#endometrial neoplasia
Text
So I have an IUD for the past 2 years…
It’s been helpful. I’ve been in remission for a year now, and it’s amazingly unstressful… but it’s not all perfect… and things have been off.
I don’t have periods anymore, but I do get these monthly days where I have lots of mucusy stuff. I call it my ghost period, because cramps too. So like there ya go.
I have the iud because of endometrial neoplasia. My oncologist said the options were taking out the uterus or putting the iud in, and other such things.
So I was trying to explain it to ai but she didn’t get it. She did help me feel a little better though.
#ghost period#iud#liletta#Paraguay’s#uterus#uterus health#endometrial cancer#endometriosis#endometrial neoplasia#ai generated#chat gpt#perioddramacentral#perioddramasonly#women’s health#uterine health#uterine fibroids#uterine cancer
1 note
·
View note
Text
US News Issues Top Hospitals List With New Health Equity Metrics
US News Issues Top Hospitals List With New Health Equity Metrics
For the seventh consecutive year, the Mayo Clinic in Rochester, Minnesota, took the top spot in the annual honor roll of best hospitals, published today by US News & World Report.
This year’s rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients…with previously unavailable…

View On WordPress
#cancer#cancer (uterine)#carcinoma#delivery of health care#endometrial carcinoma#health care facilities/manpower/services#health facilities#hospitals#malignant neoplasia#malignant uterine neoplasm#Maryland#Massachusetts#Michigan#Minnesota#Missouri#New York#Ohio#Pennsylvania#racial/ethnic disparity#surgery#tennessee#Texas#uterine cancer
0 notes
Text
Prospective Aftereffect of Human Platelet Lysate upon throughout vitro Increase of Man Cornael Endothelial Tissue Compared with Palbociclib Stone Chemical
But not exhaustive, this evaluation is actually a important guide source of experts and experts managing normal water decline management within normal water syndication techniques. DOI:15.1061/(ASCE)WR.1943-5452.0000245. (C) 2013 American Society involving City Technical engineers.We looked at outcomes of the particular obtrusive, toxigenic haptophyte Prymnesium parvum upon grazing charges, feeding habits, as well as life-history qualities involving clonal lineages of #Link# 3 daphniid zooplankton kinds. Grazing tests exposed related wholesale rates regarding P. parvum as well as a widespread environmentally friendly alga. Behavior findings uncovered zero considerable effects of P. parvum on daphniid feeding behaviours after 40 minutes, however main is reduced within appendage conquer rates after A single . Persistent exposure (Ten deb) for you to G. parvum led to significant discounts throughout daphniid growth rates, get older initially processing, fecundity, and survivorship with densities as little as 7750 cells cubic centimeters(-1). Thus, along with direct sea food death during S. parvum flowers of fifty,000-200,Thousand tissues #Link# milliliter(-1), the complete food net of the occupied program could be subjected to most likely serious negative outcomes also with nonbloom densities involving G. parvum.To compare your efficacy, security, along with tolerability of olanzapine as well as quetiapine within young people together with initial show psychosis. Fifty young people (age Of sixteen +/- A single #Link# .25) which has a initial show of psychosis had been randomized to quetiapine as well as olanzapine in the 6-month available brand study. Efficiency and unwanted effect weighing scales, and also essential signs and also research laboratory files were registered in base line, 6, 16, 25, Three months, and also One hundred and eighty times (conclusion associated with research). Out of the total test included in the research, 32 sufferers completed your demo (quetiapine and Equates to Of sixteen, olanzapine d = 16). Individuals in treatment method groupings were built with a substantial decline in almost all scientific machines with the exception of the particular damaging level of the Negative and positive Indicator Level (PANSS) regarding olanzapine and the general psychopathology size in the PANSS regarding quetiapine. The one among treatment method hands for the specialized medical weighing scales was witnessed for the patients' power along with troubles list of questions (SDQ) scale, together with better enhancement pertaining to olanzapine. Sufferers on olanzapine obtained 15.5 kilogram and sufferers in quetiapine acquired Your five.Five kg. Olanzapine along with quetiapine reduced psychotic signs and symptoms within this teenage sample. Sufferers in olanzapine acquired significantly more fat. Unwanted side effects with both drugs seemed to be more frequent compared to those noted throughout mature research.Your connection of a pseudomyxoma peritonei using a mucinous tumour of the appendix and/or the actual ovary is frequently reported in the books. Nevertheless, with this framework, endometrial. or endocervical lesions stay exceptional. All of us statement the case of the 57-year-old affected person, using pseudomyxoma peritonei connected with a low-grade mucinous neoplasia of appendix along with both sex gland.
0 notes
Text
Estradiol
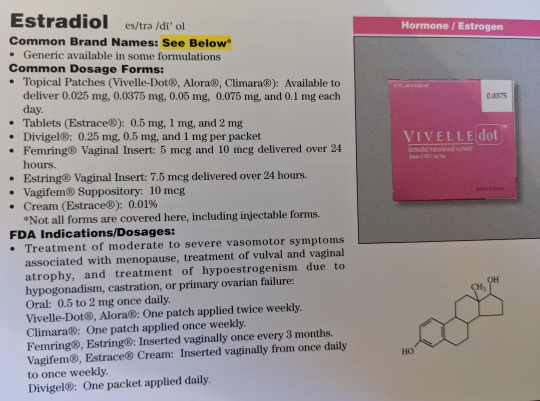

Common Brand Names: See Below
Generic available in some formulations
Common Dosage Forms:
Topical Patients (Vivelle-Dot, Alora, Climara): Available to deliver 0.025 mg, 0.05 mg, 0.075 mg, and 0.1 mg each day
Tablets (Estrace): 0.5 mg, 1 mg, 2 mg
Divigel: 0.25 mg, 0.5 mg, 1 mg per packet
Femring Vaginal Insert: 5 mcg and 10 mcg delivered over 24 hours
Estring Vaginal Insert: 7.5 mcg delivered over 24 hours
Vagifem Suppository: 10 mcg
Cream (Estrace): 0.01%
*Not all forms are covered here, including injectable forms.
FDA Indications/Dosages:
Treatment of moderate to severe vasomotor symptoms associated with menopause, treatment of vulvar and vaginal atrophy, and treatment of hypoestrogenism due to hypogonadism, castration, or primary ovarian failure: Oral: 0.5-2 mg once daily. Vivelle-Dot, Alora: One patch applied twice weekly. Climara: One patch applied once weekly. Femring, Estring: Inserted vaginally once every 3 months. Vagifem, Estrace cream: Inserted vaginally from once daily to once weekly. Divigel: One packet applied daily.
Pharmacology/Pharmacokinetics:
Estrogens promote growth and development of the vagina, uterus, and fallopian tube, and enlargement of the breasts. They are also involved in the process of menstruation. Estradiol is the more potent of the estrogens with estrone and estriol being less potent. In premenopausal women the ovarian follicle produces estradiol. In postmenopausal women the primary source of estrogen is through conversion of androstenedione to estrone. Transdermal applied estradiol avoids the first-pass metabolism of orally-administered estradiol to estrone. Estradiol has a half-life of 1 hour with reapplication estrogen levels being attained within 24 hours of removing a transdermal system.
Drug Interactions:
Barbiturates, St. John’s Wort, carbamazepine, and rifampin may increase the metabolism of estrogens. Erythromycin, clarithromycin, ketoconazole, itraconazole, ritonavir, and grapefruit juice may decrease the metabolism of estrogens.
Contraindications/Precautions:
Contraindicated in women with cancer of the breast, estrogen-dependant neoplasia, undiagnosed genital bleeding, active thromboembolic disorders or a past history of thromboembolic disorders, or during pregnancy. ESTROGEN-ALONE THERAPY INCREASES THE RISK OF STROKE, DEEP VEIN THROMBOSIS, ENDOMETRIAL CANCER, AND IN WOMEN OVER 65 YEARS OF AGE, PROBABLE DEMENTIA. Use with extreme caution in women with a family history of breast cancer or who have breast nodules, fibrocystic disease, or abnormal mammograms. Breast examinations should be performed periodically. Estrogens have been shown to increase the risk of gallbladder disease, thromboembolic disease, hepatic adenoma, high blood pressure, decreased glucose tolerance, and hypercalcemia. Use with caution in patients with a history of depression, when nursing, with liver, cardiac, or kidney dysfunction, and in those with epilepsy. Pregnancy Category X.
Adverse Effects:
Irritation of application site, EDEMA, THROMBOEMBOLIC disorders, breast tenderness, disturbances in menstruation, and depression.
Patient Consultation:
Discuss the uses and dangers of estrogen therapy (package insert).
Do not take during pregnancy.
Closely follow cyclic administration.
Water will not affect patches.
Avoid application sites that are oily, damaged, irritated, or wet.
Store in a cool, dry place away from sunlight and children.
If a dose is missed, apply it as soon as possible. Do not double doses.
Contact a physician if the above side effects are severe or persistent.
#sigler drug cards#36th edition#estradiol#vivelle-dot#alora#climara#estrace#divigel#femring#estring#vagifem#hormone/estrogen#drug facts
4 notes
·
View notes
Text
Anorexia nervosa or significant weight loss may cause hypothalamic-pituitary dysfunction that can result in amenorrhea. A lack of the normal pulsatile secretion of gonadotropin releasing hormone (GnRH) leads to a decreased stimulation of the pituitary gland to produce follicle stimulating hormone (FSH) and luteinizing hormone (LH). This leads to anovulation and amenorrhea.
The causes of hypothalamic-pituitary amenorrhea are functional (weight loss, obesity, excessive exercise), drugs (marijuana and tranquilizers), neoplasia (pituitary adenomas), psychogenic (chronic anxiety and anorexia nervosa) and certain other chronic medical conditions. In this case (anxious, underweight, anorexic pt), the next step to make a diagnosis is to obtain FSH, which would be expected to be in the low range.
Pregnancy is the most common cause of amenorrhea. It is important to consider it early in the workup to avoid unnecessary tests, procedures and treatments that may be contraindicated during pregnancy.
Hypergonadotropic amenorrhea is the result of ovarian failure or follicular resistance to gonadotropin stimulation.
In Mϋllerian agenesis or Mayer-Rokitansky-Kϋster-Hauser syndrome, there is congenital absence of the upper two-thirds of the vagina and of the uterus and fallopian tubes. Ovarian function is normal and all the secondary sexual characteristics of puberty occur at the appropriate time.
Asherman’s syndrome can be caused by curettage or endometritis. The intrauterine synechiae or adhesions result from trauma to the basal layer of the endometrium, which causes amenorrhea.
Because of the chronic unopposed estrogen exposure that accompanies women with PCOS, these individuals carry a higher risk of developing endometrial hyperplasia and cancer. Although some have suggested links between PCOS and breast and ovarian cancer, these links are related primarily to clomiphene use (in the case of ovarian cancer) and obesity (in the case of breast cancer), and not to the syndrome itself.
4 notes
·
View notes
Text
How does dysplasia differ from hyperplasia?
How does dysplasia differ from hyperplasia?
How does dysplasia differ from hyperplasia?
A 40-year-old has an endometrial biopsy report: benign endometrial hyperplasia. 1. Explain the diagnosis. 2. Which cells are implicated in this diagnosis? Compare and contrast atrophy vs. hyperplasia. 3. How does dysplasia differ from hyperplasia? 4. Does hyperplasia lead to neoplasia? Defend your answer. Use APA 7th edition and use nursing literature,…
View On WordPress
0 notes
Text
Altius Hospital - Gynecologist in Bangalore
GYNEOCOLOGISTS IN INDIA:-
Gynecologists (GYN) are doctors who have extraordinary information,aptitudes and expert ability in the medicinal and surgical care of the female conceptive framework and related issue, with the end goal that it recognizes them from different doctors and empowers them to fill in as advisors to different doctors and as essential doctors for ladies. Throughout the times of training, every obstetrician-gynecologist expands upon this wide base of information and abilities and may build up an extraordinary sort of training and changing proficient core interest. Such decent variety adds to excellent social insurance for ladies.
Inhabitant training in gynecology must incorporate four years of licensed, clinically-arranged graduate restorative instruction, which must be centered around conceptive medicinal services and mobile essential human services for ladies, including wellbeing support, malady anticipation, conclusion, treatment, discussion, and referral.
There are likewise subspecialties in gynecology, which require extra preparing: maternal-fetal medication masters are gynecologists who are set up to administer to, and to counsel on, patients with high-chance pregnancies; and regenerative endocrinologists are equipped for overseeing complex issues identified with conceptive endocrinology and barrenness, including parts of helped proliferation, for example, in vitro treatment (IVF).
Gynecology as a Career:
Gynecology is a wide and differing branch of drug, including surgery,administration of the care of pregnant ladies, gynecologic care,oncology, and essential medicinal services for ladies.
Most OB/GYNs are generalists and see an assortment of therapeutic conditions in the workplace, perform surgery, and oversee work and conveyance.Office rehearse comprises of giving ladies preventive examinations and other essential care and recognizing gynecologic issues. OB/GYNs normally assess fruitlessness, irregular uterine dying,leiomyomato,pelvic masses, pelvic organ prolapse, unusual Pap smears, pelvic agony, endometriosis, bosom issue, and urinary incontinence. Cases of minor office systems are colposcopy, endometrial biopsy, Pap smears, and vulvar biopsy. Office ultrasound is performed for gynecologic conditions. A few generalists give impressive essential care notwithstanding the commonplace gynecologic methodology. Cases of outpatient methods incorporate laser surgery, symptomatic laparoscopy, agent laparoscopy, for example, laparoscopic ovarian cystectomy, tubal ligation, analytic and agent hysteroscopy, and
endometrial removal
. Inpatient surgical systems incorporate hysterectomies performed vaginally, abdominally, and laparoscopically. Different cases of inpatient systems incorporate stomach or laparoscopic myomectomies. Obstetrical methodology incorporate cervical cerclage, enlargement and curretage, amniocentesis, Cesarean segment, circumcision, and forceps and vacuum conveyances.
There are four essential subspecialty associations in OB/GYN: gynecologic oncology, conceptive endocrinology and fruitlessness,maternal fetal prescription, and female pelvic medication and reconstructive surgery. These cooperations run three years following culmination of the underlying four-year center residency program, with one of the association years resolved to inquire about. Different cooperations are accessible in hereditary qualities and pediatric and juvenile gynecology.
Gynecologic oncology bargains principally with neoplasias of the uterus, ovary, cervix, and vulva. Conceptive endocrinology and fruitlessness incorporates the whole field of barrenness with methods,for example, IVF, GIFT, ZIFT, and fetus exchange.
The field of female pelvic prescription and reconstructive surgery assesses and treats ladies with pelvic organ prolapse, fecal/urinary incontinence, and other urinary issue. MFM masters treat pregnant ladies with convoluted therapeutic conditions, for example, HTN, DM, renal ailment, preterm work, and coagulopathies.
Around 90 percent of OB/GYNs are generalists and start rehearse in the wake of finishing a four-year residency in OB/GYN. Private practice ordinarily comprises of available time two to four days seven days, surgery coordinated and one half days seven days, and administration of work and conveyance. Generalists most ordinarily rehearse in little or extensive gatherings. Few OB/GYNs are in solo practice. Call is normally subject to rehearse estimate.
The claim to fame of OB/GYN covers an assortment of medicinal services for ladies. All things considered an OB/GYN can perform essential care, have progression of care, and give surgical administrations.
What does a Gynecologist do:
A gynecologist plays out an assortment of tests and exams concentrated on ladies' wellbeing. Gynecologists are in charge of playing out the standard yearly exam on grown-up ladies to guarantee their regenerative wellbeing. Amid this exam, the specialist will physically analyze the lady, play out a pap spread, perform STD tests, finish a bosom exam, and screen the lady's utilization of conception prevention. Gynecologists are additionally now and then affirmed as obstetricians, and will screen the soundness of the mother and the hatchling amid a pregnancy.
What is the workplace of a Gynecologist like:
Gynecologists are for the most part independently employed doctors who claim their own particular practice, or accomplice in a training with different gynecologists. Some are utilized by healing facilities, state offices,and beneficent associations. Still others work in schools and colleges doing research or are teachers in college restorative projects.
All gynecologists work in either a restorative or an instructive field, some of the time both.
Gynecologists Bangalore
are required all through the world, and the interest for specialists in this calling is just developing. In the only us, the activity advertise for gynecologists is relied upon to grow 24% throughout the following decade. Most gynecologists report that they make the most of their work, in any case,numerous likewise report that their work is unpleasant and removes a considerable measure of time from their family and social life.
What kind of personality should a gynecologist have:
A gynecologist treats the general wellbeing of their female patients, treating issues and illnesses of the female regenerative framework, for example, bosom and hormonal issues, urinary tract and pelvic issue, and disease of the cervix. Frequently than not, a gynecologist is an obstetrician also.
Thinking about the cozy idea of their work, a
gynecologist
needs tolerance when conversing with their patients. They have to make driving inquiries in a conscious and merciful path so as to get the patient to open up and completely examine what the issue is.
Humiliation can keep numerous ladies from completely examining their issues with the specialist, be it an adolescent or an elderly lady. Subsequently, building trust with the patient is basic, as this will enable the patient to unveil private issues all the more effectively. Trust is picked up by truly tuning in to what the patient is stating, giving careful consideration to even the littlest subtle elements of the patient's concern and being intensive in the exploration.
Regardless of how often the gynecologist has heard a similar issue or similar indications, she needs to recall that to the individual it is a noteworthy concern, and needs to tune in a thoughtful and empathetic way.
For More Links :
IVF Trea
tment Centre in Bangalore
|
Gynecologist in Bangalore
|
Testtube Baby in Rajajinagar
|
Gynaecology Clinic in Bangalore
|
IVF Centre in Bangalore
#Maternity in Rajajinagar#IVF Centre in Rajajinagar#Uterus Removal in Bangalore#Gynaecology Hospitals in Bangalore#Uterus Removal Surgery in Bangalore#Top Uterus Removal Surgery in Bangalore#IVF Treatment Centre in Rajajinagar
0 notes
Text
5 Reasons The Center for Cancer and Blood Disorders Best at Treating Gynecologic Cancers?
Gynecologic cancers are relatively common; more than 100,000 women each year are diagnosed with some form of Gynecologic cancers In Fort Worth. Gynecologic cancers are of three cancer types; Cervical, Ovarian/Fallopian tube (as well as peritoneal) and Endometrial (uterine). Endometrial or uterine cancer is more common than vulvar and vaginal cancers. Other related cancers include uterine sarcoma, stromal cell ovarian cancer, gestational trophoblastic neoplasia, and germ cell ovarian cancers, all of which are also treated by a gynecologic oncologist. Though often addressed as a group, every gynecological cancer is distinct with its own symptoms, risk factors, and treatments. At The Center for Cancer and Blood Disorders, board-certified doctors offer comprehensive cancer treatment to more than 12,000 patients annually at our locations in Fort Worth-central campus, Fort Worth-Southwest, Stephenville, Weatherford, Burleson, Granbury, Mineral Wells, and Arlington. We offer you the latest advances in immunotherapy, chemotherapy, radiation therapy, biological therapy, and hormonal therapy. We also give you the opportunity to access innovative cancer treatment available only through clinical trials and cancer research.
So, why The Center for Cancer and Blood Disorders are best at treating Gynecologic cancers? Because we provide the best:
• Methods for speeding recovery and reserving the quality of life.
• Highly skilled Surgeons and Oncologists who specialize exclusively in Gynecologic cancers.
• Access to a range of clinical trials and new treatments
• Genetic Testing to guide treatment and assess risk
• Programs to preserve fertility and sexual health
The Center for Cancer and Blood Disorders ' goal is to care for each patient as we would for a loved family member. We trust in treating the individual before targeting cancer. For more information on Cancer treatment, please visit www.thecentertx.com, or call us at 817-759-7000/ 866-454-6560.

0 notes
Text
Endometrial cancer in a woman undergoing hysteroscopy for recurrent IVF failure
Background
Hysteroscopy, despite being the undisputed gold standard for the examination of the uterine cavity, is controversial as a routine procedure in infertile women. However, benign intrauterine conditions are common in women suffering repeated in vitro fertilization (IVF) failure, and growing evidence suggests a unique diagnostic and therapeutic role for hysteroscopy. Endometrial malignancy, on the contrary, is unreported by large published series of women with repeated IVF failures undergoing hysteroscopy, and its impact on fertility, for obvious reasons, has not been studied.
Results
An unsuspected endometrial cancer was diagnosed in an asymptomatic 38-year-old woman undergoing hysteroscopy because of several repeated failures of in vitro fertilization and embryo transfer.

Conclusions
Endometrial cancer can be found at hysteroscopy in young women with repeated IVF failures. The possibility of repeatedly unsuccessful fertility treatments should be taken into account when counseling infertile women about conservative treatment of endometrial cancer.
During the last decades, developments in ultrasound diagnostics and increased knowledge about the determinants of assisted reproduction’s success have caused a downgrading of gynecological endoscopy’s role in the assessment of female infertility. Hysteroscopy, for instance, in spite of being the undisputed gold standard for the examination of the uterine cavity, is controversial as a routine procedure [1]. However, growing evidence suggests a unique diagnostic and therapeutic role for hysteroscopy, especially in cases of repeated failures of assisted reproductive technology [2]. In such cases, abnormal hysteroscopic findings, such as endometrial polyps, submucous fibroids, adhesions, and septa, are common [3,4,5], and hysteroscopy offers an opportunity for diagnosis and a convenient see-and-treat management [2, 6]. Endometrial malignancy, on the contrary, is unreported in large published series [3,4,5], and its impact on fertility, for obvious reasons, has not been studied.
We here present and discuss a case of unsuspected endometrial cancer which was accidentally diagnosed in a woman undergoing hysteroscopy because of repeated failure of in vitro fertilization (IVF) and embryo transfer (ET).
Methods– The data of this case report was obtained through retrospective chart review.
Results
A 38-year-old woman and her male partner had been under our care for primary infertility, at the Centre for Reproduction of Uppsala University Hospital, for 3 years. She had a normal body mass index (BMI; 22 kg/m2) and regular ovulatory menstrual cycles. Previously, she had used combined oral contraceptives followed by an intrauterine device for 10 years. Baseline infertility investigations, including hormonal assessments for TSH and prolactin, pelvic ultrasonography, and semen analysis, were unremarkable. Tubal perviousness and no abnormalities were seen at hysterosalpingo-contrast sonography.
After the diagnosis of unexplained infertility, she had undergone three ovarian stimulations, one with clomiphene citrate, and the following two with low-dose follicle-stimulating hormone (FSH) followed by intrauterine insemination. No pregnancy had been obtained. The couple had then undergone two IVF treatments after conventional controlled ovarian stimulation, each one leading to one fresh elective single embryo transfer (SET) and to several frozen single or double embryo transfers (DET). Overall, eight embryo transfers (two fresh SET, four frozen SET, and two frozen DET) had been performed, but no intrauterine clinical pregnancy was ever achieved. A biochemical pregnancy occurred after the third transfer of the series (frozen). The fifth ET (frozen) resulted in a tubal pregnancy, which was managed by laparoscopic salpingectomy.

Prior to the start of a new controlled ovarian stimulation for IVF-ET, it was agreed to perform a hysteroscopy to rule out intrauterine abnormalities, in view of the several previous failures. At hysteroscopy, a small polypoid growth, having its base at the fundal region, was seen. Pathology of the resected specimen returned a diagnosis of endometrial atypia. After counseling, a conservative treatment with oral progestins (medroxyprogesterone acetate 10 mg daily) was commenced. However, an outpatient endometrial biopsy by pipelle at a 3-month follow-up showed endometrial cancer of endometrioid type. The patient was thoroughly counseled by fertility and oncology specialists about the possible therapeutic strategies, ranging from conservative treatments with progestins to the standard surgical staging for endometrial cancer. As a result of her informed choice to undergo surgery, a total hysterectomy with bilateral salpingectomy and preservation of the ovaries was performed by the gynecologic oncology surgeons. Surgery and the postoperative period were uneventful. The final pathology report described a highly differentiated, diploid, endometrioid adenocarcinoma of the endometrium which was classified as FIGO stage IA (G1). No adjuvant treatment was needed. At all planned follow-up visits, in accordance with local guidelines, she was always disease-free and reported a 100% score on quality-of-life measures. At our last contact, 5 years after the hysterectomy, she also reported having adopted a child and enjoying her motherhood.
Discussion
Hysteroscopy is not universally considered a routine procedure for the evaluation of the uterine cavity in subfertile women [1]. However, there is a high prevalence of previously undetected intrauterine abnormalities in IVF patients, particularly following to failed treatments [3,4,5]. This gives a pragmatic measurement of the diagnostic potential of hysteroscopy, if we consider that women with failed treatments constitute a selected population which has obviously undergone several prior ultrasound exams. Besides, growing evidence, albeit of limited quality, suggests that hysteroscopic diagnosis and, when needed, treatment may improve IVF outcomes and also be cost-effective [2, 7].
Benign hysteroscopic findings are common among IVF patients, the majority of which being represented by endometrial polyps, submucous fibroids, adhesions, or uterine anomalies [3,4,5]. On the contrary, an endometrial malignancy is not an expected finding in these women. Endometrial cancer, in spite of an approximate lifetime risk of 2.8% women, is a rare occurrence before 40 years old [8, 9].
Our patient was 38 years old, and no intrauterine abnormality was ever diagnosed or suspected during 3 years of repeated fertility treatments. Hysteroscopy was only performed in view of the several failures and revealed a small polypoid growth that had not been seen at ultrasound. Polyps are an increasingly common finding [3, 10]; however, their association with malignancy is controversial in younger and asymptomatic women [11]. In our case, in spite of hysteroscopic resection and oral progestins treatment, the initially diagnosed atypia turned out to be an endometrial cancer at final diagnosis, which is a known possibility [12]. The cancer was also still present on the final specimen, meaning that it was not confined to the resected polypoid area, as often reported in the literature [12]. It seems therefore worth reminding that, although conservative treatment of early stage endometrial cancer by means of progestins and hysteroscopic resection has been proposed [9, 13], the gold standard includes a total hysterectomy [14]. In this case, following a patient-centered approach to care, the choice of undergoing hysterectomy was made by the patient after thorough information about different therapeutic alternatives. In spite of that, she could still fulfill her desire for motherhood through adoption.
Whether a link existed, in this case, between infertility and the malignancy is an intriguing albeit difficult question. Infertility does not seem to represent a strong risk factor for endometrial cancer, although some conditions such as chronic anovulation in PCOS patients imply unopposed estrogenic effect on the endometrium, hence a risk for abnormal proliferation [15]. Our patient had ovulatory cycles but had undergone various ovarian stimulations with gonadotrophins as well as hormonal replacement treatments for frozen embryo transfer. Her endometrial cancer was of endometrioid type, which is closely related to estrogens. Some studies have previously shown an increased risk for endometrial cancer in women receiving gonadotrophins and clomiphene for fertility treatment although a real causal relationship is far from demonstrated [16].

One could also wonder whether the neoplasia might have played a role in the several failed treatments experienced by our patient. While benign intrauterine conditions are thought to interfere with endometrial receptivity, the hypothesis of an association of endometrial cancer with implantation failure is suggestive but unverified. This possibility should however be kept in mind when counseling subfertile patients about conservative treatments of endometrial cancer, since much of the knowledge on fertility outcomes is based on experiences with fertile women.
Conclusions
Malignancy, albeit rare, is a possible occurrence in younger women undergoing fertility treatments. In the present case, an early diagnosis of endometrial cancer was facilitated by hysteroscopy, which was performed because of repeated IVF failures in a woman with no specific symptoms nor ultrasonographic signs of pathology. The possibility of repeatedly unsuccessful fertility treatments should be taken into account when counseling infertile women about conservative treatment of endometrial cancer.
Source – https://gynecolsurg.springeropen.com/articles/10.1186/s10397-017-1009-1
Care womens centre – Best IVF center in indore is well known one of the Best fertility hospital in Indore provides affordable ivf cost in indore as compared to others. If you are looking for infertility treatment in indore then you are at right place. At our test tube baby centre indore, have a high sucess story providing smiles to thousant of childless couple. Book an appointment https://www.carewomenscentre.com and call us 8889016663.
Please go through our social media :
like our page to no more about ivf
Facebook : https://www.facebook.com/CareWomensCentre/
Please do follow on Instagram
Instagram : https://www.instagram.com/carewomenscentre/
To More Post: Treating suspected uterine cavity abnormalities by hysteroscopy to improve reproductive outcome in women with unexplained infertility or prior to IUI, IVF, or ICSI
#Best fertility hospital in indore#ivf specialist in indore#test tube baby center in indore#ivf treatment cost in indore#Best centre for IVF in indore#affordable ivf cost in indore#infertility treatment in indore#ivf center in indore#ICSI treatment in indore#fertility centre in indore
0 notes
Text
Biomed Grid| Endometrial Sampling for Endometrial Cancer: Still the Gold Standard?
Endometrial Cancer (EC)
Is the most common gynaecological malignancy affecting women in developed countries and the second most common gynaecological malignancy world-wide, due to the higher rates of cervical cancer in the developing world [1]. The incidence of EC is steadily increasing, largely owing to an ageing population and escalating rates of obesity [2]. According to International Federation of Gynecology and Obstetrics (FIGO), EC is a major differential diagnosis of AUB in the reproductive women [3]. Despite the frequency of this disease, awareness amongst the general population is low and EC research is somewhat underfunded relative to its societal burden [4].
In the past, multiple attempts to evaluate the histological grade preoperatively were without significant success [5,6]. Dilation and curettage (D&C) were once the gold standard for endometria sampling and routinely used with an upgrade rate of 17-26%, compared to the final pathology [7-9]. In an attempt to develop a less invasive diagnostic method, office endometrial sampling became progressively popular. However, studies aimed at investigating office biopsies revealed an apparent inaccuracy in histological grading with an upgrade rate of nearly 30-50%, compared to hysterectomy pathology [10]. Cotillo et al. [11] investigated the accuracy of transcervical resectoscope (TCR) and revealed a rather optimistic finding of 97.1% correlation with the final pathology.
This could be a solution to overcome the hurdle of inevitable upgrades. This method allows direct visualization, a targeted biopsy, and theoretically a more accurate evaluation of preoperative tumour grading [11]. There is also recent progress with effort at improving the diagnostic accuracy of endometrial cancer through immunohistochemistry biomarkers targeting endometrial hyperplasia and predicting progression of endometrial hyperplasia to endometrial cancer [12]. There is need for the clinician to consider therefore the possibility of ECs when treating an abnormal uterine bleeding.
Furthermore, we experienced a case scenario where a colleague had multiple endometrial sampling done and each sample sent to different pathologist and the outcome of the histopathology reports was bizarre. The results were that of different reports establishing the inconsistencies associated with endometrial sampling for endometrial cancer. Similar, encounters have been reported in literature which is the bane of this editorial report. The great question we need an urgent answer for remains “is endometrial sampling for endometrial cancer still the gold standard?”
Abnormal Uterine Bleeding (AUB)
May be defined as any variation from the normal menstrual cycle related to reproductive status; as well as other bleeding not related to menses provides the terminology and descriptions are consistent with the FIGO Menstrual Disorders Working Group consensus statement [13,14]. AUB is the direct cause of a significant health care burden for women, their families, and society as a whole. Up to 30% of women will seek medical assistance for this problem during their reproductive years [15-17]. Patients with AUB are at risk for endometrial carcinoma and therefore AUB warrants further investigation 18. Histological endometrial assessment is indicated when a patient presents with AUB and an increased endometrial thickness on transvaginal sonography (TVS) [19,20]. Outpatient endometrial biopsy is the least invasive technique to obtain tissue for histological assessment. Endometrial biopsies have a very high sensitivity for diagnosing an endometrial (pre)malignancy in AUB women (95%) [21].
Furthermore, performing an endometrial biopsy in women with AUB with increased endometrial thickness is the most cost-effective strategy [22]. Yet, 7-68% of outpatient endometrial biopsy samples are inconclusive because the amount of tissue obtained is insufficient for a reliable histopathological diagnosis [22-25]. In such cases, a more invasive hysteroscopy or dilatation and curettage (D&C) is necessary in order to rule out endometrial carcinoma or atypical hyperplasia, which is present in 6% of these women [23]. The high failure rate due to inconclusive endometrial biopsies might affect the cost-effectiveness of the diagnostic work-up.
Reports from the literature suggest that the attempts to increase the diagnostic efficiency of outpatient endometrial biopsy by structured assessment have not yielded significant improvement in outcome. Therefore, these women cannot be reassured without further invasive, diagnostics [23]. Reviewing hospital protocols revealed that standardized sampling methods was not available in most hospitals, let alone the recommendations on using a tenaculum, entering the uterine cavity more than once, or the use of analgesia in painful procedures. In the cost-effectiveness analysis by Clark et al, the failure rate due to inconclusive endometrial biopsy samples was 12% (95% CI 0.09-0.15) based on a systematic review [22,23]. Other studies reported a failure rate of 7-68% [22-25].
The Clinical Importance of a Diagnosis of Endometrial Hyperplasia (EH)
relates to the long-term risk of progression to endometrioid EC and it is generally accepted that cytological atypia is the principal histological characteristic when assessing EHs for malignant potential [26]. However, not all EHs will progress to malignancy; some EHs occur secondary to estrogenic proliferation without an underlying malignant mechanism. These patients may be asymptomatic and, in some cases, the EH may regress without ever being detected. Several histological classification methods have been proposed aiming to correlate EH architecture and cytological features with the risk of progression to endometrioid EC [27].
The two prominent classification systems are
a. The World Health Organization (WHO) system, established in 1994 with revision in 2003, which is widely known within current clinical gynaecological practice and
b. The endometrial intraepithelial neoplasia (EIN) system, introduced in 2000 [28] and was endorsed in 2014 by the WHO as part of their most recent classification of tumours of the female reproductive organs [29].
The Endometrial Intraepithelial Neoplasia (EIN)
Classification system divides hyperplastic endometrial lesions into two groups:
a. Benign EH and
b. EIN. This is based on objective diagnostic criteria that can be determined from a haematoxylin and eosin (H&E) stained endometrial section.
These criteria emulate what the D-score achieves; however, they can be ascertained quickly by a pathologist using routine light microscopy [30]. EIN lesions are defined as monoclonal proliferations of architecturally and cytologically altered premalignant endometrial glands, which are prone to transformation to endometrioid EC [28].
Conclusion
It is mandatory for clinicians assessing AUB to recognize this disease entity as a possible differential diagnosis. Reports from literature corroborate the fact that there is a high risk of missed diagnosis with less invasive pre-operative diagnostic method of office endometrial trial sampling. The new progress in search of immunohistochemical biomarkers may eventually lay to rest the inconsistent histopathology reports for endometrial biopsy in the nearest future.

Read More About this Article:https://biomedgrid.com/fulltext/volume2/endometrial-sampling-for-endometrial-cancer-still-the-gold-standard.000585.php
For more about: Journals on Biomedical Science :Biomed Grid
#biomedgrid#American medical journal#List of open access medical journal#Journals on medical research#medical and medicinal journal#Open access clinical and medical journal
0 notes
Text
Diagnostic Gynecologic and Obstetric Pathology (3rd Edition) - eBook
Check out https://duranbooks.net/shop/diagnostic-gynecologic-and-obstetric-pathology-3rd-edition-ebook/
Diagnostic Gynecologic and Obstetric Pathology (3rd Edition) - eBook
Practice-oriented and comprehensive, the fully updated Diagnostic Gynecologic and Obstetric Pathology 3rd Edition (PDF) textbook covers the full range of obstetric and gynecologic pathology, including information on treatment and patient management. Written largely by the pathology and clinical faculty at Harvard’s Brigham and Women’s Hospital, it covers the most up-to-date information available in the field, including molecular genetics and diagnostics. Drs. Marisa R. Nucci and Christopher P. Crum are joined by new editors Brooke E. Howitt, Mana M. Parast, Scott R. Granter, and Theonia K. Boyd, to provide beautifully illustrated and complete coverage of both non-neoplastic and neoplastic disorders of the female genital system, ideal for improving pathological diagnosis.
Covers topics not often found in gynecologic pathology textbooks, such as vulvodynia, and diseases of the anus.
A comprehensive look at mesenchymal neoplasia, including not only lower genital tract and uterus but also the retroperitoneum.
Provides distinct diagnostic/differential diagnostic criteria for any potential obstetric/gynecologic specimen encountered in practice.
This enhanced eBook experience allows you to search all of the figures, text, and references from the ebook on a variety of devices.
Features more than 2,250 full-color images, key points at the end of each chapter, and an appendix with commonly used ICD-10 codes
Approaches topics from a practice-oriented point of view, beginning with clinical presentation and progressing through histopathology, differential diagnosis, and treatment for each disorder.
Emphasizes new practice issues and their biologic basis including approaches to cervical, vulvar and endometrial precursors as well as the underpinnings of cervical, endometrial and ovarian cancer.
Review
“Like previous editions, this 3rd edition is a comprehensive resource that covers a clinical and histological presentation of the disease as well as expected management plans. This is an excellent resource for any pathologist who wants to stay relevant in the evolving field of gynecologic and obstetric pathology.” – Sarah L P Rooney, BA, MD (University of Michigan Medical School) – Doody’s Score: 96, 4 Stars!
0 notes
Text
Estrogens, Conjugated (Systemic)


Brand Name: Premarin
Common Dosage Forms:
Tablets: 0.3 mg, 0.45 mg, 0.625 mg, 0.9 mg, 1.25 mg
Premarin Intravenous: 25 mg conjugated estrogens per Secule (vial)
*Also available in a formulation with methyltestosterone
FDA Indications/Precautions:
Indications for oral dosage route:
Vasomotor symptoms associated with menopause: 1.25 mg daily started on day five of cycle if menstruating, otherwise therapy is started arbitrarily.
Female hypogonadism: 2.5-7.5 mg per day in divided doses for 20 days, rest for 10 days, then repeat this schedule until bleeding occurs. If bleeding occurs before the 10 days are over, begin a 20 day estrogen-progestin cyclic regimen with Premarin 2.5-7.5 mg per day in divided doses for 20 days and during the last five days of those regimen give an oral progestin. If bleeding occurs before this regimen is completed, discontinue and resume on the fifth day of bleeding.
Female castration and primary ovarian failure: 1.25 mg a day (cyclically), adjusting dosage to the lowest level that will provide effective individual patient response.
Breast cancer (for palliation only): 10 mg three times a day for at least three months.
Prostatic carcinoma (for palliation only): 1.25-2.5 mg three times a day. Effectiveness can be judged by phosphate determinations as well as by symptomatic improvement.
Prevention of postmenopausal osteoporosis after other non-estrogen treatments have been considered: 0.625 mg daily.
Indications for intravenous dosage route:
Abnormal uterine bleeding due to hormonal imbalance in the absence of organic pathology (intravenous): One 25 mg injection given slowly. May be repeated in 6-12 hours.
Pharmacology/Pharmacokinetics:
Premarin is a mixture of naturally occurring estrogens derived from pregnant mares’ urine. It is composed of estrone, equilin, and 17-alpha-dihydroequilin along with other less prevalent estrogens. Estrogens enter cells of responsive tissues (female genital organs, breasts, hypothalamus, pituitary) and are transported into the nucleus. Inside the cell nucleus, estrogens stimulate specific RNA and protein synthesis. Estrogens also decrease the release of follicle-stimulating hormone (FSH), luteinizing hormone (LH), and luteotropic hormone due to an effect on the pituitary or hypothalamus. Estrogens are important in the development and maintenance of the female reproductive system and secondary sex characteristics.
Drug Interactions:
Barbiturates, rifampin, and/or hydantoins may increase metabolism and elimination. May increase the toxic effects of corticosteroids.
Contraindications/Precautions:
Use is contraindicated in patients with known or suspected cancer of the breast except in selected patients being treated for metastatic disease. Do not use in patients with known or suspected estrogen-dependant-neoplasia, known or suspected pregnancy, undiagnosed abnormal genital bleeding, or in patients with (or history of), thrombophlebitis, thrombosis, or thromboembolic disorders, except when used in treatment of breast or prostatic malignancy. ESTROGEN-ALONE THERAPY INCREASES THE RISK OF STROKE, DEEP VEIN THROMBOSIS, ENDOMETRIAL CANCER, IN WOMEN OVER 65 YEARS OF AGE, AND IN PROBABLE DEMENTIA. Do not use in nursing mothers. Because of increased fluid retention, use with caution in patients with hypertension, asthma, epilepsy, migraine, and cardiac or renal dysfunction. Use with caution in patients with a history of jaundice during pregnancy, diabetes, impaired liver function, and metabolic bone disorders. Pregnancy Category X.
Adverse Effects:
Rash, acne, alopecia, hirsutism, abnormal menstrual bleeding, edema, changes in weight, cholestatic jaundice, changes in cervical erosion and cervical secretions, mental depression, pyrexia, insomnia, nausea, and somnolence.
Patient Consultation:
May be taken with food or milk is GI upset occurs.
Read patient information sheet carefully.
Discontinue therapy and consult physician if pregnancy is suspected.
If a dose is missed, take it as soon as possible and return to dosing schedule.
Store in a cool, dry place away from sunlight and children.
Report any severe side effects to your physician, including pains in the legs, coughing blood, abnormal vaginal bleeding, skin yellowing, and abdominal pain.
0 notes
Text
WE TREAT ALL TYPE OF CANCER

WE TREAT ALL TYPE OF CANCER LIST
· 1Bone andewing sarcoma muscle
· 2Brain and nervous system
· 3Breast
· 4Endocrine system
· 5Eye
· 6Gastrointestinal
· 7Genitourinary and gynecologic
· 8Head and neck
· 9Hematopoetic
· 10Skin
· 11Thoracic and respiratory
· 12HIV/AIDS related
· 13Unsorted (so far)
· 14See also
· 15References
· 16External links
Bone andewing sarcoma muscle[edit]
· Chondrosarcoma
· Ewing's sarcoma
· Malignant fibrous histiocytoma of bone/osteosarcoma
· Osteosarcoma
· Rhabdomyosarcoma
· Heart cancer
Brain and nervous system[edit]
· Astrocytoma
· Brainstem glioma
· Pilocytic astrocytoma
· Ependymoma
· Primitive neuroectodermal tumor
· Cerebellar astrocytoma
· Cerebral astrocytoma
· Glioma
· Medulloblastoma
· Neuroblastoma
· Oligodendroglioma
· Pineal astrocytoma
· Pituitary adenoma
· Visual pathway and hypothalamic glioma
Breast[edit]
· Breast cancer
· Invasive lobular carcinoma
· Tubular carcinoma
· Invasive cribriform carcinoma
· Medullary carcinoma
· Male breast cancer
· Phyllodes tumor
· Inflammatory Breast Cancer
Endocrine system[edit]
· Adrenocortical carcinoma
· Islet cell carcinoma (endocrine pancreas)
· Multiple endocrine neoplasia syndrome
· Parathyroid cancer
· Pheochromocytoma
· Thyroid cancer
· Merkel cell carcinoma
Eye[edit]
· Uveal melanoma
· Retinoblastoma
Gastrointestinal[edit]
· Anal cancer
· Appendix cancer
· cholangiocarcinoma
· Carcinoid tumor, gastrointestinal
· Colon cancer
· Extrahepatic bile duct cancer
· Gallbladder cancer
· Gastric (stomach) cancer
· Gastrointestinal carcinoid tumor
· Gastrointestinal stromal tumor (GIST)
· Hepatocellular cancer
· Pancreatic cancer, islet cell
· Rectal cancer
Genitourinary and gynecologic[edit]
· Bladder cancer
· Cervical cancer
· Endometrial cancer
· Extragonadal germ cell tumor
· Ovarian cancer
· Ovarian epithelial cancer (surface epithelial-stromal tumor)
· Ovarian germ cell tumor
· Penile cancer
· Renal cell carcinoma
· Renal pelvis and ureter, transitional cell cancer
· Prostate cancer
· Testicular cancer
· Gestational trophoblastic tumor
· Ureter and renal pelvis, transitional cell cancer
· Urethral cancer
· Uterine sarcoma
· Vaginal cancer
· Vulvar cancer
· Wilms tumor
Head and neck[edit]
· Esophageal cancer
· Head and neck cancer
· Nasopharyngeal carcinoma
· Oral cancer
· Oropharyngeal cancer
· Paranasal sinus and nasal cavity cancer
· Pharyngeal cancer
· Salivary gland cancer
· Hypopharyngeal cancer
Hematopoetic[edit]
· Acute biphenotypic leukemia
· Acute eosinophilic leukemia
· Acute lymphoblastic leukemia
· Acute myeloid leukemia
· Acute myeloid dendritic cell leukemia
· AIDS-related lymphoma
· Anaplastic large cell lymphoma
· Angioimmunoblastic T-cell lymphoma
· B-cell prolymphocytic leukemia
· Burkitt's lymphoma
· Chronic lymphocytic leukemia
· Chronic myelogenous leukemia
· Cutaneous T-cell lymphoma
· Diffuse large B-cell lymphoma
· Follicular lymphoma
· Hairy cell leukemia
· Hepatosplenic T-cell lymphoma
· Hodgkin's lymphoma
· Hairy cell leukemia
· Intravascular large B-cell lymphoma
· Large granular lymphocytic leukemia
· Lymphoplasmacytic lymphoma
· Lymphomatoid granulomatosis
· Mantle cell lymphoma
· Marginal zone B-cell lymphoma
· Mast cell leukemia
· Mediastinal large B cell lymphoma
· Multiple myeloma/plasma cell neoplasm
· Myelodysplastic syndromes
· Mucosa-associated lymphoid tissue lymphoma
· Mycosis fungoides
· Nodal marginal zone B cell lymphoma
· Non-Hodgkin lymphoma
· Precursor B lymphoblastic leukemia
· Primary central nervous system lymphoma
· Primary cutaneous follicular lymphoma
· Primary cutaneous immunocytoma
· Primary effusion lymphoma
· Plasmablastic lymphoma
· Sézary syndrome
· Splenic marginal zone lymphoma
· T-cell prolymphocytic leukemia
Skin[edit]
· Basal-cell carcinoma
· Melanoma
· Skin cancer (non-melanoma)
Thoracic and respiratory[edit]
· Bronchial adenomas/carcinoids
· Small cell lung cancer
· Mesothelioma
· Non-small cell lung cancer
· Pleuropulmonary blastoma
· Laryngeal cancer
· Thymoma and thymic carcinoma
0 notes
Text
Addiction Treatment Rochester Mn
Contents
Addiction treatment centers
Cancer … az
Areas including austin
Daily online video
Family Service Rochester offers case management, counseling and therapy … Addressed are risk factors and warning signs for mental health and addiction …
Optimal route map between Addiction Treatment Rochester MN, West Center Street, Rochester, MN and Red Wing, MN. This route will be about 45 Miles. The driving route information(distance, estimated time, directions), flight route, traffic information and print the map features are placed on the top right…
Get directions, reviews and information for Addiction Treatment Rochester, MN in Rochester, MN. 110 W Center St Ste 106 Rochester MN 55902.
Home > United States > Rochester > Drug addiction treatment centers in Rochester, MN. Listings include MN Adult and Teen Challenge Rochester, Cronin Home and Teen Talk. Click on each in the list below the map for more information.
Finn is licensed as an alcohol and drug counselor in the state of Minnesota. … He has been with Mayo Clinic Addictions Services in Rochester, MN since 2007. … Glenmore, Hazelden, and the Center for Alcohol and Drug Treatment, Duluth.
If you are struggling with alcohol, drugs, meth, or dual disorders, come to New Beginnings Minnesota (formerly New Beginnings at Waverly), our alcohol and …
Residential Catholic addiction treatment center with holistic, 12-step recovery program for clergy & men & women religious, renewing their ministries.
Metro Treatment of Minnesota LP is a addiction therapy center located in Rochester, Minnesota. We have info about their recovery program options and address.
Seeking addiction treatment can feel overwhelming. We know the struggle, which is why we're uniquely qualified to help. Rochester sits in a valley alongside the Zumbro River in Olmsted County. It's Minnesota's third-largest city and is home to the iconic Plummer Building and the Minnesota…
Addiction Treatment Rochester, MN addresses drug, alcohol, and prescription drugs addiction in Rochester, Minnesota by utilizing detox, counseling, aftercare services, and more in a residential facility.
Addiction Treatment Dallas Texas Quality, effective state of the art addiction and drug rehab treatment center located in the Dallas, Texas area. Call now. Take action and call (972) 848-0221 or fill out this form to speak with a Treatment Consultant about our Dallas drug rehab center or one of our facilities across the United… Dallas, Texas 75390-9070, USA
During the 1980s, the American Medical Association lobbied state legislatures to allow impaired physicians to keep a medical license in good standing-as long as they completed addiction treatment and …
A multipronged, team-based approach that looks at chronic pain and addiction treatment, in addition to managing acute pain, can do just that. As surgeons, pain management specialists, anesthesiologist…
Written for the treatment of smokers diagnosed with cancer … az, Jacksonville, FL, and Rochester, MN; Memorial Sloan Kettering Cancer Center, New York, NY; Moffitt Cancer Center, Tampa, FL; The Ohio …
The top resources for substance abuse treatment in Rochester, MN. Options for programs range from free to the best luxury centers nationwide. If substance addiction is ruining your life, Rochester, MN has many great drug abuse centers to help you, a friend or a family member.
Heroin treatment clinics in Rochester, Minnesota can help you, or a family member, or other loved one win the battle against addiction by providing the help you need in a professional environment in Rochester in order to successfully get through stages such as getting detoxed…
Rochester, MN US. The Mayo Model of addiction treatment has long included state of the art psychiatric assessment and innovative treatment of co-morbid psychiatric disorders by a multidisciplinary team.
DULUTH, MN — Campus towns — and their waterholes … an initiative of American Addiction Centers Inc., which provides residential and outpatient addiction treatment services. The report uses 2016 U.S. …
Core components of our treatment programs draw from motivational enhancement and cognitive … Second chance: A new beginning after years of addiction.
Correspondence should be addressed to Dr. Altchuler, Mayo Clinic, 200 First Street SW, Rochester MN 55905; telephone … denial about his or her mental health may not seek needed treatment or may fail …
Looking for drug and alcohol rehab in Minnesota? We have treatment specialists available 24-7 to assist you find the best location in Minnesota that fits your …
Addiction Treatment Planner 4th Edition critical aspect of patient engagement and treatment planning and should be ….. The fourth edition of the DSM (DSM-IV)1, described two Substance Use Disorder … Heroin Addiction Treatment Treating an addiction to heroin usually involves therapy, medication, support groups and lifestyle changes. These treatments are available at both inpatient and outpatient treatment centers. Even celebrities
Since 1983, Mn Adult & Teen Challenge has been restoring hope to people struggling with drug and alcohol addiction. In addition to our effective and affordable residential Licensed Treatment, faith-based Long-Term Recovery and convenient Outpatient program, we have extensive prevention and…
About Addiction Treatment in Rochester, Without constant vigilance and ongoing support, it's easy With so many alcohol and drug treatment plans available to you in Rochester, Minnesota, getting Exploring Treatment Options In Rochester, MN? We're Available 24/7 With 31 care providers in…
Mary Marnach, MD and coauthors from Mayo Clinic, Rochester, MN, and Mayo Clinic Hospital … Versus Levonorgestrel-Releasing Intrauterine System for Treatment of Endometrial Intraepithelial Neoplasia. …
The Minnesota Association of Treatment Programs: On June 17, this coalition of drug addiction treatment providers asked the court to ensure that funding for the programs they administer would continue …
The pins on the map represent the locations of methadone clinics in Minnesota. Clicking a pin on the map will display contact information for that clinic including it's name, address, phone number, and website if available. On this page there is also a list of methadone clinics in Minnesota sorted…
Fountain Centers in Rochester is a drug and alcohol addiction rehab center. Call today … Metro Treatment of Minnesota LP Rochester Metro Treatment Center.
Just minutes from downtown Rochester, Minnesota, Oakridge has been specifically … Specialty Programs: Alcohol/Drug Addiction, Dual Diagnosis/Co- Occuring, …
Avila, 30, cultivated connections between Mexico and Nebraska for a drug trafficking cell he led in Rochester … addiction has proved more lethal, meth-related deaths are rising to unprecedented leve…
A former high school basketball star from Rochester hanged himself Friday at a state addiction-treatment center, the Star Tribune has learned, becoming the fourth suicide at a state treatment facility …
Free Alcohol, Drug and other Rehab resources in Rochester, Minnesota. … education or substance abuse treatment in Rochester, MN or in southeast Minnesota.
Common Ground is a treatment center providing outpatient and residential … Learn more here: https://lnkd.in/ecw9y7R #rochestermn #addictiontreatment # …
Fifty adult patients with chronic pain and substance dependence were admitted to an inpatient unit for treatment of addiction without primary emphasis … 200 First Street SW, Rochester, MN 55905, U.S …
Robert "Bob" L. Dietzler, 71, of Rochester, MN. died Tuesday, October 18, 2016 at his home. A gathering and celebration of life will be from 3:00-6:00 pm on Saturday, October 29, 2016, at Ranfranz and …
Newswise — CHICAGO—Female patients with locally advanced esophageal cancer that is treated with chemotherapy and radiation therapy before surgery are more likely to have a favorable response to the tr…
The multi-species fishing tournament benefits addiction treatment programs in Brainerd, Duluth, Minneapolis and Rochester. The mission of MN Adult & Teen Challenge (mntc.org) is to assist teens and ad…
Recovery is Happening is dedicated to shifting the perception of addiction. But, we … Recovery Is Happening is working to make Southeastern Minnesota region …
MN), and Mayo Clinic (Rochester, MN). The study participants were young adults aged 12-18 years who had failed two previous trials of antidepressants. They received six ketamine infusions over 2 weeks …
In Minnesota, the majority of addiction treatment admissions are related to marijuana use. However, heroin and opioid addictions have grown into a serious As of July 2016, eight patient centers began operations in Minneapolis, St. Paul, Bloomington, Rochester, St. Cloud, Moorhead, Eagan and Hibbing.
Female patients with locally advanced esophageal cancer that is treated with chemotherapy and radiation therapy before surgery are more likely to have a favorable response to the treatment than … of …
Frontiers in Addiction Treatment 2018. Rochester, MN US … The Mayo Model of addiction treatment has long included state of the art psychiatric assessment …
Addiction Treatment Melbourne Commonly Abused Drugs in Melbourne, FL; 4. Substance Abuse Hotlines; 5. Melbourne Drug and Alcohol Detox Centers; 6. local recovery meetings Near You … Call now 1-800-304-2219. The following article is will help you find treatments for drug and alcohol addiction in Melbourne, Florida. Located in Melbourne, The Hader Clinic offers a range of solution-based programs
Drug & Alcohol Detoxification Facilities in Rochester, MN … Since substance abuse treatment is an important major change in your life, we present you with a …
Live your best life. Recovery is Happening is a Rochester MN drug treatment program dedicated to helping you reach your fullest potential. Contact us today.
78 Counseling jobs available in Rochester, MN on Indeed.com. … Human Services, Social Work, Psychology, Nursing, Pre-Med, Alcohol and Drug Counseling, …
We offer the best drug rehab, alcohol rehab facilities and drug detox programs in Rochester, New York.
Crystal Meth Experiences Once methamphetamine is introduced into the system you can experience an …… This will be day two for me, I snort crystal meth I have been experiencing … Credit: Shutterstock The use of cheap and potent crystal methamphetamine (meth … For gay and queer men who use meth, the motivations are complex and often rooted in
During the 1980s, the American Medical Association lobbied state legislatures to allow impaired physicians to keep a medical license in good standing-as long as they completed addiction treatment and …
Phone, (507) 282-2500 · Address. 604 5th St SW; Rochester, Minnesota 55902 … Drug Addiction Treatment Center. … ·Located in Rochester, Minnesota.
2360 North Broadway Rochester, MN 55906. Rochester Metro Treatment Center provides opioid addiction treatment and recovery services in Rochester and surrounding areas including austin, Stewartville, St. Charles, Kasson, Pine Island, Spring Valley and Owatonna.
For more than 50 years, Zumbro Valley Health Center has worked to improve the mental and chemical health of people in Southeast Minnesota regardless of …
Dual Diagnosis Treatment Centers Nyc For more on the dual diagnosis of … to American Addiction Centers, adults who struggle with alcohol abuse are 5-10 times more likely to have ADHD than the general population. And up to a quarter (25 … The CDC study found the number of patients discharged from North Carolina hospitals with a dual diagnosis of
Whether you're in recovery, seeking help from any addiction, family or friend, register for now. You'll get exclusive free access to Daily Meditations, Speaker Tapes and daily online video AA / NA meetings. Drug Rehab in rochester – Addiction Treatment in MN.
Duluth. Minneapolis. Rochester. Saint Paul. FIND TREATMENT IN Minnesota TODAY. At Drug Treament Centers Minnesota, the goal is to provide more than just access to the top addiction and rehabilitation centers in Minnesota, our goal is also to provide you with hope.
Home > United States > Rochester > Businesses > Addiction Treatment Centers. A Common Ground 1027 7th St NW, Ste 207 Rochester, 55901. Chemical Dependency Outpatient Facility.
Merhaba trendsetter! Addiction Treatment Rochester, MN için ilk yorum yazan kişi olabilirsin. Addiction Treatment Rochester, MN yakınında daha fazla Bağımlılık Tedavi Merkezi bul. Yakındakiler. Restoranlar.
Those who do receive assistance in quitting usually receive very low intensity treatment … Rochester, MN (MVB). Send correspondence and reprint requests to Jill M. Williams, MD, Professor of Psychia…
This grant will provide families across our state with the resources they need to prevent addiction and get access to life-saving treatment and recovery services … The list of meetings is at www.eqb …
0 notes
Video
Vaginal Bleeding after menopause is abnormal and dangerous. A woman has attained menopause if she has not done menstruation for 12 months. Any vaginal bleeding after your menses has seized for up to 12 months is no longer menstruation. At this stage it is called Postmenopausal Bleeding. Postmenopausal bleeding is a sign that all is no longer well with uterus. Therefore such woman needs an extensive check-up to start the process of preventing onset of Endometrial Intraepithelial Neoplasia or Uterine Cancer. Advice any woman you know from age 45 years and above with recurrent abnormal & irregular vaginal bleeding to call us and book an appointment for extensive assessment of her uterine cavity. Uterine cancer is preventable and treatable if early detection of conditions that lead to it are diagnosed accurately and on time. Recommend us to your family members and friends suffering from any kind of abnormal and irregular vaginal bleeding. Contact 08137760565 or 08087907954 for more enquieries. https://www.instagram.com/p/CBPwKQZj7fB/?igshid=yhezl7aiw6uq
0 notes
Text
What is the study of uterine cervical lesions by Pap smear cytology and its correlation with colposcopy?
Recently ASCCP reported that combined use of cytology, colposcopy and histopathology secured the highest yield for detection of cervical neoplasia. A study conducted by the New South Wales Cervical Cancer Screening Society reported that due to routine screening http://drvikramsaraswat.co.in , cervical cancer death rates have been reduced by 74% between 1955 to 1992, and since then have continued to decline by 0.5% every year, making it the most successful cancer screening technique in history.
BETHESDA
SYSTEM 2001
2001 Bethesda System Terminology 40
•
Specimen Type: Indicate conventional smear (Pap smear) vs. liquid based vs. other
Specimen Adequacy dr.vikram saraswat |Saraswat Pathology in Agra
•
Satisfactory for evaluation (describe presence or absence of endocervical/transformation zone component and any other quality indicators, e.g., partially obscuring blood, inflammation, etc.)
•
Unsatisfactory for evaluation ... (specify reason)
•
Specimen rejected/not processed (specify reason)
•
Specimen processed and examined, but unsatisfactory for evaluation of epithelial abnormality because of (specify reason)
General Categorization (optional)
•
Negative for intraepithelial lesion or malignancy
•
Epithelial cell abnormality: See interpretation/result (specify ‘squamous’ or ‘glandular’ as appropriate)
•
Other: See interpretation/result (e.g. endometrial cells in a woman > 40 years of age)
Automated Review
•
If case examined by automated device, specify device and result.
Ancillary Testing
•
Provide a brief description Diagnosis, Diagnostics, and Efficient Treatment Plans,Pathologist. of the test methods and report the result so that it is easily understood by the clinician.
0 notes
Last Seen Blogs

bluesfreakingart
Blues art.

matt-murderdock
Western Sun of the Hand

radically-raw
Radically Raw

starlight-shine-bright
boys will be bugs, right?

mijamija1234
Felicità