#Kcentra
Text

Anticoagulation Lecture 6/21/23
Factor Xa inhibitors = rivaroxaban, apixaban (Eliquis)
Direct thrombin inhibitor = dabigatran
Vitamin K inhibitor = warfarin
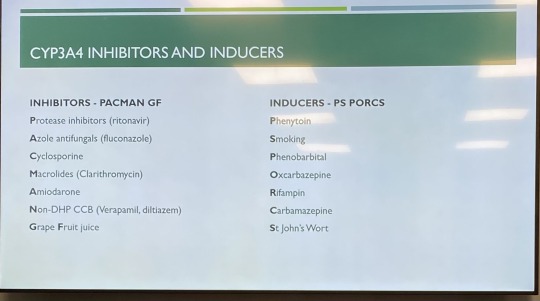
Apixaban has the lowest bleeding risk compared to the other Direct Oral Anticoagulants (DOACs); avoid in pts with BMI greater than or equal to 40 or weight more than 120 kg. Avoid dual inhibitors or inducers of CYP3A4 and P-gp.
VTE/PE tx = 10mg bid x7 days, then 5 mg bid
AFib = 5 mg bid (reduce to 2.5 mg bid if Cr greater than or equal to 1.5 or weight less than 60 kg or age greater than 80
Rivaroxaban (Xarelto) = once daily dosing compared to Eliquis
VTE/PE: 15 mg bid x21 days; then 20 mg qd
AFib: 20 mg qd with food to increase absorption
PAD/CAD: 2.5 mg bid (+antiplatelets if at increased risk)
Avoid with CYP3A4 inhibitors or inducers and P-gp
Edoxaban (Savaysa) – not used in pts with CrCl greater than 95
VTE/PE = parenteral anticoagulation for 5-10 days, then PO
VTE/PE/AFib = 60 mg qd
Does not have reversal agent like other DOACs do (which are reversed with Kcentra or andexanet)
Dabigatran (Pradaxa)
AFib: 150 mg bid; consider 110 mg bid if bleeding risk
VTE/PE: 5 days IV, then 150 mg bid
VTE ppx after THA/TKA: initial 110 mg once, then 220 mg qd x10-35 days
5-10 day bridge required for PE/VTE
Caution in pts greater than 75 years due to increased bleeding risk
Has own reversal agent (praxbind; idarucizumab)
C/I in pts with prosthetic heart valve
Store in original bottle and discard if unused after 4 months
Eliquis and Xarelto can be crushed and given via feeding tubes.
Warfarin (Coumadin)
Dosing is pt specific. Goal INR is 2-3. (2.5-3.5 if mechanical mitral valve).
Slow onset; slow time to steady state means dose taken today may not be reflected in INR for several days (2-4 days).
So many drug-drug interactions!
Metabolized by CYP pathways
Vitamin K antagonist
Dosing: recommend taking at night because INR is taken during the day, makes it easier to adjust dose.
Warfarin’s therapeutic steady state is based on half-lives of clotting factors. At least 5 days of consecutive warfarin needed for pt to be fully anticoagulated (this is why you use heparin until they get to this point).
Usually start with 5 mg qd. If bleeding risk, start with 2.5 mg qd. For obese pts or otherwise healthy/young can start with 7.5 mg qd. You go to maintenance protocol on 7th day.
Pts on VTE/PE tx are not anticoagulated the first 5 days, so use heparin IV or LMWH outpt. Once anticoagulated x24 hours, d/c heparin.
Start with 5 mg warfarin for first 3 days, then follow up with warfarin clinic on day 4. Typically, pt goes for weekly INRs. Then when at goal INR for 2 weeks, can spread out how often they f/u on their INR levels. Eventually they can go q6-8 weeks to check INR level.
VTE/PE – always bridge
AFib – risk assess to see whether heparin bridging is needed (assess bleeding risk [HASBLED]; CHA2DS2VASc for thrombotic risk).
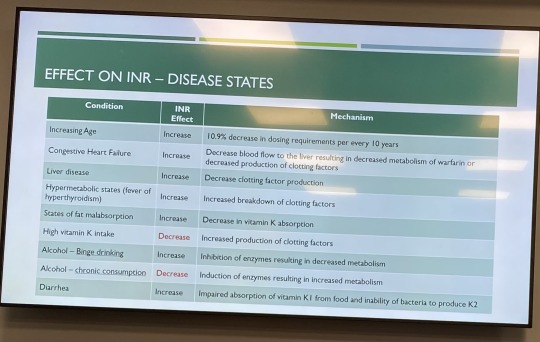
Every 10 years, the dosing needed will decrease by 10%, so as pts age, the dose of warfarin needed will decrease.
DOACs = no INR monitoring, no dietary interactions, lower rates of bleeding, limited availability of reversal agent; contraindicated in pts with mechanical heart valves
AFib – AC (anticoagulate) indefinitely
1st VTE or PE that is provoked – AC for 3 months
1st episode of VTE/PE in setting of cancer – 3 months of AC (LMWH is better than DOAC or warfarin--new research shows DOAC may actually be more effective, so can use DOAC now; LMWH not preferred)
1st episode of VTE/PE unprovoked (no idea what caused it) – AC more than or equal to 3 months
2nd VTE – AC indefinitely
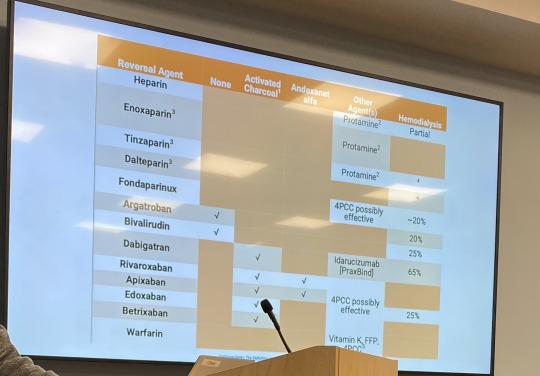
Heparin reversal – protamine (max dose is 50 mg), to reverse enoxaparin, give 1 mg protamine for each 1 mg of Lovenox
Warfarin reversal – vit K; 4 factor prothrombin compex (KCentra); FFP (if KCentra not available); KCentra is for life-threatening bleeding or if pt needs surgery for life-threatening condition
Apixaban/Rivaroxaban reversal – Kcentra (life threatening bleed or need emergency surgery; has thrombotic risk); FFP (Fresh Frozen Plasma); Andexanet Alfa. KCentra can cause clotting in 5% of pts; don’t give if you don’t need to.
Dabigatran reversal – idarucizumab (Praxbind); dosed as 5 g IV given 2.5 mg no more than 15 minutes apart)
Heparin lasts 2 hours
LMWH is preferred in pts who are pregnant (avoid warfarin). ESRD on dialysis – warfarin or Eliquis (avoid Xarelto). Obese pts – DOACs or warfarin. Cancer – use LMWH; recent study shows Eliquis is equal to or superior to LMWH in cancer pts who need anticoagulation.
Pregnancy = lovenox better, doesn’t cross placenta; UFH (unfractionated heparin) is an alternative in pts with poor renal function.
Stop heparin gtt and give Eliquis now or give 2 hours after stopping heparin gtt. Give loading dose Eliquis even if the pt was on heparin gtt.
4 notes
·
View notes
Text
Antidote for Anticoagulation Overdoses

Protamine sulfate- heparin
Kcentra/FFP- warfarin
0 notes
Text
That moment when you read about a national drug shortage and think, “that’s our bad, guys, sorry. We’re doing our best to nudge our providers away from the current ordering trend, sorry.”
13 notes
·
View notes
Text
@bitterbeebo tagged me for this
Rules: Answer the questions and tag 20 people you would like to get to know better
Name: kenny
Nicknames: kcentra / kasey
Zodiac Sign: gemini
Height:I don’t even know
Orientation: asexual aromantic
Ethnicity: canadian
Favorite Fruit: grapes
Favorite Season: winter
Favorite Book: she’s come undone
Favorite Flowers: lamprocapnos / sundews
Favorite Scent: the smell of r ain and flowers
Favorite Colour: blues,purples, black
Favorite Animal: penguins
Coffee, Tea, or Hot Chocolate: hot chocolate
Average Sleep Hours: ??? I don’t know anymore
Cat or Dog Person: cat
Favorite Fictional Character: dolores price
Number of Blankets I Sleep With: 1
Ideal Trip: australia.
I tag: @nerdpaw @twisted-trash
3 notes
·
View notes
Link
The Global Prothrombin Complex Concentrates Market is likely to gain traction due to the a significant drop in demand for its counterpart fresh frozen plasma (FFP). Fortune Business Insights has published a report, titled ‘Prothrombin Complex Concentrate Market Size, Share and Global Trend by Product Type (3-factor PCC, 4-factor PCC), Application (Congenital and Acquired Coagulation Factor deficiency), End User (Hospitals, Ambulatory Surgical Centers) and Geography Forecast till 2025. In this report, Fortune Business Insights has predicted that this market, which was valued at US$536.3 Mn in 2017, reach US$ 1,076.5 Mn and in doing so, it will exhibit a CAGR of exhibiting a CAGR of 9.1%.
Sample PDF Brochure at https://www.fortunebusinessinsights.com/enquiry/request-sample-pdf/prothrombin-complex-concentrate-market-100102
Some of the major companies that are present in the Global Prothrombin Complex Concentrates Market are;
· Grifols
· CSL Behring
· Octapharma Sweden
· Sanquin
· Shire
· Kedrion S.p.A
· China Biologic Products Holdings, Inc.
· Other players
Clinical studies have proven that fresh frozen plasma needed much longer infusion time, as compared to prothrombin complex concentrate (PCC). Besides infusion time, PCC possess some other advantages over FFP. Some notable properties that have led to PCC’s increasing adoption are its ability to reconstitute in a short span. Furthermore, PCC is available easily due to its lack of blood group specificity. In addition to the aforementioned factors, a better safety profile of PCC has influenced users to prefer them over fresh frozen plasma.
Leading Companies Are Focusing On Setting Up Plasma Collection Centres
As companies are realizing the clinical advantages of PCC over fresh frozen plasma, they are now focusing on research and development of PCC. It is seen that there is an emphasis on stocking up plasma from blood that is required in PCC. To ensure that these needs are sufficed, leading companies such as Grifols SA and Octapharma are putting in increased efforts towards setting up plasma collection centres across several countries around the world.
Kcentra Has Changed the Face of PCC, Globally
Ever since Kcentra was approved by the FDA, it has been adopted by many healthcare professionals worldwide. Kcentra has proven efficient in restoring blood coagulation, as it is packed with certain factors that help replenish various clotting factors. Kcentra played a major role in treatments for patients who are undergoing warfarin therapy. Warfarin may lead to sever and acute blood loss and to minimize such losses and restoring coagulation factors, Kcentra has been proved beneficial. Therefore, the use of PCC in warfarin induced bleeding is leading to increased adoption which in turn has boosted the global market.
Increasing Government Initiatives and Funding to Boost the Global Market
Recent updates in policies regarding usage approval have boded well for prothrombin complex concentrates. There has been a relaxation in usage of PCC in treating bleeding disorders, globally. This has encouraged research analysts and related personnel to conduct more clinical trials and propose newer usage concepts to the regulatory authorities. Moreover, increasing government funding promoting the use of PCC in surgical procedures is boosting the global market. Proven clinical efficiency of PCC has encouraged governments across the world to promote the use of PCC for treating unwanted bleeding in surgical procedures. Furthermore, few alternatives are available to treat bleeding and the existing alternatives do not come close to the standards set by PCC. This in turn has led to an increase in demand for PCC and subsequently boosted the global PCC market.
3.Market Dynamics
3.1. Market Drivers
3.2. Market Restraints
3.3. Market Opportunities
4. Key Insights
4.1. Prevalence of Coagulation Factor Deficiency – For Key Countries
4.2. Recent Industry Developments – Partnerships, Mergers & Acquisitions
4.3. Regulatory Scenario – For Key Countries
4.4. Analysis in Relation to Alternatives to PCC
4.5. Global PCC Market: Reimbursement Scenario & Key Industry Trends
Browse Complete Report Details at https://www.fortunebusinessinsights.com/industry-reports/prothrombin-complex-concentrate-market-100102
0 notes
Text
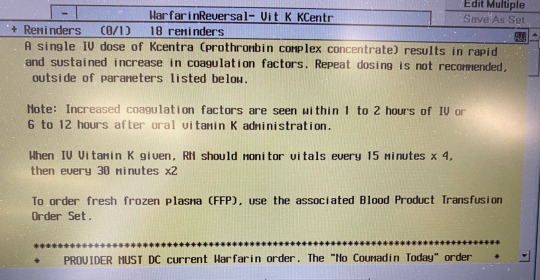
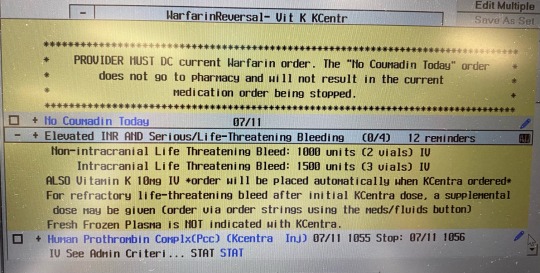
Phytonadione is vitamin K, which can be given to reverse warfarin. Today I have a pt with a supratherapeutic INR at 4.1 who takes warfarin for AFib. I ordered the order set (Warfarin reversal) - Vit K KCentra.
KCentra = prothrombin complex concentrate
3 notes
·
View notes
Text
KCentra (prothrombin complex concentrate) has all the factors affected by warfarin and proteins C and S.
1 note
·
View note
Text


Anticoagulation Pharmacy Lecture
8/23/23
Unfractionated heparin (UFH) work on factors Xa and IIa; it binds to and potentiates the action of antithrombin to facilitate inactivation of factors Xa and IIa. Monitor with activated prothrombin time (aPTT). VTE ppx: 5000 U SubQ q8. VTE tx: 80 U/kg bolus, then 18 U/kg/hr continuous infusion. Adverse effects: bleeding, thrombocytopenia, infusion reactions.
Low Molecular Weight Heparin (LMWH) acts on factor Xa and thrombin a little bit. Works the same as UFH by binding antithrombin, which inhibits factor Xa. More predictable kinetics than UFH. Reversed with protamine. Grouped in with enoxaparin.
Enoxaparin for VTE ppx for pts >120 mg is 40 mg bid
Fondaparinux is a synthetic version of a piece of heparin, works to inhibit factor Xa, no effect on thrombin. Likely safe for pt with HIT. VTE ppx: 2.5 mg qd, unless pt is under 50 kg.
Heparin Induced Thrombocytopenia (HIT) – platelet factor 4 released from platelets binds to heparin and antibodies form against that complex. This activates the plateletsà thrombocytopenia and increased coagulability. 4T score of 0-3 is less than 1% possibility that the pt has HIT. If 4T score is hight, send for SRA (Serotonin-Release Assay). You have to stop heparin and start a different anticoagulant if pt has HIT. Direct thrombin inhibitors are safe to use for AC in pts who have HIT. These are argatroban and bivalirudin. Monitor these with aPTT. There’s no reversal agent for these. These prevent and treat thrombosis in the setting of HIT or if pt doesn’t respond to heparin. Bivalirudin is cleared renally. Argatroban is cleared hepatically.
Oral Anticoagulation
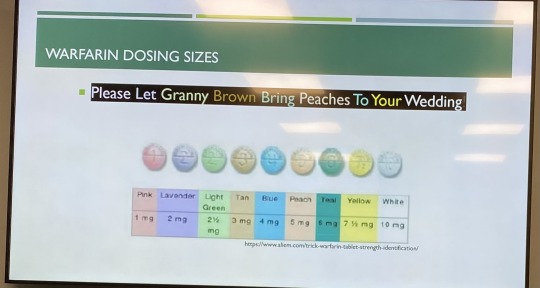
Warfarin – works on factors 7, 9, 10, and 2. It inhibits vitamin K epoxide reductase complex 1. Bridge with heparin because it inhibits proteins C and S, which are anticoagulants. Start 5 mg x2 days then check INR. Can do 2.5 mg if <50 kg; 7.5 mg if >120 kg. Vitamin K or KCentra can reverse warfarin. Warfarin pills have different colors for each strength of warfarin.
INR goals:
Non-valvular AFib: 2-3
DVT/PE: 2-3
Mitral mechanical valve: 2.5-3.5
Coagulopathies: 2-3
Factor Xa inhibitors: apixaban, rivaroxaban, edoxaban – for non-valvular AFib; no monitoring required, safe to use in HIT; reversed with KCentra or Andexanet Alfa (rivaroxaban and apixaban).
Apixaban C/I in severe hepatic disease.
Xarelto should be taken at night with evening meal (or biggest meal of the day to increase absorption); C/I with dialysis (increases bleeding risk). Pts on Xarelto who need dialysis should be on apixaban instead. Apixaban causes less GI and intracranial bleeding.
Savaysa (edoxaban) C/I in pts with CrCl > 95 mL/min
Dabigatran – direct thrombin inhibitor; no monitoring required; safe to use in HIT; reverse with PraxBind (idarucizumab). Dabigatran is very expensive. Expires 6 weeks after bottle opened. Renal adjustment.
Apixaban has been studied in cancer pts.
DOACs for obese pts: conflicting evidence; some evidence of altered kinetics. Modest reduction in AUC in pts >120 kg. AUC reduction doesn’t appear to affect the efficacy of the drug.
Warfarin reversal:
KCentra (prothrombin complex concentrate) has all the factors affected by warfarin and proteins C and S. Dosing: 1500 units for intracranial bleed; 2000 units for DOAC reversal. KCentra is very prothrombotic and dangerous; can cause a thrombotic event. The pharmacy will call you if you order it. KCentra should only be used for emergency bleeding in the ED.
You always give vitamin K (phytonadione) with KCentra. KCentra is short-term benefit. Vitamin K provides long-term benefit. Works in 12-24 hours.
INR 4 to 10, no need to give vit K. If INR >10 and no bleeding – just give vit K. If major bleed, give 5-10 mg IV vitamin K and KCentra. If pt needs urgent procuder, give KCentra.
Vitamin K dosing: 1000 units for intracranial bleed.
Andexanet and KCentra reverse apixaban (Eliquis). Andexanet binds Xa inhibitors.
Bridging: use short acting AC while waiting for long-acting AC to take effect. Can use heparin. Bridge x4-5 days and until INR is therapeutic for 2 measurements.
Heparin needs to be held 4-6 hours prior to surgery, warfarin should be held 5 days prior to surgery.
Resume warfarin 12-24 hours after surgery.
3 notes
·
View notes
Text
My pt has supratherapeutic INR of 12! Held his warfarin and ordered Kcentra, and vit k. You can also give FFP instead of KCentra, but don't give both KCentra and FFP.
It takes 24 to 48 hours for PO vitamin K to start working. IV vitamin K works faster than PO vitamin K. IV vitamin K starts working in 2 hours.
If you give PO vitamin K, re-check INR in 12 to 24 hours.
If someone has a mechanical heart valve, you don't want to give too much vitamin K because they could throw a clot. You would give 1 to 2 mg PO vitamin K to a person with a mechanical heart valve.
KCentra works faster than FFP. But KCentra has increased risk of VTE compared to FFP.
4 notes
·
View notes
Text
Kcentra = Prothrombin complex concentrate (PCC), also known as factor IX complex, is a medication made up of blood clotting factors II, IX, and X. Some versions also contain factor VII. It is used to treat and prevent bleeding in hemophilia B if pure factor IX is not available. It may also be used in those with not enough of these factors due to other reasons such as warfarin therapy. It is given by slow injection into a vein.
Prothrombin complex concentrate reverses the effects of warfarin and other vitamin K antagonist anti-coagulants and is used in cases of significant bleeding in people with a coagulopathy. It is also used when such a person must undergo an emergency operation treatment. Other uses include a deficiency of one of the included clotting factors, either congenital or due to liver disease, and hemophilia. Several guidelines, including those from the American College of Chest Physicians, recommend prothrombin complex concentrate for warfarin reversal in people with serious bleeding.
For rapid anticoagulation reversal for surgery, four-factor prothrombin complex concentrate reduces international normalized ratio (INR) decreases bleeding during surgery appears better than fresh frozen plasma. No differences in thromboembolic event was found.
The package insert states that prothrombin complex concentrate is contraindicated in patients with disseminated intravascular coagulation, a pathological activation of coagulation, because giving clotting factors would only further fuel this process. However, if the PCC is given because factor levels are low, it can restore normal coagulation. As PCC products contain heparin, they are contraindicated in patients with heparin-induced thrombocytopenia.
3 notes
·
View notes
Text
KCentra (PCC) reverses Eliquis
Prothrombin complex concentrate (PCC), also known as factor IX complex, is a medication made up of blood clotting factors II, IX, and X.[1] Some versions also contain factor VII.[2] It is used to treat and prevent bleeding in hemophilia B if pure factor IX is not available.[1][3] It may also be used in those with not enough of these factors due to other reasons such as warfarin therapy.[3] It is given by slow injection into a vein.[1]
Common side effects include allergic reactions, headache, vomiting, and sleepiness.[1][4] Other serious side effects include blood clots which may result in a heart attack, stroke, pulmonary embolism, or deep vein thrombosis.[4] Antibodies may form after long term use such that future doses are less effective.[3]
Prothrombin complex concentrate came into medical use in the 1960s.[5] It is on the World Health Organization's List of Essential Medicines, the safest and most effective medicines needed in a health system.[6][7] It is made from human plasma.[4] A version that is made by recombinant methods which only contains factor IX is also available.[8] In the United States a dose of PCC costs about US$900.[9] A number of different formulations are available globally.[10]
3 notes
·
View notes
Text
This pt had an INR of 9, which is way too high. So he was given vitamin K 10 mg IV and 2 units pRBCs. We were going to also give Kcentra, which is clotting factors II, VII, IX, and X as well as proteins C and S. After the vitamin K, his INR was 1.6. So we didn't give the Kcentra. From UpToDate:
The greatest risk of bleeding with warfarin generally occurs during the initial phase of treatment and/or during periods of international normalized ratio (INR) instability (eg, intercurrent illnesses, interacting medications). Bleeding risk is also increased by some comorbidities (eg, liver disease, kidney disease, heart failure) and other factors (eg, age, prior hemorrhage, concomitant nonsteroidal anti-inflammatory drug [NSAID] use, especially nonselective NSAIDs); these should be addressed when possible. Typical major bleeding rates reported in randomized trials are in the range of 1 to 3 percent per person-year. (See 'Mitigating bleeding risk' above and "Risks and prevention of bleeding with oral anticoagulants".)
●Treatment – The optimal approach for managing a patient with warfarin-associated bleeding or supratherapeutic INR depends on the presence of clinically significant bleeding, the degree of INR elevation, and the underlying thrombotic risk/indication for anticoagulation (table 1).
•Serious bleeding – Patients with serious or life-threatening bleeding and a prolonged INR (eg, >2) should have warfarin withheld and should receive vitamin K (10 mg) by slow intravenous infusion, along with a rapid reversal agent. We suggest a 4-factor prothrombin complex concentrate (PCC) (table 2) rather than a 3-factor PCC and/or Fresh Frozen Plasma (FFP) (Grade 2B). If 4-factor PCC is not available, a 3-factor PCC supplemented with FFP or FFP alone is appropriate. Vitamin K administration can be repeated every 12 hours for a persistently elevated INR. (See 'Serious/life-threatening bleeding' above and 'PCC products, efficacy, risks' above.)
Management of warfarin-associated intracerebral hemorrhage (ICH) is discussed separately. (See "Reversal of anticoagulation in intracranial hemorrhage".)
•Surgery – For a patient who requires urgent surgery or invasive procedure, the bleeding risk, need to reverse anticoagulation, and urgency of surgery/procedure should be determined in consultation with the surgeon/interventionist. (See 'Urgent surgery/procedure' above and "Perioperative management of patients receiving anticoagulants", section on 'Deciding whether to interrupt anticoagulation'.)
-Patients who require emergency (eg, same day) surgery and warfarin reversal should have warfarin held and should receive vitamin K and a rapid reversal agent as done for serious bleeding. We suggest a 4-factor PCC rather than FFP (Grade 2B).
-Individuals who can wait 24 hours and require warfarin reversal may be managed by holding warfarin and giving vitamin K without the use of a PCC.
-Management of warfarin around the time of elective surgery is presented separately. (See "Perioperative management of patients receiving anticoagulants".)
•Minimal bleeding – Minimal bleeding can be treated as outlined for more significant bleeding (eg, with PCC) or for supratherapeutic INR without bleeding, depending on the perceived likelihood of progression to more severe bleeding. (See 'Minimal bleeding' above.)
•INR >10 without bleeding – For individuals with an INR >10 without bleeding, warfarin therapy should be held. Oral vitamin K (2.5 to 5 mg) can be administered, depending on the bleeding risk of the patient. Nonbleeding patients should not be given a PCC or FFP solely to correct a supratherapeutic INR, as these products have associated risks. The INR is monitored daily or every other day, and warfarin is resumed at a lower dose once the INR is in the therapeutic range. (See 'INR >10 without bleeding' above and 'Vitamin K dose, route, formulation' above.)
•INR 4.5 to 10 without bleeding – For individuals with an INR between 4.5 and 10 without bleeding, warfarin is held temporarily (eg, one or two doses) with or without administration of a small dose of oral vitamin K (eg, 1 to 2.5 mg). Warfarin generally is resumed at a lower dose once the INR is in the therapeutic range. (See 'INR 4.5 to 10 without bleeding' above and 'Vitamin K dose, route, formulation' above.)
•INR <4.5 without bleeding – For individuals with an INR <4.5 without bleeding, one or more doses of warfarin may be omitted and/or the dose is reduced slightly. If the INR elevation is minimal and/or expected to be transient, no dose reduction may be necessary. Additional therapies such as vitamin K are not indicated in this setting. (See 'INR <4.5 without bleeding' above.)
●Poisoning with a superwarfarin can cause severe, prolonged coagulopathy, and patients usually require massive doses of vitamin K over months to years. (See 'Superwarfarin poisoning' above.)
●Individuals with a supratherapeutic INR should also be evaluated for possible medication errors or metabolic changes that might have caused excessive anticoagulation. Those with gastrointestinal bleeding or hematuria will require evaluation for the source of bleeding. Any individual who presents to the emergency department with head trauma while on warfarin should be considered for neuroimaging as part of the emergency assessment regardless of the presence of neurologic symptoms or the severity of the trauma. (See 'Additional evaluations' above.)
●The decision to resume anticoagulation depends on several factors including thrombotic risk, bleeding site, and modifiability of other risk factors for bleeding or supratherapeutic INR. A significant number of patients are able to resume warfarin safely. Some may be good candidates to resume anticoagulation with a different agent such as a direct oral anticoagulant (DOAC). (See 'Resumption of anticoagulation after bleeding' above and "Risks and prevention of bleeding with oral anticoagulants", section on 'Prognosis and reinitiation of anticoagulation'.)
●Management in the setting of a prosthetic heart valve is presented separately. (See "Antithrombotic therapy for prosthetic heart valves: Management of bleeding and invasive procedures", section on 'Management of overanticoagulation and bleeding'.)
ALERT: US Boxed Warning
Arterial and venous thromboembolic complications:
Patients being treated with vitamin K antagonist therapy have underlying disease states that predispose them to thromboembolic events. Weigh potential benefits of reversing vitamin K antagonist against the potential risks of thromboembolic events, especially in patients with history of a thromboembolic event. Carefully consider resumption of anticoagulation as soon as the risk of thromboembolic events outweighs the risk of acute bleeding.
Both fatal and nonfatal arterial and venous thromboembolic complications have been reported with prothrombin complex concentrate in clinical trials and postmarketing surveillance. Monitor patients receiving prothrombin complex concentrate for signs and symptoms of thromboembolic events.
Prothrombin complex concentrate was not studied in subjects who had a thromboembolic event, myocardial infarction, disseminated intravascular coagulation, cerebral vascular accident, transient ischemic attack, unstable angina pectoris, or severe peripheral vascular disease within the prior 3 months. Prothrombin complex concentrate may not be suitable in patients with thromboembolic events in the prior 3 months.
Brand Names: US
Kcentra
Brand Names: Canada
Beriplex P/N
Pharmacologic Category
Blood Product Derivative;
Hemostatic Agent;
Prothrombin Complex Concentrate (PCC)
Dosing: Adult
Note: Prothrombin complex concentrate (human) [(factors II, VII, IX, X), protein C, protein S] contains therapeutic levels of factor VII component and should not be confused with factor IX complex (human) [factors II, IX, X] (Bebulin, Profilnine).
Kcentra, Beriplex P/N [Canadian product]: Vitamin K antagonist reversal in patients with acute major bleeding or need for an urgent surgery/invasive procedure:
Note: Dosage is expressed in units of factor IX activity. Administer concurrently with vitamin K.
Weight-based dose: IV:
Pretreatment INR: 2 to <4: Administer 25 units/kg; maximum dose: 2,500 units.
Pretreatment INR: 4 to 6: Administer 35 units/kg; maximum dose: 3,500 units.
Pretreatment INR: >6: Administer 50 units/kg; maximum dose: 5,000 units.
When using a weight-based approach, repeat dosing is not recommended (studies have not evaluated clinical outcomes).
Fixed dose: IV: Initial: 1,000 to 2,000 units once; for intracranial hemorrhage use, 1,500 to 2,000 units is recommended; repeat dosing has not been adequately studied and is not typically recommended unless INR reversal is inadequate (ACC [Tomaselli 2020]; Bitonti 2019; Fuh 2020; Gilbert 2020; Khorsand 2012; Schwebach 2019).
5 notes
·
View notes
Last Seen Blogs

classyglitterdragon
Untitled

iceglade
my one wish

marketologs
Без названия
stonesandtilesmelbourne
Stones and Tiles

aventurs-bloger
Странный блог об Испании