child alters)
These roles are not hard set, they are simply labels to help explain and put words to what certain alters' jobs in the system may be. And, not all alters have a discernable role.
Introjects
Introjects are alters who form based on an existing identity. This is common in fragments, since they aren't as fully formed, but can of course also happen in fully formed alters.
There are two main catagories of introjects, however many people like to get specific with the terms they use.
Fictives are introjects of fictional characters. This can be from visual media, books, OCs, ect.
Factives are introjects of real people. This can be from friends, abusers, family, celebrities, ect.
Introjects are NOT the same as the thing they are sourced in. They are their own separate people, and should be treated as such.
One of the specific terms I mentioned could be songtives (introjects from songs). I wanted to briefly mention that as an example of the specific terms systems may use.
Co-Con/Co-Front
Co-con, or co-conciousness, is when two or more alters are present at the front. This is usually used to describe one alter fronting, with one or more other alters hanging out nearby and talking occasionally.
Co-front, or co-fronting, is when two or more alters are sharing the front together fully. Think of two people trying to drive the same car at once.
I think I've covered everything I wanted to cover. If I missed anything, said anything incorrect, or you'd like something added please feel free to send an ask or comment/reblog.
600 notes
·
View notes
Text
when the “10 tips on how to make showering easy for disabled people” list doesn’t include a shower chair or a shower/changing table or grab bars etc, i know they don’t care about us physically disabled people.
good for u that turning off the lights and lighting a scented candle instead and listening to music or put on a show and using a bath bomb etc etc helps u but like none of those tips are that beneficial for physically disabled ppl specifically.
it’s good that those tips are there but for once we’d love to be included.
27K notes
·
View notes
Text
Some funny/less paltable things you can say when people invasively ask why you have a mobility aid!
"It's a weapon."
Ignore them
Something dramatic like "Oh I was attacked by a shark" or "I got caught in a zombie apocalypse"
"It's to spice up my outfit"
"I tried to build an army of insert favorite animal and they turned on me :("
"What insert mobility aid?"
"Why do you have an insert mobility aid?"
"Why do you not have an insert mobility aid"
"Do I know you?"
"Yeah I guess I just couldn't wait for my 60s"
RB/comment your go-to when somebody asks about your mobility aid!
930 notes
·
View notes
Text
Happy disability pride to everyone whose disability makes it hard/impossible for them to leave the house.
Happy disability pride to everyone who WANTS to do something they love, but can't because of their disability.
Happy disability pride to everyone who has ever been ignored, side-eyed or scoffed at (or otherwise judged) for being themselves in public.
Happy disability pride to people in constant pain, that doesn't end or break.
Happy disability pride to people who can't/don't want an official diagnosis because it would fuck up their lives, but they need the accommodations anyway.
Happy disability pride to people who did get/have gotten/had to get a diagnosis, because they needed what came from it.
Happy disability pride to the under-represented disabilities that people don't talk about much, or that get ignored both online and IRL.
Happy disability pride to those whose disabilities get represented in ways that do not match your experience at all.
Happy disability pride to the physically and mentally disabled people who are reading this. If you are one, the other, or (more often) both, you are still a valid person who faces discrimination and hardship from ableists, and we must all band together to vouch for our rights- ALL of our rights.
Happy disability pride to all of you, I love you all, and may we get through this month, and all the rest, together.
1K notes
·
View notes
Text
they should invent walking that doesn't make you feel like you're going to keel over and die
3K notes
·
View notes
Text
if there's one thing i ask all parents to do, it's to teach their children about disability from an early age. i cannot leave my house without every child i come across staring at me and/or my mobility aid. as much as i understand children are curious, it's extremely humiliating to feel as though i'm an exhibition for able-bodied people to gawk at.
2K notes
·
View notes
Text
sometimes you’ll see wheelchair users get up and walk a bit or a cane user pick up their cane and carry it instead of using it to walk and it doesn’t mean that they’re faking or they don’t actually need it, and it doesn’t give you the right to question them or ask them to prove they’re disabled. if you see a disabled person temporarily stop using their aids, mind your business and stop assuming you know anything about their situation. people who wear glasses don’t suddenly gain sight when they take them off, and i don’t magically become able-bodied when i carry my cane instead of use it. don’t assume otherwise.
22K notes
·
View notes