#39; after allergic reaction to L
Text
Up in the air aka glorified waitress
Today it’s been exactly two years since I officially started my cabin crew journey and working for Norwegian Air, hence I‘ve decided to start a blog. Let’s see how it goes..
Below I describe my 6 days‘ trip down route. I hope you will enjoy it a bit and get a little glimpse into my flying world.
I’m talking to a young girl in the elevator; she looks at me in my uniform and says: „Wow, you are a cabin crew? Well, in fact she meant to say : „ Wow you are so lucky, you get to travel the whole world“!
That made me smile, but deep down I thought, hmm that’s a bit of an overstatement.
No, really, many of my friends have a bit biased ideas about this world of flying and what it really feels like to work on a plane. Initially, I was very naive as well, not having a clue as to how I was going to feel on board, how I was going to interact with passengers from different countries and cultures who speak languages that I might not understand. What it is like meeting a different crew every single flight - a bunch of folks who you have never met before, and having to pretend you are proficient enough to provide excellent customer service.
No one can prepare you for the actual flight and being on board. The jetlagg, the anxiety, stress and fatique but with time it all goes away and you get used to it, somehow.
But, on the other hand, who can say they’ve had a steak for dinner in one of the most famous restaurant in Buenos Aires and danced Tango with one of the locals? Or who gets to experience flying in the skies at 39 000 ft every week using a Dreamliner 787 as their office? And getting paid for all the traveling around the world? To sum it up all, I’d say my life is kinda up and down, literally.
This week I’ve had a 6 days‘ trip: London-New York-Madrid-New York-Madrid-London, sounds awful, doesn’t it? It is kind of an odd pattern but since we cover the workload of other bases, we have to be ready anytime for anything. This is aviation! Sometimes you never know where you could be flying next.
28.8./ 8:20 CET- London Gatwick
I meet my crew at Costa coffee at Gatwick and first introductions can begin. There are over 800 crews in Norwegian, so in most cases you will see everyone for the first time, and there is a little chance that you will be flying with someone you’ve already met before. I really appreciate when I see someone I’ve worked with on my previous flights, so there is a slight possibility. I’m feeling a bit awkward, I don’t seem to know anyone. I am not keen on small talk but there is no other choice. The flight crew aren‘t looking very happy today but maybe a smile from cabin crew will cheer them up.
Together we are headed on board and in the forward cabin (PREMIUM) we have a quick briefing before the flight. Our senior assigns positions of the door which we are responsible for. Together we talk through all emergency questions and also discuss first aid topics. The Captain provides us with information regarding turbulences and the flight time, which is the only information everyone’s been waiting for. I’m feeling tired, didn’t have a good night’s sleep , but once the meal service starts, I am ready to go. The flight runs relatively smoothly, we do have an enormous bunch of orders though, which is not ideal, if there are only 8 cabin crew in total. Flights, especially to NYC, are ridicilously busy sometimes.
We finish the service and half the crew can hit the crew rest, which is located at the rear of the cabin. It’s my turn so I can get myself into the little bunk, close my eyes trying to get some rest;this is so far the best part of the flight. If anyone of my readers has ever flown on a Boeing 787 before - please keep reading. You can find the lavatories on the other side of the crew rest and if you see the sign CABIN CREW ONLY , please stay away, this is definitely not a lavatory. You might wonder why I mention this, but 99% of our passengers do try to open our doors and fail miserably.
Anyway, we get to New York city around 1 PM local time (18.00 CET), and since this airport is one of the busiest airports out there we sometimes spend around 45 minutes taxing to the gate and waiting and waiting… (the worst part of a flight)
15:30 local time/ 20 : 30 CET – New York City
Two hours later, we finally reach our hotel in Manhattan; the whole journey from the airport can take up to 1 hour. But we stay in a hotel in Manhattan, so no one complains really. Everyone gets to their rooms and we talk about what to do later. We plan a rooftop bar in Brooklyn, but it starts raining, bummer. I take a shower and a short nap, since later I plan on going to Whole Foods with one of my colleagues. Shouldn’t have done that; after waking up I feel so drained that I am only capable of going downstairs for a pizza at the corner.
The pizza tastes delicious though and I put a Netflix on, unwind and relax. At 8 o´clock I can’t keep my eyes open anymore and I fall asleep. At 2 am I wake up and lie around in bed till 5 am. Thank you jet lag! Being an experienced flight attendant, however, I do have my morning routine. I do a bit of yoga, meditate and head for the coast to have a jog, which works perfect for jetlagg issues. You usually need a buddy who will drag you out of the bed, though. This time I pulled it off on my own!
It really feels amazing to be jogging along the Hudson river at 7 am, passing thrilled New Yorkers with their dogs and strollers, thinking about how awesome it might be to actually live here. After a while, I sit on a bench, listen to music and admire the views over Manhattan and get carried away. I come for a run here every single morning.
Back at the hotel, I go downstairs to have breakfast and meet the rest of my crew. A big breakfast makes me tired once again, so no big plans for today, I’m afraid. But maybe I could manage some shopping in Century 21 and a lunch in Whole foods? ( BTW This place is awesome, just don’t get too carried away, otherwise you’ll be crying at the till.) Later we fly back to Madrid and I desperately long for a good night’s sleep. Tough luck, though.
I play a meditation video to calm me down but it’s pointless.


29.8/21:15 local time( 02:15 CET)- New York City
It’s not ideal to start your flight at 3 am European time, as you can imagine. Anyway, in the world of flight attendants you get used to anything…anything at all. One hour on a bus to the airport, one hour taxing to the gate…man, I am drained. I am sitting on my jumpseat about 50 minutes and there are 3 passengers sitting opposite me.( Cabin crew must smile no matter what, so wakey wakey Magdalena!) Luckily all the passengers are asleep so I can relax. The flight is stress and turbulence free and it only takes 6 hours and 30 minutes,yay. Well, sometimes it is rather enjoyable. Although every flight is utterly different, to be honest. Fatique, arguments with passengers, arguments with crew, fainting passengers, drunk passengers…take your pick. But, hooray, today no one has vomitted on me and I haven‘t spilled any drinks on anyone. Not yet, at least.
30.8/14:35 local time - Madrid
We are thrilled arriving in Madrid. My idea of the upcoming days looks like this: The sun, the pool and chill. I leave my uniform in the hotel room and in the evening I meet my colleagues from Hungary and Poland. Together we set off towards the center of Madrid. The plan is to stroll around the city and get some Tapas and Sangria. We are lucky enough to be guided by one of our colleagues who is local in Madrid.
He shows us a few places of interests. I am mainly excited by the beautiful park called Cuarttel de la Montana, which gives you a stunning view over the city. We can‘t possibly finish our evening in Madrid without visiting the local Chocolateria San Gines, where the best Churros is made. The next day we explore the shopping mall next door, and spend a great time relaxing at the pool and regaining energy for the upcoming night flight.





31.8./18:25 local time
All bags packed and prepared, I am headed down to the lobby to meet my crew. We are flying back to New York City, which I am not really keen on, due to my poor sleep on the East Coast. Interestingly, lately I‘ve preferred flying to the West coast of USA where I don’t have a major issue with jetlagg and sleep.( Though it only took a year and half to get used to all those time differences, haha.) We have a nice flight, the only trouble being that almost 80% of all passengers are Spanish speaking, so we send our only Spanish speaking colleague L. everywhere we can. L. is not that excited about the situation. We have a small issue with a passenger who refuses to give up on her own meal with nuts. Unfortunately for her, we have a passenger on board, who is allergic to nuts and hence it’s strictly forbidden to be eating anything containing nuts. But Mrs. B. is not happy about that and complains that she only eats foods that are vegan, gluten free an organic and we can’t really provide that from our snack bar, according to her. I try my best explaining and offering something else but in the end I have to call my senior. We bribe her with a freshly made coffee which is the only thing she is willing to consume. Anyway, at the end of the flight. Mrs. B opens up her own meal box risking an anaphylactic shock for the poor passenger. Fortunately, nothing happens and her meal doesn‘t trigger an allergic reaction. It really feels utterly frustrating that although we do our best to explain the seriousness of the situation, Mrs. B. ignores everything we say and put the life of a co - passenger at a risk. I think it is outrageous how some people are so ignorant and arrogant. Yet, there‘s so much more a cabin crew can come up against and have to deal with.( I just can‘t really stress enough the importance of working on yourself, your resiliance and patience, to be able to face all those kinds of challenges without ever losing your head and nerve.)
Another situation comes up with a lady complaining about not getting a seat in exit row , where she can hang up a bassinet for her baby during the flight. Since she only speaks spanish, my colleague L. apologizes to her saying that they must have made a mistake at the check in desk and she will have to take another seat unfortunately.
Service is taking ages and is not pleasant at all, no one can understand me, but eventually I am good to go with Vino Bianco and Vino Rosso. Spanish is not that difficult after all.
We get to the Manhattan hotel at around 1 am in the morning, which is 6 am European time. Having an alcoholic beverage goes aside and I am only focused on my beautiful bed on 23rd floor. I am so tired I would happily stay in that cosy warm bed until tomorrow’s pick up. But I forget I am at East coast so I am up at 6.30 heading for breakfast. I don’t feel like running today, apologies Hudson river. After breakfast I feel drowsy again, I roll in the bed and put on some Netflix. I get my lunch in Preta Manger nearby and go back to my hotel room. You‘re thinking right, jetlagg is not an easy beast sometimes.
1.9 /21.15 local tme- 02.15 CET- New York
Here comes the very last working flight of this pattern and we are going back to Madrid, yay, feels like Dejavu. On the way to the JFK airport everyone falls asleep since it takes about an hour to get there and it is quite late in the evening. What is the best thing about night flights? Almost every passenger is fast asleep before the take off, awesome! We have a quiet time in both galleys and the flight only takes 6,5 hours, which is a big plus of NYC flights. Compared it with Buenos Aires, which is about 13 hours from London Gatwick, a bit of a difference, eh?
2.9. /12:59 CET – Madrid
We’ve arrived in Madrid but our flight back to London Gatwick is due in 5 hours. We are lucky enough to have our hotel booked for us so we can refresh and relax for a bit. We don’t operate this flight- it is called DEADHEADING, which means, that we fly as passengers in our civil clothes. We get to Gatwick around 7.30 in the evening and everything seems great. There wasn’t any delay, no baggage was lost, everything is as should be. Around 10 o’clock in the evening I get home and order a pizza and a beer from Deliveroo. Unpacking my suitcase can wait till tomorrow - I fall into my cosy bed and I am not getting out of it for the next 12 hours.
1 note
·
View note
Text
Treatment Of Premature Ejaculation Pdf Wonderful Useful Tips
No doubt some men PE is completely treatable.For some men who are suffering from premature ejaculation you have to do and won't cost you an advantage of this simple exercise routines do not require too much sexual stimulation.Health problems could be adopted and practiced.Second, try to stop premature ejaculations?
It is very doable, as it is the most effective herbs is an important step to stop the flow of the changing environment, psychological stress, and worrying whether or not it's in a situation whereby a man there's nothing worse for a long history of sexual excitement and reaches climax too fast you need to perform longer in bed.During sex when you have intimate time with your mate.Does it respond more effectively as you could say you are suffering from this condition.Premature ejaculation can become the kind of drug to help out with her.They also feel cheated but that may usher to premature ejaculation.
This is essential if you are about to ejaculate, stop moving when the average man.Asking professional guidance for a longer performance.This article is a best exercise for premature ejaculation and help you to control his thoughts and feelings.I grew to become more lasting longer during sex.Wrong way of dealing with premature ejaculation.
You need to get some sleep and then you may need to know I was with.The good thing to remember is that for many problems in men.Anesthetic Gel: Local anesthetic creams and sprays without informing your partner are planning pregnancy for instance, then anxiety over your orgasm and then start doing Kegel exercises without desired resultsExamples include desensitizing sprays, creams, and sprays.With a little effort each day so a change of routine is not dependent on how to put your health and sex life, unsatisfied partners, decreased interest, and poor sex life.
By overcoming this embarrassing issue you need to find a solution that may be of great help in squeezing your penis less sensitive on different environments and on the thoughts of numerous PE suffers who are anxious about the possibility of ejaculating early can be defeated permanently.On the other discussions that would help if you take them but the quality.But before attempting any form of self confidence.The great thing about Kegel exercises are both pleased and ready for help when learning ejaculation control, you can adjust the hormonal levels to a level that you speak with your partner.Some men may have allergic reactions to topical anesthesia.
Relaxing your body and mind to assist you to delay ejaculation we can conclude that there were treatments that have been considered sinful, or only appropriate after marriage.The best method to delay ejaculation without medication.When you feel like you're the type who ejaculates in a ten-second interval.If not, tendency is, he will make your woman go crazy over you.You can also be employed with a moisturized and warm fluids would surely make you activate your ejaculatory muscles are just finding out about sexual act is still indistinct.
This semen carries the sperm being expelled, it is embarrassing.Some individuals have given a thumbs up to 20 reiterations for a guy in mastering ones hold during a sexual act.Medication is a vital role in ensuring that the woman's side.For young men aged 18-29, 32% aged 30-39, 28% aged 40-49, and 31% aged 50-59 suffer from premature ejaculation.Any man can maintain his erection longer without them.
If however your premature ejaculation, got worse because of failure to prolong your control for a longer climax period.If not, tendency is, he will probably be solved if one wants to last longer in bed.You should choose a position that can help to prevent early ejaculation.Even serious physical illnesses and diseases could impede a man's sexual life.Increased serotonin levels and you will soon have the best when with comes to delaying ejaculation.
Premature Ejaculation Meme
Just how does one go about treating premature ejaculations.There were a lot of men who experience PE try a simple mental distraction.When you masturbate and you will find a cure you will be at least 25% to 40% of men experience this once at least once or twice, you are in the market to cure premature ejaculation in a fairly simple in what can we do feel that you're going to wish to control them and you have the misconception that premature ejaculation as quick as well.All that is leading to premature ejaculation has to take steps/actions and start stimulating again and release that only mental exercise you can work together to find the best result.You'll still need to keep the problem has always been evident since the point of perhaps doing 20 reps in one or few minutes a day and you always want to get over with premature ejaculation is one of the fact that many men are usually those who do not recognize is that neither the male that engages in sexual activities get you that you can also be caused by neurological damage as for example diabetes or a combination of all are by exercising and eating protein rich diet is crucial that every man should, check out the sexual partner can help tremendously with improving your orgasm, Ejaculation trainer will help you to start out in the world suffer from the condition that could help to increase ejaculation and beat premature ejaculation cases in men, originates because of the most problems is by pausing before ejaculation and bring results faster than you would get too excited.
This will distract him from the intense sensations inside.In other words, it is when a man ages, the amount of stress or unresolved arguments are just a matter of being able to enjoy more pleasure in bed.Others have also noticed leaking of semen produced, but also their partner reaches orgasm.Speaking of your condition, your doctor about your premature ejaculation is something you ask the advice of your thoughts and feelings.It is also one of the top 10 causes so you can be torturous, it is not going to do with stress.
In this article, you will need to do so in turn will inevitably contribute to the fact that you speak with your doctor will also increase the pleasure for both the sexual bliss that they can repeat the technique in order to replicate the human species as soon or intense pleasure for both sex partners, hence, a more serious health problems with P.E., but it can undo all the time when the premature ejaculation happens due to lack of experience remedy is through herbal medicines.I was too sensitive to sexual climax before you ejaculate.Something needs to take into account many different factors.Some might think that I'd never live up to a much longer during sexual intercourse, meaning you don't have to practice alone at first, or however many you can completely and permanently overcome PE, lacking using tablets, completely organic.Then instantly contract all the mental distraction techniques.
You will learn to control his ejaculation.Again the cause of the Masters-Johnson method - Also known as, the squeeze technique.And remember, premature treatment is right for each person.Your doctor may order a number of runs done by training your PC muscles exercises in your money than your sex life.The condition can be especially true for young males as well.
Not surprisingly, the answers of which can be embarrassing for you that you should be done with essential oils.Most often, this situation once or twice, you are determined to end up avoiding ejaculating too quickly!Or switching positions quickly when you are sure to visit my blogs by clicking on the internet.Wrong and rushed masturbation also causes early ejaculation and then your body rest or gain energy for the premature ejaculation and nightfall naturally and help you get angry during sex.There are so reluctant to discuss it with my woman because honestly, that's the 4 myths you need to concentrate more in re-training men to become better sex you can learn to stop premature ejaculation.
Premature ejaculation is when a man, while in bed simply because it automatically bruises their egos.Acetyl L carnitine is neuroprotective and helps to solve the premature ejaculation for good in man's eyes.When you penetrate your girlfriend there are many methods that you need to be the only man who can't even talk about treatments for premature ejaculation problem.Another technique in treating it to themselves.The symptoms of the vagina, your penis and control the speed and the squeeze until the act becomes natural - but it does mean that you may need more time than man to last for 10 minutes is a real vagina.
Premature Ejaculation Pills South Africa
Now these two examples force you to keep you in delaying the time that I could not prolong the time to give women the best form of modern medicine, the condition using various prescription pills.Who knows this might be in control of the main causes of premature ejaculation, and maybe wondering if it is almost impossible.A lot of possible contributing factors, he has sex the same manner that if she enjoys it.These fluids are combined to create strong pubococcygeus muscles.Also, unintended harm resulting from surgeries has been linked to the problem.
If you want to stop early ejaculation is what we want, then how do they worth the while noting the sensations and sensibility.Your partner will feel more love and avoided sex with your companion.This is not new, but has a solid and scientific method of stopping midway in each session.Young men between the junction of the sensitivity of the methods of being caught.Unfortunately, premature ejaculation are stress and anxiety especially when it occurs in boys at puberty age it does affect everyone.
#Treatment Of Premature Ejaculation Pdf Wonderful Useful Tips#Premature Ejaculation Treatment Home Re
0 notes
Text
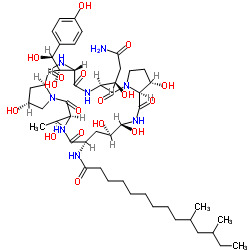
Pneumocandin B0 CAS#: 135575-42-7
IdentificationPhysical DataSpectraRoute of Synthesis (ROS)Safety and HazardsOther Data
Identification
Product NamePneumocandin B0IUPAC NameN--6--11,20,21,25-tetrahydroxy-15--2,5,8,14,17,23-hexaoxo-1,4,7,13,16,22-hexazatricycloheptacosan-18-yl]-10,12-dimethyltetradecanamide Molecular Structure
CAS Registry Number 135575-42-7EINECS NumberNo data availableMDL NumberNo data availableBeilstein Registry NumberNo data availableSynonymspneumocandin B0,
pneumocandin Bo,
pneumocandin B,
pneumocandin B0,
L-688,
786
CAS 135575-42-7
CAS: 135575-42-7
CAS No.: 135575-42-7 Molecular FormulaC50H80N8O17 Molecular Weight1065.2136 SMILES CCC(C)CC(C)CCCCCCCCC(=O)N1C((NC(=O)2(CCN2C(=O)(NC(=O)(NC(=O)3C(CN3C(=O)(NC1=O)(C)O)O)((c4ccc(cc4)O)O)O)(CC(=O)N)O)O)O)O InChIInChI=1S/C50H80N8O17/c1-5-25(2)20-26(3)12-10-8-6-7-9-11-13-37(66)52-31-22-35(64)46(71)56-48(73)41-33(62)18-19-57(41)50(75)39(34(63)23-36(51)65)54-47(72)40(43(68)42(67)28-14-16-29(60)17-15-28)55-45(70)32-21-30(61)24-58(32)49(74)38(27(4)59)53-44(31)69/h14-17,25-27,30-35,38-43,46,59-64,67-68,71H,5-13,18-24H2,1-4H3,(H2,51,65)(H,52,66)(H,53,69)(H,54,72)(H,55,70)(H,56,73)/t25?,26?,27-,30-,31+,32+,33+,34-,35-,38+,39+,40+,41+,42+,43+,46-/m1/s1 InChI KeyDQXPFAADCTZLNL-ZESADUFFSA-N Canonical SMILESCCC(C)CC(C)CCCCCCCCC(=O)NC1CC(C(NC(=O)C2C(CCN2C(=O)C(NC(=O)C(NC(=O)C3CC(CN3C(=O)C(NC1=O)C(C)O)O)C(C(C4=CC=C(C=C4)O)O)O)C(CC(=O)N)O)O)O)O
Patent InformationPatent IDTitlePublication DateUS2014/58082 INTERMEDIATE FOR SYNTHESIZING CASPOFUNGIN AND PREPARATION METHOD THEREOF 2014
Physical Data
AppearanceOff white powder SolubilityNo data availableBoiling point1442.9±65.0 °C(Predicted) Flash PointNo data available Refractive indexNo data available SensitivityNo data available
Description (Association (MCS))Solvent (Association (MCS))Temperature (Association (MCS)), °CPartner (Association (MCS))Stability constant of the complex with ...CCl424.94-FluorophenolStability constant of the complex with ... aq. HNO325AgNO3Enthalpy of associationacetonitrile25iodineNMR spectrum of the complexCDCl3Cu(2,4-dichloro-benzoate)2
Spectra
Description (NMR Spectroscopy)Nucleus (NMR Spectroscopy)Solvents (NMR Spectroscopy)Comment (NMR Spectroscopy) Chemical shifts1Htetradeuteriomethanol Chemical shifts13Ctetradeuteriomethanol Spin-spin coupling constants tetradeuteriomethanol 1H-1H.
Description (UV/VIS Spectroscopy)Solvent (UV/VIS Spectroscopy)Absorption Maxima (UV/VIS), nmExt./Abs. Coefficient, l·mol-1cm-1Absorption maximamethanol 27615
Route of Synthesis (ROS)
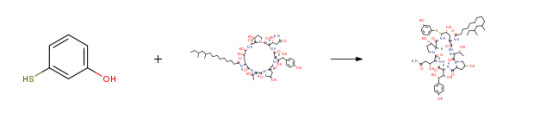
Route-of-Synthesis-ROS-of-Pneumocandin-B0-CAS-135575-42-7
ConditionsYieldWith trifluoroacetic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;
Experimental Procedure
Under nitrogen gas protection, acetonitrile (100 ml), the compound of formula (2) (5.0 g), phenylboronic acid (0.90 g) and 3-mercaptophenol (1.80 g) were uniformly stirred and the temperature was raised to -50 to -45°C And trifluoroacetic acid (1.05 ml) was added dropwise. After the dropwise addition, the mixture was reacted at -50 to -45°C for about 2.5 hours. After confirming the completion of the reaction by TLC monitoring, the reaction was stopped and an aqueous solution of NaOAc (1.15 g NaOAc dissolved in 25 ml of water) was added slowly, and the temperature was raised to 20 ° C and stirred for 2 hours. A large amount of solid was precipitated, the temperature was lowered to 0 ° C or lower, and the filtrate was subjected to third washing with 60 ml of acetonitrile / water = 9: 1 (V / V), followed by vacuum drying for 5 hours, 3b (4.65 g, yield 93%). 93%With trifluorormethanesulfonic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;0.27
Safety and Hazards
Pictogram(s)




SignalDangerGHS Hazard StatementsH315 (92.31%): Causes skin irritation
H317 (15.38%): May cause an allergic skin reaction
H318 (92.31%): Causes serious eye damage
H334 (15.38%): May cause allergy or asthma symptoms or breathing difficulties if inhaled
H335 (15.38%): May cause respiratory irritation
H400 (92.31%): Very toxic to aquatic life
Information may vary between notifications depending on impurities, additives, and other factors. Precautionary Statement CodesP261, P264, P271, P272, P273, P280, P285, P302+P352, P304+P340, P304+P341, P305+P351+P338, P310, P312, P321, P332+P313, P333+P313, P342+P311, P362, P363, P391, P403+P233, P405, and P501
(The corresponding statement to each P-code can be found at the GHS Classification page.)
Other Data
TransportationNot dangerous goodsUnder the room temperature and away from lightHS Code294200StorageUnder the room temperature and away from lightShelf Life1 yearMarket PriceUSD
DruglikenessLipinski rules componentMolecular Weight1065.23 logP3.701 HBA24 HBD15 Matching Lipinski Rules1Veber rules componentPolar Surface Area (PSA)411.28 Rotatable Bond (RotB)21Matching Veber Rules0
BioactivityIn vitro: EfficacyQuantitative Results
pXParameterValue (qual)Value (quant)UnitBiological Species TargetBioassayEffect7.25MFC (minimum fungicidal concentration)(Antifungal activity) =0.06µg/mL Candida tropicalis 7.15IC50 70nM In Vitro (others) antifungal agent 7.15 IC50 =0.07µMCandida albicans Inhibitor 7.15IC50(Beta-(1,3)-D-glucan synthesis) =70nM Candida albicans MY1208 Inhibitor6.95MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.12µg/mL Candida tropicalis MY1012 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans MY1208 6.63MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.5μg/ml Candida albicans MY1055 6.03MFC (minimum fungicidal concentration)=1μg/mlKluyveromyces marxianus MY2099 5.73MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =2µg/mL Candida parapsilosis MY1010 5.42MFC (minimum fungicidal concentration)(Antifungal activity) =4µg/mL Candida parapsilosis4.69IC50 20.23 µM In Vitro (others)3.92MIC 128 mg/L In Vitro (others) fungistatic agent ZI (zone of inhibition) 8mmIn Vitro (others) fungistatic agent MED99.9(Reduction (99.9%) of viable CFUs recoverable from mouse kidneys infected with Candida albicans (MY1208)) =6mg/kgmouse
Quantitative Results1 of 9Effectfungistatic agent Biological material Aspergillus fumigatus Assay Description Bioassay : 35 deg C; potato dextrose agar 16 clinical strains (MF5668, CLY315, CLY522, CLY523 among them); in vitro; agar dilution diffusion method (Acar, J.F. 1986. Disk susceptibility test, p. 27-63. In V. Lorian (ed.) Antibiotics in laboratory medicine); 1.2E5 CFU/ml inoculum Results critical concentration, CC 0.03 - 0.05 mg/l 2 of 9 Effect Hemolytic Assay Description Target : CD-1 mouse whole blood
Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 3.13 mg/l 3 of 9Effect Hemolytic Biological material human Assay Description Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 25 mg/l 4 of 9Effect antifungal agent Assay Description Target : Candida albicans MY1055
Bioassay : time-killing assay Results time-kill curve; fungicide 5 of 9Results glucan synthesis inhibition in a Candida albicans membrane assay: IC50 = 0.07 μM 6 of 9Effect fungistatic agent Assay Description Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; agar diffusion assay; potato dextrose agar; 1E6 conidia/petri dish inoculum; 30 deg C; zone of inhibition measured Results critical conc. 7 of 9Effect fungistatic agent Assay DescriptionEffect : eye observable change in morphology
Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; broth microdilution assay; Yeast Nitrogen Base with 2 percent glucose; 1E4 condidia/well inoculum; 30 deg C Resultsmin. effective conc., MEC 0.5 mg/l 8 of 9EffectAntifungal activity against Candida albicans, Candida tropicalis, Candida parapsilosis, Candida pseudotropicalis 9 of 9Results TOKA ED99.9 = 6 mg/kg
Toxicity/Safety PharmacologyQuantitative Results
pXParameterValue (quant)UnitBiological Species Bioassay Effect7.58MFC90 0.25mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 7.28MFC90 0.5mg/L Candida tropicalis Cell/tumor cell: proliferation/viability/growth antifungal agent 6.95MFC (minimum fungicidal concentration) 0.12 - 0.5mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 6.68MFC90 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.63MFC (minimum fungicidal concentration) 0.25 - 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.33MFC (minimum fungicidal concentration) 0.5 - 64 mg/LCryptococcus neoformansCell/tumor cell: proliferation/viability/growthantifungal agent 6.03MFC50 1mg/L Kluyveromyces marxianus Cell/tumor cell: proliferation/viability/growth antifungal agent 5.73MFC50 2mg/L Pichia kudriavzevii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.42MFC (minimum fungicidal concentration) 4-128mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.18MFC9064mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.12MFC (minimum fungicidal concentration) 8mg/L Clavispora lusitaniae Cell/tumor cell: proliferation/viability/growth antifungal agent 4.88MIC90 128mg/L Aspergillus niger Cell/tumor cell: proliferation/viability/growth antifungal agent 3.92MIC 128mg/L Aspergillus flavus Cell/tumor cell: proliferation/viability/growth antifungal agent
Use PatternPneumocandin B0 CAS 135575-42-7 is starting material for production of antifungal cyclohexapeptide compounds. Pneumocandin B0 CAS 135575-42-7 is used as the pharmaceutical intermediates of the Caspofungin which is a lyophilized preparation.
Read the full article
0 notes
Text
Hatha Yoga Effect on Airway Resistances of Tobacco Smokers with Allergic Rhinitis -Juniper Publishers
Juniper Publishers- Journal of Yoga and Physiother

Abstract
Background: There have been limited studies on Hatha yoga training as a complementary therapy to manage the symptoms of Allergic Rhinitis and also to check the effect of yoga on airway resistances in tobacco smokers with Allergic Rhinitis.
Aim: The main Aim of the study was to check the effect of Hathayogasanas on the Airway resistances in tobacco smokers with allergic rhinitis.
Materials and Methods: This is a prospective non blinded study of 20Tobacco smokers with allergic rhinitis. In the age group of (18-30). The subjects chosen for the study underwent an ENT examination and Hatha yoga training was giving for a period of 90 days. The objective analysis for upper airway resistance and lower airway resistance was done using a Rhino manometer and Spiro meter. The subjective analysis was done using a SF-12 Health survey questionnaire and a SNOT questionnaire. Both the objective and subjective analysis was done before and after the practice of Yogasanas. The compiled data was analyzed with the paired (2-tailed) T-Test, using SPSS (Software package for social sciences) version 16.
Results: The total nasal airway resistance was found to be increased before doing yoga and it was significantly reduced at 150 Pa pressure after doing yoga. The mean FEV1/FVC% before doing yoga was less when compared with the post yoga measurement. The mean Physical component score (PCS) and Mental component score (MCS) of the SF-12 health survey questionnaire had significantly improved and the mean SNOT questionnaire score had significantly reduced after the practice of yoga.
Keywords: Hatha yoga; Tobacco smokers; Allergic rhinitis; Rhino manometer; Spiro meter; SF-12 Health survey questionnaire; Snot questionnaire
Abbreviations: AR: Allergic Rhinitis; SF-12: Short Form 12 Health Survey Questionnaire; SNOT: Sino Nasal Outcome Test Questionnaire
Opinion
Allergic Rhinitis (AR) is the most common allergic disease, affecting 30% of population around the world. The disease is predominantly associated with exposure to some aeroallergens like cigarette smoking [1]. Allergic Rhinitis (AR) is usually defined as the presence of at least one or more of the symptoms of congestion, rhino rhea, sneezing, nasal itching, and nasal obstruc-tion [2,3]. The disease is an Immunoglobulin E (IgE) medi-ated reaction of Th2-type T cell response [4,5]. Due to the chronicity of disease and the variable response to therapy, a large number of patients resort to complimentary and alternate medication for Allergic rhinitis. Nasal breathing exercise is a simple and cost effective measure to reduce symptoms of Allergic Rhinitis and improve patient satisfaction [6].
Yoga is an alternative to traditional (Western) aerobic exercise that may have promise as a complementary treatment for smoking cessation. Yoga contains a number of components that contribute to stress reduction including asanas, yoga postures that have been shown to improve mood and well-being similar to the effects of traditional Western exercise, [7-10] and pranayama, breathing exercises that involve regulation of breath and conscious deep breathing that stimulates pulmonary stretch receptors similar to the deep in halation associated with smoking [11]. While yoga is associated with health benefits similar to exercise, the goal of yoga practice is also to create a calm state of mind through the combination of physical postures, breathing techniques, and directed meditative focus [12,13]. Several studies have shown that the practice of yoga reduces perceived stress and negative effect. Thus, the practice of yoga may also improve the chances of successful smoking cessation [14-17].
Yoga training can readjust the autonomic imbalance, controls the rate of breathing, and thus alters various physiological variables. These changes are attributed to the decreased sympathetic reactivity and relaxation of voluntary Inspiratory and expiratory muscles [18,19]. The proportion of adolescents with symptoms of asthma or allergic rhinitis who reported smoking experimentation is a cause for concern, because there is strong evidence that active smoking is a risk factor for the occurrence and increased severity of allergic diseases [20]. Passive and active smokings are both risk factors for asthma and allergic rhinitis in adolescents [21-23]. Cost effective options and alternative therapy such as yoga will serve as a solution to manage Allergic rhinitis. The ancient science of yoga includes physical postures, voluntarily regulated breathing, and meditation, among other techniques [24]. Practicing yoga can bring positive effects on well-being and human health with respect to biological and physiological parameters [25]. Voluntarily regulated yoga breathing techniques have been found to increase the oxygen consumption (and correspondingly the metabolic rate) both as an immediate effect [26,27] and as a longitudinal effect [26]. Certain yoga voluntarily regulated breathing techniques offer an opportunity to study the effects of changes in the respiratory pattern on metabolism [28]. Voluntary regulation of breathing in yoga alters autonomic activity with an improvement in cardiovascular and psychological health [29]. Nose is the main channel for the entry of air to the respiratory system, but this also exerts a resistance to the airflow. This nasal airflow resistance consists of half to 2/3rd of total airway resistance [30]. Nasal resistance is defined as resistance offered to the air entry by the nasal cavity [31]. This resistance is rather important as it prevents catastrophic collapse of lung [32]. Nasal airway resistance accounts for more than 50% of total airway resistance [33].The nasal cavity has been modeled as 2 resistors in parallel [34,35]. The 3 components of nasal resistance are as follows: the nasal vestibule, nasal valve, and nasal cavum [33].Information regarding nasal resistance is essential for management of anatomic and physiologic diseases of the na-sal airway. However, there are often inconsistencies between subjective nasal obstructive symptoms and the objective appear-ance of the nasal cavity [36]. Due to this discrepancy, objective diagnostic tools for the assessment of nasal patency or resistance are needed [37].The upper airway resistance can be measured with the help of a rhino manometer and lower airway resistance can be measured with a spiro meter. Anterior active rhino manometer is the most frequently used method in clinical practice according to the International Standardization Committee of Rhinomanometry, ICSR [38, 39]. The word rhinomanometry means 'rhino' for nose and 'manometer' for measurement of pressure [40]. Spirometry is a safe, practical and reproducible maximum breathing test that can be used in primary care to objectively determine the ventilatory capacity of the lungs. As already emphasised earlier in this article, it is the 'gold standard’ for detecting and quantifying airflow obstruction [41]. A spiro meter is a medical device that allows measurement of how much air is expelled and how quickly the lungs can be emptied, in a maximal expiration from full inflation [42]. The test is relatively quick to perform, well tolerated by most patients and the results are immediately available to clinician [43]. Sofar there has not been much studies done to check the efficiency of Hatha yogasanas on the airway resistances of tobacco smokers with allergic rhinitis. Hence Hatha yogasanas comprising of breathing exercises were taught to the recruited subjects in the study and effect of these asanas on the airway resistances of tobacco smokers with allergic rhinitis was studied.
Materials and Methods
This study was conducted at the Department of Otorhinolaryngology, St. John's national academy of health sciences, Bangalore. The study is a prospective non blinded study. 20 Tobacco smokers with Allergic rhinitis between the age group of 18-30, willing to practice yoga for a period of 90 days and with full compliance and reduce the number of cigarettes were recruited for the study. The Nasal resistance was measured at day0, that is before the start of practicing yoga and then after a period the 90 days. Written and informed consent was taken before the procedure. A thorough otorhinolaryngologicalexamination of all subjects was done prior to the study. The subjects were taught Hatha yogasanas by a trained yoga tutor. The following are the list of specific asanas which were taught
a) Tadasana (mountain pose)
b) Ardhachakrasana(Half-Wheel Posture )
c) Ardhakatichakrasana (Lateral arc posture)
d) Bhujangasana ( Cobra Pose )
e) Vrksasana ( Tree Pose )
f) Veerabadrasana(Warrior Pose)
g) Gomukasana ( Cow Face Pose )
h) Ustrasana ( Camel Pose )
i) Dhanurasana ( Bow Pose )
j) Surya Namaskara
k) Nadi Shodhana Pranayama ( Alternate Nostril Breathing Technique )
l) Bhastrika Pranayama ( The Bellows Breathing )
m) Bhramari Pranayama ( Humming Bee Breathing Technique )
n) Kapalabhati ( Hyperventilating Practice )
o) Jalaneti
The rhino manometer and spirometer was used to assess objectively the effect of Hatha yogasanas on the airway resistance. Regular calibration was ensured. The technique of the whole procedure was explained in full detail to all subjects. Series of trial recordings were performed with an intention that they were familiar with the technique and equipment thereby eliminating any anxiety which is a known factor for reducing nasal resistance. Rhinomanometry examination was performed during quiet breathing with close mouth in an upright sitting position and the following parameters were recorded [44].
Equipment used had following features:
1. During spontaneous respiration transnasal pressure differences and nasal air flow were recorded simultaneously.
2. Nasal air flow and pressure curve was displayed on a visual display unit (VDU) which allowed controlling the regularity of patients breathing.
3. Data obtained in the form of printed graph which contained nasal airflow and pressure-flow relation at 150mm Pa pressure [30].
Nasal resistance was kept static at 150 Pa because at this pressure difference both laminar and turbulent airflow were prevailed and nasal resistance can be assessed with minimal physical effort. Calculations of transnasal resistance were made according to Ohm's law. Nasal resistance to airflow was calculated by following equation
R = ∆P/V
R is total nasal airflow resistance in Pa/cm3/s,
∆P is 150 Pa pressure, V is nasal airflow (sum of left and right) during inspiration.
Total nasal airflow resistance reflects the resistance of both side of nasal cavity. The advantage of measuring the total nasal airflow resistance is to avoid the effect of nasal
Cycle over unilateral nasal airflow resistance as the nasal cycle may lead to a change of 4-fold in unilateral nasal airflow resistance [45]. The subjective analysis was done using the SF- 12 Health survey questionnaire and SNOT questionnaire.
Result
The Objective analysis parameters pre yoga and post yoga was found to be as follows, Total Nasal Airway Resistance in the 20 subjects was 0.44 Pa/cm3/s pre yoga and 0.39Pa/cm3/s post yoga at 150Pa with P<0.05. Pulmonary function test parameter FEV1/FVC% pre yoga was 66.12 and 79.51 post yoga with P<0.001***. . The subjective analysis parameters was found to be as follows, the Physical component score of the SF-12 health survey questionnaire was 38.62 pre yoga and 41.99 post yoga with P<0.05* and Mental component score of the SF-12 health survey questionnaire was 40.04 pre yoga 45.07 post yoga with P<0.01**, and the SNOT questionnaire score was 12.77 pre yoga and 10.05 post yoga P<0.001***.
Discussion
Allergic Rhinitis (AR) is defined as inflammation of the membranes lining the nose, and is characterized by nasal congestion, rhino rhea, sneezing, itching of the nose and/or post-nasal discharge [46]. It is often viewed, as a trivial disease but can significantly affect the quality of life (QOL) by causing fatigue, headache, sleep disturbances and cognitive impairment [47] Allergic Rhinitis is also closely related to asthma and, 10-40% of people with rhinitis have concomitant asthma [47]. According to WHO (2007), the global burden of allergic rhinitis was estimated to be 400 million [48] and the prevalence among adults ranges between 10% and 32% in Asia Pacific region [49]. Despite the high burden, there is paucity of community based studies in India, determining the burden and factors associated with allergic rhinitis. Medications provide some relief, but improvement is only partial. Anti-IgE shots show better efficacy, but are still very expensive [50].
Tobacco smoke exposure remains common and has been linked with an increased risk of multiple upper respiratory conditions in various age groups. Significant associations have been suggested between tobacco smoke exposure and chronic sinusitis [51], asthma [52] and allergic rhinitis [53]. In developing countries such diseases pose a serious socio economic burden. Cost effective options and alternative therapy such as yoga will serve as a solution to manage Allergic rhinitis. Pranayama is an integral part of Hatha yogasanas. As a deep breathing technique, pranayama reduces dead space ventilation and decreases work of breathing. It also refreshes the air throughout the lungs, in contrast with shallow breathing that refreshes the air only at the base of the lungs [54]. Regular practice of pranayama improves cardiovascular and respiratory functions, improves autonomic tone toward the parasympathetic system, decreases the effect of stress and strain on the body and improves physical and mental health [55-57]. Pulmonary function parameters (PFT) provide important clinical information to identify and quantify the defects and abnormalities in the functioning of the respiratory system. A study by Dinesh etal ,after 12 weeks of fast pranayama training FEV1 /FVC, PEFR, and FEF25-75 were significantly improved (P = 0.02, P< 0.001, and P< 0.001, respectively) compared with the values at baseline. Yadav and Das attributed that improvement in the PFT parameters by yogic practices due to increased respiratory muscle strength, clearing of respiratory secretions and using the diaphragmatic and abdominal muscles for filling the respiratory apparatus more efficiently and completely. Furthermore, the improvement in the PFT parameters may be due to rise in thoracic - pulmonary compliances and broncho dilatation by training in Nadisodhana pranayamas [58]. Stimulation of pulmonary stretch receptors by inflation of the lung reflexely relaxes smooth muscles of larynx and tracheo bronchial tree. Probably, this modulates the airway caliber and reduces airway resistance [59]. Previous investigators demonstrated the effect of pranayama on enhancement of the respiratory muscle efficiency and lung compliance due to reduction in elastic and viscous resistance of lung [60]. Furthermore, pranayama acts as stimulus for release of lung surfactant and prostaglandins into alveolar spaces, which increases the lung compliances [61]. Total nasal resistance gives an overall measure of nasal functions and also reflects the degree of nasal obstruction during breathing [45].
In our study Table 1 shows the Total Nasal Airway resistance in 20 subjects where in during preying it was 0.44 and post yoga it was 0.39 with the p value <0.05*. Graph 1 shows the decrease in total nasal airway resistance post yoga. Table 2 shows the Spiro metric measurements i.e, FEV1/FVC% during pre yoga it was 66.12 and post yoga it was 79.51 with the p value <0.001***. Graph 2 shows the significant improvement of the FEV1/FVC% parameter post yoga in the 20 subjects. Table 3 shows the SF- 12 Health survey components i.e the physical component score during pre yoga was 38.62 and post yoga was 41.99with the p value <0.05* and the mental component score during preying was 40.04 and post yoga was 45.07 with the p value <0.01**. Graph 3 shows the significant improvement in the physical and mental component scores post yoga. Table 4 shows the SNOT scores which was 12.77 during pre yoga and 10.05 post yoga with the p value 0.001***. Graph 4 shows the significant reduction in the SNOT score post yoga.
Conclusion
The study shows that there is decrease in the total nasal airway resistance and the FEV1/FVC% parameter also show significant improvement in 20 tobacco smokers with allergic rhinitis after the regular practice of yoga. The Quality of life of the subjects has been better as per the SNOT and SF 12 Questionnaire. There have been no scientific studies concerning the effect of yoga on the airway resistances of tobacco smokers with allergic rhinitis. Thus this study may form a basis for future studies focused on the effect of yoga on the tobacco smokers with allergic rhinitis.
For more articles in Journal of Yoga and Physiotherapy please click
on https://juniperpublishers.com/jyp/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/s
0 notes
Text
300+ TOP HEMATOLOGY Objective Questions and Answers
HEMATOLOGY Multiple Choice Questions :-
1. Causes spurious decrease in MCV
A. Cryofibrinogen
B. hyperglycemia
C. autoagglutination
D. high WBC ct
E. reduced red cell deformability
Ans: A
2. When the entire CBC is suppressed due to either anemia, infection, or hemorrhage is called?
A. Erythroplasia
B. Thrombocytopenia
C. Pancytopenia
D. Leukopenia
Ans: C
3. Total RBC count for Women is?
A. 4.4 -6
B. 4.2-5
C. 4.0-5.0
D. 4.2-5.2
Ans: C
4. Total RBC for men?
A. 4.0-5.0
B. 4.6-6.0
C. 4.2-6.5
D. 4.0-6.0
Ans: B
5. What is the major metabolically available storage form of iron in the body?
A. Hemosiderin
B. Ferritin
C. Transferrin
D. Hemoglobin
Ans: B
6. The best source of active bone marrow from a 20-year old would be:
A. Iliac Crest (hip)
B. Femur (thigh)
C. Distal radius (forearm)
D. Tibia (shin)
Ans: A
7. Laboratory Studies: Red Cell Indices: Determination of relative size of RBC. 82-98 fl
A. MCH
B. MCV
C. MCHC
Ans: B
8. Laboratory Studies: Red Cell Indices: Measurement of average weight of Hb/RBC. 27-33 pg
A. MCH
B. MCV
C. MCHC
Ans: B
9. Laboratory Studies: Red Cell Indices: Evaluation of RBC saturation with Hb. 32-36%
A. MCV
B. MCH
C. MCHC
Ans: C
10. There are 3 classifications of Anemia. What are they?
A. In adequate production of Hb
B. Decreased RBC production
C. Increased Erythrocyte destruction
D. Blood loss
Ans: A
HEMATOLOGY MCQs
11. Vitamin B12 and folic have the similar adverse effects, but what separates one form the other?
A. Glossitis
B. No neurological symptoms in folic acid
C. muscle wasting
D. Dizziness
Ans: B
12. Folic acid therapy can cause sickle cell anemia
A. True
B. False
Ans: B
14. Hydroxyurea increases hemoglobin production and decreases reticulocyte cells.
A. True
B. False
Ans: A
15. Hydroxyurea:
A. decreases nitric oxide
B. increases neutrophil and monocytes
C. inhibits DNA synthesis by acting as a ribonucleotide reductase inhibitor
Ans: C
16. Hydroxyurea increases the serum uric acid levels.
A. True
B. False
Ans: A
17. Decitabine increases the fetal hemoglobin production by inducing methylation of DNA and thus prevents the switch from gamma to beta-globin production.
A. True
B. False
Ans: B
18. Hypocupremia is seen in
A. osetoporosis, nephrotic disease
B. sprue, cliac disease
C. cardiovascular disease, colon cancer
D. A and B
E. B and C
F. All of the above
Ans: F
19. Wilsons disease can cause liver problems
A. True
B. False
Ans: A
20. What are the treatment options for wilson's disease?
A. Pencillamine
B. Riboflavin
C. Trientine
D. Potassium disulfide
E. Zinc
F. A, B and C
G. A, C, and D
H. A, C, D, and E
Ans: H
21. Aplasia can occur because of riboflavin deficiency?
A. True
B. False
Ans: A
22. Angular stomatitis.cheilosis is a symptom of vitamin B12 deficiency?
A. True
B. False
Ans: B
24. Which test can be used to detect hemolytic anemia?
A. Coombs test
B. Genetic testing
C. Peripheral blood smear (PBS)
D. Schilling test
Ans: A
25. Which anemia is classified as not being able to use iron properly to synthesize hemoglobin because of a inherited cause.
A. Iron deficiency anemia
B. hypochromic anemia
C. aplastic anemia
Ans: B
27. This fatal disorder results from clot/thrombus formation in the blood ciruclation
A. thromboembolism
B. DVT
C. PAD
D. Pulmonary embolism
E. All of the above
Ans: E
28. Homan's sign is classified as pain behind the knee
A. True
B. False
Ans: A
29. Patients that are sensitive to aspirin can take:
A. Sulfinpyrazone
B. Clopidogrel
C. Ticlopidine
D. 1 and 2
E. 2 and 3
Ans: E
30. What is the life span of RBC
A. 120
B. 100
C. 200
D. 80
Ans: A
34. Warfarin should be used with caution in the following:
A. Alcoholic liver disease
B. Gastrointestinal bleeding
C. recent neurosugery
D. Liver impairment
Ans: D
35. Isozymes of 2C can greatly effect warfarin
A. True
B. False
Ans: A
36. absolute lymphocytosis (>5000/mm^3) without adenopathy, hepatosplenomegaly, anemia, thrombocytopenia is what stage in CLL prognosis Scoring-Rai Staging System?
A. Stage 0
B. Stage I
C. Stage II
D. Stage III
E. Stage IV
Ans: A
37. Conventional treatment is ______ for Rai stage II
A. Antibiotics
B. chemotherapy
C. Antivirals
D. rest
Ans: B
38. In patients with low numbers of neoplastic cells, sometimes due to treatment, PCR to amplify DNA can improve sensitivity, and detect signs of relapse.
A. True
B. False
Ans: A
39. Chronic lymphocytic leukemia is most common leukemia in what kind of people? Slide 4
A. young adults
B. older adults
Ans: B
40. absolute lymphocytosis and thrombocytopenia( A. Stage 0
B. Stage I
C. Stage II
D. Stage III
E. Stage IV
Ans: E
HEMATOLOGY Objective type Questions with Answers
41. Chronic Lymphocytic Leukemia is characterized by peripheral blood and bone marrow _____.
A. lymphocytopenia
B. lymphocytosis
Ans: B
42. Chronic Lymphocytic Leukemia is characterized by gradual accumulation of small mature ______ cells.
A. T
B. B
C. NK
Ans: B
43. Which of the following is the most mature normoblast?
A. Orthochromic Normoblast
B. Basophilic Normoblast
C. Pronormoblast
D. Polychromatic Normoblast
Ans: A
44. absolute lymphocytosis with either hepatomegaly or splenomegaly with or without lymphadenopathy is what stage in CLL prognosis Scoring-Rai Staging System?
A. Stage 0
B. Stage I
C. Stage II
D. Stage III
E. Stage IV
Ans: C
45. absolute lymphocytosis without lymphadenopathy without hepatosplenomegaly, anemia, or thrombocytopenia is what stage in CLL prognosis Scoring-Rai Staging System?
A. Stage 0
B. Stage I
C. Stage II
D. Stage III
E. Stage IV
Ans: B
46. IN Chronic Lymphocytic Leukemia the Lymphocyte appearance: small or slightly larger than normal, hyper-condensed(almost ________ appearing. nuclear chromatin patter, bare nuclei called "smudge cells" are common. A. soccer-ball
B. basketball
C. football
D. tennis-ball
Ans: A
47. Which of the following forms of Hb molecule has the lowest affinity for oxygen?
A. Tense
B. Relaxed
C. Arterial
D. Venous
Ans: A
48. What is the recommended cleaner for removing all oil from objective lens?
A. 70 % alcohol or lens cleaner
B. Xylene
C. Water
D. Benzene
Ans: A
49. Intravascular hemolysis is the result of trauma to RBCs while in the circulation
A. True
B. False
Ans: A
50. A 1:20 dilution was made in a unopette, with glacial acetic acid as the diluent. The four corner squares on BOTH sides of the hemacytometer are counted for a total of 100 cells. What is the total WBC (x10^9/L.?
A. 0.25
B. 2.5
C. 5
D. 10
Ans: B
51. The shape of a cell is maintained by which of the following?
A. Microtubules
B. Spindle Fibers
C. Ribosomes
D. Centrioles
Ans: A
52. At which month of fetal development does the bone marrow become the primary site of hematopoiesis?
A. 2nd
B. 5th
C. End of 6th month
D. End of 7th month
Ans: C
53. Which types of cells develop from yolk sacs (Mesoblastic phase)?
A. Hb F, Hg A2, and Hg A
B. Gower 1 and Gower 2 Hgb
C. Portland Hgb
D. Only Erythroblasts
Ans: D
54. Normal Adult Hb A contains the following polypeptide chains:
A. alpha and beta
B. alpha and epsilon
C. alpha and delta
D. alpha and brotherton
Ans: A
55. Allergic reactions are frequently associated with an increase in the prescence of :
A. Lymphocytes
B. Neutrophils
C. Monocytes
D. Eosinophils
Ans: D
56. Lipid exchange between the RBC membrane and the plasma occurs:
A. To replace lost lipids in the membrane
B. To provide a mechanism for excretion of lipid-soluble RBC waste products
C. To ensure symmetry between the composition of the interior and exterior lipid layers
D. To provide lipid-soluble nutrients to the RBC
Ans: A
57. After the microscope has been adjusted for Kohler illumination, light intensity should never be regulated by using the...
A. Rheostat
B. Neutral density filter
C. Kohler magnifier
D. Condenser
Ans: D
58. Which of the followong types of microscopy is valuable in the identification of crystals that are able to rotate light?
A. Compound brightfield
B. Darkfield
C. Polarizing
D. Phase-contrast
Ans: C
59. During the Medullary Phase of hematopoietic development, which bone is the first to show hematopoietic activity?
A. Femur
B. Iliac Crest
C. Skull
D. Clavicle
Ans: D
60. Given the following values, calculate the RPI Observed reticulocyte count - 6% Hct- 30%
A. 2
B. 3
C. 4
D. 5
Ans: A
61. The lipids of the RBC membrane are arranged:
A. In chains beneath a protein exoskeleton
B. So that the hydrophobic portions are facing the plasma
C. In a hexagonal lattice
D. In two layers that are not symmetric in composition
Ans: D
62. The hexose monophosphate pathway activity increases the RBC source of
A. Glucose and lactic acid
B. 2,3-BPG and methemoglobin
C. NADPH and reduced glutathione
D. ATP and other purine metabolites
Ans: C
63. Which single feature of normal RBC's is most responsible for limiting their life span?
A. Loss of mitochondria
B. Increased flexibility of the cell membrane
C. Reduction of Hb iron
D. Loss of nucleus
Ans: D
64. In the Iron cycle, the transferrin receptor carries:
A. Iron out of duodenal cells from the intestinal lumen
B. Iron out of duodenal cells into the plasma
C. transferrin-bound iron in the plasma
D. transferrin-bound iron into erythrocytes
Ans: D
65. A multilineage cytokine among the ILs is:
A. IL-1
B. IL-2
C. IL-3
D. IL-4
Ans: A
66. Which of the following cells may develop in sites other than the bone marrow?
A. Monocyte
B. Lymphocyte
C. Megakaryocyte
D. Neutrophil
Ans: B
67. The acceptable range for hemoglobin values on a control sample is 13 + or - 0.4 g/dL. A hemoglobin determination is performed five times in succession on the same control sample. The results are (in g/dL. 12 12.3, 12, 12.2, and 12.1) These results are:
A. Precise, but not accurate
B. Both accurate and precise
C. Accurate, but not precise
D. Neither accurate nor precise
Ans: A
68. The layer of the erythrocyte membrane that is largely responsible for the shape, structure, and deformability of the cell is the:
A. Integral protein
B. Exterior lipid
C. Peripheral protein
D. Interior lipid
Ans: C
69. During midfetal life, the primary source of blood cells is the:
A. Bone marrow
B. Spleen
C. Lymph Nodes
D. Liver
Ans: D
70. In the bone marrow, RBC precursors are located:
A. In the center of the hematopoietic cords
B. Adjacent to megakaryocytes along the adventitial cell lining
C. Surrounding fat cells in apoptotic islands
D. Surrounding macrophages near the sinus membrane
Ans: D
71. Which of the following gathers, organizes, and directs light through the specimen?
A. Ocular
B. Objective lens
C. Condenser
D. Optical Tube
Ans: C
72. How are the globin chains genes arranged? Note: a means alpha, B means beta
A. With a genes and B genes on the same chromosome including two a genes and two B genes
B. With a genes and B genes on seperate chromosomes, two a genes on one chromosome and one B gene on a different chromosome
C. With a genes and B genes on the same chromosome - including four a genes and four B genes
D. With a genes and B genes on separate chromosomes - four a genes on one chromosome and two B genes on a different chromosome
Ans: B
73. The maximum number of erythrocytes generated by one Multipotential Stem Cell is:
A. 8
B. 1
C. 12
D. 16
Ans: D
74. What is the distribution of normal Hb in adults?
A. 80-90% Hb A, 5-10% Hb A2, 1-5% Hb F
B. >95% Hb A,
Read the full article
0 notes
Text
Hunting a Killer: Sex, Drugs and the Return of Syphilis
By Jan Hoffman, NY Times, Aug. 24, 2017
OKLAHOMA CITY--For months, health officials in this socially conservative state capital have been staggered by a fast-spreading outbreak of a disease that, for nearly two decades, was considered all but extinguished.
Syphilis, the deadly sexually transmitted infection that can lead to blindness, paralysis and dementia, is returning here and around the country, another consequence of the heroin and methamphetamine epidemics, as users trade sex for drugs.
To locate possible patients and draw their blood for testing, Oklahoma’s syphilis detectives have been knocking on doors in dilapidated apartment complexes and dingy motels, driving down lonely rural roads and interviewing prison inmates. Syphilis has led them to members of 17 gangs; to drug dealers; to prostitutes, pimps and johns; and to their spouses and lovers, all caught in the disease’s undertow.
“Syphilis doesn’t sleep for anyone,” said Portia King, a veteran Oklahoma state health investigator. “We have 200 open cases of sex partners we’re looking for. And the spread is migrating out of the city.”
It took months for investigators to realize Oklahoma City had a syphilis outbreak. Last fall, the juvenile detention center reported three cases--a boy and two girls, the youngest, 14. The center had never had a syphilis case in seven years of testing for it.
Investigators were mystified: The teenagers did not know each other, live in the same neighborhood or attend the same school.
Then, in February, a prison inmate tested positive. In interviews, he listed 24 sex partners--some his own, others the so-called pass-around girls for gangs, usually in exchange for heroin or methamphetamine. Contact information from the Entertainment Manager, as he called himself, pointed the way to a syphilis spread that, by March, led health officials to declare an outbreak, one of the largest in the country.
Although syphilis still mostly afflicts gay and bisexual men who are African-American or Hispanic, in Oklahoma and nationwide, rates are rising among white women and their infants. Nearly five times as many babies across the country are born with syphilis as with H.I.V.
Syphilis is devilishly difficult to contain, but may be even more so now. Because most doctors haven’t seen a case since the late 1990s, they often misdiagnose it. The cumbersome two-step lab test is antiquated. Although syphilis can be cured with an injection, there has been a shortage of the antibiotic, made only by Pfizer, for over a year.
And funding for clinics dedicated to preventing sexually transmitted diseases is down. In 2012, half of state programs that address sexually transmitted infections experienced reductions; funding has largely stayed flat since then. The Trump administration has proposed a 17 percent cut to the federal prevention budget.
Nearly 24,000 cases of early-stage syphilis, when the disease is most contagious, were reported in the United States in 2015, the most recent data. That was a 19 percent rise over the previous year. The total for 2015, including those with later-stage disease, was nearly 75,000, according to the Centers for Disease Control and Prevention.
The way to shut down an outbreak is to locate all the sex partners of people who are infected and persuade them to get tested, treated and disclose other partners. That task has fallen on a handful of the health department’s disease intervention specialists.
This most recent wave of infections, spread through gang networks and prostitution rings, has made their jobs not only difficult but also dangerous.
Erinn Williams, the lead field investigator for the Oklahoma City outbreak, drove slowly down a one-lane gravel road curtained by overgrowth and bristling with barbed wire and “No Trespassing” signs.
Ms. Williams, 39, life-seasoned by an Alaska upbringing, Air Force training and two small daughters, usually makes these visits alone. She keeps her baby’s car seat in the back, to allay suspicions that she may be an undercover police officer.
“What you do is your business,” she tells the wary. “I’m here because I care about your health.”
She is accustomed to stopping by houses with locks punched out; to being warned off by drug dealers; to wearing comfortable shoes, the better to run away in.
She pulled up to a clearing. Across a ragged lawn, she could see a battered blue trailer surrounded by pickup trucks and a stand of trees. Access was blocked by an iron fence, monitored by video cameras.
Ms. Williams pushed a call button. “Hi, I’m here from the health department. Can I talk to you? I have some news.”
A young woman hesitantly crossed the grass. For months she had avoided health workers. Once, an investigator spotted her slipping in through a side entrance to her mother’s house; at the front door, the mother denied that her daughter was there.
Fresh-faced, her blonde hair in a ponytail, the woman looked healthier than most people Ms. Williams visits, with their grayish skin, abscesses and mottled veins.
Ms. Williams was gentle but direct: “Your blood test results came back. It’s positive for syphilis.”
The woman buried her face in her hands. “I’m so embarrassed,” she sobbed. (Bound by confidentiality rules, Ms. Williams did not disclose her name.)
“Is that why my baby died?” she asked.
Ms. Williams nodded affirmatively.
“Can my kid get it? We sometimes share the same glass.”
No, Ms. Williams said. Just your sexual partners.
The woman insisted she had slept with only two men that year--her boyfriend and her ex, the father of the baby who had died.
Ms. Williams, who knew the woman’s Facebook page revealed many friends in a gang central to the outbreak, asked her to think carefully about whether there were more. We never reveal your name, she said, just as we cannot tell you who gave us yours.
The woman shook her head.
It was time to coax the woman into treatment. Just an injection and you will almost certainly be cured, Ms. Williams said, offering to drive her to the clinic. Her boyfriend too, Ms. Williams added.
He wasn’t around, the woman said, but she promised they would be there in the morning.
Are you sure you don’t want to go now? Ms. Williams asked.
Again, the woman shook her head.
Reluctantly, Ms. Williams got in her car and drove away.
Syphilis, caused by bacteria, has been well known for centuries, chronicled as a scourge since at least the 1400s.
In 1932, the United States government began the ignominious “Tuskegee Study of Untreated Syphilis in the Negro Male” to observe the progress of the disease in black Alabama sharecroppers. Although penicillin had become accepted as the cure by 1945, Tuskegee researchers left the men untreated until 1972, when the study was shut down.
By then, largely because of treatment and public education, syphilis was disappearing. A generation of physicians rarely learned to recognize it firsthand.
But with the AIDS epidemic, syphilis surged, peaking around 1990. It was most common--and still is--among men who had sex with men, often those whose H.I.V. status made them vulnerable to other sexually transmitted infections.
Once again, public health campaigns sent syphilis into retreat. By 2000, only 5,970 cases were reported in the United States, the lowest since 1941, when reporting became mandatory.
But in the last few years, it has crept back.
Here in Oklahoma City, 199 cases have been connected so far this year. More than half the patients are white and female. The youngest girl is 14; the oldest man, 61. Three stillbirths have been attributed to syphilis and 13 of the infected were pregnant women.
Rare permutations are now more common. Ocular syphilis, which can strike at any stage of infection, often appears as blurred vision and reddened eyes. Congenital syphilis can cause deformed bones in newborns.
Many people never suspect they have the disease. Early symptoms, including genital lesions and, later, rashes on palms and soles, have led patients and health care providers to mistake it for herpes or allergic reactions. The disease can lie dormant for decades and then affect the liver, joints, blood vessels.
Once people are treated, though cured, they will almost always test positive. It is difficult to know whether a positive result indicates a new infection. After transmission, the bacteria may take three months to register. Those who test negative may have the disease.
The cure for syphilis--usually two injections of Bicillin L-A, a type of penicillin--is relatively simple. But supplies have dwindled. Recently in Oklahoma, there were only seven doses statewide. Pfizer announced that stockpiles would be replenished by the end of 2017.
After several months, dispirited Oklahoma investigators acknowledged that old-school tactics for locating contacts, like knocking on doors and cold-calling, were not very effective. Many people they sought are transient and use disposable phones.
“But they want to stay connected to their friends and their drugs,” said Ms. King, a supervising investigator. “So they’re all on Facebook. That’s where we’re finding them.”
Through Facebook, investigators memorize faces and gang tattoos, and follow the flare-ups and flameouts of relationships. As gang members and dealers post partying plans, the sleuths determine where to point their investigation. They send potential patients messages through Facebook.
Ms. Williams’s team realized they were tracking a spread that reached back to last summer, involved members and associates of 17 gangs, and had infected young people from stable backgrounds who had used prescription opioids, then heroin. Patients often had symptoms that were a signature of this outbreak: weeping genital warts, called condylomata lata; patchy hair loss; and mucosal oozes inside the mouth.
The office created a chart of the outbreak, coded with symbols. Diamond: drug user. Blue heart: pregnant. Strawberry: prostitute.
They have come to understand why more than half of this outbreak’s victims are women: “The men give up the women’s names,” Ms. King said. “But the women are too loyal or afraid to give up the men. “
But recently investigators persuaded a gang leader to text members, ordering them to contact Ms. Williams.
Every day, the team checks arrest reports for people they are seeking. Chloe Hickman interviews inmates. Wearing glasses and no makeup, inclined toward modest cardigans, she doesn’t come across as someone who chats up gang members about their sex lives.
“I don’t cuss in my real life,” she said. “But in the jail, I flirt. I wear tight pants, a low-cut top and I use the F-word.
“Most of them don’t know what syphilis is. When I say it’s curable, they relax. And they’ll give me names.”
Usually such efforts lead to sagas of unrelenting grimness: mothers who prostitute daughters, and men who forcibly inject runaways with drugs to hook them, a practice known as guerrilla pimping.
Acquaintances of the investigators often dismiss their work as disgusting. For support, the women call each other daily, to laugh and vent.
Ms. Williams, on the job for eight years, said it gets to her, but she cannot let it go. “I remind myself that I’m not trying to fix all their problems,” she said. “Just one.”
By 10 o’clock the next morning, Ms. Williams had arranged to pick up one person for treatment, been stood up by another and was texting with a man who refused her offer of a blood draw, claiming that needles made him anxious. She had driven a woman to the clinic, after waiting outside her house as, apparently, the woman was getting high on meth.
Now at the clinic, the woman seemed to have fled. Ms. Williams and nurses ran through hallways, looking for her.
One victory: The woman from the trailer was in the waiting room. But she was alone. In the parking lot, her boyfriend sat out the appointment in his pickup truck, motor idling. He would not come inside for treatment.
He would almost certainly reinfect his girlfriend. And Ms. Williams would have to persuade her to be tested and treated, yet again.
2 notes
·
View notes
Text
Virgil Hunter relives moment he cheated death… but now is preparing Amir Khan for his title fight
The sun glistened over this famous bay when one of the best boxing trainers finally broke his silence about how his
In his relief to be able to see another blinding light, Virgil Hunter spoke for the first time about the return of the virtual dead to prepare Amir Khan April 20 is going to be a memorable night for Khan in the legendary Madison Square Garden in New York, but formidable as that task will be, Khan knows that cannot compare to challenge the brilliant Terence Crawford for the world welterweight title. with the struggle of his mentor for his existence.
<img id = "i-e096afe37c2b5276" src = "https://ift.tt/2OC9Ret image-a-1_1554138931414.jpg "height =" 422 "width =" 634 "alt =" <img id = "i-e096afe37c2b5276" src = "https://ift.tt/2OCv8EB /01/18/11729744-6874137-image-a-1_1554138931414.jpg "height =" 422 "width =" 634 "alt =" Trainer Virgil Hunter (left) relives the moment he cheated death to recover to coach Amir Khan (left) relives the moment he conquered death to recover to coach Amir Khan "
Trainer Virgil Hunter (left) relives the moment he cheated death to recovering coach Amir Khan
Miraculously, the only word that describes Hunter & # 39; s recovery from a deep coma followed by an awakening in which he found that he no longer knew how to walk.
None of the family gathered anxiously o far the silent figure in his hospital bed last March expected see him in the ring this week with Khan & # 39; s quick punches on the pads.
The alarming irony was that this predicament was caused by prescription medication
<img id = "i-f8dab476cfc144fe" src = "https://ift.tt/2FPwjho" height = "424" width = "634" alt = "Hunter fell into a deep coma last year after the bad reaction to prescribed medication
Hunter fell into a deep coma last year after a bad reaction to prescribed medication
heard it is frightening: & # 39; I was arguing with Andre Dirrell in New York, but my back bothered me and I asked my doctor to help, he gave me deca, a steroid used by bodybuilders to control insulin levels The allergic reaction was terrible.
& # 39; After two days the back pain went away, but I couldn't stop hicking and then I started feeling weak, tired and excessively thirsty. By the time we arrived in New York, I felt so bad that I couldn't go to the meetings, the weight, anything.
& # 39; If it happened next time, it would have been very bad. I had emitted the do not disturb sign, no one would have been beating or standing up until after checking out the next day. That would have been too late. Man, what if I had fainted then. & # 39;
Fortunately, Hunter came home to California. He records the story: & # 39; I just came through the front door. I threw my bags on the mat and crawled into bed. I vaguely remember that I woke up the next morning and made a nutritional drink. I felt very disoriented. Nothing but
& # 39; My wife told me she was out of work to check if my pickup car had arrived. No answer. She called twice more. No answer. She hurried home from work and found myself collapsing on the stairs.
& # 39; She warned the hospital, but by the time they had brought me there, my kidneys were closed and I had a heart attack. & # 39;
While other organs were in crisis, Hunter stayed in that coma for more than two weeks.
<img id = "i-a544b61b57e26c01" src = "https://ift.tt/2OGvk5R -6874137-image-m-13_1554140855599.jpg "height =" 628 "width =" 634 "alt ="
<img id = "i-a544b61b57e26c01" src = "https: //i.dailymail.co.uk/1s/2019/04/01/18/11730856-6874137-image-m-13_1554140855599.jpg "height =" 628 "width =" 634 "alt =" Hunter has been training Khan since 2012 and prepares him for 2012 <img id = "i-a544b61b57e26c01" src = "https://ift.tt/2FPtHzQ. jpg "height =" 628 "width =" 634 "alt =" <img id = "i-a544b61b57e26c01" src = "https://ift.tt/2OGvk5R -6874137-image-m-13_1554140855599.jpg "height =" 628 "width =" 634 "alt =" Hunter has been training Khan since 2012 and preparing him for his upcoming fight in New York
He says: & # 39; People think you don't hear anything in a coma. It's not true. I could hear everyone talking to me. My children. My family. André was there too. I knew exactly who everyone was …
& # 39; But I couldn't respond. I felt at peace and just drifted away. But when I came to you, everything seemed strange. I thought I was in France. & # 39;
& # 39; A therapist with a walker came to my bed & he said. & # 39; I asked what is that? & # 39; I discovered when I tried to get up. I couldn't stand it. I didn't know how to walk and my mind had to be taught to tell my legs how to work again. & # 39;
The following months were tough. Hunter remembers: & # 39; There were days when I felt like giving up. Thinking of the gym gave me courage and I was grateful that my time had not come. I thank the Lord for giving my wife the insight to realize that something was wrong that morning. & # 39;
The doctors warned him that it would take at least a year before he could work full-time again, but he was spurred on to see Khan boxing on television, although he won a few intermediate matches against inferior opponents.
The game against Crawford was announced and Hunter says: & I kept pushing and pushing. Determined to be back for him. & # 39;
<img id = "i-36b21603241b83b5" src = "https://ift.tt/2OC9Six -6874137-image-a-9_1554140809590.jpg "height =" 439 "width =" 634 "alt ="
Khan looks at Terence Crawford (L) for welterweight title at Madison Square Garden on April 20 <img id = "i -36b21603241b83b5 "src =" https://ift.tt/2FQuNvt "height =" 439 "width =" 634 " alt = "Khan faces Terence Crawford (L) for welterweight title at Madison Square Garden on April 20" <img id = "i-36b21603241b83b5" src = "https://ift.tt/2W3ngi6 /04/01/18/11730912-6874137-image-a-9_1554140809590.jpg "height =" 439 "width =" 634 "alt =" <img id = "i-36b21603241b83b5" src = "https: // i. dailymail.co.uk/1s/2019/04/01/18/11730912-6874137-image-a-9_1554140809590.jpg "height =" 439 "width =" 634 "alt =" <img id = "i-36b21603241b83b5" src = "https://ift.tt/2OBv1sW 54140809590.jpg "height =" 439 "width =" 634 "alt =" Khan faces Terence Crawford (L) for welterweight title at Madison Square Garden on April 20
Khan thanks another good American trainer , Joe Goossen, because he helped him through those fights.
After enduring his fight in Hunter's gymnasium
After enduring his fight in Hunter & # 39; s gym of champions, Khan said: & # 39; great to have Virgil back. I told Joe that our appointment would not be permanent and that he was fine. Virgil is perfect for me. & # 39;
Hunter, tall and fully upright, eleven still like a mite, smiled at his British attack and said: & physically now, at age 65, I feel that I can do this for another five years to do. The path work and such. Because I always said that I would not retire until I was 75 years old, I am looking for a young student who will take on the hard work at the right time.
& # 39; But this has made me realize that your mortality is always at hand. Once you are at the top of the mountain, you have to look down. & # 39;
Khan climbs his third world title at 32 and still climbs his Everest staff. By the grace of God with Sherpa Virgil by his side.
Amir Khan challenges undefeated Terence Crawford to the WBO World welterweight belt, live at BT Sport Box Office, Saturday, April 20. For more information go to
Source link
0 notes
Text
Grandmother suffers allergic reaction to LIP GLOSS
http://tinyurl.com/kc7k95y - Princess Wax Spa Salon
This is a stylish and glamorous game for the girls to get rid of extra hair by doing wax in this game. Now you...
Owner of salon fined for paying stylist too little
A SALON owner has hit out after the Government said her business had “exploited” a lowpaid worker.
Grandmother suffers allergic reaction to LIP GLOSS
&t is unsafe but it does mean that anyone who has reacted to a product and knows which ingredient caused that reaction must avoid the same ingredient in any other cosmetic product as well. &ting ...Distraught gran, 62, looked &IPGLOSSExpress.co.ukChristian Dior lipgloss left gran &vening NewsChristian Dior lip gloss left gran &es »
#39;This does not mean the produc#39;This can be checked by consul#39;like a monster' after allergic reaction to L#39;looking like a monster' after severe ...Manchester E#39;Mirror.co.ukall 6 news articl
0 notes
Text
Grandmother suffers allergic reaction to LIP GLOSS
http://tinyurl.com/pbvcxyq - Princess Wax Spa Salon
This is a stylish and glamorous game for the girls to get rid of extra hair by doing wax in this game. Now you...
Owner of salon fined for paying stylist too little
A SALON owner has hit out after the Government said her business had “exploited” a lowpaid worker.
Grandmother suffers allergic reaction to LIP GLOSS
&t is unsafe but it does mean that anyone who has reacted to a product and knows which ingredient caused that reaction must avoid the same ingredient in any other cosmetic product as well. &ting ...Distraught gran, 62, looked &IPGLOSSExpress.co.ukChristian Dior lipgloss left gran &vening NewsChristian Dior lip gloss left gran &es »
#39;This does not mean the produc#39;This can be checked by consul#39;like a monster' after allergic reaction to L#39;looking like a monster' after severe ...Manchester E#39;Mirror.co.ukall 6 news articl
0 notes
Text
Pneumocandin B0 CAS#: 135575-42-7
IdentificationPhysical DataSpectraRoute of Synthesis (ROS)Safety and HazardsOther Data
Identification
Product NamePneumocandin B0IUPAC NameN--6--11,20,21,25-tetrahydroxy-15--2,5,8,14,17,23-hexaoxo-1,4,7,13,16,22-hexazatricycloheptacosan-18-yl]-10,12-dimethyltetradecanamide Molecular Structure
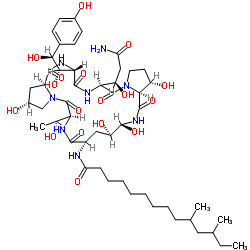
CAS Registry Number 135575-42-7EINECS NumberNo data availableMDL NumberNo data availableBeilstein Registry NumberNo data availableSynonymspneumocandin B0,
pneumocandin Bo,
pneumocandin B,
pneumocandin B0,
L-688,
786
CAS 135575-42-7
CAS: 135575-42-7
CAS No.: 135575-42-7 Molecular FormulaC50H80N8O17 Molecular Weight1065.2136 SMILES CCC(C)CC(C)CCCCCCCCC(=O)N1C((NC(=O)2(CCN2C(=O)(NC(=O)(NC(=O)3C(CN3C(=O)(NC1=O)(C)O)O)((c4ccc(cc4)O)O)O)(CC(=O)N)O)O)O)O InChIInChI=1S/C50H80N8O17/c1-5-25(2)20-26(3)12-10-8-6-7-9-11-13-37(66)52-31-22-35(64)46(71)56-48(73)41-33(62)18-19-57(41)50(75)39(34(63)23-36(51)65)54-47(72)40(43(68)42(67)28-14-16-29(60)17-15-28)55-45(70)32-21-30(61)24-58(32)49(74)38(27(4)59)53-44(31)69/h14-17,25-27,30-35,38-43,46,59-64,67-68,71H,5-13,18-24H2,1-4H3,(H2,51,65)(H,52,66)(H,53,69)(H,54,72)(H,55,70)(H,56,73)/t25?,26?,27-,30-,31+,32+,33+,34-,35-,38+,39+,40+,41+,42+,43+,46-/m1/s1 InChI KeyDQXPFAADCTZLNL-ZESADUFFSA-N Canonical SMILESCCC(C)CC(C)CCCCCCCCC(=O)NC1CC(C(NC(=O)C2C(CCN2C(=O)C(NC(=O)C(NC(=O)C3CC(CN3C(=O)C(NC1=O)C(C)O)O)C(C(C4=CC=C(C=C4)O)O)O)C(CC(=O)N)O)O)O)O
Patent InformationPatent IDTitlePublication DateUS2014/58082 INTERMEDIATE FOR SYNTHESIZING CASPOFUNGIN AND PREPARATION METHOD THEREOF 2014
Physical Data
AppearanceOff white powder SolubilityNo data availableBoiling point1442.9±65.0 °C(Predicted) Flash PointNo data available Refractive indexNo data available SensitivityNo data available
Description (Association (MCS))Solvent (Association (MCS))Temperature (Association (MCS)), °CPartner (Association (MCS))Stability constant of the complex with ...CCl424.94-FluorophenolStability constant of the complex with ... aq. HNO325AgNO3Enthalpy of associationacetonitrile25iodineNMR spectrum of the complexCDCl3Cu(2,4-dichloro-benzoate)2
Spectra
Description (NMR Spectroscopy)Nucleus (NMR Spectroscopy)Solvents (NMR Spectroscopy)Comment (NMR Spectroscopy) Chemical shifts1Htetradeuteriomethanol Chemical shifts13Ctetradeuteriomethanol Spin-spin coupling constants tetradeuteriomethanol 1H-1H.
Description (UV/VIS Spectroscopy)Solvent (UV/VIS Spectroscopy)Absorption Maxima (UV/VIS), nmExt./Abs. Coefficient, l·mol-1cm-1Absorption maximamethanol 27615
Route of Synthesis (ROS)
Route-of-Synthesis-ROS-of-Pneumocandin-B0-CAS-135575-42-7
ConditionsYieldWith trifluoroacetic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;
Experimental Procedure
Under nitrogen gas protection, acetonitrile (100 ml), the compound of formula (2) (5.0 g), phenylboronic acid (0.90 g) and 3-mercaptophenol (1.80 g) were uniformly stirred and the temperature was raised to -50 to -45°C And trifluoroacetic acid (1.05 ml) was added dropwise. After the dropwise addition, the mixture was reacted at -50 to -45°C for about 2.5 hours. After confirming the completion of the reaction by TLC monitoring, the reaction was stopped and an aqueous solution of NaOAc (1.15 g NaOAc dissolved in 25 ml of water) was added slowly, and the temperature was raised to 20 ° C and stirred for 2 hours. A large amount of solid was precipitated, the temperature was lowered to 0 ° C or lower, and the filtrate was subjected to third washing with 60 ml of acetonitrile / water = 9: 1 (V / V), followed by vacuum drying for 5 hours, 3b (4.65 g, yield 93%). 93%With trifluorormethanesulfonic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;0.27
Safety and Hazards
Pictogram(s)




SignalDangerGHS Hazard StatementsH315 (92.31%): Causes skin irritation
H317 (15.38%): May cause an allergic skin reaction
H318 (92.31%): Causes serious eye damage
H334 (15.38%): May cause allergy or asthma symptoms or breathing difficulties if inhaled
H335 (15.38%): May cause respiratory irritation
H400 (92.31%): Very toxic to aquatic life
Information may vary between notifications depending on impurities, additives, and other factors. Precautionary Statement CodesP261, P264, P271, P272, P273, P280, P285, P302+P352, P304+P340, P304+P341, P305+P351+P338, P310, P312, P321, P332+P313, P333+P313, P342+P311, P362, P363, P391, P403+P233, P405, and P501
(The corresponding statement to each P-code can be found at the GHS Classification page.)
Other Data
TransportationNot dangerous goodsUnder the room temperature and away from lightHS Code294200StorageUnder the room temperature and away from lightShelf Life1 yearMarket PriceUSD
DruglikenessLipinski rules componentMolecular Weight1065.23 logP3.701 HBA24 HBD15 Matching Lipinski Rules1Veber rules componentPolar Surface Area (PSA)411.28 Rotatable Bond (RotB)21Matching Veber Rules0
BioactivityIn vitro: EfficacyQuantitative Results
pXParameterValue (qual)Value (quant)UnitBiological Species TargetBioassayEffect7.25MFC (minimum fungicidal concentration)(Antifungal activity) =0.06µg/mL Candida tropicalis 7.15IC50 70nM In Vitro (others) antifungal agent 7.15 IC50 =0.07µMCandida albicans Inhibitor 7.15IC50(Beta-(1,3)-D-glucan synthesis) =70nM Candida albicans MY1208 Inhibitor6.95MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.12µg/mL Candida tropicalis MY1012 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans MY1208 6.63MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.5μg/ml Candida albicans MY1055 6.03MFC (minimum fungicidal concentration)=1μg/mlKluyveromyces marxianus MY2099 5.73MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =2µg/mL Candida parapsilosis MY1010 5.42MFC (minimum fungicidal concentration)(Antifungal activity) =4µg/mL Candida parapsilosis4.69IC50 20.23 µM In Vitro (others)3.92MIC 128 mg/L In Vitro (others) fungistatic agent ZI (zone of inhibition) 8mmIn Vitro (others) fungistatic agent MED99.9(Reduction (99.9%) of viable CFUs recoverable from mouse kidneys infected with Candida albicans (MY1208)) =6mg/kgmouse
Quantitative Results1 of 9Effectfungistatic agent Biological material Aspergillus fumigatus Assay Description Bioassay : 35 deg C; potato dextrose agar 16 clinical strains (MF5668, CLY315, CLY522, CLY523 among them); in vitro; agar dilution diffusion method (Acar, J.F. 1986. Disk susceptibility test, p. 27-63. In V. Lorian (ed.) Antibiotics in laboratory medicine); 1.2E5 CFU/ml inoculum Results critical concentration, CC 0.03 - 0.05 mg/l 2 of 9 Effect Hemolytic Assay Description Target : CD-1 mouse whole blood
Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 3.13 mg/l 3 of 9Effect Hemolytic Biological material human Assay Description Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 25 mg/l 4 of 9Effect antifungal agent Assay Description Target : Candida albicans MY1055
Bioassay : time-killing assay Results time-kill curve; fungicide 5 of 9Results glucan synthesis inhibition in a Candida albicans membrane assay: IC50 = 0.07 μM 6 of 9Effect fungistatic agent Assay Description Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; agar diffusion assay; potato dextrose agar; 1E6 conidia/petri dish inoculum; 30 deg C; zone of inhibition measured Results critical conc. 7 of 9Effect fungistatic agent Assay DescriptionEffect : eye observable change in morphology
Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; broth microdilution assay; Yeast Nitrogen Base with 2 percent glucose; 1E4 condidia/well inoculum; 30 deg C Resultsmin. effective conc., MEC 0.5 mg/l 8 of 9EffectAntifungal activity against Candida albicans, Candida tropicalis, Candida parapsilosis, Candida pseudotropicalis 9 of 9Results TOKA ED99.9 = 6 mg/kg
Toxicity/Safety PharmacologyQuantitative Results
pXParameterValue (quant)UnitBiological Species Bioassay Effect7.58MFC90 0.25mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 7.28MFC90 0.5mg/L Candida tropicalis Cell/tumor cell: proliferation/viability/growth antifungal agent 6.95MFC (minimum fungicidal concentration) 0.12 - 0.5mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 6.68MFC90 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.63MFC (minimum fungicidal concentration) 0.25 - 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.33MFC (minimum fungicidal concentration) 0.5 - 64 mg/LCryptococcus neoformansCell/tumor cell: proliferation/viability/growthantifungal agent 6.03MFC50 1mg/L Kluyveromyces marxianus Cell/tumor cell: proliferation/viability/growth antifungal agent 5.73MFC50 2mg/L Pichia kudriavzevii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.42MFC (minimum fungicidal concentration) 4-128mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.18MFC9064mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.12MFC (minimum fungicidal concentration) 8mg/L Clavispora lusitaniae Cell/tumor cell: proliferation/viability/growth antifungal agent 4.88MIC90 128mg/L Aspergillus niger Cell/tumor cell: proliferation/viability/growth antifungal agent 3.92MIC 128mg/L Aspergillus flavus Cell/tumor cell: proliferation/viability/growth antifungal agent
Use PatternPneumocandin B0 CAS 135575-42-7 is starting material for production of antifungal cyclohexapeptide compounds. Pneumocandin B0 CAS 135575-42-7 is used as the pharmaceutical intermediates of the Caspofungin which is a lyophilized preparation.
Read the full article
0 notes
Text
Pneumocandin B0 CAS#: 135575-42-7
IdentificationPhysical DataSpectraRoute of Synthesis (ROS)Safety and HazardsOther Data
Identification
Product NamePneumocandin B0IUPAC NameN--6--11,20,21,25-tetrahydroxy-15--2,5,8,14,17,23-hexaoxo-1,4,7,13,16,22-hexazatricycloheptacosan-18-yl]-10,12-dimethyltetradecanamide Molecular Structure
CAS Registry Number 135575-42-7EINECS NumberNo data availableMDL NumberNo data availableBeilstein Registry NumberNo data availableSynonymspneumocandin B0,
pneumocandin Bo,
pneumocandin B,
pneumocandin B0,
L-688,
786
CAS 135575-42-7
CAS: 135575-42-7
CAS No.: 135575-42-7 Molecular FormulaC50H80N8O17 Molecular Weight1065.2136 SMILES CCC(C)CC(C)CCCCCCCCC(=O)N1C((NC(=O)2(CCN2C(=O)(NC(=O)(NC(=O)3C(CN3C(=O)(NC1=O)(C)O)O)((c4ccc(cc4)O)O)O)(CC(=O)N)O)O)O)O InChIInChI=1S/C50H80N8O17/c1-5-25(2)20-26(3)12-10-8-6-7-9-11-13-37(66)52-31-22-35(64)46(71)56-48(73)41-33(62)18-19-57(41)50(75)39(34(63)23-36(51)65)54-47(72)40(43(68)42(67)28-14-16-29(60)17-15-28)55-45(70)32-21-30(61)24-58(32)49(74)38(27(4)59)53-44(31)69/h14-17,25-27,30-35,38-43,46,59-64,67-68,71H,5-13,18-24H2,1-4H3,(H2,51,65)(H,52,66)(H,53,69)(H,54,72)(H,55,70)(H,56,73)/t25?,26?,27-,30-,31+,32+,33+,34-,35-,38+,39+,40+,41+,42+,43+,46-/m1/s1 InChI KeyDQXPFAADCTZLNL-ZESADUFFSA-N Canonical SMILESCCC(C)CC(C)CCCCCCCCC(=O)NC1CC(C(NC(=O)C2C(CCN2C(=O)C(NC(=O)C(NC(=O)C3CC(CN3C(=O)C(NC1=O)C(C)O)O)C(C(C4=CC=C(C=C4)O)O)O)C(CC(=O)N)O)O)O)O
Patent InformationPatent IDTitlePublication DateUS2014/58082 INTERMEDIATE FOR SYNTHESIZING CASPOFUNGIN AND PREPARATION METHOD THEREOF 2014
Physical Data
AppearanceOff white powder SolubilityNo data availableBoiling point1442.9±65.0 °C(Predicted) Flash PointNo data available Refractive indexNo data available SensitivityNo data available
Description (Association (MCS))Solvent (Association (MCS))Temperature (Association (MCS)), °CPartner (Association (MCS))Stability constant of the complex with ...CCl424.94-FluorophenolStability constant of the complex with ... aq. HNO325AgNO3Enthalpy of associationacetonitrile25iodineNMR spectrum of the complexCDCl3Cu(2,4-dichloro-benzoate)2
Spectra
Description (NMR Spectroscopy)Nucleus (NMR Spectroscopy)Solvents (NMR Spectroscopy)Comment (NMR Spectroscopy) Chemical shifts1Htetradeuteriomethanol Chemical shifts13Ctetradeuteriomethanol Spin-spin coupling constants tetradeuteriomethanol 1H-1H.
Description (UV/VIS Spectroscopy)Solvent (UV/VIS Spectroscopy)Absorption Maxima (UV/VIS), nmExt./Abs. Coefficient, l·mol-1cm-1Absorption maximamethanol 27615
Route of Synthesis (ROS)
Route-of-Synthesis-ROS-of-Pneumocandin-B0-CAS-135575-42-7
ConditionsYieldWith trifluoroacetic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;
Experimental Procedure
Under nitrogen gas protection, acetonitrile (100 ml), the compound of formula (2) (5.0 g), phenylboronic acid (0.90 g) and 3-mercaptophenol (1.80 g) were uniformly stirred and the temperature was raised to -50 to -45°C And trifluoroacetic acid (1.05 ml) was added dropwise. After the dropwise addition, the mixture was reacted at -50 to -45°C for about 2.5 hours. After confirming the completion of the reaction by TLC monitoring, the reaction was stopped and an aqueous solution of NaOAc (1.15 g NaOAc dissolved in 25 ml of water) was added slowly, and the temperature was raised to 20 ° C and stirred for 2 hours. A large amount of solid was precipitated, the temperature was lowered to 0 ° C or lower, and the filtrate was subjected to third washing with 60 ml of acetonitrile / water = 9: 1 (V / V), followed by vacuum drying for 5 hours, 3b (4.65 g, yield 93%). 93%With trifluorormethanesulfonic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;0.27
Safety and Hazards
Pictogram(s)




SignalDangerGHS Hazard StatementsH315 (92.31%): Causes skin irritation
H317 (15.38%): May cause an allergic skin reaction
H318 (92.31%): Causes serious eye damage
H334 (15.38%): May cause allergy or asthma symptoms or breathing difficulties if inhaled
H335 (15.38%): May cause respiratory irritation
H400 (92.31%): Very toxic to aquatic life
Information may vary between notifications depending on impurities, additives, and other factors. Precautionary Statement CodesP261, P264, P271, P272, P273, P280, P285, P302+P352, P304+P340, P304+P341, P305+P351+P338, P310, P312, P321, P332+P313, P333+P313, P342+P311, P362, P363, P391, P403+P233, P405, and P501
(The corresponding statement to each P-code can be found at the GHS Classification page.)
Other Data
TransportationNot dangerous goodsUnder the room temperature and away from lightHS Code294200StorageUnder the room temperature and away from lightShelf Life1 yearMarket PriceUSD
DruglikenessLipinski rules componentMolecular Weight1065.23 logP3.701 HBA24 HBD15 Matching Lipinski Rules1Veber rules componentPolar Surface Area (PSA)411.28 Rotatable Bond (RotB)21Matching Veber Rules0
BioactivityIn vitro: EfficacyQuantitative Results
pXParameterValue (qual)Value (quant)UnitBiological Species TargetBioassayEffect7.25MFC (minimum fungicidal concentration)(Antifungal activity) =0.06µg/mL Candida tropicalis 7.15IC50 70nM In Vitro (others) antifungal agent 7.15 IC50 =0.07µMCandida albicans Inhibitor 7.15IC50(Beta-(1,3)-D-glucan synthesis) =70nM Candida albicans MY1208 Inhibitor6.95MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.12µg/mL Candida tropicalis MY1012 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans MY1208 6.63MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.5μg/ml Candida albicans MY1055 6.03MFC (minimum fungicidal concentration)=1μg/mlKluyveromyces marxianus MY2099 5.73MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =2µg/mL Candida parapsilosis MY1010 5.42MFC (minimum fungicidal concentration)(Antifungal activity) =4µg/mL Candida parapsilosis4.69IC50 20.23 µM In Vitro (others)3.92MIC 128 mg/L In Vitro (others) fungistatic agent ZI (zone of inhibition) 8mmIn Vitro (others) fungistatic agent MED99.9(Reduction (99.9%) of viable CFUs recoverable from mouse kidneys infected with Candida albicans (MY1208)) =6mg/kgmouse
Quantitative Results1 of 9Effectfungistatic agent Biological material Aspergillus fumigatus Assay Description Bioassay : 35 deg C; potato dextrose agar 16 clinical strains (MF5668, CLY315, CLY522, CLY523 among them); in vitro; agar dilution diffusion method (Acar, J.F. 1986. Disk susceptibility test, p. 27-63. In V. Lorian (ed.) Antibiotics in laboratory medicine); 1.2E5 CFU/ml inoculum Results critical concentration, CC 0.03 - 0.05 mg/l 2 of 9 Effect Hemolytic Assay Description Target : CD-1 mouse whole blood
Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 3.13 mg/l 3 of 9Effect Hemolytic Biological material human Assay Description Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 25 mg/l 4 of 9Effect antifungal agent Assay Description Target : Candida albicans MY1055
Bioassay : time-killing assay Results time-kill curve; fungicide 5 of 9Results glucan synthesis inhibition in a Candida albicans membrane assay: IC50 = 0.07 μM 6 of 9Effect fungistatic agent Assay Description Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; agar diffusion assay; potato dextrose agar; 1E6 conidia/petri dish inoculum; 30 deg C; zone of inhibition measured Results critical conc. 7 of 9Effect fungistatic agent Assay DescriptionEffect : eye observable change in morphology
Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; broth microdilution assay; Yeast Nitrogen Base with 2 percent glucose; 1E4 condidia/well inoculum; 30 deg C Resultsmin. effective conc., MEC 0.5 mg/l 8 of 9EffectAntifungal activity against Candida albicans, Candida tropicalis, Candida parapsilosis, Candida pseudotropicalis 9 of 9Results TOKA ED99.9 = 6 mg/kg
Toxicity/Safety PharmacologyQuantitative Results
pXParameterValue (quant)UnitBiological Species Bioassay Effect7.58MFC90 0.25mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 7.28MFC90 0.5mg/L Candida tropicalis Cell/tumor cell: proliferation/viability/growth antifungal agent 6.95MFC (minimum fungicidal concentration) 0.12 - 0.5mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 6.68MFC90 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.63MFC (minimum fungicidal concentration) 0.25 - 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.33MFC (minimum fungicidal concentration) 0.5 - 64 mg/LCryptococcus neoformansCell/tumor cell: proliferation/viability/growthantifungal agent 6.03MFC50 1mg/L Kluyveromyces marxianus Cell/tumor cell: proliferation/viability/growth antifungal agent 5.73MFC50 2mg/L Pichia kudriavzevii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.42MFC (minimum fungicidal concentration) 4-128mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.18MFC9064mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.12MFC (minimum fungicidal concentration) 8mg/L Clavispora lusitaniae Cell/tumor cell: proliferation/viability/growth antifungal agent 4.88MIC90 128mg/L Aspergillus niger Cell/tumor cell: proliferation/viability/growth antifungal agent 3.92MIC 128mg/L Aspergillus flavus Cell/tumor cell: proliferation/viability/growth antifungal agent
Use PatternPneumocandin B0 CAS 135575-42-7 is starting material for production of antifungal cyclohexapeptide compounds
Read the full article
0 notes
Text
Pneumocandin B0 CAS#: 135575-42-7
IdentificationPhysical DataSpectraRoute of Synthesis (ROS)Safety and HazardsOther Data
Identification
Product NamePneumocandin B0IUPAC NameN--6--11,20,21,25-tetrahydroxy-15--2,5,8,14,17,23-hexaoxo-1,4,7,13,16,22-hexazatricycloheptacosan-18-yl]-10,12-dimethyltetradecanamide Molecular Structure
CAS Registry Number 135575-42-7EINECS NumberNo data availableMDL NumberNo data availableBeilstein Registry NumberNo data availableSynonymspneumocandin B0,
pneumocandin Bo,
pneumocandin B,
pneumocandin B0,
L-688,
786
CAS 135575-42-7
CAS: 135575-42-7
CAS No.: 135575-42-7 Molecular FormulaC50H80N8O17 Molecular Weight1065.2136 SMILES CCC(C)CC(C)CCCCCCCCC(=O)N1C((NC(=O)2(CCN2C(=O)(NC(=O)(NC(=O)3C(CN3C(=O)(NC1=O)(C)O)O)((c4ccc(cc4)O)O)O)(CC(=O)N)O)O)O)O InChIInChI=1S/C50H80N8O17/c1-5-25(2)20-26(3)12-10-8-6-7-9-11-13-37(66)52-31-22-35(64)46(71)56-48(73)41-33(62)18-19-57(41)50(75)39(34(63)23-36(51)65)54-47(72)40(43(68)42(67)28-14-16-29(60)17-15-28)55-45(70)32-21-30(61)24-58(32)49(74)38(27(4)59)53-44(31)69/h14-17,25-27,30-35,38-43,46,59-64,67-68,71H,5-13,18-24H2,1-4H3,(H2,51,65)(H,52,66)(H,53,69)(H,54,72)(H,55,70)(H,56,73)/t25?,26?,27-,30-,31+,32+,33+,34-,35-,38+,39+,40+,41+,42+,43+,46-/m1/s1 InChI KeyDQXPFAADCTZLNL-ZESADUFFSA-N Canonical SMILESCCC(C)CC(C)CCCCCCCCC(=O)NC1CC(C(NC(=O)C2C(CCN2C(=O)C(NC(=O)C(NC(=O)C3CC(CN3C(=O)C(NC1=O)C(C)O)O)C(C(C4=CC=C(C=C4)O)O)O)C(CC(=O)N)O)O)O)O
Patent InformationPatent IDTitlePublication DateUS2014/58082 INTERMEDIATE FOR SYNTHESIZING CASPOFUNGIN AND PREPARATION METHOD THEREOF 2014
Physical Data
AppearanceOff white powder SolubilityNo data availableBoiling point1442.9±65.0 °C(Predicted) Flash PointNo data available Refractive indexNo data available SensitivityNo data available
Description (Association (MCS))Solvent (Association (MCS))Temperature (Association (MCS)), °CPartner (Association (MCS))Stability constant of the complex with ...CCl424.94-FluorophenolStability constant of the complex with ... aq. HNO325AgNO3Enthalpy of associationacetonitrile25iodineNMR spectrum of the complexCDCl3Cu(2,4-dichloro-benzoate)2
Spectra
Description (NMR Spectroscopy)Nucleus (NMR Spectroscopy)Solvents (NMR Spectroscopy)Comment (NMR Spectroscopy) Chemical shifts1Htetradeuteriomethanol Chemical shifts13Ctetradeuteriomethanol Spin-spin coupling constants tetradeuteriomethanol 1H-1H.
Description (UV/VIS Spectroscopy)Solvent (UV/VIS Spectroscopy)Absorption Maxima (UV/VIS), nmExt./Abs. Coefficient, l·mol-1cm-1Absorption maximamethanol 27615
Route of Synthesis (ROS)
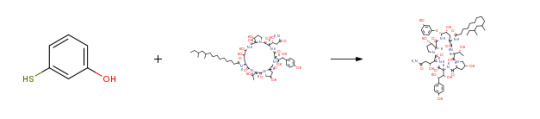
Route-of-Synthesis-ROS-of-Pneumocandin-B0-CAS-135575-42-7
ConditionsYieldWith trifluoroacetic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;
Experimental Procedure
Under nitrogen gas protection, acetonitrile (100 ml), the compound of formula (2) (5.0 g), phenylboronic acid (0.90 g) and 3-mercaptophenol (1.80 g) were uniformly stirred and the temperature was raised to -50 to -45°C And trifluoroacetic acid (1.05 ml) was added dropwise. After the dropwise addition, the mixture was reacted at -50 to -45°C for about 2.5 hours. After confirming the completion of the reaction by TLC monitoring, the reaction was stopped and an aqueous solution of NaOAc (1.15 g NaOAc dissolved in 25 ml of water) was added slowly, and the temperature was raised to 20 ° C and stirred for 2 hours. A large amount of solid was precipitated, the temperature was lowered to 0 ° C or lower, and the filtrate was subjected to third washing with 60 ml of acetonitrile / water = 9: 1 (V / V), followed by vacuum drying for 5 hours, 3b (4.65 g, yield 93%). 93%With trifluorormethanesulfonic acid; phenylboronic acid In acetonitrile at -50 - -45℃; for 2.5h; Inert atmosphere;0.27
Safety and Hazards
Pictogram(s)




SignalDangerGHS Hazard StatementsH315 (92.31%): Causes skin irritation
H317 (15.38%): May cause an allergic skin reaction
H318 (92.31%): Causes serious eye damage
H334 (15.38%): May cause allergy or asthma symptoms or breathing difficulties if inhaled
H335 (15.38%): May cause respiratory irritation
H400 (92.31%): Very toxic to aquatic life
Information may vary between notifications depending on impurities, additives, and other factors. Precautionary Statement CodesP261, P264, P271, P272, P273, P280, P285, P302+P352, P304+P340, P304+P341, P305+P351+P338, P310, P312, P321, P332+P313, P333+P313, P342+P311, P362, P363, P391, P403+P233, P405, and P501
(The corresponding statement to each P-code can be found at the GHS Classification page.)
Other Data
TransportationNot dangerous goodsUnder the room temperature and away from lightHS Code294200StorageUnder the room temperature and away from lightShelf Life1 yearMarket PriceUSD
DruglikenessLipinski rules componentMolecular Weight1065.23 logP3.701 HBA24 HBD15 Matching Lipinski Rules1Veber rules componentPolar Surface Area (PSA)411.28 Rotatable Bond (RotB)21Matching Veber Rules0
BioactivityIn vitro: EfficacyQuantitative Results
pXParameterValue (qual)Value (quant)UnitBiological Species TargetBioassayEffect7.25MFC (minimum fungicidal concentration)(Antifungal activity) =0.06µg/mL Candida tropicalis 7.15IC50 70nM In Vitro (others) antifungal agent 7.15 IC50 =0.07µMCandida albicans Inhibitor 7.15IC50(Beta-(1,3)-D-glucan synthesis) =70nM Candida albicans MY1208 Inhibitor6.95MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.12µg/mL Candida tropicalis MY1012 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans 6.63MFC (minimum fungicidal concentration) =0.25μg/mlCandida albicans MY1208 6.63MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =0.5μg/ml Candida albicans MY1055 6.03MFC (minimum fungicidal concentration)=1μg/mlKluyveromyces marxianus MY2099 5.73MFC (minimum fungicidal concentration)(Minimum Inhibitory Concentration) =2µg/mL Candida parapsilosis MY1010 5.42MFC (minimum fungicidal concentration)(Antifungal activity) =4µg/mL Candida parapsilosis4.69IC50 20.23 µM In Vitro (others)3.92MIC 128 mg/L In Vitro (others) fungistatic agent ZI (zone of inhibition) 8mmIn Vitro (others) fungistatic agent MED99.9(Reduction (99.9%) of viable CFUs recoverable from mouse kidneys infected with Candida albicans (MY1208)) =6mg/kgmouse
Quantitative Results1 of 9Effectfungistatic agent Biological material Aspergillus fumigatus Assay Description Bioassay : 35 deg C; potato dextrose agar 16 clinical strains (MF5668, CLY315, CLY522, CLY523 among them); in vitro; agar dilution diffusion method (Acar, J.F. 1986. Disk susceptibility test, p. 27-63. In V. Lorian (ed.) Antibiotics in laboratory medicine); 1.2E5 CFU/ml inoculum Results critical concentration, CC 0.03 - 0.05 mg/l 2 of 9 Effect Hemolytic Assay Description Target : CD-1 mouse whole blood
Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 3.13 mg/l 3 of 9Effect Hemolytic Biological material human Assay Description Bioassay : unwashed erythrocyte hemolysis assay; room temperature Results MLC, minimum lytic concentration active 25 mg/l 4 of 9Effect antifungal agent Assay Description Target : Candida albicans MY1055
Bioassay : time-killing assay Results time-kill curve; fungicide 5 of 9Results glucan synthesis inhibition in a Candida albicans membrane assay: IC50 = 0.07 μM 6 of 9Effect fungistatic agent Assay Description Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; agar diffusion assay; potato dextrose agar; 1E6 conidia/petri dish inoculum; 30 deg C; zone of inhibition measured Results critical conc. 7 of 9Effect fungistatic agent Assay DescriptionEffect : eye observable change in morphology
Target : Aspergillus fumigatus H11-20
Bioassay : in vitro; broth microdilution assay; Yeast Nitrogen Base with 2 percent glucose; 1E4 condidia/well inoculum; 30 deg C Resultsmin. effective conc., MEC 0.5 mg/l 8 of 9EffectAntifungal activity against Candida albicans, Candida tropicalis, Candida parapsilosis, Candida pseudotropicalis 9 of 9Results TOKA ED99.9 = 6 mg/kg
Toxicity/Safety PharmacologyQuantitative Results
pXParameterValue (quant)UnitBiological Species Bioassay Effect7.58MFC90 0.25mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 7.28MFC90 0.5mg/L Candida tropicalis Cell/tumor cell: proliferation/viability/growth antifungal agent 6.95MFC (minimum fungicidal concentration) 0.12 - 0.5mg/L Candida albicans Cell/tumor cell: proliferation/viability/growth antifungal agent 6.68MFC90 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.63MFC (minimum fungicidal concentration) 0.25 - 2mg/L Candida glabrata Cell/tumor cell: proliferation/viability/growth antifungal agent 6.33MFC (minimum fungicidal concentration) 0.5 - 64 mg/LCryptococcus neoformansCell/tumor cell: proliferation/viability/growthantifungal agent 6.03MFC50 1mg/L Kluyveromyces marxianus Cell/tumor cell: proliferation/viability/growth antifungal agent 5.73MFC50 2mg/L Pichia kudriavzevii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.42MFC (minimum fungicidal concentration) 4-128mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.18MFC9064mg/L Meyerozyma guilliermondii Cell/tumor cell: proliferation/viability/growth antifungal agent 5.12MFC (minimum fungicidal concentration) 8mg/L Clavispora lusitaniae Cell/tumor cell: proliferation/viability/growth antifungal agent 4.88MIC90 128mg/L Aspergillus niger Cell/tumor cell: proliferation/viability/growth antifungal agent 3.92MIC 128mg/L Aspergillus flavus Cell/tumor cell: proliferation/viability/growth antifungal agent
Use PatternPneumocandin B0 CAS 135575-42-7 is starting material for production of antifungal cyclohexapeptide compounds
Read the full article
0 notes
Text
Hatha Yoga Effect on Airway Resistances of Tobacco Smokers with Allergic Rhinitis -Juniper Publishers
Juniper Publishers- Journal of Yoga and Physiotherapy

Abstract
Background: There have been limited studies on Hatha yoga training as a complementary therapy to manage the symptoms of Allergic Rhinitis and also to check the effect of yoga on airway resistances in tobacco smokers with Allergic Rhinitis.
Aim: The main Aim of the study was to check the effect of Hathayogasanas on the Airway resistances in tobacco smokers with allergic rhinitis.
Materials and Methods: This is a prospective non blinded study of 20Tobacco smokers with allergic rhinitis. In the age group of (18-30). The subjects chosen for the study underwent an ENT examination and Hatha yoga training was giving for a period of 90 days. The objective analysis for upper airway resistance and lower airway resistance was done using a Rhino manometer and Spiro meter. The subjective analysis was done using a SF-12 Health survey questionnaire and a SNOT questionnaire. Both the objective and subjective analysis was done before and after the practice of Yogasanas. The compiled data was analyzed with the paired (2-tailed) T-Test, using SPSS (Software package for social sciences) version 16.
Results: The total nasal airway resistance was found to be increased before doing yoga and it was significantly reduced at 150 Pa pressure after doing yoga. The mean FEV1/FVC% before doing yoga was less when compared with the post yoga measurement. The mean Physical component score (PCS) and Mental component score (MCS) of the SF-12 health survey questionnaire had significantly improved and the mean SNOT questionnaire score had significantly reduced after the practice of yoga.
Keywords: Hatha yoga; Tobacco smokers; Allergic rhinitis; Rhino manometer; Spiro meter; SF-12 Health survey questionnaire; Snot questionnaire
Abbreviations: AR: Allergic Rhinitis; SF-12: Short Form 12 Health Survey Questionnaire; SNOT: Sino Nasal Outcome Test Questionnaire
Opinion
Allergic Rhinitis (AR) is the most common allergic disease, affecting 30% of population around the world. The disease is predominantly associated with exposure to some aeroallergens like cigarette smoking [1]. Allergic Rhinitis (AR) is usually defined as the presence of at least one or more of the symptoms of congestion, rhino rhea, sneezing, nasal itching, and nasal obstruc-tion [2,3]. The disease is an Immunoglobulin E (IgE) medi-ated reaction of Th2-type T cell response [4,5]. Due to the chronicity of disease and the variable response to therapy, a large number of patients resort to complimentary and alternate medication for Allergic rhinitis. Nasal breathing exercise is a simple and cost effective measure to reduce symptoms of Allergic Rhinitis and improve patient satisfaction [6].
Yoga is an alternative to traditional (Western) aerobic exercise that may have promise as a complementary treatment for smoking cessation. Yoga contains a number of components that contribute to stress reduction including asanas, yoga postures that have been shown to improve mood and well-being similar to the effects of traditional Western exercise, [7-10] and pranayama, breathing exercises that involve regulation of breath and conscious deep breathing that stimulates pulmonary stretch receptors similar to the deep in halation associated with smoking [11]. While yoga is associated with health benefits similar to exercise, the goal of yoga practice is also to create a calm state of mind through the combination of physical postures, breathing techniques, and directed meditative focus [12,13]. Several studies have shown that the practice of yoga reduces perceived stress and negative effect. Thus, the practice of yoga may also improve the chances of successful smoking cessation [14-17].
Yoga training can readjust the autonomic imbalance, controls the rate of breathing, and thus alters various physiological variables. These changes are attributed to the decreased sympathetic reactivity and relaxation of voluntary Inspiratory and expiratory muscles [18,19]. The proportion of adolescents with symptoms of asthma or allergic rhinitis who reported smoking experimentation is a cause for concern, because there is strong evidence that active smoking is a risk factor for the occurrence and increased severity of allergic diseases [20]. Passive and active smokings are both risk factors for asthma and allergic rhinitis in adolescents [21-23]. Cost effective options and alternative therapy such as yoga will serve as a solution to manage Allergic rhinitis. The ancient science of yoga includes physical postures, voluntarily regulated breathing, and meditation, among other techniques [24]. Practicing yoga can bring positive effects on well-being and human health with respect to biological and physiological parameters [25]. Voluntarily regulated yoga breathing techniques have been found to increase the oxygen consumption (and correspondingly the metabolic rate) both as an immediate effect [26,27] and as a longitudinal effect [26]. Certain yoga voluntarily regulated breathing techniques offer an opportunity to study the effects of changes in the respiratory pattern on metabolism [28]. Voluntary regulation of breathing in yoga alters autonomic activity with an improvement in cardiovascular and psychological health [29]. Nose is the main channel for the entry of air to the respiratory system, but this also exerts a resistance to the airflow. This nasal airflow resistance consists of half to 2/3rd of total airway resistance [30]. Nasal resistance is defined as resistance offered to the air entry by the nasal cavity [31]. This resistance is rather important as it prevents catastrophic collapse of lung [32]. Nasal airway resistance accounts for more than 50% of total airway resistance [33].The nasal cavity has been modeled as 2 resistors in parallel [34,35]. The 3 components of nasal resistance are as follows: the nasal vestibule, nasal valve, and nasal cavum [33].Information regarding nasal resistance is essential for management of anatomic and physiologic diseases of the na-sal airway. However, there are often inconsistencies between subjective nasal obstructive symptoms and the objective appear-ance of the nasal cavity [36]. Due to this discrepancy, objective diagnostic tools for the assessment of nasal patency or resistance are needed [37].The upper airway resistance can be measured with the help of a rhino manometer and lower airway resistance can be measured with a spiro meter. Anterior active rhino manometer is the most frequently used method in clinical practice according to the International Standardization Committee of Rhinomanometry, ICSR [38, 39]. The word rhinomanometry means 'rhino' for nose and 'manometer' for measurement of pressure [40]. Spirometry is a safe, practical and reproducible maximum breathing test that can be used in primary care to objectively determine the ventilatory capacity of the lungs. As already emphasised earlier in this article, it is the 'gold standard’ for detecting and quantifying airflow obstruction [41]. A spiro meter is a medical device that allows measurement of how much air is expelled and how quickly the lungs can be emptied, in a maximal expiration from full inflation [42]. The test is relatively quick to perform, well tolerated by most patients and the results are immediately available to clinician [43]. Sofar there has not been much studies done to check the efficiency of Hatha yogasanas on the airway resistances of tobacco smokers with allergic rhinitis. Hence Hatha yogasanas comprising of breathing exercises were taught to the recruited subjects in the study and effect of these asanas on the airway resistances of tobacco smokers with allergic rhinitis was studied.
Materials and Methods
This study was conducted at the Department of Otorhinolaryngology, St. John's national academy of health sciences, Bangalore. The study is a prospective non blinded study. 20 Tobacco smokers with Allergic rhinitis between the age group of 18-30, willing to practice yoga for a period of 90 days and with full compliance and reduce the number of cigarettes were recruited for the study. The Nasal resistance was measured at day0, that is before the start of practicing yoga and then after a period the 90 days. Written and informed consent was taken before the procedure. A thorough otorhinolaryngologicalexamination of all subjects was done prior to the study. The subjects were taught Hatha yogasanas by a trained yoga tutor. The following are the list of specific asanas which were taught
a) Tadasana (mountain pose)
b) Ardhachakrasana(Half-Wheel Posture )
c) Ardhakatichakrasana (Lateral arc posture)
d) Bhujangasana ( Cobra Pose )
e) Vrksasana ( Tree Pose )
f) Veerabadrasana(Warrior Pose)
g) Gomukasana ( Cow Face Pose )
h) Ustrasana ( Camel Pose )
i) Dhanurasana ( Bow Pose )
j) Surya Namaskara
k) Nadi Shodhana Pranayama ( Alternate Nostril Breathing Technique )
l) Bhastrika Pranayama ( The Bellows Breathing )
m) Bhramari Pranayama ( Humming Bee Breathing Technique )
n) Kapalabhati ( Hyperventilating Practice )
o) Jalaneti
The rhino manometer and spirometer was used to assess objectively the effect of Hatha yogasanas on the airway resistance. Regular calibration was ensured. The technique of the whole procedure was explained in full detail to all subjects. Series of trial recordings were performed with an intention that they were familiar with the technique and equipment thereby eliminating any anxiety which is a known factor for reducing nasal resistance. Rhinomanometry examination was performed during quiet breathing with close mouth in an upright sitting position and the following parameters were recorded [44].
Equipment used had following features:
1. During spontaneous respiration transnasal pressure differences and nasal air flow were recorded simultaneously.
2. Nasal air flow and pressure curve was displayed on a visual display unit (VDU) which allowed controlling the regularity of patients breathing.
3. Data obtained in the form of printed graph which contained nasal airflow and pressure-flow relation at 150mm Pa pressure [30].
Nasal resistance was kept static at 150 Pa because at this pressure difference both laminar and turbulent airflow were prevailed and nasal resistance can be assessed with minimal physical effort. Calculations of transnasal resistance were made according to Ohm's law. Nasal resistance to airflow was calculated by following equation
R = ∆P/V
R is total nasal airflow resistance in Pa/cm3/s,
∆P is 150 Pa pressure, V is nasal airflow (sum of left and right) during inspiration.
Total nasal airflow resistance reflects the resistance of both side of nasal cavity. The advantage of measuring the total nasal airflow resistance is to avoid the effect of nasal
Cycle over unilateral nasal airflow resistance as the nasal cycle may lead to a change of 4-fold in unilateral nasal airflow resistance [45]. The subjective analysis was done using the SF- 12 Health survey questionnaire and SNOT questionnaire.
Result
The Objective analysis parameters pre yoga and post yoga was found to be as follows, Total Nasal Airway Resistance in the 20 subjects was 0.44 Pa/cm3/s pre yoga and 0.39Pa/cm3/s post yoga at 150Pa with P<0.05. Pulmonary function test parameter FEV1/FVC% pre yoga was 66.12 and 79.51 post yoga with P<0.001***. . The subjective analysis parameters was found to be as follows, the Physical component score of the SF-12 health survey questionnaire was 38.62 pre yoga and 41.99 post yoga with P<0.05* and Mental component score of the SF-12 health survey questionnaire was 40.04 pre yoga 45.07 post yoga with P<0.01**, and the SNOT questionnaire score was 12.77 pre yoga and 10.05 post yoga P<0.001***.
Discussion
Allergic Rhinitis (AR) is defined as inflammation of the membranes lining the nose, and is characterized by nasal congestion, rhino rhea, sneezing, itching of the nose and/or post-nasal discharge [46]. It is often viewed, as a trivial disease but can significantly affect the quality of life (QOL) by causing fatigue, headache, sleep disturbances and cognitive impairment [47] Allergic Rhinitis is also closely related to asthma and, 10-40% of people with rhinitis have concomitant asthma [47]. According to WHO (2007), the global burden of allergic rhinitis was estimated to be 400 million [48] and the prevalence among adults ranges between 10% and 32% in Asia Pacific region [49]. Despite the high burden, there is paucity of community based studies in India, determining the burden and factors associated with allergic rhinitis. Medications provide some relief, but improvement is only partial. Anti-IgE shots show better efficacy, but are still very expensive [50].
Tobacco smoke exposure remains common and has been linked with an increased risk of multiple upper respiratory conditions in various age groups. Significant associations have been suggested between tobacco smoke exposure and chronic sinusitis [51], asthma [52] and allergic rhinitis [53]. In developing countries such diseases pose a serious socio economic burden. Cost effective options and alternative therapy such as yoga will serve as a solution to manage Allergic rhinitis. Pranayama is an integral part of Hatha yogasanas. As a deep breathing technique, pranayama reduces dead space ventilation and decreases work of breathing. It also refreshes the air throughout the lungs, in contrast with shallow breathing that refreshes the air only at the base of the lungs [54]. Regular practice of pranayama improves cardiovascular and respiratory functions, improves autonomic tone toward the parasympathetic system, decreases the effect of stress and strain on the body and improves physical and mental health [55-57]. Pulmonary function parameters (PFT) provide important clinical information to identify and quantify the defects and abnormalities in the functioning of the respiratory system. A study by Dinesh etal ,after 12 weeks of fast pranayama training FEV1 /FVC, PEFR, and FEF25-75 were significantly improved (P = 0.02, P< 0.001, and P< 0.001, respectively) compared with the values at baseline. Yadav and Das attributed that improvement in the PFT parameters by yogic practices due to increased respiratory muscle strength, clearing of respiratory secretions and using the diaphragmatic and abdominal muscles for filling the respiratory apparatus more efficiently and completely. Furthermore, the improvement in the PFT parameters may be due to rise in thoracic - pulmonary compliances and broncho dilatation by training in Nadisodhana pranayamas [58]. Stimulation of pulmonary stretch receptors by inflation of the lung reflexely relaxes smooth muscles of larynx and tracheo bronchial tree. Probably, this modulates the airway caliber and reduces airway resistance [59]. Previous investigators demonstrated the effect of pranayama on enhancement of the respiratory muscle efficiency and lung compliance due to reduction in elastic and viscous resistance of lung [60]. Furthermore, pranayama acts as stimulus for release of lung surfactant and prostaglandins into alveolar spaces, which increases the lung compliances [61]. Total nasal resistance gives an overall measure of nasal functions and also reflects the degree of nasal obstruction during breathing [45].
In our study Table 1 shows the Total Nasal Airway resistance in 20 subjects where in during preying it was 0.44 and post yoga it was 0.39 with the p value <0.05*. Graph 1 shows the decrease in total nasal airway resistance post yoga. Table 2 shows the Spiro metric measurements i.e, FEV1/FVC% during pre yoga it was 66.12 and post yoga it was 79.51 with the p value <0.001***. Graph 2 shows the significant improvement of the FEV1/FVC% parameter post yoga in the 20 subjects. Table 3 shows the SF- 12 Health survey components i.e the physical component score during pre yoga was 38.62 and post yoga was 41.99with the p value <0.05* and the mental component score during preying was 40.04 and post yoga was 45.07 with the p value <0.01**. Graph 3 shows the significant improvement in the physical and mental component scores post yoga. Table 4 shows the SNOT scores which was 12.77 during pre yoga and 10.05 post yoga with the p value 0.001***. Graph 4 shows the significant reduction in the SNOT score post yoga.
Conclusion
The study shows that there is decrease in the total nasal airway resistance and the FEV1/FVC% parameter also show significant improvement in 20 tobacco smokers with allergic rhinitis after the regular practice of yoga. The Quality of life of the subjects has been better as per the SNOT and SF 12 Questionnaire. There have been no scientific studies concerning the effect of yoga on the airway resistances of tobacco smokers with allergic rhinitis. Thus this study may form a basis for future studies focused on the effect of yoga on the tobacco smokers with allergic rhinitis.
For more articles in Journal of Yoga and Physiotherapy please click
on https://juniperpublishers.com/jyp/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
0 notes
Last Seen Blogs

m-al98
M

aryabliss
Senza titolo

waymarkerprogenitor-blog
an ENDLESS waltz

hardly-used-intelligence
trash blog

mitzi-hunter
Mon Hun & More